misoprostol for preventing postpartum hemorrhage and for postabortion care harshad sanghvi patricia...
TRANSCRIPT

Misoprostol for Preventing Postpartum Hemorrhage and for
Postabortion Care
Harshad SanghviPatricia Stephenson
MAQ 2006 Mini University, 27 0ctober 2006

Session Objectives
Describe the importance of PPH and postabortion complications as causes of maternal death.Describe the efficacy and safety of misoprostol for prevention of PPH and for medical management of postabortion care.Describe potential barriers to program implementation and scale up and ways to overcome them.

PPH: Magnitude of the Problem
About 30% of all maternal deaths worldwide are due to bleeding.
PPH is the most common cause of maternal death.
Most of deaths due to bleeding occur postpartum.

Definition of PPHDefinition of PPH
PPH : Blood loss greater than 500 ml Severe PPH: Blood loss greater than 1000 ml
PPH : Blood loss greater than 500 ml Severe PPH: Blood loss greater than 1000 ml
Any blood loss that causes a physiologic change that threatens a woman’s life

Incidence of PPH
Blood Loss (n = 434)Blood Loss (n = 434)
Mean + SE 265.18 + 10.95
Range 20 - 1600
Median 200
Mode 100
Acute PPH 57 (13.2 %)
Acute severe PPH
8 (1.8 %)
Goudar, Eldavitch, Bellad, 2003

Etiology of PPH
Uterine atony (~3/4 cases)
Other •Episiotomy•Retained placenta•Trauma - uterine rupture, inversion,
cervical laceration, vaginal hematoma•Postpartum infections•Rarely : Coagulopathy

Risk Factors for PPH
Risk Factors for PPH
Preeclampsia, previous PPH, multiple gestation, arrest of descent, maternal hypotension,
coagulation disorder, Asian or Hispanic, delivery with forceps or vacuum, augmented labor,
nulliparity, multiparity, polyhydramnios, underlying anemia
Preeclampsia, previous PPH, multiple gestation, arrest of descent, maternal hypotension,
coagulation disorder, Asian or Hispanic, delivery with forceps or vacuum, augmented labor,
nulliparity, multiparity, polyhydramnios, underlying anemia
Up to 90% of women who experience PPH have no identifiable risk factors

Prevention of PPH
Active management of third stage of labor (AMSTL)
• Uterotonic after birth of baby
• Controlled cord traction
• Fundal massage
Restricting episiotomy & unnecessary obstetric interventions
Prevention & treatment of anemia due to iron deficiency, hook worm, malaria

Active vs. Expectant Management
Management of third stage of labor
Blood Loss > 500 mls
Blood loss > 1000 mls
Expectant (n=3126)
13.6% 2.6%
Active (n=3158)
5.2% 1.7%
Relative risk 0.38 (0.32-0.46)
0.33(0.21-0.51)
Number needed to treat
12 (10-15) 57(42-89)
Prendiville, Elbourne, McDonald, The Cochrane Library issue 3, 2003
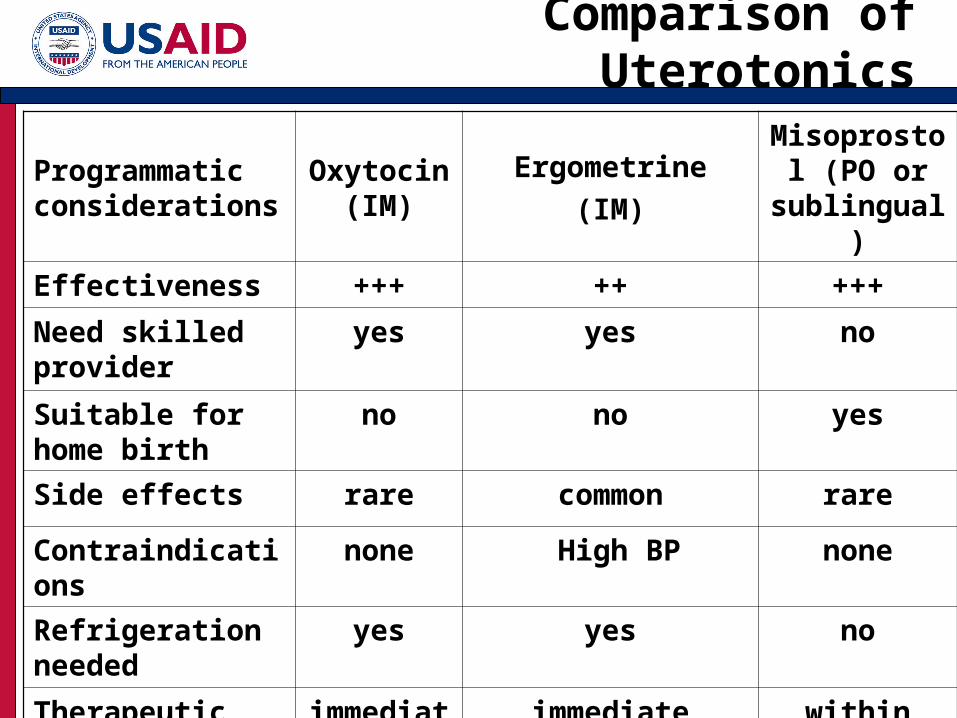
Comparison of Uterotonics
Programmatic considerations
Oxytocin (IM)
Ergometrine(IM)
Misoprostol (PO or
sublingual)
Effectiveness +++ ++ +++
Need skilled provider
yes yes no
Suitable for home birth
no no yes
Side effects rare common rare
Contraindications
none High BP none
Refrigeration needed
yes yes no
Therapeutic effect
immediate
immediate within minutes

