module 11 hemiplegic shoulder 1
TRANSCRIPT
www.ebrsr.com
11. Painful Hemiplegic Shoulder Robert Teasell MD, Norine Foley MSc, Sanjit K. Bhogal MSc
Key Points Spasticity and hemiplegic shoulder pain are related. It is uncertain whether shoulder subluxation causes hemiplegic shoulder pain. It is uncertain if prolonged positioning or strapping helps to prevent or reduce hemiplegic shoulder pain. There is limited evidence that shoulder slings prevent the development of subluxation. Aggressive range of motion exercises (i.e. pullies) results in a markedly increased incidence of painful shoulder; a gentler range of motion program is preferred. Adding ultrasound treatments is not helpful while NSAIDs may be helpful. It is unclear whether injections with botulinum toxin reduce pain or improve passive range of motion. Corticosteroid injections do not appear to improve hemiplegic shoulder pain or range of motion.
The Evidence-Based Review of Stroke Rehabilitation (EBRSR) reviews current practices in stroke rehabilitation.
Contacts: EBRSR 801 Commissioners Road East
London, Ontario, Canada
N6C 5J1
Phone: 519.685.4000
Web: www.ebrsr.com
Functional electrical stimulation may help to reduce or prevent shoulder subluxation, but does not appear to reduce pain. Deinnervation of the subscapularis muscle may reduce shoulder pain and improve passive range of motion, more so than deinervation of the pectoralis major muscle. There is some evidence that alternative therapies such as massage, aromatherapy combined with acupressure can reduce shoulder pain. Oral corticosteroids appear to improve shoulder-hand syndrome for at least the first 4 weeks. Mirror therapy can reduce pain associated with shoulder hand syndrome.
Last updated July 2010
11. Painful Hemiplegic Shoulder pg. 1 of 65
www.ebrsr.com
Table of Contents Key Points .......................................................................................... 1
Table of Contents ................................................................................. 2
11. Painful Hemiplegic Shoulder.............................................................. 3
11.1 Incidence of Hemiplegic Shoulder Pain .......................................................3 11.1 Causes of Hemiplegic Shoulder Pain ..........................................................4 11.2 Shoulder Subluxation..............................................................................5
11.2.1 Pathophysiology................................................................................ 5 11.2.2 Scapular Rotation .............................................................................. 7 11.2.3 Pain in Shoulder Subluxation................................................................. 9
11.3 Spasticity, Contractures and Hemiplegic Shoulder Pain (HSP) .......................12 11.3.1 Spastic Muscle Imbalance .................................................................. 14 11.3.2 Frozen or Contracted Shoulder ............................................................ 16
11.4 Rotator Cuff Disorders..........................................................................18 11.5 Functional Impact of Painful Hemiplegic Shoulder ......................................18 11.6 Management of the Painful Hemiplegic Shoulder.........................................20
11.6.1 Positioning of the Hemiplegic Shoulder................................................... 21 11.6.2 Slings and Other Aids ....................................................................... 22 11.6.3 Strapping the Hemiplegic Shoulder ....................................................... 25 11.6.4 Active Therapies in the Hemiplegic Shoulder ............................................ 26 11.6.6 Electrical Stimulation in the Hemiplegic Shoulder ....................................... 28 11.6.7 Surgery as Treatment for Muscle Imbalance............................................. 35 11.6.8 Botulinum Toxin Injections as Treatment for HSP....................................... 35 11.6.9 Steroid Injections as Treatment for HSP.................................................. 38 11.6.10 Aromatherapy/Acupressure Treatment for Shoulder Pain............................ 41 11.6.11 Massage Therapy .......................................................................... 41 11.6.12 Subscapular Nerve Block for the Treatment for Shoulder Pain ...................... 42 11.6.13 Summary of the Management of Hemiplegic Shoulder ............................... 43
11.7 Complex Regional Pain Syndrome (CRPS) .................................................44 11.7.1 Stages and Symptoms of CRPS ........................................................... 44 11.7.2 Pathophysiology of CRPS .................................................................. 45 11.7.2 Incidence of CRPS........................................................................... 46 11.7.3 Diagnostic Tests of CRPS .................................................................. 49 11.7.4 Treatment of CRPS .......................................................................... 49 11.7.5 Pharmacological Treatment of CRPS .................................................... 50 11.7.6 Mirror Imagery as a Treatment for CRPS ................................................ 51 11.7.7 Passive Range of Motion Exercises for the Prevention of CRPS ..................... 53 11.7.8 Calcitonin for the Prevention of CRPS .................................................... 54
11.8 Summary............................................................................................56 References................................................................................................58
11. Painful Hemiplegic Shoulder pg. 2 of 65
www.ebrsr.com
11. Painful Hemiplegic Shoulder
11.1 Incidence of Hemiplegic Shoulder Pain Shoulder pain resulting from hemiplegia is a common clinical consequence of a focal cerebral insult resulting from a vascular lesion (ie. hemorrhagic or ischemic stroke). The incidence of shoulder pain varies between studies, with estimates which range from 48% to 84% (Najenson et al. 1971, Poulin de Courval et al. 1990). The results of several studies reporting on the incidence of HSP are presented in Table 11.1 Shoulder pain, by itself, can result in significant disability (Najenson et al. 1971, Poduri 1993) and although it can occur as early as 2 weeks post stroke, an onset time of 2-3 months post stroke is more typical (Poduri 1993). In a recent prospective study, Gamble et al. (2002) reported that 52/152 (34%) developed shoulder pain following stroke, 28% by two weeks and 87% by two months. By 6 months, the pain had resolved in 80% of the patients. Lindgren et al. (2007) reported that 74 (24%) of 305 patients with first ever stroke, who remained from an original cohort of 416 patients, experienced shoulder pain by month 16. Approximately half
of these patients developed pain between stroke onset and 4 months. Rajaratnam et al. (2007) identified three factors that predict, with 98% accuracy, the development of hemiplegic shoulder pain following acute stroke: a positive Neer test, moderate or greater shoulder pain during the performance of the hand behind the neck manoeuvre and a difference of greater than 10 degrees of passive external rotation at the shoulder joint. Depression, reduction to light touch and reduction to temperature sensation have also been associated with shoulder pain (Gamble et al. 2000). Shoulder pain can negatively affect rehabilitation outcomes as good shoulder function is a prerequisite for successful transfers, maintaining balance, performing activities of daily living and for effective hand function (Risk et al. 1984). Lo et al. (2005) catalogued the different types of shoulder dysfunction based on both clinical and arthrographic findings and reported that 16% of patients of a cohort of 32 patients with hemiplegic shoulder pain within one-year of stroke had shoulder-hand syndrome, 4% had rotator cuff tears and 50% suffered from frozen shoulder. 63% of patients had a single type of shoulder dysfunction while 34% had two types.
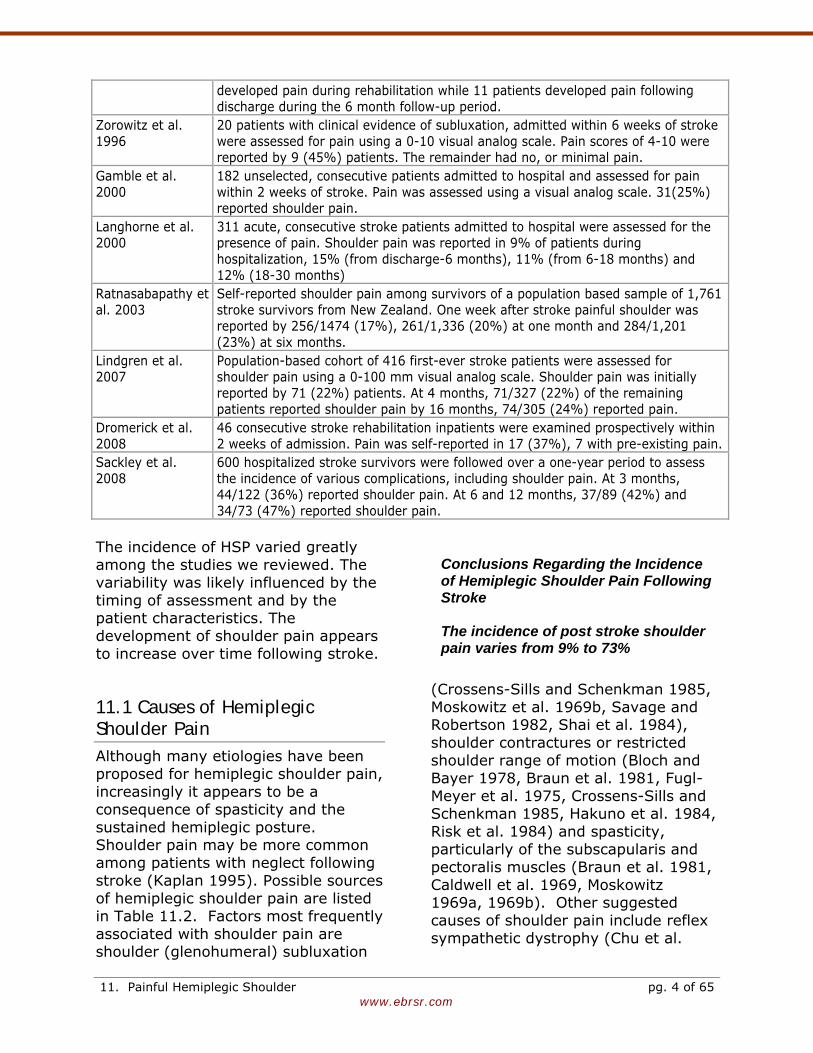
Table 11.1 Incidence of Hemiplegic Shoulder Pain Author, Year Incidence Bohannon et al. 1986
The charts of 50 patients with hemiplegia secondary to stroke admitted for inpatient rehabilitation were reviewed. Pain, assessed during passive shoulder external rotation, was reported by 36 (73%) patients
Van Ouwemaller et al. 1986
219 stroke patients initially hospitalized for stroke were assessed and followed up for an average of 11 months, were studied. 157 (72%) reported experiencing shoulder pain on at least one occasion during the study period.
Jesperson et al. 1995
Retrospective chart review of 173 admissions for inpatient stroke rehabilitation. Self-reported shoulder pain was reported by 38 (22%) patients. 27 patients
11. Painful Hemiplegic Shoulder pg. 3 of 65
www.ebrsr.com
developed pain during rehabilitation while 11 patients developed pain following discharge during the 6 month follow-up period.
Zorowitz et al. 1996
20 patients with clinical evidence of subluxation, admitted within 6 weeks of stroke were assessed for pain using a 0-10 visual analog scale. Pain scores of 4-10 were reported by 9 (45%) patients. The remainder had no, or minimal pain.
Gamble et al. 2000
182 unselected, consecutive patients admitted to hospital and assessed for pain within 2 weeks of stroke. Pain was assessed using a visual analog scale. 31(25%) reported shoulder pain.
Langhorne et al. 2000
311 acute, consecutive stroke patients admitted to hospital were assessed for the presence of pain. Shoulder pain was reported in 9% of patients during hospitalization, 15% (from discharge-6 months), 11% (from 6-18 months) and 12% (18-30 months)
Ratnasabapathy et al. 2003
Self-reported shoulder pain among survivors of a population based sample of 1,761 stroke survivors from New Zealand. One week after stroke painful shoulder was reported by 256/1474 (17%), 261/1,336 (20%) at one month and 284/1,201 (23%) at six months.
Lindgren et al. 2007
Population-based cohort of 416 first-ever stroke patients were assessed for shoulder pain using a 0-100 mm visual analog scale. Shoulder pain was initially reported by 71 (22%) patients. At 4 months, 71/327 (22%) of the remaining patients reported shoulder pain by 16 months, 74/305 (24%) reported pain.
Dromerick et al. 2008
46 consecutive stroke rehabilitation inpatients were examined prospectively within 2 weeks of admission. Pain was self-reported in 17 (37%), 7 with pre-existing pain.
Sackley et al. 2008
600 hospitalized stroke survivors were followed over a one-year period to assess the incidence of various complications, including shoulder pain. At 3 months, 44/122 (36%) reported shoulder pain. At 6 and 12 months, 37/89 (42%) and 34/73 (47%) reported shoulder pain.
The incidence of HSP varied greatly among the studies we reviewed. The variability was likely influenced by the timing of assessment and by the patient characteristics. The development of shoulder pain appears to increase over time following stroke.
Conclusions Regarding the Incidence of Hemiplegic Shoulder Pain Following Stroke The incidence of post stroke shoulder pain varies from 9% to 73%
11.1 Causes of Hemiplegic Shoulder Pain Although many etiologies have been proposed for hemiplegic shoulder pain, increasingly it appears to be a consequence of spasticity and the sustained hemiplegic posture. Shoulder pain may be more common among patients with neglect following stroke (Kaplan 1995). Possible sources of hemiplegic shoulder pain are listed in Table 11.2. Factors most frequently associated with shoulder pain are shoulder (glenohumeral) subluxation
(Crossens-Sills and Schenkman 1985, Moskowitz et al. 1969b, Savage and Robertson 1982, Shai et al. 1984), shoulder contractures or restricted shoulder range of motion (Bloch and Bayer 1978, Braun et al. 1981, Fugl-Meyer et al. 1975, Crossens-Sills and Schenkman 1985, Hakuno et al. 1984, Risk et al. 1984) and spasticity, particularly of the subscapularis and pectoralis muscles (Braun et al. 1981, Caldwell et al. 1969, Moskowitz 1969a, 1969b). Other suggested causes of shoulder pain include reflex sympathetic dystrophy (Chu et al.
11. Painful Hemiplegic Shoulder pg. 4 of 65
www.ebrsr.com
1981, Davis et al. 1977, Perrigot et al. 1975), or injury to the rotator cuff musculotendinous unit (Najenson et al. 1971, Nepomuceno et al. 1974). The role of central post stroke pain in the etiology of shoulder pain is unclear (Walsh 2001). In a recent study, the first of its kind, MRI was used to examine a potential association between structural changes in hemiplegic shoulder and pain (Shah et al. 2008). In a series of 89 patients with shoulder pain, 35% of subjects exhibited a tear of at least one rotator cuff, biceps or deltoid muscle and 53% exhibited tendinopathy of at least one rotator cuff, bicep or deltoid muscle, rotator cuff tears and rotator cuff and deltoid tendinopathies. These changes were not related to severity of shoulder pain.
11.2 Shoulder Subluxation
11.2.1 Pathophysiology Shoulder subluxation is best defined as changes in the mechanical integrity of the glenohumeral joint causing a palpable gap between the acromion and humeral head. The most reliable clinical measurement of the subacromial space used in clinical research is calipers (Boyd 1992). The glenohumeral joint is multiaxial and has a range of motion, which exceeds that of other joints in the body. To achieve this mobility the glenohumeral joint must sacrifice stability. Stability is achieved through the rotator cuff, a musculotendinous sleeve which maintains the humeral head in the glenoid fossa, while at the same time allowing shoulder mobility. During the initial period following a stroke the hemiplegic arm is flaccid or hypotonic. Therefore the shoulder musculature, in particular the rotator cuff musculotendinous sleeve, cannot perform its function of maintaining the humeral head in the glenoid fossa and there is a high risk of shoulder subluxation.
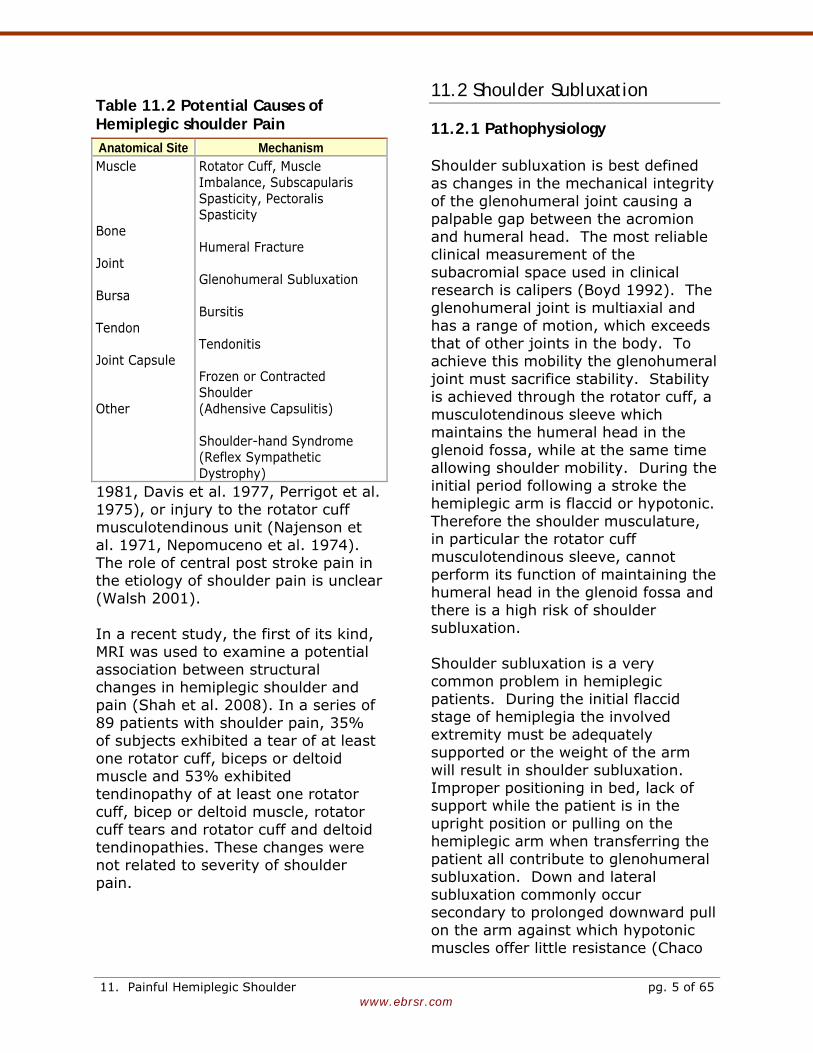
Table 11.2 Potential Causes of Hemiplegic shoulder Pain Anatomical Site Mechanism Muscle Bone Joint Bursa Tendon Joint Capsule Other
Rotator Cuff, Muscle Imbalance, Subscapularis Spasticity, Pectoralis Spasticity Humeral Fracture Glenohumeral Subluxation Bursitis Tendonitis Frozen or Contracted Shoulder (Adhensive Capsulitis) Shoulder-hand Syndrome (Reflex Sympathetic Dystrophy)
Shoulder subluxation is a very common problem in hemiplegic patients. During the initial flaccid stage of hemiplegia the involved extremity must be adequately supported or the weight of the arm will result in shoulder subluxation. Improper positioning in bed, lack of support while the patient is in the upright position or pulling on the hemiplegic arm when transferring the patient all contribute to glenohumeral subluxation. Down and lateral subluxation commonly occur secondary to prolonged downward pull on the arm against which hypotonic muscles offer little resistance (Chaco
11. Painful Hemiplegic Shoulder pg. 5 of 65
www.ebrsr.com
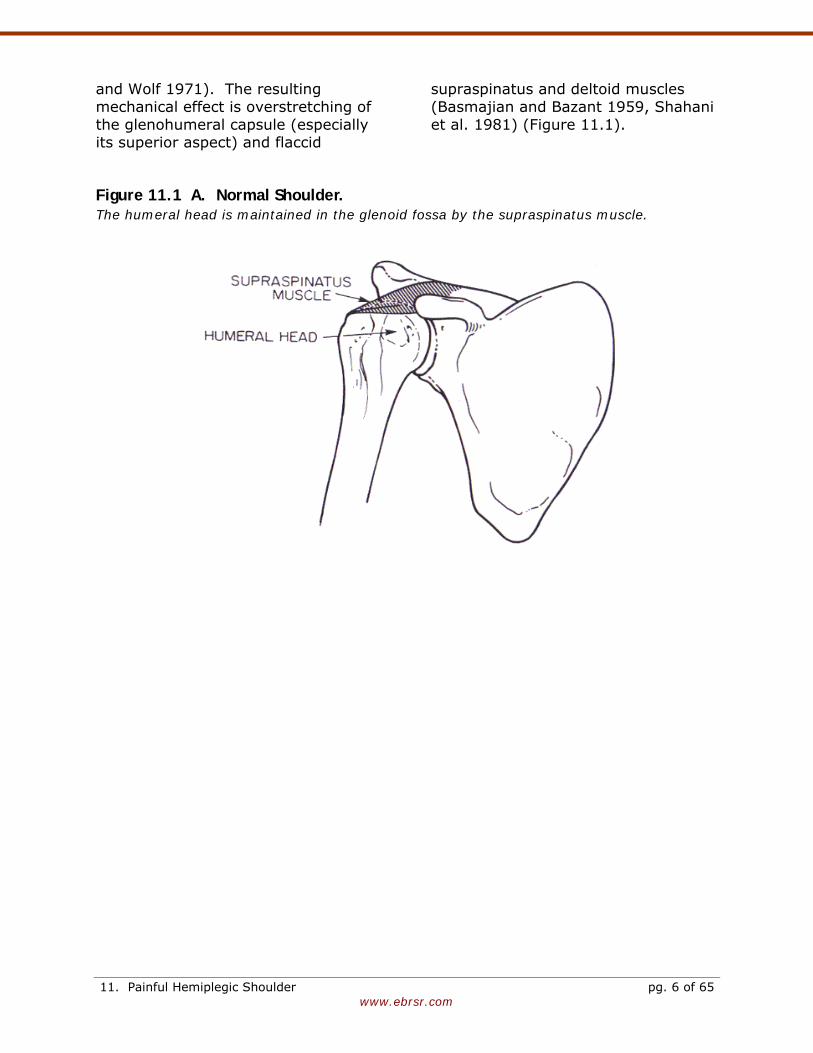
and Wolf 1971). The resulting mechanical effect is overstretching of the glenohumeral capsule (especially its superior aspect) and flaccid
supraspinatus and deltoid muscles (Basmajian and Bazant 1959, Shahani et al. 1981) (Figure 11.1).
Figure 11.1 A. Normal Shoulder. The humeral head is maintained in the glenoid fossa by the supraspinatus muscle.
11. Painful Hemiplegic Shoulder pg. 6 of 65
www.ebrsr.com
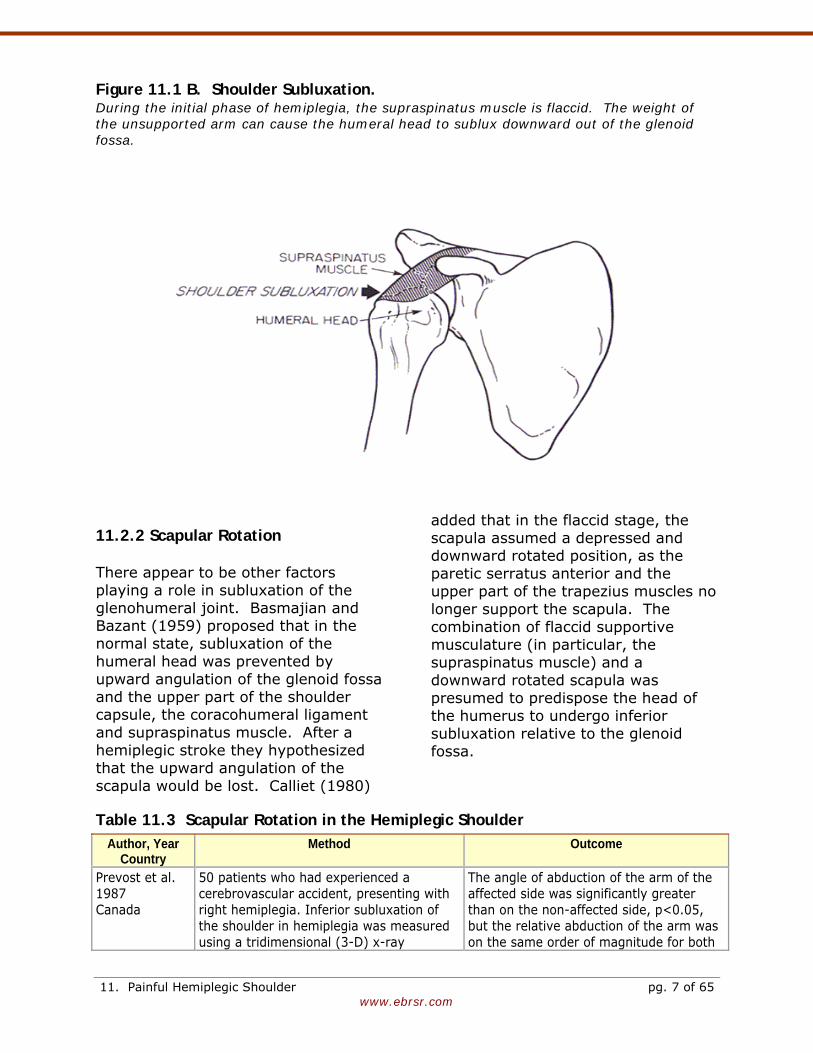
Figure 11.1 B. Shoulder Subluxation. During the initial phase of hemiplegia, the supraspinatus muscle is flaccid. The weight of the unsupported arm can cause the humeral head to sublux downward out of the glenoid fossa.
11.2.2 Scapular Rotation There appear to be other factors playing a role in subluxation of the glenohumeral joint. Basmajian and Bazant (1959) proposed that in the normal state, subluxation of the humeral head was prevented by upward angulation of the glenoid fossa and the upper part of the shoulder capsule, the coracohumeral ligament and supraspinatus muscle. After a hemiplegic stroke they hypothesized that the upward angulation of the scapula would be lost. Calliet (1980)
added that in the flaccid stage, the scapula assumed a depressed and downward rotated position, as the paretic serratus anterior and the upper part of the trapezius muscles no longer support the scapula. The combination of flaccid supportive musculature (in particular, the supraspinatus muscle) and a downward rotated scapula was presumed to predispose the head of the humerus to undergo inferior subluxation relative to the glenoid fossa.
Table 11.3 Scapular Rotation in the Hemiplegic Shoulder Author, Year
Country Method Outcome
Prevost et al. 1987 Canada
50 patients who had experienced a cerebrovascular accident, presenting with right hemiplegia. Inferior subluxation of the shoulder in hemiplegia was measured using a tridimensional (3-D) x-ray
The angle of abduction of the arm of the affected side was significantly greater than on the non-affected side, p<0.05, but the relative abduction of the arm was on the same order of magnitude for both
11. Painful Hemiplegic Shoulder pg. 7 of 65
www.ebrsr.com
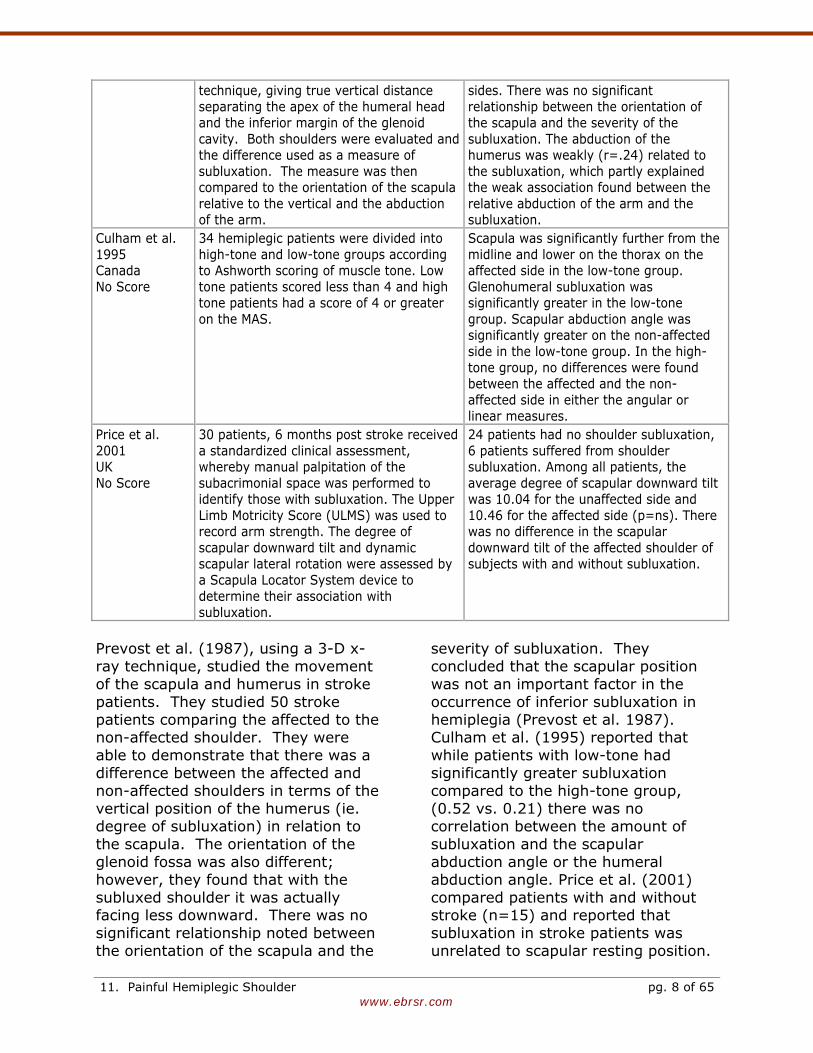
technique, giving true vertical distance separating the apex of the humeral head and the inferior margin of the glenoid cavity. Both shoulders were evaluated and the difference used as a measure of subluxation. The measure was then compared to the orientation of the scapula relative to the vertical and the abduction of the arm.
sides. There was no significant relationship between the orientation of the scapula and the severity of the subluxation. The abduction of the humerus was weakly (r=.24) related to the subluxation, which partly explained the weak association found between the relative abduction of the arm and the subluxation.
Culham et al. 1995 Canada No Score
34 hemiplegic patients were divided into high-tone and low-tone groups according to Ashworth scoring of muscle tone. Low tone patients scored less than 4 and high tone patients had a score of 4 or greater on the MAS.
Scapula was significantly further from the midline and lower on the thorax on the affected side in the low-tone group. Glenohumeral subluxation was significantly greater in the low-tone group. Scapular abduction angle was significantly greater on the non-affected side in the low-tone group. In the high-tone group, no differences were found between the affected and the non-affected side in either the angular or linear measures.
Price et al. 2001 UK No Score
30 patients, 6 months post stroke received a standardized clinical assessment, whereby manual palpitation of the subacrimonial space was performed to identify those with subluxation. The Upper Limb Motricity Score (ULMS) was used to record arm strength. The degree of scapular downward tilt and dynamic scapular lateral rotation were assessed by a Scapula Locator System device to determine their association with subluxation.
24 patients had no shoulder subluxation, 6 patients suffered from shoulder subluxation. Among all patients, the average degree of scapular downward tilt was 10.04 for the unaffected side and 10.46 for the affected side (p=ns). There was no difference in the scapular downward tilt of the affected shoulder of subjects with and without subluxation.
Prevost et al. (1987), using a 3-D x-ray technique, studied the movement of the scapula and humerus in stroke patients. They studied 50 stroke patients comparing the affected to the non-affected shoulder. They were able to demonstrate that there was a difference between the affected and non-affected shoulders in terms of the vertical position of the humerus (ie. degree of subluxation) in relation to the scapula. The orientation of the glenoid fossa was also different; however, they found that with the subluxed shoulder it was actually facing less downward. There was no significant relationship noted between the orientation of the scapula and the
severity of subluxation. They concluded that the scapular position was not an important factor in the occurrence of inferior subluxation in hemiplegia (Prevost et al. 1987). Culham et al. (1995) reported that while patients with low-tone had significantly greater subluxation compared to the high-tone group, (0.52 vs. 0.21) there was no correlation between the amount of subluxation and the scapular abduction angle or the humeral abduction angle. Price et al. (2001) compared patients with and without stroke (n=15) and reported that subluxation in stroke patients was unrelated to scapular resting position.
11. Painful Hemiplegic Shoulder pg. 8 of 65
www.ebrsr.com
These authors also reported that the normal scapula tilts downward to a greater degree found in other studies.
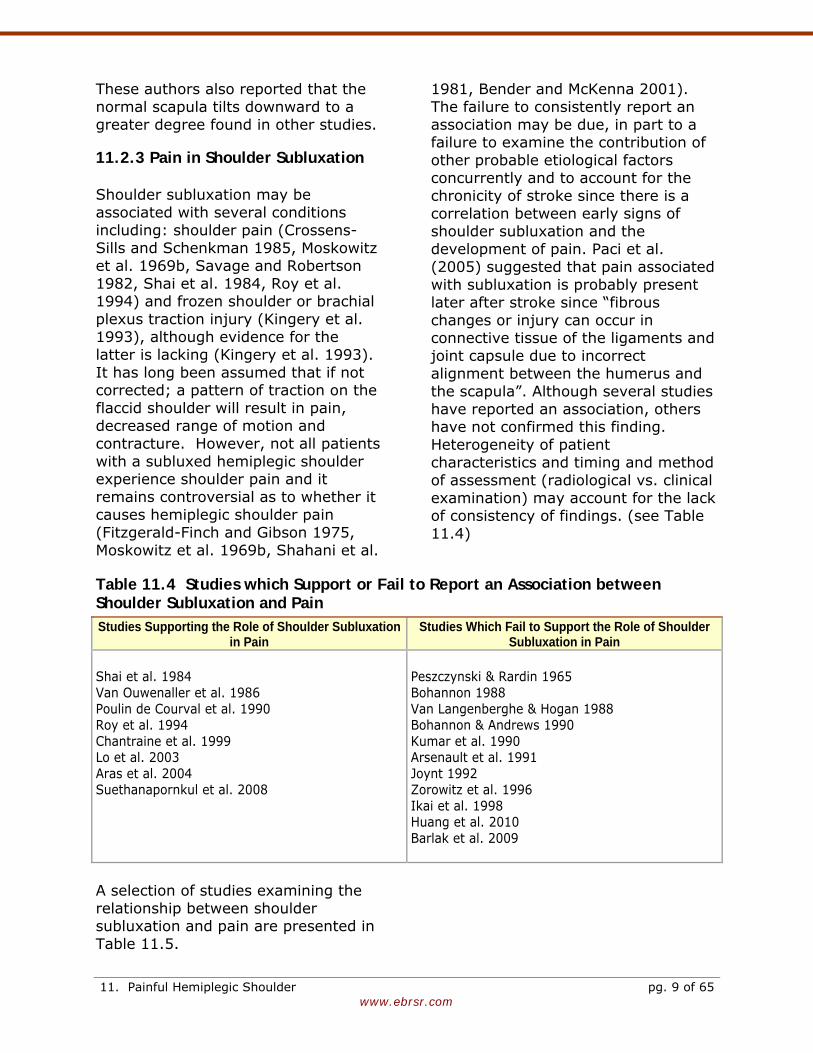
11.2.3 Pain in Shoulder Subluxation Shoulder subluxation may be associated with several conditions including: shoulder pain (Crossens-Sills and Schenkman 1985, Moskowitz et al. 1969b, Savage and Robertson 1982, Shai et al. 1984, Roy et al. 1994) and frozen shoulder or brachial plexus traction injury (Kingery et al. 1993), although evidence for the latter is lacking (Kingery et al. 1993). It has long been assumed that if not corrected; a pattern of traction on the flaccid shoulder will result in pain, decreased range of motion and contracture. However, not all patients with a subluxed hemiplegic shoulder experience shoulder pain and it remains controversial as to whether it causes hemiplegic shoulder pain (Fitzgerald-Finch and Gibson 1975, Moskowitz et al. 1969b, Shahani et al.
