moving and handling policy - whatdotheyknow€¦ · subject moving and handling policy...
TRANSCRIPT

HS04 Moving and Handling
1
MOVING AND HANDLING POLICY
Subject Moving and Handling Policy incorporating moving and handling
training
Applicable to All employees of South London Healthcare NHS Trust
Date Issued April 2010
Dates policy reviewed: Not applicable
Next review due date March 2012
Original Policy written by: Julie Seal. Moving and Handling Adviser (QMS)
Policy reviewed by: Julie Seal. Moving and Handling Adviser (QMS)
Lead responsible for policy: Antony Pays. Head of Safety & Emergency Planning
Approved by: H&S Committees for; PRUH 20/01/10 QMS 14/01/10 QE 13/01/10 Executive H&S Committee 10/02/10 Amended Feb 2011 – Health and Safety Compliance Committee
Authorised by: Jonathan Pearce
Signature
Related policies: HSO1: Health and Safety Policy
TMO3: Risk Management Strategy
TMO4: Risk Management Policy and Procedures
TM12: Serious Untoward Incident Policy
IPC08: Infection Prevention Policy and Strategic Framework
Occupational Health Policy
HSO2: Display screen equipment Policy

HS04 Moving and Handling
2
TM17: Pressure Ulcer Prevention & Management Policy
HS11: Provision of Work Equipment
HS10: PPE Policy
HSO6: Lone Worker
HSO9: New & Expectant Mothers
CONTENTS
Policy Statement………………………………………………………………………………..3
Responsibilities.………………………………………………………………………………...3
Guidelines linked to Policy……………………………………………………………………3
1. ROLES AND DUTIES……………………………………………………………………….4
2. TRAINING…………………………………………………………………………………….10
3. RISK ASSESSMENTS……………………………………………………………………...15
4. DOCUMENTATION…………………………………………………………………………17
5. EQUIPMENT………………………………………………………………………………...18
6. SPECIAL ADVICE…………………………………………………………………………..19
7. BUILDING AND REFURBISHMENT……………………………………………………….19
8. AUDIT………………………………………………………………………………………...20
9. PFI HOSPITALS…………………………………………………………………………….20
10. PROCESS FOR MONITORING………………………………………………………….21
11. DEFINITIONS……………………………………………………………………………….22
12. REFERENCES AND FURTHER READING…………………………………………….23

HS04 Moving and Handling
3
13. CONSULTATION PLAN…………………………………………………………………..25
14. EQUALITY IMPACT ASSESSMENT…………………………………………………….26
15. MOVING & HANDLING PERFORMANCE CRITERIA
– PRACTICAL TECHNIQUES TAUGHT……………………………………………………28.
Policy Statement.
The Trust Board and Chief Executive of South London Healthcare NHS Trust accept their legal responsibilities under the 1974 Health and Safety at Work Act, and associated Acts and Regulations. In observing these responsibilities, the Trust is committed to creating a safe environment for all staff, visitors and patients, where hazardous Moving and Handling activities are avoided, or the risk of harm from them reduced as far as is reasonably practicable.
Responsibilities
It is the duty of the Trust Board to assure itself that the organisation has in place a policy which clearly identifies the responsibilities of the Trust in relation to ensuring a safe working environment for staff. It does so by the receipt of regular reports from named Executive Directors which include the presence of a policy, training to enable staff to fulfil the requirements of the policy and incidents of moving and handling errors, omissions and resultant injuries.
The Trust Chief Executive is responsible for compliance with regulations and must ensure that the infrastructure detailed in this policy is in place. This responsibility cannot be delegated. The day to day management of this policy will be delegated to departmental managers / heads of departments.
The Trust Board will, as far as reasonably practicable, take steps to meet their responsibilities under the Health and Safety at Work Act (1974). The management of Health and Safety at Work Regulations 1999 and the Manual Handling Operations Regulations 1992 (as amended), which came into effect on 1st January 1993, supplement the employers‟ existing responsibilities with specific duties. These regulations require that the employer should avoid hazardous Moving and Handling or where not possible to avoid, carry out suitable and sufficient (ergonomic) assessments of the risks and to reduce those risks as far as is „reasonably practicable‟.
All staff agree as part of their contract of employment to comply with their individual duties under the Health and Safety at Work Act (1974) and associated regulation relating to the Moving and Handling of people and inanimate objects. They also agree to co-operate fully with their employer, enabling the Trust to carry out its Health and Safety duties under the Act and associated regulation relating to Moving and Handling.

HS04 Moving and Handling
4
This policy applies to all staff employed by South London Healthcare Trust and includes permanent staff, agency staff, PFI partners (where applicable) and other contractors and students on placements.
This policy is supported by guidelines on how to apply the policy. These guidelines are contained in the following section.
Guidelines
This section provides guidance on how to meet all the requirements of the law, standardise processes, procedures, training and recording methods across South London Healthcare NHS Trust.
The Health and Safety Executive has recommended five important steps for success:
A policy
Competent staff to put the policy into effect
Assessment of risks with appropriate measures to avoid them
Measures of performance
Reviews of performance
1.0 ROLES AND DUTIES
1.1 Managers – All clinical and non clinical departments
Be aware of moving and handling operations within their department
To implement Moving and Handling regulations within their department
Avoid the need for employees to undertake any moving and handling operations which involve a risk of injury, so far as is reasonably practicable
Avoid the need for staff to undertake prolonged or repetitive poor postures during the use of work systems or equipment, as far as is reasonably practicable
Make a full and sufficient assessment of any hazardous moving and handling operations that cannot be avoided in order to reduce the risk of injury, in line with the Moving and Handling Operations Regulations (2002).
Carry out risk assessments for staff working alone out of hours and those staff working off site
Make a clear record of the assessment and communicate its findings to all staff involved

HS04 Moving and Handling
5
Monitor and review moving and handling assessments when there is a reason to suppose that they are no longer valid due to a change in working conditions, personnel involved or a significant change in the moving and handling operations affecting the nature of the task or the load
Report any risks to the Trust Moving and Handling Adviser that cannot be managed at department level.
To ensure that working practices and procedures are designed to reduce the risk of injuries to the lowest level, this will include adequate staffing levels and working environments
Provide information on training availability and ensure that all staff receive appropriate training as defined in this policy and outlined in the Trust Trained Needs Analysis ( Statutory and Mandatory Training Policy) and before any moving and handling tasks are undertaken
Responsibility for ensuring that permanent staff within their sphere of responsibility attend training as identified in the TNA, and maintain records to this effect and for the following up and reporting of staff who fail to attend training.
Ensure that mechanical aids are provided, are easily accessible and properly maintained
Ensure that moving and handling requirements are clearly identified when recruiting staff so that appropriate advice can be given at pre- employment health screening
Make allowances for any known health problem which might have a bearing on an existing employee‟s ability to carry out moving and handling operations in safety, including new and expectant mothers
Refer to occupational health if there is a good reason to suspect that an individuals state of health might significantly increase the risk of injury from moving and handling operations
To ensure that all accidents, incidents and near misses are reported in a timely manner via the correct reporting structure
Pay particular attention to vulnerable staff groups, such as students and new or inexperienced staff, ensuring they receive appropriate departmental induction, support and supervision and are made fully aware of Moving and Handling hazards, risk assessments and safe systems of work and records are kept of these interactions
1.2 Managers with responsibility for patient care.
In addition to the responsibilities for Managers of all departments the following responsibilities apply:
Moving and Handling is a core clinical competence for Nurses, Midwifes and allied professionals and should be managed as such.

HS04 Moving and Handling
6
To identify a Registered Nurse/ Midwife or Allied Health professional to assist in the implementation of responsibilities identified in this policy, who will undertake in-depth training to qualify as departmental Moving and Handling Core trainer.
Allow sufficient time for Core Trainers to discharge their responsibilities
To ensure that patients are encouraged to assist with their own moving and handling requirements via communication and education by staff, if this is not contrary to the patients needs and abilities
To ensure that every patient admitted to the Department, either by emergency or elective admission, has a moving and handling risk assessment carried out prior to any non-emergency moving and handling operation being performed.
Ensure the continued assessment of the capabilities and rehabilitation needs of patients in order to determine which methods of handling should be used.
To ensure the patient specific risk assessment will be carried out daily as a minimum or as and when a moving and handling situation changes
To ensure all documentation provides evidence of timely assessment by inclusion of date, time and signature of the assessing member of staff
To ensure the outcome of general and patient specific risk assessment will be communicated to all relevant staff
Ensure that special situations such as the handling of bariatric (very heavy) patients are thoroughly assessed and managed on a case by case basis to ensure the safety and dignity of both patient and staff
To ensure that Moving and Handling aids, whenever identified as appropriate via the Moving and Handling risk assessment, are used wherever they can reduce the risk of injury whilst maintaining a balance with the needs of the patient
To ensure avoidance of controversial manoeuvres, e.g. drag lifts, Australian lifts etc when moving patients
Through assessment o anticipate patient falls and ensure proactive management using the site specific Falls Policy
Carry out risk assessments to ensure the safety of both staff and patient where the member of staff is working in another institution or in a patients home
Adhere to all Trust Infection Control protocols and Manufacturers cleaning instructions relating to the handling of patients and decontamination of equipment
1.3 Core Trainers – Clinical areas

HS04 Moving and Handling
7
These will be Registered Nurses‟, Midwifes or Allied Health Professionals who have received comprehensive Moving and Handling training. Core Trainers linked to clinical areas would complete a 5 day accredited trainer‟s course. The Core Trainers provide a link between the relevant department and the Trust Moving and Handling Advisor.
Moving and Handling core trainers can provide training within their level of certified competence. Their responsibilities are:
To assist the department manager in executing their responsibilities
Monitor and reinforce the Moving and Handling Policy and culture within their department/area.
Promote a minimal lift environment within the department
To assess and monitor new and existing staff to ensure safer Moving and Handling techniques are maintained and poor practice is discouraged
To provide and maintain records and documented evidence of teaching given to staff in the department
Undertake General Moving and Handling risk assessments in their area, reporting any medium and high risk assessed activities or issues to the manager via a corrective action plan
Advise clinical staff on how to carry out patient moving and handling risk assessments and complete handling care plans taking into account patients‟ equality and diversity and special needs, ensuring race, disability, gender, sexual orientation, age and religion are considered..
Audit moving and handling compliance in their area and report back to the appropriate Manager on areas of non- compliance
Review provision of equipment to identify whether suitable and sufficient moving and handling equipment and aids are available and are properly maintained and report any shortcomings to the Manager via a corrective action plan
Liaise with the Trust Moving and Handling adviser on any areas of concern or non compliance with the policy.
Maintain their competence by the way of specialist update training to remain in the role
1.4 Clinical Link staff
Link staff can be Registered or non –Registered Nursing Staff or Allied Health Professionals or Assistants, who have a good working knowledge and understanding of the ward or department and the patient‟s needs within that area. Existing Link staff will undertake a 1 day specialist update annually to maintain their status as well as attending the Trust Clinical Update Training.
Their role will be:

