morbidity meeting chronic osteomyelitis
TRANSCRIPT
Morbidity Meeting
By: Dr.Inayat Ullah
PGY-III Paeds
Shifa International Hospital Islamabad.
Case
l A Young 14 years old Girl with multifocal
Disseminated unresolving chronic
Osteomyelitis with underlying abscess.
Biodata
l Patient Name: A.B.C.
l MR# 17813514
l Age: 14 years
l Sex: Female
l Location: Swabi
l Admitted via : ER
l D.O.A: 01/05/2017 2300H
02/05/2017
l Fever..............25 days
l Backache.......25 days
l Bilateral hip pain....25 days.
HOPI
• Patient was in her usual state of health 25
days back when she developed high grade
fever, undocumented, intermittent and was
associated with back pain of mild to
moderate intensity with radiation into hip
right joint area.
• She is also bed ridden for the last 20 days
due to above symptoms.
Past History
• Had jaundiced 2 week agoand diagnosed
to be having Hep A for which she
remained admitted at local hospital and
was given supportive symptomatic
treatment.

On examiantion
l Vitals:
l HR:140/min
l RR: 23/min
l Temp: 38.5C
l Pain Score 6/10
l B.P: 100/60mmHg
On Examiantion
l Sick looking dehydrated, jaundiced, malnourished girl, febrile to touch and pale looking not in obvious distress
l CVS: S1+S2+0
l CNS: Intact no focal deficit, no SOMI.
l RESP: good air entry no added sounds, NVB.
l GIT: Abd soft non tender mild tenderness in RIF.
l MSS: Tenderness in right hip area and decreased range of motions.
1)Osteomyelitis of hip bone with
associated abscess
2)Septic arthritis of hip joint
3)Traumatic arthritis of hip
Admission plan
CBC CRP, RFT, ELECTROLYTES, ESR, LFT'S, BLOOD
C/S, URINE R/E, C/S, CT ABDOMEN AND PELVIS AND
CXR Were done.
Inj Ceftriaxone 1.5 g BD
Inj Vancomycin 700 mg q8H
Inj Ketorolac 15 mg iv q8 hourly
D/Saline @ 100 ml/hr.
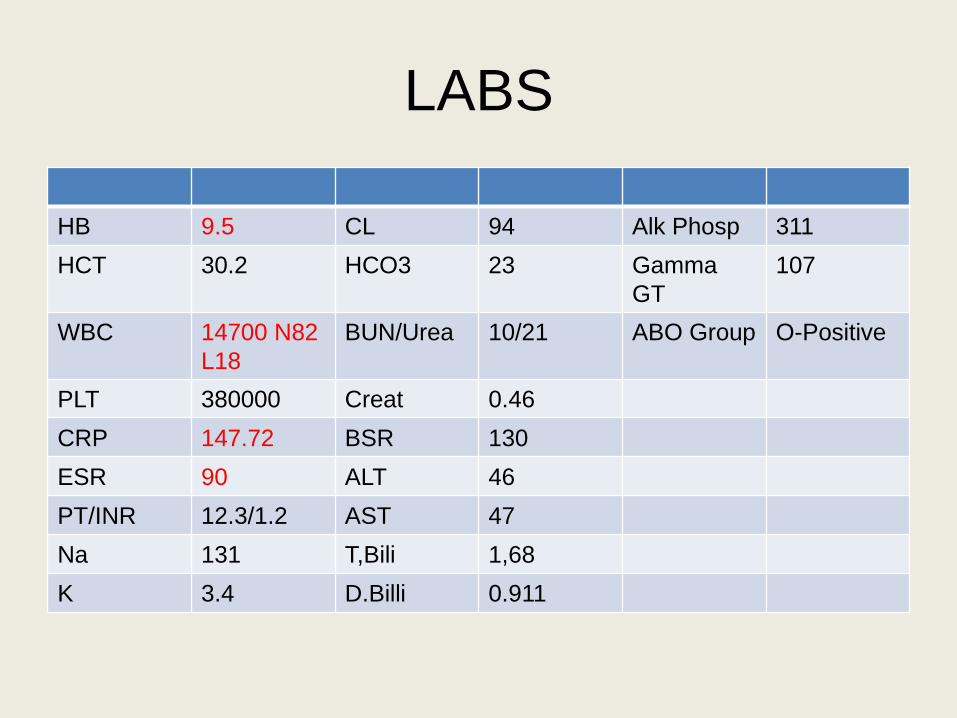
LABS
HB 9.5 CL 94 Alk Phosp 311
HCT 30.2 HCO3 23 Gamma
GT
107
WBC 14700 N82
L18
BUN/Urea 10/21 ABO Group O-Positive
PLT 380000 Creat 0.46
CRP 147.72 BSR 130
ESR 90 ALT 46
PT/INR 12.3/1.2 AST 47
Na 131 T,Bili 1,68
K 3.4 D.Billi 0.911
Ultrasound report 02/05/17
• Echomixed area in right psaos muscle likely represent abscess
• Bilateral minimal pleural effusion.
• CT Abd/Pelvis:
• Large loculated thick walled partially enhancing hypodense area containing air loculi in R illiacus muscle with edema around consistent with abscess. Subtle reaction along R illiac bone tiny air loculiwithin illiacbone, extending and involving lower ribs.
• Findings are suggestive of infective process
Morning round plan
Interventional Radiology to Drain pus
Antibiotics Vancomycin and Meropenum
(instead of ceftriaxone) to continue.
Nutritional rehabilitation
PCM Protocol
02/05/2017
65 ml pus aspirated under ultrasound
guide successfully
Specimens were sent for Routine c/s,
fungal c/s, Gram stain, AFB Stain, AFB
C/S
Gene Xpert and anaerobic culture.
