monitoring depth of anaesthesia
TRANSCRIPT
Monitoring Depth of Anaesthesia
Presentation by :Dr. Ketaki Didolkar
Guided by :Dr. Abhay Bodhey


AIM OF MONITORING :AIM OF MONITORING : Guarantee the safety of anaesthesia as well as the Guarantee the safety of anaesthesia as well as the
painlessness of surgery.painlessness of surgery. Overall incidence of intra-operative awareness- Overall incidence of intra-operative awareness-
0.2-3 % 0.2-3 % Incidence >40% in patients of cardiac surgery, Incidence >40% in patients of cardiac surgery,
caesarean section, multiple trauma & caesarean section, multiple trauma & haemodynamically unstable patients.haemodynamically unstable patients.
A 2001 study reported that 56.3% of a group of patients who had awakened during surgery met the diagnostic criteria for ‘post traumatic stress disorder’—as late as 17 years after their operation.


AIM OF MONITORING :AIM OF MONITORING :
Intra-operative awareness is Intra-operative awareness is a major medicolegal liability a major medicolegal liability to anaesthetists & it is our to anaesthetists & it is our prime responsibility to prime responsibility to diagnose and avoid it at all diagnose and avoid it at all costs !!!!costs !!!!

HISTORICAL BACKGROUND :HISTORICAL BACKGROUND : DioscoridesDioscorides first used the term ‘anaesthesia’ to first used the term ‘anaesthesia’ to
describe narcotic effect of plant mandragora.describe narcotic effect of plant mandragora. O.W. Holmes O.W. Holmes coined the term ‘anaesthesia’ to coined the term ‘anaesthesia’ to
describe the new phenomenon that made surgical describe the new phenomenon that made surgical procedures possible.procedures possible.
Plomley Plomley (1847) first attempted to define depth of (1847) first attempted to define depth of anaesthesia by describing 3 stages- intoxication, anaesthesia by describing 3 stages- intoxication, excitement and narcosis.excitement and narcosis.
John Snow John Snow (1847) described ‘five degrees of (1847) described ‘five degrees of narcotism’ ; the first 3 included induction of narcotism’ ; the first 3 included induction of anaesthesia by ether & last 2 represented surgical anaesthesia by ether & last 2 represented surgical anaesthesia.anaesthesia.

HISTORICAL BACKGROUND :HISTORICAL BACKGROUND :
Guedel Guedel (1937) gave the classic description of clinical signs of (1937) gave the classic description of clinical signs of ether anaesthesia. Included 4 stages: analgesia, delirium, ether anaesthesia. Included 4 stages: analgesia, delirium, surgical anaesthesia & respiratory paralysis.surgical anaesthesia & respiratory paralysis.
HISTORICAL BACKGROUND :HISTORICAL BACKGROUND : ArtusioArtusio (1954) expanded Guedel’s stage 1 into 3 planes : (1954) expanded Guedel’s stage 1 into 3 planes :
1)1) No amnesia & analgesiaNo amnesia & analgesia
2)2) Total amnesia & partial analgesiaTotal amnesia & partial analgesia
3)3) Complete amnesia & analgesia Complete amnesia & analgesia
WoodbridgeWoodbridge (1957) defined 4 components of anaesthesia : (1957) defined 4 components of anaesthesia :
I.I. Sensory blockade of afferent impulsesSensory blockade of afferent impulses
II.II. Motor blockade of efferent impulses Motor blockade of efferent impulses
III.III. Reflex blockade of RS, CVS, GI tractReflex blockade of RS, CVS, GI tract
IV.IV.Mental block or unconsciousnessMental block or unconsciousness
Prys – Roberts Prys – Roberts (1987) defined anaesthesia as a state in (1987) defined anaesthesia as a state in which the patient neither perceives nor recalls noxious stimuli which the patient neither perceives nor recalls noxious stimuli as a result of drug induced unconsciousness.as a result of drug induced unconsciousness.
MODERN CONCEPT :MODERN CONCEPT : In modern times, anaesthesia is a complex interaction In modern times, anaesthesia is a complex interaction
of multiple stimuli applied, the diverse responses of multiple stimuli applied, the diverse responses measured & the drug induced probability of measured & the drug induced probability of nonresponsiveness to stimuli.nonresponsiveness to stimuli.
The The hypnotic agents hypnotic agents produce such profound CNS produce such profound CNS depression that the most powerful surgical stimulus depression that the most powerful surgical stimulus cannot arouse patient from state of cannot arouse patient from state of nonresponsiveness.nonresponsiveness.
The The analgesicsanalgesics & & LA LA attenuate the surgical stimuli.attenuate the surgical stimuli. The interaction between analgesics & hypnotics is The interaction between analgesics & hypnotics is
thus fundamental to understanding & defining thus fundamental to understanding & defining anaesthetic depth.anaesthetic depth.

