moving mountains - congress of neurological … (nsi) and the american ... and unique educational...
TRANSCRIPT

SPRING 2009
IS THE OFFICIAL NEWSMAGAZINE OF THE CONGRESS OF NEUROLOGICAL SURGEONS
<10>
THE 80-HOUR WORK WEEK:RESTRICTIONS ON RESIDENT
EDUCATION
<28>
NEUROSURGEONS,INTENSIVISTS AND THE
FUTURE OF NEUROCRITICALCARE
MOVING MOUNTAINSCan We Handle a 48-Hour Resident Work Week?
Extending the Neurosurgical Workforce.

For More Information: [email protected] www.cns.org Toll Free: 877 517 1CNS Phone: 847 240 2500
Congress of Neurological Surgeons
2009 ANNUAL MEETING New Orleans, Louisiana
October 24-29, 2009
Registration Now Open atwww.cns.org!
Join us in New Orleans, Louisiana for the 2009 CNS AnnualMeeting, as we explore our theme A Culture of Excellence.
The Congress of Neurological Surgeons is Pleased to Announce aJoint Meeting with the Neurological Society ofIndia (NSI) and the American Association ofSouth Asian Neurosurgeons (AASAN)!
• 3-D Live Cadaveric Demonstrations
• Top Ten Abstracts Session
• CNS Neurosurgical Forum• Consensus Sessions • IML
Look for these ground-breaking original scienceand unique educational offerings!
Call for Abstracts Submit your abstract online at www.cns.org.Deadline: April 10, 2009.
Dr. APJ Abdul KalamSpecial LecturerMonday, October 26
Dr. Kalam, the former Presidentof India and an aeronauticalengineer by training, hasmade significant lifelongcontributions to the IndianSpace and Defense Programsand the education field.
Bobby JindalInvited for the 3rd Annual Julian T. Hoff LecturerTuesday, October 27
Governor Jindal, sworn in as Governor of Louisiana onJanuary 14, 2008, becamethe youngest currentgovernor in the United States. He has quicklybecome one of the mostrecognized names in politicsand is considered by many tobe on the fast-track to thenation’s highest office.
Walter Isaacson10th Annual Walter E. Dandy OratorTuesday, October 27
Mr. Isaacson is the Presidentand CEO of the AspenInstitute. He has been theChairman and CEO of CNNand the editor of TimeMagazine. He is the author of many best-sellers,including his most recent,Einstein: His Life andUniverse.
Peter Agre, MD4th Annual John ThompsonHistory of Medicine LecturerWednesday, October 28
Dr. Agre was awarded theNobel Prize in Chemistry in2003 for his discovery ofaquaporins. Currently ViceChancellor of Science andTechnology at Duke University,Dr. Agre’s research is focusedon the structural andfunctional characterization of aquaporins.
Terry Orlick, PhDMichael L. J. Apuzzo Lectureron Creativity and InnovationWednesday, October 28
Dr. Orlick is a leading authorand innovator in his creativeapproach to focus training and high level performancepsychology. His life’s work hascentered on creating a cultureof excellence and teachingand coaching the key mentalskills required to attain andsustain the highest levels ofperformance.
Don’t Miss These Outstanding Lecturers at the 2009 CNS Annual Meeting!
09AM_Ad_Speakers1r4_Q_CNS:CNSQ_CongressQuarterly 3/10/09 3:30 PM Page 1

Spring 2009Volume 10, Number 2
EDITORS:James S. Harrop, MD, FACSJamie S. Ullman, MD, FACSEDITORIAL BOARD:Aviva Abosch, MDP. David Adelson, MD, FACS, FAAPLaurie L. BehnckeEdward C. Benzel, MDNicholas M. Boulis, MDBob S. Carter, MD, PhDLangston Holly, MDZachary Litvack, MDAndre Machado, MD, PhDDaniel Michael, MDKatie O. Orrico, JDCharles Prestigiacomo, MD, FACSAlfredo Quinones-Hinojosa, MDAnn Ritter, MDJason Schwalb, MDAshwini D. Sharan, MDMichael Y. Wang, MDChristopher E. Wolfla, MDSTAFF EDITOR:April L. BoozeCOPY EDITOR:Paula NovashDESIGNER:Westbound PublicationsPUBLISHER:Carole PippinPRODUCTION MANAGER:Paul Cook
CONGRESS OF NEUROLOGICAL SURGEONS2008-2009 OFFICERS
PRESIDENT: P. David Adelson, MD, FACS, FAAPPRESIDENT ELECT: Gerald E. Rodts, Jr., MDVICE-PRESIDENT:Joel D. MacDonald, MDSECRETARY:Christopher E. Wolfla, MDTREASURER:Daniel K. Resnick, MDPAST-PRESIDENT:Anthony L. Asher, MD, FACS
CONGRESS OF NEUROLOGICAL SURGEONS MISSION STATEMENT:The Congress of Neurological Surgeons exists to enhance health andimprove lives worldwide through the advancement of education and scientific exchange.
Congress Quarterly is the official newsmagazine of the Congressof Neurological Surgeons®, located at 10 N. Martingale Road,Suite 190, Schaumburg, IL 60173. Members of the Congress of Neurological Surgeons® may call 847.240.2500 with inquiriesregarding their member subscription to Congress Quarterly.Congress Quarterly is published quarterly by Lippincott Williams& Wilkins, 351 W. Camden St., Baltimore, MD 21201-2436.
© 2009 by the Congress of Neurological Surgeons®. No part of this publication may be reproduced in any form or language without written permission from the publisher. Published free of charge for the Congressmembership with additional distribution. Annual Subscription rates:Domestic institution $86; International institution $121; Single copy $27.Send address changes to Congress Quarterly, Lippincott Williams &Wilkins, 16522 Hunters Green Parkway, Hagerstown, MD 21740-2116.Library of Congress ISSN: 1935-1526.
EDITORS’ NOTE
In this issue of the , we reflect on some of the numerous changes that the neuro-surgery community has endured over the last decade. Depending on the perspective of the individual(s) affected, these changes can either have a positive or negativeimpact on them as well as society. Thus, the challenge with implementing or adaptingto these changes is to unite all members or individuals affected such that they all havea common collective positive and united goal.
Neurosurgery as a community has been founded on the principal of a medical prac-tice focused on the simple philosophy of “excellent patient care.” This directive hasserved our profession well over the years. During this period, physicians have directedmedical care and education with internal oversight and little external pressures. Thefederal government, as the largest provider of health resources in the United States,also has the same ultimate goal and philosophy, but under the auspices of finite healthcare resources. Recently, the Institute of Medicine provided analysis for policy makerson overall patient care and physician effectiveness specifically directed at the incidenceand etiology of medical errors and patient safety. These issues of fatigue and medicalerrors were correlated to length of work hours and felt to adversely impact patientcare. Thus the federal government has initiated an 80-hour work week (increased to88 hours for several neurosurgery programs).
The medical community, as a result of these changes, had the dilemma of fewer resident patient care hours while still maintaining and improving quality patient care.This conflict has brought forward several initiatives in the neurosurgery community.Institutions have adapted to the work restrictions through reconstructing resident rota-tions in the form of a night float system, in addition to obtaining further non-residentpatient care assistance. Thus the concept of “workforce extenders” was developed inorder to maintain and potentially maximize patient care. These “teams” have devel-oped in all aspects of neurosurgical practice in terms of the Operating Room (FirstAssistants, RNFA, Surgical Assistants), hospital care (CRNP, PA) and office settings(CRNP, PA). Further, the goal of improving patient care has fostered the developmentof multidisciplinary neurosurgical patients’ groups with specialty approaches in termsof ICU teams and hospitalist services.
In this issue, first we have defined individuals affected through these changes witharticles from organized national neurosurgery, residents and fellowships. In addition,we are fortunate to have an international perspective of work hour restrictions by AlanCrockard as the European community is presently approaching a 48 hour work week.In addition, individuals from each “workforce extenders” group or team have com-posed an article detailing a definition of the scope of their field and how their membersinteract with the Neurosurgery team and patients. While each hospital has implementedan individual system, again the common goal is quality patient care.
The positive effect of these changes in terms of work hour’s restrictions has beenresident education in terms of a greater focus and “off-time” to comprehend neurosur-gical teachings. However, the corollary is that there is also less time available for directsurgical training in the operating room. The CNS, being committed to the education of neurosurgeons, is putting significant resources to improving quality patient care.This has resulted in new teaching methodologies such as the integrated medical learning (IML) courses at the national meeting and the web-based Congress ofNeurological Surgeons University (http://univ.cns.org). We are fortunate to have twoarticles discussing recent additions to the CNSU educational curriculum: PediatriceHandbooks and the 2009 Webinar Series. This issue is dedicated to all members ofthe neurosurgery team which promote continued quality patient care and education.
Editor Contact Information: [email protected] or 847.240.2500
James S. Harrop, MD, FACS Jamie S. Ullman, MD, FACS

CONTENTS
SPRING 2009 5
04 Editors’ NoteJames S. Harrop and Jamie S. Ullman
06 President’s MessageP. David Adelson
THE NEUROSURGERY WORKFORCE
08 The Neurosurgery Workforce ofthe FutureJames S. Harrop
10 The 80-hour Work Week:Restrictions on ResidentEducationDaniel L. Barrow
12 Neurosurgery Subspecialization,Fellowships and CASTDavid G. Piepgras
14 The 80-hour Work Week From aResident’s PerspectiveKrystal Tomei
16 Can the Neurosurgery WorkforceHandle a 56-hour Week?Alan Crockard
19 Physician Assistants Contributeto Quality of Life forNeurosurgeons and PatientsBrenda D. Hill and Ian Jones
21 The Nurse Practitioner and TheNeurosurgical Healthcare TeamJennifer Malone
23 Registered Nurse FirstAssistants and theNeurosurgical TeamDiane L. Ferrara and Rita Griffith
25 What Surgical Assistants Do toHelp Neurosurgeons asWorkforce ExtendersDaniel D. Baird
28 Neurosurgeons, Intensivists andthe Future of Neurocritical CareAlex B. Valadka, Michael Fehlings,Erol Veznedaroglu and P. David Adelson
31 Hospitalists on theNeurosurgical TeamScott A. Flanders and Patrick J. Cawley
SECTION NEWS
34 News and Upcoming Events inFunctional NeurosurgeryJason M. Schwalb
INSIDE THE CNS
37 Proposed Bylaws AmendmentAlan Scarrow
39 The CNS University ofNeurosurgery Launches NewWebinar Series Jamie S. Ullman
40 The CNS University ofNeurosurgery Introduces the E-Handbook Ann M. Ritter
INTERNATIONAL REPORT
42 The CNS Goes to Dubrovnik:Highlights of the Joint Meetingwith the Croatian NeurologicalSociety Miroslav Vukic, Josip Paladino andCharles Y. Liu
THE CNSQ BACK PAGE Images in Neurosurgery

In this issue of the , the editorsaddress important concerns within theneurosurgical community as they relate to
workforce and our ability to sufficiently andsafely provide care to patients. Due to innu-merable pressures both financial and tempo-ral, the practicing neurosurgeon is beingforced to do more and more with less and less.Unfortunately, these significant financial andworkforce pressures will likely continue toworsen given the economic and political climate, and will impact the neurosurgicaldelivery of healthcare. Whether due to declin-ing reimbursement, increasing medical liabili-ty concerns both real and perceived, impossi-ble requirements for emergency coverage(such that every neurosurgeon would have tocover two trauma centers/emergency rooms24/7/365), the limited number of board certi-fied/eligible neurosurgeons, residents in training with insufficient hours, or limited neu-rosurgical physician extenders, these issueshave strained our ability to adequately extendthe neurosurgical physician workforce andprovide care for all who require assessmentand management.
As a result, the delivery of high-quality care isbeing marginalized through the introduction ofless educated, less specialized providers. Withnon-neurosurgical physicians performing neuro-surgical procedures, physician extenders or res-idents as primary deliverers of care, newlytrained neurosurgeons lacking the volume andtime in training of their predecessors, and lessaccess due to funding cuts that force further reli-ability and coverage gaps, the practicing neuro-surgeon is attempting to keep up with the everincreasing demand for complex neurosurgicalcare and oversight with reduced resources at hisdisposal.
For community neurosurgeons, the inabilityto have adequate backup and to keep up withan elective caseload has forced many to beginto defer emergency coverage and cranial neuro-surgery. As well, with the imposition of multipleregulatory and oversight agencies and man-dates, we can expect that as more time is pulled
away from direct and urgent patient healthcarein the United States other specialties will try andfill the void and practice “neurosurgery.”Unfortunately, many of these regulatory imposi-tions arise from numerous diverse, uneducatedand unsophisticated groups which have notstudied the impact and result of these man-dates. Unlike physicians who see the impactfirsthand, these individuals implement “treat-ment plans” that have resulted in the decre-ment in physician reimbursement and theexpectation and forced unreimburseable timeand care of an already strained workforce.
These issues are not solely relegated to com-munity neurosurgeons; they have also changedthe expectations of university neurosurgeons intheir performance of academic neurosurgery.One prime example is in academic settings, thereduction in resident work hours has forcedmany to give up time and effort that was previ-ously “protected” for use in moving the field andpatient care forward. Activities that were expect-ed as part of the legacy of being an academicneurosurgeon, such as participating and gener-ating research in translational, basic, and clinicalsciences; teaching; and advancing our knowl-edge in the care of patients has been limited.
PRESIDENT’S MESSAGE
> AS PROFESSIONALSWE MUST CONTINUETO PROVIDE HIGH-QUALITY CARE WITHAN EYE TOWARDSCOST EFFICIENCYAND EFFICACY. <
P. David Adelson, MD, FACS, FAAPPresident, Congress ofNeurological Surgeons
The 2008 CNS Annual Meeting audience
experiences innovative educational science
during the 3-D Live Cadaveric Demonstration.
6 WWW.CNS.ORG