HS04 Moving and Handling
8
To assist the Core trainer in executing their responsibilities, including training within their level of competence.
Monitor the moving and handling culture within their department/area and report any issues to the Core Trainer and manager.
Promote a minimal lift environment within the department
Link staff are required to attend training as per site specific protocols, minimum annually, and have a job description for the role
1.5 Managers – Non clinical departments
In addition to the responsibilities for Managers of all departments the following responsibilities apply:
To identify 1 member of staff (Link staff), as a minimum, or more depending on the size of the department and the nature of the moving and handling operations involved, to assist in the implementation of duties and responsibilities identified in this policy, within the department / area of work.
Allow sufficient time for the nominated person to discharge their duties
1.6 Non – Clinical areas Link Staff
To assist the Department Manager in executing their responsibilities as identified in the policy
Monitor the moving and handling culture within their department/area and report any issues to the Manager.
Promote a minimal lift environment within the department
Liaise with the Trust Moving and Handling adviser on any areas of concern or non compliance with the policy.
Will undertake any specialist moving and Handling training relevant to the department where appropriate ie Moving and handling of Medical Gases.
1.7 Students
Students must have received appropriate moving & Handling training from their educational establishment before embarking on a clinical placement
Students must ensure they are supervised when implementing moving & handling techniques with patients or when handling inanimate loads

HS04 Moving and Handling
9
1.8 Mentors/Clinical Supervisors
It is the responsibility of the nominated mentor or supervisor to ensure that the student has received appropriate moving & handling training from their educational establishment when they begin placement
Students must be supervised when implementing moving & handling techniques with patients or when handling inanimate loads
1.9 Employees must
Comply with existing policies on moving and handling and co-operate fully with the implementation of relevant policies and site specific protocols.
Report any risks to the department manager
Ensure safer systems of work are followed as identified by risk assessment
Adhere to and work from risk assessments and safe systems of work
Use Moving and Handling aids whenever identified as appropriate via Moving and Handling risk assessment
Ensure they can demonstrate their Moving and Handling activities are directly linked to the relative Moving and Handling risk assessment
Participate in statutory and mandatory and other relevant training as provided by the Trust
Report immediately to the Line manager any shortcomings in their training, knowledge, skill, competency, ability or experience, which compromises their safe working practice relative to Moving and Handling, working postures and documented risk assessments
Avoid all controversial manoeuvres as identified by training.
Promptly report any accidents, incidents or near misses at work relating to Moving and Handling to their Manager using the correct reporting procedure.
Report to their manager any issues relating to their health and fitness that may have an adverse effect on their Moving and Handling safety or ability (including pregnancy)
Wear suitable clothing and shoes at work, and will avoid items or accessories that may injure patients or the handler during handling
Report any working or workplace conditions that have an adverse effect on their musculoskeletal health
Ensure that equipment is clean as per manufacturers instructions and in visually good condition prior to use
1.10 Trust Moving and Handling Adviser responsibilities

HS04 Moving and Handling
10
Advise on ergonomics of the work environment
Advice on the prevention of hazardous Moving and Handling activities and associated equipment, load, individual capabilities, task and environment
Developing and providing a framework of training in Moving and Handling, risk assessments, safer systems of work, posture and ergonomics
Reviewing accident / incident and near miss forms involving Moving and Handling, posture and ergonomics
Advise on risk assessments and complex Moving and Handling problem solving
Regular audit of compliance with risk assessments
Audit of Moving and Handling equipment and reporting concerns via action plan to Managers
Regular review of the Moving and Handling policy associated protocols and appendices
Support a programme of risk assessment of Moving and Handling practice across the Trust, carrying out risk assessments and corrective action plans where appropriate and helping Managers and their delegates to undertake risk assessments
Monitor the risk data base and report any unresolved risks that cannot be dealt with at departmental level or by the Moving and Handling Adviser to the Health, Safety and Security Committee
Contribute to the Trust‟s wider risk assessment programme, providing specialist advice on Moving and Handling factors
Support named trust competent persons e.g. Core Trainers and Link staff to help ensure that best practice is promoted locally, through observation and formal risk assessment processes.
Work with managers and / or occupational health when staff are returning to work after Musculo-Skeletal Injuries to achieve a safe and timely return to work
Rectify unsafe practice amongst their own teams
Provide progress reports for the Trust on Moving and Handling activities, to include data on training, incidents and risk management as required
Contribute to the Trust‟s Health, Safety and Security Committee as a specialist adviser for Moving and Handling.
1.11 Occupational Health Department Seeking advice from the Moving & Handling Advisor if required
Carry out appropriate pre-employment screening when requested to identify those persons for whom moving & handling tasks would present a particular risk and advise managers of any restrictions on practice

HS04 Moving and Handling
11
Provide early assessment following injury as a result of moving & handling
Arrange a final assessment regarding suitability for return to full duties and if required having a staged return to work negotiated with the manager concerned.
2.0 Training The risk of injury from a Moving and Handling task will be increased where workers do not have the information or the training necessary to enable them to work safely. Effective training will complement a safe system of work, and has an important part to play in reducing the risk of Moving and Handling injury. Training is not a substitute for a safe system of work. To enable staff to complete training it is essential that a) training programmes are in place b) staff are informed about their individual training requirements c) staff are released from the workplace to attend training. Moving and l handling training should be based o promoting the right culture to achieve safer working practices. Such training should not be seen as an annual chore but should be seen as an integral, on-going process involving regular refresher components. Emphasis in training should be on increasing understanding and helping workers to risk assess their tasks as opposed to specific lifting technique training.
When workers are given appropriate training, it is important that their Managers and senior staff are also aware of the good practices that have been recommended. Therefore managers and senior staff should regularly attend the training and encourage the workforce to adopt appropriate techniques and ensure they continue to be used, to ensure both staff and patient safety. The Trust will ensure the availability of training provision for all staff to receive information and training on Moving and Handling relevant to their role or duties within the Trust, in line with the Training Needs Analysis (TNA). Training will take the form of structured, formal learning either: in the classroom, departmental based learning, e-learning, Q&A learning, competence based or any other type of learning identified as effective and measurable. Formal training records will be kept of all training undertaken by employees of the Trust and entered on the Training Database.
2.1 Training Booking
Staff members should discuss attendance times with their manager before they book the course. Managers who book courses for their staff should inform staff of the requirements for the course, especially where suitable attire is essential for practical handling.

HS04 Moving and Handling
12
The training should be booked using the course and site specific instructions. However, requests for Departmental training need to be discussed and agreed with the trainer and on completion, records will be handed to the L&OD Service for database entry.
2.2 Induction training
All Inductees will receive classroom based Moving and Handling Theory training prior to commencing work. Clinical staff will attend clinical practical training prior to commencing work. Staff whose role will include a high content of inanimate object handling will attend the first available inanimate object practical training session.
2.2 Theory training – all staff (Minimum 2 hours) Moving and Handling theory training will consist of information provision on:-
1. Current Legislation 2. Hospital policy 3. Professional guidelines 4. Statistics 5. Basic anatomy 6. Causes of back injuries – static and repetitive poor postures, including seated postures. 7. Principles of efficient body movement / how to prevent back injuries 8. Ergonomic Risk Assessment 9. Principles of inanimate object handling 10. Responsibility for accident reporting
(NB: All staff attending refresher moving and handling training MUST provide certificated evidence of successful completion of e-learning or other Moving and Handling Theory module prior to attendance at any practical patient or inanimate object handling training session, depending on site specific protocols) 2.3 Practical training – Clinical staff (Minimum 3 hours)
1. Safe use of beds
2. Unsafe handling techniques
3. Normal movement
4. Patient specific risk assessment
5. Safer patient handling techniques – from The Guide to Handling of Patients. No 5
6. Use of equipment
7. Problem solving
8. Dealing with emergencies ie:- fallen patient

HS04 Moving and Handling
13
2.4 Practical training – Inanimate object handling (Minimum 2 hours)
1. Unsafe handling techniques
2. Inanimate object risk assessments
3. Safer handling techniques (from Getting to grips with Moving and Handling, A short
guide for Employees, HSE)
4. Use of equipment
5. Problem solving
2.5 Theory training, – Volunteers, site specific (1 hour minimum)
All Volunteers will receive classroom based Moving and Handling theory training as part of their induction programme to the Trust. Volunteers will only be expected to move and handle inanimate objects and are prohibited from patient moving and handling.
2.6 Frequency of Training
After the initial Induction training, staff will be required to receive refresher training as detailed below. THE FOLLOWING LIST IS NOT EXHAUSTIVE. CONTACT MOVING AND HANDLING ADVISER FOR FURTHER INFORMATION / GUIDANCE
High Risk groups
ANNUAL REFRESHER -THEORY AND PRACTICAL
Staff involved in moving and handling of patients or potentially hazardous inanimate loads or prolonged poor posture as a major part of their work activities
e.g, All Nursing Staff, All Midwifery Staff, Occupational therapists, Physiotherapists
Radiographers, Surgeons, Dentists, Orthoptists, Podiatrists, Porters, Stores personnel,
Estates staff, Pharmacists, Medical records Administrators.
Medium Risk Groups
EVERY 18 MONTH REFRESHER – ALTERNATE “E”LEARNING AND FACE TO FACE
Non- patient handlers, staff involved in the moving and handling of inanimate

