mitral valve repair - greek young · pdf filethan mitral stenosis. ... 106 gillinov and...
TRANSCRIPT

Mitral Valve Repair
A. Marc Gillinov and Delos M. Cosgrove
Surgical repair of the dysfunctional mitral valve dates back to the early twentieth century when several surgeons developed techniques to try to correct mitral stenosis. '-' Mitral insufficiency was approached by only a few surgeons because it was a more complex lesion than mitral stenosis. Initial surgical attempts to treat mitral insufficiency included maneuvers to block the regurgitant jet and the introduction of the annuloplasty concept by Glover and Davila6 in 1938. Lillehei et a17 were the first to attempt to correct pure mitral insuffi- ciency by annuloplasty in 1957, and it appeared that mitral valve repair would become an important proce- dure for cardiac surgeons. However, with the first mitral valve replacement by Starr and Edwards8 in 1961, most surgeons abandoned attempts at mitral valve repair, favoring the reliable results obtained with valve replacement.
The modern era of mitral valve repair was initiated by Carpentier. In 1971, Carpentier et a19 presented the anatomic changes that occur in patients with mitral insufficiency, laying the foundation for a systematic and reproducible approach to mitral valve repair. During the next 2 decades, many surgeons made important contributions to the art and science of mitral valve repair.1°-14 As a result of these innovations and the excellent results obtained, mitral valve repair has become the procedure of choice to correct mitral insufficiency of all origins. l4
Numerous studies have documented that mitral valve repair performed by standardized techniques is repro- ducible and associated with low operative morbidity and r n ~ r t a l i t y . ~ ~ - ~ ~ The advantages of mitral valve re- pair over mitral valve replacement include a lower operative mortality, better preservation of left ventricu- lar function, and higher freedom from thromboembo- lism, anticoagulant-related hemorrhage, and endoyardi- tis.1°-14 Given these advantages, an increasing proportion of surgeons are using mitral valvuloplasty to treat mitral insufficiency.
Although mitral valve repair is the preferred treat- ment for mitral insufficiency of all origins, it has its greatest application and success in correcting mitral insufficiency in patients with degenerative valvular disease. 13-" Carpentier and others have shown that the feasibility of mitral valve repair extends to 95% of patients with degenerative valvular disease versus only 75% of patients with rheumatic or ischemic valvular disease.14 Degenerative disease is the most common
cause of mitral insufficiency in North America, account- able for more than 50% of cases in recent surgical series. '' The most commonly encountered lesion in degenerative mitral valve disease is posterior chordal rupture; other lesions include anterior chordal rup- ture, chordal elongation, annular dilatation, and annu- lar calcification.16 The posterior leaflet is more com- monly affected by degenerative change than is the anterior leaflet, and annular dilatation is limited to the posterior mitral a n n ~ d u s . ~ , ~ ~ Using a variety of repair techniques tailored to the specific pathoanatomy encoun- tered, Deloche et all4 have documented 93% freedom from reoperation after repair of insufficient degenera- tive mitral valves.