Glaringly, resident workforce reductionswere imposed without studying how the loss ofa professional, knowledgeable workforcewould impact patient care, communication andgaps in coverage. Yet these same individualsplan further reductions without study of thepotential negative consequences on health-care delivery by physicians, particularly neuro-surgeons. Similarly, financial pressures withregard to reimbursement, medical liability, etc.all have limited the funding for research anddevelopment in our university settings, andalso our ability to develop clinician scientistswho can truly bridge the bench-to-bedside con-cepts needed to improve the delivery of highquality, state-of-the-art patient care.
While it has become incumbent upon us toaccept these new regulatory impositions,
often without input or question, we also needto be proactive in developing potential solu-tions that will not negatively impact the deliv-ery of patient care. As professionals we mustcontinue to provide high-quality care with aneye towards cost efficiency and efficacy. Weneed to continue to educate the public, ourlegislators and the regulatory agencies aboutthe negative impact that poorly thought out,unfunded mandates and financial cuts canhave on care, access, and future scientific andpublic health developments. We need to showthat continued cuts in reimbursement, contin-ued high medical liability costs, restrictions inworkforce, and forced imposition of indicatorsthat are not reflective of quality and have littlevalue to true patient outcome are actuallydetrimental, interfering and taking further
time away from physician-patient interactionand relationships as well as from endeavorsthat move the field forward.
It is important that we continue to be proac-tive in developing better and proven solutions.Our strategies may include staying active in ournational professional societies and in our com-munities for education and advocacy; proposing,developing and implementing regionalized neu-rological emergency care centers; and develop-ing and assessing outcome measures that trulydefine neurosurgical quality. Neurosurgeons, astrue professionals and true advocates for theirpatients must maintain credibility by participat-ing at all levels of the process through legislativeaction, advocacy, research and development,and education. As a small but very vocal profes-sion, we can make a difference. <
WWW.CNS.ORG 7
> NEUROSURGEONS,AS TRUE PROFES-SIONALS AND TRUEADVOCATES FORTHEIR PATIENTSMUST MAINTAINCREDIBILITY BYPARTICIPATING ATALL LEVELS OF THEPROCESS THROUGHLEGISLATIVEACTION, ADVOCACY,RESEARCH ANDDEVELOPMENT, AND EDUCATION. <
8 WWW.CNS.ORG

WWW.CNS.ORG 9
This is dedicated to exploring theissues related to the delivery of care forthe neurosurgical patient of the future.
This particular topic has come under intensescrutiny subsequent to the creation of the feder-al government resident work hour restrictions. Ina previous era, the resident (one who resides inthe hospital, hence the name) was the soleprovider for in-hospital neurosurgical patientcare. However, the safety concerns raised byhaving fatigued physicians caring for patientswhile concurrently dedicating their efforts toeducation was fraught with difficulty. Allowingresidents time off in order to concentrate onpatient care and education has created a void.The reality is that surgical specialties are uniquein that the operating theater serves an essentialcomponent or “classroom” for resident educa-tion. Unfortunately with the limited resources ofresident training hours, the time in the operatingroom and dedicated to patient care hours hasdecreased.
Thus, necessity is the mother of all inven-tions and efforts to fill these needs are illustratedin the recent changes to the neurosurgical workforce. Numerous approaches have beenexplored to facilitate the delivery of superiorpatient care while simultaneously educating thenext generation of neurosurgeons. This has been formatted into three major sections toreview these strategies. The first section ana-
lyzes resident work hour restrictions as theyrelate to the delivery of education and discussespotential future workforce restrictions based onalready occurring global changes.• Daniel Barrow: Secretary, American Board of
Neurological Surgery (ABNS) discusses theresident work hour restriction on education.
• David G. Piepgras, Secretary of the Committeeon Accreditation of Subspecialty Training forThe Society of Neurological Surgeons, focus-es on the influence of fellows in the future resident education paradigm.
• Krystal Tomei provides the Neurosurgery Resident perspective.
• Alan Crockard analyzes how further workhour restrictions will impact residents andpatient care through his insight as EmeritusProfessor of Surgical Neurology.
In the second section, the was very fortu-nate to have a number of thought leaders intheir respective societies provide insight into theevolution of the neurosurgery patient care team.This section discusses the role of physician workextenders. Specifically articles were obtainedthrough the:• Association of Neurosurgical Physician
Assistants (ANSPA) – President Brenda Hill,PA-C and Ian Jones, PA-C.
• American Academy of Nurse Practitioners(AANP) – Jennifer Malone RN, CRNP.
• National Association of Registered NurseFirst Assistants (NARNFA) – Diane L. Ferrara,MSN, CRNP, RNFA and Rita Griffith, RN, MS,CRNFA.
• National Surgical Assistant Association (NSAA)– President Daniel D. Baird, CSA, MSc, MBA.
Lastly, there is a trend towards the developmentof sub-specialty focus to the delivery of patientcare, including the appearance of hospitalistservices and dedicated critical care teams. • AANS/CNS Section on Neurotrauma and
Critical Care Section has provided an arti-cle on Neurosurgeons and the IntensiveCare Unit composed by Alex B. Valadka,Michael Fehlings, Erol Veznedaroglu and P. David Adelson.
• The Society of Hospital Medicine has pre-sented the role of the primary care providerand its evolution. Pat Cawley and ScottFlanders provide their outlook as hospitalistsand care for the neurosurgery patient.
We have compiled this issue of the to pro-vide a balanced discussion, and have includedcontributions and insights from physicians, nurs-es and physician assistants. From evaluatingtheir viewpoints, and yours, we anticipate muchfuture discussion that further highlights theseimportant issues. <
James S. Harrop, MD,FACSTHE NEUROSURGERY
WORKFORCE OF THE FUTUREA COMMUNITY OF LEARNING

Does the 80-hour work restriction create a void inpatient care?The services provided by residents prior to theintroduction of the work hour restrictions werelegitimate and essential to patient care. Theneed for that care has not been reduced sincethe institution of the 80-hour work week in2003. In fact, the acuity of patient care inmany academic medical centers has risenover the past five years with increased region-alization for many of the most critically ill neu-rosurgical patients. The recent proposal by theInstitute of Medicine to further restrict workshifts to less than 16 hours may exacerbatethe problem.
Since patient service needs have not beenreduced, other healthcare providers havebeen utilized to fill the gaps. One of the worri-some voids in patient care has been lack ofcontinuity in resident physician care, resultingin a marked increase in handoffs from onephysician to another. Adherence to strict workhours can lead to medical errors attributableto more frequent patient handoffs, fragmenta-tion, and loss of continuity of care. One studydemonstrated that compliance with the 80-hour work week resulted in an average of 15handoffs per patient. Thus, residents are lessfamiliar with their patients’ medical issues.
Some experts have expressed concern thatthe greatest void in patient care is yet to comein the form of a new generation of physicianswith inadequate training. Work hour restrictionsmay create a generation of surgeons with great-ly reduced surgical experience and expertise.Learning episodes in neurosurgery training areoften greater than 16 hours. Unless the resi-
dency training programs are extended consider-ably, residents in neurosurgery may receive 25to 50% less training than residents receivedprior to 2003. One can reasonably ask whetherany patient would choose to be treated by aneurosurgeon who receives half the training oftoday's practitioners.
Although the imposition of work hourrestrictions on residents may have unintendedconsequences, it also provides an opportunityto re-evaluate our educational programs.Some of the work previously handled by resi-dents did not contribute to their educationand can be adequately performed by others.
What are residency programsdoing to fill this void? Concerns about resident fatigue must be bal-anced with the need to adequately train neu-rosurgical residents and ensure quality patientcare. The solutions to fill the patient care voidcreated by reduced resident work hours are asdiverse as the residency training programsthemselves. There is no “one size fits all” solu-tion to this challenge. The solutions dependon such factors as the number of residents inthe training program, the presence of fellows,the clinical volume of the program, the num-ber of affiliated hospitals in the training pro-gram and the resources of the institution.Potential solutions include use of residents ona night float system, addition of physicianextenders (including physician assistants andnurse practitioners) to the healthcare team,use of hospitalist service, development of neu-rocritical care services and elimination of cer-tain rotations including research opportuni-ties. Some programs have successfully met
these demands through increasing the num-ber of residents in the program.
In our own training program, we haveaddressed the problem through a multi-faceted approach that includes the develop-ment of a neurocritical care service integratedinto the Department of Neurosurgery, with par-ticipating neurologists trained in stroke neurol-ogy and critical care medicine. This providesan opportunity for increased educationalexperiences for the resident while providingcontinuous medical care for our most criticallyill patients. We have also been supported byour hospital in the recruitment of additionalnurse practitioners and physician assistantsas extenders. A night float rotation has beeninstituted to assure compliance with theACGME work hour restrictions. These changeshave been instituted to ensure that formaleducational opportunities and research rota-tions are protected.
What will be the impact on resident education? Residentmatch process? All agree that physician exhaustion is not goodfor residents or for patient care. An increasedemphasis on the importance of sleep is recog-nized and required of the medical profession. Inour attempts to solve one set of problems, how-ever, we may be creating others. Resident dutyhours do not stand alone. The hours a residentworks are part of a complex matrix of tightlyinterrelated issues that influence the value ofeducation including the quality of the GME pro-gram, supervision of residents’ activities, insti-tutional support and the quality of patient care.The current 80-hour restriction is relatively new
THE 80-HOUR WORK WEEK: RESTRICTIONS ON RESIDENT EDUCATION
Daniel L. Barrow, MDMBNA Bowman Professor and ChairmanDepartment of NeurosurgeryDirector, Emory Stroke CenterEmory University School of MedicineSecretary, American Board of Neurological Surgery
10 WWW.CNS.ORG

and has yet to be thoroughly examined forimpact on education, patient care and residentwell-being. Due to the relatively recent institu-tion of the shorter work week, there is little con-clusive data on the effects of the current resi-dency duty hour limits. The potential effect ofthe 16-hour limit recommended by the Instituteof Medicine is even more speculative, but alsopotentially more disquieting.
One study noted that since the 80-hourwork week went into effect, 75% of neurosur-gical residents and 98% of program directorsthought that patient care suffered from a lackof familiarity of residents with their patients.The decreased hours may also lead to anincreased length of time needed to receiveappropriate training, which in turn likely willhave implications for the US physician work-
force in years to come. A few case studieshave suggested that reduced work hours havenegatively impacted residency education.These studies, however, should be interpretedwith caution since many residencies with fouror five years of training have only had theirfirst cohort emerge. Thus doing a pre-periodanalysis is possible, but no post-period analy-sis is available yet. <
WWW.CNS.ORG 11
> ONE CAN REASONABLY ASK WHETHER ANYPATIENT WOULD CHOOSE TO BE TREATED BY ANEUROSURGEON WHO RECEIVES HALF THETRAINING OF TODAY'S PRACTITIONERS. <

12 WWW.CNS.ORG
The term “fellowship” as applied to med-ical education has generally referred toadditional or supplemental training in a
subspecialty or focused area beyond that ofthe residency; trainees engaged in this supple-mental education have commonly been called“fellows.” The Accreditation Council forGraduate Medical Education (ACGME) definesa fellowship (or “subspecialty program”) as a“structured educational experience followingcompletion of a prerequisite specialty programin graduate medical education designed toconform to the Program Requirements of aparticular subspecialty.” This ACGME defini-tion appropriately emphasizes requirementsfor educational structure with defined pro-gram requirements occurring post-residency.With few, if any, exceptions, ACGME accreditedfellowships are a minimum of one year induration.
In the past, and to some degree in the pres-ent as well, neurosurgical fellowships havebeen less well defined and structured andwith the exception of the jointly sponsored(Radiology, Neurosurgery and Neurology)Fellowship in Interventional Neuroradiology,none are ACGME accredited. Neurosurgery’slack of ACGME accredited fellowships is owedlargely to deliberate decisions made in 1994by our specialty’s leadership on educationalmatters, the American Board of NeurologicalSurgery (ABNS), the Residency ReviewCommittee (RRC) for Neurological Surgery,and The Society of Neurological Surgeons(SNS) with the support of the leadership of theAANS and CNS. In their joint deliberations,these organizations deemed it advisable toencourage subspecialty training opportunities
enfolded into the elective time of the neuro-surgical residency and to allow flexibility in theduration of these experiences (possibly lessthan 12 months ). Further, it was recognizedthat these areas of enhanced, focused sub-specialty education were not exclusive in con-tent but rather an expansion of the estab-lished neurosurgery residency curriculum. Assuch, neurosurgery’s concept of a subspecial-ty curriculum did not meet the ACGME’sexpectation of a new distinct body of knowl-edge for subspecialty accreditation. Therefore,in the U.S. and Canada as well, neurosurgery’srecognition, accreditation and certification ofsubspecialists have been more conservativethan that of other specialties.
While the movement towards neurosurgi-cal subspecialization of practice, especially inacademic medical centers, gained momen-tum in the 1970s and 80s (including the devel-opment of AANS and eventually the CNS JointSections) the ABNS opposed certification foradditional subspecialty training and expertise,initially in the area of critical care. In 1990,with growing pressure from those in the fieldof Pediatric Neurosurgery, the ABNS and RRCfor Neurological Surgery approved ACGMEaccreditation of subspecialty training in pedi-atric neurosurgery, but rescinded this decisionwithin two years owing to objections from abroad spectrum of neurosurgeons who includ-ed children in their general neurosurgery prac-tices. This reversal was paramount in the deci-sion of the leadership of pediatric neuro-surgery to move towards formalization of a cur-riculum for, and accreditation of, pediatricneurosurgery fellowships under the AmericanSociety of Pediatric Neurosurgery and eventu-
al certification of subspecialists by their ownAmerican Board of Pediatric NeurologicSurgery. This schism within neurosurgery wasregarded by many as an unhealthy splinteringof our small specialty with implications for dis-enfranchisement of non certificate holdersand more broadly for the established generalneurosurgery residency training. In response,the ABNS in 1994 reaffirmed its opposition toformal accreditation of subspecialty trainingor subcertification for neurosurgeons whodevote their practice to a subspecialty area.
In spite of this position, neurosurgery’seducational leadership and most practitionershave been well aware of the laudable forcesand motivation for subspecialization, primaryamong them being:• An enhanced environment for the develop-
ment of new technology, focused researchand academic pursuits.
• Improved clinical skills of the practitionerand outcomes for patients.
• Our specialty’s ability to meet competitionfrom other subspecialties such as orthope-dic spine, neuro-otology, and endovascularradiology.
• “Marketability” in clinical practice.
In acknowledging the merits of subspecializa-tion and the growing demand for subspecialtytraining in multiple areas of neurosurgery, theofficers of The Society of NeurologicalSurgeons in 1998 proposed a strategy forrecognition and accreditation of subspecialtytraining (fellowships) in neurosurgery outsidethe purview of the ACGME. At a NeurosurgerySummit Meeting in 1999 with representationfrom the leadership of the SNS, the ABNS, the
NEUROSURGERY SUBSPECIALIZATION,FELLOWSHIPS AND CAST
David G. Piepgras, MDProfessor of NeurosurgeryMayo Clinic College of MedicineRochester, Minnesota