PAIN & ANAESTHETICS PAIN & ANAESTHETICS

FACTORS AFFECTING CORRECT DRUG FACTORS AFFECTING CORRECT DRUG DOSES: DOSES:
The lack of a universally accepted The lack of a universally accepted definition of definition of "consciousness.”"consciousness.”
The increased use of The increased use of combinations of anaesthetic combinations of anaesthetic agents rather than single drugs. agents rather than single drugs.
Changes in the patient's response to anaesthesia over Changes in the patient's response to anaesthesia over the the course of the operation.course of the operation.
AgeAge-related differences in responsiveness to specific -related differences in responsiveness to specific anaesthetics anaesthetics
SexSex : Women appear to emerge from anaesthesia : Women appear to emerge from anaesthesia more rapidly than men. more rapidly than men.
Individual variation Individual variation in sensitivity to anaesthesiain sensitivity to anaesthesia

MEMORY AND ANAESTHESIA:MEMORY AND ANAESTHESIA: Anaesthesia , with increasing depth , progressively Anaesthesia , with increasing depth , progressively
decreases the ability of brain to carry out tasks and to decreases the ability of brain to carry out tasks and to remember them afterwards.remember them afterwards.
Memory is affected much before noticeable autonomic Memory is affected much before noticeable autonomic responses are seen.responses are seen.
Types of memory :-Types of memory :- Short -termShort -term Long –termLong –term
Procedural / Implicit Procedural / Implicit } } effortless effortless retrievalretrieval
Declarative : 1) Somatic / ImplicitDeclarative : 1) Somatic / Implicit
2) Episodic / Explicit - efforts required 2) Episodic / Explicit - efforts required
STAGES OF AwARENESS :STAGES OF AwARENESS :(GRIFFITH & JONES)(GRIFFITH & JONES)
1.1. Conscious awareness with explicit recallConscious awareness with explicit recall
2.2. Conscious awareness with no explicit recallConscious awareness with no explicit recall
3.3. Unconscious awareness with implicit recallUnconscious awareness with implicit recall
4.4. No awarenessNo awareness


Specific drugS & depth of Specific drugS & depth of anaeStheSia :anaeStheSia :
inhalational agentS :inhalational agentS : Purposeful movement of any part of the body in Purposeful movement of any part of the body in
response to noxious perioperative stimuli is the most response to noxious perioperative stimuli is the most useful clinical sign of depth of anaesthesiauseful clinical sign of depth of anaesthesia
Eger & Merkel therefore defined MAC as the minimum Eger & Merkel therefore defined MAC as the minimum alveolar concentration of inhaled anaesthetic required alveolar concentration of inhaled anaesthetic required to prevent 50% of subjects from responding to painful to prevent 50% of subjects from responding to painful stimuli with gross purposeful movementstimuli with gross purposeful movement
Tracheal intubation represents stronger noxious stimulus than all surgical stimuli

inhalational agentS :inhalational agentS : MAC has been expanded as :MAC has been expanded as : MAC-awake :(Stoelting)minimum alveolar MAC-awake :(Stoelting)minimum alveolar
concentration that would allow opening of eyes on concentration that would allow opening of eyes on verbal command during emergence from anaesthesiaverbal command during emergence from anaesthesia
MAC-intubation : (Yakaitis)minimum alveolar MAC-intubation : (Yakaitis)minimum alveolar concentration that would inhibit movement & coughing concentration that would inhibit movement & coughing during endotracheal intubation.during endotracheal intubation.
MAC-BAR : (Roizen)minimum alveolar concentration that would prevent adrenergic response to skin incision as measured by venous concentration of catecholamines

