mitochondrial disorders: overview of diagnostic tools and ... · jour ped biochemistry pg 2.jpg ......
TRANSCRIPT
Jour Ped Biochemistry.jpg
/ "
Journal of
Biochemistry Special Issue: Mitochondrial, Metabolic and Nutritional Disorders Associated with Neurodevelopmental Disorders Guest Editor: Richard E. Frye
LAST NUMBER OF
THIS VOLUME
/ "
Journal of
Biochemistry Special Issue: Mitochondrial, Metabolic and Nutritional Disorders Associated with Neurodevelopmental Disorders Guest Editor: Richard E. Frye
LAST NUMBER OF
THIS VOLUME
Jour Ped Biochemistry pg 2.jpg
Journal of Pediatric Biochemistry Volume 2, Number 4, 2012
Special Issue: Mitochondrial , Metabolic and Nutritional Disorders Associated with Neurodevelopmental Disorders Guest Editor: Richard E. Frye
CONTENTS
RE Frye and D.A. Rossignol Mitochondrial and metabolic abnormalilies in neurodevelopmenlal disorders 177
RE Frye and D.A. Rossignol Melabolic disorders and abnonmal~ies associated with autism spectrum disorder 181
F.D. Kendall Milochondrial disorders: Overview of diagnoslic tools and new diagnoslic trends 193
L. P. van den Heuvel. J.AM. Smeitink and R.J. T. Rodenburg New approaches to diagnosing m~ochondrial abnonmalilies: Taking the next step . 205
A Chauhan. F. Gu and V. Chauhan Mitochondrial respiratory chain defects in autism and other neurodevelopmental disorders 213
A EI-Ansary Oxidative stress and mitochondrial dysfunction as key players in neurological disorders of childhood 225
RE Frye and D.A. Rossignol Treatments for mitochondrial dysfunction associated with autism spectrum dis-o~e~ 241
M. C. DeSoto and R. T. Hit/an Synthetic folic acid supplementation during pregnancy may increase the risk of developing autism 251
D.A. Rossignol and R. E. Frye Folate receptor alpha autoimmunity and cerebral folate deficiency in autism spectrum disorders 263
Author Index Volume 2 (2012) 273
~ VISIT OUR WEBSITE ON WWW . IOSPRESS . NL ~
Journal of Pediatric Biochemistry Volume 2, Number 4, 2012
Special Issue: Mitochondrial, Metabolic and Nutritional Disorders Associated with Neurodevelopmental Disorders Guest Editor: Richard E. Frye
CONTENTS
R.E. Frye and D.A. Rossignol Mitochondrial and metabolic abnormalities in neurodevelopmental disorders 177
R.E. Frye and D.A. Rossignol Metabclic disorders and abnonmal~ies associated with autism spectrum disorder 181
F. D. Kendall Mitochondrial disorders: Overview of diagnostic tools and new diagnostic trends 193
L. P. van den Heuvel. J.A.M. Smeitink and R.J. T. Rodenburg New approaches to diagnosing m~ochondrial abnonmal~ies: Taking the next step . 205
A. Chauhan, F. Gu and V. Chauhan Mitochondrial respiratory chain defects in autism and other neurodevelopmental disorders 213
A. EI·Ansary Oxidative stress and mitochondrial dysfunction as key players in neurological disorders of childhood 225
R.E. Frye and D.A. Rossignol Treatments for mitochondrial dysfunction associated with autism spectrum dis-o~ers 241
M. C. DeSoto and R. T. Hit/an Synthetic folic acid supplementation during pregnancy may increase the risk of developing autism 251
D.A. Rossignol and R.E. Frye Folate receptor alpha autoimmunity and cerebral folate deficiency in autism spectrum disorders 263
Author Index Volume 2 (2012) 273
~ V ISIT OUR WEBSITE ON WWW . IOSPRESS . NL ~
Journal of Pediatric Biochemistry 2 (2012) 193–203 193DOI 10.3233/JPB-120061IOS Press
Review Article
Mitochondrial disorders: Overview ofdiagnostic tools and new diagnostic trends
Fran D. KendallVirtual Medical Practice, LLC, 5579 Chamblee Dunwoody Rd, Ste 110, Atlanta, GA 30338, USATel.: +1 404 720 0820; Fax: +1 404 793 0775; E-mail: [email protected]
Abstract. Mitochondrial disorders typically present with widespread, clinical features in all age groups and ethnicities and areoften progressive and degenerative in nature. Because their clinical presentation is so variable and typically leads to widespreadmultisystem problems, diagnosis based on history and physical findings alone is often difficult, particularly for physiciansunfamiliar with this group of diseases. Traditional diagnostic tools, which include invasive muscle biopsies for a variety ofhistological studies, functional assays, and enzymology, are costly, typically require a surgical procedure, are not definitivelydiagnostic in all cases and generate data that for the non-mitochondrial specialist is often difficult to interpret. Recent advanceswith expanded gene testing, in some cases utilizing easily obtainable urine samples, and noninvasive enzymatic testing are provingto increase patient accessibility to testing modalities and will likely lead to more rapid and accurate diagnosis, and ultimatelyimprove management and treatment of affected individuals.
Keywords: Mitochondrial, disease, diagnose, test, symptom, gene, buccal swab, muscle biopsy, next gen sequencing
1. Introduction
Mitochondrial disorders are a known but poorly un-derstood group of diseases with a broad neurodevelop-mental impact affecting all ethnicities and age groups.Associated problems range from seizure disorders tomemory loss and dementia to weakness and includeother system involvement such as cardiac or hepaticsymptomatology. Diagnostic options are complex andoften not definitively diagnostic. Developing a clearunderstanding of clinical presentation and associatedradiographic and laboratory abnormalities will allowinvestigating clinicians to evaluate suspectedmitochon-drial patients more accurately leading to more timelyinstitution of a therapeutic regimen for improved qual-ity of life of affected individuals.