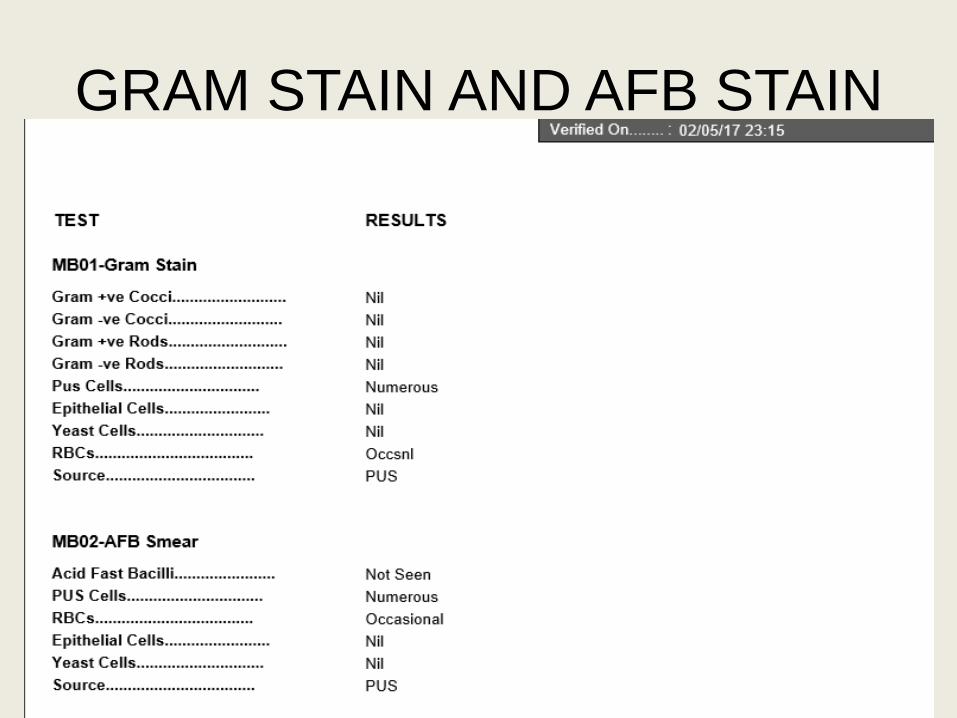
GRAM STAIN AND AFB STAIN
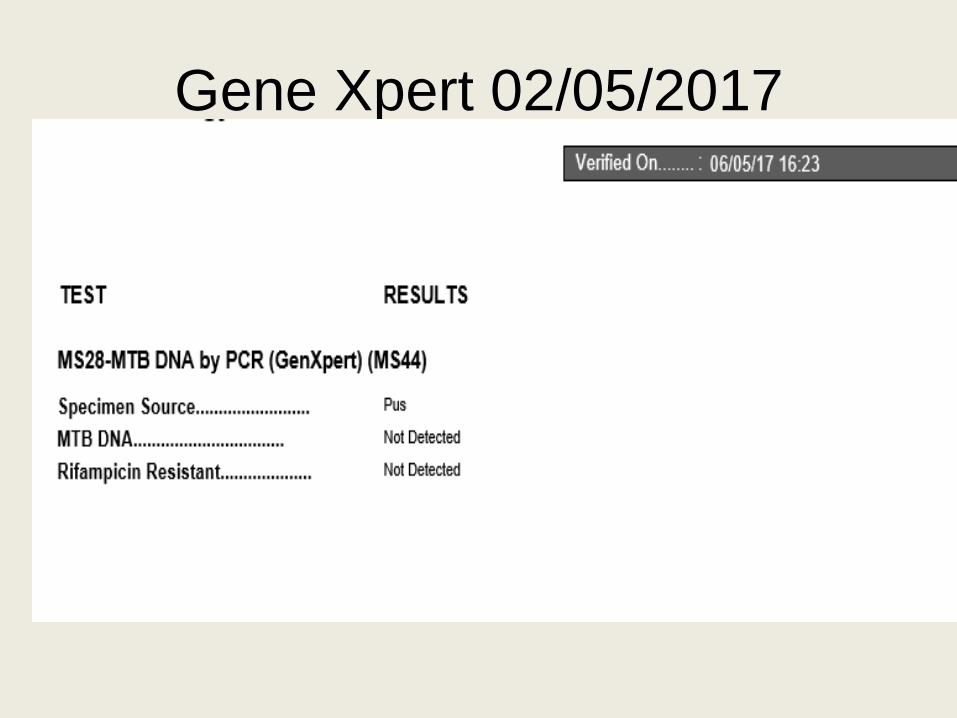
Gene Xpert 02/05/2017

Treatment Plan
Antibiotics continued
Clindamycin started 450 mg q8H
Amikacin 175 mg q8 hourly started
Vancomycin discontinued
High protein and high calorie diet started
and TPN weaned down.
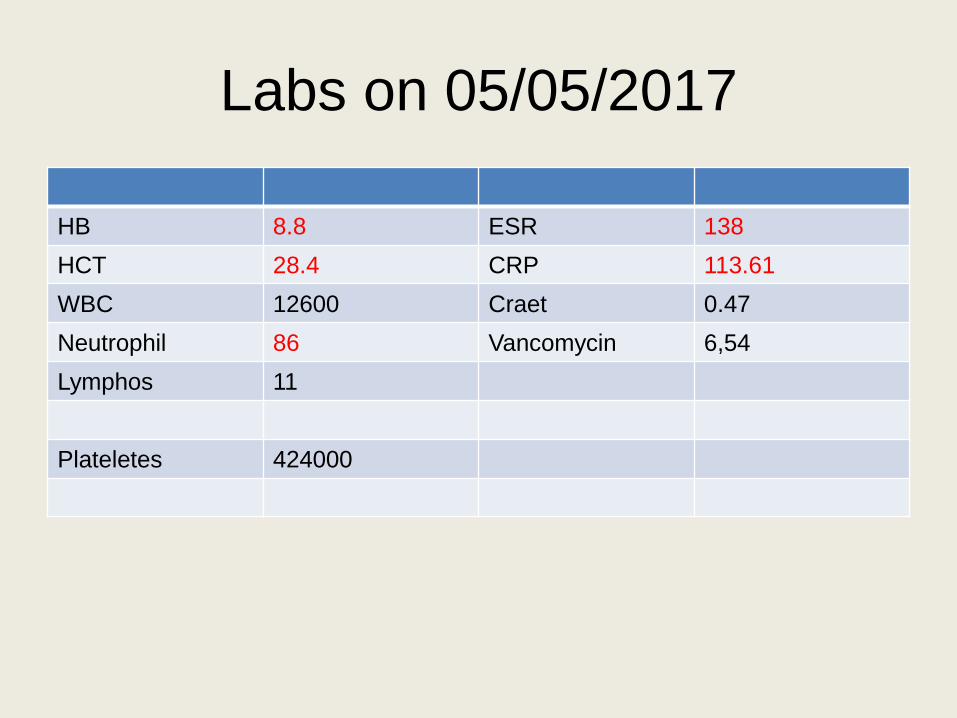
Labs on 05/05/2017
HB 8.8 ESR 138
HCT 28.4 CRP 113.61
WBC 12600 Craet 0.47
Neutrophil 86 Vancomycin 6,54
Lymphos 11
Plateletes 424000
07/05/2017
Had persistent spiking fever
Backache
OE
Nontoxic with abdominal distension and RIF tenderness
Plan:
Pediatric surgery consult/Ortho consult.
Ultrasound abd/pelvis
08/05/2017
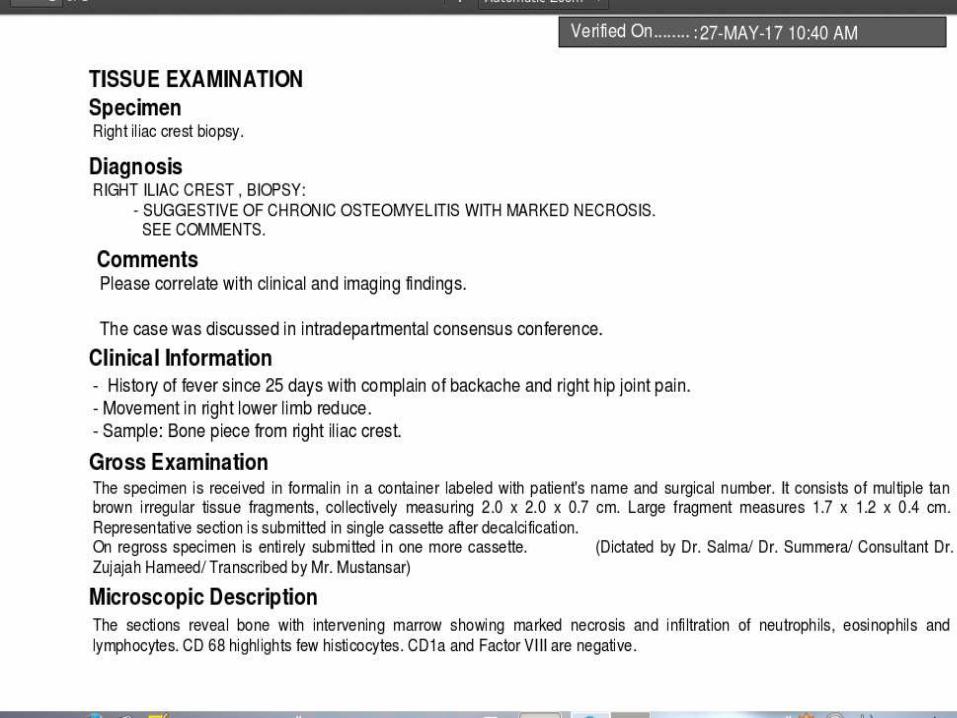
Ortho planned for biopsy of multiple cystic
lesions from illiac crest
Pediatric surgery planned after discussing
with ortho laparoscopic abscess drainage
08/05/2017
Patient underwent incision and drainage of
pelvic collection and biopsy of illiac crest
the same day by pediatric surgeon and
orthopedic surgeon.