MAC may be modified by use of nitrous oxide,opioids MAC may be modified by use of nitrous oxide,opioids & other anaesthetics& other anaesthetics
The haemodynamic responses to surgical stimuli do The haemodynamic responses to surgical stimuli do not correlate well with end tidal concentration of not correlate well with end tidal concentration of inhaled anaesthetics.inhaled anaesthetics.
inhalational agentS :inhalational agentS :
nonopioid intravenouS agentS: nonopioid intravenouS agentS: induction of anaeStheSia induction of anaeStheSia
Plasma drug concentration peaks in half to one minute Plasma drug concentration peaks in half to one minute & declines rapidly due to redistribution& declines rapidly due to redistribution
Depth of anaesthesia follows plasma drug Depth of anaesthesia follows plasma drug concentrationconcentration
Clinical endpoints for assessment-Clinical endpoints for assessment-
1.1. Loss of verbal responsivenessLoss of verbal responsiveness
2.2. Loss of eyelid reflexLoss of eyelid reflex
3.3. Loss of corneal reflexLoss of corneal reflex Strongest stimulation during induction is laryngoscopy Strongest stimulation during induction is laryngoscopy
& intubation& intubation Analgesics are needed to maintain haemodynamicsAnalgesics are needed to maintain haemodynamics

nonopioid intravenouS agentS: nonopioid intravenouS agentS: Maintenance of anaeStheSiaMaintenance of anaeStheSiaPlasma levels of anaesthetic agents are accurate Plasma levels of anaesthetic agents are accurate predictors of brain levels of the drug & good indicators predictors of brain levels of the drug & good indicators of anaesthetic depthof anaesthetic depth
Clinical endpoints for assessment :Clinical endpoints for assessment :
1.1. Loss of eyelid reflexLoss of eyelid reflex
2.2. Loss of corneal reflexLoss of corneal reflex
3.3. Absence of movement in response to sqeezing Absence of movement in response to sqeezing trapeziustrapezius
Opioids in large doses need to be added when precise Opioids in large doses need to be added when precise haemodynamic control is necessary as in CADhaemodynamic control is necessary as in CAD

t.i.v.a.t.i.v.a.‘‘Minimum infusion rate’ is used to compare Minimum infusion rate’ is used to compare requirements of anaestheticsrequirements of anaesthetics
The 50% effective dose & 95 % effective dose The 50% effective dose & 95 % effective dose infusion rates are calculated using movement infusion rates are calculated using movement response to skin incisionresponse to skin incision
IV bolus of anaesthetic combined with maintenance IV bolus of anaesthetic combined with maintenance infusion can produce steady state plasma infusion can produce steady state plasma concentration of the drug to maintain anaesthetic concentration of the drug to maintain anaesthetic depth.depth.
opioidS :opioidS :CpCp50 50 is steady state plasma concentration of opioid is steady state plasma concentration of opioid
which will prevent purposeful movement to noxious which will prevent purposeful movement to noxious stimuli in 50% populationstimuli in 50% population
Clinical events which indicate inadequate infusion Clinical events which indicate inadequate infusion rates-rates-
1)1) Increase in systolic BP more than 15 mmHg above Increase in systolic BP more than 15 mmHg above normal for the patientnormal for the patient
2)2) Heart rate > 90/m in absence of hypovolemiaHeart rate > 90/m in absence of hypovolemia
3)3) Somatic : movement, swallowing, coughing or opening Somatic : movement, swallowing, coughing or opening eyeseyes
4)4) Autonomic : lacrimation, sweating, flushingAutonomic : lacrimation, sweating, flushing
aSSeSSMent of depth aSSeSSMent of depth of anaeStheSia :of anaeStheSia :
Subjective methodsSubjective methods ::– Autonomic changesAutonomic changes– Changes in pupil diameterChanges in pupil diameter– Isolated forearm techniqueIsolated forearm technique
Objective methodsObjective methods ::– E.E.G. & derived indicesE.E.G. & derived indices– Spontaneous surface electromyogramSpontaneous surface electromyogram– Lower oesophageal contractilityLower oesophageal contractility– Heart rate variabilityHeart rate variability– Evoked potentialsEvoked potentials
claSSification of MethodS :claSSification of MethodS :