RRC for Neurological Surgery, the AANS andthe CNS, this proposal was endorsed with thefollowing recommendations:• “Certification” for supplemental training
may be provided by the sponsoring fellow-ship program but there will be no subspe-cialty certification by the ABNS.
• The RRC will evaluate fellowships only inregard to their impact on resident training:training of fellows must not adverselyaffect the residents’ educational experi-ence.
• Flexibility in regard to timing and durationof additional subspecialty training is desir-able; enfolding subspecialty training intoresidency elective time should be pre-served and encouraged.
At its annual meeting in May 1999 The Societyof Neurological Surgeons (whose membershipis comprised of the majority of North Americanneurosurgical training directors) adopted a res-olution for accreditation of subspecialty train-ing and its programs aimed at promoting andassuring quality subspecialty education.
Structure, policies and procedures for pro-vision of oversight and accreditation of sub-specialty training in fellowships were subse-quently formalized and adopted under theSNS Committee on Accreditation ofSubspecialty Training (CAST). As this processhas matured and with input from the variousjoint sections and fellowship training directors,important principles pertaining to neurosurgi-cal subspecialty training have been adopted.These include:1. Completion of ACGME approved residency
training is sufficient to allow practice of neu-
rosurgery. Post-residency fellowship is notneeded for either competent practice of orreimbursement for delivery of neurosurgicalpatient care within the definition of neuro-surgery promulgated by the ABNS and theRRC for Neurological Surgery.
2. The development and management ofaccreditation of neurosurgical fellowships byThe Society of Neurological Surgeonsthrough the CAST structure is in the bestinterest of neurosurgery by helping to ensurethe quality of the educational experience.
3. “Fellowships” are a post-graduate subspe-cialty training experience. Fellowships areusually one year in duration, but in certaininstances may be shorter or longer asdetermined by the qualifications of thetrainee, the body of knowledge, and theskills to be learned.
4. “Enfolded subspecialty training” is done dur-ing the residency years. This type of trainingdoes not constitute a “fellowship,”but it mayin itself be of sufficient depth and breadth toprovide a higher level of subspecialty expert-ise than that achieved during the usual resi-dency training.
5. Training requirements for the aforementionedpostgraduate fellowship are established bythe subspecialty, preferably through its neuro-surgical joint section, and will specify durationand components of training, requirements forfacilities, faculty, affiliated services and mini-mum case material at the fellowship site.Fellowship requirements must include a cur-riculum for knowledge and procedural objec-tives to be attained in the fellowship.Requirements can stipulate minimum caserequirements for each fellow.
Specific information regarding CAST, exist-ing subspecialty educational curricula andaccreditation requirements can be found onthe SNS website at www.societyns.org.
As of December 2008, there are CASTaccredited fellowships in Neurologic Surgery ofthe Spine, Peripheral Nerve, CerebrovascularNeurosurgery, Pediatric Neurosurgery,Neurosurgical Oncology, Stereotactic andFunctional Neurosurgery, and EndovascularNeurosurgery, with programs in NeurosurgicalCritical Care soon to be added.
The primary goals and objectives of SNSaccreditation of subspecialty training, as origi-nally conceived, remain:• To assure quality in training programs
through established clinical and didacticas well as institutional and faculty require-ments.
• To maintain cohesiveness in neurosurgery.• To demonstrate neurosurgery’s pre-emi-
nence in defining its subspecialties andrequired training for competence in gener-al and focused practice.
• To promote the subspecialties within theneurosurgical domain. <
WWW.CNS.ORG 13

14 WWW.CNS.ORG
Neurological surgeons comprise aunique community. With a small com-plement of physicians, the fact that we
assume a great responsibility to our patientsis inevitable. I was aware of this when I decid-ed upon neurosurgery as a career, when Iinterviewed for residency, when I matched. Iremained cognizant of it during my neurologi-cal surgery residency. I knew I was entering afield where the demands on my time would besignificant, where lengthy cases are not a rari-ty and where emergencies are unpredictable.It is a field where complications carry thepotential to be immediately life threatening,and waiting for more convenient opportunitiesis not always an option. Like any field in medi-cine, our patients put their lives in our hands,and that is not a responsibility to be takenlightly. I know I am not unique in my stance.Many of my colleagues are aware of thesenuances to our profession, and generally weare not shy about sharing these with prospec-tive residency applicants. However, there hasbeen a transformation in medical educationthat has impacted resident training, and thisinfluence is anything but subtle.
In 2003, the Accreditation Council forGraduate Medical Education (ACGME) estab-lished regulations entitled “Resident DutyHours in the Learning and WorkingEnvironment.” These new regulations were theresult of an effort to improve patient safetyrelated to resident fatigue. Such stipulationsas an 80-hour workweek, maximum 30-hourshifts, and 10 hours off between shifts wereintended to improve patient safety and alsoimprove resident safety and well-being. Thecurrent medical literature has produced con-
flicting studies on the outcome of the ACMGEregulations in regards to patient safety as wellas medical education.
In general, the ACGME regulations havehad a positive impact on resident training,allowing for more time for independent read-ing, personal endeavors and family obliga-tions. Moreover, few would argue that therehave been many measures taken by residenttraining programs to accommodate these reg-ulations. Now in their sixth year since imple-mentation, the shortcomings of these dutyhour regulations and their broad approach toresident training are becoming more appar-ent. The requirements for training of the vari-ous subspecialties within medicine are vastlydifferent, yet a single set of recommendationswas made to apply to all residents regardlessof specialty. From the beginning, certain spe-cialties had to make significantly morechanges in their training programs to accom-modate these regulations. In theory, thedemands of resident training programs shouldbe reflective of the demands of the post-resi-dency practice for those specialties. Yet withincertain fields we have created a significantdiscord between training and practice.
Last November, the Institute of Medicine(IOM) released their report on resident dutyhours, “Resident Duty Hours: EnhancingSleep, Supervision and Safety” with increas-ingly stringent regulations on resident workhours. Their recommendations include sup-porting 16-hour shifts (or 30-hour shifts with aguarantee for five hours of uninterruptedsleep during that shift), increasing time offbetween shifts depending on the time orlength of shift, removing the ability to average
THE 80-HOUR WORK WEEK FROM A RESIDENT’S PERSPECTIVE
Krystal Tomei, MDPGY-3 Neurosurgery ResidentUMDNJ – New Jersey Medical School
> NOW IN THEIRSIXTH YEAR SINCEIMPLEMENTATION,THE SHORTCOMINGSOF THESE DUTYHOUR REGULATIONSAND THEIR BROADAPPROACH TO RESIDENT TRAININGARE BECOMINGMORE APPARENT. <

WWW.CNS.ORG 15
days off and on-call days over four weeks,increasing total days off per month to five, andimplementing tighter regulations on moon-lighting. Through my involvement in organizedmedicine, I have had the opportunity to partic-ipate in several discussions that involved resi-dents from varying medical specialties regard-ing these proposed regulations. The IOMreport has already raised contention amongresidents. Not surprisingly, surgical and non-surgical residents hold different opinions onthe IOM recommendations and resident dutyhours in general. Residents have raised con-cerns about how these regulations take awayfrom continuity of patient care. We have con-cerns about whether we will have to sacrificeeducational opportunities that extend our dutyhours beyond regulation. And most important-ly, we are concerned about external regulatorybodies dictating our training.
As neurosurgical residents, we must advo-cate for patient safety as well as our own edu-cation, understanding the delicate balancebetween the two. Our duty as resident physi-cians is to facilitate the care of patients in col-laboration with our attendings. Our duty asstudents in our field is to acquire that knowl-edge and experience that allows us to under-stand the fundamentals of peri-operative neu-rosurgical patient care and to acquire the sur-gical techniques to treat neurosurgical disor-ders. Achieving both of these duties within thecurrent confines of resident work hours provesdifficult at times. Patient courses are unpre-dictable, complications occur, surgeries takelonger than expected, emergencies areinevitable. Patient care needs can rarely bemet within the allowed 80 hours per week. Ourattending assumes responsibility when a caseruns late, an emergency goes to the OR in themiddle of the night, and when they have elec-tive cases scheduled for the following day. Willtoday’s generation of residents be able to dothe same? Unfortunately, we do not have thatdata yet. Our residency extends beyond thetime that duty hour regulations have been ineffect, and this new generation of physicians
has yet to graduate into practice.As residents, we are required to work with-
in the confines of these regulations. As advo-cates for our own education, we must do whatwe can to make up for the discord betweenthese severe and ubiquitous regulations andthe reality that is a neurosurgical residency. Iknow many of my colleagues, myself included,who have contacted the person on call to seehow our patient was doing, who have followedup on a CT from home, and who have spentcountless hours at home preparing for cases,reading about neurosurgical pathology, anddoing whatever we can to supplement our owneducation. Such is the duty that we assumedwhen we accepted the responsibility ofbecoming a neurological surgeon.
Medical education has entered a new era.Though we must remain cognizant of issuesrelated to patient safety, equal weight shouldbe placed upon resident education and pre-paredness. Ancillary staff and physician exten-ders represent a means to increase patientsafety and care while allowing residents tofocus their time on education. However,increased ancillary staff cannot augment resi-dent educational experiences. The discordbetween residents’ work hours and those ofpracticing physicians demands that our spe-cialty work with all interested parties to amendthese inconsistencies. Is the best solution anexemption for chief residents, such that theirwork schedules can mimic that of a typicalfirst year in practice while they still haveattending supervision? Or perhaps a gradedwork hour increase based upon the postgrad-uate year is possible, to allow for increasinghours and responsibility based on seniority. I look forward to hearing a strong neurosurgi-cal voice as we continue to determine howbest to balance all interests and not compro-mise patient safety or resident education. <
> MEDICAL EDUCATIONHAS ENTERED A NEW ERA. THOUGHWE MUST REMAINCOGNIZANT OFISSUES RELATED TO PATIENT SAFETY,EQUAL WEIGHTSHOULD BE PLACEDUPON RESIDENTEDUCATION ANDPREPAREDNESS. <

16 WWW.CNS.ORG
> THE SHORTENED WORKWEEK … REQUIRES A MAJOR RESTRUCTURING OF THE NEUROSURGICAL TEAM TOENSURE CLINICAL SERVICEAND PATIENT SAFETY. <

WWW.CNS.ORG 17
The short answer is yes, but with difficul-ty. At the moment, the shortened workweek is in place in the UK by law, and
something like it has been practiced inScandinavia for more than a decade. However,it requires a major restructuring of the neuro-surgical team to ensure clinical service andpatient safety. A fundamental question iswhether, in a 56-hour work week, the trainingprograms can produce replicas of the previousgenerations of neurosurgeons (and further-more, is this really what the neurosurgicalestablishment wants?) Will it require longerthan six years to adequately train our resi-dents? And even more fundamentally, is theexisting system the best way to provide thepublic with the clinical neurosurgical care itrequires in a rapidly changing world? Can thesame surgeon, for example, deliver up-to-datecare for movement disorders and complexspinal problems?
Historically, the line between healthcaredelivery and training has been blurred.Learning “on the job” has produced highlyexperienced clinicians, but it is unclear justhow much of the working day has been actualtraining and how much a cheap and conven-ient way of delivering patient care. With theimplementation of shorter working hours intheir respective professions, airline pilots andnurses have had to confront this dilemma; inboth cases, the explicit allocation of serviceand training hours has allowed these profes-sionals to achieve both goals. But a significantincrease in the workforce is required, and notall end up as senior captains or directors ofnursing. Indirectly the neurosurgery workforcehas been moving in this direction with increas-
ing use of physician extenders. However, theexplicit roles have not yet been widely accept-ed, hampering the redefinition of the neuro-surgical curriculum.
As with school and university programs, sowith postgraduate curricula: new topics areeasily added without a re-evaluation of originaltopics, and the course expands to unmanage-able levels. Something similar occurs withworking practices; decisions must be made asto how many patient rounds occur each day,and when and by whom management deci-sions are made on the rounds. When thesame pyramidal team provides 24/7 carethere are clear lines of referral and responsi-bility. With shift systems and compulsory restperiods, new ways of working to ensure conti-nuity of patient care are essential and must bedocumented.
There are massive changes in society (ofwhich patients and physicians are a part) withcounter currents and contradictions. Patientswant treatment by fully-trained physicians.Medical school graduates (now 70% female inthe UK) want the very best training, but alsoseek a life outside medicine.
The European Working Time Directive(EWTD) is a “Health and Safety” law passed bythe European Union Parliament for the protec-tion of all workers; however, it does not applyto self employed individuals. It is strictlyobserved in (mainly) Western Europe, but upto half of the countries have yet to fully complywith the 56-hour rule, particularly in the med-ical field and in Eastern and Mediterraneancountries. In some countries there are “novel”two hospital contracts for juniors, which com-bined would exceed EWTD limits. Currently,
CAN THE NEUROSURGERYWORKFORCE HANDLE A 56-HOUR WEEK?
Alan Crockard, DSc, FRCS, FRCS (Ed), FDS, RCS (Eng) Emeritus Professor of Surgical NeurologyVictor Horsley Department of NeurosurgeryThe National Hospital for Neurology and Neurosurgery
> EVEN MORE FUNDAMENTALLY, IS THE EXISTINGSYSTEM THE BESTWAY TO PROVIDETHE PUBLIC WITHTHE CLINICAL NEUROSURGICALCARE IT REQUIRES? <

