mitral valve disease bleeding (≥2u or surgery for rebleeding) 12.6% non-cerebral thromboembolism...
TRANSCRIPT

Mitral Valve Disease James Hermiller, MD, FACC, FSCAI
St Vincent Heart Center Indianapolis, IN
Disclosures
• Consulting Fees/Honoraria
• Speaker Bureau
• Abbott, BSC, Medtronic, Edwards and St Jude
• Medicines Company, Astra-Zeneca
Affiliation/Financial Relationship Company
• Introduction
• Transcatheter Repair
– MitraClip
– Annular Approaches
• TMVR
• Summary/Conclusions
Outline

Complexity Mitral Valve Aortic Valve
Complex Simple
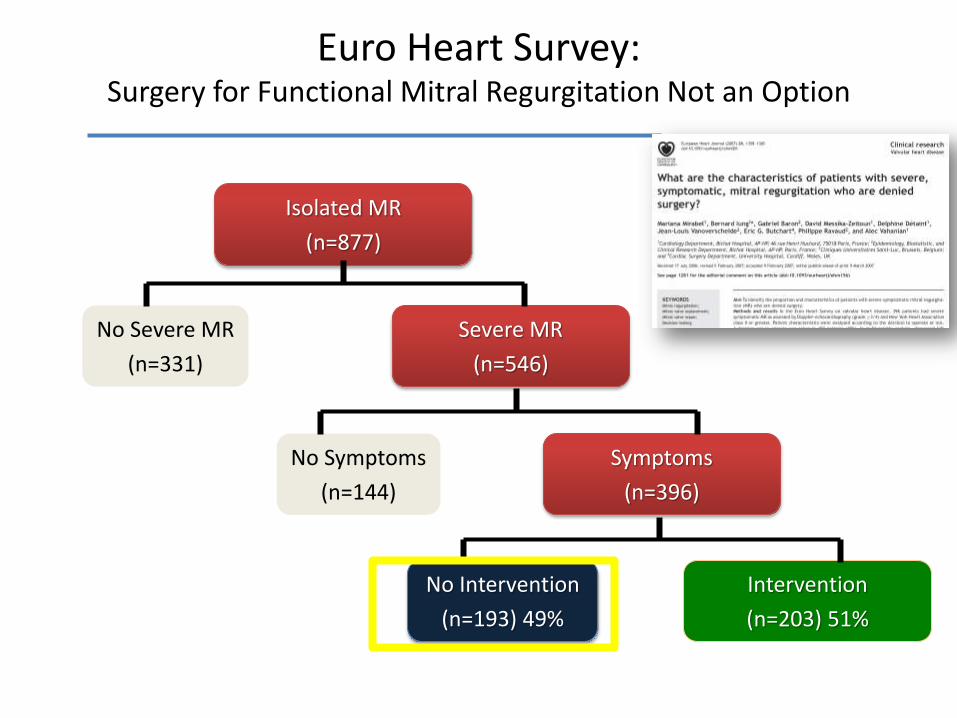
Euro Heart Survey: Surgery for Functional Mitral Regurgitation Not an Option
Isolated MR
(n=877)
Severe MR
(n=546)
No Severe MR
(n=331)
No Symptoms
(n=144)
Symptoms
(n=396)
No Intervention
(n=193) 49%
Intervention
(n=203) 51%
Mirabel et al, European
Heart J 2007;28:1358-
1365

• Introduction
• Transcatheter Repair
– MitraClip
– Annular Approaches
• TMVR
• Summary/Conclusions
Outline
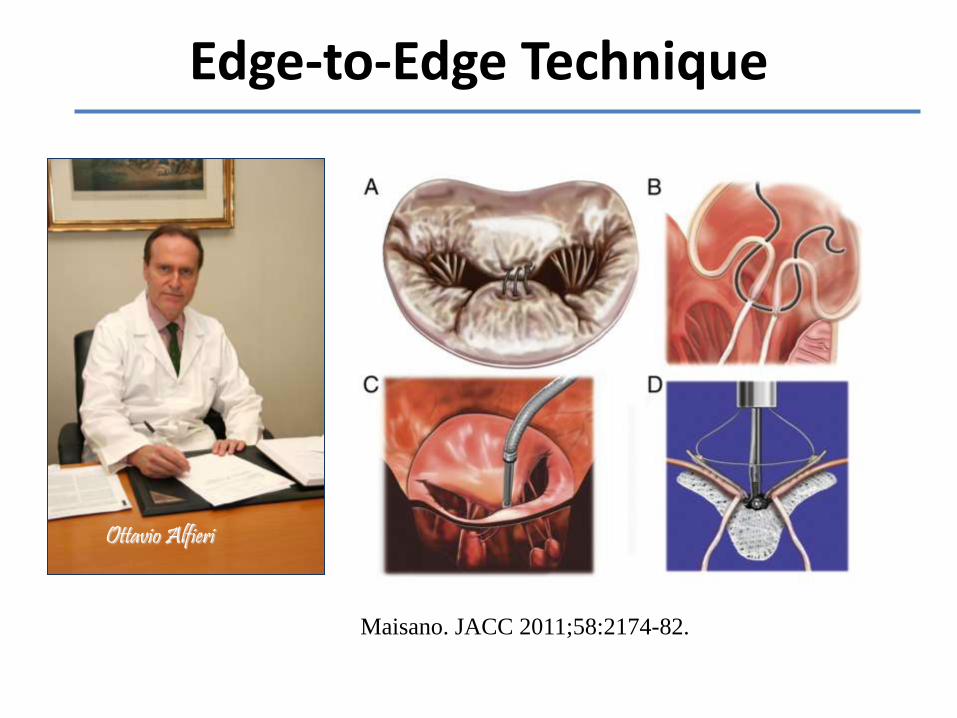
Edge-to-Edge Technique
Maisano. JACC 2011;58:2174-82.
Ottavio Alfieri


In the Beginning: Lost

In the Beginning: Confused
Steerable Sleeve
Delivery Catheter
Guiding Catheter
MitraClip

In the Beginning: Off Target
Ahah!!!!
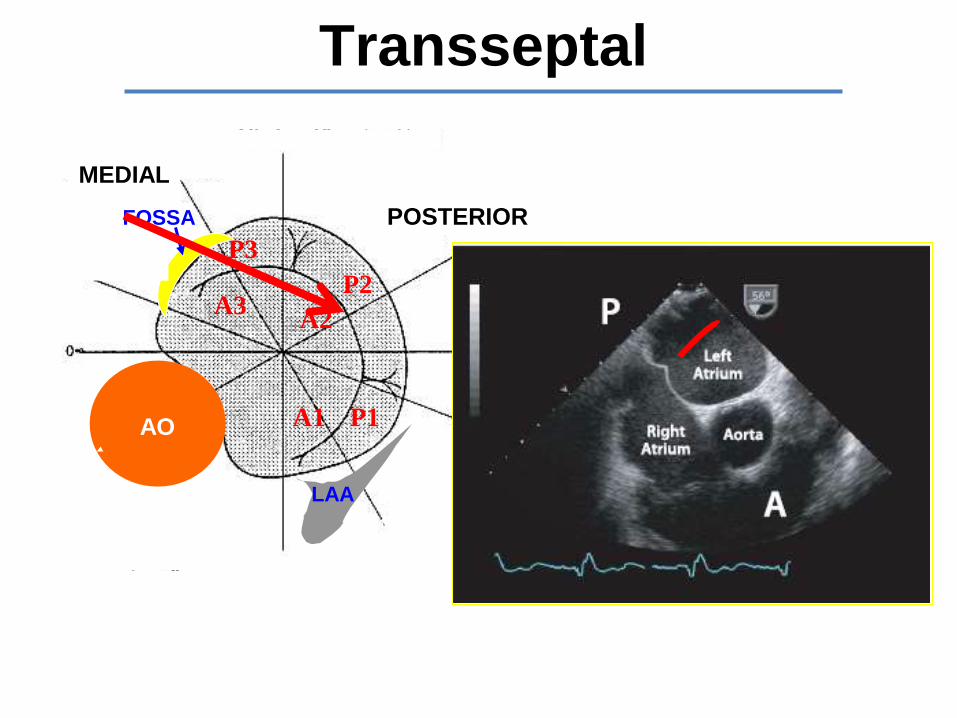
LAA
300
600
300
A1
A2 A3
P1
P2
P3
FOSSA
AO
LATERAL
MEDIAL
ANTERIOR
POSTERIOR
Transseptal
Essential: 3D Imaging
3D TEE
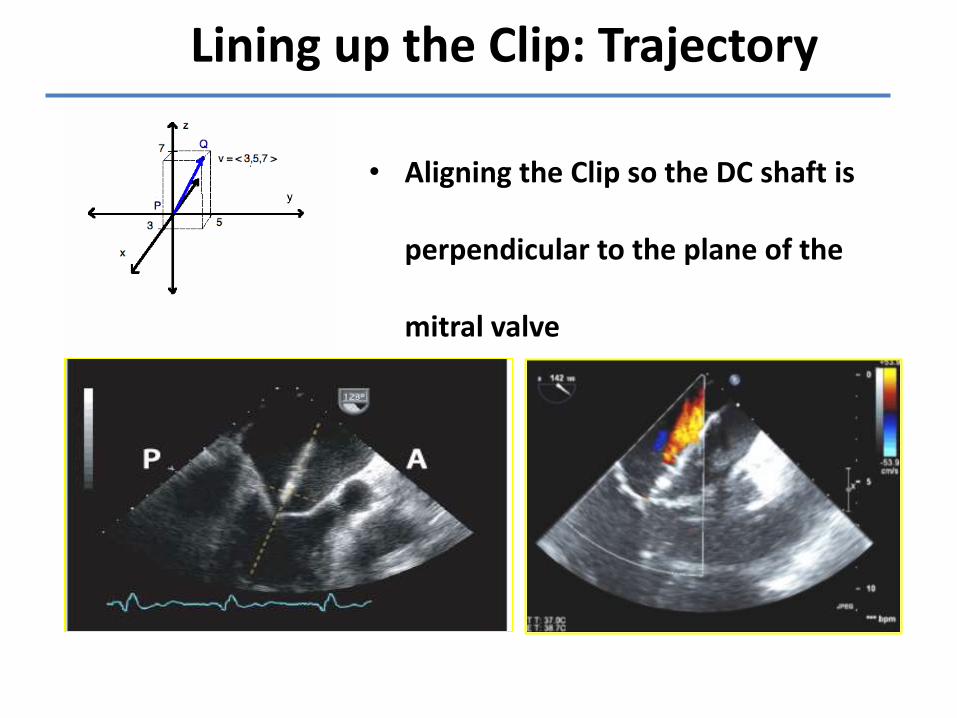
• Aligning the Clip so the DC shaft is
perpendicular to the plane of the
mitral valve
Lining up the Clip: Trajectory
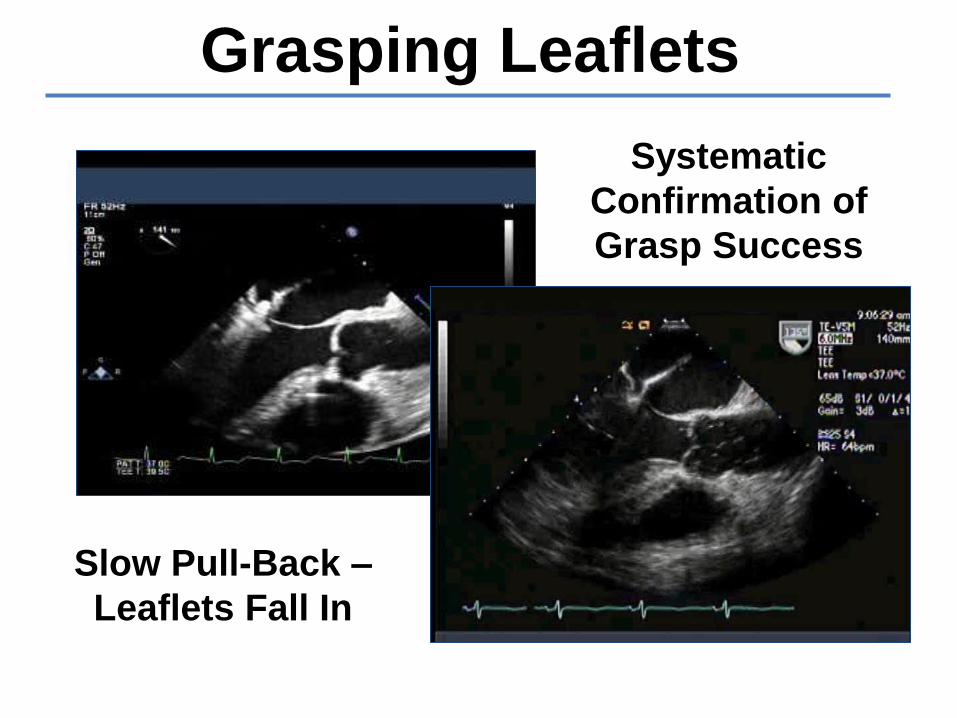
Grasping Leaflets
Slow Pull-Back –
Leaflets Fall In
Systematic
Confirmation of
Grasp Success
Confirming: Leaflet Grasp
Wait Look

