morphological findings and value of placental examination at fetal and perinatal autopsy
TRANSCRIPT
APMIS 107: 3 3 7 4 5 , 1999 Printed in Denmark . All rights reserved
Copyright 8 A P M I S 1999
ISSN 0903-4641
Morphological findings and value of placental examination at fetal and perinatal autow
LISE GRUPE LARSEN'y2 and NIELS GRA2M2*3
'Department of Pathology, Central Hospital, Naestved, 'Department of Pathology, Rigshospitalet, Copenhagen and 2Pathological-Anatomical Institute, Herlev Hospital, Denmark
Larsen, L. G. & Grrem, N. Morphological findings and value of placental examination at fetal and perinatal autopsy. APMIS 1999; 107:3374.
The purpose of this study was to report on the morphological findings in placentae from abortions, stillbirths and perinatal deaths, and to assess the value of the results of the placental examinations. The material included 341 placentae and their matched autopsies. Fifty placentae came from abor- tions induced for medical reasons, 194 from spontaneous abortions, 84 from stillbirths, and 13 from livebirths. Histological slides from all placentae were reviewed and the placental diagnoses were related to the autopsy diagnoses. Frequently observed placental lesions were inflammation of the membranes and/or umbilical cord, placental edema, vascular lesions, single umbilical artery, and degenerative lesions. The placental examination in pregnancies terminating with fetal or perinatal death was of value in half the cases. Some placental lesions provide us with clues when assessing the cause of fetal death, but such lesions are rare. Two important groups of lesions, acute inflammation of the mem- branes and/or umbilical cord and lesions consistent with uteroplacental vascular insufficiency, seen mainly as infarction and decidual arteriopathy, were observed. Gross examination is informative, though microscopic examination is often necessary.
Key words: Placenta; morphology; abortion; stillbirth; perinatal death.
Lise Grupe Larsen, Department of Pathology, Central Hospital, DK-4700 Nrestved, Denmark.
The events of a pathological pregnancy leading to fetal death, stillbirth or perinatal death are not always obvious from the clinical history and an autopsy of the fetus or the infant, including an examination of the placenta, might be an im- portant diagnostic tool ( 1 , 15, 16). The placenta does not die with the fetus. The placenta un- dergoes morphological changes, and these changes have to be taken into account at the examination (5 ) . However, the placenta will not be macerated at intrauterine death to the same degree as the fetus, and microscopically the pla- centa might look viable even some time after the death of the fetus. Examination of the placental
Received June 22, 1998. Accepted September 22, 1998.
tissue might provide important information about the pathological pregnancy (22).
The present study reports on placental mor- phology at abortion, stillbirth and perinatal death, and compares the findings of the placen- tal examination with the results of the autop- sies, in order to evaluate the extent to which placental examination provides valuable infor- mation about the cause of death and other au- topsy results.
MATERIALS AND METHODS
Patients The material consisted of 341 placentae belonging
to a consecutive series of 425 fetal and perinatal aut- opsies performed at the Pathological-Anatomical In-
331

LARSEN er al
stitute, Copenhagen County Hospital in Herlev, dur- ing the 5-year period 1989-1993. During this period the institute performed fetal and perinatal autopsies for the hospitals in Copenhagen County, covering a population of roughly 600,000.
Of the 341 placentae included in the study, 50 came from abortions induced for medical reasons (ges- tational age 13-27 weeks), 194 from spontaneous abortions (gestational age 9-27 weeks), 84 from stillbirths (gestational age 28-43 weeks), and 13 from live births (gestational age 19-39 weeks; 12 died 0-7 days and 1 died 8-28 days after delivery).
In 84 of the 425 consecutive autopsy cases, no pla- centa or only fragments had been sent for examina- tion. These 84 cases included 12 abortions induced for medical reasons, 36 spontaneous abortions, 11 stillbirths, and 25 live births. From these figures it is clear that the 13 livebirths examined in the material represent only a fraction of autopsied neonates in the population; it is difficult and often impossible to ob- tain placenta from children who die some time after delivery.
The study was approved by the Local Ethics Com- mittee and the Danish Data Protection Agency.
Autopsies The fetuses, infants and placentae were submitted
for routine examination, which was performed by one of the two authors, or under their close supervision. The purposes of the autopsies were: 1) to confirm and improve the previous clinical diagnosis, 2) to demon- strate possible complications of diagnostic and thera- peutic procedures, 3) to form a basis for counselling the parents, and 4) to form a basis for perinatal audit. The autopsies were performed according to a protocol which remained unchanged during the 5-year period. In brief, an autopsy included reading the clinical re- port, external examination, radiography, internal ex- amination and full organ microscopy. Tissue or cells were taken for chromosomal or biochemical studies before or at the autopsy in selected cases. An autopsy report was issued.