18 WWW.CNS.ORG
the proposal to reduce the working week to 48hours by August 2009 is being hotly debatedthroughout the European Union. The timerestrictions currently only apply to trainees,but soon it is proposed that consultants willalso be similarly limited. If enforced, it willhave profound effect on medical working prac-tices and income.
So how does this rota system work? First,the 56-hour week is averaged over one tothree months and time off given in lieu of longshifts. For instance, a 24-hour “on call” shiftmust have a five-hour rest period, avoidanceof all non-urgent operating, and relief of dutiesby 11:00 am the following morning for a mini-mum 20 hours off duty. There might be TWO24-hour “on call” episodes in a month. For therest of the time, 14-hour shifts allow continu-ity and adequate handover built in from theday to night shifts. There is one completeweek off in 13 weeks (this is not vacationtime, but may be added to vacation or studyleave). Thus in a six month period the individ-ual junior might be legitimately “off service” (2+ 2 = 4 weeks and agreed study leave for sayfour days). This is a huge commitment of staff,requiring a minimum of ELEVEN staff to covera 30-bed unit.
What are the “knock on” implications of these rotas?1. Shorter exposure times of individual
trainees to the individual consultant sur-geon’s practices.
2. Fewer opportunities to participate in opera-tive surgery. Thus the “quotas” of indexedoperative procedures to be presented atthe completion of training are less.
3. Small neurosurgical units may not be ableto operate the junior “on call” rotas andmust either amalgamate with neighbouringunits or close.
4. Currently, (to ensure continuity of care) con-sultant neurosurgeons are exempt fromthe 56-hour week. But they too will have tobe compliant by 2013.
5. Subspeciality training (i.e., neurovascular,spinal, epilepsy) may have to be acquiredby “Fellowship“ training, in effect lengthen-ing the residency program for all but themore “general” neurosurgery, whateverthat might be.
And the quality of training? According to theChairman of the UK Specialty TrainingCommittee, Michael Powell, it is still too early toassess the “knock on” effect of EWTD. Thosecurrently coming up for completion of traininghave had some experience under the old 80-hour system. The reduction in recorded “LogBook” cases reveals less hands-on experience,and with the specialty final exams there is aworryingly low pass rate on the first attempt. Allof this might indirectly increase the trainingtime, if the desired end result is to produce aneurosurgeon similar (in experience and knowl-edge) to those graduating 10 years ago.
Some medical specialities are less adverse-ly affected than neurosurgery. Surgical special-ities such as urology and cardiac surgery aredoing considerably less open procedures, thustraining in them might change considerably.
The current government’s aim is to expandprimary healthcare. With a differential increasein remuneration to levels at or above the top ofthe hospital consultant pay scale coupled with
a shorter training period for this speciality, it islikely that there will be a progressive shift fromhospital based medicine to physicians in fami-ly practice.
What happens if the European Parliamentsucceeds in reducing the work week to 48 hoursfor one and all? May the Lord help the sick. <
> WHAT HAPPENS IF THE EUROPEAN PARLIAMENTSUCCEEDS IN REDUCING THE WORK WEEK TO 48HOURS FOR ONE AND ALL? <

WWW.CNS.ORG 19
Physician Assistants (PAs) enhance qual-ity patient care by fostering a team envi-ronment that supports neurosurgical
patients with their unique problems andcomorbidities. Within the physician-PA rela-tionship, Physician Assistants exercise auton-omy in medical decision-making and provide abroad range of diagnostic and therapeuticservices. They are healthcare professionalslicensed to practice medicine with physiciansupervision.
Physician Assistants manage many detailsof patients’ pre- and post-surgical care, ensur-ing personalized clinical attention, continuity ofcare and shortened hospital stays. This allowssurgeons more time to concentrate on surgery,research and managing difficult cases.
On a typical day, the PA rounds on inpa-tients, including coordinating discharges fromthe hospital. During clinic he or she conductsinitial consultations with new patients, takingdetailed medical histories and presenting hisor her findings to the Surgeon. The team con-fers and delineates treatment plans. The PAeducates patients both pre- and post-opera-tively. Many times the Neurosurgeon does nothave a lot of time pre-operatively to spend withpatients, and the PA helps, by taking a littlemore time to talk to families, making sure theyare calm before surgery. The PA sees patientsfor their first visit after surgery includingsuture removal in the office, and also takecalls as needed from patients.
Pain management is another area wherePAs provides a very necessary service to
patients. They make adjustments as neededfor patients and provide medication, which areboth important time-savers for the supervisingphysician.
The PA’s key role as a first assistant reflectsthe neurosurgeon’s trust in him or her, basedon years of shared surgical experience. ThePA’s highly developed technical abilities andknowledge of anatomy make them effectivefirst assistants in the operating room. In somecases the PA identifies the surgical site andmakes the initial incision as the Neurosurgeonreviews the studies in the room. During the pro-cedure the PA helps by being a closely attunedright hand to the surgeon, handling a widerange of surgical tasks. The PA closes most ofthe surgical wounds from deep to superficial,helps with post-operative orders and checks onpatients after their arrival in the recovery room.The American College of Surgeons recognizesPhysician Assistants as qualified FirstAssistants.
PHYSICIANASSISTANTSCONTRIBUTE TO QUALITY OF LIFE FORNEUROSURGEONSAND PATIENTS
> THE PHYSICIANASSISTANT IS A TRUEEXTENSION OF THESURGEON BECAUSE OFHIS OR HER MEDICALMODEL EDUCATION, ASWELL AS PHILOSOPHYAND COMMITMENT TOPHYSICIAN-DIRECTED,PATIENT-CENTEREDCARE. <
PHYSICIAN ASSISTANTS (PAs)
Physician Assistants are health care professionals licensed, or in the case of those employed by the federal government they are credentialed, to prac-tice medicine with physician supervision. As part of their comprehensive responsibilities, PAs conduct physical exams, diagnose and treat illnesses,order and interpret tests, counsel on preventive health care, assist in surgery, and write prescriptions.
Brenda D. Hill, PA-CPresident, Association ofNeurosurgical PhysicianAssistantsHonolulu, HI
Ian Jones, PA-CWinnipeg, Manitoba,Canada

20 WWW.CNS.ORG
In some practices the PA takes first call,and is the first responder to the ER and seesall consults in the hospital. The Neurosurgeonsees all admissions and consults within 24hours and is able to see such patients with allthe information required to make a surgicaldecision.
The Physician Assistant is a true extensionof the surgeon because of his or her medicalmodel education, as well as philosophy andcommitment to physician-directed, patient-centered care. PAs maintain their competencyby national certification and mandatory con-tinuing medical education. Their generalist medical education provides a solid foundation from which to address the diverseaspects of neurosurgical practice, includingperforming physical exams, diagnosing condi-tions and developing treatment plans, pre-scribing medication and assisting in surgery.
Physician Assistants are hired through hos-pitals, private practices, managed care organ-izations and universities where they areemployed in research and teaching and aretypically credentialed under the medical staffbylaws. Currently all 50 states cover medicalservices provided by PAs under Medicare andMedicaid. Reimbursement is paid to the PA’semployer. Private insurers generally covermedical services provided by PAs when theyare included as part of the physician’s bill oras part of a global fee for surgery.
Twenty-five percent of approximately70,000 clinical practicing PAs work in surgicalspecialties or sub-specialties. Approximately2.4% are Neurosurgical Physician Assistants.
There has been an increase in the utiliza-tion of Neurosurgical PAs since the mandate
that changed resident hours. One of the mostvaluable aspects of using PAs is the continuitythey provide the patient on a service wheremedical students rotate every six weeks andresidents change yearly. One concern raisedby the limits on resident duty hours is thepotential for increased numbers of hand-offsof patients between residents. One studyshowed that the restricted working hours forresidents were associated with delayed order-ing of tests and increased rates of in-hospitalcomplications. A PA can help to mitigate theseerrors of miscommunication and the delays
that tend to occur with frequent patient hand-offs. If you have a PA, it’s like having a goodresident who never leaves.
The team relationship is exemplary; mutualrespect fosters a collegial and effective workenvironment that promotes the sharing ofideas regarding patient care and professionalissues.
The abilities of a PA are further developedand enhanced by the nature of the profession-al physician-PA relationship that is the founda-tion of the philosophy behind these truePhysician Extenders. <

WWW.CNS.ORG 21
In the early 1960s, due to limited health-care resources for under-served popula-tions and a nationwide physician shortage,
the role of NPs evolved. Over time and with afederal initiative to increase greater access toproviders of primary care, NP programs flour-ished. With the inception of healthcare reformin the 1990s, there were an increased num-ber and acuity of patients, demands to short-en lengths of hospital stays, limited residentphysician access due to an 80-hour workweek initiative, and increasing demands onattending physicians; these factors furtherexpanded the role of the NP.
The first program to successfully prepareNPs for practice was developed by the teamof Loretta Ford, a nurse, and Henry Silver, aphysician, at the University of Colorado in1965 (American Academy of NursePractitioners, 2008). Neurosurgical NPs prac-ticed in collaboration with the attending neu-
rosurgeon(s) and other members of the teamin both the clinic and inpatient settings to pro-vide comprehensive patient care.
Nurse Practitioners’ healthcare roles con-sist of obtaining health histories, performingcomplete physical examinations, enteringorders, performing and interpreting diagnos-tic studies, providing diagnosis and treatmentof acute and chronic medical conditions, pre-scribing medications, providing health teach-ing and counseling, and referring patients toother health care providers.
How are Nurse PractitionersEducated and Credentialed?Currently, to practice at entry level requires aMaster’s degree. Nurse Practitioners mustfirst earn a Bachelor's degree in nursing andthen a graduate degree in an NP program,although some NPs also complete a doctoraldegree. NPs then define an area of education-
al focus, such as neonatal, pediatric, family,adult, gerontologic, oncology, women'shealth, mental health and acute care.Presently, half of NPs practice in the primarycare setting while the remainder are in sub-specialty areas such as neurosurgery, emer-gency, cardiovascular, orthopaedics, etc.Typically a NP practicing in a neurosurgerypractice, which treats adolescents and adultpatients, has earned an Acute Care or AdultNurse Practitioner degree. In addition to earn-ing a Master's degree, NPs are encouraged tobecome board certified by taking a standard-ized national examination for their chosenspecialty. However, board certification is notrequired by all state licensing boards.
Credentialing is the administrativeprocess by which an individual or institutionexamines the information about a practition-er's record of education, clinical training,licensure, DEA and board certifications, liabil-
THE NURSEPRACTITIONERAND THENEUROSURGICALHEALTHCARETEAM
Jennifer Malone, MSN,CRNP
NURSE PRACTITIONERS (NPs)
Nurse Practitioners (NPs) are advanced practice nurses who provide comprehensive preventive and acute health care services to individuals across the life-span. Nurse Practitioners are experienced registered nurses (RNs) who have earned additional education and clinical skills to practice in an advanced capac-ity. Thus, NPs are also referred to as Advance Practice Nurses or APNs.
> PRESENTLY, HALF OF NPs PRACTICE IN THE PRIMARY CARE SETTING WHILE THEREMAINDER ARE IN SUB-SPECIALTY AREASSUCH AS NEUROSURGERY, EMERGENCY, CARDIOVASCULAR, ORTHOPAEDICS, ETC. <

ity insurance, continuing education, andexperience or actions. Nurse Practitionerssubmit their application for credentials, whichis then reviewed by the institution to ensurethat the applicant is consistently meeting fed-eral and state standards of practice in theirprofession.
How Many NPs are in NorthAmerica Now? How Many Willthere be in Five Years?The 2005 "National Sample Survey ofRegistered Nurses" reported by the HealthResources Services Administration showed141,209 NPs in the United States, and in2006 there were estimated to be 145,000(American College of Nurse Practitioners,2008). A 2006 report from the CanadianInstitute for Health Information estimated1,582 licensed NPs across Canada withapproximately 929 employed in an active NProle (Canadian Nurses Association, 2008,and Issa, 2008). There are 325 colleges anduniversities in the United States who prepareapproximately 6,000 new NPs annually(American Academy of Nurse Practitioners,2008). Applying that data, there will be closeto 175,000 new NPs in the United States fiveyears from now.
Do Roles Vary Depending onAcademic or Private Practice? Neurosurgical NPs have a similar scope ofpractice in both academic and private set-tings. There are, however, variations of rolesbetween the clinic and inpatient settings withthe obvious differences of managing outpa-tient concerns such as new and follow-up eval-
uations, compared to the acute care needs ofthe hospitalized patient. Additionally, the neu-rosurgical NP role can vary by state as eachoutlines the scope of practice for NPs in theirrespective Nurse Practice Acts.
Nurse Practitioners with a specific clinicalfocus, such as neurosurgery, may enhance thescope of their practice to meet the needs ofthe neurosurgical patient by completing addi-tional training to perform advanced clinicalprocedures such as management of ventricu-lostomy and lumbar drains, drain removal,insertion of central lines, arterial lines, shuntreprogramming, spinal cord stimulator andintrathecal pump programming, and applica-tion and removal of halo orthoses (Herrmannand Zambrowski, 2005 and Yeager, Dale-Shaw, Casavant, and Burns, 2006).Depending upon the individual state NursePractice Acts (Cary and Smolenski, 2008, andSherwood, Brown, Fay, and Wardell, 1997),NPs can perform these procedures with addi-tional training and proper credentialing.
What is the Impact on PhysicianEducation?Legislative restrictions on the amount ofpatient care hours that residents are able toprovide have created a demand for more NPsin the acute care setting. Inpatient care wasonce solely the responsibility of the housestaff physicians, but with the 80-hour workweek, resident education for the practice ofsurgery has limited this role. Thus in order tocontinue a high level of patient care, NPs pro-vide coverage when residents are attendingrequired educational meetings or in the oper-ating theater.
In their 2007 study examining the impactof nurse practitioners on physician education,Bahouth et al. reported resident physiciansnoted a positive experience when rotating onservices with NPs versus those without NPs.The surgical residents reported an "increasedability to concentrate during formal educationand operating room time since the NP pro-vides continuity in care during the residenttime away from the unit."
In summary, NPs are increasingly indemand and are being utilized in variousroles due in part to the increased number andacuity of patients needing primary, tertiaryand specialty care; the requirements createdby the health care reforms of the 1990s; andthe passage of the resident 80-hour workweek law. The NP role will continue to evolveand include even more patient care responsi-bilities in addition to the direct and indirectenhancement of resident physician training,with the overall team goal of improved patienthealth care.
ReferencesAmerican Academy of Nurse Practitioners (2008).About NPs. Retrieved 12/20/08. Available at:http://www.aanp.org/AANPCMS2/AboutAANP/About+NPs.htm.
<
22 WWW.CNS.ORG
> NURSE PRACTITIONERS WITH A SPECIFIC CLINICAL FOCUS, SUCH AS NEUROSURGERY, MAY ENHANCE THE SCOPE OF THEIR PRACTICE TO MEET THE NEEDS OF THE NEUROSURGICAL PATIENT. <