1981, Bender and McKenna 2001). The failure to consistently report an association may be due, in part to a failure to examine the contribution of other probable etiological factors concurrently and to account for the chronicity of stroke since there is a correlation between early signs of shoulder subluxation and the development of pain. Paci et al. (2005) suggested that pain associated with subluxation is probably present later after stroke since “fibrous changes or injury can occur in connective tissue of the ligaments and joint capsule due to incorrect alignment between the humerus and the scapula”. Although several studies have reported an association, others have not confirmed this finding. Heterogeneity of patient characteristics and timing and method of assessment (radiological vs. clinical examination) may account for the lack of consistency of findings. (see Table 11.4)
Table 11.4 Studies which Support or Fail to Report an Association between Shoulder Subluxation and Pain Studies Supporting the Role of Shoulder Subluxation
in Pain Studies Which Fail to Support the Role of Shoulder
Subluxation in Pain Shai et al. 1984 Van Ouwenaller et al. 1986 Poulin de Courval et al. 1990 Roy et al. 1994 Chantraine et al. 1999 Lo et al. 2003 Aras et al. 2004 Suethanapornkul et al. 2008
Peszczynski & Rardin 1965 Bohannon 1988 Van Langenberghe & Hogan 1988 Bohannon & Andrews 1990 Kumar et al. 1990 Arsenault et al. 1991 Joynt 1992 Zorowitz et al. 1996 Ikai et al. 1998 Huang et al. 2010 Barlak et al. 2009
A selection of studies examining the relationship between shoulder subluxation and pain are presented in Table 11.5.
11. Painful Hemiplegic Shoulder pg. 9 of 65
www.ebrsr.com
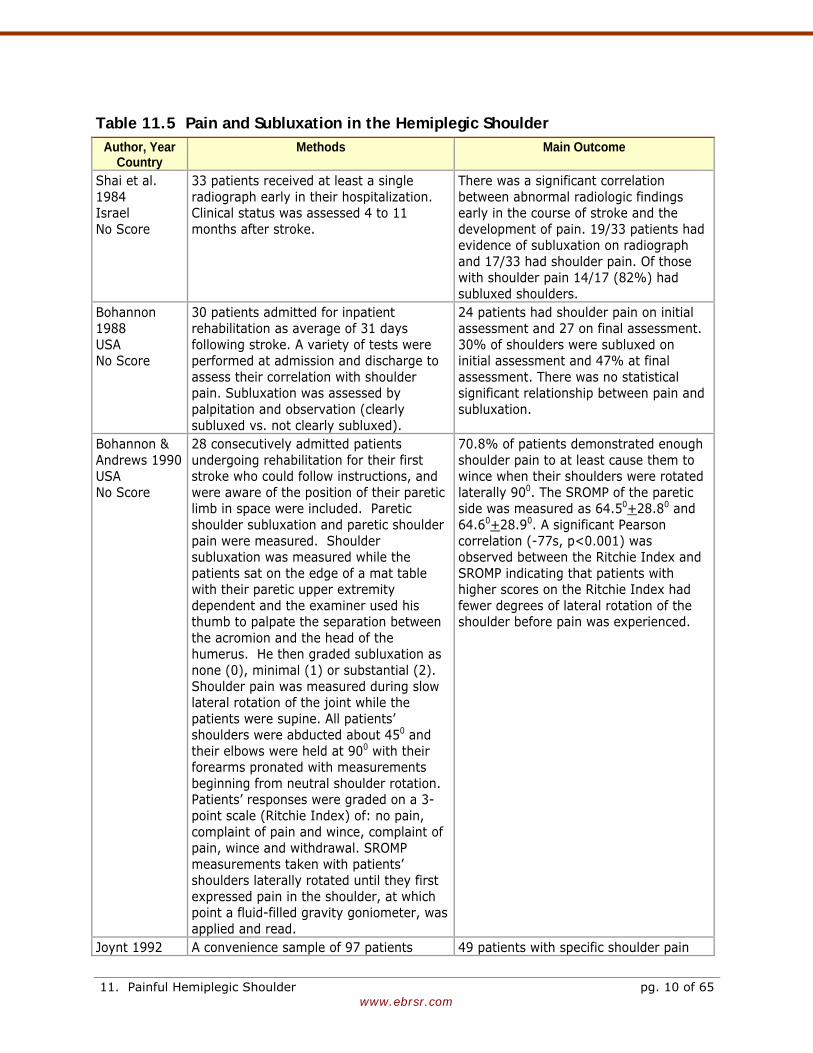
Table 11.5 Pain and Subluxation in the Hemiplegic Shoulder Author, Year
Country Methods Main Outcome
Shai et al. 1984 Israel No Score
33 patients received at least a single radiograph early in their hospitalization. Clinical status was assessed 4 to 11 months after stroke.
There was a significant correlation between abnormal radiologic findings early in the course of stroke and the development of pain. 19/33 patients had evidence of subluxation on radiograph and 17/33 had shoulder pain. Of those with shoulder pain 14/17 (82%) had subluxed shoulders.
Bohannon 1988 USA No Score
30 patients admitted for inpatient rehabilitation as average of 31 days following stroke. A variety of tests were performed at admission and discharge to assess their correlation with shoulder pain. Subluxation was assessed by palpitation and observation (clearly subluxed vs. not clearly subluxed).
24 patients had shoulder pain on initial assessment and 27 on final assessment. 30% of shoulders were subluxed on initial assessment and 47% at final assessment. There was no statistical significant relationship between pain and subluxation.
Bohannon & Andrews 1990 USA No Score
28 consecutively admitted patients undergoing rehabilitation for their first stroke who could follow instructions, and were aware of the position of their paretic limb in space were included. Paretic shoulder subluxation and paretic shoulder pain were measured. Shoulder subluxation was measured while the patients sat on the edge of a mat table with their paretic upper extremity dependent and the examiner used his thumb to palpate the separation between the acromion and the head of the humerus. He then graded subluxation as none (0), minimal (1) or substantial (2). Shoulder pain was measured during slow lateral rotation of the joint while the patients were supine. All patients’ shoulders were abducted about 450 and their elbows were held at 900 with their forearms pronated with measurements beginning from neutral shoulder rotation. Patients’ responses were graded on a 3-point scale (Ritchie Index) of: no pain, complaint of pain and wince, complaint of pain, wince and withdrawal. SROMP measurements taken with patients’ shoulders laterally rotated until they first expressed pain in the shoulder, at which point a fluid-filled gravity goniometer, was applied and read.
70.8% of patients demonstrated enough shoulder pain to at least cause them to wince when their shoulders were rotated laterally 900. The SROMP of the paretic side was measured as 64.50+28.80 and 64.60+28.90. A significant Pearson correlation (-77s, p<0.001) was observed between the Ritchie Index and SROMP indicating that patients with higher scores on the Ritchie Index had fewer degrees of lateral rotation of the shoulder before pain was experienced.
Joynt 1992 A convenience sample of 97 patients 49 patients with specific shoulder pain
11. Painful Hemiplegic Shoulder pg. 10 of 65
www.ebrsr.com
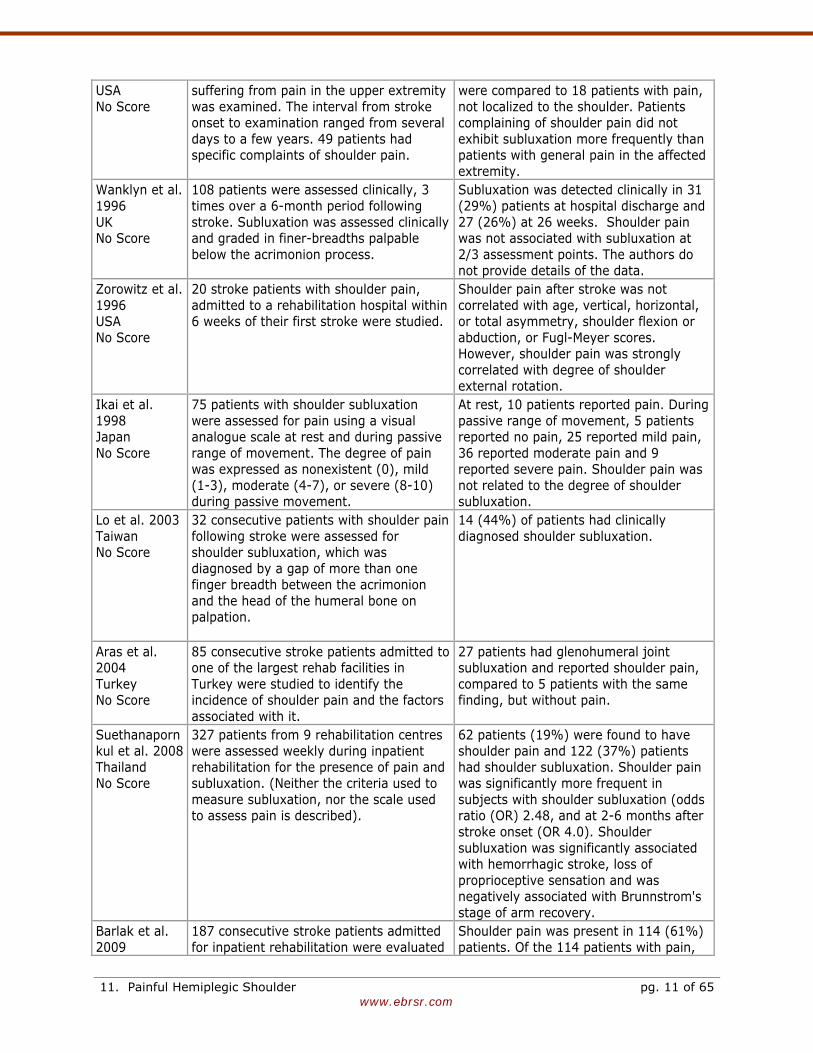
USA No Score
suffering from pain in the upper extremity was examined. The interval from stroke onset to examination ranged from several days to a few years. 49 patients had specific complaints of shoulder pain.
were compared to 18 patients with pain, not localized to the shoulder. Patients complaining of shoulder pain did not exhibit subluxation more frequently than patients with general pain in the affected extremity.
Wanklyn et al. 1996 UK No Score
108 patients were assessed clinically, 3 times over a 6-month period following stroke. Subluxation was assessed clinically and graded in finer-breadths palpable below the acrimonion process.
Subluxation was detected clinically in 31 (29%) patients at hospital discharge and 27 (26%) at 26 weeks. Shoulder pain was not associated with subluxation at 2/3 assessment points. The authors do not provide details of the data.
Zorowitz et al. 1996 USA No Score
20 stroke patients with shoulder pain, admitted to a rehabilitation hospital within 6 weeks of their first stroke were studied.
Shoulder pain after stroke was not correlated with age, vertical, horizontal, or total asymmetry, shoulder flexion or abduction, or Fugl-Meyer scores. However, shoulder pain was strongly correlated with degree of shoulder external rotation.
Ikai et al. 1998 Japan No Score
75 patients with shoulder subluxation were assessed for pain using a visual analogue scale at rest and during passive range of movement. The degree of pain was expressed as nonexistent (0), mild (1-3), moderate (4-7), or severe (8-10) during passive movement.
At rest, 10 patients reported pain. During passive range of movement, 5 patients reported no pain, 25 reported mild pain, 36 reported moderate pain and 9 reported severe pain. Shoulder pain was not related to the degree of shoulder subluxation.
Lo et al. 2003 Taiwan No Score
32 consecutive patients with shoulder pain following stroke were assessed for shoulder subluxation, which was diagnosed by a gap of more than one finger breadth between the acrimonion and the head of the humeral bone on palpation.
14 (44%) of patients had clinically diagnosed shoulder subluxation.
Aras et al. 2004 Turkey No Score
85 consecutive stroke patients admitted to one of the largest rehab facilities in Turkey were studied to identify the incidence of shoulder pain and the factors associated with it.
27 patients had glenohumeral joint subluxation and reported shoulder pain, compared to 5 patients with the same finding, but without pain.
Suethanapornkul et al. 2008 Thailand No Score
327 patients from 9 rehabilitation centres were assessed weekly during inpatient rehabilitation for the presence of pain and subluxation. (Neither the criteria used to measure subluxation, nor the scale used to assess pain is described).
62 patients (19%) were found to have shoulder pain and 122 (37%) patients had shoulder subluxation. Shoulder pain was significantly more frequent in subjects with shoulder subluxation (odds ratio (OR) 2.48, and at 2-6 months after stroke onset (OR 4.0). Shoulder subluxation was significantly associated with hemorrhagic stroke, loss of proprioceptive sensation and was negatively associated with Brunnstrom's stage of arm recovery.
Barlak et al. 2009
187 consecutive stroke patients admitted for inpatient rehabilitation were evaluated
Shoulder pain was present in 114 (61%) patients. Of the 114 patients with pain,
11. Painful Hemiplegic Shoulder pg. 11 of 65
www.ebrsr.com
Turkey No Score
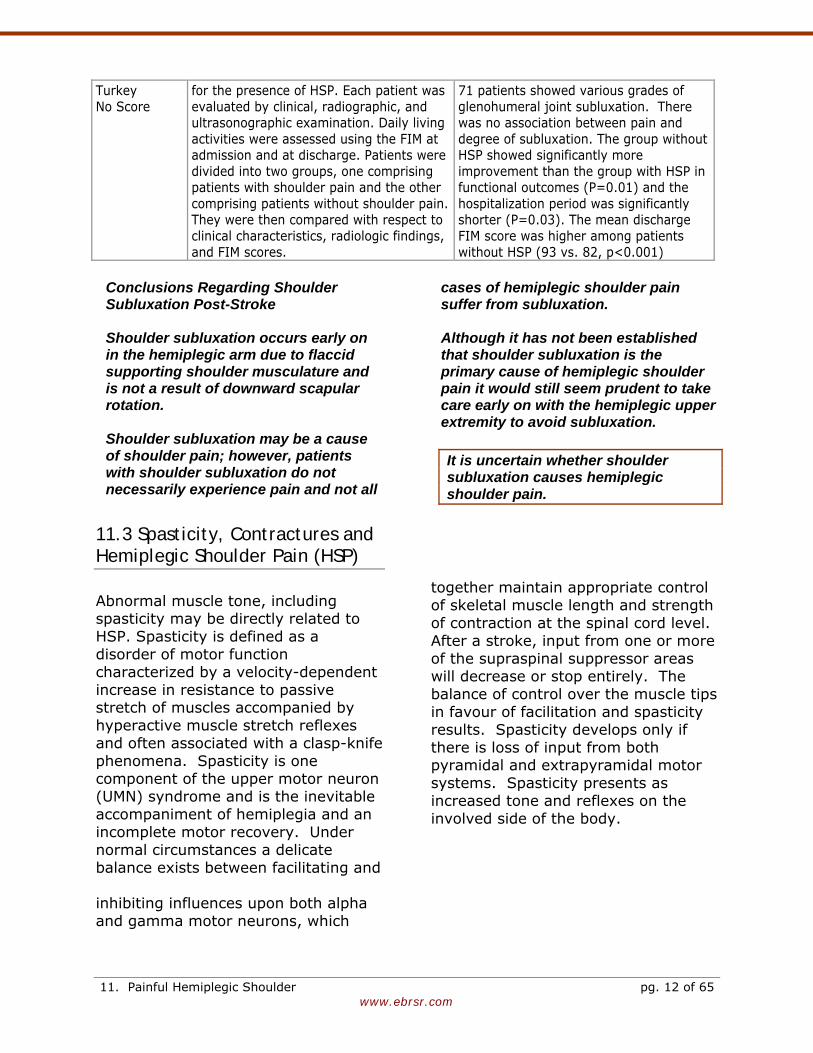
for the presence of HSP. Each patient was evaluated by clinical, radiographic, and ultrasonographic examination. Daily living activities were assessed using the FIM at admission and at discharge. Patients were divided into two groups, one comprising patients with shoulder pain and the other comprising patients without shoulder pain. They were then compared with respect to clinical characteristics, radiologic findings, and FIM scores.
71 patients showed various grades of glenohumeral joint subluxation. There was no association between pain and degree of subluxation. The group without HSP showed significantly more improvement than the group with HSP in functional outcomes (P=0.01) and the hospitalization period was significantly shorter (P=0.03). The mean discharge FIM score was higher among patients without HSP (93 vs. 82, p<0.001)
Conclusions Regarding Shoulder Subluxation Post-Stroke Shoulder subluxation occurs early on in the hemiplegic arm due to flaccid supporting shoulder musculature and is not a result of downward scapular rotation. Shoulder subluxation may be a cause of shoulder pain; however, patients with shoulder subluxation do not necessarily experience pain and not all
cases of hemiplegic shoulder pain suffer from subluxation. Although it has not been established that shoulder subluxation is the primary cause of hemiplegic shoulder pain it would still seem prudent to take care early on with the hemiplegic upper extremity to avoid subluxation. It is uncertain whether shoulder subluxation causes hemiplegic shoulder pain.
11.3 Spasticity, Contractures and Hemiplegic Shoulder Pain (HSP)
Abnormal muscle tone, including spasticity may be directly related to HSP. Spasticity is defined as a disorder of motor function characterized by a velocity-dependent increase in resistance to passive stretch of muscles accompanied by hyperactive muscle stretch reflexes and often associated with a clasp-knife phenomena. Spasticity is one component of the upper motor neuron (UMN) syndrome and is the inevitable accompaniment of hemiplegia and an incomplete motor recovery. Under normal circumstances a delicate balance exists between facilitating and inhibiting influences upon both alpha and gamma motor neurons, which
together maintain appropriate control of skeletal muscle length and strength of contraction at the spinal cord level. After a stroke, input from one or more of the supraspinal suppressor areas will decrease or stop entirely. The balance of control over the muscle tips in favour of facilitation and spasticity results. Spasticity develops only if there is loss of input from both pyramidal and extrapyramidal motor systems. Spasticity presents as increased tone and reflexes on the involved side of the body.
11. Painful Hemiplegic Shoulder pg. 12 of 65
www.ebrsr.com
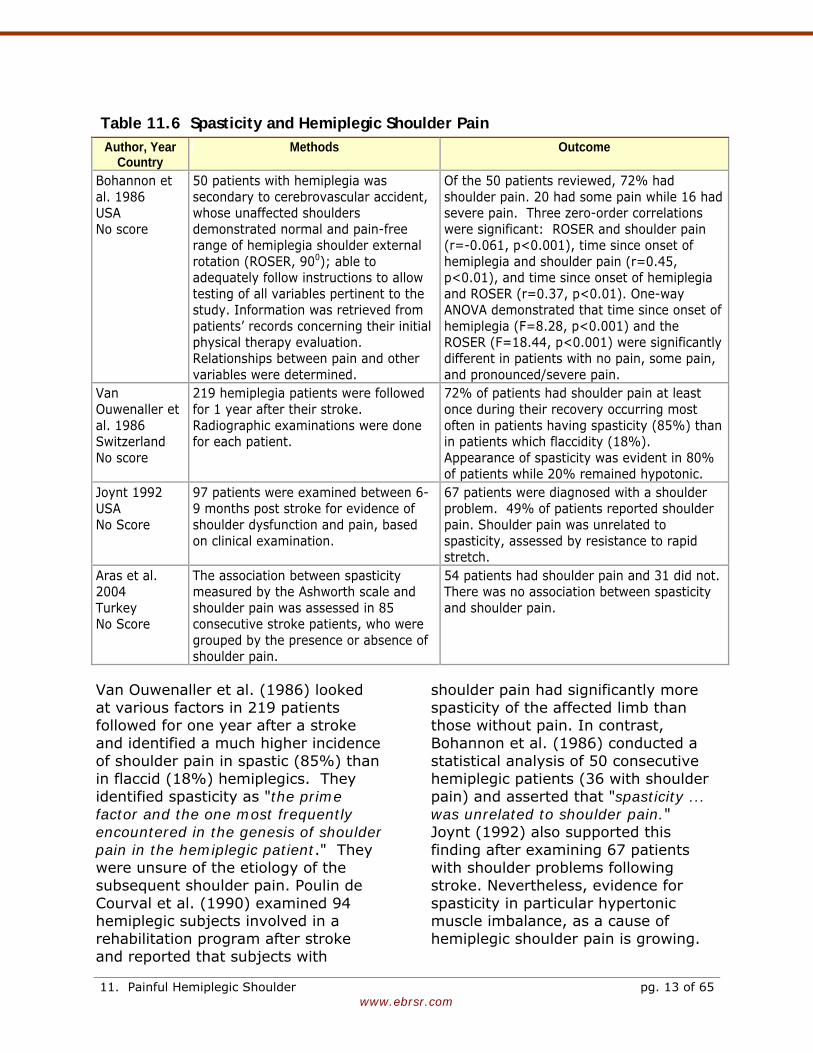
Table 11.6 Spasticity and Hemiplegic Shoulder Pain Author, Year
Country Methods Outcome
Bohannon et al. 1986 USA No score
50 patients with hemiplegia was secondary to cerebrovascular accident, whose unaffected shoulders demonstrated normal and pain-free range of hemiplegia shoulder external rotation (ROSER, 900); able to adequately follow instructions to allow testing of all variables pertinent to the study. Information was retrieved from patients’ records concerning their initial physical therapy evaluation. Relationships between pain and other variables were determined.
Of the 50 patients reviewed, 72% had shoulder pain. 20 had some pain while 16 had severe pain. Three zero-order correlations were significant: ROSER and shoulder pain (r=-0.061, p<0.001), time since onset of hemiplegia and shoulder pain (r=0.45, p<0.01), and time since onset of hemiplegia and ROSER (r=0.37, p<0.01). One-way ANOVA demonstrated that time since onset of hemiplegia (F=8.28, p<0.001) and the ROSER (F=18.44, p<0.001) were significantly different in patients with no pain, some pain, and pronounced/severe pain.
Van Ouwenaller et al. 1986 Switzerland No score
219 hemiplegia patients were followed for 1 year after their stroke. Radiographic examinations were done for each patient.
72% of patients had shoulder pain at least once during their recovery occurring most often in patients having spasticity (85%) than in patients which flaccidity (18%). Appearance of spasticity was evident in 80% of patients while 20% remained hypotonic.
Joynt 1992 USA No Score
97 patients were examined between 6-9 months post stroke for evidence of shoulder dysfunction and pain, based on clinical examination.
67 patients were diagnosed with a shoulder problem. 49% of patients reported shoulder pain. Shoulder pain was unrelated to spasticity, assessed by resistance to rapid stretch.
Aras et al. 2004 Turkey No Score
The association between spasticity measured by the Ashworth scale and shoulder pain was assessed in 85 consecutive stroke patients, who were grouped by the presence or absence of shoulder pain.
54 patients had shoulder pain and 31 did not. There was no association between spasticity and shoulder pain.
Van Ouwenaller et al. (1986) looked at various factors in 219 patients followed for one year after a stroke and identified a much higher incidence of shoulder pain in spastic (85%) than in flaccid (18%) hemiplegics. They identified spasticity as "the prime factor and the one most frequently encountered in the genesis of shoulder pain in the hemiplegic patient." They were unsure of the etiology of the subsequent shoulder pain. Poulin de Courval et al. (1990) examined 94 hemiplegic subjects involved in a rehabilitation program after stroke and reported that subjects with
shoulder pain had significantly more spasticity of the affected limb than those without pain. In contrast, Bohannon et al. (1986) conducted a statistical analysis of 50 consecutive hemiplegic patients (36 with shoulder pain) and asserted that "spasticity ... was unrelated to shoulder pain." Joynt (1992) also supported this finding after examining 67 patients with shoulder problems following stroke. Nevertheless, evidence for spasticity in particular hypertonic muscle imbalance, as a cause of hemiplegic shoulder pain is growing.
11. Painful Hemiplegic Shoulder pg. 13 of 65

www.ebrsr.com
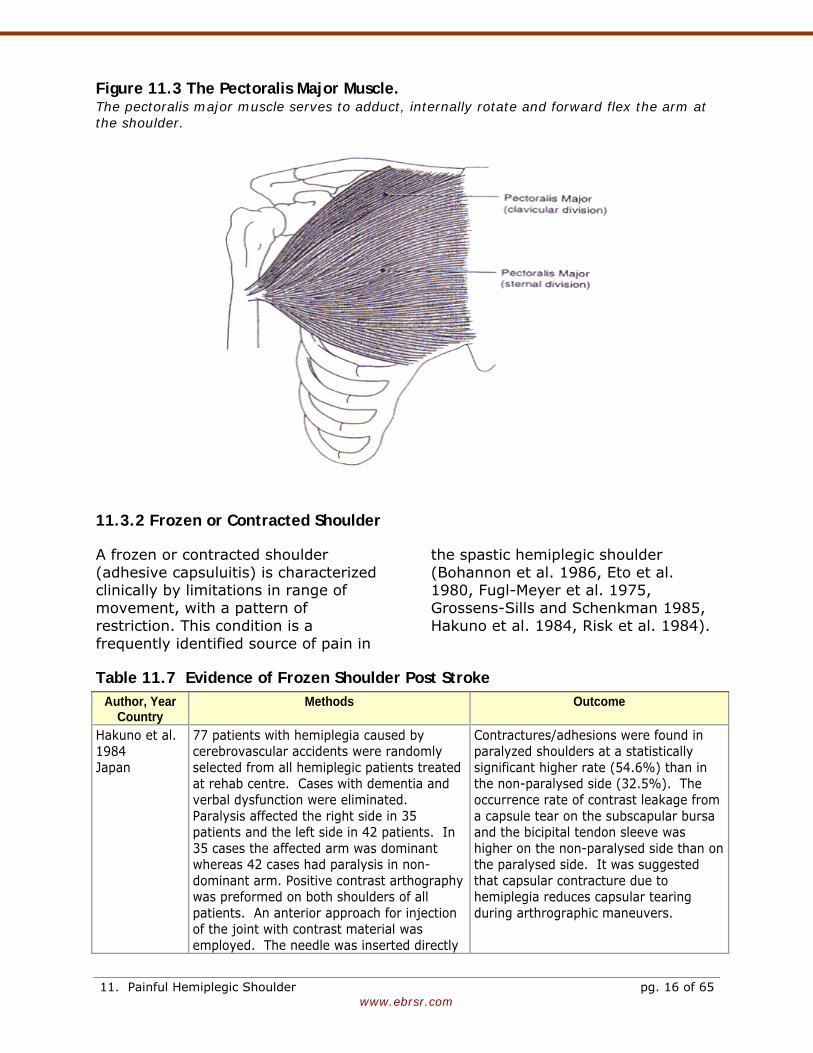
11.3.1 Spastic Muscle Imbalance Hemiplegia following stroke is characterized by typical posturing reflecting hypertonic muscle patterns. Flexor tone predominates in the hemiplegic upper extremity and results in scapular retraction and depression as well as internal rotation and adduction of the shoulder. This posture is the consequence of ablation of higher centers and subsequent release of motor groups from pyramidal and extrapyramidal control. In stroke recovery, this "synergy pattern" of muscles is inevitable where recovery is incomplete. One consequence of this is the development of spastic muscle imbalance about the shoulder joint. Clinically the internal rotators of the shoulder predominate after a stroke involving that arm and external rotation is one of the last areas of shoulder function to recover. Hence, during recovery motor units are not appropriately recruited or turned off; the result is simultaneous co-contraction of agonist and antagonist muscles. A shortened agonist in the synergy pattern becomes stronger and the constant tension of the agonist can become painful. Stretching of these tightened spastic muscles causes more pain. Shortened muscles inhibit movement, reduce range of motion, and prevent other movements especially at the shoulder where external rotation of the humerus is necessary for arm abduction greater than 90 degrees. Muscles that contribute to spastic internal rotation/adduction of the shoulder include the subscapularis, pectoralis major, teres major and latissimus dorsi muscles. However, two muscles in particular have been implicated as most often being spastic leading to
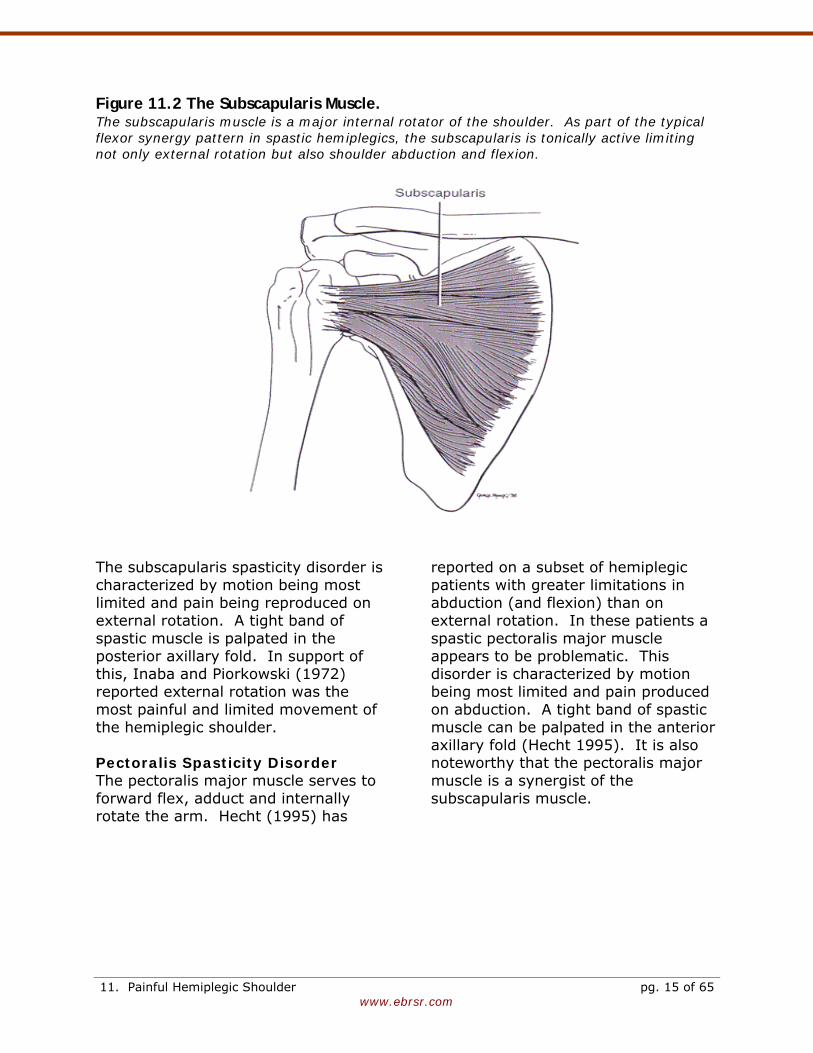
muscle imbalance. These are the subscapularis and pectoralis major muscles. Subscapularis Spasticity Disorder The subscapularis muscle originates on the undersurface of the scapula and inserts on the lesser tuberosity of the humerus as well as the capsule of the shoulder joint (Figure 11.2). It is a major internal rotator of the shoulder (Hollinshead and Jenkins 1981). The subscapularis muscle also participates in arm abduction and extension from a flexed position (Cole and Tobis 1990). In normal individuals, nerve impulses to the subscapularis are inhibited during arm abduction; the muscle then relaxes and allows the humerus to externally rotate, thus preventing impingement of the greater tuberosity on the acromion (Codman 1934). As part of the typical flexor synergy pattern in spastic hemiplegics, internal rotators, including the subscapularis muscle, are tonically active. This limits shoulder abduction, flexion and external rotation. Bohannon et al. (1986) found limitation of external rotation of the hemiplegic shoulder was the factor which most correlated with hemiplegic shoulder pain. Zorowitz et al. (1996) also found that limitation in shoulder external rotation correlated strongly with pain. Hecht (1995) specifically linked this problem to the subscapularis muscle when he noted, "The subscapularis muscle is the primary cause of shoulder pain in spastic hemiplegia where external rotation is most limited. Although other muscles may contribute to spasticity, pain and functional contracture, the subscapularis is the keystone of the abnormal synergy pattern."
11. Painful Hemiplegic Shoulder pg. 14 of 65
www.ebrsr.com
Figure 11.2 The Subscapularis Muscle. The subscapularis muscle is a major internal rotator of the shoulder. As part of the typical flexor synergy pattern in spastic hemiplegics, the subscapularis is tonically active limiting not only external rotation but also shoulder abduction and flexion.
The subscapularis spasticity disorder is characterized by motion being most limited and pain being reproduced on external rotation. A tight band of spastic muscle is palpated in the posterior axillary fold. In support of this, Inaba and Piorkowski (1972) reported external rotation was the most painful and limited movement of the hemiplegic shoulder. Pectoralis Spasticity Disorder The pectoralis major muscle serves to forward flex, adduct and internally rotate the arm. Hecht (1995) has
reported on a subset of hemiplegic patients with greater limitations in abduction (and flexion) than on external rotation. In these patients a spastic pectoralis major muscle appears to be problematic. This disorder is characterized by motion being most limited and pain produced on abduction. A tight band of spastic muscle can be palpated in the anterior axillary fold (Hecht 1995). It is also noteworthy that the pectoralis major muscle is a synergist of the subscapularis muscle.
11. Painful Hemiplegic Shoulder pg. 15 of 65
www.ebrsr.com
Figure 11.3 The Pectoralis Major Muscle. The pectoralis major muscle serves to adduct, internally rotate and forward flex the arm at the shoulder.
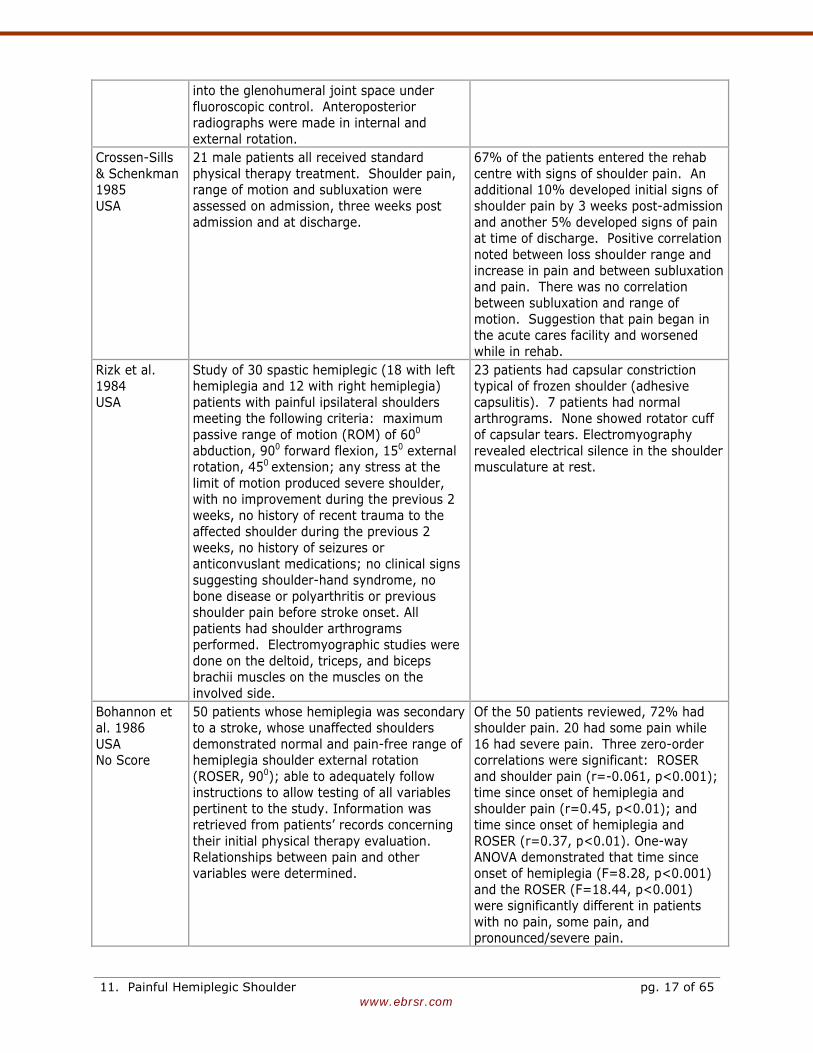
11.3.2 Frozen or Contracted Shoulder A frozen or contracted shoulder (adhesive capsuluitis) is characterized clinically by limitations in range of movement, with a pattern of restriction. This condition is a frequently identified source of pain in
the spastic hemiplegic shoulder (Bohannon et al. 1986, Eto et al. 1980, Fugl-Meyer et al. 1975, Grossens-Sills and Schenkman 1985, Hakuno et al. 1984, Risk et al. 1984).
