motor control of the spine in acute, recurrent and chronic ... · impairments, adaptations, and...
TRANSCRIPT

12/9/2013
1
Motor Control of the Spine in Acute, Recurrent and Chronic LBP:
Impairments, Adaptations, and Clinical Applications
George J Beneck, PhD, PT, OCS Jo Armour Smith, PT, MManTher, OCS
PHYSICAL FACTORS
Delitto et al., JOSPT, 2012
DEMOGRAPHIC FACTORS
WORK/LEISURE ACTIVITY
PSYCHOSOCIAL FACTORS
INDIVIDUAL WITH LOW BACK PAIN
ANTHROPOMETRIC FACTORS
• The production of coordinated movement
• Interaction between the individual, task and environment
• Multiple systems and processes
What is motor control?
Shumway Cook & Woollacott., 2007

12/9/2013
2
• Musculoskeletal system
• Central nervous system
• Sensory/perceptual processes
• Cognitive processes
What is motor control?
Individual muscle systems
How may motor control be altered?
• Amplitude of muscle activity
• Timing of muscle activity
• Muscle co-contraction
• Adaptability of muscle activation
Altered motion

12/9/2013
3
How may motor control be altered?
• Adaptability = variability
• Some variability is associated with stable performance of a task
• Allows individual to achieve task under changing environmental conditions and task constraints
• Altered variability is associated with ageing and some musculoskeletal disorders
How may motor control be adapted?
PAIN
SPASM ISCHEMIA
PAIN
AGONIST ANTAGONIST
• Some consistent adaptations across individuals • Some inconsistent adaptations between individuals • Complex due to redundancy of trunk muscle system
Motor control and low back pain
Delitto et al., JOSPT, 2012
ACUTE/SUB-ACUTE LBP
RECURRENT LBP
RECURRENT LBP
RECURRENT LBP
CHRONIC LBP
TIME
12/9/2013
4
INDIVIDUAL MUSCLE SYSTEMS INTEGRATED SPINAL CONTROL
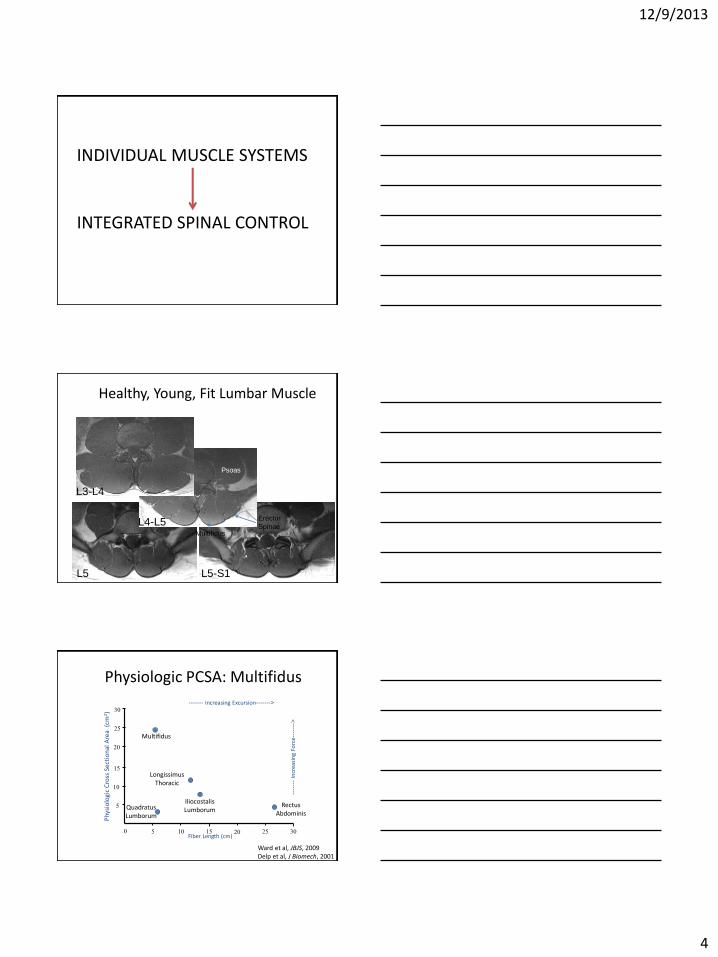
Healthy, Young, Fit Lumbar Muscle
L5-S1 L5
L4-L5
L3-L4
Psoas
Multifidus
Erector
Spinae
Physiologic PCSA: Multifidus
25
0
10
5
5 15 10 20 25 30 Fiber Length (cm)
Phy
sio
logi
c C
ross
Sec
tio
nal
Are
a (
cm2)
------- Increasing Excursion------->
----
---
Incr
easi
ng
Forc
e---
----
>
Rectus Abdominis
Longissimus Thoracic
Iliocostalis Lumborum
Multifidus
15
20
30
Ward et al, JBJS, 2009 Delp et al, J Biomech, 2001
Quadratus Lumborum
12/9/2013
5
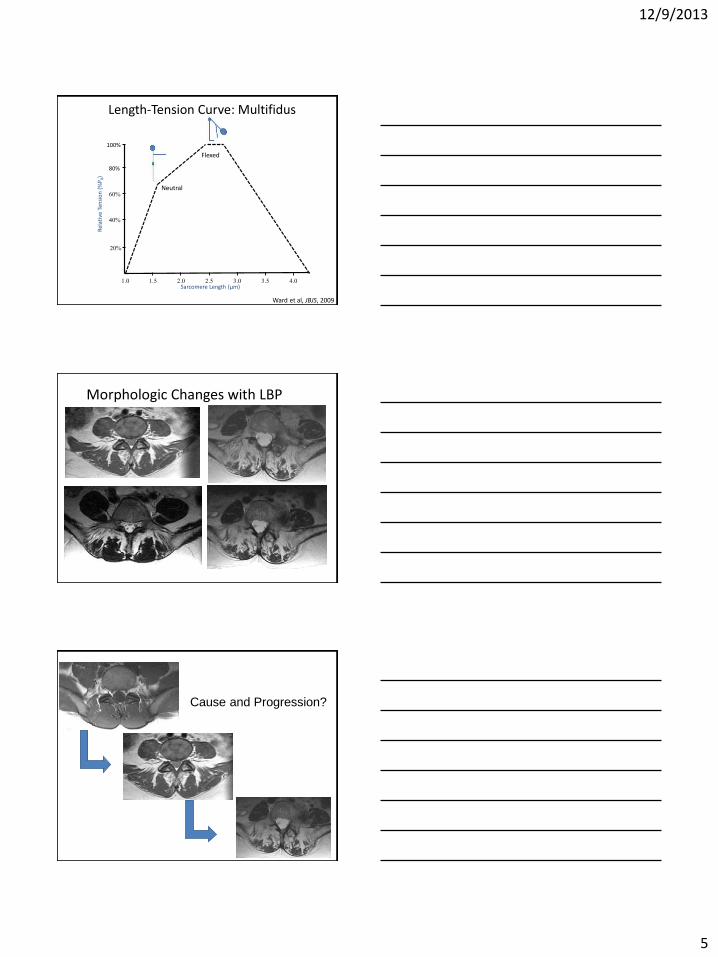
Length-Tension Curve: Multifidus
80%
60%
1.0
40%
20%
1.5 2.5 2.0 3.0 3.5 4.0 Sarcomere Length (µm)
Rel
ativ
e Te
nsi
on
(%
P0)
100%
Neutral
Flexed
Ward et al, JBJS, 2009
Morphologic Changes with LBP
Cause and Progression?