WWW.CNS.ORG 23
The reduction in resident work hoursnecessitates a restructuring of the neu-rosurgical team to ensure the continuity
of quality care and patient safety. RegisteredNurse First Assistants (RFNAs) are qualifiedsurgical assistants who have helped fill thevoid in the surgical field. The American Collegeof Surgeons acknowledges the benefit ofRNFAs by stating that when co-surgeons orresidents are unavailable to serve as assis-tants-at-surgery, a non-physician health pro-fessional should be allowed to perform therole if the practice privileges of such an indi-vidual are based upon verified credentials,reviewed and approved by the hospital creden-tialing committee, and within the defined lim-its of state law.
The Association of periOperative RegisteredNurses (AORN) adopted the first official state-ment on RNFAs in 1984, and defined the roleas a perioperative registered nurse who worksin collaboration with the surgeon and health-care team members to achieve optimal patientoutcomes. The RNFA must have acquired thenecessary knowledge, judgment and skills spe-cific to the expanded role of RNFA clinical prac-tice. Intraoperatively, the RNFA practices at thedirection of the surgeon and does not concur-rently function as a scrub nurse.
Registered Nurse First Assistants areRegistered Nurses. Most have CNOR (CertifiedNurse Operating Room) certification, whichrequires two years and 2,400 hours of operat-ing room nursing experience to qualify to sitfor the certification exam. Alternatively, theymay be master-prepared, board-certifiedAdvanced Practice Nurses (APNs). (The term“Advanced Practice Nurse” is used to describeNurse Practitioners, Certified RegisteredNurse Anesthetists, Clinical Nurse Specialistsand Certified Nurse Midwives). An approvedpost graduate RNFA education program,which includes one year with didactic and clin-ical components, must be completed. An APNor Bachelor’s degree-prepared RNFA may takethe CRNFA certification exam through theCompetency and Credentialing Institute (CCI)after obtaining 2,000 hours of experience.Although encouraged, this is not required.
The reduction in resident work hoursrequires resourceful time management andefficient use of the neurosurgical team. As effi-ciency becomes the focus in healthcare, thevalue of the RNFA becomes increasingly evi-dent. Registered Nurse First Assistants canfocus and apply their nursing expertise, surgi-cal training and knowledge of the surgicalpatient to facilitate improved patient care. This
REGISTERED NURSE FIRST ASSISTANTS AND THENEUROSURGICAL TEAM
Diane L. Ferrara, MSN,CRNP, RNFA
Rita Griffith, RN, MS,CRNFA
> THE REDUCTION INRESIDENT WORKHOURS REQUIRESRESOURCEFUL TIMEMANAGEMENT ANDEFFICIENT USE OFTHE NEUROSURGICALTEAM. AS EFFICIENCYBECOMES THEFOCUS IN HEALTH-CARE, THE VALUE OFTHE RNFA BECOMESINCREASINGLY EVIDENT. <
REGISTERED NURSE FIRST ASSISTANTS (RNFAs)
Registered Nurse First Assistants (RNFAs) are experienced operating room registered nurses who have completed an additional specialty educationprogram providing them the necessary skills to first assist with surgery under the direction of a surgeon. Registered Nurse First Assistants promotecollaboration, provide stability and facilitate the surgical process to ensure that surgical patients receive consistent and superior care.

24 WWW.CNS.ORG
comprehensive understanding enables RNFAsto reduce operating time and costs, and alsomaximize surgeon efficiency. Registered NurseFirst Assistants work toward providing optimalcare and improving patient outcomes cost-effectively while supporting the surgical team.Their collaboration extends to the surgeon,anesthesia team, additional nursing person-nel, the patient and his or her family, fromadmission through discharge. This holisticcompassionate care is the trademark of nurs-es and the RNFA is in a prime position to offerall of these services to the neurosurgical team.
Registered Nurse First Assistants provideconsistency and guidance in the fluctuatingoperative environment. They are the bridgebetween surgeons and nurses by learning theroutines and preferences of the individual sur-geons, communicating them to the surgicalteam, and enacting them. Registered NurseFirst Assistants are the stable element in theOR as the residents, nurses and anesthesiapersonnel rotate through. Through their expe-rience, they serve as valuable educationalresources for medical students, residents,nurses and surgeons.
Examples of RNFA interaction with the neuro-surgical team include:• Evaluating and assessing patients in the
preoperative holding area.• Verifying that preoperative documentation
is complete and accurate. • Marking the surgical site.• Transferring the patient to the OR.• Supporting anesthesia personnel and
nurses in preparing the patient for surgery.• Positioning and applying position devices
as needed.• Prepping and draping the surgical site.• Participating in the time out.• Exposing the surgical site and assisting
with the surgical procedure by handlingand cutting tissue, using instruments and
medical devices, providing exposure andhemostasis, suturing, closing the incisionand applying dressings.
• Assessing the patient’s motor and neurostatus after he or she awakens in the OR.
• Writing postoperative orders and notesaccording to established protocols.
• Transferring the patient to the post-anesthesia unit.
• Participating in postoperative rounds.• Assisting with discharge planning and
identifying appropriate communityresources as needed.
Registered Nurse First Assistants behaviorsmay vary depending on patient populations,practice environments, services provided,accessibility of human and fiscal resources,institutional policy and state nurse practiceacts.
Registered Nurse First Assistants can directlysupport resident education by:• Evaluating patients in the holding area in
the morning, allowing the residents moretime to do morning rounds.
• Supporting in facilitating the surgicalprocess.
• Assisting with closure of large incisions.• Facilitating the turnover of cases in the
OR, allowing residents to attend to otherpatients during that time.
• Freeing up residents in the evening byclosing, waking, and transferring thepatients, enabling residents to startevening rounds earlier.
• Covering while residents are at education-al meetings and conferences.
• Allowing residents to efficiently use theirtime and potentially decrease their workhours.Financial reimbursement for RNFAs is
dependent on a multitude of factors includingexperience and region of the country. In gener-
al, it is reported that RNFAs are compensated10-15% more than perioperative nurses, withmean incomes from $60,000-$70,000.
In 2007, the National Association of RNFirst Assistants (NARNFA) completed adescriptive and demographic survey of 2,500RNFAs. The survey results showed that 53% ofRNFAs are hospital employed and that thehospitals had at least four RNFAs on staff. Theremaining RNFAs were self employed (25%) orphysician employed (32%). Several stateshave legislation that enable the RNFA to be anindependent contractor, be self-employed, orwork in a group of surgical assistants. Thisallows the RNFA to bill the insurance carrier asa separate healthcare provider, the same asan assistant surgeon would. Whether in anacademic setting, physician-based practice, or as an independent contractor, the RNFA is capable of providing detailed care and continuity that is rewarding for the patient, the surgeon and nurse.
References1 www.NARNFA.com, National Association of
RN First Assistants
<
WWW.CNS.ORG 25
There are several organizations that certi-fy and license surgical assistants. Eachorganization agrees that surgical assist-
ing is a specialty allied health profession thatrequires specific training and education overand above a degree in science, nursing, physi-cian assisting or other healthcare professions.Minimum educational requirements are uni-versity level microbiology, patho-physiology,pharmacology, anatomy and physiology, and
medical terminology, in addition to the specif-ic allied health education each professionrequires. All recognized certifying bodiesrequire surgical assistants to submit to aboard examination that is focused on surgicalassisting knowledge and skills. The CertifiedSurgical Assistant (C.S.A.) is required to sit fora national board exam administered by theNational Surgical Assistant Association, and isqualified to sit for this exam only after com-
WHAT SURGICALASSISTANTS DO TO HELPNEUROSURGEONSAS WORKFORCEEXTENDERS
Daniel D. Baird, CSA,MSc, MBAPresidentNational SurgicalAssistant Association
SURGICAL ASSISTANTS
As defined by the American College of Surgeons, the non-physician surgical assistant, often referred to as a “first assistant,” is an experienced alliedhealth professional who assists the surgeon by aiding exposure, providing hemostasis, closing wounds and performing other intra-operative functionsthat help ensure a safe operation with optimal results for the patient. Under the direction and supervision of the surgeon, the surgical assistant alsoperforms pre-operative and post-operative duties, which facilitate proper patient care.


WWW.CNS.ORG 27
pleting a recognized and accredited surgicalassisting program or by holding a certificationin another surgery-related allied health profes-sion for three years. These surgical assistantcandidates are then only eligible to sit for theCSA exam after completing 2,250 hours ofsurgical first-assisting. These eligibility require-ments are verified by a rigorous process ofevaluating education, recommendations fromsurgeons and then by validating case logs.
There are several pathways of eligibility forentrance into the surgical assisting profes-sion, such as military medical programs, nurs-ing and physician assistant programs, as wellas surgical technology programs emphasizingsurgical assisting. The most commonly accept-ed method is graduation from a surgicalassisting education program which is accredit-ed by the Commission on Accreditation ofAllied Health Education Programs (CAAHEP),the only accrediting body approved by periop-erative physician organizations such as theAmerican College of Surgeons, AmericanAcademy of Anesthesiologists, AmericanMedical Association and the AmericanAcademy of Physicians.
Surgical assisting is a thriving and rapidlygrowing profession, with an estimated 5,000practitioners in the United States, a numberthat could easily double in the next few years.The trend of augmenting surgical teams withsurgical assistants will continue to be intensi-fied by the critical shortage of physicians,especially in surgical disciplines such as neu-rosurgery. The number of neurosurgical-specif-ic surgical assistants is not known.
Surgical assistants are commonly found inprivate practices, outpatient clinics, private
hospitals and teaching hospitals. Surgicalassistants are often looked upon to help trainsurgical residents on such important skills asretraction and suturing, and are found teach-ing in medical education programs around thecountry.
Surgical assistants are employed and com-pensated in many different ways. It is notuncommon to find surgical assistants in hospi-tal surgery departments where they are paidby the hospital; in private practices where theyare paid by the surgical group practice; and inpartnerships of independent contractorswhere they are both contracted and paid bythe hospital or the surgeon. It is also commonpractice for surgical assistants to bill apatient’s insurance, either independently or incoordination with a surgeon, for their services.
Surgical assistants are integral membersof the surgical team, often aiding the hospitalstaff with an in-depth understanding of proce-dures, the specifics of each patient, and con-summate knowledge of a surgeon’s prefer-ences and techniques. This unique ability tohelp the surgeon perform more effectively andto help the surgical staff operate more effi-ciently is believed to be critical to the optimaloutcome for surgical patients.
Regardless of where surgical assistantswork or how they are employed, their roleremains the same: to work intraoperativelyunder the direction and supervision of the sur-geon to ensure optimal outcomes for the sur-gical patient. <
> SURGICAL ASSISTING IS ATHRIVING AND RAPIDLY GROWINGPROFESSION, WITH AN ESTIMATED 5,000PRACTITIONERS INTHE UNITED STATES,A NUMBER THATCOULD EASILY DOUBLE IN THE NEXT FEW YEARS. <

This series of commentaries explores theadequacy of the neurosurgery work-force, the educational impact of the
shortened resident work week, and the role of“physician extenders” and other medical spe-cialties in caring for neurosurgical patients.This particular article discusses the role thatneurosurgeons have in neurocritical care andtheir evolving relationship with critical carephysicians.
Our main message is that neurosurgeonsare essential to neurocritical care and thatthe introduction of intensivists to a neurosur-gical service must be done in a way thatestablishes a collaborative relationship thatrespects the unique knowledge and skills ofneurosurgeons. The primary role of the neuro-surgeon in directing the management of criti-cally ill neurosurgical patients must be main-tained. If this is done well, the resulting “win-win” situation benefits everyone, especiallypatients. However, a poorly conceived mar-riage between neurosurgeons and criticalcare physicians may create confusion, ineffi-ciency, and worst of all, misunderstandingsand errors.
Popularity of Neurocritical CareWhy is interest in neurocritical care undergo-ing such apparently rapid growth? One answeris the 80-hour work week, which affects neuro-surgery residents as much as other residents,if not more so. Neurosurgery residents arespending less time in the ICU because, inorder to master surgical technique, they oftenspend as much of their 80 hours as possiblein the operating room.
Another reason is the relentless decline incompensation rates for physicians’ profession-al services. The corresponding pressure tospend one’s time in high-reimbursing activi-ties means that many neurosurgeons mustspend more hours in the operating room andless time taking care of their patients in theICU setting. For non-surgeons, however, criticalcare billing is often quite lucrative, especiallywhen procedures are included.
Lifestyle and workforce are other factors.Many younger physicians opt for specialties orpractice settings that give them ample freetime, whereas some older physicians opt forearly retirement. In some regions, the numberof neurosurgeons willing to put up with the
long and unpredictable hours involved in criti-cal and emergency care has decreased.
The above factors compound an evolvingshortage in neurosurgical human resources.Because of society’s focus on primary care andon areas of health care with greater visibility,the shortage of available neurosurgeons whoare willing and able to look after critically ill neu-rosurgical patients has fallen below the radarscreen of health policy officials and the public.
These factors may come together to createa void in many ICUs that have traditionallybeen run by the neurosurgery service. Otherproviders are stepping forward to fill the void.Note that, in many cases, these physiciansentered the neuro ICU not because of anygreater knowledge or experience, but merelybecause of geography and convenience: theyare often able to spend more time in the ICUthan the neurosurgeons.
Potential ProblemsThe literature contains many articles reportingthe advantages that intensivists bring to a neu-rosurgery service. These are generally meas-ured in administrative endpoints like length of
NEUROSURGEONS, INTENSIVISTSAND THE FUTURE OFNEUROCRITICAL CARE
Alex B. Valadka, MD,FACS
Michael Fehlings, MD,PhD, FRCSC, FACS
Erol Veznedaroglu, MD P. David Adelson, MD,FACS, FAAP
28 WWW.CNS.ORG