Specimen were sent for c/s, gram stain,
AFB C/S, Histopathology and gene Xpert
Post-op patient remained stable
Drain was inserted in wound.
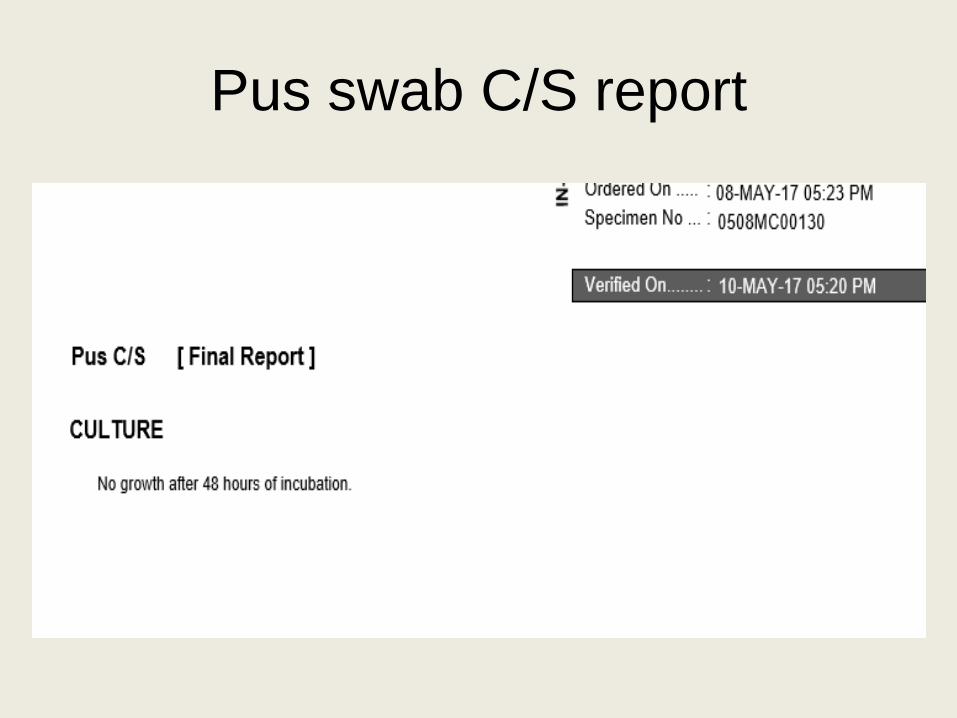
Pus swab C/S report
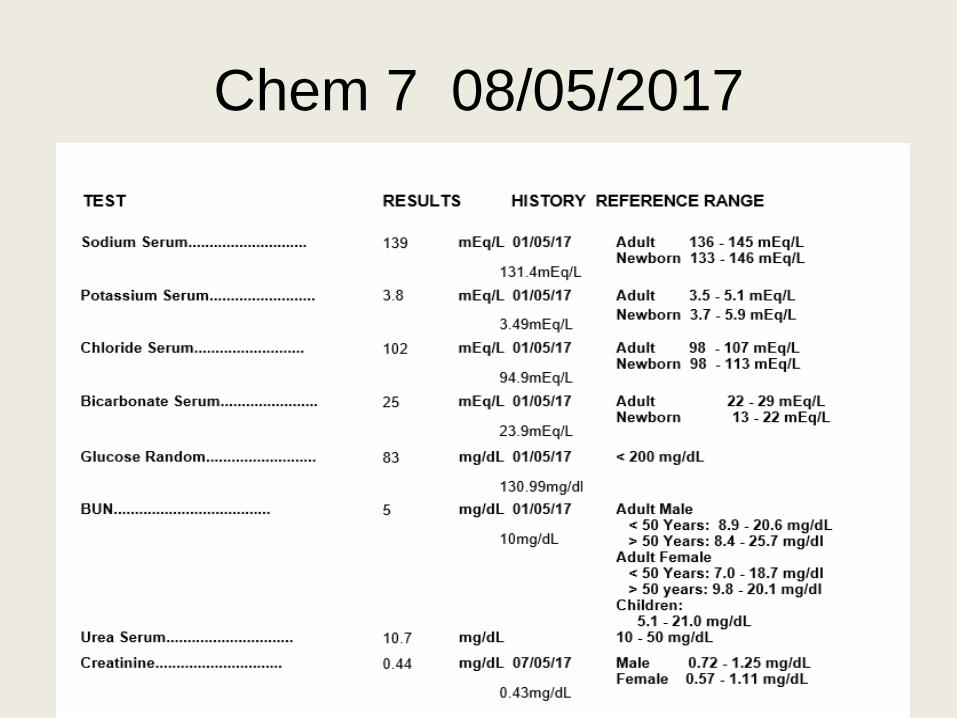
Chem 7 08/05/2017
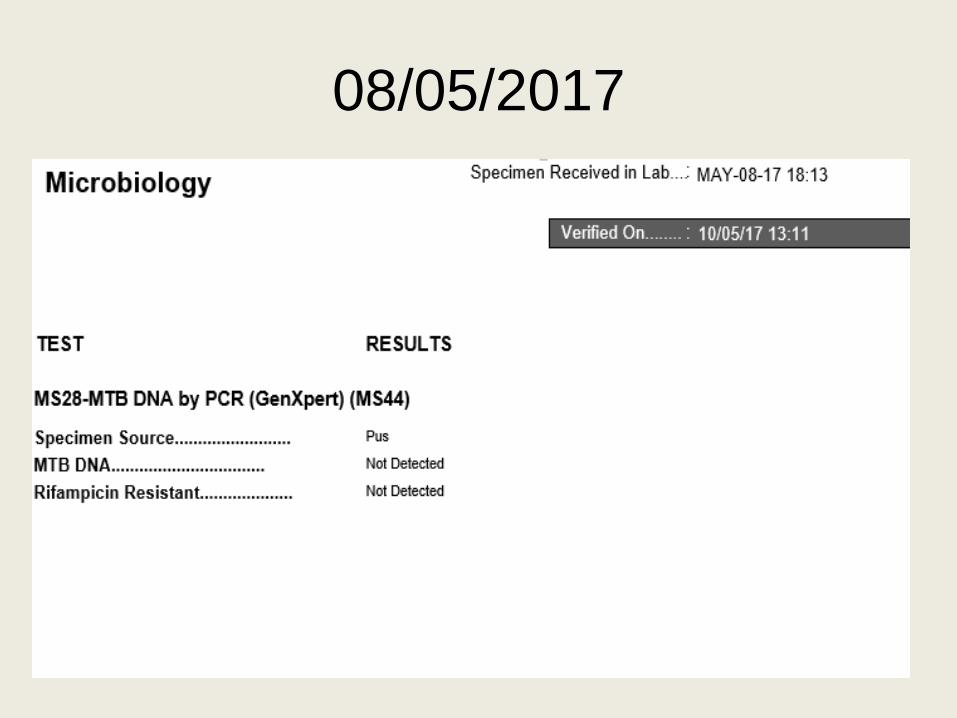
08/05/2017
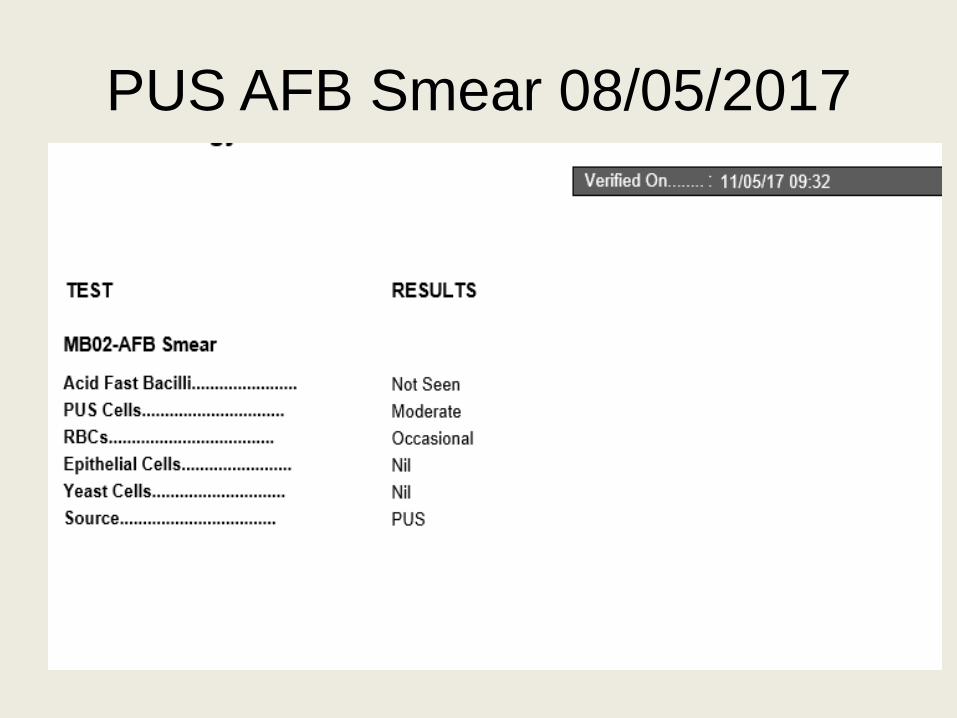
PUS AFB Smear 08/05/2017
10/05/2017
Patient had spiking fever
Otherwise good oral intake
Temp: 103F
Face flushed and rash on upper abdomen
Plan:
Follow cultures and biopsy
Send CBC,. CRP, LDH, ANA and Blood c/s in am.
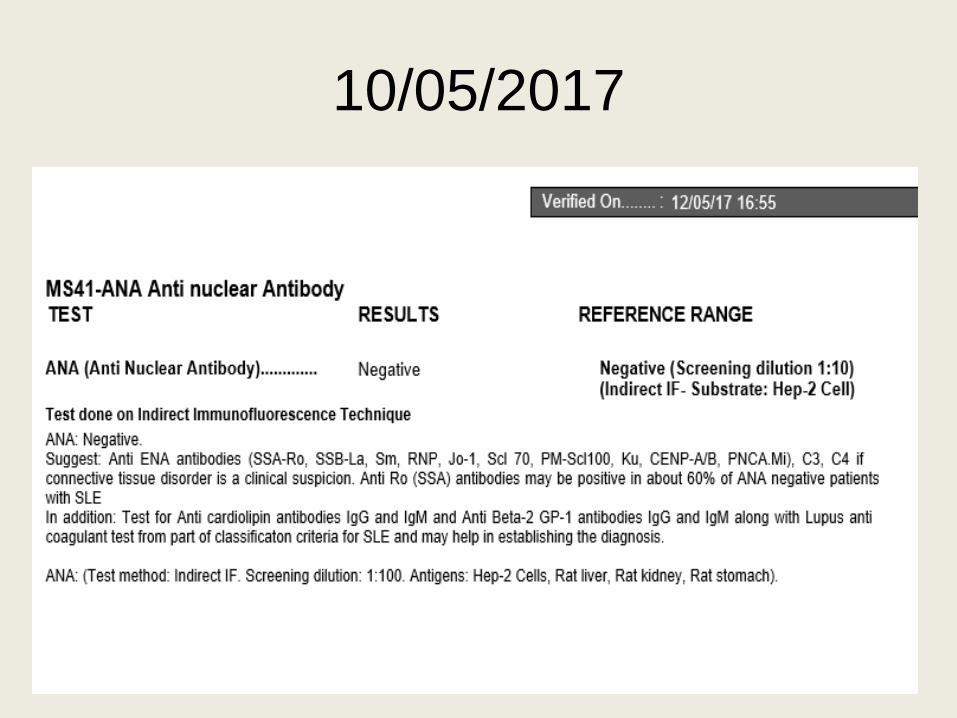
