methodology cross sectional study. study population: 130...
TRANSCRIPT
Methodology
Cross Sectional Study.
Study population:
Patients who are dyslipidemic (LDL-C 100 mg/dl diabetics and /or CAD patients, LDL-C
130 mg/dl others)will be recruited for the study. Patients will be recruited from Out Patient
Department (OPD) of Medicine, and Cardiology JIPMER.
Intervention:
Atorvastatin 10 and 40 mg for 6 weeks.
Methodology
Patients will be recruited from Out Patient Department (OPD) Department of Medicine, and
Cardiology JIPMER. Patients who are dyslipidemic will be recruited for the study and they will
be initiated on atorvastatin treatment based on their lipid levels for 6 weeks. At the end of 6
weeks their lipid profile will be assessed for lipid response and plasma will be collected for
assessment of drug and metabolite levels. The effect of genetic polymorphisms on the percentage
reduction in LDL-C level will be evaluated.
List of candidate genes to be studied:
1. HMGCR: Gene encoding for HMGCoA Reductase enzyme -a rate limiting enzyme in the
synthesis of cholesterol
2. CP7A1- Gene encoding for Cholesterol 7 alpha hydroxylase-a rate limiting enzyme in the
synthesis of bile acids. Bile acid is formed by the metabolism of cholesterol.
3. LDLR- Gene encoding for LDL- receptor on the surface of the hepatocytes.
4. MDR-1- Gene encoding for multi-drug resistance protein involved in the efflux of drugs.
5. APOE- Gene encoding for Apolipoprotein E which acts as a ligand for LDL receptor as well
as for transport of cholesterol.
6. CYP3A5- Gene encoding for CYP3A5 enzyme which metabolises Atorvastatin.
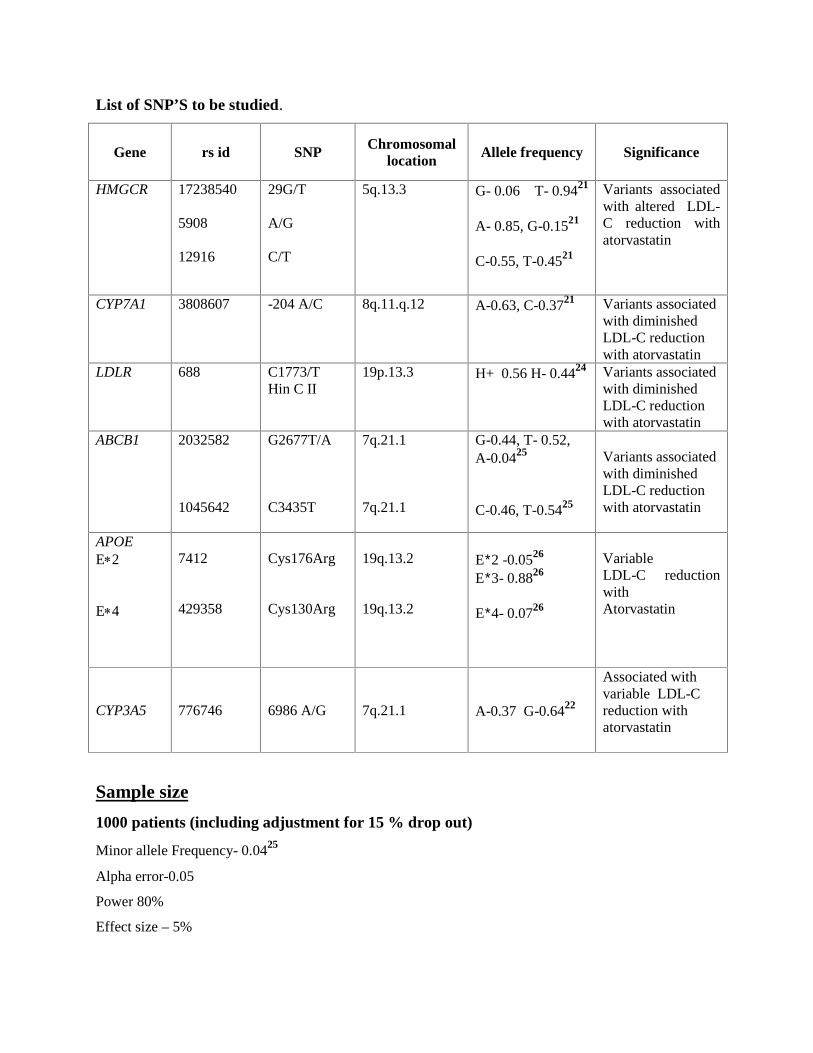
List of SNP’S to be studied.
