mindfulness martial arts 1 - excellence for child and … effects than self-report and parent-report...
TRANSCRIPT

Mindfulness Martial Arts 1
Evaluation Implementation Grant 1155
Mindfulness Martial Arts:
An Innovative Treatment for Youth with Learning Disabilities and
Co-occurring Mental Health Difficulties
Integra
Dr. Karen Milligan
Director of Research & Psychology
Paul Badali, M.S.W.
Child and Family Therapist
Dr. Marjory Phillips
Director of Clinical Services and Community Consultation
October 2010

Mindfulness Martial Arts 2
Executive Summary
Learning Disabilities (LDs) are the most common form of disability for children aged 5 to 14
years, effecting over three million Canadians (Stats Canada, 2006). While difficulties in academics are
most commonly associated with LDs, the impact of LDs extend beyond the classroom, with rates of
mental health difficulties being 2 to 3 times higher in youth with LD (LDAC, 2007). Integra is the only
children’s mental health centre in Canada dedicated to treating children and youth with learning
disabilities and co-occurring mental health issues. This work necessitates adapting mental health
treatments to capitalize on learning and processing strengths, while accommodating for areas of
weakness or challenge. The experience of repeated failure in youth with LDs is common and as such
many youth avoid challenging work, including addressing mental health issues. It is therefore essential
to develop creative ways of engaging youth and assisting them in facing challenges.
Mindfulness Martial Arts (MMA: Badali, 2002; Badali & Milligan, 2009) was developed at
Integra in 2002 in response to these needs. MMA is a manualized group treatment, developed for
youth (aged 12-18) with LDs and co-occurring self-regulation difficulties. MMA integrates mindfulness
meditation, cognitive behavior therapy, and behavior modification into a 20-week martial arts group
training program. Martial arts acts as an active component of change (e.g., promoting planning,
inhibition, flexibility) and a non-stigmatizing milieu that youth find highly engaging. Parents are
involved to promote generalization of skills. The goal of MMA is to improve youth’s self-awareness
and ability to face challenges, so that they can learn and apply new, more adaptive coping strategies.
While previous research has suggested that MMA is effective in reducing anxiety and externalizing
behaviour problems in youth with LDs, questions remained about how MMA brings about change, how
change is best measured, and delivery of the program. The present study addressed these questions
with three specific objectives.
1. Does MMA impact self-awareness, behavioural regulation, and attributions of control?
2. Given the exponential growth of MMA in recent years and the associated increase in therapists
leading the group, is MMA being implemented consistently across group and therapist?

Mindfulness Martial Arts 3
3. When examining processes of change, are performance-based measures associated with
stronger effects than self-report and parent-report questionnaire measures?
To address these three objectives, a mixed methods approach to program evaluation was utilized,
including a range of questionnaires, performance-based measures, qualitative interviews and video-
taped observations. Forty-six youth (age 12-16) enrolled in MMA consented to participate in the study
and 34 youth (5 girls, 29 boys) completed both the pre- and post-testing sessions. All youth met
Integra’s intake criteria for learning disability and presented with mental health difficulties, including
ADHD, Asperger Syndrome, anxiety, depression, externalizing behavior problems, and peer relation
difficulties. Participants completed a range of questionnaire, computer, drawing, and interview tasks
designed to assess self-awareness of emotions and thoughts, behavioural regulation, and attributions
of control at the beginning and end of treatment. Parents and teachers were also asked to complete
questionnaires about participants’ behaviour and regulation abilities before and after treatment. Six
boys and 5 parents also completed semi-structured interviews to investigate gains made in MMA and
the components or processes that support these gains. Using a modified grounded theory framework,
themes were extracted from transcripts by two independent readers and then primary themes were
determined through discussion. To assess treatment fidelity, sessions were coded across group
leaders and results were compared to examine consistency with the manual and across instructors.
All three objectives were met. Results consistently suggested that MMA has a positive impact
on self-awareness and behavioural regulation. For example, in an interview examining the ability of
youth to talk about negative or stressful life experiences, youth demonstrated increased ability to
differentiate and identify emotions and talk about their thoughts. Youth also demonstrated gains in
behavioural regulation. For example, on a trail-making task that required youth to shift between two
concepts, youth showed improved ability to shift or flexibly respond from pre- to post-treatment.
Performance-based measures appeared to provide a more sensitive assessment of processes than
self- or parent-report measures and allowed for more specific interpretation of processes of change.
These results were further reinforced by findings of the qualitative interviews. Overall, youth
and parents were highly satisfied and felt the program was helpful. Respondents emphasized the
Mindfulness Martial Arts 4
importance of milieu, speaking about the desire to develop mastery in martial arts and be part of a
socially valued activity. The relationship with the MMA therapist, or sensei, was identified as
paramount. Mindfulness strategies were reported to improve youth’s self-awareness and this enabled
them to be calm, stop and think, and change patterns of automatic responding. The type of gains
made differed depending on the youth’s presenting concerns. All respondents reported that change
took time.
These results are extremely encouraging to Integra staff and stakeholders and they support
our movement towards dissemination of MMA to other children’s mental health agencies. The results
also highlight challenges that many youth with LDs have in regards to self-awareness and behavioural
regulation and they support targeting these processes to promote a diverse range of mental health
outcomes.
A key step in the process of dissemination is demonstrating that MMA can be delivered in a
consistent manner, with similar results across therapists. Results were positive and moreover the
process of assessing treatment fidelity has led to essential manual revisions that will continue to
support the standardized delivery of MMA. Our next steps for dissemination will include completing the
final revision of the manual and developing a training program for therapists.
As the popularity of MMA grows, Integra management has been faced with the challenge of
determining how long youth should be allowed to participate in the program. The present results
reinforce our belief that change takes time for youth with LDs and youth continue to benefit from the
program beyond the beginner level. We will continue to collect data on key outcomes to examine the
question of length of treatment longitudinally.
A major limitation of the present study was the absence of a control group. We are planning
future studies of MMA that will address its impact on self-awareness and behavioural regulation (using
performance-based measures) and how changes in these processes may promote mental health
outcomes.
Mindfulness Martial Arts 5
Table of Contents
Introduction .............................................................................................................................................7 Support for the Feasibility and Efficacy of MMA .....................................................................................9 Study Objectives.....................................................................................................................................9
Impact of MMA on Self-awareness and Emotion Regulation............................................................10 Impact of MMA on Behavioural Regulation.......................................................................................11 Impact of MMA on Attributions of Control .........................................................................................11 Identifying Sensitive Measures of Change........................................................................................12 Assessment of Treatment Fidelity.....................................................................................................12
Overall Methodology.............................................................................................................................13
Study 1: Quantitative Study ..............................................................................................................13
Participants ...................................................................................................................................13 Procedure .....................................................................................................................................14 Measures ......................................................................................................................................14 Data Analysis ................................................................................................................................17 Results ..........................................................................................................................................17
Study 2: Qualitative Evaluation .........................................................................................................21
Participants ...................................................................................................................................21 Procedure .....................................................................................................................................21 Results ..........................................................................................................................................22
Study 3: Process Evaluation .............................................................................................................26
Verification of Learning Disability Diagnosis .................................................................................26 Client Satisfaction and Impressions of MMA.................................................................................26 Treatment Fidelity .........................................................................................................................27
Methodological Strengths and Challenges ...........................................................................................28 Discussion & Lessons Learned.............................................................................................................30
Enhancing Interest, Knowledge and Capacity for Research and Program Evaluation at Integra.....30 Development of Relationships with Stakeholders to Support Future Research in MMA ..................30 Enhancement of Knowledge of MMA and Key Processes to Consider in Treatment of Youth with LDs....................................................................................................................................................31 Challenges in Balancing Clinical Needs and Research Protocol......................................................32 Relationship with the Centre for Excellence in Children’s Mental Health .........................................32
Conclusions and Recommendations ....................................................................................................32
MMA Increases Self-Awareness and Behavioural Regulation..........................................................33 Engagement of Youth and the Importance of Milieu.........................................................................34 Beginner and Advanced MMA: How long is long enough?...............................................................34
Knowledge Exchange ...........................................................................................................................35 References............................................................................................................................................37 Appendix A: Mindfulness Martial Arts Logic Model...............................................................................40 Appendix B: Information Letters and Consents ....................................................................................41
Mindfulness Martial Arts 6
Appendix C: MMA Program Evaluation Procedure Chart ....................................................................46 Appendix D: Figures & Tables ..............................................................................................................51 Appendix E: Interview Information Letter, Consents, and Guide ..........................................................57 Appendix F: Qualitative Model ..............................................................................................................63 Appendix G: Client Satisfaction Evaluations and Summaries...............................................................64 Appendix H: Treatment Fidelity Coding Scheme..................................................................................69 Appendix I: Qualitative and Quantitative Posters Submitted ................................................................71
Mindfulness Martial Arts 7
Introduction
Learning Disabilities (LDs) refer to a variety of neurologically-based disorders that affect a
person’s ability to take in, understand, remember or express information (Silver et al., 2008; LDAC,
2002). LDs are the most common form of disability for children aged 5 to 14 years, effecting over three
million Canadians (Stats Canada, 2006). While difficulties in academics are most commonly
associated with LDs, the impact of LDs extend beyond the classroom, with rates of mental health
difficulties being 2 to 3 times higher in youth with LDs (LDAC, 2007). One third of youth with an LD
have ADHD (Wilcutt & Pennington, 2000) and approximately 10% have significant behaviour problems
(Lowe et al., 2007). Peer rejection, neglect, and victimization are experienced by approximately 50%
(Wiener, Harris & Shirer, 1990; Mishna, 2003) and friendships tend to be unstable and impoverished
(Wiener & Schneider, 2002; Wiener & Sunohara, 1998).
Integra is the only children’s mental health centre in Canada dedicated to treating children and
youth with LDs and co-occurring mental health issues. This work necessitates adapting mental health
treatments to capitalize on learning and processing strengths, while accommodating for areas of
weakness or challenge. The experience of repeated failure in youth with LDs is common and as such
many youth avoid challenging work, including addressing mental health issues. It is therefore essential
to develop creative ways of engaging youth and assisting them in facing challenges.
Mindfulness Martial Arts (MMA) was developed at Integra by Paul Badali, Registered Social
Worker, in 2002. The impetus for the program was the need for a creative way to engage youth in
treatment who would not otherwise engage. MMA was developed on the premise that self-awareness
and the ability to self-monitor thoughts, feelings, and behaviours provides an essential foundation
needed to benefit from skill-based treatment (e.g., social skills training) and mental health
interventions (e.g., problem-solving skills training). As depicted in the MMA Logic Model (see
Appendix A), MMA involves 20 weekly 1.5 hour group sessions followed by brief meetings with youth
and parents. Each MMA group comprises 8 youth and is led by a child and family therapist (with
graduate level training) who has qualifications in mindfulness meditation and martial arts. MMA is
individualized for cognitive/learning profiles, specific mental health needs, and levels of motor
Mindfulness Martial Arts 8
coordination to ensure high levels of success, motivation, and meaning. The following treatment
components are involved. Mindfulness Practices foster non-judgmental attention to the present
moment which allows youth to recognize their feelings, thoughts, and consider effective coping
strategies before reactively employing less effective means of emotion regulation (e.g., avoidance).
Increased self-awareness may reduce emotional reactivity, thereby decreasing impulsivity and
increasing attention and tolerance for ambiguity/uncertainty and discomfort (Chawla & Ostafin, 2007).
Mindfulness approaches have been shown to be effective for adult mental health disorders (e.g.,
depression, anxiety, pain; Baer, 2003) and improving emotion regulation (Ortner, Kilner, & Zelazo,
2007). Research examining mindfulness treatments in children also suggests positive outcomes,
including decreased aggression (Singh et al., 2007), anxiety (Semple, Reid & Miller, 2005), and
impulsivity, and increased attention and flexibility (Cayoun, 2008). From this state of self-awareness,
youth are optimally prepared to benefit from Cognitive Behavior Therapy (CBT) strategies that focus
on changing the way youth think about and respond to emotions, such as anxiety, sadness, and anger
(Kendall, 2000). Behavior activation and modification strategies (e.g., response-cost point system;
Barkley, 1997) motivate youth to fully participate in treatment and to generalize use of strategies to life
outside of the treatment setting. Youth are positively reinforced for attendance, participation, and
home practice, as well as progress towards meeting their own well-being and mental health goals.
Weekly sessions with parents are designed to promote generalization of strategies and concepts
outside of the treatment setting. Martial Arts Training acts as an engaging milieu and an active
component of change. Martial Arts enhance treatment by providing “active physical routes for the
discovery and expression of emotion” (Weiser et al., 1995, p. 118). Persistence, flexibility, and trust in
group members are developed within the context of self-defense challenges. Martial arts training,
which includes philosophical and meditation components, has been shown to have therapeutic effects
including improved body image, attention, self-regulation and social relationships, as well as reduced
aggression (Lakes & Hoyt, 2004; Zivin et. al., 2001).
Mindfulness Martial Arts 9
Support for the Feasibility and Efficacy of MMA
Since 2002, more than 160 youth have participated in MMA, with an impressive 96%
completing treatment. In 2005/06, Integra received a program evaluation grant from the Centre of
Excellence to systematically evaluate MMA. Analysis of change scores on self-report and parent-
report measures of behaviour, mood, and self-perception (N=26) revealed improvements in self-
esteem and perceptions of self efficacy, impulsivity, and externalizing problems. This research led to a
follow-up collaborative study of MMA with the University of Toronto (Haydicky, 2009; Haydicky,
Wiener, Badali, & Milligan, submitted. Sixty-five boys (ages 12-18) with learning disabilities and mental
health disorders were assigned to MMA or a waitlist control group. Boys with ADHD showed
significantly greater improvement on parent-rated externalizing behaviour, oppositional defiant
problems, and conduct problems compared to waitlist controls. Boys with elevated hyperactive/
impulsive symptomatology also showed significantly more gains on parent-rated social problems and
monitoring skills. Boys with elevated levels of anxiety pre-treatment, reported decreased levels of
anxiety post-treatment, compared to waitlist controls.
Study Objectives
While previous research has highlighted the promise of MMA as an effective treatment for
youth with LDs and co-occurring ADHD or anxiety, clinicians and researchers at Integra continued to
wonder about changes in processes, such as self-awareness, behavioural regulation, and mastery
motivation/attributions of control, that might promote mental health outcomes. The clinical and
research teams also wondered if the measures used to assess behavioural regulation in previous
research were sensitive enough to detect effects and whether performance-based measures would
show stronger results than self-report and parent-report questionnaire measures. Based on these
questions and a thorough review of the literature, three key processes (i.e., self-awareness,
behavioural regulation, and attributions) that may mediate changes in behavioural outcomes were
identified for study. The first objective of the study was to examine the impact of MMA on these
processes. The second objective was to examine new measures of processes that may be more
sensitive to change than traditional questionnaire measures. Given the exponential growth of MMA in
Mindfulness Martial Arts 10
recent years and the associated increase in therapists leading the group, the third objective was to
determine if MMA was being implemented consistently across group and therapist.
Impact of MMA on Self-awareness and Emotion Regulation
Youth with LDs frequently avoid interactions, activities, thoughts and emotions associated with
failure or distress. They often do so by withdrawing from stressful situations or engaging in problem
behaviors that facilitate avoidance or distract them from troubling thoughts and feelings (Ducharme &
Harris, 2005). Experiential avoidance coined by Hayes et al. (1996) is a process of avoiding unwanted
private thoughts, feelings and sensations and an unwillingness to experience these private events,
while deliberately making efforts to control or escape them (Kashdan, Barrios, Forsyth, Steger, 2005).
The paradox of experiential avoidance is that attempting to hide or inhibit unpleasant thoughts,
feelings and body sensations, while somewhat effective in the short-term, serves to increase the
frequency and distress of these same experiences (Gross, 1998, 2002; Wegner, 1994). For example,
a youth with an LD may experience intense anxiety and frustration about school work, difficulty
relating to peers, and feel ineffectual in completing work, such that they begin to avoid attending
school or choose to be home schooled. This response precludes participation in the activities and
developmental experiences that support youth in developing life skills and competencies, which may
promote mental health outcomes. Developing adaptive emotion regulation abilities that promote
positive responses is essential.
Emotion regulation is “the intrinsic and extrinsic processes responsible for monitoring,
evaluating, and modifying, emotional reactions, especially their intensive and temporal features, to
accomplish one’s goals” (Thompson, 1994; pp. 27-28). Moses and Barlow (2006) have argued that
current psychological interventions can be enhanced by incorporating the development of emotion
regulation skills within the context of disorder-specific treatment. Few treatments for youth incorporate
a focus on emotion regulation, and specifically acceptance, resilience, and modification of negative
emotions, which has been most strongly and consistently related to mental health (Berking et al.,
2008). Given that emotion regulation difficulties are common in youth with LDs (Bauminger & Kimhi-
Mindfulness Martial Arts 11
Kind, 2008) and underlie many forms of mental health difficulties in childhood (Bradley, 2003),
treatments are needed that target this essential skill.
Increasing self-awareness and emotion regulation are considered foundational skills in MMA.
Through mindfulness and meditation exercises youth learn to “be” present with challenging thoughts
and feelings, regulate their emotions, and break patterns of automatic, habitual reacting. Self-
awareness is also incorporated into other components, such as martial arts to facilitate the
development of an increasing awareness of one’s body and movement and cognitive therapy to
enhance awareness of one’s thoughts and associated feelings.
Impact of MMA on Behavioural Regulation
MMA was developed on the assumption that as youth become more self-aware, they have the
foundation to begin to improve their ability to regulate their behaviour. Two key processes involved in
behavioral regulation are the ability to inhibit patterns of automatic responding and the ability to flexibly
move from one response strategy to another. Behavioural regulation and executive function difficulties
are well documented in youth with ADHD. While fewer studies have been completed with youth with
LDs, results suggest similar challenges. Seidman, Biederman, Monuteaux, Doyle & Faraone (2001)
found that boys with co-occurring ADHD and LD performed significantly worse compared to boys with
ADHD and no LD on executive function measures, including the Stroop Task which measures
inhibition and cognitive flexibility.
Impact of MMA on Attributions of Control
The experiential avoidance style of coping used by many youth with LDs frequently leads
youth to believe that they are not capable of producing positive outcomes. Further, positive outcomes
that do occur are frequently attributed to unstable and external factors (e,g., “luck”). In contrast,
negative outcomes are thought to be due to internal, stable, and global factors (Ayres, Cooley & Dunn,
1989). This attribution stance leads to decreased levels of mastery motivation and reinforces a pattern
of avoidance.
MMA is designed to enhance mastery motivation and attributions of control. First, motivation is
enhanced because youth are engaged in a socially valued activity. Second, the program is strength-
Mindfulness Martial Arts 12
based and graduated so that youth work at skills that are at or slightly above their current skill level,
with the level of difficulty being gradually increased (e.g., meditation starts with 1 minute and the
length is gradually increased). This promotes success and the desire of youth to challenge
themselves. Therapists reinforce the relation between the student’s effort and positive outcome (e.g.,
praise, points, promotion to next martial arts belt).
Identifying Sensitive Measures of Change
In addition to targeting key outcomes identified, another objective of the present research was
to pilot new measures of processes related to behavioural regulation. Recent research completed in
collaboration with the University of Toronto found that youth with LDs provide less accurate appraisals
of their difficulties when presented with likert scales as compared to forced-choice questions
(Haydicky, Timmermanis, & Weiner, 2009). Given the potential impact of this finding on our ability to
detect change, new approaches to measurement were used. We consulted with clinical and research
staff at Integra and expert stakeholders in the field to select and design methodology (e.g.,
performance based measures of processes, forced-choice questions) that would address this
limitation.
A second methodological objective was to integrate the richness of qualitative research into
our findings. There was a sense among the clinical team that the quantitative measures used did not
always fully capture the changes the youth were making and did not address questions related to
processes of change.