HS04 Moving and Handling
14
objects on a less regular basis
eg, Non- clinical Managers, Ancillary staff, Technicians, Administrative staff, Scientists.
2.7 Number of delegates
The maximum number of delegates per session per trainer;-
Theory = 15
Practical = 10 (unless room size and equipment provision are inadequate)
2.8 Service specific Training
Practical training relevant to individual departments and Moving and Handling operations can be arranged through discussion with the Moving and Handling Department when the need has been identified by a risk assessment.
2.9 Process for Checking Compliance with Moving and Handling Training o Managers are responsible for ensuring their staff attend mandatory training, as identified in
the trust training needs analysis, that training is accurately recorded, and that non-attendance is followed up.
o Moving and handling training attendance must be reviewed as part of the annual appraisal process for all staff.
o All records of moving and handling training must be available for review and monitoring of attendance at divisional and Trust level.
o Training attendance is monitored and reported as a Trust key performance indicator.
Process for follow up of non-attendees/non-compliant staff
If for any reason a member of staff cannot attend a booked training session/programme the member of staff MUST inform their line manager who will inform the trainer/specialist as required. If appropriate, the line manager should arrange for another member of staff to attend. If training is cancelled or the member of staff is not able to attend for any reason the manager will be required to release staff to attend the next available session. Failure to cancel will be reported as a non attendance DNA . If staff fail to comply with /attend training the HR and Learning & Organisational Development Service Administration Team will implement the following process to follow-up staff who fail to attend Moving & Handling training:
Managers will be notified by email of staff members who fail to attend

HS04 Moving and Handling
15
The relevant divisional Director of the service concerned will be notified if staff continue to fail to comply with attendance requirements. The divisional Director will be required to take action on behalf of the HR and Learning & Organisational Development Service.
Quarterly reports on non-attendance will be sent to all divisional Directors to ensure the organisation is risk-aware.
The Trust will not tolerate more than one more failure to attend training. For a second failure to attend, the manager will follow up in writing, pointing out that attendance is a condition of employment.
All correspondence must be filed in the staff member‟s personal file.
Any member of Bank staff who is non-compliant with mandatory training will not be offered further shifts within the Trust.
2.10 Process for follow up of Medical Staff who fail to comply
The following stages are to be followed for Medical Staff:
The Medical Education Manager will make initial contact with the doctor concerned to ascertain if there are any problems in the completion of the mandatory training modules i.e. an elearning package + a practical session.
If after one month the mandatory training modules are not completed, the Medical Education Manager will write to the Educational Supervisor for doctors in training (Associate Medical Director for Trust funded doctors) and the doctor concerned to confirm the modules yet to be completed and the final date for certificate submission. The letter will also state that if these timescales are not met, future Study leave for CPD will not be approved until they can demonstrate they have completed the mandatory training or are progressing with a schedule to complete the training.
If after a further month the completion of the mandatory training modules is still outstanding the Medical Education Manager will write to the Director of Medical Education and the Educational Supervisor for doctors in training (Associate Medical Director for Trust funded doctors) and the doctor concerned. This second letter will inform them that there has been a failure to complete, or schedule to complete, mandatory training and that they are therefore in breach of contract.
3.0 RISK ASSESSMENTS
There are two types of moving & handling risk assessments undertaken in the Trust. These are General Risk Assessments for moving and handling loads both animate and in-animate and the Patient Handling Assessment forms.
3.1 General Risk Assessments
As part of their health and safety responsibilities each Manager must ensure that any hazardous Moving and Handling activities in their area that cannot be avoided are subjected to a suitable and sufficient assessment to reduce risk.
Risk assessments will embrace all patient moving and handling and hazardous inanimate load handling within South London Healthcare NHS Trust

HS04 Moving and Handling
16
It is sometimes acceptable to do a Generic Assessment – or Standard Operating procedure (SOP), or Departmental Standardised Handling procedure, one that is common to several employees or to more than one site or type of work, for example, Operating Theatres. However if specific factors exist that prevent the generic approach from adequately controlling the risk factors then a specific risk assessment should be done.
All handling hazards considered to be reasonably foreseeable and yet unavoidable, should be subjected to a risk assessment to reduce the risk via safer systems of work, particularly for critical handling scenarios such as falls, fire, evacuation, Bariatric patients, cardiac arrest, collapse situations – i.e. bath, chair, bed.
Unresolved risks should be entered on the risk database by the Manager responsible. The Moving and Handling Adviser will monitor the risk data base and report unresolved risks to the health, safety and Security Committee
3.2 Patient Specific Risk assessment / care plan
All patients admitted to any hospital within South London healthcare NHS Trust will undergo a Manual Handling Risk Assessment on admission, using the correct documents relative to each site.
Following the decision that a patient is not independently mobile, a patient Moving and Handling risk assessment should be completed, or already be in existence and a safe system of work decided upon. This should be clearly documented and accessible, and all staff made aware. The assessment must be reviewed regularly or when a change has occurred.
The Risk Assessment will be located by the patients bed along with other Risk Assessments such as Falls, Waterlow, etc. This documentation must accompany the patient when visiting other departments within the Trust where the patient may need to be handled i.e. Radiography.
In certain circumstances it may be necessary for the Nursing staff to refer a patient who requires specialist handling to a therapist; similarly the decision may be made independently by the therapist, therefore it is essential that there are good channels of communication within the multi disciplinary team regarding the sharing and recording of Moving and Handling information.
It will not be necessary to complete a specific Moving and Handling risk assessment for individual patients attending clinics or outpatient settings who clearly do not require Moving and Handling, however these units should have generic (or in some cases specific) safe systems of work for dealing with reasonably foreseeable Moving and Handling needs that may arise i.e. collapse or hoisting.
3.3 Therapeutic Handling
Local therapeutic Moving and Handling risk assessments should reflect the guidance promoted by ACPIN (2001), the Association of Physiotherapists in Neurology, guidance on Manual Handling in Physiotherapy 2008, Manual Handling 2006 published by the College of Occupational Therapists. These guidance documents assist in the local risk assessment policies for therapeutic Moving and Handling tasks. Their overall recommendation remains that a full risk assessment should be carried out and documented, prior to any Moving and Handling manoeuvre being undertaken (the core of this assessment process reflects the Moving and Handling Operations Regulation (1992) guidelines). They do not recommend the delegation of these techniques to other healthcare professionals, unless adequate training and competence can be demonstrated.
HS04 Moving and Handling
17
3.4 Patient Moving and Handling
South London Healthcare NHS Trust is committed to using safer patient handling principles: “The aim is to eliminate hazardous Moving and Handling in all but the most exceptional or life threatening situations”. Patients should be encouraged to assist in their own transfers and handling aids must be used whenever they can reduce the risk of injury. Handling patients manually may continue only if it does not involve lifting most or all of a patient‟s weight. Care must also be taken when supporting a patient and pushing and pulling should be kept to a minimum. Staff should assess the capabilities and rehabilitation needs of a patient to decide on which, if any handling aids are suitable”.
3.5 Working with Babies and Children
The concept of eliminating all manual lifting may not be useful for staff working in these areas. Where avoidance of Manual Handling is impractical, it is still important to avoid or reduce the risk of injury by taking into account postural controls during the delivery of Babies and when assisting in the care of babies and children etc. This can be achieved by looking at ergonomic issues; for example, the design of cots is more relevant than the weight of the baby inside it. Full risk assessments should be carried out where appropriate.
3.6 Inanimate object risk assessment
The Moving and Handling Operations Regulations (1992) (Appendix 2) apply to all Moving and Handling of loads. (Load, being person, object, or animal). The regulations should be followed for all inanimate object handling.
Avoid hazardous Moving and Handling operations so far as is reasonably practicable.
Make a suitable and sufficient assessment of any hazardous Moving and Handling operations that cannot be avoided (Appendix 6)
Reduce the risk of injury from those operations so far as is reasonably practicable. Where possible, mechanical assistance should be provided, for example a trolley.
3.7 Organisational overview of risk assessment
The Executive Health and Safety Committee is responsible for the organisational overview of risk assessments, through quarterly review of the Trust risk register. Risks identified through risk assessments are entered onto the Trust risk register, using the Trust risk management system, in accordance with the Trust risk management policy. Those risks which cannot be managed locally will be escalated, as appropriate, to the Executive Health and Safety Committee.
4.0 Documentation
Documentation is becoming increasingly important when defending litigation claims by employees and patients alike. Site specific Risk assessments, general documentation and other relevant information will be