2. Mitochondria and mitochondrial diseasedefined
Housed within our body’s cells, the mitochondriacreate energy, or ATP, through the complex chemi-
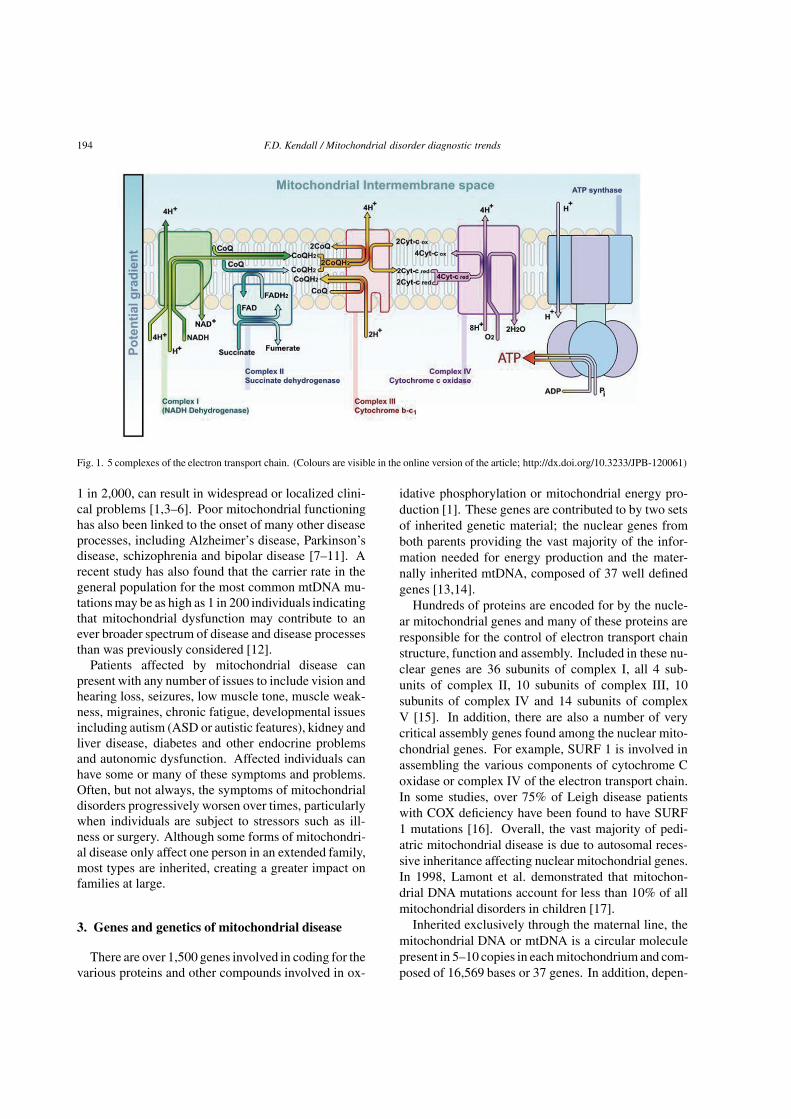
cal reactions that occur in the electron transport chainembedded within the mitochondrial inner membrane.Composed of five complexes, the electron transportchain or respiratory chain generates ATP through anelectrochemical gradient utilizing the breakdown prod-ucts of food in conjunction with phosphate and oxygen(Fig. 1). Over 1,500 genes encode for various proteinsthat ultimately come together like jigsaw puzzle piecesto create energy [1].
Some individuals are born with changes in one ofthese many genes that ultimately alter their mitochon-drial functioning, or sustain injury to the mitochondrialsystem through othermechanisms,such as the drug tox-icity demonstrated with a group of AIDS drugs, eitherof which can result in decreased energy production andmitochondrial disease symptoms [2]. This secondarymitochondrial dysfunction is due to the mitochondriabecoming “sick” or “toxic” due to changes in the cells.
Mitochondrial disorders are a group of diseases thatalter the body’s ability to adequately convert food in-to the energy needed for bodily functions. These dis-eases, which affect up to 1 in 5,000 individuals withseveral more recent studies suggesting a frequency of
1879-5390/12/$27.50 2012 – IOS Press and the authors. All rights reserved
194 F.D. Kendall / Mitochondrial disorder diagnostic trends
Fig. 1. 5 complexes of the electron transport chain. (Colours are visible in the online version of the article; http://dx.doi.org/10.3233/JPB-120061)
1 in 2,000, can result in widespread or localized clini-cal problems [1,3–6]. Poor mitochondrial functioninghas also been linked to the onset of many other diseaseprocesses, including Alzheimer’s disease, Parkinson’sdisease, schizophrenia and bipolar disease [7–11]. Arecent study has also found that the carrier rate in thegeneral population for the most common mtDNA mu-tations may be as high as 1 in 200 individuals indicatingthat mitochondrial dysfunction may contribute to anever broader spectrum of disease and disease processesthan was previously considered [12].
Patients affected by mitochondrial disease canpresent with any number of issues to include vision andhearing loss, seizures, low muscle tone, muscle weak-ness, migraines, chronic fatigue, developmental issuesincluding autism (ASD or autistic features), kidney andliver disease, diabetes and other endocrine problemsand autonomic dysfunction. Affected individuals canhave some or many of these symptoms and problems.Often, but not always, the symptoms of mitochondrialdisorders progressively worsen over times, particularlywhen individuals are subject to stressors such as ill-ness or surgery. Although some forms of mitochondri-al disease only affect one person in an extended family,most types are inherited, creating a greater impact onfamilies at large.
3. Genes and genetics of mitochondrial disease
There are over 1,500 genes involved in coding for thevarious proteins and other compounds involved in ox-
idative phosphorylation or mitochondrial energy pro-duction [1]. These genes are contributed to by two setsof inherited genetic material; the nuclear genes fromboth parents providing the vast majority of the infor-mation needed for energy production and the mater-nally inherited mtDNA, composed of 37 well definedgenes [13,14].
Hundreds of proteins are encoded for by the nucle-ar mitochondrial genes and many of these proteins areresponsible for the control of electron transport chainstructure, function and assembly. Included in these nu-clear genes are 36 subunits of complex I, all 4 sub-units of complex II, 10 subunits of complex III, 10subunits of complex IV and 14 subunits of complexV [15]. In addition, there are also a number of verycritical assembly genes found among the nuclear mito-chondrial genes. For example, SURF 1 is involved inassembling the various components of cytochrome Coxidase or complex IV of the electron transport chain.In some studies, over 75% of Leigh disease patientswith COX deficiency have been found to have SURF1 mutations [16]. Overall, the vast majority of pedi-atric mitochondrial disease is due to autosomal reces-sive inheritance affecting nuclear mitochondrial genes.In 1998, Lamont et al. demonstrated that mitochon-drial DNA mutations account for less than 10% of allmitochondrial disorders in children [17].
Inherited exclusively through the maternal line, themitochondrial DNA or mtDNA is a circular moleculepresent in 5–10 copies in eachmitochondrium and com-posed of 16,569 bases or 37 genes. In addition, depen-

F.D. Kendall / Mitochondrial disorder diagnostic trends 195
Table 1Possible symptoms of mitochondrial disease
BrainDevelopmental delays Migraines SeizuresDementia Autistic Features Atypical cerebral palsyNeuro-psychiatric disturbances Mental retardation Strokes
NervesAbsent reflexes Fainting Neuropathic painWeakness (may be intermittent) Dysautonomia – temperature instability and other dysautonomic problems
MusclesWeakness Irritable bowel syndrome Gastroesophogeal refluxCramping Hypotonia Diarrhea or constipationGastrointestinal problems Muscle pain
DysmotilityPseudo-obstruction
KidneysRenal tubular acidosis or wasting
HeartCardiomyopathy Cardiac conduction defects (heart blocks)
LiverLiver failure Hypoglycemia (low blood sugar)
Ears & EyesVisual loss and blindness Optic atrophy Acquired strabismusPtosis Hearing loss and deafness Retinitis pigmentosaOphthalmoplegia
Pancreas & Other GlandsDiabetes and exocrine pancreatic failure (inability to make digestive enzymes)Parathyroid failure (low calcium)
SystemicFailure to gain weight Unexplained vomiting Respiratory problemsFatigue Short stature
dent on the cell type, there are hundreds to thousands ofmitochondria per cell. These 37 mitochondrial genesencode for 22 tRNAs, 13 polypeptides of the respirato-ry chain including 7 subunits of complex I, one subunitof complex III, 3 subunits of complex IV and 2 subunitsof complex V, and two ribosomal RNAs [13,14].