SuBJective MethodS :SuBJective MethodS :
1. autonoMic changeS :1. autonoMic changeS :
Include sudden hypertension, tachycardia, sweating, Include sudden hypertension, tachycardia, sweating, tearing or mydriasistearing or mydriasis
Commonly used as clinical indicators of lightening of Commonly used as clinical indicators of lightening of depth of anaesthesiadepth of anaesthesia
Patient response to surgical stimulus (PRST) score Patient response to surgical stimulus (PRST) score includes 4 haemodynamic parameters : Pressure includes 4 haemodynamic parameters : Pressure (BP), Rate (pulse rate), Sweating & Tearing (BP), Rate (pulse rate), Sweating & Tearing
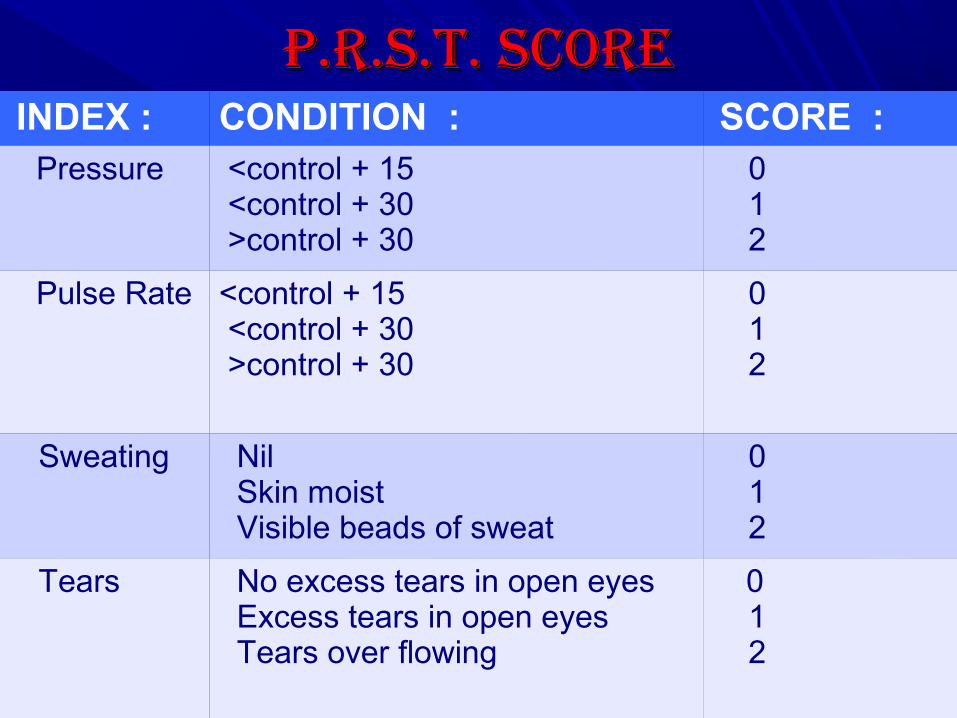
p.r.S.t. Scorep.r.S.t. Score INDEX : CONDITION : SCORE : Pressure <control + 15
<control + 30 >control + 30
0 1 2
Pulse Rate <control + 15 <control + 30 >control + 30
0 1 2
Sweating Nil Skin moist Visible beads of sweat
0 1 2
Tears No excess tears in open eyes Excess tears in open eyes Tears over flowing
0 1 2

diSadvantageS :diSadvantageS : These changes are also seen with intra-operative These changes are also seen with intra-operative
events like hypotension, dehydration, hypoxia, events like hypotension, dehydration, hypoxia, hypothermia, hyperthermia or sudden blood loss.hypothermia, hyperthermia or sudden blood loss.
Patient factors like built & baseline tone also affectPatient factors like built & baseline tone also affect Drugs like beta blockers , inotropes, vasodilators, anti-Drugs like beta blockers , inotropes, vasodilators, anti-
hypertensives also lead to such haemodynamic hypertensives also lead to such haemodynamic changes while opioids & muscle relaxants suppress changes while opioids & muscle relaxants suppress them.them.
Haemodynamic response to noxious stimuli does not Haemodynamic response to noxious stimuli does not necessarily signify awareness nor does lack of necessarily signify awareness nor does lack of haemodynamic changes guarantee unconsciousnesshaemodynamic changes guarantee unconsciousness