HS04 Moving and Handling
18
maintained across South London Healthcare NHS trust. The aim will be to uniform all documentation relating
to Moving and Handling across all sites within an agreed timescale.
4.1 Patient specific documentation
For patients on Care Pathways the relevant Moving and Handling Risk Assessment and Care Plan sections must be completed and maintained throughout the episode of care to ensure compliance with relevant Legislation across South London Healthcare NHS Trust. Where a Care Pathway is not being used or is not sufficiently detailed a Risk assessment document must be used.
5.0 Equipment
As part of the assessment process Managers and Core Trainers may identify the need for mechanical aids or other Moving and Handling devices in order to eliminate or reduce the risk of injury from Moving and Handling. Equipment will be provided by each department to eliminate Moving and Handling wherever possible. This includes height adjustable and electrically-operated equipment, including beds and cots. Where Moving and Handling cannot be eliminated, equipment will be provided to reduce the risk. This includes items such as trolleys, hoists and low friction slide sheets to allow loads to be slid rather than lifted. The use of single patient use disposable equipment, such as slide/glide sheets, hoist slings etc should be implemented across all sites of South London Healthcare NHS Trust to assist in Infection Control within the Trust. Where non disposable equipment is still in use, cleaning and laundering protocols will remain as per site specific protocols. Responsibility for the selection and purchase of such aids will rest with the individual Managers, with advice from the Moving and Handling Adviser and trialled to determine any handling or postural implications it may involve for staff or patients during its movement or use. However, the selection of Moving and Handling equipment should take into account the following factors i.e.:
reduce the Moving and Handling load for staff
be able to reduce the need for sustained or poor posture
be easy to operate
be capable of lifting/moving the load safely
be capable of lifting/moving the load in the intended location
be compatible with other equipment being used
be in sound condition and properly maintained in accordance with LOLER and PUWER Regulations 1998.
be suitable for the condition and comfort of the patient
lifting hoists must be able to lift patients from floor level
ease of cleaning and is supplied with cleaning instructions from the manufacturer
A list of moving and handling equipment including serial numbers and maintenance schedules should be kept by each department and Facilities depts. within the Trust. Staff should be fully conversant in the use of any Moving and Handling equipment in their area and aware of the requirement to use such aids. If a hoist is non-compliant with LOLER checks or not functioning it must be taken out of service and reported to the appropriate Help Desk. Staff and patients must not be put at risk and if another hoist cannot be shared the Moving & Handling Advisor must be told immediately
HS04 Moving and Handling
19
The Department Core Trainer or the Moving and Handling Adviser will review equipment needs and audit annually to recommend level of equipment required related to case mix and dependency.
This recommendation will be submitted to the Departmental Manager/PFI Contracts manager along with an action plan.
The Supplies Department, the PFI and the PFI contracts dept. will consider the purchase and management of Moving and Handling Equipment Trust wide in discussion with the Moving & Handling Advisor and other stakeholders.
5.1 Maintenance of equipment. Arrangements for equipment maintenance and repair will follow site specific policies and procedures and will be maintained and serviced as per LOLER and PUWER (1998) Regulations. All equipment will be labelled to indicate the Safe Working Load (SWL). For those patients exceeding the standard equipment available please refer to the Heavy Patient procedures on the local intranets All lifting accessories are compatible for the lifting device All lifting equipment and accessories (hoists and slings and extra stretcher attachments) are maintained and kept in good working order through six monthly LOLER checks. Any equipment that is faulty or has not been LOLER checked must be labelled, taken out of service with immediate effect and reported via the appropriate site specific guidelines. Replacement equipment will either be borrowed from another department, if practicable, or hired in as per site specific protocols.
5.2 Hospital beds
Each patient‟s handling needs must be taken into consideration when selecting the type of bed appropriate to the patients‟ clinical needs. The standard King‟s Fund type bed is now considered suitable only for patients who are fully mobile. This type of patient is becoming increasingly rare in hospitals today.
Electronic variable posture beds should be used where care staff have to handle dependent patients, as they considerably reduce the amount of moving and handling in the daily routine of care staff while promoting patient independence.
In line with the Health and Safety Executive SIM 7/2007/10, where there is a high level of patient dependency and therefore frequent patient handling operations the provision of profiling beds is considered a reasonably practicable control measure in the management of the risk of musculoskeletal injury and as such should be provided i.e. the current position is that the HSE expects Electric Profiling Beds to be in use where needed to avoid hazardous manual handling of individual patients.
6.0 Specialist Advice
The Trust Moving & Handling Advisor (see 1.10) and Trainers are available to provide specialist assessment, advice and training. They are contactable by:
HS04 Moving and Handling
20
Email: [email protected] or [email protected]
Tel. 0208 836 ext. 6545
Information and advice is available on the local hospital intranet pages
The role of the Trust Moving & Handling Link Workers (see 1.3), and Core Trainers (see 1.4) is to provide advice to colleagues.
7.0 Building and Refurbishment
Moving and Handling issues will be considered at the design stage of every refurbishment, rebuild or new build project. For high risk areas, and for any major refurbishment or rebuild, ergonomics advice should be sought.
8.0 Audit
8.1 Internal Audit
The Hospital Moving and Handling Adviser will complete a moving and handling audit regularly as per site specific protocols, using the correct site specific documentation, to monitor the application of the system and training in each department/team/area and instigate corrective action if necessary. (See 1.1.0) The outcome of the audit will be presented to the department manager with recommendations for improvement.
The results of internal audits will be presented to the Health, Safety and Security Committee twice yearly, by the Moving and Handling Adviser.
Random visual observations will take place by the Moving and Handling Adviser, of staff carrying out moving and handling activities to check correct procedures and correct use of moving and handling equipment. Any non-compliance will be reported to the Department manager
9.0 PFI HOSPITALS.
As the Queen Elizabeth, Woolwich and Bromley Hospitals are the permanent host employers sharing the workplace with other Employers, in this case their PFI partners, they will co-operate with these Employers in order to comply with the Manual handling Operations Regulation, 1992. They will co-ordinate and communicate their Risk management processes in order to comply with the processes being taken by the other Employers to control risks. A reciprocal degree of co-operation, co-ordination and communication is expected of the South London Healthcare NHS Trust and the PFI partners / employers.
HS04 Moving and Handling
21
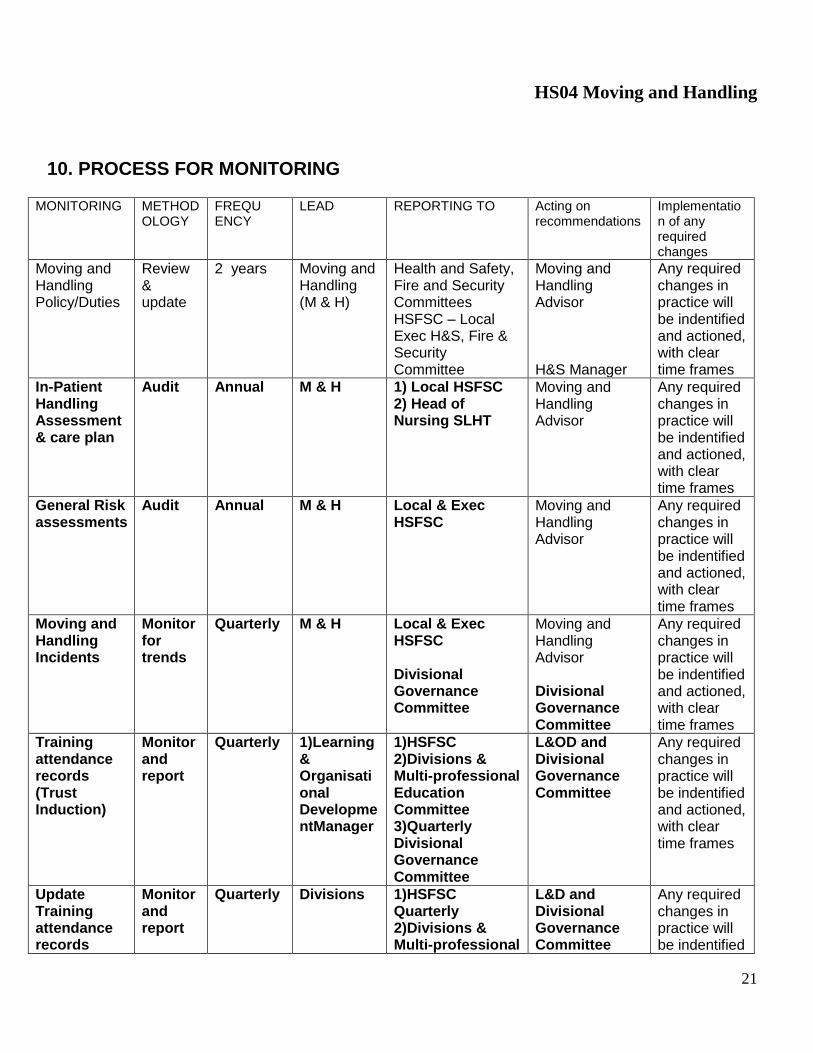
10. PROCESS FOR MONITORING
MONITORING METHODOLOGY
FREQU ENCY
LEAD REPORTING TO Acting on recommendations
Implementation of any required changes
Moving and Handling Policy/Duties
Review & update
2 years Moving and Handling (M & H)
Health and Safety, Fire and Security Committees HSFSC – Local Exec H&S, Fire & Security Committee
Moving and Handling Advisor H&S Manager
Any required changes in practice will be indentified and actioned, with clear time frames
In-Patient Handling Assessment & care plan
Audit Annual M & H 1) Local HSFSC 2) Head of Nursing SLHT
Moving and Handling Advisor
Any required changes in practice will be indentified and actioned, with clear time frames
General Risk assessments
Audit Annual M & H Local & Exec HSFSC
Moving and Handling Advisor
Any required changes in practice will be indentified and actioned, with clear time frames
Moving and Handling Incidents
Monitor for trends
Quarterly M & H
Local & Exec HSFSC Divisional Governance Committee
Moving and Handling Advisor Divisional Governance Committee
Any required changes in practice will be indentified and actioned, with clear time frames
Training attendance records (Trust Induction)
Monitor and report
Quarterly 1)Learning & Organisational DevelopmentManager
1)HSFSC 2)Divisions & Multi-professional Education Committee 3)Quarterly Divisional Governance Committee
L&OD and Divisional Governance Committee
Any required changes in practice will be indentified and actioned, with clear time frames
Update Training attendance records
Monitor and report
Quarterly Divisions 1)HSFSC Quarterly 2)Divisions & Multi-professional
L&D and Divisional Governance Committee
Any required changes in practice will be indentified

HS04 Moving and Handling
22
Education Committee 3)Quarterly Divisional Governance Committee
and actioned, with clear time frames
Specialist Advice
Report Annual M & H HSFSC L&OD Manager
Moving and Handling Advisor
Any required changes in practice will be indentified and actioned, with clear time frames
Action Plans Review Quarterly M & H HSFSC Health and Safety Committee
Any required changes in practice will be indentified and actioned, with clear time frames
11. DEFINITIONS
Assessment of Risk Identification of hazards present and the evaluation of the extent of the risk involved.
Emergency An unforeseen combination of circumstances or the resulting state that calls for immediate action. There are four situations that can be described as emergencies. In these situations the victim must be moved to safety immediately and there is no time to get equipment or plan the move. Risks may have to be taken. The situations are where the person is:
In water in imminent danger of drowning.
In an area that is actually on fire or is filling with smoke.
In danger from bomb or bullet.
In danger from a collapsing building or some other structure.
Employers Hospital or other legitimate place of work where the moving and handling operation occurs.
Exceptional or situations where speed of response is essential. These
HS04 Moving and Handling
23
life threatening situations are foreseeable and there should be plans for dealing
circumstances with:
Cardiac or respiratory arrest
Collapsed patients and staff in a range of situations
Fire, bomb and other evacuations
Hazard Something with potential to cause harm.
Injury Does not include injury from the condition or properties of a load, other than injury resulting from the shape, size, weight, external state, rigidity or lack of rigidity of a load or from the movement of the contents, and „injured‟ shall be construed accordingly.
Loads A load in this context must be a discrete moveable object. This can be a person or an inanimate object. This includes, for example, a patient receiving medical attention. An implement, tool or machine is not considered to constitute a load while in use for its intended purpose.
Moving and
handling operations Means any transporting or supporting of a load (including the lifting, putting down, pushing, pulling, carrying or moving thereof) by hand or bodily force. The human effort may be direct or indirect. Introducing mechanical assistance, e.g. a powered hoist, may reduce but not eliminate moving and handling, since human effort is still required to move, steady or position the load.
Risk The likelihood of harm being realised. Risk therefore reflects both the likelihood of that harm and its severity.
12. References and further reading A Guide to the reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) HSE 1995. HMSO Back Care (RCN). The Guide to the Handling of People. 5th Edition 2005 (ISBN – 09530582-9-8) Backs to Work. A Guide to back care and Manual Handling. Nicola Hunter (2000) Getting to Grips with Manual Handling. A short guide for employers. HSE Guidance on Manual Handling in Treatment ACPIN 2001 (CSP) HSAC 1998 Manual Handling in the Health Services (ISBN 0 7176 1248 1)

