miller fisher syndrome
TRANSCRIPT

Dr. Md Rashedul Islam FCPS, MRCP(UK)
Registrar, Neurology, BIRDEM

A 57 years old diabetic right handed gentleman,
hailing from Mirpur, got admitted in BIRDEM
General Hospital on 11th March,14 with the
complaints of-
• Double vision for 6 days
• Difficulty in walking for 4 days
According to the statement of the patient, he was reasonably well 6 days back. Then he developed double vision which was sudden on onset, constant, more marked on eye movement & not associated with diuranal variation. He also had complaints of headache which was sudden on onset, global, dull aching in nature, mild to moderate in severity. It was not associated with radiation, vomiting. There was no exacerbating factors & it was relieved with medication.

• He also had complaints of difficulty in walking for last 4 days which was gradual on onset due weakness of lower limbs progressing to upper limbs rapidly. It was associated with numbness of limbs. There was no associated back pain, vertigo on standing, palpitation, shortness of breath, swallowing difficulties, slurring of speech. He doesn't give h/o cough & diarrhea.

H/O Present illness
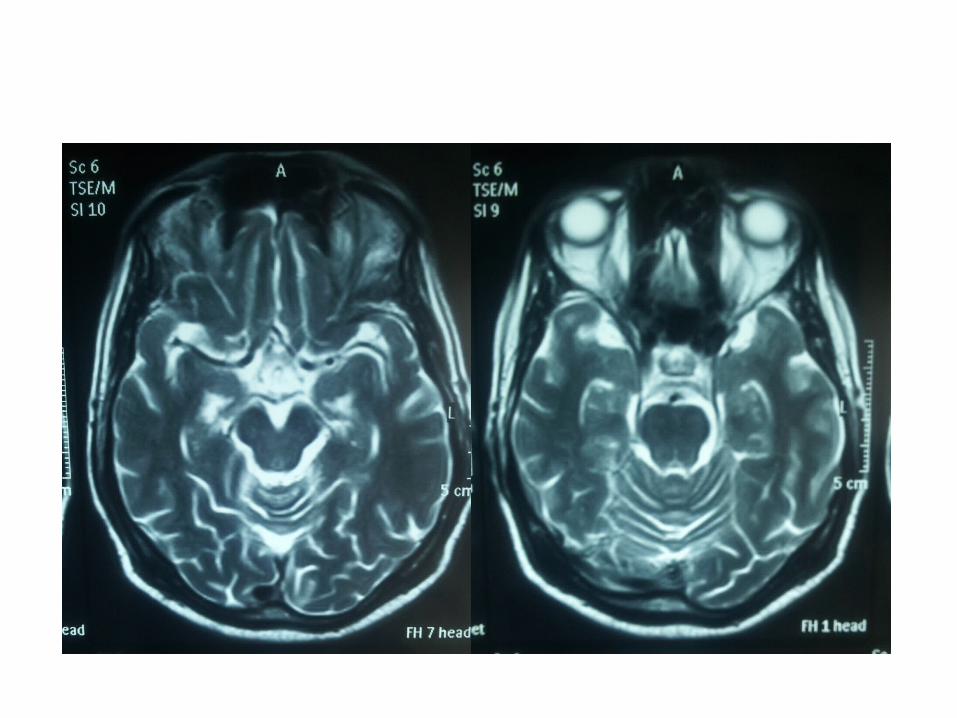
He consulted an endocrinologist for these problems as he assumed that it might be due to high blood sugar. He was advised for CT scan & subsequent MRI of brain & diagnosed as a case of DMT2, Acute ischaemic stroke, cranial polyangitis due to diabetes with DPN. He was treated with insulin, aspirin, atorvastatin & vtamin B complex. He got admitted in Neurology, BIRDEM as he was not improving.
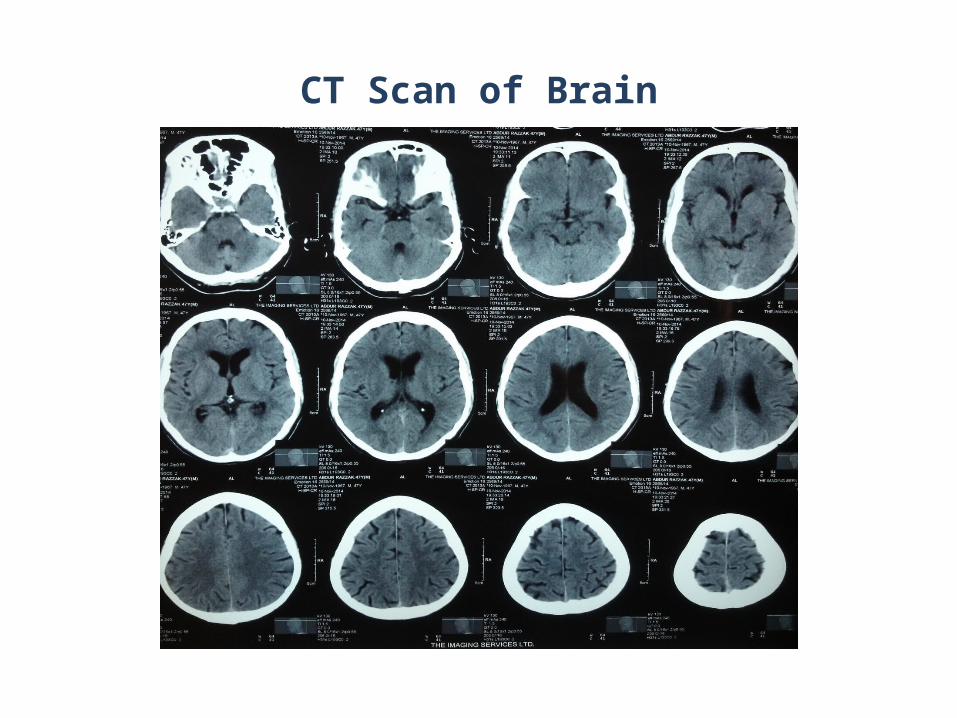
CT Scan of Brain