MitraClip Smoking Relaxing Transseptal Location Vector into Valve Grasping/Verifying Grasp Patient Selection Imaging (3D TEE)

MitraClip
• Surgical candidates- 5 year EVEREST II randomized trial
• High risk global experience
– Improved symptoms, procedural safety, short stays
– Decreased heart failure hospitalizations
– Expanded anatomic substrates
• High risk FMR US COAPT Trial
– Randomized MitraClip vs GDMT ± CRT
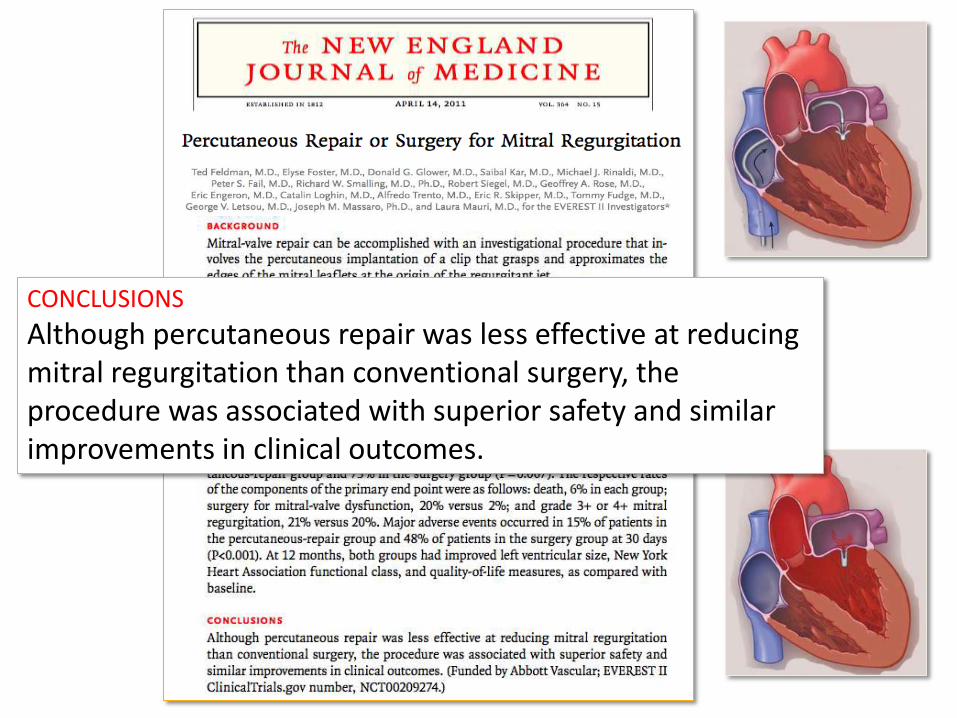
CONCLUSIONS
Although percutaneous repair was less effective at reducing mitral regurgitation than conventional surgery, the procedure was associated with superior safety and similar improvements in clinical outcomes.
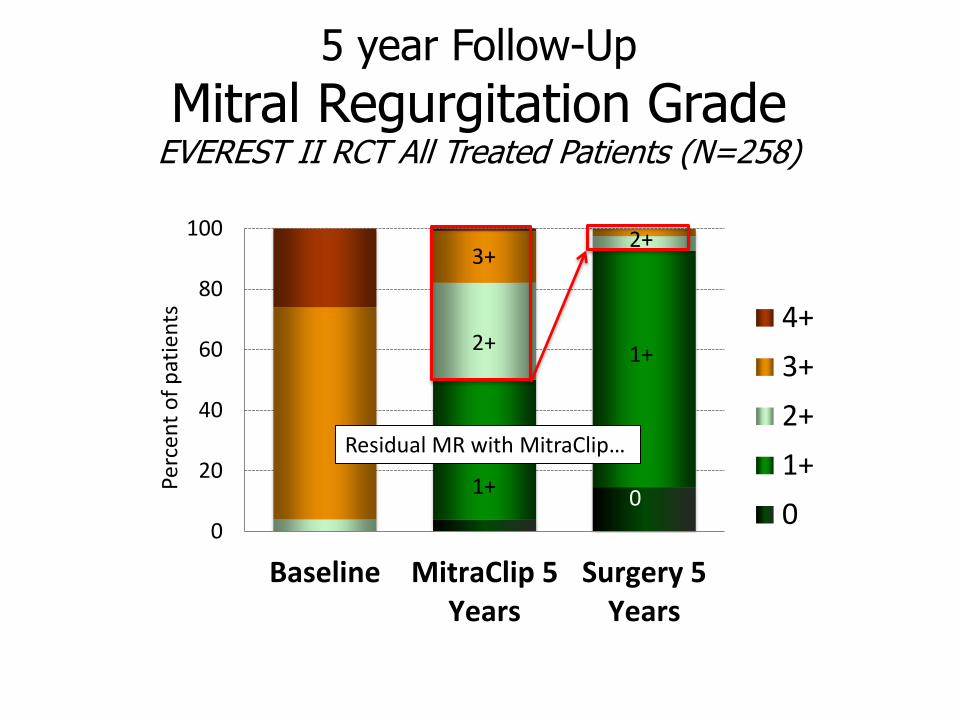
5 year Follow-Up
Mitral Regurgitation Grade EVEREST II RCT All Treated Patients (N=258)
0
20
40
60
80
100
Baseline MitraClip 5Years
Surgery 5Years
4+
3+
2+
1+
0
Perc
ent
of
pat
ien
ts
3+ 2+ 1+
Residual MR with MitraClip…
2+ 1+ 0
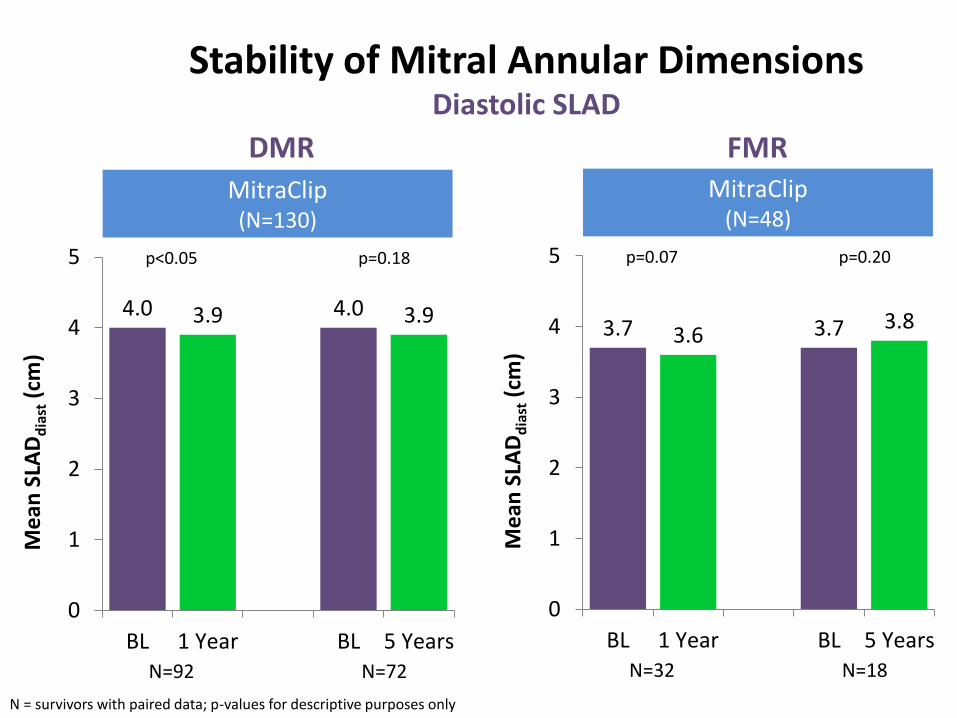
Stability of Mitral Annular Dimensions Diastolic SLAD
3.7 3.6 3.7 3.8
0
1
2
3
4
5
BL 1 Year BL 5 Years
Me
an S
LAD
dia
st (
cm)
N = survivors with paired data; p-values for descriptive purposes only
N=32 N=18
MitraClip (N=48)
p=0.07 p=0.20
4.0 3.9 4.0 3.9
0
1
2
3
4
5
BL 1 Year BL 5 Years
Me
an S
LAD
dia
st (
cm)
N=92 N=72
MitraClip (N=130)
p<0.05 p=0.18
DMR FMR

Long-Term MitraClip Device Safety EVEREST II RCT
Through 1 Year # (%) of patients
1 Year to 5 Years # (%) of patients
Single Leaflet Device Attachment (SLDA)
10 (6.3%) 0 (0.0%)
MV stenosis 1 (0.6%) 0 (0.0%)
Device Embolization 0 (0.0%) 0 (0.0%)
Based on N=158 who were implanted with 1 or 2 MitraClip devices