HS04 Moving and Handling
24
Health and Safety at Work Act (1974) Health and Safety Executive (2006) Health and Safety Statistics Health and Safety Executive 2007 SIM 7/2007/10 PUBLIC SECTOR PROGRAMME 2007/08- HEALTH AND SOCIAL CARE SERVICES UNIT (HSCSU): ELECTRIC PROFILING BEDS Health and Safety Executive 2007 Manual Handling Training. Investigation of current practices and development of guidelines. Research Report RR583. HSE Books Lifting Operations and Lifting Equipment Regulations (1998) Management of Health and Safety at Work Regulations (1999) HMSO Manual Handling Operations Regulations (1992) (as amended) Standards in Manual Handling (Third ed. 2010) National Back Exchange Manual Handling Training Guidelines (2001) National back Exchange Manual Handling Training Guidelines (1996) Royal College of Nursing Manual Handling. Putting you in the picture. A guide to back care and Moving and Handling for health care workers. Worksafe (2003) National Back Exchange. Trainer guidelines (2002)
Nursing and Midwifery Council (2002) Practioner-client relationships and the prevention of abuse.
NMC (2002) The Code of professional Conduct Ferguson-Burt (2007) Profiling Beds. A literature review. Column. Vol 19.2 Summer 2007. National Back Exchange ISBN 1461-0922 Provision and Use of Work equipment regulations (1992) (Revised 1998) Royal College of Nursing (1996) Code of practice for the Handling of Patients. Royal College of Nursing (2002) Introducing a Safer Patient Handling Policy. Ref 000603 Royal College of Nursing (2003) Manual Handling Assessments in Hospitals and the Community Ref 000 605 Training. Back in Work Campaign Info sheet No.4. NHS (2002) Understanding Egonomics at Work. HSE

HS04 Moving and Handling
25
13. Consultation and Proposed Implementation Plan
Number & title of document:
Moving & Handling Policy
Date finalised: April 2010
Groups and individuals involved in the development and consultation:
Health & Safety Managers and Advisors
Health & Safety Committees from the three legacy sites
Implementation Lead: Print name and contact details:
Tony Pays
Estates & Facilities, Head of Safety & Emergency Planning
0208 302 2678 ext 4747
Previous document already being used?
Yes
If yes, in what format and where?
Trust Intranet and Trust policy files held locally
Proposed action to retrieve out-of-date copies of the document:
Intranet version replaced by updated document by Trust Policy Co-ordinator, Trust policy file copies updated locally triggered by receipt of global email.
Is training required to support implementation?
No
Outline plan to deliver training, if required:
Not applicable
To be disseminated to: How it will be disseminated
By whom? Timescale Paper or Electronic
All staff Global email Communications 2 weeks after approval
All Staff Placed on Trust Intranet
Tony Pays 1 week after approval
Outline any additional activities planned to support implementation:
None

HS04 Moving and Handling
26
14.Initial Equality Impact Assessment
Directorate/Care Group/Dept
Service/Policy title Assessor (s) New or existing
Policy /service
Date of Assessment
HEALTH AND SAFETY Moving and Handling
Policy
Julie Seal Revision 1ST
November 2009
1. Who is responsible for the Service
(function) or policy that is being
assessed?
Julie Seal. Manual Handling Adviser (QMS)
2. Describe the aims, objectives and
purpose of the service/policy.
Reduction in musculoskeletal injuries to staff and patients through compliance with Moving and
Handling Operations Regulations (1992)
3. Are there associated objectives of
the service/policy? - If so please
explain.
e.g. National Service Framework
National Targets
Legislative Compliance
4. Who will benefit from this
service/policy?
Staff, patients, visitors
HS04 Moving and Handling
27
HS04 Moving and Handling
28
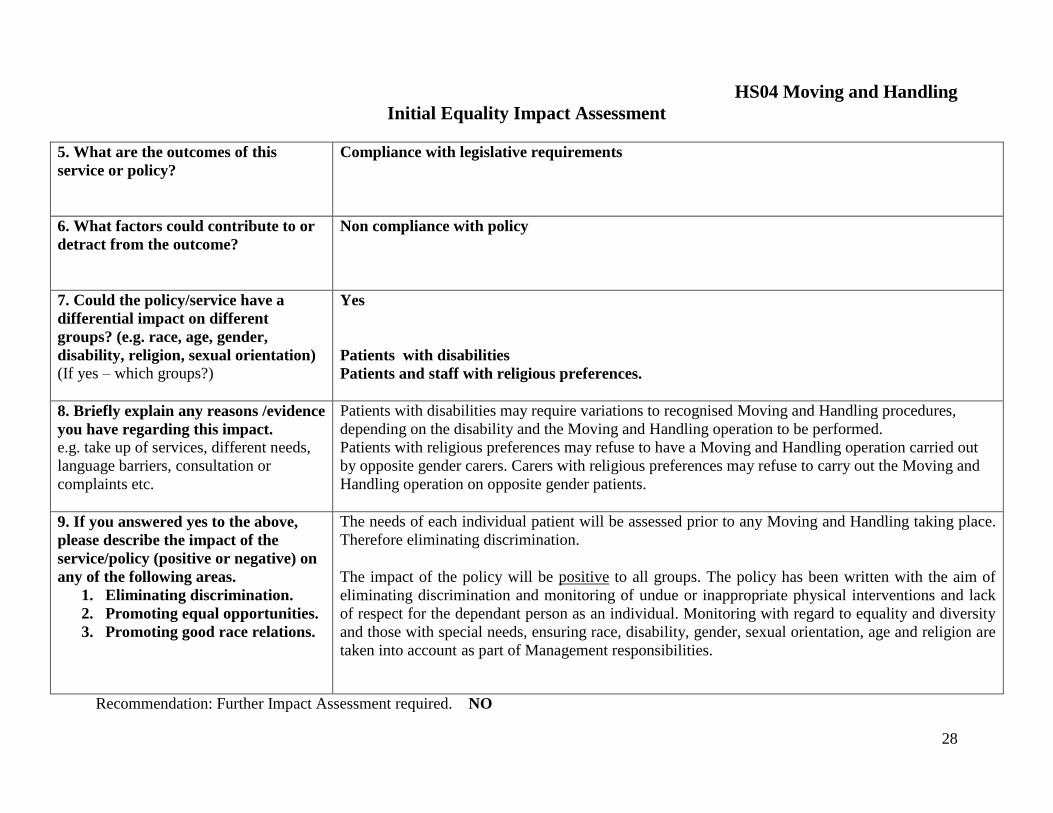
Initial Equality Impact Assessment
5. What are the outcomes of this
service or policy?
Compliance with legislative requirements
6. What factors could contribute to or
detract from the outcome?
Non compliance with policy
7. Could the policy/service have a
differential impact on different
groups? (e.g. race, age, gender,
disability, religion, sexual orientation)
(If yes – which groups?)
Yes
Patients with disabilities
Patients and staff with religious preferences.
8. Briefly explain any reasons /evidence
you have regarding this impact.
e.g. take up of services, different needs,
language barriers, consultation or
complaints etc.
Patients with disabilities may require variations to recognised Moving and Handling procedures,
depending on the disability and the Moving and Handling operation to be performed.
Patients with religious preferences may refuse to have a Moving and Handling operation carried out
by opposite gender carers. Carers with religious preferences may refuse to carry out the Moving and
Handling operation on opposite gender patients.
9. If you answered yes to the above,
please describe the impact of the
service/policy (positive or negative) on
any of the following areas.
1. Eliminating discrimination.
2. Promoting equal opportunities.
3. Promoting good race relations.
The needs of each individual patient will be assessed prior to any Moving and Handling taking place.
Therefore eliminating discrimination.
The impact of the policy will be positive to all groups. The policy has been written with the aim of
eliminating discrimination and monitoring of undue or inappropriate physical interventions and lack
of respect for the dependant person as an individual. Monitoring with regard to equality and diversity
and those with special needs, ensuring race, disability, gender, sexual orientation, age and religion are
taken into account as part of Management responsibilities.
Recommendation: Further Impact Assessment required. NO

HS04 Moving and Handling
29

HS04 Moving and Handling
30
Performance Criteria
15. MOVING AND HANDLING PERFORMANCE CRITERIA
GENERIC HANDLING
A suitable and sufficient risk assessment must be performed prior to attempting any manual handling manoeuvre.
Application: These performance criteria can be utilised to assess competency for a wide range of
manual handling tasks. Competency Statement: The handler performs the manual handling operation selected in a manner that minimises the risk of injury to all individuals participating in the manoeuvre.
Performance Criteria: Performance criteria assessed during formal teaching sessions: 1. The handler positions themselves appropriately to perform the manoeuvre. Close
enough to the load to reduce any bending or stretching that could otherwise be required. 2. The handler positions feet and legs to form a stable base. Both feet should be flat on
the floor with the leading foot pointing in the direction of movement. 3. The leg muscles and bodyweight are used to achieve the movement. This is achieved
by keeping the knees relaxed and transferring power through the larger leg muscles. Rhythm and momentum can be used (preferably single cycle) to move the load avoiding jerking.
4. The back is maintained in a suitable erect posture throughout the manoeuvre 5. The shoulders are kept even and in alignment to avoid twisting 6. A firm, comfortable grip is taken at a suitable point in relation to the load using both the
palm and fingers of the hand. 7. The arms are positioned to allow the load to be held as close to the body as is
reasonably practicable. 8. The head is held up and not twisted to maintain a natural posture and ensure that
obstacles can be seen. 9. Clear, appropriate commands are used, e.g. “Ready – Steady – Lift/Slide” when team
handling other individuals are involved. Performance criteria specific to assessments conducted in the workplace or during problem solving sessions: 10. Where equipment is required the handler must identify the appropriate item and
use it correctly.

