molecular diagnosis of genetic epilepsy nagi alhaj prof of molecular biology assist, faculty...
TRANSCRIPT

MOLECULAR DIAGNOSIS OF GENETIC EPILEPSY
Nagi ALHajProf of Molecular Biology
Assist,Faculty Medicine ,
Sana’a ,University, YemenConsultant of Genetic Center 48
MH

Overview on Genetic EpilepsyA genetic contribution to etiology has been estimated to be present in about 40% of patients with epilepsy..
Three major groups:
•Mendelian disorders, in which a single major locus can account for segregation of the disease trait
•Non-mendelian or 'complex' diseases, in which the pattern of familial clustering can be accounted for by the interaction of the maternal inheritance pattern of mitochondrial DNA
•Chromosomal disorders, in which a gross cytogenetic abnormality is present.

• The ‘common’ non-familial idiopathic epilepsies tend to display ‘complex’ inheritance.
• They including various forms of
• Idiopathic generalised epilepsy (IGE)
• Juvenile myoclonic epilepsy (JME)
• Childhood absence epilepsy (CAE)

Genetics and Mutation • Mutations in over 2,000 genes have now been identified in
patients with more than 3,000 different disease phenotypes.
For the clinicians and their patients, it is becoming increasingly
important to obtain a genetic diagnosis
• Identifying the genetic aetiology of a disease may influence clinical management and will provide information regarding risk to future pregnancies.
• With the advent of high-throughput capillary sequencers and sequence analysis software, direct sequencing provides an accurate method for single gene analysis.
The inheritance pattern can be
autosomal dominant, autosomal recessive, or X-linked.
Mutations in a single gene may be associated with different types of seizures (clinical heterogeneity),
and, conversely, mutations in different genes can cause the same epilepsy phenotype (genetic heterogeneity).

Traditional nomenclature of inherited epilepsy:
Different mutations in different genes can result in similar phenotypes
Different mutations within one gene can result in different phenotypes
Different mutations in different genes can result in different phenotypes
An identical mutation within one gene can result in different phenotypes in different individuals (cause: environment, other genes)

Mutation identification begins with aphenotype and proceeds toward the genotype
genotype phenotype



The diagram showsthe distribution of all genetic differences that had been mapped to chromosome 1 at the time this diagram was drawn.

mutationsite
Mutation identification by linkage analysis
• Genome scan has been replaced by mutational analysis but in a small number of families in whom the mutation cannot be identified
• Remains the only method for the genetic diagnosis of carriers.
Mutational analysis can be used to identify cells or DNA that have genotype and allele frequency differences from the normal genome.

Mutant alleles generating defects in particular proteins could disrupt the dance .
Cells homozygous for a mutant allele might be unable to complete chromosome duplication or mitosis or cytokinesis because a required component of the molecular machinery is missing or unable to function.
A genetic map of part of the human
X chromosome.

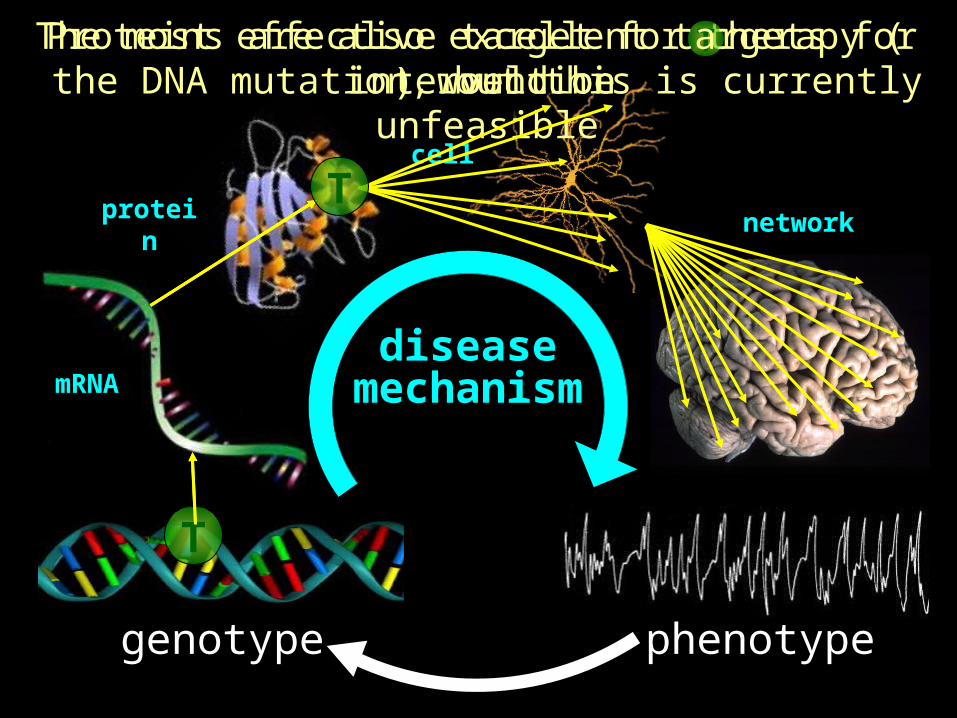
genotype phenotype
mechanismdisease
Elucidation of a disease mechanism presents a much more complex set of challenges
mRNA
protein
cell
network