6-Month Landmark Analysis
97.1% 98.7% 1 year 91.4%
93.7% 5 years
Kaplan-Meier Freedom From MV Surgery in MitraClip Group or Re-operation in Surgery Group
MitraClip
Surgery
EVEREST II RCT
Feldman T et al. N Engl J Med 2011;364:1395-1406
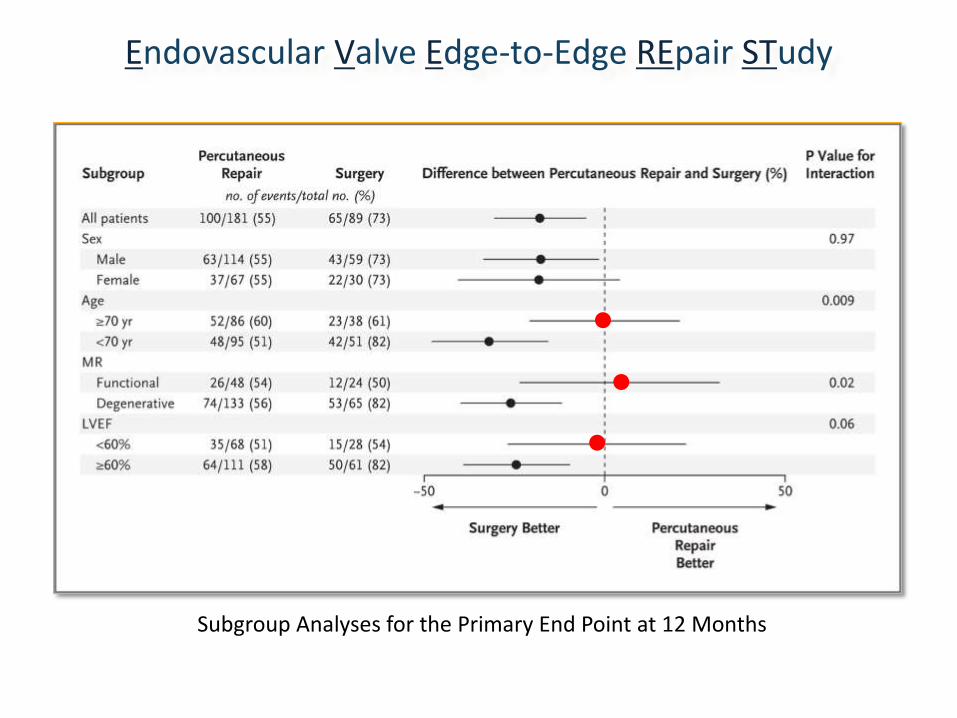
Subgroup Analyses for the Primary End Point at 12 Months
Endovascular Valve Edge-to-Edge REpair STudy
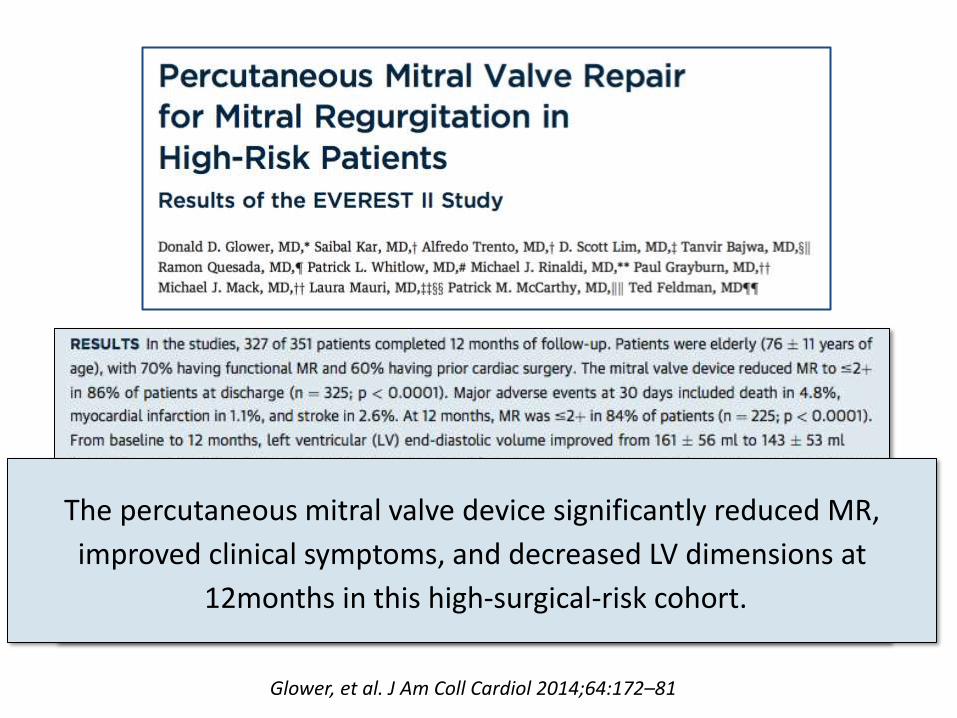
Glower, et al. J Am Coll Cardiol 2014;64:172–81
The percutaneous mitral valve device significantly reduced MR,
improved clinical symptoms, and decreased LV dimensions at
12months in this high-surgical-risk cohort.
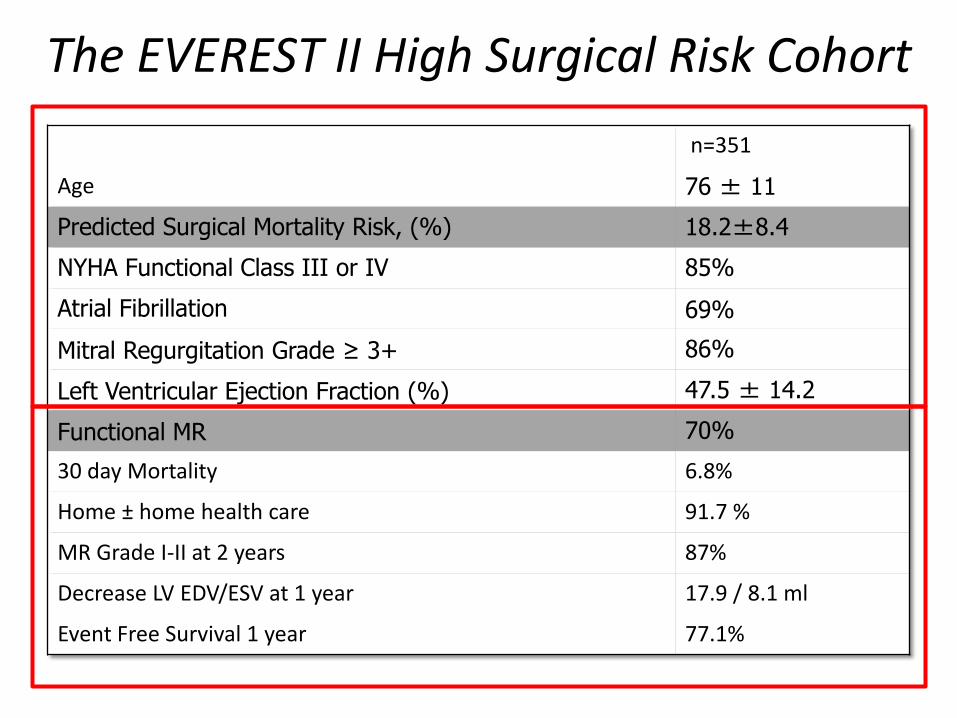
The EVEREST II High Surgical Risk Cohort
n=351
Age 76 ± 11
Predicted Surgical Mortality Risk, (%) 18.2±8.4
NYHA Functional Class III or IV 85%
Atrial Fibrillation 69%
Mitral Regurgitation Grade ≥ 3+ 86%
Left Ventricular Ejection Fraction (%) 47.5 ± 14.2
Functional MR 70%
30 day Mortality 6.8%
Home ± home health care 91.7 %
MR Grade I-II at 2 years 87%
Decrease LV EDV/ESV at 1 year 17.9 / 8.1 ml
Event Free Survival 1 year 77.1%
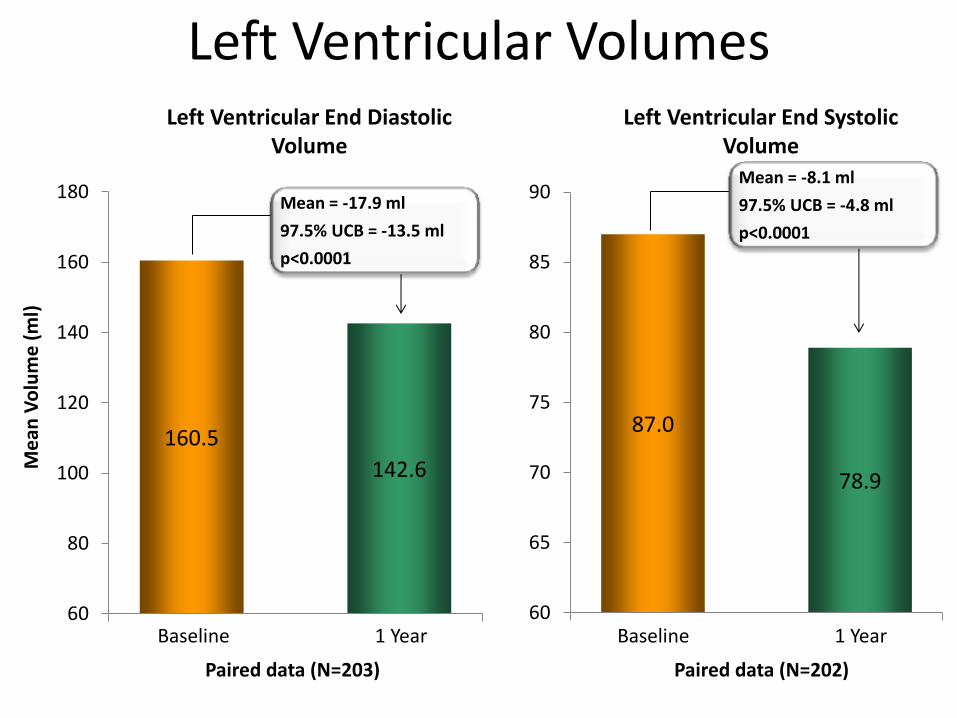
Left Ventricular Volumes
160.5
142.6
60
80
100
120
140
160
180
Me
an V
olu
me
(m
l)
87.0
78.9
60
65
70
75
80
85
90
Baseline 1 Year Baseline 1 Year
Paired data (N=203) Paired data (N=202)
Left Ventricular End Diastolic Volume
Left Ventricular End Systolic Volume
Mean = -17.9 ml
97.5% UCB = -13.5 ml
p<0.0001
Mean = -8.1 ml
97.5% UCB = -4.8 ml
p<0.0001
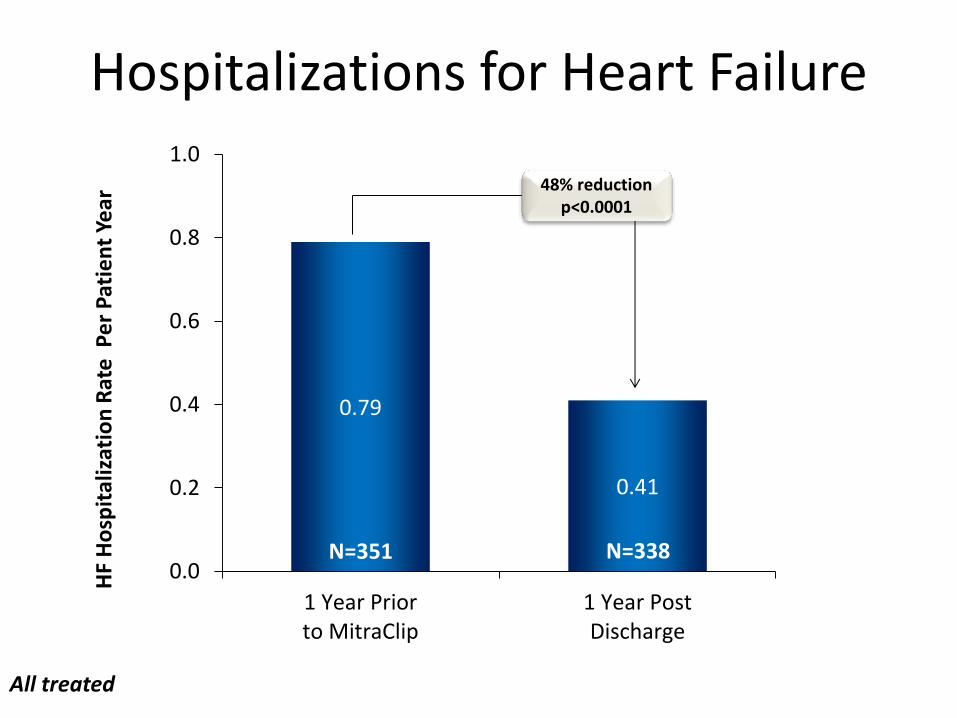
Hospitalizations for Heart Failure
0.79
0.41
0.0
0.2
0.4
0.6
0.8
1.0
1 Year Priorto MitraClip
1 Year PostDischarge
HF
Ho
spit
aliz
atio
n R
ate
Pe
r P
atie
nt
Year
48% reduction p<0.0001
N=351 N=338
All treated
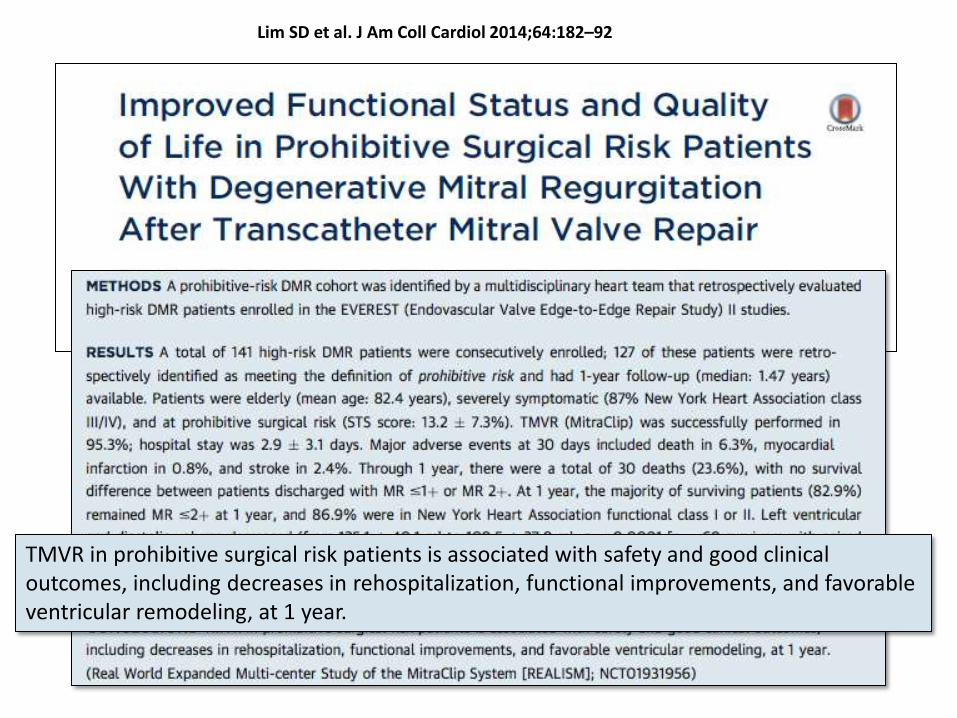
Lim SD et al. J Am Coll Cardiol 2014;64:182–92
TMVR in prohibitive surgical risk patients is associated with safety and good clinical outcomes, including decreases in rehospitalization, functional improvements, and favorable ventricular remodeling, at 1 year.