Mutations arise in mtDNA de novo or are maternal-ly inherited. In most cases, mtDNA point mutationsare inherited whereas large deletions are de novo innature [18].
Another unique feature of the mtDNA is heteroplas-my in which mutated mtDNA may be present in vary-ing amounts with wild type DNA within the same cell.When the percentage ofmutantmtDNA (mutation load)reaches a certain threshold the function of that tissuemay become impaired [18]. The mutation load variesby tissue type, age and specific mutation. Thus, themutation load varies within and between tissues lead-ing to a broad spectrum of clinical symptoms that canrange from healthy and asymptomatic to severely im-pacted [4]. In certain tissues, like blood, there may beselection against some of these mutations with prefer-ential retention of cells with normal mtDNA.
Additional modes of inheritance for mitochondrialdisease include sporadic cases, autosomal dominantforms and X-linked disorders.
4. Clinical features of mitochondrial energydisorders
When faced with a multitude of issues and problems,mitochondrial disease will often become a considera-tion at some point during the evaluation of a complex,undiagnosed patient. Several clinical features or find-ings that are highly suggestive of mitochondrial diseaseinclude the presence of widespread, seemingly unre-lated multisystem problems (Table 1). Mitochondrialdisorders can be the “great mimicker” presenting withany number of these issues often causing confusion forevaluating physicians.
Certain biochemical abnormalities including persis-tent, significant elevations in lactate, the presence ofKreb Cycle intermediates on urine organic acid anal-ysis, specifically in patients over one year of age, ora deficiency in plasma carnitine are all indicators ofmitochondrial disorders [19–21]. In one study, 21 outof 48 patients (43.8%) with a mitochondrial myopathywere found to have elevated esterified carnitine levelswith a concurrent decrease in free carnitine. Four ofthe 21 patients were also shown to have both free andtotal carnitine deficiencies in plasma (Table 2).
Brain MRI abnormalities, including specific Leighdisease lesions, will typically place a patient into an en-
196 F.D. Kendall / Mitochondrial disorder diagnostic trends
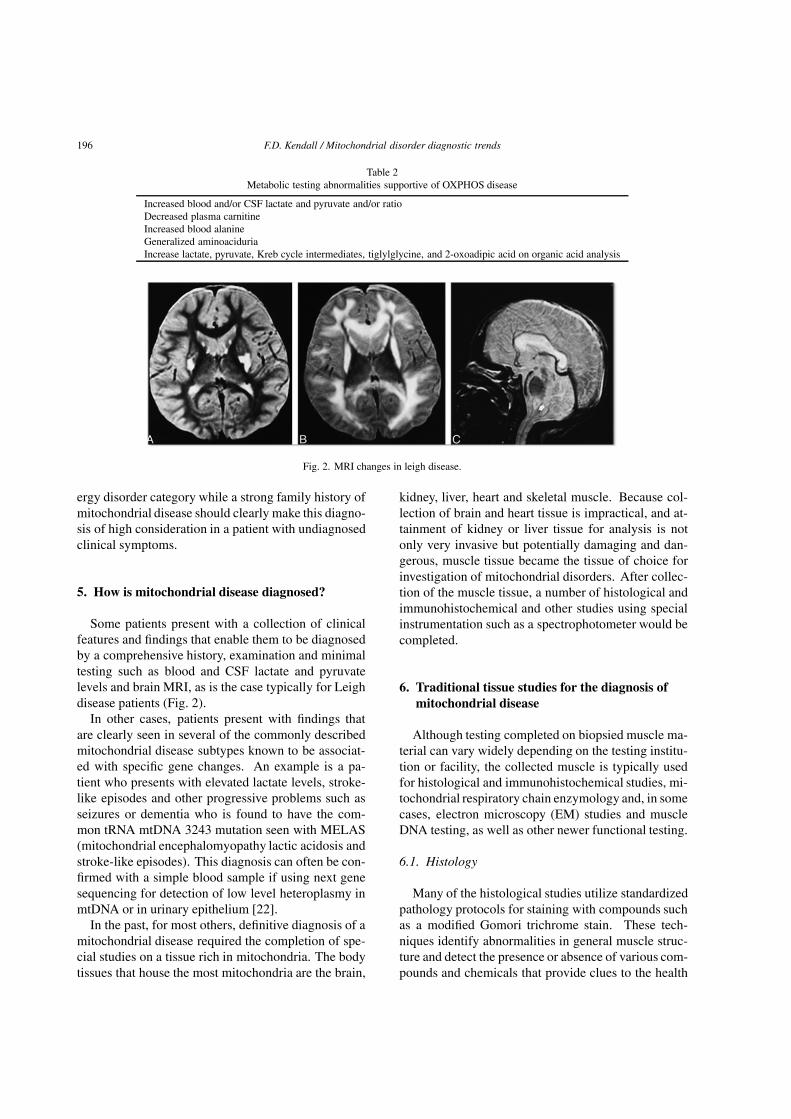
Table 2Metabolic testing abnormalities supportive of OXPHOS disease
Increased blood and/or CSF lactate and pyruvate and/or ratioDecreased plasma carnitineIncreased blood alanineGeneralized aminoaciduriaIncrease lactate, pyruvate, Kreb cycle intermediates, tiglylglycine, and 2-oxoadipic acid on organic acid analysis
Fig. 2. MRI changes in leigh disease.
ergy disorder category while a strong family history ofmitochondrial disease should clearly make this diagno-sis of high consideration in a patient with undiagnosedclinical symptoms.
5. How is mitochondrial disease diagnosed?
Some patients present with a collection of clinicalfeatures and findings that enable them to be diagnosedby a comprehensive history, examination and minimaltesting such as blood and CSF lactate and pyruvatelevels and brain MRI, as is the case typically for Leighdisease patients (Fig. 2).
In other cases, patients present with findings thatare clearly seen in several of the commonly describedmitochondrial disease subtypes known to be associat-ed with specific gene changes. An example is a pa-tient who presents with elevated lactate levels, stroke-like episodes and other progressive problems such asseizures or dementia who is found to have the com-mon tRNA mtDNA 3243 mutation seen with MELAS(mitochondrial encephalomyopathy lactic acidosis andstroke-like episodes). This diagnosis can often be con-firmed with a simple blood sample if using next genesequencing for detection of low level heteroplasmy inmtDNA or in urinary epithelium [22].
In the past, for most others, definitive diagnosis of amitochondrial disease required the completion of spe-cial studies on a tissue rich in mitochondria. The bodytissues that house the most mitochondria are the brain,
kidney, liver, heart and skeletal muscle. Because col-lection of brain and heart tissue is impractical, and at-tainment of kidney or liver tissue for analysis is notonly very invasive but potentially damaging and dan-gerous, muscle tissue became the tissue of choice forinvestigation of mitochondrial disorders. After collec-tion of the muscle tissue, a number of histological andimmunohistochemical and other studies using specialinstrumentation such as a spectrophotometer would becompleted.