12/9/2013
6
Atrophy & Fat Replacement
• When? – Acute? – Subacute? – Chronic?
• Where? – Generalized? – Unilateral or bilateral? – 1 segments? 5 segments?
• Why? – Reflex inhibition? – Deconditioning? – Denervation? – Aging? – Surgical procedures?
Morphologic Changes with LBP
• Acute unilateral LBP – mean symptom duration: 13 days
– Atrophy at painful side and segment
• 31% reduced cross-sectional area (CSA) - unilateral
Hides et al, Spine, 1994 Ultrasound Images
Hides et al, JOSPT, 2008
Morphologic Changes with LBP
Early Chronic Unilateral LBP (Ave: 3 months)
– Painful side and segment: 21% reduced CSA
Barker et al, Spine, 2004
12/9/2013
7
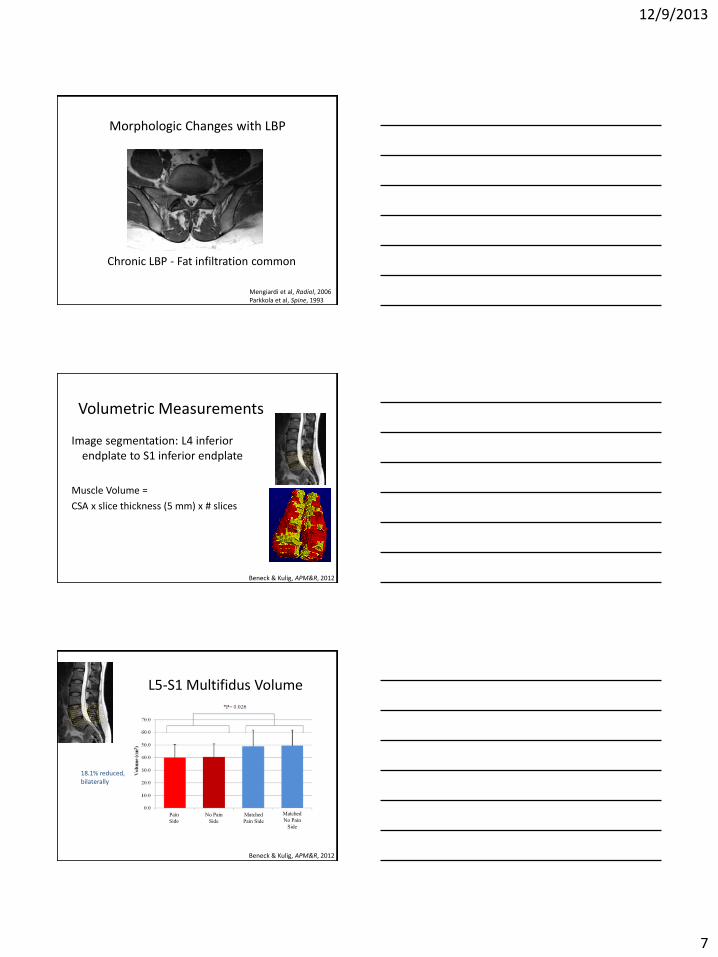
Morphologic Changes with LBP
Chronic LBP - Fat infiltration common
Mengiardi et al, Radiol, 2006 Parkkola et al, Spine, 1993
Volumetric Measurements
Image segmentation: L4 inferior endplate to S1 inferior endplate
Muscle Volume =
CSA x slice thickness (5 mm) x # slices
Beneck & Kulig, APM&R, 2012
L5-S1 Multifidus Volume
18.1% reduced, bilaterally
No Pain
Side
Matched
No Pain
Side
Pain
Side
Matched
Pain Side
Beneck & Kulig, APM&R, 2012
12/9/2013
8
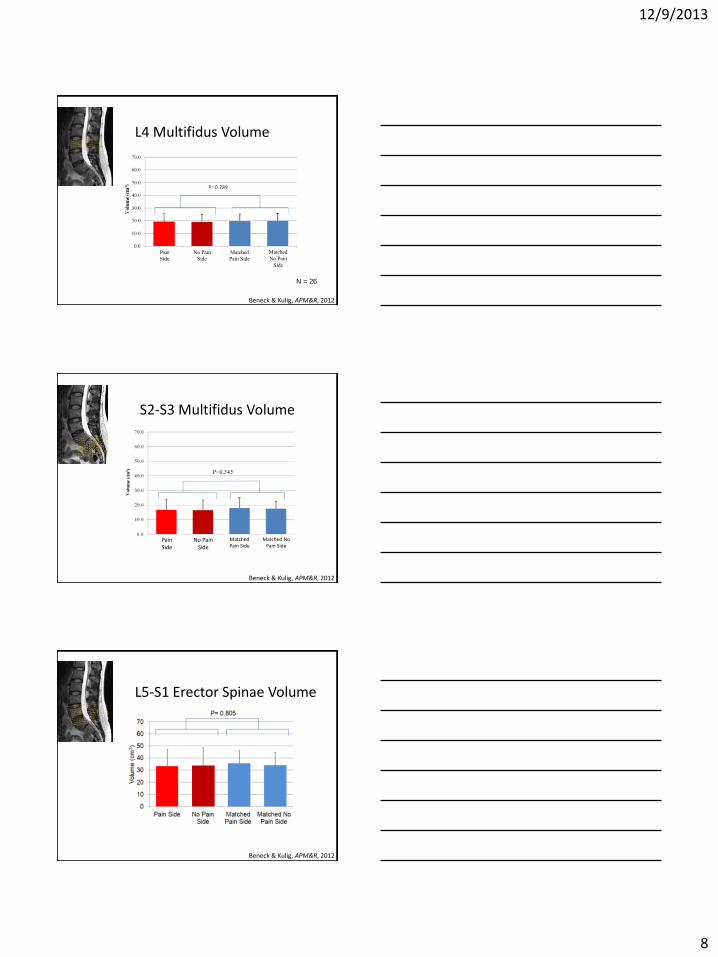
L4 Multifidus Volume
N = 26
No Pain
Side
No Pain
Side
Matched
No Pain
Side
Pain
Side
Matched
Pain Side
Beneck & Kulig, APM&R, 2012
S2-S3 Multifidus Volume
No Pain
Side No Pain
Side
Matched No Pain Side
Pain Side
Matched Pain Side
Beneck & Kulig, APM&R, 2012
L5-S1 Erector Spinae Volume
Beneck & Kulig, APM&R, 2012
12/9/2013
9
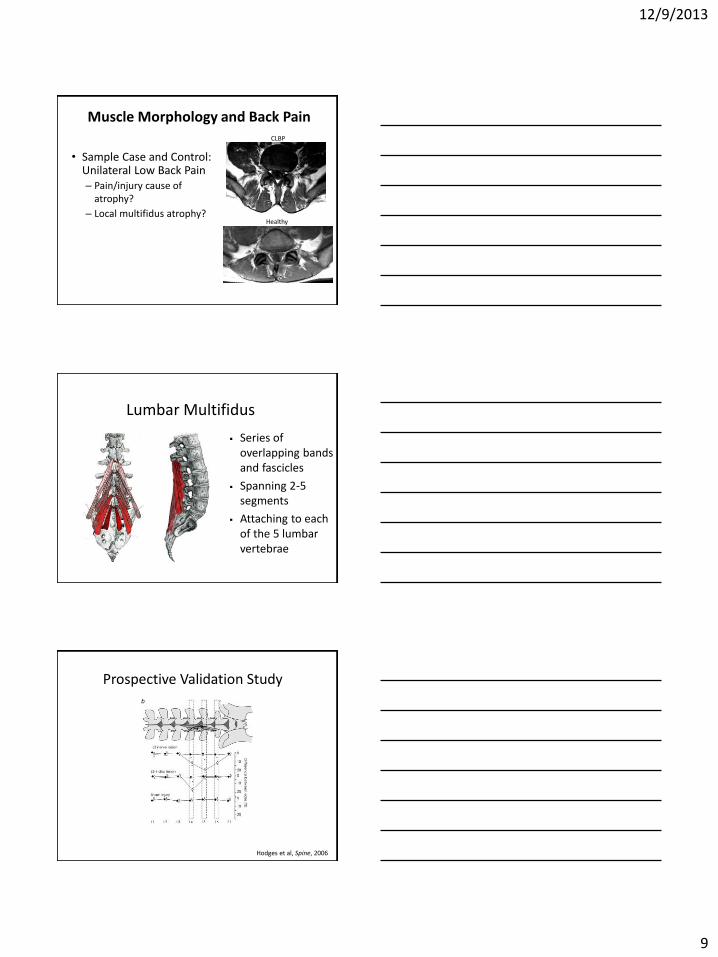
Muscle Morphology and Back Pain
• Sample Case and Control: Unilateral Low Back Pain – Pain/injury cause of
atrophy? – Local multifidus atrophy?
Healthy
CLBP
Lumbar Multifidus
Series of overlapping bands and fascicles
Spanning 2-5 segments
Attaching to each of the 5 lumbar vertebrae
Prospective Validation Study
Hodges et al, Spine, 2006

12/9/2013
10
Prospective Validation Study
Atrophy of deep fibers? Intervertebral Disc
Fat Infiltration
Multifidus
Campbell et al, Muscle & Nerve, 1998 Kader et al, Clin Radiol, 2000 Hodges et al, Spine, 2006
Deep Fibers = Short Fibers
Multifidus Atrophy Localized to Painful Region
L5
L5
T12 T12
Healthy: matched for age, size and activity
Low Back Pain

12/9/2013
11
Back Extensor Fatigability
• Low Endurance
–Associated with LBP1-5
–A Risk Factor for LBP6-8
Sorensen test: max holding time
1. Crossman, Spine, 2004 2. Nourbakhsh, JOSPT, 2002 3. Mannion, J Rehab Res & Dev, 1997 4. Tsuboi, Appl Physiol Occup Physiol, 1994 5. Nicolaisen, Scand J Rehab Med, 1985 6. Adams, Spine, 1999 7. Alaranta, Clin Biomech, 1995 8. Biering-Sorensen, Spine, 1984
Back Extensor Endurance
• Sorensen Test Limitations
– 37% stopped for reasons other than fatigue1
• EMG fatigue testing
Hz 50 100 150 200 250 300 350 400 450 500
300 250 200 150 100 50
Power Spectral Analysis
Ropponen et al, JOSPT, 2005
MF Slope
• The median frequencies are plotted over time. • The slope is the best-fit line of the median
frequencies.

12/9/2013
12
30 Second Hold
-0.70
-0.60
-0.50
-0.40
-0.30
-0.20
-0.10
0.00
No
rmali
zed
Med
ian
Fre
qu
en
cy S
lop
e,
Mean
(S
EM
)
P=0.650
Deep Multifidus
Superficial Multifidus
Thoracic Longissimus
Lumbar Longissimus
Beneck et al, J Electromyogr Kinesiol, 2013
Results – Low Back Pain
-0.70
-0.60
-0.50
-0.40
-0.30
-0.20
-0.10
0.00
No
rmal
ized
Med
ian
Fre
qu
ency
Sl
op
e, M
ean
(SE
M)
Deep Multifidus
Superficial Multifidus
Thoracic Longissimus
Lumbar Longissimus
P=0.013 Simple Contrasts
P=0.135
P=0.114
DM vs TES
SM vs TES
LES vs TES
First 30 sec
Last 30 sec
* * * * * * *
*
P=0.008 Main Effect, Time P=0.027 Interaction, Time x Muscle
Beneck et al, J Electromyogr Kinesiol, 2013
Slope Change: Deep Multifidus
Time (sec)
0 - 30 0 - 30
Time (sec)
100 100
Rela
tive c
han
ge
Rela
tive c
han
ge
CLBP Healthy
Beneck et al, J Electromyogr Kinesiol, 2013
12/9/2013
13
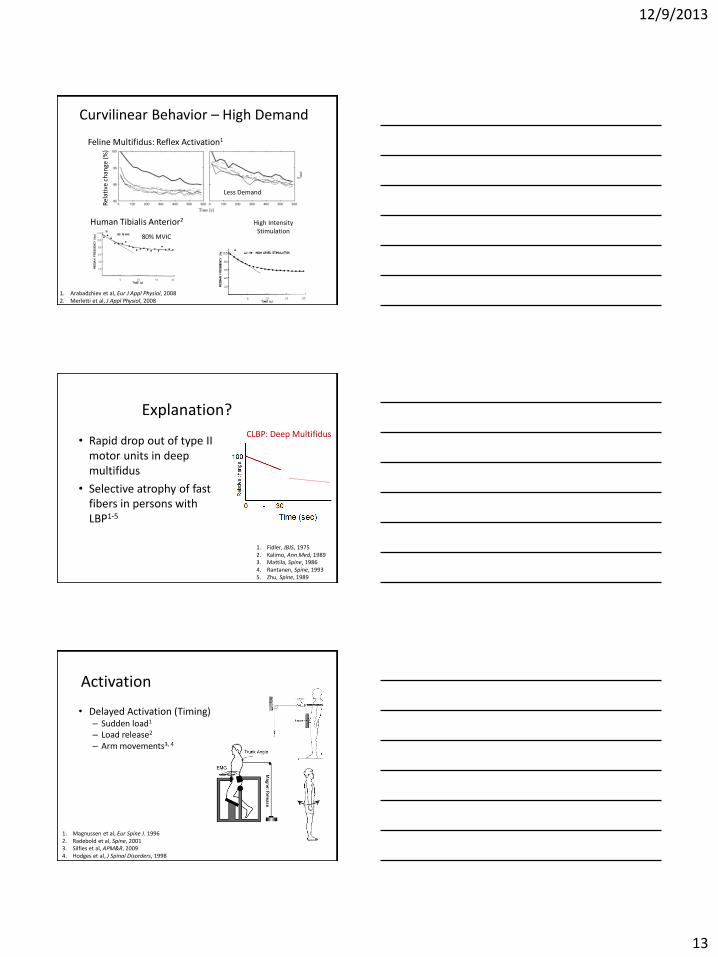
Curvilinear Behavior – High Demand
Feline Multifidus: Reflex Activation1
Human Tibialis Anterior2
80% MVIC
High Intensity Stimulation
Less Demand
1. Arabadzhiev et al, Eur J Appl Physiol, 2008 2. Merletti et al, J Appl Physiol, 2008
Rel
ativ
e ch
ange
(%
)
Explanation?
• Rapid drop out of type II motor units in deep multifidus
• Selective atrophy of fast fibers in persons with LBP1-5
CLBP: Deep Multifidus
1. Fidler, JBJS, 1975 2. Kalimo, Ann Med, 1989 3. Mattila, Spine, 1986 4. Rantanen, Spine, 1993 5. Zhu, Spine, 1989
Activation
• Delayed Activation (Timing) – Sudden load1 – Load release2 – Arm movements3, 4
1. Magnussen et al, Eur Spine J. 1996 2. Radebold et al, Spine, 2001 3. Silfies et al, APM&R, 2009 4. Hodges et al, J Spinal Disorders, 1998

