mortality and demographic data 2012 - ministry of health · web viewmortality and demographic...
TRANSCRIPT

Mortality and Demographic Data2012

CopyrightThe copyright owner of this publication is the Ministry of Health, which is part of the New Zealand Crown.
The Ministry of Health permits the reproduction of material from this publication without prior notification, provided that all the following conditions are met. The content is not distorted or changed. The information is not sold. The material is not used to promote or endorse any product or service. The material is not used in an inappropriate or misleading context, having regard
to the nature of the material. Any relevant disclaimers, qualifications or caveats included in the publication are
reproduced. The New Zealand Ministry of Health is acknowledged as the source.
DisclaimerThe purpose of this publication is to inform discussion and assist policy development. The opinions expressed in the publication do not necessarily reflect the official views of the Ministry of Health.
All care has been taken in the production of this publication; the data was considered to be accurate at the time of publication, but may be subject to slight changes over time as further information is received. It is advisable to check the current status of figures given here with the Ministry of Health before quoting or using them in further analysis.
The Ministry of Health makes no warranty, expressed or implied, nor assumes any legal liability or responsibility for the accuracy, correctness, completeness or use of the information or data in this publication. Further, the Ministry of Health will not be liable for any loss or damage arising directly or indirectly from the information or data presented in this publication.
Citation: Ministry of Health. 2015. Mortality and Demographic Data 2012. Wellington: Ministry of Health.
Published in November 2015by the Ministry of Health
PO Box 5013, Wellington 6145, New Zealand
ISBN: 978-0-947491-08-6 (online)HP 6276
This document is available at health.govt.nz

This work is licensed under the Creative Commons Attribution 4.0 International licence. In essence, you are free to: share, ie, copy and redistribute the material in any medium or format; adapt, ie, remix, transform and build upon the material. You must give appropriate credit, provide a link to the licence and indicate if changes were made.

AcknowledgementsMany people have assisted in the production of this publication. In particular, the Ministry of Health thanks the peer reviewers for their valuable contribution.
The Ministry of Health would also like to thank the following organisations: Department of Internal Affairs, Births, Deaths and Marriages Ministry of Justice, coroners and the Coronial Services Unit Land Transport New Zealand Water Safety New Zealand district health boards.
iv Mortality and Demographic Data 2011

Mortality and Demographic Data 2012 v

ContentsAcknowledgements iii
Introduction 1Late data 1Ethnicity data and analysis 3Statistical notes 3Further mortality data 4
Mortality 2012: Quick facts 5Number of deaths 5Age-standardised rates 5Selected causes of mortality 2012 5
Mortality in New Zealand 6Overview of mortality statistics 6Selected causes of mortality 12Mortality by region 14
Selected trends 20All cancers 21Lung cancer 26Female breast cancer 29Prostate cancer 32Malignant melanoma of the skin 35Cervical cancer 38Ischaemic heart disease 41Cerebrovascular disease 46Diabetes mellitus 51Motor vehicle accidents 55Suicide 60Maternal mortality 65
Further mortality-related information 68Accompanying online tables 68Ministry of Health publications 68Publications by other organisations 68Population data used for calculating rates 69Additional data available from the Ministry of Health 69
Explanatory notes 71
vi Mortality and Demographic Data 2012

Mortality 71Population 73Ethnicity 74Statistical notes 75
References 77
List of tablesTable 1: Mortality rates, by age group, sex and ethnicity, 2012 7Table 2: Number of deaths and mortality rates, by sex, 1980–2012 8Table 3: Mortality rates from selected causes, by sex and ethnicity, 2012 12Table 4: Number of deaths and mortality rates from all cancers, by sex,
1980–2012 22Table 5: Age distribution of deaths from all cancers, percentages and rates,
by ethnicity and sex, 2012 23Table 6: Number of deaths and mortality rates from lung cancer, by sex,
1980–2012 27Table 7: Age distribution of deaths from lung cancer, percentages and rates,
by ethnicity and sex, 2012 28Table 8: Number of deaths and mortality rates from breast cancer in
females,1980–2012 30
Table 9: Age distribution of deaths from breast cancer in females, percentages and rates, by ethnicity, 2012 31
Table 10: Number of deaths and mortality rates from prostate cancer, 1980–2012 33
Table 11: Age distribution of deaths from prostate cancer in males, percentages and rates, by ethnicity, 2012 34
Table 12: Number of deaths and mortality rates from malignant melanoma of the skin, by sex, 1980–2012 36
Table 13: Age distribution of deaths from malignant melanoma of the skin, percentages and rates, by ethnicity and sex, 2012 37
Table 14: Number of deaths and mortality rates from cervical cancer, 1980–2012 39
Table 15: Age distribution of deaths from cervical cancer, percentages and rates, by ethnicity, 2012 40
Table 16: Number of deaths and mortality rates from ischaemic heart disease, by sex, 1980–2012 42
Table 17: Age distribution of deaths from ischaemic heart disease, percentages and rates, by ethnicity and sex, 2012 43
Table 18: Number of deaths and mortality rates from cerebrovascular disease, by sex, 1980–2012 47
Table 19: Age distribution of deaths from cerebrovascular disease, percentages and rates, by ethnicity and sex, 2012 48
Mortality and Demographic Data 2012 vii

Table 20: Number of deaths and mortality rates from diabetes mellitus, by sex,1980–2012 52
Table 21: Age distribution of deaths from diabetes mellitus, percentages and rates, by ethnicity and sex, 2012 53
Table 22: Number of deaths and mortality rates from motor vehicle accidents, by sex, 1980–2012 56
Table 23: Age distribution of deaths from motor vehicle accidents, percentages and rates, by ethnicity and sex, 2012 57
Table 24: Number of deaths and mortality rates from suicide, by sex, 1980–2012 61
Table 25: Age distribution of deaths from suicide, percentages and rates, by ethnicity and sex, 2012 62
Table 26: Number of maternal deaths and maternal mortality rates, 1980–2012 66
Table 27: Maternal deaths by underlying cause, 2008–2012 67Table 28: Mortality data available from the Ministry of Health 70Table 29: Codes used to define amenable mortality 72Table 30: The WHO World Standard Population 76
List of figuresFigure 1: Stages of processing cause of death data in New Zealand 2Figure 2: Number of deaths and mortality rates, by sex, 1950–2012 6Figure 3: Mortality rates, by sex and ethnicity, 1996–2012 9Figure 4: Mortality rates for the five major causes of mortality, 1980–2012 10Figure 5: Age at death, rates by ethnicity, 2012 10Figure 6: Amenable mortality rates per 100,000 people aged 0–74 years, by
sex and ethnicity, 2000–2012 11Figure 7: Mortality rates, by DHB region, total population, 2012 14Figure 8: Mortality rates, by DHB region, Māori population, 2012 15Figure 9: Mortality rates, by DHB region, non-Māori population, 2012 16Figure 10:Comparison of DHB region mortality rates for Māori and non-Māori,
2012 18Figure 11:Number of deaths and mortality rates from all cancers, by sex,
1950–2012 21Figure 12:Mortality rates from all cancers, by sex and ethnicity, 1996–2012 24Figure 13:Mortality rates from all cancers, by DHB region, total population,
2012 25Figure 14:Number of deaths mortality rates from lung cancer, by sex, 1950–
2012 26Figure 15:Mortality rates from lung cancer, by sex and ethnicity, 1996–2012 28
viii Mortality and Demographic Data 2012

Figure 16:Number of deaths and mortality rates from breast cancer in females,1950–2012 29
Figure 17:Mortality rates from breast cancer in females, by ethnicity, 1996–2012 31
Figure 18:Number of deaths and mortality rates from prostate cancer, 1950–2012 32
Figure 19:Mortality rates from prostate cancer, by ethnicity, 1996–2012 34Figure 20:Number of deaths and mortality rates from malignant melanoma of
the skin, by sex, 1950–2012 35Figure 21:Number of deaths and mortality rates from cervical cancer, 1950–
2012 38Figure 22:Mortality rates from cervical cancer, by ethnicity, 1996–2012 40Figure 23:Number of deaths and mortality rates from ischaemic heart disease,
by sex, 1950–2012 41Figure 24:Mortality rates from ischaemic heart disease, by sex and ethnicity,
1996–2012 43Figure 25:Mortality rates from acute myocardial infarction (ICD I21) and
chronic ischaemic heart disease (ICD I25), by sex and ethnicity, 2012 44
Figure 26:Mortality rates from ischaemic heart disease, by DHB region, total population, 2012 45
Figure 27:Number of deaths and mortality rates from cerebrovascular disease, by sex, 1950–2012 46
Figure 28:Number of deaths and mortality rates from cerebrovascular disease, by sex and ethnicity, 1996–2012 48
Figure 29:Mortality rates from cerebrovascular disease, by specific disease classification and sex, 2012 49
Figure 30:Mortality rates from cerebrovascular disease, by DHB region, total population, 2012 50
Figure 31:Number of deaths and mortality rates from diabetes mellitus, by sex,1950–2012 51
Figure 32:Mortality rates from diabetes mellitus, by sex and ethnicity, 1996–2012 53
Figure 33:Mortality rates from diabetes mellitus, by diabetes type and sex, 2012 54
Figure 34:Number of deaths and mortality rates from motor vehicle accidents, by sex, 1950–2012 55
Figure 35:Mortality rates from motor vehicle accidents, by sex and ethnicity, 1996–2012 58
Figure 36:Mortality and hospitalisation rates from motor vehicle accidents, and ratio of hospitalisation rate to mortality rate, 1996–2012 59
Figure 37:Number of deaths and mortality rates from suicide, by sex, 1950–2012 60
Mortality and Demographic Data 2012 ix

Figure 38:Mortality rates from suicide, by sex and ethnicity, 1996–2012 62Figure 39:Male mortality and hospitalisation rates from intentional self-harm,
and ratio of hospitalisation rate to mortality rate, 1996–2012 63Figure 40:Female mortality and hospitalisation rates from intentional self-
harm, and ratio of hospitalisation rate to mortality rate, 1996–2012 64Figure 41:Number of maternal deaths and maternal mortality rates, 1950–
2012 65
x Mortality and Demographic Data 2012

IntroductionMortality and Demographic Data 2012 presents data on the underlying cause of each death registered in New Zealand in the 2012 calendar year. The causes of death were coded to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification, Sixth Edition (ICD-10-AM). In this publication, the abbreviation ICD is used to refer to the ICD-10-AM coding system (National Centre for Classification in Health 2008).
Underlying cause of death, as defined by the World Health Organization (WHO), is ‘(a) the disease or injury which initiated the train of morbid events leading directly to death, or (b) the circumstances of the accident or violence which produced the fatal injury’ (WHO 1979).
The three main sources of information for mortality data are: certificates of cause of death from doctors and coroners post-mortem reports death registration forms, which are usually completed by a funeral director.
Figure 1 illustrates the stages of processing cause of death data in New Zealand.
Late dataAt the time of publication of this document, the Ministry of Health was unable to assign specific ICD codes to a small number of deaths due to the extended length of time that some coronial inquiries take. These deaths are included in the statistics under the ICD codes R99 (‘other ill-defined and unspecified causes of mortality’) and X59 (‘exposure to unspecified factor’). Because the Ministry of Health Mortality Collection is a dynamic database, the Ministry will update the records for these deaths with specific underlying cause of death codes once it receives coroners’ findings. This means there may be small differences between later extracts of mortality data and data contained in this publication.
The data for this publication was extracted on 11 March 2015. At that time, the deaths of one infant (aged under one year) and six adults were provisionally coded to underlying causes R99 and X59, and the deaths of six infants, four children (aged 1–14 years), 12 youths (aged 15–24 years) and 102 adults (aged 25 years and over) were provisionally coded to other causes. Coronial inquiries had not been completed for these deaths.
Mortality and Demographic Data 2012 1

Figure 1: Stages of processing cause of death data in New Zealand
Data processing by Ministry of Health
Data dissemination by Ministry of Health
Data collection
Key
Other deathSudden
unexpected death
Doctor certifies cause(s) of death Death registration Coroner’s
investigation
Police investigation
Autopsy
Other (eg, toxicology
report)
Births, Deaths and Marriages Registry (BDM)
Coroner’s report (cause
of death)
NZ Coroner’s Information
System
Ministry of HealthMortality Collection
Amalgamation and record checks
Manual coding of causes of death,
validation and editing process
Release of body
form
Query process
Resolved queries
Cancer Registry
Hospital data
Traffic deaths data
Drownings data
Media reports
Validation and finalisation of
deaths file
Cause(s) of death revised
Unresolved queries
Summary publication series (eg, Mortality and Demographic Data, Suicide Facts,
Fetal and Infant Deaths)
Further data extraction, analysis and reporting as required
Additional information sources
Attach a National Health Index number
Death event
ProcessDecision SubprocessDocumentDatabase External data Start/End
2 Mortality and Demographic Data 2012

Ethnicity data and analysisTwo ethnic groupings are used in the Mortality and Demographic Data publication: Māori and non-Māori. The Māori population includes everyone who was identified as Māori, and the non-Māori population includes everyone else.
Because of changes in the Births, Deaths, Marriages and Relationships Registration Act 1995 that came into force in September 1995, Māori and non-Māori rates from 1996 onwards are not comparable with earlier data. For this reason, the ethnicity trend data in this publication covers a smaller range (ie, 1996 to 2012) than that of the total population data (see ‘Ethnicity’ within this document’s ‘Explanatory notes’ for a discussion of ethnicity coding).
Statistical notesIn this publication, numbers are generally presented to one decimal place. However, calculations are made from the full string (ie, all the numbers after the decimal place), thereby providing more precise reporting.
Age-specific and age-standardised ratesThis publication uses age-specific and age-standardised rates.
Age-specific mortality rates represent the number of deaths in relation to the population size of a particular age group. The number of deaths within an age group is divided by the population of that age group and then multiplied by 100,000.
Age-standardised rates account for differences in population structure, and can be used to compare groups with different age structures (eg, males and females, or Māori and non-Māori) and data from different years. In the present publication, the population structure used is the WHO World Standard Population, and age-standardised rates are per 100,000 population (see ‘Statistical notes’ within ‘Explanatory notes’).
Confidence intervalsWhere appropriate, confidence intervals have been calculated at the 95% or 99% level to aid the interpretation of mortality incidence (Keyfitz 1966). A confidence interval is a range of values used to illustrate the uncertainty around a single value (such as an age-standardised rate). Confidence intervals are calculated with a stated probability; for example 95% (which would indicate that there is a 95% chance that the true value lies within the confidence interval).
Note that Māori populations have lower numbers relative to the total population. This can result in greater variance (and thus larger confidence intervals) when calculating age-standardised rates. Any precise calculations made in the present publication (such as percentage differences between ethnic mortality rates) must be interpreted with this caveat in mind.
Mortality and Demographic Data 2012 3

Further mortality dataStatistical mortality data tables are available online in Excel format alongside this Mortality and Demographic Data 2012 publication at: www.health.govt.nz/publication/mortality-2012-online-tables. The tables published on this page contain mortality data for the complete range of ICD-10-AM classifications, in sex and five-year age groupings. The data is grouped at national, regional and ethnic group (Māori, Pacific, Asian and non-Māori) level.
Other Ministry of Health publications contain further mortality-related data. These include publications on fetal and infant deaths, suicide, and cancer incidence and mortality.
More detailed information on numbers and rates of live births and on fetal, neonatal and post-neonatal deaths is published in the annual publication series Fetal and Infant Deaths (www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/fetal-and-infant-deaths-series).
Information on hospitalisations and mortality from suicide can be found in Suicide Facts: Deaths and intentional self-harm hospitalisations (www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/suicide-facts-deaths-and-intentional-self-harm-hospitalisations-series).
Information on cancer registrations and mortality can be found in Cancer: New Registrations and Deaths (www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/cancer-new-registrations-and-deaths-series).
For a complete listing of other mortality-related data, see ‘Further mortality-related information’.
4 Mortality and Demographic Data 2012