Assessment of Treatment Fidelity
The final objective of the proposed study was to assess treatment fidelity. Since the
development of MMA in 2002, the program has grown at an exponential rate. MMA is currently offered
5 days a week and there are three therapists delivering the treatment, as well as volunteer co-leaders.
We were therefore interested in assessing if the program is being delivered in a consistent manner
across groups and if it is consistent with the MMA manual (Badali, 2009). Examining treatment fidelity
was considered important to Integra staff in order to determine if there was an effect of therapist on
outcome. We were also interested if the manual in its current form could be followed in a standardized
Mindfulness Martial Arts 13
manner, as this would inform revisions to the manual and the eventual dissemination of MMA to other
clinicians.
Overall Methodology
A mixed methods approach to program evaluation was utilized for the present study and
included a range of questionnaires, performance-based measures, qualitative interviews and video-
taped observations. The proposed research was reviewed and approved by the Integra Board
Research Committee and was in accordance with the Ethical Guidelines of the American
Psychological Association. Given the comprehensive and complex nature of the quantitative,
qualitative, and process evaluations involved in this study, the methodology and results for each study
will be presented in 3 separate sections: Quantitative Study; Qualitative Study; and Process
Evaluation.
Study 1: Quantitative Study
Participants
All Integra clients participating in Mindfulness Martial Arts were invited to participate in the
program evaluation study. Of these 60, 46 consented to participate in the study. Thirty-four students (5
girls, 29 boys) completed both the pre- and post-testing sessions. Four did not complete MMA, one
was very ill at the time of post-test, and five chose to not participate in the post-testing session.
Participants ranged in age from 12 to 18 (mean age of participant in the study was 167.41 months
(13.95 years), standard deviation = 19.9 months). All youth met Integra’s intake criteria for learning
disability (at least average level of cognitive ability with significantly lower academic achievement and
challenges in at least one area of processing) and presented with mental health difficulties, including
ADHD, Asperger’s Syndrome, anxiety, depression, externalizing behavior problems, and peer relation
difficulties. For 22 of the participants, this was their first MMA group. Twelve participants were in the
advanced group, having taken a mean of 1.75 groups (SD = 1.05).

Mindfulness Martial Arts 14
Procedure
In August 2009 and February 2010, all students registered in MMA received a letter of
introduction and an invitation to participate in the program evaluation of Mindfulness Martial Arts (see
Appendix B). The principal investigator or research coordinator called each family and asked if they
were willing to participate. If they consented, they were invited to Integra to participate in a one-hour
individual testing session.
The individual testing session was conducted by a research assistant with graduate training in
clinical psychology. Parent and youth consent forms (see Appendix B) were completed at the
beginning of the session. Youth completed all measures in counter-balanced order (see Appendix C
for Procedure Chart). Parents were asked to complete the BRIEF and Conners-3 while waiting for
their child. If parents did not accompany their child to the session, questionnaires were sent home and
reminder phone calls were made to encourage questionnaire completion. Due to difficulties
encountered in completing and returning questionnaires, we moved to an online system, in which
parents could securely complete questionnaires and information was automatically accessible to the
research team. This method was associated with a higher rate of questionnaire return. In order to
obtain information on outcomes at school, teachers were asked to complete two behaviour
questionnaires (Conners-3 and BRIEF) before and after treatment. Participants were asked to
nominate the teacher that knew them best. Questionnaires were delivered to teachers via youth or
their parents, and each participant was given points towards earning their martial arts belt if the
questionnaires were returned.
Measures
Self-Awareness of Emotions and Thoughts
Children’s Acceptance and Mindfulness Questionnaire (CAMM; Greco, Smith, & Baer, 2008)
The CAMM is a 10-item self-report questionnaire assessing youth’s ability to attend to feelings,
thoughts, and bodily sensations, to act with awareness of present moment, and to accept internal
events without judgment (see Appendix C).
Mindfulness Martial Arts 15
Positive and Negative Experience Interview
This interview was developed by the Integra research team based on research in the area of
autobiographical memory (e.g., Raes, Hermans, de Decker, Eelen, & Williams, 2003; Foley Centre,
1997). In the negative condition, youth were asked to tell the examiner about the most negative,
stressful, or upsetting event of their life. They were told to be as specific as possible. After being given
the opportunity to answer independently, they were asked specific questions about the event that
tapped into their thoughts and feelings about the event. The positive condition required youth to talk
about the best experience of their life and followed the same format (see Appendix C for interview
script). All youth completed the positive and negative conditions and the order of the conditions was
counter balanced. Interviews were taped and transcribed. Following the guidelines of Fivush, Marin,
Crawford, Reynold, & Brewin (2007), change in the proportion of emotion and cognition words was
used as the measure of self-awareness of emotions and thoughts. Linguistic Inquiry and Word Count,
a text analysis software program designed by Pennebaker, Booth, and Francis (2007), was used to
semantically categorize and compute word counts.
Behaviour Regulation
The Behavior Rating Inventory of Executive Functions (BRIEF: Gioia, Isquith, Guy & Kenworthy,
2000). The BRIEF is an 86-item parent and teacher-completed questionnaire. Respondents rate the
youth’s behavioural regulation (inhibition, shifting, emotion control) and metacognitive skills (initiate,
working memory, plan/organize, organization of materials, monitor) on a 3-point scale. The BRIEF
demonstrates high internal consistency and moderate correlations between parent and teacher report.
Construct validity and concurrent validity have been supported by a number of studies with clinical
populations (Straus, Sherman & Spreen, 2006).
Test of Variables of Attention (TOVA: Greenberg & Kindschi, 1996)
TOVA is a visual continuous performance test that requires the youth to press a microswitch each
time a target stimulus is displayed and to inhibit responding to a non-target stimulus. The test is 22
minutes in length and includes a practice trial to ensure understanding of task instructions. There is
evidence of internal consistency by blocks as well as evidence of temporal reliability (see Riccio,
Mindfulness Martial Arts 16
Reynolds, & Lowe, 2001 for a review). Commission errors reflect impulsive responding, whereas
omission errors are a measure of inattention.
D-KEFS Trail Making Test (Delis, Kaplan, & Kramer, 2001)
This test was used to assess changes in shifting ability or cognitive flexibility. The test consists of 5
conditions, including Number-Letter Switching in which the participant has to draw a line connecting
numbers and letter in order switching between the two categories. For this study, the performance on
the Number-Letter Switching Task was used. Motor speed was controlled for given that a number of
participants have graphomotor difficulties.
Emotion Interference Task (EIT: Buodo et al., 2002)
This computer-based information processing measure of emotion regulation is used to assess if youth
are able to disengage from emotionally salient material in order to complete a simple task. Participants
view 10 neutral, 10 pleasant, and 10 unpleasant scenes from the International Affective Picture
System (IAPS) (Lang et al. 2001) in random order for 6,000 ms each. At 4,000 ms (4 s SOA) after
picture onset, a tone is presented. Participants press a button as quickly as possible to indicate
whether the tone is high or low and reaction time is measured. Poor emotion regulation is associated
with longer response times while viewing unpleasant pictures. The EIT has been used to successfully
detect significant changes in mindfulness treatment research (Ortner et al., 2007). Given the large age
range of the children and the ethical requirement to ensure pictures were not too disturbing, the
valence of pictures differed within the positive and negative set. Normative data (Lang et al., 2001)
was used to rank the pictures according to their valence. The five with the highest negative valence
were used to complete the negative reaction time score. The same procedure was used for positive.
Five of the neutral pictures were randomly chosen and used to calculate the neutral score.
Attributions of Control
Children’s Attributional Style Questionnaire - Revised (Thompson et al., 1998)
The CASQ-R is a 24-item forced choice questionnaire that assesses attributional style on
internal/external control, global/specific, and stable/unstable dimensions (see Appendix C).
Mindfulness Martial Arts 17
Externalizing Behaviour Problems
We had originally proposed to give parents and teacher the Child Behaviour Checklist and
Teacher Report Form to assess internalizing and externalizing behaviour. Given results from the
Haydicky et al., 2009 study that emphasized the role of ADHD symtomatology in moderating the
impact of MMA on behavioural outcomes, we decided to focus our evaluation on a measure of
attention and externalizing behaviour problems. The Conners-3 was completed by parents and
teacher before and after treatment. This measure assesses inattentive, hyperactive and impulsive
symptomatology.
Administering the teacher questionnaires presented numerous challenges. First, many youth
were starting high school or were in high school but had new teachers who were not adequately
familiar with their behavior. As such, we waited three weeks into MMA to distribute the teacher
questionnaires. To improve questionnaire return rates, youth received points toward their belt if their
teacher questionnaires were returned. Despite reminders to parents and youth, return rates were very
low, with only 8 teachers completing the questionnaire pre- and post-treatment. Given these low return
rates this measure was not included in our findings and is discussed further under methodological
limitations.
Data Analysis
Paired-sample t-tests or Repeated Measure Analysis of Variance (ANOVAs) were completed
to examine changes from pre- to post- treatment for each of the measures. Given the heterogeneity of
presenting mental health concerns, the presence of significant symptoms on the ADHD-inattentive
and hyperactive-impulsive subscales of the Conners-3 were examined as a moderator. Given that our
sample contained boys and girls at both beginner and advanced level MMA, gender and level of MMA
were also examined as potential moderators.
Results
Self-Awareness of Emotions and Thoughts
Paired sample t-tests were completed to determine if the proportion of cognition and emotion
words used by youth when talking about negative and positive emotional experienced increased from
Mindfulness Martial Arts 18
pre- to post-treatment. Youth were more likely to use emotion words in the pre-than post-treatment
interview and these words were more likely to reflect anger rather than anxiety or sadness.
Interestingly, while the youth used significantly fewer emotion words in the post-treatment session,
their use of cognitive words significantly increased. Furthermore, they used more sadness and anxiety
words than in their pre-treatment interview, while anger word use did not significantly change (see
Figure 1, Appendix D). Repeated measures ANOVAs indicated that gender, level of MMA (beginner or
advanced), and ADHD status did not significantly moderate these results. These results suggest that
while youth are aware of anger emotions at the beginning of treatment, they may have less
understanding of emotions relating to sadness and anxiety, which may at times underlie anger
responses. As youth become better able to identify and differentiate their emotions, they are able to
identify sadness and anxiety more readily. These results further suggest that youth make a transition
from using emotion labels to using both emotion and cognitive labels. This suggests a deeper level of
self-understanding.
Repeated measures ANOVAs were completed to determine if youth reported a higher level of
acceptance of thoughts and feelings and mindfulness from pre- to post-treatment. While scores on the
CAMM were found to increase, the difference from pre-test (M = 13, SD = 5.95) to post-test (M =
13.85, SD = 5.84) was not significant.
In addition to highlighting changes in self-awareness as a result of MMA, these results suggest
that the measurement tool selected is important. For youth with LDs, questionnaire measures that
require them to reflect on their mental experience may be less sensitive than performance-based
measures that reflect their use of a specific skill.
Behavioural Regulation
Repeated Measures ANOVAs were completed to examine changes in impulsivity (as
measured by the TOVA Commission error score) and attention (as indicated by the TOVA Omission
error score) pre- to post-treatment. Results indicated that youth in the Beginner group made significant
improvements in impulsivity from pre- to post-treatment (TOVA Commission errors, F (1,21)=4.68,
p=.04, Figure 2, Appendix D). Youth in the advanced program did not show significant changes in
Mindfulness Martial Arts 19
impulsivity, F (1,10) = 0.08, ns). No significant differences were found for changes in attention (TOVA
Omission errors) from pre- to post-treatment for either the beginner or advanced groups. Given the
high rates of co-occurring ADHD symptomatology in our sample, we examined if having clinically
significant levels of hyperactive-impulsive symptoms on the Conners-3 moderated changes in
impulsivity. Results confirmed this hypothesis. Only youth with these symptoms demonstrated
significant decreases in impulsivity (F (1,18)=6.93, p=.02).
Repeated Measures ANOVAs were also completed for the D-KEFS Trail Making Test –
Number letter switching task controlling for motor speed (Delis, Kaplan, Kramer, 2001) to assess for
changes in cognitive flexibility. Significant improvements were found from pre- to post-treatment (F (1,
30) = 4.85, p=.03). When MMA level (beginner vs. advanced) and gender were examined as
moderators of outcome, no significant differences by group were found. Furthermore, ADHD
symptomatology did not significantly moderate results.
Youth also completed an emotionally charged information processing task (Emotion
Interference Task) to determine if youth made gains in emotion regulation ability. Paired-sample t-
tests indicated that there is a trend toward youth making significant gains in reaction times for negative
pictures (pre M = 3860, SD = 1197, post M = 3477, SD = 977, t (33) = 1.91 p=.06), suggesting that
youth improved their ability to process negative emotional material and regulate the associated
emotion. When reaction time for neutral pictures was controlled for, the reaction time remained higher
after treatment, but was not significantly different. Reaction times did not significantly differ from pre-
to post-treatment on positive or neutral pictures, suggesting that gains made in information processing
of emotional material are specific to the negative domain (the area targeted by MMA). Gender, MMA
level (beginner vs. advanced), and ADHD symptomatology did not significantly moderate results.
Parents also reported significant changes in behavioural regulation on the BRIEF. For
beginner and advanced levels, parents completed a questionnaire examining executive functions
(BRIEF). Paired t-tests indicated that youth made significant gains in both behavioural regulation (t
(24) = 2.42, p=.02) and meta-cognition (t (24) = 2.78, p=.01). On the individual subscales, significant
differences were only indicated for emotional control (t (24) = 2.52, p=.02). When beginner and
Mindfulness Martial Arts 20
advanced groups were examined separately, only the beginner group showed significant gains from
pre- to post-test for behavioural regulation (t (16) = 2.80 , p=.01) and meta-cognition (t (15) = 2.25 ,
p=.04). See Table 1, Appendix D.
Taken together, these results suggest that youth make significant gains in the area of
behavioural regulation, including impulsivity, cognitive flexibility, and emotion regulation. It is
interesting to note that parents only reported differences for beginner level MMA youth while MMA
level did not significantly moderate most performance-based measures. It is possible that this
difference is reflective of a change in perceived level of impairment and behavioural regulation rather
than behavioural regulation alone and that perceived impairment may be change more significantly at
the beginner than advanced levels (McAuley, Chen, Goos, Schachar, & Crosbie, 2010).
Attributions of Control
Repeated Measures ANOVAs were used to assess changes in attributions of control. No
significant differences were found between pre- and post-treatment for positive attributions (internal,
global, stable and totals subscales). For negative attributions, no significant differences were found
from pre- to post-treatment for internal, global, and totals subscales. Contrary to our hypotheses,
youth attributions about negative events being stable significantly increased from pre- to post-
treatment (F (1, 32) = 9.27 p=.005). These differences were not significantly moderated by level
(beginner or advanced), gender, or presence of significant ADHD symptomatology. This result is
contrary to the lessons of MMA and is not consistent with the reports of youth in the qualitative
evaluation detailed below. It is possible that the self-report questionnaire format of this questionnaire
may have influenced the results.
Externalizing Behaviour Problems
To examine changes in externalizing behaviour problems, paired-sample t-tests were
completed for each of the subscales of the Conners-3. These analyses indicated no significant
changes pre- to post-treatment (see Table 2, Appendix D).

Mindfulness Martial Arts 21
Study 2: Qualitative Evaluation
The qualitative evaluation involved individual, in-depth interviews with 6 students and 5
parents. Interviews followed a semi-structured guide that was developed by the research and MMA
clinical team. Parallel forms of the same question were developed for each group interviewed (see
Appendix E).
Participants
In February 2010 (end of first session of MMA), a poster inviting families to participate in
interviews about their experience in MMA was posted in the dojo (waiting room area). Families were
also contacted by phone and invited to participate. We attempted to have a representative sample of
students from all MMA classes (beginner and advanced) and with different mental health presenting
problems (4 with LD and ADHD, 2 with LD and anxiety and peer relation difficulties).
Procedure
Youth and/or parents were invited to come to Integra to complete the interview. Interviews
were conducted by Emily Case, Psychology Consultant, who had been trained in qualitative research
as part of our previous Evaluation Implementation Grant from the Centre. Consent was completed
with each family (see Appendix E). Interviews were audiotaped and ranged from approximately 30
minutes to 1.5 hours long. Interviews were transcribed verbatim by a transcription service. Using a
grounded theory framework, Dr. Karen Milligan and Emily Case analyzed all transcripts and identified
common themes. The use of two psychology staff to discuss themes that emerged allowed for
“investigator triangulation” (i.e., the use of two or more investigators to examine the same
phenomenon) in interpreting the data; such collaboration can reduce the risk of biased interpretation
that could occur if only one individual were to analyze the data. The goal of the analyses was to
extract categories or themes that emerged directly from what the participants had to say and were
thus grounded in the data. This allowed for a much richer understanding of the processes being
investigated than could be afforded by quantitative data alone. A visual framework was developed to
Mindfulness Martial Arts 22
capture the themes and the inter-relations. The framework was shared with MMA clinical staff and
feedback and thoughts about interpretation was encouraged and integrated into the model.
Results
Multiple outcomes and processes were identified that were quite consistent with the beliefs of
clinical staff. Given the significant similarities and overlap between parent and youth interviews, a
single theoretical model for MMA was developed based on themes extracted from parent and youth
interviews. See Figure 3, Appendix D.
Youth came into the program with diverse presenting issues, including peer and family relation
difficulties, anxiety, impulsivity, inattention, and anger regulation. Using martial arts to engage youth in
treatment was consistently viewed as important by parents and youth.
“…You know, at first I was a tad skeptical that they could disguise behaviour modification inside a martial arts program but I’m amazed, I mean it’s a perfect fit and I see it now. I get
it…”
Many of the youth discussed their desire to develop mastery in a socially valued activity.
“Well I just wanted to have a feeling of pride. I just kind of needed some pride. I needed…I wanted to get a good feeling in me to have accomplished something important and I’ve been working hard.” “Oh yeah, like it feels rewarding I guess, like when you do achieve, like when you learn, like when you get down a certain move.”
The relationship with the therapist or “sensei” was also described as being essential to the MMA
process.
“I love [sensei], I think he is amazing, he knows his stuff so well. He is so good with the boys, he is so good with my son, he is so good with me. I love [sensei], I just think he really knows what he is doing. [My son] really wanted to take martial arts, even before we know of this program, so I guess he can get martial arts at the same time as what [sensei] calls back door therapy.”
The Sensei was not seen as a therapist.
“MMA and more or less {sensei] kind of gave me little things, helped me, encouraged me. A
mentor, kind of.”
Mindfulness Martial Arts 23
The youth and parents reported that youth felt heard, respected, and safe.
“He had great respect for [sensei]. So, the rest was easy.” “And there’s no, you know, there should never be judgment in therapy, but with [sensei] you really do not feel any judgment and I know [youth] doesn’t at all. [Youth] doesn’t see [sensei] as a therapist and that’s a good thing.”
“I think part of it is the instructors. I think because he, he just doesn’t let things, I don’t think,
just kind of go, but yet he comes across as an ally as opposed to someone who is…Where I
think with the class, he’s heard. The instructors have more experience with the kids in this way.
They allow them to speak their mind, but at the same time make them also listen to, say, the
other side so that the child understands that there’s, it goes both ways.”
“And I like that he’s taking it at a place that I think is safe.”
A number of parents noted that the therapeutic relationship between the student and the sensei was
strength-based and one that fostered mastery motivation and the belief that students could be
successful.
“I think it’s that whole idea of the flexibility and perseverance, knowing that something is tough but they still need to put that effort into it and they’ll see successes.” “I think for what I see it’s the whole perseverance, the idea of if things get tough you still have to keep plugging away at it. To me, that’s the one message that comes across. So, it could be if they’re talking about a move in the martial arts that you have to…it might take a bit of practice or whatever, but also that idea spills over into your whole life, especially of course into school which is where they struggle with their learning disabilities. But it’s like a life skill and I kind of feel that, to me, that’s the main thing that I got that I felt was best.”