12/9/2013
14
Influence of Anticipation on Activation
• Self-initiated
–Rapid Arm Movements1
• Feedforward activation – deep fibers only
– Loading2
• Earlier activation
• Feedforward activation – deep fibers only
1. Moseley & Hodges, Spine, 2002 2. Moseley et al, J Physiol, 2003
Impaired Activation with Recurrent LBP
• Rapid Arm Movements1 – Onset time delayed (20 ms) only
in deep fibers on side of LBP
• Loading Response – Anticipation did not result in
earlier activation in patients with disc herniation2
– Bilateral reduction in amplitudes in deep fibers prior to load release with unilateral LBP3.
1. MacDonald et al, Pain, 2009 2. Leinonen et al, Spine, 2001 3. MacDonald et al, Spine, 2010
Physiologic PCSA: Psoas
25
0
10
5
5 15 10 20 25 30 Fiber Length (cm)
Physio
log
ic C
ross S
ectional A
rea
(cm
2) ------- Increasing Excursion------->
----
---
Incre
asin
g F
orc
e--
----
->
Rectus
Abdominis
Longissimus
Thoracic
Iliocostalis
Lumborum
Multifidus
15
20
30
Quadratus
Lumborum
Regev et al, Spine, 2011
Psoas
12/9/2013
15
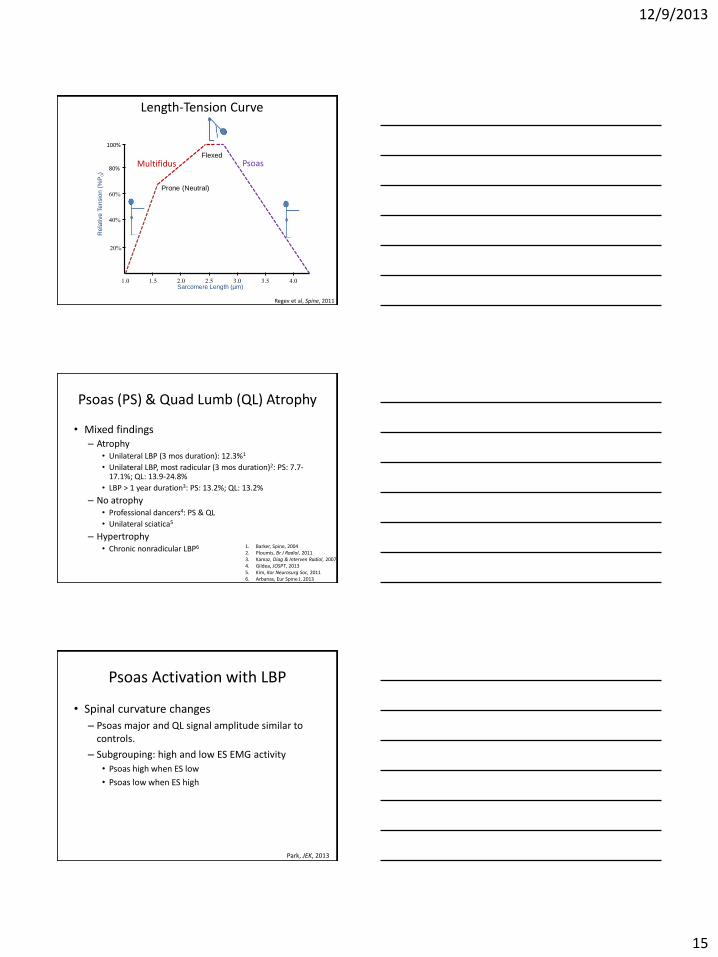
Length-Tension Curve
80%
60%
1.0
40%
20%
1.5 2.5 2.0 3.0 3.5 4.0 Sarcomere Length (µm)
Re
lative
Te
nsio
n (
%P
0)
100%
Prone (Neutral)
Flexed
Multifidus Psoas
Regev et al, Spine, 2011
Psoas (PS) & Quad Lumb (QL) Atrophy
• Mixed findings – Atrophy
• Unilateral LBP (3 mos duration): 12.3%1
• Unilateral LBP, most radicular (3 mos duration)2: PS: 7.7-17.1%; QL: 13.9-24.8%
• LBP > 1 year duration3: PS: 13.2%; QL: 13.2%
– No atrophy • Professional dancers4: PS & QL
• Unilateral sciatica5
– Hypertrophy • Chronic nonradicular LBP6 1. Barker, Spine, 2004
2. Ploumis, Br J Radiol, 2011 3. Kamaz, Diag & Interven Radiol, 2007 4. Gildea, JOSPT, 2013 5. Kim, Kor Neurosurg Soc, 2011 6. Arbanas, Eur Spine J, 2013
Psoas Activation with LBP
• Spinal curvature changes
– Psoas major and QL signal amplitude similar to controls.
– Subgrouping: high and low ES EMG activity
• Psoas high when ES low
• Psoas low when ES high
Park, JEK, 2013
12/9/2013
16
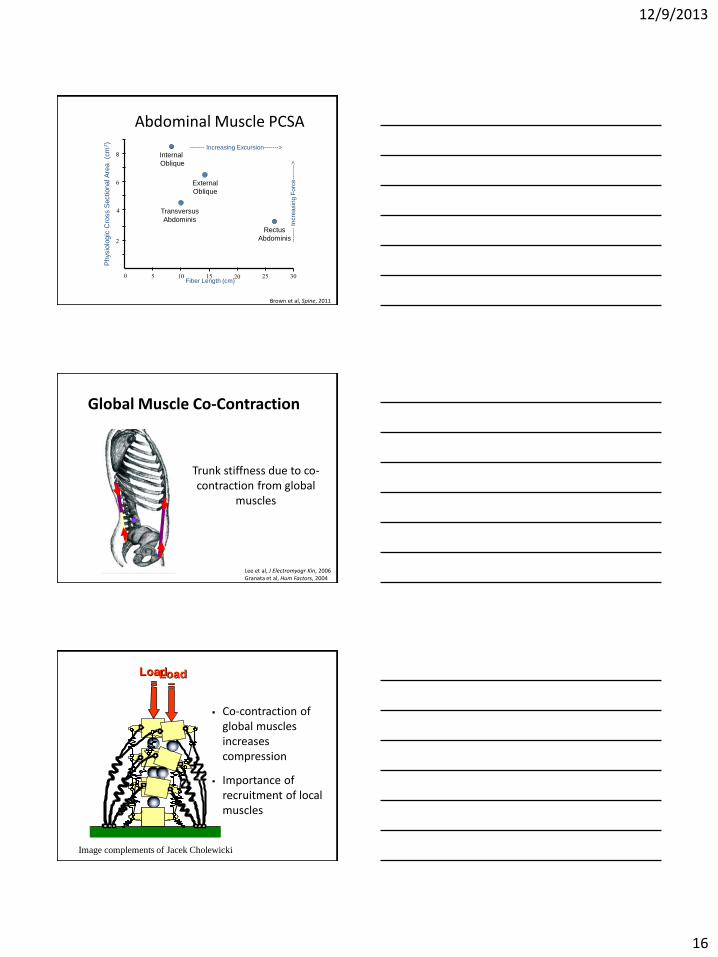
Abdominal Muscle PCSA
Brown et al, Spine, 2011
8
6
0
4
2
5 15 10 20 25 30 Fiber Length (cm)
Physio
log
ic C
ross S
ectional A
rea
(cm
2)
------- Increasing Excursion------->
----
---
Incre
asin
g F
orc
e--
----
->
Rectus
Abdominis
Transversus
Abdominis
External
Oblique
Internal
Oblique
Trunk stiffness due to co-contraction from global
muscles
Global Muscle Co-Contraction
Lee et al, J Electromyogr Kin, 2006 Granata et al, Hum Factors, 2004
Load Load
Co-contraction of global muscles increases compression
Importance of recruitment of local muscles
Image complements of Jacek Cholewicki
12/9/2013
17
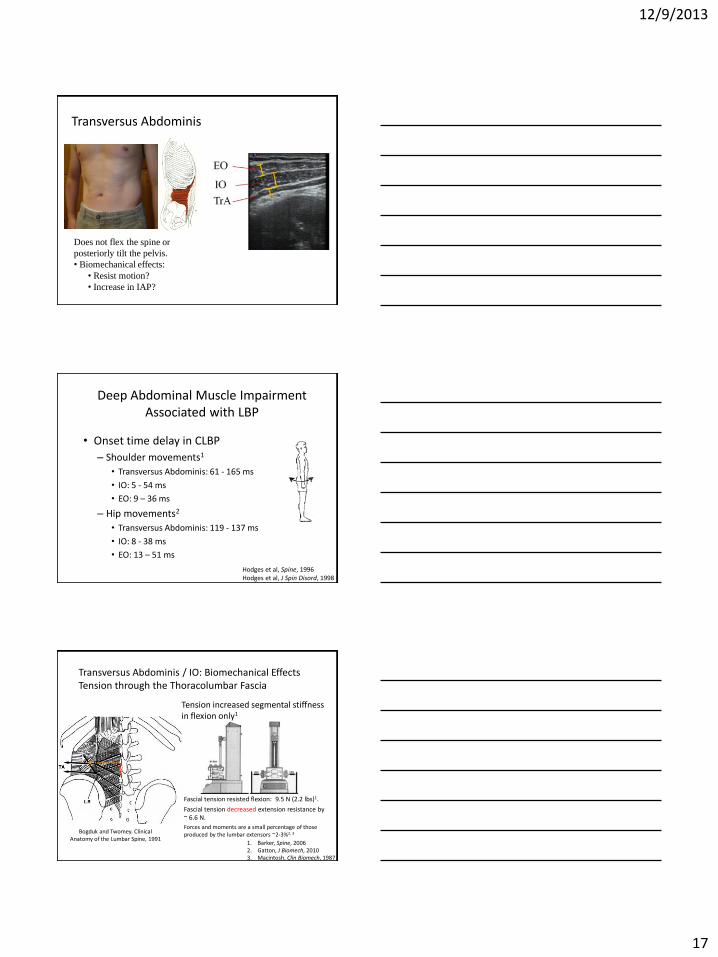
Transversus Abdominis
Does not flex the spine or
posteriorly tilt the pelvis.
• Biomechanical effects:
• Resist motion?
• Increase in IAP?
Deep Abdominal Muscle Impairment Associated with LBP
• Onset time delay in CLBP
– Shoulder movements1
• Transversus Abdominis: 61 - 165 ms
• IO: 5 - 54 ms
• EO: 9 – 36 ms
– Hip movements2
• Transversus Abdominis: 119 - 137 ms
• IO: 8 - 38 ms
• EO: 13 – 51 ms
Hodges et al, Spine, 1996 Hodges et al, J Spin Disord, 1998
Bogduk and Twomey. Clinical Anatomy of the Lumbar Spine, 1991
Tension increased segmental stiffness in flexion only1
Fascial tension resisted flexion: 9.5 N (2.2 lbs)1.
Fascial tension decreased extension resistance by ~ 6.6 N.
Forces and moments are a small percentage of those produced by the lumbar extensors ~2-3%2, 3
Transversus Abdominis / IO: Biomechanical Effects Tension through the Thoracolumbar Fascia
1. Barker, Spine, 2006 2. Gatton, J Biomech, 2010 3. Macintosh, Clin Biomech, 1987
12/9/2013
18
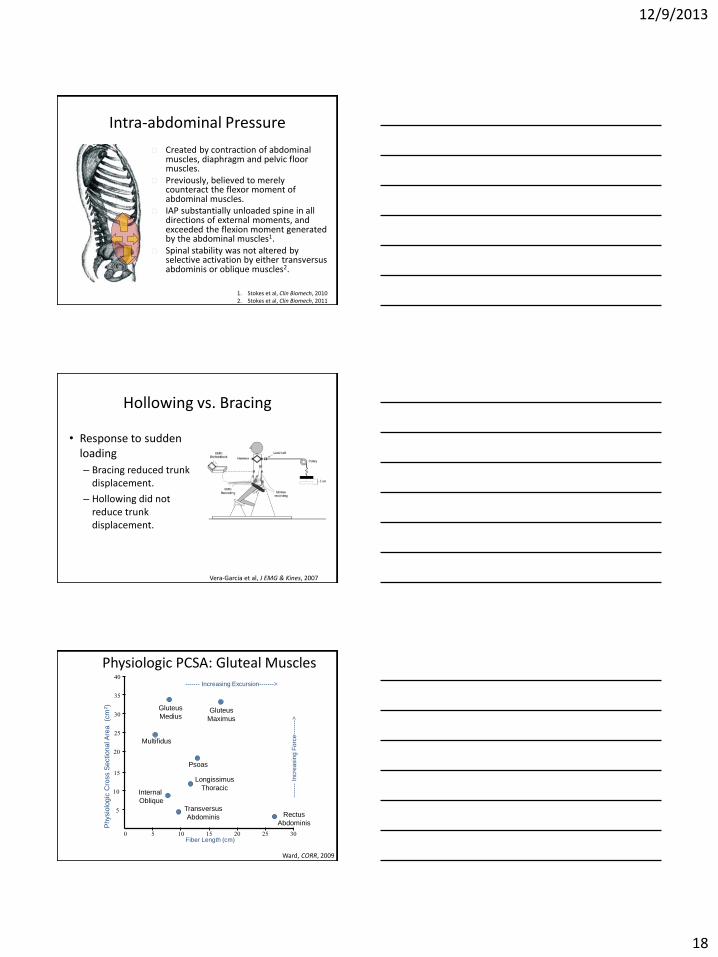
Intra-abdominal Pressure
Created by contraction of abdominal muscles, diaphragm and pelvic floor muscles.
Previously, believed to merely counteract the flexor moment of abdominal muscles.
IAP substantially unloaded spine in all directions of external moments, and exceeded the flexion moment generated by the abdominal muscles1.
Spinal stability was not altered by selective activation by either transversus abdominis or oblique muscles2.
1. Stokes et al, Clin Biomech, 2010 2. Stokes et al, Clin Biomech, 2011
Hollowing vs. Bracing
• Response to sudden loading
– Bracing reduced trunk displacement.
– Hollowing did not reduce trunk displacement.
Vera-Garcia et al, J EMG & Kines, 2007
Physiologic PCSA: Gluteal Muscles
25
0
10
5
5 15 10 20 25 30 Fiber Length (cm)
Physio
log
ic C
ross S
ectional A
rea
(cm
2)
------- Increasing Excursion------->
----
---
Incre
asin
g F
orc
e--
----
->
Rectus
Abdominis
Longissimus
Thoracic
Multifidus
15
20
30
Ward, CORR, 2009
Psoas
35
40
Internal
Oblique Transversus
Abdominis
Gluteus
Medius Gluteus
Maximus
12/9/2013
19
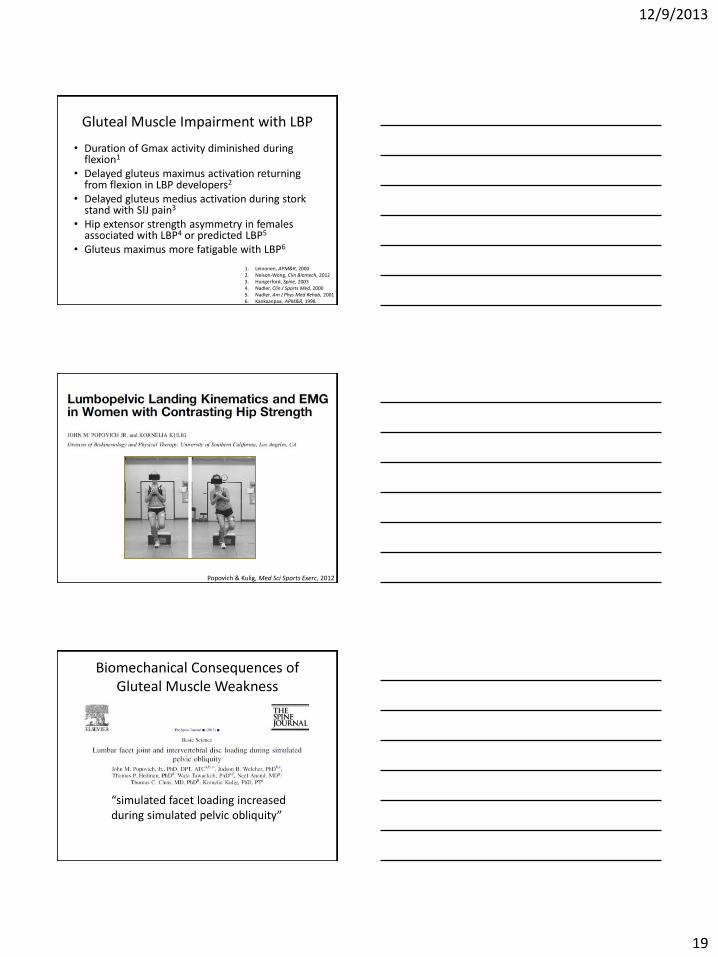
Gluteal Muscle Impairment with LBP
• Duration of Gmax activity diminished during flexion1
• Delayed gluteus maximus activation returning from flexion in LBP developers2
• Delayed gluteus medius activation during stork stand with SIJ pain3
• Hip extensor strength asymmetry in females associated with LBP4 or predicted LBP5
• Gluteus maximus more fatigable with LBP6
1. Leinonen, APM&R, 2000 2. Nelson-Wong, Clin Biomech, 2012 3. Hungerford, Spine, 2003 4. Nadler, Clin J Sports Med, 2000 5. Nadler, Am J Phys Med Rehab, 2001 6. Kankaanpaa, APM&R, 1998
Popovich & Kulig, Med Sci Sports Exerc, 2012
Biomechanical Consequences of Gluteal Muscle Weakness
“simulated facet loading increased during simulated pelvic obliquity”
12/9/2013
20
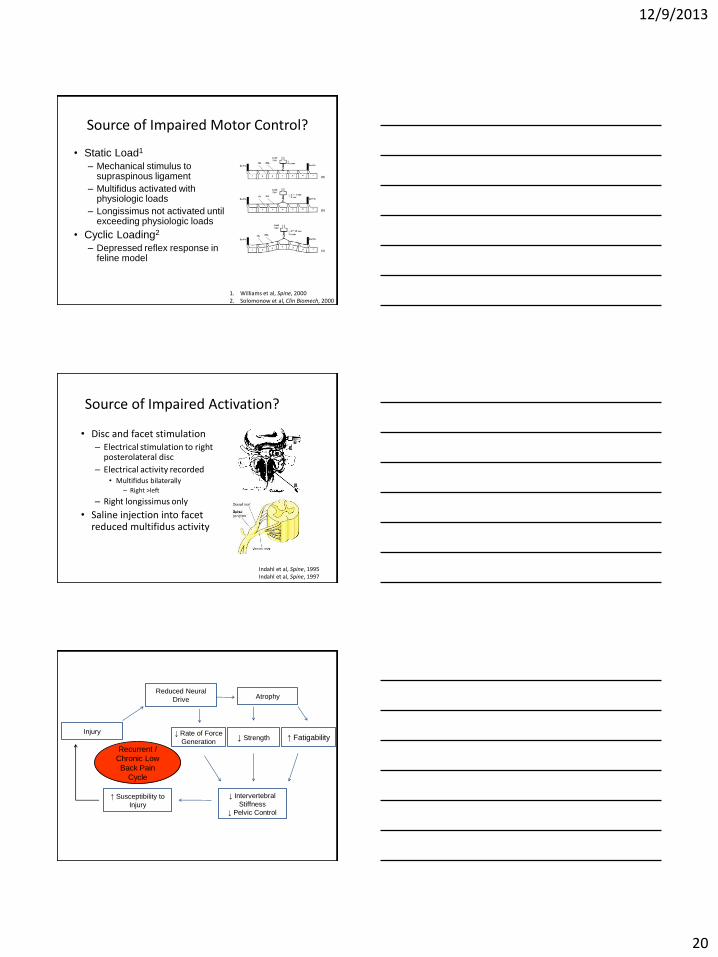
Source of Impaired Motor Control?
• Static Load1
– Mechanical stimulus to supraspinous ligament
– Multifidus activated with physiologic loads
– Longissimus not activated until exceeding physiologic loads
• Cyclic Loading2
– Depressed reflex response in feline model
1. Williams et al, Spine, 2000 2. Solomonow et al, Clin Biomech, 2000
Source of Impaired Activation?
• Disc and facet stimulation – Electrical stimulation to right
posterolateral disc
– Electrical activity recorded • Multifidus bilaterally
– Right >left
– Right longissimus only
• Saline injection into facet reduced multifidus activity
Indahl et al, Spine, 1995 Indahl et al, Spine, 1997
Recurrent /
Chronic Low
Back Pain
Cycle
Injury
Reduced Neural
Drive Atrophy
↑ Fatigability ↓ Strength ↓ Rate of Force
Generation
↓ Intervertebral
Stiffness
↓ Pelvic Control
↑ Susceptibility to
Injury