Mortality 2012: Quick factsNumber of deaths
2012 mortality
Male Female Total
Māori 1643 1421 3064
Non-Māori 13,505 13,708 27,213
Total 15,148 15,129 30,277
Age-standardised rates2012 mortality rates
Male Female Total
Māori 743.3 567.6 649.3
Non-Māori 425.1 305.9 362.0
Total 463.0 332.7 393.6
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Selected causes of mortality 2012Condition Total
deathsPercentage of deaths by sex
Māori rate Non-Māori rate Total rate
Male Female Male Female Male Female Male Female
All cancer 8905 53.2 46.8 209.5 192.5 135.9 101.1 143.4 109.0
Lung cancer‡ 1628 54.7 45.3 65.4 66.4 23.9 15.7 27.1 19.7
Female breast cancer 617 … 100.0 … 26.5 … 16.9 … 17.7
Prostate cancer 607 100.0 … 18.1 … 16.4 … 17.0 …
Melanoma of the skin 354 62.7 37.3 0.9 0.8 7.2 3.8 6.8 3.6
Cervical cancer 56 … 100.0 … 3.7 … 1.6 … 1.8
Ischaemic heart disease 5339 55.3 44.7 140.3 77.2 78.5 40.0 85.2 43.8
Cerebrovascular disease 2612 37.1 62.9 30.3 31.7 25.7 28.4 27.1 29.6
Diabetes mellitus 807 53.3 46.7 48.3 33.8 9.9 6.6 12.8 8.6
Suicide 550 73.5 26.5 25.3 10.5 16.3 5.2 18.5 6.4
Motor vehicle accidents 347 73.5 26.5 22.4 6.3 9.3 3.2 11.3 3.7
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
‡ Includes cancer of the trachea, bronchus and lung.
... = Not applicable.
Mortality and Demographic Data 2012 5

Mortality in New ZealandThis section presents an overview of national mortality statistics in 2012, describes trends in mortality over time and examines selected major causes of mortality in 2012.
Overview of mortality statisticsThere were 30,277 deaths registered in New Zealand in 2012. The number of deaths generally increased over time (Figure 2). This trend is not surprising bearing in mind that the total population of New Zealand increased at the same time. A more useful measure of mortality is the age-standardised mortality rate, allowing comparisons to be made over time and between differing groups.1 From 1950 to 2012, the mortality rate showed a strong downward trend when adjusted for age. In 2012 there were 393.6 deaths per 100,000 population.
Figure 2: Number of deaths and mortality rates, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
In 2012, there were equivalent numbers of male and female deaths (15,148 male deaths and 15,129 female deaths). However, the age-standardised rates showed a different trend; the male rate was 1.4 times higher than the female rate (463.0 deaths per 100,000 males compared to 332.7 per 100,000 females). This disparity is due to the differing age distributions of male and female deaths. Male mortality
1 For information on age-standardised rates see ‘Statistical notes’.
6 Mortality and Demographic Data 2012

occurred more frequently in the younger age groups compared to female mortality (see definition of age-standardised rates in ‘Statistical notes’).
Māori accounted for one in every ten deaths in 2012 (1643 males and 1421 females). The mortality rate for Māori was 1.8 times the non-Māori rate (649.3 and 362.0 deaths per 100,000 population respectively). Across all age and ethnic groups, males had higher mortality rates than females in 2012 (Table 1).
Table 1: Mortality rates, by age group, sex and ethnicity, 2012
Age-specific rate by age group (years) Age-standardised
rate<1 1–14 15–24 25–44 45–64 65–74 75+
Māori population
Male 640.3 32.3 125.2 214.7 956.2 3132.4 8936.2 743.3
Female 589.0 22.8 64.1 97.7 674.6 2728.0 7376.0 567.6
Total 615.3 27.7 95.2 152.5 807.5 2917.4 8038.3 649.3
Non-Māori population
Male 478.9 14.3 66.4 90.9 413.0 1685.3 7387.7 425.1
Female 376.8 12.3 28.2 58.8 279.7 1040.6 6842.2 305.9
Total 428.9 13.3 48.0 74.5 344.8 1353.5 7075.2 362.0
Total population
Male 523.1 18.6 81.5 111.8 466.8 1785.6 7671.7 463.0
Female 434.6 14.8 35.7 65.1 320.5 1162.7 7035.5 332.7
Total 479.8 16.7 58.9 87.4 391.6 1464.7 7306.6 393.6
Notes:
Age-specific rates are per 100,000 population in each age group.
Age-standardised rates are per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 7

The mortality rate for both males and females declined steadily between 1980 and 2012; rates halved over this time (Table 2). In 2012, the male mortality rate was 54.3% lower than in 1980, and the female rate was 47.4% lower.
Table 2: Number of deaths and mortality rates, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 14,338 1013.6 12,350 633.1 26,688 795.1
1981 13,672 935.8 11,475 564.4 25,147 726.2
1982 13,834 927.2 11,713 564.8 25,547 721.4
1983 13,986 920.0 12,021 562.9 26,007 717.2
1984 13,773 888.6 11,610 531.4 25,383 685.5
1985 14,534 922.4 12,950 575.1 27,484 725.7
1986 14,533 892.1 12,519 545.6 27,052 698.1
1987 14,472 873.4 12,958 554.3 27,430 694.5
1988 14,567 865.8 12,840 535.7 27,407 681.7
1989 14,332 836.3 12,712 522.2 27,044 661.3
1990 13,967 795.7 12,557 506.2 26,524 633.9
1991 13,810 775.6 12,680 497.3 26,490 620.3
1992 14,573 793.1 12,679 476.9 27,252 615.9
1993 14,178 755.3 13,031 480.8 27,209 601.1
1994 14,169 738.0 12,924 463.1 27,093 583.1
1995 14,528 742.3 13,428 471.4 27,956 589.6
1996 14,523 723.8 13,856 471.3 28,379 581.8
1997 14,297 680.1 13,315 433.9 27,612 542.9
1998 13,661 635.0 12,796 408.0 26,457 508.5
1999 14,348 649.3 13,876 427.5 28,224 526.0
2000 13,817 609.2 12,906 391.1 26,723 487.6
2001 14,166 606.7 13,968 402.4 28,134 493.0
2002 14,195 590.4 14,164 398.7 28,360 484.0
2003 14,066 568.6 13,995 385.8 28,061 467.7
2004 14,201 556.8 14,435 388.8 28,636 464.3
2005 13,494 514.8 13,647 357.8 27,141 429.9
2006 14,023 518.0 14,366 364.9 28,389 434.9
2007 14,333 511.8 14,268 355.3 28,601 427.2
2008 14,591 503.7 14,721 356.9 29,312 424.8
2009 14,615 488.5 14,589 346.0 29,204 412.1
2010 14,337 461.9 14,304 330.2 28,641 391.6
2011 14,941 464.4 15,348 343.2 30,289 400.4
2012 15,148 463.0 15,129 332.7 30,277 393.6
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
8 Mortality and Demographic Data 2012

From 1996 to 2012, Māori males consistently had the highest mortality rate (Figure 3). In 2012, the mortality rate for Māori males was 1.7 times the non-Māori male rate. Among females, the rate for Māori was 1.9 times the rate for non-Māori.
Between 1996 and 2012, age-standardised mortality rates for all groups decreased. Males experienced a slightly greater decrease compared to females over this time. From 2011 to 2012, Māori males were the only group to show an increase in their mortality rate.
Figure 3: Mortality rates, by sex and ethnicity, 1996–2012
Notes: rates per 100,000 population, age-standardised to WHO World Standard Population.
From 1980 to 2012 the five major causes of death were cancer, ischaemic heart disease, cerebrovascular disease, chronic lower respiratory disease and other forms of heart disease. In 2012, these five major causes accounted for two thirds (65.9%) of all deaths. Cancer accounted for 29.4% of deaths, ischaemic heart disease accounted for 17.6%, and the remaining three together accounted for 18.9% (Figure 4).
Between 1980 and 2012, mortality rates for all five major causes decreased. Specifically: ischaemic heart disease and cerebrovascular disease rates decreased by more
than two-thirds (71.0% and 68.8% respectively) rates for chronic lower respiratory diseases and other forms of heart disease
halved (declining by 53.3% and 50.0% respectively) the rate for cancer decreased by 23.6%.
Mortality and Demographic Data 2012 9

Figure 4: Mortality rates for the five major causes of mortality, 1980–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Māori had higher age-specific mortality rates than non-Māori for all five-year age groups under 85 years (Figure 5). Across each of these age groups, the mortality rate for the Māori population ranged from 1.4 to 3.2 times that of the non-Māori population. This ethnic disparity was greatest in those aged 10–14 years, where the Māori rate was more than three times that of the non-Māori rate. For those aged 85 years and over Māori and non-Māori mortality rates were comparable.
Figure 5: Age at death, rates by ethnicity, 2012
Note: rates per 100,000 population in each age group.
10 Mortality and Demographic Data 2012

The term ‘amenable mortality’ refers to potentially preventable deaths that might have been prevented if health services had been delivered more effectively or if patients had accessed services earlier (either in primary care or in hospital). Amenable mortality includes deaths from some types of infection and cancer; maternal, perinatal and infant conditions/complications; injuries; and a range of chronic disorders (see ‘Amenable mortality’ within ‘Explanatory notes’ for further information). Figure 6 shows amenable mortality rates for Māori and non-Māori by sex from 2000 to 2012.
From 2000 to 2012 New Zealand’s amenable mortality rate decreased across all groups. Over this time, the rate for Māori was between 2.4 and 2.9 times the rate for non-Māori. For both ethnic groups the amenable mortality rate was higher for males than for females.
Figure 6: Amenable mortality rates per 100,000 people aged 0–74 years, by sex and ethnicity, 2000–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population aged 0–74 years.
Mortality and Demographic Data 2012 11

Selected causes of mortalityTable 3 shows age-standardised mortality rates for selected causes of death for Māori, non-Māori and the total population in 2012.
Table 3: Mortality rates from selected causes, by sex and ethnicity, 2012
ICD code Cause of death Māori population Non-Māori population Total population
Male Female Total Male Female Total Male Female Total
C00–C96, D45–D47
Total cancer 209.5 192.5 199.4 135.9 101.1 116.5 143.4 109.0 124.0
C33–C34 Lung cancer* 65.4 66.4 65.7 23.9 15.7 19.5 27.1 19.7 23.1
C50 Breast cancer 0.0 26.5 14.5 0.0 16.9 8.9 0.0 17.7 9.4
C61 Prostate cancer 18.1 … … 16.4 … … 17.0 … …
C43 Melanoma of the skin 0.9 0.8 0.8 7.2 3.8 5.4 6.8 3.6 5.1
C53 Cervical cancer … 3.7 … … 1.6 … … 1.8 …
I00–I99 Diseases of the circulatory system
239.1 164.9 199.3 132.7 90.6 111.0 144.6 98.7 120.7
I05–I09 Chronic rheumatic heart disease
3.7 6.6 5.3 1.2 1.4 1.3 1.5 1.8 1.7
I10–I15 Hypertensive disease 11.8 10.5 11.2 3.5 3.2 3.4 4.2 3.7 4.0
I20–I25 Ischaemic heart disease 140.3 77.2 106.2 78.5 40.0 58.0 85.2 43.8 63.0
I30–I52 Other forms of heart disease§ 42.7 27.2 34.3 15.8 12.3 14.1 18.3 13.8 16.0
I60–I69 Cerebrovascular disease 30.3 31.7 31.2 25.7 28.4 27.7 27.1 29.6 29.0
J40–J47 Chronic lower respiratory diseases
52.7 53.7 53.0 21.2 16.5 18.3 23.8 19.1 20.9
J40–J44 COPD‡ 45.7 46.2 45.8 19.8 14.6 16.7 22.0 16.8 18.8
E10–E14 Diabetes mellitus 48.3 33.8 40.6 9.9 6.6 8.1 12.8 8.6 10.6
X60–X84 Suicide 25.3 10.5 17.6 16.3 5.2 10.6 18.5 6.4 12.3
V00–V99 Transport accidents 28.2 6.3 16.8 10.9 3.6 7.2 13.6 4.0 8.7
V02–V89≠ Motor vehicle accidents 22.4 6.3 14.1 9.3 3.2 6.2 11.3 3.7 7.4
F00–F09 Organic, including symptomatic, mental disorders~
8.4 10.8 10.0 10.6 12.8 12.1 11.0 13.1 12.5
J09–J18 Pneumonia and influenza 11.6 8.7 10.0 7.6 6.8 7.2 8.3 7.2 7.7
Q00–Q99 Congenital anomalies 3.5 2.6 3.0 4.9 2.8 3.9 4.5 3.0 3.7
X85–Y09 Assault 4.3 1.0 2.6 0.8 1.2 1.0 1.4 1.2 1.3
All causes of death 743.3 567.6 649.3 425.1 305.9 362.0 463.0 332.7 393.6
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.* Includes cancer of the trachea, bronchus and lung.‡ Chronic obstructive pulmonary disease.§ Includes pericardial diseases, valve disorders, myocarditis, cardiomyopathy, conduction disorders, cardiac arrest and heart
failure, but excludes chronic rheumatic heart disease.≠ Selected codes from the V02–V89 range.~ Includes dementia, amnesic syndrome, delirium and other mental disorders due to brain damage and dysfunction and to
physical disease.... = Not applicable.
The highest mortality rates in the total population in 2012 were from cancer and diseases of the circulatory system (of which ischaemic heart disease and cerebrovascular disease were the top two causes).
12 Mortality and Demographic Data 2012

The highest mortality rates in the Māori population in 2012 were from cancer and diseases of the circulatory system (of which ischaemic heart disease and chronic lower respiratory diseases were the top two causes).
Lung cancer was the leading cause of cancer death for Māori males, non-Māori males and Māori females in 2012; breast cancer was the leading cause of cancer death for non-Māori females.
Sex-based differences in mortalityTable 3 shows that mortality rates for males were generally higher than for females in 2012. For example, males had a mortality rate: for all causes that was 1.4 times the rate for females from transport accidents that was more than three times the female rate from suicide that was nearly three times the female rate from ischaemic heart disease and melanoma that was nearly twice the female
rate from diabetes, congenital anomalies and lung cancer that was almost 1.5 times
the female rate.
Female mortality rates were higher than the equivalent male rates for cerebrovascular disease; organic, including symptomatic, mental disorders; and chronic rheumatic heart disease.
Ethnicity-based differences in mortalityIn 2012, Māori had a total mortality rate that was 1.8 times the rate for non-Māori (the age-standardised rates were 649.3 and 362.0 respectively).
Māori had higher mortality rates than non-Māori for most of the causes shown in Table 3, except for melanoma and congenital anomalies.
In 2012, the two largest differences between mortality rates for Māori and non-Māori were for: diabetes mellitus, where the rate for Māori was five times that for non-Māori
(the age-standardised rates were 40.6 and 8.1 respectively) chronic rheumatic heart disease, where the rate for Māori was four times that
for non-Māori (the age-standardised rates were 5.3 and 1.3 respectively).
In addition, Māori had mortality rates for lung cancer and hypertensive diseases that were more than three times the equivalent non-Māori rate. Māori rates for chronic lower respiratory diseases (including chronic obstructive pulmonary disease), assault, transport accidents, cervical cancer and other forms of heart disease were at least twice the equivalent non-Māori rates.
Note that the percentages and rates discussed here present a snapshot from 2012. Mortality rates for Māori tend to vary more widely than those for non-Māori, due to the lower number of deaths they are based on. It is useful, whenever possible, to examine the pattern of their incidence over several years. This helps to determine
Mortality and Demographic Data 2012 13

whether the mortality figures for a particular year and condition are a statistical spike or representative of the general trend.
Selected causes of death, broken down by sex and ethnicity, are discussed further in ‘Selected trends’.
Mortality by regionThis section presents mortality data by district health board (DHB) region of residence by age-standardised rate. Note that the populations used in this section are different to the populations used in the remainder of the publication. This means that some results in this section differ very slightly from those given in other sections (see ‘Population’ within ‘Explanatory notes’).
Total populationFigure 7 presents the mortality rate and the 99% confidence intervals for each DHB region for 2012. Four DHB regions had mortality rates that were significantly lower than the national rate: Waitemata, Nelson Marlborough, Auckland and Capital & Coast. Five had mortality rates that were significantly higher than the national rate: Tairāwhiti, Whanganui, Lakes, Northland and South Canterbury. The remaining DHB regions had rates with 99% confidence limits that overlapped with the New Zealand mortality rate, meaning they were not significantly different from the national rate (see ‘Confidence intervals’ within ‘Explanatory notes’).
Figure 7: Mortality rates, by DHB region, total population, 2012
Notes:
14 Mortality and Demographic Data 2012