HS04 Moving and Handling
31
A. MOVING A PATIENT UP/DOWN THE BED/TROLLEY ON SLIDE SHEETS
A suitable and sufficient risk assessment must be performed prior to attempting any manual handling manoeuvre.
Suitability: The most suitable method is when the patient can be accessed from the ends of the bed depending on which direction they need to move. At least two handlers are recommended for the manoeuvre. However, following a suitable risk assessment regarding the size and ability of the patient, more carers may be required to assist at each side of the patient.
Competency statement: The handler slides the patient up/down the bed/trolley in a manner that minimises the risk of injury to both the handlers and patient.
Performance Criteria: Performance criteria to be assessed during formal teaching sessions:
A handling assessment is completed, updated and referred to
The patient is positioned supine on flat handled slide sheets to facilitate the movement effectively and comfortably.
1. The Handlers positions themselves at the end of the bed/trolley towards which they
need to move the patient. They are at one end (not the side) of the bed facing towards the opposite end.
2. The handler‟s feet are hip width apart with the leading foot braced against the bed
frame or as close as possible to the bed. The trailing foot is a comfortable step behind
3. Throughout the move, the knees of the handler should be soft to allow them to
transfer their weight from over their leading leg, through their base and onto the trailing leg, in order to effect the movement. Momentum - By taking their weight forward over the leading leg immediately prior to the manoeuvre backwards, a safer and smoother and more comfortable technique will be effected for both Handler and patient.
4. The back is kept in a suitable erect posture during the movement by having the bed
at the correct height for the Handlers
5. The Handlers reach forward comfortably to the slide sheet handles keeping the shoulders in alignment and avoiding twisting
6. The handler grips the handles of the top slide sheet in front of them without over-
reaching.
7. The arms are comfortably outstretched to the slide sheet handles

HS04 Moving and Handling
32
8. As the movement is effected by the transfer of weight to the trailing leg the Handlers
heads are raised into alignment with the spine.
9. Clear, appropriate commands are given by one of the Handlers. Ready? – Steady – Move. Both Handlers‟ bodyweight move forward on the command Ready. The momentum gained then initiates the movement of bodyweight backwards thus effecting the change of position for the patient.
Performance criteria specific to assessments conducted in the workplace or during problem solving sessions:
10. To make a more effective movement two extension handles can be attached to either side of the slide sheet via handles at the patient‟s hip level. This must not involve the Handler in over-reaching.
11. If the Handlers are unable to access from the ends of the bed/table then they should
stand either side of the bed/trolley at the patient‟s hip level, facing one end of the bed and with their back to the direction they and the patient will travel. They hold the appropriate slide sheet handle close to them and at that level with their inner hand. The other hand is supported on their own thigh. The outer foot is forward and their bodyweights will move forward and then back onto the inner trailing foot to effect the movement

HS04 Moving and Handling
33
B. INSERTION & REMOVAL OF SLIDE SHEETS
A suitable and sufficient risk assessment must be performed prior to attempting any manual handling manoeuvre.
Suitability: Suitable for use when a patient needs assistance to roll on a bed /trolley; move up/down the bed/trolley; for insertion of a suitably sized sling; to facilitate a supine lateral transfer. Two people are required to carry out these manoeuvres, with an extra person required if inserting
a hoist sling. Competency statement: The handlers move the patient in a manner that minimises the risk of injury to both the
handlers and patient. Performance Criteria: Performance criteria to be assessed during formal teaching sessions are below for Method 2:
A handling assessment is completed and referred to
Assessment should define whether standard or extra large size slide sheets are required
Two flat slide sheets with non-handled sides together are prepared
Assessment should define whether the slide sheets are inserted directly under the patient i.e. on top of the sheet, or between the bed surface and the sheet
A decision is made as to the method of insertion:- Method 1 – Insertion while patient rolled on side Method 2 - Insertion while patient lying supine
Method 1 – Insertion while patient rolled. This is carried out while the patient is rolled onto their side as in the “Rolling” Competency. Handler 2 holds the slide sheet in the middle third of its length and either rolls/concertinas approximately 1/3rd the width of the slide sheet which is then placed on the bed close to the patient. The rolled/concertinaed slide sheet edge is then gently pushed under the rolled patient between bed and patient. Ensuring that there is adequate length of slide sheet under the patient‟s head and adequate width of slide sheet for the patient‟s hips and shoulders, the patient is rolled onto their back in a controlled manner. The rolled/concertinaed slide sheets are then pulled through from under the patient by Handler 1, beginning at the lumbar region
of the patient. This should avoid rolling the patient again.
Method 2 - Insertion while patient lying supine
1. With the slide sheets prepared Handlers 1 & 2 position themselves on either side of the trolley/bed facing each other. The slide sheets are either placed lengthways on the bed surface or rest on the patient. The slide sheets are then rolled or folded over, equivalent to two hand-holds length, from top to bottom leaving the two ends underneath. The roll is then flipped over so that the two ends are on top leaving the roll underneath. This is then positioned under the head (and pillow) of the patient and gently pulled into position under their shoulders. The Handlers now face forward at the level of the patients shoulders, close to but at right angles to the bed.

HS04 Moving and Handling
34
2. The feet of both Handlers are hip-width apart with their outer leading foot forward and
the trailing foot a comfortable step behind, as close to the bed as possible.
3. Throughout the move the knees of the Handlers should be soft to allow them to transfer their weight, initially forward onto their leading leg and then backwards through their base and onto the trailing leg to effect the gradual unfurling of the slide sheets. As each part of the slide sheets are unfurled the Handlers must step back and repeat the process until the slide sheets are flat under the patient.
4. The backs of the Handlers should be kept in a suitable erect posture during the
movement as the movement is effected through weight transference.
5. As the Handler‟s outer arms exert some traction on the upper two ends of the slide sheets at about the patient‟s shoulder level, the inner arm facilitates gradual unfurling of the slide sheet downwards under the patient towards the foot-end of the bed. The Handlers‟ shoulders should stay in alignment to avoid twisting.
6. The outer hand grips the top two slide sheets at the patient‟s shoulder level exerting
some tension between the two Handlers‟ grips. The inner hand slides under the roll of slide sheet and holds the roll at the top end. As the slide sheet is unfurled these grips have to be re-instated at the next level to be unfurled, until the slide sheets are flat under the patient.
7. The arms are comfortably positioned always maintaining a stance close to the bed
and at the corresponding level being unfurled
8. The Handlers heads should be raised and in spinal alignment as they make the weight transfer movement through their bases which effects the movement of unfurling the slide sheets
9. Clear appropriate commands are used e.g. Ready? - Steady – Move as each part of
the slide sheet is unfurled under the patient. This maintains co-ordination between the Handlers.
Performance criteria specific to assessments conducted in the workplace or during problem solving
sessions:
10. If the slide sheets become difficult to unfurl the Handlers must not keep exerting pulling forces. By inserting their hands into the slide sheet roll on either side of the patient difficult areas can be eased/smoothed out.
11. Removal of the slide sheets is effected when each Handler passes the corner of a
slide sheet across to the other (usually at the foot end), always passing it under the slide sheet. The receiving Handler then gently withdraws the leading edge of the slide sheet from under the patient keeping in line with the force required to effect the movement.
12. In theatres the insertion of the slide sheets has to be from the feet end of the patient.
The slide sheet are rolled/folded in the same way but placed with the ends on top under the patients legs, with the roll just above the level of the table-break. The Handlers face towards the foot-end of the table and unfurl the slide sheets towards and under the patient‟s head, using the techniques described above.

HS04 Moving and Handling
35
C. LIFTING A BOX FROM A LOW LEVEL
A suitable and sufficient Risk Assessment must be performed prior to attempting any Manual Handling Manoeuvre.
Suitability:
Suitable for use when the area is cleared of obstacles and there is adequate space to adopt a safe posture and the load has been assessed as within the capability of the handler. If the assessment identifies the need for assistance from more handlers or for the use of appropriate equipment then this should be followed.
Competency statement:
The handler lifts the box in a manner, which minimises the risk of injury to themselves.
Performance Criteria: Performance criteria assessed during formal teaching sessions:
Assessment of the load, environment and equipment available
Appropriate positioning of the load prior to the manoeuvre
1. The handler positions themselves close to the load facing in the direction of travel.
2. The leading foot is placed beside the load, level with it and facing in the direction of movement. The trailing foot is hip width away and a comfortable distance behind, facing slightly outwards.
3. The knees of the handler should be relaxed and flex to allow the body to sink down
beside the load. One knee should be placed on the floor to stabilise the handler when assessing the load and taking a grip. Gradually straightening the knees and rising in the direction of the movement can then carry out the lift.
4. The back is maintained in an erect posture throughout the lift raising the head as the
body rises
5. The shoulders are kept even and in alignment to avoid twisting
6. A firm comfortable grip is taken using the palm and fingers of both hands. One hand will support the load and the other maintain the load close against the body
7. The arms are bent to hold the load against the pelvic/waist area of the body.
8. The head is raised looking in the direction of movement to see obstacles and to align
the spine
9. If there is more than one handler the process must be explained to all and clear commands used i.e. READY? – STEADY – LIFT.
With Aids – These must be chosen appropriately and loaded/unloaded safely according to instructions.