Baseline Demographics and Comorbidities
Characteristic Prohibitive Risk DMR
N = 127
Age (mean ± SD) 82 ± 9 years
Patients over 75 years of age 84%
Male Gender 55%
Coronary Artery Disease 73%
Prior Myocardial Infarction 24%
Previous Cardiovascular Surgery 48%
Atrial Fibrillation History 71%
Prior Stroke 10%
Diabetes 30%
Moderate to Severe Renal Disease 28%
Chronic Obstructive Pulmonary Disease 32%
STS Mortality Risk (mean ± SD) [v2.73, replacement] 13.2 ± 7.3%
SF-36 QoL Physical Component Score (mean ± SD) 32.0 ± 8.7
SF-36 QoL Mental Component Score (mean ± SD) 46.1 ± 12.5
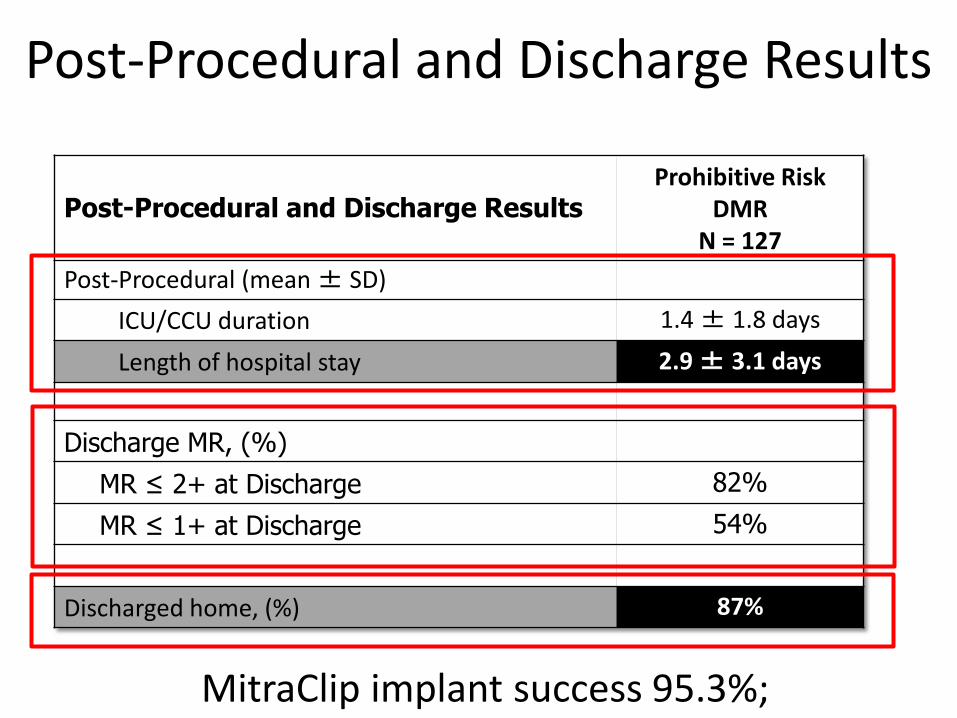
Post-Procedural and Discharge Results
Post-Procedural and Discharge Results Prohibitive Risk
DMR N = 127
Post-Procedural (mean ± SD)
ICU/CCU duration 1.4 ± 1.8 days
Length of hospital stay 2.9 ± 3.1 days
Discharge MR, (%)
MR ≤ 2+ at Discharge 82%
MR ≤ 1+ at Discharge 54%
Discharged home, (%) 87%
MitraClip implant success 95.3%;
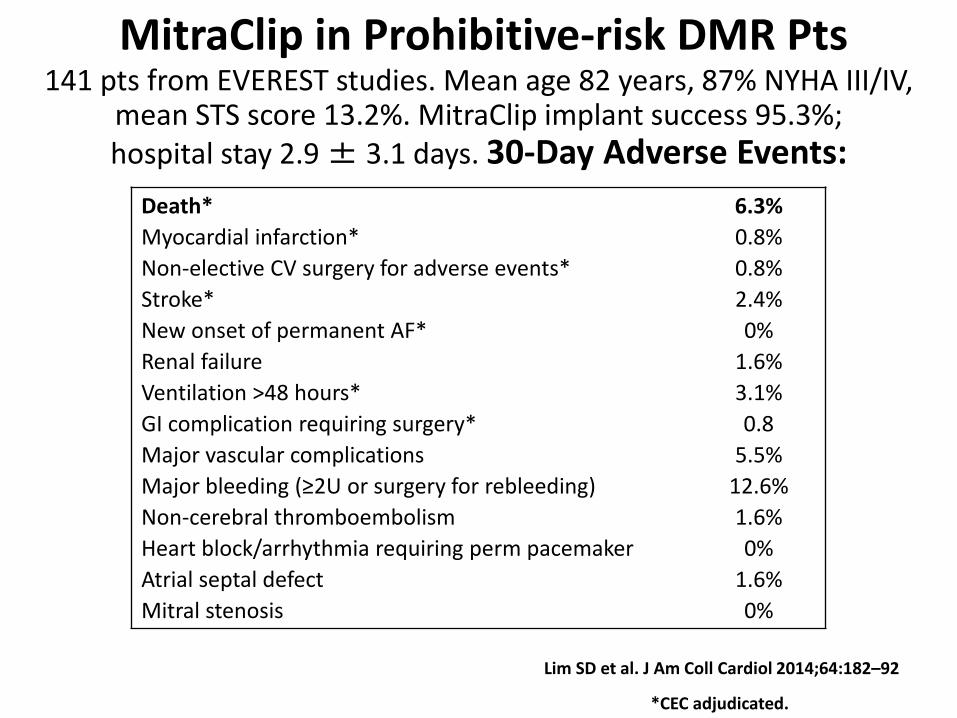
Death* 6.3%
Myocardial infarction* 0.8%
Non-elective CV surgery for adverse events* 0.8%
Stroke* 2.4%
New onset of permanent AF* 0%
Renal failure 1.6%
Ventilation >48 hours* 3.1%
GI complication requiring surgery* 0.8
Major vascular complications 5.5%
Major bleeding (≥2U or surgery for rebleeding) 12.6%
Non-cerebral thromboembolism 1.6%
Heart block/arrhythmia requiring perm pacemaker 0%
Atrial septal defect 1.6%
Mitral stenosis 0%
MitraClip in Prohibitive-risk DMR Pts 141 pts from EVEREST studies. Mean age 82 years, 87% NYHA III/IV,
mean STS score 13.2%. MitraClip implant success 95.3%; hospital stay 2.9 ± 3.1 days. 30-Day Adverse Events:
*CEC adjudicated.
Lim SD et al. J Am Coll Cardiol 2014;64:182–92
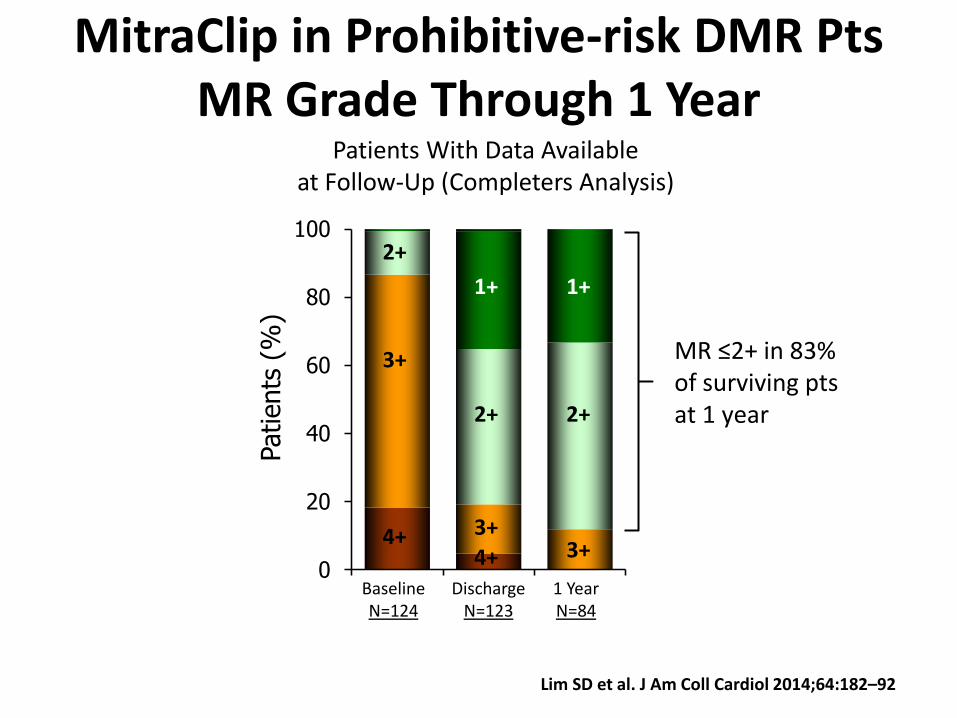
MitraClip in Prohibitive-risk DMR Pts MR Grade Through 1 Year
0
20
40
60
80
100
Patients
(%
) 2+
4+
Baseline N=124
Discharge N=123
1 Year N=84
3+
4+
3+ 3+
2+ 2+
1+ 1+
Patients With Data Available at Follow-Up (Completers Analysis)
MR ≤2+ in 83% of surviving pts at 1 year
Lim SD et al. J Am Coll Cardiol 2014;64:182–92

MitraClip in Prohibitive-risk DMR Pts
141 pts from EVEREST studies. Mean age 82 years, 87% NYHA III/IV, mean STS score 13.2%. LV Remodeling, Functional Class and Rehospitilization for CHF
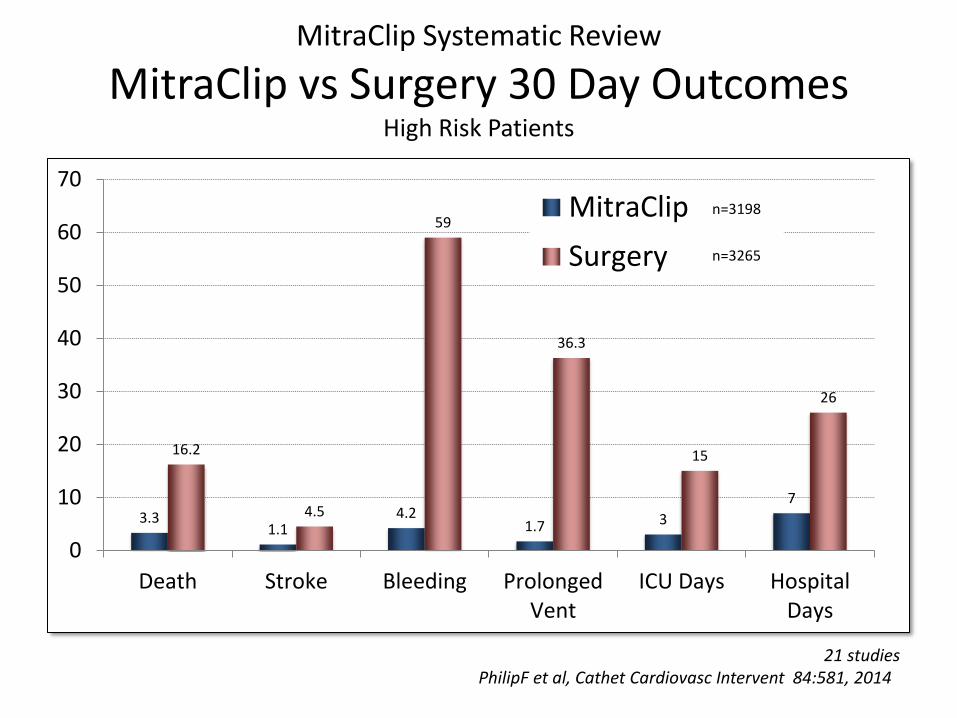
MitraClip Systematic Review
MitraClip vs Surgery 30 Day Outcomes High Risk Patients
3.3 1.1
4.2 1.7 3
7
16.2
4.5
59
36.3
15
26
0
10
20
30
40
50
60
70
Death Stroke Bleeding ProlongedVent
ICU Days HospitalDays
MitraClip
Surgery
21 studies PhilipF et al, Cathet Cardiovasc Intervent 84:581, 2014
n=3198
n=3265
FDA MitraClip Approval October 24th, 2013
The MitraClip is approved for treatment of patients with
3+-4+ primary (degenerative) MR who are at “prohibitive risk” for mitral valve surgery and are likely to benefit
from MR reduction
History
• 87 year old man with a history of moderate MR and MVP
• Stable when he developed flash pulmonary edema 3 months prior to presentation
• Echo revealed 4+ MR with a flail leaflet; EF 60%; Flow reversal in Pas
• Refractory CHF – Turned down for OHS
• Offered Hospice – He declined