genotype phenotype
The number of potential defects increasesexponentially with each emergent stage of complexity
mRNA
protein
cell
network
mechanismdisease
Not all potential defects arise from each mutation

cell
network
genotype phenotype
Not all potential defects arise from each mutation
mRNA
protein
mechanismdisease
The most effective target for therapy ( ) would bethe DNA mutation, but this is currently unfeasible
T
T
cell
network
genotype phenotype
mRNA
protein
mechanismdisease
The most effective target for therapy ( ) would bethe DNA mutation, but this is currently unfeasible
T
T
T
Proteins are also excellent targets for intervention
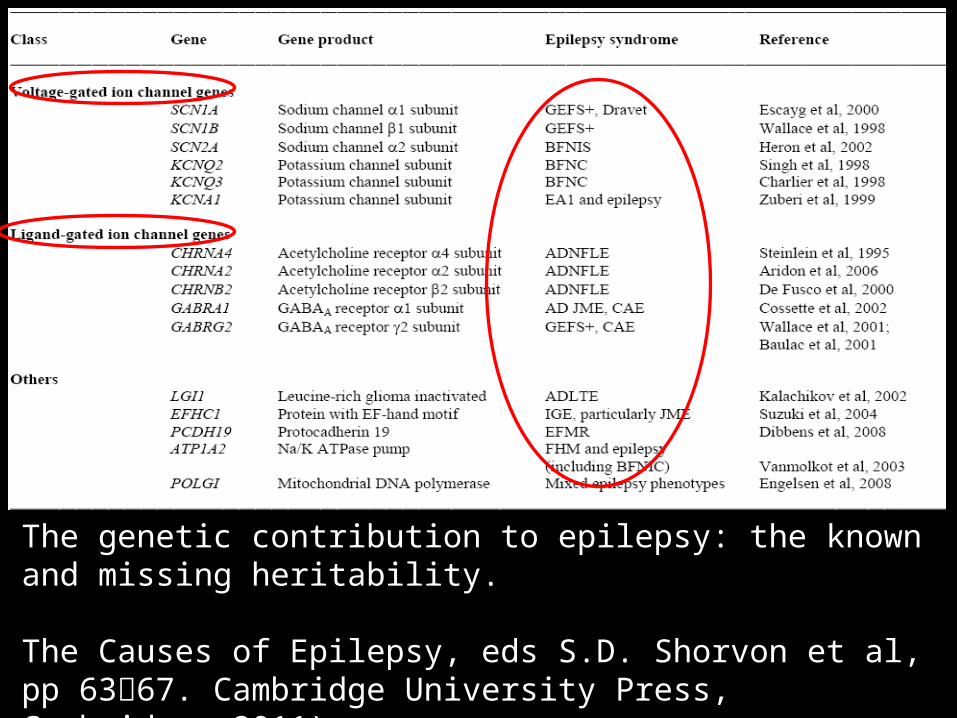
The genetic contribution to epilepsy: the known and missing heritability.
The Causes of Epilepsy, eds S.D. Shorvon et al, pp 6367. Cambridge University Press, Cambridge, 2011).
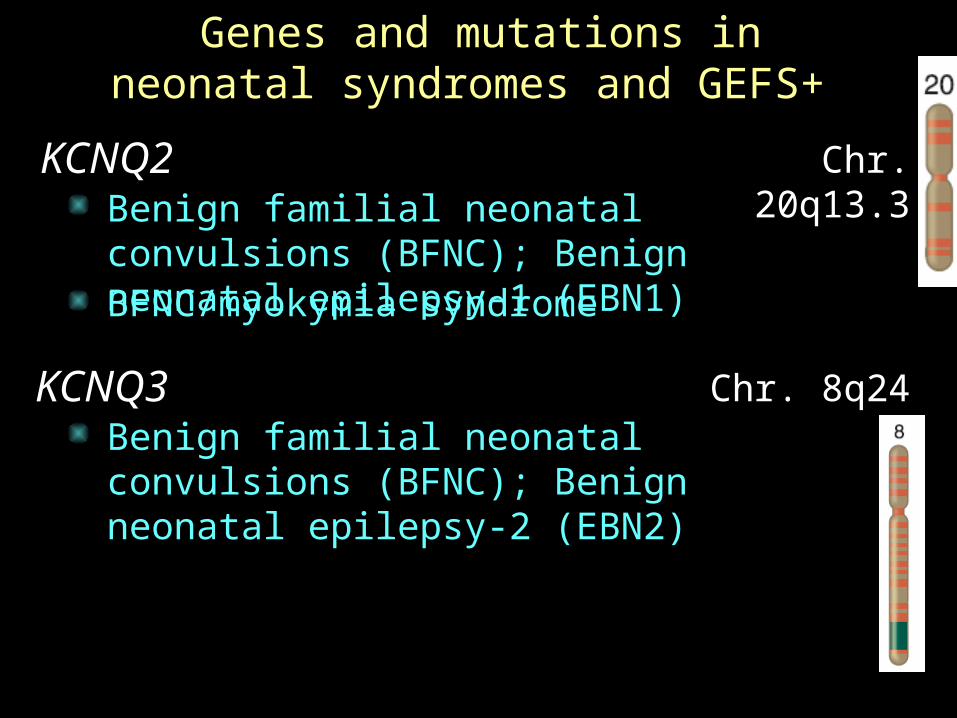
Genes and mutations in neonatal syndromes and GEFS+
KCNQ2 Chr. 20q13.3Benign familial neonatal convulsions (BFNC); Benign neonatal epilepsy-1 (EBN1)BFNC/myokymia syndrome
KCNQ3 Chr. 8q24Benign familial neonatal convulsions (BFNC); Benign neonatal epilepsy-2 (EBN2)
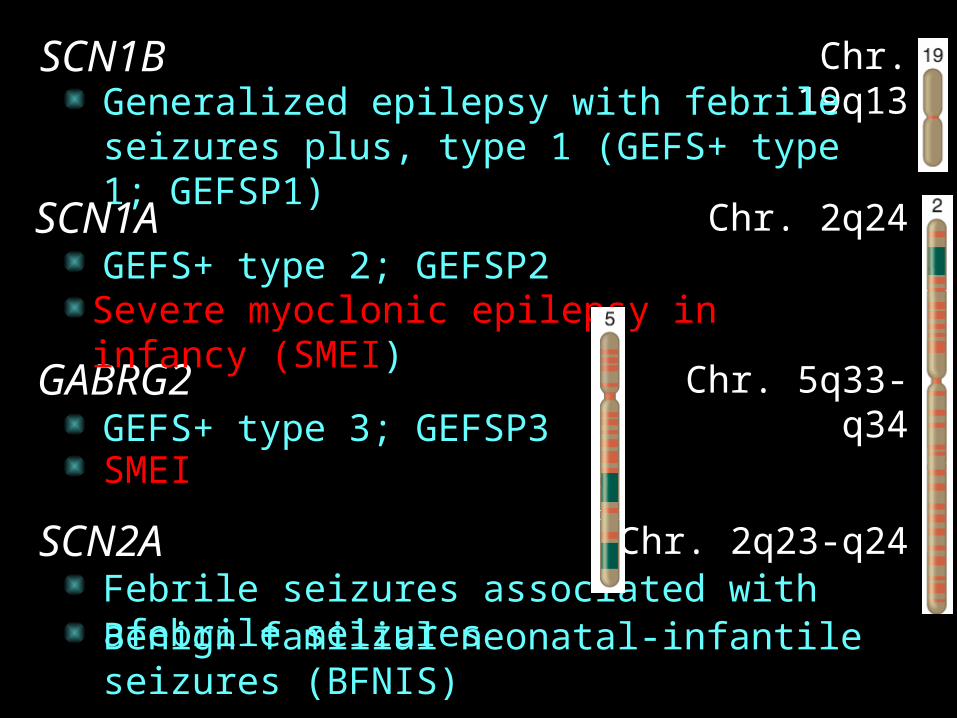
SCN1B Chr. 19q13Generalized epilepsy with febrile seizures plus, type 1 (GEFS+ type 1; GEFSP1)
SCN1A Chr. 2q24GEFS+ type 2; GEFSP2
GABRG2 Chr. 5q33-q34GEFS+ type 3; GEFSP3
SCN2A Chr. 2q23-q24Febrile seizures associated with afebrile seizures
Severe myoclonic epilepsy in infancy (SMEI)
SMEI
Benign familial neonatal-infantile seizures (BFNIS)

