model heart attack systems of care race / north carolina james g. jollis, m.d. co-director, race
TRANSCRIPT

Model Heart AttackSystems of Care
RACE / North Carolina
James G. Jollis, M.D.
Co-Director, RACE

RACEReperfusion in AMI in Carolina
Emergency departments
• North Carolina
• RACE Pilot
– Design and lessons
• RACE
– Design and lessons

North Carolina
• Population 8,541,221 11th
• Size 48,711 square miles 29th
• 14 PCI hospitals, ~100 non-PCI hospitals
• Relative size– Connecticut and Massachusetts combined
• 4 times area, same population
– Minnesota
• ½ area, 2 times population

North Carolina EMS Milestones
1910
1st air ambulance built in NC
1917
Earliest air ambulance rescue service
Outer Banks to Norfolk hospitals

North Carolina EMS Milestones
1968
One of the 1st Paramedic training programs in U.S.
Haywood County, North Carolina

North Carolina EMS Milestones
1968
Dr. Ralph Feichter, Waynesville internist
+Rescue Squad Volunteersintensive training in cardiac pathophysiology,
electrocardiography, arrhythmia recognition, pharmacology (cardio-active drugs) and CPR.
+2 mobile intensive care vehicles

North Carolina EMS Milestones
2003-2006 RACEReperfusion in AMI in Carolina Emergency Departments

RACEReperfusion in AMI in Carolina
Emergency departments
• North Carolina
• RACE Pilot
– Design and lessons
• RACE
– Design and lessons

RACE pilot 2003
• Improve AMI care at the point of greatest mortality / potential benefit
– Increase the rate of reperfusion– Increase the speed of reperfusion

AMI ReperfusionHow are we doing?
0
10
20
30
40
50
60
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
IV LyticIV Lytic
PPCIPPCI
Year of DischargeYear of Discharge
NRMI 2NRMI 2 NRMI 3NRMI 3 NRMI 4NRMI 4 NRMI 5NRMI 5
Pat
ien
ts,
%P
atie
nts
, %
Immediate CABG
- Range 0.9 % -
1.7 %
6.96.9
39%39%4747
23%23%

0
10
20
30
40
50
60
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
IV LyticIV Lytic
PPCIPPCI
Year of DischargeYear of Discharge
NRMI 2NRMI 2 NRMI 3NRMI 3 NRMI 4NRMI 4 NRMI 5NRMI 5
Pat
ien
ts,
%P
atie
nts
, %
Immediate CABG
- Range 0.9 % -
1.7 %
6.96.9
39%39%4747
23%23%
None 37%None 37%
AMI ReperfusionHow are we doing?

15
25
35
45
55
65
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Year of DischargeYear of Discharge
≤ 65 Yrs
> 65 Yrs
NRMI 2NRMI 2 NRMI 3NRMI 3 NRMI 4NRMI 4 NRMI 5NRMI 5
Pat
ien
ts,
%P
atie
nts
, %
58.858.853%53%
30.930.923%23%
AMI ReperfusionHow are we doing? - Age

RACE pilot 2003

40 mile radius40 mile radius40 mile radius40 mile radius
5 local EDs within 5 local EDs within 40 miles40 miles5 local EDs within 5 local EDs within 40 miles40 miles

Referring MD Referring MD
Call Duke ED, CCU Fellow, or CAD staffCall Duke ED, CCU Fellow, or CAD staff
OLD: >180 minOLD: >180 min
CCU AttendingCCU Attending
ICC FellowICC Fellow ICC AttendingICC Attending
Cath TeamCath Team
Primary PCIPrimary PCI
Fax ECG
Referring MD Referring MD
Call 1-866-MI-2-DUKECall 1-866-MI-2-DUKE
NEW: 100-120 minNEW: 100-120 min
CCU Fellow, Attending, Life FlightCCU Fellow, Attending, Life Flight
ICC Fellow, cath teamICC Fellow, cath team
ICC Attending
ICC Attending
Primary PCIPrimary PCI
Find best transport
Transfer for Primary PCI: Systematic ApproachTransfer for Primary PCI: Systematic Approach
Fax ECG Fax ECG