10/05/2017
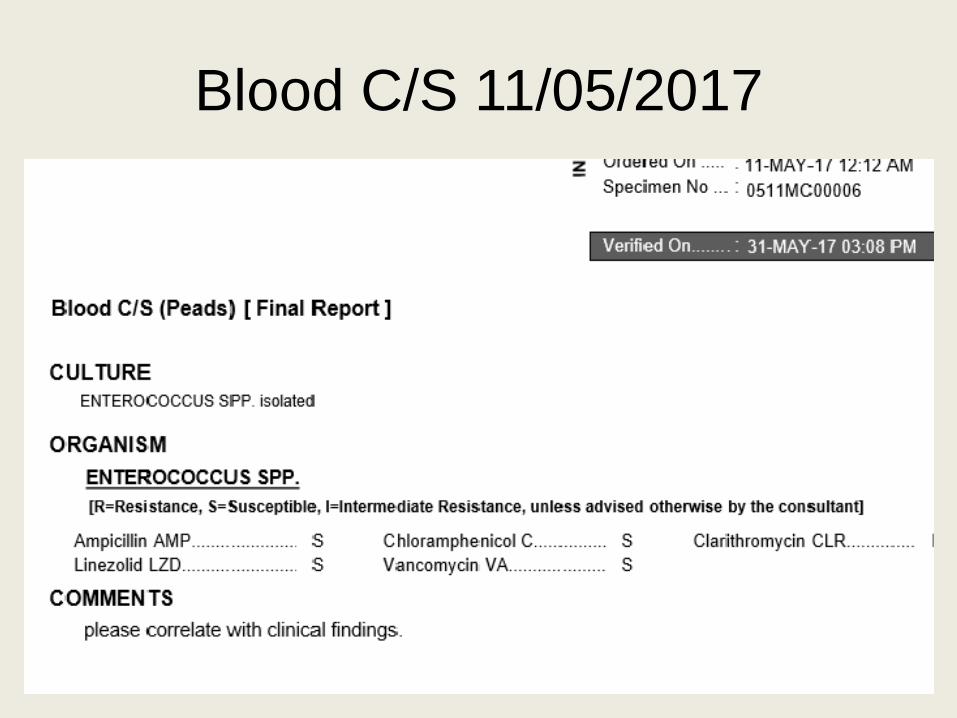
Blood C/S 11/05/2017

12/05/2017
She was clinically improved
Tolerating orally well and was a bit
mobilized.
Discharged home with OPD follow-up after
5 days on
Drain still in situ.
Inj Ceftriaxone 2 gram IV OD for 5 days.
Tab Metronidazol 400 mg TID
OPD Follow-up 15/05/2017
• Clinically improved
• Fever spikes improved
• Ambulatory at the moment
• Vitals: Spo2: 98, HR:134, Temp: 38.4C
• Plan: Tab Metronidazole 400 mg TID 1 week
• Tab Ciprofloxacin 250 mg BD 1 week
• Drain removed and advised follow-up after 1
week.
