modified stage 2 2015 2017 2016 reporting requirements meaningful use requirement final... ·...
TRANSCRIPT

Modified Stage 2 2015 ‐ 2017
2016 Reporting Requirements For Eligible Providers (EP)
1

Illinois Health Information TechnologyRegional Extension Center (ILHITREC)
SUPPORT PROVIDED BY ILHITREC: ILHITREC is under contract with the Illinois Department of Health and Family Services (HFS), to provide education, outreach and support to Medicaid providers for the Electronic Health Record Medical Incentive Payment Program (eMIPP). ILHITREC partners with the Illinois Critical Access Hospital Network (ICAHN) and Central Illinois Health Information Exchange (CIHIE) for support in this mission and collaborates with the Chicago Health Information Technology Regional Extension Center based at Northwestern University which serves the City of Chicago.
2

Speaker Biographies
Brenda Simms, RN, BSN, CHTS‐CPBrenda Simms is a Clinical Informatics Specialist at ILHITREC. She works with physicians, practice managers, clinical staff, billing representatives, physicians and EHR vendors to successfully plan, coordinate and implement an electronic health record (EHR) system, as well as assist practices with workflow redesign and development of required quality reporting. Brenda also worked for a time with the Central Illinois Health Information Exchange (CIHIE) to facilitate the implementation and effective adoption of HIE.
Kerri Lanum, MSKerri Lanum is a Clinical Informatics Specialist at ILHITREC. She is an expert in the design and implementation of innovative technologies to support physician and nursing practice workflows. She is certified in eClinicalWorks, Epic Care Ambulatory and Healthy Planet EMR Products. She has been the lead for Quality programs including Meaningful Use, PQRS, HEDIS and ACO projects. She has a passion for educating providers and medical office staff on how to track their quality data to improve patient care.
3
Speaker Biographies
Lauren Wiseman, MSN, RN‐BCLauren Wiseman is the Clinical Services Manager for Central Illinois Health Information Exchange (CIHIE). She works with participating healthcare organizations providing clinical project management, promoting effective adoption of HIE and providing Meaningful Use support with ILHITREC as a Clinical Informatics Specialist. She is an active member of the Health Information Management and Systems Society (HIMSS) and the American Nurses Association (ANA). Lauren holds the ANCC board certification in Nursing Informatics and CPHIMSS.
Carrie Galbraith, FASPRCarrie Galbraith is the Director of the Physician Recruitment Services for the Illinois Critical Access Hospital Network (ICAHN) and a Clinical Informatics Specialist for ILHITREC. Carrie works with participating healthcare organizations providing Meaningful Use support through a grant from ILHITREC. ICAHN provides resources, services, and efficiencies to Critical Access Hospitals in Illinois. Through its partnership with ILHITREC, ICAHN is able to continue its mission to strengthen Illinois critical access hospitals through collaboration. Carrie has actively worked with physicians, CEO, and physician practices for 15 years, 9 of those years with Critical Access Hospitals and Rural Health Clinic.
4
INTRODUCTION
5
Disclaimer
The target audience of this presentation is Eligible Providers, but some references will be made related to Eligible Hospitals.
This webinar is based on official guidance provided by the Centers for Medicare and Medicaid Services (CMS) and the Office of the National Coordinator (ONC), experiences from ILHITREC, and other Regional Extension Centers.
This presentation was prepared as a tool to assist providers enrolled in the EHR Incentive Program administered by CMS. The ultimate responsibility for compliance, submission and response to any remittance from CMS rests with the provider. Medicare policy changes frequently. It is highly recommended that providers and their designee review rules and regulations frequently.
The focus of this presentation is Modified Stage 2 Final Rule (2015-2017) & 2016 Reporting Requirements for Eligible Providers. The contents apply to both the Medicare and Medicaid EHR Incentive Programs through CMS and the ONC.
6
The “Word Salad” of Meaningful Use
7
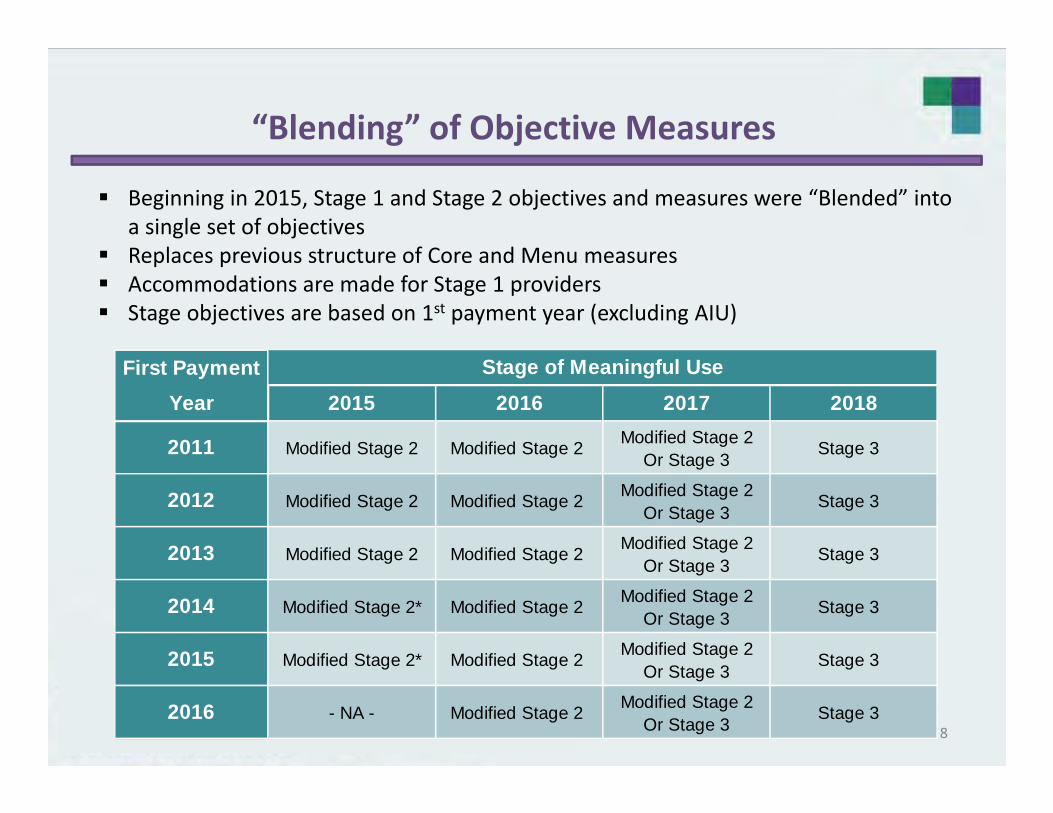
“Blending” of Objective Measures
Beginning in 2015, Stage 1 and Stage 2 objectives and measures were “Blended” into a single set of objectives
Replaces previous structure of Core and Menu measures Accommodations are made for Stage 1 providers Stage objectives are based on 1st payment year (excluding AIU)
First PaymentYear 2015 2016 2017 2018
Modified Stage 2Or Stage 3
Modified Stage 2Or Stage 3
Modified Stage 2Or Stage 3
Modified Stage 2Or Stage 3
Modified Stage 2Or Stage 3
Modified Stage 2Or Stage 3
Stage of Meaningful Use
2011 Modified Stage 2 Modified Stage 2 Stage 3
2012 Modified Stage 2 Modified Stage 2 Stage 3
2013 Modified Stage 2 Modified Stage 2 Stage 3
2016 - NA - Modified Stage 2 Stage 3
2014 Modified Stage 2* Modified Stage 2 Stage 3
2015 Modified Stage 2* Modified Stage 2 Stage 3
8

Progression of Stages for Eligible Providers
9
10

Participation Timeline
Attest to Modified Stage 2 (with accommodations for Stage 1 providers)2015
Attest to Modified Stage 2 (Some alternate exclusions remain for providers)
Last Year to Register and Attest to Begin Medicaid Participation in the program and receive an incentive.