HS04 Moving and Handling
36
D. ROLLING
A suitable and sufficient risk assessment must be performed prior to attempting any manual handling manoeuvre.
Suitability: Suitable for use when the patient can be accessed from either side of the couch/bed. At least two handlers are recommended for the manoeuvre However, following a suitable risk assessment regarding the size and ability of the patient, one carer may perform it, or alternatively six to eight carers for a very large dependent patient.
Competency statement: The handler rolls the patient onto their side in a manner that minimises the risk of injury to both the handlers and patient.
Performance Criteria: Performance criteria to be assessed during formal teaching sessions:
A handling assessment is completed, updated and referred to
The patient is positioned appropriately to facilitate movement, promote independence and avoid injury through rolling onto their hands.
The patient may be positioned on flat handled slide sheets to facilitate the roll more effectively and comfortably.
1. The handler positions themselves on the side of the bed towards which the patient
will roll, facing the opposite side of the bed, standing at the level corresponding to between the level of the patient‟s hip and shoulder region
2. The handler‟s feet are hip width apart with the leading foot braced against the bed
frame or as close as possible to the bed. The trailing foot is a comfortable step behind
3. Throughout the move, the knees of the handler should be relaxed to allow them to
transfer their weight from their leading leg, through their base and onto the trailing leg in order to effect the movement. Momentum is gained - By taking their body weight forward over the leading leg prior to moving their weight backwards and a safer and smoother and more comfortable technique will be effected.
4. The back is kept in a suitable upright posture during the movement 5. The reach should be even, keeping the shoulders in alignment to avoid twisting 6. The handler places their hands on the pelvic and shoulder girdles of the patient,
avoiding pulling on the arms or knee. 7. Not using slide sheets:
a. the arms of the handler are comfortably outstretched, the movement of the patient being achieved by the transfer of the carer‟s bodyweight.
Using Slide sheets:

HS04 Moving and Handling
37
b. the arms of the Handler 1 are comfortably outstretched ready to move their weight onto the trailing leg as the patient rolls towards them. Handler 2 on the opposite side of the bed and facing Handler 1 takes hold of the handles of the top glide sheet at the level of the shoulders and hips of the patient, having adopted a base with one foot forward close to the bed and the other a comfortable step behind.
8 Not using slide sheets:
a. The handler‟s head is held up as the movement is effected. The transfer of bodyweight is initially towards and then away from the patient, giving momentum and a smoother, more comfortable movement.
Using slide sheets: b. Both handlers bring their heads up into spinal alignment as the
technique is effected.
9. Not using slide sheets: a. The handler must use clear appropriate commands e.g. Ready? -
Steady – Roll. The patient rolls onto their side as the handlers weight is transferred
Using slide sheets: b. Handler 1 uses clear commands e.g. Ready? - Steady –Roll. Handler
2 effects the rolling of the patient as they transfer their bodyweight, initially forwards and then back away from the patient, keeping the arms comfortably outstretched. This can be a slow and steady manoeuvre. If the roll is incomplete, reposition and repeat.
Performance criteria specific to assessments conducted in the workplace or during problem
solving sessions:
10. For very large patients other methods may be taught to reduce any reaching across the patient

HS04 Moving and Handling
38
E. SITTING TO STANDING
A suitable and sufficient risk assessment must be performed prior to attempting any manual handling manoeuvre.
i.e. The handler identifies whether or not the patient is capable of weight bearing and balance before commencing this manoeuvre.
Suitability:
Suitable for use when handlers can access the patient by standing to the sides, i.e. the patient is seated in a chair or wheelchair. Two handlers are recommended for this manoeuvre although, following a suitable risk assessment, one may perform it.
Competency Statement: The handler stands the patient in a manner that minimises the risk of injury to all individuals involved in the manoeuvre.
Performance Criteria: Performance criteria assessed during formal teaching sessions: 1. The handler stands to the side of the patient facing forward and as close to the chair as
possible.
2. The inner trailing foot of the handler should be level with the patient‟s hips and shoulders.
The lead foot should be in line with the patient‟s feet, facing in the direction of movement.
3. The knees of the handler should be flexed to allow their body weight to be rocked from the
trailing leg to the leading leg whilst keeping the centre of balance of the patient inside their
base. Handlers must not swing their arms to achieve patient movement. Knees can be
straightened to stand with the patient when the command to stand is given.
4. The back is maintained in an erect posture throughout the manoeuvre with the
bottom tucked in. The whole body is moved in time with the commands, by transferring weight from the trailing foot to the lead foot, in order to utilise the body weight of the handler and maintain alignment of the back.
5. The shoulders are kept even and in alignment to avoid twisting 6. a. Without aids:
The trailing hand should be placed down the patient‟s back as far as is possible without
compromising the carer‟s posture. The lead hand should be placed in order to exert control of
the patient‟s balance on completion of the manoeuvre. This may be achieved by placing the
lead hand below the shoulder closest to the handler, or by taking the nearest hand to the
handler using a “palm to palm” grip with the patient‟s thumb over the palm of the handler.
b. Using the transfer belt:
HS04 Moving and Handling
39
The trailing hand takes firm hold of the belt loop-handle closest to the handler situated at the back of the patient. The lead hand of the handler is placed below the patient‟s shoulder closest to the handler or the nearest hand to the handler using a “palm to palm” grip with the patient‟s thumb over the palm of the handler.
7. a. Without aids:
The trailing arm is kept close to the bodies of both handler and patient by positioning the handler as close to the patient as possible. The handler avoids over-extending the lead arm by holding close to them wherever possible ensuring that the patient‟s arm is kept low and flexed at the elbow.
b. Using the transfer belt:
By holding the belt loop-handles on the side nearest the handler they avoid the need to over-reach and bend forward excessively.
8. The head of the handler is held up and not twisted, looking forward in the direction of
travel. 9. Clear, appropriate commands are used, e.g. “Ready – Steady – Stand”, in time with
the rocking motion of the handler‟s body with both patient and handler straightening their legs on the command to stand.
Performance criteria specific to assessments conducted in the workplace or during problem solving sessions:
10. The handler identifies whether or not the patient is capable of weight bearing and balance before commencing the manoeuvre.
11. The handler must identify that the patient is correctly positioned in their seat to be capable of standing when assisted.
12. Having identified that the use of the transfer belt is not contra-indicated by any pre-existing condition that the patient may have, the handler selects appropriately sized equipment to minimise discomfort. There should be no more than a 10 to 15 cm gap at the front of the belt once fitted correctly.
HS04 Moving and Handling
40
F. SUPINE LATERAL TRANSFER
A suitable and sufficient risk assessment must be performed prior to attempting any manual-handling manoeuvre.
Suitability: Suitable for use when the patient requires transferring from bed/bed or bed/ trolley and if, when the two surface are adjacent to each other there is sufficient access at both sides of the trolley/bed to allow safe movement technique for the handlers. At least three handlers are recommended for the manoeuvre. However, following a suitable risk assessment regarding the size and ability of the patient more handlers may be required.
Competency statement: The handlers transfer the patient in a manner that minimises the risk of injury to both the handlers and patient.
Performance Criteria: Performance criteria to be assessed during formal teaching sessions:
A handling assessment is completed and referred to
The patient is positioned appropriately on two flat, handled glide sheets to facilitate movement and patient comfort. Extension handles are inserted appropriately.
Approximately half the Pat-slide is inserted under the patient
1. Handlers 1 & 2 position themselves on the far side of the surface/bed onto which the patient will transfer across, facing the opposite side of the surface/bed, one standing above and the other below the patient‟s pelvic region. Handler 3 positions themselves on the opposite side of the surface/bed facing Handlers 1&2 at a level between the patient‟s pelvis and shoulder.
2. The feet of Handlers 1&2 are hip width apart with the leading foot forward and as
close to the bed as possible, the trailing foot a comfortable step behind. Handler 3 adopts a similar stance on the opposite side of the bed.
3. Throughout the move the knees of Handlers 1&2 should be soft to allow them to
transfer their weight, initially forward onto their leading leg and then through their base onto the trailing leg, in order to effect the transfer movement. Meanwhile Handler 3 is transferring weight initially from the trailing leg and through onto the leading leg to assist the movement.
4. The backs of all handlers should be kept in a suitable erect posture during the
movement. Handlers 1 & 2 must not arch their back to complete the movement. Instead they may need to take a further step back to allow more movement. Handler 3 must not over-reach and compromise spinal posture.
5. Handlers 1&2 should be able to reach the extension handles keeping their reach
even and shoulders in alignment to avoid twisting. Handler 1 will hold the two top straps; Handler 2 the bottom two straps. Handler 3 positions between the shoulder and pelvis of the patient, in order to keep the shoulders in alignment.

HS04 Moving and Handling
41
6. Stage 1- Handlers 1&2 hold the extension straps comfortably but must not wrap
them around their hands. Handler 3 places the palms of their hands on the pelvic and shoulder girdles of the patient in order to assist by pushing across gently. Stage 2 - As the patient is moved halfway across Handler 3 can no longer assist the movement due to compromised posture. Handlers 1 & 2 step back in to the bed and hold the top slide sheet handles prior to the final weight transference to move the patient into position on the new surface/bed.
7. The arms of the Handlers are comfortably outstretched, the movement of the
patient being achieved by the transfer of the carer‟s bodyweight, i.e. Handlers 1 & 2 transferring their weight back through their base and Handler 3 taking weight forward.
8. The handler‟s heads are in alignment as the movement is effected
9. The handler must use clear appropriate commands telling the group how far to
move the patient at each stage e.g. Ready? - Steady – Move! Performance criteria specific to assessments conducted in the workplace or during problem solving
sessions:
10. If clinically required a Handler must be allocated for management of the patient‟s head during the transfer.
11. The extension handles to promote better spinal positioning and handgrip for the
handlers must be inserted into the handles of the top slide sheet:- one near the feet; one at the head and neck region and the remaining two spaced around the heavier pelvic region
12. The pat-slide should be inserted between the sheet and slide sheets from the side
of the bed to which the patient is moving, avoiding rolling the patient
13. If required a third slide sheet is put on the receiving surface to facilitate patient positioning.
14. The two transfer surfaces are then brought together at a corresponding height that
suits the handlers. Brakes on. Bed ends removed in a safe manner, if necessary.
HS04 Moving and Handling
42
G. Hoisting with the Arjo Maxilift/Maximove
Patient considerations: No hip instability
Amputees need to have appropriate amputee sling
Check patient‟s weight to ensure does not exceed the Safe Working Load (SWL) of the hoist
Maxilift SWL = 160kg/25stone
Maximove SWL = 190kg./30stone.
If patient exceeds these weights refer to your local Heavy patient Procedure
Resources required: Hoist
Suitable size of sling (fold in half length-ways and ensure covers from coccyx to top of patient‟s head
Check no holes or frayed thread in the sling and clips intact
Check hoist battery is charged
2 trained and competent members of staff as a minimum dependent on the risk assessment
Technique
Roll patient to fit sling
Position hoist and lower boom adequately to avoid lifting the patient when fitting the sling to the hoist
Attach sling to four-point spreader bar and check for a positive click
Lift with the hoist or lower the bed down
Manoeuvre hoist to receiving surface ensuring any turning of the hoist does not involve twisting the carer‟s spine
Lower hoist, position patient upright with the spreader bar before they are lowered onto chair/commode
If the chair tips as the patient is lowered this will enable a better seated position for the patient
Lower boom adequately prior to removing clips to prevent lifting patient‟s weight
When removing leg channels of the sling ensure posture is not compromised (kneel on floor)
When removing leg channels of sling ensure the ends are either tucked under themselves and peeled away or slide sheets inserted – to avoid sheering the patient‟s skin
If hoisted into chair/commode – sit patient forward with carer on either side facing patient and supporting from scapula with close hands , step back and remove sling.
From Floor
As above but position hoist legs wide, one under head (with pillow) and one under the knees
To reposition up the bed
Raise patient with hoist, as above.
Put bed brakes off, move bed down into position and lower patient onto bed. Never apply brakes to the hoist - unless on a slope or left unattended
Infection Control. Washable slings should be used for one patient only and kept in their locker. They
must be laundered prior to use with another patient according to the Laundry and
Cleaning Procedure for Manual Handling Equipment in SLHT.