6. Traditional tissue studies for the diagnosis ofmitochondrial disease
Although testing completed on biopsied muscle ma-terial can vary widely depending on the testing institu-tion or facility, the collected muscle is typically usedfor histological and immunohistochemical studies, mi-tochondrial respiratory chain enzymology and, in somecases, electron microscopy (EM) studies and muscleDNA testing, as well as other newer functional testing.
6.1. Histology
Many of the histological studies utilize standardizedpathology protocols for staining with compounds suchas a modified Gomori trichrome stain. These tech-niques identify abnormalities in general muscle struc-ture and detect the presence or absence of various com-pounds and chemicals that provide clues to the health

F.D. Kendall / Mitochondrial disorder diagnostic trends 197
Fig. 3. Muscle with ragged red fibers. (Colours are visible in theonline version of the article; http://dx.doi.org/10.3233/JPB-120061)
and function of the biopsied muscle tissue and its mi-tochondria.
The sub-sarcolemmal accumulation of mitochondriaon muscle pathology is considered a hallmark of mi-tochondrial disorders. This accumulation can be vi-sualized utilizing a modified Gomori trichrome stain(ragged red fibers) or with a stain for succinate dehy-drogenase, the latter for the detection of ragged-bluefibers [23,24] (Fig. 3). Increased SDH (succinic dehy-drogenase) staining can also be found in regeneratingmuscle fibers.
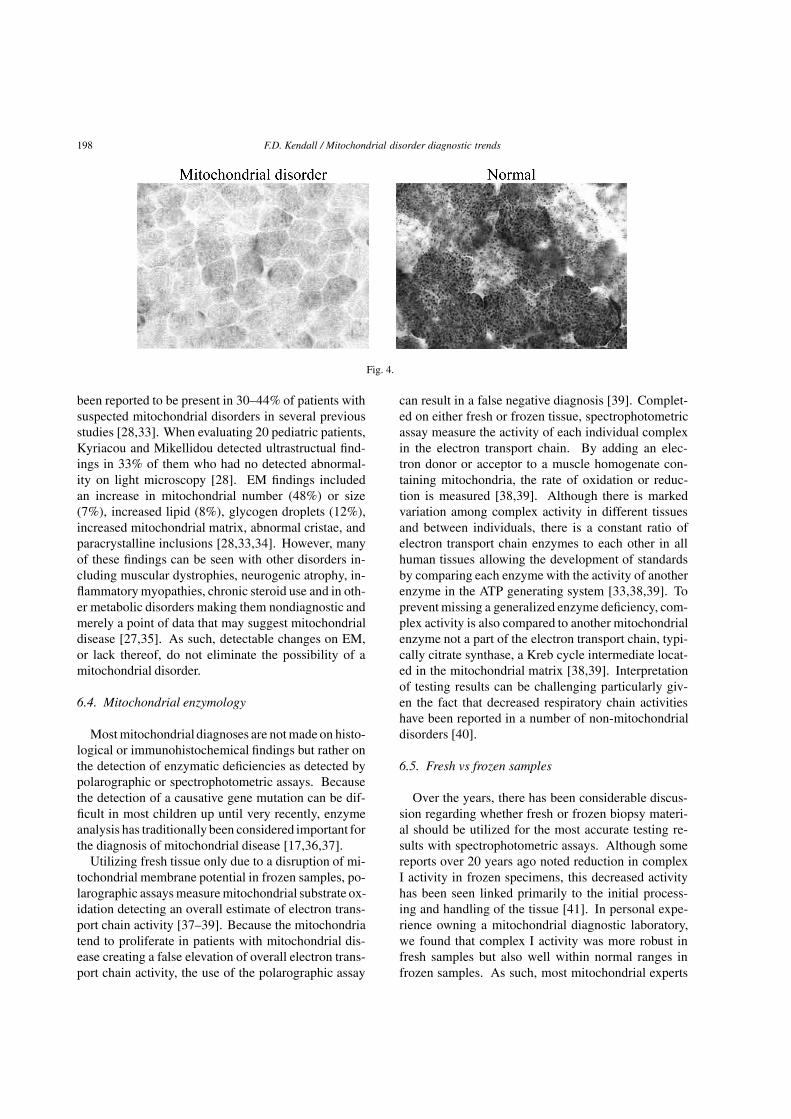
In normal muscle biopsies, virtually all fibers havestaining for CytochromeC oxidase (COX), type I fibersbeing more darkly stained than type II. Cytochromeoxidase-negative fibers are not evident in healthy indi-viduals under the age of 30 years and their presenceis considered pathologic [25]. A diffuse reduction inCOX staining can be seen in Leigh syndromewith COXdeficiency, as demonstrated in (Fig. 4).
Other histological changes that may be seen withbut are not diagnostic of mitochondrial disease includethe presence of excessive lipid, particularly in raggedred fibers. Other nonspecific but frequent findings areinternal nuclei, atrophic fibers, fiber hypertrophy, fibertype grouping, type I or type II fiber atrophy, glycogenand inflammation [24–27].
Overall, the most common pathologic finding onlight microscopy of muscle specimens in mitochondri-
al disorders is a generalized increase in the number ofcytochrome oxidase-negative fibers [28]. However, inmany cases, abnormalities on light microscopy are notpresent at all [24,29]. In 2004, Patterson demonstratedthat 50% of patients with mitochondrial disorders hadnormal light microscopy, findings documented previ-ously by Rollins et al. when they evaluated 118 musclespecimens from mitochondrial patients of all ages [26,30]. Rollins et al. also noted that ragged-redfibers werefound in only 2.5% of cases and cytochrome oxidase-negative fibers in 7% of patients [26]. An additionalevaluation of 177 children withmitochondrial disordersby Lamont et al. noted ragged-redfibers or cytochromeoxidase negativefibers in 89% of childrenwith mtDNAmutations in comparison to similar findings in only17% of patients with no identifiable mtDNA gene de-fect [31]. These findings suggest that light microscopyfindings are more prevalent in mitochondrial patientswith detectable mtDNA mutations. Additional studieshave found that some patients will develop histologi-cal changes over time indicating that detectable abnor-malities may develop with disease progression there-fore making them less likely to be seen in children, ingeneral, when compared to adults [25]. These variousstudies indicate that while muscle pathology may con-tribute to the diagnosis of mitochondrial disease andis more commonly abnormal with mitochondrial DNAmutations and in adult patients, the presence of normalhistological findings does not exclude a mitochondrialdisorder, particularly in children [30].
6.2. Immunohistochemistry
In some laboratories, additional mitochondrial en-zyme immunohistochemistry studies using mtDNA-encoded respiratory chain subunits such as COX II(Subunit II of complex IV) or ND1 (Subunit I of com-plex I) or nDNA-encoded respiratory chain subunitssuch as COX IV (Subunit IV of complex IV) or FeS(Iron sulfur subunit of complex III) are utilized to de-tect the specific presence or absence of very specificsubunit proteins.