Depending on the autopsy findings the 341 autop- sies were divided into 9 groups each with common features: 149 autopsies with no specific pathology, 74 with chromosomal abnormalities and/or malfor- mations, 2 with metabolic disease, 4 with hydrops- fetalis, 6 with oligohydramnios, 32 with intrauterine pneumonia, 18 with growth retardation, 16 with se- quelae of asphyxia, and 40 with multiple gestation (twins or triplets).
The degree of maceration was assessed as none, mild, moderate or severe according to Wigglesworth & Singer (27).
Placentae The placentae were fixed in 10% buffered formalin
shortly after delivery. They were weighed after the umbilical cord and the free membranes had been re-
moved. Abnormalities were recorded as well as num- bers and estimated volume of macroscopically visible focal lesions. Sampling for microscopic examination routinely included two to three full-thickness blocks of placental parenchyma, one block of extraplacental membranes, one block with a section of the umbilical cord and blocks from macroscopically visible focal lesions. The tissue was embedded in paraffin and 5 pm sections were cut and stained with haematoxylin- eosin. A separate report not including autopsy data was issued.
Review After the 5-year period, reports on the placental
examinations and matching histological slides were reviewed by one of the authors (LGL). Placental lesions were recorded according to a predetermined list, applying the definitions of Macpherson (1 6) and Kaplan et al. (1 1). The observed lesions were divided into groups and listed in a system modified from Ku- plan et al. (1 1) and Langston et al. (1 5) .
Inflammation of the membranes and the placental parenchyma as well as edema of the villi was graded as mild, moderate or severe. The degree of inflam- mation of the membranes was assessed according to reference slides as mild (few and small foci), moder- ate (more diffuse and intense), or severe (widespread intense infiltrate with or without necrosis). The amount of infarction and fibrin deposition was noted as the percentage of the lesions in the total placenta. Decidual arteriopathy was defined as arteries in de- cidual regions without physiological changes or with atherosis. The other lesions were listed as present or absent. Abruption is not mentioned in this study as the clinical information on the deliveries was insuf- ficient. Information on some macroscopic obser- vations is missing in this retrospective study, e.g. the length of the umbilical cord, and some microscopic observations were too difficult to report objectively, e.g. trophoblast hyperplasia. Other lesions with a rare occurrence, such as maternal floor infarction, were not represented in this material.
Table 1 shows the total observed lesions and in Table 2 the lesions are related to the mode of abor- tion or delivery. The most frequently observed pla- cental lesions are related to the autopsy groups in Table 3 and to the degree of maceration in Table 4.
Assessment of value of placental examination The value of the placental examination (Table 5 )
for fulfillment of the purposes of the autopsy was assessed by matching the autopsy report and the pla- cental findings using the following terms: 1) Conclus- ive: the placental examination contributed conclus- ively to the combined autopsy and placental exami- nation, e.g. findings of multiple chorioangiomas and a growth retarded fetus. 2) Important: with the re- sults of the placental examination the assessment of the course of the pathological pregnancy was more
338
VALUE OF PLACENTAL EXAMINATION
reliable, e.g. demonstration of moderate or severe acute chorioamnionitis. 3) Supplementary: the results of the placental examination supported the results of the autopsy, but no new information for the assess- ment of the course of the pathological pregnancy was found, e.g a single umbilical artery and a fetus with malformations. 4) Doubtful: lesions described in the literature as occurring in pathological pregnancies and in normal pregnancies as well, e.g. true knot of the umbilical cord, but with no tissue reaction. 5) Noncontributary: postmortem degenerative changes or minor lesions, and noncontributary for the results of the combined autopsy and placental examination, e.g. postmortem changes such as fibrous sclerosis of
the stem villi and villous fibrosis matching a macer- ated fetus.
In the evaluation of inflammation of the mem- branes and of villous edema only moderate or severe lesions were considered significant.