Direct Activation of Duke Cath Lab based on Pre-hospital ECG by Durham EMS
(preliminary data)
Population n Door-to-balloon Time
Historical 15 104 (75, 131)
EMS not using hotline 12 89 (78,100)
EMS using hotline 20 58 (54,71)
David Strauss 2005

RACE pilot 2003
Lessons from RACE pilot1) Fix your own primary PCI system
first2) Data are exceedingly difficult to
collect without funding or government or payer mandate– Issues include HIPAA, IRB, fear of
release, OIG opinion that PRO hospital data are protected, resources

RACEReperfusion in AMI in Carolina
Emergency departments
• North Carolina
• RACE Pilot
– Design and lessons
• RACE
– Design and lessons
RACEReperfusion in AMI in North
Carolina Emergency Departments
OBJECTIVES
• Regional approach to overcoming systematic
barriers
1) Increase reperfusion rate
2) Increase speed of reperfusion
Organizeregions
Baselinedata
Intervention Postdata
CQI…
2 years

RACEReperfusion in AMI in North
Carolina Emergency Departments
• AMI Guideline based
• PCI or Lytics
– Support “best available therapy”
according to resources / local conditions

RACEPartners

RACEOrganization
• Funded by BCBS of NC Foundation, Genentech, Participating hospitals
• Quality improvement project for state ACC
• Independent oversight board– Leaders in ACC (Douglas), acute MI care (O’Neill, Califf, Brodie), emergency medicine
(Mears), BC/BS (Harris).
• Steering committee– Participating physicians and hospitals
• Coordination– Mayme Lou Roettig, Director; 5 Regional Coordinators
• ~70 hospitals (10 PCI, 60 no-PCI)
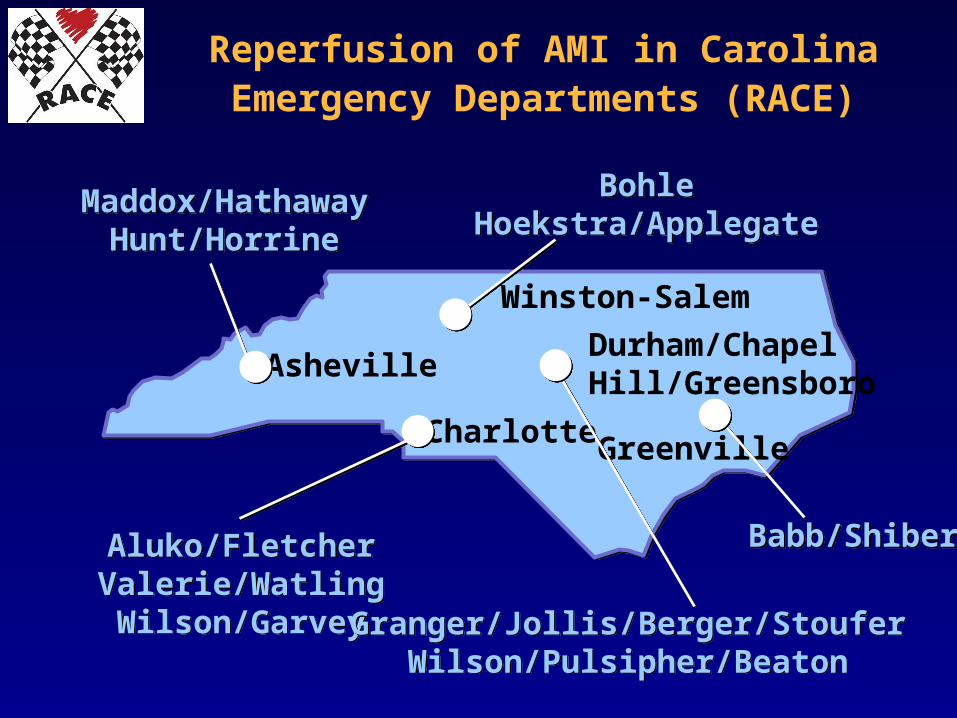
Asheville
Winston-Salem
Durham/Chapel Hill/Greensboro
GreenvilleCharlotte
Reperfusion of AMI in Carolina Emergency Departments (RACE)
Maddox/HathawayHunt/Horrine
Maddox/HathawayHunt/Horrine
BohleHoekstra/Applegate
BohleHoekstra/Applegate
Babb/ShiberBabb/ShiberAluko/FletcherValerie/WatlingWilson/Garvey
Aluko/FletcherValerie/WatlingWilson/Garvey Granger/Jollis/Berger/Stoufer
Wilson/Pulsipher/BeatonGranger/Jollis/Berger/Stoufer
Wilson/Pulsipher/Beaton