6.3. Electron microscopy
Although used frequently in the past, a recent studyreviewing the utility of electron microscopy (EM) inthe diagnosis of mitochondrial patients found that itdid not provide additional diagnostic informationwhenevaluating suspected mitochondrial cases [32]. How-ever, in children, ultrastructure changes on EM have
198 F.D. Kendall / Mitochondrial disorder diagnostic trends
Fig. 4.
been reported to be present in 30–44% of patients withsuspected mitochondrial disorders in several previousstudies [28,33]. When evaluating 20 pediatric patients,Kyriacou and Mikellidou detected ultrastructual find-ings in 33% of them who had no detected abnormal-ity on light microscopy [28]. EM findings includedan increase in mitochondrial number (48%) or size(7%), increased lipid (8%), glycogen droplets (12%),increased mitochondrial matrix, abnormal cristae, andparacrystalline inclusions [28,33,34]. However, manyof these findings can be seen with other disorders in-cluding muscular dystrophies, neurogenic atrophy, in-flammatory myopathies, chronic steroid use and in oth-er metabolic disorders making them nondiagnostic andmerely a point of data that may suggest mitochondrialdisease [27,35]. As such, detectable changes on EM,or lack thereof, do not eliminate the possibility of amitochondrial disorder.
6.4. Mitochondrial enzymology
Most mitochondrial diagnoses are notmade on histo-logical or immunohistochemical findings but rather onthe detection of enzymatic deficiencies as detected bypolarographic or spectrophotometric assays. Becausethe detection of a causative gene mutation can be dif-ficult in most children up until very recently, enzymeanalysis has traditionally been considered important forthe diagnosis of mitochondrial disease [17,36,37].
Utilizing fresh tissue only due to a disruption of mi-tochondrial membrane potential in frozen samples, po-larographic assays measure mitochondrial substrate ox-idation detecting an overall estimate of electron trans-port chain activity [37–39]. Because the mitochondriatend to proliferate in patients with mitochondrial dis-ease creating a false elevation of overall electron trans-port chain activity, the use of the polarographic assay
can result in a false negative diagnosis [39]. Complet-ed on either fresh or frozen tissue, spectrophotometricassay measure the activity of each individual complexin the electron transport chain. By adding an elec-tron donor or acceptor to a muscle homogenate con-taining mitochondria, the rate of oxidation or reduc-tion is measured [38,39]. Although there is markedvariation among complex activity in different tissuesand between individuals, there is a constant ratio ofelectron transport chain enzymes to each other in allhuman tissues allowing the development of standardsby comparing each enzyme with the activity of anotherenzyme in the ATP generating system [33,38,39]. Toprevent missing a generalized enzyme deficiency, com-plex activity is also compared to another mitochondrialenzyme not a part of the electron transport chain, typi-cally citrate synthase, a Kreb cycle intermediate locat-ed in the mitochondrial matrix [38,39]. Interpretationof testing results can be challenging particularly giv-en the fact that decreased respiratory chain activitieshave been reported in a number of non-mitochondrialdisorders [40].
6.5. Fresh vs frozen samples
Over the years, there has been considerable discus-sion regarding whether fresh or frozen biopsy materi-al should be utilized for the most accurate testing re-sults with spectrophotometric assays. Although somereports over 20 years ago noted reduction in complexI activity in frozen specimens, this decreased activityhas been seen linked primarily to the initial process-ing and handling of the tissue [41]. In personal expe-rience owning a mitochondrial diagnostic laboratory,we found that complex I activity was more robust infresh samples but also well within normal ranges infrozen samples. As such, most mitochondrial experts

F.D. Kendall / Mitochondrial disorder diagnostic trends 199
find frozen sample results reliable when collected inhospital or laboratory settings that frequently processsuch samples utilizing standardized collection proto-cols. Certainly, the logistics of having patients eval-uated only in centers completing fresh muscle sampleis unrealistic in most cases making the use of frozentissue the only acceptable mode for tissue diagnosis.
6.6. Other tissue assays
More easily obtainable skin fibroblasts or other non-muscle tissues such as liver and heart have been uti-lized on many occasions to measure electron transportchain activity in patients. One study noted, though,that half of all children with deficiencies in their mus-cle have normal enzyme activity in cultured fibroblastslikely due to the fact that cells with electron transportchain defects are fragile and die in culture [37]. How-ever, modification of culture medium, to include theaddition of uridine and pyruvate, or alteration of tech-nique has allowed the survival of abnormal mitochon-dria, preventing false positive results and increasing theaccuracy of skin fibroblast assays [38,39,42]. Somemitochondrial disorders affect specific tissues, such asthe heart and liver, with electron transport chain abnor-malities non-detectable in muscle specimens [43,44].As such, in certain cases, enzymatic assays should betargeted to the affected tissue preventing false negativeresults in biopsied muscle tissue.
7. Additional tissue studies: Respirometry, bluenative and clear native gels and western blottesting
Over the last several years, additional testing toolsare being utilized by some testing laboratories with theaim of increased understanding of mitochondrial func-tionality. Overall, these various techniques can provideadditional information regarding the functionality ofthe mitochondrial OXPHOS system in a given individ-ual, findings that might not have been detectable utiliz-ing the standardized histology, immunohistochemistryand enzymology studies.
7.1. High resolution respirometry
High resolution respirometry has been used to mea-sure oxygen consumption employing an instrumentsuch as Oxygraph 2K. Using freshly isolated samplesonly, high resolution respirometry measures the inte-
grated activities of all complexes in the electron trans-port chain system in cells or isolated mitochondria un-der conditions more reflective of in vivo functioningthat isolated traditional enzyme assays [45–47]. Thistype of measurement may also identify mitochondrialdefects that are not detectable with enzymatic analysisof the electron transport chain on frozen samples [48,49]. In addition, a recent study by Janssen et al foundthat 30% of patients with abnormal functional studieson fresh mitochondria had normal enzyme assays in-dicating that these diagnoses would have been missedhad only frozen tissue been studied [50].
7.2. Blue native gel electrophoresis
The mitochondrial respiratory chain consists ofmulti-subunit protein complexes embedded in the in-ner mitochondrial membrane. This complex system iscomposed of 13 mtDNA encoded subunits and dozensof other nuclear encoded subunits, the latter requiringimportation into the mitochondria for assembly. Bluenative gel electrophoresis (BNGE) separates proteincomplexes by electrophoresis according to their nativemolecular weight in the presence of Coomassie Bril-liant Blue. The protein complexes are extracted frommembranes with a mild detergent and subsequently ex-posed to the dye, which confers the negative chargerequired for electrophoretic separation without alter-ing their native confirmation. This technique has beenslightly modified over the years by several other groupsbut has essentially remained the same [51–54]. Byscreening for the presence or absence of certain bandsrepresenting these various protein complexes and su-percomplexes, this technique can detect a number ofmitochondrial complex assembly defects.
7.3. Clear native electrophoresis
One variation on the BNGE technique is the ClearNative electrophoresis (CNE). This process utilizes adifferent buffer system that allows for the separationof proteins with high isolectric point (that pH at whicha particular molecule or surface carries no electricalcharge and will no longer migrate in an electrical field)in the absence of the blue dye. Although CNE haslower resolution when compared to BNGE, it has theadvantage of allowing for staining methods that aretypically hampered by the blue dye, such as those forcomplex III [53].