Successful mitral valve repair includes four critical components: (1) accurate assessment of the mechanism of valvular dysfunction; (2) consistent and excellent exposure of the mitral valve; (3) precise application of repair techniques; and (4) intraoperative assessment of the results of repair. Each of these components has been standardized to ensure optimal results. The mechanism of valvular dysfunction is determined by intraoperative transesophageal echocardiography and surgical exami- nation of the valve. When the heart is approached by median sternotomy, exposure of the mitral valve is obtained through a lateral left atriotomy, with adjunc- tive maneuvers used as needed. Specific repair tech- niques will be discussed in detail later. Intraoperative transesophageal echocardiography is used to assess the success of repair.
From 1985 to 1997, 1,072 patients had isolated primary mitral valvuloplasty for degenerative mitral valve disease at The Cleveland Clinic Foundation (Cleve- land, OH). During this time period, techniques for valve assessment, exposure, and repair evolved consid- erably. As noted, transesophageal echocardiography has become essential for the determination of the mechanism of mitral regurgitation preoperatively and the assessment of the results of valve repair after bypass surgery. The development of a self-retaining retractor has greatly facilitated operative exposure of the mitral valve. Specific repair techniques have evolved in re- sponse to an improved understanding of the physiology of the mitral valve and studies documenting risk factors for failed mitral valve r e ~ a i r . l ~ - ~ l Procedural risk factors for failed mitral valve repair include the use of chordal shortening techniques,18 residual mitral regur-
Operative Techniques in Thoracic and Cardiovascular Surgery, Vol3, No 2 (May), 1998: pp 95-108 95
96
gitation at the completion of repair,lg and failure to use a ring annuloplasty.21 At Cleveland Clinic, leaflet pro- lapse is corrected by techniques other than chordal shortening, and mitral regurgitation must be 1 + or less at the completion of repair. Virtually all patients receive an annuloplasty, and this is accomplished using the Cosgrove-Edwards Annuloplasty System (Baxter Health-
GILLINOV AND COSGROVE
care, Newport Beach, CA).17 With a design based on an understanding of the normal physiology and patho- anatomy of the mitral valve, this annuloplasty system includes a universally flexible band that produces a measured plication of the posterior annulus. The Cos- grove-Edwards Annuloplasty System is easily applied, and early results have been excellent.17
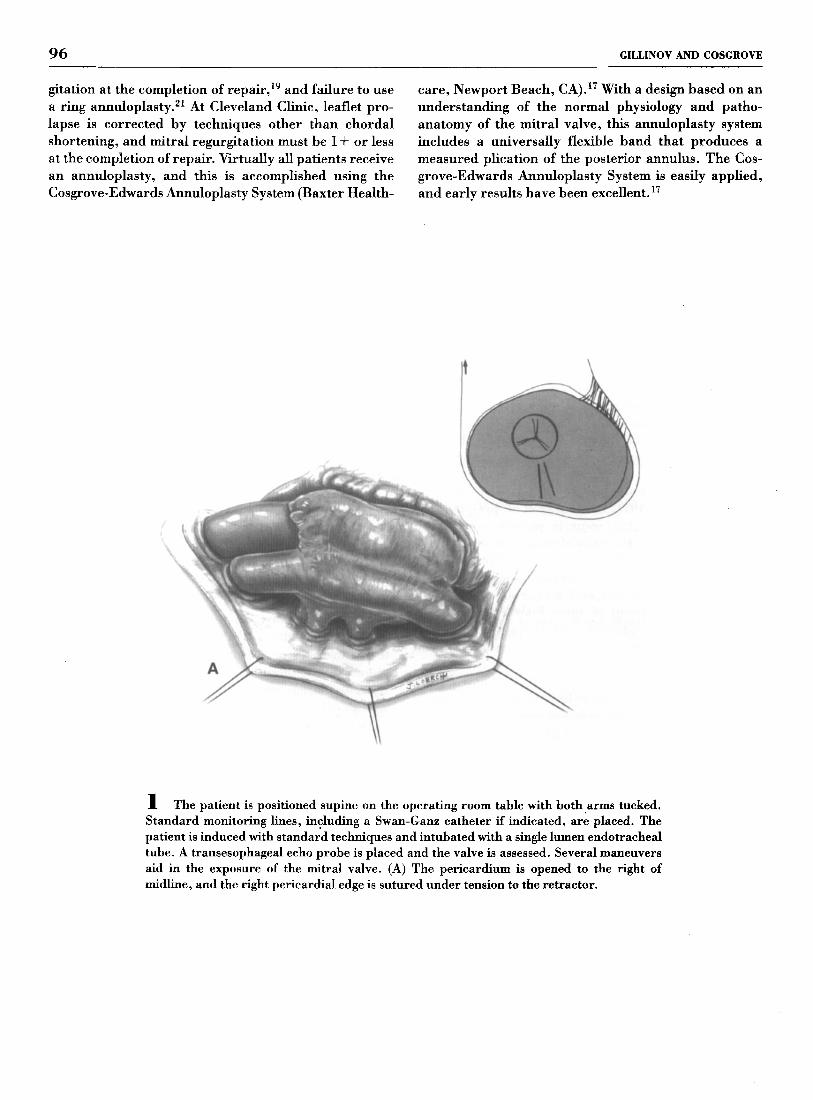
1 The patient is positioned supine on the operating room table with both arms tucked. Standard monitoring lines, including a Swan-Ganz catheter if indicated, are placed. The patient is induced with standard techniques and intubated with a single lumen endotracheal tube. A transesophageal echo probe is placed and the valve is assessed. Several maneuvers aid in the exposure of the mitral valve. (A) The pericardium is opened to the right of midline, and the right pericardial edge is sutured under tension to the retractor.