Unknown Chr. 19q12-q13.1Benign familial infantile convulsions, type 1 (BFIS type 1; BFIC1)
Unknown Chr. 16p12-q12BFIS type 2; BFIC2
Unknown Chr. 16p12-p11.2Rolandic epilepsy, paroxysmal exercise-induced dystonia, writer's cramp (RE-PED-WC)
Unknown Chr. 16p13Autosomal recessive (familial) benign idiopathic myoclonic epilepsy of infancy (FIME)
Paroxysmal kinesigenic choreoathetosis (PKC)
Infantile convulsions and paroxysmal choreoathetosis (ICCA)

Traditional nomenclature of inherited epilepsy:
Syndrome “A”:
Gene 1 Gene 2 Gene 3 Gene 4
Phenotype:
Syndrome “B”:
Syndrome “C”:
Syndrome “D”:
Syndrome “E”:
Syndrome “F”:
Syndrome “G”:
etc…
Gene 1 Gene 2 Gene 3 Gene 4
BB
Gene 2 Gene 1
Gene 3 Gene 1
Gene 1
Gene 4
Gene 2
Gene 2
Gene 3
D F,G EEEC CCA A A AAMutations:

Gene-centric nomenclature of inherited epilepsy:
Gene 1: Phenotypic range A, B, C, D
etc…
Gene 2:
Gene 3:
Gene 4:
Phenotypic range A, B, E, F, G
Phenotypic range A, S, E
Phenotypic range A, E
Both “Traditional” and “Gene-centric” nomenclatures have specific advantages and disadvantages
Gene 1 Gene 2 Gene 3 Gene 4
AMutations:
BPhenotype: AB C D A ACF,G EEE CA
Molecular Diagnosis

PATIENT HISTORY FOR MOLECULAR GENETIC TESTING
(1) The Infantile Epilepsy includes sequencing and deletion/duplication analysis of 38 genes causing Mendelian forms of epilepsy with onset of seizures during the first year of life.
38 gene activity, including•voltage-gated sodium channels,• the voltage-gated calcium channels,• and gamma-aminobutyric acid (GABAA) receptors.