200 F.D. Kendall / Mitochondrial disorder diagnostic trends
7.4. Western blot testing
Western blot analysis (sometimes called the proteinimmunoblot) is a widely used analytical technique todetect specific proteins in a given sample of tissue ho-mogenate or extract. In the case of mitochondrial dis-ease, the presence or absence of certain proteins inthe various complexes is determined utilizing this tech-nique. Gel electrophoresis is used to separate nativeor denatured proteins by the length of the polypeptide(denaturing conditions) or by the 3-D structure of theprotein (native/non-denaturing conditions). The pro-teins are then transferred to a membrane (typically ni-trocellulose or PVDF), where they are probed usingantibodies specific to the target protein [55,56].
8. Problems with traditional invasive testing
Over recent years, many problems have come to lightwith the use of traditional mitochondrial muscle test-ing. Muscle studies are, obviously, invasive and theneed for general anesthesia and a surgical procedureplaces many fragile patients at risk for associated com-plications. Several mitochondrial experts report patientdeaths following invasive muscle biopsy.
Although there is significant variability in testingcost depending on the laboratory providing service andwhat is ordered as part of an evaluation, the final costvarieswidely and ranges from$5,000 to $10,000 for ba-sic histology and enzymology to a staggering $50,000+in some laboratories who complete additional DNAtesting and sequencing, blue native gels and other func-tional assays.
In addition to cost and safety issues, it is well knownthat the detection of mitochondrial enzymatic abnor-malities on muscle tissue is not definitively diagnosticin all cases. Abnormal mitochondrial enzymology hasbeen seen in many other disease processes includingAlzheimer’s disease, Parkinson’s disease and other dis-orders including some reported cases of Prader-Willisyndrome making it clear that other disease process-es can alter mitochondrial enzyme activity and maycloud the true underlying primary pathology in a givenpatient [11,57].
In my own personal experience I have rediagnoseda number of patients previously labeled as primary mi-tochondrial respiratory chain disease based on abnor-mal complex activity on muscle enzymologywith a va-riety of other diagnoses to include SCN1A gene mu-tations, various chromosomal abnormalities, thiamine
responsive PDH deficiency and in one case, hypophos-phatemic rickets (not associated with a Fanconi syn-drome but as a primary entity).
Because of these problematic cases, definitive diag-nosis of mitochondrial disease is often being reservedby many mitochondrial specialists for those patientswith a confirmed mitochondrial gene mutation, a chal-lenging requirement for patients given that until veryrecently most disease causing mutations had yet to beelucidated [17].
9. New trends in mitochondrial disease diagnosis
Recent trends in new testing development are provid-ing alternative approaches to a traditional muscle biop-sy evaluation. These techniques include non-invasiveenzyme testing utilizing skin cells and lymphocytes,next generation sequencing for the detection of low lev-el heteroplasmic mtDNA mutations in blood, and ex-panded nuclear gene testing which now screens hun-dreds of the known mitochondrial genes utilizing ablood sample [58,59].
Dr. Michael Goldenthal and his group at Drexel Uni-versity and St. Christopher’sHospital for Children haverecently developed an assay thatmeasuresmitochondri-al complex I and IV activity, the particularly prevalenttargets in mitochondrial defects, in buccal swab sam-ples. Using a cohort of 164 suspected mitochondrialdisease patients, when buccal swabs were analyzed bycombined micro-spectrophotometry and enzyme im-munocapture, 96 patients showed significant deficiencyin either complex I or IV activity, compared to valuesfrom 68 patients without defect and 63 age-matchedunaffected control subjects. Moreover, their findingsshowed that of 32 patients with demonstrated complexI or IV deficiency in skeletal muscle, 26 (81%) had ananalogous deficient buccal complex activity as com-pared to values obtained from the unaffected controls,supporting the validity of this approach [60]. They havealso begun to corroborate their complex I findings witha novel in-gel assay of complex I activity using patientbuccal extracts. In addition, they are expanding theirassays to include complexes II and III activity mea-surements. Overall, this less invasive approach appearsto have diagnostic utility in identifying mitochondri-al dysfunction in large numbers of children or adultssuspected of having mitochondrial disease without thecost and risks associated with more traditional invasiveprocedures as demonstrated by its use in a suspectedMERRF patient [61]. In addition, the use of a non-

F.D. Kendall / Mitochondrial disorder diagnostic trends 201
invasive study allows the advantage of repeat testingfor the purpose of monitoring disease progression andpossible response to a variety of treatment modalities.
Although many mtDNA mutations, such as the 3243A>G MELAS mutation, are usually measurable inblood leukocytes, the level of mutation declines overtime [62]. Thus even in severely affected patients pre-senting with MELAS, the level of m 3243 A>G maybe very low, or even escape detection. This has led tothe use of muscle tissue for years as the gold standardfor the measurement of heteroplasmy in mitochondrialDNA mutations to both confirm diagnosis and predictthe incidence of specific clinical features or severityof disease. However, the development of several newmethods of heteroplasmic detection utilizing a rangeof noninvasive tissues has proven to be useful and isleading to the elimination of the invasive biopsy. Inmany cases, the use of next generation sequencing, atechnique that allows the sequencing of a large numberof amplicons (pieces of DNA formed as the product ofamplification events such as PCR) in parallel availablethrough a number of laboratories, enables the detectionof heteroplasmic mtDNA mutations down to a level of1%–2%, eliminating the need for muscle testing [63].In addition, a study looking at MELAS patients foundthat screening of m. 3243A>G mutation load in urinaryepithelium was a better predictor of outcome than thepresent gold standard of skeletal muscle [22].
Until very recently, confirmation of a mitochondrialdisease through identification of a causative gene mu-tation occurred infrequently. In a study reviewing 118children, a genetic defect of any type was identified inonly 5% of patients investigated [64]. Out of the 1,500known mitochondrial genes only the mtDNA and a se-lect few nuclear genes could be screened for on a rou-tine basis up until 2010. However, during 2011, sev-eral laboratories have developed expanded gene panelslooking at hundred of the nuclear encoded mitochon-drial disease related genes utilizing blood specimensmaking confirmatory diagnostic testing likely to occurin more and more cases moving forward.
10. Conclusion
Mitochondrial disorders have a far larger footprintand impact thanwas previously notedwith an incidenceof at least 1 in 5,000 individuals [1,3–6]. Recent stud-ies have also shown than 1 in 200 newborns carry oneof the ten common mtDNA mutations, perhaps con-tributing to the onset or developmentof many common-
place diseases such as diabetes and heart disease [12].However, traditional diagnostic tools for mitochondrialdisease have been invasive, costly and, in many cases,not definitively diagnostic. In addition, although sever-al sets of diagnostic criteria have been developed overthe last few decades based on combinations of clinical,laboratory, pathologic, biochemical, and genetic find-ings, they have not proven all that effective or practicalin the clinical setting. In many cases, the diagnosisof a mitochondrial disorder remains a clinical diagno-sis based on the acumen of the treating physician [65].However, innovative new techniques are revolutioniz-ing mitochondrialmedicine providing less invasive andmore definitive diagnostic options for the evaluation ofsuspected mitochondrial patients. This will undoubt-edly broaden the testing availability to a wider range ofpatients and lead to more accurate diagnosis and ulti-mately improved management and treatment of affect-ed individuals.