MV REPAIR 97
1 (continued) (B) Adhesions over the left ventricle are lysed to the permit rotation of the heart. The pericardial reflection onto the superior vena cava is incised, enhancing the mobility of the right atrium when the left atrium is retracted.
98 GILLINOV AND COSGROVE
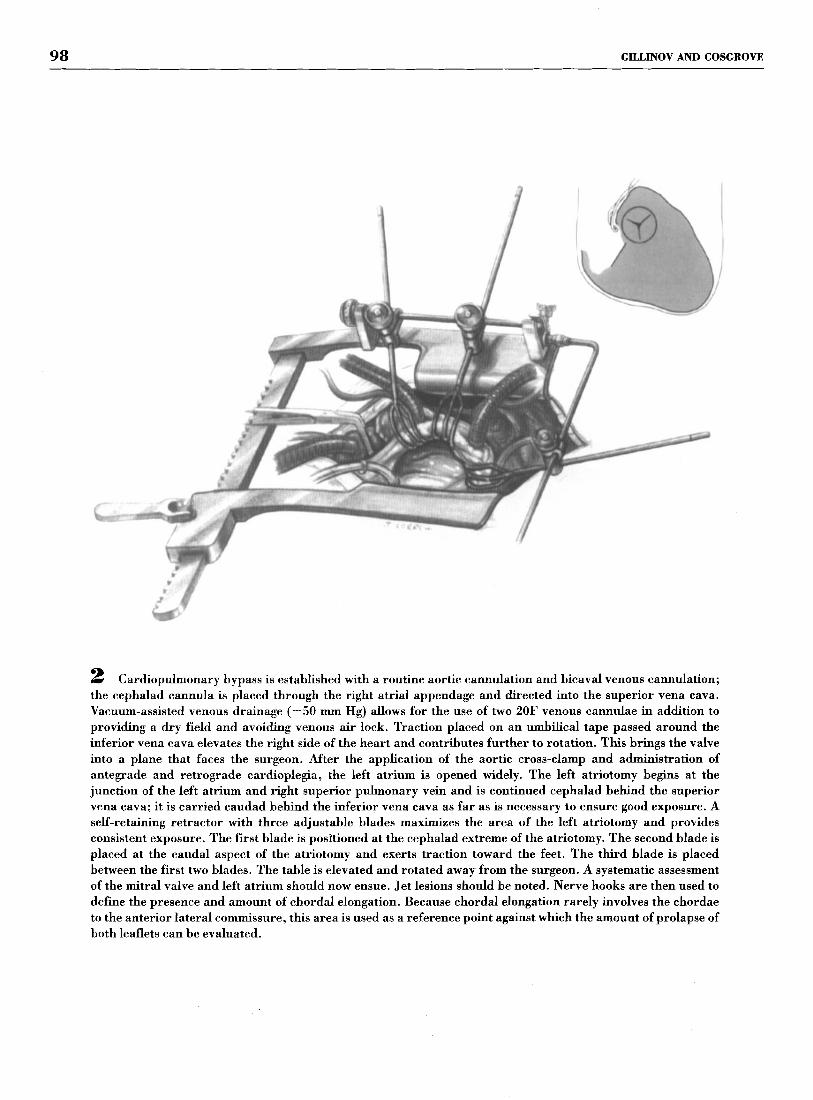
2 Cardiopulmonary bypass is established with a routine aortic cannulation and bicaval venous cannulation; the cephalad cannula is placed through the right atrial appendage and directed into the superior vena cava. Vacuum-assisted venous drainage (-50 mm Hg) allows for the use of two 20F venous cannulae in addition to providing a dry field and avoiding venous air lock. Traction placed on an umbilical tape passed around the inferior vena cava elevates the right side of the heart and contributes further to rotation. This brings the valve into a plane that faces the surgeon. After the application of the aortic cross-clamp and administration of antegrade and retrograde cardioplegia, the left atrium is opened widely. The left atriotomy begins at the junction of the left atrium and right superior pulmonary vein and is continued cephalad behind the superior vena cava; it is carried caudad behind the inferior vena cava as far as is necessary to ensure good exposure. A self-retaining retractor with three adjustable blades maximizes the area of the left atriotomy and provides consistent exposure. The first blade is posfioned at the cephalad extreme of the atriotomy. The second blade is placed at the caudal aspect of the atriotomy and exerts traction toward the feet. The third blade is placed between the first two blades. The table is elevated and rotated away from the surgeon. A systematic assessment of the mitral valve and left atrium should now ensue. Jet lesions should be noted. Nerve hooks are then used to define the presence and amount of chordal elongation. Because chordal elongation rarely involves the chordae to the anterior lateral commissure, this area is used as a reference point against which the amount of prolapse of both leaflets can be evaluated.