RESULTS
Observation of placental lesions Of the cases, 30i were from single pregnan-
cies and 40 were from twin or triplet pregnan-
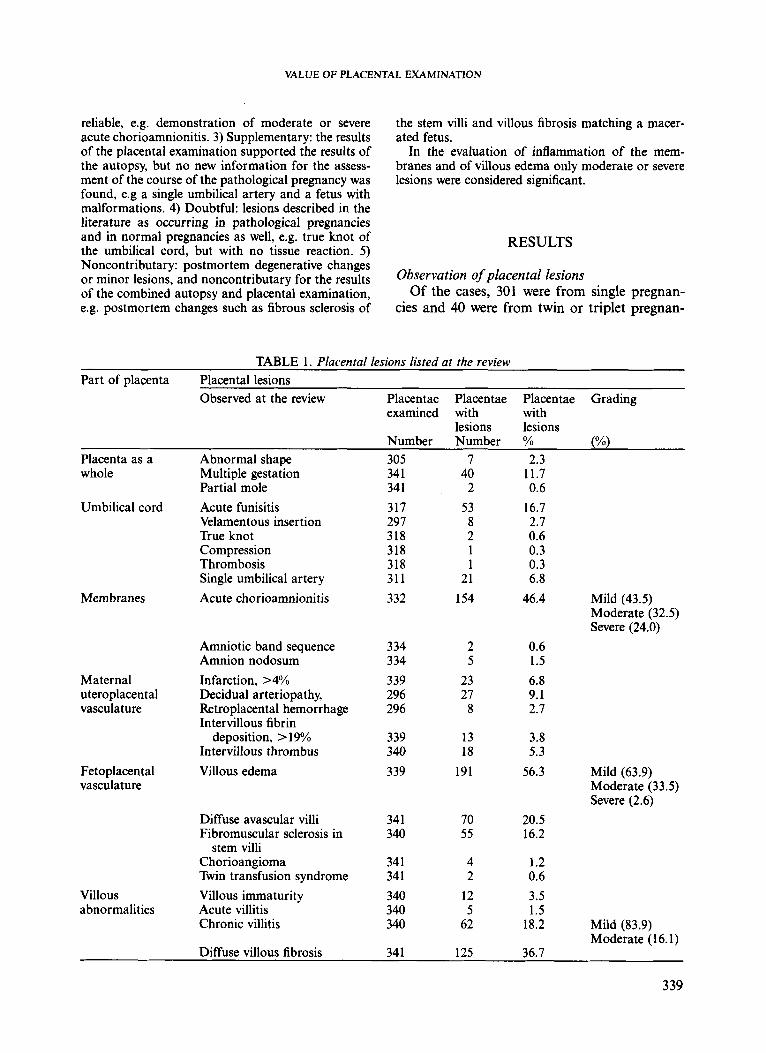
TABLE 1. Placental lesions listed at the review Part of placenta Placental lesions
Observed at the review Placentae Placentae Placentae Grading examined with with
lesions lesions Number Number % (%I
Placenta as a whole
Umbilical cord
Membranes
Maternal uteroplacental vasculature
Fetoplacental vasculature
Villous abnormalities
Abnormal shape Multiple gestation Partial mole Acute funisitis Velamentous insertion True knot Compression Thrombosis Single umbilical artery Acute chorioamnionitis
Amniotic band sequence Amnion nodosum Infarction, >4% Decidual arteriopathy, Retroplacental hemorrhage Intervillous fibrin
deposition, > 19% Intervillous thrombus Villous edema
Diffuse avascular villi Fibromuscular sclerosis in
Chorioangioma Twin transfusion syndrome Villous immaturity Acute villitis Chronic villitis
stem villi
305 34 1 34 1 317 297 318 318 318 31 1 332
334 334 339 296 296
339 340 339
34 1 340
34 1 34 1 340 340 340
7 40 2
53 8 2 1 1
21 154
2 5
23 27
8
13 18
191
70 55
4 2
12 5
62
2.3 11.7 0.6
16.7 2.7 0.6 0.3 0.3 6.8
46.4
0.6 1.5 6.8 9.1 2.7
3.8 5.3
56.3
20.5 16.2
1.2 0.6 3.5 1.5
18.2
Mild (43.5) Moderate (32.5) Severe (24.0)
Mild (63.9) Moderate (33.5) Severe (2.6)
Mild (83.9) Moderate (16.1)
Diffuse villous fibrosis 34 1 125 36.7
339

LARSEN er al.
cies. At the review, some placental lesions were observed more frequently, i.e. in more than 5% of the reviewed placentae (Table I). These in- cluded inflammation or related lesions (acute chorioamnionitis, acute funisitis and villous edema), vascular lesions (placental infarction, decidual arteropathy, chronic villitis and inter- villous thrombus), single umbilical artery and degenerative lesions (diffuse avascular villi, stem
villous fibromuscular sclerosis and villous fi- brosis). The rest of the lesions were observed only occasionally.