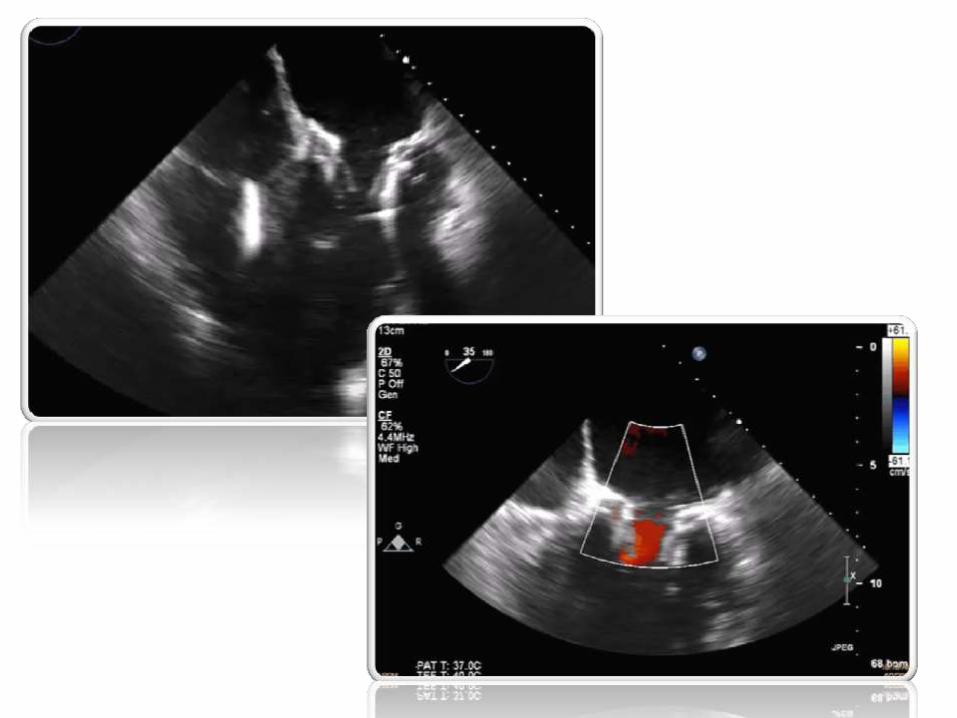
Pre-TEE
Pre TEE
Pre TEE Intercommisural
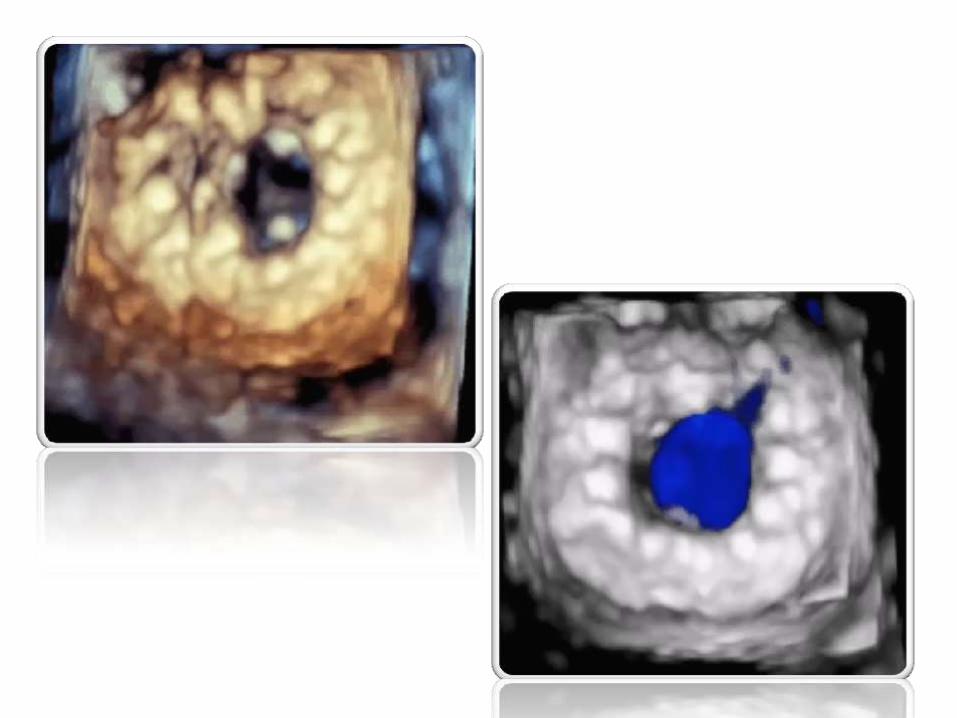
Pre-Imaging – 3D
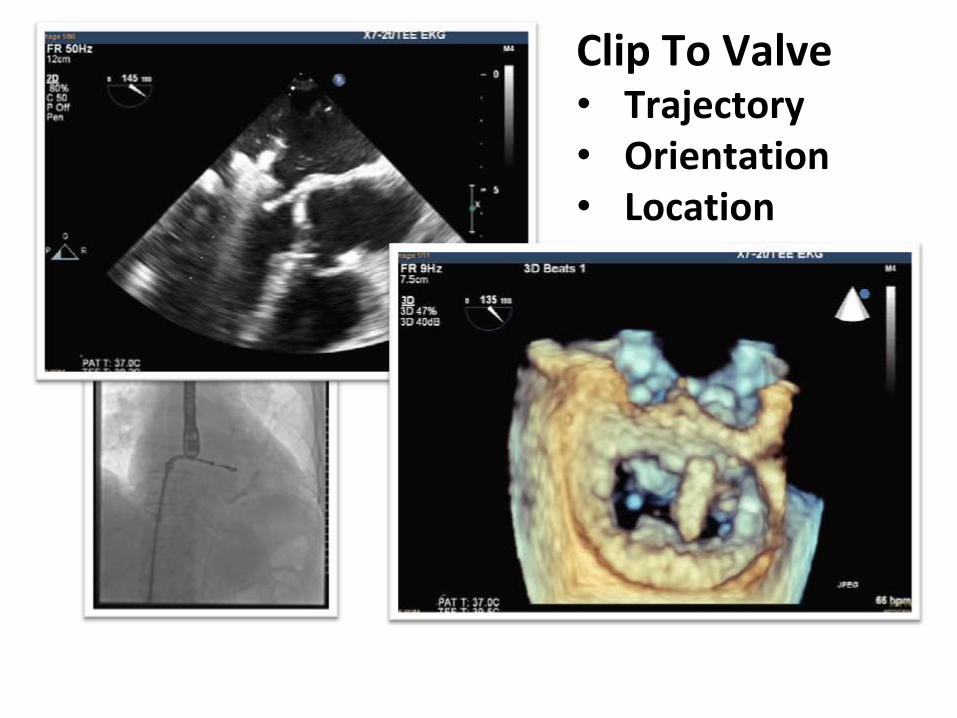
Clip To Valve • Trajectory • Orientation • Location

2nd Clip

Confirm Grasp, R/O MS, and Release 2nd Clip
Follow Up
• Home following day
• Uneventful hospital course
6 months
• Echo – 1+ mild MR
• Functional class 1
• Back golfing
• Walking 3 miles
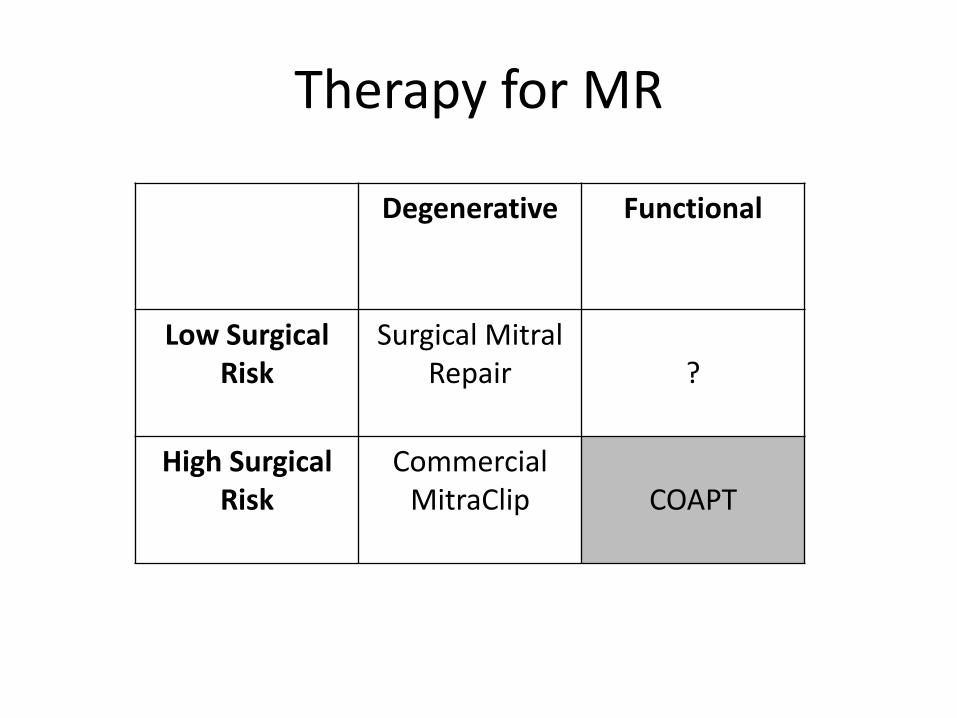
Therapy for MR
Degenerative Functional
Low Surgical Risk
Surgical Mitral Repair
?
High Surgical Risk
Commercial MitraClip
COAPT
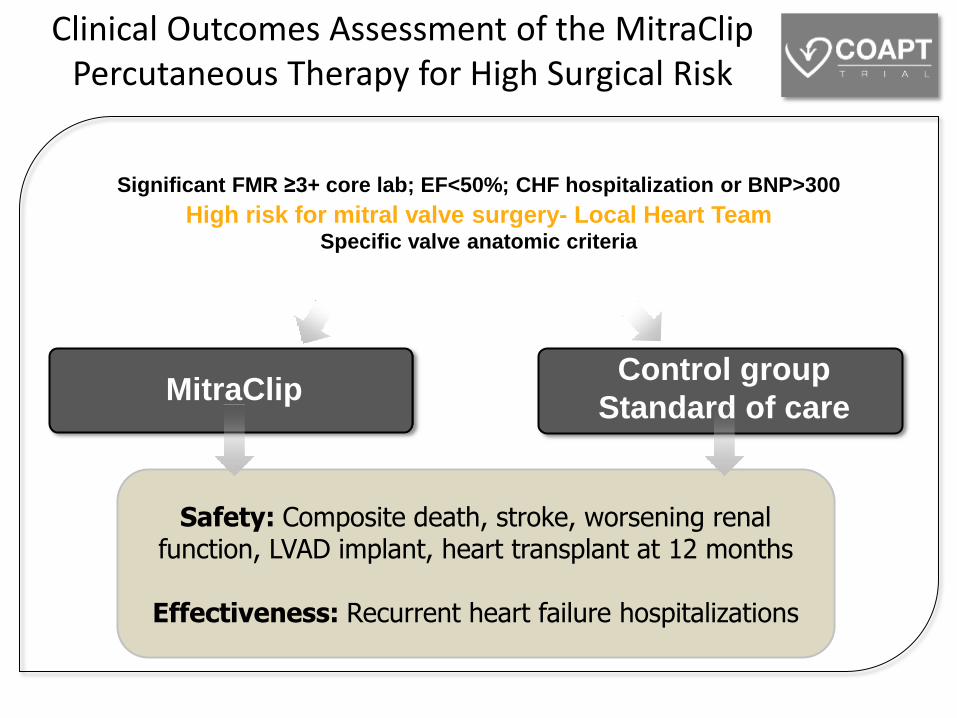
Safety: Composite death, stroke, worsening renal function, LVAD implant, heart transplant at 12 months
Effectiveness: Recurrent heart failure hospitalizations
~430 patients enrolled at up to 75 US sites
Randomize 1:1
Control group
Standard of care
High risk for mitral valve surgery- Local Heart Team
Specific valve anatomic criteria
MitraClip
Significant FMR ≥3+ core lab; EF<50%; CHF hospitalization or BNP>300
Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy for High Surgical Risk
Protocol conditionally approved by FDA July 26, 2012
COAPT Inclusion
• Symptomatic functional MR (≥3+) – Cardiomyopathy ischemic or non-ischemic
• LVEF ≥20% and ≤50%
• HF hospitalization ≤12 months and/or a corrected BNP ≥300 pg/ml or NT-proBNP ≥1500 pg/ml ≤90 days
• TTE on optimal therapy ≥30 days after: – any change in GDMT
– revascularization and/or implant of CRT
Version 5.1 November 11, 2013