12/9/2013
21
Source of Impaired Activation?
• Cortical Inhibition? – Porcine Model – Acute Injury1
• MEPs (cortical motor-evoked potentials) recorded in deep and superficial multifidus at L3-5 at side of IV disc lesion.
• MEP amplitudes increased (36%), not decreased on the side of the disc lesion.
• Increased corticomotor excitability suggests a compensatory response to reduced excitability at the spinal cord.
– Reduced cortical excitability in humans with chronic low back pain2
1. Hodges, Eur J Neurosci, 2009 2. Strutton et al, J Spin Disord & Tech, 2005
Source of Impaired Activation?
• Cortical Changes?
– Using TMS mapping, fascicles of
multifidus and erector spinae are
controlled by discrete neuronal regions
within the motor cortex1
– Loss of discrete organization of lumbar
extensors in persons with recurrent LBP2 1. Tsao et al, Clin Neurophys, 2011 2. Tsao et al, Spine, 2011
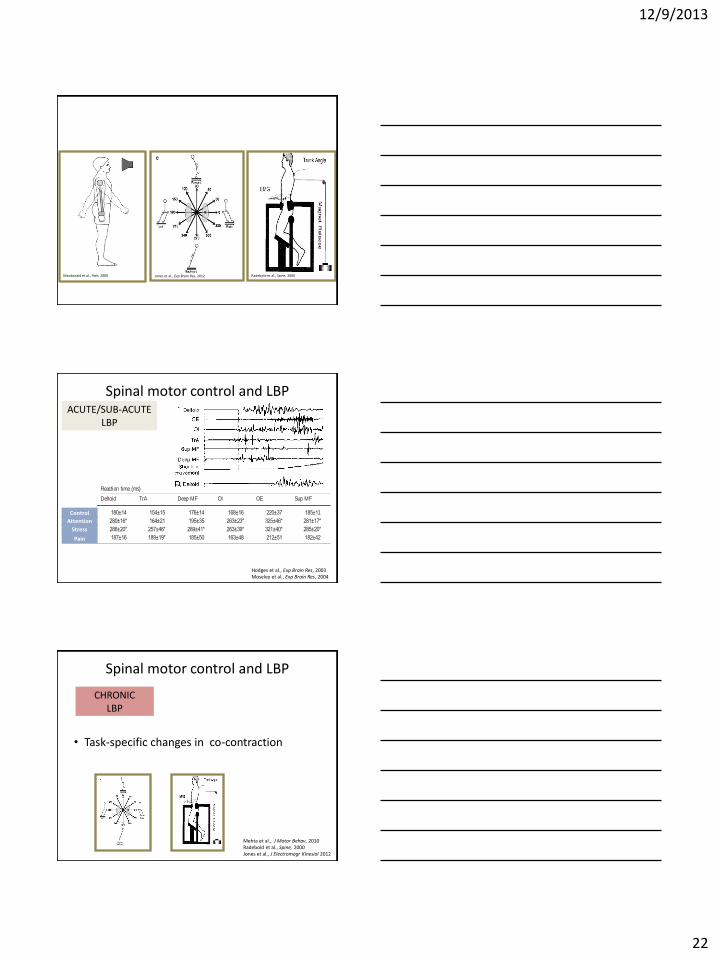
How do we assess integrated spinal motor control?
1) Postural perturbations
• Anticipated/unanticipated
• Postural control
• Mid-range spinal motion
Macdonald et al., Pain, 2009
12/9/2013
22
Macdonald et al., Pain, 2009 Jones et al., Exp Brain Res, 2012 Radebold et al., Spine, 2000
Spinal motor control and LBP ACUTE/SUB-ACUTE
LBP
Hodges et al., Exp Brain Res, 2003 Moseley et al., Exp Brain Res, 2004
Control
Attention
Stress
Pain
acceleration again entered simultaneously asacovariate, wasused tocompare themean rectified EMG amplitude for each epoch, for eachmuscle, between conditions. Post hoc testing of EMG onset latencybetween conditions, and the epoch data between conditions, wasundertaken with Duncan’s multiple range test. Significance was setat the 0.05% level of probability.
Results
Stress and pain
Figure 2A–C demonstrates the reported distress and pain,HR and GSR during the control and experimentalconditions. No subjects reported a change in back painduring arm movements. All three measures were greaterduring thestressful task and pain than during theattention-demanding task and control (P<0.01 for both). There wereno differences in these measures between control and theattention-demanding task. Taken together, these measuresindicate that the experimental protocol was effective atselectively targeting attention-demand and stress.
Arm movements
There was no difference in peak shoulder accelerationbetween conditions (P>0.53 for all), which suggests thatthe task was performed in a similar manner during eachcondition. Less than 15% of trials for each subject wereexcluded or rejected because of difficulty in detectingonset. Raw EMG from a representative subject (Fig. 3)and group data (Fig. 4) for the control and experimentalconditions show the general effects of attention-demand,stressful attention-demand and pain on themovement task.The mean ±SD latency of the onset of deltoid and trunkmuscle activation is presented in Table 1. Attention-demand caused an increase in the RT of the task (asevidenced by increased RT of arm movement and deltoidEMG) (P<0.01), but had no effect on activation of thedeep trunk muscles. Stressful attention-demand caused asimilar increase in the RT of the task but also caused adelay in response of the deep trunk muscles (P<0.01)(Fig. 4A). Therefore, relative to the onset of deltoid EMG,the deep trunk muscles were active earlier during atten-tion-demand than during the other conditions (P<0.01).During pain, RT of deltoid and the superficial trunk
Fig. 2 A Means±SD for reported distress (circles) and pain (boxes)during the control and experimental conditions assessed on 11-pointnumerical rating scales (NRS). B Means ±SD for heart rate (HR) asa proportion of mean HR during the control trials, for theexperimental conditions. C Mean ±SD for galvanic skin response
Table 1 Mean ±SD reaction time of deltoid and the trunk muscles (TrA transversus abdominis, Deep MF deep multifidus, OI obliquusinternus, OE obliquus externus, Sup MF superficial multifidus) during single arm movements under control and experimental conditions
Condition Reaction time (ms)
Deltoid TrA Deep MF OI OE Sup MF
Control 180±14 154±15 176±14 168±16 220±37 185±11
Attention-demand 280±16* 164±21 195±35 263±23* 325±46* 281±17*
Stress 286±20* 257±46* 289±41* 263±39* 321±40* 285±20*
Pain 187±16 189±19* 185±50 163±48 212±51 182±42
*Significant difference from control (P<0.01)
67
Mehta et al., J Motor Behav, 2010 Radebold et al., Spine, 2000 Jones et al., J Electromogr Kinesiol 2012
Spinal motor control and LBP
• Task-specific changes in co-contraction
CHRONIC LBP
12/9/2013
23
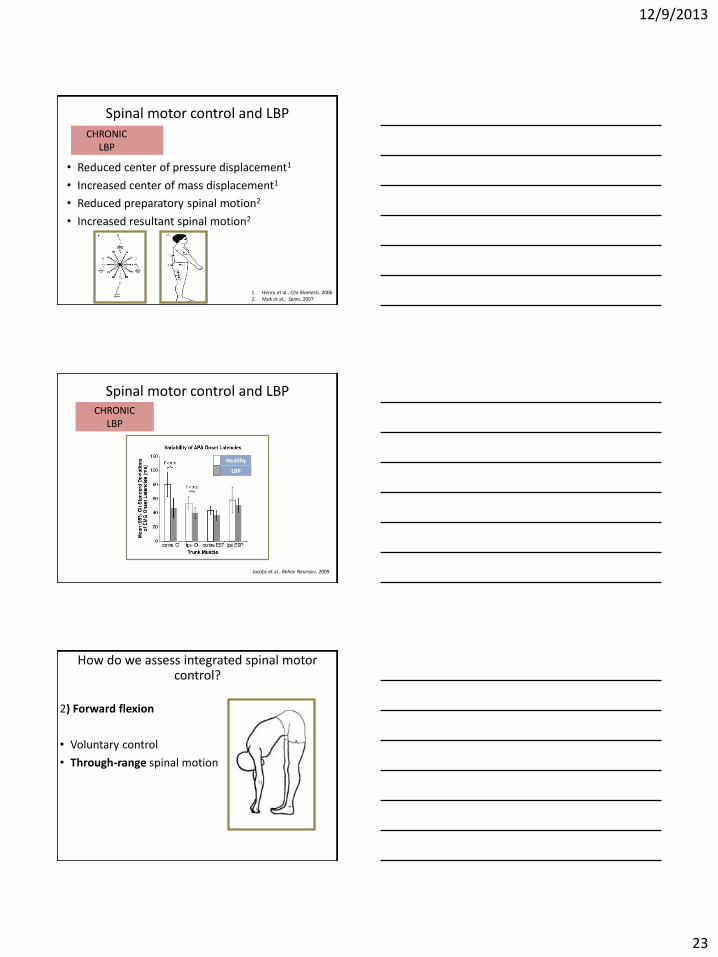
• Reduced center of pressure displacement1
• Increased center of mass displacement1
• Reduced preparatory spinal motion2
• Increased resultant spinal motion2
Spinal motor control and LBP CHRONIC LBP
1. Henry et al., Clin Biomech, 2006 2. Mok et al., Spine, 2007
Spinal motor control and LBP
Jacobs et al., Behav Neurosci, 2009
Healthy
LBP
CHRONIC LBP
2) Forward flexion
• Voluntary control
• Through-range spinal motion
How do we assess integrated spinal motor control?
12/9/2013
24
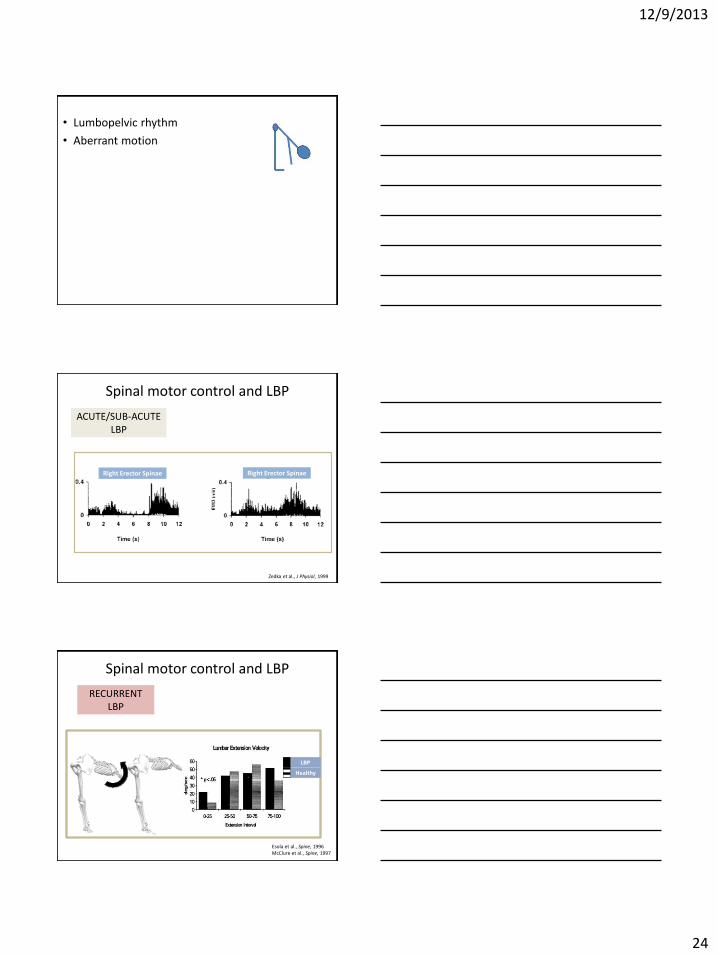
• Lumbopelvic rhythm
• Aberrant motion
Spinal motor control and LBP
ACUTE/SUB-ACUTE LBP
Zedka et al., J Physiol, 1999
Right Erector Spinae Right Erector Spinae
Esola et al., Spine, 1996 McClure et al., Spine, 1997
Spinal motor control and LBP
RECURRENT LBP
LBP
Healthy
12/9/2013
25
Leinonen et al., Arch Phys Med Rehabil, 2000
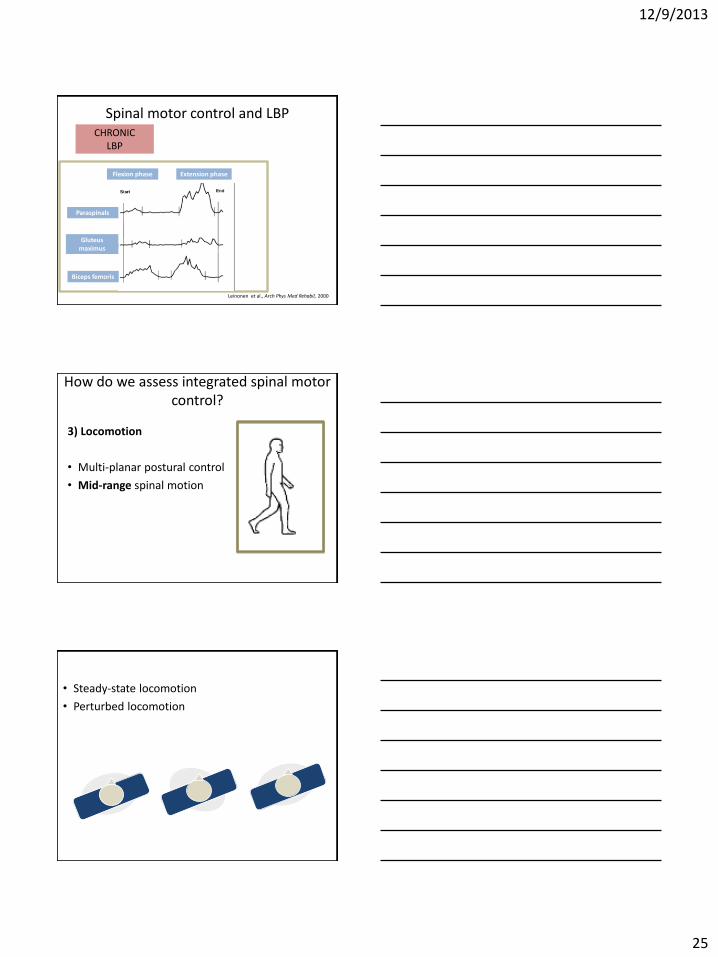
Spinal motor control and LBP CHRONIC
LBP
Flexion phase Extension phase
Paraspinals
Gluteus maximus
Biceps femoris
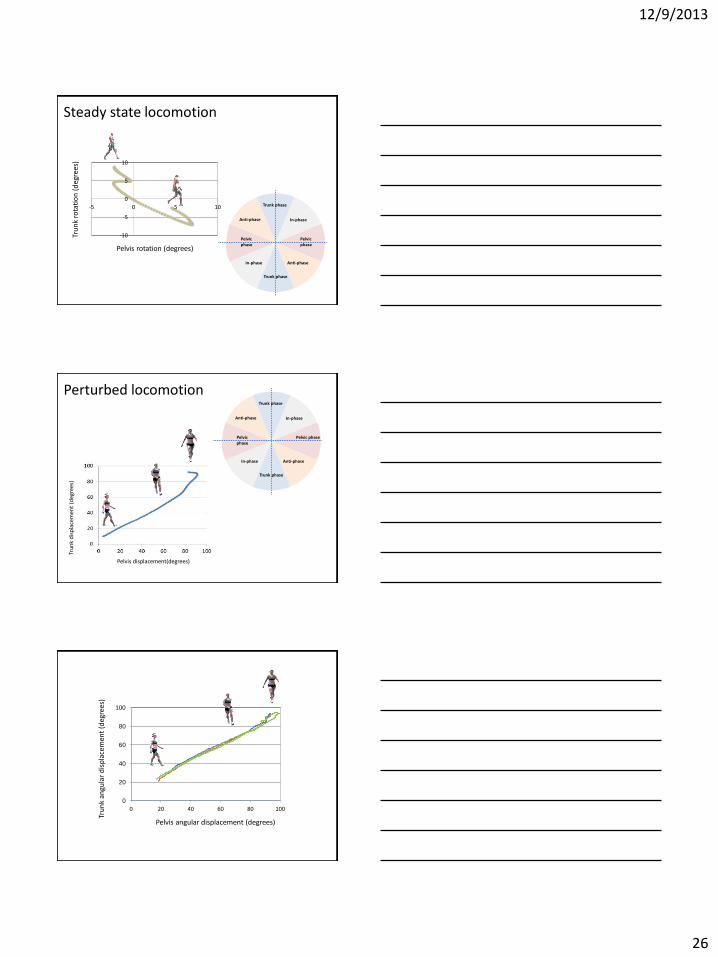
3) Locomotion
• Multi-planar postural control
• Mid-range spinal motion
How do we assess integrated spinal motor control?
• Steady-state locomotion
• Perturbed locomotion
12/9/2013
26
Pelvis rotation (degrees)
Tru
nk
rota
tio
n (
deg
rees
)
-10
-5
0
5
10
-5 0 5 10 Trunk phase
Trunk phase
Pelvic phase
Pelvic phase
In-phase
In-phase Anti-phase
Anti-phase
Steady state locomotion
Trunk phase
Trunk phase
Pelvic phase Pelvic phase
In-phase
In-phase Anti-phase
Anti-phase
Pelvis displacement(degrees)
Tru
nk
dis
pla
cem
ent
(deg
rees
)
Perturbed locomotion
0
20
40
60
80
100
0 20 40 60 80 100
Pelvis angular displacement (degrees)
Tru
nk
angu
lar
dis
pla
cem
ent
(deg
rees
)
12/9/2013
27
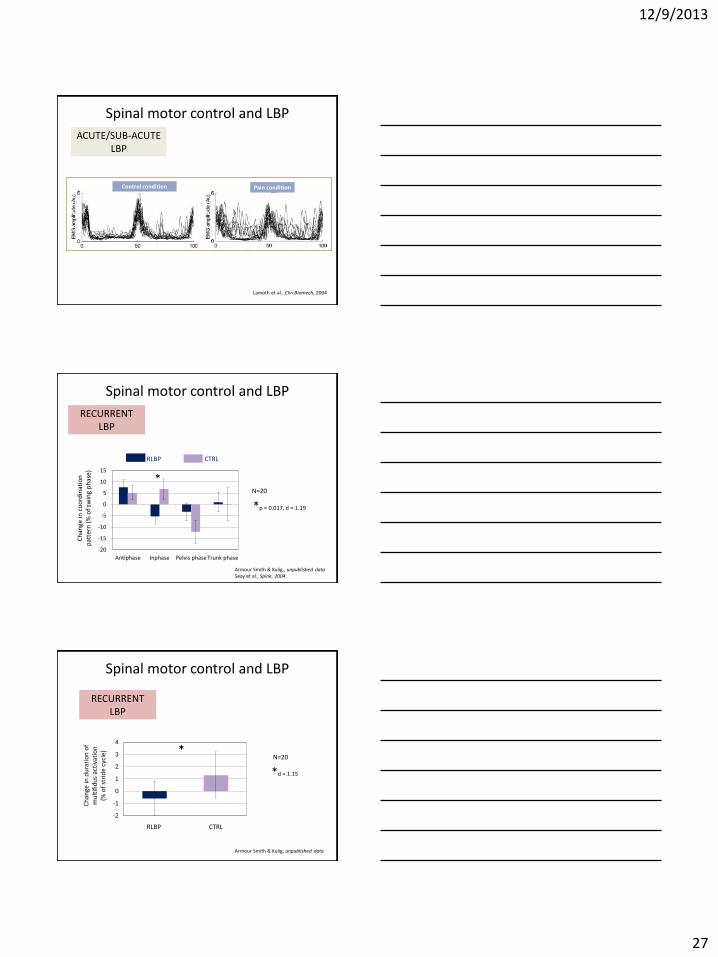
Spinal motor control and LBP
ACUTE/SUB-ACUTE LBP
Lamoth et al., Clin Biomech, 2004
Control condition Pain condition
Spinal motor control and LBP
-20
-15
-10
-5
0
5
10
15
Antiphase Inphase Pelvis phase Trunk phase
Armour Smith & Kulig., unpublished data Seay et al., Spine, 2004
RECURRENT LBP
Ch
ange
in c
oo
rdin
atio
n
pat
tern
(%
of
swin
g p
has
e)
N=20
*p = 0.017, d = 1.19
RLBP CTRL
Spinal motor control and LBP
RECURRENT LBP
-2
-1
0
1
2
3
4
N=20
Ch
ange
in d
ura
tio
n o
f m
ult
ifid
us
acti
vati
on
(%
of
stri
de
cycl
e)
RLBP CTRL
*d = 1.15
Armour Smith & Kulig, unpublished data