In Table 2 the placental lesions are related to groups of abortions or deliveries. A single um- bilical artery was related to abortions induced for medical reasons. Acute inflammation of the membranes and/or umbilical cord as well as vill- ous edema was related to spontaneous abor-
TABLE 2. Placental lesions observed in the material (number) & related to abortion/delivery (%) Placental lesion Placentae Abortion or delivery
with lesions Abortions Spontaneous Stillbirths Live- at the review induced for abortions births
medical reasons (n=50) (n= 194) (n=84) (n=13) YO % YO % Number
Placenta as a whole Abnormal shape Multiple gestation Partial mole
Umbilical cord Acute funisitis Velamentous insertion True knot Compression Trombosis Single umbilical artery
Acute choriooamnionitis Membranes
mild moderatehevere
Amniotic band sequence Amnion nodosum
Infarction >4% Decidual arteriopathy Retroplacental haemorrhage Intervillous fibrin position > 19% Intervillous thrombus
Fetoplacental vasculature Villous edema
Maternal uteroplacental vasculature
mild moderatekevere
Diffuse avascular villi Fibromusculare Sclerosis in stem villi Chorioangioma Twin transfusion
Villous abnormalities Villous immaturity Acute villitis Chronic villitis Diffuse villous fibrosis
7 40 2
0 0 0
71.4 62.5
100
28.6 32.5 0
0 5.0 0
53 8 2 1 1
21
11.3 0 0 0 0
52.4
71.7 25.0 50.0 0 0
23.8
13.2 75.0 50.0
100 100 23.8
3.8 0 0 0 0 0
67 87 2 5
19.4 3.4 0
40.0
49.3 79.3
100 0
28.3 13.9 0
20.0
3.0 3.4 0
40.0
23 27 8
13 18
8.7 11.1 0 7.7 5.6
34.8 70.4 37.5 38.5 50.0
56.5 18.5 62.5 53.8 44.4
122 69 70
18.9 18.8 7.1
68.0 69.6 65.7
11.5 8.7
1.6 2.9 0 27.2
55 4 2
1.8 0 0
45.5 25.0 0
50.9 75.0 50.0
1.8 0
50.0
25.0 20.0 19.4 10.4 -
12 5
62 125
41.7 40.0 71.0 62.4
25.0 40.0
9.6 25.6
8.3 0 0 1.6
340

VALUE OF PLACENTAL EXAMINATION
< < < I I
i 7 ! I
1
I "
,
I
c,
i
i
r C
t 8 r C : 0 c C
E ,[ c
s z
s z
ww w W
o o * o o o o o - . o
tions. Lesions indicating vascular insufficiency, such as placental infarction, decidual arteriopa- thy, intervillous fibrin deposition and chronic villitis, were observed in spontaneous abortions and stillbirths. Degenerative lesions, such as dif- fuse avascular villi, stem villous fibromuscular sclerosis and villous fibrosis, were often ob- served in spontaneous abortions.
Frequently observed placental lesions were related to the autopsy groups, but specific lesions were only found in a few groups (Table 3). In the group of autopsies with no specific pathology, inflammatory and degenerative lesions of the placenta were observed. When intrauterine pneumonia was observed at au- topsy, inflammation was often seen in the mem- branes or in the umbilical cord. In the group of fetuses with intrauterine growth retardation, half of the placentae showed lesions of vascular insufficiency. For the rest of the autopsy groups, no specific placental lesions were found or there were too few cases for further conclusions to be drawn.
The frequently observed placental lesions were related to the degree of maceration at au- topsy (Table 4). If inflammation was observed in the placenta, the fetus was most often pre- served with no maceration. When degenerative placental lesions were observed, more fetuses were macerated.
Value of placental examination The value of the placental examination for
the overall assessment of the case is shown in Table 5. The placental examination was assessed as conclusive in 1.7% of the placentae. This group revealed two partial moles, one matching a triploid fetus and the other matching a fetus with normal karyotype and pneumonia; in one placenta 20% of the parenchyma was replaced by multiple chorioangiomas and the stillborn infant was growth retarded; in a case of amni- otic band sequence, a foot of the macerated fetus was observed in the placental membranes; and in a twin pregnancy, the appearance of the two placental parts matched with transfusion syndrome showing one placental part congested and the other part pale with empty villous capil- laries.
The placental diagnosis was important for the purposes of the autopsy in 120 cases (35.2%). Of these, moderate or severe inflam-
341

LARSEN et al.