The importance of relationships also extended to peers and the importance of being part of a social
group.
“I think that sense of belonging to a group and feeling that they’re like him. Because a lot of kids he deals with he feels they’re really different and they either look down on him or [are] aggressive towards him or he doesn’t relate to them, doesn’t know how to interact with them and become friends with them. He desperately wants to have friends and he’s the kind of kid that just didn’t know how to do it and he thought it would impress to talk a lot. Here he’s learned to be quiet and mindful.”
Mindfulness Martial Arts 24
“While they’re in that classroom those kids are normal again. I mean, they’re with a gang of kids who are like them, who have similar problems, and they empathize with each other and they care for each other.”
The inclusion of parents in the supportive milieu was also viewed as essential, particularly from the
parents' perspective. Many parents requested that this be continued at the Advanced level.
“But the involvement of the parents, it really gets us part of it and helps us support it because we understand it, and understanding what is trying to be accomplished each week and what the things he’s doing or supposed to be doing. It makes us feel comfortable about what’s happening and it helps us understand what we need to do to support what he’s doing. There’s brilliance in that sense, that it involves the parents I think in a really constructive, appropriate fashion.”
Taken together, this engaging and supportive therapeutic milieu formed the foundation for the
implementation of the treatment components. The mindful moment was regarded as the most helpful
mindfulness strategies taught. Youth and parents reported that the mindful moment helped them
become more self-aware and calm and be present in the moment.
“A mindful moment is when you stop and breathe and reflect so you can become aware of what you’re feeling. It makes me feel better, being aware and know that thinks will change. Everything changes, nothing stays the same. That’s what I live by.”
“Yeah, I guess because when you’re meditating that’s what you’re thinking, like, you notice thoughts that enter your mind and then you have to go back to being, just being with everything, so you know of just realized everything that’s going on around you.” “I have ADHD so I get hyper and the mindfulness helps in keeping me calm.” “I guess we saw the mindfulness part of it was an important component in that he would learn how to sit back and accept what was going on and take responsibility for what was happening in his life and learn how to look at it in a way that he would be able to influence his life and gain more sense of ability to influence his world.”
From this place of self-awareness and calm, youth found that they were able to use mindful self-talk
and the “Be” mantra to help them cope with challenging thoughts, feelings, and situations.
“Well one of the big things we did in class is just be. So, you have to be with…like, if you’re upset, you “Just Be” with it. And as I said before, you realize why you’re upset. You don’t need to change it or anything. It’s just being with your upset and not trying to change. Like saying, oh, I’m all happy and stuff when you’re upset. That will cause stress.”
Mindfulness Martial Arts 25
Parents reported that they found that their children were better able to consider the perspective of
another.
“…he’s more in tune with realizing how people think I guess and how people are. I think it comes from that whole mindfulness thing because they talk so much about it and all the mantras are so inclusive.” “…and he just seems to be much more in touch with emotions in general, whether it’s his or maybe other peoples.”
Mindful self talk and the “Be” mantra, as well as the ability to take the perspective of others was
associated with a number of positive outcomes, including the ability to stop and think before acting
and being able to change typical response patterns and try new ways of responding.
“…but there was an instance [Youth] got really mad, and we got mad at [Youth], my husband and I, and he got really mad at us, and I said to [Youth] don’t yell at me, speak to me. And he stopped, and this is what [Sensei] teaches them, to stop, and he told me exactly, he verbalized what he was feeling; he’s never done that in his life. He told me what I was doing that was making him angry and he was able to tell me and he was able to calm down and I attribute that to MMA.” “I let certain things slide rather than getting all defensive.”
While improvement in self-awareness and behavioural regulation was common among
participants, the outcomes of this improvement differed depending on the presenting needs of the
youth. Parents and youth reports included improved relationships with peers, parents, and siblings,
fewer behavior problems at school, ability to persist with challenges in schoolwork, standing up for
themselves with bullies, and being seen as more mature by adults. Parents and youth all indicated
that change took time and that many goals were still in progress. Most reported that changes were not
apparent until approximately two thirds through the group.
Overall, the qualitative interviews with the parents and youth supported Integra’s hypotheses
about the processes of change and the importance of finding a way to engage youth. These results
are also consistent with the quantitative findings in Study 1 that reflect increased self-awareness and
behavioural regulation.
Mindfulness Martial Arts 26
Study 3: Process Evaluation
Three main process indicators were selected for the present study: verification of learning
disability, client satisfaction and impressions of MMA, and examination of treatment fidelity.
Verification of Learning Disability Diagnosis
All youth participating in MMA had a psychoeducational assessment completed prior to coming
to Integra. As part of our intake process, Integra Intake Worker, Judy Schutt, reviewed all assessment
to ensure that the child had formally been given a diagnosis of a learning disability. If a formal
diagnosis had not been met, Dr. Karen Milligan, Director of Research and Psychology, reviewed the
file to determine if the youth met Integra’s LD criteria, including: (1) average to above average
intellectual functioning; (2) significantly lower academic functioning than would be predicted on the
basis of intelligence; and (3) impairments in at least one of the processes contributing to learning,
such as phonological processing, memory, or visual-motor coordination. All youth who participated in
the present study met these criteria.
Client Satisfaction and Impressions of MMA
During the final session of the MMA program, youth in the beginner and advanced programs
were asked to complete a questionnaire to assess their impressions of the program and the gains they
had made. Parents of the beginners completed a similar questionnaire. Overall, student and parent
questionnaire results are presented below. See Appendix G for questionnaire and separate summary
for beginner and advanced youth.
Youth Evaluation of the MMA
Based on the MMA Student Evaluation (n = 53), students at the Beginner and Advanced levels
reported enhanced self-awareness upon completion of the program. After MMA, students reported a
greater tendency to recognize personal thoughts and feelings. Following MMA, students enhanced
their understanding of the importance of practice and the concept that things and thoughts may
change. Prior to the program, 43.4% of students reported a limited ability to accept both good and bad
things. After participation, 41.5% and 35.8% of students subsequently felt able to do so most or all of
the time, respectively. In comparison to 24.5% of respondents who initially felt responsible for their
Mindfulness Martial Arts 27
success sometimes, 54.7% of students assumed full responsibility after the program. Students also
reported an increased tendency to recognize personal “mean” behaviour, as well as the ability to stop
and think before acting. Generally, students rated martial arts as their favourite component of the
program. They enjoyed being part of a club and valued the stripe system and certificates. The mindful
moment was reported to be their least favourite component of the program. Students found the class
schedule to be suitable and their level of enthusiasm to attend sessions increased over the duration of
the program.
Parent Evaluation of MMA
Based on the MMA Parent Evaluation (n = 17), parents observed greater confidence and enhanced
self-awareness in youth upon completion of the program. After MMA, parents reported that youth were
more likely to think before acting and to persist when faced with difficulties. Before the program,
35.3% of parents felt that their child rarely adapted to challenging situations. Subsequently, 83.3%
suggested that their child demonstrated adaptability some or most of the time. Parents also reported
that their child was now getting along well with others, feeling responsible for personal success and
feeling good about themselves more consistently. Following MMA, the proportion of parents who felt
their child sometimes expressed thoughts and feelings appropriately increased from 47.1% to 64.7%,
and an additional 29.4% of parents felt their child was doing so most of the time. Overall, parents
found individual meetings with the MMA instructor to be the most beneficial, followed by martial arts
practice, the meditation CD, parent orientation, and charting target behaviour. Parents identified
situation exercises as being the least helpful component. Most parents thought the class schedule
was suitable and 88.2% would recommend MMA to a friend’s child.
Treatment Fidelity
Given the exponential growth of MMA during the past few years and the expansion in the
number of therapists leading groups, we were interested to examine if the groups were being
implemented as intended, both in terms of treatment delivery and treatment adherence. To assess
these areas, the research team met with MMA developer, Paul Badali, to review the manual and to
discuss key elements of treatment adherence, which included relational (e.g., providing praise),
Mindfulness Martial Arts 28
instructional (e.g., use of role play or modeling) and physical characteristics (e.g., lights out, use of
bell). A Research Opportunity Student from the University of Toronto (Jessica Suddaby), who has a
strong background in martial arts and was completing an undergraduate degree in psychology, was
trained on the coding system by Dr. Karen Milligan. Once a high level of agreement was established
(i.e., over 80% in all areas), four sessions of 20 (representing 20% of sessions) across all three MMA
leaders (total 12 sessions) were randomly chosen and coded. An additional coder coded 25% of these
sessions to ensure adequate levels of inter-rater reliability. Inter-rater reliability was 84% for treatment
adherence and 100% for treatment delivery. Results of the inter-rater reliability differences for
treatment adherence were helpful in identifying areas where more clarity was required in the MMA
manual.
To assess levels of treatment fidelity, percent adherence was calculated for each of the 4
sessions across the three MMA leaders. There was a high level of fidelity across the three group
leaders in terms of their style of treatment delivery (94% to 98%). Differences typically reflected
physical characteristics, such as having the lights turned off during meditation or using the bell.
Consistent with these findings, when instructor was examined as a moderator of gains made on
quantitative measures, no significant differences were found. This suggests that gains made by
participants are not dependent on which of the three therapists led their class.
A good level of treatment adherence was also found (81%). It is important to note that the main
difference between instructors was on the types of martial arts skills taught. This result was
anticipated as therapists need to assess the level of ability of their students and teach in a graduated
manner that places skills to be learned at or just above their level of ability. This ensures a high level
of success and promotes engagement in treatment.
Methodological Strengths and Challenges
There were a number of methodological strengths and challenges in this research. Improving
methodology was an important objective of this study. Certainly, results support our hypothesis that
performance-based measures, such as the D-KEFS Trails, TOVA and Interviews, are more sensitive
to the changes youth made than self-report questionnaires (e.g., CASQ, CAMM). Given the academic
Mindfulness Martial Arts 29
and processing difficulties many youth with LDs face, coupled with the potential for difficulty reflecting
on their experiences with accuracy, these measures may be less valid. This is consistent with
research on youth with LDs that showed that such individuals tend to exhibit a positive illusory bias
when completing questionnaires about their challenges (i.e., they report they are doing better than
they are; Haydicky et al., 2009).
We had also planned to improve on our previous studies by including information on youth at
school, from the perspective of their teachers. Unfortunately, this was extremely difficult and we were
only able to obtain complete data from 8 of our participants. Many of our youth were entering Grade 9
in September and did not know any of the teachers at their new school. However, return rates were
also low for youth who could identify a teacher. Providing teachers with an incentive (e.g., free
admittance to our community consultation workshops) may be helpful for future studies. We have also
started administering questionnaires on a secure online site. This has been helpful in increasing
parent questionnaire completion and may similarly be helpful for teachers.
As indicated in the qualitative model, youth came into MMA with a diverse range of goals and
presenting challenges and left the program having made gains in an equally diverse range of areas.
Examination of youth goals from the client satisfaction surveys also mirrored this heterogeneity. This
diversity presented tremendous challenge for selecting key behavioural outcomes, as some youth
present with these difficulties and others did not. While we were able to examine the potential
moderating role of presenting problems, such as ADHD, our sample was too small and diverse to
examine all presenting problems, including anxiety, Asperger syndrome, and peer relation difficulties.
It is possible that this heterogeneity may have contributed to the lack of significant findings on the
outcome measure examining externalizing behaviour, as this may not have been a presenting concern
for all youth. A general measure that examines a broad construct such as resilience or general level of
functioning may be more likely to capture the diverse ways in which youth enact the processing
changes made.
Finally, the cohort (pre-post) design of the present study does not account for changes that
youth may have made over time without treatment. Our clinical observations suggest that outcomes
Mindfulness Martial Arts 30
for many youth tend to get worse without treatment, particularly during the transition to high school.
Future research using a randomized control design is needed to better understand the impact of
MMA.
Discussion & Lessons Learned
Enhancing Interest, Knowledge and Capacity for Research and Program Evaluation at Integra
This evaluation project was an excellent experience for all staff at Integra in terms of
generating knowledge and interest in program evaluation. Progress with and results of the evaluation
were shared with staff throughout the course of the grant in the form of research meetings that
included the MMA supervisor (Paul Badali), clinical team meetings, staff meetings, and board
meetings. This has assisted in creating an interest in evaluation for many of the staff and moreover a
culture of curiosity. By the end of this project, the staff appeared more interested in research and
program evaluation and the research team is now much more integrated into the clinical team. The
Director of Research and Psychology attends bi-weekly clinical team meetings and provides updates
on the research, as well as receives essential feedback from the front-line staff. Program evaluation
activities are currently being undertaken in many of our group programs and clinicians are
independently seeking out support from the Integra research team to assist them in developing client
satisfaction surveys (e.g., Young Warriors program for 9 to 11 year olds with ADHD and emotion
regulation difficulties) and needs surveys to inform the development of new programs (e.g.,
development of a parenting program).
Development of Relationships with Stakeholders to Support Future Research in MMA
At the outset of this project, we were fortunate to have a strong network of stakeholders to
assist with this project. For example, Judy Weiner (Integra Board Member and Professor at the
University of Toronto) was helpful in providing information on attribution measures and providing
guidance based on her previous evaluation of MMA. Jill Haydicky, a graduate student at the University
of Toronto who completed her MA thesis on MMA, assisted with participant testing, scoring and data
collection. Three other students from the University of Toronto also assisted with these tasks, one of
which was an undergraduate research opportunity program student. This was an excellent opportunity
Mindfulness Martial Arts 31
for students to learn more about youth with learning disabilities and develop program evaluation skills.
In addition to further developing our relationship with the University of Toronto, we were able to
expand our stakeholders to include Dr. Maggie Toplak from York University. Dr. Toplak provided
guidance in terms of the selection of measures to evaluate cognitive flexibility. Since this initial
consultation, she has joined the Integra board and is now a member of our Research Committee. We
also had the opportunity to discuss methods for coding treatment fidelity with Dr. Leena Augimeri of
the Child Development Institute, a children’s mental health agency in Toronto. Development of this
relationship has been helpful in terms of sharing resources on writing contracts for university
partnerships and measuring the progression of services toward evidence-based status. This research
relationship has also helped to consolidate collaboration and good will between our children mental
health agencies at a broader systems level.
In addition to these stakeholders, we have established a number of new relationships with
researchers that will assist us in furthering our research on MMA. Based on preliminary evidence
showing the promise of MMA as an effective intervention for youth with self-regulation difficulties, we
recently developed a research team that will examine the effectiveness of MMA for youth with
Asperger Syndrome and self-regulation difficulties. This team includes Dr. Wendy Roberts, an expert
in Autism at the Hospital for Sick Children and Dr. Louis Schmidt, an expert in psychophysiological
measurement of emotion regulation from McMaster University who will assist us in examining if MMA
has an impact on youth at the biological level.
Enhancement of Knowledge of MMA and Key Processes to Consider in Treatment of Youth
with LDs
Given that our Clinical Director and Director of Research and Psychology (Members of Senior
Management, Dr. Phillips and Dr. Milligan) are relatively new to Integra, this project provided us with
the opportunity to examine MMA in a more in depth manner. We were able to bring this information to
Integra Senior Management (with the assistance of MMA developer and supervisor, Paul Badali) to
inform treatment planning discussions regarding the management of the growth of the program (e.g.,
Mindfulness Martial Arts 32
staffing, space, number of groups youth can attend) and planning for its wider dissemination (e.g.,
treatment manual revision).
Our work on this study has also highlighted the importance of targeting emotion regulation in
our treatments for youth with LDs and reinforced some of our assessment and treatment practices.
For example, we use emotion and behaviour regulation ability as factor of triaging youth into specific
social competence groups. David Jurasek, a child and family therapist and MMA leader has also
developed Young Warriors, based on some of the components of the MMA program, to target emotion
regulation skills in children aged 9 to 11 with ADHD and emotion regulation difficulties.
Challenges in Balancing Clinical Needs and Research Protocol
While Integra staff and stakeholders worked very well during the course of the project, some
challenges were experienced in trying to balance clinical needs of the agency and the research
protocol. For example given limited staffing and space, the number of youth involved in the beginner
program was minimized by the number of youth enrolled in the advanced program. Males and
females were also integrated in the winter session, whereas they were separated in the fall session.
While differences were not indicated between our male and female participants on the measures
completed, the integration of genders could still have impacted the program and this program change
is therefore a possible confound.
Relationship with the Centre for Excellence in Children’s Mental Health
We found the Centre to be exceptionally helpful, particularly in terms of providing support for
the qualitative component of the study and discussing knowledge translation and exchange activities.
The regular check-ins provided Integra staff with opportunities to share progress with Centre staff and
to incorporate ideas in a timely fashion. There were no specific recommendations for the Centre.
Conclusions and Recommendations
Mindfulness Martial Arts is an innovative treatment for youth with learning disabilities and co-
occurring mental health disorders that has been operational for 8 years. Using a mixed method
design, we addressed three objectives: (1) to extend findings from our previous evaluations by
Mindfulness Martial Arts 33
examining the impact of MMA on three key processes of change (e.g., self-awareness, behavioural
regulation, and attributions of control) that may promote mental health outcomes; (2) to examine
performance-based measures of processes that may be more sensitive to change than traditional
questionnaire measures; and (3) to determine if MMA is implemented consistently across different
groups and therapists. Overall, the findings were positive and support the promise of MMA as an
effective intervention. In addition to stimulating interest and increasing knowledge of program
evaluation at Integra, this project enhanced our knowledge of key processes that may underlie the
diverse behavioural outcomes made by youth, including self-awareness, behavioural regulation, and
therapeutic milieu, and stimulated discussion about how long youth should remain in treatment.
MMA Increases Self-Awareness and Behavioural Regulation
Increasing self-awareness and developing emotional and behavioural regulation skills is
considered to be a key component of MMA. Based on his experience working with youth with LDs and
the literature, Paul Badali, the developer of MMA, has suggested that youth must learn to be present
with their experience before they are able to effectively implement cognitive and problem-solving
strategies that are common to many empirically-based/informed mental health treatments. In the
current study, interviews with youth and parents suggested that MMA assisted them in becoming more
self-aware, calm and present in the moment. It is from this state of “calm” that youth reported that they
were able to use self-talk and mantras and perspective-taking to assist them in coping with the
challenge at hand. The impact of MMA on emotional and behavioural regulation was echoed in the
qualitative component of the study. Specifically, MMA was associated with significant improvements in
behavioural regulation on both performance-based measures and parent report measures. This
included significant reductions in impulsivity and significant improvements in cognitive flexibility and
emotion regulation. Furthermore, when speaking about stressful life experiences youth were able to
talk about a wider range of negative emotions and reflect more on the thoughts that may underlie
feeling or situations. Youth attributed gains in behavioural regulation and emotion control to the
mindfulness components of treatment (e.g., meditation, mindful moment), indicating that it impacted
Mindfulness Martial Arts 34
their self-awareness and that it enabled them to be calm, think straight, stop and think, and change
patterns of automatic responding.
While these findings confirm the impact of MMA on self-awareness and behavioural regulation
in youth, the process of completing this research and in particular creation of the logic model, measure
selection, and results interpretation, has helped staff at all levels to deepen their understanding by
better operationalizing these constructs. This has assisted Paul Badali in making improvements to the
manual to focus more on activities that target specific processes (e.g., inclusion of yoga, more
emphasis on mindful self-talk) and be more descriptive of the goal for each session and cohesive in
weaving it through the session components.