2. changeS in pupil diaMeter :2. changeS in pupil diaMeter : Guedel’s stages of ether anaesthesia describe initial Guedel’s stages of ether anaesthesia describe initial
pupillary constriction followed by dilatation as pupillary constriction followed by dilatation as anaesthesia deepens.anaesthesia deepens.
These changes are affected by circulating These changes are affected by circulating catecholamines, atropine & opioids.catecholamines, atropine & opioids.
Pupillary light reflex is also affected by opioids & Pupillary light reflex is also affected by opioids & anoxia .anoxia .

3.iSolated forearM techniQue :3.iSolated forearM techniQue : Tourniquet inflated on an arm of patient prior to Tourniquet inflated on an arm of patient prior to
administering intravenous muscle relaxant isolates administering intravenous muscle relaxant isolates forearm & allows it to remain free to move in response forearm & allows it to remain free to move in response to verbal command in light plane of anaesthesia.to verbal command in light plane of anaesthesia.
Limitations :Limitations : Nonspecific startle response may be wrongly Nonspecific startle response may be wrongly
interpreted as consciousnessinterpreted as consciousness Higher dose of muscle relaxant required in IFT to Higher dose of muscle relaxant required in IFT to
prevent movementprevent movement Inability to move arm despite consciousness is Inability to move arm despite consciousness is
complained by some patientscomplained by some patients
oBJective MethodS :oBJective MethodS :

1.electroencephalograM :1.electroencephalograM :
EEG is a low voltage (1-50 µv) deflection recorded EEG is a low voltage (1-50 µv) deflection recorded from surface of scalp by electrodes.from surface of scalp by electrodes.
Noninvasive indicator of cerebral functionNoninvasive indicator of cerebral function Represents cortical electrical activity derived from Represents cortical electrical activity derived from
excitatory & inhibitory postsynaptic activityexcitatory & inhibitory postsynaptic activity This electrical activity has physiologic correlates This electrical activity has physiologic correlates
relevant to depth of anaesthesiarelevant to depth of anaesthesia Cerebral physiology & metabolism both affect the EEG Cerebral physiology & metabolism both affect the EEG
& anaesthetic drugs affect both cerebral physiology & & anaesthetic drugs affect both cerebral physiology & EEGEEG

1.ELECTROENCEPHALOGRAM :1.ELECTROENCEPHALOGRAM : Effects of noxious stimulus on EEG :Effects of noxious stimulus on EEG : Desynchronization with appearance of fast rhythmsDesynchronization with appearance of fast rhythms Appearance of 6 -10 Hz spindlesAppearance of 6 -10 Hz spindles Bursts of 1-3 Hz slow wavesBursts of 1-3 Hz slow waves Anaesthetic drugs result in low frequency EEG & burst Anaesthetic drugs result in low frequency EEG & burst
suppression at high concentration suppression at high concentration

EEG INDICES :EEG INDICES :1) Compressed spectral array (CSA): 1) Compressed spectral array (CSA): The individual frequency distributions of EEG can be The individual frequency distributions of EEG can be
considered as time slices and joined together into a considered as time slices and joined together into a 3D plot is called CSA3D plot is called CSA
During peaks of anaesthesia, CSA shows low During peaks of anaesthesia, CSA shows low frequency activityfrequency activity
At recovery and lighter planes CSA shows high At recovery and lighter planes CSA shows high frequency activity with decreased low frequency frequency activity with decreased low frequency waveswaves
Disadvantages include difficulty to comprehend the Disadvantages include difficulty to comprehend the changes & to quantify themchanges & to quantify them