TABLE 4. The most frequent placental diagnoses related to the degree of maceration of the fetus or infant Placental lesions All Degree of maceration
None Mild Moderate Severe ?
N N (%) N (%) N (%) N (%) N Acute chorioamnionitis moderatehevere 87 68 (78.2) 6 (6.9) 7 (8.0) 6 (6.9) 0 Acute funisitis 53 36 (67.9) 2 (3.8) 9 (17.0) 6 (11.3) 0 Villous edema moderatehevere 69 49 (71.0) 2 (2.9) 14 (20.3) 4 (5.8) 0 Diffuse avascular villi 70 7 (10.0) 2 (2.9) 29 (41.4) 31 (44.3) 1 Fibromuscular sclerosis 55 13 (23.6) 6 (10.9) 19 (34.5) 17 (30.9) 0 Diffuse villous fibrosis 125 35 (28.0) 10 (8.0) 40 (32.0) 39 (31.2) 1 Maceration was graded according to Wigglesworth & Singer (27). N: Number. ?: Grade of maceration unknown.
mation of membranes, funisitis or acute villitis cord was observed in 88 placentae. Vascular lesions observed in 31 placentae included con- siderable infarctions, decidual arteriopathy, re- troplacental hematoma and intervillous fibrin deposition. In the third group in order of im- portance, compression of the umbilical cord with tissue reaction was observed in one case.
In 24 placentae (7.1%), the examinations were assessed as supplementary. In 12 cases, a single umbilical artery was observed, and chromo- somal abnormalities or malformations were re- ported in the matching fetuses. Four placentae were edematous and the infants were hydropic, three were of unknown etiology, and one au- topsy showed adenoid cystic malformation of the lung. The rest of the supplementary placen- tal diagnoses were thrombus in an umbilical ar- tery, moderate inflammation and amnion nodo- sum in four autopsies with oligohydramnios; and placental granulomas and peripheral retro-
TABLE 5. Value of placental examination for ful- fillment of the purposes of the total examination
Value of placental examination Number % Conclusive 6 1.7 Important
(inflammation*) (vascular lesions) (other)
Supplementary Doubtful Noncontributarv
88 25.8 31 9.1
1 0.3 24 7.1 27 7.9
164 48.1 Total 341 100 * Acute moderate and severe inflammation of the
membranes; funisitis or acute villitis was included.
342
placental hematoma in cases with signs of as- phyxia at autopsy.
In 27 placental examinations (7.9%), the di- agnoses were doubtful as to the result of the combined examination of fetus and placenta. These lesions were umbilical cord lesions such as true knots without tissue reaction, vel- amentous insertion, and single umbilical artery in singletons, twins or triplets without malfor- mations. Other lesions were villous edema and decidual arteriopathy in fetuses without specific pathology at autopsy.
The placental examination was assessed as noncontributory in 164 placentae (48.1Y0). Many of these changes were signs of postmor- tem degeneration, such as stromal fibrosis, dif- fuse avascular villi and fibrous sclerosis of the vessels. Other lesions of no known significance for the result of the combined examination of the fetus and placenta were foci of immature villi in the second trimester, small chorioangi- omas, intervillous thrombus, minimal edema or minimal chorioamnionitis.
DISCUSSION
Placental lesion were observed with different frequency (Tables 1 & 2). The most frequent lesions were inflammation and edema, vascular lesions, single umbilical artery and degenerative lesions, as reported previously (1).