WWW.CNS.ORG 29
stay, number of ventilator days, infection rates,etc. Because of publication bias and author-ship bias, the reader would expect such stud-ies to report a benefit. It is harder to demon-strate increases in what most clinicians wouldconsider more clinically relevant endpoints,such as improved management of intracranialpressure, accurate detection of neurologicaldeterioration, judicious use of resources, orother key aspects of neurocritical care.
Some hospitals use a “closed” ICU model,in which only the ICU team can manage andwrite orders on ICU patients. However, neuro-surgeons may still be held accountable by hos-pital administration for cost, length of stay andother variables that are beyond their control.Families may become confused because theystill view the neurosurgeon as the primaryphysician and the one who bears responsibili-ty for patient care.
A current popular approach to critical careemphasizes “the team,” with attending physi-cians, fellows, residents, nurses, respiratorytherapists, pharmacists, physical therapists andothers all having a role to play. Unfortunately,work hour limitations, teaching conferences andshift changes for the many team members mayimpede continuity of patient care. Subtlechanges in neurological exams may be missed,but in other cases, misunderstandings mayprompt a mistaken diagnosis of neurologicaldeterioration. The result may be costly andpotentially deleterious transport for unneces-sary CT scans and other tests that might nothave been ordered by the neurosurgeon whoknows the patient and has been following him orher throughout the hospital course. Frequenthandoffs are necessary, but so many team
members changing shifts so frequently meansthat sign-outs occupy more and more time.
Assuring uniform levels of competence isalso difficult when so many individuals fromdifferent specialties are represented. Forexample, a patient who is aphasic from a focalleft temporal lesion may be mistaken to be“unresponsive” from a diffuse cerebralprocess, and thus his extubation may beunnecessarily delayed. We all tend to focus onwhat we know. Thus, non-neurosurgeons mayfocus on organ systems other than the brainand spinal cord, perhaps to the extent thatimportant neurologic issues are overlooked.
Another important consideration is that ICU-based physicians may not appreciate the fullscope of a patient’s illness, which includes ini-tial presentation, possible surgery, ICU stay,rehabilitation, and long-term follow-up. At the
same time, neurosurgery residents miss a criti-cal part of that spectrum if they do not addressthe critical care portion of a patient’s recovery.A thorough grounding in neurosurgical criticalcare is essential to understanding the founda-tions of neurosurgery, including cerebral bloodflow and metabolism, spinal cord and peripher-al nerve recovery, and the interplay between thenervous system and systemic physiology.Continuity across the spectrum improvespatient care, increases a physician’s experi-ence and knowledge, and provides importantreassurance and constancy to families.
When one considers all of the aboveissues, it is clear that neurosurgeons have akey role to play in directing the managementof critically ill neurosurgical patients and thatmodels which exclude neurosurgeons fromthis role are inherently flawed.
> A CURRENT POPULAR APPROACH TO CRITICAL CARE EMPHASIZES “THE TEAM,”WITH ATTENDING PHYSICIANS, FELLOWS, RESIDENTS, NURSES, RESPIRATORY THERAPISTS, PHARMACISTS, PHYSICAL THERAPISTS AND OTHERS ALL HAVING A ROLE TO PLAY. <

SolutionsFortunately, there is good news on the hori-zon. In increasing numbers, neurosurgeons inboth private and academic groups are makingemergency care the major focus of their prac-tices. In hospitals with a large volume of emer-gencies, it may be more efficient for one ortwo members of the neurosurgical service tofocus on these cases rather than have everyneurosurgeon in the group attempt to juggleemergency cases with an elective schedule.Specialists in emergency work generally play alarge role in the ICU management of theirpatients because this management is oftenfairly straightforward for those who have com-pleted a neurosurgical residency. Componentsof successful practices of this type include asupportive hospital administration that recog-nizes the contribution of trauma and otheremergencies to a hospital’s margin; support-ive colleagues within neurosurgery and amongother specialties; payment of call stipends;and nonparticipation in managed care con-tracts. Neurosurgeons in these roles are ideal-ly suited to direct the care of the intensivistsand other ICU team members.
The satisfactions of an emergency-basedneurosurgical practice have not been lost onresidents, among whom there seems to begrowing interest in this area. Do younger neuro-surgeons interested in this field need a criticalcare fellowship? The answer is “no,” becauseevery ABNS-certified neurosurgeon’s certifi-cate acknowledges his or her expertise in thecritical care management of neurosurgicalpatients. However, it is also true that such a fel-lowship may make it easier to find a job in thisarea. A fellowship in spine, cerebrovascular,
tumor, functional/stereotactic or pediatric neu-rosurgery is not a requirement to perform high-quality work in these areas, but such addition-al training may help boost a residents’ expo-sure beyond what was available during resi-dency. It might also jump-start a career andserve to shorten the time during which one hasto “pay dues” as a young neurosurgeon. Finally,completion of a fellowship may help resolvebattles with hospital credentialing committeesabout adequacy of training and scope of prac-tice. The Society of Neurological Surgeons hasoutlined program requirements for advancedtraining in neurocritical care, which can becompleted with little (if any) extra time addedto residency. (http://www.societyns.org/fellow-ships/requirements-neurocritical_care.html)
In summary, excluding attending and resi-dent neurosurgeons from clinical decision-making in neurocritical care and replacingthem with non-neurosurgical intensivists mayhave significant drawbacks, including ineffi-cient use of resources, weakened residenteducation, and potentially compromisedpatient care. Ideal systems call for otherhealthcare professionals to assist neurosur-geons in the ICU instead of attempting toreplace them. A truly team-based approach,which recognizes the key role of the neurosur-geon in directing the management of the criti-cally ill neurosurgical patient, is the modelwhich achieves the greatest benefits. <
30 WWW.CNS.ORG
> FORTUNATELY,THERE IS GOOD NEWSON THE HORIZON. IN INCREASING NUMBERS, NEUROSURGEONS IN BOTH PRIVATE AND ACADEMICGROUPS ARE MAKING EMERGENCYCARE THE MAJORFOCUS OF THEIRPRACTICES. <

WWW.CNS.ORG 31
Hospitalists are physicians whose pri-mary professional focus is the generalmedical care of hospitalized patients.
Many patients are referred to hospitalists bytheir primary care physicians (PCPs) for treat-ment during hospitalization and are thenreturned to the care of their PCPs after dis-charge. Fueled by documented efficiencygains and quality benefits, hospitalist-basedinpatient care has grown rapidly over the pastdecade. Recent data from the AmericanHospital Association suggest there are over20,000 hospitalists in the U.S. practicing atover 50% of the nation’s hospitals. The num-ber of hospitalists is expected to exceed30,000 by 2010. One of the variables mostlikely to shift the projected number of hospital-ists upward is the increasing role they are play-ing in the care of surgical patients.
Today’s surgeon caring for hospitalizedpatients faces the same demands PCPs haveexperienced over the past decade: 1) anaccountability for quality and 2) the need forincreased productivity and efficiency. ForPCPs who were trying to juggle these demandsfor both outpatients and inpatients, theinvolvement of a hospitalist has allowed themto narrow their focus. Now they are able to letthe hospitalist worry about quality, safety, andefficiency issues for hospitalized patients.Surgeons in teaching hospitals have facedsimilar challenges, but have relied heavily on
residents and fellows to manage much ofpatients’ postsurgical hospital care.
General internists and subspecialists werecertainly always available for medically com-plex patients, but most day-to-day manage-ment fell to the surgeons. Work-hour restric-tions, combined with an increasingly older andmore medically complex patient population,have resulted in the need to consider newmodels of care. Increasingly, models of surgi-cal co-management have been developing inhospitals with robust hospitalist programs.
Surgical co-management differs from tradi-tional consultation in many ways. First, co-man-agement is often arranged prior to the patientbeing hospitalized. A hospitalist or group ofhospitalists may have an arrangement with agroup of surgeons to co-manage all of theirhospitalized patients, or more often, the sub-set with complex comorbid illness. The sur-geons remain the attending of record in someprograms, but in others, it is the hospitalistwho assumes the role of attending physicianwith the surgeon managing exclusively opera-tive issues. In both models it is common for thehospitalist co-managers to write orders anddaily progress notes, manage acute issues,communicate with family and referring physi-cians, and facilitate care transitions.
The literature describing outcomes withsuch models has been limited to a few pro-grams and most often involves co-manage-
HOSPITALISTS ON THENEUROSURGICAL TEAM
Scott A. Flanders, MDAssociate Professor ofMedicine, University ofMichiganPresident-Elect, Societyof Hospital Medicine
Patrick J. Cawley, MDPresident, Society ofHospital Medicine
> RECENT DATA FROM THE AMERICANHOSPITALASSOCIATION SUGGEST THERE ARE OVER 20,000HOSPITALISTS IN THE U.S. PRACTICINGAT OVER 50% OF THE NATION’S HOSPITALS. <

32 WWW.CNS.ORG
> THE GROWTH OF HOSPITAL MEDICINE HAS BEEN FUELED BY THERECOGNITION THAT HOSPITALISTS IMPROVE THE EFFICIENCY OFINPATIENT CARE WHILE SIMULTANEOUSLY FOCUSING ON IMPROVINGQUALITY AND SAFETY. <

WWW.CNS.ORG 33
ment with hospitalists and orthopedists. TheHospitalist Orthopedic Team (HOT) trial ran-domized 526 patients undergoing elective hipor knee replacement at the Mayo Clinic.Hospitalist co-management was associatedwith modest reductions in length of stay andminor complications. A follow-up study fromthe same institution evaluated 466 patientsover age 65 hospitalized with hip fracture. Co-managed patients went to surgery faster andwere discharged faster after surgery. Neitherstudy demonstrated mortality benefits.Importantly, however, the HOT trial did demon-strate increased surgeon and nurse satisfac-tion. Older literature from the “pre-hospitalist”era has also addressed a variety of co-manage-ment models and in several cases has shownco-management by internists and geriatriciansto be associated with positive outcomes.
The experience with hospitalist co-manage-ment of neurosurgical patients is more limit-ed, but at least one preliminary communica-tion from the University of California, SanFrancisco (UCSF) suggests successful modelsdo exist. Evaluation of the first year of a hospi-talist-led neurosurgery co-management serv-ice at UCSF (on which hospitalists actively co-managed the sickest 30% of the patients andwere immediately available to consult on theothers) led to tremendous increases in per-ceived quality of care among both neurosur-geons and nurses.
Despite early positive reports, concernsremain about widespread application of theco-management model. Theoretically, in well-designed programs surgeons and hospitalistswould work together collaboratively underclear rules of engagement with mutual
respect and accountability to the needs of allmembers of the team. Unfortunately, this isnot always the case. Anecdotally, many pro-grams struggle with lopsided power structureswhere the surgeons dictate the care of thepatients and expect the hospitalist to carry outtheir every wish. Such programs are oftenviewed by the hospitalists who work in themas being designed by surgeons and hospitalsfor the sole purpose of making surgeonshappy and allowing them to operate on morecases without being “burdened” by the routineday-to-day postoperative care of patients.
Hospitalists in these programs also reportsignificant concerns about accountability andmedico-legal issues that arise when patientsdevelop postoperative complications or areadmitted to the hospitalist (instead of the neu-rosurgeon) in the middle of the night with aneurosurgical problem. If the neurosurgeondecides not to see the patients or deal withproblems in a timely fashion, patients sufferand the hospitalist is now exposed to liabilityrisk. To avoid these problems, programs mustbe developed with the primary goal of improv-ing quality of care (including patient andprovider satisfaction) while also attempting tomaximize efficiency.
Even if they are designed well, co-manage-ment programs remain challenged by impor-tant external forces including reimbursementshortfalls and workforce shortages.Hospitalist and co-management programs arerarely financially self-sustaining, especially ifthey provide “unreimburseable” services suchas 24/7 availability. They often require finan-cial support from hospitals which see a sub-stantial return on their investment in hospital-
ist programs (largely through improved effi-ciency). While some hospitals have directlysupported co-management programs (UCSF’smodel is one example), others may be reluc-tant to invest without some support-in-kindfrom the surgeons. If the hospitalists are man-aging much of the routine postoperative care,some hospitals have argued that the surgeonsshould share a portion of the “global fee” fromthe surgery to support the co-managementprogram. That issue has been a sticking pointin several negotiations we are aware of. Andfinally, hospital medicine faces a severe work-force shortage. Most hospitalists are generalinternists, and with a growing demand for hos-pitalists combined with declining interests ingeneral medicine careers among medical stu-dents, there now exist over 10 hospitalist jobopenings for every prospective candidate.Increasing the demand for hospitalists bydeveloping more surgical co-management pro-grams further aggravates the existing work-force shortages and as a result, may not befeasible in the short term.
While the concerns we raise are real, thereare many examples of programs which havesuccessfully overcome them. The growth ofhospital medicine has been fueled by therecognition that hospitalists improve the effi-ciency of inpatient care while simultaneouslyfocusing on improving quality and safety.Surgical co-management programs are likelyto experience the same benefits from hospital-ists that hospitals have seen. If the challengescan be overcome and successful co-manage-ment programs developed, hospitalists willlikely be viewed as valuable members of theneurosurgical team. <
> WITH A GROWING DEMAND FOR HOSPITALISTS COMBINED WITHDECLINING INTERESTS IN GENERAL MEDICINE CAREERS AMONG MEDICALSTUDENTS, THERE NOW EXIST OVER 10 HOSPITALIST JOB OPENINGS FOREVERY PROSPECTIVE CANDIDATE. <