HS04 Moving and Handling
43
Wipe-clean slings must be wiped with:
NON INFECTED Use soap and water or use a Deb Cutan multi surface soapy wipe
FOUL/INFECTED Use Chlor-clean solution (1000ppm sodium chloride) between
patients
All hard surfaces which have had contact with the patient e.g. elbow support, handholds and
commode seat if used, should be wiped down between patients with:
NON INFECTED Use soap and water or use a Deb Cutan multi surface soapy wipe
FOUL/INFECTED Use Chlor-clean solution (1000ppm sodium chloride)

HS04 Moving and Handling
44
ARJO SARA PLUS STANDING HOIST
GUIDELINES FOR USE
Compiled by: Sheila Muffett - Moving & Handling Advisor
Date: April 2007
Review Date:
Comments on this document to: Moving & Handling Co-ordinator
Email: [email protected] Tel. 0208 836 654

HS04 Moving and Handling
45
H. ARJO Sara Plus/Encore Standing Hoist Guidelines
UNDERLYING GUIDANCE All Users require training prior to use. Each individual handler needs to complete a risk assessment prior to use (see Appendix 1). Physiotherapists need to complete the Therapeutic Manual Handling Risk Assessment (see Appendix 2). Physiotherapists may advise as part of multi-disciplinary goal setting. Decide your objective for using the Standing hoist. Assess patient‟s suitability for using the hoist. Always communicate your intentions to the patient. Be aware of safe posture during application/removal of slings and other appliances e.g. footplate, knee pad commode and battery (all of which are heavy).
If the footplate is removed for walking, two people should carry this out, one on each side. When the patient is in standing the knee support can be removed in a similar way, after having applied the hoist brakes.
CHECKS PRIOR TO USING Prior to using the standing hoist ensure that the:
Battery is charged.
Hoist has been serviced every 6 months and there is a visible date.
Weight of patient does not exceed safe working load (190kg/30stone).
Correct size and type of sling must be selected: The loops of the sling must be 3-4 inches from the hip bone. Velcro waist strap must overlap a minimum 4 inches.
Check stitching and clips on sling. If frayed or broken the sling must be withdrawn from use and replaced.
Patients must have adequate tone in the hips and knees.
Patients must be alert and compliant.
Do not use this hoist with confused patients.
Two handlers must always be available when standing a patient with the standing
hoist.
USE of hoist:
PUT THE BRAKES ON WHILE
connecting/disconnecting patient & sling to/from hoist
If the walking harness is used:
Position the walking harness using a small slide sheet.
Ensure that all straps are securely fastened: 2 waist straps – connect to top loop at each side of sling. 2 safety straps – connect to side of boom arm. 2 leg straps – connect to harness.

HS04 Moving and Handling
46
If other standing slings are used:
Ensure the waist straps of the sling are securely fastened by the main ropes
Bring Sara Plus hoist to patient placing heels at the rear of the foot plate (this ensures a straight leg position).
Adjust knee plate just below the knee.
Invite the patient to place arms onto the arm rests.
If the patient has an arm weakness velcro wrist straps can be purchased.
If the patient has a lower limb weakness velcro leg straps can be purchased.
Secure tensioning ropes into side loops of sling.
NB:
Raising the rope will release the tension in order to slacken the rope.
To tighten pull the rope towards the main column of the hoist and lower into slot.
Fully tighten both ropes to ensure patient is in a „nose over toes‟ position. The handler with the remote control stands next to patient to guide and
reassure.
GENERAL POINTS This hoist is not for transporting the patient from one area of the ward to another unless:
The walking process is being professionally applied i.e. with the physio‟s
The commode seat can be used to support the patient comfortably for toileting or for short transportation to the ward toilet.
If the commode seat is used the legs of the hoist must be kept in. It is dangerous to try and widen the hoist legs with the commode seat in
situ.
The hoist should be used for transferring the patient from the sitting to sitting position e.g. bed to chair:
Ensure patient‟s calves are in contact with the chair/bed prior to lowering into the sitting position.
Ensure chair is appropriate width to accommodate the hoist legs when they are widened.
Check all straps are secure.
Check leg position – widen the hoist base.
Operate handset.
Once patient comes to rest, remove sling in reverse order and remove hoist.
Infection Control. Washable slings should be used for one patient only and kept in their locker. They
must be laundered prior to use with another patient according to the Laundry and
Cleaning Procedure for Manual Handling Equipment in SLHT.
Wipe-clean slings must be wiped with:
HS04 Moving and Handling
47
NON INFECTED Use soap and water or use a Deb Cutan multi surface soapy wipe FOUL/INFECTED Use Chlor-clean solution (1000ppm sodium chloride) between patients All hard surfaces which have had contact with the patient e.g. elbow support, handholds and commode seat if used, should be wiped down between patients with: NON INFECTED Use soap and water or use a Deb Cutan multi surface soapy wipe FOUL/INFECTED Use Chlor-clean solution (1000ppm sodium chloride) References Arjo SARA Plus Operating and Product Care Instructions Oct. 2006 Arjo SARA Preventive Maintenance schedule May 2006

HS04 Moving and Handling
48
KJAERULFF MINILIFTER
STANDING HOIST
GUIDELINES FOR USE
Compiled by: Sheila Muffett - Moving & Handling Advisor
Date: 2008
Review Date: 2010
Comments on this document to: Moving & Handling Co-ordinator

HS04 Moving and Handling
49
I. KJAERULFF Minilifter Standing Hoist Guidelines
UNDERLYING GUIDANCE All Users require training prior to use.
A Patient Handling Risk Assessment must be completed prior to use. Physiotherapists need to complete a Therapeutic Manual Handling Risk
Assessment. Physiotherapists may advise as part of multi-disciplinary goal setting.
Decide your objective for using the Standing hoist. Assess patient‟s suitability for using the hoist Always communicate your intentions to the patient. Physiotherapists may remove the footplate for standing/walking practice.
Ensure that a good posture is adopted prior to removing this appliance.
Be aware of safe posture during application/removal/adjustment of slings and other
appliances e.g. footplate and knee pad.
CHECKS PRIOR TO USING Prior to using the standing hoist ensure that the:
The hoist is unplugged and the Emergency STOP button is not pushed in.
Battery is charged – N.B. this cannot be assessed while the hoist is plugged in or the Emergency stop button is pushed in.
Hoist has been serviced every 6 months and there is a visible date.
Weight of patient does not exceed safe working load (SWL) (123kgs/19stone).
Correct size and type of sling must be selected: The loops of the sling must be 3-4 inches from the hip bone. Velcro waist strap must overlap a minimum 4 inches.
Check stitching on sling. If frayed or broken the sling must be withdrawn from use and replaced.
Patients must have adequate tone in the hips and knees.
Patients must be alert and compliant.
Do not use this hoist with confused patients.
Two handlers must always be present when transferring/standing a patient with the standing hoist.
USE of hoist: PUT THE BRAKES ON WHILE connecting/disconnecting patient & sling to/from hoist unless for documented therapeutic purposes
Ensure that:- o Using the pocket on the back of the sling push down with your hand
and position the sling low on the patient‟s hips. If required, position the sling using a small slide sheet – this must be removed prior to standing the patient.
o The buckle of the sling is securely fastened and tightened to a comfortable fit.
o The loops of the sling, on both the attachments, are the same colour, equal length, and securely connected.

HS04 Moving and Handling
50
o Any slack in the connection of the sling is taken up and the screws are securely tightened up.
o The hoist is brought to the patient placing heels near the rear of the foot plate (this helps to gain a straight leg position depending on the build of the patient).
o Adjust knee plate to just below the knees and against the legs o Invite the patient to grip with their hand/hands onto the handholds. o If the patient has a flaccid arm it can be safely contained in the sleeve
provided on the side of the sling. The handler with the remote control stands next to patient to guide and reassure.
GENERAL POINTS This hoist is not for transporting the patient from one area of the ward to another unless:
The walking process is being professionally applied i.e. with the physiotherapist/s The hoist should be used for transferring the patient from the sitting to sitting position e.g. bed to chair; chair to wheelchair: When sitting the patient down ensure that :-
Patient‟s calves are in contact with the chair/bed prior to lowering into the sitting position.
Chair/wheelchair is appropriate width to accommodate the hoist legs when they are widened.
Straps are secure.
Leg position of hoist is correct – widen the hoist base.
Handset is operated with full attention on the procedure.
When patient comes to rest, remove sling in reverse order and remove hoist.
EMERGENCY LOWERING DEVICES If the handset fails to lower the patient there are two options to lower the patient safely to the chair:-
Carefully push the tip of a pen into the Emergency lower indentation just below the Emergency Stop button
Raise the top part of the red emergency lower device found at the base of the actuator. Add your own weight to raiser bar as the patient‟s weight is supported by the chair.
Infection Control. Washable slings should be used for one patient only and kept in their locker. They
must be laundered prior to use with another patient according to the Laundry and
Cleaning Procedure for Manual Handling Equipment in SLHT.
Wipe-clean slings must be wiped with:
NON INFECTED Use soap and water or use a Deb Cutan multi surface soapy wipe FOUL/INFECTED Use Chlor-clean solution (1000ppm sodium chloride) between patients
HS04 Moving and Handling
51
All hard surfaces which have had contact with the patient e.g. elbow support, handholds and commode seat if used, should be wiped down between patients with: NON INFECTED Use soap and water or use a Deb Cutan multi surface soapy wipe FOUL/INFECTED Use Chlor-clean solution (1000ppm sodium chloride)