Acute chorioamnionitis is accepted as an im- portant entity leading to premature onset of la- bour, fetal infection and several associated com- plications (2, 15, 16, 28). In many instances,

VALUE OF PLACENTAL EXAMINATION
pathogens are not recovered by conventional aerobic and anaerobic bacteriological methods (28), and many cases with histological evidence of membrane inflammation have been reported as clinically silent (9). Acute inflammation of the membranes or the umbilical cord, in this study deemed an important placental diagnosis, was observed in 88 placentae (25.8%), most often related to spontaneous abortions (Tables 2 & 5 ) . If the autopsy revealed infection of the fetus, the placenta was often inflamed. Further- more, in the autopsy group with no specific pathology, the placental examination often showed inflammation (Table 3). Only moderate or severe inflammation of the membranes was included in the study in order to be sure that the influence of the inflammation was considerable. There is no correlation between mild chor- ioamnionitis and fetal infection or positive bac- terial cultures (28). Marked inflammation has been identified as an indicator of significant in- fection of the fetus and of premature labour (9). Labour might be stimulated as a response to the infection due to production of prostaglandins and of cytokines from activated macrophages. The produced substances attract inflammatory cells from fetal vessels in the membranes or in the umbilical cord. In cases of acute chor- ioamnionitis without fetal infection, fetal com- promise is due to increased metabolic demands of the fetus or vasoconstriction of umbilical cord vessels on account of the accumulation of thromboxanes and prostaglandins (2, 16). Mor- bidity and mortality in association with chor- ioamnionitis have also been related to placental edema (lo), because the edema of the villi com- promises the fetal blood flow (19). The placental edema in this study was not observed more fre- quently if the membranes or the umbilical cord were inflamed. The incidence of acute chor- ioamnionitis varies in different series, but has been reported to be as high as 85% (20). Micro- scopic examination is necessary for the diag- nosis. The distribution of the inflammation in the membranes is thought to be diffuse (20). Sampling one block of the free membranes and two blocks of placental tissue including the chorionic plate is believed to be sufficient to re- veal considerable inflammation (20), but no sys- tematic studies on sampling have been pub- lished. Reporting of acute chorioamnionitis and of acute funisitis is important when discussing
the actual pregnancy (9). Acute funisitis indi- cates an infection prior to fetal death, since the inflammatory response is only possible in a live fetus (16). An observation of acute chor- ioamnionitis with Gram-positive cocci might in- dicate an infection by P-hemolytic streptococci with a risk of recurrence in the next pregnancy (8), but the importance of most of the inflam- matory lesions with respect to future pregnan- cies is unknown.
Lesions indicating uteroplacental vascular in- sufficiency, including infarctions, decidual art- eriopathy, retroplacental hematoma and in- creased intervillous fibrin deposition, were ob- served in 31 placentae (9.1%). The lesions of vascular insufficiency reflect impaired maternal perfusion of the intervillous space (16, 24). In normal pregnancies, dilation of the spiral arter- ies by invasion of intermediate trophoblast in the 14th to 20th gestational week is an essential part of placentation with the establishment of an adequate maternal blood flow (16). If tro- phoblast invasion is inhibited, vascular insuf- ficiency results. Infarction of the placental par- enchyma occurs, and the artery wall might change, which is seen as atherosis (13, 14). The consequent fetoplacental ischaemia is the pri- mary event in many placentae from pregnancies complicated with growth retardation and/or preeclampsia (12, 16, 23). The uteroplacental and fetoplacental circulation regulate each other, with disturbances on the one side leading to disturbances on the other (18). It is generally assumed that destruction of 20% of the placen- tal parenchyma may result in fetal death (4). However, the outcome for the fetus depends on the functional capacity of the surviving tissue rather than the proportion of the placenta that has been destroyed, and an infarction of 5% of the placental parenchyma might indicate more diffuse and serious lesions of the vasculature in- volving a greater part of the placenta (4). Pla- cental infarction and/or decidual arteriopathy was observed in about half the growth-retarded fetuses or infants in this material, and these lesions were rarely observed in the other groups of autopsies (Table 3). In most cases of chronic villitis, no infection is observed and chronic villitis has been related to conditions of low ut- eroplacental circulation (23), but in the present material, chronic villitis was not specific in the autopsy group with growth retardation. In the
343

LARSEN et al.
further examination of placenta on suspicion of vascular insufficiency, other lesions not included in this study such as fetal erythroblastosis (2, 25), iron deposition in villi (17, 18, 24), tropho- blast volume (2, 16) and occurrence of endovas- cular trophoblast in decidual arteries (14) might contribute to the diagnosis. The listed lesions of uteroplacental vascular insufficiency are associ- ated with preeclampsia, maternal hypertension and growth retardation, and for some of the lesions a risk of recurrence in future pregnancies (1 5).
The finding of a single umbilical artery was assessed as a supplementary observation. The phenomenon is reported in 1% of pregnancies (11). A single umbilical artery or amniotic bands are markers of dysmorphogenesis (4). If a single artery is observed, the frequency of associated congenital anomalies varies in dif- ferent studies from 20% to 50% (1 1, 16). We observed such combinations in more than half the cases with chromosomal anomalies and malformations in the fetus in the supplemen- tary group (Table 3). However, cases with a single umbilical artery were also reported in the autopsy groups without signs of dysmor- phogenesis. In multiple pregnancies, a single artery is seen more frequently (3), as indicated in our material.
Serious umbilical cord lesions as seen in this material with compression of the cord and tissue reaction are very important, and should be confirmed microscopically with thrombus, bleeding or inflammatory reactions (16).