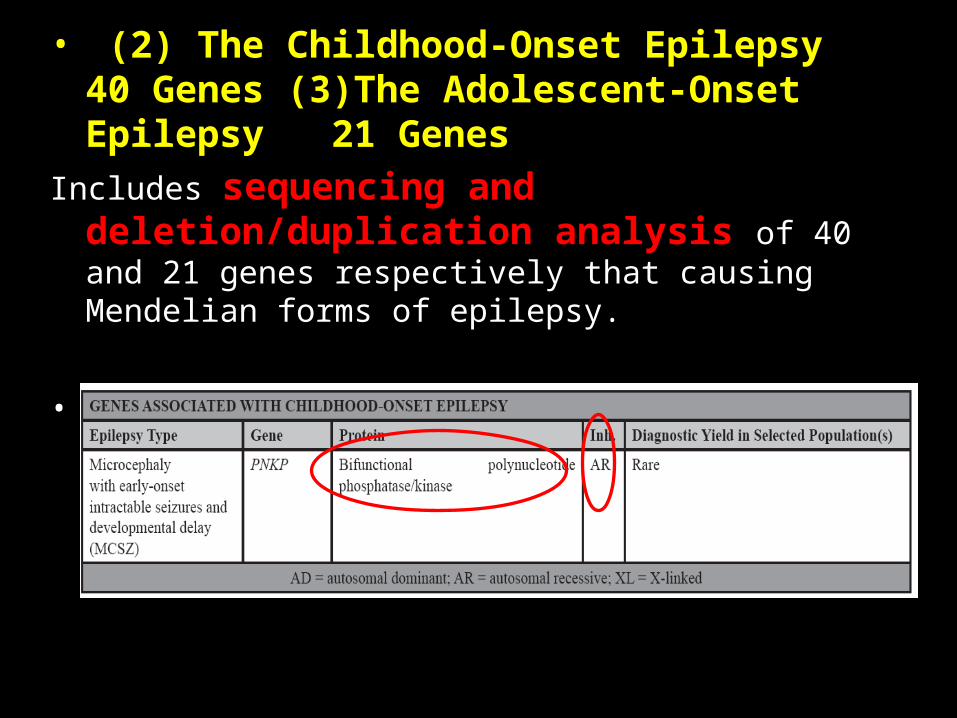
• (2) The Childhood-Onset Epilepsy 40 Genes (3)The Adolescent-Onset Epilepsy 21 Genes
Includes sequencing and deletion/duplication analysis of 40 and 21 genes respectively that causing Mendelian forms of epilepsy.
• Genes that encode nicotinic acetylcholine receptors and calcium channels,

Methodology(1) Infantile Epilepsy Panel (2) The Childhood-Onset Epilepsy(3) The Adolescent-Onset Epilepsy
Using genomic DNA obtained from blood, ~ 570 coding exons and the flanking splice junctions of 38 genes are sequenced simultaneously by (next-generation sequencing).
(1) The sequence is assembled and compared to published genomic reference sequences.
(2) Sanger sequencing is used to compensate for low coverage and refractory amplifications in regions where pathogenic mutations have been previously published.

DNA in the Cell
Target Region for PCRTarget Region for PCR
chromosome
cell nucleus
Double stranded DNA molecule
Individual nucleotides