References
[1] Zhu X, Peng X, Guan MX, Yan Q. Pathogenic mutations ofnuclear genes associated with mitochondrial disorders. ActaBiochim Biophys Sin 2009; 41(3): 179-187.
[2] Pfeffer G, Cote HC, Montaner JS, Li CC, Jitratkosol M, MezeiMM. Ophthalmoplegia and ptosis: Mitochondrial toxicity inpatients receiving HIV therapy. Neurology 2009; 73(1): 71-72.
[3] Chinnery PF. Mitochondrial Disorders Overview. GeneRe-views [Internet]. Seattle (WA): University of Washington,Seattle; 1993–2000 Jun 08 [updated 2010 Sep 16].
[4] Tarnopolsky M, Raha S. Mitochondrial myopathies: diag-nosis, exercise intolerance, and treatment options. Med SciSports Exerc 2005; 37(12): 2086-2093.
[5] Van Adel B, Tarnopolsky M. Metabolic myopathies: update2009. J Clin Neuromuscul Dis 2009; 10(3): 97-121.
[6] Schaefer AM, McFarland R, Blakely EL et al. Prevalence ofmitochondrialDNAdisease in adults. AnnNeurol 2008; 63(1):35-39.
[7] Mancuso M, Calsolaro V, Orsucci D et al. Mitochondria, cog-nitive impairment, and Alzheimer’s disease. Int J AlzheimersDis 2009. pii: 951548.
[8] Prabakaran S, Swatton JE, Ryan MM et al. Mitochondrial dys-function in schizophrenia: evidence for compromised brainmetabolism and oxidative stress. Mol Psychiatry 2004; 9(7):684-697.
[9] Gegg M, Schapira AH. PINK1-parkin-dependent mitophagyinvolves ubiquination of mitofusins 1 and 2: Implications forParkinson disease pathogenesis. Autophagy 2011; 7(2): 243-245.
[10] Lutz AK, Exner N, Fett ME et al. Loss of parkin or PINK1function increases Drp1-dependent mitochondrial fragmenta-tion. J Biol Chem 2009; 284(34): 22938-22951.
[11] Toung, LT. Is bipolar disorder a mitochondrial disease? JPsychiatry Neurosci 2007; 32(3): 160-161.
202 F.D. Kendall / Mitochondrial disorder diagnostic trends
[12] Elliott HR, Samuels DC, Eden JA, Relton CL, Chinnery PF.Pathogenic mitochondrial DNA mutations are common in thegeneral population. Am J Hum Genet 2008; 83(2): 254-260.
[13] Nass S, Nass MM. Intramitochondrial fibers with DNA char-acteristics. I. Fixation and electron staining reactions. J CellBiol 1963; 19: 593-611.
[14] Nass S, Nass MM. Intramitochondrial fibers with DNA char-acteristics. II. Enzymatic and other hydrolytic treatments. JCell Biol 1963; 19: 613-629.
[15] Gillis LA, Sokol RJ. Gastrointestinal manifestations of mito-chondrial disease. Gastroenterol Clin North Am 2003; 32(3):789-817.
[16] Tiranti V, Jaksch M, Hofmann S et al. Loss-of-function mu-tations of SURF-1 are specifically associated with Leigh syn-drome with cytochrome c oxidase deficiency. Ann Neurol1999; 46(2): 161-166.
[17] Lamont PJ, Surtees R, Woodward CE, Leonard JV, Wood NW,Harding AE. Clinical and laboratory findings in referrals formitochondrial DNA analysis. Arch Dis Child 1998; 79(1):22-27.
[18] Longo N. Mitochondrial Encephalopathy. Neurol Clin N Am2003; 21: 817-831.
[19] Campos Y, Huertas R, Lorenzo G et al. Plasma carnitine in-sufficiency and effectiveness of L-carnitine therapy in patientswith mitochondrial myopathy. Muscle Nerve 1993; 16(2):150-153.
[20] Hsu CC, Chuang YH, Tsai JL et al. CPEO and carnitine defi-ciency overlapping in MELAS syndrome. Acta Neurol Scand1995; 92(3): 252-255.
[21] Dougherty F. Metabolic testing in Mitochondrial Disease.Semin Neurol 2001; 21(3): 303-308.
[22] Whittaker RG, Blackwood JK, Alston CL et al. Urine het-eroplasmy is the best predictor of clinical outcome in them.3243A>G mtDNA mutation. Neurology 2009; 72(6): 568-569.
[23] Engel WK, Cunningham GG. Rapıd examınatıon of muscletıssue. An ımproved trıchrome method for fresh-frozen bıopsysectıons. Nerology 1963; 13: 919-923.
[24] Shoffner JM. Mitochondrial myopathy diagnosis. Neurol Clin2000; 18: 105-123.
[25] Jackson MJ, Schaefer JA, Johnson MA, Morris AA, TurnbullDM, Bindoff LA. Presentation and clinical investigation of mi-tochondrial respiratory chain disease: A study of 51 patients.Brain 1995; 188: 339-357.
[26] Rollins S, Prayson RA, McMahon JT, Cohen BH. Diagnosticyield of muscle biopsy in patients with clinical evidence ofmitochondrial cytopathy. Am J Clin Pathol 2001; 116(3): 326-330.
[27] Lindal S, Lund I, Torbergsen T et al. Mitochondrial diseasesand myopathies: A series of muscle biopsy specimens withultrastructural changes in the mitochondria. Ultrastruct Pathol1992; 16(3): 263-275.
[28] Kyriacou K, Mikellidou C, Hadjianastasiou A, MiddletonL, Panousopoulos A, Kyriakides T. Ultrastructural diagnosisof mitochondrial encephalomyopathies revisited. UltrastructPathol 1999; 23(3): 163-170.
[29] Taylor RW, Schaefer AM, Barron MJ, McFarland R, TurnbullDM. The diagnosis of mitochondrial muscle disease. Neuro-muscul Disord 2004; 14(4): 237-245.
[30] Patterson K. Mitochondrial muscle pathology. Pediatr DevPathol 2004; 7(6): 629-632.
[31] Lamont PJ, Surtees R, Woodward CE, Leonard JV, Wood NW,Harding AE. Clinical and laboratory findings in referrals for
mitochondrial DNA analysis. Arch Dis Child 1998; 79(1):22-27.
[32] Graves T, Phadke R, Holton JL,Hanna MG, Rahman S, Bhard-waj N. PONM21 electron microscopy does not add to the diag-nostic accuracy of muscle biopsy for suspected mitochondrialdisease. J Neurol Neurosurg Psychiatry 2010; 81: e65
[33] DiMauro S, Bonilla E, De Vivo DC. Does the patient have amitochondrial encephalomyopathy? J Child Neurol 1999; 14:S23-35.
[34] Stadhouders AM, Sengers RC. Morphological observations inskeletal muscle from patients with a mitochondrial myopathy.J Inherited Metab Dis 1987; 10(Suppl.1): 62-80.