Rare placental diagnoses will often provide crucial information about the course of a path- ological pregnancy. The placental examination can provide the definitive clue, as in the six con- clusive cases (1.7%) in the present study. In one placenta, multiple chorioangiomas were ob- served replacing 20% of the placental paren- chyma. Chorangiomas are benign vascular tu- mors associated with perinatal morbidity and mortality, because fetal growth is affected by the shunting of fetal blood from functioning villous tissue (23). In the case with amniotic band se- quence, the fetus was too macerated for proper examination, but on examination of the mem- branes, fetal remnants were observed. Twin transfusion syndrome might be difficult to an- ticipate clinically (26) and the report on the pla- cental examination with marked difference of
the two placental parts grossly and microscopi- cally is important (7). The diagnosis of partial mole, especially in the second trimester, might be difficult to obtain on gross examination of the placenta, but on careful examination of the placental disc, the cystic villi are observed and microscopy will confirm the observation. In all six conclusive cases, the macroscopic examina- tion indicated the pathological condition, but a histological examination was helpful in con- firmation of the diagnosis. Of these placental diagnoses, only moles have a risk of recurrence in future pregnancies (21).
The observed degenerative lesions, such as stem villous fibromuscular sclerosis (1 6.2%), diffuse avascular villi (20.5%) and villous fi- brosis (36.7%), are regarded as postmortal phenomena ( 5 , 6), often related to maceration (Table 4) and especially found in the group of spontaneous abortions (Table 2). These de- generative lesions are probably a reaction sec- ondary to cessation of fetal blood flow at fetal death (16). The significance of the lesions is highly questionable and probably of no import- ance. Morphological changes in the placenta following intrauterine death are marked after 2 weeks (6). Other focal but important lesions might be diagnosed even at that time, but dif- fuse lesions seem to be hidden in the degenerat- ive changes.
Lesions in the large group of placentae pro- viding no contributary information, besides the degenerative lesions described above, were sub- chorionic fibrin deposition, foci of immature villi, small chorioangiomas and intervillous thrombi. At present, the relation of the lesions to fetal death is unknown. Whether mild acute chorioamnionitis is the early stage of inflam- mation or is related to lesser pathogenicity than a more severe grade of inflammation is un- known, and mild inflammation has no relation to fetal morbidity (28).
The results of the present study showed that placental examination in pregnancies terminat- ing with fetal or perinatal death was of value in half the cases, in agreement with Agapitos et al. (1). If clinicians, microbiologists and pathol- ogists continue to work in close collaboration, even better results might be obtained (4). How- ever, assessment of the value of placental exami- nations is subjective and in some cases it is dif- ficult to interpret the placental findings.
344
VALUE OF PLACENTAL EXAMINATION
REFERENCES
1. Agapitos, E.. Papadopoulou, C., Kavantzas. N. , Papoulias, J., Antonaki, V. & Davaris, P.: The contribution of pathological examination of the placenta in the investigation of the causes of foetal mortality. Arch. Anat. Cytol. Path 44: 5- 11, 1996.
2. Altshuler, G.: Role of the placenta in perinatal pathology (revisited). Pediatric Pathol. 16: 207- 233, 1996.
3. Bernirschke, K.: Examination of the placenta. Obstet. Gynecol. 18: 309-333, 1961.
4. Driscoll, S. G.: Placental examination in a clin- ical setting. Arch. Pathol. Lab. Med. 115: 668- 671, 1991.
5. Fox, H.: Morphological changes in the human placenta following fetal death. J. Obstet. Gynaec- 01. Br. Commonw. 75: 839-843, 1968.
6. Genest, D. R.: Estimating the time of death in stillborn fetuses. 11. Histologic evaluation of the placenta; a study of 71 stillborns. Obstet. Gyne-
7. Gersell, D. J.: ASCP survey on placental exami- nation. Am. J. Clin. Pathol. 109: 127-143, 1998.
8. Gotoff; S. P. & Boyer, K. M.: Prevention of group B streptococcal early onset sepsis. Pediatr. Infect. Dis. J. 8: 268-270, 1989.
9. van Hoeven, K. H., Anyaegbunam, A., Hochster, H., Whitty, J. E., Distant. J., Crawford, C. & Factor, S. M.: Clinical significance of increasing histologic severity of acute inflammation in the fetal membranes and umbilical cord. Pediatr. Pathol. Lab. Med. 16: 731-744, 1996.