Extract and discard plasma, taking care not to remove the buffy coat.
Genetic Lab 48 MH
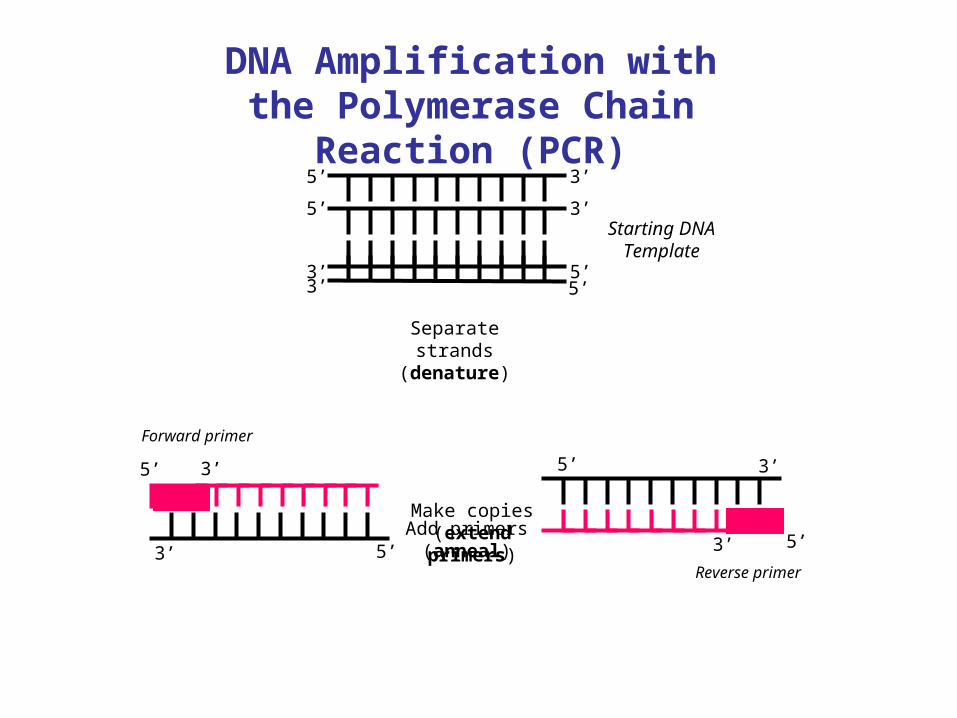
Make copies (extend primers)
Starting DNA Template
5’
5’
3’
3’
5’
5’
3’
3’
Add primers (anneal) 5’3’
3’5’
Forward primer
Reverse primer
DNA Amplification with the Polymerase Chain Reaction
(PCR)
Separate strands
(denature)
5’
5’3’
3’