12/9/2013
28
Spinal motor control and LBP
CHRONIC LBP
Healthy LBP
Lamoth et al., Eur Spine J, 2006
Arendt-Nielson et al., Pain, 1996
Healthy LBP
CHRONIC LBP
Vogt et al., Man Ther, 2003
Healthy
LBP
CHRONIC LBP
Thoracic paraspinals
Lumbar paraspinals
Gluteus Maximus
Biceps Femoris
12/9/2013
29
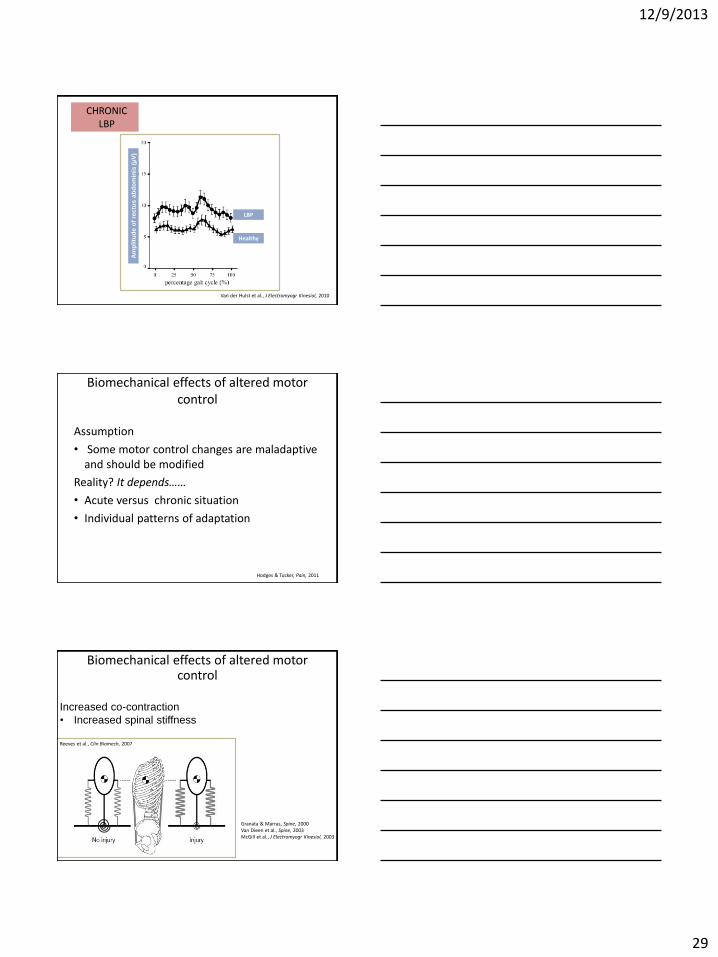
Van der Hulst et al., J Electromyogr Kinesiol, 2010
Healthy
LBP
CHRONIC LBP
Am
pli
tud
e o
f re
ctu
s a
bd
om
inis
(µ
V)
Biomechanical effects of altered motor control
Assumption
• Some motor control changes are maladaptive and should be modified
Reality? It depends……
• Acute versus chronic situation
• Individual patterns of adaptation
Hodges & Tucker, Pain, 2011
Biomechanical effects of altered motor control
Reeves et al., Clin Biomech, 2007
Increased co-contraction
• Increased spinal stiffness
Granata & Marras, Spine, 2000 Van Dieen et al., Spine, 2003 McGill et al., J Electromyogr Kinesiol, 2003