2016
Attest to either Modified Stage 2or full version of Stage 32017
2018 Attest to full version of Stage 3
11
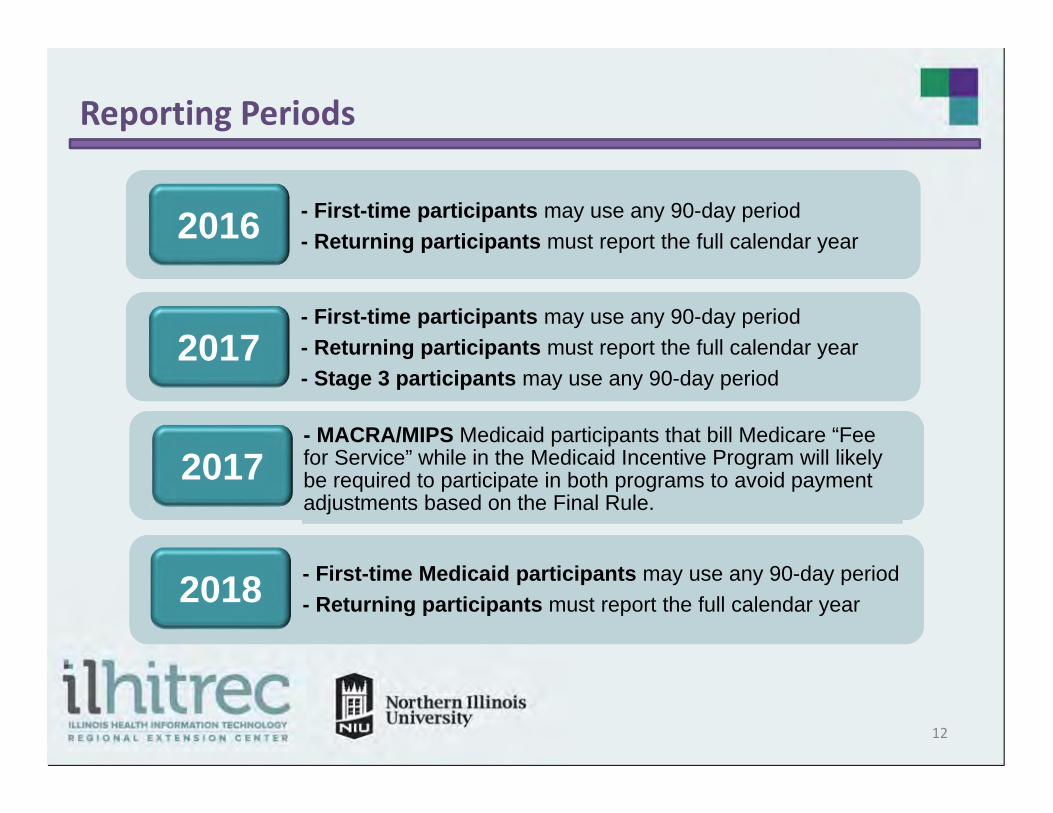
Reporting Periods
2016
2017
2018
- First-time participants may use any 90-day period - Returning participants must report the full calendar year
- First-time participants may use any 90-day period- Returning participants must report the full calendar year- Stage 3 participants may use any 90-day period
- First-time Medicaid participants may use any 90-day period- Returning participants must report the full calendar year
- MACRA/MIPS Medicaid participants that bill Medicare “Fee for Service” while in the Medicaid Incentive Program will likely be required to participate in both programs to avoid payment adjustments based on the Final Rule.
2017
12
Providers Practicing in Multiple Locations
Eligible Providers who practice in multiple locations must take some additional steps in order to successfully participate in the Incentive Program
Example: Provider worked for Employer A from Jan – March Provider works for Employer B from May – December Provider attested to AIU in 2013 Provider attested to MU in 2014 (First time participate) Provider attested to MU in 2015 Provider required to attest to a Full Calendar Year in 2016 Provider required to combined MU data for multiple locations to meet
requirements for attestation of full calendar year
Reference: CMS: Guide for Eligible Professionals Practicing in Multiple Locations (Update March 2016)
CMS:https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2016_EPMultipleLocations.pdf
13
EHR Certification
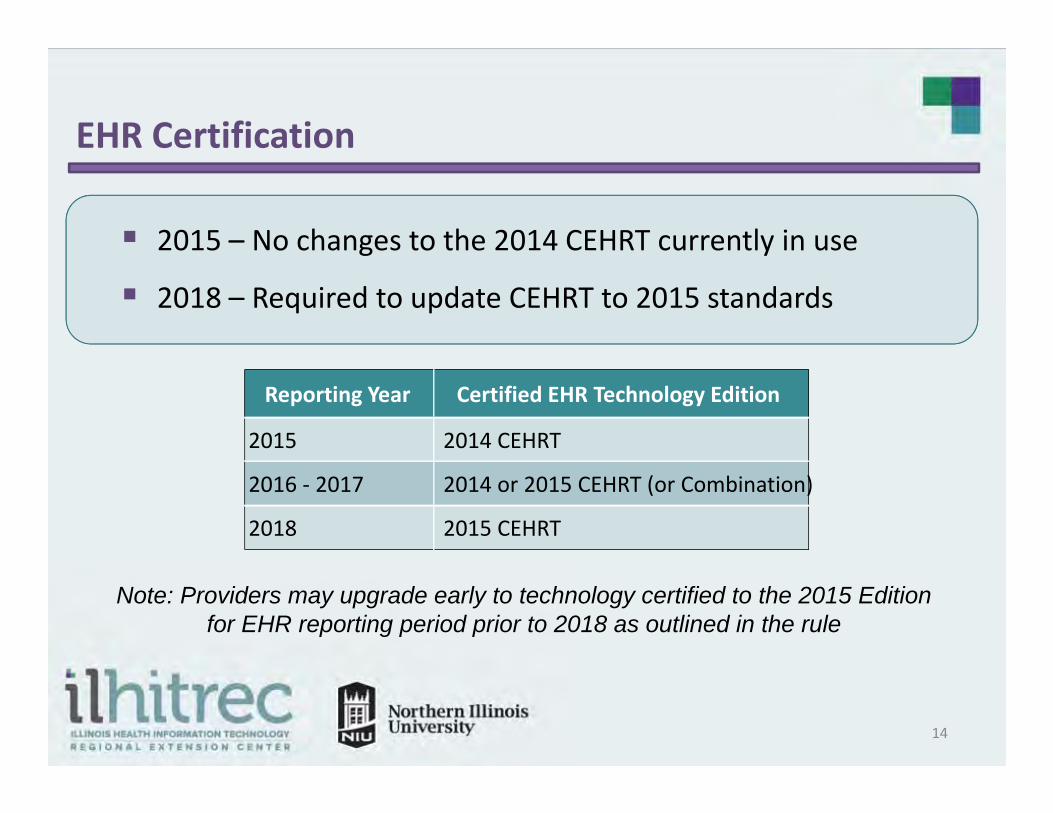
2015 – No changes to the 2014 CEHRT currently in use
2018 – Required to update CEHRT to 2015 standards
Note: Providers may upgrade early to technology certified to the 2015 Editionfor EHR reporting period prior to 2018 as outlined in the rule
14
Reporting Year Certified EHR Technology Edition
2015 2014 CEHRT
2016 ‐ 2017 2014 or 2015 CEHRT (or Combination)
2018 2015 CEHRT
Major Changes to Objectives Beginning in 2016
Many of the alternate exclusions that were available in 2015 are not applicable in 2016.
OBJECTIVE 3 - CPOE: CPOE measure 1 changes from 40% to 60% Alternate exclusion for Measure 2 and 3 New Participants in 2016 may claim exclusion
Providers may attest to CPOE, all three measures
OBJECTIVE 9 Secure Electronic Messaging: ONE patient during reporting period must have at least 1 secure
message sent using CEHRT electronic messaging functionality.
15
Major Changes to Objectives Beginning in 2016
Many of the alternate exclusions that were available in 2015 are not applicable in 2016.
OBJECTIVE 10 – Public Health Reporting: EPs scheduled to be either Stage 1 or Stage 2 Attest to TWO PH measures
EPs may claim an exclusion to either Syndromic Surveillance or Specialized Registry
An alternate exclusion may only be claimed for up to two measures, the provider must either attest to or meet the meet the exclusion requirement for the remaining measure.
Reminder: Register with MURS within 60 days of starting reporting period and register any new providers to your organization.