Case History
• 79 year old man s/p prior CABG with a 6 month
history of refractory CHF and severe MR, despite maximum medical therapy. No LBBB.
• Several comorbidities including Creatinine or 2.0
mg/dl, atrial fibrillation, DM, prior CVA (complete recovery)
• Echo revealed 4+ MR caused by functional valve disease and EF of 25%; turned down by two surgeons
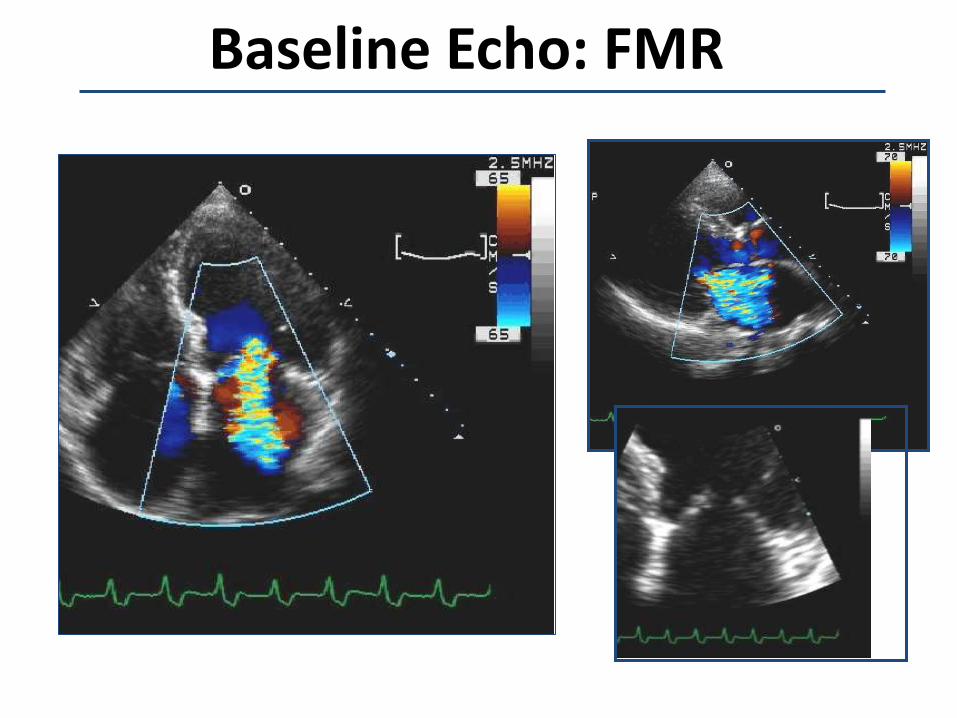
Baseline Echo: FMR

MitraClip Placement
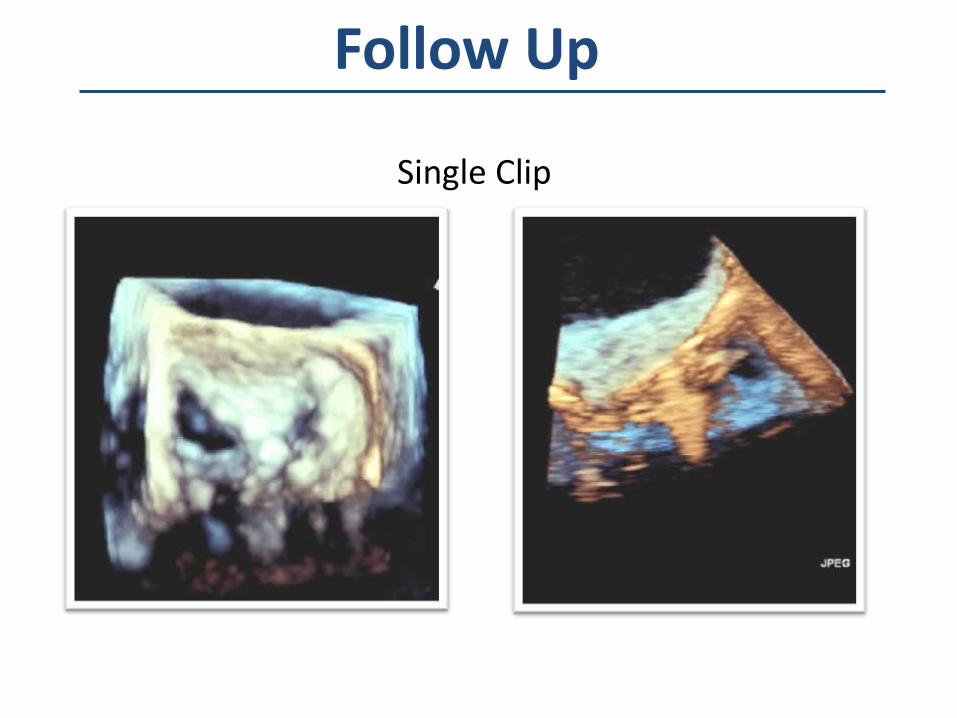
Follow Up
Single Clip

Follow Up
• Trace MR after one clip – Device time 43 min
• Home the following day
• No rehospitalizations
• 2 Year follow up – EF 30-35% with
mild
• 1+ MR; Functional Class II
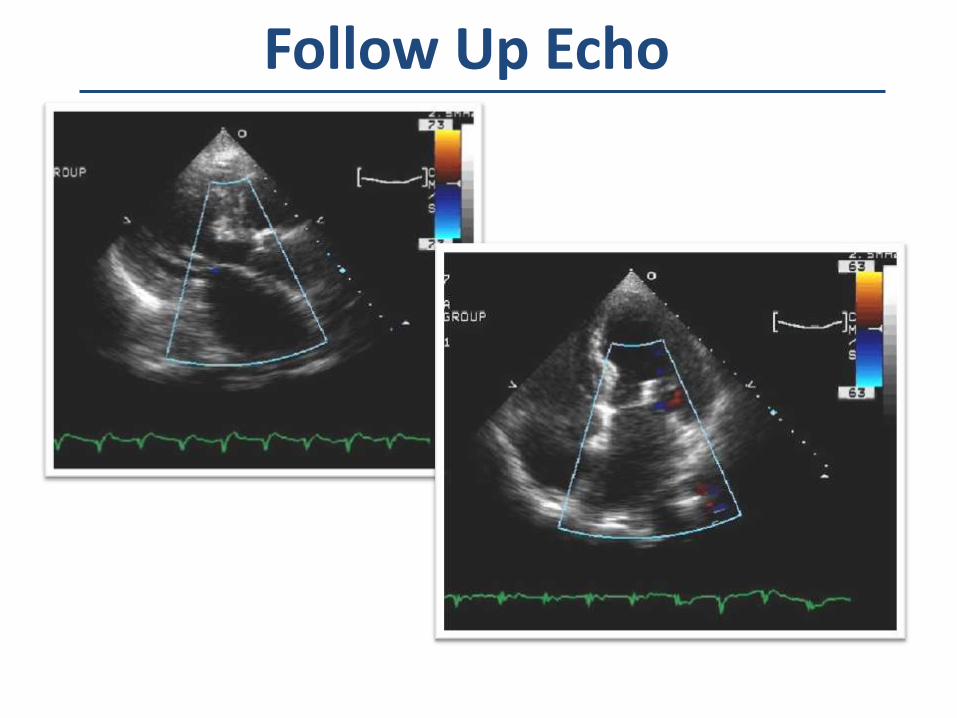
Follow Up Echo
• Introduction
• Transcatheter Repair
– MitraClip
– Annular Approaches
• TMVR
• Summary/Conclusions
Outline
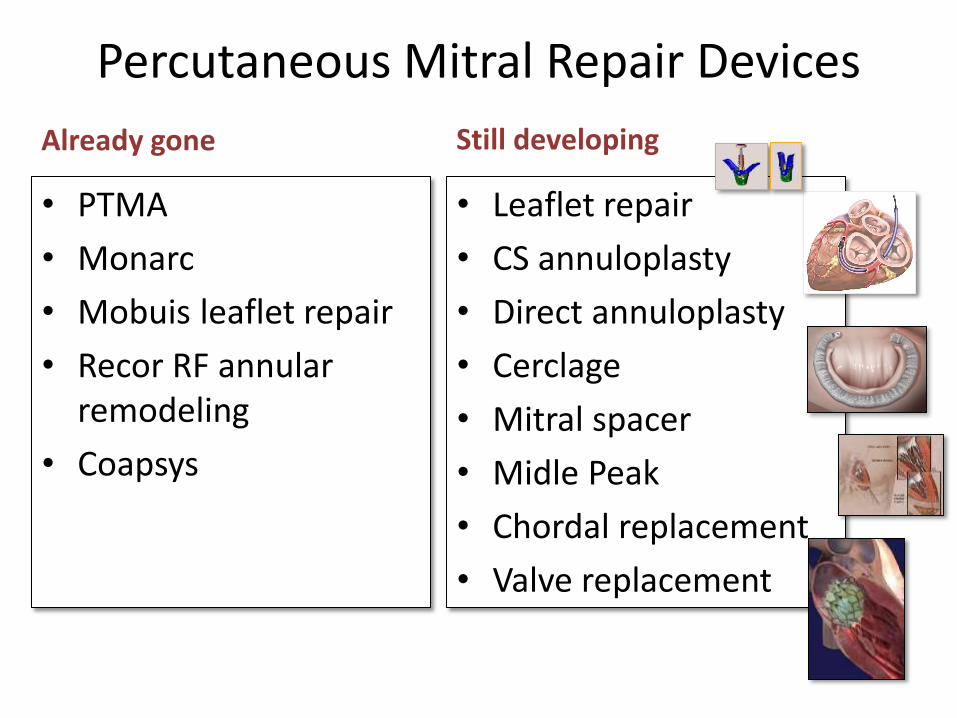
Percutaneous Mitral Repair Devices
• PTMA
• Monarc
• Mobuis leaflet repair
• Recor RF annular remodeling
• Coapsys
• Leaflet repair
• CS annuloplasty
• Direct annuloplasty
• Cerclage
• Mitral spacer
• Midle Peak
• Chordal replacement
• Valve replacement
Already gone Still developing