Gene rs id SNP Chromosomallocation Allele frequency Significance
HMGCR 17238540
5908
12916
29G/T
A/G
C/T
5q.13.3 G- 0.06 T- 0.9421
A- 0.85, G-0.1521
C-0.55, T-0.4521
Variants associatedwith altered LDL-C reduction withatorvastatin
CYP7A1 3808607 -204 A/C 8q.11.q.12 A-0.63, C-0.3721 Variants associatedwith diminishedLDL-C reductionwith atorvastatin
LDLR 688 C1773/THin C II
19p.13.3 H+ 0.56 H- 0.4424 Variants associatedwith diminishedLDL-C reductionwith atorvastatin
ABCB1 2032582
1045642
G2677T/A
C3435T
7q.21.1
7q.21.1
G-0.44, T- 0.52,A-0.0425
C-0.46, T-0.5425
Variants associatedwith diminishedLDL-C reductionwith atorvastatin
APOEE2
E4
7412
429358
Cys176Arg
Cys130Arg
19q.13.2
19q.13.2
E2 -0.0526
E3- 0.8826
E4- 0.0726
VariableLDL-C reductionwithAtorvastatin
CYP3A5 776746 6986 A/G 7q.21.1 A-0.37 G-0.6422
Associated withvariable LDL-Creduction withatorvastatin
Sample size
1000 patients (including adjustment for 15 % drop out)
Minor allele Frequency- 0.0425
Alpha error-0.05
Power 80%
Effect size – 5%
Inclusion criteria
1. Newly diagnosed dyslipidemic patients
2. Patients of both gender aged 30- 65 yrs
3. Patients of Tamilian origin.(Those who are living in Tamilnadu/Puducherry for the past 3
generations and those whose mother tongue is Tamil)
Exclusion criteria
1. Patients with impaired liver or kidney function .
2. Patients receiving CYP3A4 inducers (Barbiturates, carbamazepine, glucocorticoids,
pioglitazone, phenytoin, rifampin).
3. Patients receiving CYP3A4 inhibitors (erythromycin, fluconazole, itraconazole,
ketoconazole, ritonavir, troleandomycin).
4. Pregnant and lactating women.
5. Patients on other lipid lowering agents
6. Patients with hypothyroidism.
7. Patients with LDL-C >250 mg/dl.
8. Triglycerides >400 mg/dl.
9. Patients who had/have a change in anti-diabetic drug/dose one month prior to the study and
during the study period.
Study Procedure
Clinical Evaluations:
Patients fulfilling the inclusion and exclusion criteria and volunteering to give informed consent
will be enrolled for the study. Informed written consent will be obtained from all subjects.
Patient characteristics namely age, sex, BMI, waist circumference, blood pressure and relevant
history will be obtained.
Blood collection and storage:
Initial visit- 7ml of fasting blood sample will be collected in an anticoagulant(EDTA) container
after an overnight fasting for 12-14 hrs and plasma and blood components will be separated and
stored at -80C until analysis of lipid profiles and genotyping. At the end of the study 5 ml of

venous blood will be collected after overnight fasting and 5ml after 2 hours of drug intake to
estimate the drug and metabolite levels.
Genotyping:
The genomic DNA will be isolated from whole blood using phenol-chloroform method.
Genotyping will be done by allelic discrimination assay in Real Time PCR using Taqman
Technology.
Chromatography:
The plasma levels of atorvastatin and its metabolites will be determined using Liquid
Chromatography/ Mass Spectroscopy. 27
Statistical analysis:
All the continuous study variables will be given as Mean± SD and paired t test will be used to
analyze pre & post lipid parameters and one way ANOVA will be carried out to analyze the data
between groups. Pearson’s chi square test was used for statistical comparisons between the
groups wild-type versus variants, CAD versus CAD-free, and comparison of percentage
reduction across genotypes. Chi square test will be used to see if the genotypes are in Hardy
Weinberg equilibrium.
Multivariate analysis using logistic regression analysis will be done for the data obtained to find
the association between the genotype and lipid levels and between other variables
Plasma levels of atorvastatin will be compared by C/D values (Concentration/Dose). Spearman
Rank Correlation will be used to analyze the relationship between genotype & atorvastatin
plasma level. P value less than 0.05 was considered to be significant.
Patient Data Sheet
Title of the study: Pharmacogenetics of lipid lowering response ofAtorvastatin among dyslipidemic Tamilian Population.
Date: Serial no:
Patient is enrolled from...Medicine/ Cardiology Out Patient Department, JIPMER, Pondicherry.
Name: Age: Sex:
Hospital no:
Address:
Phone no:
Religion: Caste: Sub-division
Baseline characteristics:
Height: Weight: BMI: kg/m2 Waist circumference: W/H ratio
Alcohol consumption : Never
Occasional
Regular
Smoking : Never 1-10 /day 11-20 /day > 20cig/day
Beedi/Cigarette
Duration of Smoking: _________ months/years
Tobacco Chewers : Yes / No
Dietary habits : Vegetarian / non-vegetarian (egg/fish/meat predominantly)
Occupation:
Educational status: Ill-literate/ literate
Monthly income:

Physical activity.