10. Ilagan, N. B., Elias. E. G., Liang, K. C. , Kazzi, G. , Piligian, J. & Khatib, G.: Perinatal and neo- natal significance of bacteria-related placental villous edema. Acta Obstet. Gynecol. Scand. 69:
11. Kaplan, C. , Lowell, D. M. & Salafia, C.: College of American Pathologists Conference XIX on the Examination of the Placenta: report of the Working Group on the Definition of Structural Changes Associated with Abnormal Function in the Maternal/Fetal/Placental Unit in the Second and Third Trimesters. Arch. Pathol. Lab. Med.
12. Khong. T. Y., De Wolj; F., Robertson, W. B. & Brosens, I. : Inadequate maternal vascular re- sponse to placentation in pregnancies compli- cated by pre-eclampsia and by small-for-ges- tational-age infants. Br. J. Obstet. Gynaecol. 93:
13. Khong, T. Y.: Acute atherosis in pregnancies complicated by hypertension, small-for-ges- tational-age infants, and diabetes mellitus. Arch. Pathol. Lab. Med. 115: 122-725, 1991.
14. Khong, T. Y.. Sawyer, I. H. & Heryet, A. R.: An
C O ~ . 80: 585-592, 1992.
287-290, 1990.
115: 709-716, 1991.
1049-1059, 1986.
immunohistologic study of endothelialization of uteroplacental vessels in human pregnancy - evi- dence that endothelium is focally disrupted by trophoblast in preeclampsia. Am. J. Obstet. Gynecol. 167: 751-756, 1992.
15. Lungston, C. , Kaplan, C., Macpherson. T., Man- ci, E.. Peevy, K., Clark, B., Murtagh. C. , Cox, S. & Glenn, G.: Practice guideline for examina- tion of the placenta. Arch. Pathol. Lab. Med. 121: 449476, 1997.
16. Macpherson, T.: Fact and fancy. What can we really tell from the placenta? Arch. Pathol. Lab. Med. 115: 672-681, 1991.
17. McDermott, M. & Gillan, J. E.: Chronic reduc- tion in fetal blood flow is associated with placen- tal infarction. Placenta 16: 165-1 70, 1995.
18. McDermott, M . & Gillan, J. E.: Trophoblast basement membrane haemosiderosis in the pla- cental lesion of fetal artery thrombosis: a marker for disturbance of maternofetal transfer? Pla- centa 16: 171-178, 1995.
19. Naeye, R. L., Maisels, M. J., Lorenz, R. P. & Botti, J. J.: The clinical significance of placental villous edema. Pediatrics 71: 588-594, 1983.
20. Nordenvall, M. & Sandstedt, B.: Chorioamnio- nitis in relation to gestational outcome in a Swed- ish population. Eur. J. Obstet. Gynecol. Reprod. Biol. 36: 59-67, 1990.
21. Parazzini, F., Mangili, G., La Vecchia, C . , Negri, E., Bocciolone, L. & Fasoli, M.: Risk factors for gestational trophoblastic disease: a separate analysis of complete and partial hydatidiform moles. Obstet. Gynecol. 78: 1039-1045, 1991.
22. Rayburn, W. , Sander, C., Barr, M. & Rygiel, R.: The stillborn fetus: placental histologic examina- tion in determining a cause. Obstet. Gynecol. 65:
23. Rayburn, W., Sander, C. & Compton, A,: Histo- logic examination of the placenta in the growth- retarded fetus. Am. J. Perinatol. 6: 58-81, 1989.
24. Redline, R. W. & Patterson, P.: Patterns of pla- cental injury. Arch. Pathol. Lab. Med. 118: 698- 701, 1994.
25. Salafia, C. M. , Minior, V. K., Pezzullo, J. C., Po- pek, E. J., Rosenkrantz, T. S. & Vintzileos, A . M.: Intrauterine growth restriction in infants of less than thirty-two weeks’ gestation: associated placental pathologic features. Am. J. Obstet. Gynecol. 173: 1049-1057, 1995.
26. Sander, C. M.: What’s new in placental pathol- ogy. Pathol. Annu. 30: 59-93, 1995.
27. Wigglesworth, J. S. & Singer, D. B.: Fetal death and the macerated stillborn fetus. In: Perinatal Pathology. Blackwell Scientific Publications, Bos- ton 1996, p. 264.
28. Zhang, J. , Kraus, F. T. & Aquino, T. I.: Chor- ioamnionitis: a comparative histologic, bacteriol- ogic, and clinical study. Int. J. Gynecol. Pathol.
637-641, 1985.
4: 1-10, 1985.
345