Engagement of Youth and the Importance of Milieu
Both youth and parents emphasized the importance of the MMA milieu, speaking about the
power of marital arts to engage youth in treatment through a “backdoor therapy.” Youth were intrigued
by martial arts and expressed their desire to achieve mastery in and be part of a socially-valued
activity. Discussion of these results with the MMA leaders reinforced these findings, with the
suggestion that youth appear to be pushing themselves to continue trying to master skills even when
faced with challenge. In addition to mastery, the relationship with the sensei (e.g., feeling heard and
safe, with clear expectations) was identified as paramount. These results have stimulated discussion
about treatment delivery in our other programs and the challenge of engaging children and youth while
decreasing the perceived stigma of receiving mental health care.
Beginner and Advanced MMA: How long is long enough?
Given the exponential growth of MMA, MMA therapists and Senior Management have been
trying to plan for growth. One of the major challenges we have faced is that supporting youth in
making behavioural changes that promote mental health takes time. As evidenced by the qualitative
interviews, youth and parents reported that it took at least 13 weeks before they began to see gains
and advanced youth noted that it was not until the advanced program that they began to really
consolidate the skills learned. These qualitative results support allowing youth to continue in MMA at
Mindfulness Martial Arts 35
the advanced level. The finding that there were no differences between beginner and advanced levels
on most of the quantitative measures also suggests that youth are making gains in these processes at
different times in the program depending on their needs. We, however, continue to be curious about
the length of involvement in MMA and when gains made may plateau. To address this issue, we
examined common measures that we had used in previous evaluations to determine if we could use
our larger database of information to inform this treatment decision. The only measure that was
common across our studies (due to updated versions of measures) was the BRIEF. Using the BRIEF
data, we are going to use multi-level modeling to address the question regarding length of treatment.
These analyses require large sample sizes and we still require more data on youth who have taken 3
or 4 sessions. We will continue to collect this data over the next year.
We also learned from parents how valuable the parent sessions are and that they would like
them to be continued at the advanced level. Management and the clinical team are currently
discussing strategies for keeping parents involved and informed about the content of sessions,
progress made and strategies for generalization. Strategies may include weekly email updates (as is
being used in our Young Warriors program) and monthly meetings with parents to review progress.
We will continue to provide reports to families at the end of each session to assist with maintenance
and generalization of skills and strategies learned.
Knowledge Exchange
This project is of high relevance to a number of partners and stakeholders. Knowledge
exchange has already begun and will continue over the next two years. As reported above, knowledge
exchange and translation involving all levels of staff at Integra was integrated throughout the research
process. Given the number of different measures used in the study, Integra staff have been receiving
updates on the findings of different measures during the last few months of the grant period. Similarly,
the results have been shared with the Integra Board research committee and they have played an
important role in interpreting findings and discussing future directions. A formal presentation of all
results is planned for December 2010 and will be presented to Integra staff and the Integra Board.
Mindfulness Martial Arts 36
Knowledge translation activities have also extended outside of Integra. The results of the
project have been shared with our newly formed team of researchers (Principal Investigator at Integra)
who are going to examine the effectiveness of MMA for youth with Asperger Syndrome and self-
regulation disorders. A comprehensive knowledge translation strategy has been integrated into this
study that will assist Integra in developing partnerships needed to complete an independent
randomized control trial of the program, an essential step in moving MMA towards evidence-based
status.
Through discussions with Senior Management, MMA leaders, and the Integra Board, the focus
of the MMA research team over the next year will be on dissemination. In November 2010, we will be
posting the results of our study on our website and will be sending a summary to families who
participated in the study. We have submitted conference presentation abstracts to the Biennial
Meeting of the Society for Research in Child Development (Montreal, April 2011; see Appendix H) and
plan to submit an abstract to the 18th National Conference on Learning Disabilities (PEI, September
2011). We also plan to write at least two papers for publication based on these findings and submit
them to peer-reviewed journals, such as Intervention in School and Clinic and The Journal of Learning
Disabilities.
In addition to the dissemination of research findings, we also are moving towards
disseminating MMA to clinicians outside of Integra. The assessment of treatment fidelity completed as
part of this study was essential to this endeavor. The process of completing the treatment fidelity
assessment and providing supervision highlighted important formatting changes for the MMA manual
that would improve standardized implementation. Paul Badali is currently completing these revisions.
When this is complete, Integra will plan our wider dissemination of MMA, including the possibility of a
train-the-trainer program.
In summary, the present study has incited optimism and excitement about the effectiveness of
MMA for youth with LD and self-regulation disorders. Integra staff are energized to move forward in
the process of dissemination and establishment of MMA as an evidence-based treatment.
Mindfulness Martial Arts 37
References Ayres, R., Cooley, E., & Dunn, C. (1990). Self-concept, attribution, and persistence in learning
disabled students. Journal of School Psychology, 28, 153-163. Badali, P. (2002/2009). Mindfulness Martial Arts. Unpublished Manual. Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review.
Clinical Psychology: Science and Practice, 10(2), 125-143. Barkley, R.A. (1997) Defiant Children: A clinician’s manual for assessment and parent training. The
Guilford Press Berking, M., Wupperman, P., Reichardt, A., Pejic, T., Dippel, A., & Znoj, H. (2008). Emotion-regulation
skills as a treatment target in psychotherapy. Behavior Research and Therapy, 46, 1230-1237.
Buodo, G., Sarlo, M., & Palomba, D. (2002). Attentional resources measured by reaction times highlight differences within pleasant and unpleasant, high arousing stimuli. Motivation and Emotion, 26, 123–138.
Cayoun, B. (2008). The role of somatosensory feedback in Attention Deficit Hyperactivity Disorder:
four cases treated with Mindfulness–integrated CBT. Presented at APS, Australia. Chawla, N., & Ostafin, B. (2007). Experiential avoidance as a functional dimensional approach to
psychopathology: An empirical review. Journal of Clinical Psychology, 63, 871–890. Delis, D. C., Kaplan, E., & Kramer, J. H. (2001a). Delis-Kaplan Executive Function System (D-KEFS).
San Antonio, TX: The Psychological Corporation. Fivush, R., Marin, K.A., Crawford, M., Reynolds, M., & Brewin, C.R. (2007). Children’s Narratives
and Well-being. Cognition and Emotion, 21 (7), 1414-1434. Gioia, G.A., Isquith, P.K., Guy, S. C., & Kenworthy, L. (2000). Behavior Rating Inventory of Executive
Function: Professional Manual. Lutz, FL: Psychological Assessment. Greco, L.A., Smith, G., & Baer, R.A. (2008). Children’s Acceptance and Mindfulness Questionnaire.
Unpublished Measure. University of Missouri – St. Louis. Greenberg, L. M., & Kindschi, C. L. (1996). T.O.V.A. clinical guide. Los Alamitos, CA: Universal
Attention Disorders, Inc. Gross, J.J. (1998). The emerging field of emotion regulation: an integrative review. Review of General
Psychology,2, 271-299. Gross, J.J. (2002). Emotion regulation: Affective, cognitive, and social consequences.
Psychophysiology, 39, 281-291. Haydicky, J. (2009). Mindfulness Training for Adolescents with Learning Disabilities. Unpublished
Masters Thesis. University of Toronto.
Mindfulness Martial Arts 38
Haydicky, J., Wiener, J., Badali, P., Ducharme, J., Milligan, K. (submitted). Mindfulness Training for Adolescents with Learning Disabilities.
Hayes, S., Wilson, K., Gifford, E., & Folette, V. (1996). Experiential avoidance and behavioral
disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64(6), 1152-1168.
Kashdan, T.B., Barrios, V., Forsyth, J.P., & Steger, M.F. (2006). Experiential avoidance as a
generalized psychological vulnerability: Comparisons with coping and emotion regulation strategies. Behavior Research and Therapy, 9, 1301-1320.
Lakes, K. & Hoyt, W. (2004). Promoting self-regulation through school-based martial arts training.
Applied Developmental Psychology 25, 283–302. Lang, E. J., Bradley, M. M., & Cuthbert, B. N. (2001). The international affective picture system.
Gainesville: NIMH Center for the Study of Emotion and Attention. Learning Disabilities Association of Canada (2002). Official definition of learning disabilities. Retrieved
July 22, 2009, from http://www.ldac-taac.ca/Defined/defined_new-e.asp. Learning Disabilities Association of Canada (2007). Putting a face on learning disabilities. Retrieved
July 2010, from Learning Disabilities Association of Canada (2002). Official definition of learning disabilities. Retrieved July 22, 2009, from http://www.ldac-taac.ca/Defined/defined_new-e.asp.
Lowe, K., Allen, D., Jones, E., Brophy, S., Moore, K., & James, W. (2007). Challenging behaviors: Prevalence and topographies. Journal of Intellectual Disability Research, 51(8), 625-636.
Mishna, F. (2003). Learning disabilities and bullying: Double jeopardy. Journal of Learning
Disabilities, 36, 336-348. Moses, E.B., & Barlow, D.H. (2006). A new unified treatment approach for emotional disorders based
on emotion science. Current Directions in Psychological Science, 15, 146-150. Ortner, C. M. N., & Kilner, S., & Zelazo, P. D. (2007). Mindfulness meditation and emotional
interference in a simple cognitive task. Motivation and Emotion, 31, 271-283. Ortner, C. N.M., Kilner, S.J., & Zelazo, P.D. (2007). Mindfulness meditation and reduced emotional
interference on a cognitive task. Motivation and Emotion, 31, 271-283. Pennebaker, J.W., Booth, R.J., & Francis, M.E. (2007). Linguistic Inquiry and Word Count (LIWC). Raes, F., Hermans, D., de Decker, A., Eelen, P, & Williams, J. (2003). Autobiographical memory
specificity and affect regulation: an experimental approach. Emotion, 3, 201-206. Seidman, L. J., Biederman, J., Monuteaux, M. C., Doyle, A. E., & Faraone, S. V. (2001). Learning
disabilities and executive dysfunction in boys with attention-deficit/hyperactivity disorder. Neuropsychology, 15(4), 544-556.
Semple, R. J., Reid, E. F. G., & Miller, L. (2005). Treating anxiety with mindfulness: An open trial of
mindfulness training for anxious children. Journal of Cognitive Psychotherapy, 19, 379-392.
Mindfulness Martial Arts 39
Silver, C.H., Ruff, R.M., Iverson, G.L., Barth, J.T., Broshek, D.K., Bush, S.S., Koffler, S.P. & Reynolds, C.R. (2008). Learning disabilities: The need for neuropsychological evaluation. Archives of Clinical Neuropsychology, 23, 217-219.
Singh, N. N., Lancioni, G. E., Singh Joy, S. D., Winton, A. S. W., Sabaawi, M., Wahler, R. G., Singh, J.
(2007). Adolescents with conduct disorder can be mindful of their aggressive behavior. Journal of Emotional and Behavioral Disorders, 15(1), 56-63.
Strauss, E., Sherman, E.M.S., & Spreen, O. (2006). A compendium of neuropsychological tests:
Administration, norms and commentary (3rd ed). New York: Oxford University Press. Thompson, M., Kaslow, N.J., Weiss, B., & Nolen-Hoeksema, S. (1998). Children’s Attributional Style
Questionnaire-Revised: Psychometric Evaluation. Psychological Assessment, 10, 166-170. Thompson, R.A. (1994). Emotion regulation: A theme in search of a definition. Monographs for the
Society of Child Development, 59, 25-52. Wegner, D.M. (1994). Ironic processes of mental control. Psychological Review, 101, 34-52. Weiser, M., & Kutz, I., & Kutz, S., &Weiser, D. (1995). Psychotherapeutic Aspects of the Martial Arts
[Electronic Version]. American Journal of Psychotherapy, 49, 118-127. Wiener, J. & Schneider, B. (2002). A multisource exploration of friendship patterns of children with
learning disabilities. Journal of Abnormal Child Psychology, 30(2), 127-141. Wiener, J. & Sunohara, G. (1998). Parents' perceptions of the quality of friendship of their children
with learning disabilities. Learning Disabilities Research and Practice, 13, 242-257. Wiener, J., Harris, P. J., & Shirer, C. (1990). Achievement and Social Behavioral Correlates of Peer
Status in Children with Learning Disabilities. Learning Disability Quarterly, 13, 114-127. Willcutt, E.K. & Pennington, B.F. (2000). Comorbidity of reading disability and attention-
deficit/hyperactivity disorder: Differences by gender and subtype. Journal of Learning Disabilities, 33, 179-191.
Zivin, G., Hassan, N.R., Depaula G.F., Monti, D.A, Harlan, C., Hossain, K.D.&Patterson, K. (2001). An
affective approach to violence prevention: Traditional martial arts in middle school. Adolescence, 36, 443-459.
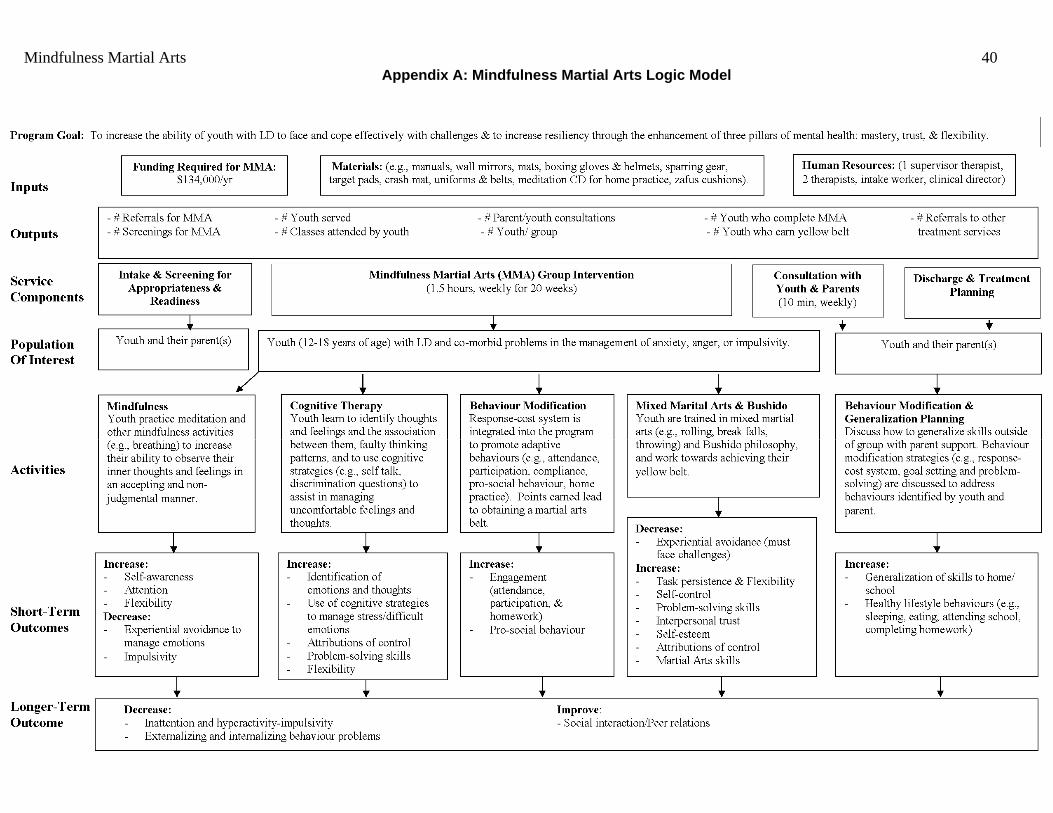
Mindfulness Martial Arts 40 Appendix A: Mindfulness Martial Arts Logic Model

Mindfulness Martial Arts 41
Appendix B: Information Letters and Consents
January 21, 2010 Dear Parent/Guardian/Study Participant: Over the past couple of years, we have been conducting a formal program evaluation of the Mindfulness Martial Arts (MMA) program developed by Paul Badali, Child and Family Therapist at Integra. The purpose of this research has been to better understand the gains youth make while in the program and to further develop and improve MMA. To date, results of this research are positive. Youth who participate in MMA show improvements in areas such as flexibility in dealing with challenges, organization, attention, and impulsivity. This winter, we are completing a more in depth study that will examine if MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour. This study is headed by Dr. Karen Milligan, Director of Research and Psychology at Integra, and is funded by a grant awarded to Integra by the Provincial Centre for Excellence in Child and Youth Mental Health. We would like to invite you to take part in this study. Participation will involve completion of questionnaires by youth and their parents at the beginning (February 2010) and end (June 2010) of the MMA program. Youth will also be asked to participate in an individual interview at these times. During this interview they will be asked about challenging and successful situations they have experienced, to complete some computer games, and to look at a series of emotional pictures. The interview will take approximately 1.5 hours. We will also ask you to have your child’s teacher complete two questionnaires at the beginning and end of MMA so that we can examine if the benefits of MMA extend to the school setting. If you and your child decide to participate, your interview and information will be kept confidential and will only be reviewed by those directly involved in the research. All of the data collected for this study will be securely stored by the researchers at Integra. Any research reports that result from this study will be in a group format, with all identifying information of participants removed. Videotapes will be destroyed following completion of the study. Participation in this research is voluntary. If you decide not to participate, it will not impact on the services that you and your child receive at Integra and you may decide at any time to withdraw your permission. Other than investment of time, there are no known risks associated with participation in the study. One potential risk is that some youth may feel some discomfort when talking about challenging situations or answering questions about their feelings, thoughts, or behaviour. Youth will also be asked to view some emotional pictures for approximately 5 seconds each. These pictures are part of an International Affective Picture System that has been used in research with children as young as age 7. It is possible that some youth may experience some discomfort from these pictures. We will discuss this potential risk with youth during the consent procedure. They will be told that they may skip any question/picture, request a break, or withdraw from the study at any time without penalty. Parents and youth are encouraged to speak with Integra Child and Family therapists if they require further support. We believe that this research will make an important contribution to our knowledge about the treatment of social-emotional difficulties associated with learning disabilities and to the further development of the MMA program. We would be grateful for your participation. If you have any questions, or if you would like additional information, please call Paul Badali, MMA Program Leader (416- 486-8055 ext. 228) or Dr. Karen Milligan, Director of Research and Psychology (416-486-8055, ext. 232). Thank you for your consideration of this request. Sincerely, Paul Badali, M.S.W., RSW Dr. Karen Milligan, C. Psych. Program Leader Director of Research and Psychology