In 32 cycles at 100% efficiency, 1.07 billion copies of targeted DNA region are created
In 32 cycles at 100% efficiency, 1.07 billion copies of targeted DNA region are created
PCR Copies DNA Exponentially through Multiple Thermal
Cycles
Original DNA target region
Thermal cycleThermal cycleThermal cycle
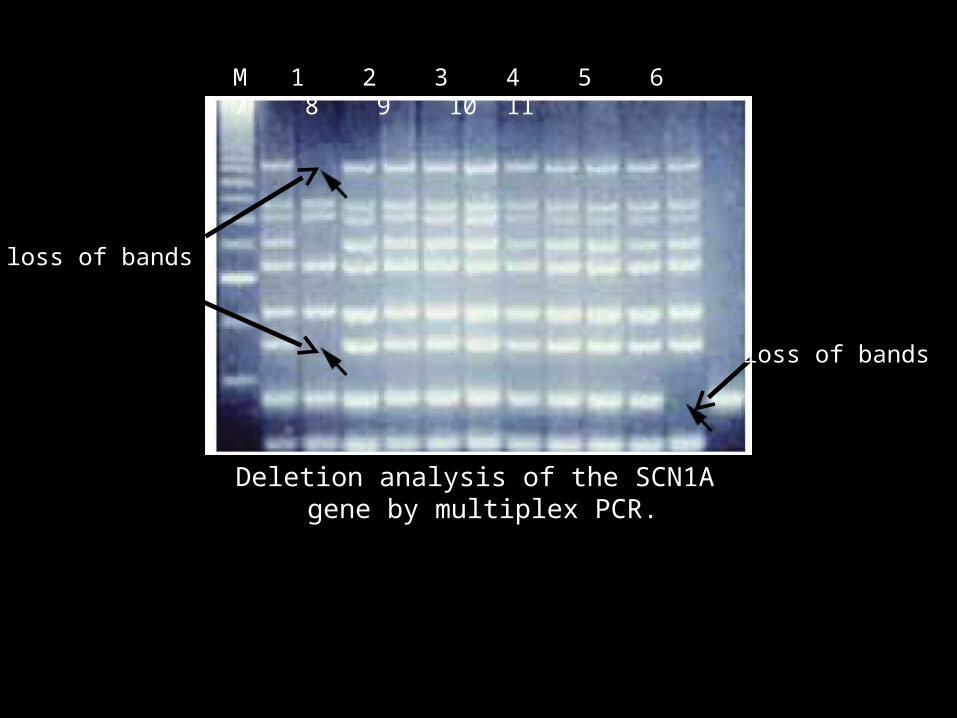
Deletion analysis of the SCN1A gene by multiplex PCR.
M 1 2 3 4 5 6 7 8 9 10 11
loss of bands
loss of bands
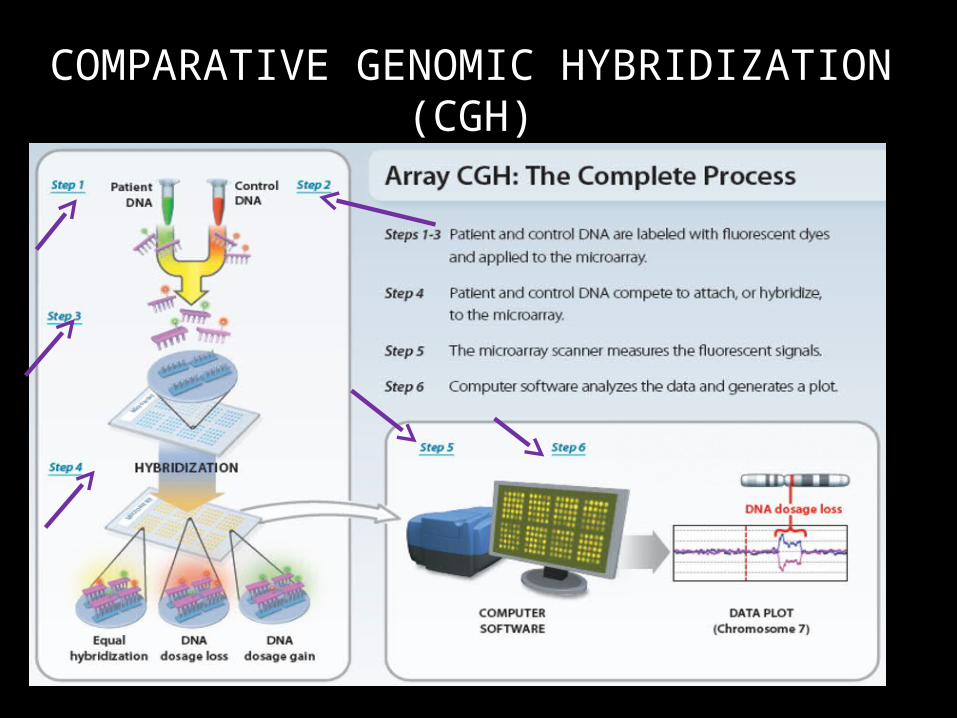
COMPARATIVE GENOMIC HYBRIDIZATION (CGH)
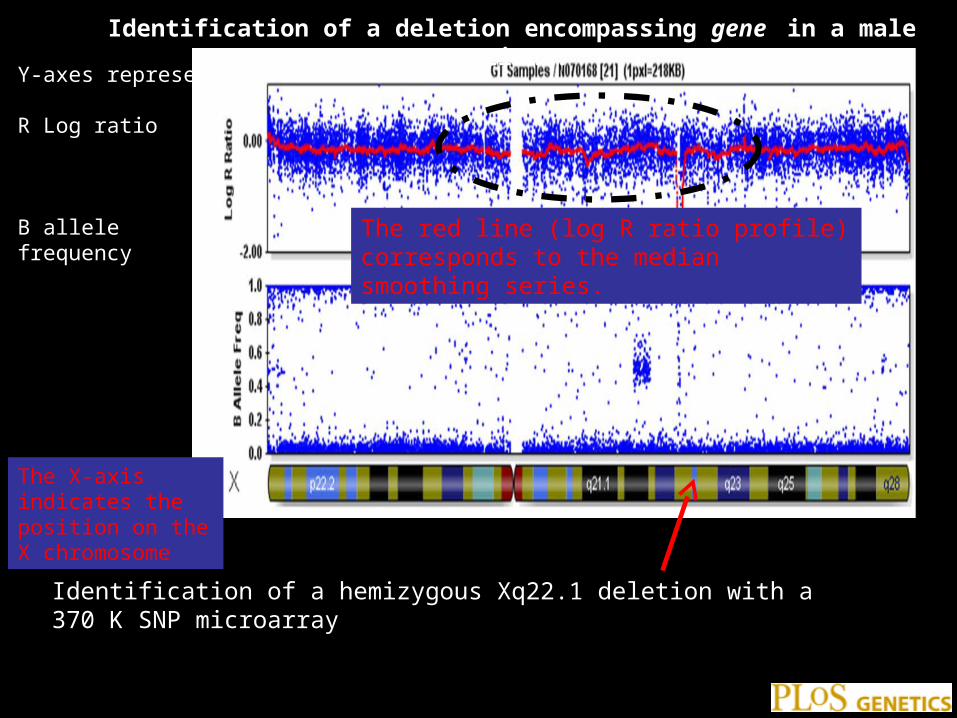
Identification of a deletion encompassing gene in a male patient.
•
Identification of a hemizygous Xq22.1 deletion with a 370 K SNP microarray
Y-axes represent R Log ratio
B allele frequency The red line (log R ratio profile) corresponds to the median smoothing series.
The X-axis indicates the position on the X chromosome
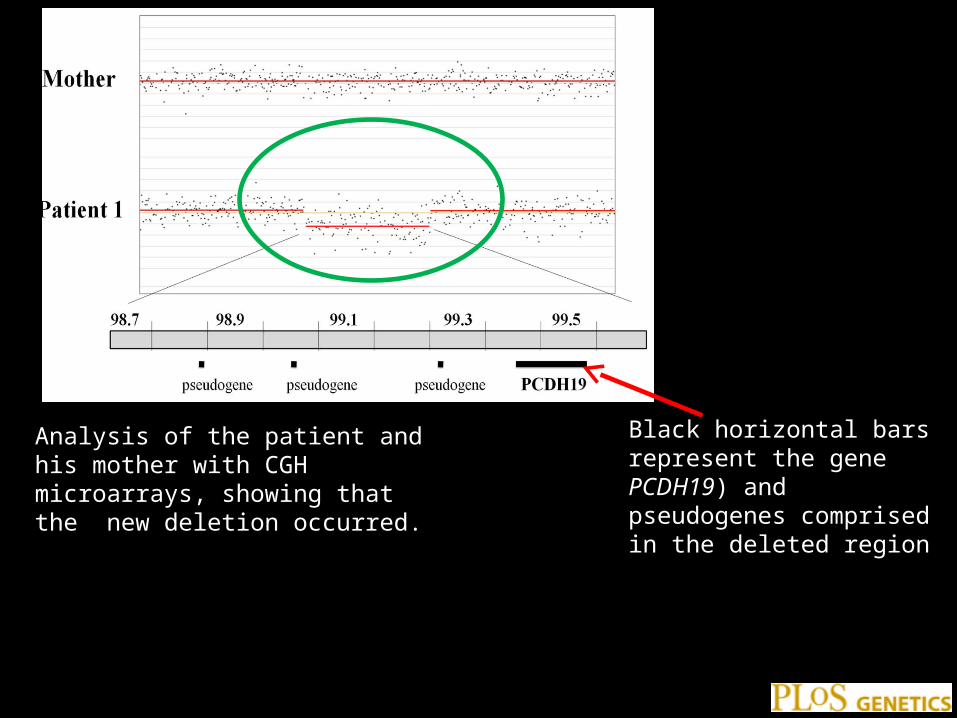
Figure 1. Identification of a deletion encompassing PCDH19 in a male patient.
•
Analysis of the patient and his mother with CGH microarrays, showing that the new deletion occurred.
Black horizontal bars represent the gene PCDH19) and pseudogenes comprised in the deleted region