MV REPAIR 99
3 The visualization of specific components of the mitral apparatus may require additional maneuvers. (A) The exposure of the posterior medial papillary muscle is enhanced by placing a folded sponge between the diaphragm and the heart. (B) The anterior lateral papillary muscle is exposed by placing a sponge anteriorly between the apex of the heart and the pericardium. Additionally, pressure on the right ventricular outflow tract may aid in exposure of the annulus at the anterolateral commissure.

100 GILLINOV AND COSGROVE
4 (A) A flail portion of the posterior leaflet is treated by resection of the unsupported portion of the leaflet. (B) One or two pledgetted sutures are used to reinforce the annulus at the site of leaflet resection, and the leaflet is repaired with running 5-0 multifilament nonabsorbable sutures. Although the middle scallop of the posterior leaflet is most commonly affected, up to 60% of the posterior leaflet may be resected. A posterior annuloplasty completes the repair.

MV REPAIR 101
5 Ruptured chordae in separate areas of the posterior leaflet are repaired by separate leaflet resections.

102 GILLINOV AND COSGROVE
6 To effectively create a new commissure, ruptured chordae at a commissure are treated by resection of the unsupported portion of the leaflet and reapproximation of the anterior and posterior leaflets and annulus.

MV REPAIR 103
7 ventricular surface of the anterior leaflet and suturing it to the unsupported free edge.
The free edge of the anterior leaflet may be supported by detaching a convenient secondary chord from the

104 GILLINOV AND COSGROVE
8 A flail portion of the anterior leaflet may be supported by performing a quadrangular resection of the posterior leaflet and transferring that portion of the posterior leaflet with its supporting chordae to the anterior leaflet. The posterior leaflet is then repaired, as described previously.

MV REPALR 105
9 Sliding leaflet repair. This technique is used in conjunction with a quadrangular resection when it is judged that the posterior leaflet is too tall (> 1.5 cm), posing an increased risk for systolic anterior motion of the anterior leaflet of the mitral valve. (A) After quadrangular leaflet resection, the remaining posterior leaflet is detached from the annulus; a 1 to 2 mrn scallop of posterior leaflet may be resected along the rim of its attachment to the annulus. (B) With the posterior leaflet detached from the annulus, annuloplasty sutures are placed. The segments of the posterior leaflet are then advanced and reattached to the annulus using running 4-0 monofilament sutures; deep bites are taken through the posterior leaflet, thereby imbricating tissue and further reducing the leaflet height. (C) The site of the quadrangular resection is repaired as previously described, and a posterior annuloplasty completes the repair.

106 GILLINOV AND COSGROVE
10 All mitral valve repairs are reinforced by a posterior annuloplasty. In the case of isolated annular dilatation, posterior annuloplasty may be all that is necessary for mitral valve repair. The ring size is determined by measuring the area of the anterior leaflet. (A) Sutures are placed in the posterior annulus from fibrous trigone to fibrous trigone and then passed through the annuloplasty band. (B) The handle is removed to facilitate tying, but remains attached to aid in the removal of the frame. (C) When all sutures have been tied. the frame is removed.