EEG INDICES :EEG INDICES :2) Spectral edge frequency (SEF) : Defined as 2) Spectral edge frequency (SEF) : Defined as
frequency below which 95 % of EEG power is frequency below which 95 % of EEG power is contained.contained.
3) Median frequency (MF) : Defined as frequency above 3) Median frequency (MF) : Defined as frequency above & below which 50% of EEG power spectrum is & below which 50% of EEG power spectrum is distributed.distributed.
4) Bispectral index (BIS) 4) Bispectral index (BIS)
BISPECTRAL BISPECTRAL INDEXINDEX
BISPECTRAL INDEX :BISPECTRAL INDEX : Developed in 1987, by Aspect Medical Systems in Developed in 1987, by Aspect Medical Systems in
Massachusetts Massachusetts It is a numerical index ranging from 100 (awake) to 0 It is a numerical index ranging from 100 (awake) to 0
(no detectable EEG activity) (no detectable EEG activity) The BIS correlates with level of responsiveness & The BIS correlates with level of responsiveness &
provides an excellent prediction of the level of provides an excellent prediction of the level of consciousness with propofol, midazolam & isoflurane consciousness with propofol, midazolam & isoflurane anaesthesia anaesthesia
The bispectral index itself is a complex mathematical algorithm that allows a computer inside the BIS monitor to analyze data from a patient's electroencephalogram (EEG) during surgery.

Multiple clinically relevant measures like movement, Multiple clinically relevant measures like movement, haemodynamics, drug concentrations, consciousness, haemodynamics, drug concentrations, consciousness, recall are considered alongwith concurrent EEG data.recall are considered alongwith concurrent EEG data.
Advanced multivariate statistical analysis is used to Advanced multivariate statistical analysis is used to correlate components of the multiple EEG signal correlate components of the multiple EEG signal processing approaches with the clinical data to create processing approaches with the clinical data to create the univariate BIS indexthe univariate BIS index
The BIS index measures hypnotic components of the The BIS index measures hypnotic components of the anaesthetic & is insensitive to analgesic components.anaesthetic & is insensitive to analgesic components.
BIS is useful monitor to adjust anaesthetic dosages & BIS is useful monitor to adjust anaesthetic dosages & decreases incidence of haemodynamic disturbances & decreases incidence of haemodynamic disturbances & leads to improved recoveryleads to improved recovery
BISPECTRAL INDEX :BISPECTRAL INDEX :

DESCRIPTION :DESCRIPTION :
The BIS system is integrated into patient The BIS system is integrated into patient monitoring devices . monitoring devices .
The BIS system displays both raw data from The BIS system displays both raw data from the EEG and a single number between 100 the EEG and a single number between 100 (indicating an awake patient) and 0 (indicating (indicating an awake patient) and 0 (indicating the absence of brain activity) that represents the absence of brain activity) that represents the patient's degree of sedation.the patient's degree of sedation.
The target number for most anesthetized The target number for most anesthetized patients is between 40 and 60.patients is between 40 and 60.
BIS ELECTRODESBIS ELECTRODES::


DEvELOPING THE BIS INDEX :DEvELOPING THE BIS INDEX :

BIS & DOSAGE TITRATION BIS & DOSAGE TITRATION Physical signs Clinical
pictureBIS value
Management
1. Hypertension Light High Consider hypnotic / analgesic doses
Tachycardia 40-60 Analgesic dose / antihypertensive
Movement Low Decrease hypnotic dose / start antihypertensive
Autonomic response
2.Stable vitals Adequate High Consider hypnotic / analgesic doses
40-60 Observe
Low Consider decrease in both drug doses
3.Hypotension Deep High Consider hypnotic / analgesic doses
Arrhythmias Rule out other etiologies
BP support
40-60 Rule out other etiologies
BP support
Low Decrease both drug doses
BP support
LIMITATIONS Of BIS :LIMITATIONS Of BIS :BIS values are affected by the choice of anesthetic BIS values are affected by the choice of anesthetic agent. A patient with a BIS score of 60 agent. A patient with a BIS score of 60 anesthetized with one combination of agents may anesthetized with one combination of agents may be more deeply sedated than another patient with be more deeply sedated than another patient with the same score but anesthetized with a different the same score but anesthetized with a different combination of drugs. combination of drugs.
The BIS monitor appears unable to accurately The BIS monitor appears unable to accurately track changes in consciousness produced by track changes in consciousness produced by certain anaesthetics, specifically ketamine and certain anaesthetics, specifically ketamine and nitrous oxide. nitrous oxide.
The changes in the BIS algorithm resulting from The changes in the BIS algorithm resulting from updating and refinement of the producer’supdating and refinement of the producer’s

