mini implants
TRANSCRIPT

connective tissue diseases other than rheumatoid arthritisare associated with increased bone resorption and peri-implant infections. Before recommending DI therapy, theclinician should verify the severity of the patient’s salivaryflow impairment and medical condition.
Although no evidence indicates immunocompromisedstatus contraindicates DI therapy, medical advice shouldbe sought before beginning treatment. Strict anti-infectivemeasures should be maintained for these patients.
Patients with severe ectodermal dysplasia and severeoligodontia or hypodontia are often managed with DI,especially if there is a limited amount of bone. The implantsuccess rates in these patients are excellent. The mostappropriate age for dental implant treatment in growingchildren has yet to be identified. Dental implants may notbe ideal for patients with oral lichen planus because ofthe limited capacity of the involved epithelium to adhereto the titanium surface. Peri-implant mucositis and peri-implantitis appear to be slightly more common in patientswith oral lichen planus than in control patients. Desquama-tive gingivitis is associated with a greater incidence of peri-implant mucositis. Disease manifestations are not alteredby implant placement. Careful long-term monitoring ofboth oral lichen planus lesions and dental implants isneeded to detect possible malignant transformation.
For patients with neuropsychiatric disorders, DI treat-ment can be successful, but poor oral hygiene, oral paraf-unctions, harmful habits, and behavioral problems arecommon in such patients and can compromise theoutcome. Appropriate patient selection and adequate med-ical advice are essential before implant therapy is under-taken in these individuals.
Although titanium has been considered an inert mate-rial, more recent findings note the development of titaniumallergy that can play a critical role in implant failure. It is esti-mated that 0.6% of DI patients have titanium allergy. A
significantly higher risk of positive allergic reactions hasbeen noted in patients who have allergic symptoms afterimplant placement or unexplained implant failures. Patientsallergic to other metals are more likely to have titanium al-lergy and should be evaluated before treatment. Long-termclinical and radiologic follow-up is recommended, alongwith consideration of alternative materials.
Clinical Significance.—There are few abso-lute contraindications to the use of DI therapy.However, several conditions can increase therisk of either failure of this treatment or thedevelopment of complications. Cliniciansshould always consider the range of treatmentoptions available for the individual patient’scase andweigh the potential advantages and dis-advantages, along with patient preferences andwishes. Patients with systemic conditionsshould be assessed using a cost-benefitapproach to their quality of life and life expec-tancy. Implant surgical procedures must alwaysbe conducted with strict asepsis, minimaltrauma, and the avoidance of stress or unaccept-able hemorrhage. Patients must be onboardwith close maintenance therapy, optimal oralhygiene behaviors, and the avoidance of smok-ing or other risk factors that can compromisedental implant treatment.
Diz P, Scully C, Sanz M: Dental implants in the medically compro-mised patient. J Dent 41:195-206, 2013
Reprints available from P Diz, Stomatology Dept, School of Medi-cine and Dentistry, Santiago de Compostela Univ, c/Entrerr�ıos sn,15782 Santiago de Compostela, La Coru~na, Spain; e-mail:[email protected]
Mini implants
Background.—Insufficient quality and/or quantity ofavailable bone can compromise the surgical placement ofdental implants. Patients who have narrow alveolar ridgesand want dental implants may require residual ridgeaugmentation or guided bone regeneration procedures,vertical distraction osteogenesis, ridge split or ridge expan-sion procedures, or the use of reduced diameter implantswith or without bone grafting. Mini implants used for defin-itive prosthodontics treatment offer the advantages of low
cost, ability to be placed in narrow or wide ridges, simplifiedtreatment procedures with no steep learning curve for thepractitioner, usually being placed in flapless surgical proce-dures, and a one-piece design that allows immediateloading in a single clinical visit. Disadvantages include theneed for multiple implants because of unpredictabilityand lack of guidelines based on scientific evidence, limitedinformation about long-term survival, potential for fractureof the implant during placement, lack of forgiveness