Table 11.7 Evidence of Frozen Shoulder Post Stroke Author, Year
Country Methods Outcome
Hakuno et al. 1984 Japan
77 patients with hemiplegia caused by cerebrovascular accidents were randomly selected from all hemiplegic patients treated at rehab centre. Cases with dementia and verbal dysfunction were eliminated. Paralysis affected the right side in 35 patients and the left side in 42 patients. In 35 cases the affected arm was dominant whereas 42 cases had paralysis in non-dominant arm. Positive contrast arthography was preformed on both shoulders of all patients. An anterior approach for injection of the joint with contrast material was employed. The needle was inserted directly
Contractures/adhesions were found in paralyzed shoulders at a statistically significant higher rate (54.6%) than in the non-paralysed side (32.5%). The occurrence rate of contrast leakage from a capsule tear on the subscapular bursa and the bicipital tendon sleeve was higher on the non-paralysed side than on the paralysed side. It was suggested that capsular contracture due to hemiplegia reduces capsular tearing during arthrographic maneuvers.
11. Painful Hemiplegic Shoulder pg. 16 of 65
www.ebrsr.com
into the glenohumeral joint space under fluoroscopic control. Anteroposterior radiographs were made in internal and external rotation.
Crossen-Sills & Schenkman 1985 USA
21 male patients all received standard physical therapy treatment. Shoulder pain, range of motion and subluxation were assessed on admission, three weeks post admission and at discharge.
67% of the patients entered the rehab centre with signs of shoulder pain. An additional 10% developed initial signs of shoulder pain by 3 weeks post-admission and another 5% developed signs of pain at time of discharge. Positive correlation noted between loss shoulder range and increase in pain and between subluxation and pain. There was no correlation between subluxation and range of motion. Suggestion that pain began in the acute cares facility and worsened while in rehab.
Rizk et al. 1984 USA
Study of 30 spastic hemiplegic (18 with left hemiplegia and 12 with right hemiplegia) patients with painful ipsilateral shoulders meeting the following criteria: maximum passive range of motion (ROM) of 600 abduction, 900 forward flexion, 150 external rotation, 450 extension; any stress at the limit of motion produced severe shoulder, with no improvement during the previous 2 weeks, no history of recent trauma to the affected shoulder during the previous 2 weeks, no history of seizures or anticonvuslant medications; no clinical signs suggesting shoulder-hand syndrome, no bone disease or polyarthritis or previous shoulder pain before stroke onset. All patients had shoulder arthrograms performed. Electromyographic studies were done on the deltoid, triceps, and biceps brachii muscles on the muscles on the involved side.
23 patients had capsular constriction typical of frozen shoulder (adhesive capsulitis). 7 patients had normal arthrograms. None showed rotator cuff of capsular tears. Electromyography revealed electrical silence in the shoulder musculature at rest.
Bohannon et al. 1986 USA No Score
50 patients whose hemiplegia was secondary to a stroke, whose unaffected shoulders demonstrated normal and pain-free range of hemiplegia shoulder external rotation (ROSER, 900); able to adequately follow instructions to allow testing of all variables pertinent to the study. Information was retrieved from patients’ records concerning their initial physical therapy evaluation. Relationships between pain and other variables were determined.
Of the 50 patients reviewed, 72% had shoulder pain. 20 had some pain while 16 had severe pain. Three zero-order correlations were significant: ROSER and shoulder pain (r=-0.061, p<0.001); time since onset of hemiplegia and shoulder pain (r=0.45, p<0.01); and time since onset of hemiplegia and ROSER (r=0.37, p<0.01). One-way ANOVA demonstrated that time since onset of hemiplegia (F=8.28, p<0.001) and the ROSER (F=18.44, p<0.001) were significantly different in patients with no pain, some pain, and pronounced/severe pain.
11. Painful Hemiplegic Shoulder pg. 17 of 65

www.ebrsr.com
Lo et al. 2003 Taiwan No Score
32 consecutive patients with shoulder pain following stroke were assessed for shoulder subluxation, which was diagnosed by a gap of more than one finger breadth between the acrimonion and the head of the humeral bone on palpation.
16 (54%) of patients had rotator cuff tears diagnosed by arthrograpy.
In summary, while shoulder subluxation is not always associated with shoulder pain, spasticity generally is. The problem of hemiplegic shoulder pain appears to be due to a combination of spastic muscle imbalance and a frozen contracted shoulder. However, overaggressive stretching of the shoulder through an aggressive stretching program may simply aggravate pain (see Treatment), as it does not address the issue of spastic muscle imbalance.
Conclusions Regarding Spastic Hemiplegic Shoulder There is an association between spasticity and the development of hemiplegic shoulder pain. Spasticity and subsequent frozen shoulder are the most likely causes of hemiplegic shoulder pain.
Spasticity and hemiplegic shoulder pain are related.
11.4 Rotator Cuff Disorders
Because shoulder pain is so often associated with rotator cuff disorder in a non-stroke population it should not be surprising that it would be seen as a potentially common cause of hemiplegic shoulder pain. However, Risk et al. (1984) failed to demonstrate any evidence of rotator cuff tears on arthrography in 30 patients with hemiplegic shoulder pain (Risk et al. 1984). A similar study
(Nepomuceno and Miller 1974) reported a 33% incidence of rotator cuff tears in painful shoulders after strokes. Najenson et al. (1971) reported that 13 of 32 (40%) patients with severe paralysis of the upper extremity were found to have a rupture of the rotator-cuff ligament based on arthrographic findings. Partial tears of the rotator cuff musculature are common and it is always difficult determining whether they were present premorbidly even in previously asymptomatic patients. Joynt (1992) diagnosed 67 stroke patients as having hemiplegic shoulder pain. 28 patients received a subacromial injection of 1% lidocaine; approximately half obtained moderate or marked relief of pain and improved range of motion. However, this provides only indirect evidence of rotator cuff disorders as a possible cause of hemiplegic shoulder pain. Generally, hemiplegic shoulder pain is not commonly associated with rotator cuff disorders.
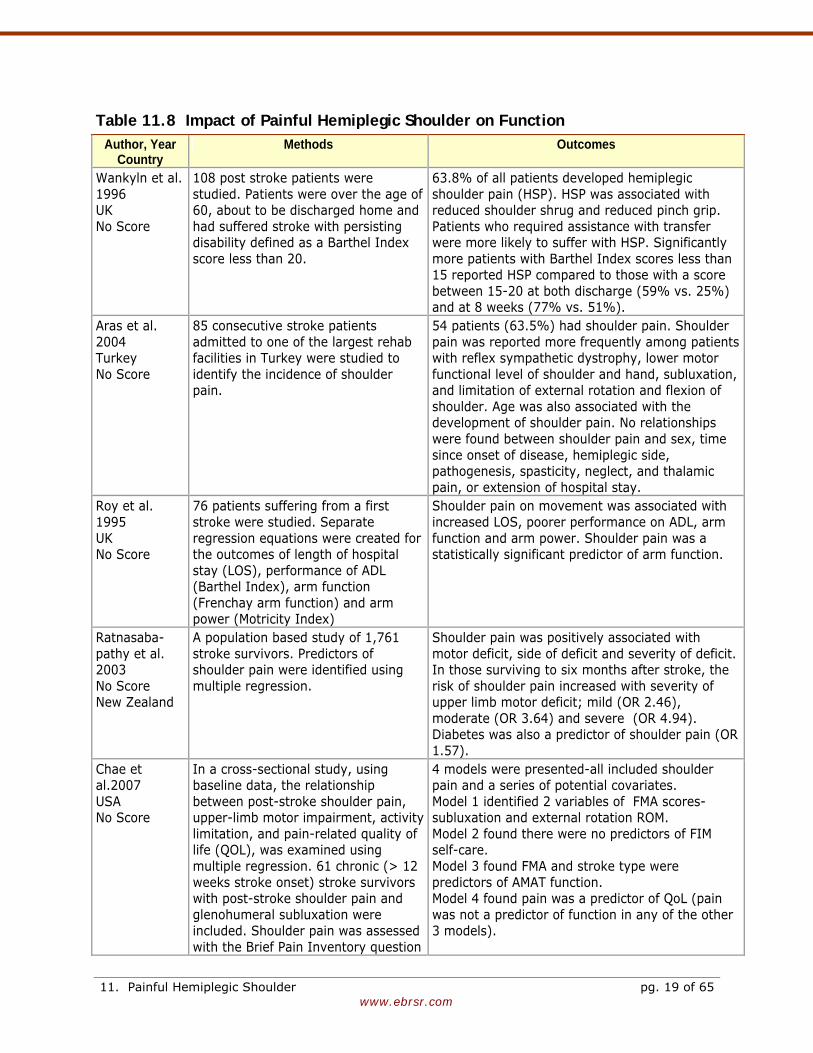
11.5 Functional Impact of Painful Hemiplegic Shoulder A painful hemiplegic shoulder can be very limiting and has the potential to further add to the disability seen with hemiplegia. However, a clear relationship between post-stroke shoulder pain and motor recovery has not been shown. The results from several studies have been conflicting.
11. Painful Hemiplegic Shoulder pg. 18 of 65
www.ebrsr.com
Table 11.8 Impact of Painful Hemiplegic Shoulder on Function Author, Year
Country Methods Outcomes
Wankyln et al. 1996 UK No Score
108 post stroke patients were studied. Patients were over the age of 60, about to be discharged home and had suffered stroke with persisting disability defined as a Barthel Index score less than 20.
63.8% of all patients developed hemiplegic shoulder pain (HSP). HSP was associated with reduced shoulder shrug and reduced pinch grip. Patients who required assistance with transfer were more likely to suffer with HSP. Significantly more patients with Barthel Index scores less than 15 reported HSP compared to those with a score between 15-20 at both discharge (59% vs. 25%) and at 8 weeks (77% vs. 51%).
Aras et al. 2004 Turkey No Score
85 consecutive stroke patients admitted to one of the largest rehab facilities in Turkey were studied to identify the incidence of shoulder pain.
54 patients (63.5%) had shoulder pain. Shoulder pain was reported more frequently among patients with reflex sympathetic dystrophy, lower motor functional level of shoulder and hand, subluxation, and limitation of external rotation and flexion of shoulder. Age was also associated with the development of shoulder pain. No relationships were found between shoulder pain and sex, time since onset of disease, hemiplegic side, pathogenesis, spasticity, neglect, and thalamic pain, or extension of hospital stay.
Roy et al. 1995 UK No Score
76 patients suffering from a first stroke were studied. Separate regression equations were created for the outcomes of length of hospital stay (LOS), performance of ADL (Barthel Index), arm function (Frenchay arm function) and arm power (Motricity Index)
Shoulder pain on movement was associated with increased LOS, poorer performance on ADL, arm function and arm power. Shoulder pain was a statistically significant predictor of arm function.
Ratnasaba-pathy et al. 2003 No Score New Zealand
A population based study of 1,761 stroke survivors. Predictors of shoulder pain were identified using multiple regression.
Shoulder pain was positively associated with motor deficit, side of deficit and severity of deficit. In those surviving to six months after stroke, the risk of shoulder pain increased with severity of upper limb motor deficit; mild (OR 2.46), moderate (OR 3.64) and severe (OR 4.94). Diabetes was also a predictor of shoulder pain (OR 1.57).
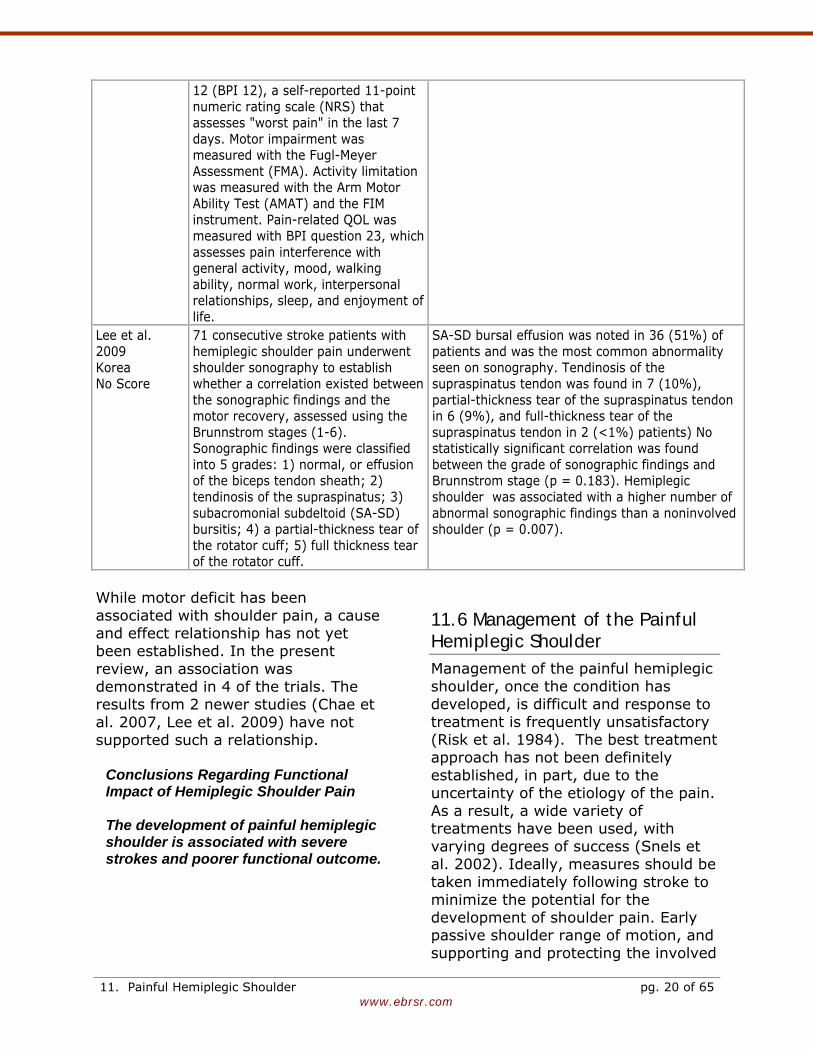
Chae et al.2007 USA No Score
In a cross-sectional study, using baseline data, the relationship between post-stroke shoulder pain, upper-limb motor impairment, activity limitation, and pain-related quality of life (QOL), was examined using multiple regression. 61 chronic (> 12 weeks stroke onset) stroke survivors with post-stroke shoulder pain and glenohumeral subluxation were included. Shoulder pain was assessed with the Brief Pain Inventory question
4 models were presented-all included shoulder pain and a series of potential covariates. Model 1 identified 2 variables of FMA scores- subluxation and external rotation ROM. Model 2 found there were no predictors of FIM self-care. Model 3 found FMA and stroke type were predictors of AMAT function. Model 4 found pain was a predictor of QoL (pain was not a predictor of function in any of the other 3 models).
11. Painful Hemiplegic Shoulder pg. 19 of 65
www.ebrsr.com
12 (BPI 12), a self-reported 11-point numeric rating scale (NRS) that assesses "worst pain" in the last 7 days. Motor impairment was measured with the Fugl-Meyer Assessment (FMA). Activity limitation was measured with the Arm Motor Ability Test (AMAT) and the FIM instrument. Pain-related QOL was measured with BPI question 23, which assesses pain interference with general activity, mood, walking ability, normal work, interpersonal relationships, sleep, and enjoyment of life.
Lee et al. 2009 Korea No Score
71 consecutive stroke patients with hemiplegic shoulder pain underwent shoulder sonography to establish whether a correlation existed between the sonographic findings and the motor recovery, assessed using the Brunnstrom stages (1-6). Sonographic findings were classified into 5 grades: 1) normal, or effusion of the biceps tendon sheath; 2) tendinosis of the supraspinatus; 3) subacromonial subdeltoid (SA-SD) bursitis; 4) a partial-thickness tear of the rotator cuff; 5) full thickness tear of the rotator cuff.
SA-SD bursal effusion was noted in 36 (51%) of patients and was the most common abnormality seen on sonography. Tendinosis of the supraspinatus tendon was found in 7 (10%), partial-thickness tear of the supraspinatus tendon in 6 (9%), and full-thickness tear of the supraspinatus tendon in 2 (<1%) patients) No statistically significant correlation was found between the grade of sonographic findings and Brunnstrom stage (p = 0.183). Hemiplegic shoulder was associated with a higher number of abnormal sonographic findings than a noninvolved shoulder (p = 0.007).
While motor deficit has been associated with shoulder pain, a cause and effect relationship has not yet been established. In the present review, an association was demonstrated in 4 of the trials. The results from 2 newer studies (Chae et al. 2007, Lee et al. 2009) have not supported such a relationship.
Conclusions Regarding Functional Impact of Hemiplegic Shoulder Pain The development of painful hemiplegic shoulder is associated with severe strokes and poorer functional outcome.
11.6 Management of the Painful Hemiplegic Shoulder Management of the painful hemiplegic shoulder, once the condition has developed, is difficult and response to treatment is frequently unsatisfactory (Risk et al. 1984). The best treatment approach has not been definitely established, in part, due to the uncertainty of the etiology of the pain. As a result, a wide variety of treatments have been used, with varying degrees of success (Snels et al. 2002). Ideally, measures should be taken immediately following stroke to minimize the potential for the development of shoulder pain. Early passive shoulder range of motion, and supporting and protecting the involved
11. Painful Hemiplegic Shoulder pg. 20 of 65
www.ebrsr.com
shoulder, in the initial flaccid stage are regarded as important steps to reduce the development of shoulder pain.
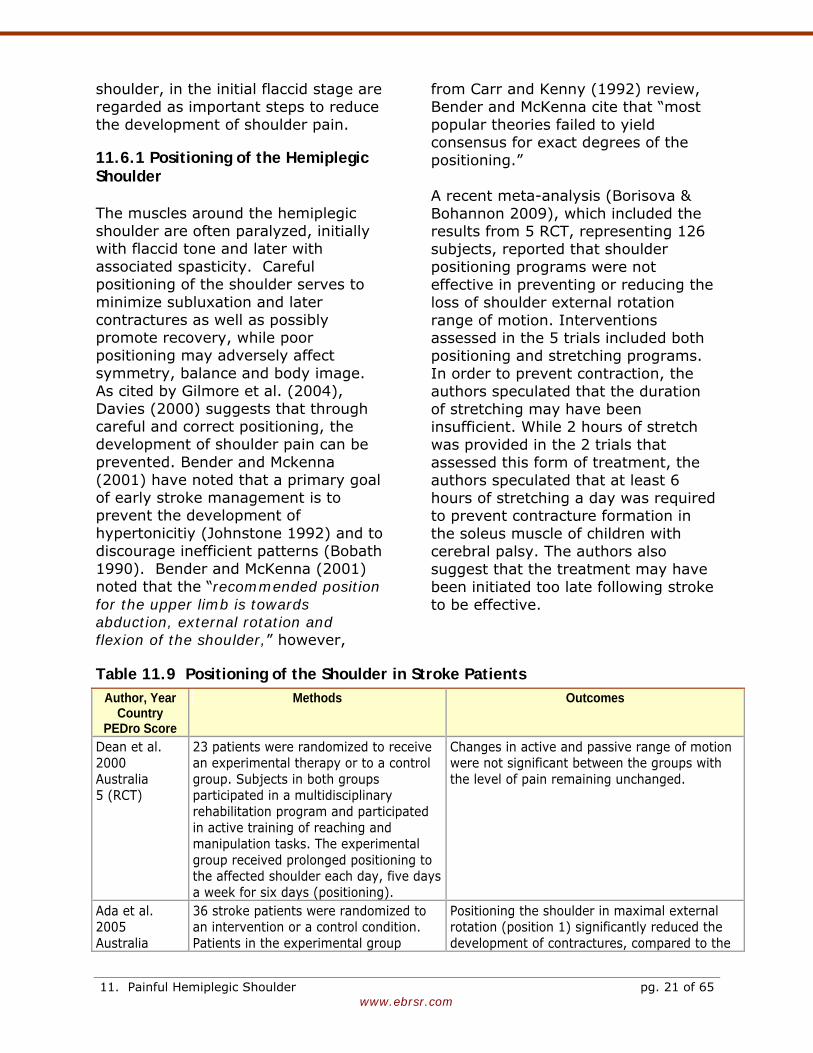
11.6.1 Positioning of the Hemiplegic Shoulder The muscles around the hemiplegic shoulder are often paralyzed, initially with flaccid tone and later with associated spasticity. Careful positioning of the shoulder serves to minimize subluxation and later contractures as well as possibly promote recovery, while poor positioning may adversely affect symmetry, balance and body image. As cited by Gilmore et al. (2004), Davies (2000) suggests that through careful and correct positioning, the development of shoulder pain can be prevented. Bender and Mckenna (2001) have noted that a primary goal of early stroke management is to prevent the development of hypertonicitiy (Johnstone 1992) and to discourage inefficient patterns (Bobath 1990). Bender and McKenna (2001) noted that the “recommended position for the upper limb is towards abduction, external rotation and flexion of the shoulder,” however,
from Carr and Kenny (1992) review, Bender and McKenna cite that “most popular theories failed to yield consensus for exact degrees of the positioning.” A recent meta-analysis (Borisova & Bohannon 2009), which included the results from 5 RCT, representing 126 subjects, reported that shoulder positioning programs were not effective in preventing or reducing the loss of shoulder external rotation range of motion. Interventions assessed in the 5 trials included both positioning and stretching programs. In order to prevent contraction, the authors speculated that the duration of stretching may have been insufficient. While 2 hours of stretch was provided in the 2 trials that assessed this form of treatment, the authors speculated that at least 6 hours of stretching a day was required to prevent contracture formation in the soleus muscle of children with cerebral palsy. The authors also suggest that the treatment may have been initiated too late following stroke to be effective.
Table 11.9 Positioning of the Shoulder in Stroke Patients Author, Year
Country PEDro Score
Methods Outcomes
Dean et al. 2000 Australia 5 (RCT)
23 patients were randomized to receive an experimental therapy or to a control group. Subjects in both groups participated in a multidisciplinary rehabilitation program and participated in active training of reaching and manipulation tasks. The experimental group received prolonged positioning to the affected shoulder each day, five days a week for six days (positioning).
Changes in active and passive range of motion were not significant between the groups with the level of pain remaining unchanged.
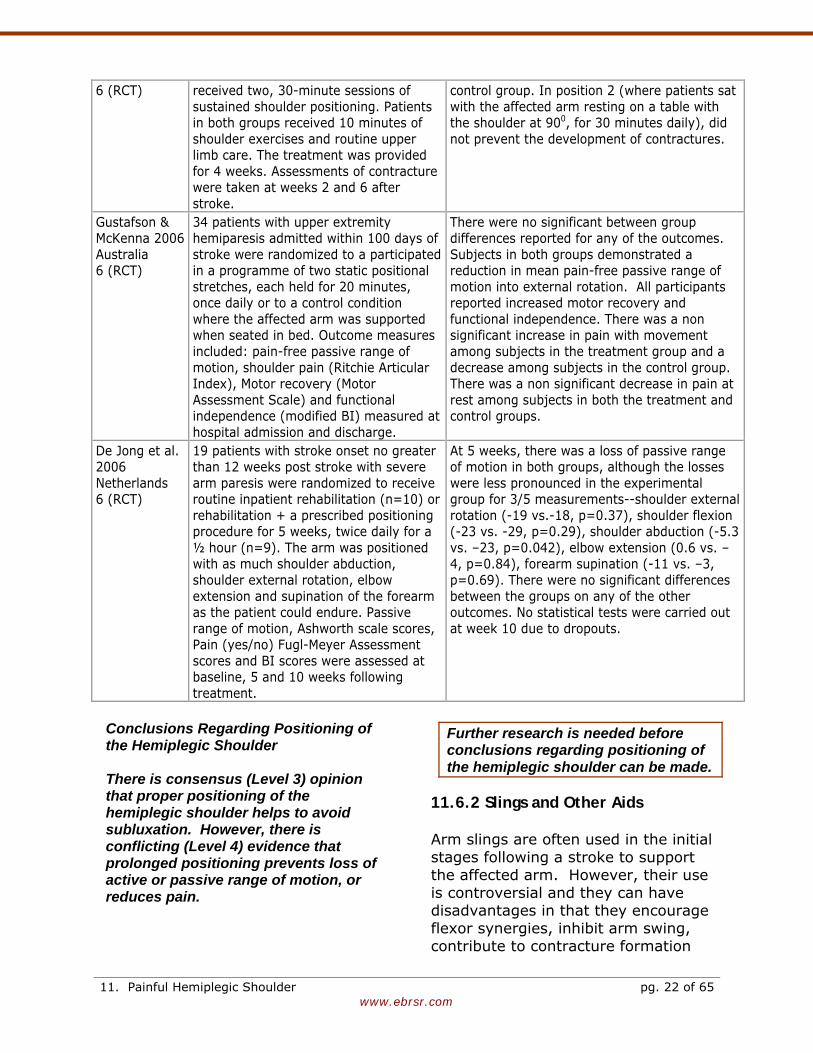
Ada et al. 2005 Australia
36 stroke patients were randomized to an intervention or a control condition. Patients in the experimental group
Positioning the shoulder in maximal external rotation (position 1) significantly reduced the development of contractures, compared to the
11. Painful Hemiplegic Shoulder pg. 21 of 65
www.ebrsr.com
6 (RCT) received two, 30-minute sessions of sustained shoulder positioning. Patients in both groups received 10 minutes of shoulder exercises and routine upper limb care. The treatment was provided for 4 weeks. Assessments of contracture were taken at weeks 2 and 6 after stroke.
control group. In position 2 (where patients sat with the affected arm resting on a table with the shoulder at 900, for 30 minutes daily), did not prevent the development of contractures.
Gustafson & McKenna 2006 Australia 6 (RCT)
34 patients with upper extremity hemiparesis admitted within 100 days of stroke were randomized to a participated in a programme of two static positional stretches, each held for 20 minutes, once daily or to a control condition where the affected arm was supported when seated in bed. Outcome measures included: pain-free passive range of motion, shoulder pain (Ritchie Articular Index), Motor recovery (Motor Assessment Scale) and functional independence (modified BI) measured at hospital admission and discharge.
There were no significant between group differences reported for any of the outcomes. Subjects in both groups demonstrated a reduction in mean pain-free passive range of motion into external rotation. All participants reported increased motor recovery and functional independence. There was a non significant increase in pain with movement among subjects in the treatment group and a decrease among subjects in the control group. There was a non significant decrease in pain at rest among subjects in both the treatment and control groups.
De Jong et al. 2006 Netherlands 6 (RCT)
19 patients with stroke onset no greater than 12 weeks post stroke with severe arm paresis were randomized to receive routine inpatient rehabilitation (n=10) or rehabilitation + a prescribed positioning procedure for 5 weeks, twice daily for a ½ hour (n=9). The arm was positioned with as much shoulder abduction, shoulder external rotation, elbow extension and supination of the forearm as the patient could endure. Passive range of motion, Ashworth scale scores, Pain (yes/no) Fugl-Meyer Assessment scores and BI scores were assessed at baseline, 5 and 10 weeks following treatment.
At 5 weeks, there was a loss of passive range of motion in both groups, although the losses were less pronounced in the experimental group for 3/5 measurements--shoulder external rotation (-19 vs.-18, p=0.37), shoulder flexion (-23 vs. -29, p=0.29), shoulder abduction (-5.3 vs. –23, p=0.042), elbow extension (0.6 vs. –4, p=0.84), forearm supination (-11 vs. –3, p=0.69). There were no significant differences between the groups on any of the other outcomes. No statistical tests were carried out at week 10 due to dropouts.
Conclusions Regarding Positioning of the Hemiplegic Shoulder
There is consensus (Level 3) opinion that proper positioning of the hemiplegic shoulder helps to avoid subluxation. However, there is conflicting (Level 4) evidence that prolonged positioning prevents loss of active or passive range of motion, or reduces pain.
Further research is needed before conclusions regarding positioning of the hemiplegic shoulder can be made.
11.6.2 Slings and Other Aids Arm slings are often used in the initial stages following a stroke to support the affected arm. However, their use is controversial and they can have disadvantages in that they encourage flexor synergies, inhibit arm swing, contribute to contracture formation
11. Painful Hemiplegic Shoulder pg. 22 of 65
www.ebrsr.com
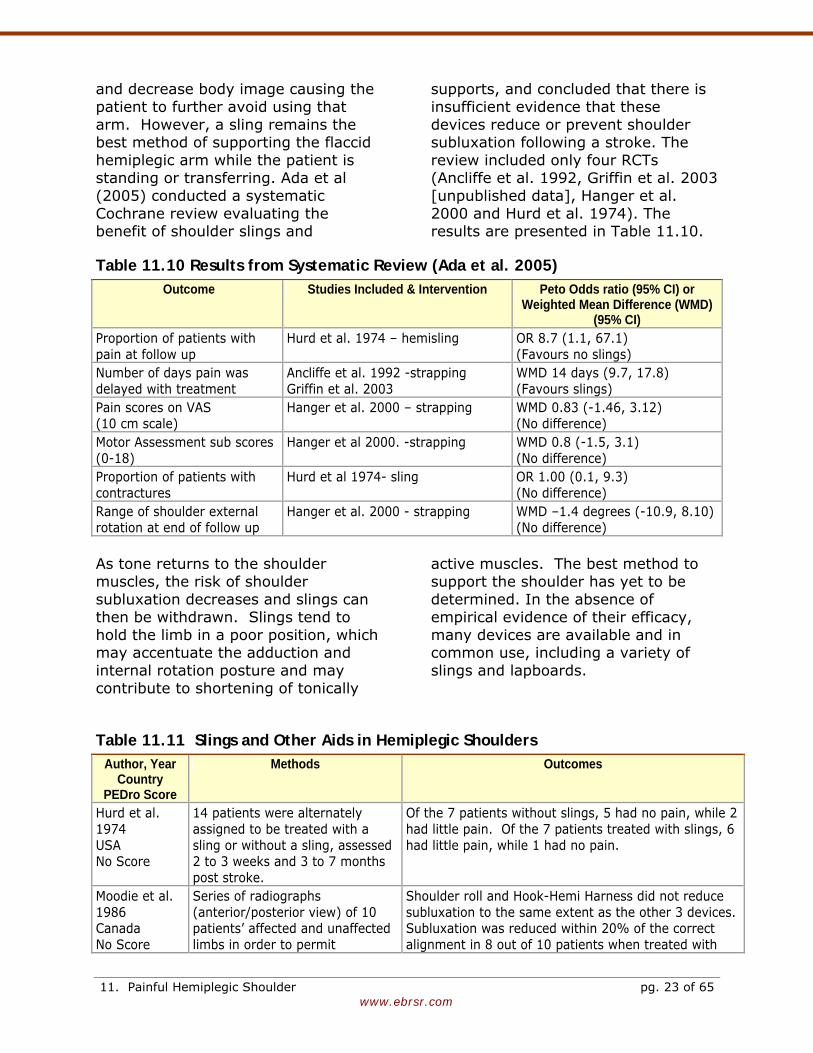
and decrease body image causing the patient to further avoid using that arm. However, a sling remains the best method of supporting the flaccid hemiplegic arm while the patient is standing or transferring. Ada et al (2005) conducted a systematic Cochrane review evaluating the benefit of shoulder slings and
supports, and concluded that there is insufficient evidence that these devices reduce or prevent shoulder subluxation following a stroke. The review included only four RCTs (Ancliffe et al. 1992, Griffin et al. 2003 [unpublished data], Hanger et al. 2000 and Hurd et al. 1974). The results are presented in Table 11.10.
Table 11.10 Results from Systematic Review (Ada et al. 2005) Outcome Studies Included & Intervention Peto Odds ratio (95% CI) or
Weighted Mean Difference (WMD) (95% CI)
Proportion of patients with pain at follow up
Hurd et al. 1974 – hemisling OR 8.7 (1.1, 67.1) (Favours no slings)
Number of days pain was delayed with treatment
Ancliffe et al. 1992 -strapping Griffin et al. 2003
WMD 14 days (9.7, 17.8) (Favours slings)
Pain scores on VAS (10 cm scale)
Hanger et al. 2000 – strapping WMD 0.83 (-1.46, 3.12) (No difference)
Motor Assessment sub scores (0-18)
Hanger et al 2000. -strapping WMD 0.8 (-1.5, 3.1) (No difference)
Proportion of patients with contractures
Hurd et al 1974- sling OR 1.00 (0.1, 9.3) (No difference)
Range of shoulder external rotation at end of follow up
Hanger et al. 2000 - strapping WMD –1.4 degrees (-10.9, 8.10) (No difference)
As tone returns to the shoulder muscles, the risk of shoulder subluxation decreases and slings can then be withdrawn. Slings tend to hold the limb in a poor position, which may accentuate the adduction and internal rotation posture and may contribute to shortening of tonically
active muscles. The best method to support the shoulder has yet to be determined. In the absence of empirical evidence of their efficacy, many devices are available and in common use, including a variety of slings and lapboards.
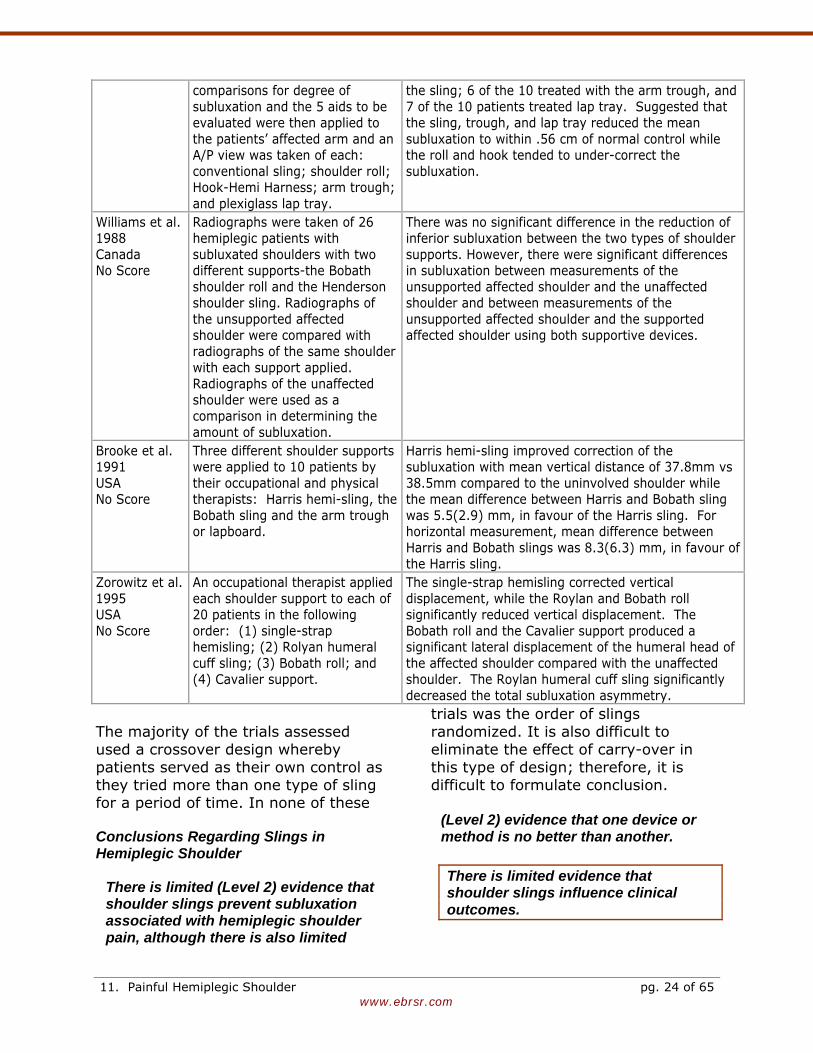
Table 11.11 Slings and Other Aids in Hemiplegic Shoulders Author, Year
Country PEDro Score
Methods Outcomes
Hurd et al. 1974 USA No Score
14 patients were alternately assigned to be treated with a sling or without a sling, assessed 2 to 3 weeks and 3 to 7 months post stroke.
Of the 7 patients without slings, 5 had no pain, while 2 had little pain. Of the 7 patients treated with slings, 6 had little pain, while 1 had no pain.
Moodie et al. 1986 Canada No Score
Series of radiographs (anterior/posterior view) of 10 patients’ affected and unaffected limbs in order to permit
Shoulder roll and Hook-Hemi Harness did not reduce subluxation to the same extent as the other 3 devices. Subluxation was reduced within 20% of the correct alignment in 8 out of 10 patients when treated with
11. Painful Hemiplegic Shoulder pg. 23 of 65
www.ebrsr.com
comparisons for degree of subluxation and the 5 aids to be evaluated were then applied to the patients’ affected arm and an A/P view was taken of each: conventional sling; shoulder roll; Hook-Hemi Harness; arm trough; and plexiglass lap tray.
the sling; 6 of the 10 treated with the arm trough, and 7 of the 10 patients treated lap tray. Suggested that the sling, trough, and lap tray reduced the mean subluxation to within .56 cm of normal control while the roll and hook tended to under-correct the subluxation.