16
Modified Stage 2 Objectives for Eligible Providers
Modified Stage 2 Alternative Measures First Time Participants
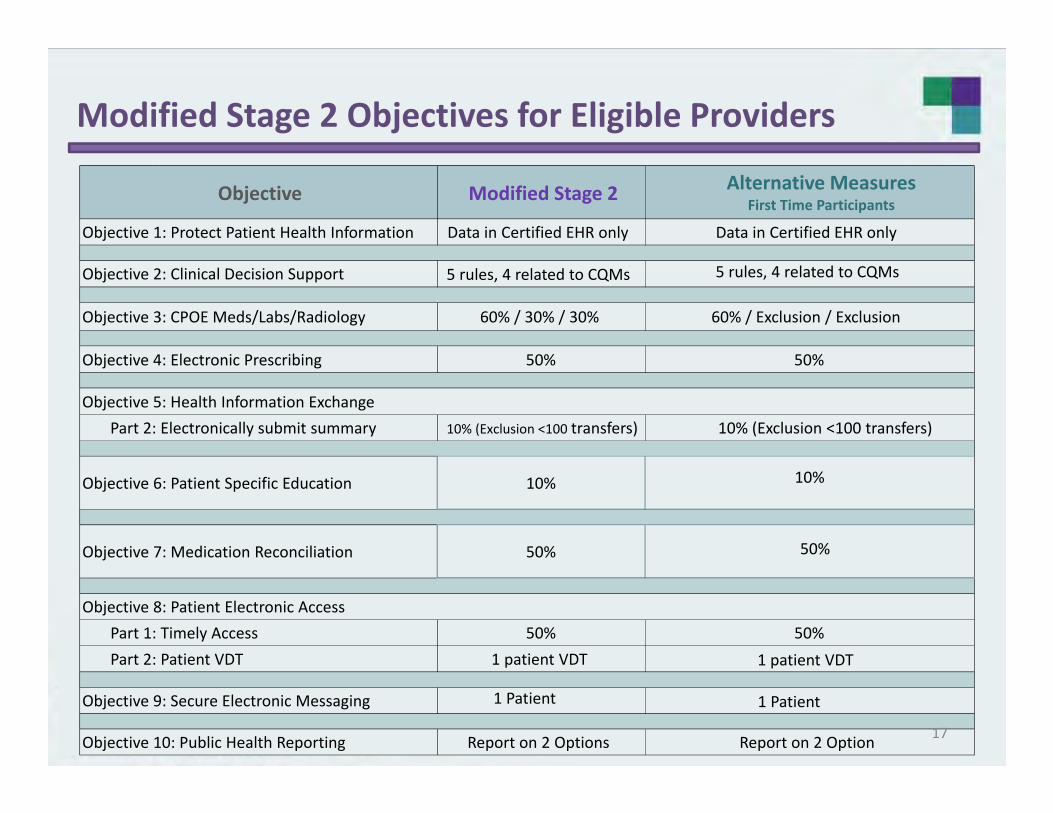
Data in Certified EHR only Data in Certified EHR only
5 rules, 4 related to CQMs 5 rules, 4 related to CQMs
Objective 3: CPOE Meds/Labs/Radiology 60% / 30% / 30% 60% / Exclusion / Exclusion
Objective 4: Electronic Prescribing 50% 50%
Objective 5: Health Information ExchangePart 2: Electronically submit summary 10% (Exclusion <100 transfers) 10% (Exclusion <100 transfers)
Objective 6: Patient Specific Education 10% 10%
50% 50%
Objective 8: Patient Electronic AccessPart 1: Timely Access 50% 50%Part 2: Patient VDT 1 patient VDT 1 patient VDT
Objective 9: Secure Electronic Messaging 1 Patient 1 Patient
Objective 10: Public Health Reporting Report on 2 Options Report on 2 Option
Objective
Objective 7: Medication Reconciliation
Objective 1: Protect Patient Health Information
Objective 2: Clinical Decision Support
17
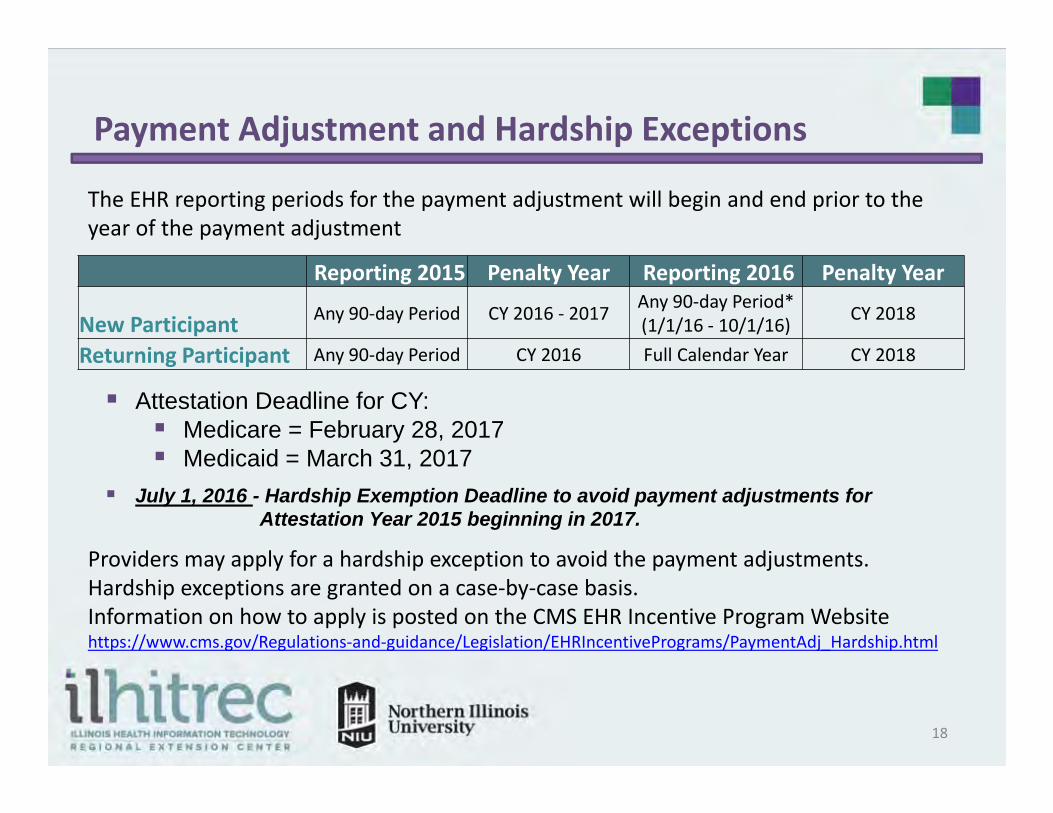
Payment Adjustment and Hardship Exceptions
Reporting 2015 Penalty Year Reporting 2016 Penalty Year
New Participant Any 90‐day Period CY 2016 ‐ 2017 Any 90‐day Period* (1/1/16 ‐ 10/1/16) CY 2018
Returning Participant Any 90‐day Period CY 2016 Full Calendar Year CY 2018
The EHR reporting periods for the payment adjustment will begin and end prior to the year of the payment adjustment
Providers may apply for a hardship exception to avoid the payment adjustments.Hardship exceptions are granted on a case‐by‐case basis.Information on how to apply is posted on the CMS EHR Incentive Program Websitehttps://www.cms.gov/Regulations‐and‐guidance/Legislation/EHRIncentivePrograms/PaymentAdj_Hardship.html
Attestation Deadline for CY: Medicare = February 28, 2017 Medicaid = March 31, 2017
July 1, 2016 - Hardship Exemption Deadline to avoid payment adjustments forAttestation Year 2015 beginning in 2017.
18

Medicaid Alternate Attestation
What if I meet Meaningful Use but Do Not have 30% Patient Volume?
Meaningful Use Attestation is performed in the Medicare EHR Attestation System
• Provider Avoids the Payment Adjustment for Attestation Year.
• Provider Does Not receive an Incentive Payment for Attestation Year.