34 WWW.CNS.ORG
Parkinson’s Disease
The first report from the VA cooperativestudy of deep brain stimulation versuscontinued medical management in the
treatment of Parkinson’s Disease (PD)appeared in January (Weaver et al. JAMA.2009 Jan 7;301(1):63-73). This study random-ized 255 patients to surgery or continuedmedical management. Within the surgicalarm, patients were randomized to bilateralsubthalamic nucleus (STN) or pallidal (GPi)deep brain stimulation (DBS). In this initialreport, results from the two targets werepooled. Outcomes in the surgical arm weresuperior to best medical therapy in terms ofmotor improvements and quality of life at sixmonths. However, the surgical group did have
a higher rate of serious adverse events,including falls, dystonia, hardware failures,infections and one death secondary to intrac-erebral hemorrhage. This study and othersconfirm that there is a cognitive price to payfor improved motor function and quality of life,with mild changes in verbal fluency and work-ing memory. With this study, there are now fiverandomized controlled trials that demonstratesuperiority of surgical treatment to continuedmedical management in appropriately chosenpatients with PD (Vitek et al. Ann Neurol. 2003May;53(5):558-69; Esselink et al. Neurology.2004 Jan 27;62(2):201-7; Deuschl et al. NEngl J Med. 2006 Aug 31;355(9):896-908;Schupbach et al. Neurology. 2007 Jan23;68(4):267-71). The challenge is determin-ing when a patient has failed medical therapyand should be referred to a surgical center.The Functional community looks forward tosubsequent reports from the VA cooperativestudy with longer outcomes and subgroupanalysis, especially the comparison betweenthe two surgical targets.
In addition to DBS, Ceregene completed itsPhase II trial of intraputaminal neurturin genetherapy for PD. Although not yet published,Ceregene has issued a press release statingthat the trial failed to show efficacy of the vec-tor over placebo. Neurologix has started itsPhase II trial of glutamic acid decarboxylasegene therapy delivered to the STN for PD.
Psychiatric DiseaseA consortium of American and Belgian neuro-surgeons published long-term results of openlabel ventral striatal DBS for Obsessive-Compulsive Disorder (OCD) in 26 patients(Greenberg et al. Mol Psychiatry 2008). Overan eight-year period, they refined their targetwith decreased current required for therapyand increased efficacy, although the numberof patients was small. On the basis of theseresults, Medtronic received a Human DeviceExemption for ventral striatal DBS for medical-ly refractory OCD from the FDA in February2009. A French consortium published a beau-tifully designed and executed trial of STN DBSfor OCD using a randomized, blindedcrossover design (Mallet et al. N Engl J Med.2008 Nov 13;359(20):2121-34). The targetwithin the STN was more anterior and medialto what is usually used for PD. This trialdemonstrated significant benefit in theactive therapy arm, both in reduction of OCDsymptoms as measured by the Yale-BrownObsessive Compulsive Score (Y-BOCS) andimprovement in Global Assessment ofFunction. This trial has set the bar quite highfor subsequent studies of surgical treatmentof psychiatric disease.
Both American and Canadian groups hadsignificant publications on open label trials ofDBS for Treatment Resistant Depression(Malone et al. Biol Psychiatry 2008; Lozano et
SECTION NEWS
NEWS AND UPCOMING EVENTS IN FUNCTIONAL NEUROSURGERYSIGNIFICANT ADVANCES IN FUNCTIONAL NEUROSURGERYTOOK PLACE IN 2008 AND EARLY 2009
Jason M. Schwalb, MDDetroit, MI

WWW.CNS.ORG 35
al. Biol Psychiatry. 2008 Sep 15;64(6):461-7)using different targets. The American group hasused a similar target in the ventral striatum towhat they are using for OCD. The Toronto grouphas targeted the subgenual cingulate gyrus(Brodmann Area 25). Both had similar responseand remission rates, but the power require-ments were much higher with the ventral stri-atal target. The FDA granted St. Jude Medical,which holds a US patent for Area 25 DBS forTRD, an Investigational Device Exemption (IDE)for a Phase II study. Medtronic is sponsoring aPhase II study of Area 25 DBS in Germany. TheAmerican consortium is recruiting for theirPhase II study of ventral striatal DBS for TRD.
EpilepsyThe efficacy of resective surgery for medicallyrefractory epilepsy is well established. However,new technology is emerging, in addition to vagalnerve stimulation, for patients with medicallyrefractory epilepsy who are not candidates forresective surgery. Although not published, datawas presented from the prospective, randomized,blinded SANTE trial of thalamic anterior nucleusstimulation for medically refractory epilepsy at the2008 American Epilepsy Society meeting.Medtronic issued a press release stating thatthere was a significant decrease in seizure fre-quency as well as an improvement in quality of life.Neuropace has completed enrollment in its pivotal
trial of its RNS device for epilepsy. Unlike thedevice used in SANTE, which delivers continuousstimulation, the RNS device acts as a demandpacemaker or defibrillator, delivering a pulse whenan algorithm detects seizure activity. We look for-ward to the published results of these two trials.
StrokeDr. Robert Levy presented the results of thePhase III EVEREST study of short-term motor cor-tex stimulation for treatment of stroke patientswith upper extremity hemiparesis at the 2008CNS meeting. Unfortunately, in spite of promisingopen label studies, there was no increased ben-efit of stimulation versus rehabilitation alone.Although they did not reach statistical signifi-cance, subgroup analyses suggested that somepatients benefited from stimulation. These analy-ses may provide a focus for subsequent trials.
It is an exciting time in Functional Neurosurgery.The ability to turn stimulators on and off hasgiven us the ability to perform randomized, con-trolled, blinded trials much more easily than withother surgical techniques. There has been excep-tional refinement of outcomes measure with ourNeurology and Psychiatry colleagues. <
The quadrennial meeting of the World Societyof Stereotactic and Functional Neurosurgery(WSSFN) will take place in Toronto from May24-27 at the Fairmount Royal York Hotel. Theexciting program can be accessed throughwww.wssfn.org. Members of the ASSFN areautomatically members of the WSSFN andcan register at a reduced rate.
The Movement Disorder Society holds itsannual meeting June 7-11 in Paris(www.movementdisorders.org). TheInternational Neuromodulation Society holdsits meeting in Seoul in September (www.neuromodulation.com). The North AmericanNeuromodulation Society (NANS) holds itsannual meeting in Las Vegas in December(http://www.neuromodulation.com/chapter/northamerica). World Parkinson Congress andASSFN meetings next take place in 2010.

For More [email protected] Free: 877 517 1CNS Phone: 847 240 2500
Congress of Neurological Surgeons
2009 ANNUAL MEETINGNew Orleans, Louisiana October 24–29, 2009
Let Your Voice Be Heard at the2009 CNS Annual Meeting.Consensus Sessions offer attendees a chance to contribute to the advancement oforganized neurosurgery by weighing in on critical socioeconomic issues and publicpolicy topics. Available Tuesday and Wednesday, you can participate in one or all!
Consensus Session I:The Role of Mid-level Health Care Providers in ModernNeurosurgery Practice.Moderator: Edward C. Benzel
Consensus Session II:Individual Practice Options for Insurance Plan Participation.Moderators: Joshua M. Rosenow, Richard W. Byrne
Consensus Session III:Regionalizing Emergency Cerebrovascular Care.Moderators: Jamie Sue Ullman, Henry H. Woo
Consensus Session IV:Defining Quality Measures in Neurosurgery.Moderator: Robert Weil
These unique workshops allow attendees the opportunity to truly be a part of theCNS Annual Meeting and the future of neurosurgery!
The Congress of Neurological Surgeons is Pleased toAnnounce a Joint Meeting with theNeurological Society of India (NSI) and the American Association of South Asian Neurosurgeons (AASAN)!
Registration Now Open at www.cns.org!
CNS09AM_ConsensusSessions:CQM 3/26/09 2:45 PM Page 1

WWW.CNS.ORG 37
Current Language
ARTICLE IV
Membership Section 1. Members. There shall be ten (10)classes of membership in the Congress:Active Membership, Honorary Membership,Senior Membership, Inactive Membership,International Membership, InternationalVista Membership, Resident Membership,Associate Membership, Medical Student,and Affiliate Membership. Only active mem-bers shall be entitled to vote. The member-ship may be international in scope, andthere is no limit to the number of members.
Proposed Language
ARTICLE IV
MembershipSection 1. Members. There shall be ten (10)classes of membership in the Congress:Active Membership, Honorary Membership,Senior Membership, Inactive Membership,International Membership, InternationalVista Membership, Resident Membership,Associate Membership, Medical Student,and Affiliate Membership. Only Active, ActiveInternational, and Active International Vistamembers shall be entitled to vote. The mem-bership may be international in scope, andthere is no limit to the number of members.
Under the current CNS Bylaws, it is possible for the motivated reader to interpret Article IV,Sections 1 and 4 with contradictions as to the voting membership of the CNS. Article IV, Section1 states that “only active members shall be entitled to vote” (emphasis added). While Article IV,Section 4 states that both Active International Members and Active International Vista Membersshall “have all of the rights, privileges, duties and obligations of an Active Member” with theexception of holding a position of officer in the CNS (both may serve as members or chairpersonsof committees however).
The following amendment to Article IV, Section 1 would resolve any ambiguity that may existbetween Article IV, Sections 1 and 4 and clarify that Active, Active International Members andActive International Vista Members are all voting members of the CNS. <
PROPOSEDBYLAWSAMENDMENT
INSIDE THE CNS
Alan Scarrow, MDChair, CNS BylawsCommittee


If you are looking for something to do on thethird Tuesday of every month, look no fur-ther. The CNS University of Neurosurgery
(CNSU) has launched its new CME-generatingWebinar series. From the convenience of theoffice or home, attendees can partake of a livelecture series featuring experts from variousdisciplines talking about current and practice-relevant topics.
On January 13, 2009, the CNSU presentedits first webinar on pediatric neurosurgery,Management of Arachnoid Cysts. Mark Kriegerfrom the University of Southern Californiaexpertly moderated this webinar, while SeanMcNatt from Denver’s Children’s Hospital andRichard Anderson from New York’s ColumbiaPresbyterian Hospital, presented Fenestrationof Arachnoid Cysts and Shunting of ArachnoidCysts, respectively. Through interactive audi-ence polling and active discussion, the webi-nar was well-received by all participants.
Since its inception, the webinar series hasincluded Current Practice in the Treatment ofPeripheral Nerve Trauma, with Allen Manikerfrom New York’s Beth Israel Medical Center.This lecture was presented on February 17,2009 with excellent attendance. On March 17,2009, Drs. James Harrop, Michael Wang andAllan Levi, presented a three-part discussionof thoracolumbar trauma management. Alongwith audience polling and case discussions,the session was lively and informative for all.
In April, we look forward to the SurgicalManagement of Brain Arteriovenous Malform-ations, with Hunt Batjer and Bernard Bendok.In May, we will discuss how government regu-lations affect neurosurgical practice with rep-resentatives from the Council of State
Neurosurgical Societies. To round out the firstsix months of this series, Drs. Charles Wilsonand Philip Theodosoupolos will discuss man-agement of pituitary tumors.
The webinar series is an exciting new offer-ing of the CNSU to advance neurosurgical edu-cation and obtain CME credit without having totravel. Signing on is easy and affordable. Eachprogram is $25 and prospective attendees canaccess registration through the CNSU athttp://www.cns.org/university/webinar/index.asp. We encourage all to go to the CNSU site athttp://univ.cns.org/ to take advantage of fur-ther University programs. In addition, we arelooking forward to presenting a new look to theCNSU site in the Fall, where one will find evenmore exciting content and course offerings.
Do not delay. Register for CNS UniversityWebinars today! <
THE CNSUNIVERSITY OFNEUROSURGERYLAUNCHES NEW WEBINARSERIES
Jamie S. Ullman, MD,FACS
WWW.CNS.ORG 39
> THE WEBINARSERIES IS ANEXCITING NEWOFFERING OF THECNSU TO ADVANCENEUROSURGICALEDUCATION ANDOBTAIN CME WITHOUT HAVING TO TRAVEL. <

40 WWW.CNS.ORG
A Neurosurgical Resident is called to the ER to see a 5-year old with a laundry list of symptomswho just had a CT of the head. There it is…an enhancing mass in the posterior fossa with hydro-cephalus (photos at right).
• What could it be? • What should be done with the hydrocephalus? • Does this correlate with the symptoms?• What to do?
The Congress of Neurological Surgeons web site is the next move. Grabbing her smart phone,she accesses the Pediatric eHandbook at the CNS University of Neurosurgery. She clicks onInfratentorial Tumors and reads about the differential diagnosis and current management pro-tocols. She picks up the phone seven minutes later, “Dr. Ritter, I have a 5-year old female thatlooks to have a posterior fossa tumor. It looks like a medulloblastoma, or less likely an ependy-moma. There is hydrocephalus, but she does not need a ventriculostomy at this time. I amgoing to admit her to the PICU, start steroids and order an MRI of the head and spine for themorning…”
The neurosurgical community is movingswiftly into the future with revolutionaryapplications of technical practices mak-
ing their way into the operating room and radi-ology suites. For example, electrodes are beingplaced into the subthalamic nucleus toimprove the dyskinesia of a Parkinson’s patientand Interventional Neurosurgeons can placecoils into a ruptured PCOM aneurysm usingbiplanar fluoroscopy. The ability to retrieveaccurate, up-to-date information needs to meetthese same rapidly changing demands.
The use of the internet has left our goldstandard textbooks collecting dust on theshelves. Even the Residents’ NeurosurgicalHandbook is rarely seen in a white coat pock-et anymore. Instead, it rests alone in the callroom with the binding barely cracked. It is eas-ier to Google “Medullobastoma” and read themost recent EMedicine article on the topic
than flip through a volume of our most valuedtextbooks, which are usually locked behind theAttending’s office door or in the neurosurgerylibrary in the next building.
The CNS and Pediatric Section have startedthe revolution with neurosurgical eHandbooks,which can be accessed from the CNS web site or downloaded onto a smart phone.Pediatric Neurosurgery: On Call, is the first inthe series of texts that provide accurate med-ical information in a timely manner. Thisresource is now available on the CNSUniversity of Neurosurgery site underEducational Tools, http://univ.cns.org or thedirect link http://www.cns.org/university/pedi-atrics/index.asp. This joint venture betweenthe pediatric neurosurgical population and theCNS makes it a powerful, unique educationaltool that is easily accessible from any comput-er or PDA.
Ann M. Ritter, MDVCUHS at ChippenhamCampus
THE CNSUNIVERSITY OFNEUROSURGERYINTRODUCES THEE-HANDBOOK