Williams et al. 1988 Canada No Score
Radiographs were taken of 26 hemiplegic patients with subluxated shoulders with two different supports-the Bobath shoulder roll and the Henderson shoulder sling. Radiographs of the unsupported affected shoulder were compared with radiographs of the same shoulder with each support applied. Radiographs of the unaffected shoulder were used as a comparison in determining the amount of subluxation.
There was no significant difference in the reduction of inferior subluxation between the two types of shoulder supports. However, there were significant differences in subluxation between measurements of the unsupported affected shoulder and the unaffected shoulder and between measurements of the unsupported affected shoulder and the supported affected shoulder using both supportive devices.
Brooke et al. 1991 USA No Score
Three different shoulder supports were applied to 10 patients by their occupational and physical therapists: Harris hemi-sling, the Bobath sling and the arm trough or lapboard.
Harris hemi-sling improved correction of the subluxation with mean vertical distance of 37.8mm vs 38.5mm compared to the uninvolved shoulder while the mean difference between Harris and Bobath sling was 5.5(2.9) mm, in favour of the Harris sling. For horizontal measurement, mean difference between Harris and Bobath slings was 8.3(6.3) mm, in favour of the Harris sling.
Zorowitz et al. 1995 USA No Score
An occupational therapist applied each shoulder support to each of 20 patients in the following order: (1) single-strap hemisling; (2) Rolyan humeral cuff sling; (3) Bobath roll; and (4) Cavalier support.
The single-strap hemisling corrected vertical displacement, while the Roylan and Bobath roll significantly reduced vertical displacement. The Bobath roll and the Cavalier support produced a significant lateral displacement of the humeral head of the affected shoulder compared with the unaffected shoulder. The Roylan humeral cuff sling significantly decreased the total subluxation asymmetry.
The majority of the trials assessed used a crossover design whereby patients served as their own control as they tried more than one type of sling for a period of time. In none of these
trials was the order of slings randomized. It is also difficult to eliminate the effect of carry-over in this type of design; therefore, it is difficult to formulate conclusion.
Conclusions Regarding Slings in Hemiplegic Shoulder
There is limited (Level 2) evidence that shoulder slings prevent subluxation associated with hemiplegic shoulder pain, although there is also limited
(Level 2) evidence that one device or method is no better than another.
There is limited evidence that shoulder slings influence clinical outcomes.
11. Painful Hemiplegic Shoulder pg. 24 of 65
www.ebrsr.com
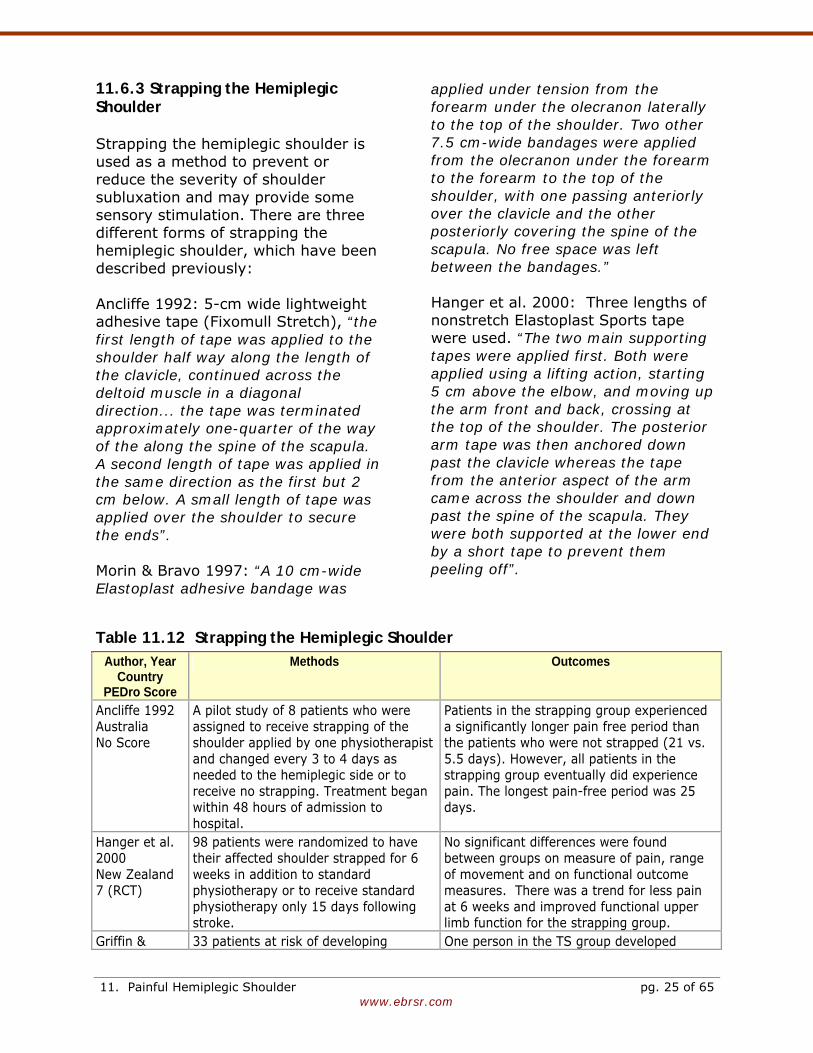
11.6.3 Strapping the Hemiplegic Shoulder Strapping the hemiplegic shoulder is used as a method to prevent or reduce the severity of shoulder subluxation and may provide some sensory stimulation. There are three different forms of strapping the hemiplegic shoulder, which have been described previously: Ancliffe 1992: 5-cm wide lightweight adhesive tape (Fixomull Stretch), “the first length of tape was applied to the shoulder half way along the length of the clavicle, continued across the deltoid muscle in a diagonal direction... the tape was terminated approximately one-quarter of the way of the along the spine of the scapula. A second length of tape was applied in the same direction as the first but 2 cm below. A small length of tape was applied over the shoulder to secure the ends”. Morin & Bravo 1997: “A 10 cm-wide Elastoplast adhesive bandage was
applied under tension from the forearm under the olecranon laterally to the top of the shoulder. Two other 7.5 cm-wide bandages were applied from the olecranon under the forearm to the forearm to the top of the shoulder, with one passing anteriorly over the clavicle and the other posteriorly covering the spine of the scapula. No free space was left between the bandages.” Hanger et al. 2000: Three lengths of nonstretch Elastoplast Sports tape were used. “The two main supporting tapes were applied first. Both were applied using a lifting action, starting 5 cm above the elbow, and moving up the arm front and back, crossing at the top of the shoulder. The posterior arm tape was then anchored down past the clavicle whereas the tape from the anterior aspect of the arm came across the shoulder and down past the spine of the scapula. They were both supported at the lower end by a short tape to prevent them peeling off”.
Table 11.12 Strapping the Hemiplegic Shoulder Author, Year
Country PEDro Score
Methods Outcomes
Ancliffe 1992 Australia No Score
A pilot study of 8 patients who were assigned to receive strapping of the shoulder applied by one physiotherapist and changed every 3 to 4 days as needed to the hemiplegic side or to receive no strapping. Treatment began within 48 hours of admission to hospital.
Patients in the strapping group experienced a significantly longer pain free period than the patients who were not strapped (21 vs. 5.5 days). However, all patients in the strapping group eventually did experience pain. The longest pain-free period was 25 days.
Hanger et al. 2000 New Zealand 7 (RCT)
98 patients were randomized to have their affected shoulder strapped for 6 weeks in addition to standard physiotherapy or to receive standard physiotherapy only 15 days following stroke.
No significant differences were found between groups on measure of pain, range of movement and on functional outcome measures. There was a trend for less pain at 6 weeks and improved functional upper limb function for the strapping group.
Griffin & 33 patients at risk of developing One person in the TS group developed
11. Painful Hemiplegic Shoulder pg. 25 of 65
www.ebrsr.com
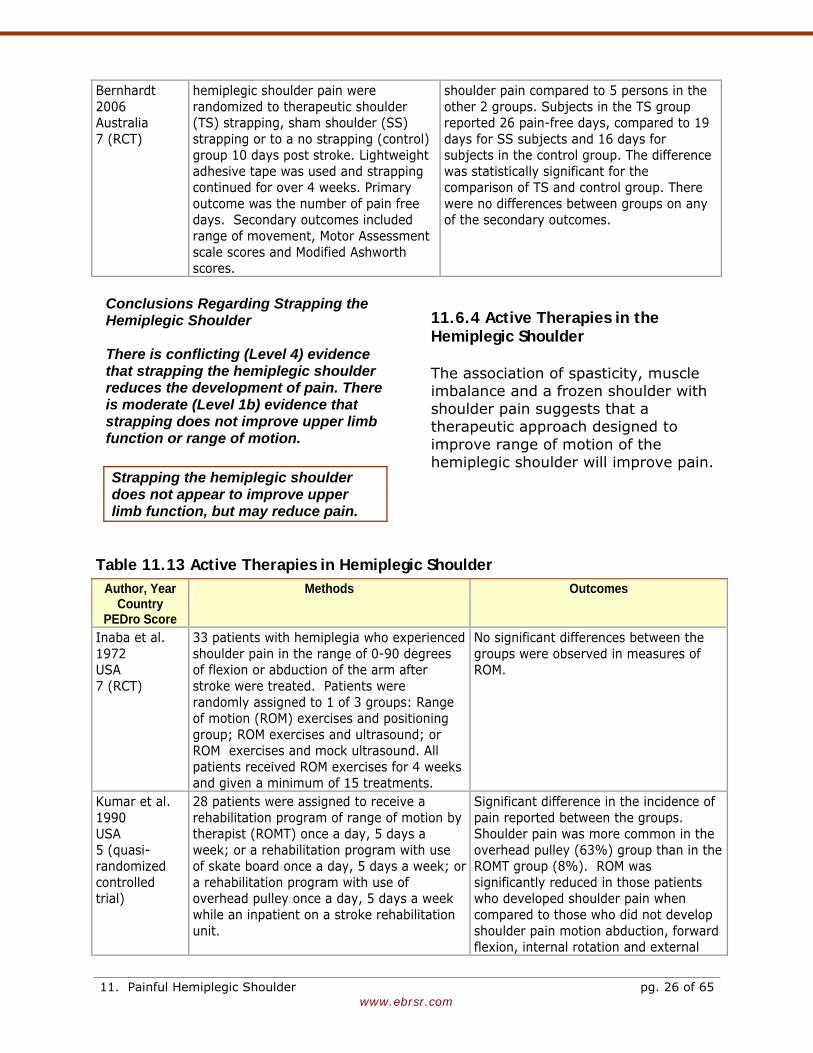
Bernhardt 2006 Australia 7 (RCT)
hemiplegic shoulder pain were randomized to therapeutic shoulder (TS) strapping, sham shoulder (SS) strapping or to a no strapping (control) group 10 days post stroke. Lightweight adhesive tape was used and strapping continued for over 4 weeks. Primary outcome was the number of pain free days. Secondary outcomes included range of movement, Motor Assessment scale scores and Modified Ashworth scores.
shoulder pain compared to 5 persons in the other 2 groups. Subjects in the TS group reported 26 pain-free days, compared to 19 days for SS subjects and 16 days for subjects in the control group. The difference was statistically significant for the comparison of TS and control group. There were no differences between groups on any of the secondary outcomes.
Conclusions Regarding Strapping the Hemiplegic Shoulder There is conflicting (Level 4) evidence that strapping the hemiplegic shoulder reduces the development of pain. There is moderate (Level 1b) evidence that strapping does not improve upper limb function or range of motion.
Strapping the hemiplegic shoulder does not appear to improve upper limb function, but may reduce pain.
11.6.4 Active Therapies in the Hemiplegic Shoulder The association of spasticity, muscle imbalance and a frozen shoulder with shoulder pain suggests that a therapeutic approach designed to improve range of motion of the hemiplegic shoulder will improve pain.
Table 11.13 Active Therapies in Hemiplegic Shoulder Author, Year
Country PEDro Score
Methods Outcomes
Inaba et al. 1972 USA 7 (RCT)
33 patients with hemiplegia who experienced shoulder pain in the range of 0-90 degrees of flexion or abduction of the arm after stroke were treated. Patients were randomly assigned to 1 of 3 groups: Range of motion (ROM) exercises and positioning group; ROM exercises and ultrasound; or ROM exercises and mock ultrasound. All patients received ROM exercises for 4 weeks and given a minimum of 15 treatments.
No significant differences between the groups were observed in measures of ROM.
Kumar et al. 1990 USA 5 (quasi-randomized controlled trial)
28 patients were assigned to receive a rehabilitation program of range of motion by therapist (ROMT) once a day, 5 days a week; or a rehabilitation program with use of skate board once a day, 5 days a week; or a rehabilitation program with use of overhead pulley once a day, 5 days a week while an inpatient on a stroke rehabilitation unit.
Significant difference in the incidence of pain reported between the groups. Shoulder pain was more common in the overhead pulley (63%) group than in the ROMT group (8%). ROM was significantly reduced in those patients who developed shoulder pain when compared to those who did not develop shoulder pain motion abduction, forward flexion, internal rotation and external
11. Painful Hemiplegic Shoulder pg. 26 of 65
www.ebrsr.com
rotation. Shoulder subluxation was found in 46% of all patients with no significant difference between treatment groups.
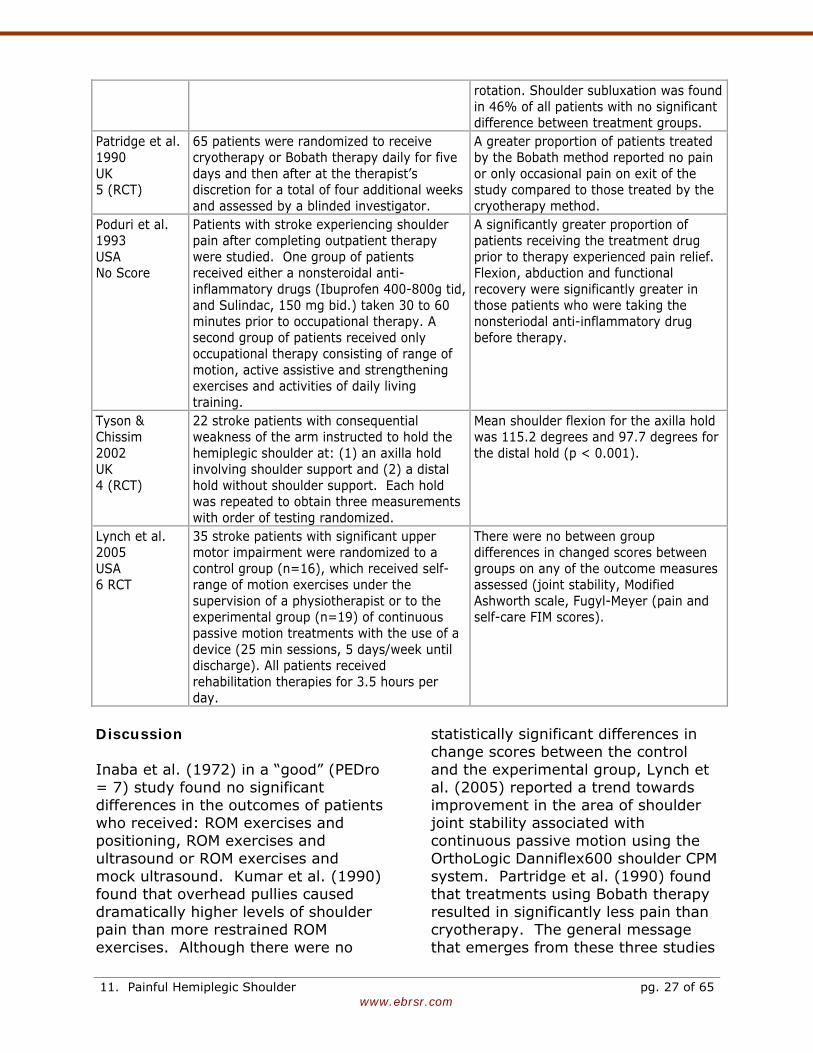
Patridge et al. 1990 UK 5 (RCT)
65 patients were randomized to receive cryotherapy or Bobath therapy daily for five days and then after at the therapist’s discretion for a total of four additional weeks and assessed by a blinded investigator.
A greater proportion of patients treated by the Bobath method reported no pain or only occasional pain on exit of the study compared to those treated by the cryotherapy method.
Poduri et al. 1993 USA No Score
Patients with stroke experiencing shoulder pain after completing outpatient therapy were studied. One group of patients received either a nonsteroidal anti-inflammatory drugs (Ibuprofen 400-800g tid, and Sulindac, 150 mg bid.) taken 30 to 60 minutes prior to occupational therapy. A second group of patients received only occupational therapy consisting of range of motion, active assistive and strengthening exercises and activities of daily living training.
A significantly greater proportion of patients receiving the treatment drug prior to therapy experienced pain relief. Flexion, abduction and functional recovery were significantly greater in those patients who were taking the nonsteriodal anti-inflammatory drug before therapy.
Tyson & Chissim 2002 UK 4 (RCT)
22 stroke patients with consequential weakness of the arm instructed to hold the hemiplegic shoulder at: (1) an axilla hold involving shoulder support and (2) a distal hold without shoulder support. Each hold was repeated to obtain three measurements with order of testing randomized.
Mean shoulder flexion for the axilla hold was 115.2 degrees and 97.7 degrees for the distal hold (p < 0.001).
Lynch et al. 2005 USA 6 RCT
35 stroke patients with significant upper motor impairment were randomized to a control group (n=16), which received self-range of motion exercises under the supervision of a physiotherapist or to the experimental group (n=19) of continuous passive motion treatments with the use of a device (25 min sessions, 5 days/week until discharge). All patients received rehabilitation therapies for 3.5 hours per day.
There were no between group differences in changed scores between groups on any of the outcome measures assessed (joint stability, Modified Ashworth scale, Fugyl-Meyer (pain and self-care FIM scores).
Discussion Inaba et al. (1972) in a “good” (PEDro = 7) study found no significant differences in the outcomes of patients who received: ROM exercises and positioning, ROM exercises and ultrasound or ROM exercises and mock ultrasound. Kumar et al. (1990) found that overhead pullies caused dramatically higher levels of shoulder pain than more restrained ROM exercises. Although there were no
statistically significant differences in change scores between the control and the experimental group, Lynch et al. (2005) reported a trend towards improvement in the area of shoulder joint stability associated with continuous passive motion using the OrthoLogic Danniflex600 shoulder CPM system. Partridge et al. (1990) found that treatments using Bobath therapy resulted in significantly less pain than cryotherapy. The general message that emerges from these three studies
11. Painful Hemiplegic Shoulder pg. 27 of 65

www.ebrsr.com
is that an active ROM exercise approach is preferable to more passive modalities but an overly aggressive approach (i.e. overhead pullies) resulted in a very high incidence of hemiplegic shoulder pain when compared to a gentler approach.
Conclusions Regarding Active Therapies in the Hemiplegic Shoulder There is moderate (Level 1b) evidence that aggressive range of motion therapies, using overhead pullies results in increased rates of shoulder pain. There is moderate (Level 1b) evidence that Bobath therapy for the hemiplegic shoulder is associated with greater pain reduction than passive cryotherapy (application of local cold therapy). There is moderate (Level 1b) evidence that gentle exercises to improve range of motion are the preferred approach. There is moderate (Level 1b) evidence that adding ultrasound therapy to range of motion exercises does not change outcomes. There is limited (Level 2) evidence that providing an oral nonsteriodal anti-inflammatory drug leads to less pain, improved range of motion and improved functional recovery in stroke patients with shoulder pain receiving occupational therapy. There is moderate (Level 1b) evidence that static positional stretches performed daily during rehabilitation are associated with increasing pain and decreasing range of motion.
Aggressive range of motion exercises (i.e. pullies) results in a markedly increased incidence of painful shoulder; a gentler range of motion program is preferred. Adding ultrasound treatments is not helpful while NSAIDs may be helpful.
11.6.6 Electrical Stimulation in the Hemiplegic Shoulder Electrical neuromuscular stimulation is a term used to describe the application of electrical current to the skin, or directly into muscle that stimulates motor nerves and muscle fibres resulting in improved contractility and greater muscle bulk. The treatment can be used to improve muscle strength, joint misalignment, muscle tone, sensory deficits and self-reported pain intensity (Price & Pandyan, 2000). Electrical stimulation is typically administered by two methods, functional electrical stimulation (FES) or transcutaneous electrical nerve stimulation (TENS). The distinction that is usually made between these two forms of treatment is that lower intensity, higher frequency stimulation is associated with TENS. It is more commonly used to treat pain. Patients usually describe a “pins-and-needles sensation.” FES has been described as “bursts of electrical stimulation applied to the nerves or muscles affected by the stroke, with the goal of strengthening muscle contraction and improving motor control.” (Gresham et al. 1995). The supraspinatus and posterior deltoid muscles are most likely to be treated as they are important muscles in maintaining the correct alignment of the glenohumeral joint (Paci et al. 2005). Theoretically, FES should help to compensate or facilitate flaccid shoulder muscles, which in turn
11. Painful Hemiplegic Shoulder pg. 28 of 65
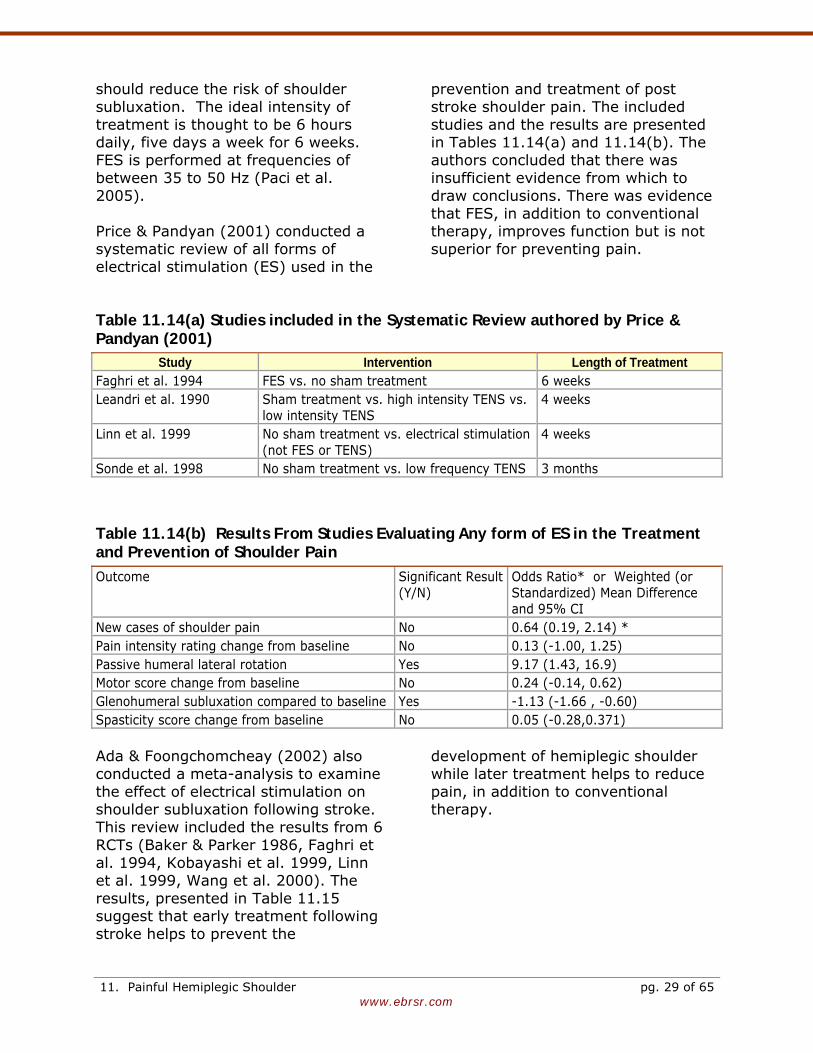
www.ebrsr.com
should reduce the risk of shoulder subluxation. The ideal intensity of treatment is thought to be 6 hours daily, five days a week for 6 weeks. FES is performed at frequencies of between 35 to 50 Hz (Paci et al. 2005). Price & Pandyan (2001) conducted a systematic review of all forms of electrical stimulation (ES) used in the
prevention and treatment of post stroke shoulder pain. The included studies and the results are presented in Tables 11.14(a) and 11.14(b). The authors concluded that there was insufficient evidence from which to draw conclusions. There was evidence that FES, in addition to conventional therapy, improves function but is not superior for preventing pain.
Table 11.14(a) Studies included in the Systematic Review authored by Price & Pandyan (2001)
Study Intervention Length of Treatment Faghri et al. 1994 FES vs. no sham treatment 6 weeks Leandri et al. 1990 Sham treatment vs. high intensity TENS vs.
low intensity TENS 4 weeks
Linn et al. 1999 No sham treatment vs. electrical stimulation (not FES or TENS)
4 weeks
Sonde et al. 1998 No sham treatment vs. low frequency TENS 3 months
Table 11.14(b) Results From Studies Evaluating Any form of ES in the Treatment and Prevention of Shoulder Pain Outcome Significant Result
(Y/N) Odds Ratio* or Weighted (or Standardized) Mean Difference and 95% CI
New cases of shoulder pain No 0.64 (0.19, 2.14) * Pain intensity rating change from baseline No 0.13 (-1.00, 1.25) Passive humeral lateral rotation Yes 9.17 (1.43, 16.9) Motor score change from baseline No 0.24 (-0.14, 0.62) Glenohumeral subluxation compared to baseline Yes -1.13 (-1.66 , -0.60) Spasticity score change from baseline No 0.05 (-0.28,0.371) Ada & Foongchomcheay (2002) also conducted a meta-analysis to examine the effect of electrical stimulation on shoulder subluxation following stroke. This review included the results from 6 RCTs (Baker & Parker 1986, Faghri et al. 1994, Kobayashi et al. 1999, Linn et al. 1999, Wang et al. 2000). The results, presented in Table 11.15 suggest that early treatment following stroke helps to prevent the
development of hemiplegic shoulder while later treatment helps to reduce pain, in addition to conventional therapy.
11. Painful Hemiplegic Shoulder pg. 29 of 65
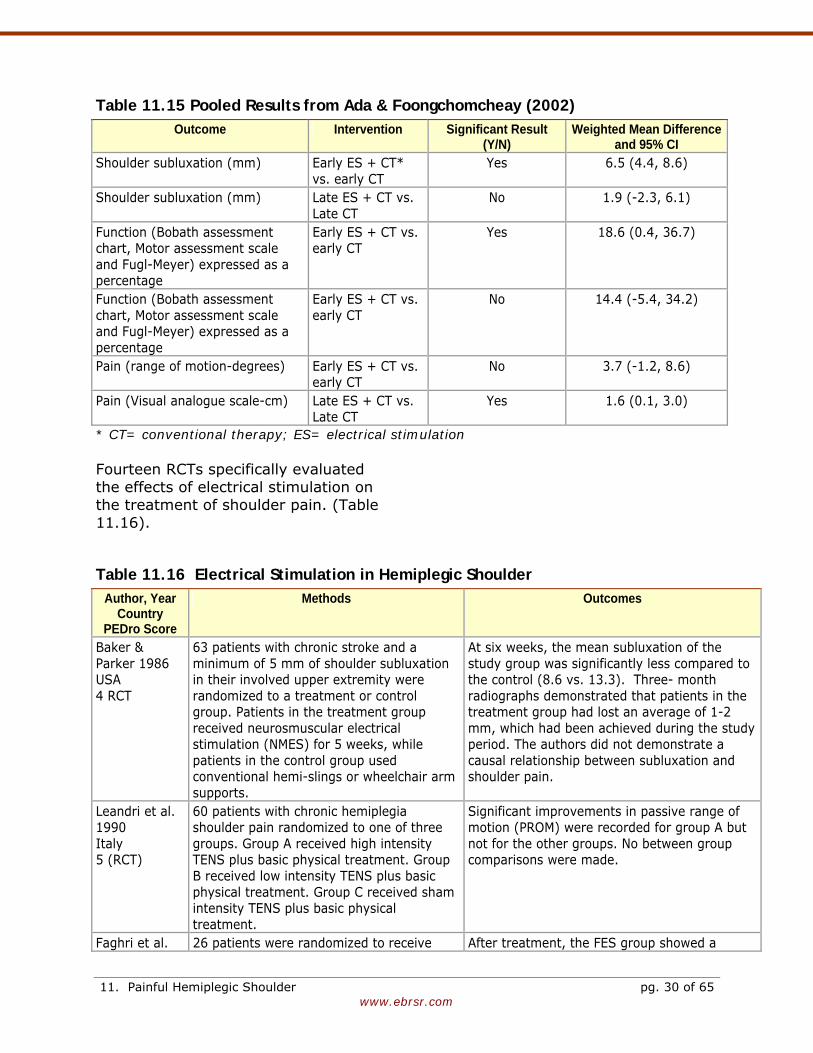
www.ebrsr.com
Table 11.15 Pooled Results from Ada & Foongchomcheay (2002) Outcome Intervention Significant Result
(Y/N) Weighted Mean Difference
and 95% CI Shoulder subluxation (mm)
Early ES + CT* vs. early CT
Yes 6.5 (4.4, 8.6)
Shoulder subluxation (mm) Late ES + CT vs. Late CT
No 1.9 (-2.3, 6.1)
Function (Bobath assessment chart, Motor assessment scale and Fugl-Meyer) expressed as a percentage
Early ES + CT vs. early CT
Yes 18.6 (0.4, 36.7)
Function (Bobath assessment chart, Motor assessment scale and Fugl-Meyer) expressed as a percentage
Early ES + CT vs. early CT
No 14.4 (-5.4, 34.2)
Pain (range of motion-degrees) Early ES + CT vs. early CT
No 3.7 (-1.2, 8.6)
Pain (Visual analogue scale-cm) Late ES + CT vs. Late CT
Yes 1.6 (0.1, 3.0)
* CT= conventional therapy; ES= electrical stimulation Fourteen RCTs specifically evaluated the effects of electrical stimulation on the treatment of shoulder pain. (Table 11.16).
Table 11.16 Electrical Stimulation in Hemiplegic Shoulder Author, Year
Country PEDro Score
Methods Outcomes
Baker & Parker 1986 USA 4 RCT
63 patients with chronic stroke and a minimum of 5 mm of shoulder subluxation in their involved upper extremity were randomized to a treatment or control group. Patients in the treatment group received neurosmuscular electrical stimulation (NMES) for 5 weeks, while patients in the control group used conventional hemi-slings or wheelchair arm supports.
At six weeks, the mean subluxation of the study group was significantly less compared to the control (8.6 vs. 13.3). Three- month radiographs demonstrated that patients in the treatment group had lost an average of 1-2 mm, which had been achieved during the study period. The authors did not demonstrate a causal relationship between subluxation and shoulder pain.
Leandri et al. 1990 Italy 5 (RCT)
60 patients with chronic hemiplegia shoulder pain randomized to one of three groups. Group A received high intensity TENS plus basic physical treatment. Group B received low intensity TENS plus basic physical treatment. Group C received sham intensity TENS plus basic physical treatment.
Significant improvements in passive range of motion (PROM) were recorded for group A but not for the other groups. No between group comparisons were made.
Faghri et al. 26 patients were randomized to receive After treatment, the FES group showed a
11. Painful Hemiplegic Shoulder pg. 30 of 65
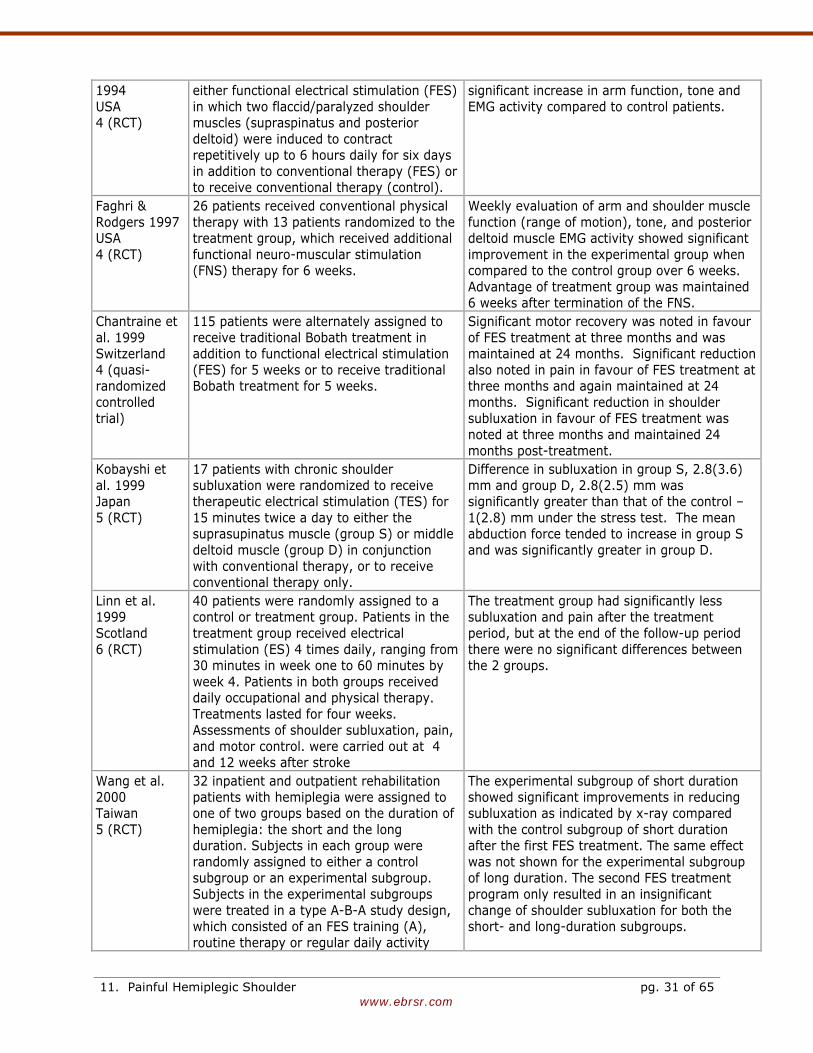
www.ebrsr.com
1994 USA 4 (RCT)
either functional electrical stimulation (FES) in which two flaccid/paralyzed shoulder muscles (supraspinatus and posterior deltoid) were induced to contract repetitively up to 6 hours daily for six days in addition to conventional therapy (FES) or to receive conventional therapy (control).
significant increase in arm function, tone and EMG activity compared to control patients.
Faghri & Rodgers 1997 USA 4 (RCT)
26 patients received conventional physical therapy with 13 patients randomized to the treatment group, which received additional functional neuro-muscular stimulation (FNS) therapy for 6 weeks.
Weekly evaluation of arm and shoulder muscle function (range of motion), tone, and posterior deltoid muscle EMG activity showed significant improvement in the experimental group when compared to the control group over 6 weeks. Advantage of treatment group was maintained 6 weeks after termination of the FNS.
Chantraine et al. 1999 Switzerland 4 (quasi-randomized controlled trial)
115 patients were alternately assigned to receive traditional Bobath treatment in addition to functional electrical stimulation (FES) for 5 weeks or to receive traditional Bobath treatment for 5 weeks.
Significant motor recovery was noted in favour of FES treatment at three months and was maintained at 24 months. Significant reduction also noted in pain in favour of FES treatment at three months and again maintained at 24 months. Significant reduction in shoulder subluxation in favour of FES treatment was noted at three months and maintained 24 months post-treatment.
Kobayshi et al. 1999 Japan 5 (RCT)
17 patients with chronic shoulder subluxation were randomized to receive therapeutic electrical stimulation (TES) for 15 minutes twice a day to either the suprasupinatus muscle (group S) or middle deltoid muscle (group D) in conjunction with conventional therapy, or to receive conventional therapy only.
Difference in subluxation in group S, 2.8(3.6) mm and group D, 2.8(2.5) mm was significantly greater than that of the control –1(2.8) mm under the stress test. The mean abduction force tended to increase in group S and was significantly greater in group D.