19
OBJECTIVE OVERVIEW
20
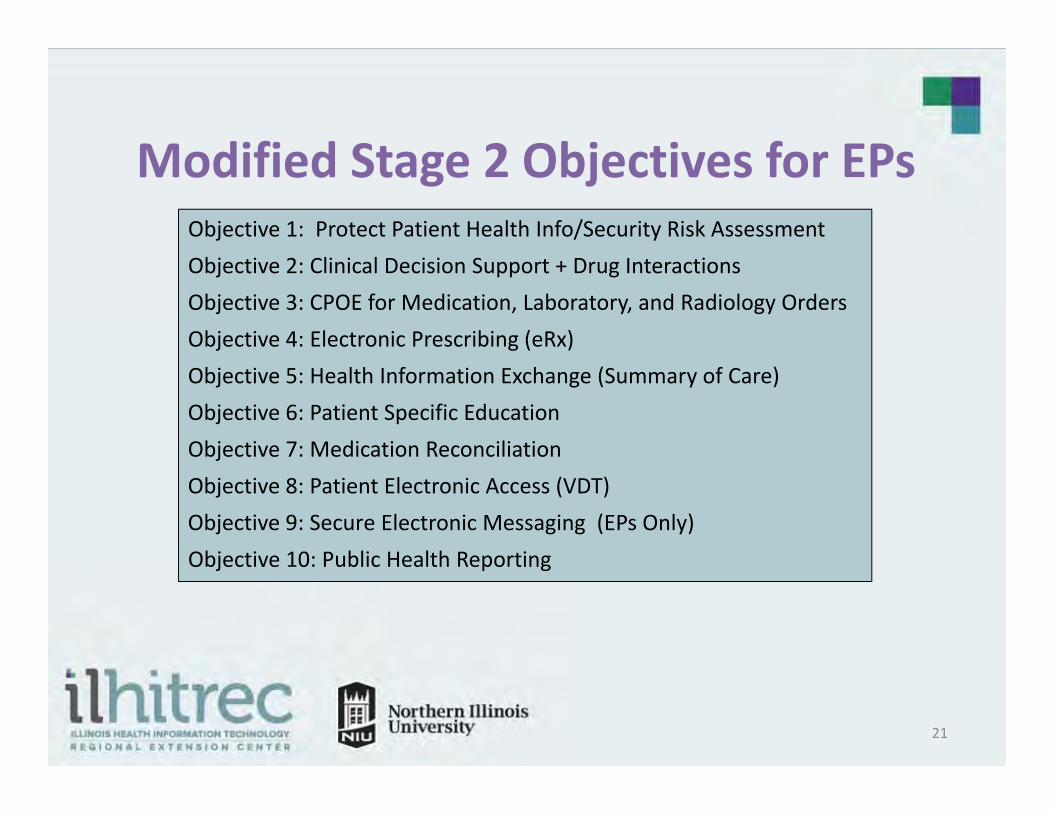
Modified Stage 2 Objectives for EPsObjective 1: Protect Patient Health Info/Security Risk AssessmentObjective 2: Clinical Decision Support + Drug InteractionsObjective 3: CPOE for Medication, Laboratory, and Radiology OrdersObjective 4: Electronic Prescribing (eRx)Objective 5: Health Information Exchange (Summary of Care)Objective 6: Patient Specific EducationObjective 7: Medication ReconciliationObjective 8: Patient Electronic Access (VDT)Objective 9: Secure Electronic Messaging (EPs Only)Objective 10: Public Health Reporting
21
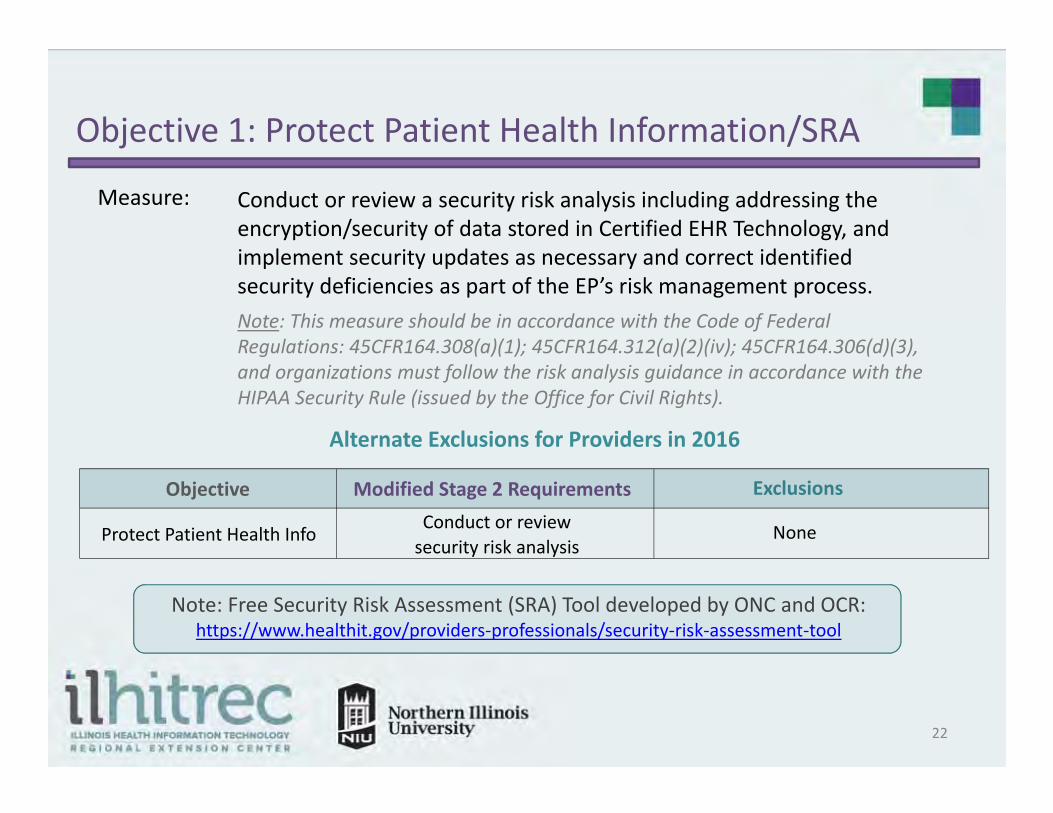
Objective 1: Protect Patient Health Information/SRA
Conduct or review a security risk analysis including addressing the encryption/security of data stored in Certified EHR Technology, and implement security updates as necessary and correct identified security deficiencies as part of the EP’s risk management process. Note: This measure should be in accordance with the Code of Federal Regulations: 45CFR164.308(a)(1); 45CFR164.312(a)(2)(iv); 45CFR164.306(d)(3), and organizations must follow the risk analysis guidance in accordance with the HIPAA Security Rule (issued by the Office for Civil Rights).
Measure:
Alternate Exclusions for Providers in 2016
Note: Free Security Risk Assessment (SRA) Tool developed by ONC and OCR: https://www.healthit.gov/providers‐professionals/security‐risk‐assessment‐tool
22
Objective Modified Stage 2 Requirements Exclusions
Protect Patient Health Info Conduct or review security risk analysis
None

Objective 2: Clinical Decision Support + Drug Interactions
Measure 1: Implement five clinical decision support interventions related to four or more clinical quality measures at a relevant point in patient care for the entire EHR reporting period.
Measure 2: The EP has enabled and implemented the functionality for drug‐drug and drug allergy interaction checks for the entire reporting period.Exclusion: Any EP who writes fewer than 100 medication orders during the reporting period.
Alternate Exclusions and Specifications for Providers in 2016
Measure Modified Stage 2 Requirements Attestation Requirements
1. Clinical Decision Support 5 rules, 4 related to CQMs Entire reporting period
2. Drug Interactions Functionality Enabled Must attest “Yes” to be in compliance
23
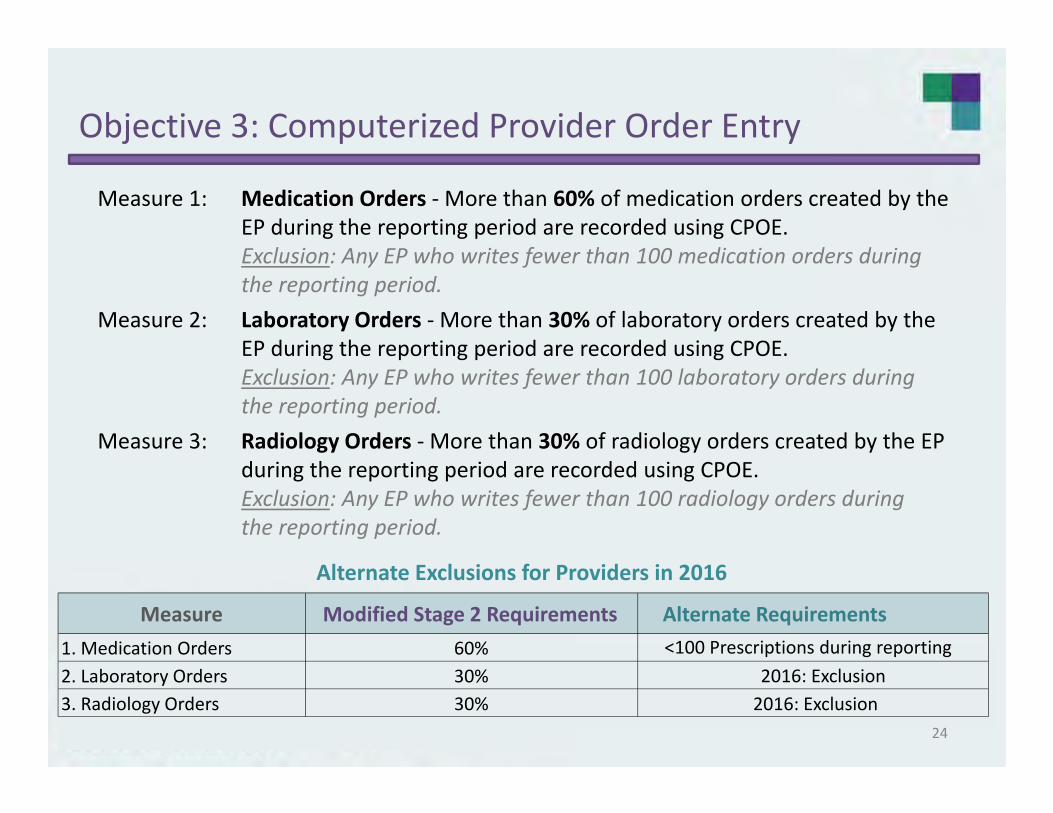
Objective 3: Computerized Provider Order Entry
Measure 1: Medication Orders ‐More than 60% of medication orders created by the EP during the reporting period are recorded using CPOE.Exclusion: Any EP who writes fewer than 100 medication orders during the reporting period.