OPD Follow-up 23/05/17
• Fever still persits low grade
• Oral intake improved
• On/off abdominal pain and backache
• On exam: systemic exam normal
• Oral ulceration
• Warm and red local area
• Advised CBC, CRP Bone Scan and Blood C/S
• But they didn’t comply and lost to follow-up.
14/06/2017 IPD
• Fever………………15 days.
• Wound dehiscence/discharge……5 days.
• Pain in right lower limb……..5 days
• On exam
• BP 11O/67, HR 134bpm, RR 25/min Temp;38C
• Wound in right iliac region with pus discharge
• Seen by pediatric surgery advised MRI and Orthopedic opinion
14/06/2017 IPD
• Antibiotics were started and orthopedic
consulted
• Inj Cefazolin 300 mg q6 hourly
• Inj Gentamicin 70 mg q8 hourly
• Inj Metronidazole 300 mg q8 hourly
• Analgesic paracetamol and ketorolac.
14/06/17
• Pus sent for Gram Stain and culture
• Gram stain and culture came out to be
negative
• Immunoglobulin level were in normal
range
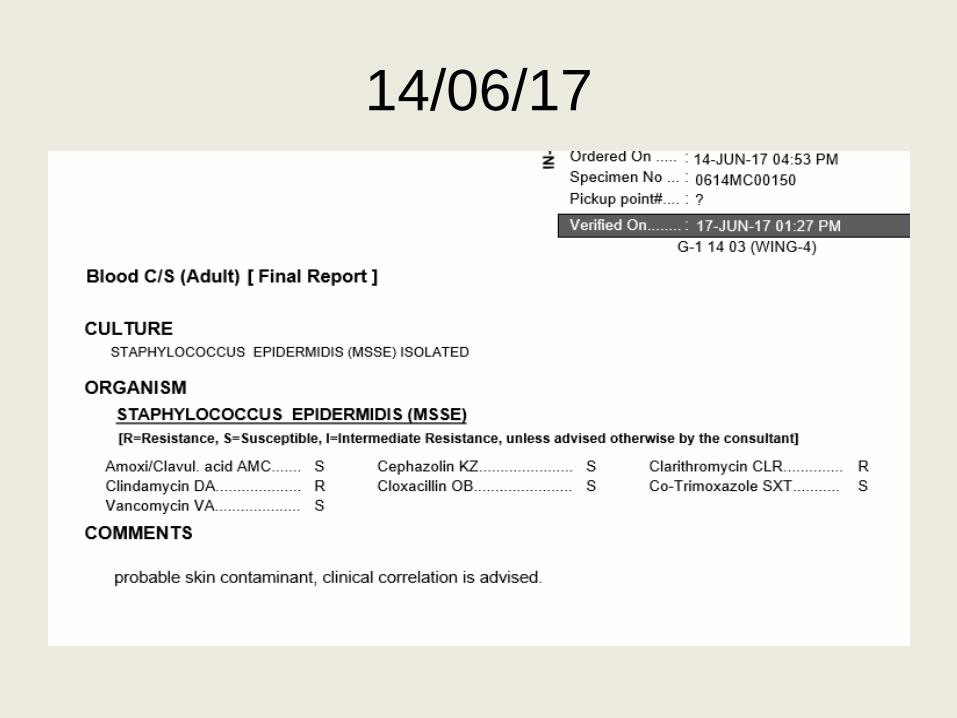
14/06/17
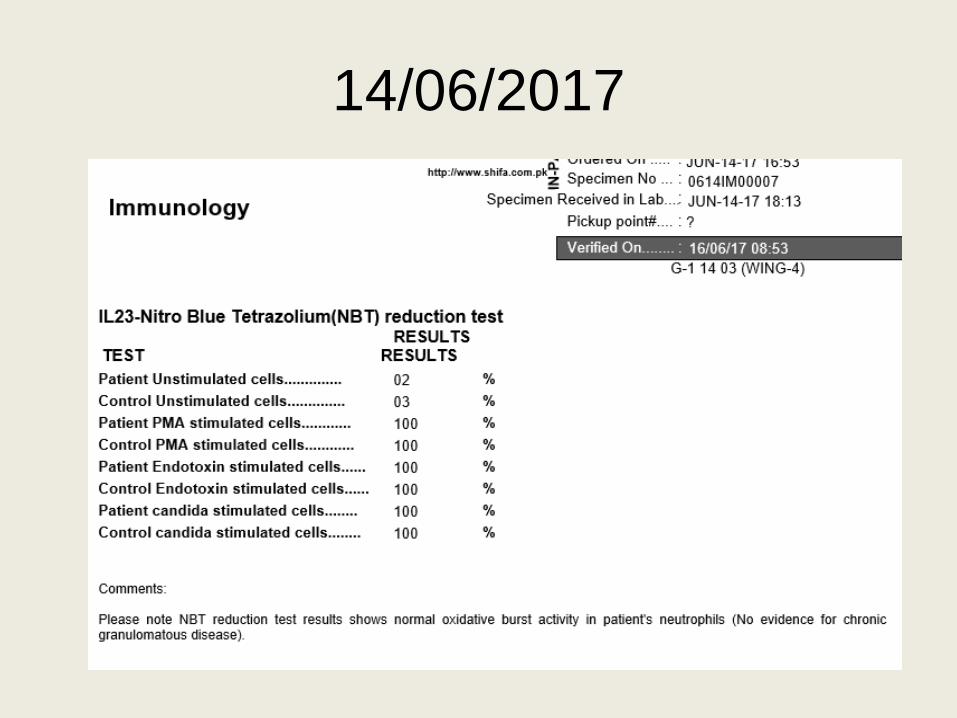
14/06/2017
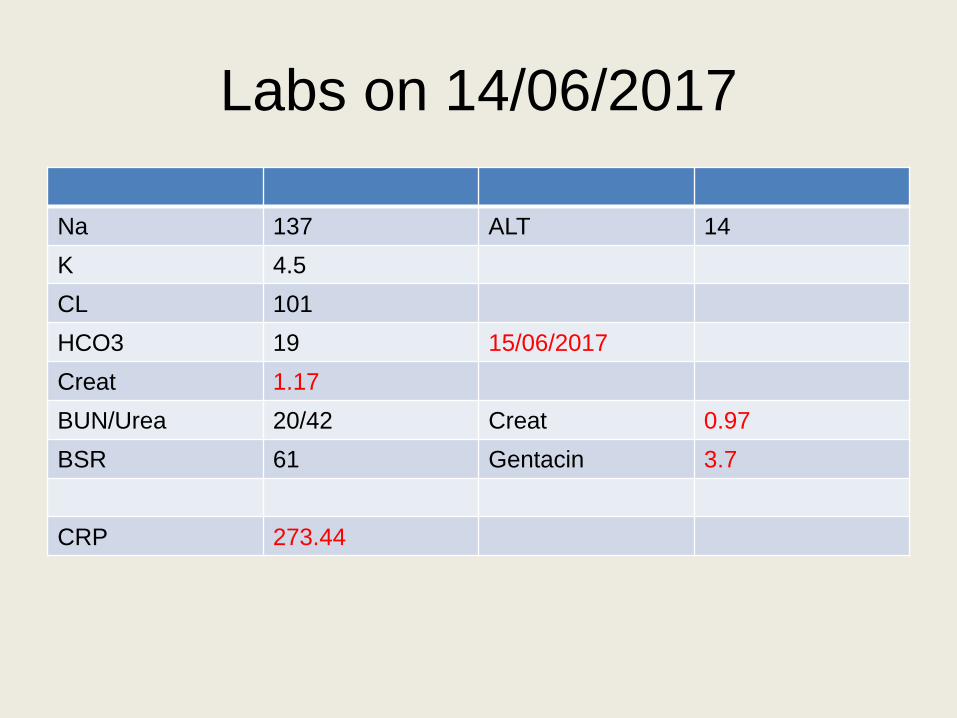
Labs on 14/06/2017
Na 137 ALT 14
K 4.5
CL 101
HCO3 19 15/06/2017
Creat 1.17
BUN/Urea 20/42 Creat 0.97
BSR 61 Gentacin 3.7
CRP 273.44
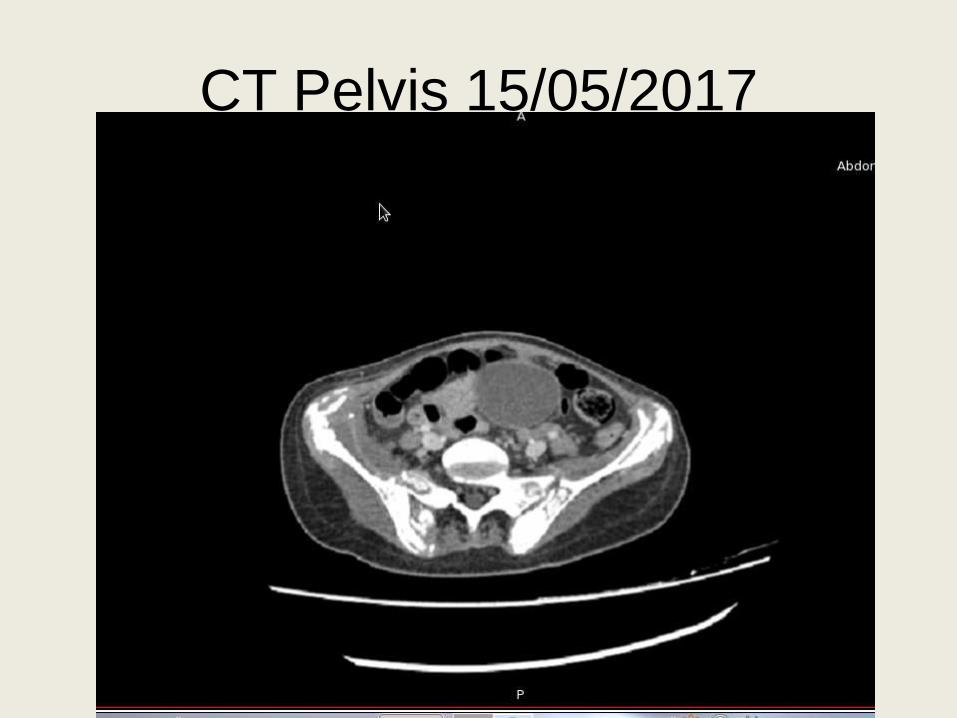
CT Pelvis 15/05/2017
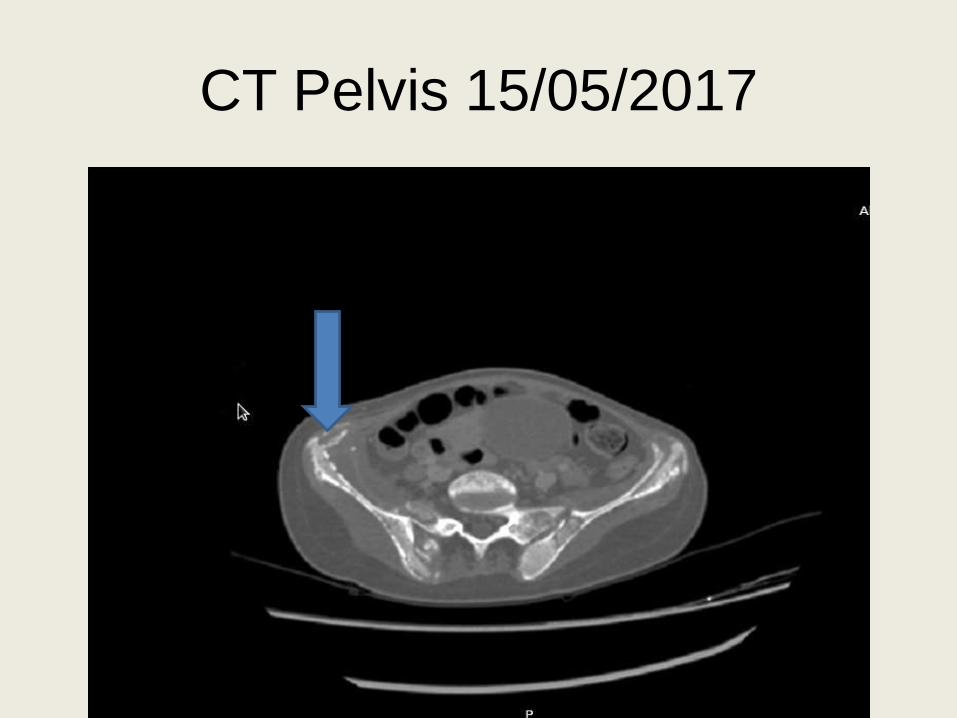
CT Pelvis 15/05/2017
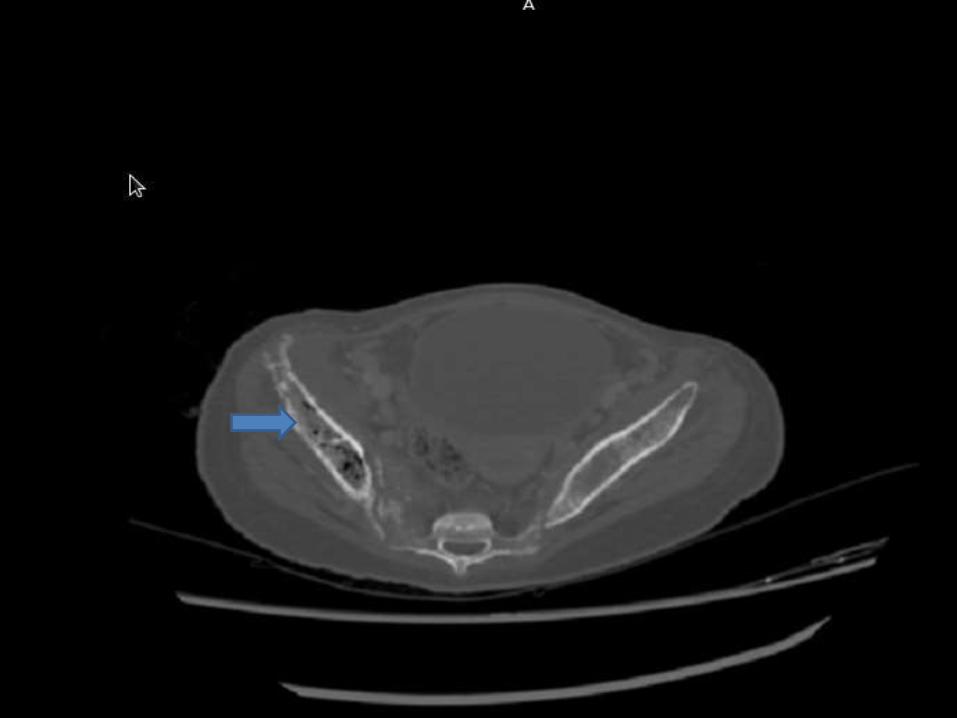
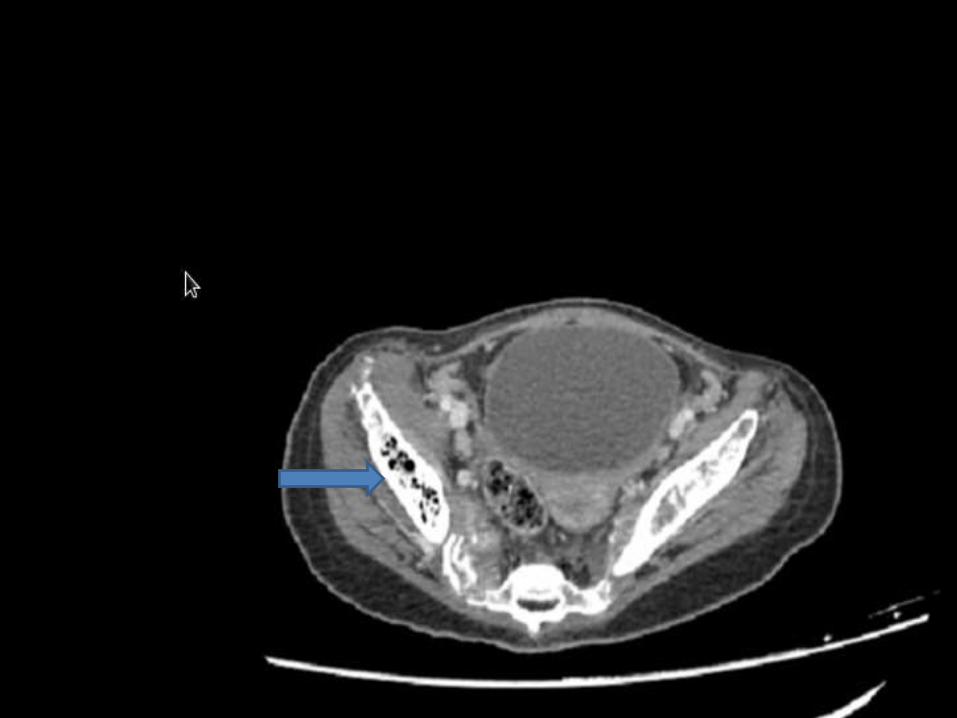
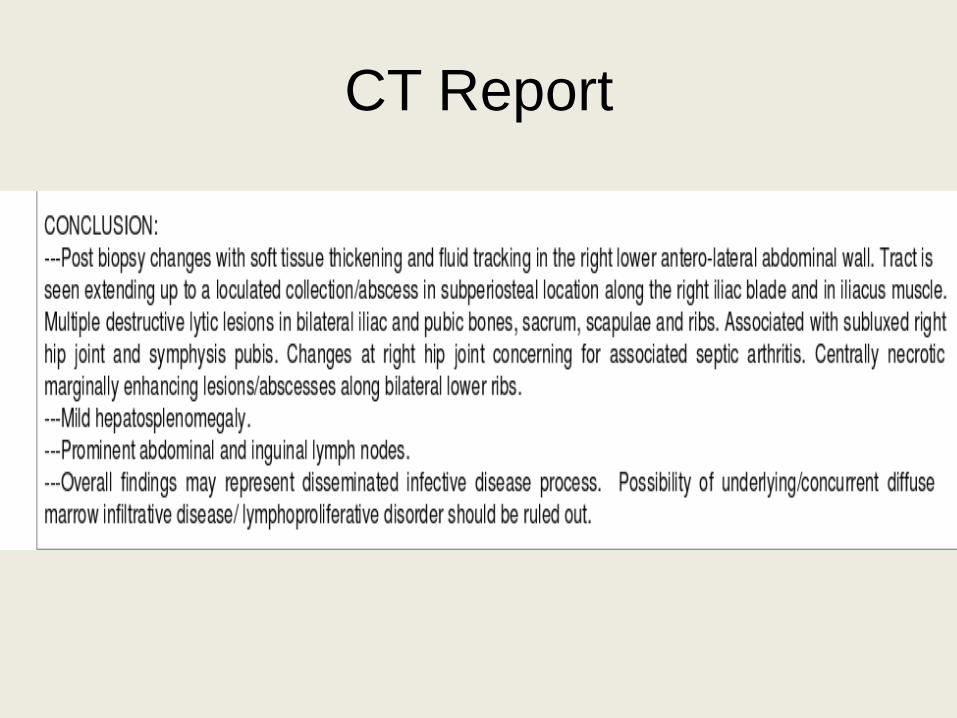
CT Report
16/06/2017
• Still C/O Pain
• Had been afebrile and range of motion at
local joint is decreased.
• CT Scan Pelvis done
• Seen by orthopedics and done
• Right hip Incision and drainage, wound
wash out, advised to continue antibiotics
18/06/2017
• Remained afebrile