Linn et al. 1999 Scotland 6 (RCT)
40 patients were randomly assigned to a control or treatment group. Patients in the treatment group received electrical stimulation (ES) 4 times daily, ranging from 30 minutes in week one to 60 minutes by week 4. Patients in both groups received daily occupational and physical therapy. Treatments lasted for four weeks. Assessments of shoulder subluxation, pain, and motor control. were carried out at 4 and 12 weeks after stroke
The treatment group had significantly less subluxation and pain after the treatment period, but at the end of the follow-up period there were no significant differences between the 2 groups.
Wang et al. 2000 Taiwan 5 (RCT)
32 inpatient and outpatient rehabilitation patients with hemiplegia were assigned to one of two groups based on the duration of hemiplegia: the short and the long duration. Subjects in each group were randomly assigned to either a control subgroup or an experimental subgroup. Subjects in the experimental subgroups were treated in a type A-B-A study design, which consisted of an FES training (A), routine therapy or regular daily activity
The experimental subgroup of short duration showed significant improvements in reducing subluxation as indicated by x-ray compared with the control subgroup of short duration after the first FES treatment. The same effect was not shown for the experimental subgroup of long duration. The second FES treatment program only resulted in an insignificant change of shoulder subluxation for both the short- and long-duration subgroups.
11. Painful Hemiplegic Shoulder pg. 31 of 65
www.ebrsr.com
without FES training (B), and another FES training (A). Each period lasted for 6 wk. FES training program, consisted of five sessions/week.
Yu et al. 2001 USA 6 (RCT)
10 hemiplegic stroke patients with at least 1 fingerbreadth of glenohumeral subluxation received 3 randomly ordered pairs of neuromuscular stimulation (NMES) to the suprasinatus and poterior deltoid muscles of the subluxated shoulder. The stimulation types were percutaneous-NMES (perc-NMES) and transcutaneous-NMES (trans-NMES). After each stimulation pain was evaluated with the visual analog scale (VAS) and the McGill Pain Questionnaire (MPQ).
Pain scores were significantly lower for perc-NMES than trans-NMES as assessed by the VAS and the MPQ.
Renzenbrink & Ijerman 2004 Netherlands No Score
15 stroke survivors with chronic (> six months) hemiplegia and a therapy-resistant painful shoulder with subluxation were studied. Shoulder subluxation was indicated by at least 1/2 fingerbreadth of glenohumeral separation on palpation. Patients received 6 hours of Percutaneous Neuromuscular electrical stimulation (P-NMES) per day for a total of six weeks.
A significant reduction in pain was found on the Brief Pain Inventory. Pain reduction was still present at six months follow-up. All domains, in particular bodily pain, of the SF-36 showed improvement in the short term. After six months of follow-up, bodily pain was still strongly and significantly reduced, whereas social functioning and role physical demonstrated a nonsignificant improvement of more than 10% compared with baseline.
Yu et al. 2004 USA 7 (RCT)
7 site, single-blinded, randomized clinical trial. 61 chronic stroke survivors with shoulder pain and subluxation volunteered to be randomized to receive intramuscular neuromuscular electric stimulation (NMES) to the supraspinatus, posterior deltoid, middle deltoid, and trapezius for 6 hours a day for 6 weeks or to the control condition of a cuff-type sling for 6 weeks. Main outcome measure Brief Pain Inventory question.
The main outcome measure was the Pain outcome measure Brief Pain Inventory question 12 (BPI 12), an 11-point numeric rating scale, assessed at the end of treatment, and at 3 and 6 months post treatment. Post stroke shoulder pain was significantly less in the NMES group compared to control at 3 and 6 months following treatment.
Chae et al. 2005 USA 7 (RCT)
12 month follow up from Yu et al. 2004. Treatment success was defined as a minimum 2-point reduction in Brief Pain Inventory question 12 at all post treatment assessments. Secondary measures included pain-related quality of life (Brief Pain Inventory question 23), subluxation, motor impairment, range of motion, spasticity, and activity limitation.
22 patients in the intervention group and 21 patients received 12-month assessments. The electrical stimulation group exhibited a significantly higher success rate than controls (63% vs. 21%). Repeated-measure analysis of variance revealed significant treatment effects on post treatment Brief Pain Inventory questions 12 and 23. There were no other significant between group differences.
Church et al. 2006 UK 9 (RCT)
176 stroke patients (≤10 days post-stroke) were randomly assigned to receive surface neuromuscular electrical stimulation (sNMES) or placebo with a sham stimulator for 4 weeks. Both groups received standard stroke unit care. One and 3-month assessments included Action Research Arm
There was no significant difference in the ARAT scores, the primary outcome, between groups. There were no other significant differences between the groups with the exception of: the gross and grasp subsections of the ARAT, the arm section of the MI and the Frenchay Arm Test, where the control group fared better at 3
11. Painful Hemiplegic Shoulder pg. 32 of 65
www.ebrsr.com
Test (ARAT), Frenchay Arm Test, Motricity Index (MI), Star Cancellation Test, pain scales, disability, global health status, and Oxford Handicap Scale.
months.
Chae et al. 2007 USA 7 (RCT)
Secondary analyses from Yu et al. 2004 & Chae et al. 2005. Forward stepwise regression was used to identify factors predictive of treatment success among participants assigned to the electrical stimulation group. Treatment success was defined as at least a 2-point reduction on the Brief Pain Inventory Question 12 at 12 months following treatment.
Time from stroke onset was most predictive of treatment success. Subjects were divided according to the median value of stroke onset: early (<77 weeks) versus late (> 77 weeks). Electrical stimulation was effective in reducing poststroke shoulder pain for the early group (94% vs 7%, p < .001) but not for the late group (31% vs 33%). FIM score was the second strongest predictor. Factors which were not predictive included age, stroke type, gender, Fugl-Meyer score and side of hemiplegia.
Fil et al. 2010 Turkey 5 (RCT)
48 patients admitted to hospital within 2 days of acute stroke were randomized to receive either rehabilitation according to Bobath concepts or Bobath-based therapy + high-voltage pulsed galvanic stimulation of the supraspinatus and deltoid muscles for 10 min, 2 x/day for the duration of the hospital stay. Outcomes were assessed before and after treatment. Two radiological methods were used to measure the horizontal, vertical and total asymmetry and vertical distance values of the shoulder joint. Motor functions of the arm were evaluated with the Motor Assessment Scale.
Patients remained in hospital and received treatment for an average of 12 days. Shoulder subluxation occurred in 9 (37.5%) subjects in the control group, whereas it was not observed in the study group. All shoulder joint displacement values were higher in the control group than in the study group (horizontal asymmetry P = 0.0001, vertical asymmetry P = 0.0001, total asymmetry P = 0.0001, vertical range P = 0.002.
Koyuncu et al. 2010 Turkey 4 (RCT)
50 rehabilitation inpatients with shoulder subluxation and shoulder pain were randomized to receive a 4-week treatment of conventional rehab or conventional rehab + 20 sessions of FES (1 hr/day x 5 days/wk, frequency 36 Hz) to the supraspinatus and posterior deltoid muscles. The shoulder pain of all patients during resting, passive range of motion (PROM) and active range of motion (AROM) was measured with the visual analog scale (VAS) while the shoulder subluxation levels were evaluated with the classification developed by Van Langenberghe and by using the millimetric measurements on anteroposterior shoulder X-ray before and after the physical treatment and rehabilitation program and compared.
There were no significant between group differences in terms of pain, PROM or AROM. However, there was a significant difference between the two groups for the amount of change in shoulder subluxation in favor of the study group.
Discussion Most of the RCTs reviewed reported a benefit associated with electrical
stimulation, although there was variability in the outcomes assessed: range of motion, muscle tone, EMG
11. Painful Hemiplegic Shoulder pg. 33 of 65
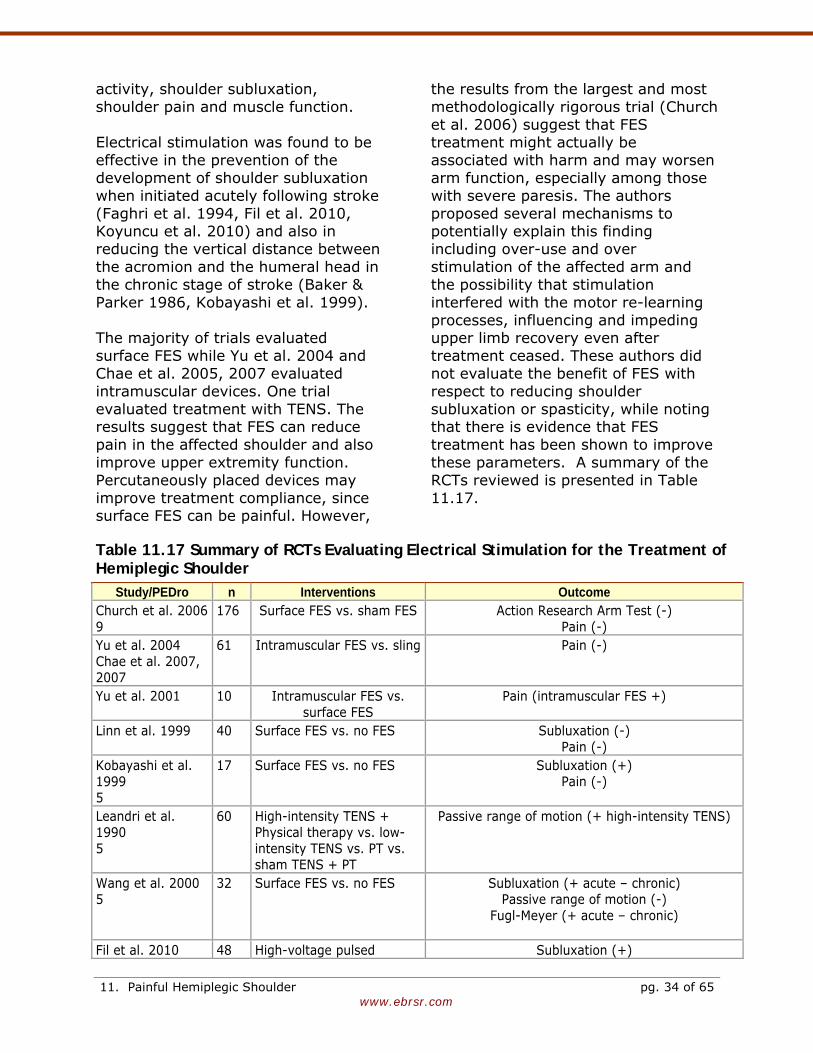
www.ebrsr.com
activity, shoulder subluxation, shoulder pain and muscle function. Electrical stimulation was found to be effective in the prevention of the development of shoulder subluxation when initiated acutely following stroke (Faghri et al. 1994, Fil et al. 2010, Koyuncu et al. 2010) and also in reducing the vertical distance between the acromion and the humeral head in the chronic stage of stroke (Baker & Parker 1986, Kobayashi et al. 1999). The majority of trials evaluated surface FES while Yu et al. 2004 and Chae et al. 2005, 2007 evaluated intramuscular devices. One trial evaluated treatment with TENS. The results suggest that FES can reduce pain in the affected shoulder and also improve upper extremity function. Percutaneously placed devices may improve treatment compliance, since surface FES can be painful. However,
the results from the largest and most methodologically rigorous trial (Church et al. 2006) suggest that FES treatment might actually be associated with harm and may worsen arm function, especially among those with severe paresis. The authors proposed several mechanisms to potentially explain this finding including over-use and over stimulation of the affected arm and the possibility that stimulation interfered with the motor re-learning processes, influencing and impeding upper limb recovery even after treatment ceased. These authors did not evaluate the benefit of FES with respect to reducing shoulder subluxation or spasticity, while noting that there is evidence that FES treatment has been shown to improve these parameters. A summary of the RCTs reviewed is presented in Table 11.17.
Table 11.17 Summary of RCTs Evaluating Electrical Stimulation for the Treatment of Hemiplegic Shoulder
Study/PEDro n Interventions Outcome Church et al. 2006 9
176 Surface FES vs. sham FES Action Research Arm Test (-) Pain (-)
Yu et al. 2004 Chae et al. 2007, 2007
61 Intramuscular FES vs. sling Pain (-)
Yu et al. 2001 10 Intramuscular FES vs. surface FES
Pain (intramuscular FES +)
Linn et al. 1999 40 Surface FES vs. no FES Subluxation (-) Pain (-)
Kobayashi et al. 1999 5
17 Surface FES vs. no FES Subluxation (+) Pain (-)
Leandri et al. 1990 5
60 High-intensity TENS + Physical therapy vs. low-intensity TENS vs. PT vs. sham TENS + PT
Passive range of motion (+ high-intensity TENS)
Wang et al. 2000 5
32 Surface FES vs. no FES Subluxation (+ acute – chronic) Passive range of motion (-)
Fugl-Meyer (+ acute – chronic)
Fil et al. 2010 48 High-voltage pulsed Subluxation (+)
11. Painful Hemiplegic Shoulder pg. 34 of 65
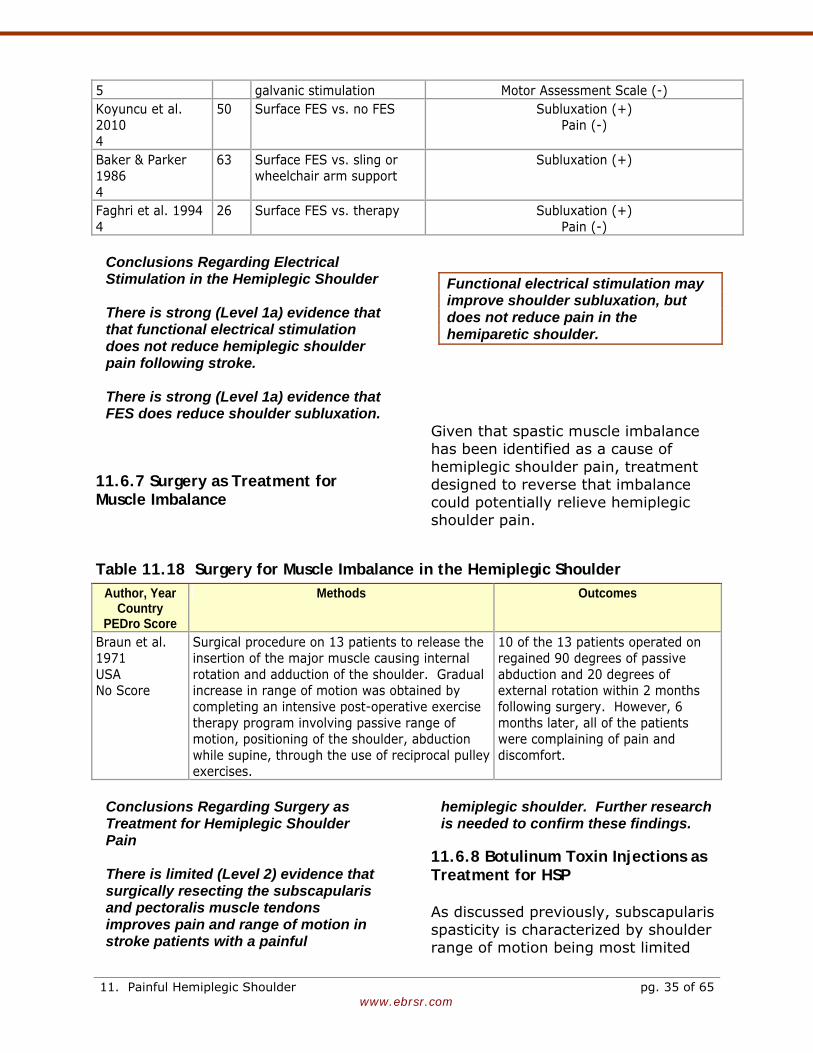
www.ebrsr.com
5 galvanic stimulation Motor Assessment Scale (-) Koyuncu et al. 2010 4
50 Surface FES vs. no FES Subluxation (+) Pain (-)
Baker & Parker 1986 4
63 Surface FES vs. sling or wheelchair arm support
Subluxation (+)
Faghri et al. 1994 4
26 Surface FES vs. therapy Subluxation (+) Pain (-)
Conclusions Regarding Electrical Stimulation in the Hemiplegic Shoulder There is strong (Level 1a) evidence that that functional electrical stimulation does not reduce hemiplegic shoulder pain following stroke.
There is strong (Level 1a) evidence that FES does reduce shoulder subluxation.
Functional electrical stimulation may improve shoulder subluxation, but does not reduce pain in the hemiparetic shoulder.
11.6.7 Surgery as Treatment for Muscle Imbalance
Given that spastic muscle imbalance has been identified as a cause of hemiplegic shoulder pain, treatment designed to reverse that imbalance could potentially relieve hemiplegic shoulder pain.
Table 11.18 Surgery for Muscle Imbalance in the Hemiplegic Shoulder Author, Year
Country PEDro Score
Methods Outcomes
Braun et al. 1971 USA No Score
Surgical procedure on 13 patients to release the insertion of the major muscle causing internal rotation and adduction of the shoulder. Gradual increase in range of motion was obtained by completing an intensive post-operative exercise therapy program involving passive range of motion, positioning of the shoulder, abduction while supine, through the use of reciprocal pulley exercises.
10 of the 13 patients operated on regained 90 degrees of passive abduction and 20 degrees of external rotation within 2 months following surgery. However, 6 months later, all of the patients were complaining of pain and discomfort.
Conclusions Regarding Surgery as Treatment for Hemiplegic Shoulder Pain There is limited (Level 2) evidence that surgically resecting the subscapularis and pectoralis muscle tendons improves pain and range of motion in stroke patients with a painful
hemiplegic shoulder. Further research is needed to confirm these findings.
11.6.8 Botulinum Toxin Injections as Treatment for HSP As discussed previously, subscapularis spasticity is characterized by shoulder range of motion being most limited
11. Painful Hemiplegic Shoulder pg. 35 of 65
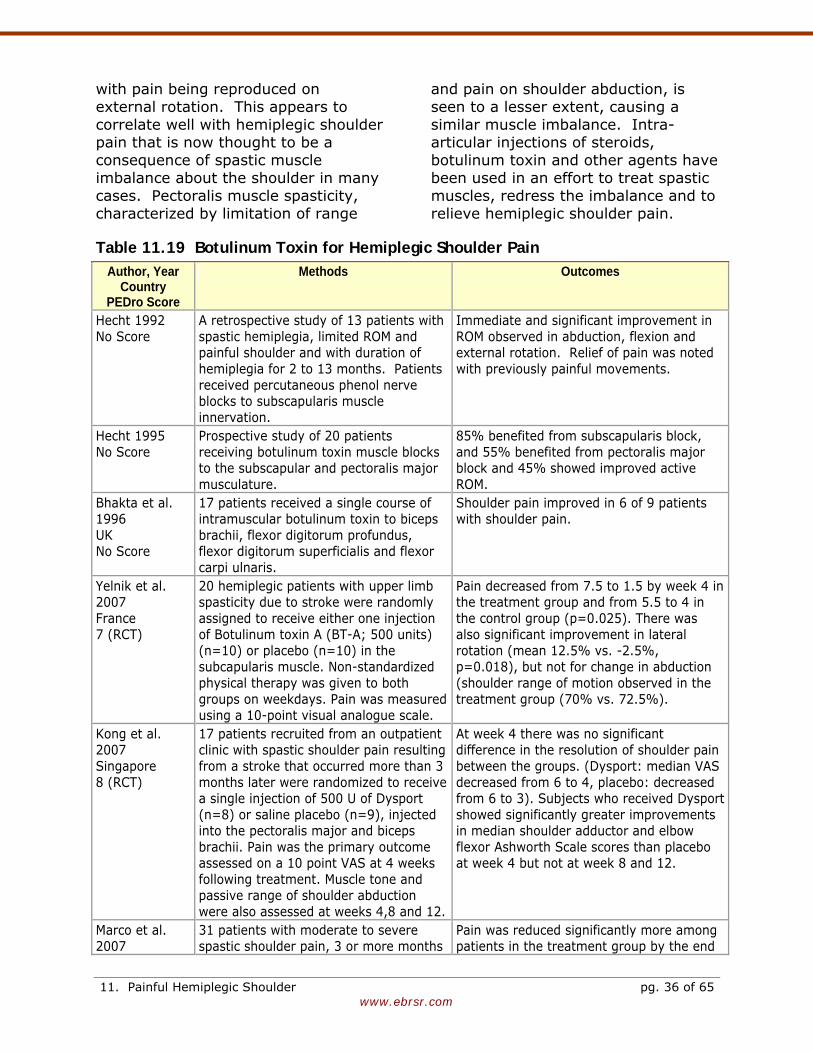
www.ebrsr.com
with pain being reproduced on external rotation. This appears to correlate well with hemiplegic shoulder pain that is now thought to be a consequence of spastic muscle imbalance about the shoulder in many cases. Pectoralis muscle spasticity, characterized by limitation of range
and pain on shoulder abduction, is seen to a lesser extent, causing a similar muscle imbalance. Intra-articular injections of steroids, botulinum toxin and other agents have been used in an effort to treat spastic muscles, redress the imbalance and to relieve hemiplegic shoulder pain.
Table 11.19 Botulinum Toxin for Hemiplegic Shoulder Pain Author, Year
Country PEDro Score
Methods Outcomes
Hecht 1992 No Score
A retrospective study of 13 patients with spastic hemiplegia, limited ROM and painful shoulder and with duration of hemiplegia for 2 to 13 months. Patients received percutaneous phenol nerve blocks to subscapularis muscle innervation.
Immediate and significant improvement in ROM observed in abduction, flexion and external rotation. Relief of pain was noted with previously painful movements.
Hecht 1995 No Score
Prospective study of 20 patients receiving botulinum toxin muscle blocks to the subscapular and pectoralis major musculature.
85% benefited from subscapularis block, and 55% benefited from pectoralis major block and 45% showed improved active ROM.
Bhakta et al. 1996 UK No Score
17 patients received a single course of intramuscular botulinum toxin to biceps brachii, flexor digitorum profundus, flexor digitorum superficialis and flexor carpi ulnaris.
Shoulder pain improved in 6 of 9 patients with shoulder pain.
Yelnik et al. 2007 France 7 (RCT)
20 hemiplegic patients with upper limb spasticity due to stroke were randomly assigned to receive either one injection of Botulinum toxin A (BT-A; 500 units) (n=10) or placebo (n=10) in the subcapularis muscle. Non-standardized physical therapy was given to both groups on weekdays. Pain was measured using a 10-point visual analogue scale.
Pain decreased from 7.5 to 1.5 by week 4 in the treatment group and from 5.5 to 4 in the control group (p=0.025). There was also significant improvement in lateral rotation (mean 12.5% vs. -2.5%, p=0.018), but not for change in abduction (shoulder range of motion observed in the treatment group (70% vs. 72.5%).
Kong et al. 2007 Singapore 8 (RCT)
17 patients recruited from an outpatient clinic with spastic shoulder pain resulting from a stroke that occurred more than 3 months later were randomized to receive a single injection of 500 U of Dysport (n=8) or saline placebo (n=9), injected into the pectoralis major and biceps brachii. Pain was the primary outcome assessed on a 10 point VAS at 4 weeks following treatment. Muscle tone and passive range of shoulder abduction were also assessed at weeks 4,8 and 12.
At week 4 there was no significant difference in the resolution of shoulder pain between the groups. (Dysport: median VAS decreased from 6 to 4, placebo: decreased from 6 to 3). Subjects who received Dysport showed significantly greater improvements in median shoulder adductor and elbow flexor Ashworth Scale scores than placebo at week 4 but not at week 8 and 12.
Marco et al. 2007
31 patients with moderate to severe spastic shoulder pain, 3 or more months
Pain was reduced significantly more among patients in the treatment group by the end
11. Painful Hemiplegic Shoulder pg. 36 of 65
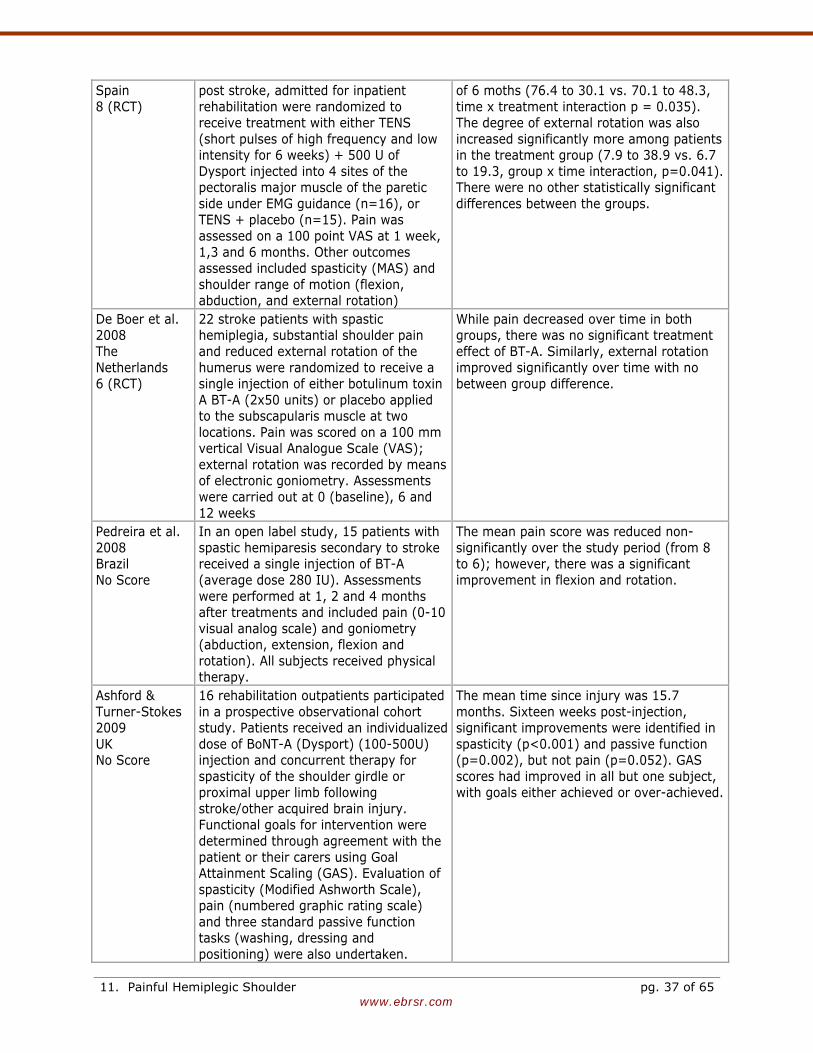
www.ebrsr.com
Spain 8 (RCT)
post stroke, admitted for inpatient rehabilitation were randomized to receive treatment with either TENS (short pulses of high frequency and low intensity for 6 weeks) + 500 U of Dysport injected into 4 sites of the pectoralis major muscle of the paretic side under EMG guidance (n=16), or TENS + placebo (n=15). Pain was assessed on a 100 point VAS at 1 week, 1,3 and 6 months. Other outcomes assessed included spasticity (MAS) and shoulder range of motion (flexion, abduction, and external rotation)
of 6 moths (76.4 to 30.1 vs. 70.1 to 48.3, time x treatment interaction p = 0.035). The degree of external rotation was also increased significantly more among patients in the treatment group (7.9 to 38.9 vs. 6.7 to 19.3, group x time interaction, p=0.041). There were no other statistically significant differences between the groups.
De Boer et al. 2008 The Netherlands 6 (RCT)
22 stroke patients with spastic hemiplegia, substantial shoulder pain and reduced external rotation of the humerus were randomized to receive a single injection of either botulinum toxin A BT-A (2x50 units) or placebo applied to the subscapularis muscle at two locations. Pain was scored on a 100 mm vertical Visual Analogue Scale (VAS); external rotation was recorded by means of electronic goniometry. Assessments were carried out at 0 (baseline), 6 and 12 weeks
While pain decreased over time in both groups, there was no significant treatment effect of BT-A. Similarly, external rotation improved significantly over time with no between group difference.
Pedreira et al. 2008 Brazil No Score
In an open label study, 15 patients with spastic hemiparesis secondary to stroke received a single injection of BT-A (average dose 280 IU). Assessments were performed at 1, 2 and 4 months after treatments and included pain (0-10 visual analog scale) and goniometry (abduction, extension, flexion and rotation). All subjects received physical therapy.
The mean pain score was reduced non-significantly over the study period (from 8 to 6); however, there was a significant improvement in flexion and rotation.
Ashford & Turner-Stokes 2009 UK No Score
16 rehabilitation outpatients participated in a prospective observational cohort study. Patients received an individualized dose of BoNT-A (Dysport) (100-500U) injection and concurrent therapy for spasticity of the shoulder girdle or proximal upper limb following stroke/other acquired brain injury. Functional goals for intervention were determined through agreement with the patient or their carers using Goal Attainment Scaling (GAS). Evaluation of spasticity (Modified Ashworth Scale), pain (numbered graphic rating scale) and three standard passive function tasks (washing, dressing and positioning) were also undertaken.
The mean time since injury was 15.7 months. Sixteen weeks post-injection, significant improvements were identified in spasticity (p<0.001) and passive function (p=0.002), but not pain (p=0.052). GAS scores had improved in all but one subject, with goals either achieved or over-achieved.
11. Painful Hemiplegic Shoulder pg. 37 of 65
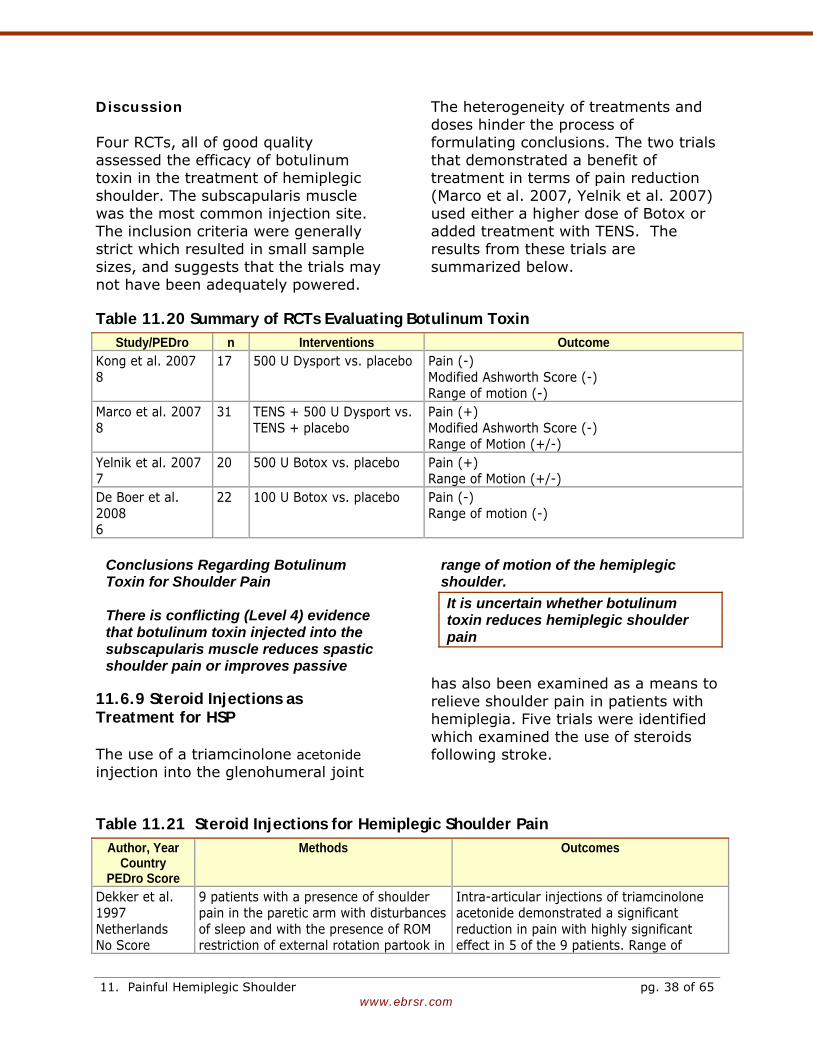
www.ebrsr.com
Discussion Four RCTs, all of good quality assessed the efficacy of botulinum toxin in the treatment of hemiplegic shoulder. The subscapularis muscle was the most common injection site. The inclusion criteria were generally strict which resulted in small sample sizes, and suggests that the trials may not have been adequately powered.
The heterogeneity of treatments and doses hinder the process of formulating conclusions. The two trials that demonstrated a benefit of treatment in terms of pain reduction (Marco et al. 2007, Yelnik et al. 2007) used either a higher dose of Botox or added treatment with TENS. The results from these trials are summarized below.
Table 11.20 Summary of RCTs Evaluating Botulinum Toxin Study/PEDro n Interventions Outcome
Kong et al. 2007 8
17 500 U Dysport vs. placebo Pain (-) Modified Ashworth Score (-) Range of motion (-)
Marco et al. 2007 8
31 TENS + 500 U Dysport vs. TENS + placebo
Pain (+) Modified Ashworth Score (-) Range of Motion (+/-)
Yelnik et al. 2007 7
20 500 U Botox vs. placebo Pain (+) Range of Motion (+/-)
De Boer et al. 2008 6
22 100 U Botox vs. placebo Pain (-) Range of motion (-)
Conclusions Regarding Botulinum Toxin for Shoulder Pain There is conflicting (Level 4) evidence that botulinum toxin injected into the subscapularis muscle reduces spastic shoulder pain or improves passive
range of motion of the hemiplegic shoulder. It is uncertain whether botulinum toxin reduces hemiplegic shoulder pain
11.6.9 Steroid Injections as Treatment for HSP The use of a triamcinolone acetonide injection into the glenohumeral joint
has also been examined as a means to relieve shoulder pain in patients with hemiplegia. Five trials were identified which examined the use of steroids following stroke.
Table 11.21 Steroid Injections for Hemiplegic Shoulder Pain Author, Year
Country PEDro Score
Methods Outcomes
Dekker et al. 1997 Netherlands No Score
9 patients with a presence of shoulder pain in the paretic arm with disturbances of sleep and with the presence of ROM restriction of external rotation partook in
Intra-articular injections of triamcinolone acetonide demonstrated a significant reduction in pain with highly significant effect in 5 of the 9 patients. Range of
11. Painful Hemiplegic Shoulder pg. 38 of 65
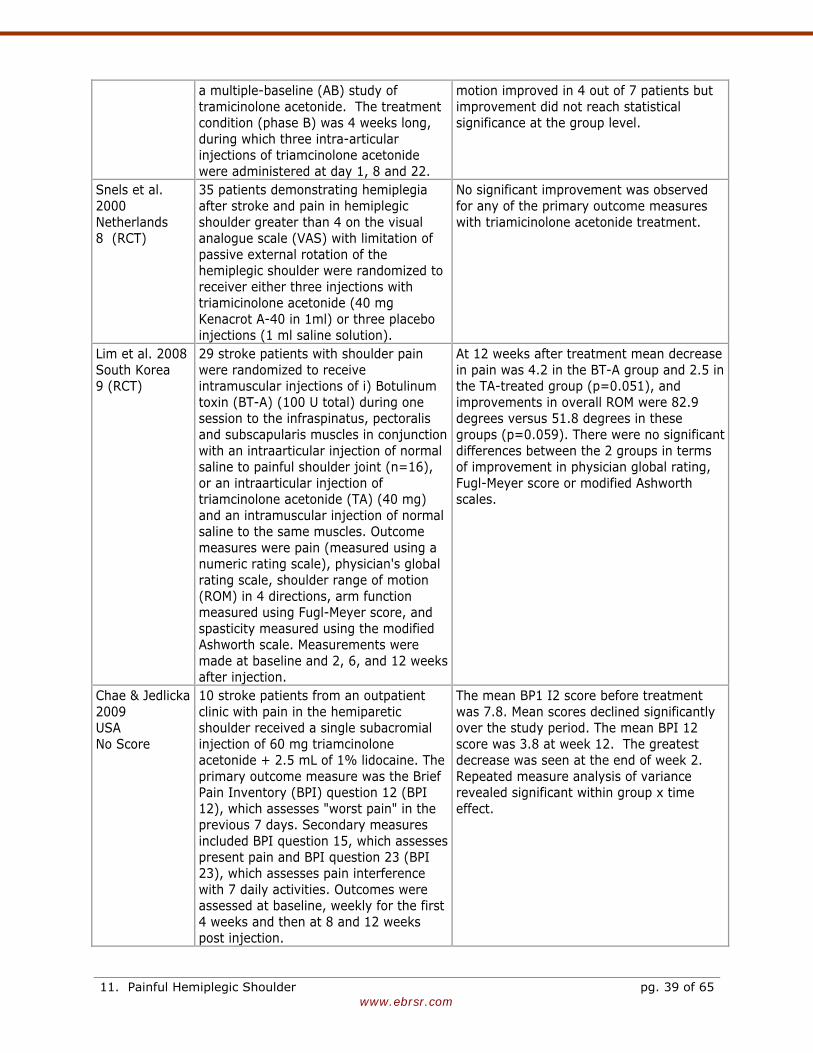
www.ebrsr.com
a multiple-baseline (AB) study of tramicinolone acetonide. The treatment condition (phase B) was 4 weeks long, during which three intra-articular injections of triamcinolone acetonide were administered at day 1, 8 and 22.
motion improved in 4 out of 7 patients but improvement did not reach statistical significance at the group level.
