midterm operative results of midline lumbar interbody
TRANSCRIPT

Midterm operative results of midline lumbar
interbody fusion using cortical bone trajectory
screws for lumbar degenerative spondylolisthesis
T. Tsutsumimoto, M. Yui, H. Misawa
Spine Center, Yodakubo Hospital, Nagawa, Japan

Background
Midline lumbar interbody fusion (MIDLIF) using cortical bone trajectory (CBT)
screws is an alternative method to the traditional posterior lumbar fusion using
pedicle screws. Because CBT screw entry points are much closer to the midline
than traditional pedicle screw entry points, and the trajectory is directed from
inferomedial to superolateral, MIDLIF using CBT screws offers the ability to perform
the decompression and fusion through the same surgical window, with the
advantages of decreased approach-related morbidity. However, there is a paucity of
evidence demonstrating the midterm clinical effectiveness of this technique in
patients with lumbar degenerative spondylolisthesis (LDS).

Purpose
To evaluate the midterm operative results of the MIDLIF using CBT
screws in patients with LDS.

Patients
Mean age at surgery (range), y 57.9 (42–76)
Sex (female/male) 13/8
Level (L3-4/L4-5) 3/18
Follow-up period (range), y 3.2 (2–5)
Inclusion criteria
Patients with single-level LDS and same-level
stenosis, who underwent a single-level MIDLIF
using CBT screws
No previous lumbar surgery
22 cases
21 cases
2 years follow-up or more
Retrospective analysis: 2012-2015

Surgical technique
N Flex
1. In the prone position, a midline 5-cm incision was made on
the skin over the spinous processes at the listhetic segment.
2. The dorsolumbar fascia was incised, and bilateral muscle
dissection was performed along the spinous processes over
the lamina gently up to the lateral edge of the pars
interarticularis and facet joints.
3. The holes for CBT screws were created from the inferomedial
to superolateral direction under fluoroscopic control. Care
was taken to avoid injury to the upper joint capsule during
the procedure.
4. Bilateral laminotomy and facetectomy were performed. We
routinely perform bilateral facetectomy to obtain the local
bone as much as possible, perform slip reduction easily, and
increase segmental lordosis as much as possible.
5. After the intervertebral disc removal, the interbody cages and
the local bone harvested during the decompression were
placed.
6. The CBT screws were finally placed. Subsequently, slip
reduction was accomplished under the fluoroscopic control by
pulling the CBT screws within the listhetic vertebrae
posteriorly by using a rod persuader placed over the cranial
screw head. Finally, the screws were compressed into each
other to create lordosis.
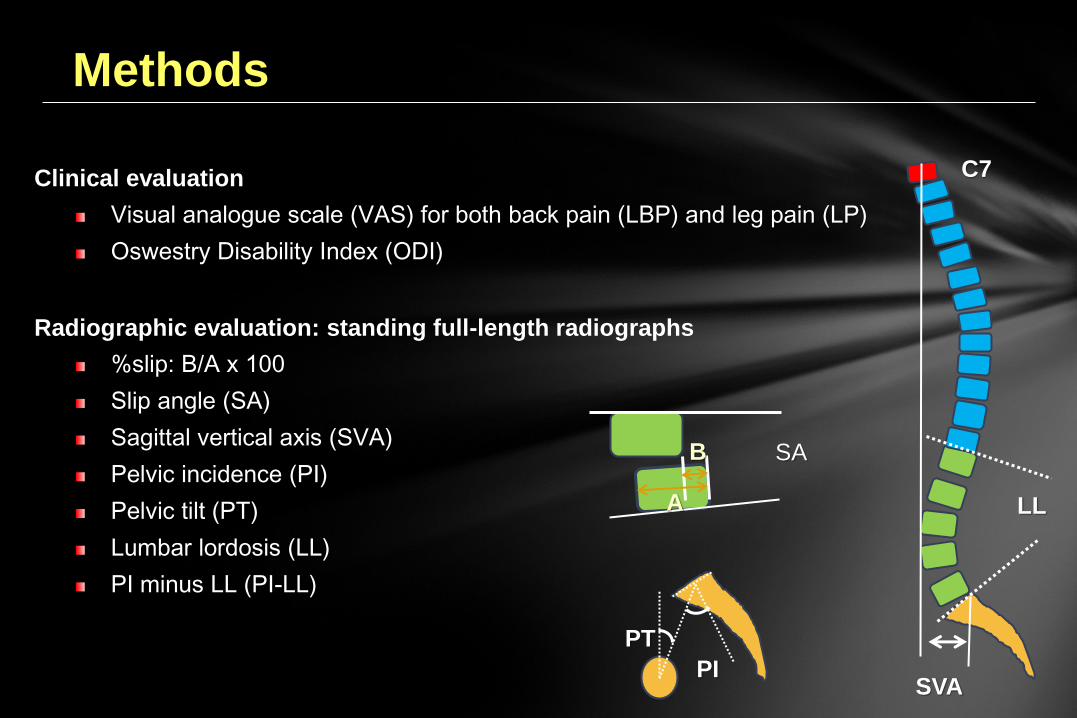
Methods
Clinical evaluation
Visual analogue scale (VAS) for both back pain (LBP) and leg pain (LP)
Oswestry Disability Index (ODI)
Radiographic evaluation: standing full-length radiographs
%slip: B/A x 100
Slip angle (SA)
Sagittal vertical axis (SVA)
Pelvic incidence (PI)
Pelvic tilt (PT)
Lumbar lordosis (LL)
PI minus LL (PI-LL)
LL
SVA
C7
PT
PI
A
B SA

Outcomes of MIDLIF using CBT screws (2–5 years)
The average intraoperative blood loss was 193.2 ml, with an average operative time of 176.8 minutes.
No intraoperative complications, including dural tear, pedicle fractures, and nerve root injury, occurred.
There was a case of surgical site infection, which was cured by debridement and antibiotics with implant retention.
Union was achieved in 85.7% (18/21) of patients.

During the follow-up period, one case underwent reoperation because of lumbar disc herniation at the cranial adjacent level three years after surgery.
Preop (N = 20) Postop (N= 20) P
ODI 36.2% (14.0–84.0%) 7.3% (0–10%) <0.01
VAS-LBP 5.4 (0–10) 0.5 (0–2.7) <0.01
VAS-LP 7.3 (1.5–10) 0.8 (0–4.4) <0.01
Outcomes of MIDLIF using CBT screws (2–5 years)

Outcomes of MIDLIF using CBT screws (2–5 years)
Preop Postop P
SA° 8.3 10.7 <0.01
%slip 16.7 4.0 <0.01
SVA (mm) 48.4 27.6 0.01
PT° 19.5 15.4 <0.01
LL° 38.5 43.9 0.01
PI° 51.1 50.1 0.09
PI-LL° 12.7 6.2 <0.01
Radiographic parameters

Conclusion
MIDLIF using CBT screws is safe, and the midterm operative
results are acceptable. This technique seems to be an
encouraging alternative to traditional lumbar fusion surgery in
LDS patients.
None of the authors has any potential conflict of interest.