Level 1 Level 2 Level 3 Level 4Level 1 -Inactive lifestyle(Sitting most of the day and drive or ride wherever possible)
Level 2 –Moderately active lifestyle(sit most of the day ,but take occasional ,low intensity exercise)
Level 3- Active lifestyle(job requires physical labour and/or some amount of regular exercise 4- 5 times a week
Level 4- Very active lifestyle/athlete(job requires heavy physical labour or involved in a programme of intense
aerobic exercise of over 10 hours per week with a resting heartbeat of below 60 bpm)
Associated medical illness of the patient:
H/O Diabetes Mellitus - Yes No Duration
H/O Hypertension - Yes No Duration
H/O Angina/M.I Yes NoFamily history of Angina/M.I Yes No
History of chronic illness/other disease.
Investigations
Blood pressure: SBP DBPHeart rate
Lipid profileTime interval TC TG HDL-C LDL-C
Baseline
6wks
ECG Report
Coronary angiogram report
Month & Year of diagnosis of CAD:
Atorvastatin dose:
Concomitant medication
s.no Name of the drug Dose duration

Information about patient genotype status
Gene Rs id Genotype status
HMGCR 17238540
5908
12916
CYP7A1 3808607
LDLR 688
MDR1 2032582
1045642
APOE 7412
429358
CYP3A5 776746
Baseline diagnostic information:
LFT Baseline Post treatment
ALT
AST
RFT
BUN
Creatinine
FBS
Hb1ac
Creatine phosphokinase
TSH
Sample Code:
Adverse Reactions associated with Atorvastatin use:
Gastrointestinal disturbances
Headaches
Central nervous system disturbances
Sleep disorders
Myalgia,
Hepatotoxicity
Myopathy.
Rhabdomyolysis
1
Reference
1. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on
Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment
Panel III) Final Report. Circulation 2002;106:3143–21.
2. Keefe JHO, Carter MD, Lavie CJ. Primary and Secondary Prevention of Cardiovascular
Diseases: A Practical Evidence-Based Approach. Mayo Clinic Proceedings. 2009
Aug;84(8):741–57.
3. Grundy SM, Cleeman JI, Merz CN, Brewer HB , Clark LT, Hun-ninghake DB, Pasternak
RC, Smith SC Jr, Stone NJ. Implications of recent clinical trials for the National Cholesterol
Education Program Adult Treatment Panel III guidelines. Circulation.2004;110:227–39.
4. Waters DD, Brotons C, Chiang C-W, Ferrières J, Foody J, Jukema JW, et al. Lipid
Treatment Assessment Project 2. Circulation. 2009 ;120(1):28–34.
5. Kathiresan S, Melander O, Anevski D, Guiducci C, Burtt NP, Roos C, et al. Polymorphisms
Associated with Cholesterol and Risk of Cardiovascular Events. N Engl J Med.
2008;358(12):1240–9.
6. Shah SH. Genetics of LDL Cholesterol. emedicine.medscape.com/article/1783664-overview
7. Thompson JF, Man M, Johnson KJ, Wood LS, Lira ME, Lloyd DB,Banerjee P, Milos PM,
Myrand SP, Paulauskis J, Milad MA, Sasiela WJ. An association study of 43 SNPs in 16
candidate genes with atorvastatin response. Pharmacogenomics J. 2005;5: 352–8.
8. Lin Y, Mousa SS, Elshourbagy N, Mousa SA. Current status and future directions in lipid
management: emphasizing low-density lipoproteins, high-density lipoproteins, and
triglycerides as targets for therapy. Vasc Health Risk Manag. 2010;6:73–85.
9. Sanmukhani J, Shah V. Statins: Cost analysis in Indian scenario from eight major clinical
trials J Postgrad Med 2010;56:196-200.
10. Voora D, Shah SH, Reed CR, Zhai,J , Crosslin DR, Messer C, Salisbury BA , Ginsburg
GS. Pharmacogenetic Predictors of Statin-Mediated Low-Density Lipoprotein Cholesterol
Reduction and Dose Response. Circ Cardiovasc Genet 2008;1:100-106.
11. Mega JL, Morrow DA, Brown A, Christopher P. Cannon , Sabatine MJ. Identification of
Genetic Variants Associated With Response to Statin Therapy. Arterioscler Thromb Vasc
Biol 2009; 29;1310-15.
12. Thompson JF, Hyde CL, Wood LS, Paciga SA, Hinds DA, Cox DR, et al. Comprehensive
Whole-Genome and Candidate Gene Analysis for Response to Statin Therapy in the
Treating to New Targets (TNT) Cohort / Clinical Perspective. Circulation: Cardiovascular
Genetics. 2009 Apr 1;2(2):173 -81.