Mindfulness Martial Arts 42
MINDFULNESS MARTIAL ARTS (MMA) EVALUATION INFORMED CONSENT – PARENT/GUARDIAN
√ I understand that Integra staff members are interested in hearing from youth and parents about their impressions of MMA and learning more specifically about how MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour. √ I understand that I will be asked to complete two questionnaires about my child’s behaviour at the beginning and at the end of MMA. This will take approximately 25 minutes. √ I understand that the information collected will be kept confidential and will be stored in a secure location at Integra. I understand that only the Director of Research and Psychology at Integra, Dr. Karen Milligan, and those directly involved in the research will have access to the information. √ I understand that if I decide not to participate in this study, it will not impact on the services that I or my family receive at Integra. √ I understand that I may withdraw my permission at any time. √ I understand that any information that is used for presentations or publications will be presented with all identifying information removed. √ I understand that if I have any questions or would like additional information, I may contact Dr. Karen Milligan, Director of Research & Psychology (416 486 8055 ext. 232) at any time. Name of parent/guardian: _______________________________ ________ Name of Child: _______________________________ Signature of parent/guardian:____________________________ Witness: ____________________________________________ Date: _____________________________
Mindfulness Martial Arts 43
MINDFULNESS MARTIAL ARTS (MMA) EVALUATION INFORMED CONSENT – YOUTH
√ I understand that Integra staff members are interested in hearing from youth and parents about their impressions of MMA and learning more specifically about how MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour. √ I understand that I will be asked to complete a brief set of questionnaires and a drawing task, play some computer games, and view some emotional pictures. I will also be asked about positive and challenging situations I have experienced. This will take approximately 1 hour. My parents and a teacher of my choosing will be asked to complete two questionnaires. √ One potential risk is that I may feel some discomfort when talking about challenging situations, viewing pictures, or answering questions about my feelings, thoughts, or behaviour. My Integra Child and Family therapist is aware of the study and will provide support if needed. √ I understand that the information collected will be kept confidential and will be stored in a secure location at Integra. I understand that only the Director of Research and Psychology at Integra, Dr. Karen Milligan, and those directly involved in the research will have access to the information. √ I understand that if I decide not to participate in this study, it will not impact on the services that I or my family receive at Integra. I may skip any question/task, request a break, or withdraw from the study at any time without penalty. √ I understand that any information that is used for presentations or publications will be presented with all identifying information removed. √ I understand that if I have any questions or would like additional information, I may contact Dr. Karen Milligan, Director of Research & Psychology (416 486 8055 ext. 232) at any time. Name of Youth: _______________________________ Signature of youth:_____________________________ Name of parent/guardian: _______________________________ ________ Signature of parent/guardian (if under 18):____________________________ Witness: ____________________________________________ Date: _____________________________

Mindfulness Martial Arts 44
September 2010 Dear Teacher: Your student is currently participating in the Mindfulness Martial Arts program at Integra (a children’s mental health centre for youth with learning disabilities). Over the past couple of years, we have been conducting a formal program evaluation of the Mindfulness Martial Arts (MMA) program developed by Paul Badali, Child and Family Therapist at Integra. The purpose of this research has been to better understand the gains youth make while in the program and to further develop and improve MMA. To date, results of this research are positive. Youth who participate in MMA show improvements in areas such as flexibility in dealing with challenges, organization, attention, and impulsivity. We are completing a more in depth study that will examine if MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour and to see if these changes extend to the school setting. This study is headed by Dr. Karen Milligan, Director of Research and Psychology at Integra, and is funded by a grant awarded to Integra by the Provincial Centre for Excellence in Child and Youth Mental Health. Your student and his/her family are participating in this research study and have provided consent for us to request your participation. We would greatly appreciate it if you would complete the enclosed questionnaires within the next week and return them to us to help us understand how youth are functioning at the beginning of MMA. We will be requesting that you complete the questionnaires again in February to help us identify how youth change after participation in the program. We believe that this research will make an important contribution to our knowledge about the treatment of social-emotional difficulties associated with learning disabilities and to the further development of the MMA program. We would be grateful for your participation. If you have any questions, or if you would like additional information, please call me at 416-486-8055, ext. 232. Thank you for your consideration of this request. Sincerely, Karen Milligan, Ph.D., C.Psych. Director of Research and Psychology
Mindfulness Martial Arts 45
February 2010 Dear Teacher: As you are aware, your student is currently participating in the Mindfulness Martial Arts (MMA) program at Integra (a children’s mental health centre for youth with learning disabilities). We are currently completing research study that examines if MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour. We are specifically interested in seeing if these changes extend to the school setting. We greatly appreciate your assistance in completing questionnaires this past September. To better understand how youth change and the gains they make due to participation in MMA, we are asking teachers to complete the same questionnaires at the end of treatment. We would greatly appreciate it if you would complete the enclosed questionnaires within the next week and return them to us in the enclosed envelope. Your student and his/her family are participating in this research study and have provided consent for us to request your participation. We believe that this research will make an important contribution to our knowledge about the treatment of social-emotional difficulties associated with learning disabilities and further the development of the MMA program. We would be grateful for your participation. If you have any questions, or if you would like additional information, please feel free to call me at 416-486-8055, ext. 232. Thank you for your consideration of this request. Sincerely, Karen Milligan, Ph.D., C.Psych. Director of Research and Psychology
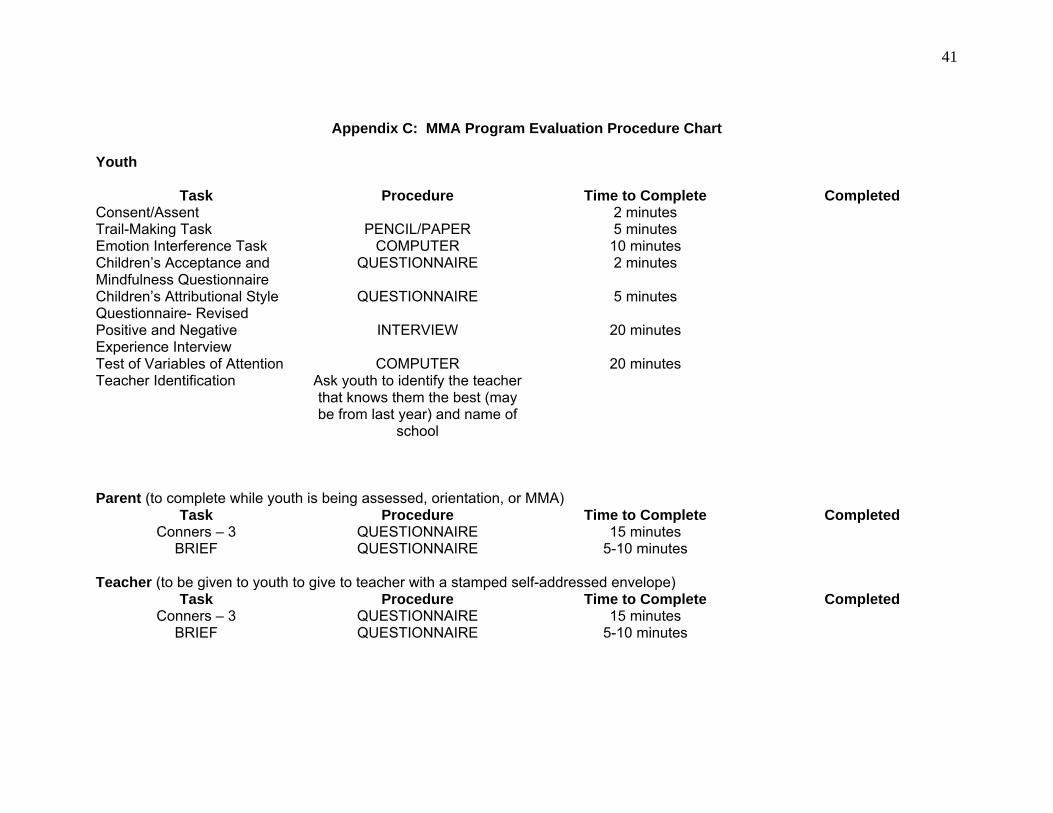
41
Appendix C: MMA Program Evaluation Procedure Chart
Youth
Task Procedure Time to Complete Completed Consent/Assent 2 minutes Trail-Making Task PENCIL/PAPER 5 minutes Emotion Interference Task COMPUTER 10 minutes Children’s Acceptance and Mindfulness Questionnaire
QUESTIONNAIRE 2 minutes
Children’s Attributional Style Questionnaire- Revised
QUESTIONNAIRE 5 minutes
Positive and Negative Experience Interview
INTERVIEW 20 minutes
Test of Variables of Attention COMPUTER 20 minutes Teacher Identification Ask youth to identify the teacher
that knows them the best (may be from last year) and name of
school
Parent (to complete while youth is being assessed, orientation, or MMA) Task Procedure Time to Complete Completed
Conners – 3 QUESTIONNAIRE 15 minutes BRIEF QUESTIONNAIRE 5-10 minutes
Teacher (to be given to youth to give to teacher with a stamped self-addressed envelope)
Task Procedure Time to Complete Completed Conners – 3 QUESTIONNAIRE 15 minutes
BRIEF QUESTIONNAIRE 5-10 minutes
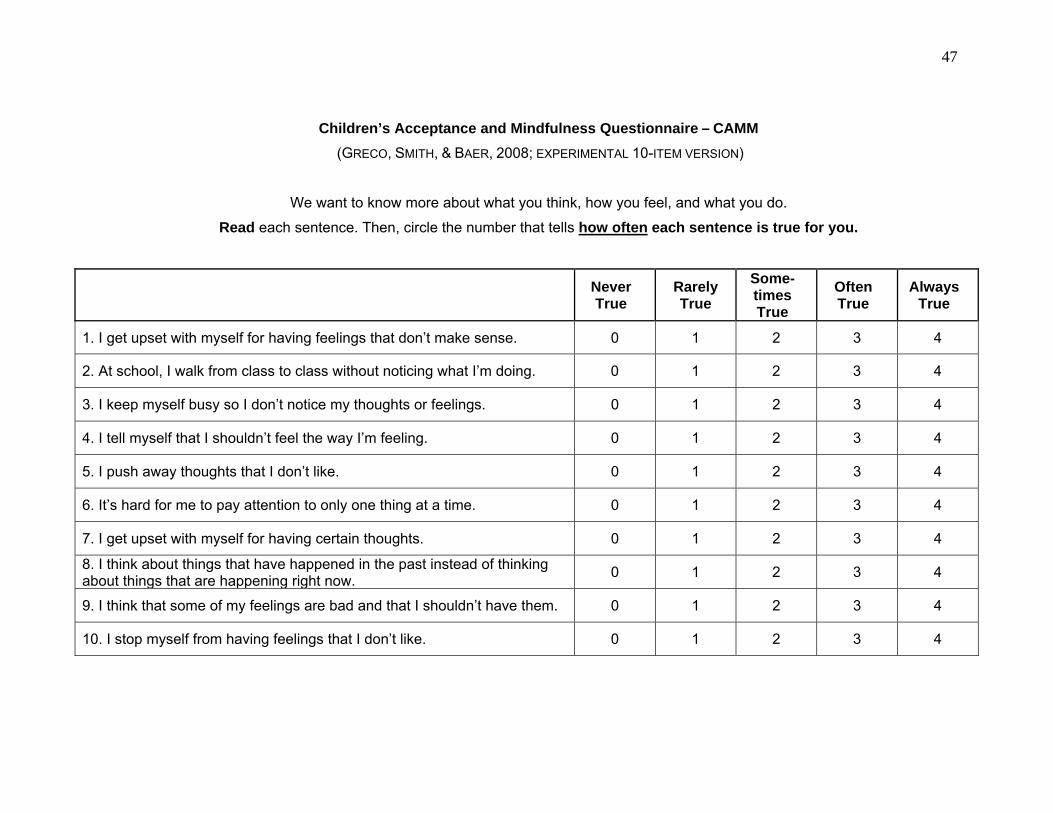
47
Children’s Acceptance and Mindfulness Questionnaire – CAMM
(GRECO, SMITH, & BAER, 2008; EXPERIMENTAL 10-ITEM VERSION)
We want to know more about what you think, how you feel, and what you do.
Read each sentence. Then, circle the number that tells how often each sentence is true for you.
Never True
Rarely True
Some-times True
Often True
Always True
1. I get upset with myself for having feelings that don’t make sense. 0 1 2 3 4
2. At school, I walk from class to class without noticing what I’m doing. 0 1 2 3 4
3. I keep myself busy so I don’t notice my thoughts or feelings. 0 1 2 3 4
4. I tell myself that I shouldn’t feel the way I’m feeling. 0 1 2 3 4
5. I push away thoughts that I don’t like. 0 1 2 3 4
6. It’s hard for me to pay attention to only one thing at a time. 0 1 2 3 4
7. I get upset with myself for having certain thoughts. 0 1 2 3 4
8. I think about things that have happened in the past instead of thinking about things that are happening right now.
0 1 2 3 4
9. I think that some of my feelings are bad and that I shouldn’t have them. 0 1 2 3 4
10. I stop myself from having feelings that I don’t like. 0 1 2 3 4
48
Children’s Attributional Style Questionnaire - Revised 1. You get an “A” on a test.
A. I am smart. B. I am good in the subject that the test was in.
2. Some kids that you know say that they do not like you.
A. Once in a while people are mean to me. B. Once in a while I am mean to other people.
3. A good friend tells you that he hates you.
A. My friend was in a bad mood that day. B. I wasn’t nice to my friend that day.
4. A person steals money from you.
A. That person is not honest. B. Many people are not honest.
5. Your parents tell you that something you make is very good.
A. I am good at making some things. B. My parents like some things I make.
6. You break a glass.
A. I am not careful enough. B. Sometimes I am not careful enough.
7. You do a project with a group of kids and it turns out badly.
A. I don’t work well with the people in that particular group. B. I never work well with groups.
8. You make a new friend.
A. I am a nice person. B. The people that I meet are nice.
9. You have been getting along well with your family.
A. I am usually easy to get along with when I am with my family. B. Once in a while I am easy to get along with when I am with my family.
10. You get a bad grade in school.
A. I am not a good student. B. Teachers give hard tests.
11. You walk into a door and you get a bloody nose.
A. I wasn’t looking where I was going. B. I have been careless lately.
12. You have a messy room.
A. I did not clean my room that day. B. I usually do not clean my room.
13. Your mother makes you your favorite dinner.
A. There are a few things that my mother will do to please me. B. My mother usually likes to please me.
49
14. A team that you are on loses a game. A. The team members don’t help each other when they play together. B. That day the team members didn’t help each other.
15. You do not get your chores done at home.
A. I was lazy that day. B. Many days I am lazy.
16. You go to an amusement park and you have a good time.
A. I usually enjoy myself at amusement parks. B. I usually enjoy myself in many activities.
17. You go to a friend’s party and you have fun.
A. Your friend usually gives good parties. B. Your friend gave a good party that day.
18. You have a substitute teacher and she likes you.
A. I was well behaved during class that day. B. I am almost always well behaved during class.
19. You make your friends happy.
A. I am usually a fun person to be with. B. Sometimes I am a fun person to be with.
20. You put a hard puzzle together.
A. I am good at putting puzzles together. B. I am good at doing many things.
21. You try out for a sports team and do not make it.
A. I am not good at sports. B. The other kids who tried out are very good at sports.
22. You fail a test.
A. All tests are hard. B. Only some tests are hard.
23. You hit a home run in a ball game.
A. I swung the bat just right. B. The pitcher threw an easy pitch.
24. You do the best in your class on a paper.
A. The other kids in my class did not work hard on their papers. B. I worked hard on the paper.
From the Children’s Attributional Scale Questionnaire – Revised, by N.J. Kaslow and S. Nolen-Hoeksema, 1991. Unpublished manuscript. Copyright 1991, by N.J. Kaslow and S. Nolen-Hoeksema.
50
Positive & Negative Experience Interview
Everyone experiences ups and downs in their life. Sometimes, we experience things that make us feel great and other times we may have experiences that are extremely difficult, painful, or upsetting. I am going to ask you about these experiences. Try to talk about them as best you can. There are no right or wrong answers – just whatever comes to your mind. PLEASE VIDEOTAPE or TAPE RECORD Negative Experience Tell me about the most stressful, painful, or upsetting experience that you have ever had. Try your best to remember a specific time in which you felt REALLY negative emotions, such as sadness, worry, pain, guilt, or embarrassment. Remember, this should be the most stressful, painful, or upsetting experience you have ever had. Even though this memory may be hard to talk about, just try your best to tell me as much as you can. Please remember to be specific. Give participant opportunity to recall as much as they can independently. Query – Can you tell me anything else about this experience? Positive Experience Tell me about the best experience of your whole life. This should be an experience that stands out in your memory as a time that you felt REALLY great. You may have felt very happy, excited, proud, loved or any other really positive emotion. Just tell me about what comes to mind. Try your best to tell me as much as you can. Please remember to be specific. Give participant opportunity to recall as much as they can independently. Query – Can you tell me anything else about this experience?