ABI Prism 310 Genetic Analyzer

3’-TAAATGATTCC-5’
ATT
ATTTACTAA
ATTTACT ATTTAC
ATTTATTTA
AT
ATTTACTA
ATTTACTAAGATTTACTAAGG
A
DNA template5’ 3’
Primer anneals Extension produces a series of ddNTP
terminated products each one base different in length
Each ddNTP is labeled with a different color fluorescent dye
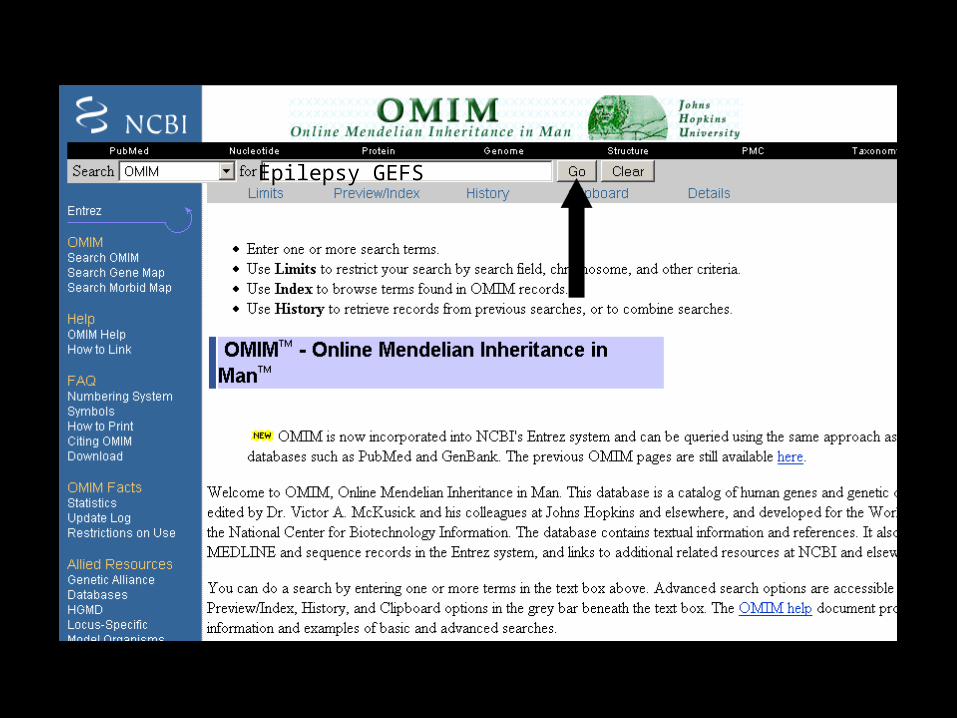
Epilepsy GEFS

OMIM Record Link to Gene
Coriell Cell RepositoriesHuman Gene Mutation Database
Epilepsy GEFS