CARILLON Mitral Contour System
Coronary Sinus- Indirect Annuloplasty
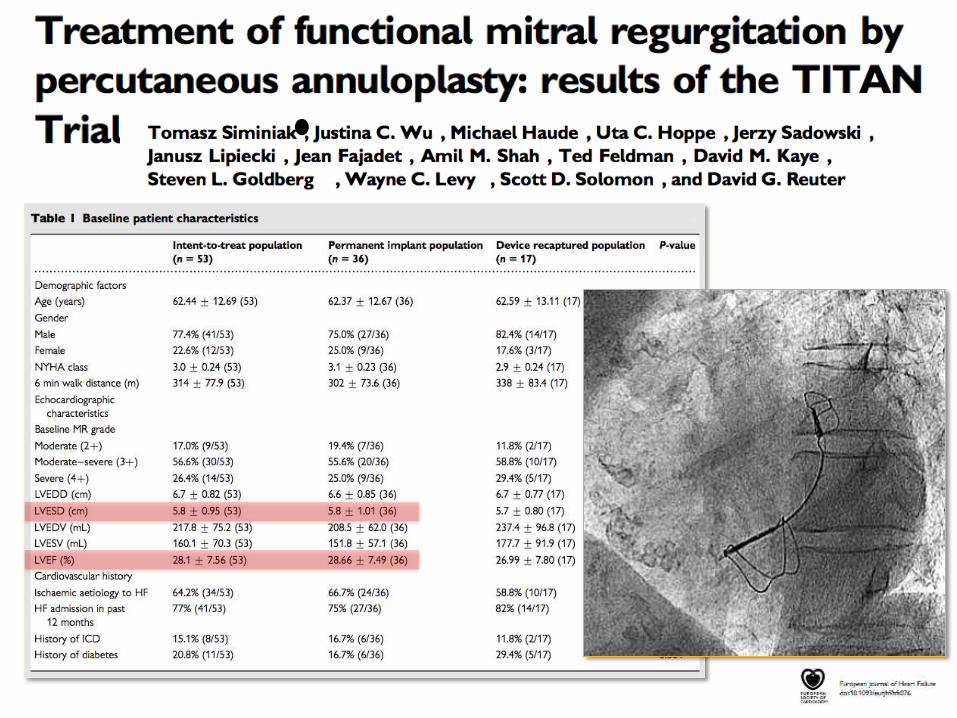
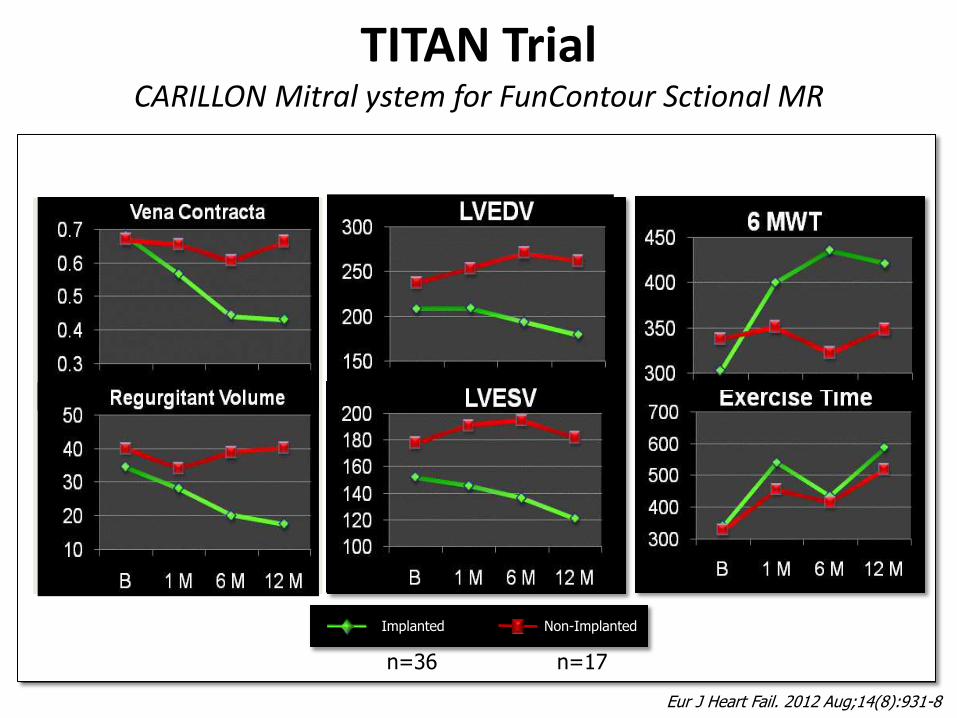
TITAN Trial CARILLON Mitral ystem for FunContour Sctional MR
Non-Implanted Implanted
n=36 n=17
40% reduction in MR Reverse remodeling Functional improvement
Eur J Heart Fail. 2012 Aug;14(8):931-8
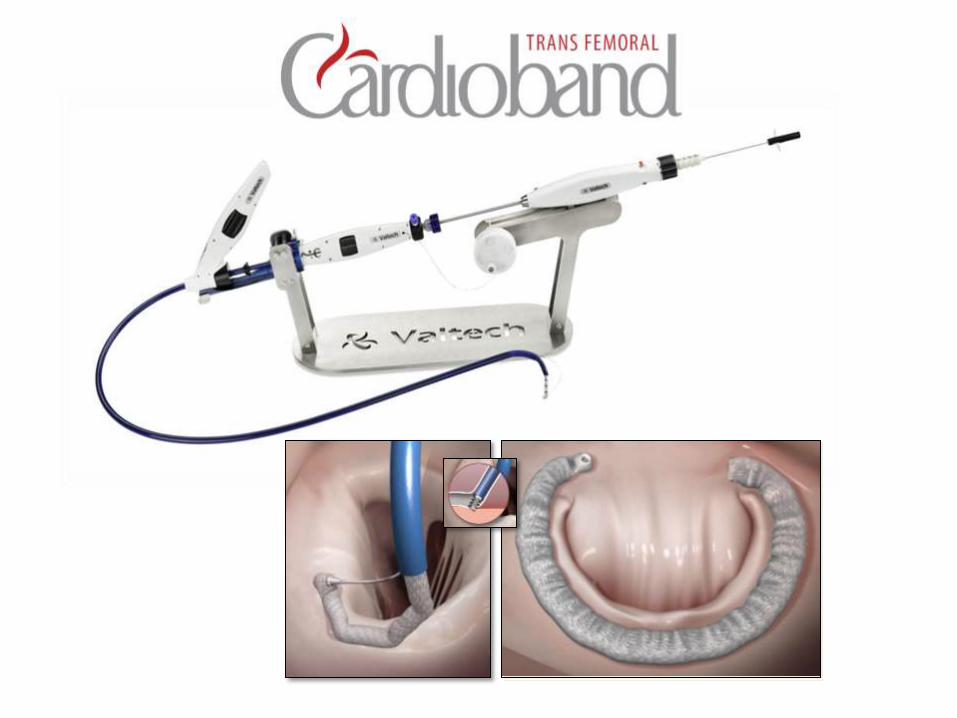
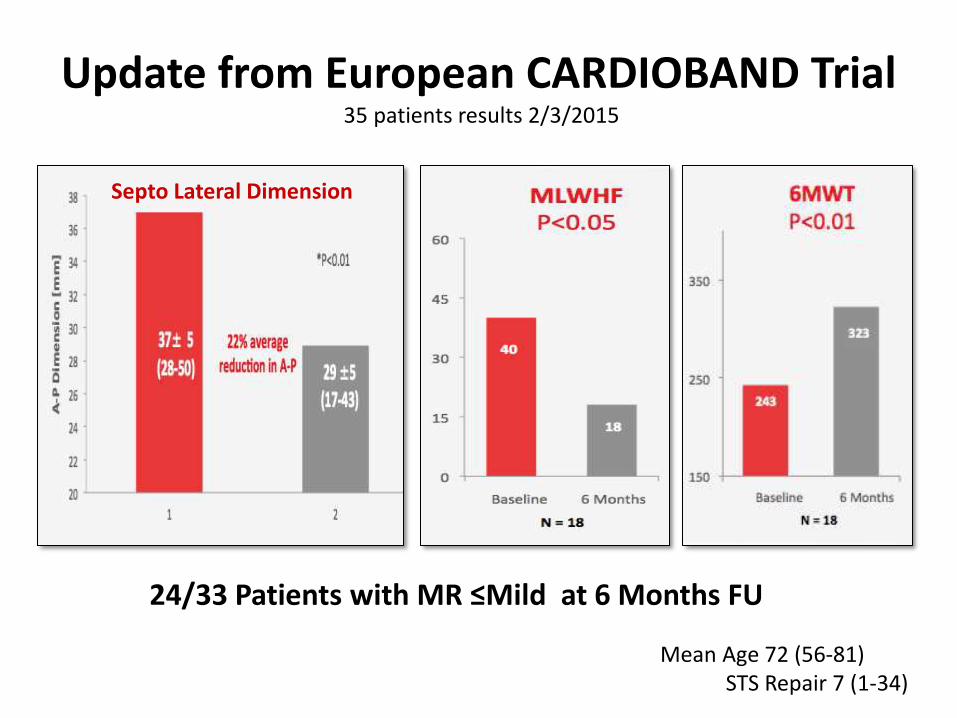
24/33 Patients with MR ≤Mild at 6 Months FU
Update from European CARDIOBAND Trial 35 patients results 2/3/2015
Septo Lateral Dimension
Mean Age 72 (56-81) STS Repair 7 (1-34)
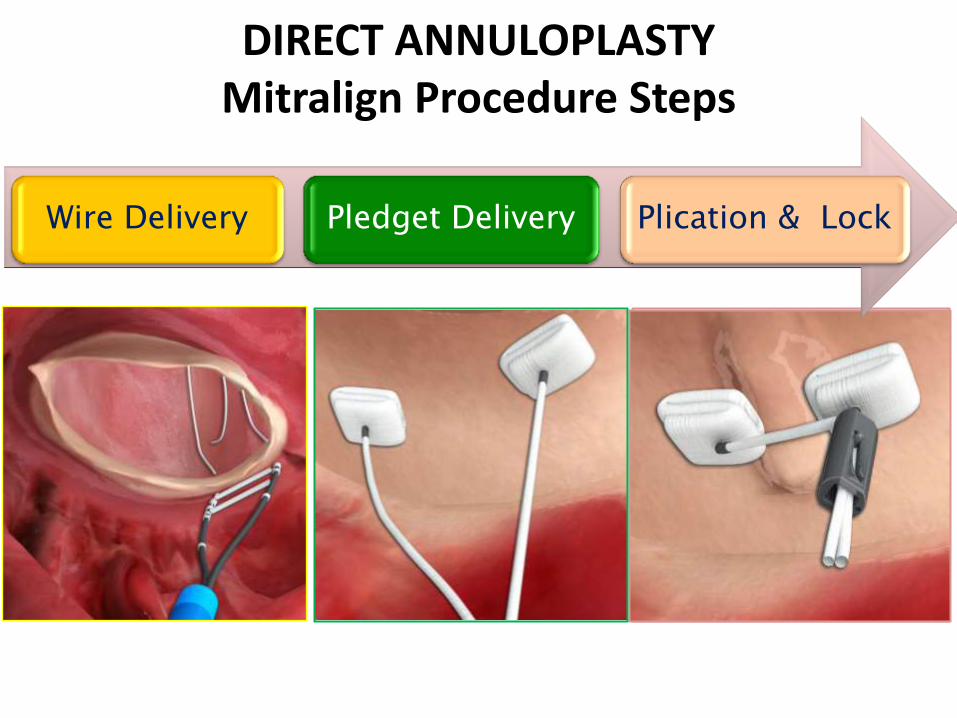
DIRECT ANNULOPLASTY Mitralign Procedure Steps
Wire Delivery Pledget Delivery Plication & Lock