The dashed vertical line is the national rate.
Rates per 100,000 population, age-standardised to WHO World Standard Population; 99% confidence intervals.
Māori and non-Māori mortality by DHB regionFigure 8 shows mortality rates by DHB region of residence for Māori in 2012 compared with the national mortality rate for Māori.
All five DHBs in the South Island (South Canterbury, West Coast, Nelson Marlborough, Southern and Canterbury) had a mortality rate for Māori that was significantly lower than the national rate. No DHB had a rate that was significantly higher than the national rate. South Canterbury DHB had the lowest Māori mortality rate (249.7 deaths per 100,000). Whanganui and Wairarapa DHBs had the highest Māori mortality rates (827.0 and 822.1 deaths per 100,000 respectively).
The rates for some DHBs have very wide confidence intervals, due to low mortality numbers (eg, South Canterbury (7) and West Coast (10)). Rates for these DHBs should be interpreted with caution.
Figure 8: Mortality rates, by DHB region, Māori population, 2012
Notes:
The dashed vertical line is the national rate for Māori.
Rates per 100,000 Māori population, age-standardised to WHO World Standard Population; 99% confidence intervals.
Mortality and Demographic Data 2012 15

Figure 9 shows mortality rates by DHB region for non-Māori in 2012 compared with the rate for all non-Māori.
Six DHB regions had a mortality rate for non-Māori that was significantly different from the national rate; three were higher (South Canterbury, Whanganui and Southern) and three were lower (Waitemata, Bay of Plenty and Auckland).
The DHB regions with the highest mortality rates for the non-Māori population were South Canterbury (446.6 deaths per 100,000), Whanganui (433.4 per 100,000) and Tairāwhiti (433.0 per 100,000). The DHB region with the lowest non-Māori mortality rate was Waitemata (316.1 per 100,000).
Figure 9: Mortality rates, by DHB region, non-Māori population, 2012
Notes:
The dashed vertical line is the national rate for non-Māori.
Rates per 100,000 non-Māori population, age-standardised to WHO World Standard Population; 99% confidence intervals.
16 Mortality and Demographic Data 2012

Figure 10 combines the same information as Figures 8 and 9 in map form. The different shades shown on the maps distinguish ranges in DHB rates, lighter shades represent lower rates and darker shades represent higher rates. Mortality rates for Māori were generally higher than the corresponding rates for non-Māori, particularly in the North Island.
Some factors that influence regional mortality rates have not been adjusted for in the data presented. They include: demographic factors (such as sex, ethnicity, deprivation and socioeconomic
status) geographic factors (such as the average distance travelled to access health
services) population risk factors (such as smoking rates, obesity rates, diabetes rates, mix
of occupations and occupational mortality rates, and population health literacy).
For example, different regions have different proportions of Māori in their populations, and Māori exhibit higher rates of mortality. Similarly, smoking and obesity rates are known to be higher among people living in more deprived areas (Ministry of Health 2012), and some DHBs have a relatively higher proportion of such areas. This data cannot be used to assess the quality of care being provided by DHBs to their populations.
Mortality and Demographic Data 2012 17

Figure 10: Comparison of DHB region mortality rates for Māori and non-Māori, 2012
Southern
Waikato
Canterbury
West Coast
Lakes
Northland
Nelson Marlborough
Taranaki
Tairāwhiti
Whanganui
MidCentral
Hawke's Bay
South Canterbury
Bay of Plenty
Wairarapa
Waitemata
Counties Manukau
Hutt Valley
Capital & Coast
Auckland
Māori mortality rate<350
350–449
450–549
550–649
≥650
Māori
18 Mortality and Demographic Data 2012

Southern
Waikato
Canterbury
West Coast
Lakes
Northland
Nelson Marlborough
Taranaki
Tairāwhiti
Whanganui
MidCentral
Hawke's Bay
South Canterbury
Bay of Plenty
Wairarapa
Waitemata
Counties Manukau
Hutt Valley
Capital & Coast
Auckland
Non-Māorimortality rate
<350
350–449
450–549
550–649
≥650
Non-Māori
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 19

20 Mortality and Demographic Data 2012

Selected trendsThis section examines mortality statistics for several conditions in greater depth. These analyses, while addressing the most salient conditions, are not intended to be a definitive account of the mortality and health issues facing the New Zealand population.
Conditions covered in this section are: all cancers (malignant neoplasm) lung cancer (malignant neoplasm of the trachea, bronchus and lung) female breast cancer (malignant neoplasm of the female breast) prostate cancer (malignant neoplasm of the prostate) melanoma of the skin (malignant melanoma of the skin) cervical cancer (malignant neoplasm of the cervix uteri) ischaemic heart disease (angina pectoris, myocardial infarction and other forms
of acute and chronic ischaemic heart disease) cerebrovascular disease (cerebral haemorrhage (subarachnoid, intracerebral
and other non-traumatic), cerebral infarction, occlusion and stenosis of precerebral and cerebral arteries and other cerebrovascular diseases)
diabetes mellitus, Type 1 (insulin dependent) and Type 2 (adult onset diabetes) motor vehicle accidents (accidents associated with motorised land transport) suicide (intentional self-harm) maternal mortality (direct and indirect obstetric deaths).
Mortality and Demographic Data 2012 21

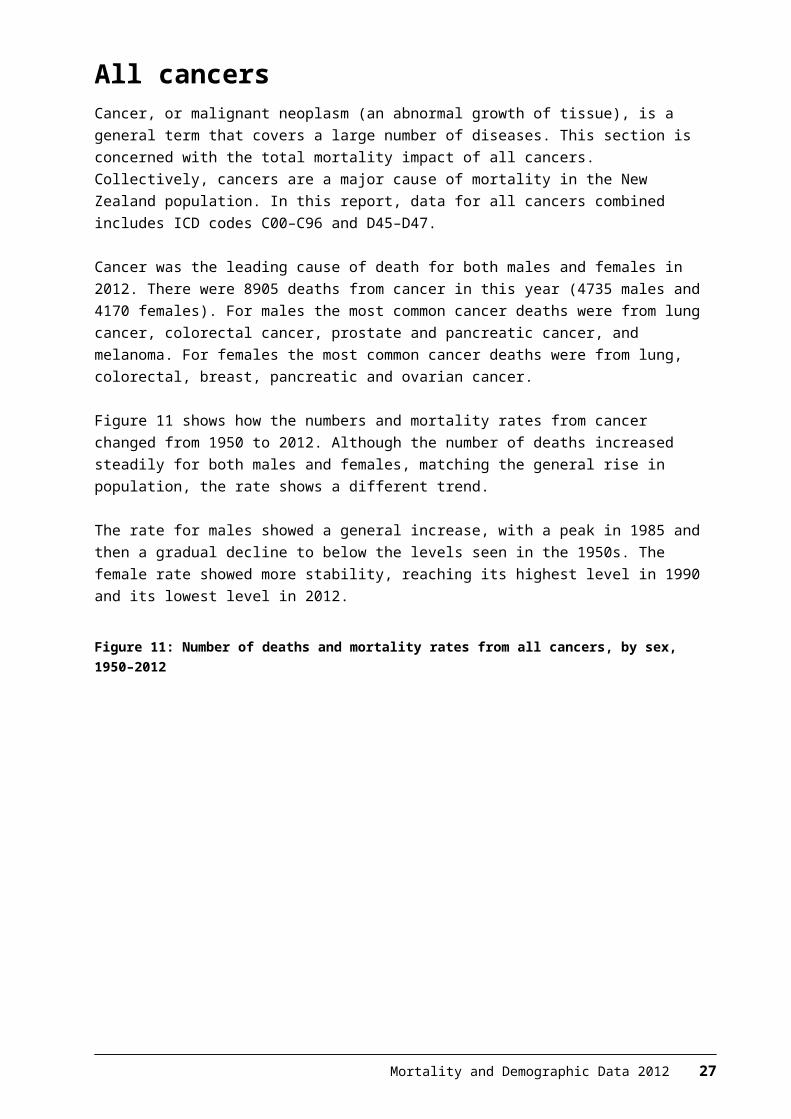
All cancersCancer, or malignant neoplasm (an abnormal growth of tissue), is a general term that covers a large number of diseases. This section is concerned with the total mortality impact of all cancers. Collectively, cancers are a major cause of mortality in the New Zealand population. In this report, data for all cancers combined includes ICD codes C00–C96 and D45–D47.
Cancer was the leading cause of death for both males and females in 2012. There were 8905 deaths from cancer in this year (4735 males and 4170 females). For males the most common cancer deaths were from lung cancer, colorectal cancer, prostate and pancreatic cancer, and melanoma. For females the most common cancer deaths were from lung, colorectal, breast, pancreatic and ovarian cancer.
Figure 11 shows how the numbers and mortality rates from cancer changed from 1950 to 2012. Although the number of deaths increased steadily for both males and females, matching the general rise in population, the rate shows a different trend.
The rate for males showed a general increase, with a peak in 1985 and then a gradual decline to below the levels seen in the 1950s. The female rate showed more stability, reaching its highest level in 1990 and its lowest level in 2012.
Figure 11: Number of deaths and mortality rates from all cancers, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
In 2012 the cancer mortality rate for males was 1.3 times the female rate. Males consistently had a higher mortality rate than females from 1980 to 2012 (Table 4). Mortality rates generally declined over this time; the rate for males in 2012 was
22 Mortality and Demographic Data 2012

27.7% lower than the equivalent rate in 1980, and the female rate was 21.3% lower.
Table 4: Number of deaths and mortality rates from all cancers, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 2952 198.4 2513 138.5 5465 162.3
1981 3061 202.6 2527 134.6 5588 162.2
1982 3076 199.3 2647 138.7 5723 162.6
1983 3166 200.4 2771 142.3 5937 165.7
1984 3237 202.7 2651 133.1 5888 160.8
1985 3318 204.5 2849 140.2 6167 165.6
1986 3364 200.9 2857 137.2 6221 163.1
1987 3375 198.5 3035 144.3 6410 165.8
1988 3444 200.6 3037 141.5 6481 165.2
1989 3492 199.6 3139 145.6 6631 166.9
1990 3548 199.0 3198 145.7 6746 166.2
1991 3541 195.1 3251 145.4 6792 165.2
1992 3771 201.7 3110 133.8 6881 161.5
1993 3812 199.8 3282 138.6 7094 163.4
1994 3834 196.3 3332 137.6 7166 161.3
1995 3918 196.9 3504 143.8 7422 164.5
1996 3872 189.3 3589 142.1 7461 160.8
1997 3834 179.6 3448 130.7 7282 150.6
1998 3911 178.5 3671 134.9 7582 152.4
1999 4063 181.3 3611 130.7 7674 151.4
2000 4120 178.1 3500 123.2 7620 146.1
2001 4166 175.7 3644 124.6 7810 145.5
2002 4125 168.9 3675 120.9 7800 140.7
2003 4292 170.1 3735 121.7 8027 141.8
2004 4246 164.1 3899 124.1 8145 140.7
2005 4184 156.6 3787 116.9 7971 133.6
2006 4144 151.3 3950 118.5 8094 132.4
2007 4539 159.4 3980 117.3 8519 135.1
2008 4561 154.9 4005 115.3 8566 132.3
2009 4402 145.4 4035 112.6 8437 126.8
2010 4511 143.9 4082 110.6 8593 125.2
2011 4650 143.3 4241 112.6 8891 125.9
2012 4735 143.4 4170 109.0 8905 124.0
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 23

In 2012, the mortality rate from all cancers for Māori was 199.4 deaths per 100,000 Māori. For non-Māori the mortality rate was 116.5 deaths per 100,000 non-Māori.
The distribution of cancer-related deaths was skewed toward the 65 years and over age group. However, a large proportion of cancer-related deaths also occurred in the 45–64 years age band. Cancer deaths were relatively rare in people aged under 45 years (Table 5).
Table 5: Age distribution of deaths from all cancers, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific mortality rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
<25 2.0 1.6 1.8 0.5 0.5 0.5 4.9 4.5 4.7 3.3 3.0 3.2
25–44 5.2 5.1 5.1 2.0 3.8 2.8 29.2 28.1 28.6 17.2 27.4 22.5
45–64 36.1 42.8 39.6 19.7 22.6 21.0 282.1 335.7 310.4 173.3 161.9 167.5
65+ 56.7 50.5 53.4 77.9 73.1 75.7 1597.4 1349.2 1462.0 1261.3 861.3 1045.1
Note: rates per 100,000 population.
Compared with non-Māori, a greater proportion of Māori deaths occurred in the youngest three age groups (almost half of Māori cancer deaths occurred in those aged less than 65; for non-Māori this figure was 24.3%).
24 Mortality and Demographic Data 2012

Between 1996 and 2012, the Māori population had a consistently higher rate of cancer deaths than the non-Māori population. Māori males had a higher rate than Māori females in every year except 2008 (Figure 12).
There was a significant difference in cancer mortality rates between non-Māori males and non-Māori females between 1996 and 2012 (using 95% confidence intervals).2 The difference between the rates for Māori males and Māori females was not significant in 2012.
In 2012, the rate of cancer deaths for Māori males was 1.5 times that for non-Māori males. The rate for Māori females was 1.9 times that for non-Māori females.
Figure 12: Mortality rates from all cancers, by sex and ethnicity, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
2 Confidence intervals were calculated for all rates, although they are not shown in Figure 12. For more information on confidence intervals, see ‘Statistical notes’.
Mortality and Demographic Data 2012 25

Figure 13 shows cancer mortality rates by DHB region for the total population in 2012. One DHB (Southern) showed a rate that was significantly above the national rate; two DHBs had rates that were significantly lower (Auckland and Waitemata). All other DHBs had rates that were not significantly different to the New Zealand rate.
Figure 13: Mortality rates from all cancers, by DHB region, total population, 2012
Notes:
The dashed vertical line is the national rate.
Rates per 100,000 population, age-standardised to WHO World Standard Population; 99% confidence intervals.
26 Mortality and Demographic Data 2012
Lung cancerThis section covers ICD codes C33 and C34 (C33: malignant neoplasm of trachea; C34: malignant neoplasm of bronchus and lung). In this publication, these conditions are collectively referred to as lung cancer.
Lung cancer was the leading cause of cancer death in 2012, accounting for 18.3% of cancer deaths (1628 deaths). The majority of those who died from lung cancer were males (54.7%). In 2012, the mortality rate for males was higher than the female rate (27.1 deaths per 100,000 males compared to 19.7 deaths per 100,000 females).
Figure 14 shows trends in numbers and rates of death from lung cancer for both males and females from 1950 to 2012. Mortality rates for males peaked in the mid-1980s and then showed a strong downward trend. Female rates showed a general upward trend from 1950 before stabilising in the 1990s.
Figure 14: Number of deaths mortality rates from lung cancer, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 27