Measure 2: Laboratory Orders ‐More than 30% of laboratory orders created by the EP during the reporting period are recorded using CPOE.Exclusion: Any EP who writes fewer than 100 laboratory orders during the reporting period.
Measure 3: Radiology Orders ‐More than 30% of radiology orders created by the EP during the reporting period are recorded using CPOE.Exclusion: Any EP who writes fewer than 100 radiology orders during the reporting period.
Alternate Exclusions for Providers in 2016
Measure Modified Stage 2 Requirements Alternate Requirements1. Medication Orders 60% <100 Prescriptions during reporting2. Laboratory Orders 30% 2016: Exclusion3. Radiology Orders 30% 2016: Exclusion
24
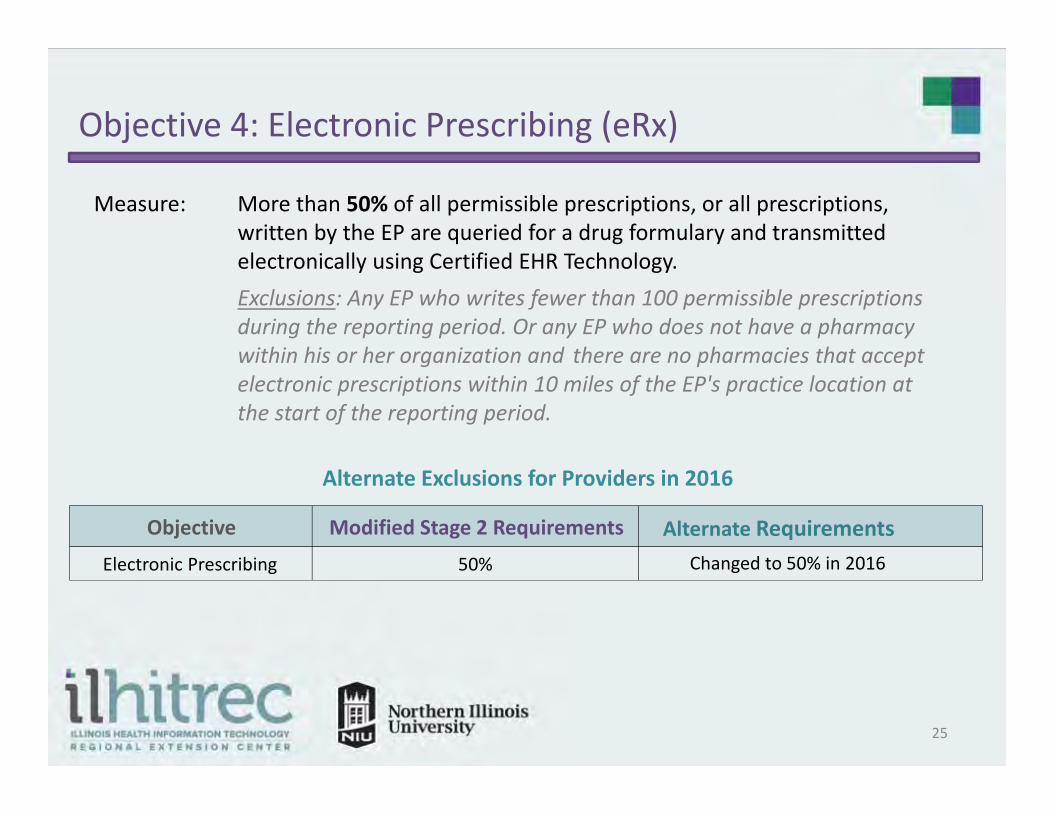
Objective 4: Electronic Prescribing (eRx)
Measure: More than 50% of all permissible prescriptions, or all prescriptions, written by the EP are queried for a drug formulary and transmitted electronically using Certified EHR Technology.Exclusions: Any EP who writes fewer than 100 permissible prescriptions during the reporting period. Or any EP who does not have a pharmacy within his or her organization and there are no pharmacies that accept electronic prescriptions within 10 miles of the EP's practice location at the start of the reporting period.
Alternate Exclusions for Providers in 2016
Objective Modified Stage 2 Requirements Alternate RequirementsElectronic Prescribing 50% Changed to 50% in 2016
25
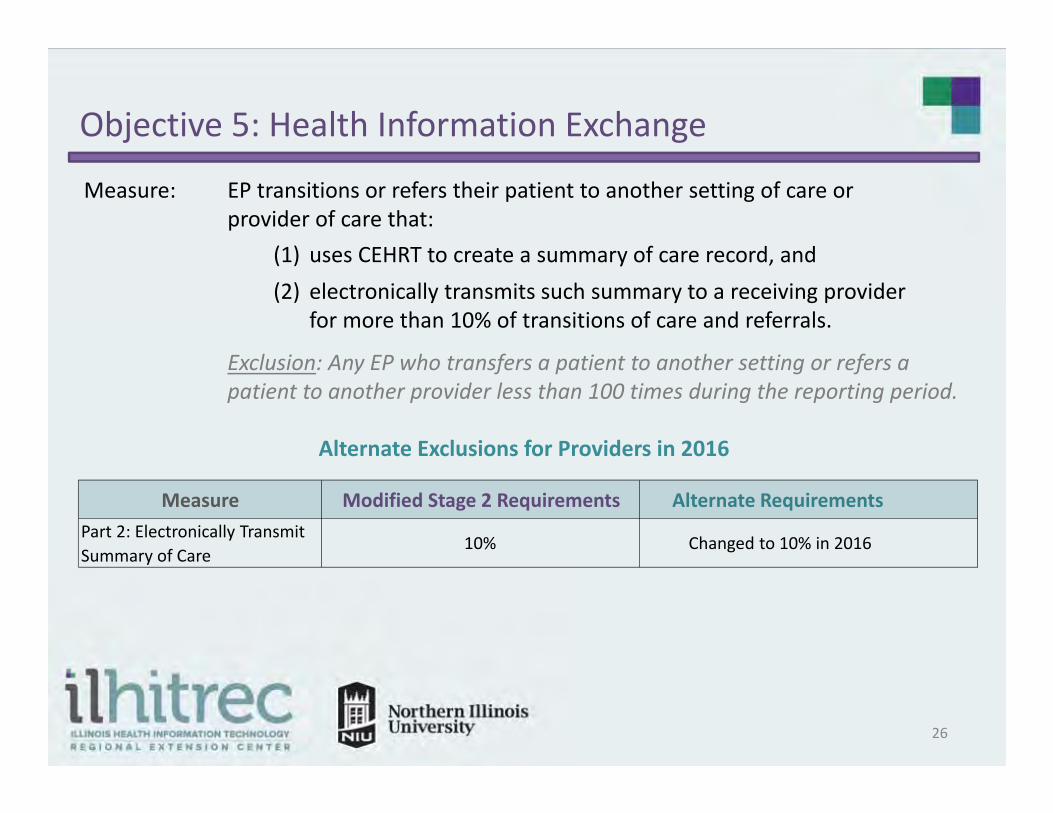
Objective 5: Health Information Exchange
Measure: EP transitions or refers their patient to another setting of care or provider of care that:
Exclusion: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100 times during the reporting period.
(1) uses CEHRT to create a summary of care record, and (2) electronically transmits such summary to a receiving provider
for more than 10% of transitions of care and referrals.