• Not in distress or pain, drain in place
• Gram stain showed numerous pus cells
otherwise no growth of organism
• Advised to repeat CBC, CRP, Creat, ESR,
HIV and IgE levels.
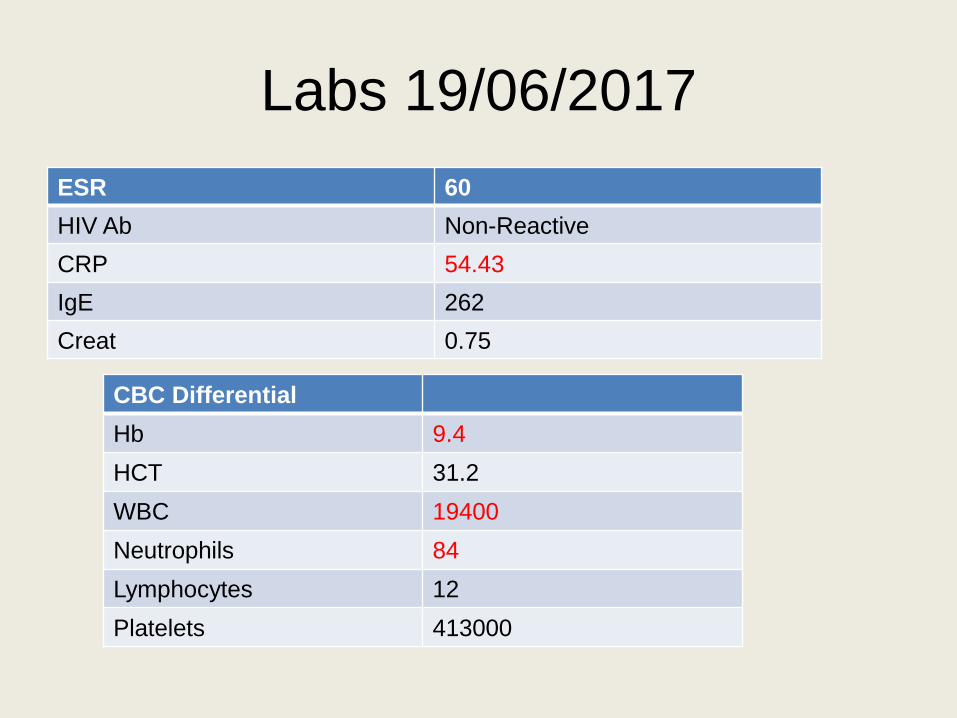
Labs 19/06/2017
ESR 60
HIV Ab Non-Reactive
CRP 54.43
IgE 262
Creat 0.75
CBC Differential
Hb 9.4
HCT 31.2
WBC 19400
Neutrophils 84
Lymphocytes 12
Platelets 413000
Current status of patient
• Still admitted with on/off fever spikes and severe pain in local area still fluid draining from drains inserted after orthopedic surgery
• Antibiotics
• Cefazolin 750 mg q8 hourly IV
• Metronidazole 300 mg IV q8 hourly
• Gentamicin 70 mg q8 hourly IV
• Co-Trimoxazole 160 mg q12 hourly orally
• Nalbuphine and gravinate for IV analgesia Q6h
• Paracetamol 500 mg IV q8H
Questions
What may have contributed to this patient’s morbidity?