Table 6 shows deaths from lung cancer from 1980 to 2012. The mortality rate for males declined by more than half over this time (51.9%), while the rate for females showed the opposite trend, increasing by 36.2%. The number of male deaths in 2012 was comparable to the number of male deaths in 1980. For females, the number of deaths in 2012 was almost three times the number of deaths in 1980.
Table 6: Number of deaths and mortality rates from lung cancer, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 868 56.4 265 14.5 1133 32.8
1981 889 57.3 298 15.8 1187 33.8
1982 844 53.4 298 15.4 1142 31.7
1983 948 58.3 291 15.0 1239 34.0
1984 975 59.4 307 15.2 1282 34.4
1985 866 52.6 331 16.6 1197 31.9
1986 949 55.5 329 15.9 1278 33.1
1987 950 54.7 396 18.9 1346 34.5
1988 892 51.2 395 18.4 1287 32.7
1989 896 50.5 411 19.7 1307 32.9
1990 903 50.0 433 20.2 1336 33.0
1991 869 47.1 427 19.8 1296 31.6
1992 947 50.0 445 19.5 1392 32.5
1993 892 46.1 444 19.4 1336 30.9
1994 919 46.3 484 20.7 1403 31.7
1995 892 44.3 514 21.6 1406 31.5
1996 904 43.8 502 20.2 1406 30.5
1997 882 40.8 530 21.2 1412 29.6
1998 855 38.8 526 20.2 1381 28.1
1999 874 38.6 569 21.4 1443 28.8
2000 860 37.0 546 19.7 1406 27.3
2001 841 35.1 594 21.4 1435 27.3
2002 866 35.1 605 20.7 1471 26.9
2003 848 33.4 618 21.6 1466 26.6
2004 929 35.9 626 21.5 1555 27.8
2005 864 32.3 587 19.2 1451 25.0
2006 798 29.2 659 21.2 1457 24.7
2007 864 30.3 664 20.4 1528 24.7
2008 889 30.1 745 22.6 1634 25.7
2009 876 28.8 717 21.0 1593 24.4
2010 893 28.7 757 21.2 1650 24.6
2011 909 28.0 773 21.2 1682 24.2
2012 891 27.1 737 19.7 1628 23.1
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
28 Mortality and Demographic Data 2012

The great majority of lung cancer deaths occurred in those aged 45 years and over (Table 7). Among Māori, a greater percentage of deaths occurred in those aged 45–64 years (the percentage for this age group was almost twice that of the equivalent non-Māori percentage), and the Māori age-specific rate was 3.6 times that of non-Māori. In the 65 years and over age group, the Māori rate was three times that of non-Māori.
Table 7: Age distribution of deaths from lung cancer, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
<25 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
25–44 2.9 1.8 2.3 1.1 1.4 1.2 5.1 3.4 4.2 1.6 1.6 1.6
45–64 35.7 41.7 39.0 21.8 20.7 21.4 88.7 110.8 100.4 33.6 23.1 28.2
65+ 61.4 56.5 58.8 77.1 77.9 77.4 549.5 512.7 529.2 218.5 142.0 177.1
Note: rates per 100,000 population.
In 2012, the mortality rate from lung cancer for Māori was 65.7 deaths per 100,000. The mortality rate for non-Māori was 19.5 deaths per 100,000.
The mortality rate from lung cancer in Māori males was 2.7 times that for non-Māori males in 2012 (Figure 15). The rate for Māori females was more than four times that for non-Māori females.
Between 1996 and 2012, mortality rates for Māori males and females from lung cancer were higher than the equivalent non-Māori rates. During this period, the mortality rate for Māori males from lung cancer decreased by 38.5%, while the Māori female rate showed no obvious trend.
Figure 15: Mortality rates from lung cancer, by sex and ethnicity, 1996–2012
Mortality and Demographic Data 2012 29

Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Female breast cancerBreast cancer was the third leading cause of cancer death among females in 2012 after lung and colorectal cancer.3 National breast screening commenced at the end of 1998 for women aged 50–69 years; from July 2008 the minimum screening age was lowered to 45.4
This section covers ICD code C50 (malignant neoplasm of breast).
A total of 617 females died from breast cancer in 2012; this accounted for 14.8% of female deaths from cancer.
Although the number of deaths due to breast cancer increased between 1950 and 2012, when adjusted for age and the change in population, the rate showed a general downward trend after the mid-1980s (Figure 16). The mortality rate for 2012 (17.7 deaths per 100,000 females) was the lowest over the entire period.
Figure 16: Number of deaths and mortality rates from breast cancer in females, 1950–2012
Note: rates per 100,000 female population, age-standardised to WHO World Standard Population.
3 This section discusses cancer of the female breast; breast cancer can occur in males but is rare (there was one male death in 2012).
4 For further information on the BreastScreen Aotearoa programme, see the National Screening Unit’s website: www.nsu.govt.nz
30 Mortality and Demographic Data 2012

From 1980 to 2012 the number of female deaths increased, reaching a peak in 1996 before stabilising. Over this time the mortality rate for females from breast cancer decreased by 40.1% (Table 8).
Table 8: Number of deaths and mortality rates from breast cancer in females, 1980–2012
Year No. Rate
1980 509 29.5
1981 478 27.3
1982 524 29.4
1983 537 29.8
1984 504 26.8
1985 565 29.5
1986 529 27.6
1987 607 31.5
1988 593 30.0
1989 605 30.0
1990 635 31.2
1991 588 28.6
1992 569 26.6
1993 584 26.6
1994 567 25.5
1995 638 28.4
1996 681 28.6
1997 620 25.8
1998 629 25.2
1999 647 25.3
2000 622 23.6
2001 615 22.7
2002 625 22.4
2003 647 23.1
2004 642 22.4
2005 648 21.7
2006 614 20.3
2007 643 20.8
2008 618 19.1
2009 658 19.9
2010 641 19.1
2011 636 18.3
2012 617 17.7
Note: rates per 100,000 female population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 31

For Māori, the highest proportion of deaths from breast cancer was in women aged 45–64 years; this age group accounted for 60.3% of Māori deaths from breast cancer. For non-Māori women, the highest proportion was in women aged 65 and over; accounting for 57.2% of non-Māori breast cancer deaths (Table 9).
Table 9: Age distribution of deaths from breast cancer in females, percentages and rates, by ethnicity, 2012
Age group (years)
Percentage Age-specific rate
Māori female Non-Māori female Māori female Non-Māori female
<25 0.0 0.0 0.0 0.0
25–44 9.6 7.9 7.9 8.4
45–64 60.3 34.9 69.7 37.1
65+ 30.1 57.2 118.7 99.7
Note: rates per 100,000 population.
In 2012, Māori females had a breast cancer mortality rate that was 1.6 times the non-Māori rate (Figure 17). There were 26.5 deaths per 100,000 Māori females, compared to 16.9 deaths per 100,000 non-Māori females.
For most years from 1996 to 2012, Māori rates were significantly higher than non-Māori rates (using 95% confidence intervals).5 The Māori mortality rate for breast cancer shows greater variability than that of non-Māori. This may be partially explained by the lower number of Māori deaths (73 in 2012). There was no significant change in breast cancer death rates among Māori between 1996 and 2012. For non-Māori females, the mortality rate for 2012 was significantly lower than the 1996 rate.
Figure 17: Mortality rates from breast cancer in females, by ethnicity, 1996–2012
5 Confidence intervals were calculated for all rates, although they are not shown in Figure 17. For more information on confidence intervals, see “Confidence intervals’ within ‘Statistical notes’.
32 Mortality and Demographic Data 2012

Note: rates per 100,000 female population, age-standardised to WHO World Standard Population.
Prostate cancerProstate cancer was the most common cancer registered for males in 2012,6 and was also the third leading cause of male cancer death. This section covers ICD code C61 (malignant neoplasm of prostate).
There were 607 deaths from prostate cancer in 2012 (an age-standardised rate of 17.0 deaths per 100,000 male population), accounting for 12.8% of total male cancer deaths.
Between 1950 and 2012 mortality rates from prostate cancer showed an overall increase until a peak in 1995 (Figure 18). Thereafter, rates showed a downward trend. The 2012 rate was similar to rates in the 1950s. Over that time, the number of deaths from prostate cancer steadily increased to a reach a peak in 2008 before stabilising.
Figure 18: Number of deaths and mortality rates from prostate cancer, 1950–2012
Note: rates per 100,000 male population, age-standardised to WHO World Standard Population.
6 See the publication series Cancer: New Registrations and Deaths atwww.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/cancer-new-registrations-and-deaths-series
Mortality and Demographic Data 2012 33

Table 10 shows numbers and mortality rates for prostate cancer deaths between 1980 and 2012. Over this time the mortality rate declined by 24.4%.
Table 10: Number of deaths and mortality rates from prostate cancer, 1980–2012
Year No. Rate
1980 311 22.4
1981 293 20.2
1982 289 20.3
1983 325 21.8
1984 335 21.5
1985 351 22.5
1986 360 22.1
1987 365 21.5
1988 402 23.7
1989 425 24.5
1990 436 24.5
1991 423 23.1
1992 478 25.5
1993 520 26.9
1994 517 25.8
1995 554 27.3
1996 502 24.0
1997 525 24.3
1998 524 23.3
1999 552 23.8
2000 594 24.9
2001 592 24.1
2002 591 23.3
2003 556 21.0
2004 583 21.5
2005 564 19.9
2006 559 19.4
2007 574 19.0
2008 670 21.5
2009 562 17.3
2010 589 17.4
2011 585 16.5
2012 607 17.0
Note: rates per 100,000 male population, age-standardised to WHO World Standard Population.
34 Mortality and Demographic Data 2012

Prostate cancer mortality in 2012 primarily occurred in the 65 and over age group, for both Māori and non-Māori (Table 11). The distribution of deaths for this particular cancer was more skewed toward the older age group than it was for cancer deaths as a whole.
Table 11: Age distribution of deaths from prostate cancer in males, percentages and rates, by ethnicity, 2012
Age group (years)
Percentage Age-specific rate
Māori male Non-Māori male Māori male Non-Māori male
<25 0.0 0.0 0.0 0.0
25–44 0.0 0.0 0.0 0.0
45–64 15.6 6.8 8.9 8.0
65+ 84.4 93.2 172.5 202.2
Note: rates per 100,000 male population.
In 2012 the mortality rate for Māori from prostate cancer was marginally higher (10.6% higher) than the rate for non-Māori (Figure 19). There were 18.1 deaths per 100,000 Māori males, compared to 16.4 deaths per 100,000 non-Māori males.
Between 1996 and 2012, the mortality rate for Māori was highly variable; the 1996 rate was not significantly different to the 2012 rate (using 95% confidence intervals).7 Over this time period there was an overall decrease in the mortality rate for prostate cancer in non-Māori; the 2012 rate was significantly lower than the 1996 rate.
Figure 19: Mortality rates from prostate cancer, by ethnicity, 1996–2012
Note: rates per 100,000 male population, age-standardised to WHO World Standard Population.
7 Confidence intervals were calculated for all rates, although they are not shown in Figure 19. For more information on confidence intervals, see ‘Confidence intervals’ within ‘Statistical notes’.
Mortality and Demographic Data 2012 35

Malignant melanoma of the skinThis section covers ICD code C43 (malignant melanoma of skin). Malignant melanoma of the skin was the fifth leading cause of cancer deaths for males and the seventh leading cause for females in 2012.
There were 354 deaths from malignant melanoma of the skin in 2012, representing 4.0% of total cancer deaths. Almost two-thirds of those who died from this condition (62.7%) were males.
Melanoma mortality rates increased for both males and females from 1950 to the late 1970s. From then on, male rates continued to increase, while female rates remained fairly stable, ranging from 2.8 to 4.0 deaths per 100,000. In 2012 the rate for males was almost twice the female rate (Figure 20).
Figure 20: Number of deaths and mortality rates from malignant melanoma of the skin, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
36 Mortality and Demographic Data 2012

From 1980 to 2012 the mortality rate from melanoma increased by 34.7% for males and 21.7% for females (Table 12). The number of male deaths from melanoma in 2012 was three times the number of deaths in 1980. For females, the number of deaths in 2012 was 2.6 times the number of deaths in 1980.
Table 12: Number of deaths and mortality rates from malignant melanoma of the skin, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 74 5.1 50 2.9 124 3.9
1981 74 5.0 47 2.8 121 3.8
1982 84 5.5 57 3.4 141 4.3
1983 80 4.9 54 3.1 134 4.0
1984 90 5.6 71 4.0 161 4.7
1985 100 6.3 60 3.2 160 4.6
1986 88 5.3 71 3.6 159 4.4
1987 83 5.0 67 3.5 150 4.2
1988 101 5.8 69 3.4 170 4.5
1989 95 5.5 71 3.5 166 4.4
1990 115 6.5 73 3.4 188 4.9
1991 109 6.2 71 3.4 180 4.7
1992 99 5.5 83 3.8 182 4.5
1993 112 6.0 82 3.5 194 4.6
1994 114 6.0 79 3.4 193 4.6
1995 126 6.5 71 3.2 197 4.6
1996 107 5.3 87 3.7 194 4.4
1997 121 5.8 80 3.2 201 4.3
1998 143 6.6 105 4.0 248 5.2
1999 146 6.7 85 3.3 231 4.8
2000 155 7.0 98 3.7 253 5.2
2001 156 6.7 88 3.1 244 4.7
2002 149 6.3 86 3.1 235 4.6
2003 174 7.1 111 3.6 285 5.2
2004 152 6.1 97 3.0 249 4.4
2005 156 6.1 113 3.7 269 4.8
2006 173 6.4 114 3.4 287 4.7
2007 178 6.4 114 3.4 292 4.8
2008 202 7.2 115 3.2 317 5.1
2009 213 7.2 113 3.3 326 5.1
2010 199 6.5 125 3.5 324 4.9
2011 243 7.8 116 3.2 359 5.3
2012 222 6.8 132 3.6 354 5.1
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 37

Melanoma is uncommon among Māori. In 2012 there were three Māori deaths from melanoma of the skin, or 0.8 deaths per 100,000 Māori. Non-Māori had a mortality rate of 5.4 deaths per 100,000 in the same year.
Table 13: Age distribution of deaths from malignant melanoma of the skin, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
<25 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
25–44 0.0 0.0 0.0 2.3 9.2 4.8 0.0 0.0 0.0 1.0 2.3 1.7
45–64 0.0 50.0 33.3 23.1 28.5 25.1 0.0 1.6 0.8 10.4 7.2 8.8
65+ 100.0 50.0 66.7 74.7 62.3 70.1 6.4 5.4 5.8 62.3 26.0 42.6
Note: rates per 100,000 population.
38 Mortality and Demographic Data 2012

Cervical cancerThis section covers ICD code C53 (malignant neoplasm of cervix uteri). There were 56 deaths from cervical cancer in 2012, accounting for 1.3% of total female cancer deaths.
From 1950 to 2012, the mortality rate from cervical cancer declined by almost 80% from 8.1 to 1.8 deaths per 100,000 females (Figure 21).
Figure 21: Number of deaths and mortality rates from cervical cancer, 1950–2012
Note: rates per 100,000 female population, age-standardised to WHO World Standard Population
Mortality and Demographic Data 2012 39