Gene
Links to Everywhere (almost)Epilepsy GEFS

Gene
NTNM
records GeneUniGeneGene Model
GEFS Genome Maps
GEFS

Detection of 9 different point mutations of PCDH19 in 11 female patients by direct sequencing.
•
Sequence electropherograms of the mutations and the missense variant (c.3319C>G/p.Arg1107Gly) identified in association with the c.859G>T/p.Glu287X nonsense mutation.
The A of the ATG translation initiation codon in the reference sequence
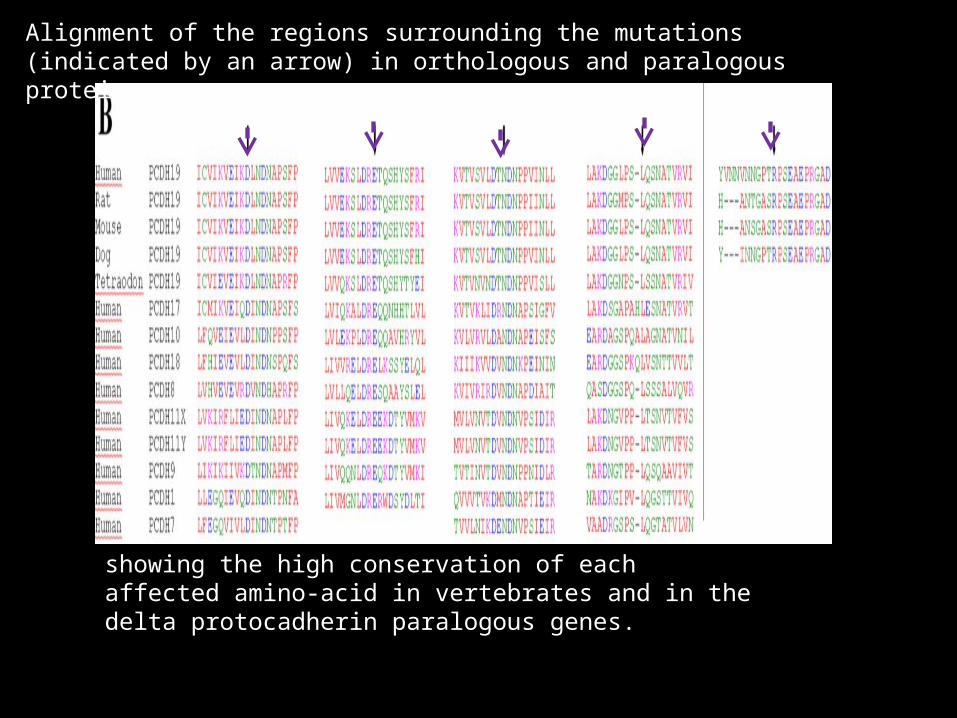
Alignment of the regions surrounding the mutations (indicated by an arrow) in orthologous and paralogous proteins,
showing the high conservation of each affected amino-acid in vertebrates and in the delta protocadherin paralogous genes.
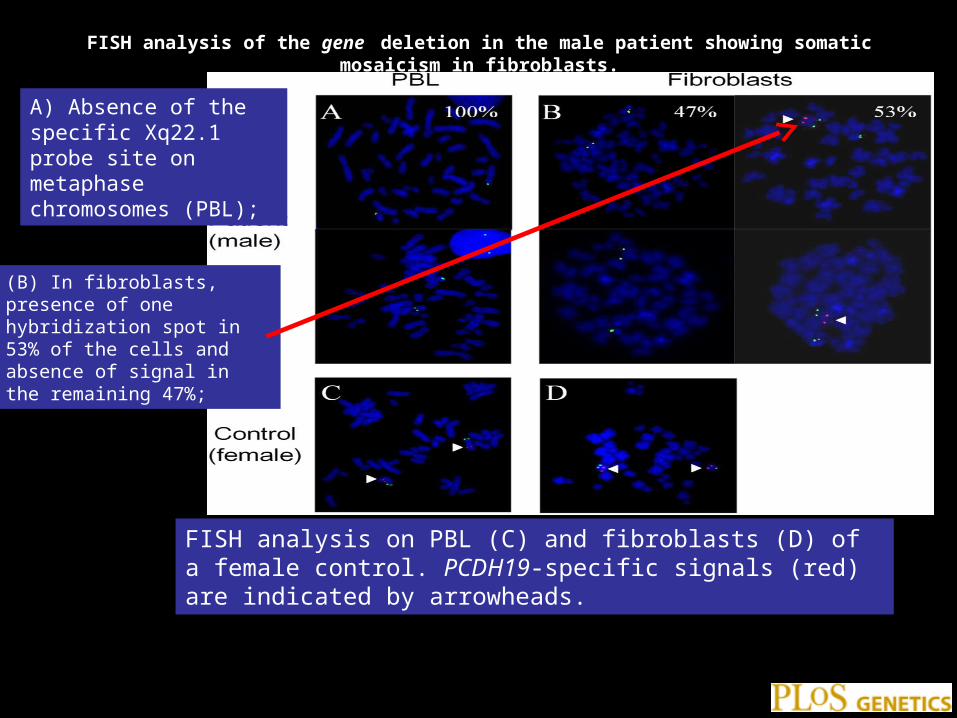
FISH analysis of the gene deletion in the male patient showing somatic mosaicism in fibroblasts.
•
FISH analysis on PBL (C) and fibroblasts (D) of a female control. PCDH19-specific signals (red) are indicated by arrowheads.
A) Absence of the specific Xq22.1 probe site on metaphase chromosomes (PBL);
(B) In fibroblasts, presence of one hybridization spot in 53% of the cells and absence of signal in the remaining 47%;