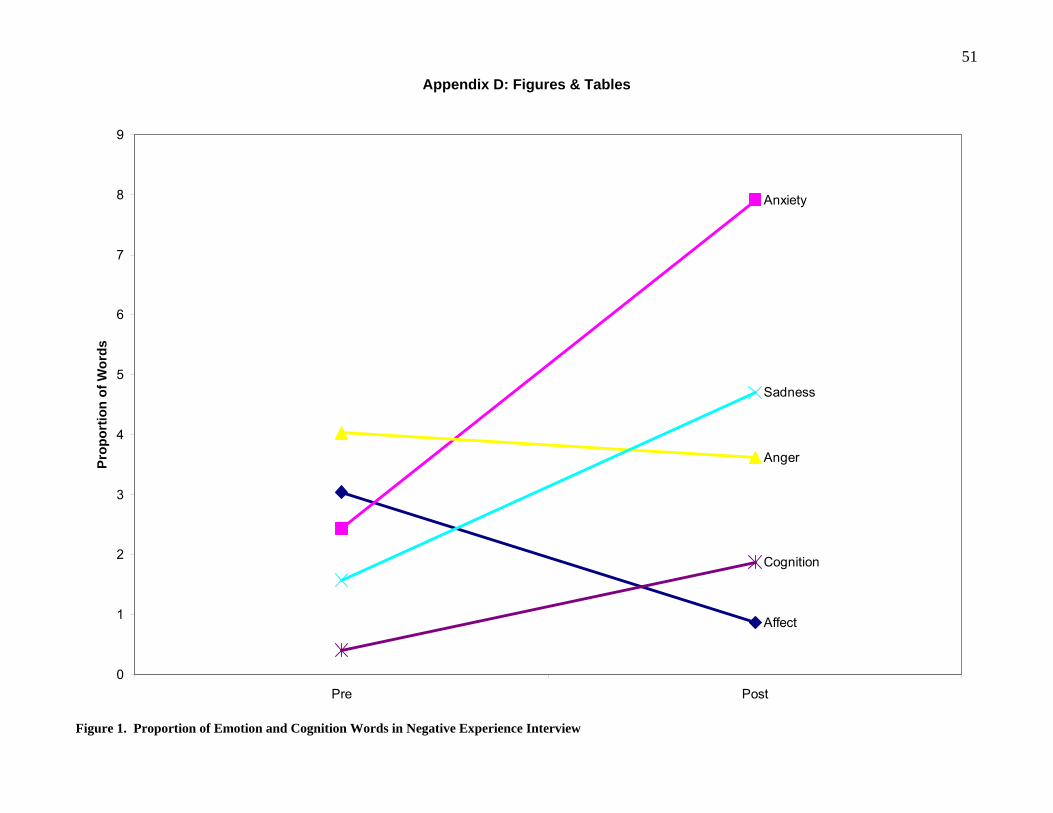
51
Appendix D: Figures & Tables
Affect
Anxiety
Anger
Sadness
Cognition
0
1
2
3
4
5
6
7
8
9
Pre Post
Pro
po
rtio
n o
f W
ord
s
Figure 1. Proportion of Emotion and Cognition Words in Negative Experience Interview
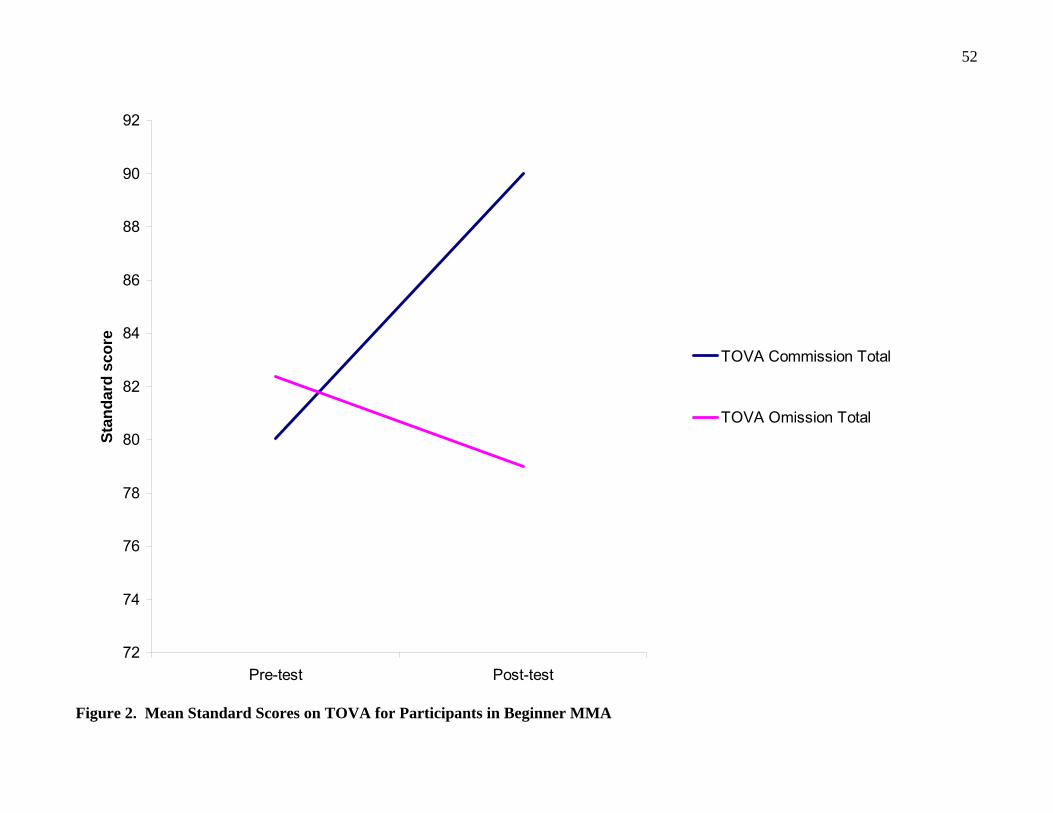
52
72
74
76
78
80
82
84
86
88
90
92
Pre-test Post-test
Sta
nd
ard
sco
re
TOVA Commission Total
TOVA Omission Total
Figure 2. Mean Standard Scores on TOVA for Participants in Beginner MMA
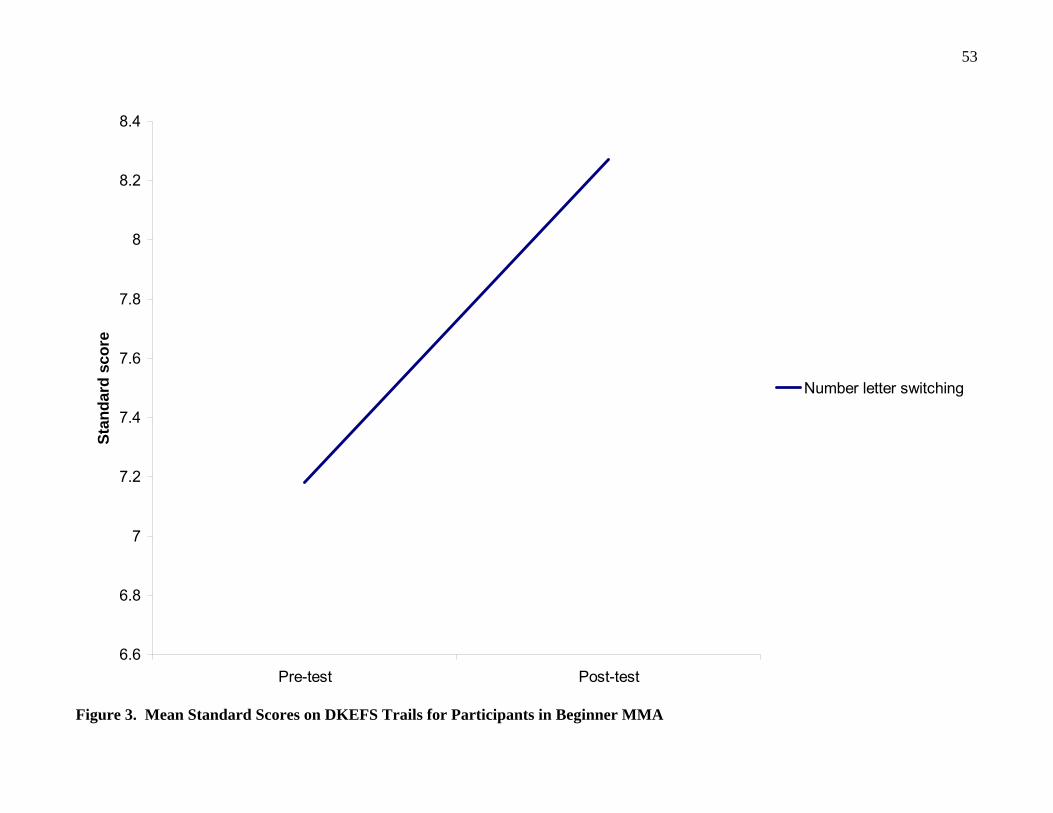
53
6.6
6.8
7
7.2
7.4
7.6
7.8
8
8.2
8.4
Pre-test Post-test
Sta
nd
ard
sco
re
Number letter switching
Figure 3. Mean Standard Scores on DKEFS Trails for Participants in Beginner MMA
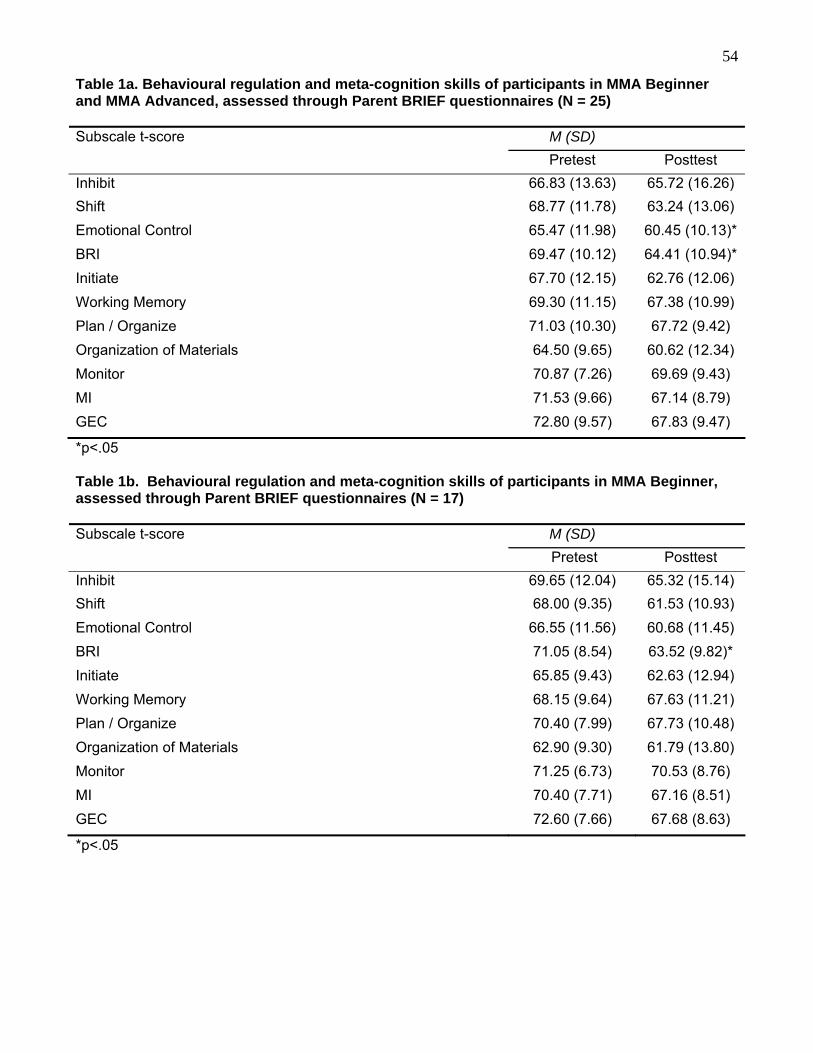
54
Table 1a. Behavioural regulation and meta-cognition skills of participants in MMA Beginner and MMA Advanced, assessed through Parent BRIEF questionnaires (N = 25)
M (SD) Subscale t-score
Pretest Posttest
Inhibit 66.83 (13.63) 65.72 (16.26)
Shift 68.77 (11.78) 63.24 (13.06)
Emotional Control 65.47 (11.98) 60.45 (10.13)*
BRI 69.47 (10.12) 64.41 (10.94)*
Initiate 67.70 (12.15) 62.76 (12.06)
Working Memory 69.30 (11.15) 67.38 (10.99)
Plan / Organize 71.03 (10.30) 67.72 (9.42)
Organization of Materials 64.50 (9.65) 60.62 (12.34)
Monitor 70.87 (7.26) 69.69 (9.43)
MI 71.53 (9.66) 67.14 (8.79)
GEC 72.80 (9.57) 67.83 (9.47)
*p<.05 Table 1b. Behavioural regulation and meta-cognition skills of participants in MMA Beginner, assessed through Parent BRIEF questionnaires (N = 17)
M (SD) Subscale t-score
Pretest Posttest
Inhibit 69.65 (12.04) 65.32 (15.14)
Shift 68.00 (9.35) 61.53 (10.93)
Emotional Control 66.55 (11.56) 60.68 (11.45)
BRI 71.05 (8.54) 63.52 (9.82)*
Initiate 65.85 (9.43) 62.63 (12.94)
Working Memory 68.15 (9.64) 67.63 (11.21)
Plan / Organize 70.40 (7.99) 67.73 (10.48)
Organization of Materials 62.90 (9.30) 61.79 (13.80)
Monitor 71.25 (6.73) 70.53 (8.76)
MI 70.40 (7.71) 67.16 (8.51)
GEC 72.60 (7.66) 67.68 (8.63)
*p<.05

55
Behavioural regulation and meta-cognition skills of participants in MMA Advanced, assessed through Parent BRIEF questionnaires (N = 8)
M (SD) Subscale t-score
Pretest Posttest
Inhibit 61.20 (15.50) 66.50 (19.04)
Shift 70.30 (16.08) 66.50 (16.54)
Emotional Control 63.30 (13.13) 60.00 (7.54)
BRI 66.30 (12.62) 66.10 (13.23)
Initiate 71.40 (16.27) 63.00 (10.85)
Working Memory 71.60 (13.98) 66.90 (11.14)
Plan / Organize 72.30 (14.31) 67.70 (7.53)
Organization of Materials 67.70 (10.01) 58.40 (9.18)
Monitor 70.10 (8.57) 68.10 (10.91)
MI 73.80 (12.91) 67.10 (9.76)
GEC 73.20 (13.07) 68.10 (11.41)
Table 2a. Conners-3 Parent Rating Scale (N = 23)
M (SD) Subscale t-score
Pretest Posttest
Inattention 71.60 (11.37) 71.61 (12.93)
Hyperactivity / Impulsivity 67.53 (14.94) 68.18 (15.98)
Learning Problems 67.27 (14.65) 70.54 (14.13)
Executive Functioning 66.30 (10.10) 66.37 (11.16)
Aggression 63.37 (14.86) 64.39 (14.01)
Peer Relations 77.63 (15.48) 73.29 (17.13)
Conners 3 Global Index 70.33 (13.70) 69.11 (14.01)
DSM-IV-TR ADHD Inattentive 69.67 (10.22) 68.32 (11.59)
DSM-IV-TR ADHD Hyperactive-Impulsive 66.50 (15.82) 68.36 (16.03)
DSM-IV-TR Conduct Disorder 59.27 (14.06) 56.96 (13.80)
DSM-IV-TR Oppositional Defiant 64.83 (13.64) 63.79 (14.54)
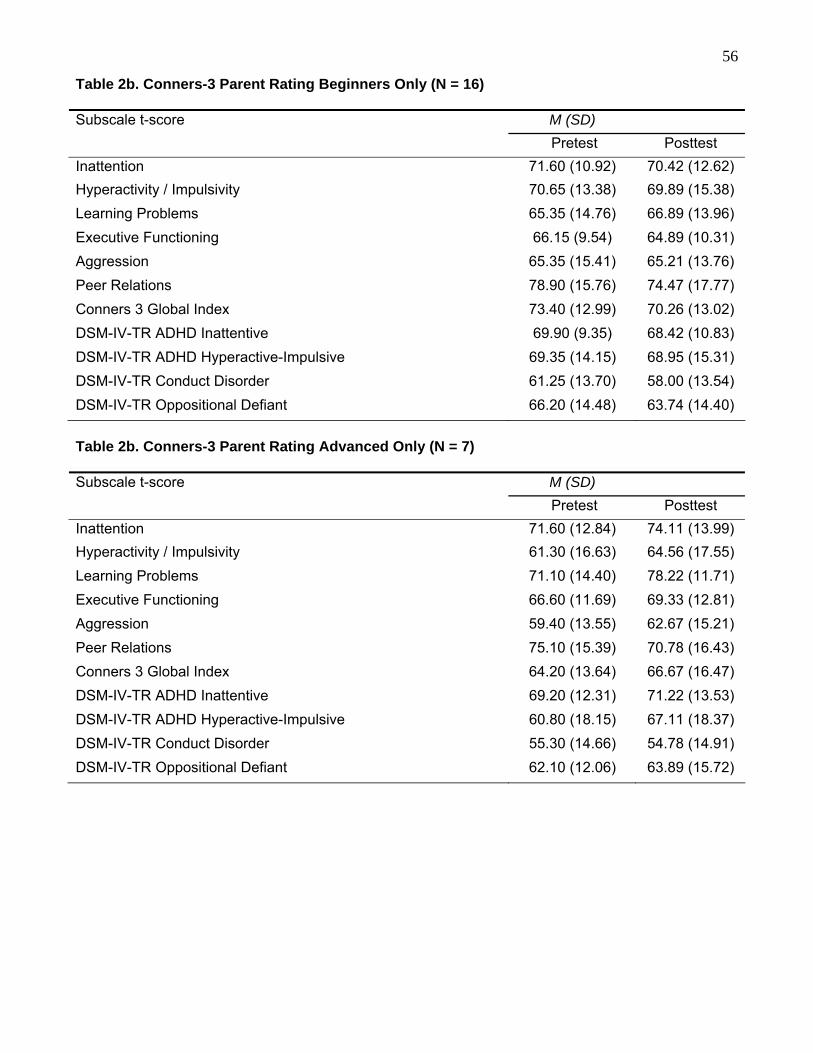
56
Table 2b. Conners-3 Parent Rating Beginners Only (N = 16)
M (SD) Subscale t-score
Pretest Posttest
Inattention 71.60 (10.92) 70.42 (12.62)
Hyperactivity / Impulsivity 70.65 (13.38) 69.89 (15.38)
Learning Problems 65.35 (14.76) 66.89 (13.96)
Executive Functioning 66.15 (9.54) 64.89 (10.31)
Aggression 65.35 (15.41) 65.21 (13.76)
Peer Relations 78.90 (15.76) 74.47 (17.77)
Conners 3 Global Index 73.40 (12.99) 70.26 (13.02)
DSM-IV-TR ADHD Inattentive 69.90 (9.35) 68.42 (10.83)
DSM-IV-TR ADHD Hyperactive-Impulsive 69.35 (14.15) 68.95 (15.31)
DSM-IV-TR Conduct Disorder 61.25 (13.70) 58.00 (13.54)
DSM-IV-TR Oppositional Defiant 66.20 (14.48) 63.74 (14.40)
Table 2b. Conners-3 Parent Rating Advanced Only (N = 7)
M (SD) Subscale t-score
Pretest Posttest
Inattention 71.60 (12.84) 74.11 (13.99)
Hyperactivity / Impulsivity 61.30 (16.63) 64.56 (17.55)
Learning Problems 71.10 (14.40) 78.22 (11.71)
Executive Functioning 66.60 (11.69) 69.33 (12.81)
Aggression 59.40 (13.55) 62.67 (15.21)
Peer Relations 75.10 (15.39) 70.78 (16.43)
Conners 3 Global Index 64.20 (13.64) 66.67 (16.47)
DSM-IV-TR ADHD Inattentive 69.20 (12.31) 71.22 (13.53)
DSM-IV-TR ADHD Hyperactive-Impulsive 60.80 (18.15) 67.11 (18.37)
DSM-IV-TR Conduct Disorder 55.30 (14.66) 54.78 (14.91)
DSM-IV-TR Oppositional Defiant 62.10 (12.06) 63.89 (15.72)
57
Appendix E: Interview Information Letter, Consents, and Guide
June 23, 2009 Dear Parent(s), As you know, we have been conducting a formal program evaluation of Mindfulness Martial Arts (MMA) in order to better understand the gains youth make while in the program and to further develop and improve MMA. We appreciate your assistance with this project. We are planning a more in depth study next year to examine if MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour. As one component of this evaluation, we will be inviting a small number of youth and parents to participate in an interview, asking for their observations and feedback about MMA in a more in-depth format. To prepare for this larger study, we would like to complete interviews with a couple of families from this past session of MMA. This will assist us in refining our interview and will guide our research to ensure that we are able to fully capture the experience of parents and youth. We would like to invite you to take part in this pilot study. If you are willing, we would contact you at the end of June/early July to arrange a convenient time to meet. Interviews, which are expected to be approximately 1 hour in length, will be conducted in-person at Integra and will be videotaped in order that we can later review them. We will interview you and your child separately. If you decide not to participate, it will not impact on the services that you and your child receive at Integra and you may decide at any time to withdraw your permission. Your interview and information will be kept confidential and will only be reviewed by those directly involved in the research. The program evaluation is being headed by Dr. Karen Milligan, Director of Research and Psychology at Integra. Dr. Lesley Daniels, a psychologist at Integra, will be assisting with the interview phase of the research. If you have any questions or concerns about this phase of the project, please do not hesitate to contact us. You may also direct questions to Paul Badali who is familiar with our research plans. Sincerely, Karen Milligan, Ph.D., C.Psych. Lesley Daniels, Ph.D., C.Psych. Director of Research & Psychology Psychologist Integra Integra 25 Imperial St. 25 Imperial St. Toronto, ON, M5P 1B9 Toronto, ON, M5P 1B9 416 486 8055 ext. 232 416 486 8055 ext. 240 [email protected] [email protected]
58
MINDFULNESS MARTIAL ARTS (MMA) EVALUATION
INFORMED CONSENT √ I understand that Integra staff members are interested in hearing from youth and parents about their impressions of MMA and learning more specifically about how MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour. √ I understand that I will be asked to participate in an interview, asking for our observations and feedback about MMA in an in-depth format. This will take approximately one-hour and will be scheduled at a time that is convenient for my family. √ I understand that the information collected will be kept confidential and will be stored in a secure location at Integra. I understand that only the Director of Research and Psychology at Integra, Dr. Karen Milligan, and those directly involved in the research will have access to the information. √ I understand that if I decide not to participate in this study, it will not impact on the services that my child and our family receive at Integra. √ I understand that I may withdraw my permission at any time. √ I understand that any information from our interviews that are used for presentations or publications will be presented with all identifying information removed. √ I understand that the videotape used for the present interview will be stored in a secure location at Integra and destroyed upon completion of the research. √ I understand that if I have any questions or would like additional information, I may contact Dr. Karen Milligan, Director of Research & Psychology (416 486 8055 ext. 232) at any time. Name of participant: _______________________________ ________ Signature of parent/guardian:____________________________ Witness: _____________________________________________ Date: _____________________________
59
MINDFULNESS MARTIAL ARTS (MMA) EVALUATION INFORMED CONSENT
√ I understand that Integra staff members are interested in hearing from youth and parents about their impressions of MMA and learning more specifically about how MMA changes the way in which youth view challenges and their awareness of and ability to manage their emotions and behaviour. √ I understand that I will be asked to participate in an interview, asking for my observations and feedback about MMA in an in-depth format. This will take approximately one-hour and will be scheduled at a time that is convenient for my family. √ I understand that the information collected will be kept confidential and will be stored in a secure location at Integra. I understand that only the Director of Research and Psychology at Integra, Dr. Karen Milligan, and those directly involved in the research will have access to the information. √ I understand that if I decide not to participate in this study, it will not impact on the services that I or my family receive at Integra. √ I understand that I may withdraw my permission at any time. √ I understand that any information from our interviews that are used for presentations or publications will be presented with all identifying information removed. √ I understand that the videotape used for the present interview will be stored in a secure location at Integra and destroyed upon completion of the research. √ I understand that if I have any questions or would like additional information, I may contact Dr. Karen Milligan, Director of Research & Psychology (416 486 8055 ext. 232) at any time. Name of participant: _______________________________ ________ Participant’s date of birth: Month: _________ Day:_______ Year:_______ Name of parent/guardian: _______________________________ Permission granted: Yes:___________ No: _____________ Signature of parent/guardian:____________________________ Witness: ____________________________________________ Date: _____________________________
60
Qualitative Interview Guide This part of our research involves asking you questions about your experience in the MMA program in order to get a more in-depth perspective than we could get using questionnaires. PART A – General Evaluation First, we’d like to find out more about what you thought of MMA in general.