Snels et al. 2000 Netherlands 8 (RCT)
35 patients demonstrating hemiplegia after stroke and pain in hemiplegic shoulder greater than 4 on the visual analogue scale (VAS) with limitation of passive external rotation of the hemiplegic shoulder were randomized to receiver either three injections with triamicinolone acetonide (40 mg Kenacrot A-40 in 1ml) or three placebo injections (1 ml saline solution).
No significant improvement was observed for any of the primary outcome measures with triamicinolone acetonide treatment.
Lim et al. 2008 South Korea 9 (RCT)
29 stroke patients with shoulder pain were randomized to receive intramuscular injections of i) Botulinum toxin (BT-A) (100 U total) during one session to the infraspinatus, pectoralis and subscapularis muscles in conjunction with an intraarticular injection of normal saline to painful shoulder joint (n=16), or an intraarticular injection of triamcinolone acetonide (TA) (40 mg) and an intramuscular injection of normal saline to the same muscles. Outcome measures were pain (measured using a numeric rating scale), physician's global rating scale, shoulder range of motion (ROM) in 4 directions, arm function measured using Fugl-Meyer score, and spasticity measured using the modified Ashworth scale. Measurements were made at baseline and 2, 6, and 12 weeks after injection.
At 12 weeks after treatment mean decrease in pain was 4.2 in the BT-A group and 2.5 in the TA-treated group (p=0.051), and improvements in overall ROM were 82.9 degrees versus 51.8 degrees in these groups (p=0.059). There were no significant differences between the 2 groups in terms of improvement in physician global rating, Fugl-Meyer score or modified Ashworth scales.
Chae & Jedlicka 2009 USA No Score
10 stroke patients from an outpatient clinic with pain in the hemiparetic shoulder received a single subacromial injection of 60 mg triamcinolone acetonide + 2.5 mL of 1% lidocaine. The primary outcome measure was the Brief Pain Inventory (BPI) question 12 (BPI 12), which assesses "worst pain" in the previous 7 days. Secondary measures included BPI question 15, which assesses present pain and BPI question 23 (BPI 23), which assesses pain interference with 7 daily activities. Outcomes were assessed at baseline, weekly for the first 4 weeks and then at 8 and 12 weeks post injection.
The mean BP1 I2 score before treatment was 7.8. Mean scores declined significantly over the study period. The mean BPI 12 score was 3.8 at week 12. The greatest decrease was seen at the end of week 2. Repeated measure analysis of variance revealed significant within group x time effect.
11. Painful Hemiplegic Shoulder pg. 39 of 65
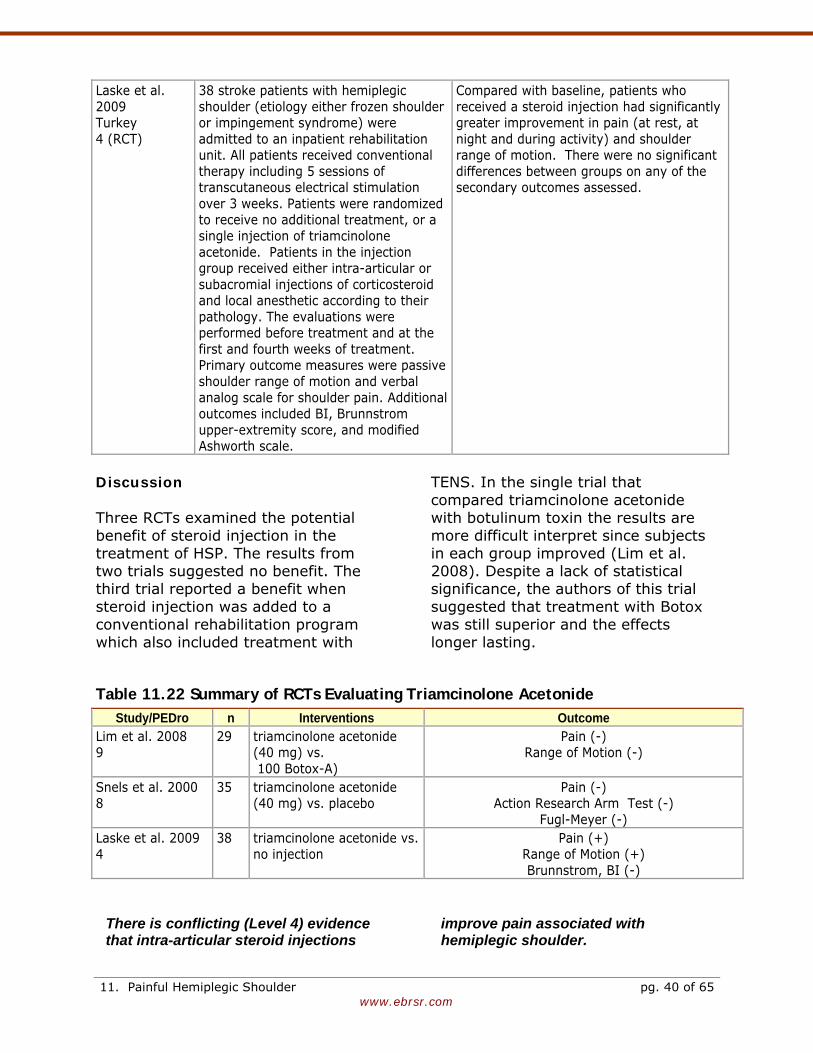
www.ebrsr.com
Laske et al. 2009 Turkey 4 (RCT)
38 stroke patients with hemiplegic shoulder (etiology either frozen shoulder or impingement syndrome) were admitted to an inpatient rehabilitation unit. All patients received conventional therapy including 5 sessions of transcutaneous electrical stimulation over 3 weeks. Patients were randomized to receive no additional treatment, or a single injection of triamcinolone acetonide. Patients in the injection group received either intra-articular or subacromial injections of corticosteroid and local anesthetic according to their pathology. The evaluations were performed before treatment and at the first and fourth weeks of treatment. Primary outcome measures were passive shoulder range of motion and verbal analog scale for shoulder pain. Additional outcomes included BI, Brunnstrom upper-extremity score, and modified Ashworth scale.
Compared with baseline, patients who received a steroid injection had significantly greater improvement in pain (at rest, at night and during activity) and shoulder range of motion. There were no significant differences between groups on any of the secondary outcomes assessed.
Discussion Three RCTs examined the potential benefit of steroid injection in the treatment of HSP. The results from two trials suggested no benefit. The third trial reported a benefit when steroid injection was added to a conventional rehabilitation program which also included treatment with
TENS. In the single trial that compared triamcinolone acetonide with botulinum toxin the results are more difficult interpret since subjects in each group improved (Lim et al. 2008). Despite a lack of statistical significance, the authors of this trial suggested that treatment with Botox was still superior and the effects longer lasting.
Table 11.22 Summary of RCTs Evaluating Triamcinolone Acetonide Study/PEDro n Interventions Outcome
Lim et al. 2008 9
29 triamcinolone acetonide (40 mg) vs. 100 Botox-A)
Pain (-) Range of Motion (-)
Snels et al. 2000 8
35 triamcinolone acetonide (40 mg) vs. placebo
Pain (-) Action Research Arm Test (-)
Fugl-Meyer (-) Laske et al. 2009 4
38 triamcinolone acetonide vs. no injection
Pain (+) Range of Motion (+) Brunnstrom, BI (-)
There is conflicting (Level 4) evidence that intra-articular steroid injections
improve pain associated with hemiplegic shoulder.
11. Painful Hemiplegic Shoulder pg. 40 of 65
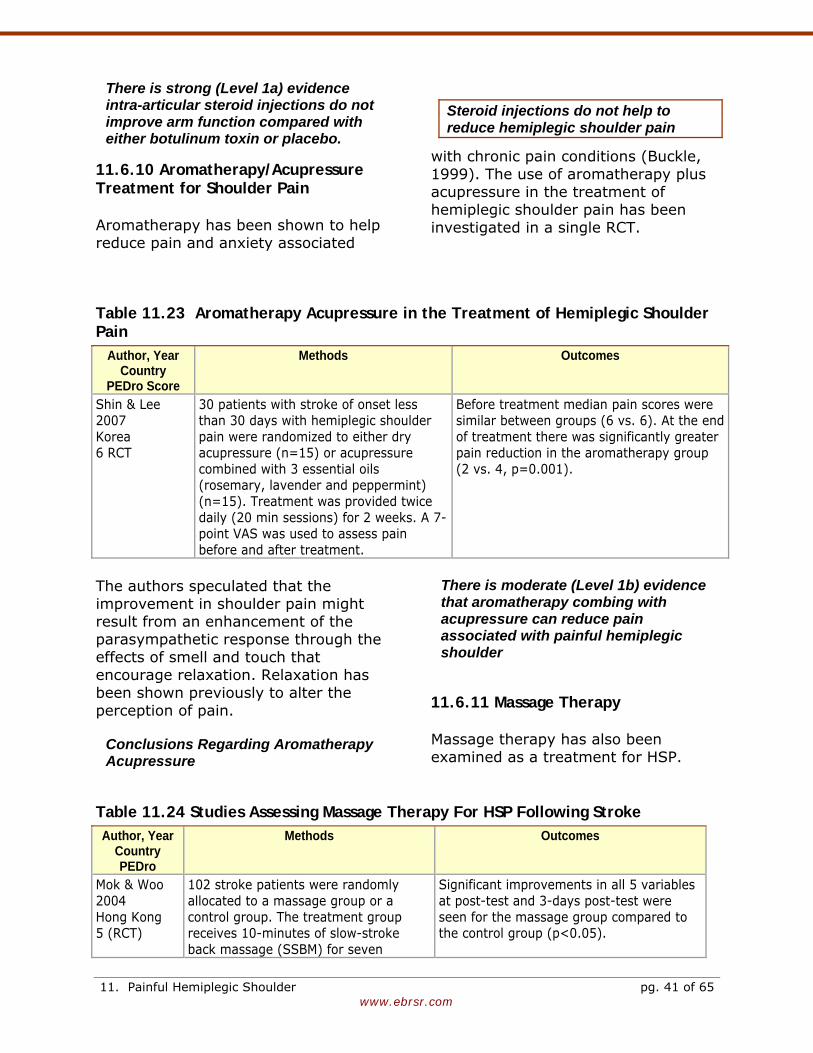
www.ebrsr.com
There is strong (Level 1a) evidence intra-articular steroid injections do not improve arm function compared with either botulinum toxin or placebo.
Steroid injections do not help to reduce hemiplegic shoulder pain
11.6.10 Aromatherapy/Acupressure Treatment for Shoulder Pain Aromatherapy has been shown to help reduce pain and anxiety associated
with chronic pain conditions (Buckle, 1999). The use of aromatherapy plus acupressure in the treatment of hemiplegic shoulder pain has been investigated in a single RCT.
Table 11.23 Aromatherapy Acupressure in the Treatment of Hemiplegic Shoulder Pain
Author, Year Country
PEDro Score
Methods Outcomes
Shin & Lee 2007 Korea 6 RCT
30 patients with stroke of onset less than 30 days with hemiplegic shoulder pain were randomized to either dry acupressure (n=15) or acupressure combined with 3 essential oils (rosemary, lavender and peppermint) (n=15). Treatment was provided twice daily (20 min sessions) for 2 weeks. A 7-point VAS was used to assess pain before and after treatment.
Before treatment median pain scores were similar between groups (6 vs. 6). At the end of treatment there was significantly greater pain reduction in the aromatherapy group (2 vs. 4, p=0.001).
The authors speculated that the improvement in shoulder pain might result from an enhancement of the parasympathetic response through the effects of smell and touch that encourage relaxation. Relaxation has been shown previously to alter the perception of pain.
Conclusions Regarding Aromatherapy Acupressure
There is moderate (Level 1b) evidence that aromatherapy combing with acupressure can reduce pain associated with painful hemiplegic shoulder
11.6.11 Massage Therapy Massage therapy has also been examined as a treatment for HSP.
Table 11.24 Studies Assessing Massage Therapy For HSP Following Stroke Author, Year
Country PEDro
Methods Outcomes
Mok & Woo 2004 Hong Kong 5 (RCT)
102 stroke patients were randomly allocated to a massage group or a control group. The treatment group receives 10-minutes of slow-stroke back massage (SSBM) for seven
Significant improvements in all 5 variables at post-test and 3-days post-test were seen for the massage group compared to the control group (p<0.05).
11. Painful Hemiplegic Shoulder pg. 41 of 65
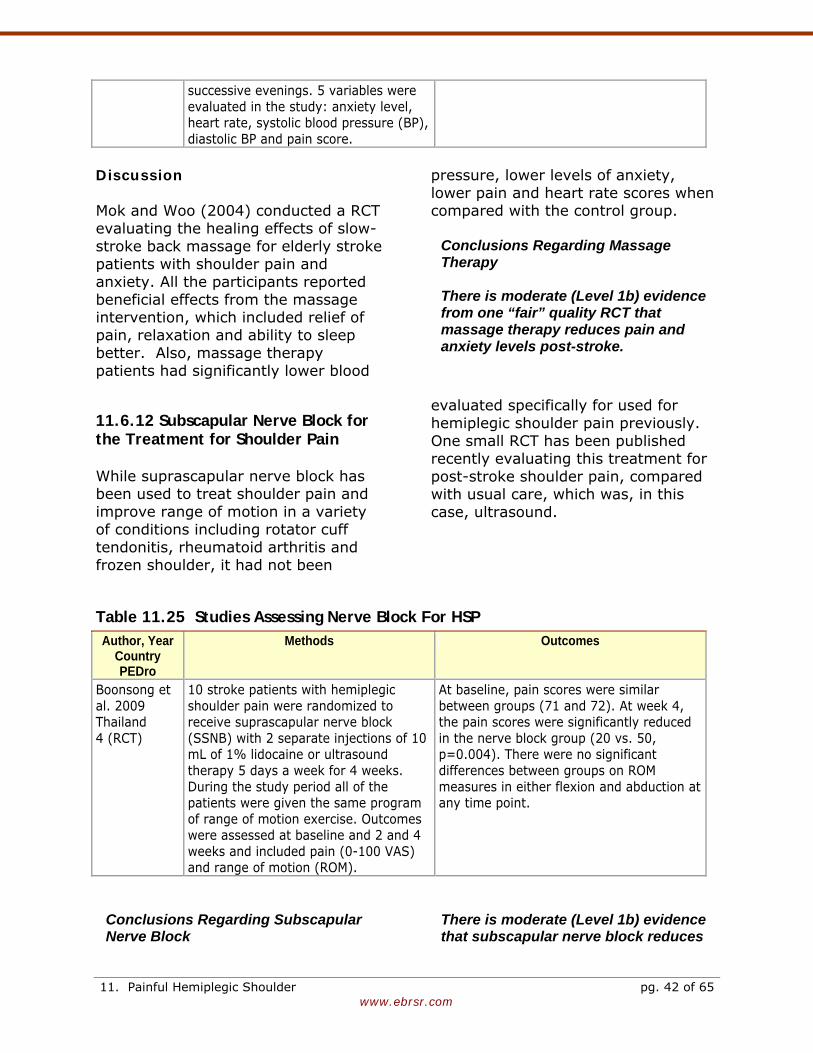
www.ebrsr.com
successive evenings. 5 variables were evaluated in the study: anxiety level, heart rate, systolic blood pressure (BP), diastolic BP and pain score.
Discussion Mok and Woo (2004) conducted a RCT evaluating the healing effects of slow-stroke back massage for elderly stroke patients with shoulder pain and anxiety. All the participants reported beneficial effects from the massage intervention, which included relief of pain, relaxation and ability to sleep better. Also, massage therapy patients had significantly lower blood
pressure, lower levels of anxiety, lower pain and heart rate scores when compared with the control group.
Conclusions Regarding Massage Therapy There is moderate (Level 1b) evidence from one “fair” quality RCT that massage therapy reduces pain and anxiety levels post-stroke.
11.6.12 Subscapular Nerve Block for the Treatment for Shoulder Pain While suprascapular nerve block has been used to treat shoulder pain and improve range of motion in a variety of conditions including rotator cuff tendonitis, rheumatoid arthritis and frozen shoulder, it had not been
evaluated specifically for used for hemiplegic shoulder pain previously. One small RCT has been published recently evaluating this treatment for post-stroke shoulder pain, compared with usual care, which was, in this case, ultrasound.
Table 11.25 Studies Assessing Nerve Block For HSP Author, Year
Country PEDro
Methods Outcomes
Boonsong et al. 2009 Thailand 4 (RCT)
10 stroke patients with hemiplegic shoulder pain were randomized to receive suprascapular nerve block (SSNB) with 2 separate injections of 10 mL of 1% lidocaine or ultrasound therapy 5 days a week for 4 weeks. During the study period all of the patients were given the same program of range of motion exercise. Outcomes were assessed at baseline and 2 and 4 weeks and included pain (0-100 VAS) and range of motion (ROM).
At baseline, pain scores were similar between groups (71 and 72). At week 4, the pain scores were significantly reduced in the nerve block group (20 vs. 50, p=0.004). There were no significant differences between groups on ROM measures in either flexion and abduction at any time point.
Conclusions Regarding Subscapular Nerve Block
There is moderate (Level 1b) evidence that subscapular nerve block reduces
11. Painful Hemiplegic Shoulder pg. 42 of 65
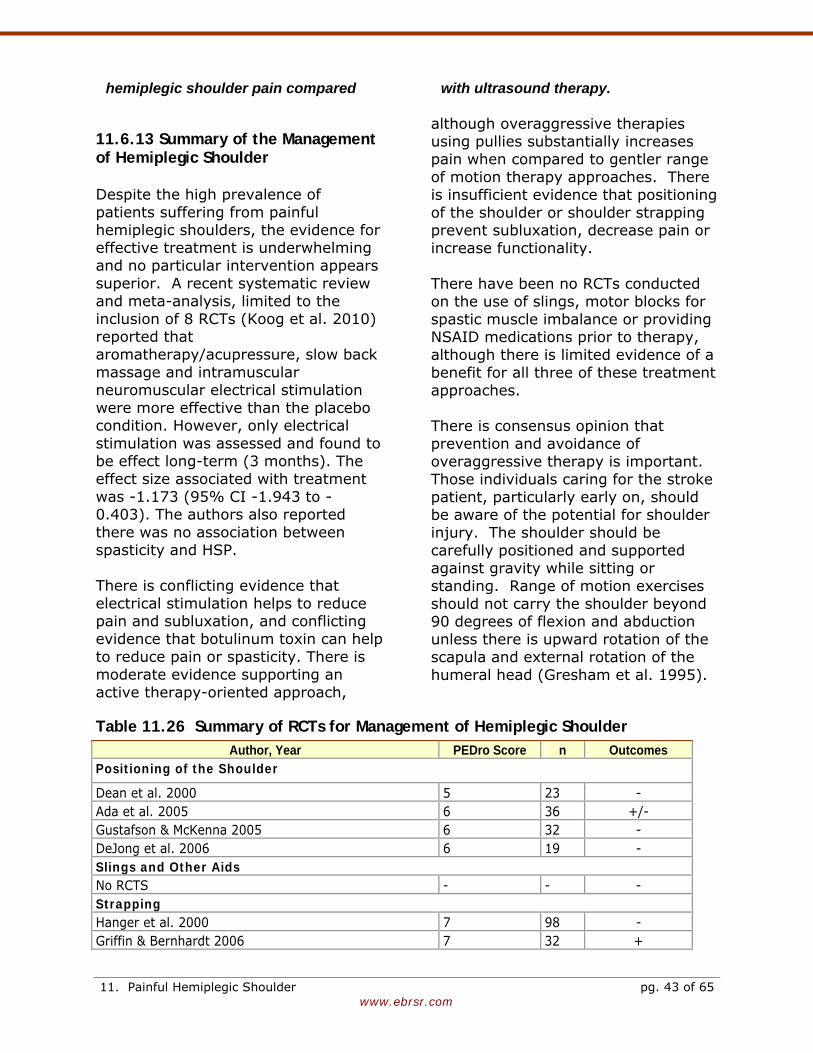
www.ebrsr.com
hemiplegic shoulder pain compared with ultrasound therapy.
11.6.13 Summary of the Management of Hemiplegic Shoulder Despite the high prevalence of patients suffering from painful hemiplegic shoulders, the evidence for effective treatment is underwhelming and no particular intervention appears superior. A recent systematic review and meta-analysis, limited to the inclusion of 8 RCTs (Koog et al. 2010) reported that aromatherapy/acupressure, slow back massage and intramuscular neuromuscular electrical stimulation were more effective than the placebo condition. However, only electrical stimulation was assessed and found to be effect long-term (3 months). The effect size associated with treatment was -1.173 (95% CI -1.943 to -0.403). The authors also reported there was no association between spasticity and HSP. There is conflicting evidence that electrical stimulation helps to reduce pain and subluxation, and conflicting evidence that botulinum toxin can help to reduce pain or spasticity. There is moderate evidence supporting an active therapy-oriented approach,
although overaggressive therapies using pullies substantially increases pain when compared to gentler range of motion therapy approaches. There is insufficient evidence that positioning of the shoulder or shoulder strapping prevent subluxation, decrease pain or increase functionality. There have been no RCTs conducted on the use of slings, motor blocks for spastic muscle imbalance or providing NSAID medications prior to therapy, although there is limited evidence of a benefit for all three of these treatment approaches. There is consensus opinion that prevention and avoidance of overaggressive therapy is important. Those individuals caring for the stroke patient, particularly early on, should be aware of the potential for shoulder injury. The shoulder should be carefully positioned and supported against gravity while sitting or standing. Range of motion exercises should not carry the shoulder beyond 90 degrees of flexion and abduction unless there is upward rotation of the scapula and external rotation of the humeral head (Gresham et al. 1995).
Table 11.26 Summary of RCTs for Management of Hemiplegic Shoulder Author, Year PEDro Score n Outcomes
Positioning of the Shoulder
Dean et al. 2000 5 23 - Ada et al. 2005 6 36 +/- Gustafson & McKenna 2005 6 32 - DeJong et al. 2006 6 19 - Slings and Other Aids No RCTS - - - Strapping Hanger et al. 2000 7 98 - Griffin & Bernhardt 2006 7 32 +
11. Painful Hemiplegic Shoulder pg. 43 of 65
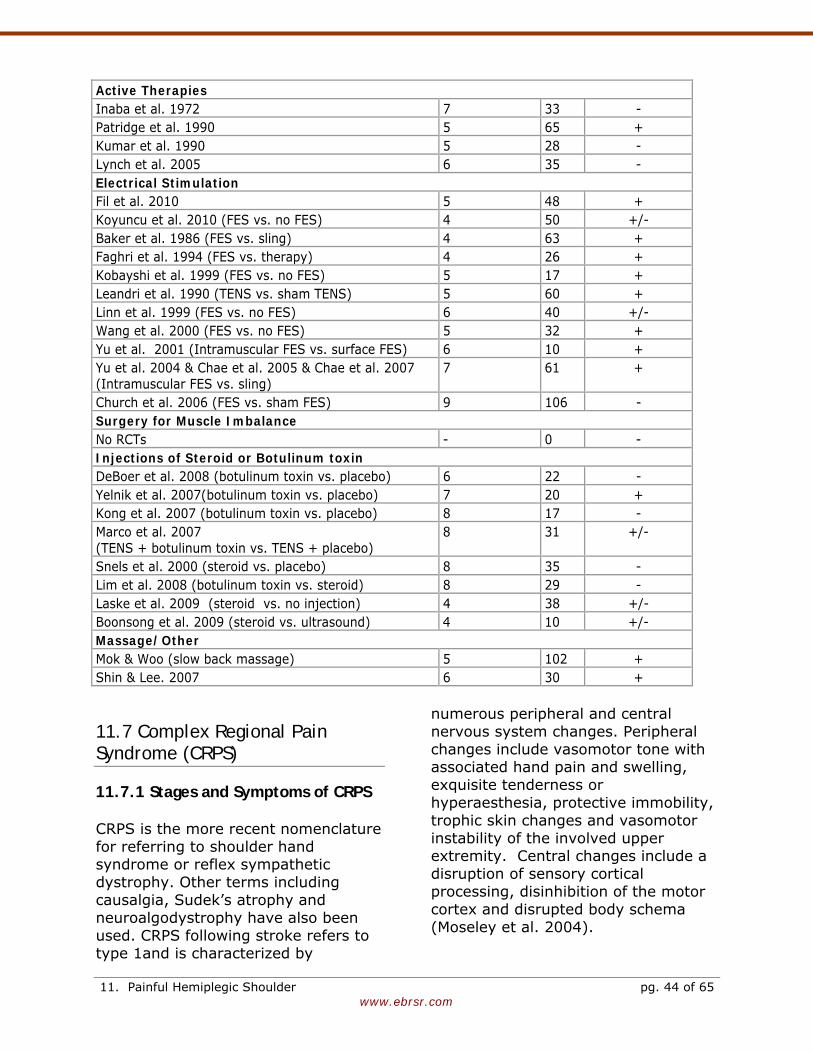
www.ebrsr.com
Active Therapies Inaba et al. 1972 7 33 - Patridge et al. 1990 5 65 + Kumar et al. 1990 5 28 - Lynch et al. 2005 6 35 - Electrical Stimulation Fil et al. 2010 5 48 + Koyuncu et al. 2010 (FES vs. no FES) 4 50 +/- Baker et al. 1986 (FES vs. sling) 4 63 + Faghri et al. 1994 (FES vs. therapy) 4 26 + Kobayshi et al. 1999 (FES vs. no FES) 5 17 + Leandri et al. 1990 (TENS vs. sham TENS) 5 60 + Linn et al. 1999 (FES vs. no FES) 6 40 +/- Wang et al. 2000 (FES vs. no FES) 5 32 + Yu et al. 2001 (Intramuscular FES vs. surface FES) 6 10 + Yu et al. 2004 & Chae et al. 2005 & Chae et al. 2007 (Intramuscular FES vs. sling)
7 61 +
Church et al. 2006 (FES vs. sham FES) 9 106 - Surgery for Muscle Imbalance No RCTs - 0 - Injections of Steroid or Botulinum toxin DeBoer et al. 2008 (botulinum toxin vs. placebo) 6 22 - Yelnik et al. 2007(botulinum toxin vs. placebo) 7 20 + Kong et al. 2007 (botulinum toxin vs. placebo) 8 17 - Marco et al. 2007 (TENS + botulinum toxin vs. TENS + placebo)
8 31 +/-
Snels et al. 2000 (steroid vs. placebo) 8 35 - Lim et al. 2008 (botulinum toxin vs. steroid) 8 29 - Laske et al. 2009 (steroid vs. no injection) 4 38 +/- Boonsong et al. 2009 (steroid vs. ultrasound) 4 10 +/- Massage/Other Mok & Woo (slow back massage) 5 102 + Shin & Lee. 2007 6 30 +
11.7 Complex Regional Pain Syndrome (CRPS)
11.7.1 Stages and Symptoms of CRPS CRPS is the more recent nomenclature for referring to shoulder hand syndrome or reflex sympathetic dystrophy. Other terms including causalgia, Sudek’s atrophy and neuroalgodystrophy have also been used. CRPS following stroke refers to type 1and is characterized by
numerous peripheral and central nervous system changes. Peripheral changes include vasomotor tone with associated hand pain and swelling, exquisite tenderness or hyperaesthesia, protective immobility, trophic skin changes and vasomotor instability of the involved upper extremity. Central changes include a disruption of sensory cortical processing, disinhibition of the motor cortex and disrupted body schema (Moseley et al. 2004).
11. Painful Hemiplegic Shoulder pg. 44 of 65
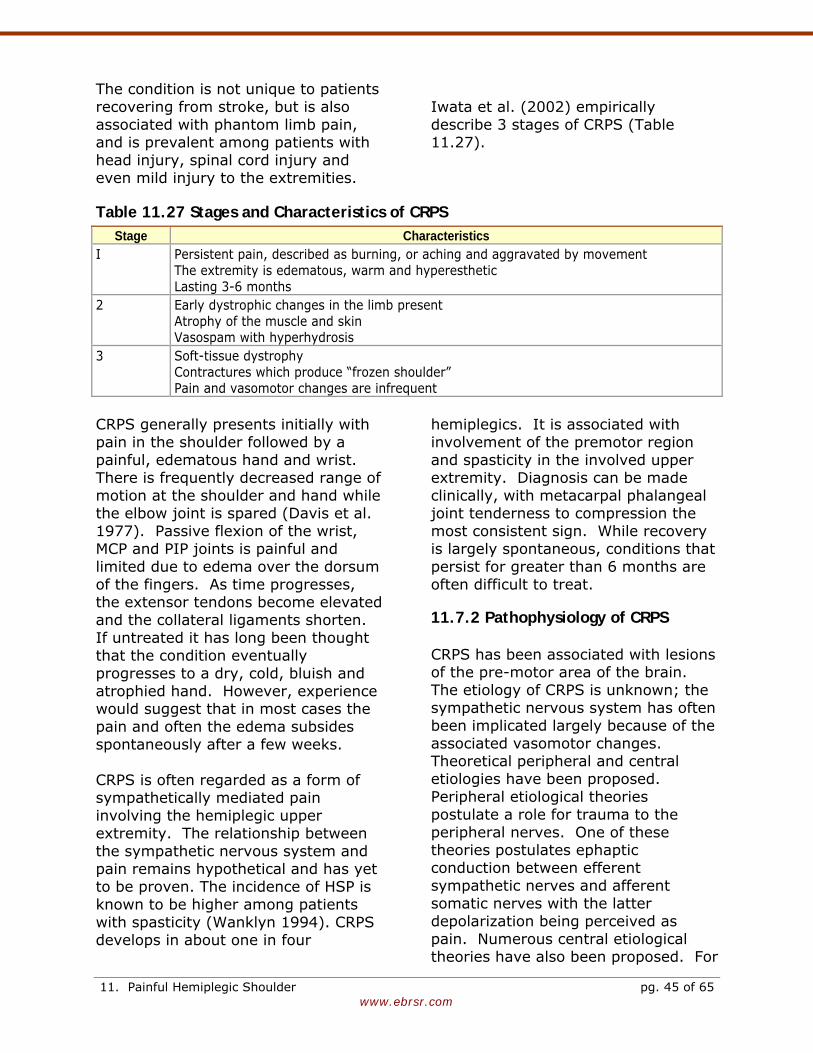
www.ebrsr.com
The condition is not unique to patients recovering from stroke, but is also associated with phantom limb pain, and is prevalent among patients with head injury, spinal cord injury and even mild injury to the extremities.
Iwata et al. (2002) empirically describe 3 stages of CRPS (Table 11.27).
Table 11.27 Stages and Characteristics of CRPS Stage Characteristics
I Persistent pain, described as burning, or aching and aggravated by movement The extremity is edematous, warm and hyperesthetic Lasting 3-6 months
2 Early dystrophic changes in the limb present Atrophy of the muscle and skin Vasospam with hyperhydrosis
3 Soft-tissue dystrophy Contractures which produce “frozen shoulder” Pain and vasomotor changes are infrequent
CRPS generally presents initially with pain in the shoulder followed by a painful, edematous hand and wrist. There is frequently decreased range of motion at the shoulder and hand while the elbow joint is spared (Davis et al. 1977). Passive flexion of the wrist, MCP and PIP joints is painful and limited due to edema over the dorsum of the fingers. As time progresses, the extensor tendons become elevated and the collateral ligaments shorten. If untreated it has long been thought that the condition eventually progresses to a dry, cold, bluish and atrophied hand. However, experience would suggest that in most cases the pain and often the edema subsides spontaneously after a few weeks. CRPS is often regarded as a form of sympathetically mediated pain involving the hemiplegic upper extremity. The relationship between the sympathetic nervous system and pain remains hypothetical and has yet to be proven. The incidence of HSP is known to be higher among patients with spasticity (Wanklyn 1994). CRPS develops in about one in four
hemiplegics. It is associated with involvement of the premotor region and spasticity in the involved upper extremity. Diagnosis can be made clinically, with metacarpal phalangeal joint tenderness to compression the most consistent sign. While recovery is largely spontaneous, conditions that persist for greater than 6 months are often difficult to treat.
11.7.2 Pathophysiology of CRPS CRPS has been associated with lesions of the pre-motor area of the brain. The etiology of CRPS is unknown; the sympathetic nervous system has often been implicated largely because of the associated vasomotor changes. Theoretical peripheral and central etiologies have been proposed. Peripheral etiological theories postulate a role for trauma to the peripheral nerves. One of these theories postulates ephaptic conduction between efferent sympathetic nerves and afferent somatic nerves with the latter depolarization being perceived as pain. Numerous central etiological theories have also been proposed. For
11. Painful Hemiplegic Shoulder pg. 45 of 65
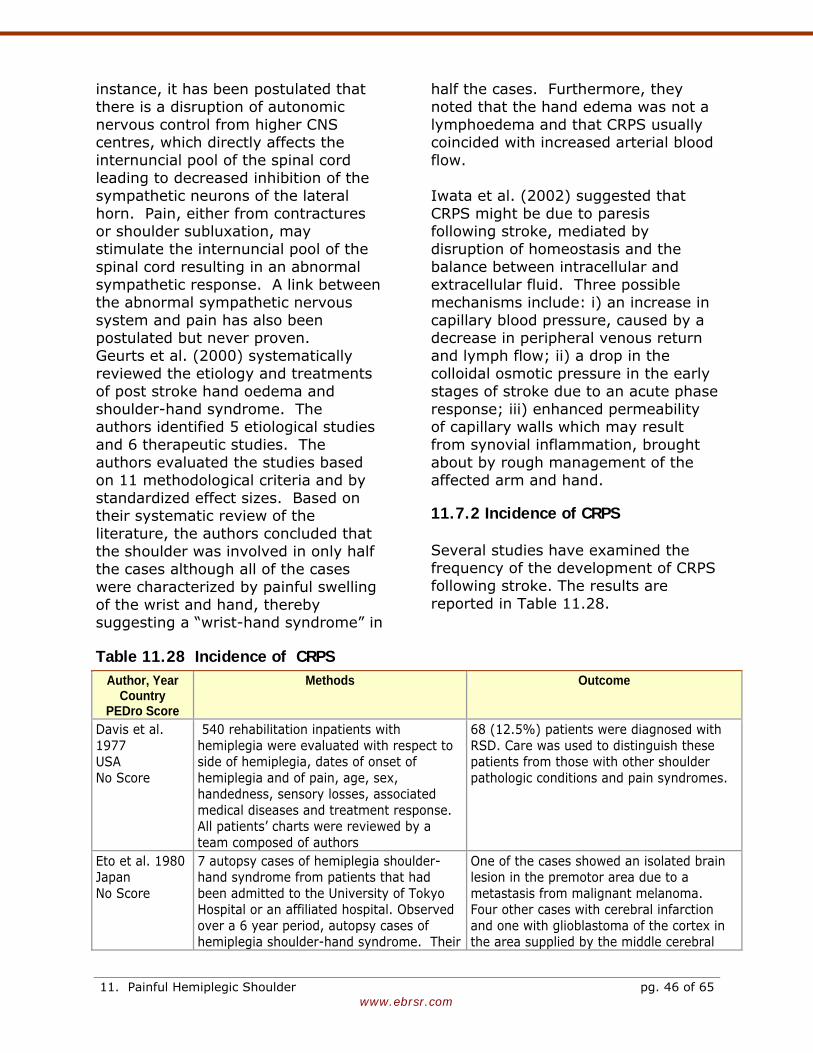
www.ebrsr.com
instance, it has been postulated that there is a disruption of autonomic nervous control from higher CNS centres, which directly affects the internuncial pool of the spinal cord leading to decreased inhibition of the sympathetic neurons of the lateral horn. Pain, either from contractures or shoulder subluxation, may stimulate the internuncial pool of the spinal cord resulting in an abnormal sympathetic response. A link between the abnormal sympathetic nervous system and pain has also been postulated but never proven. Geurts et al. (2000) systematically reviewed the etiology and treatments of post stroke hand oedema and shoulder-hand syndrome. The authors identified 5 etiological studies and 6 therapeutic studies. The authors evaluated the studies based on 11 methodological criteria and by standardized effect sizes. Based on their systematic review of the literature, the authors concluded that the shoulder was involved in only half the cases although all of the cases were characterized by painful swelling of the wrist and hand, thereby suggesting a “wrist-hand syndrome” in
half the cases. Furthermore, they noted that the hand edema was not a lymphoedema and that CRPS usually coincided with increased arterial blood flow. Iwata et al. (2002) suggested that CRPS might be due to paresis following stroke, mediated by disruption of homeostasis and the balance between intracellular and extracellular fluid. Three possible mechanisms include: i) an increase in capillary blood pressure, caused by a decrease in peripheral venous return and lymph flow; ii) a drop in the colloidal osmotic pressure in the early stages of stroke due to an acute phase response; iii) enhanced permeability of capillary walls which may result from synovial inflammation, brought about by rough management of the affected arm and hand.