12/9/2013
30
Biomechanical effects of altered motor control
Reeves et al., Clin Biomech, 2007
Increased co-contraction
• Increased spinal load1
• Impaired postural control2,3
• Decreased damping4
1. Marras et al., Spine, 2001 2. Mok et al., Spine, 2007 3. Reeves et al., Exp Brain Research, 2006 4. Hodges et al., J Biomech, 2009
Clinical application
Can we assess • muscle morphology? • muscle activation timing? • co-contraction • altered coordination? • altered variability? • response to changing movement
patterns?
Which individuals have these problems?
• Potentially all sub-groups
• Substantial individual variability
• Equivocal findings for relationship between motor control impairments and current classification systems
• Acute/sub-acute/chronic low back pain with movement coordination impairments
Clinical presentation of LBP
Fritz et al., JOSPT, 2007 Kiesel et al., JOSPT, 2007 Silfies et al., Arch Phys Med Rehabil,2009 Zielinski et al., Arch Phys Med Rehabil,2013 Delitto et al., JOSPT, 2012
12/9/2013
31
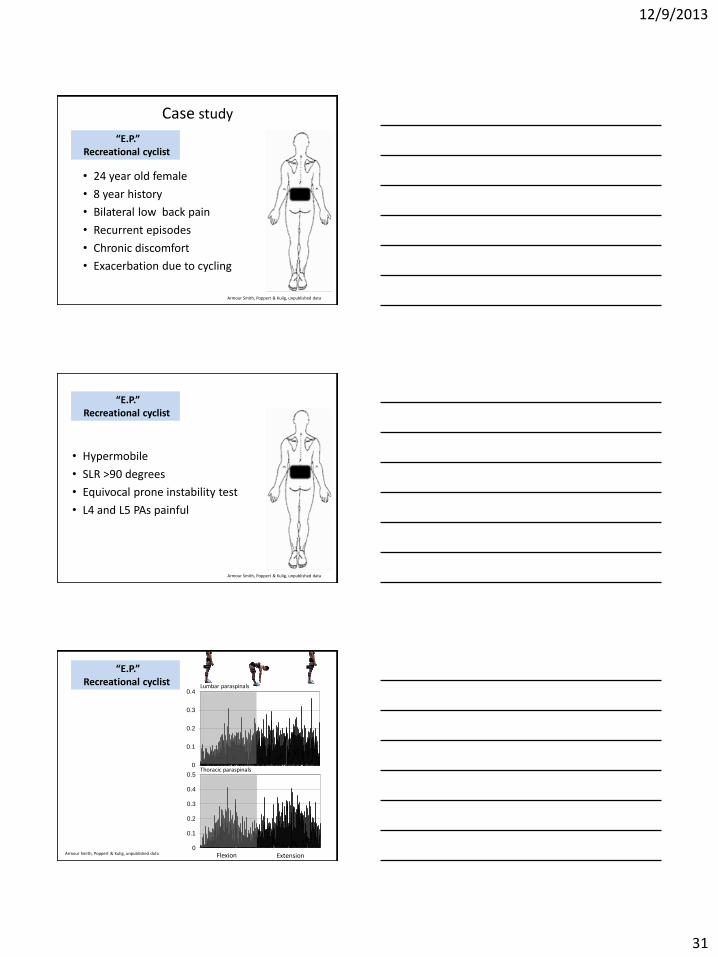
Case study
• 24 year old female
• 8 year history
• Bilateral low back pain
• Recurrent episodes
• Chronic discomfort
• Exacerbation due to cycling
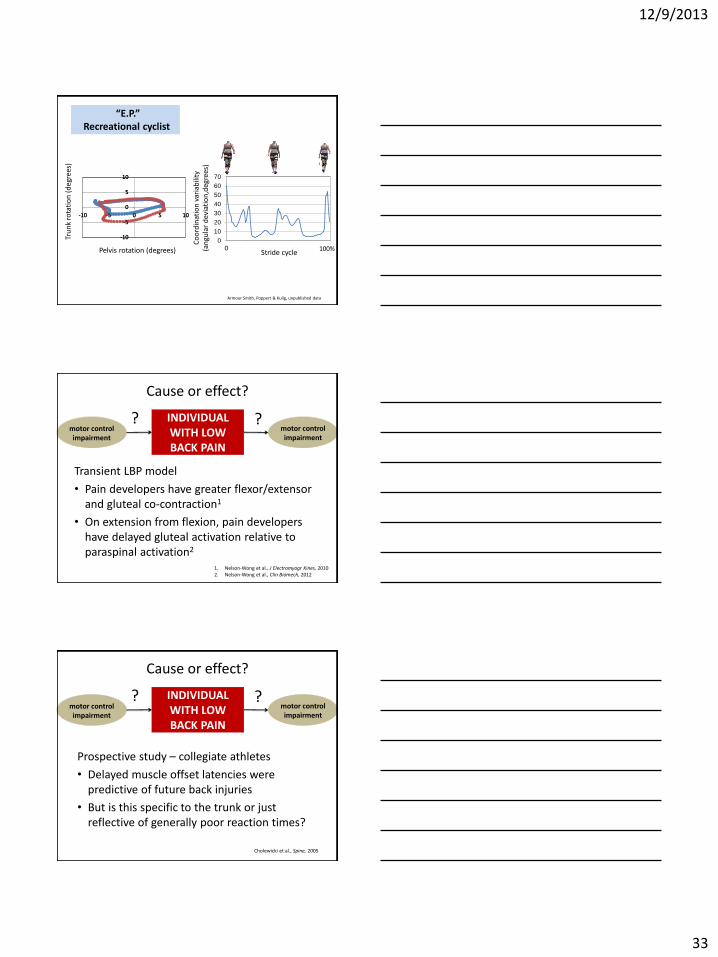
“E.P.” Recreational cyclist
Armour Smith, Poppert & Kulig, unpublished data
• Hypermobile
• SLR >90 degrees
• Equivocal prone instability test
• L4 and L5 PAs painful
“E.P.” Recreational cyclist
Armour Smith, Poppert & Kulig, unpublished data
“E.P.” Recreational cyclist
0
0.1
0.2
0.3
0.4
0
0.1
0.2
0.3
0.4
0.5
Flexion Extension Armour Smith, Poppert & Kulig, unpublished data
Lumbar paraspinals
Thoracic paraspinals