Direct Annuloplasty - Transventricular Approach Mitralign System
Wire Placement Pledget Delivery
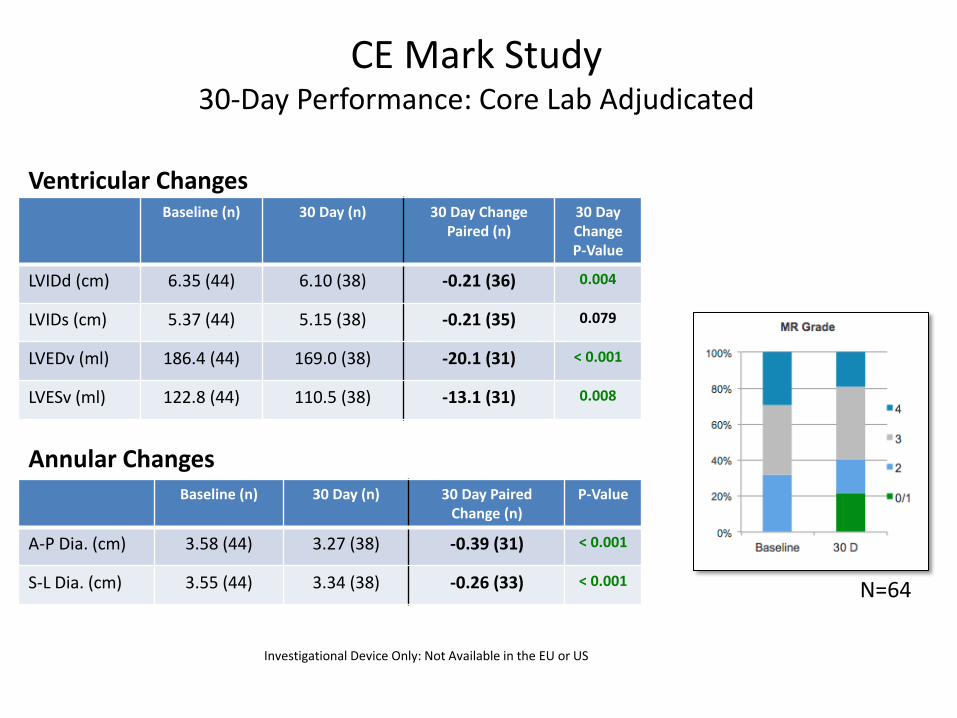
CE Mark Study 30-Day Performance: Core Lab Adjudicated
Baseline (n) 30 Day (n) 30 Day Change Paired (n)
30 Day Change P-Value
LVIDd (cm) 6.35 (44) 6.10 (38) -0.21 (36) 0.004
LVIDs (cm) 5.37 (44) 5.15 (38) -0.21 (35) 0.079
LVEDv (ml) 186.4 (44) 169.0 (38) -20.1 (31) < 0.001
LVESv (ml) 122.8 (44) 110.5 (38) -13.1 (31) 0.008
Ventricular Changes
Baseline (n) 30 Day (n) 30 Day Paired Change (n)
P-Value
A-P Dia. (cm) 3.58 (44) 3.27 (38) -0.39 (31) < 0.001
S-L Dia. (cm) 3.55 (44) 3.34 (38) -0.26 (33) < 0.001
Annular Changes
Investigational Device Only: Not Available in the EU or US
N=64
.J Am Coll Cardiol. 2015;65:1190–5
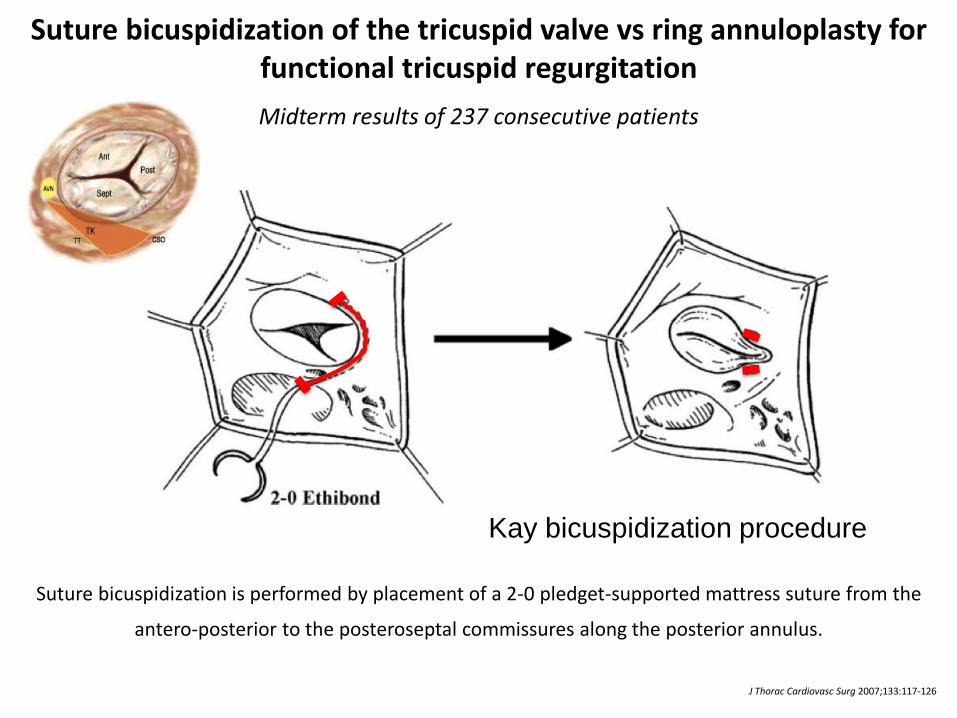
Suture bicuspidization is performed by placement of a 2-0 pledget-supported mattress suture from the
antero-posterior to the posteroseptal commissures along the posterior annulus.
Suture bicuspidization of the tricuspid valve vs ring annuloplasty for functional tricuspid regurgitation
Midterm results of 237 consecutive patients
J Thorac Cardiovasc Surg 2007;133:117-126
Kay bicuspidization procedure
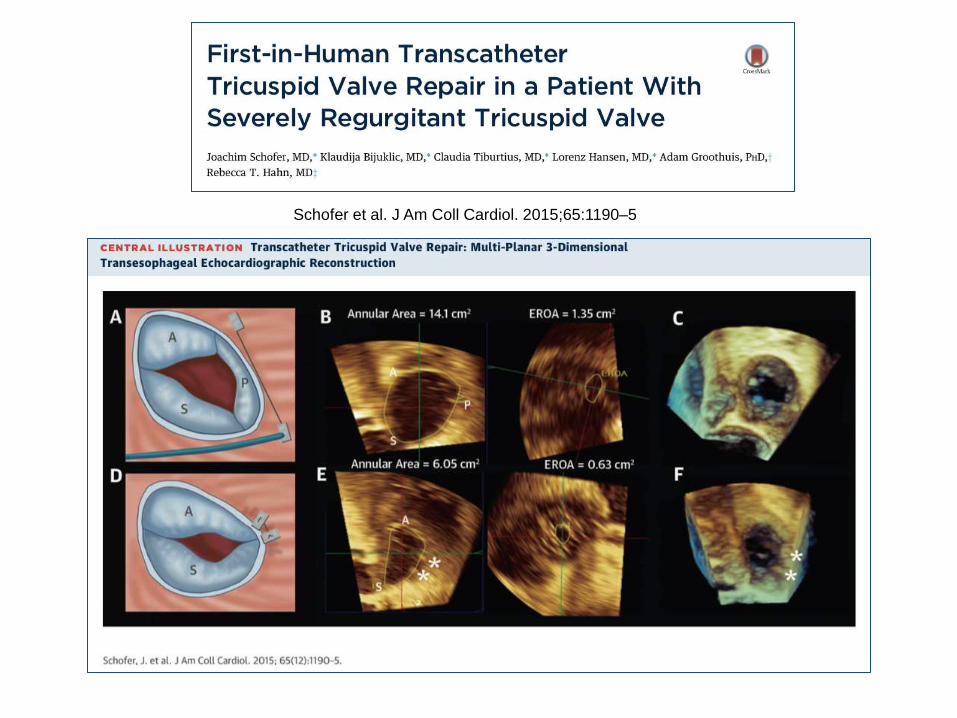
Schofer et al. J Am Coll Cardiol. 2015;65:1190–5
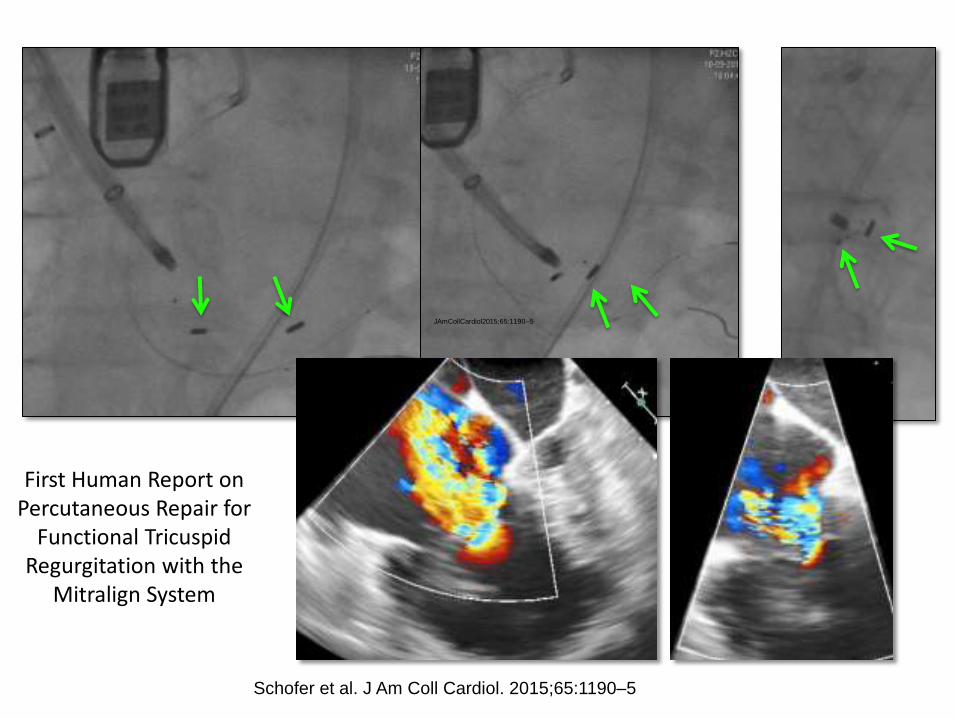
First Human Report on Percutaneous Repair for
Functional Tricuspid Regurgitation with the
Mitralign System
JAmCollCardiol2015;65:1190–5
Schofer et al. J Am Coll Cardiol. 2015;65:1190–5

• Introduction
• Transcatheter Repair
– MitraClip
– Annular Approaches
• TMVR
• Summary/Conclusions
Outline
Mitral Replacement Technologies
• CardiaAQ
• Neovasc TIARA
• Tendyne
• Edwards FORTIS
• Endovalve
• M-Valve
• Medtronic
• Valtech
• Lutter
• MitrAssist
• Caisson
• MitraSeal
• Twelve
• HighLife
• Others….
Mitral Replacement FIRSTS IN HUMAN
• CardiaAQ 2012
• Tendyne Temp implants 2013
• Neovasc Tiara January 2014
• Edwards FORTIS February 2014
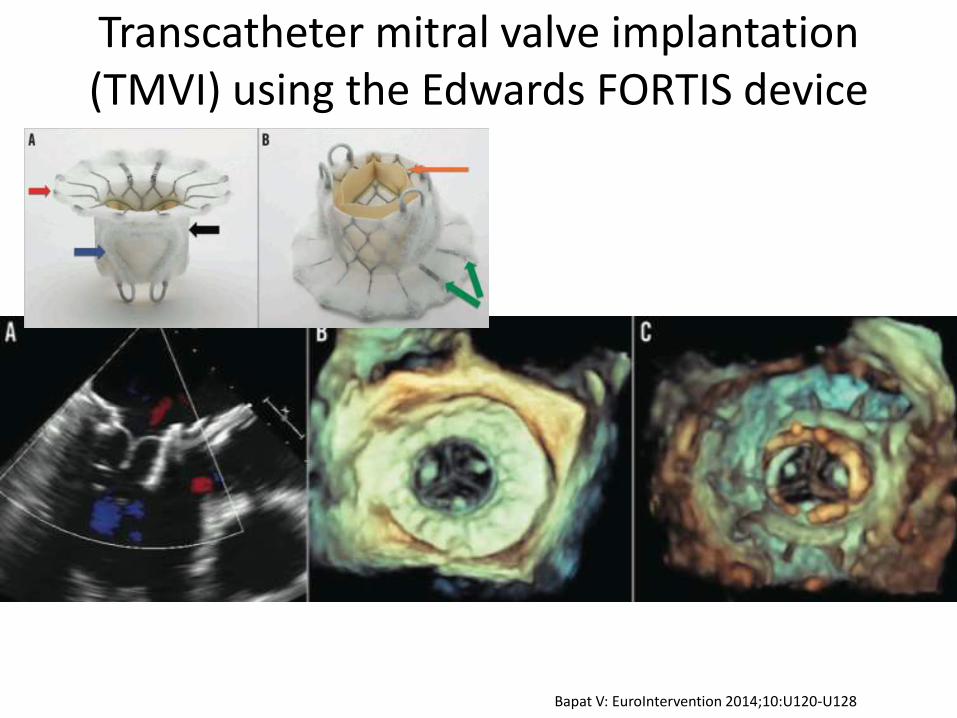
Transcatheter mitral valve implantation (TMVI) using the Edwards FORTIS device
Bapat V: EuroIntervention 2014;10:U120-U128
• Introduction
• Transcatheter Repair
– MitraClip
– Annular Approaches
• TMVR
• Summary/Conclusions
Outline
• Unmet need in high risk patients with MR
• MitraClip safe and effective
– Less MR reduction than surgical repair
– Approved in US for high surgical-risk patients with degenerative MR
– >80% have <2+ MR, short hospital duration, fewer repeat hospitalizations, favorable LV remodeling and functional/QOL outcomes
– Functional MR – enroll in COAPT
• Annular approaches –Early
• TMVR – even earlier - Infancy
Conclusion

Thanks for your attention!