11.7.2 Incidence of CRPS Several studies have examined the frequency of the development of CRPS following stroke. The results are reported in Table 11.28.
Table 11.28 Incidence of CRPS Author, Year
Country PEDro Score
Methods Outcome
Davis et al. 1977 USA No Score
540 rehabilitation inpatients with hemiplegia were evaluated with respect to side of hemiplegia, dates of onset of hemiplegia and of pain, age, sex, handedness, sensory losses, associated medical diseases and treatment response. All patients’ charts were reviewed by a team composed of authors
68 (12.5%) patients were diagnosed with RSD. Care was used to distinguish these patients from those with other shoulder pathologic conditions and pain syndromes.
Eto et al. 1980 Japan No Score
7 autopsy cases of hemiplegia shoulder-hand syndrome from patients that had been admitted to the University of Tokyo Hospital or an affiliated hospital. Observed over a 6 year period, autopsy cases of hemiplegia shoulder-hand syndrome. Their
One of the cases showed an isolated brain lesion in the premotor area due to a metastasis from malignant melanoma. Four other cases with cerebral infarction and one with glioblastoma of the cortex in the area supplied by the middle cerebral
11. Painful Hemiplegic Shoulder pg. 46 of 65
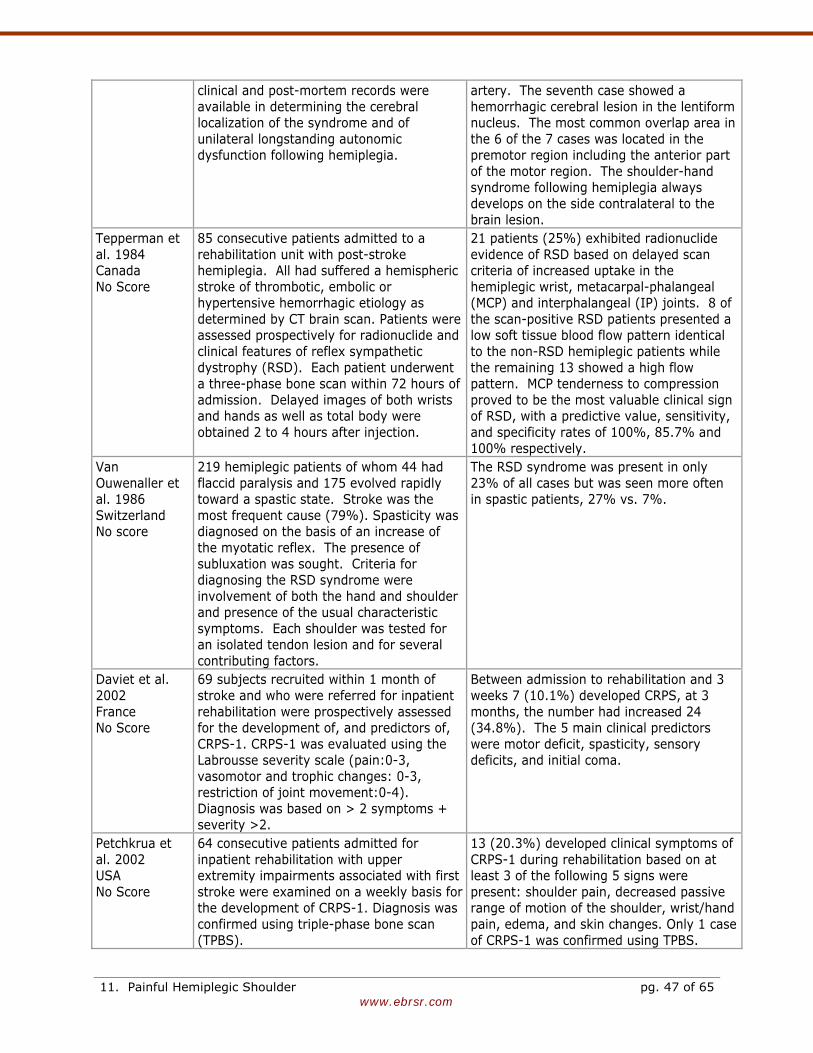
www.ebrsr.com
clinical and post-mortem records were available in determining the cerebral localization of the syndrome and of unilateral longstanding autonomic dysfunction following hemiplegia.
artery. The seventh case showed a hemorrhagic cerebral lesion in the lentiform nucleus. The most common overlap area in the 6 of the 7 cases was located in the premotor region including the anterior part of the motor region. The shoulder-hand syndrome following hemiplegia always develops on the side contralateral to the brain lesion.
Tepperman et al. 1984 Canada No Score
85 consecutive patients admitted to a rehabilitation unit with post-stroke hemiplegia. All had suffered a hemispheric stroke of thrombotic, embolic or hypertensive hemorrhagic etiology as determined by CT brain scan. Patients were assessed prospectively for radionuclide and clinical features of reflex sympathetic dystrophy (RSD). Each patient underwent a three-phase bone scan within 72 hours of admission. Delayed images of both wrists and hands as well as total body were obtained 2 to 4 hours after injection.
21 patients (25%) exhibited radionuclide evidence of RSD based on delayed scan criteria of increased uptake in the hemiplegic wrist, metacarpal-phalangeal (MCP) and interphalangeal (IP) joints. 8 of the scan-positive RSD patients presented a low soft tissue blood flow pattern identical to the non-RSD hemiplegic patients while the remaining 13 showed a high flow pattern. MCP tenderness to compression proved to be the most valuable clinical sign of RSD, with a predictive value, sensitivity, and specificity rates of 100%, 85.7% and 100% respectively.
Van Ouwenaller et al. 1986 Switzerland No score
219 hemiplegic patients of whom 44 had flaccid paralysis and 175 evolved rapidly toward a spastic state. Stroke was the most frequent cause (79%). Spasticity was diagnosed on the basis of an increase of the myotatic reflex. The presence of subluxation was sought. Criteria for diagnosing the RSD syndrome were involvement of both the hand and shoulder and presence of the usual characteristic symptoms. Each shoulder was tested for an isolated tendon lesion and for several contributing factors.
The RSD syndrome was present in only 23% of all cases but was seen more often in spastic patients, 27% vs. 7%.
Daviet et al. 2002 France No Score
69 subjects recruited within 1 month of stroke and who were referred for inpatient rehabilitation were prospectively assessed for the development of, and predictors of, CRPS-1. CRPS-1 was evaluated using the Labrousse severity scale (pain:0-3, vasomotor and trophic changes: 0-3, restriction of joint movement:0-4). Diagnosis was based on > 2 symptoms + severity >2.
Between admission to rehabilitation and 3 weeks 7 (10.1%) developed CRPS, at 3 months, the number had increased 24 (34.8%). The 5 main clinical predictors were motor deficit, spasticity, sensory deficits, and initial coma.
Petchkrua et al. 2002 USA No Score
64 consecutive patients admitted for inpatient rehabilitation with upper extremity impairments associated with first stroke were examined on a weekly basis for the development of CRPS-1. Diagnosis was confirmed using triple-phase bone scan (TPBS).
13 (20.3%) developed clinical symptoms of CRPS-1 during rehabilitation based on at least 3 of the following 5 signs were present: shoulder pain, decreased passive range of motion of the shoulder, wrist/hand pain, edema, and skin changes. Only 1 case of CRPS-1 was confirmed using TPBS.
11. Painful Hemiplegic Shoulder pg. 47 of 65
www.ebrsr.com
Gokkaya et al. 2006 Turkey No Score
A cohort of 95 stroke patients admitted for inpatient rehabilitation, which usually occurred 4 to 6 weeks post stroke, were evaluated for the presence of RSD and glenohumerol joint subluxation at admission.
29 patients (30.5%) developed RSD. Their rehabilitation stays were, on average, 10 days longer compared with patients without RSD. Patients in the lower categories of Brunnstrom scores tended to develop RSD more frequently. The presence of shoulder subluxation was also more frequent among patients with RSD (72.4% vs. 24.2%, p<0.001).
Kocabas et al. 2007 Turkey No Score
82 patients were evaluated for the presence of CRPS-1 weeks 2, 6, 14 and 28 after suffering a stroke. Diagnosis was based on the presence of pain, edema of the wrist and fingers, change in colour/temperature of the hand and limited ROM of the shoulder and hand.
The incidence of CRPS-I was 48.8% in the first 28 weeks. During the 6th, 14th and 28th week, it was present in 12%, 30% and 40% subjects, respectively.
Barlak et al. 2009 Turkey No Score
187 consecutive stroke patients admitted for inpatient rehabilitation were evaluated for the presence of HSP. Each patient was evaluated by clinical, radiographic, and ultrasonographic examination. Daily living activities were assessed using the FIM at admission and at discharge. Patients were divided into two groups, one comprising patients with shoulder pain and the other comprising patients without shoulder pain. They were then compared with respect to clinical characteristics, radiologic findings, and FIM scores.
Shoulder pain was present in 114 (61%) patients. 70 patients had complex regional pain syndrome-type I. There was no correlation between presence or absence of CPRS-1 and degree of subluxation. A significantly higher percentage of patients with CPRS-1 were either in Brunnstrom recovery stage I or II
There is a wide range of reported prevalence of CRPS following stroke. Part of variability can be attributed to timing and form of assessment used. While the incidence of RSD appears to range between 12-32%, Petchkrua et al. (2000) suggested that the incidence of RSD is over-estimated and the results from previous studies were obtained before patients routinely received early intensive inpatient rehabilitation. At admission to hospital and once a week until discharge, patients admitted to an acute rehabilitation facility were evaluated for shoulder pain, decreased passive range of motion of the shoulder, wrist/hand pain, edema, and skin changes. If three of these five criteria were positive, patients underwent a triple-phase bone scan
(TPBS). Bone scan findings consistent with CRPS type 1 were taken as confirming the diagnosis. Of 64 subjects, 13 underwent bone scans, with only one (1.56%) positive result. The authors noted it was possible that patients were discharged before they developed symptoms of RSD. However, the results from several newer studies suggest the incidence is higher. Since both of these studies originated in the same country, the results may not be generalizable. The authors themselves speculate that the poor economic conditions with limited patient care capabilities likely contributed to the high prevalence (Kocabas et al. 2007)
Conclusions Regarding the Incidence of CRPS Post Stroke
11. Painful Hemiplegic Shoulder pg. 48 of 65
www.ebrsr.com
The incidence of CRPS post stroke ranges from 12%-48% and may be influenced by the timing as well as the type of assessment.
11.7.3 Diagnostic Tests of CRPS Several approaches to diagnose CRPS have been used, although no one single test will identify all persons with SHS. Three sets of criteria are used routinely: International Association for the Study of Pain (IASP) 1994 consensus criteria (Staton-Hicks et al. 1995), Bruehl’s criteria (Bruehl et al. 1999) and Veldman’s criteria (Veldman et al. 1993). The sensitivities and specificities of these sets of criteria range from 70% to 100% and 36% to 94%, respectively. Common features among these criteria include: pain, allodynia, hyperalgesia, edema, sweating changes, and limitations in range of motion. Quisel et al. (2005) have suggested that although diagnosis through instrumentation, bone scans (scintigraphy) and radiophraphy are common, there is limited evidence that these techniques add to the accuracy of the diagnosis. Routine radiographs of the involved upper extremity may demonstrate a patchy, periarticular demineralization (Sudek's atrophy) as early as 3-6 months after the onset of clinical signs. The most sensitive diagnostic test is the technetium diphosphonate bone scan which demonstrates increased periarticular uptake (mostly at the shoulder and wrist) in the affected upper extremity. Bone scan abnormalities appear earlier than the x-ray changes. Tepperman et al. (1984) found 25% of hemiplegic patients demonstrated evidence of reflex sympathetic dystrophy in the involved upper extremity although only two-thirds went on to develop the
clinical syndrome. Temporary resolution of symptoms with sympathetic blockade is considered diagnostic despite potential difficulties with the technique in terms of diagnostic validity. Thermography, in controlled studies, has failed to consistently diagnose reflex sympathetic dystrophy and is not considered a valid test. However, Kozin et al. (1981) suggested that that clinical measurements such as grip strength, tenderness and ring size were more accurate diagnostic indicator of RSD. Iwata et al. (2002) have suggested that a ratio of the circumference of the middle finger (affected:unaffected) greater than 1.06 at four weeks post stroke was predictive of RSD
Conclusions Regarding CRPS CRPS is a painful clinical entity, which is not understood from a pathophysiological basis. The diagnosis is made clinically. Most cases appear to improve with time.
11.7.4 Treatment of CRPS Prevention of shoulder problems and aggressive early treatment are recommended to prevent the development of a non-functional painful upper extremity. The various treatment options are outlined in Table 11.29. A one to two week course of high dose corticosteroids and/or sympathetic blocks either in the form of stellate ganglion blocks or guanethedine local venous blocks may be tried in persistent disabling cases. Constraint-induced movement therapy and sensory discrimination training have
11. Painful Hemiplegic Shoulder pg. 49 of 65
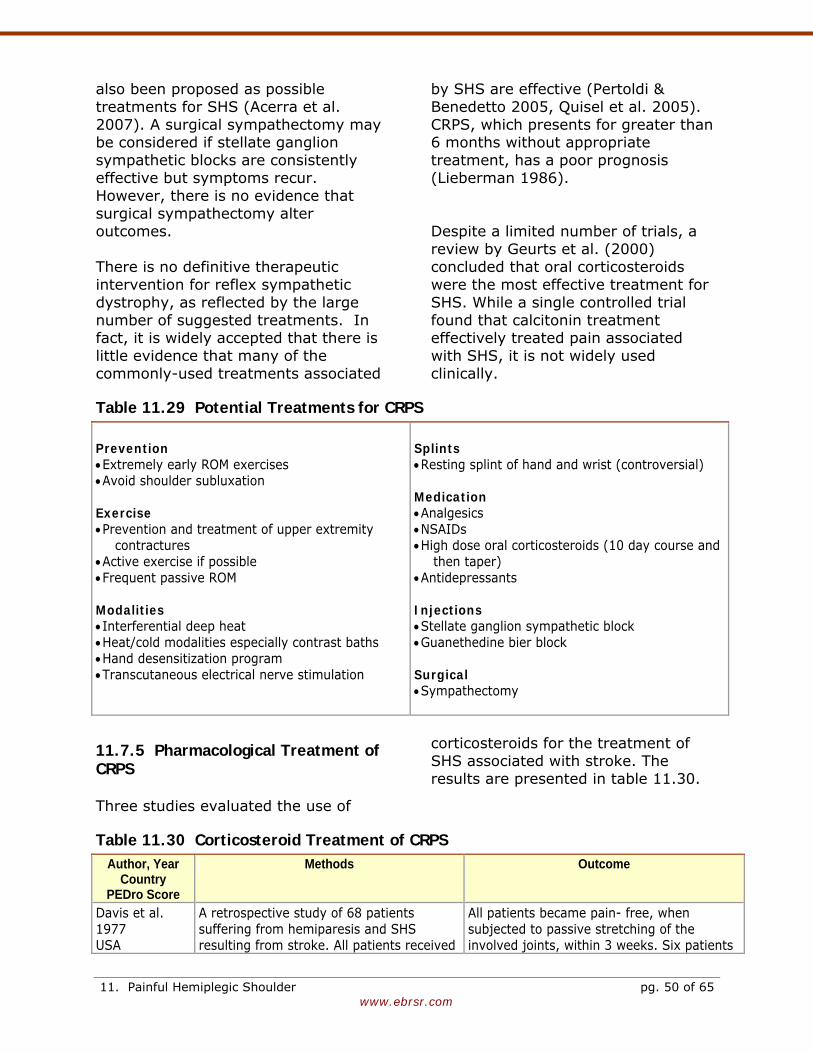
www.ebrsr.com
also been proposed as possible treatments for SHS (Acerra et al. 2007). A surgical sympathectomy may be considered if stellate ganglion sympathetic blocks are consistently effective but symptoms recur. However, there is no evidence that surgical sympathectomy alter outcomes. There is no definitive therapeutic intervention for reflex sympathetic dystrophy, as reflected by the large number of suggested treatments. In fact, it is widely accepted that there is little evidence that many of the commonly-used treatments associated
by SHS are effective (Pertoldi & Benedetto 2005, Quisel et al. 2005). CRPS, which presents for greater than 6 months without appropriate treatment, has a poor prognosis (Lieberman 1986). Despite a limited number of trials, a review by Geurts et al. (2000) concluded that oral corticosteroids were the most effective treatment for SHS. While a single controlled trial found that calcitonin treatment effectively treated pain associated with SHS, it is not widely used clinically.
Table 11.29 Potential Treatments for CRPS Prevention • Extremely early ROM exercises • Avoid shoulder subluxation Exercise • Prevention and treatment of upper extremity
contractures • Active exercise if possible • Frequent passive ROM Modalities • Interferential deep heat • Heat/cold modalities especially contrast baths • Hand desensitization program • Transcutaneous electrical nerve stimulation
Splints • Resting splint of hand and wrist (controversial) Medication • Analgesics • NSAIDs • High dose oral corticosteroids (10 day course and
then taper) • Antidepressants Injections • Stellate ganglion sympathetic block • Guanethedine bier block Surgical • Sympathectomy
11.7.5 Pharmacological Treatment of CRPS Three studies evaluated the use of
corticosteroids for the treatment of SHS associated with stroke. The results are presented in table 11.30.
Table 11.30 Corticosteroid Treatment of CRPS Author, Year
Country PEDro Score
Methods Outcome
Davis et al. 1977 USA
A retrospective study of 68 patients suffering from hemiparesis and SHS resulting from stroke. All patients received
All patients became pain- free, when subjected to passive stretching of the involved joints, within 3 weeks. Six patients
11. Painful Hemiplegic Shoulder pg. 50 of 65

www.ebrsr.com
No Score 16 mg of an oral steroid (triamcinolone diacetate) daily for 14 to 21 days. Patients self-described their pain.
experienced a relapse of their pain, which resolved during a second course of treatment.
Braus et al. 1994 Germany 5 (RCT)
36 hemiplegic patients secondary to a stroke of the middle cerebral artery and exhibited definite shoulder-hand syndrome were studied. Patients were randomized to orally receive either 8 mg methylprednisolone or a placebo over 4 weeks. All patients received daily physical therapy. For patients in the placebo group, if no improvement was noted in shoulder-hand syndrome then they were given 4 weeks of corticosteroid treatment as per the experimental group.
No significant improvement was noted in shoulder-hand syndrome in the placebo group after 4 weeks at which time all patients switched over the corticosteroid protocol. Patients receiving the corticosteroid treatment demonstrated significant improvement in shoulder-hand syndrome that was maintained at 6 months. 31 of the 36 patients became almost symptom free within 10 days of treatment with low dose oral corticosteroids.
Kalita et al. 2006 India 7 (RCT)
60 patients who developed CRPS-I following stroke were randomly assigned to receive 40 mg prednisolone or 20 mg piroxicam (NSAID) daily. CRPS-I was assessed at 1 month using a 0-14 point scale. The primary end point was a 2 or more point reduction in CRPS score.
Symptoms of CRPS developed a median of 28 days post stroke. In the prednisolone group, 83.3% patients showed significant improvement, compared to 16.7% in the piroxicam group. The mean change in CRPS score in prednisolone group was 6.47 (95%CI 4.37-7.36), whereas in piroxicam group it was only 0.47.
Discussion The efficacy of corticosteroids for the treatment of CRPS-1 has not been well-studied. In only 2 RCTs identified, one in which placebo was used and one in which a NSAID was used as the alternative treatment. Steroids were demonstrated to be of benefit. Braus et al. (1994) reported that oral corticosteroids improved CRPS-1 symptoms for at least 4 weeks. Kalita et al. (2005) also reported a significant decrease in symptoms with steroids.
Conclusions Regarding Oral Corticosteroids in CRPS There is moderate (Level 1b) evidence that oral corticosteroids improve CRPS for at least the first 4 weeks. Oral corticosteroids appear to improve CRPS for at least the first 4 weeks.
11.7.6 Mirror Imagery as a Treatment for CRPS Mirror therapy is a technique that uses visual feedback about motor performance to improve rehabilitation outcomes. It can be used to improve motor performance, which is discussed in other chapters. Although it is more commonly associated with the treatment of phantom limb pain it may also be useful in the treatment of CRPS-1 post stroke. It is believed that mirror imagery helps to create a movement illusion of the affected arm with the brain. These mirror illusions are believed to compensate for a reduced or absent propreoceptive input and to re-establish the normal pain free relationship between sensory feedback and motor intention, resolving the pain state.
11. Painful Hemiplegic Shoulder pg. 51 of 65
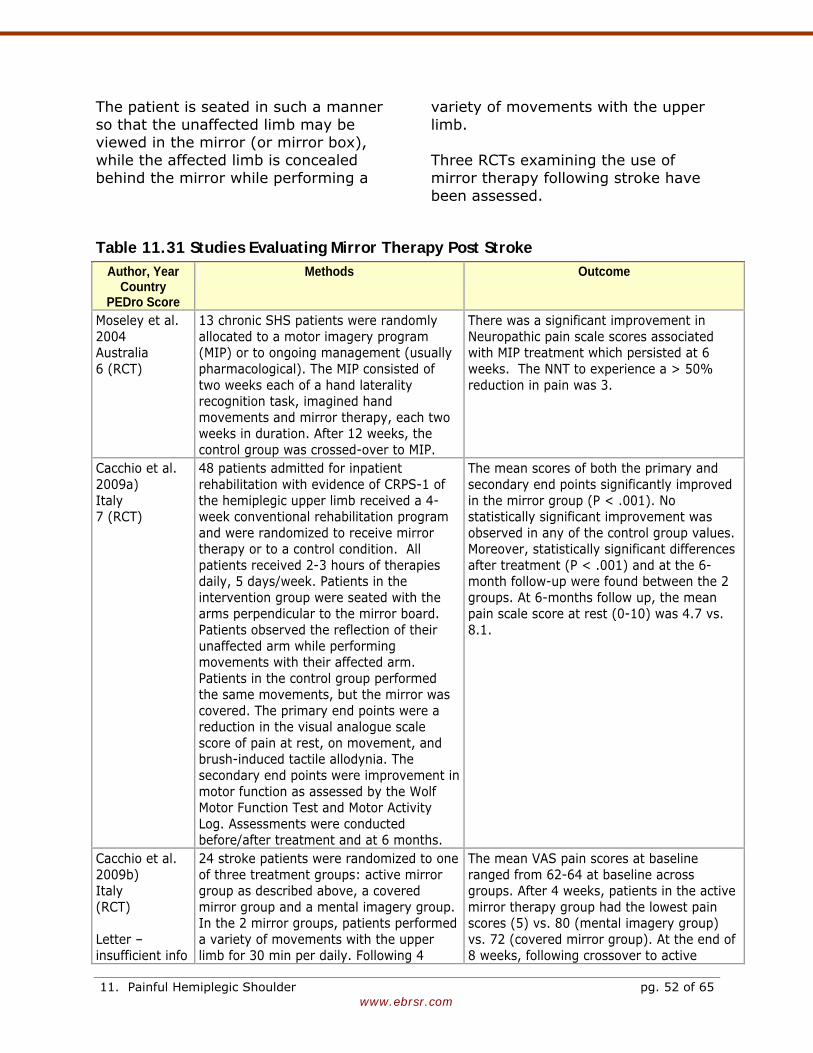
www.ebrsr.com
The patient is seated in such a manner so that the unaffected limb may be viewed in the mirror (or mirror box), while the affected limb is concealed behind the mirror while performing a
variety of movements with the upper limb. Three RCTs examining the use of mirror therapy following stroke have been assessed.
Table 11.31 Studies Evaluating Mirror Therapy Post Stroke Author, Year
Country PEDro Score
Methods Outcome
Moseley et al. 2004 Australia 6 (RCT)
13 chronic SHS patients were randomly allocated to a motor imagery program (MIP) or to ongoing management (usually pharmacological). The MIP consisted of two weeks each of a hand laterality recognition task, imagined hand movements and mirror therapy, each two weeks in duration. After 12 weeks, the control group was crossed-over to MIP.
There was a significant improvement in Neuropathic pain scale scores associated with MIP treatment which persisted at 6 weeks. The NNT to experience a > 50% reduction in pain was 3.
Cacchio et al. 2009a) Italy 7 (RCT)
48 patients admitted for inpatient rehabilitation with evidence of CRPS-1 of the hemiplegic upper limb received a 4-week conventional rehabilitation program and were randomized to receive mirror therapy or to a control condition. All patients received 2-3 hours of therapies daily, 5 days/week. Patients in the intervention group were seated with the arms perpendicular to the mirror board. Patients observed the reflection of their unaffected arm while performing movements with their affected arm. Patients in the control group performed the same movements, but the mirror was covered. The primary end points were a reduction in the visual analogue scale score of pain at rest, on movement, and brush-induced tactile allodynia. The secondary end points were improvement in motor function as assessed by the Wolf Motor Function Test and Motor Activity Log. Assessments were conducted before/after treatment and at 6 months.
The mean scores of both the primary and secondary end points significantly improved in the mirror group (P < .001). No statistically significant improvement was observed in any of the control group values. Moreover, statistically significant differences after treatment (P < .001) and at the 6-month follow-up were found between the 2 groups. At 6-months follow up, the mean pain scale score at rest (0-10) was 4.7 vs. 8.1.
Cacchio et al. 2009b) Italy (RCT) Letter –insufficient info
24 stroke patients were randomized to one of three treatment groups: active mirror group as described above, a covered mirror group and a mental imagery group. In the 2 mirror groups, patients performed a variety of movements with the upper limb for 30 min per daily. Following 4
The mean VAS pain scores at baseline ranged from 62-64 at baseline across groups. After 4 weeks, patients in the active mirror therapy group had the lowest pain scores (5) vs. 80 (mental imagery group) vs. 72 (covered mirror group). At the end of 8 weeks, following crossover to active
11. Painful Hemiplegic Shoulder pg. 52 of 65
www.ebrsr.com
to enable scoring
weeks of treatment, subjects in the 2 non-active mirror therapy groups were crossed over to the active mirror therapy group. Outcome measures, assessed at baseline and 8 weeks included pain on a VAS scale (0-100) and the Wolf-motor function test.
therapy the mean VAS pain scores were 10 or lower.
Among the 3 studies described above, one (Moseley et al. 2004) included mirror therapy as one component of the three- part treatment Motor Imagery Program (MIP). The mechanisms underlying motor imagery remain unclear, although it is known that both real and imagined movements activate similar cortical networks. Proposed mechanisms include reconciliation of motor output and sensory feedback, activation of mirror neurons and graded activation of cortical motor networks (Acerra et al. 2007). In the first phase of the treatment hand laterality recognition, avoidance of activation of the primary motor cortex was achieved by only initiating activation in the pre-motor cortices. In the second stage, patients were asked to imagine their own hand placed in the same position as a picture selected from 28 pictures chosen at random. In the final stage, pictures of the unaffected hand were placed into a cardboard mirror box. Patients were asked to adopt the posture in the picture (n=20) times with both hands, but to discontinue if they experienced pain.
Moseley et al. (2004) reported that treatment with MIP was more effective than ongoing medical management of CRPS. Patients experienced significant reductions in pain and swelling associated with treatment, which persisted for at least 6 weeks. The authors also noted that 6 weeks after completing the MIP program, approximately 50% of patients no longer fulfilled the diagnostic criteria for CRPS1. Mirror therapy, when provided as a single intervention was found to be more effective in reducing pain than either sham mirror therapy or mental practice. The effects were also reported to be long lasting. (Cacchio et al. 2009a).
Conclusions Regarding Mirror Therapy Post Stroke There is strong (Level 1a) evidence that mirror therapy can reduce pain associated with shoulder-hand syndrome. A mirror therapy program appears to improve shoulder-hand syndrome.
11.7.7 Passive Range of Motion Exercises for the Prevention of CRPS In addition to treatment of CRPS-1, there are also strategies to prevent its development. Although physiotherapy is regarded as the cornerstone of integrated treatment, no controlled
trials have been conducted to evaluate its effect in preventing the development of CRPS. A single trial using historical controls evaluated the benefit of an exercise program to reduce the development of CRPS following stroke (Table 11.32).
11. Painful Hemiplegic Shoulder pg. 53 of 65
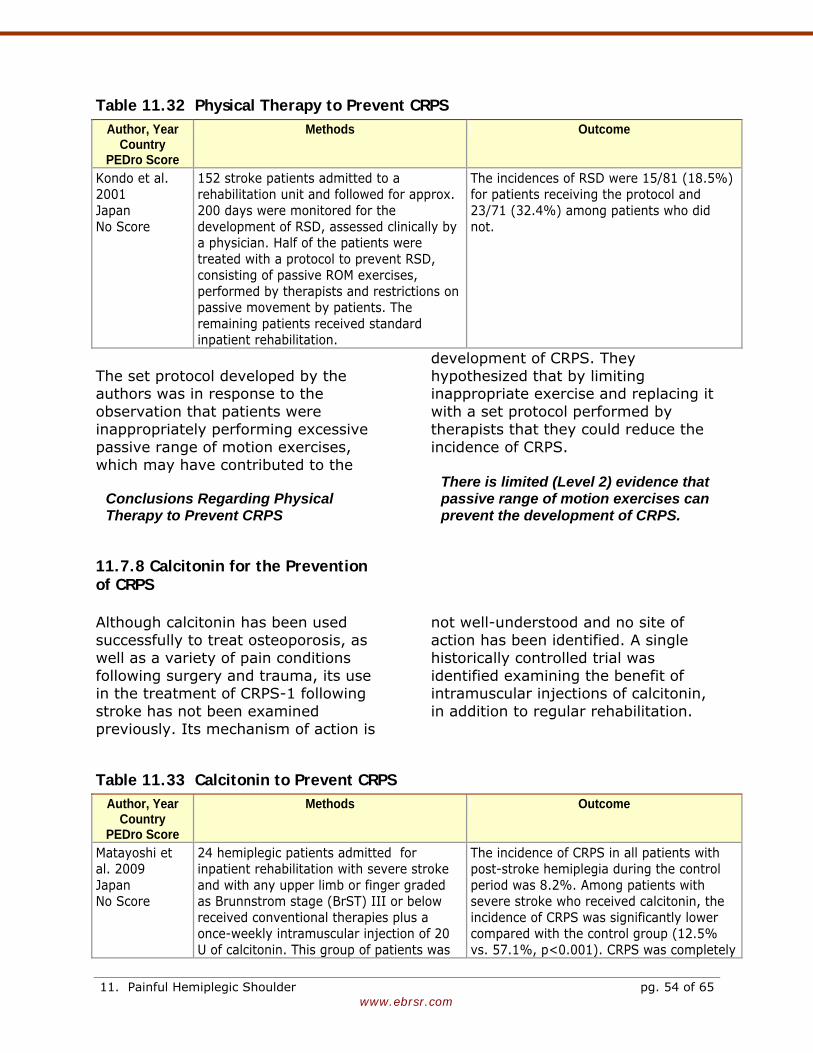
www.ebrsr.com
Table 11.32 Physical Therapy to Prevent CRPS Author, Year
Country PEDro Score
Methods Outcome
Kondo et al. 2001 Japan No Score
152 stroke patients admitted to a rehabilitation unit and followed for approx. 200 days were monitored for the development of RSD, assessed clinically by a physician. Half of the patients were treated with a protocol to prevent RSD, consisting of passive ROM exercises, performed by therapists and restrictions on passive movement by patients. The remaining patients received standard inpatient rehabilitation.
The incidences of RSD were 15/81 (18.5%) for patients receiving the protocol and 23/71 (32.4%) among patients who did not.
The set protocol developed by the authors was in response to the observation that patients were inappropriately performing excessive passive range of motion exercises, which may have contributed to the
development of CRPS. They hypothesized that by limiting inappropriate exercise and replacing it with a set protocol performed by therapists that they could reduce the incidence of CRPS.
Conclusions Regarding Physical Therapy to Prevent CRPS
There is limited (Level 2) evidence that passive range of motion exercises can prevent the development of CRPS.
11.7.8 Calcitonin for the Prevention of CRPS Although calcitonin has been used successfully to treat osteoporosis, as well as a variety of pain conditions following surgery and trauma, its use in the treatment of CRPS-1 following stroke has not been examined previously. Its mechanism of action is
not well-understood and no site of action has been identified. A single historically controlled trial was identified examining the benefit of intramuscular injections of calcitonin, in addition to regular rehabilitation.
Table 11.33 Calcitonin to Prevent CRPS Author, Year
Country PEDro Score
Methods Outcome
Matayoshi et al. 2009 Japan No Score
24 hemiplegic patients admitted for inpatient rehabilitation with severe stroke and with any upper limb or finger graded as Brunnstrom stage (BrST) III or below received conventional therapies plus a once-weekly intramuscular injection of 20 U of calcitonin. This group of patients was
The incidence of CRPS in all patients with post-stroke hemiplegia during the control period was 8.2%. Among patients with severe stroke who received calcitonin, the incidence of CRPS was significantly lower compared with the control group (12.5% vs. 57.1%, p<0.001). CRPS was completely
11. Painful Hemiplegic Shoulder pg. 54 of 65
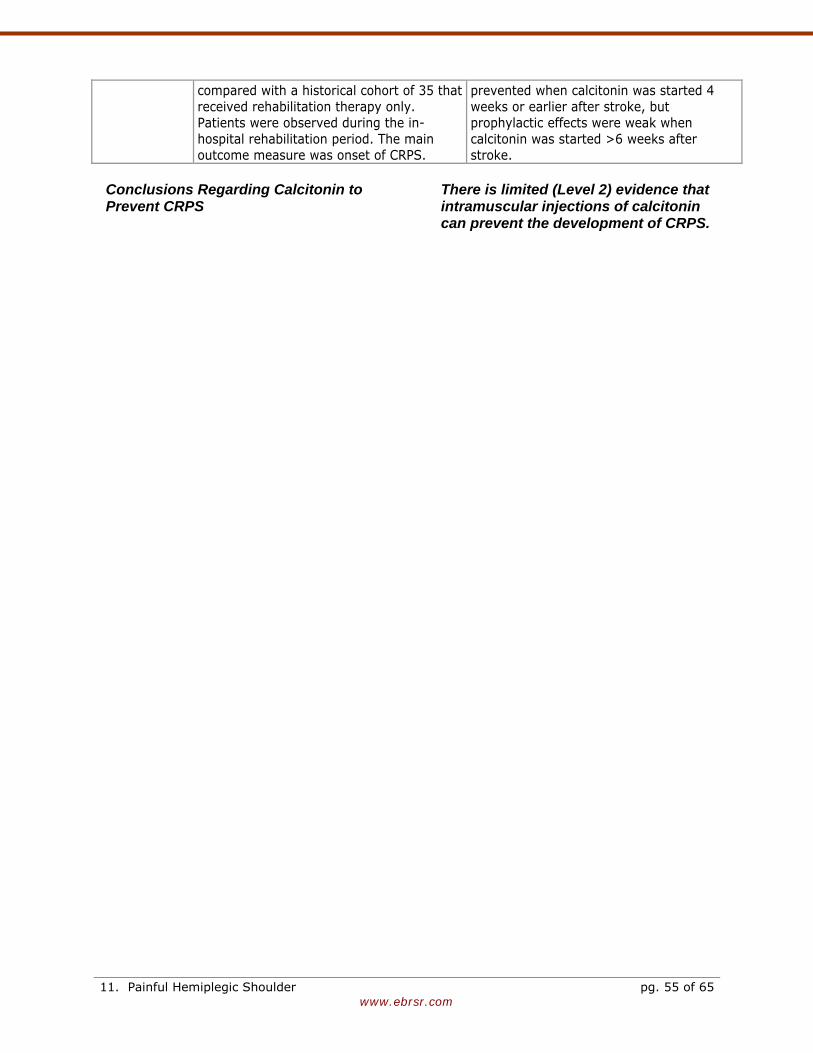
www.ebrsr.com
compared with a historical cohort of 35 that received rehabilitation therapy only. Patients were observed during the in-hospital rehabilitation period. The main outcome measure was onset of CRPS.
prevented when calcitonin was started 4 weeks or earlier after stroke, but prophylactic effects were weak when calcitonin was started >6 weeks after stroke.