Mv REPAIR 107
After completing all repair maneuvers, the valve is inspected to ensure that there are no areas of leaflet prolapse. The left ventricle is filled with saline to assess leaflet mobility and coaptation. The left atriotomy is closed in standard fashion and the heart deaired as much as possible before removing the aortic cross- clamp. After a period of recovery, the heart is allowed to fill and eject, and mitral valve function is assessed by transesophageal echocardiography. If the repair is successful (mitral regurgitation 1+ or less), the patient is separated from cardiopulmonary bypass and the valve is once again assessed by transesophageal echocar- diography. Hemostasis is achieved, pacing wires and chest tubes are placed, and the wound is closed in the standard fashion.
COMMENTS At the Cleveland Clinic Foundation, from 1985 to 1997, 1,072 patients with degenerative mitral valve disease had isolated primary valve repair for mitral insuffi- ciency. The mean age of these patients was 58 & 12.5 years (range, 18-84 years); 65% were men. The repair techniques that were used included annuloplasty (89%0), posterior leaflet resection (8l%0), posterior sliding re- pair (22%), chordal transfer (21%), and chordal short- ening (10%). There were three hospital deaths (0.3%). Long-term follow-up was available in 1,062 of 1,069 hospital survivors (99.3%). Ten-year actuarial survival was 81%. Risk factors for late death included anterior leaflet prolapse, chordal shortening, annuloplasty alone, older age, renal dysfunction, and atrial fibrillation. At 10 years, freedom from thromboembolism was 8870, from endocarditis 99%, from anticoagulant-related hem- orrhage 9970, and from reoperation 93%. Of the 30 patients who required reoperation for late mitral valve dysfunction, 16 (53%) had repair failure secondary to progressive degenerative disease. Anterior leaflet pro- lapse, chordal shortening, annuloplasty alone, leaflet resection without annuloplasty, and no intraoperative echocardiogram increased the risk of late reoperation.
These long-term results of mitral valve repair for degenerative mitral valve insufficiency parallel those obtained by Carpentier's group. l4 Although the stan- dardization of techniques for mitral valve repair has allowed widespread application of this operation, refme- ment and innovation continue in this area of cardiac surgery. Significant changes in mitral valve repair technique have occurred during the last decade. As noted previously, the introduction of transesophageal echocardiography has been of great value in determin- ing the mechanism of mitral regurgitation and assessing the success of subsequent repair. Development of the sliding leaflet technique has allowed successful mitral valve repair in the setting of a tall posterior leaflet. Careful analysis of the results of large series has shown
that chordal shortening increases the risk of late repair failure.18.20 At this time, anterior leaflet prolapse should be corrected by chordal transfer or the creation of an artifical chordae.20J2 Failure to perform a ring annulo- plasty increases the risk of repair failure.'l Therefore, nearly all mitral valve repairs in adults should be accompanied by a ring annuloplasty. An improved understanding of the anatomy and physiology of the mitral annulus suggests that a flexible posterior annulo- plasty will preserve physiological function and correct annular dilatation.17 An analysis of the first 300 pa- tients who received the Cosgrove-Edwards Annulo- plasty System showed excellent results, with no in- stances of systolic anterior motion of the mitral valve and 97% freedom from reoperation at 1 year.
The most dramatic technical change in mitral valve surgery during the last 10 years has been the recent development of minimally invasive approaches to the mitral valve. Successful mitral valve repair has been accomplished using a right thorac0tomy,2~ right paraster- nal in~ision, '~ partial stern~tomy, '~ and port-access techniques.26 Each approach provides good exposure of the mitral valve and allows either mitral valve repair or replacement. At Cleveland Clinic, the current pre- ferred approach for isolated mitral valve repair is the partial sternotomy. This approach, coupled with a transseptal incision, provides excellent exposure of the mitral valve. Early results with minimally invasive mitral valve surgery have been encouraging.
Mitral valve repair is the procedure of choice to correct mitral regurgitation caused by degenerative disease. Although standardized techniques for mitral valve repair were developed more than 2 decades ago, operative techniques continue to evolve. Continued assessment of the results of mitral valve repair and the recent interest in minimally invasive approaches to the mitral valve will undoubtedly result in further refine- ment in techniques for mitral valve repair.
1.
2.
3.
4.
5.
6.
7.
8.
REFERENCES Allen DS, Graham EA: Intracardiac surgery-A new method: Report. JAMA 79:1028,1922 Cutler EC, Levine SA: Cardiotomy and valvulotomy for mitral stenosis: Experimental observations and clinical notes concerning an operated case with recovery. Boston Med Surg J 188:1023,1923 Souttar HS: The surgical treatment of mitral stenosis. Br Med J 2:603, 1925 Harken DE, Ellis LB, Ware PF, et al: The surgical treatment of mitral stenosis: Valvuloplasty. N Engl J Med 239:801,1948 Bailey CP: The surgical treatment of mitral stenosis (mitral eommissur- otomy). Dis Chest 15:377,1949 Glover RP, D a d a JC: Reflections on the development of cardiac surgery, in D a d a JC (ed): Second Henry Ford Hospital International Symposium on Cardiac Surgery. New York, M I , Appleton-Century- Crofts, 1975, p 3 Lillehei CW, Gott VL, Dewall RA, et al: Surgical correction of pure mitral insufficiency by annuloplasty under direct vision. Lancet 77:446, 1957 Starr A, Edwards ML: Mitral replacement: Clinical experience with a ball valve prosthesis. Ann Surg 154:726,1961