YOUTH PARENT Notes 1. What did you like about the MMA program?* Why?
1. What did you like about the MMA program? Why?
2. What didn’t you like about the MMA program?* Why?
2. What didn’t you like about the MMA program? Why?
3. What is the most important part of the MMA program? How did it help you? (prompt for specific example – e.g., at home/ school, with friends, etc.)
3. What do you think is the most important part of the MMA program? How did it help your child? (prompt for specific example – e.g., at home/ school, with friends, etc.)
4. What was your goal for the MMA program? Why did you choose this goal / Why was this something you wanted to work on?
4. What was your child’s goal for the MMA program? Why do you think he/she chose this goal?
5. How successful do you think you were in achieving your goal?
5. How successful was he/she in achieving his/her goal?
6. What parts of the MMA program helped you to achieve your goal?*
6. What about the MMA program helped him/her to achieve his/her goal?
7. What (other) changes do you see in yourself now that you have completed MMA? When did you first notice these changes?
7. What (other) changes do you see in your child now that he/she has completed MMA? When did you first notice these changes?
*May prompt re: specific program components -group sessions -parent/youth meeting with therapist -meditation/mindfulness activities -home practice -martial arts -the point system -thought reports/coping strategies
61
PART B – Evaluation of Program Components Now, we’d like to ask you to think about the different parts of the MMA program and how they might have helped you / your child.
YOUTH PARENT Notes 1. Bushido a) What does Bushido mean to you? b) How has learning about Bushido changed you? Sample prompts: … how you feel about yourself … how you act around others … how you think … how you handle problems/conflicts c) Tell about a recent time when you used or remembered the concept of Bushido. 2. MMA program goals/outcomes How has MMA* helped you to (or “What did you learn in MMA that helped you...”): a) handle challenges or stress / solve problems? b) become more aware of your thoughts and feelings? c) deal with difficult/upsetting thoughts and feelings? d) be more flexible / “go with the flow” / handle changes? e) have more self-control (e.g., calm down, think before you act) f) get along better with others g) feel more confident / feel better about yourself?
(Prompt for specific examples)
1. MMA program goals/outcomes What changes have you noticed in terms of your child’s ability to: a) handle challenges or stress / solve problems? b) become more aware of his/her thoughts and feelings? c) deal with difficult/upsetting thoughts and feelings? d) be more flexible / “go with the flow” / deal with changes? e) have more self-control (e.g., calm down, think before he/she acts) f) get along better with others g) feel more confident / feel better about himself/herself?
(Prompt for specific examples)
*May prompt re: specific program components -group sessions -parent/youth meeting with therapist -meditation/mindfulness activities -home practice -martial arts -the point system -thought reports/coping strategies

62
PART C – Application Now we’d like to ask you to think about some recent situations in your life / your child’s life.
YOUTH PARENT Notes 1. Tell about a (recent) time when you faced a big challenge. How did you handle it?
1. Tell about a (recent) time when your child faced a big challenge. How did he/she handle it?
2. Tell about a (recent) time when you had a conflict with a peer. How did you handle it?
2. Tell about a (recent) time when your child had a conflict with a peer. How did he/she handle it?
3. Tell about a (recent) time when something really bad happened to you. Why did it happen?
4. Tell about a (recent) time when something really good happened to you. Why did it happen?
5. What do you do when you find it difficult to get along with someone?
3. What does your child do when he/she finds it difficult to get along with someone?
6. What do you do when you feel worried, angry, or upset about something?
4. What does your child do when he/she feels worried, angry, or upset about something?
PART D – Summary Finally, we’d like to ask you a few more general questions about your experience in MMA.
YOUTH PARENT Notes 1. What was most challenging about the MMA program?
1. What do you think your child found most challenging about the MMA program?
2. What could make the MMA program better?
2. What could make the MMA program better?
3. How do you think MMA helps youth with learning disabilities?
3. How do you think MMA helps youth with learning disabilities?
4. If you had a message for your therapist/sensei, what would it be?
4. If you had a message for the therapist/sensei, what would it be?
5. If you were going to tell other youth about MMA, what would you say?
5. If you had a message about MMA for other parents, what would it be?
6. If you had the opportunity, would you take part in MMA again? Why/why not?
6. If you had the opportunity, would you take part in MMA again? Why/why not?
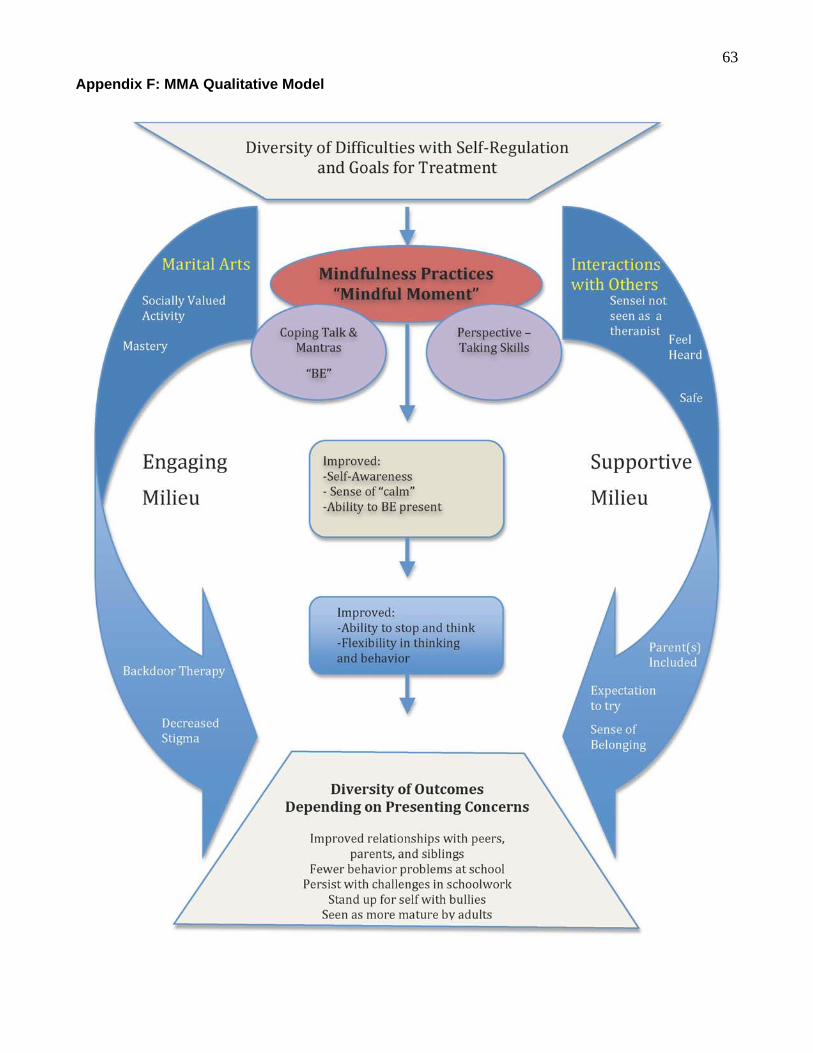
63
Appendix F: MMA Qualitative Model
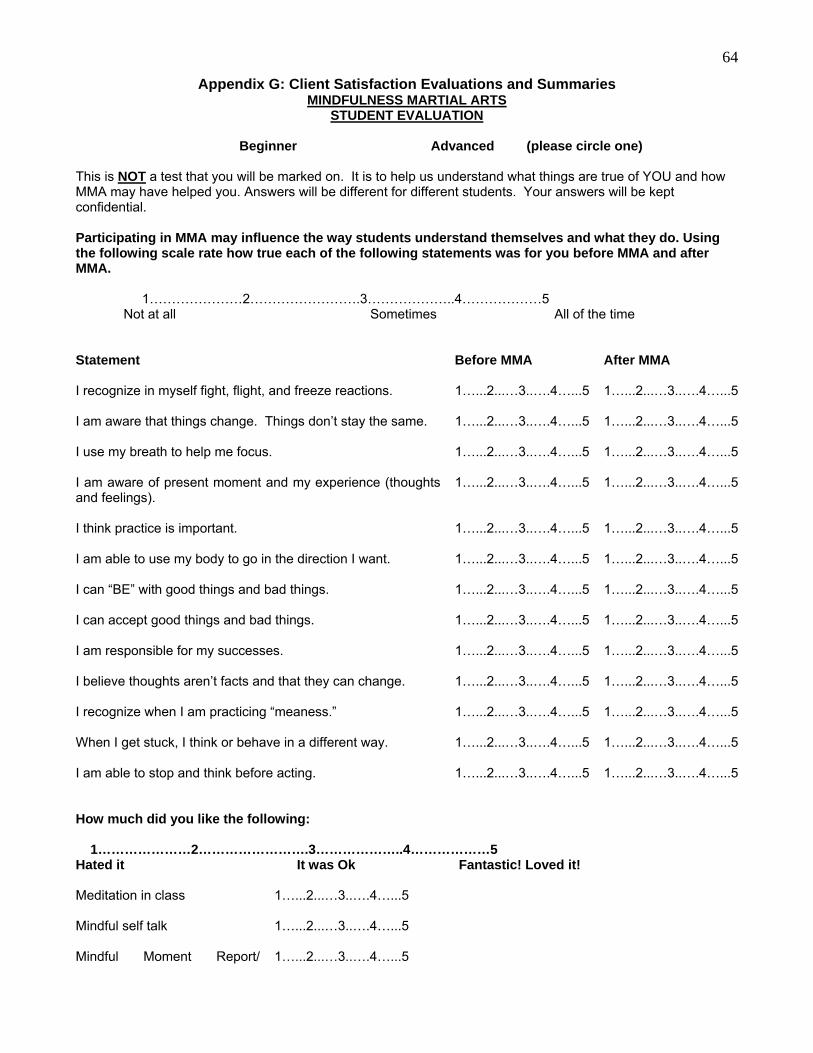
64
Appendix G: Client Satisfaction Evaluations and Summaries MINDFULNESS MARTIAL ARTS
STUDENT EVALUATION
Beginner Advanced (please circle one) This is NOT a test that you will be marked on. It is to help us understand what things are true of YOU and how MMA may have helped you. Answers will be different for different students. Your answers will be kept confidential. Participating in MMA may influence the way students understand themselves and what they do. Using the following scale rate how true each of the following statements was for you before MMA and after MMA. 1…………………2…………………….3………………..4………………5
Not at all Sometimes All of the time Statement Before MMA After MMA I recognize in myself fight, flight, and freeze reactions. I am aware that things change. Things don’t stay the same. I use my breath to help me focus. I am aware of present moment and my experience (thoughts and feelings). I think practice is important. I am able to use my body to go in the direction I want. I can “BE” with good things and bad things. I can accept good things and bad things. I am responsible for my successes. I believe thoughts aren’t facts and that they can change. I recognize when I am practicing “meaness.” When I get stuck, I think or behave in a different way. I am able to stop and think before acting.
1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5
1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5
How much did you like the following: 1…………………2…………………….3………………..4………………5 Hated it It was Ok Fantastic! Loved it! Meditation in class Mindful self talk Mindful Moment Report/
1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5
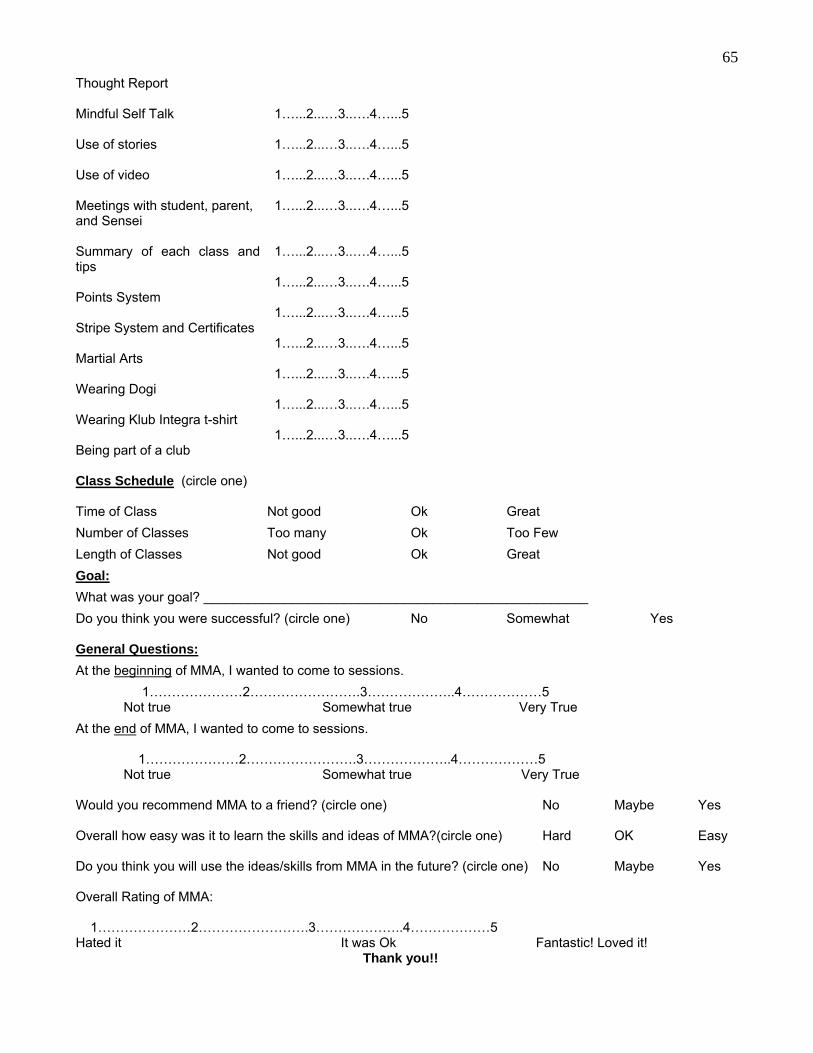
65
Thought Report Mindful Self Talk Use of stories Use of video Meetings with student, parent, and Sensei Summary of each class and tips Points System Stripe System and Certificates Martial Arts Wearing Dogi Wearing Klub Integra t-shirt Being part of a club
1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5
Class Schedule (circle one) Time of Class Not good Ok Great
Number of Classes Too many Ok Too Few
Length of Classes Not good Ok Great
Goal:
What was your goal? ____________________________________________________
Do you think you were successful? (circle one) No Somewhat Yes General Questions:
At the beginning of MMA, I wanted to come to sessions.
1…………………2…………………….3………………..4………………5 Not true Somewhat true Very True
At the end of MMA, I wanted to come to sessions. 1…………………2…………………….3………………..4………………5
Not true Somewhat true Very True Would you recommend MMA to a friend? (circle one) No Maybe Yes Overall how easy was it to learn the skills and ideas of MMA?(circle one) Hard OK Easy Do you think you will use the ideas/skills from MMA in the future? (circle one) No Maybe Yes Overall Rating of MMA: 1…………………2…………………….3………………..4………………5 Hated it It was Ok Fantastic! Loved it!
Thank you!!
66
MMA Student Evaluation of the program - Beginner Following completion of the Beginner MMA program (n = 13), students demonstrated enhanced self-awareness through increased acknowledgement of personal thoughts and feelings, “mean” behaviour, and their fight, flight, and freeze reactions. Before participation, 61.6% of students reported that they had a limited understanding of the concept that things change. Upon completion of MMA, 38.5% and 53.8% of students reported an awareness of change at some or all times, respectively. This was accompanied by an increase in the proportion of students who felt they could “be” with and accept both good and bad things more consistently. When faced with difficulties, students subsequently reported thinking before acting, behaving differently when stuck, and using their breath to help them focus. Students identified the martial arts component as being their favourite aspect of the program, while the mindful moment report was their least. Generally, students enjoyed being part of a club and wearing Gui and Klub Integra t-shirts. They highly valued the stripe system and certificates, class summaries, and meetings with their parents and Sensei. After the program, 69.2% of students felt they had met their MMA goals and 61.5% now acknowledged full responsibility for their own success. MMA Student Evaluation of the program - Advanced After participation in the Advanced MMA program (n = 16), students showed greater self-awareness through the increased ability to recognize personal thoughts and feelings, “mean” behaviour, and their fight, flight, and freeze reactions. Before participation, 37.6% of students acknowledged a limited understanding of the concept that things change. Following MMA, 31.3% and 62.5% of students reported awareness of this concept at some or all times, respectively. A greater proportion of students also reported that they could “be” with and accept both good and bad things more consistently. Students reported a greater tendency to think before acting and to behave differently when stuck. Before MMA, 37.5% of students reported never having used their breath to focus. The same proportion of students subsequently claimed that they employ this technique all the time. Students identified the martial arts component as being their most favourable, while the mindful moment report was their least. They valued being part of a club and wearing Gui and Klub Integra t-shirts. Students appreciated the stripe system and certificates, class summaries, and meetings with their parents and Sensei. After the program, 68.8% of students felt that they would use the ideas and skills gained through MMA in the future. INTEGRA
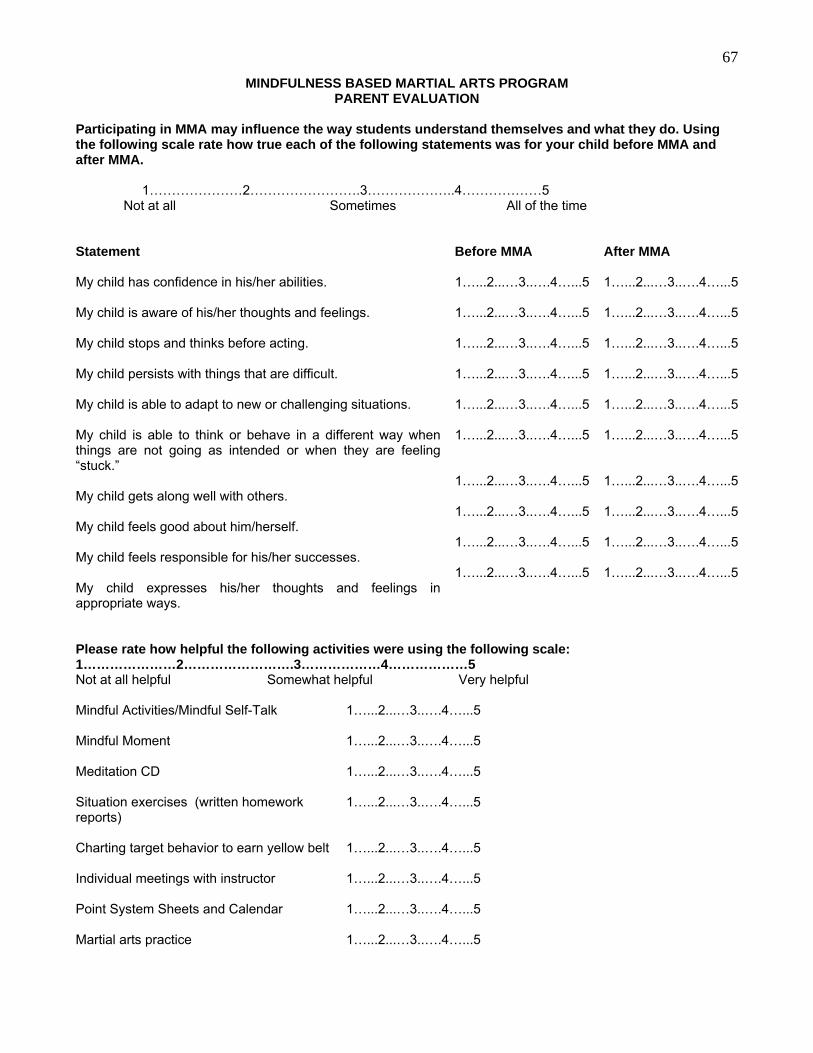
67
MINDFULNESS BASED MARTIAL ARTS PROGRAM PARENT EVALUATION
Participating in MMA may influence the way students understand themselves and what they do. Using the following scale rate how true each of the following statements was for your child before MMA and after MMA. 1…………………2…………………….3………………..4………………5
Not at all Sometimes All of the time Statement Before MMA After MMA My child has confidence in his/her abilities. My child is aware of his/her thoughts and feelings. My child stops and thinks before acting. My child persists with things that are difficult. My child is able to adapt to new or challenging situations. My child is able to think or behave in a different way when things are not going as intended or when they are feeling “stuck.” My child gets along well with others. My child feels good about him/herself. My child feels responsible for his/her successes. My child expresses his/her thoughts and feelings in appropriate ways.