Between 1980 and 2012, the number of women dying from cervical cancer decreased by 40.4% (Table 14). One factor in this decrease seen may have been the establishment of the National Cervical Screening Programme in 1991.8
Table 14: Number of deaths and mortality rates from cervical cancer, 1980–2012
Year No. Rate
1980 94 5.8
1981 95 5.5
1982 110 6.4
1983 90 5.3
1984 98 5.8
1985 97 5.5
1986 89 4.8
1987 117 6.3
1988 99 5.3
1989 85 4.6
1990 101 5.5
1991 106 5.3
1992 84 4.1
1993 80 3.8
1994 77 3.7
1995 96 4.6
1996 82 3.8
1997 73 3.2
1998 77 3.2
1999 71 3.0
2000 66 2.7
2001 63 2.4
2002 65 2.4
2003 58 2.1
2004 71 2.7
2005 54 1.9
2006 52 1.7
2007 65 2.2
2008 59 1.9
2009 44 1.4
2010 52 1.7
2011 53 1.7
2012 56 1.8
Note: rates per 100,000 female population, age-standardised to WHO World Standard Population.
8 For further information on the National Cervical Screening Programme, see the National Screening Unit‘s website: www.nsu.govt.nz
40 Mortality and Demographic Data 2012

In 2012, the majority (90.9%) of Māori deaths from cervical cancer were females under 65 years (Table 15). The corresponding proportion for non-Māori was 55.6%.
Table 15: Age distribution of deaths from cervical cancer, percentages and rates, by ethnicity, 2012
Age group (years)
Percentage Age-specific rate
Māori female Non-Māori female Māori female Non-Māori female
<25 0.0 0.0 0.0 0.0
25–44 27.3 17.8 3.4 1.6
45–64 63.6 37.8 11.1 3.3
65+ 9.1 44.4 5.4 6.4
Note: rates per 100,000 female population.
Māori accounted for one-fifth (19.6%) of cervical cancer deaths in 2012. The mortality rate for Māori was 2.4 times the non-Māori rate: there were 3.7 deaths per 100,000 Māori females compared with 1.6 deaths per 100,000 non-Māori females.
There was a significant decrease in cervical cancer mortality rates for both Māori and non-Māori women between 1996 and 2012. The mortality rate for Māori decreased by 71.4% over this time, while the rate for non-Māori decreased by 46.0% (Figure 22). Note that the Māori numbers were low (eg, only 11 deaths in 2012).
Figure 22: Mortality rates from cervical cancer, by ethnicity, 1996–2012
Note: rates per 100,000 female population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 41

Ischaemic heart diseaseIschaemic (or coronary) heart disease is a condition in which fatty deposits accumulate in the cells lining the wall of the coronary arteries – a process called atherosclerosis. The progressive narrowing and hardening of the arteries over time results in an inability to provide adequate oxygen to the heart muscle (called ischaemia). This can cause damage to the heart muscle or, in more severe cases, lead to myocardial infarction (a heart attack). This section covers ICD codes I20–I25.
Ischaemic heart disease was the second leading cause of death after cancer in 2012, accounting for 5339 deaths (17.6% of all deaths). Males accounted for 55.3% of these deaths.
Mortality rates from ischaemic heart disease for males and females in 2012 were the lowest they have been since 1950 (Figure 23). From 1950, males consistently had a higher mortality rate than females, although this gap became less marked after its peak in the late 1960s and early 1970s.
Figure 23: Number of deaths and mortality rates from ischaemic heart disease, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
42 Mortality and Demographic Data 2012

From 1980 to 2012 the mortality rate from ischaemic heart disease declined by 71.0% (Table 16). The male mortality rate was consistently higher than the female rate over this time: it was approximately twice the equivalent female rate for most of the period. In 2012 the male rate was 1.9 times the female rate.
Table 16: Number of deaths and mortality rates from ischaemic heart disease, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 4413 304.4 3046 149.2 7459 217.4
1981 4259 285.3 2883 134.7 7142 201.6
1982 4362 285.0 2939 133.6 7301 200.9
1983 4241 274.8 2904 128.3 7145 192.6
1984 4245 268.2 2951 127.5 7196 189.6
1985 4234 262.9 3106 128.8 7340 188.8
1986 4346 263.4 3109 126.6 7455 187.4
1987 4379 260.1 3235 128.7 7614 187.8
1988 4173 243.4 3079 118.8 7252 174.9
1989 4071 233.4 2964 111.9 7035 166.3
1990 3884 217.5 2923 108.4 6807 157.3
1991 3789 208.6 2954 105.8 6743 151.7
1992 4064 217.3 3034 104.0 7098 155.1
1993 3842 201.0 3056 102.7 6898 146.7
1994 3718 190.5 2901 94.9 6619 137.2
1995 3810 191.2 2887 90.8 6697 135.9
1996 3729 182.0 2904 87.8 6633 130.1
1997 3614 168.0 2755 79.9 6369 119.4
1998 3479 158.1 2724 75.3 6203 112.3
1999 3646 160.9 2925 79.2 6571 115.6
2000 3269 140.3 2704 71.2 5973 102.2
2001 3389 140.2 2982 75.2 6371 104.1
2002 3333 134.2 2954 71.4 6287 99.8
2003 3243 126.7 2953 68.4 6196 94.9
2004 3366 127.6 2947 67.0 6313 94.4
2005 3057 111.8 2750 60.5 5807 83.9
2006 3133 110.9 2779 58.6 5912 82.5
2007 3015 103.4 2619 54.4 5634 77.2
2008 2960 97.4 2594 51.9 5554 72.9
2009 3039 96.6 2514 48.6 5553 70.7
2010 2900 88.0 2489 47.5 5389 66.3
2011 2934 85.9 2600 47.3 5534 65.4
2012 2952 85.2 2387 43.8 5339 63.0
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 43

In 2012, the mortality rate from ischaemic heart disease for Māori was 106.2 deaths per 100,000. The rate for non-Māori was 58.0 deaths per 100,000.
In 2012, the majority of ischaemic heart disease deaths occurred in the 65 years and over age group (which accounted for 81.3% of male deaths and 93.9% of female deaths from this condition). Māori deaths from ischaemic heart disease tended to occur at a younger age than non-Māori: 40.2% of Māori deaths from this condition occurred in those aged under 65 years, compared to 10.5% of non-Māori deaths (Table 17).
Table 17: Age distribution of deaths from ischaemic heart disease, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
<25 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.2 0.1
25–44 4.2 1.7 3.2 1.2 0.5 0.9 15.2 3.4 8.9 6.8 2.1 4.4
45–64 41.1 30.3 37.0 14.6 3.4 9.5 209.3 85.5 143.9 79.6 14.8 46.5
65+ 54.7 68.0 59.8 84.2 96.0 89.5 1003.2 653.0 812.9 846.3 679.7 756.2
Note: rates per 100,000 population.
Of the four groups represented in Figure 24, the Māori male population had the highest rate of ischaemic heart disease deaths in 2012. This rate was 1.8 times the rate for non-Māori males. The rate for Māori females was 1.9 times the rate for non-Māori females.
Between 1996 and 2012, the rate for Māori males was consistently higher than rates for all other groups shown in Figure 24. The rate for Māori males was also the only rate that increased between 2011 and 2012.
44 Mortality and Demographic Data 2012

Figure 24: Mortality rates from ischaemic heart disease, by sex and ethnicity, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
The five conditions that make up the ischaemic heart disease ICD classification grouping for mortality coding are: I20 angina pectoris I21 acute myocardial infarction I22 subsequent myocardial infarction I24 other acute ischaemic heart diseases I25 chronic ischaemic heart disease.
Of these conditions, acute myocardial infarction (I21) and chronic ischaemic heart disease (I25) together account for the majority of the ischaemic heart disease deaths reported for 2012 (98.7%). Chronic ischaemic heart disease alone was responsible for 53.7%.
Figure 25 compares age-standardised mortality rates, by ethnicity and sex, from acute myocardial infarction and chronic ischaemic heart disease in 2012. The figure suggests the pattern of mortality incidence for these two conditions is generally similar. Males had a higher age-standardised mortality rate (within the ethnic groups) for both conditions.
Mortality and Demographic Data 2012 45

Figure 25: Mortality rates from acute myocardial infarction (ICD I21) and chronic ischaemic heart disease (ICD I25), by sex and ethnicity, 2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population; 95% confidence intervals.
Three DHB regions (Tairāwhiti, Whanganui and Hawke’s Bay) had an ischaemic heart disease death rate that was significantly higher than the national rate (Figure 26). Two DHBs had a rate that was significantly lower (Waitemata and Auckland).
Figure 26: Mortality rates from ischaemic heart disease, by DHB region, total population, 2012
46 Mortality and Demographic Data 2012

Notes:
The dashed vertical line is the national rate.
Rates per 100,000 population, age-standardised to WHO World Standard Population; 99% confidence intervals.
Mortality and Demographic Data 2012 47

Cerebrovascular diseaseCerebrovascular disease is a general term that encompasses a variety of diseases affecting the arteries that supply the brain. This condition is commonly associated with stroke (ie, the sudden death of brain cells due to lack of oxygen when the blood flow to part of the brain is impaired by blockage or rupture of an artery in the brain). A stroke is sometimes called a cerebrovascular accident. Risk factors associated with the narrowing of the arteries (atherosclerosis) that characterises cerebrovascular disease include high blood cholesterol level, high blood pressure, smoking, diabetes and a family history of atherosclerotic disease. Atherosclerosis also occurs with ageing. This section covers ICD codes I60–I69.
Cerebrovascular disease was the third leading cause of death in the total population in 2012, after cancer and ischaemic heart disease.
There were 2612 deaths from cerebrovascular disease in 2012, the majority of which (62.9%) were females.
For each year between 1950 and 2012 there were more female deaths from cerebrovascular disease compared to males (Figure 27). Mortality rates from cerebrovascular disease were similar, and sharply declined for both males and females from the early 1970s to 2012.
Figure 27: Number of deaths and mortality rates from cerebrovascular disease, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
48 Mortality and Demographic Data 2012

In 2012 the mortality rate from cerebrovascular disease for males was 72.0% lower than it was in 1980, and the rate for females was 67.1% lower (Table 18). Males and females had similar annual mortality rates over this period.
Table 18: Number of deaths and mortality rates from cerebrovascular disease, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 1288 96.8 1870 90.0 3158 92.8
1981 1175 84.4 1745 79.4 2920 82.3
1982 1155 80.7 1651 72.6 2806 76.6
1983 1229 84.1 1708 73.5 2937 78.2
1984 1108 74.5 1703 71.4 2811 73.0
1985 1160 76.0 1723 69.7 2883 72.9
1986 1145 70.5 1710 67.7 2855 69.8
1987 1076 66.3 1675 64.4 2751 65.8
1988 1077 64.8 1616 59.2 2693 62.5
1989 1072 63.3 1597 58.3 2669 60.8
1990 1021 57.9 1579 56.6 2600 57.9
1991 1036 58.1 1624 56.0 2660 57.6
1992 1113 60.5 1621 54.0 2734 56.8
1993 1061 55.9 1727 56.0 2788 56.4
1994 1096 56.6 1631 50.4 2727 53.4
1995 1070 53.9 1645 49.0 2715 51.5
1996 1045 51.3 1614 47.2 2659 49.1
1997 966 44.9 1600 44.5 2566 45.1
1998 960 43.5 1532 41.6 2492 42.7
1999 1129 49.3 1706 44.5 2835 47.0
2000 1048 44.6 1620 41.4 2668 42.9
2001 1036 42.4 1748 42.7 2784 43.1
2002 1078 42.7 1751 41.3 2829 42.3
2003 969 37.4 1723 39.8 2692 39.3
2004 1050 38.8 1756 38.9 2806 39.4
2005 940 33.7 1647 36.0 2587 35.5
2006 1000 34.6 1673 35.8 2673 35.8
2007 987 32.9 1638 33.4 2625 33.7
2008 970 30.9 1641 32.9 2611 32.4
2009 937 29.0 1551 30.7 2488 30.4
2010 945 28.1 1522 29.2 2467 29.1
2011 1012 28.7 1653 30.6 2665 30.2
2012 969 27.1 1643 29.6 2612 29.0
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 49

Among non-Māori, 94.0% of deaths from cerebrovascular disease occurred in those aged 65 years and over in 2012 (Table 19). Among Māori, a greater proportion of deaths occurred in younger age groups; 34.4% of Māori deaths from this condition occurred below the age of 65. The equivalent figure for non-Māori was 6.0%.
Table 19: Age distribution of deaths from cerebrovascular disease, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
<25 1.7 1.4 1.5 0.0 0.0 0.0 0.5 0.6 0.6 0.0 0.0 0.0
25–44 3.4 6.9 5.3 1.2 0.9 1.0 2.5 5.6 4.2 2.3 2.7 2.5
45–64 37.3 19.4 27.5 7.5 3.5 5.0 39.0 22.2 30.1 13.9 10.7 12.3
65+ 57.6 72.2 65.6 91.3 95.6 94.0 217.3 280.6 251.5 313.5 481.3 404.3
Note: rates per 100,000 population.
In 2012, Māori had a mortality rate from cerebrovascular disease of 31.2 deaths per 100,000. The mortality rate for non-Māori was 27.7 deaths per 100,000.
Of the four population groups shown in Figure 28, Māori females had the highest age-standardised mortality rate for cerebrovascular disease in 2012, followed by Māori males. From 1996 to 2012, the rate for all groups decreased. In particular, the rate for Māori males and non-Māori males declined by 49%. The disparity between Māori and non-Māori rates appears to be narrowing over time.
Figure 28: Number of deaths and mortality rates from cerebrovascular disease, by sex and ethnicity, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
50 Mortality and Demographic Data 2012

The seven codes that make up the cerebrovascular disease ICD classification grouping for mortality coding are: I60 subarachnoid haemorrhage I61 intracerebral haemorrhage I62 other non-traumatic intracranial haemorrhage I63 cerebral infarction I64 stroke, not specified as haemorrhage or infarction I67 other cerebrovascular diseases I69 sequelae9 of cerebrovascular disease.
‘Stroke, not specified as haemorrhage or infarction’ (I64) accounted for 40.4% of cerebrovascular disease-related mortality in 2012. The three other major causes of cerebrovascular disease-related mortality in 2012 were: I69 sequelae of cerebrovascular disease (17.3%) I63 cerebral infarction (15.2%) I61 intracerebral haemorrhage (12.6%).
Together, these four conditions accounted for the majority (85.5%) of mortality from cerebrovascular disease in 2012.
Females had significantly higher rates of mortality from stroke (I64) and subarachnoid haemorrhage (I60) in 2012 (Figure 29).
Figure 29: Mortality rates from cerebrovascular disease, by specific disease classification and sex, 2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population; 95% confidence intervals.
9 The term ‘sequelae’ refers to conditions that follow as a consequence of a disease.
Mortality and Demographic Data 2012 51

Figure 30 shows cerebrovascular disease mortality rates by DHB region of residence for the total population in 2012. Northland DHB had a rate that was significantly lower than the national rate. All other DHB regions had rates that were not significantly different to the national rate.
Figure 30: Mortality rates from cerebrovascular disease, by DHB region, total population, 2012
Notes:
The dashed vertical line is the national rate.
Rates per 100,000 population, age-standardised to WHO World Standard Population; 99% confidence intervals.
52 Mortality and Demographic Data 2012