Misoprostol mystery madness (boo!)

Clinical demonstration study 1
Oral Misoprostol reduced PPH incidence to 6%Double-blind placebo controlled study 2
Oral Misoprostol reduced need for treatment of PPH from 8.4% 2.8%
Rectal Misoprostol vs. Syntometrin for 3rd stage 3
Similar reduction in length of 3rd stage, postpartum blood loss and postpartum hemoglobin; Higher BP with Syntometrin
Oral Misoprostol vs. Placebo 4
PPH: 7% vs 15%Need for therapeutic Oxytocin: 16% vs. 38%
Misoprostol: Evidence
1: El-Refaey, 1997; 2: Hofmeyr, 1998; 3: Bamigboye, 1998; 4: Surbek, 1999

Double-blind placebo controlled WHO multi-center RCT: Oxytocin vs. Misoprostol in hospital 1
8 countries Oxytocin (n=9266); Misoprostol (n=9264)Severe PPH (1000cc): 3% vs. 4%Misoprostol – higher incidence of shivering
Conclusion: Oxytocin preferred over Misoprostol
Double blind placebo controlled RCT in rural Guinea Bissau: Misoprostol vs. Placebo
Misoprostol alone reduces severe PPH (1000mls+) 11% vs. 17% RR 0.66 (0.44-0.98)
More Evidence
1: Gulmezoglu,et al., Lancet 2001, Høj BMJ 2005
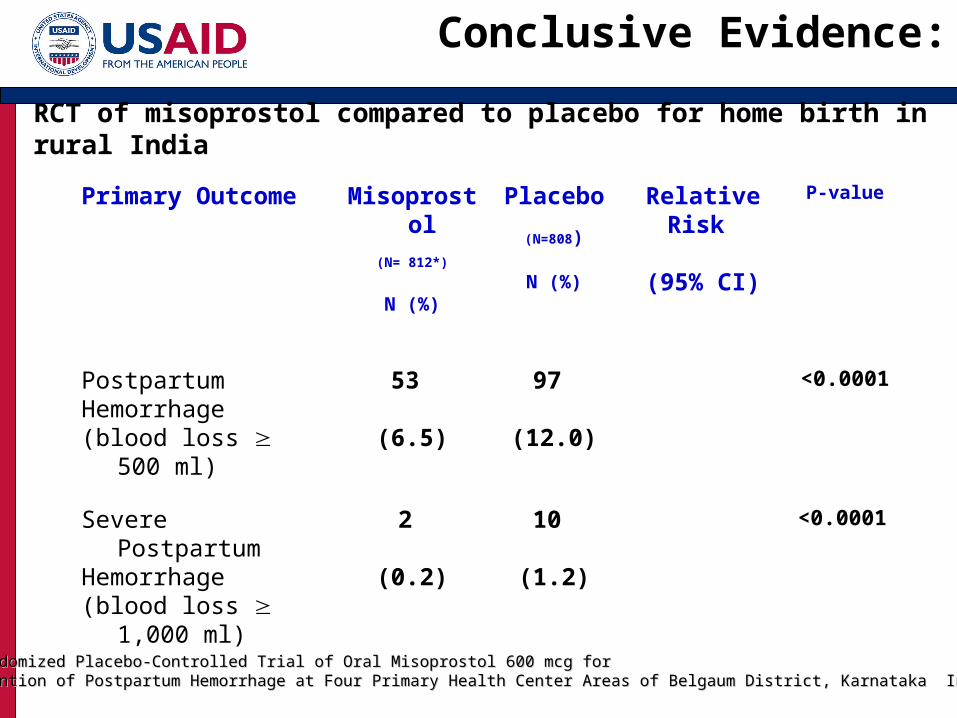
RCT of misoprostol compared to placebo for home birth in rural India
Primary Outcome Misoprostol
(N= 812*)
N (%)
Placebo
(N=808)
N (%)
RelativeRisk
(95% CI)
P-value
Postpartum Hemorrhage(blood loss 500
ml)
53
(6.5)
97
(12.0)
0.53
(0.39, 0.74)
<0.0001
Severe Postpartum Hemorrhage (blood loss 1,000
ml)
2
(0.2)
10
(1.2)
0.20
(0.04, 0.91)
<0.0001
A Randomized Placebo-Controlled Trial of Oral Misoprostol 600 mcg for A Randomized Placebo-Controlled Trial of Oral Misoprostol 600 mcg for Prevention of Postpartum Hemorrhage at Four Primary Health Center Areas of Belgaum District, Karnataka IndiaPrevention of Postpartum Hemorrhage at Four Primary Health Center Areas of Belgaum District, Karnataka India
Conclusive Evidence:

Blood Loss Distribution
MM PP
9595thth Percentile Percentile
M: 500 mlM: 500 ml
P: 800 mlP: 800 ml
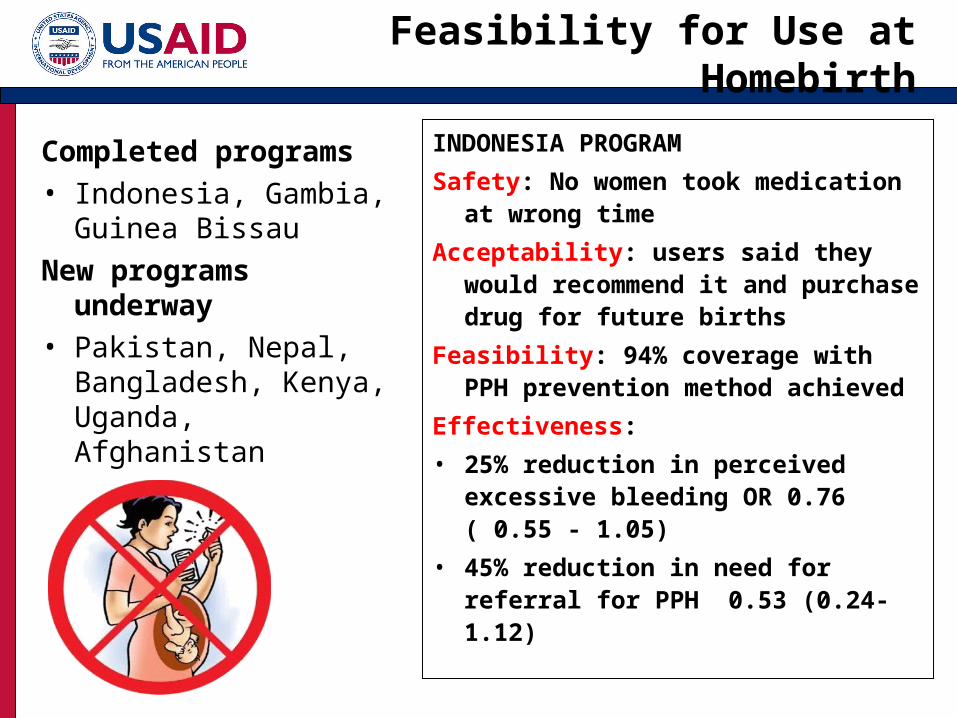
Completed programs• Indonesia, Gambia,
Guinea BissauNew programs
underway• Pakistan, Nepal,
Bangladesh, Kenya, Uganda, Afghanistan
INDONESIA PROGRAM
Safety: No women took medication at wrong time
Acceptability: users said they would recommend it and purchase drug for future births
Feasibility: 94% coverage with PPH prevention method achieved
Effectiveness:
• 25% reduction in perceived excessive bleeding OR 0.76 ( 0.55 - 1.05)
• 45% reduction in need for referral for PPH 0.53 (0.24-1.12)
Feasibility for Use at Homebirth
Treatment of PPH
Even under the best circumstances, all PPH is not preventable
Once severe PPH occurs, death can follow very rapidly