Was it preventable or not?
What is the current acceptable morbidity and mortality
associated with this condition?
What are the current evidence based guidelines for the
treatment of this condition?
What are the lessons learned for future management?
Osteomyelitis
• Haematogenous infection is the most common, acute or subacute.
• Long bones are most often affected in children.
• Most unifocal, 5–20 % multifocal.
• In neonates, OM is often multifocal with associated SA.
• Chronic recurrent multifocal osteomyelitis
• Rare inflammatory condition.
• Recurrent, sterile, lytic lesions.
• Often in the clavicle, humerus, and tubular bones.
Etiology
• Neonates
• Group B streptococcus (GBS), Methicillin sensitive Staphylococcus
aureus, (MSSA), Escherichia coli
• Gram-negatives, Candida albicans
• <2 years
• MSSA, Kingella kingae, Streptococcus pneumoniae , non-typeable
Haemophilus spp., E. coli
, MSSA PVL (uncommon in the UK), MRSA PVL
• 2–5 years
• MSSA, K. kingae , group A streptococcus (GAS), S. pneumoniae,
non-typeable Haemophilus spp., MSSA PVL MRSA PVL, Coxeilla
burnettii.
Etiology cont’d
• >5 years
• MSSA, MSSA PVL (uncommon in the UK), MRSA PVL
• Other much rarer organisms (consider in immunosuppressed
children or other risk factors)
• H. influenzae type b (unimmunized), coagulase-negative
Staphylococcus (subacute), Pseudomonas spp., Neisseria
gonorrhoeae, Neisseria meningitidis
• Mycobacterium tuberculosis Salmonella spp. (sickle cell disease),
Bartonella henselae , non-tuberculous mycobacteria, Klebsiella
spp., Fusobacterium (often multifocal), Aspergillus Candida
albicans

Signs symptoms of osteomyelitis
Child
• Usually short history, with an ill child in pain.
• Fever frequent, but may be absent.
• Refusal to move the limb or to weight bear, limp, erythema, bone or
• limb swelling, local tenderness.
• In SA there is a unifocal hot, immobile, tender peripheral joint, with pain on passive joint movement.
• May have no focal signs.
Chronic/multifocal osteomyelitis.
• Subacute or chronic osteomyelitis
• Longer history, maybe weeks, with no systemic symptoms.
• Often no fever. Less acute local signs with limp, refusal to move the limb or weight bear, local bony swelling or tenderness.
• Chronic recurrent multifocal osteomyelitis
• Initially indistinguishable from acute/subacute OM.
• Histology non-specific.
• Pain may be severe, persistent and debilitating.
Risk factors and differentials
• Risk factors
• Trauma, sickle cell disease, immunodeficiency, penetrating wounds,
• bone fixators or plates, varicella infection (GAS).
• Differential diagnosis
• Trauma including non-accidental injury, malignancy (osteosarcoma, leukaemia, neuroblastoma), reactive arthritis, haemarthrosis,
• Henoch–Schönlein purpura, juvenile idiopathic arthritis, tuberculosis.
Investigations
• Blood tests
• C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) more reliably increased than white cell count but normal values do not absolutely exclude OM or SA (although osteoarticularinfection is less likely if CRP and ESR are normal).
• Microbiological culture of blood (all cases), joint fluid (from aspiration), periosteal pus or bone biopsy.
• Difficult cases may require molecular diagnostic techniques (e.g. 16S rDNA polymerase chain reaction (PCR), targeted multiplex PCR)
Imaging
• Plain radiographs are often unhelpful in acute presentations as osteolytic changes/periosteal elevation occur 10–21 days after the onset of symptoms. They are important as a baseline assessment, to exclude trauma and in subacutepresentations.
• Ultrasonography is useful for identifying deep effusions in SA and
• subperiosteal collections in OM.
• Magnetic resonance imaging MRI with enhancement has best diagnostic sensitivity and specificity.
• Technetium radionuclide bone scan ( 99mTc)
• High sensitivity and specificity but used less often due to the radiation burden
• May give false-negative results in infancy
Management
• Multidisciplinary including paediatricians,
orthopaedic surgeons, radiologists and
microbiologists.
• Little high quality evidence to guide
therapy, but established, consistent
practice.
Surgical management
• Often not required in OM with early radiographic signs.
• Surgical drainage in acute OM is indicated if no response to antibiotics
• after 48–72 hours or if radiological evidence of a substantial pus collection.
• Urgent wash-out and drainage of SA in hip, aspiration and irrigation in other joints, to reduce pressure on growth plate.
• More aggressive surgical management if PVL MSSA or MRSA suspected or confirmed.
• Immobilize any surgically treated limb or focus of infection.
Medical management
• Start empirical intravenous antibiotics on clinical
diagnosis of acute OM or SA.
• Use high doses:
• Neonates to <3 months: intravenous cefotaxime
amoxicillin as in suspected sepsis/meningitis
• ≥ 3 months to ≤ 5 years:
• intravenous cefuroxime monotherapy
• ≥ 6 years:
• intravenous flucloxacillin or clindamycin monotherapy.
• Optimize antimicrobial treatment if organism is identified.

Medical management
• In simple unifocal disease
• a rapid switch to oral therapy may be appropriate:
• Neonates to <3 months:
• consider intravenous to oral switch after 14–21 days if:
• Afebrile+ pain-free for at least 24 hours
• And CRP <20 mg/L or CRP decreased by ≥ 2/3 of highest value.
• Child ≥3 months:
• consider intravenous to oral switch after 48–72 hours if :
• Afebrile + pain-free for at least 24 hours
• andCRP <20 mg/L or CRP decreased by ≥ 2/3 of highest value.
Medical managementWhen switching to oral antibiotics, dose, administration frequency, and
• palatability must be considered.
• Suggested pragmatic empirical oral antibiotic choices where organism
• remains unknown. Use high doses:
• Neonatal- 1–2 months-2 month – 2 years-2–5 years
• : Co-amoxiclav suspension three times daily
• 6–8 years
• : Co-amoxiclav suspension three times daily or
• flucloxacillin four times daily (only if child can take tablets)
• 9–18 years
• : Flucloxacillin four times daily or clindamycin four times daily
• Antibiotic therapy is continued for a total of 3–4 weeks in SA and 4–6 weeks
in OM
Complex disease
• Complex disease (multifocal significant bone destruction,
resistant/unusual pathogen immunosuppressed, sepsis, or
shock) requires prolonged intravenous antibiotic therapy and
the total length of antibiotic course may need to exceed 6
weeks.
• Treatment of complex disease should be managed in
conjunction with experts in bone and joint infection.
• Prolonged intravenous therapy can be given in the community
in some cases
• Chronic recurrent multifocal osteomyelitis: Use simple
analgesia and non-steroidal anti-inflammatory drugs (NSAIDs);
refer to paediatric rheumatologist if alternative or experimental
therapies are considered necessary
Prognosis
• Outcome
• Most children with simple disease are discharged without long-term care or further assessment of growth or function.
• Significant risk of deep venous thrombosis and thromboembolism in children with OM.
• In severe diseases, risk of joint stiffness, limb shortening, dislocation (acutely neonates), and avascular necrosis of affected epiphysis.
• Delay in starting antibiotics for 7-10 days leads to permanent loss of bone structure and future growth abnormality.
• Future research
• The optimal duration of therapy is unknown and shorter treatment courses should be studied in randomized clinical trials.
• The safety of early oral switching in OM and SA should be further investigated in randomized clinical trials.

References
• Manual of Childhood infections by Mike
Sharland 3rd edition (Blue Book) by Royal
College Of Paediatrics and Child Health
(RCPCH)