Diabetes mellitusThis section covers ICD codes E10–E14. Diabetes mellitus, commonly known as diabetes, is a chronic disease associated with abnormally high levels of glucose in the blood (hyperglycaemia). There are two main types of diabetes: Type 1 (insulin-dependent diabetes mellitus) and Type 2 (adult-onset diabetes). Type 2 diabetes is much more common than Type 1.
A person with Type 1 diabetes does not produce sufficient insulin – they might make only a little, or none at all. Type 1 diabetes usually starts in the teenage years or when puberty begins, although onset can occur later in life.
A person with Type 2 diabetes produces insulin, but the cells upon which the insulin should act are not sufficiently sensitive to its action. Type 2 diabetes commonly starts later in life (typically in people over 30 years of age). Common risk factors include: genetic predisposition (eg, ethnicity or a family history of Type 2 diabetes), obesity and lack of exercise. It is associated with lower socioeconomic status. People suffering from Type 2 diabetes can become insulin-dependent as the disease progresses.
Diabetes can lead to other health conditions, including kidney failure, eye disease, foot ulceration and heart disease.
There were 807 deaths from diabetes mellitus in 2012. Males accounted for 53.3% of these.
From 1950 to the late 1960s the mortality rate from diabetes mellitus for males was generally lower than that for females (Figure 31). From 1970 to 2012 the male rate was consistently higher than the female rate. In 2012 the male rate was 1.5 times the female rate.
Mortality and Demographic Data 2012 53

Figure 31: Number of deaths and mortality rates from diabetes mellitus, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
While the total number of deaths from diabetes mellitus peaked in 2008, the mortality rate has generally been declining since 2000 (Table 20). In 2012, the mortality rate for females was 8.6 deaths per 100,000, and for males it was 12.8 deaths per 100,000.
Table 20: Number of deaths and mortality rates from diabetes mellitus, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 198 13.8 248 12.4 446 13.1
1981 201 13.8 187 9.6 388 11.2
1982 184 12.0 190 9.2 374 10.4
1983 197 13.0 172 8.0 369 10.1
1984 149 10.0 192 8.9 341 9.2
1985 204 12.5 193 8.7 397 10.3
1986 202 11.9 207 9.6 409 10.5
1987 184 11.0 189 8.5 373 9.6
1988 192 11.3 205 8.9 397 10.0
1989 196 11.5 209 9.0 405 10.0
1990 203 11.4 211 9.3 414 10.1
1991 226 12.3 177 7.4 403 9.6
1992 220 11.6 238 9.7 458 10.5
1993 228 12.0 231 9.4 459 10.6
54 Mortality and Demographic Data 2012

1994 228 11.8 258 10.1 486 10.7
1995 255 13.0 253 10.0 508 11.2
1996 306 15.0 289 10.5 595 12.4
1997 316 14.8 317 10.6 633 12.5
1998 387 17.8 343 11.3 730 14.2
1999 385 17.3 355 11.5 740 14.1
2000 408 17.6 394 12.3 802 14.6
2001 405 17.1 377 11.4 782 13.9
2002 427 17.2 378 11.1 805 13.8
2003 436 17.2 411 11.9 847 14.3
2004 438 16.9 405 11.2 843 13.7
2005 447 16.7 392 10.8 839 13.4
2006 447 16.1 413 11.2 860 13.4
2007 440 15.5 407 10.5 847 12.9
2008 463 15.6 414 10.6 877 12.9
2009 482 15.8 387 9.3 869 12.3
2010 391 12.5 377 9.0 768 10.7
2011 438 13.7 397 9.4 835 11.5
2012 430 12.8 377 8.6 807 10.6
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Diabetes mortality in 2012 was largely confined to those aged 45 years and older. Only a small proportion of deaths occurred below this age (Table 21). Within the Māori population, a greater proportion of deaths from diabetes occurred in the 45–64-year age group than in the equivalent age group within the non-Māori population (41.6% of deaths occurred in this age group for Māori compared to 13.7% for non-Māori).
Table 21: Age distribution of deaths from diabetes mellitus, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
<25 0.0 0.0 0.0 0.6 0.0 0.3 0.0 0.0 0.0 0.3 0.0 0.2
25–44 2.9 2.4 2.7 0.6 1.4 1.0 3.8 2.2 3.0 0.4 0.8 0.6
45–64 43.7 39.0 41.6 16.2 10.8 13.7 79.8 50.7 64.4 10.8 6.3 8.5
65+ 53.4 58.5 55.7 82.6 87.8 85.0 351.4 259.0 301.2 101.9 83.0 91.7
Note: rates per 100,000 population.
Of the four population groups represented in Figure 32, Māori males had the highest age-standardised mortality rate for diabetes mellitus, followed by Māori females. The age-standardised rate for Māori was five times the rate for non-Māori in 2012 (Māori had a mortality rate of 40.6 deaths per 100,000, compared with 8.1 deaths per 100,000 non-Māori).
Mortality and Demographic Data 2012 55

Figure 32: Mortality rates from diabetes mellitus, by sex and ethnicity, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
The four codes that make up the diabetes mellitus ICD classification grouping are: E10 Type 1 diabetes mellitus E11 Type 2 diabetes mellitus E13 other specified diabetes mellitus E14 unspecified diabetes mellitus.
Type 2 diabetes mellitus (E11) accounted for the majority (94.5%) of diabetes mortality in 2012. Very few deaths (7) were classified as unspecified diabetes mellitus (E14). There were no deaths classified as other specified diabetes mellitus (E13) in 2012.
Figure 33 shows mortality rates for Type 1 (E10) and Type 2 (E11) diabetes mellitus by sex in 2012. Males had a significantly higher rate of Type 2 diabetes mortality than females.
56 Mortality and Demographic Data 2012

Figure 33: Mortality rates from diabetes mellitus, by diabetes type and sex, 2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population; 95% confidence intervals.
Mortality and Demographic Data 2012 57

Motor vehicle accidentsThe classification ‘motor vehicle accidents’ primarily covers accidents associated with motorised transport (both on-road and off-road), including cars, two- or three-wheeler vehicles and heavy transport vehicles. It also includes pedestrians or cyclists involved in accidents with motor vehicles. The classification excludes road traffic accidents that did not include some form of motorised transport; for example, a collision between a pedestrian and a pedal cyclist, or a collision between a pedal cyclist and a railway train. It also excludes accidents involving watercraft and aircraft. The ICD codes from the V02–V89 range discussed here therefore exclude those that do not meet these criteria.
Motor vehicle accidents are a major cause of mortality in New Zealand and other industrialised countries. The first recorded motor vehicle accident fatality in New Zealand was in Christchurch in 1908. For most of the 20th century, the motor vehicle accident rate rose in concert with the increasing number of vehicles on New Zealand roads. Since the late 1980s this trend has reversed, and there has been a steady decline in deaths from motor vehicle accidents. This decline may be related to a variety of factors, including a greater societal awareness of the dangers of drink driving, excessive speed and driver fatigue; a rise in seatbelt use; better trauma treatment; and the increasing safety of roads and modern motor vehicles. The open road speed limit in New Zealand has varied over the years from 80 km/h (set in 1948 and again in 1974) to 100 km/h (the current limit, set in 1985). Blood alcohol and breath testing procedures were introduced in New Zealand in 1969, and seatbelt use became compulsory in 1975. Speed cameras were introduced in 1993.
Mortality rates from motor vehicle accidents peaked in the 1970s and generally declined from this point forward (Figure 34). In 2011 mortality rates were the lowest of all years shown for both sexes (9.8 deaths per 100,000 for males and 3.3 deaths per 100,000 for females). In 2012 the mortality rate was 11.3 deaths per 100,000 for males and 3.7 per 100,000 for females.
Figure 34: Number of deaths and mortality rates from motor vehicle accidents, by sex, 1950–2012
58 Mortality and Demographic Data 2012

Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
From 1980 to 2012 the rate of motor vehicle accident deaths declined by around two-thirds (58.7% among males and 66.8% among females) (Table 22). Males had a consistently higher rate of motor vehicle accident deaths over this time; in 2012 the male rate was three times the female rate.
Table 22: Number of deaths and mortality rates from motor vehicle accidents, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 438 27.4 184 11.3 622 19.3
1981 476 29.6 231 13.6 707 21.6
1982 538 33.0 192 11.6 730 22.2
1983 461 27.6 186 10.8 647 19.2
1984 517 30.8 193 11.1 710 21.0
1985 516 30.4 231 13.4 747 21.8
1986 567 33.7 215 12.4 782 23.0
1987 570 33.4 265 15.0 835 24.2
1988 537 31.6 206 11.5 743 21.5
1989 557 32.5 242 13.8 799 23.1
1990 545 31.7 219 12.2 764 22.0
1991 471 27.8 210 11.7 681 19.7
1992 462 27.1 194 10.9 656 18.8
1993 438 25.3 179 10.0 617 17.6
1994 419 24.0 183 10.0 602 16.9
1995 407 23.4 205 10.9 612 17.1
1996 381 21.9 156 8.5 537 15.1
1997 383 20.8 167 8.6 550 14.5
Mortality and Demographic Data 2012 59

1998 358 19.4 171 8.7 529 14.0
1999 349 18.7 184 9.1 533 13.8
2000 322 17.3 157 7.7 479 12.5
2001 318 17.2 151 7.2 469 12.1
2002 314 16.2 142 6.8 456 11.4
2003 336 17.2 158 7.4 494 12.3
2004 314 15.6 149 7.1 463 11.2
2005 307 15.2 127 6.0 434 10.6
2006 283 13.6 120 5.1 403 9.2
2007 300 14.7 150 6.6 450 10.6
2008 261 12.7 135 5.8 396 9.2
2009 286 13.5 134 5.7 420 9.5
2010 296 13.4 120 4.9 416 9.1
2011 221 9.8 84 3.3 305 6.5
2012 255 11.3 92 3.7 347 7.4
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Motor vehicle accident deaths within the Māori population were more common in the younger age groups in 2012 (Table 23). More than two-thirds of Māori deaths (69.3%) occurred in those below the age of 45, compared to 51.0% of non-Māori deaths.
Māori had higher age-specific rates of motor vehicle accident deaths than non-Māori in all age groups. Māori aged 25–44 and 45–64 years had mortality rates that were approximately three times higher than the corresponding non-Māori rates in 2012.
Table 23: Age distribution of deaths from motor vehicle accidents, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
<25 33.8 25.0 31.8 27.3 25.0 26.6 12.5 2.8 7.8 8.4 3.2 5.9
25–44 32.4 55.0 37.5 27.8 15.3 24.3 27.9 12.3 19.7 10.7 2.1 6.3
45–64 25.0 10.0 21.6 20.9 20.8 20.8 30.2 3.2 15.9 8.0 2.9 5.4
65+ 8.8 10.0 9.1 24.1 38.9 28.2 38.3 10.8 23.4 17.0 9.0 12.6
Note: rates per 100,000 population.
Māori had a motor vehicle accident mortality rate more than twice that of non-Māori in 2012 (14.1 deaths per 100,000, compared with 6.2 deaths per 100,000 non-Māori).
60 Mortality and Demographic Data 2012

For all groups shown in Figure 35, mortality rates were significantly lower in 2012 compared with 1996 (using 95% confidence intervals).10 Of rates for these groups, the rate for Māori males showed the biggest decline, decreasing by 38.4% over this time.
In 2012, the mortality rate for Māori males was 2.4 times the rate for non-Māori males. For females, the Māori rate was twice the non-Māori rate.
Figure 35: Mortality rates from motor vehicle accidents, by sex and ethnicity, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Figure 36 shows the rate of hospitalisations alongside the mortality rate from motor vehicle accidents between 1996 and 2012. Both the hospitalisation and the mortality rates showed a significant decline over this period. The motor vehicle accident mortality rate fell from 15.1 per 100,000 total population in 1996 to 7.4 per 100,000 in 2012. The hospitalisation rate fell from 236.6 per 100,000 total population in 1996 to 148.3 per 100,000 in 2012.
The ratio line shows how many motor vehicle hospitalisation incidents occurred for every mortality incident over these years. In 2012, for example, there were 20 motor vehicle accident-related hospitalisations for every death. The general upward trend of the ratio line suggests that people injured in a motor vehicle accident were less likely to die over this time period.
10 Confidence intervals were calculated for all rates, although they are not shown in Figure 35. For more information on confidence intervals, see ‘Confidence intervals’ within ‘Statistical notes’.
Mortality and Demographic Data 2012 61

Figure 36: Mortality and hospitalisation rates from motor vehicle accidents, and ratio of hospitalisation rate to mortality rate, 1996–2012
Notes:
Rates per 100,000 population, age-standardised to WHO World Standard Population.
In the interests of making the data comparable between DHBs, the hospitalisation data used to produce this figure excludes short-stay emergency department events.11
Some events will have been included in both the hospitalisation and the mortality count, taking into account people who were injured then subsequently died in hospital.
11 For further information see the short-stay emergency department data factsheet: www.health.govt.nz/publication/factsheet-short-stay-emergency-department-events
62 Mortality and Demographic Data 2012

SuicideThe ICD codes X60–X84 covers acts of intentional self-harm. Mortality from intentional self-harm is commonly referred to as suicide. This section provides an overview of suicide mortality; for a more detailed analysis see the Ministry of Health publication series Suicide Facts: Deaths and Intentional Self-harm Hospitalisations.12 The numbers presented here are taken from the final data for 2012 suicide mortality, and so differ slightly from the provisional data in the 2012 Suicide Facts publication.
In 2012, 550 suicides occurred in New Zealand, as determined following coronial investigation. Males made up three-quarters (73.5%) of these deaths.
After 1950, the male suicide rate reached a peak in 1995, then declined to a rate of 18.5 deaths per 100,000 males in 2012 (Figure 37). The female rate remained relatively stable between 1950 and 2012. In 2012 the rate for females was 6.4 deaths per 100,000.
Figure 37: Number of deaths and mortality rates from suicide, by sex, 1950–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Between 1980 and 2012 the male suicide rate was consistently higher than the female rate (Table 24). The biggest disparity occurred in 2000, when the male rate was more than 4.5 times the female rate. In 2012 the male rate was almost three times the female rate.
12 www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/suicide-facts-deaths-and-intentional-self-harm-hospitalisations-series
Mortality and Demographic Data 2012 63

Table 24: Number of deaths and mortality rates from suicide, by sex, 1980–2012
Year Male Female Total
No. Rate No. Rate No. Rate
1980 225 14.8 112 7.0 337 10.8
1981 241 15.8 79 4.8 320 10.2
1982 257 16.3 107 6.6 364 11.3
1983 250 15.5 102 6.2 352 10.7
1984 297 18.3 92 5.4 389 11.7
1985 255 15.5 83 4.9 338 10.0
1986 301 18.3 113 6.6 414 12.3
1987 363 21.7 100 5.8 463 13.6
1988 381 22.4 103 5.7 484 13.9
1989 372 21.8 93 5.3 465 13.4
1990 363 21.1 92 5.1 455 13.0
1991 380 22.3 94 5.4 474 13.7
1992 397 23.1 96 5.4 493 14.1
1993 349 19.9 94 5.2 443 12.5
1994 409 23.1 103 5.5 512 14.1
1995 427 23.9 116 6.3 543 15.0
1996 428 23.8 112 6.1 540 14.7
1997 440 23.7 121 6.3 561 14.8
1998 445 23.7 132 6.8 577 15.1
1999 385 20.4 131 6.8 516 13.4
2000 375 20.0 83 4.2 458 11.9
2001 388 20.3 119 5.9 507 12.9
2002 353 18.0 113 5.6 466 11.6
2003 376 18.4 141 6.6 517 12.4
2004 379 18.6 109 5.2 488 11.7
2005 380 18.6 131 6.0 511 12.2
2006 388 18.6 138 6.3 526 12.2
2007 371 17.4 116 5.0 487 11.0
2008 381 17.6 139 6.2 520 11.8
2009 393 17.9 117 5.0 510 11.3
2010 386 17.3 149 6.6 535 11.8
2011 377 17.0 116 5.1 493 10.9
2012 404 18.5 146 6.4 550 12.3
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
In 2012, a high proportion of Māori suicide deaths occurred in the younger age groups. More than half of all Māori suicide deaths (58.0%) were among those aged 5–24 years. The proportion in the equivalent age-group for non-Māori was 21.1%. Conversely, a higher proportion of non-Māori suicide deaths occurred among those aged 65 and over, compared with the equivalent Māori age group (13.2% for non-Māori and 0.8% for Māori).
64 Mortality and Demographic Data 2012