Alternate Exclusions for Providers in 2016
Measure Modified Stage 2 Requirements Alternate RequirementsPart 2: Electronically Transmit Summary of Care
10% Changed to 10% in 2016
26
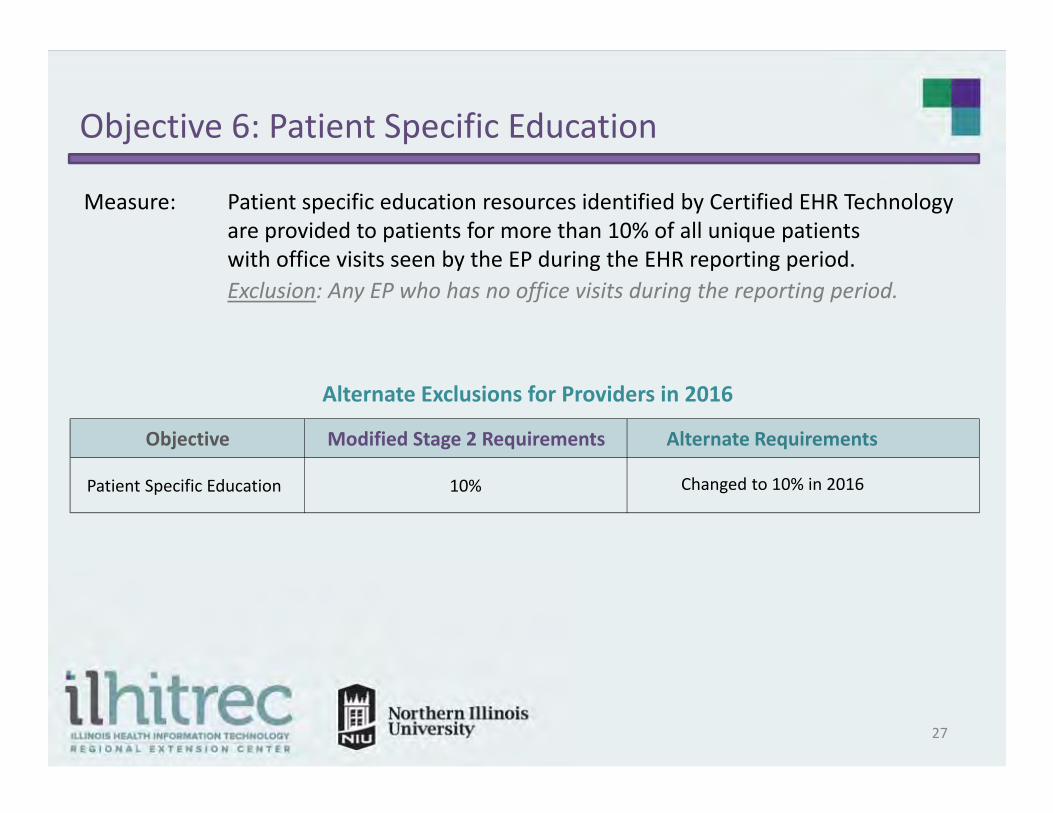
Objective 6: Patient Specific Education
Measure: Patient specific education resources identified by Certified EHR Technology are provided to patients for more than 10% of all unique patients with office visits seen by the EP during the EHR reporting period.Exclusion: Any EP who has no office visits during the reporting period.
Alternate Exclusions for Providers in 2016
Objective Modified Stage 2 Requirements Alternate Requirements
Patient Specific Education 10% Changed to 10% in 2016
27

Objective 7: Medication Reconciliation
Measure: EP performs medication reconciliation for more than 50% of transitions of care in which the patient is transitioned into the care of the EP.Exclusion: Any EP who was not the recipient of any transitions of care during the EHR reporting period.
Alternate Exclusions for Providers in 2016
Objective Modified Stage 2 Requirements Alternate Requirements
Medication Reconciliation 50% Changed to 50% in 2016
28
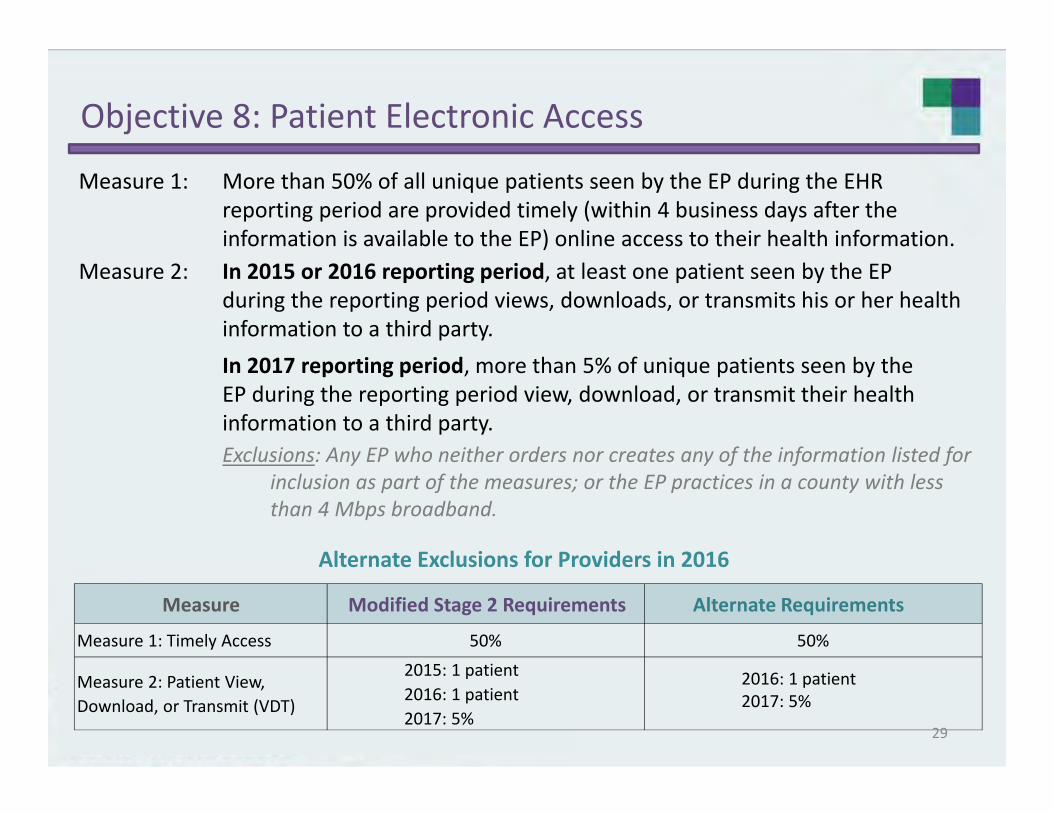
Objective 8: Patient Electronic Access
Measure 1: More than 50% of all unique patients seen by the EP during the EHR reporting period are provided timely (within 4 business days after the information is available to the EP) online access to their health information.
Measure 2: In 2015 or 2016 reporting period, at least one patient seen by the EP during the reporting period views, downloads, or transmits his or her health information to a third party.In 2017 reporting period, more than 5% of unique patients seen by the EP during the reporting period view, download, or transmit their health information to a third party.Exclusions: Any EP who neither orders nor creates any of the information listed for
inclusion as part of the measures; or the EP practices in a county with less than 4 Mbps broadband.
Alternate Exclusions for Providers in 2016
Measure Modified Stage 2 Requirements Alternate Requirements
Measure 1: Timely Access 50% 50%
Measure 2: Patient View, Download, or Transmit (VDT)
2015: 1 patient 2016: 1 patient2017: 5%
2016: 1 patient2017: 5%
29
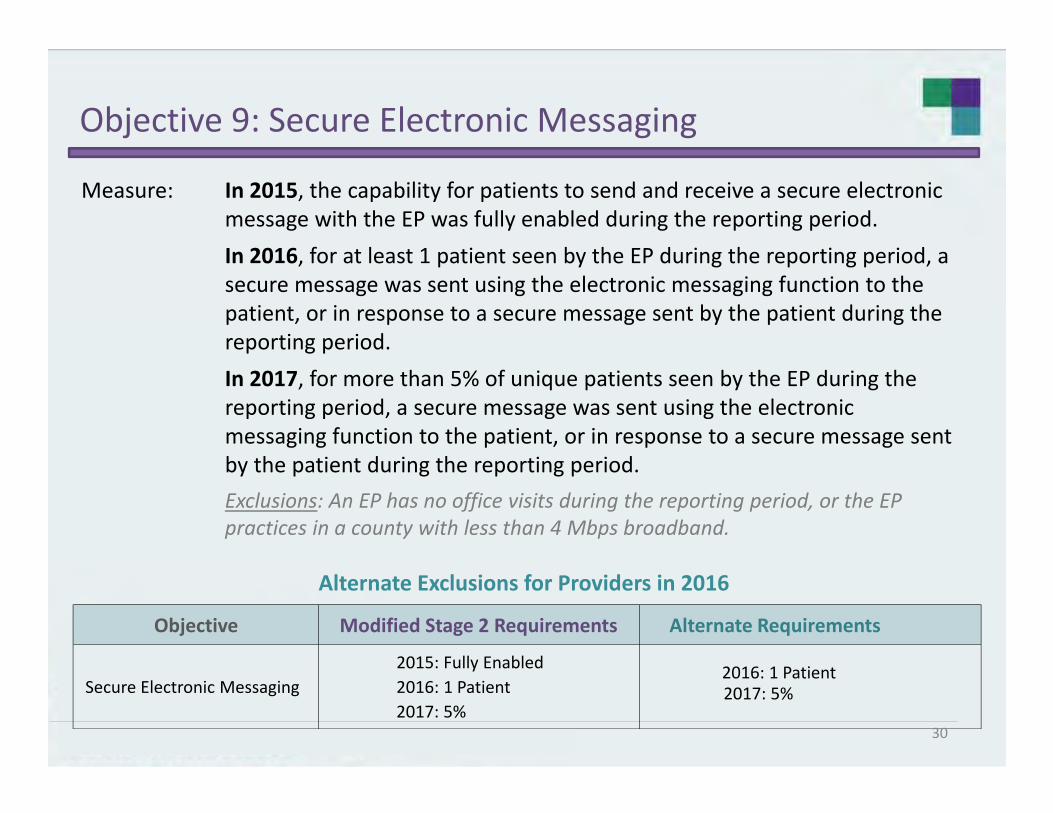
Objective 9: Secure Electronic Messaging
Measure: In 2015, the capability for patients to send and receive a secure electronic message with the EP was fully enabled during the reporting period.In 2016, for at least 1 patient seen by the EP during the reporting period, a secure message was sent using the electronic messaging function to the patient, or in response to a secure message sent by the patient during the reporting period.In 2017, for more than 5% of unique patients seen by the EP during the reporting period, a secure message was sent using the electronic messaging function to the patient, or in response to a secure message sent by the patient during the reporting period.Exclusions: An EP has no office visits during the reporting period, or the EP practices in a county with less than 4 Mbps broadband.