1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5
1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5
Please rate how helpful the following activities were using the following scale: 1…………………2…………………….3………………4………………5 Not at all helpful Somewhat helpful Very helpful Mindful Activities/Mindful Self-Talk Mindful Moment Meditation CD Situation exercises (written homework reports) Charting target behavior to earn yellow belt Individual meetings with instructor Point System Sheets and Calendar Martial arts practice
1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5 1…...2...…3..….4…...5
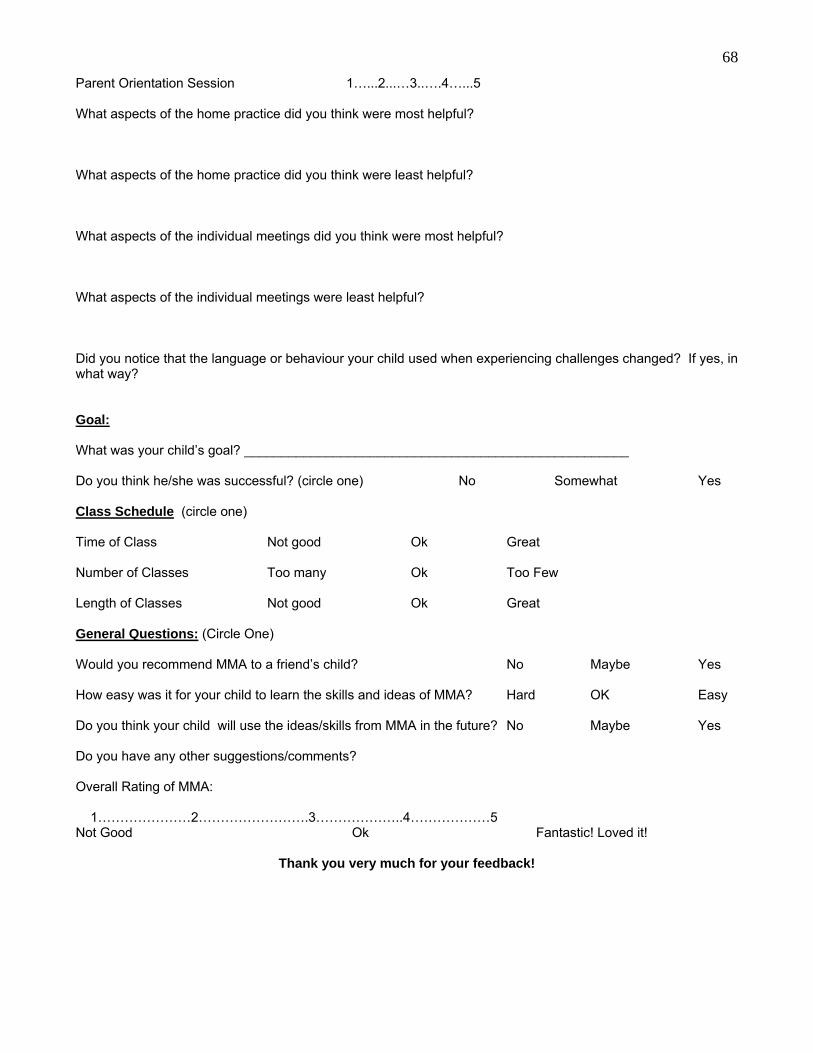
68
Parent Orientation Session 1…...2...…3..….4…...5 What aspects of the home practice did you think were most helpful? What aspects of the home practice did you think were least helpful? What aspects of the individual meetings did you think were most helpful? What aspects of the individual meetings were least helpful? Did you notice that the language or behaviour your child used when experiencing challenges changed? If yes, in what way? Goal: What was your child’s goal? ____________________________________________________ Do you think he/she was successful? (circle one) No Somewhat Yes Class Schedule (circle one) Time of Class Not good Ok Great Number of Classes Too many Ok Too Few Length of Classes Not good Ok Great General Questions: (Circle One) Would you recommend MMA to a friend’s child? No Maybe Yes How easy was it for your child to learn the skills and ideas of MMA? Hard OK Easy Do you think your child will use the ideas/skills from MMA in the future? No Maybe Yes Do you have any other suggestions/comments? Overall Rating of MMA: 1…………………2…………………….3………………..4………………5 Not Good Ok Fantastic! Loved it!
Thank you very much for your feedback!
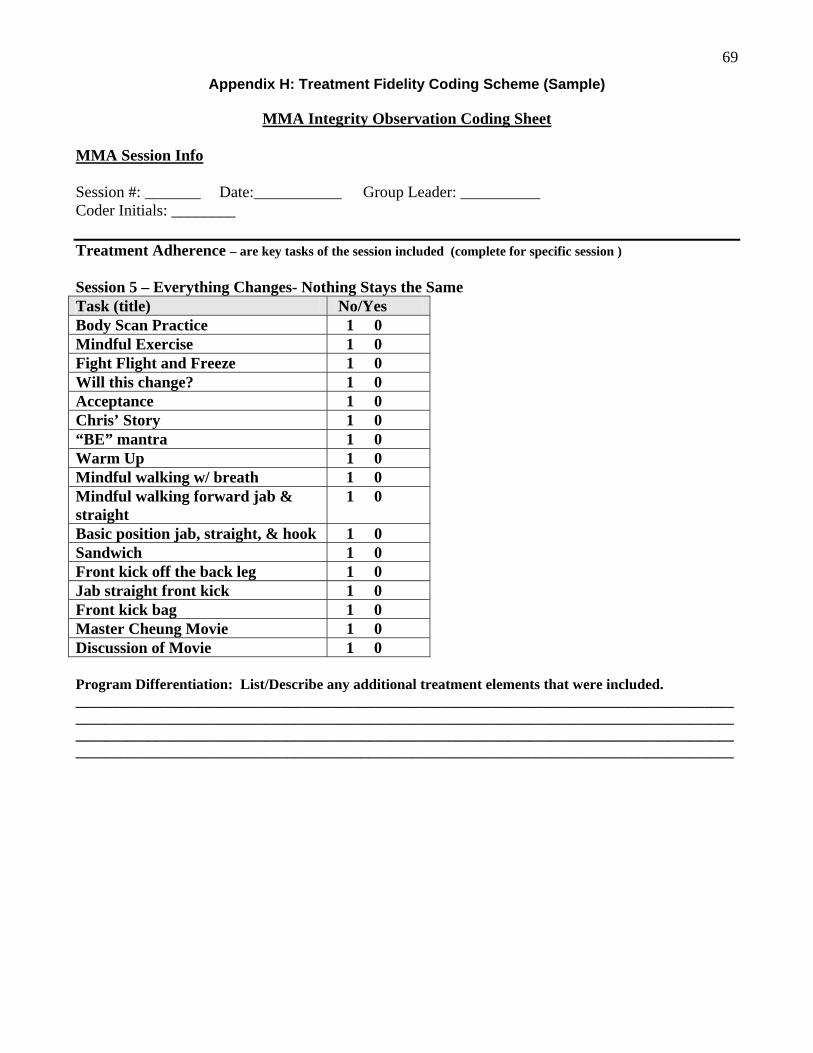
69
Appendix H: Treatment Fidelity Coding Scheme (Sample)
MMA Integrity Observation Coding Sheet
MMA Session Info Session #: _______ Date:___________ Group Leader: __________ Coder Initials: ________ Treatment Adherence – are key tasks of the session included (complete for specific session ) Session 5 – Everything Changes- Nothing Stays the Same Task (title) No/Yes Body Scan Practice 1 0 Mindful Exercise 1 0 Fight Flight and Freeze 1 0 Will this change? 1 0 Acceptance 1 0 Chris’ Story 1 0 “BE” mantra 1 0 Warm Up 1 0 Mindful walking w/ breath 1 0 Mindful walking forward jab & straight
1 0
Basic position jab, straight, & hook 1 0 Sandwich 1 0 Front kick off the back leg 1 0 Jab straight front kick 1 0 Front kick bag 1 0 Master Cheung Movie 1 0 Discussion of Movie 1 0 Program Differentiation: List/Describe any additional treatment elements that were included. ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
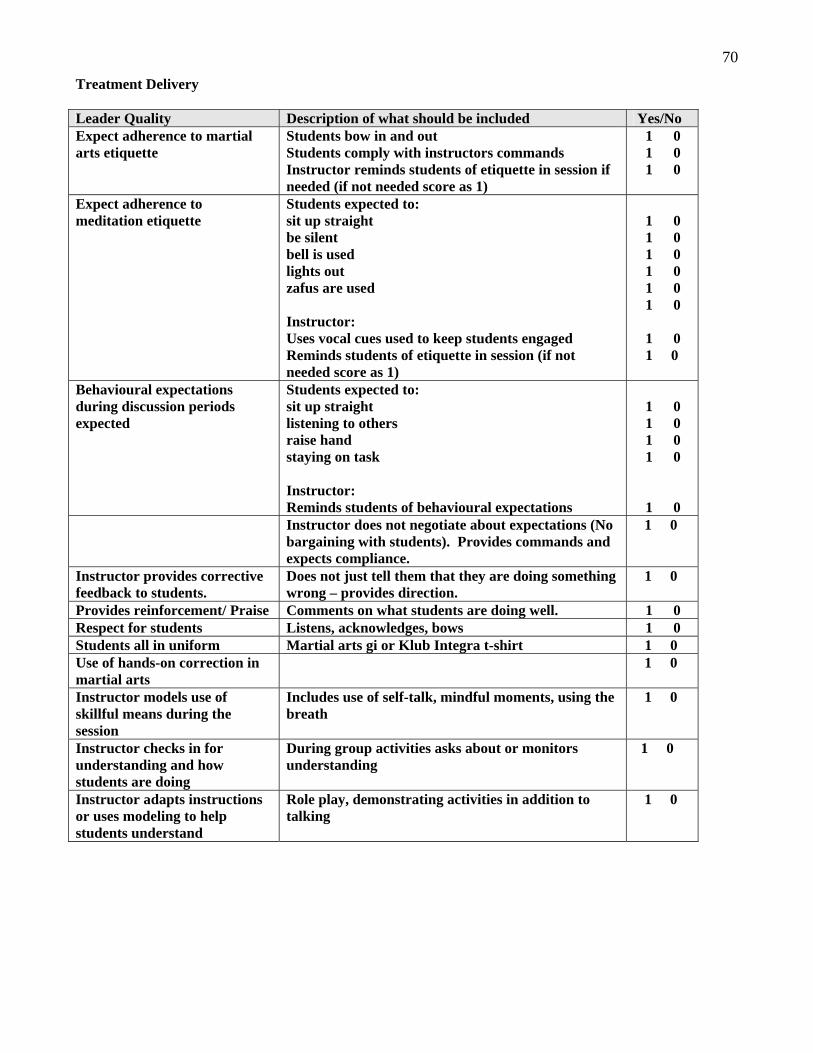
70
Treatment Delivery Leader Quality Description of what should be included Yes/No Expect adherence to martial arts etiquette
Students bow in and out Students comply with instructors commands Instructor reminds students of etiquette in session if needed (if not needed score as 1)
1 0 1 0 1 0
Expect adherence to meditation etiquette
Students expected to: sit up straight be silent bell is used lights out zafus are used Instructor: Uses vocal cues used to keep students engaged Reminds students of etiquette in session (if not needed score as 1)
1 0 1 0 1 0 1 0 1 0 1 0 1 0 1 0
Behavioural expectations during discussion periods expected
Students expected to: sit up straight listening to others raise hand staying on task Instructor: Reminds students of behavioural expectations
1 0 1 0 1 0 1 0
1 0 Instructor does not negotiate about expectations (No
bargaining with students). Provides commands and expects compliance.
1 0
Instructor provides corrective feedback to students.
Does not just tell them that they are doing something wrong – provides direction.
1 0
Provides reinforcement/ Praise Comments on what students are doing well. 1 0 Respect for students Listens, acknowledges, bows 1 0 Students all in uniform Martial arts gi or Klub Integra t-shirt 1 0 Use of hands-on correction in martial arts
1 0
Instructor models use of skillful means during the session
Includes use of self-talk, mindful moments, using the breath
1 0
Instructor checks in for understanding and how students are doing
During group activities asks about or monitors understanding
1 0
Instructor adapts instructions or uses modeling to help students understand
Role play, demonstrating activities in addition to talking
1 0
71
Appendix I: Qualitative and Quantitative Posters
Qualitative Poster Submission to SRCD
Mindfulness Martial Arts: Engaging and Promoting Resilience in Youth with Learning Disabilities and Self-Regulation Difficulties
While persistent academic struggles are common in youth with learning disabilities (LD), many
also experience significant social-emotional difficulties (e.g., anxiety, depression, behavior problems,
ADHD, peer relation difficulties; e.g., Capozzi et. al., 2008). While overlapping cognitive/processing
difficulties may account for such co-morbidities, the lived experiences of youth with LD may also play
a contributing role. Due to repeated patterns of difficulties and failures, youth may avoid challenging
interactions, activities, thoughts and emotions associated with failure or distress, either by withdrawing
from the situation or engaging in problem behaviors that facilitate avoidance or distraction (Ducharme
& Harris, 2005). This cycle of experiential avoidance reduces discomfort but, in the long term, may
increase risk for psychopathology and prevent participation in activities that support resilience.
Mindfulness Martial Arts (MMA, Badali, 2002) is a manualized group treatment, developed for
youth (aged 12-18) with LD and co-occurring self-regulation difficulties, to diminish experiential
avoidance. MMA integrates mindfulness meditation, cognitive behavior therapy, and behavior
modification into a 20-week martial arts group training program. Martial arts acts as an active
component of change (e.g., promoting planning, inhibition, flexibility) and a non-stigmatizing milieu
that youth find highly engaging. Parents are involved to promote generalization of skills. The goal of
MMA is to improve youth’s self-awareness and ability to face challenges, so that they can learn and
apply new, more adaptive coping strategies.
Six boys and five parents completed semi-structured interviews to investigate gains made in
MMA and the components or processes that support these gains. Interviews were audiotaped and
transcribed. The boys (aged 12-16) all had a diagnosed LD. Four presented with co-occurring ADHD
and two with anxiety and peer relation difficulties. Using a modified grounded theory framework,
themes were extracted from transcripts by two independent readers and then primary themes were
determined through discussion.
72
Multiple outcomes and processes were identified. Overall, youth and parents were highly
satisfied and felt the program was helpful. Respondents emphasized the importance of milieu,
speaking about the desire to master martial arts and be part of a socially valued activity. The
relationship with the sensei (e.g., feeling heard and safe, with clear expectations) was identified as
paramount. Many youth reported that they did not like the mindfulness practices (e.g., meditation) but
acknowledged that it was the most important part of MMA. Youth recognized its impact on their self-
awareness and that it enabled them to be calm, think straight, stop and think, and change patterns of
automatic responding. Mindful self-talk assisted youth in coping with challenges and persisting. While
therapy was uniform across youth, the type of gains made differed depending on the youth’s
presenting concerns/goals. Gains were seen as “a work in progress” and all respondents reported that
change took time (e.g., second half of MMA).
These results suggest that MMA may be an effective resiliency-based treatment for youth with
LD and a range of self-regulation disorders. Results highlight the importance of milieu in engaging
youth, active components of change, and outcomes to explore in future quantitative controlled studies.
73
Quantitative Poster Submission to SRCD
Mindfulness Martial Arts: Improving Executive Functions in Youth with Learning Disabilities and Self-Regulation Difficulties
Youth with Learning Disabilities (LD) are at increased risk for self-regulation difficulties, such
as Attention-Deficit/Hyperactivity Disorder (ADHD; e.g., Capozzi et. al., 2008). Executive function
weaknesses, common to both LD and ADHD populations, are linked to a variety of behavioral and
developmental outcomes (e.g., Blair & Razza, 2007). Given this relation, executive functions are
considered a key process to target in treatment.
Mindfulness interventions may be helpful in addressing executive function weaknesses.
Mindfulness meditation has been shown to improve self-observation, selfcontrol, and attention in
adults (Baer, 2003). In youth, improvements in flexibility (Zylowska et al., 2008) and metacognitive
skills, including working memory, planning, and organization (Flook et al., 2010) have been reported.
Mindfulness Martial Arts (MMA) is a manualized group treatment (Badali, 2002) for youth
(aged 12-18) with LD and self-regulation difficulties. The program is designed to improve self-
awareness, as well as the ability of youth to be present with challenges, in order to learn and apply
new, more adaptive coping strategies. MMA integrates mindfulness meditation, cognitive behavior
therapy, and behavior modification into a 20-week martial arts group training program. Martial arts
acts as an active component of change (e.g., promoting planning, motor control, inhibition, and
flexibility), in a nonstigmatizing milieu that youth find highly engaging. MMA shows promise as an
effective intervention for youth with LD and either externalizing or internalizing symptoms. Compared
to waitlist controls, youth with LD and ADHD showed a significant decrease in parent-reported
externalizing behaviors, while youth with LD and anxiety demonstrated decreased levels of anxiety
(Haydicky et al., submitted). The purpose of the present study was to extend these findings by
examining the impact of MMA on executive functions, which could, in part, underlie observed
behavioral changes.
Participants were 26 youth (Mage = 13, SD= 1.5) with LD and self-regulation difficulties (e.g.,
ADHD, externalizing and/or internalizing behaviors) enrolled at a children’s mental health centre for
74
youth with LD and mental health difficulties. The Test of Variables of Attention (TOVA; Greenberg et
al., 2008) and the Delis-Kaplan Executive Function System Trail-Making test (Delis, Kaplan, &
Kramer, 2001) were completed pre- and post-intervention to investigate changes in attention,
impulsivity and flexibility. Given the high rates of comorbidities between LD, ADHD and executive
functions weaknesses, the Conners-3 was completed by parents at pre-test to identify youth with
clinically significant symptoms of ADHD.
Repeated Measures ANOVAs indicated significant improvements in impulsivity, overall (TOVA
Commission errors, F(1,21)=4.68, p=.04). When groups were divided by clinically significant levels of
hyperactive-impulsive symptoms, only youth with these symptoms demonstrated significant decreases
in impulsivity (F(1,18)=6.93, p=.02). No statistically significant differences were noted for attention
(TOVA Omission Errors). A trend towards improved flexibility was also found (Trails Number-Letter
Switching, F (1, 22) = 3.79, p=.06), with no significant differences based on ADHD
symptoms. See Figure 2. Taken together, these results provide preliminary support for the
effectiveness of MMA in improving inhibition and flexibility in youth with LD and selfregulation
difficulties. Further research using a control group and larger sample size is needed.