WWW.CNS.ORG 41
This Pediatric eHandbook is now availableto medical students, neurosurgery residents,pediatric subspecialty fellows (pediatric inten-sive care, pediatric neurosurgical, and pedi-atric neurology, and emergency room fellows,etc), physician extenders and anyone elseattempting to locate data on the web. It pro-vides vital initial information for those in neuro-surgical training while in the emergency room,clinic or during a patient’s late night consult.Pediatric Neurosurgery: On Call is specificallyfocused on the management of pediatric headand cervical trauma. The references in eachchapter can be a preliminary location for themost recent review of the literature.
There are abundant benefits from an elec-tronic textbook or handbook. This formatallows for easy revision of references, newtechniques, pictures, tables and/or any con-tent. This information can be uploaded at the
time of the handbook update or at any timethe authors feel it necessary. There is no wait-ing time for the revisions or proofs from thepublisher, and the lengthy “time to print” isabolished. The use of electronic books pro-vides instantaneous updates!
The way that we acquire information ischanging daily – today’s knowledge is receivedat revolutionary speed via the Internet. TheCNS web site is transforming to meet theseeducational needs. The CNS is getting thereearly, anticipating new means of communica-tion, meeting that anticipation head on, there-by helping our professionals be as knowledge-able as they can be.
The CNS and the Pediatric Section areproud to be at the forefront of this revolution.We are also happy to report, that the secondhandbook in this series, Spine eHandbook, iscurrently underway. <
Child with vermian or fourth ventricular tumor andassociated hydrocephalus. The Pediatric eHandbookprovides information to help Residents formulate a dif-ferential diagnosis and treatment plan.

42 WWW.CNS.ORG
Stradun Street: Night Scene on Stradun Street in Dubrovnik.
> THIS MEETING WAS AN IMPORTANT EVENT FOR THE CROATIANNEUROSURGICAL SOCIETY. IT WILL SERVE AS A PLATFORM FOR FURTHER AFFIRMATION OF THE PROFESSIONAL ACTIVITIES IN OUR SOCIETY AS A WHOLE, AS WELL AS OUR INTERNATIONAL PROFILE BOTH REGIONALLY AND GLOBALLY. <

The 5th Congress of the CroatianNeurosurgical Society in partnership withthe Congress of Neurological Surgeons
was held in Dubrovnik on September 2-5,2008. This joint meeting, the culmination ofyears of cooperation and friendship betweenthe Croatian Neurosurgical Society and theCNS, was a resounding success and providedfurther evidence of the increased internationalfocus of the CNS.
Croatia is a small Mediterranean countrysituated in the southeast of Europe with a pop-ulation of approximately 4.5 million. The coastof Croatia is 1200 kilometers long and thereare more than 1000 islands along the coast-line. Croatia borders Italy, Slovenia andHungary to the north and Serbia, Montenegroand Bosnia and Hercegovina to the east andsouth, respectively.
The Croatian Neurosurgical Society wasofficially formed on June 12, 1992 after thedisbanding of the Jugoslavian NeurosurgicalSociety. Croatian neurosurgeons officiallywithdrew their membership in the JugoslavianNeurosurgical Society following the start ofJugoslav aggression towards Croatia. Croatiadeclared independence which was interna-tionally recognized on January 15, 1992.
The beginnings of neurosurgery in Croatiareach as far back as the 19th century. Generalsurgeon Theodor Wickerhauser published adetailed article regarding craniotomy tech-nique in 1894. The article appeared in thepublication ''Physician News'' which is stillpublished today. The first brain tumor removalarticles date back to 1901 while the first clini-cal data concerning the operative treatment oftrigeminal neuralgia can be traced to 1904.
Esteemed physicians Sercer, Blaskoviç andPadovan (Otolaryngologists) were the pioneersof transsphenoidal pituitary resections inCroatia with the first operative procedures dat-ing back to 1922.
In the period after World War II (from1946), the first neurosurgical unit in Croatiawas formed in Zagreb. In 1972, neurosurgerywas recognized as a specialty and was sepa-rated from the educational and clinical pro-gram in general surgery by the decision of theManaging Board of Zagreb Medical School.Independent residency in neurosurgery aswell as an educational faculty program in neu-rosurgery were introduced several years later.The first microscope-assisted surgical treat-ments were performed in the late seventieswhile the first computed tomography scan wasinstalled in 1975. After Zagreb, neurosurgicalwards and units were starting to emerge inCroatia. In Zagreb, there are currently threeactive neurosurgical units with one unit func-tioning in Split, Rijeka, Zadar, Pula, Osijek andSlavonski Brod.
Today, the Croatian Neurosurgical Societyconsists of 78 members with 64 specialists(59 active and five retired) and 14 neurosurgi-cal residents, who cover all aspects of the dis-cipline ranging from neurotraumatology,spinal surgery, neuro-oncology, functional andstereotactic surgery to radiosurgery.Endovascular procedures are being performedin cooperation with interventional radiologists.
The central neurosurgical institution inCroatia is the Clinical Department of
INTERNATIONAL REPORT
THE CNS GOES TO DUBROVNIK:HIGHLIGHTS OF THE JOINT MEETING WITH THE CROATIANNEUROLOGICAL SOCIETY
Josip Paladino, MD, PhD
Charles Y. Liu, MD, PhDMiroslav Vukic, MD, PhD
CNS participants before social event: Charles Liu, P. David Adelson, Ashwini Sharan, and Nelson Oyesiku.
WWW.CNS.ORG 43

44 WWW.CNS.ORG
Neurosurgery at the Clinical Medical CentreZagreb (Head Professor Josip Paladino) whichis certified by the European Association ofNeurosurgical Societies (EANS) as the Centreof Excellence for education in neurosurgery.
The Current Managerial Board ofthe Croatian NeurosurgicalSociety includes: Professor Josip Paladino, PresidentProfessor Lucijan Negovetic (retired),
Vice-PresidentProfessor Pavle Miklic, SecretaryProfessor Miroslav Vukic, Treasurer
Members of both the Croatian society andthe CNS have helped create and maintain theexcellent relationship enjoyed by our two organ-izations. There are several Active InternationalCNS members in Croatia and professorMiroslav Vukic is a member of the InternationalCommittee of the CNS. Every three years since1999, a National Croatian NeurosurgicalSociety Congress is held with strong connec-tions and cooperation from the CNS.
Beverly C. Walters (Rhode Island) andJamshid Ghajar (New York) were the first neu-rosurgeons from the US to participate in theCroatian Neurosurgical Society Congress inOpatija in 1999. Special gratitude for creatingand sustaining the excellent relations betweenthe Croatian Neurosurgical Society and theCNS goes to Dr. Walters who, since her firstvisit to Croatia in 1998, has visited 24 timesand performed complex neurosurgical proce-dures on many prominent Croatians such asan esteemed neurosugery professor and high-ly positioned government officials, free ofcharge. Dr. Walters has donated microsurgicalinstruments and held many presentations andseminars on cervical spine surgery. She isresponsible for several United States fellow-ships performed by Croatian NeurosurgicalSociety members in 2000 and 2006.
In the 4th Croation Neurosurgical SocietyCongress held in November 2005 (CNS members participating: Beverly C. Walters,
Nelson C. Oyesiku, Chandranath Sen, RichardD. Bucholz, Andrew Youkilis), Dr. Walters pro-posed that the jubilee 5th Congress would beheld as a joint meeting with the CNS inDubrovnik. The idea was met with a warmreception from then CNS InternationalCommittee chairs Drs. Gail Rosseau and Ali Rezai and was finally realized in Dubrovnikin September 2008. The success of the meet-ing resulted from cooperation between theCroatian Neurosurgical Society; the localorganizing committee led by Kresimir Rotim;the CNS; Charles Y. Liu; and members of theExecutive Committee led by then CNSPresident, Tony Asher.
The meeting, under the auspices ofCroatia's President and the city of Dubrovnik,was attended by 142 participants from 15countries and offered a wide range of qualityclinical, as well as scientific, topics. CurrentCNS President David Adelson led the CNS del-egation, which also included Past Presidents ofthe CNS, Nelson C. Oyesiku and RichardEllenbogen, as well as other prominent mem-bers such as Chandranath Sen, LalighamSekhar, Domagoj Coric, Charles Y. Liu, Daniel
K. Resnick, Ashwini Sharan and, of course,Beverly C. Walters. Prominent leaders of neuro-surgery worldwide were also central to the suc-cess of the meeting, including EANS PresidentJohannes Schramm, Jurgen Tonn, MarcosTatagiba, Vinko Dolenc, Vedran Deletis, andmany others too numerous to mention whosecontribution were very much appreciated.
This meeting was an important event forthe Croatian Neurosurgical Society. It willserve as a platform for further affirmation ofthe professional activities in our society as awhole, as well as our international profile bothregionally and globally. The City of Dubrovnik,with its tourist and cultural attributes, was,most certainly, delightful, and the culturalexperience for all attendees was very memo-rable. We would like to extend our deepestthanks to all the members of the CNS partici-pating in this event on behalf of the CroatianNeurosurgical Society and we are hoping forfurther cooperation with our transatlantic col-leagues. <
CNS participants enjoying boat cruise with President of Croatian Neurosurgical Society, Josip Paladino.
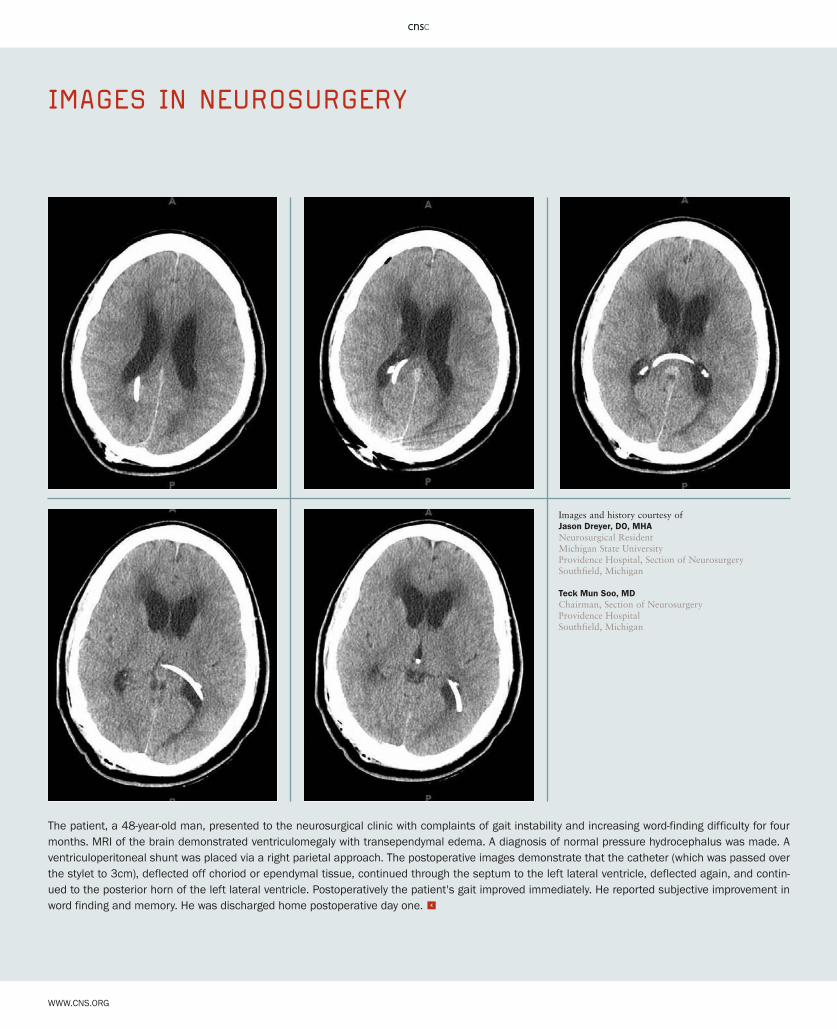
WWW.CNS.ORG
The patient, a 48-year-old man, presented to the neurosurgical clinic with complaints of gait instability and increasing word-finding difficulty for fourmonths. MRI of the brain demonstrated ventriculomegaly with transependymal edema. A diagnosis of normal pressure hydrocephalus was made. Aventriculoperitoneal shunt was placed via a right parietal approach. The postoperative images demonstrate that the catheter (which was passed overthe stylet to 3cm), deflected off choriod or ependymal tissue, continued through the septum to the left lateral ventricle, deflected again, and contin-ued to the posterior horn of the left lateral ventricle. Postoperatively the patient's gait improved immediately. He reported subjective improvement inword finding and memory. He was discharged home postoperative day one. <
IMAGES IN NEUROSURGERY
Images and history courtesy of Jason Dreyer, DO, MHANeurosurgical ResidentMichigan State UniversityProvidence Hospital, Section of NeurosurgerySouthfield, Michigan
Teck Mun Soo, MDChairman, Section of NeurosurgeryProvidence HospitalSouthfield, Michigan