Alternate Exclusions for Providers in 2016
Objective Modified Stage 2 Requirements Alternate Requirements
Secure Electronic Messaging2015: Fully Enabled2016: 1 Patient2017: 5%
2016: 1 Patient2017: 5%
30
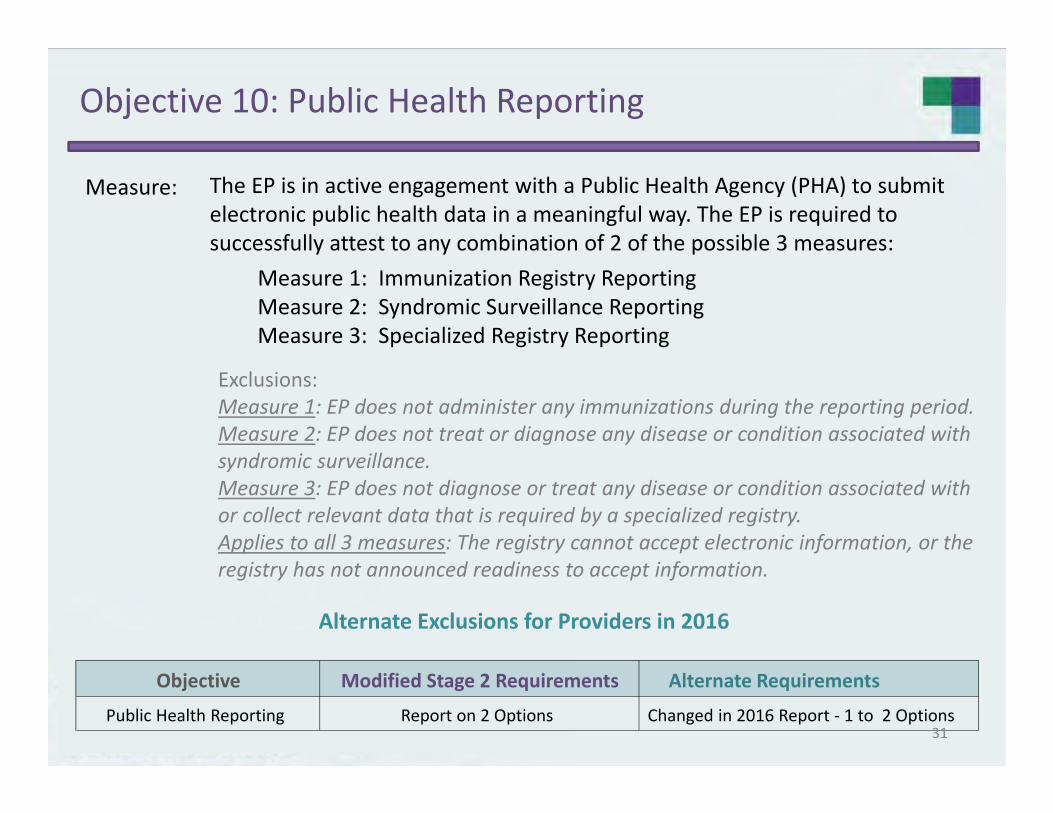
Objective 10: Public Health Reporting
Measure:
Alternate Exclusions for Providers in 2016
The EP is in active engagement with a Public Health Agency (PHA) to submit electronic public health data in a meaningful way. The EP is required to successfully attest to any combination of 2 of the possible 3 measures:
Measure 1: Immunization Registry ReportingMeasure 2: Syndromic Surveillance ReportingMeasure 3: Specialized Registry Reporting
Exclusions: Measure 1: EP does not administer any immunizations during the reporting period.Measure 2: EP does not treat or diagnose any disease or condition associated with syndromic surveillance. Measure 3: EP does not diagnose or treat any disease or condition associated with or collect relevant data that is required by a specialized registry.Applies to all 3 measures: The registry cannot accept electronic information, or the registry has not announced readiness to accept information.
Objective Modified Stage 2 Requirements Alternate Requirements
Public Health Reporting Report on 2 Options Changed in 2016 Report ‐ 1 to 2 Options31

Objective 10: Public Health Reporting
Measure 3:
Alternate Exclusions for Providers in 2016
Specialized Registry Reporting: There are no certification and standards criteria specified in the ONC 2014 Edition EHR Technology Criteria objective:To meet the measure, the EPs would need to electronically submit data specifications, and vocabularies required by the specialized registry. This is maintained by Public Health Agencies or other national organizations like the CDC/NCHS.
Potential Suggestions: Suggestion 1: Electronic submission to Prescription Drug Monitoring Program (PDMP)Suggestion 2: Illinois Cancer Registry if the provider treats or diagnoses cancer conditionsSuggestion 3: Electronic submissions to CDC/Nations Center for Health Statistics (NCHS) Specifically
The National Ambulatory Medical Care Survey.The National Hospital Medical Care Survey.
Suggestion 4: Professional Organizations EPs are members of and submit data to electronically.