12/9/2013
32
“E.P.” Recreational cyclist
-20
0
20
40
60
80
0 10 20 30 40 50
Extension phase
Hip
an
gle
(d
eg
ree
s)
Lumbar spine angle
(degrees)
Armour Smith, Poppert & Kulig, unpublished data
“E.P.” Recreational cyclist
0 100% Stride cycle
Am
plit
ud
e
Armour Smith, Poppert & Kulig, unpublished data
“E.P.” Recreational cyclist
Pelvis rotation (degrees)
Tru
nk
rota
tio
n (
deg
rees
)
Armour Smith, Poppert & Kulig, unpublished data
-10
-5
0
5
10
-10 -5 0 5 10
-10
-5
0
5
10
-10 -5 0 5 10
12/9/2013
33
“E.P.” Recreational cyclist
-10
-5
0
5
10
-10 -5 0 5 10
Pelvis rotation (degrees)
Tru
nk
rota
tio
n (
deg
rees
)
-10
-5
0
5
10
-10 -5 0 5 10
0
10
20
30
40
50
60
70
Co
ord
inat
ion
var
iab
ility
(a
ngu
lar
dev
iati
on
,deg
rees
)
0 100% Stride cycle
Armour Smith, Poppert & Kulig, unpublished data
Cause or effect?
Transient LBP model
• Pain developers have greater flexor/extensor and gluteal co-contraction1
• On extension from flexion, pain developers have delayed gluteal activation relative to paraspinal activation2
1. Nelson-Wong et al., J Electromyogr Kines, 2010 2. Nelson-Wong et al., Clin Biomech, 2012
INDIVIDUAL WITH LOW BACK PAIN
motor control impairment
motor control impairment
? ?
Cause or effect?
INDIVIDUAL WITH LOW BACK PAIN
motor control impairment
motor control impairment
? ?
Prospective study – collegiate athletes
• Delayed muscle offset latencies were predictive of future back injuries
• But is this specific to the trunk or just reflective of generally poor reaction times?
Cholewicki et al., Spine, 2005

12/9/2013
34
Pain-spasm-pain model
PAIN
spasm ischemia
Why is motor control different in individuals with LBP?
Travell et al., JAMA, 1942 Van Dieen et al., J Electromyogr and Kines, 2003 Hodges & Tucker, Pain, 2011
Pain - adaptation model
Lund et al., Can J Physiol Pharm, 1991 Van Dieen et al., J Electromyogr and Kines, 2003 Hodges & Tucker, Pain, 2011
agonist
PAIN
antagonist
Why is motor control different in individuals with LBP?
• Adaptation specific to muscle, task, and individual
• Complex due to complexity and redundancy of trunk muscle system
Why is motor control different in individuals with LBP?
– Musculoskeletal system
– Central nervous system
– Sensory/perceptual processes
– Cognitive processes
12/9/2013
35
Sensory/perceptual and cognitive processes
CHRONIC LBP
Effects of:
• Anticipation of back pain1
• Fear avoidance2
• Diffuse impairments in body perception3
• Diffuse impairments in sensory processing3
• Altered cognitive control of motor activities4
1. Moseley et al., Brain, 2004 2. Al-Obaidi et al., Int J Rehabil Res, 2003 3. Wand et al., Man Ther, 2011 4. Lamoth et al., J NeuroEngineering Rehabil, 2008
• Delay in APA onset and reduction in variability of APA onset prolonged in some healthy subjects1
• Associated with pain beliefs1
• Altered cognitive control of locomotion in persons with CLBP2
CHRONIC LBP
1. Moseley & Hodges, Behav Neurosci, 2006 2. Lamoth et al., J NeuroEngineering Rehabil, 2008
Sensory/perceptual and cognitive processes
ACUTE/SUB-ACUTE LBP
How do we modify trunk motor control?
• Manual techniques
• Exercise interventions
• Motor (re)learning
12/9/2013
36
Extensor Activation Post Manipulation (sEMG)
• EMG amplitude decreased1
• EMG amplitude diminished at painful segment only after manipulation2
• Increase in sEMG amplitude during MVIC after manipulation3
1. DeVocht, JMPT, 2005 2. Lehman, JMPT, 2001 3. Keller, JMPT, 2000
Multifidus Post Manipulation Activation - US
Multifidus Post Manipulation Activation - US
• On average, total group (N=81) had greater activation at L4-5 at 3-4 days.
• MF increase in thickness explained only 7% of variance in ODI score
• Responders (≥30% ODI reduction) experienced significantly more activation at 3-4 days, but not immediately or 1 week later.
Koppenhaver, J Orthop Sports Phys Ther, 2011

12/9/2013
37
Multifidus Post Manipulation Activation - US
• Variables together resulted in an adjusted R2 of 0.27 - change in LM thickness 1 week post-manipulation.
1. Acute LBP
2. Moderately good prognosis without focal and irritable symptoms
3. Signs of spinal instability
Koppenhaver et al, JEK, 2012
Abdominal Activation Post Manipulation
• Feedforward activation improved post-manipulation in healthy individuals with delay1
• Case series meeting manipulation CPR – 6 of 9 patients increased TrA muscle thickness during ADIM post-manipulation2
• Rapid shoulder flexion – persons with LBP (not control group) exhibited higher amplitudes in both IO and EO (fine-wire EMG)3
– Persons with LBP – increased IO and EO activation post-manipulation. TrA and RA: no change.
1. Marshall, JMPT, 2006 2. Raney, JOSPT, 2007 3. Ferreira, Man Ther, 2007
Abdominal Activation Post Manipulation
• N=81, met and did not meet manipulation CPR1 – TrA thickness change decreased immediately post
SMT during ADIM.
– IO thickness change decreased immediately post SMT during ASLR.
– No change 1 week post SMT.
– No change in those who improved from manipulation.
• Case series – met stabilization CPR: “No significant differences in resting, contracted, or percent thickness change in the TrA or IO were found over the 3 time periods.”2
1. Koppenhaver, JOSPT, 2011 2. Konitzer, JOSPT, 2011
12/9/2013
38
• Does isolated muscle training affect timing of postural activation in short and long term?
• Isolated muscle training may help to redistribute muscle activation
• Isolated muscle training may affect motor cortical spatial representation
Is motor control intervention effective?
Tsao et al., J Electromyogr Kinesiol, 2008 Vasseljen et al., Spine, 2012 Tsao et al., J Pain, 2010 Tsao et al., Eur J Pain, 2010
• Motor skill training (versus general exercise) can alter corticospinal excitability and cortical representation
• Strength training increases excitability, but skill training alters representation
Is motor control intervention effective?
Boudreau et al., Man Ther, 2010 Adkins et al., J Appl Physiol, 2006 Fisher et al., JOSPT, 2013
Intervention
• Multi-modal intervention may improve timing of gluteus maximus activation1
• Trunk/hip strengthening intervention reduced pain but had variable outcome on co-contraction during prolonged standing2
• Task-specific training may alter coordination and movement patterns3
• Movement re-education may reduce symptoms4
1. Leinonen et al., Arch Phys Med Rehabil, 2000 2. Nelson Wong et al., J Electromyogr Kinesiol, 2010 3. Hoffman et al., Man Ther, 2012 4. Van Dillen et al., Man Ther, 2009

12/9/2013
39
Multifidus Atrophy Localized to Painful Region - Postural Cuing
L5
L5
T12 T12
Healthy: matched for age, size and activity
Low Back Pain
• Short Lordosis
– Verbal Cue: “Push your tailbone up over your head”
• Unilateral activation
– Short lordosis cue
– “Swing your tailbone to the right”
• Palpatory feedback
Training with Postural Cuing
Multifidus Longissimus Thoracic
L5
T12
Postural Cuing Activation Lower Lumbar
12/9/2013
40
Postural Cuing Activation Kneeling Side Bridge
Exercises
1. CONTRALATERAL ARM/LEG EXT
2. SIDE PLANK ON KNEES
3. PRONE LEG LIFT
4. PRONE TRUNK EXTENSION
6. VARC 15˚ 5. VARC 45˚
Is motor control intervention effective?
• 12 week progressive intervention
• Motor learning and strengthening
• Trunk and lower extremity musculature
“E.P.” Recreational cyclist
Kulig et al., Phys Ther, 2009 Flanagan, Kulig & PTCLINRESNET, JOSPT, 2010