CT Scan of Brain




H/O past illness: Nothing contributory Socioeconomic history: He belongs to a middle class family
Personal history:
He is non alcoholic, non smoker

Family history:
Nothing significant
Treatment history:
Insulin
Tab. Vit B complex
Tab. Aspirin
Tab. Atorvastatin
General examination:
Appearance: ill looking, anxiousBuilt: average Decubitus: on choiceAnaemiaJaundiceCyanosisOedemaDehydrationClubbingKoilonychiaLeukonychia
Absent

General examination:
Neck vein: not engorged
Thyroid: not enlarged
Lymph node: not palpable
Skin pigmentation & body hair distribution: normal
Pulse: 78 b/min
BP: 120/70 mmHg
Temp:98 F
RR: 16 breaths/min

• Higher psychic function : Conscious, Oriented• Speech: Normal• Cranial nerves :
Bilateral complete opthalmoplegia with right sided lower motor type VII nerve palsy
• Fundus: Normal• GCS: 15/15
NERVOUS SYSTEM EXAMINATION


Muscle Rt. UL Lt. UL Rt. LL Lt. LL
Bulk Normal Normal Normal Normal
Tone Decreased Decreased
Decreased Decreased
Power 3/5 3/5 3/5 3/5
Involuntary movement
Absent Absent Absent Absent
MOTOR FUNCTION:

Reflex B T S K A Abd Plantar
Right Absent
Absent
Absent
Absent
Absen
t
Absent Flexor
Left Absent
Absent
Absent
Absent
Absen
t
Absent
Flexor

Sensory system:
Pain Temp Touch Vibration
Position sense
Right upper limb
Intact
Right lower limb
Left upper limb
Left lower limb

• Sign of Meningeal irritation - Absent
• Cerebellar sign : Absent
• Gait: Ataxic

Systemic examinations
Other systemic examination was normal

A 57years old diabetic gentleman got admitted in neurology with the complaints of double vision which was sudden on onset, more marked on eye movement & not associated with diurnal variation. He also had complaints of headache which was sudden on onset, global, dull aching in nature, mild to moderate in severity. It was not associated with radiation, vomiting.
Salient feature

Salient feature
He also had complaints of difficulty in walking for last 4 days which was gradual on onset due to weakness of lower limbs progressing to upper limbs rapidly. It was associated with numbness of limbs. There was no associated back pain, vertigo on standing, palpitation, shortness of breath, swallowing difficulties, slurring of speech. He doesn't give h/o cough & diarrhea.

• On examination, he was anxious, ill looking, bilateral complete opthalmoplegia with right sided lower motor type VIIth nerve palsy, Generalized hypotonia, diminished muscle power, generelized areflexia with bilateral planter flexor. All modalities of sensation were intact with ataxic gait.

Provisional diagnosis
• Guillain-Barre Syndrome(Miller Fisher Variant)
• Diabetes Mellitus Type 2
• Leukoaraiosis / Periventricular white matter disease

Differential diagnosis
• Mononeuritis cranial multiplex due to?
Vasculitis/Diabetes

Investigations
CBC:
Hb % - 14.2
WBC -6800 cu/mm
Neu-65 %
Lymph- 30%
Mono -3 %
Eosino- 1.1%
Platelet- 195000
ESR- 30mm in 1st hour
S. Electrolytes
Na-137 mmol/l
K-4.5 mmol/lCl: 106 mmol/lHCO3: 26 mmol/lCa- 9.3 mmol/lMg- 0.9 mmol/lPhosphate-3.7

Lipid profile:
TG: 176 mg/dl
T. Chol : 164 mg/dl
LDL: 95 mg/dl
HDL:36 mg/dl
LFT:
ALT: 34 iu/L
AST: 37 iu/L
RFT:
S. Creatinine: 0.8mmol/l
S Urea: 29 mmol/l
HbA1c: 7.2%

Sugar - Nil
Albumin – Nil
Ketone- Nil
Epi. cell: A few /HPF
Pus cell: 1-2 /HPF
RBC: Nil
URINE R/M/E
Chest X-Ray
NORMAL

ECG
Normal

Nerve conduction study
• Pure motor polyneuropathy-• Possibilities are:
• AMAN• Other motor polyradiculoneuroapthy

CSF study
• Appearance: clear
• Protein: 66g/L
• Sugar: 4.2mmol/L( Corresponding blood glucose-6.8 mmol/l)
• Cell count:
• Total WBC : Nil
• Total RBC: Nil
• Bacterial antigen: Negative

Final diagnosis:
• Guillain-Barre Syndrome(Miller Fisher Variant)
• Diabetes Mellitus Type 2
• Leukoaraiosis / Periventricular white matter disease

Treatment:
Short acting insulin
I/V immunoglobulin
Daily physiotherapy
Vitamin B
Patient was counseled about Course and prognosis of the disease

Hospital course
• He showed significant improvement with treatment.
• Gait & opthalmoplegia was improved
Follow UP
Patient was advised to follow up in Neurology after 1 month for further clinical evaluation & management.