LIMITATIONS Of BIS :LIMITATIONS Of BIS : database make it difficult to compare results database make it difficult to compare results
obtained by different investigators using different obtained by different investigators using different versions of the BIS monitor. versions of the BIS monitor.
BIS values are difficult to correlate with other BIS values are difficult to correlate with other measurements of anaesthetic depth or altered measurements of anaesthetic depth or altered consciousness like serum concentrations of consciousness like serum concentrations of anesthetic agents. anesthetic agents.
Standard BIS scores are not useful in monitoring Standard BIS scores are not useful in monitoring special patient populations, particularly critically ill special patient populations, particularly critically ill patients with unstable body temperatures and patients with unstable body temperatures and patients with dementia. patients with dementia.

USES Of BIS :USES Of BIS :Reduces cost by decreasing anaesthetic use & stay in Reduces cost by decreasing anaesthetic use & stay in PACUPACU
Provides a useful guide for titration of anaesthetic Provides a useful guide for titration of anaesthetic agents in cardiac surgery, elderly & paediatric patientsagents in cardiac surgery, elderly & paediatric patients
Reduces the incidence of intraoperative awarenessReduces the incidence of intraoperative awareness

SPONTANEOUS SURfACE SPONTANEOUS SURfACE ELECTROMyOGRAMELECTROMyOGRAM

SpontaneouS Surface SpontaneouS Surface electromyogramelectromyogram
In patients who are not completely paralyzed, In patients who are not completely paralyzed, spontaneous surface electromyogram (SEMG) can be spontaneous surface electromyogram (SEMG) can be recorded from various muscle groups, especially recorded from various muscle groups, especially facial, abdominal and neck muscles.facial, abdominal and neck muscles.
The level of SEMG has been observed to fall during The level of SEMG has been observed to fall during anaesthesia and to rise to pre-anaesthetic levels just anaesthesia and to rise to pre-anaesthetic levels just before awakening.before awakening.

lower oeSophageal lower oeSophageal contractilitycontractility
lower oeSophageal lower oeSophageal contractilitycontractility
The non-striated muscles in the lower half of The non-striated muscles in the lower half of oesophagus retain their potential activity even after full oesophagus retain their potential activity even after full skeletal muscle paralysis.skeletal muscle paralysis.
Provide two prime derivativesProvide two prime derivatives
1] Spontaneous lower oesophageal 1] Spontaneous lower oesophageal contractions(SLOG)contractions(SLOG)
These are non-propulsive spontaneous contractions These are non-propulsive spontaneous contractions mediated via vagal motor nuclei and reticular mediated via vagal motor nuclei and reticular activating system in the brain stem. The frequency of activating system in the brain stem. The frequency of these movements is increased as the dose of the these movements is increased as the dose of the anaesthetic is reduced.anaesthetic is reduced.

lower oeSophageal lower oeSophageal contractilitycontractility
2] Provoked lower oesophageal contractions(PLO)2] Provoked lower oesophageal contractions(PLO)
These are obtained by inflation of a small balloon in These are obtained by inflation of a small balloon in the lower oesophagus. The brief inflation of small the lower oesophagus. The brief inflation of small
balloon provokes a secondary pulsatile response, balloon provokes a secondary pulsatile response, which increases in amplitude as anaesthetic depth which increases in amplitude as anaesthetic depth decreases.decreases.
heart rate heart rate variabilityvariability
heart rate variabilityheart rate variability Normally heart rate increases during inspiration and Normally heart rate increases during inspiration and
decreases during expiration, through a predominantly decreases during expiration, through a predominantly parasympathetic reflex connecting stretch receptors in parasympathetic reflex connecting stretch receptors in the lungs and aorta to vagal motor neurons the lungs and aorta to vagal motor neurons innervating the heart. This is called innervating the heart. This is called respiratory sinus respiratory sinus arrhythmia(RSA).arrhythmia(RSA).
It is typically characterized by greater than 10% It is typically characterized by greater than 10% variation in the ECG P-wave interval over 5 minutesvariation in the ECG P-wave interval over 5 minutes
There is reduction in RSA during anaesthesia together There is reduction in RSA during anaesthesia together with increase in RSA during recovery or light planes.with increase in RSA during recovery or light planes.
heart rate variabilityheart rate variability In addition, surgical stimulation during light In addition, surgical stimulation during light
anaesthesia elicits a greater increase on RSA than anaesthesia elicits a greater increase on RSA than seen during lightening anaesthesia alone.seen during lightening anaesthesia alone.