Conclusions Regarding Calcitonin to Prevent CRPS
There is limited (Level 2) evidence that intramuscular injections of calcitonin can prevent the development of CRPS.
11. Painful Hemiplegic Shoulder pg. 55 of 65

www.ebrsr.com
11.8 Summary 1. Shoulder subluxation occurs early
following a stroke.
2. Hemiplegic shoulder pain is associated with shoulder subluxation and spasticity, but not with scapular rotation.
3. There appears to be an important r
for the subscapularis muscle and to a lesser extent pectoralis major musculature, which develop greater tonic activity on the hemiparetic side with subsequent muscle imbalance about the shoulder.
ole
vidence
vidence
t of 1b)
4. The development of painful
hemiplegic shoulder is associated with severe strokes and poorer functional outcome.
5. There is conflicting (Level 4) e
that prolonged positioning prevents loss of active or passive range of motion, or reduces pain.
6. There is limited (Level 2) evidence
that shoulder slings prevent subluxation associated with hemiplegic shoulder pain.
7. There is conflicting (Level 4) e
that strapping the hemiplegicshoulder reduces the developmenpain. There is moderate (Level evidence that strapping the hemiplegic shoulder does not improve range of motion or upper limb function.
8. There is moderate (Level 1b)
evidence that the use of overhead pullies results in hemiplegic shoulder pain and should be avoided.
9. There is moderate (Level 1b)
evidence that a gentle range of motion program by a therapist results
helps reduce hemiplegic shoulder pain.
10. There is limited (Level 2) evidence
that surgically resecting the subscapularis and pectoralis muscle tendons improves pain and range of motion in stroke patients with a painful hemiplegic shoulder.
11. There is limited (Level 2) evidence
that oral non-steroidal anti-inflammatories can reduce pain during therapy sessions.
12. There is strong (Level 1a) evidence
that that functional electrical stimulation does not reduce hemiplegic shoulder pain following stroke, but does reduce shoulder subluxation or prevent its development.
13. There is conflicting (Level 4)
evidence that botulinum toxin injected into the subscapularis muscle reduces spastic shoulder pain and improves passive range of motion of the hemiplegic shoulder.
14. There is conflicting (Level 4)
evidence that intra-articular steroid injections improve pain associated with hemiplegic shoulder. There is strong (Level 1a) evidence intra-articular steroid injections do not improve arm function compared with either botulinum toxin or placebo.
15. There is moderate (Level 1b)
evidence that subscapular nerve block reduces hemiplegic shoulder pain compared with ultrasound therapy.
16. There is moderate (Level 1b)
evidence that aromatherapy combing with acupressure can reduce pain
11. Painful Hemiplegic Shoulder pg. 56 of 65
www.ebrsr.com
associated with painful hemiplegic shoulder.
17. There is moderate (Level 1b)
evidence that massage therapy reduces pain and anxiety levels post-stroke.
18. CRPS is a poorly understood
clinical entity. Most cases improve with time.
19. There is moderate (Level 1b)
evidence that oral corticosteroids improves CRPS for at least the first 4 weeks.
20. There is moderate (Level 1b)
evidence that a modified imagery
program can reduce pain associated with shoulder-hand syndrome.
21. There is limited (Level 2) evidence
that passive range of motion exercises can prevent the development of CRPS-1.
22. There is strong (Level 1a) evidence
that mirror therapy can reduce pain associated with shoulder-hand syndrome.
23. There is limited (Level 2) evidence
that intramuscular injections of calcitonin can prevent the development of CRPS.
11. Painful Hemiplegic Shoulder pg. 57 of 65
www.ebrsr.com
References Acerra NE, Souvlis T, Moseley GL. Stroke,
complex regional pain syndrome and phantom limb pain: can commonalities direct future management? J Rehabil Med. 2007;39:109-114.
Ada L, Foongchomcheay A. Efficacy of electrical
stimulation in preventing or reducing subluxation of the shoulder after stroke: a meta-analysis. Aust J Physiother 2002; 48(4):257-267.
Ada L, Goddard E, McCully J, Stavrinos T,
Bampton J. Thirty minutes of positioning reduces the development of shoulder external rotation contracture after stroke: A randomized controlled trial. Arch Phys Med Rehabil 2005;86:230-234.
Ada L, Foongchomcheay A, Canning C.
Supportive devices for preventing and treating subluxation of the shoulder after stroke. Cochrane Database Syst Rev 2005;CD003863.
Ancliffe J. Strapping the shoulder in patients
following a cerebrovascular accident (CVA): A pilot study. Australian Journal of Physiotherapy 1992;38:37-39.
Aras MD, Gokkaya NK, Comert D, Kaya A,
Cakci A. Shoulder pain in hemiplegia: results from a national rehabilitation hospital in Turkey. Am J Phys Med Rehabil 2004;83:713-719
Arsenault AB, Silodean M, Duil E, Riley E.
Clinical significance of the V-shaped space in the subluxed shoulder of hemiplegics. Stroke 1991;22:867-871.
Ashford S, Turner-Stokes L. Management of
shoulder and proximal upper limb spasticity using botulinum toxin and concurrent therapy interventions: a preliminary analysis of goals and outcomes. Disabil Rehabil 2009;31:220-226.
Baker LL, Parker K. Neuromuscular electrical
stimulation of the muscles surrounding the shoulder. Phys Ther 1986;66:1930-1937.
Basmajian JV, Bazant FJ. Factors preventing
downward dislocation of adducted shoulder joint: electromyographic and morphological study. J Bone Joint Surg (Am) 1959;41:1182-1186.
Barlak A, Unsal S, Kaya K, Sahin-Onat S, Ozel
S. Poststroke shoulder pain in Turkish stroke patients: relationship with clinical factors and functional outcomes. Int J Rehabil Res 2009;32:309-315.
Bender L, Mckenna K. Hemiplegic shoulder
pain: Defining the problem and its management. Disabil Rehabil 2001;23(16):698-705.
Bhakta BB, Cozens JA, Bamford JM,
Chamberalin M. Use of botulinum toxin in stroke patients with severe upper limb spasticity. J Neurol Neurosurg Psychiatr 1996; 61:30-35.
Bloch R, Bayer N. Prognosis in stroke. Cl
Orthop Related Res 1978;131:10-14. Bobath B. Adult hemiplegia: Evaluation and
assessment (3rd ed). Heinemann, London, 1990.
Bohannon RW. Relationship between shoulder
pain and selected variables in patients with hemiplegia. Clin Rehabil 1988; 2: 111-117.
Bohannon RW, Andrews AW. Shoulder
subluxation and pain in stroke patients. Am J Occup Ther 1990; 44(6):507-509.
Bohannon RW, Larkin PA, Smith MB, Horton
MG. Shoulder pain in hemiplegia: statistical relationship with five variables. Arch Phys Med Rehabil 1986;67:514-516.
Boonsong P, Jaroenarpornwatana A, Boonhong
J. Preliminary study of suprascapular nerve block (SSNB) in hemiplegic shoulder pain. J Med Assoc Thai 2009;92:1669-1674.
Borisova Y, Bohannon RW. Positioning to
prevent or reduce shoulder range of motion impairments after stroke: a meta-analysis. Clin Rehabil 2009;23:681-686.
Boyd EA. Clinical measures of shoulder
subluxation: their reliability. Can J Public Health 1992;83 Suppl 2:524-8.
Braun RM, West F, Mooney V, Nickel RL, Roper
B, Caldwell C. Surgical treatment of the painful shoulder contracture in the stroke patient. J Bone Joint Surg (Am) 1971;53:1307-1312.
11. Painful Hemiplegic Shoulder pg. 58 of 65
11. Painful Hemiplegic Shoulder pg. 59 of 65 www.ebrsr.com
Braus DF, Krauss JK, Strobel J. The shoulder-hand syndrome after stroke: a prospective clinical trial. Ann Neurol 1994; 36(5):728-733.
Bruehl S, Harden RN, Galer BS, et al. External
validation of IASP diagnostic criteria for Complex Regional Pain Syndrome and proposed research diagnostic criteria. International Association for the Study of Pain. Pain 1999;81:147-154.
Brooke MM, de Lateur BJ, Diana-Rigby GC,
Questad KA. Shoulder subluxation in hemiplegia: effects of three different supports. Arch Phys Med Rehabil 1991;72:582-586.
Cacchio A, De BE, De B, V, Santilli V, Spacca
G. Mirror therapy in complex regional pain syndrome type 1 of the upper limb in stroke patients. Neurorehabil Neural Repair 2009a;23:792-799.
Cacchio A, De BE, Necozione S, di OF, Santilli
V. Mirror therapy for chronic complex regional pain syndrome type 1 and stroke. N Engl J Med 2009b;361:634-636.
Cailliet R. The shoulder in hemiplegia.
Philadelphia, PA, F.A. Davis Co., 1980. Caldwell CB, Wilson DJ, Brown RM. Evaluation
and treatment of the upper extremity in the hemiplegic stroke patient. Clin Orthop 1969;63:69-93.
Carr EK, Kenney FD. Positioning of the stroke
patient: a review of the literature. Int J Nurs Stud 1992;29(4):355-369.
Chae J, Yu DT, Walker ME, et al. Intramuscular
Electrical Stimulation for Hemiplegic Shoulder Pain: A 12-Month Follow-Up of a Multiple-Center, Randomized Clinical Trial. Am J Phys Med Rehabil 2005;84:832-842.
Chae J, Ng A, Yu DT, et al. Intramuscular
electrical stimulation for shoulder pain in hemiplegia: does time from stroke onset predict treatment success? Neurorehabil Neural Repair 2007;21:561-567.
Chae J, Mascarenhas D, Yu DT, Kirsteins A,
Elovic EP, Flanagan SR, Harvey RL, Zorowitz RD, Fang ZP. Poststroke shoulder pain: its relationship to motor impairment, activity limitation, and quality of life. Arch Phys Med Rehabil 2007;88:298-301.
Chae J, Jedlicka L. Subacromial corticosteroid injection for poststroke shoulder pain: an exploratory prospective case series. Arch Phys Med Rehabil 2009;90:501-506.
Chaco J, Wolf E. Subluxation of the
glenohumeral joint in hemiplegia. Am J Phys Med 1971; 50:139-143.
Chantraine A, Baribeault A, Uebelhart D,
Gremion G. Shoulder pain and dysfunction in hemiplegia: effects of functional electrical stimulation. Arch Phys Med Rehabil 1999;80:328-331.
Chu Ds, Petrillo C, Davis SW, Eichberg R.
Shoulder-hand syndrome: Importance of early diagnosis and treatment. J Am Ger Soc 1981; 29:58-60.
Church C, Price C, Pandyan AD, Huntley S,
Curless R, Rodgers H. Randomized Controlled Trial to Evaluate the Effect of Surface Neuromuscular Electrical Stimulation to the Shoulder After Acute Stroke. Stroke 2006;37:2995-3001.
Codman EA. The Shoulder. Boston, Thomas
Todd Co, 1934. Cole TM, Tobis JS. Measurement of
musculoskeletal function. In: Kottke FJ, Lehmann JF (eds). Krusen's Handbook of Physical Medicine and Rehabilitation. Philadelphia, Saunders, p.25, 1990.
Crossens-Sills J, Schenkman M. Analysis of
shoulder pain, range of motion, and subluxation in patients with hemiplegia. Phys Ther 1985; 65:731.
Culham EG, Noce RR, Bagg SD. Shoulder
complex position and glenohumeral subluxation in hemiplegia. Arch Phys Med Rehabil 1995;76:857-64.
Daviet JC, Preux PM, Salle JY, Lebreton F,
Munoz M, Dudognon P, Pelissier J, Perrigot M. Clinical factors in the prognosis of complex regional pain syndrome type I after stroke: a prospective study. Am J Phys Med Rehabil 2002;81:34-39.
Davis SW, Pestrillo CR, Eischberg RD, Chu DS.
Shoulder-hand syndrome in a hemiplegic population: a 5-year retrospective study. Arch Phys Med Rehab 1977;58:353-355.
11. Painful Hemiplegic Shoulder pg. 60 of 65 www.ebrsr.com
Dean CM, Mackey FH, Katrak P. Examination of shoulder positioning after stroke: A randomised controlled pilot trial. Aust J Physiother 2000;46:35-40.
de Boer KS, Arwert HJ, de Groot JH, Meskers
CG, Mishre AD, Arendzen JH. Shoulder pain and external rotation in spastic hemiplegia do not improve by injection of botulinum toxin A into the subscapular muscle. J Neurol Neurosurg Psychiatry 2008;79:581-583.
de Jong LD, Nieuwboer A, Aufdemkampe G.
Contracture preventive positioning of the hemiplegic arm in subacute stroke patients: a pilot randomized controlled trial. Clin Rehabil. 2006;20:656-667.
Dekker JH, Wagenaar RC, Lankhorst GJ, de
Jong BA. The painful hemiplegic shoulder: effects of intra-articular triamcinolone acetonide. Am J Phys Med Rehabil 1997;76:43-48.
Dromerick AW, Edwards DF, Kumar A.
Hemiplegic shoulder pain syndrome: frequency and characteristics during inpatient stroke rehabilitation. Arch Phys Med Rehabil 2008;89:1589-1593.
Eto F, Yoshikawa M, Ueda S, Hirai S. Post-
hemiplegic shoulder-hand syndrome with special reference to related cerebral localization. J Am Ger Soc 1980;28:13-17.
Faghri PD, Rodgers MM, Glaser RM, Bors JG,
Ho C, Akuthota P. The effects of functional electrical stimulation on shoulder subluxation, arm function recovery, and shoulder pain in hemiplegic stroke patients. Arch Phys Med Rehabil 1994;75:73-79.
Faghri PD. The effects of neuromuscular
stimulation-induced muscle contraction versus elevation on hand edema in CVA patients. J Hand Ther 1997;10:29-34.
Fil A, Armutlu K, Atay AO, Kerimoglu U, Elibol
B. The effect of electrical stimulation in combination with Bobath techniques in the prevention of shoulder subluxation in acute stroke patients. Clin Rehabil 2010. (e-publ)
Fitzgerald-Finch OP, Gibson II: Subluxation of
shoulder in hemiplegia. Age Ageing 1975;4:16-18.
Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S. Post-stroke hemiplegic patient: I. Method for evaluation of physical performance. Scand J Rehab Med 1975;7:13-31.
Gamble GE, Barberan E, Bowsher D, Tyrrell PJ,
Jones AK. Post stroke shoulder pain: more common than previously realized. Eur J Pain 2000;4:313-315
Gamble GE, Barberan E, Laasch HU, Bowsher
D, Tyrrell PJ, Jones AK. Poststroke shoulder pain: a prospective study of the association and risk factors in 152 patients from a consecutive cohort of 205 patients presenting with stroke. Eur J Pain 2002;6:467-474.
Geurts A, Visschers B, van Limbeek J, Ribbers
G. Systematic review of aetiology and treatment of post-stroke hand oedema and shoulder-hand syndrome. Scan J Rehab Med 2000;32:4-10.
Gilmore PE, Spaulding SJ, Vandervoort AA.
Hemiplegic shoulder pain: implications for occupational therapy treatment. Can J Occup Ther 2004; 71(1):36-46.
Gokkaya NK, Aras M, Yesiltepe E et al. Reflex
sympathetic dystrophy in hemiplegia. Int J Rehabil Res. 2006;29:275-279.
Griffin A, Bernhardt J. Strapping the hemiplegic
shoulder prevents development of pain during rehabilitation: a randomized controlled trial. Clin Rehabil 2006; 20(4):287-295.
Gresham GE, Duncan PW, Staston WB, et al.
Post-Stroke Rehabilitation Guideline Panel. Post-Stroke Rehabilitation. Clinical Practice Guidelilne No. 16 CAHCPR Publication No. 95-0662), Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research, May 1995.
Griffin A, Bernhardt J. Strapping the hemiplegic
shoulder prevents development of pain during rehabilitation: a randomized controlled trial. Clin Rehabil 2006; 20(4):287-295.
Gustafsson L, McKenna K. A programme of
static positional stretches does not reduce hemiplegic shoulder pain or maintain shoulder range of motion--a randomized
11. Painful Hemiplegic Shoulder pg. 61 of 65 www.ebrsr.com
controlled trial. Clin Rehabil 2006; 20(4):277-286.
Hakuno A, Sashika H, Ohkawa T, Itoh R.
Arthrographic findings in hemiplegic shoulders. Arch Phys Med Rehab 1984; 65:706-711.
Hanger HC, Whitewood P, Brown G, Ball MC,
Harper J, Cox R, Sainsbury R. A randomized controlled trial of strapping to prevent post-stroke shoulder pain. Clin Rehabil 2000;14:370-380.
Hecht JS. Subscapular nerve block in the
painful hemplegic shoulder. Arch Phys Med Rehabil 1992;73:1036-1039.
Hecht JS. The role of spasticity in hemiplegic
shoulder pain and what to do about it. 57th Annual Assembly of American Academy of Physical Medicine and Rehabilitation, Orlando, Florida, November 17, 1995, pp. 248-255.
Hollinshead WH, Jenkins DB. Functional
anatomy of the limbs and back. Philadelphia, Saunders p.105, 1981.
Huang YC, Liang PJ, Pong YP, Leong CP, Tseng
CH. Physical findings and sonography of hemiplegic shoulder in patients after acute stroke during rehabilitation. J Rehabil Med 2010;42:21-26.
Hurd MM, Farrell KH, Waylonis GW. Shoulder
sling for hemiplegia: friend or foe? Arch Phys Med Rehabil 1974;55:519-522.
Ikai T, Tei K, Yoshida K, Miyano S, Yonemoto
K. Evaluation and treatment of shoulder subluxation in hemiplegia: relationship between subluxation and pain. Am J Phys Med Rehabil 1998; 77(5):421-426.
Inaba MK, Piorkowski M. Ultrasound in
treatment of painful shoulder in patients with hemiplegia. J Phys Ther 1972;52:737-741.
Iwata M, Kondo I, Sato Y, Satoh K, Soma M,
Bar-Or O. Prediction of reflex sympathetic dystrophy in hemiplegia by evaluation of hand edema. Arch Phys Med Rehabil 2002; 83(10):1428-1431.
Janig W, Baron R. Complex regional pain
syndrome is a disease of the central nervous system. Clin Auton Res 2002;12:150-164.
Jespersen HF, Jorgensen HS, Nakayama H, Olsen TS. Shoulder pain after a stroke. Int J Rehabil Res 1995;18:273-276.
Johnstone M. The stroke patient: Principles of
rehabilitation. Churchill Livingstone, Edinburgh, 1982.
Joynt RL. The source of shoulder pain in
hemiplegia. Arch Phys Med Rehabil 1992;73:409-413.
Kaplan M. Hemiplegic shoulder pain--early
prevention and rehabilitation. West J Med. 1995 Feb;162(2):151-2.
Kaplan PE, Meredith J, Taft G, Betts HB.
Stroke and brachial plexus injury: A difficult problem. Arch Phys Med Rehab 1977;38:415-18.
Kalita J, Vajpayee A, Misra UK. Comparison of
prednisolone with piroxicam in complex regional pain syndrome following stroke: a randomized controlled trial. QJM 2006;99:89-95.
Kingery WS, Date ES, Bobobo CR. The
absence of brachial plexus injury in stroke. AM J Phys Med Rehab 1993; 72:127-175.
Kobayashi H, Onishi H, Ihashi K, Yagi R, Handa
Y. Reduction in subluxation and improved muscle function of the hemiplegic shoulder joint after therapeutic electrical stimulation. J Electromyogr Kinesiol 1999;9:327-336.
Kocabas H, Levendoglu F, Ozerbil OM, Yuruten
B. Complex regional pain syndrome in stroke patients. Int J Rehabil Res 2007;30:33-38.
Kondo I, Hosokawa K, Soma M, Iwata M,
Maltais D. Protocol to prevent shoulder-hand syndrome after stroke. Arch Phys Med Rehabil 2001; 82(11):1619-1623.
Kong KH, Neo JJ, Chua KS. A randomized
controlled study of botulinum toxin A in the treatment of hemiplegic shoulder pain associated with spasticity. Clin Rehabil. 2007;21:28-35.
Koog YH, Jin SS, Yoon K, Min BI. Interventions
for hemiplegic shoulder pain: systematic review of randomised controlled trials. Disabil Rehabil 2010;32:282-291.
11. Painful Hemiplegic Shoulder pg. 62 of 65 www.ebrsr.com
Koyuncu E, Nakipoglu-Yuzer GF, Dogan A, Ozgirgin N. The effectiveness of functional electrical stimulation for the treatment of shoulder subluxation and shoulder pain in hemiplegic patients: A randomized controlled trial. Disabil Rehabil 2010;32:560-566.
Kozin F, McCarty D, Sims J. Genant H. Reflex
sympathetic dystrophy: I. Clinical and histological studies: evidence for bilaterality, response to corticosteroids and articular involvement. Am J Med 1976;60:321-331(a).
Kozin F, Genant HK, Bekerman C, McCarty DJ.
Reflex sympathetic dystrophy syndrome: II. Roentgenographic and scintigraphic evidence of bilaterality and of periarticular accentuation. Am J Med 1976;60:332-338(b).
Kozin F, Ryan LM, Carrera GF, Soin JS,
Wortman RL. Reflex sympathetic dystrophy syndrome (RSDS): III Scintigraphic studies, further evidence for the therapeutic efficacy of systemic corticosteroids, and proposed diagnostic criteria. Am J Med 1981;70 23-30.
Kozin F. Two unique shoulder disorders:
Adhesive capsulitis and reflex sympathetic dystrophy syndrome. Postgrad Med 1983;73(5):207-216.
Kumar R, Metter EJ, Mehta AJ, Chew T.
Shoulder pain in hemiplegia. The role of exercise. Am J Phys Med Rehabil 1990; 69(4):205-208.
Langhorne P, Stott DJ, Robertson L, MacDonald
J, Jones L, McAlpine C, Dick F, Taylor GS, Murray G. Medical complications after stroke: a multicenter study. Stroke 2000;31:1223-1229.
Laske E, Gunduz B, Celik EC. The effects of
local shoulderinjections in hemiplegic shoulder pain. Am J Phys Med Rehabil 2009;88:805-814.
Lee IS, Shin YB, Moon TY, Jeong YJ, Song JW,
Kim DH. Sonography of patients with hemiplegic shoulder pain after stroke: correlation with motor recovery stage. AJR Am J Roentgenol 2009;192:W40-W44.
Lieberman JS. Hemiplegia: Rehabilitation of
the upper extremity. In: Kaplan PE, Cerullo
LJ (eds.): Stroke Rehabilitation. Stoneman, MA, Butterworth Publishers, p.95-117, 1986.
Lim JY, Koh JH, Paik NJ. Intramuscular
botulinum toxin-A reduces hemiplegic shoulder pain: a randomized, double-blind, comparative study versus intraarticular triamcinolone acetonide. Stroke 2008;39:126-131.
Lindgren I, Jonsson AC, Norrving B et al.
Shoulder pain after stroke: a prospective population-based study. Stroke . 2007;38:343-348.
Linn SL, Granat MH, Lees KR. Prevention of
shoulder subluxation after stroke with electrical stimulation. Stroke 1999;30:963-968.
Lo SF, Chen SY, Lin HC, Jim YF, Meng NH, Kao
MJ. Arthrographic and clinical findings in patients with hemiplegic shoulder pain. Arch Phys Med Rehabil 2003;84:1786-1791.
Lynch D, Ferraro M, Krol J, Trudell CM, Christos
P, Volpe BT. Continuous passive motion improves shoulder joint integrity following stroke. Clin Rehabil 2005;19:594-599.
Marco E, Duarte E, Vila J et al. Is botulinum
toxin type A effective in the treatment of spastic shoulder pain in patients after stroke? A double-blind randomized clinical trial. J Rehabil Med. 2007;39:440-447.
Matayoshi S, Shimodozono M, Hirata Y, Ueda
T, Horio S, Kawahira K. Use of calcitonin to prevent complex regional pain syndrome type I in severe hemiplegic patients after stroke. Disabil Rehabil 2009;31:1773-1779.
Mok E, Woo CP. The effects of slow-stroke back
massage on anxiety and shoulder pain in elderly stroke patients. Complement Ther Nurs Midwifery 2004;10:209-216.
Moodie NB, Brisbin J, Morgan AM. Subluxation
of the glenohumeral joint in hemiplegia: Evaluation of supportive devices. Physiother Can 1986;38:151-157.
Morin L, Bravo G. Strapping the hemiplegic
shoulder: A radiographic evaluation of its efficacy to reduce subluxation. Physiother Can 1997; 49:103-108.
Moseley GL. Graded motor imagery is effective
for long-standing complex regional pain
11. Painful Hemiplegic Shoulder pg. 63 of 65 www.ebrsr.com
syndrome: a randomised controlled trial. Pain 2004;108:192-198.
Moskowitz E. Complications in rehabilitation of
hemiplegic patients. Med Clin North Am 1969;53 541-559(a).
Moskowitz E, Goodman CR, Smith E, Balthazar
E, Mellins HZ. Hemiplegic shoulder. NY State J Med 1969; 69:548-550(b).
Najenson T, Yacubovich E, Pikelini S. Rotator
cuff injury in hemiplegic patients. Scand J Rehab Med 1971; 3:131-137.
Nepomuceno CS, Miller JM III. Shoulder
arthrography in hemiplegic patients. Arch Phys Med Rehab 1974; 55:49-51.
Paci M, Nannetti L, Rinaldi LA. Glenohumeral
subluxation in hemiplegia: An overview. J Rehabil Res Dev 2005; 42(4):557-568.
Partridge CJ, Edwards SM, Mee R, Van
Langenberghe HV. Hemiplegic shouldar pain: a study of two methods of phsyiotherapy treatment. Clin Rehabil 1990;4:43-49.
Patterson JR, Zabransky R, Grabois M, Ferro P.
Evaluation of the effectivenss of sling orthoses for the correction of glenhummeral subluxation in the hemiplegic. Archives Phys Med Rehabil 1984;65:635.
Pedreira G, Cardoso E, Melo A. Botulinum toxin
type A for refractory post-stroke shoulder pain. Arq Neuropsiquiatr 2008;66:213-215.
Perrigot M, Bussel B, Pierrot Deseilligny E, Held
JP. L'epaule de l'hemiplegique. Ann Med Phys 1975;18:175-187.
Pertoldi S, Di BP. Shoulder-hand syndrome
after stroke. A complex regional pain syndrome. Eura Medicophys 2005;41:283-292.
Petchkrua W, Weiss DJ, Patel RR.
Reassessment of the incidence of complex regional pain syndrome type 1 following stroke. Neurorehabil Neural Repair 2000;14:59-63.
Poduri KR. Shoulder pain in stroke patients
and its effects on rehabilitation. J Stroke Cerebrovasc Dis 1993;3:261-266.
Post MW, Visser-Meily JM, Boomkamp-Koppen HG, Prevo AJ. Assessment of oedema in stroke patients: comparison of visual inspection by therapists and volumetric assessment. Disabil Rehabil 2003;25:1265-1270.
Poulin de Courval L, Barsauskas A, Berenbaum
B, Dehaut F, Dussault R, Fontaine FS, Labrecque R, Leclerc C, Giroux F. Painful shoulder in the hemiplegic and unilateral neglect. Arch Phys Med Rehabil. 1990 Aug;71(9):673-6.
Prevost R, Arsenault AB, Dutil E, Drouin G.
Rotation of the scapular and shoulder subluxation in hemiplegia. Arch Phys Med Rehab 1987;68:786-790.
Price CI, Pandyan AD. Electrical stimulation for
preventing and treating post-stroke shoulder pain: a systematic Cochrane review. Clin Rehabil 2001;15:5-19.
Quisel A, Gill JM, Witherell P. Complex regional
pain syndrome: which treatments show promise? J Fam Pract 2005;54:599-603.
Quisel A, Gill JM, Witherell P. Complex regional
pain syndrome underdiagnosed. J Fam Pract 2005;54:524-532.
Rajaratnam BS, Venketasubramanian N,
Kumar PV, Goh JC, Chan YH. Predictability of simple clinical tests to identify shoulder pain after stroke. Arch Phys Med Rehabil 2007;88:1016-1021.
Ratnasabapathy Y, Broad J, Baskett J, Pledger
M, Marshall J, Bonita R. Shoulder pain in people with a stroke: a population-based study. Clin Rehabil 2003;17:304-311.
Rizk TE, Christopher RP, Pinals RS, Salazar JE,
Higgins C. Arthrographic studies in painful hemiplegic shoulders. Arch Phys Med Rehab 1984;65:254-55.
Rommel O, Malin JP, Zenz M, Janig W.
Quantitative sensory testing, neurophysiological and psychological examination in patients with complex regional pain syndrome and hemisensory deficits. Pain 2001;93:279-293.
Roper TA, Redford S, Tallis RC. Intermittent
compression for the treatment of the oedematous hand in hemiplegic stroke: a
11. Painful Hemiplegic Shoulder pg. 64 of 65 www.ebrsr.com
randomized controlled trial. Age Ageing 1999;28:9-13.
Roy CW, Sands M, Hill L, Harrison, Marshall S.
The effect of shoulder pain on outcome of acute hemiplegia. Clin Rehabil 1995;9:21-27.
Roy CW, Sands MR, Hill LD. Shoulder pain in
acutely admitted hemiplegics. Clinical Rehabilitation 1996;18:497-501.
Renzenbrink GJ, IJzerman MJ. Percutaneous
neuromuscular electrical stimulation (P-NMES) for treating shoulder pain in chronic hemiplegia. Effects on shoulder pain and quality of life. Clin Rehabil 2004;18:359-365.
Sackley C, Brittle N, Patel S, Ellins J, Scott M,
Wright C, Dewey ME. The prevalence of joint contractures, pressure sores, painful shoulder, other pain, falls, and depression in the year after a severely disabling stroke. Stroke 2008;39:3329-3334.
Savage R, Robertson L. Relationship between
adult hemiplegic shoulder pain and depression. Physiother Can 1982;34:86-90.
Shah RR, Haghpanah S, Elovic EP, Flanagan
SR, Behnegar A, Nguyen V, Page SJ, Fang ZP, Chae J. MRI findings in the painful poststroke shoulder. Stroke 2008;39:1808-1813.
Shahani BT, Kelly EB, Glasser S. Hemiplegic
shoulder subluxation. Arch Phys Med Rehab 1981;62:519.
Shai G, Ring H, Costeff H, Solzi P.
Glenohumeral malalignment in hemiplegic shoulder. Scan J Rehab Med 1984; 16:133-136.
Shin BC, Lee MS. Effects of aromatherapy
acupressure on hemiplegic shoulder pain and motor power in stroke patients: a pilot study. J Altern Complement Med. 2007;13:247-251.
Snels IA, Beckerman H, Twisk JW, Dekker JH,
Peter DK, Koppe PA, Lankhorst GJ, Bouter LM. Effect of triamcinolone acetonide injections on hemiplegic shoulder pain : A randomized clinical trial. Stroke 2000;31:2396-2401.
Snels IA, Dekker JH, van der Lee JH, Lankhorst GJ, Beckerman H, Bouter LM. Treating patients with hemiplegic shoulder pain. Am J Phys Med Rehabil 2002;81:150-160.
Stanton-Hicks M, Janig W, Hassenbusch S,
Haddox JD, Boas R, Wilson P. Reflex sympathetic dystrophy: changing concepts and taxonomy. Pain 1995;63:127-133.
Steinbrocker D. Shoulder-hand syndrome: present perspective. Arch Phys Med Rehab 1969;49:388-395.
Suethanapornkul S, Kuptniratsaikul PS,
Kuptniratsaikul V, Uthensut P, Dajpratha P, Wongwisethkarn J. Post stroke shoulder subluxation and shoulder pain: a cohort multicenter study. J Med Assoc Thai 2008;91:1885-1892.
Tahmoush AJ. Causalgia: redefinition as a
clinical pain syndrome. Pain 1981;10:187. Tepperman PS, Greyson ND, Hilbert L, et al.
Reflex sympathetic dystrophy in hemiplegia. Arch Phys Med Rehab 1984;65(8):442-447.
Tyson SF and Chissim C. The immediate effect
of handling technique on range of movement in the hemiplegic shoulder. Clin Rehabil 2002;16:137-140.
Van Ouwenwaller C, Laplace PM, Chantraine A.
Paniful shoulder in hemiplegia. Arch Phys Med Rehabil 1986; 67:23-26.
Veldman PH, Reynen HM, Arntz IE, Goris RJ.
Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet 1993;342:1012-1016.
Walsh K. Management of shoulder pain in
patients with stroke. Postgrad Med J 2001;77:645-649.
Wang RY, Chan RC, Tsai MW. Functional
electrical stimulation on chronic and acute hemiplegic shoulder subluxation. Am J Phys Med Rehabil 2000;79:385-390.
Wanklyn P. The painful hemiplegic shoulder:
pathogenesis, diagnosis and management. Rev Clin Gerontol 1994;4:245-251.
Wanklyn P, Forester A, Young J. Hemiplegics
houlder pain (HSP): natural history and investigation of associated features. Disabil Rehabil 1996;18:497-501.
11. Painful Hemiplegic Shoulder pg. 65 of 65 www.ebrsr.com
Williams R, Taffs L, Minuk T. Evaluation of two support methods for the subluxated shoulder of hemiplegic patients. Phys Ther 1988;68:1209-1214.
Yelnik AP, Colle FM, Bonan IV, Vicaut E.
Treatment of shoulder pain in spastic hemiplegia by reducing spasticity of the subscapular muscle : A randomized, double-blind, placebo-controlled study of botulinum toxin A. J Neurol Neurosurg Psychiatry 2007;78 :845-848.
Yu DT, Chae J, Walker ME, Hart RL, Petroski
GF. Comparing stimulation-induced pain during percutaneous (intramuscular_ and transcutaneous neuromuscular electric stimulation for treatment shoulder subluxation in hemiplegia. Arch Phys Med Rehabil 2001;82:756-60.
Zorowitz RD, Idank D, Ikai T, Hughes MB,
Johnston MV. Shoulder subluxation after stroke: A comparison of four supports. Arch Phys Med Rehabil 1995;76:763-771.
Zorowitz RD, Hughes MB, Idank D, Ikai T,
Johnston V. Shoulder pain and subluxation after stroke: Correlation or coincidence? Am JOccup Ther 1996;50:194-201.