Volume 59 � Issue 1 � 2014 41
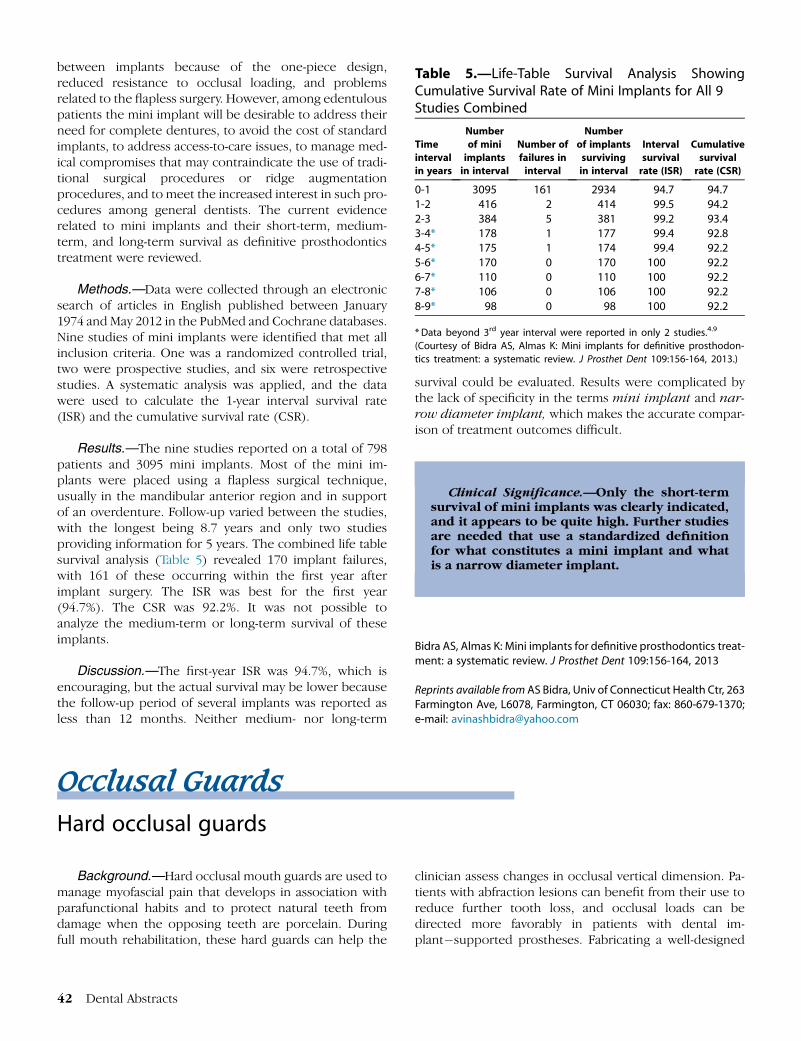
Table 5.—Life-Table Survival Analysis ShowingCumulative Survival Rate of Mini Implants for All 9Studies Combined
Time
interval
in years
Number
of mini
implants
in interval
Number of
failures in
interval
Number
of implants
surviving
in interval
Interval
survival
rate (ISR)
Cumulative
survival
rate (CSR)
0-1 3095 161 2934 94.7 94.71-2 416 2 414 99.5 94.22-3 384 5 381 99.2 93.43-4* 178 1 177 99.4 92.84-5* 175 1 174 99.4 92.25-6* 170 0 170 100 92.26-7* 110 0 110 100 92.27-8* 106 0 106 100 92.28-9* 98 0 98 100 92.2
*Data beyond 3rd year interval were reported in only 2 studies.4.9
(Courtesy of Bidra AS, Almas K: Mini implants for definitive prosthodon-
tics treatment: a systematic review. J Prosthet Dent 109:156-164, 2013.)
between implants because of the one-piece design,reduced resistance to occlusal loading, and problemsrelated to the flapless surgery. However, among edentulouspatients the mini implant will be desirable to address theirneed for complete dentures, to avoid the cost of standardimplants, to address access-to-care issues, to manage med-ical compromises that may contraindicate the use of tradi-tional surgical procedures or ridge augmentationprocedures, and to meet the increased interest in such pro-cedures among general dentists. The current evidencerelated to mini implants and their short-term, medium-term, and long-term survival as definitive prosthodonticstreatment were reviewed.
Methods.—Data were collected through an electronicsearch of articles in English published between January1974 and May 2012 in the PubMed and Cochrane databases.Nine studies of mini implants were identified that met allinclusion criteria. One was a randomized controlled trial,two were prospective studies, and six were retrospectivestudies. A systematic analysis was applied, and the datawere used to calculate the 1-year interval survival rate(ISR) and the cumulative survival rate (CSR).
Results.—The nine studies reported on a total of 798patients and 3095 mini implants. Most of the mini im-plants were placed using a flapless surgical technique,usually in the mandibular anterior region and in supportof an overdenture. Follow-up varied between the studies,with the longest being 8.7 years and only two studiesproviding information for 5 years. The combined life tablesurvival analysis (Table 5) revealed 170 implant failures,with 161 of these occurring within the first year afterimplant surgery. The ISR was best for the first year(94.7%). The CSR was 92.2%. It was not possible toanalyze the medium-term or long-term survival of theseimplants.
Discussion.—The first-year ISR was 94.7%, which isencouraging, but the actual survival may be lower becausethe follow-up period of several implants was reported asless than 12 months. Neither medium- nor long-term
42 Dental Abstracts
survival could be evaluated. Results were complicated bythe lack of specificity in the terms mini implant and nar-row diameter implant, which makes the accurate compar-ison of treatment outcomes difficult.
Clinical Significance.—Only the short-termsurvival of mini implants was clearly indicated,and it appears to be quite high. Further studiesare needed that use a standardized definitionfor what constitutes a mini implant and whatis a narrow diameter implant.
Bidra AS, Almas K: Mini implants for definitive prosthodontics treat-ment: a systematic review. J Prosthet Dent 109:156-164, 2013
Reprints available fromAS Bidra, Univ of Connecticut Health Ctr, 263Farmington Ave, L6078, Farmington, CT 06030; fax: 860-679-1370;e-mail: [email protected]
Occlusal GuardsHard occlusal guards
Background.—Hard occlusal mouth guards are used tomanage myofascial pain that develops in association withparafunctional habits and to protect natural teeth fromdamage when the opposing teeth are porcelain. Duringfull mouth rehabilitation, these hard guards can help the
clinician assess changes in occlusal vertical dimension. Pa-tients with abfraction lesions can benefit from their use toreduce further tooth loss, and occlusal loads can bedirected more favorably in patients with dental im-plant�supported prostheses. Fabricating a well-designed