While Māori had higher age-specific mortality rates from suicide in the younger age groups (those aged less than 45 years), rates for Māori aged 45 years and over were lower than the corresponding rates for non-Māori. Table 25 shows the 2012 percentage distribution of deaths and age-specific mortality rates from suicide for five age groupings for Māori and non-Māori.
Table 25: Age distribution of deaths from suicide, percentages and rates, by ethnicity and sex, 2012
Age group (years)
Percentage Age-specific rate
Māori Non-Māori Māori Non-Māori
Male Female Total Male Female Total Male Female Total Male Female Total
5–14 6.1 8.1 6.7 0.6 1.8 0.9 6.8 4.3 5.6 0.9 0.9 0.9
15–24 45.1 64.9 51.3 21.4 16.5 20.2 57.2 38.4 48.0 25.9 7.3 16.9
25–44 36.6 24.3 32.8 34.8 31.2 33.9 38.1 10.1 23.2 22.9 6.6 14.6
45–64 11.0 2.7 8.4 30.1 36.7 31.8 16.0 1.6 8.4 19.9 7.8 13.7
65+ 1.2 0.0 0.8 13.0 13.8 13.2 6.4 0.0 2.9 15.8 4.8 9.9
Note: rates per 100,000 population.
In 2012, Māori had a mortality rate from suicide of 17.6 deaths per 100,000, compared with 10.6 deaths per 100,000 non-Māori.
Compared with their female counterparts, both Māori males and non-Māori males had significantly higher mortality rates in 2012 (Figure 38).13
Figure 38: Mortality rates from suicide, by sex and ethnicity, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
13 Confidence intervals were calculated for all rates, although they are not shown in Figure 38. For more information on confidence intervals, see ‘Confidence intervals’ within ‘Statistical notes’.
Mortality and Demographic Data 2012 65

Figures 39 and 40 show the rate of intentional self-harm hospitalisations alongside the mortality rate for suicide between 1996 and 2012 for males and females. Note that the hospitalisation figures exclude short-stay emergency department data, in line with the methodology used for motor vehicle accident hospitalisations in this publication and in line with that used in the Suicide Facts publication series.
There is a distinct difference between males and females in regard to intentional self-harm hospitalisation rates relative to suicide mortality rates. Males have a lower ratio of hospitalisations to deaths than females.
Figure 39: Male mortality and hospitalisation rates from intentional self-harm, and ratio of hospitalisation rate to mortality rate, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
66 Mortality and Demographic Data 2012

Figure 40: Female mortality and hospitalisation rates from intentional self-harm, and ratio of hospitalisation rate to mortality rate, 1996–2012
Note: rates per 100,000 population, age-standardised to WHO World Standard Population.
Mortality and Demographic Data 2012 67

Maternal mortalityAccording to the WHO a maternal death is ‘the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes’ (WHO 2004).
The WHO categorises maternal deaths into two groups:1. Direct obstetric deaths: those resulting from obstetric complications of the
pregnant state (pregnancy, labour or puerperium), from interventions, omissions, incorrect treatment, or from a chain of events resulting from any of the above.
2. Indirect obstetric deaths: those resulting from previous existing disease or disease that developed during pregnancy and was not due to direct obstetric causes but that was aggravated by the physiologic effects of pregnancy.
These definitions exclude maternal deaths occurring 42 days after the termination (end) of pregnancy. This section covers ICD codes O00-O95, O98-O99.
The number of maternal deaths in New Zealand each year is relatively small, so annual maternal death rates may vary substantially. Caution is advised when comparing rates over time.
A total of seven maternal deaths occurred in 2012, equating to a rate of 11.3 deaths per 100,000 live births.
The number and rate of maternal deaths decreased markedly from the 1950s to the late 1970s (Figure 41). There were 52 deaths in 1950 (105.2 deaths per 100,000 live births) compared to six deaths in 1979 (11.5 deaths per 100,000). From the late 1970s the decline in the rate of maternal deaths slowed and became more stable compared to previous years.
68 Mortality and Demographic Data 2012

Figure 41: Number of maternal deaths and maternal mortality rates, 1950–2012
Note: rates per 100,000 live births.
From 1980 to 2012 the number of maternal deaths ranged between two (in both 1981 and 1995) and 13 (in 2007) (Table 26). The highest rate of maternal deaths over this period was 20.0 deaths per 100,000 live births in 2007. The lowest rate was 3.5 deaths per 100,000 live births in 1995.
Table 26: Number of maternal deaths and maternal mortality rates, 1980–2012
Year Direct Indirect Total
Number Rate Number Rate Number Rate
1980 7 13.8 0 0.0 7 13.8
1981 2 3.9 0 0.0 2 3.9
1982 7 14.0 0 0.0 7 14.0
1983 7 13.9 2 4.0 9 17.8
1984 3 5.8 0 0.0 3 5.8
1985 6 11.6 1 1.9 7 13.5
1986 6 11.4 3 5.7 9 17.0
1987 4 7.2 3 5.4 7 12.7
1988 5 8.7 5 8.7 10 17.4
1989 4 6.9 2 3.4 6 10.3
1990 3 5.0 1 1.7 4 6.6
1991 7 11.7 2 3.3 9 15.0
1992 2 3.4 3 5.1 5 8.4
1993 6 10.2 4 6.8 10 17.0
1994 4 7.0 0 0.0 4 7.0
1995 2 3.5 0 0.0 2 3.5
1996 4 7.0 0 0.0 4 7.0
Mortality and Demographic Data 2012 69

1997 2 3.5 1 1.7 3 5.2
1998 1 1.7 3 5.2 4 6.9
1999 3 5.2 1 1.7 4 7.0
2000 2 3.5 3 5.3 5 8.8
2001 0 0.0 3 5.3 3 5.3
2002 4 7.3 4 7.3 8 14.7
2003 3 5.3 1 1.8 4 7.1
2004 1 1.7 3 5.1 4 6.8
2005 3 5.1 2 3.4 5 8.5
2006 4 6.6 3 5.0 7 11.6
2007 7 10.7 6 9.2 13 20.0
2008 3 4.6 3 4.6 6 9.2
2009 5 7.9 5 7.9 10 15.8
2010 2 3.1 3 4.6 5 7.7
2011 2 3.2 5 8.0 7 11.3
2012 2 3.2 5 8.1 7 11.3
Note: rates per 100,000 live births.
From 2008 to 2012, indirect maternal deaths accounted for 60% of all maternal deaths (Table 27). Of the 21 women who died of an indirect maternal cause between 2008 and 2012, the majority died as a result of diseases of the circulatory system (8 women) and diseases of the respiratory system complicating pregnancy, childbirth and the puerperium (7 women). The remaining women died as a result of either: endocrine, nutritional and metabolic diseases mental disorders and diseases of the nervous system diseases of the skin and subcutaneous tissue, or other specified diseases and conditions complicating pregnancy, childbirth and
the puerperium.
Direct maternal deaths made up the remaining 40%. Of the 14 women who died of a direct maternal cause, five women died as a result of an obstetric embolism.
Table 27: Maternal deaths by underlying cause, 2008–2012
Underlying cause of death by ICD 3-character code
2008 2009 2010 2011 2012 2008–2012
Number Number Percent
Direct maternal deaths (O00–O95) 3 5 2 2 2 14 40.0
Pre-existing hypertension complicating pregnancy, childbirth and the puerperium (O10)
– – – 1 – 1 2.9
Gestational (pregnancy-induced) hypertension with significant proteinuria (O14)
1 1 – – – 2 5.7
Maternal care for other conditions predominantly related to pregnancy (O26)
– – 1 – – 1 2.9
Other disorders of amniotic fluid and membranes (O41)
– – – – 1 1 2.9
Placental disorders (O43) 1 – – – – 1 2.9
70 Mortality and Demographic Data 2012

Other obstetric trauma (O71) – 1 – – – 1 2.9
Other complications of labour and delivery, not elsewhere classified (O75)
– – 1 – – 1 2.9
Venous complications in the puerperium (O87) – – – 1 – 1 2.9
Obstetric embolism (O88) 1 3 – – 1 5 14.3
Indirect maternal deaths (O98–O99) 3 5 3 5 5 21 60.0
Other maternal diseases classifiable elsewhere but complicating pregnancy, childbirth and the puerperium (O99)
3 5 3 5 5 21 60.0
Total maternal deaths 6 10 5 7 7 35 100.0
Live births 65,333 63,285 64,699 62,174 62,035 – –
Mortality and Demographic Data 2012 71

Further mortality-related informationAccompanying online tablesStatistical mortality data tables are available online in Excel format alongside the Mortality and Demographic Data publication at: www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/mortality-and-demographic-data-series
The tables published on this page contain mortality data for the complete range of ICD-10-AM classifications, in sex and five-year age groupings. The data is grouped at national, regional and ethnic group level.
Ministry of Health publicationsFurther detailed information may be found in the following Ministry of Health publications: Further detailed information on numbers and rates of live births, and fetal,
neonatal and post-neonatal deaths, is published in the annual series Fetal and Infant Deaths(www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/fetal-and-infant-deaths-series).
Further information on cancer incidence and mortality can be found in the annual series Cancer: New registrations and deaths (www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/cancer-new-registrations-and-deaths-series).
Information on hospitalisations and mortality from intentional self-harm can be found in the annual series Suicide Facts: Deaths and intentional self-harm hospitalisations(www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/suicide-facts-deaths-and-intentional-self-harm-hospitalisations-series). Suicide prevention information can be found at www.health.govt.nz/our-work/mental-health-and-addictions/working-prevent-suicide
These publications, and others produced by the Ministry of Health, can be found through www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets
Publications by other organisationsSerious injury outcome indicator reportsStatistics New Zealand produces annual serious injury outcome indicator reports. These reports include numbers and rates of death from suicide, assault and motor vehicle traffic crashes (MVTC). The information for these reports is also sourced from the New Zealand Mortality Collection, and is therefore broadly comparable
72 Mortality and Demographic Data 2012

with the information published in Mortality and Demographic Data. However, the Mortality Collection is a dynamic database; any small discrepancies in data between the two publications are therefore likely to be due to updates to records in the database over time.
The serious injury outcome indicator reports also present data on ‘serious non-fatal intentional self-harm injury’ and ‘serious non-fatal MVTC injury’. These indicators cover only a subset of the self-harm hospitalisation data and motor vehicle accidents data analysed in this publication, and therefore cannot be directly compared.
For more information and access to the serious injury outcome indicator reports see www.stats.govt.nz/browse_for_stats/health/injuries/serious-injury-outcome-indicators-reports.aspx
For further information relating to the methodology, classifications and processes used to produce this publication, and how they differ between publications, contact [email protected]
Population data used for calculating ratesFor population and other demographic data, contact the Ministry of Health (email: [email protected]) or Statistics New Zealand (www.stats.govt.nz or email: [email protected]).
Additional data available from the Ministry of HealthThe Ministry of Health collects and records the information presented in Table 28 for all deaths in New Zealand. For a full listing of available fields, refer to the Mortality Collection Data Dictionary (available at: www.health.govt.nz/publication/mortality-collection-data-dictionary).
You may require information not included in this report or in the accompanying online tables. The Ministry of Health is able to produce customised data extracts tailored to your needs. These may incur a charge (at Official Information Act rates). If you require additional data or analysis, contact:
Analytical ServicesMinistry of HealthPO Box 5013Wellington, 6145New ZealandPhone (04) 496 2000Fax (04) 816 2898Email: [email protected] visit: www.health.govt.nz
Mortality and Demographic Data 2012 73

The Ministry of Health welcomes comments and suggestions about this publication.
Table 28: Mortality data available from the Ministry of Health
Item Notes
1 Health care user number
Also known as National Health Index number. Restricted access.
2 Domicile code Based on Statistics New Zealand Standard Area Unit code used for the 2006 Census.
3 Sex Male, female, indeterminate.
4 Ethnicity Based on Statistics New Zealand Standard Classification 1996 (Level 2); for example, NZ Māori, NZ European or Pākeha, Other European, Samoan, Chinese and so on. Up to three ethnicities are recorded and prioritised.
5 Age Age in days, weeks, months or years, as applicable.
6 Date of birth Day, month, year.
7 Country of birth From Statistics New Zealand Standard Country Code list, 1986.
8 Time deceased was in New Zealand
Number of years in New Zealand if not born in New Zealand.
9 Date of death Day, month, year.
10 Year of registration Year in which the death was registered.
11 Place died Place of death as recorded on the death registration.
12 Underlying cause of death
Codes from ICD-10-AM from 2000 onwards.
13 Selected contributing disease or condition
Codes from ICD-10-AM for selected conditions that contributed to death but were not the underlying cause of death (eg, diabetes mellitus, drug abuse and injuries) from 2000 onwards.
14 Mesh block Statistics New Zealand’s smallest area unit code, based on deceased’s residential address, from 2003 onwards. Restricted access.
15 Cot death indicator Sudden infant death syndrome indicator.
16 Maternal death indicator
Indicates whether the death is the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.
17 Pregnancy-related indicator
Indicates if a woman died while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death.
18 Post-mortem code Indicates whether a post-mortem was performed and/or used in classification by the Ministry of Health.
19 Death certifier code Certified by doctor, or coroner with/without inquest, coroner’s interim report.
20 Death information source code
Code indicating the most accurate source of the information used to classify the underlying cause of death; for example, Births, Deaths and Marriages, Coronial Services, Land Transport New Zealand, Water Safety New Zealand.
21 Comments Free text field for additional comments relating to the death (eg, may include details of accidents or time sequence of conditions). Restricted access.
22 Occupation Text description of deceased’s usual occupation (or former occupation, if retired). Collected since 1998.
23 Work-related indicator
Recorded if the cause of death was known to be due to an accident while at work from 2000 onwards.
24 Alcohol-involved indicator
Records if alcohol consumption preceded death, when reported from 2000 onwards. Only recorded for deaths certified by a coroner.
25 Blood alcohol level Recorded in mg/100 mL blood, when reported from 2000 onwards. Only recorded for deaths certified by a coroner.
26 Birthweight Weight at birth in grams. Recorded when known for deaths of infants less than one year of age and for stillbirths.
74 Mortality and Demographic Data 2012

Item Notes
27 Gestation Gestation (in weeks) of infant at birth. Recorded when known for deaths of infants less than one year of age and for stillbirths.
Mortality and Demographic Data 2012 75