Clinical Interventions
Basic EmOC• Management of shock • Uterotonics • Bimanual compression• Suturing of
lacerations• Aortic compression• Manual removal of
placenta
Comprehensive EmOC
• Uterine artery ligation• B-lynch procedure• Hysterectomy• Blood transfusion

Promising Interventions
Home based Life Saving Skills
MisoprostolHydrostatic tamponade

Issues and Challenges
Policy and supportive environmentSupply chain logisticsHuman capacity and trainingCommunity involvement and mobilizationReferral links


13% of maternal deaths due to abortion.15-20% of recognized pregnancies are miscarried or become nonviable.20 million unsafe abortions occur each year.
Postabortion Complications: Magnitude of the Problem

Definitions
Early: before 12 weeksLate: between 12 & 20 weeksThreatened miscarriage: spotting or cramping in 1st 20 weeks – usually with a viable continuing pregnancyIncomplete: expulsion of only part of the uterine contents or rupture of the membranesComplete: expulsion of all products of conceptionMissed: retention of a dead embryo or fetus

Treatment Options
SurgeryManual vacuum aspiration (MVA)Electric/foot pump vacuum aspirationSharp curettage
Expectant managementMedical management with misoprostol

Misoprostol: Indications
Indication: Treatment of incomplete abortion and
missed abortion for women with uterine size less than or equal to 12 weeks LMP
Contraindications:Sepsis or pelvic infectionShockSuspicion of ectopic pregnancyIUD in place (remove)

Misoprostol 600 mcg
MVA RR(95% CI)
Complete Evacuation
96.3 91.5 1.05(0.98 -1.14)
Complications
0.9% 9.8% 0.01(0.01-0.78)
Acceptability
94.2% 94.7%
Source: Weeks et al 2005Increased bleeding for 6 hours, decreased pain with misoprostol
Evidence: Uganda

Evidence: Vietnam: Dose
Nguyen et al Contraception 2005• No difference in outcomes with single
dose of 600mcg misoprostol or with two doses.
• Most (96%) women tolerated side effects of bleeding up to 4 days and cramping for a day

Misoprostol: Evidence
Zhang et al NEJM 2005RCT N=652 women compared 800 mcg misoprostol vaginally with vacuum aspiration for missed abortion.84% of miso group and 97% of VA group had complete uterine evacuation by day 8Both groups satisfied with treatmentMiso instead of aspiration used in an outpatient setting reduces the costs of services
Evidence: Efficacy
Success rates66-100% for incomplete abortion using recommended dose of 600 mcg orally60-93% for missed abortion using recommended dose of 800 mcg vaginallyHighest success rates are achieved with extended follow up (7-14 days) to allow completion of expulsion
Evidence: Safety
Side effects: (short lived)Nausea and vomitingDiarrheaFever, chillsCrampingBleeding

Potential Advantages
Misoprostol may help expand PAC services: in most resource constrained environments surgical services are not available beyond the district hospital.Availability of MVA and other surgical equipment is a significant bottleneck.Medical management may reduce the need for surgically trained health manpower.Lower cost; few side effects; most side effects mild and of short duration.Additional follow up required may provide opportunities for family planning counseling and services.

Drawbacks
It is not for everyone.Even if indicated, some women will still require surgical treatment.Providers still need to be trained to correctly diagnose missed or incomplete abortion and rule out contraindications. Takes longer to evacuate the uterus and may require a follow up visit – women may be lost to follow up.

Issues and Challenges
How do we:Expand PAC services to health centers and health posts?Train lower-level providers to safely administer misoprostol?Involve the community as a resource?Structure services to promote family planning?Overcome policy barriers of registration of misoprostol for off-label uses?