CMS FAQ: https://questions.cms.gov/faq.php?faqId=11988
CMS: https://www.cms.gov/Medicare/Quality‐Initiatives‐Patient‐Assessment‐Instruments/PQRS/Downloads/2015QCDRPosting.pd
Objective Modified Stage 2 Requirements Alternate Requirements
Specialized Registry Reporting Report on 2 Options Changed in 2016 Report ‐ 1 to 2 Options32
Clinical Quality Measures
No changes to CQM selection or reporting scheme (EPs must report on 9 of the 64 approved CQMs)
For EHR reporting period in 2016 (and for providers participating for first time in 2016), providers attest to any continuous 90‐day period of CQM data
Registration and Attestation site – Providers also have option to electronically report CQM data using established methods for electronic reporting
For 2016 and subsequent years, providers beyond first year of Meaningful Use may attest to one full calendar year of CQM data or electronically report CQM data using established methods for electronic reporting outlined
33
Proposed Stage 3 Objectives for Eligible Providers
Objective 1: Protect Patient Health Information
Objective 2: Electronic Prescribing
Objective 3: Clinical Decision Support
Objective 4: Computerized Provider Order Entry
Objective 5: Patient Electronic Access to Health Information
Objective 6: Coordination of Care through Patient Engagement
Objective 7: Health Information Exchange
Objective 8: Public Health and Clinical Data Registry
34
PT1

Slide 34
PT1 Patty Tobin, 10/14/2015
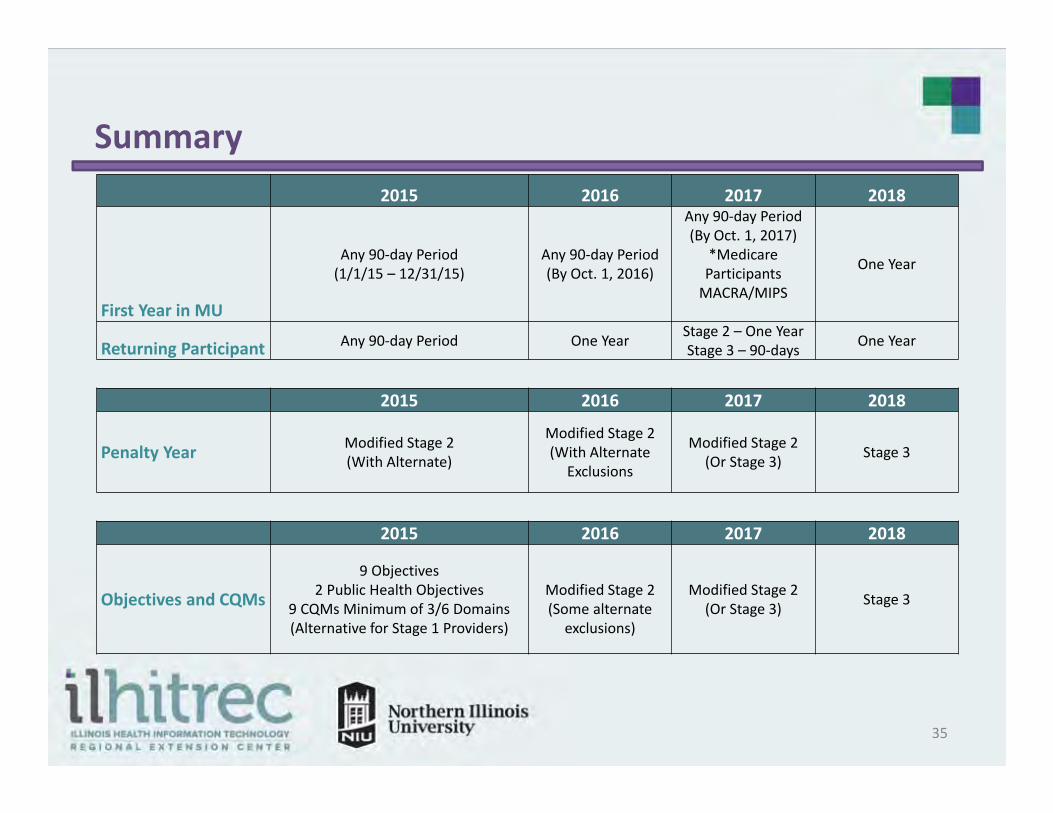
2015 2016 2017 2018
First Year in MU
Any 90‐day Period (1/1/15 – 12/31/15)
Any 90‐day Period(By Oct. 1, 2016)
Any 90‐day Period(By Oct. 1, 2017)
*MedicareParticipants MACRA/MIPS
One Year
Returning Participant Any 90‐day Period One Year Stage 2 – One YearStage 3 – 90‐days One Year
2015 2016 2017 2018
Penalty Year Modified Stage 2(With Alternate)
Modified Stage 2(With Alternate
Exclusions
Modified Stage 2(Or Stage 3) Stage 3
2015 2016 2017 2018
Objectives and CQMs
9 Objectives2 Public Health Objectives
9 CQMs Minimum of 3/6 Domains(Alternative for Stage 1 Providers)
Modified Stage 2(Some alternate
exclusions)
Modified Stage 2(Or Stage 3) Stage 3
Summary
35

36
HEALTH INFORMATION EXCHANGE
Another look at Objective 5
37

Objective 5: Health Information Exchange
Measure: EP transitions or refers their patient to another setting of care or provider of care that:
Exclusion: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100 times during the reporting period.
(1) uses CEHRT to create a summary of care record, and (2) electronically transmits such summary to a receiving provider
for more than 10% of transitions of care and referrals.
Alternate Exclusions for Providers in 2016
Measure Modified Stage 2 Requirements Alternate RequirementsPart 2: Electronically Transmit Summary of Care
10% Changed to 10% in 2016
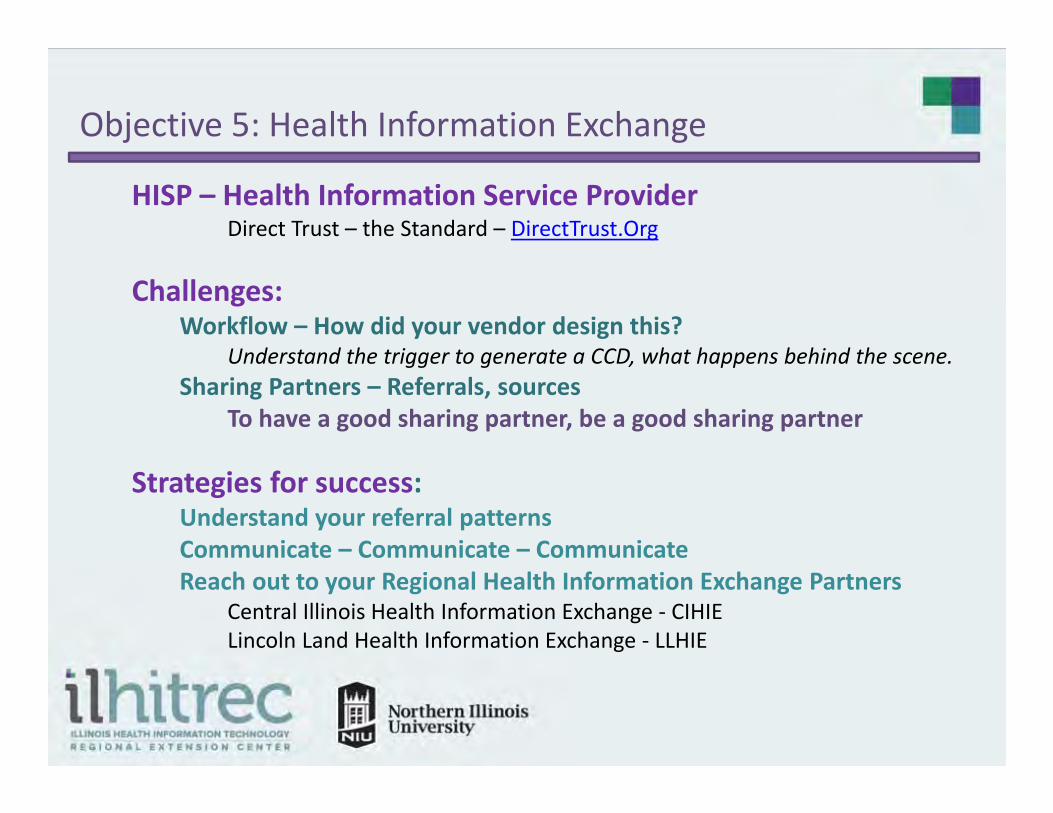
Objective 5: Health Information Exchange
HISP – Health Information Service ProviderDirect Trust – the Standard – DirectTrust.Org
Challenges:Workflow – How did your vendor design this?
Understand the trigger to generate a CCD, what happens behind the scene.Sharing Partners – Referrals, sources
To have a good sharing partner, be a good sharing partner
Strategies for success:Understand your referral patternsCommunicate – Communicate – CommunicateReach out to your Regional Health Information Exchange Partners
Central Illinois Health Information Exchange ‐ CIHIELincoln Land Health Information Exchange ‐ LLHIE
Additional References
Final Rule – Modification 2015 ‐2017 https://s3.amazonaws.com/public‐inspection.federalregister.gov/2015‐25595.pdf
CMS EHR Incentive Program https://www.cms.gov/Regulations‐and‐Guidance/Legislation/EHRIncentivePrograms/index.html
CMS FAQs https://www.cms.gov/Regulations‐and‐Guidance/Legislation/EHRIncentivePrograms/FAQ.html
2016 Requirements https://www.cms.gov/Regulations‐and‐
guidance/Legislation/EHRIncentivePrograms/2015ProgramRequirements.html
https://www.cms.gov/Regulations‐and‐Guidance/Legislation/EHRIncentivePrograms/Downloads/2016_EPMultipleLocations.pdf
IDPH Public Health Objectives https://murs.illinois.gov/
https://questions.cms.gov/faq.php?faqId=11988
https://www.cms.gov/Medicare/Quality‐Initiatives‐Patient‐Assessment‐instruments/PQRS/Downloads/2015QCDRPosting.pd
40
CMS Approved Specialty RegistriesThis is not an exhaustive listing
Vizient: Defined by CDC https://www.vizientinc.com/documents/Vizient_Specialized_Registry_2016.pdf
Pinnacle: Diabetes Collaborative Registry http://cvquality.acc.org/NCDR‐Home/Data‐Collection/How‐to‐Collect‐Data.aspx
Zirmed: Improve Population Health https://www.cms.gov/Medicare/Quality‐Initiatives‐Patient‐Assessment
Instruments/PQRS/Downloads/2016QualifiedRegistries.pdf
Dartnet: Clinical Quality Improvement Benchmarking System http://www.dartnet.info/PracticePerformanceRegistry.htm
CECity Genesis Registry: The American College of Physicians Genesis Registry
www.medconcert.com/genesis
Prescription Drug Monitor Program: (FAQ 11988) Illinois Does Have a Drug Monitoring Program Must submit electronically not just query
41

Questions?
Contact Information:
Brenda [email protected]
Kerri [email protected]
Lauren [email protected]
Othershttp://www.ILHITREC.org
[email protected](815) 753‐5900 42