108
9. Carpentier A, Deloche A, Dauptain J, et al: A new reconstructive operation for correction of mitral and tricuspid insufficiency. J Thorac Cardiovasc Surg 6l:l-13, 1971
10. Cosgrove DM, Chavez AM, Lytle BW, et al: Results of mitral valve reconstruction. Circulation 74:182-187, 1986 (suppl)
11. Galloway AC, Covin SB, Baumann G, et al: Long-term results of mitral valve reconstruction with Carpentier techniques in 148 patients with mitral insufficiency. Circulation 78:197-1105,1988 (suppl)
12. Duran CMG: Perspectives in reparative surgery for acquired valvular disease. Adv Card Surg 4: 1-23,1993
13. David TE, Armstrong S, Sun Z, et al: Late results of mitral valve repair for mitral regurgitation due to degenerative disease. Ann Thorac Surg 56:7-14,1993
14. Deloche A, Jebara VA, Relland JY, et al: Valve repair with Carpentier techniques: The second decade. J Thorac Cardiovasc Surg 99:990-1002, 1990
15. Muehrcke DM, Cosgrove DM: Mitral valvuloplasty, in Edmunds LH (ed): Cardiac Surgery in the Adult. New York, NY, McGraw-Hill, 1997, pp 991-1024
16. Cosgrove DM: Surgery for degenerative mitral valve disease. Semin Thorac Cardiovasc Surg 2:183-193, 1989
17. Cosgrove DM, Arcide JM, Rodriguez L, et al: Initial experience with the Cosgrove-Edwards Annuloplasty System. Ann Thorac Surg 60:499-504, 1995
18. Smedira NG, Selman R, Cosgrove DM, et al: Repair of anterior leaflet prolapse: Chordal transfer is superior to chordal shortening. J Thorac Cardiovasc Surg 112:287-292,1996
19. Fix J, Isada L, Cosgrove DM, et al: Do patients with less than “echo-perfect’’ results from mitral valve repair by intraoperative echocardiography have a different outcome? Circulation 88:3948,1993
GILLINOV AND COSGROVE
20. Gillinov AM, Cosgrove DM, Lytle BW, et al: Reoperation for failure of mitral valve repair. J Thorac Cardiovasc Surg 113:467-475,1997
21. Cohn LH, Couper GS, Aranki SF, et al: Long-term reaults of mitral valve reconstruction for regurgitation of the myxomatous valve. J Thorac Cardiovasc Surg 107:143-151,1994
22. Zussa C, Polesel E, Da Col U, et al: Seven-year experience with chordal replacement in floppy mitral valve. J Thorac Cardiovasc Surg 108:37- 41,1994
23. Chitwood RW, Elbeery JR, Moran JF, et al: Minimally invasive mitral valve repair using transthoracic aortic occlusion. Ann Thorac Surg
24. Navia JL, Cosgrove DM: Minimally invasive mitral valve operations. Ann Thorac Surg 62:1542-154,1996
25. Gundry SR, Shattuck OH, Razzouk GI, et al: Cardiac operations in adults and children via ministernotomy: Facile minimally invasive cardiac surgery. Ann Thorac Surg (in press)
26. Schwarta DS, Ribakove GH, Grossi EA, et al: Minimally invasive mitral valve replacement: Port-access technique, feasibility, and myocardial functional preservation. J Thorac Cardiovasc Surg 113: 1022-1031,1997
63:1477-1479,1997
From the Department of Thoracic and Cardiovascular Surgery, The Cleveland Clinic Foundation, Cleveland, OH.
Address reprint requests to Delos M. Cosgrove, MD, Department of Thoracic and Cardiovascular Surgery/F25, The Cleveland Clinic Foundation, 9500 Euclid Ave, Cleveland, OH 44195.
Copyright 0 1998 by W.B. Saunders Company 1085-5637/98/0302-0002$8.00/0