Explanatory notesMortalityDeathsEvery death occurring in New Zealand must be registered with Births, Deaths and Marriages. Deaths should be registered within three working days of burial or cremation, although the law does not impose any limit on the time after which a death may not be registered.
This information, along with stillbirth registration data, is supplied to the Ministry of Health. The Ministry of Health then matches death and stillbirth registrations from the Registry with individuals’ National Health Index numbers. This combined information comprises the death registration data held in the National Mortality Collection (MORT).
The statistics in this publication relate to registrations during the year 2012, rather than the actual number of deaths during the year 2012.
Causes of deathThe ICD-10-AM was used to classify causes of death throughout this report (National Centre for Classification in Health 2008). The WHO regularly revises the ICD publication, and issues updates in the form of new revisions; for example, ICD-10 is the Tenth Revision.
If more than one cause is entered on a medical certificate, the Mortality Collection follows WHO mortality rules and guidelines (as specified in ICD-10) for identifying the underlying cause of death. This is largely determined from the statement of the certifying doctor or coroner, but reference is also made to post-mortem reports received, and cancer registrations. On some occasions, coded hospital inpatient event summaries are compared with entries on the medical certificate in order to obtain more specific information. Information is also obtained from letters to certifying doctors and medical records departments, from data supplied by Land Transport New Zealand and Water Safety New Zealand, from the internet and from Coronial Services.
When a death is due to an external cause, such as an accident, the external cause and not the resulting injury is coded as the underlying cause of death. For example, if a death is due to a head injury as a result of a motor vehicle crash, the motor vehicle crash will be coded as the cause of death. Sites and types of injuries are coded as contributing causes, if reported.
Amenable mortalityThe ICD-10-AM codes used to define amenable mortality in this publication are shown in the following table.
76 Mortality and Demographic Data 2012

Table 29: Codes used to define amenable mortality
Group Condition ICD-10-AM code(s) Notes
Infections Pulmonary tuberculosis A15–A16
Meningococcal disease A39
Pneumococcal disease A40.3, G00.1, J13
HIV/AIDS B20–B24
Cancers Stomach cancer C16
Rectal cancer C19–C21
Bone and cartilage cancer C40–C41
Melanoma of skin C43
Female breast cancer C50 Females only
Cervical cancer C53
Prostate cancer C61
Testis cancer C62
Thyroid cancer C73
Hodgkin lymphoma C81
Acute lymphoblastic leukaemia C91.0 Ages 0–44 years
Maternal and infant
Complications of pregnancy O00–O96, O98–O99
Complications of perinatal period P01–P03, P05–P94
Cardiac septal defect Q21
Chronic disorders
Diabetes E10–E14
Valvular heart disease I01, I05–I09, I33–I37
Hypertensive diseases I10–I13
Coronary disease I20–I25
Pulmonary embolism I26
Heart failure I50
Cerebrovascular diseases I60–I69
COPD J40–J44
Asthma J45–J46
Peptic ulcer disease K25–K27
Cholelithiasis K80
Renal failure N17–N19
Injuries Land transport accidents excluding trains
V01–V04, V06–V14, V16–V24, V26–V34, V36–V44, V46–V54, V56–V64, V66–V74, V76–V79, V80.0–V80.5, V80.7–V80.9, V82–V86, V87.0–V87.5, V87.7–V87.9, V88.0–V88.5, V88.7–V88.9, V89, V98–V99
Include V00 if using ICD-10-AM-VI (from 2008 onwards)
Accidental falls on same level W00–W08, W18
Fire X00–X09
Suicide X60–X84
Treatment injury Y60–Y82
Mortality and Demographic Data 2012 77

Cancer mortalityIn the third edition of the International Classification of Diseases for Oncology (ICD-O), the range of neoplasms considered to be malignant was expanded. Specifically, polycythaemia vera, myelodysplastic syndromes and chronic myeloproliferative disorders are considered to be malignant in the third edition of ICD-O, whereas in the second edition these diseases were considered to be of uncertain behaviour. The ICD-10 codes for these additional malignancies are in the range D45–D47. This change took effect from 2003. Mortality and Demographic Data 2004 was the first publication in this series to include the D45–D47 range in cancer analyses.
Motor vehicle accident deathsThe ICD 10 AM codes used to define motor vehicle accident deaths in this publication are:V02–V04, V09.0–V09.3, V12–V14, V19.0–V19.2, V19.4–V19.6, V20–V79, V80.3–V80.5, V81.0–V81.1, V82.0–V82.1, V83.0–V83.3, V84.0–V84.3, V85.0–V85.3, V86.0–V87.8,V88.0–V88.8, V89.0, V89.2 and V89.9.
Maternal mortalityThe ICD-10-AM codes used to define maternal mortality in this publication are O00–O95: direct obstetric deaths and O98–O99: indirect obstetric deaths. This is in line with the WHO definition.
In addition to the summarised maternal mortality data in this publication, the Perinatal and Maternal Mortality Review committee within the Health Quality and Safety Commission publishes more detailed maternal mortality information in their annual report: see www.hqsc.govt.nz/our-programmes/mrc/pmmrc/publications-and-resources/publication/2123/
DomicileIn general, the domicile code of the deceased is classified according to the usual residence at time of death. The domicile code used for health collections is the four-digit Health Domicile Code originally created by Statistics New Zealand from its six-digit Census Area Unit Code. In 2012, the Health Domicile Code used was based on the 2006 Census Area Unit Code.
PopulationChanges to estimating the population in New ZealandStatistics New Zealand produces national population estimates based on the concept of the ‘usually resident population’ (since 1991). Previously, both national and subnational estimates were based on the ‘de facto population’ concept, which included all people in New Zealand at a given time, including overseas visitors, and excluded New Zealanders temporarily overseas on Census night. Statistics New Zealand considers that the resident population concept produces a more accurate estimate.
78 Mortality and Demographic Data 2012

The most significant outcome of this change is that the resulting demographic indices are slightly lower. This is because of a smaller numerator (because registrations of births, deaths and marriages of overseas visitors while in New Zealand are excluded) and a bigger denominator (due to the slightly larger population estimates).
Population data usedThe populations used to calculate rates in this report are available online in Excel format alongside this publication.
Mortality rates for 2012 were calculated using the following population data sets supplied by Statistics New Zealand: estimated resident population by age and sex, mean year ended 31 December
2012 estimated resident population for Māori and non-Māori by age and sex, mean
year ended 31 December 2012* estimated resident population by age, sex and DHB as at 30 June 2012.
Populations used were updated with 2013 Census results except for those marked with an asterisk (*), which were based on 2006 Census results.
Maternal mortality rates were calculated using the number of live-born babies registered with Births, Deaths and Marriages in each calendar year.
Rates presented for years prior to 2012 are as published in the ‘Mortality and Demographic Data’ series. They were calculated using the estimated resident population available at the time of release, and have not been recalculated for this report.
EthnicityEthnicity data for deaths mainly come from Births, Deaths and Marriages. Ethnicity data is provided to funeral directors by family members or others assisting with the death registration and recorded on the BDM28 Notification of Death for Registration form.
Ethnicity data for the New Zealand population is based on prioritised ethnicity. Changes in ethnicity recording came into effect in September 1995. Previously, ethnicity had been based on ancestry, with only one ethnic group ascribed to each individual (the ‘sole ethnic origin’ concept). The 1995 changes introduced the self-identified ethnicity model, which allows an individual to choose multiple ethnicities based on their preferences or self-concept. Multiple selected ethnicities are then prioritised into a hierarchy.
The system recognises the following key characteristics of ethnicity. Ethnicity is self-perceived, so people should identify their own ethnic affiliation
whenever feasible.
Mortality and Demographic Data 2012 79
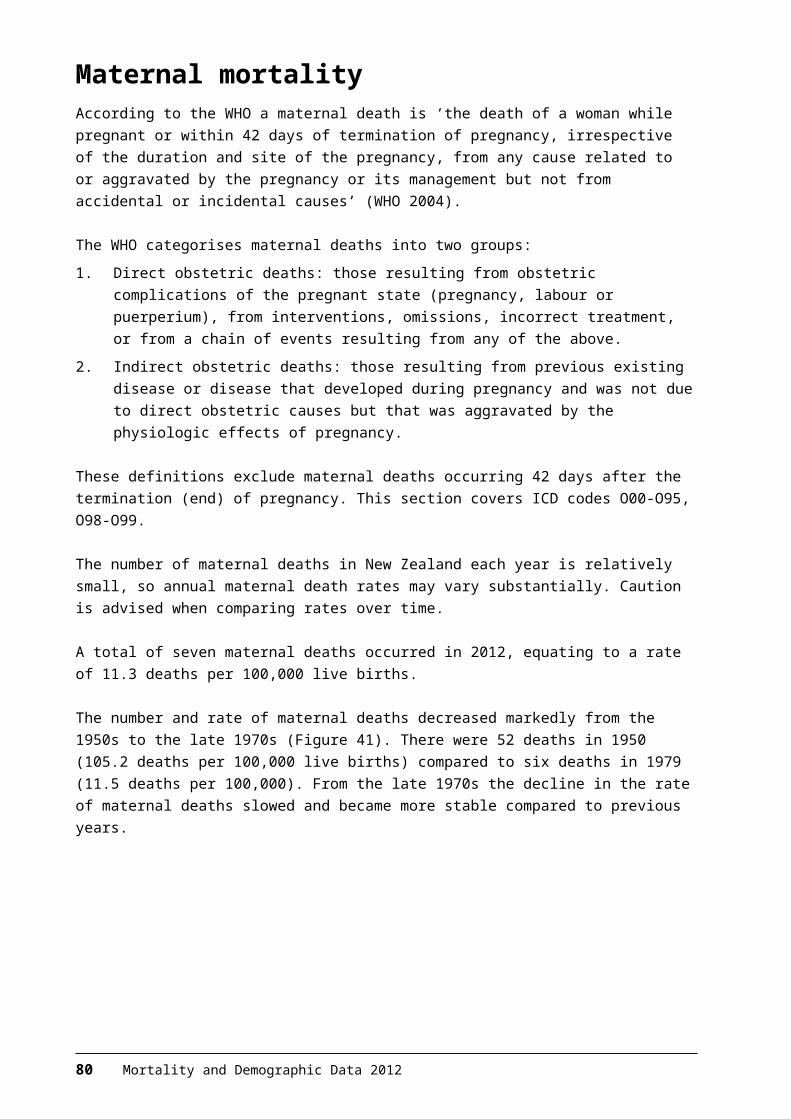
A person can belong to more than one ethnic group. The ethnicities with which a person identifies can change over time or in
different contexts.
Ethnicity is a social construct of group affiliation and identity. The present Ministry of Health statistical standard for ethnicity states that ‘ethnicity is the ethnic group or groups that people identify with or feel they belong to’. Thus, ethnicity is self-perceived, complex and multidimensional.
This definition is based on the work of Anthony Smith (Smith 1986).
PrioritisationIn this publication, all individuals who identified as Māori (including those who identified with more than one ethnic group) are presented as Māori. All other individuals are presented as non-Māori, including those with no recorded ethnicity (Ministry of Health 2004). The aim of prioritisation is to ensure that when it is necessary to assign people to a single ethnic group, ethnic groups that are small or important in terms of policy are not swamped by the European ethnic group. This method is also a more robust method of dealing with the low rate of multiple ethnicities in health sector data.
Further information on ethnicity data protocols for the health and disability sector is available at www.health.govt.nz/publication/ethnicity-data-protocols-health-and-disability-sector
Statistical notesAge-specific ratesAn age-specific rate is the rate at which a particular event (eg, death or disease incidence) occurs in each age group of a population as some unit of the population-at-risk or person-years-at-risk.
An age-specific rate is simply the crude rate for the specific age group. For example, to calculate the age-specific rate of a disease for people aged 45–49, the total number of cases in the age group is divided by the population in that age group and multiplied by a constant (a unit of population: 100,000 in this publication). This process produces death rates showing the number of deaths per 100,000 population in each age group in a particular year (Borman 1995).
Age-standardised ratesAge-standardised death rates adjust for differences in age distribution of the populations being compared. Age-standardised rates are artificially created figures that allow comparisons to be made with differing groups; they should only be compared with other adjusted rates that have been computed using the same ‘standard’ population.
Age-standardised rates are calculated by multiplying age-specific rates by a standard population. The standard population used in these calculations is the
80 Mortality and Demographic Data 2012

WHO World Standard Population (Table 30). The WHO World Standard Population is a widely used New Zealand and international standard.
Different population standards will produce different mortality rates, different rankings for causes of death and different confidence intervals. For example, comparing the WHO standard population used in this publication and a Māori population shows that the all-cause mortality rate for Māori is higher using the WHO standard, and that the relative rankings of some causes of Māori death (eg, deaths from external causes) are lower (Robson et al 2007).
Further information on age-specific and age-standardised rates can be found in the Ministry of Health/Public Health Commission document Standardising Rates of Disease: see www.health.govt.nz/publication/standardising-rates-disease
Table 30: The WHO World Standard Population
Age group Population
0–4 8860
5–9 8690
10–14 8600
15–19 8470
20–24 8220
25–29 7930
30–34 7610
35–39 7150
40–44 6590
45–49 6040
50–54 5370
55–59 4550
60–64 3720
65–69 2960
70–74 2210
75–79 1520
80–84 910
85+ 635
Total 100,035
Source: Waterhouse et al 1976
Confidence intervalsConfidence intervals have been calculated for age-standardised rates at the 95% or 99% level using the method presented in Keyfitz (1966).
A confidence interval is a range of values used to describe the uncertainty around a single value (such as an age-standardised rate). It is used to estimate the true value in a population, such as the underlying or true rate. Confidence intervals are calculated with a stated probability; for example 95% (which would indicate that there is a 95% chance that the true value lies within the confidence interval).
Mortality and Demographic Data 2012 81
Confidence intervals may assist in comparing rates over time or between different groups. If two confidence intervals do not overlap, then it is reasonable to assume that the difference is not due to chance. If two confidence intervals do overlap, it would only be possible to make any conclusion about the significance of any difference between the rates by conducting a statistical test of difference.
Note that the use of a standardised population such as the WHO World Standard Population tends to produce wider Māori confidence intervals than the use of a Māori-specific population.
82 Mortality and Demographic Data 2012

ReferencesAhmad O, Boschi-Pinto C, Lopez A, et al. 2001. Age Standardization of Rates: A new WHO standard. GPE Discussion Paper Series: No. 31. Geneva: World Health Organization.
Borman B. 1995. Standardising Rates of Disease. Wellington: Public Health Commission.
Keyfitz N. 1966. Sampling variance of standardized mortality rates. Human Biology 38: 309–17.
Ministry of Health. 2004. Ethnicity Data Protocols for the Health and Disability Sector. Wellington: Ministry of Health.
Ministry of Health. 2012. The Health of New Zealand Adults 2011/12: Key findings for the New Zealand Health Survey. Wellington: Ministry of Health.
National Centre for Classification in Health. 2008. The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification, Sixth Edition (ICD-10-AM). Sydney: National Centre for Classification in Health.
Robson B, Purdie G, Cram F, et al. 2007. Age standardisation – an indigenous standard? Emerging Themes in Epidemiology 4(3).
Smith A. 1986. The Ethnic Origins of Nations. Oxford: Blackwell Publishers Ltd.
Statistics New Zealand. 2014a. Serious Injury Outcome Indicators – Technical Report 2014. Wellington: Statistics New Zealand.
Statistics New Zealand. 2014b. Serious Injury Outcome Indicators: 2000–13. Wellington: Statistics New Zealand.
Waterhouse J, Muir C, Correa P, et al (eds). 1976. Cancer Incidence in Five Continents, Vol III. IARC Scientific Publications No. 15. Lyon, France: International Agency for Research on Cancer.
WHO. 1979. Medical Certification of Cause of Death: Instruction for physicians on use of international form of medical certificate of cause of death. Geneva: World Health Organization.
WHO. 2004. International Classification of Diseases (ICD), Tenth Revision. Geneva: World Health Organization.
Mortality and Demographic Data 2012 83