RACEData
• PCI hospitals – NRMI
• Non PCI hospitals– Consecutive chart review
• Rate of reperfusion
• Time of reperfusion

RACEManual
Optimal system specifications by point of care EMS ED Transfer Receiving hospital Cath. Lab Other system issues –
payers, regulations
RACERACEReperfusion in Acute myocardial infarctionReperfusion in Acute myocardial infarctionin Carolina Emergency Departmentsin Carolina Emergency Departments
Operations ManualOperations Manual
Granger CB, Jollis JG, et al.Granger CB, Jollis JG, et al.For the North Carolina For the North Carolina RACE steering committeeRACE steering committeeVersion 1.2Version 1.2January 2006January 2006

RACEInterventions
• EMS– In the field ECG
• Regional ECG training courses• Securing funding for ECG equipment

RACEInterventions
•PCI hospital
- Map out process
- ED physician can make decision about PCI without the need for consultation / confirmation
- Single contact number
- Single interventionalist on call for system
- Accept to cath. lab without bed availability
- Streamline registration process
- NRMI in place

RACEInterventions

RACE Additional lessons

RACE Additional lessons
• Requires “donated” efforts of 100’s of
physicians, nurses, administrators, EMTs,
public officials, professional organizations
– Chris Granger, Peter Berger, Magnus Ohman,
Greg Mears, Sid Smith ….

RACE Additional lessons
• Maintain current referral lines
• Physician leadership in ED, Cardiology, and
administration

RACE Additional lessons
Regional structure guides “politics”
- 3 PCI hospitals / 3 Cardiology groups
- 1 PCI hospital / 6 Cardiology groups
- 1 PCI hospital / 1 Cardiology group
- Non-PCI hospital
- Network spoke vs. independent
- Academic hospitals with NIH ranking as primary focus

RACE Additional lessons
• Hospital administration / State legislature buy in
– Smaller hospitals
• All hospitals should treat AMI
– PCI hospitals
• All hospitals at the table
• Establish single contact number and system for
rapid PCI before contacting regional hospitals

RACE Additional lessons
• Data – pre and post intervention
• Quality assurance project
– No protected health information
“there is a reasonable basis to believe the
information can be used to identify the
individual ”
– IRB process potentially one of the greatest
systematic barriers to improving care

RACE Additional lessons
• ED physicians “control” much of STEMI care
and want a single regimen.

RACE Additional lessons
What
Would
Trauma
Do?

RACE Additional lessons
Heart disease 700,000
– Myocardial infarction 200,000
Accidents 100,000
– MVA 60,000
National Center for Health Statistics 2005
3 times as many die from AMI than from trauma
What Would Trauma Do“Golden hour”
• Accept patient regardless of bed availability
• Dummy registration
• Code trauma– Priority
– Everyone knows their role
– Single trauma physician on call
– Single phone call activation
• EMS transport priority
• 24/7 hospital capabilities
• Regionalized system

Top Ten List
10. Use local ambulance to transport pts within 50 miles
9. Keep patient on local ambulance stretcher
8. Give heparin bolus (70 U/kg) and no IV infusion
7. Establish protocol for lytics vs PCI for each ED
6. Establish single call number to PCI centers that "automatically" activates cath lab
5. Record calls and playback for QI
4. Provide standardized feedback reports to each ED
3. Prehospital ECGs for all CP patients
2. "Certify" all EMTs to read ST elevation on ECGs, call from ambulance to activate cath lab
1. Create EMS, ED, cardiology team with committed leadership


• North Carolina– Demographics– EMS history
• RACE pilot– Goal – increase reperfusion – save lives– Duke system– Lessons
• Fix your own system first• Data exceedingly challenging to collect without funding, legal or payer mandate
• RACE– Structure– Timeline– Intervention– Examples
• Flow chart• Telephone call• RACE manual
• Additional lessons• Top 10 interventions

RACEInterventions
• PCI hospital
– Single contact number
– ED physician makes decision
– 2 methods of transport
– Reperfuse with fastest / safest
approach