2
13. Hoenig MR, Kostner KM, Read SJ, Walker PJ, Atherton JJ. Implications of the obesity
epidemic for statin therapy: shifting cholesterol metabolism to a high synthesis and low
dietary absorption state. Endocr Metab Immune Disord Drug Targets. 2007 Sep;7(3):153-
66.
14. Chasman DI, Posada D, Subrahmanyan L, Cook NR, Stanton VP, Ridker PM.
Pharmacogenetic Study of Statin Therapy and Cholesterol Reduction. JAMA: The Journal
of the American Medical Association. 2004 Jun 16;291(23):2821 -27.
15. Chien K-L, Wang K-C, Chen Y-C, Chao C-L, Hsu H-C, Chen M-F, et al. Common
sequence variants in pharmacodynamic and pharmacokinetic pathway-related genes
conferring LDL cholesterol response to statins. Pharmacogenomics. 2010 Mar;11(3):309-17.
16. Poduri A, Khullar M, Bahl A, Sehrawat BS, Sharma Y, Talwar KK. Common variants of
HMGCR, CETP, APOAI, ABCB1, CYP3A4, and CYP7A1 genes as predictors of lipid-
lowering response to atorvastatin therapy. DNA Cell Biol. 2010 Oct;29(10):629-37.
17. Hutz MH, Fiegenbaum M. Impact of genetic polymorphisms on the efficacy of HMG-CoA
reductase inhibitors. Am J Cardiovasc Drugs. 2008;8(3):161-70.
18. Kivisto KT, Niemi M, Schaeffeler E, Pitkala K, Tilvis R, Fromm MF, et.al.,Lipid-lowering
response to statins is affected by CYP3A5 polymorphism. Pharmacogenetics 2004;14:523–
25.
19. Kajinami K, Takekoshi N, Brousseau ME, Ordovas JM, SchaeferEJ. Additive gene-gene
interaction between CYP7A1 and APOE as genetic determinants of LDL cholesterol-
lowering response to atorvastatin (abstract). J Am Coll Cardiol 2004; 43(Suppl A):505A.
20. Zhu H, Tucker HM, Grear KE, Simpson JF, Manning AK, Cupples LA, et al. A Common
Polymorphism Decreases Low-Density Lipoprotein Receptor Exon 12 Splicing Efficiency
and Associates with Increased Cholesterol. Hum Mol Genet. 2007 Jul 15;16(14):1765–72.
21. Poduri A, Khullar M, Bahl A, Sharma YP, Talwar KK. A combination of proatherogenic
single-nucleotide polymorphisms is associated with increased risk of coronary artery disease
and myocardial infarction in Asian Indians. DNA Cell Biol. 2009 Sep;28(9):451-60.
22. Krishnakumar D, Gurusamy U, Dhandapani K, Surendiran A, Baghel R, Kukreti R,
Gangadhar R, Prayaga U, Manjunath S, Adithan C. Genetic polymorphisms of drug-
metabolizing phase I enzymes CYP2E1, CYP2A6 and CYP3A5 in South Indian
population.Fundam Clin Pharmacol. 2011 Jan 25. [Epub ahead of print].
23. Harikrishnan S, Rajeev E , Tharakan JA, Titus T, Ajithkumar VK, Sivasankaran S,
Krishnamoorthy KM, NairK. Do we Achieve target lipid levels with statins in patients with
Coronary Artery Disease? KMJ August 2008; 2:5-9.
3
24. Salazar LA, Hirata MH, Giannini SD, Forti N, DiamenteJ, Issa JS, and Hirata RDC. Effects
of Ava II and Hinc II Polymorphisms at the LDL Receptor Gene on Serum Lipid Levels of
Brazilian Individuals With High Risk for Coronary Heart Disease. Journal of Clinical
Laboratory Analysis 1999; 13:251–8.
25. Umamaheswaran G, Krishnakumar D, Kayathiri D, Rajan D, Shewade DG, Steven AD et
al. Inter and intra ethnic differences in the distribution of the molecular variants of TPMT,
UGT1A1 and MDR1 genes in south Indian population. Mol Biol Rep. DOI:
10.1007/s11033-012-1456-8 [Epub ahead of print].
26. Padmaja N. Pharmacogenomics of Coronary Heart Disease in a South Indian
Population.Ph.D Thesis. Pondicherry University 2009.
27. Guillén D, Cofán F, Ros E, Millán O, Cofán M, Rimola A, et al. Determination of
atorvastatin and its metabolite ortho-hydroxyatorvastatin in human plasma by on-line anion-
exchange solid-phase extraction and liquid chromatography tandem mass spectrometry.
Analytical and Bioanalytical Chemistry. 2009 Jun 9;394(6):1687–96.