12/9/2013
41
Is motor control intervention effective?
• Multifidus
• Transversus Abdominis
• Quadruped progression
• Abdominal progression
• Squat/lunge progression
• Modified paraspinal progression
12/9/2013
42
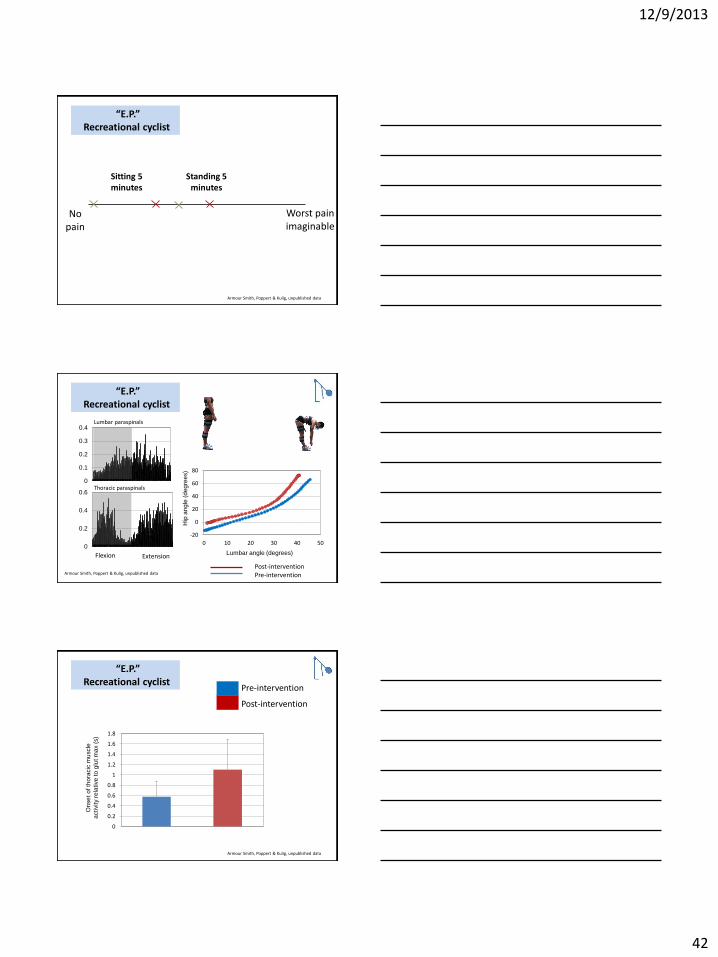
“E.P.” Recreational cyclist
No pain
Worst pain imaginable
Sitting 5 minutes
Standing 5 minutes
Armour Smith, Poppert & Kulig, unpublished data
0
0.1
0.2
0.3
0.4
0
0.2
0.4
0.6
“E.P.” Recreational cyclist
-20
0
20
40
60
80
0 10 20 30 40 50
Flexion Extension
Post-intervention Pre-intervention
Hip
an
gle
(d
eg
ree
s)
Armour Smith, Poppert & Kulig, unpublished data
Lumbar paraspinals
Thoracic paraspinals
Lumbar angle (degrees)
“E.P.” Recreational cyclist
Pre-intervention
Post-intervention
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
On
se
t o
f th
ora
cic
mu
scle
activity r
ela
tive
to
glu
t m
ax
(s)
Armour Smith, Poppert & Kulig, unpublished data

12/9/2013
43
“E.P.” Recreational cyclist
Co
ord
inat
ion
var
iab
ility
(a
ngu
lar
dev
iati
on
, deg
rees
)
0
20
40
60
80
100% Stride cycle
0%
Du
ratio
n o
f th
ora
cic
mu
scle
activity
(% o
f str
ide
cycle
)
0
5
10
15
20
25
30
Pre-intervention
Post-intervention
Armour Smith, Poppert & Kulig, unpublished data
Intervention
Boudreau et al., Man Ther, 2010
Recognize individual adaptations to pain
Maximize neuroplasticity
• Motor skill training
• Cognitive effort
• Quality not quantity of repetition
• Modulate complexity of task and environment
Framework for intervention
MUSCLE PERFORMANCE
load
reps duration
12/9/2013
44
CONTROL
cognition
context complexity
Framework for intervention
12/9/2013
45
12/9/2013
46
Selected References • Beneck GJ, Baker LL, Kulig K. Spectral analysis of EMG using intramuscular electrodes reveals non-linear fatigability characteristics in persons with
chronic low back pain. J Electromyogr Kinesiol. 2013;23:70-7.
• Beneck GJ, Kulig K. Multifidus atrophy is localized and bilateral in active persons with chronic unilateral low back pain. Arch Phys Med Rehabil.
2012;93:300-6.
• Boudreau, SA., Farina D, & Falla D. The role of motor learning and neuroplasticity in designing rehabilitation approaches for musculoskeletal pain disorders. Man Ther., 2010; 15: 410–414.
• Brown SH, Ward SR, Cook MS, Lieber RL. Architectural analysis of human abdominal wall muscles: implications for mechanical function. Spine (Phila
Pa 1976). 2011;36:355-62.
• Delitto A, George SZ, Van Dillen L, et al. Low back pain. J Orthop Sports Phys Ther. 2012; 42: A1-A57.
• DeVocht JW, Pickar JG, Wilder DG. Spinal manipulation alters electromyographic activity of paraspinal muscles: a descriptive study. J Manipulative
Physiol Ther. 2005;28:465-471.
• Esola MA, McClure PW. Fitzgerald GK, & Siegler S. Analysis of lumbar spine and hip motion during forward bending in subjects with and without a history of low back pain. Spine.1996;21: 71–78.
• Fisher BE, Lee YY, Pitsch EA, et al. Method for Assessing Brain Changes Associated With Gluteus Maximus Activation. J Orthop Sports Phys Ther.2013: 43: 214-221.
• Flanagan SP, Kulig K, & PTClinResNet. Time courses of adaptation in lumbar extensor performance of patients with a single-level microdiscectomy during a physical therapy exercise program. J Orthop Sports Phys Ther.2010; 40: 336–344.
• Ferreira ML, Ferreira PH, Hodges PW. Changes in postural activity of the trunk muscles following spinal manipulative therapy. Man Ther.
2007;12:240-8.
• Gatton ML, Pearcy MJ, Pettet GJ, Evans JH. A three-dimensional mathematical model of the thoracolumbar fascia and an estimate of its biomechanical effect. J Biomech. 2010;43:2792-7.
• Henry S, Hitt J, Jones S, & Bunn J. Decreased limits of stability in response to postural perturbations in subjects with low back pain. Clin Biomech,
2006;21: 881–892.
• Hodges PW, Galea MP, Holm S, Holm AK. Corticomotor excitability of back muscles is affected by intervertebral disc lesion in pigs. Eur J Neurosci. 2009;29:1490-500.
• Hodges PW, & Tucker K. Moving differently in pain: A new theory to explain the adaptation to pain. Pain. 2011; 152: S90–S98.
• Hodges P, van den Hoorn W, Dawson A, & Cholewicki J.. Changes in the mechanical properties of the trunk in low back pain may be associated with recurrence. J Biomech. 2009; 42: 61–66.
• Hoffman SL, Johnson MB, Zou D, Harris-Hayes M, & Van Dillen LR. Effect of classification-specific treatment on lumbopelvic motion during hip rotation in people with low back pain. Man Ther. 2011;16: 344–350.
• Konitzer LN, Gill NW, Koppenhaver SL. Investigation of abdominal muscle thickness changes after spinal manipulation in patients who meet a clinical prediction rule for lumbar stabilization. J Orthop Sports Phys Ther. 2011;41:666-74.
• Koppenhaver SL, Fritz JM, Hebert JJ, et al. Association between changes in abdominal and lumbar multifidus muscle thickness and clinical improvement after spinal manipulation. J Orthop Sports Phys Ther. 2011;41:389-99.
• Kulig K, Beneck GJ, Selkowitz DM, et al. An intensive progressive exercise program reduces disability and improves functional performance in patients after single-level lumbar microsdiskectomy. Phys Ther. 2009: 89: 1145-1157.
• Lamoth C, Daffertshofer A, Meijer O, Beek P. How do persons with chronic low back pain speed up and slow down? Gait and Posture. 2006; 23: 230-239.
• MacDonald D, Moseley GL, Hodges PW. People with recurrent low back pain respond differently to trunk loading despite remission from symptoms. Spine (Phila Pa 1976). 2010;35:818-24.
• Marras WS, Davis KG, Ferguson SA, Lucas BR, & Gupta P. Spine loading characteristics of patients with low back pain compared with asymptomatic individuals. Spine. 2001; 26, 2566–2574.
• Marshall P, Murphy B. The effect of sacroiliac joint manipulation on feed-forward activation times of the deep abdominal musculature. J Manip Phys Ther. 2006;29:196-202.
• Mok NW, Brauer SG, & Hodges PW. Failure to use movement in postural strategies leads to increased spinal displacement in low back pain. Spine. 2007; 32: E537–43.
• Nelson-Wong E, & Callaghan JP. Is muscle co-activation a predisposing factor for low back pain development during standing? A multifactorial approach for early identification of at-risk individuals. J Electromyogr Kinesiol. 2010; 20: 256–263.
• Popovich JM Jr, Kulig K. Lumbopelvic landing kinematics and EMG in women with contrasting hip strength. Med Sci Sports Exerc. 2012;44:146-53.
• Raney NH, Teyhen DS, Childs JD. Observed changes in lateral abdominal muscle thickness after spinal manipulation: a case series using rehabilitative ultrasound imaging. J Orthop Sports Phys Ther. 2007;37:472-479.
• Regev GJ, Kim CW, Tomiya A, et al. Psoas muscle architectural design, in vivo sarcomere length range, and passive tensile properties support its role as a lumbar spine stabilizer. Spine (Phila Pa 1976). 2011;36:E1666-74.
• Silfies SP, Mehta R, Smith SS, & Karduna AR. Differences in Feedforward Trunk Muscle Activity in Subgroups of Patients With Mechanical Low Back Pain. Arch Phys Med Rehabil. 2009;90: 1159–1169.
• Stokes IA, Gardner-Morse MG, Henry SM. Intra-abdominal pressure and abdominal wall muscular function: Spinal unloading mechanism. Clin Biomech. 2010;25:859-66.
• Tsao H, Danneels LA, Hodges PW. Smudging the motor brain in young adults with recurrent low back pain. Spine. 2011; 36: 1721-1727.
• Tsao H, Danneels L, Hodges PW. Individual fascicles of the paraspinal muscles are activated by discrete cortical networks in humans. Clin Neurophysiol. 2011;122:1580-7.
• Tsao H, Druitt TR, Schollum TM, Hodges PW. Motor training of the lumbar paraspinal muscles induces immediate changes in motor coordination in patients with recurrent low back pain. J Pain. 2010;11:1120-8.
• van der Hulst M, Vollenbroek-Hutten MM, Rietman JS, & Hermens HJ. Lumbar and abdominal muscle activity during walking in subjects with chronic low back pain: Support of the “guarding” hypothesis? J Electromyogr Kinesiol. 2010; 20: 31–38.
• van Dieën JH, Selen LPJ, & Cholewicki J. Trunk muscle activation in low-back pain patients, an analysis of the literature. J Electromyogr Kinesiol. 2003; 13: 333–351.
• Ward SR, Kim CW, Eng CM, et al. Architectural analysis and intraoperative measurements demonstrate the unique design of the multifidus muscle for lumbar spine stability. J Bone Joint Surg Am. 2009;91:176-85.