evoked potentialSevoked potentialS
evoked potentialS (ep)evoked potentialS (ep) Show the response of more localized areas of the Show the response of more localized areas of the
brainstem, midbrain and cerebral cortex to specific brainstem, midbrain and cerebral cortex to specific areas.areas.
Recording of EPs consisting of recording EEG epochs Recording of EPs consisting of recording EEG epochs and time-referencing them to sensory stimuli that have and time-referencing them to sensory stimuli that have been applied in a repeated fashion.been applied in a repeated fashion.
For intra-operative monitoring, 3 types of EPs are For intra-operative monitoring, 3 types of EPs are commonly used:commonly used:
1}SEP (somatosensory EP) is recorded over the 1}SEP (somatosensory EP) is recorded over the somatosensory cortex in response to tibial, peronial or somatosensory cortex in response to tibial, peronial or median nerve stimulation.median nerve stimulation.
2}VEP (Visual EP)is recorded over occipital cortex in 2}VEP (Visual EP)is recorded over occipital cortex in response to photic stimulation of the eyes. response to photic stimulation of the eyes.

evoked potentialS (ep)evoked potentialS (ep)3}AEP (auditory EP) is recorded at primary auditory 3}AEP (auditory EP) is recorded at primary auditory
cortex in response to auditory canal stimulation by cortex in response to auditory canal stimulation by audible clicks.audible clicks.It is most commonly used for the It is most commonly used for the assessment of anaesthetic drug effect. assessment of anaesthetic drug effect.
• As the concentration of potent inhaled anaesthetic As the concentration of potent inhaled anaesthetic increases, the latencies of SEP, VEP and AEP increases, the latencies of SEP, VEP and AEP increase and amplitudes decrease.increase and amplitudes decrease.
• In contrast, NIn contrast, N22O produces a dose-related decrease in O produces a dose-related decrease in
the amplitude of VEP and SEP, but no effect on the amplitude of VEP and SEP, but no effect on latency.latency.

auditory evoked potential auditory evoked potential indexindex
Derived from auditory evoked potential and represents Derived from auditory evoked potential and represents a single numerical variable for monitoring depth of a single numerical variable for monitoring depth of anaesthesia.anaesthesia.
Calculated from the amplitude difference between Calculated from the amplitude difference between successive segments of the AEP curve.successive segments of the AEP curve.
AEP index of 37 is 100% specific and 52% sensitive AEP index of 37 is 100% specific and 52% sensitive for unconsciousness.for unconsciousness.
AEP index is highly sensitive for distinguishing the AEP index is highly sensitive for distinguishing the transition from unconsciousness to consciousness. transition from unconsciousness to consciousness.
futurefuture
futurefuture
The only reliable way of determining The only reliable way of determining depth of anaesthesia will require a depth of anaesthesia will require a measure of cerebral activity and measure of cerebral activity and localization of the activity to specific localization of the activity to specific cortical regions and areas in cortical regions and areas in brainstem, in real time.brainstem, in real time.

poSition emiSSion tomography (pet)poSition emiSSion tomography (pet)
PET scanning studies have PET scanning studies have revealed that propofol anaesthesia revealed that propofol anaesthesia has a widespread suppressive effect has a widespread suppressive effect on cerebral metabolism. on cerebral metabolism.

ultra SenSitive Super conducting ultra SenSitive Super conducting quantum interference device (SquidS)quantum interference device (SquidS)
Non invasive method, which measures Non invasive method, which measures functional activity of brain.functional activity of brain.
Although expensive at present this may Although expensive at present this may provide the ultimate monitor to the provide the ultimate monitor to the anaesthesiologists. anaesthesiologists.

thank you ….