[35] Jackson MJ, Schaefer JA, Johnson MA, Morris AA, TurnbullDM,Bindoff LA. Presentation and clinical investigation of mi-tochondrial respiratory chain disease: A study of 51 patients.Brain 1995; 188: 339-357.
[36] Casademont J, Perea M, Lopez S, Beato A, Miro O, Cardel-lach F. Enzymatic diagnosis of oxidative phosphorylation de-fects on muscle biopsy: Better on tissue homogenate or ona mitochondrial-enriched suspension? Med Sci Monit 2004;10(9): CS49-53.
[37] Thorburn DR, Chow CW, Kirby DM. Respiratory chain en-zyme analysis in muscle and liver. Mitochondrion 2004; 4(5-6): 363-375.
[38] Rustin P, ChretienD, BourgeronT. Biochemical andmolecularinvestigations in respiratory chain defects. Clin Chim Acta1994; 228(1): 35-51.
[39] Chretien D, Rustin P. Mitochondrial oxidative phosphoryla-tion: Pitfalls and tips in measuring and interpreting enzymeactivities. J Inherit Metab Dis 2003; 26(2-3): 189-198.
[40] Hui J, Kirby DM, Thorburn DR, Boneh A. Decreased ac-tivities of mitochondrial respiratory chain complexes in non-mitochondrial respiratory chain diseases. Dev Med Child Neu-rol 2006; 48(2): 132-136.
[41] Dimauro S, Tay S, Mancuso M. Mitochndrial encephalomy-opathies: Diagnostic approach. Ann NY Acad Sci 2004; 1011:217-231.
[42] Hodges SD, Snyder FF. Mitochondrial function dependentproliferation assay for the diagnosis of mitochondrial disordersin human fibroblasts. Nucleosides Nucleotides Nucleic Acids2004; 23(8-9): 1269-1274.
[43] Munnich A, Rotig A, Chretien D et al. Clinical presentation ofmitochondrial disorders in childhood. J Inherited Metab Dis1996; 19(4): 521-527.
[44] Panetta J, Gibson K, Kirby DM, Thorburn DR, Boneh A. Theimportance of liver biopsy in the investigation of possible mi-tochondrial respiratory chain disease. Neuropediatrics 2005;36(4): 25625-9.
[45] Sperl W, Skladal D, Gnaiger E et al. High resolution respirom-etry of permeabilized skeletal muscle fibers in the diagnosis ofneuromuscular disorders. Mol Cell Biochem 1997; 174(1-2):71-78.
[46] Chowdhury SK, Drahota Z, Floryk D, Calda P, Houstek J. Ac-tivities of mitochondrial oxidative phosphorylation enzymesin cultured amniocytes. Clin Chim Acta 2000; 298(1-2): 157-173.
[47] Villani G, Attardi G. In vivo control of respiration by cy-tochrome c oxidase in human cells. Free Radic Biol Med 2000;29(34): 202-210.
[48] Janssen AJ, Smeitink JA, van den Heuvel LP. Some practicalaspects of providing a diagnostic service for respiratory chaindefects. Ann Clin Biochem 2003; 40(Pt1): 3-8.
[49] Puchowicz MA, Varnes ME, Cohen BH, Friedman NR, KerrDS, Hoppel CL. Oxidative phosphorylation analysis:assessing
F.D. Kendall / Mitochondrial disorder diagnostic trends 203
the integrated functional activity of human skeletal musclemitochondrial – case studies. Mitochondrion 2004; 4(5-6):377-385.
[50] Janssen AJ, Trijbels FJ, Sengers RC et al. Measurement of theenergy-generating capacity of human muscle mitochondria:Diagnostic procedure and application to human pathology.Clin Chem 2006; 52(5): 860-871.
[51] Schagger H, von Jagow G. Blue native electrophoresis forisolation of membrane protein complexes in enzymaticallyactive form. Anal Biochem 1991; 199(2): 223-231.
[52] Nijtmans LG, Henderson NS, Holt IJ. Blue Native elec-trophoresis to study mitochondrial and other protein complex-es. Methods 2002; 26(4): 327-334.
[53] Wittig I, Schagger H. Features and applications of blue-nativeand clear-native electrophoresis. Proteomics 2008; 8: 3974-3990.
[54] Wumaier Z, Nubel E, Wittig I, Schagger H. Chapter 8 Two-dimensional native electrophoresis for fluorescent and func-tional assays of mitochondrial complexes. Methods Enzymol2009; 456: 153-168.
[55] Towbin H, Staehelin T, Gordon J. Electrophoretic transfer ofproteins from polyacrylamine gels to nitrocellulose sheets:procedure and some applications. Proc Natl Acad Sci USA1979; 76(9): 4350-4354.
[56] Renart J, Reiser J, Stark GR. Transfer of proteins from gels todiazobenzyloxymethyl-paper and detection with antisera: Amethod for studying antibody specificity and antigen structure.Proc Natl Acad Sci USA 1979; 76(7): 3116-3120.
[57] Wassmer E, Robinson BH, Tein I. Dual pathology in twohypotonic children with Prader-Willi syndrome and musclemitochondrial Complex I deficiency. Arch Dis Child 2003; 88:70-71.
[58] Giulivi C, Zhang YF, Omanska-Klusek A et al. Mitochondrialdysfunction in autism. JAMA 2010; 304(21): 2389-2396.
[59] Zaragoza MV, Fass J, Diegoli M, Lin D, Arbustini E. Mi-tochondrial DNA variant discovery and evaluation in humanCardiomyopathies through next-generation sequencing. PloSOne 2010 5(8): e12295.
[60] Goldenthal MJ, Damle S, Shah N et al. Non-invasive Eval-uation of Mitochondrial Dysfunction in Children by BuccalSwab. Poster Presentation at Mitochondrial Medicine 2011meetings of the UMDF (United Mitochondrial Disease Foun-dation) in June 2011, Chicago, Il.
[61] Yorns WR Jr, Valencia I, Jayaraman A, Sheth S, Legido A,Goldenthal MJ. Buccal swab analysis of mitochondrial en-zyme deficiency and DNA defects in a child with suspectedmyoclonic epilepsy and ragged red fibers (MERRF). J ChildNeurolpres 2012; 27(3): 398-401.
[62] Rahman S, Poulton J, Marchington D, Suomalainen A. De-crease of 3243 A toG mtDNAmutation from blood in MELASsyndrome: A longitudinal study. Am J Hum Genet 2001;68(1): 238-240.
[63] Bennett S. Solexa Ltd. Pharmacogenomics 2004 Jun; 5(4):433-438.
[64] Bernier FP, BonehA, Dennett X, Chow CW, ClearyMA, Thor-burn DR. Diagnostic criteria for respiratory chain disorders inadults and children. Neurology 2002; 59(9): 1406-1411.
[65] Koenig, MK. Presentation and Diagnosis of MitochondrialDisorders in Children. Pediatr Neurol 2008; 38: 305-313.
[66] Kendall F. Bridging the Gap between Autism Spectrum Disor-ders and Mitochondrial Disease. Autism Science Digest April2011; (1): 42-46.
[67] Dougherty F. Metabolic testing in Mitochondrial Disease.Semin Neurol 2001; 21(3): 303-308.