mri findings in kallmann syndrome h. zaghouani ben alaya, z. achour, m.bhouri, m. limeme, s....
TRANSCRIPT
MRI findings in Kallmann syndrome
H. ZAGHOUANI BEN ALAYA, Z. ACHOUR, M.BHOURI, M. LIMEME, S. MAJDOUB, H.
AMARA, D. BAKIR, CH. KRAIEM
HN27
INTRODUCTION:Kallmann syndrome is an inherited disorder characterized by hypogonadotrophic hypogonadism and anosmia or hyposmia.
KS is due to abnormal migration of gonado-tropin-releasing hormone (GnRH) as well as olfactory neurons from olfactory placode to the forebrain and hypothalamus during fetal life.
Structural olfactory tract abnormalities are well seen on MRI
PURPOSE:
the aim of this work is to describe the MR appearance of the olfactory bulbs and tracts in patients with Kallmann syndrome,
MIETHODS:
High-resolution MR scans were performed in two patients with Kallmann syndrome.
Coronal T2 weighted contiguous sections were obtained through the olfactory bulbs and tracti.
RESULTS:
Cases:A 15-year-old female and 20-year-old male adressed to MRI for hypogonadotrophic hypogonadism ((Serum LH < 1.5 IU/L, Serum FSH < 1.5 IU/L, Testosterone <20 ng/dl) and hyposmia.
Coronal T2-weighted MR images through the anterior fossa shows: aplasia of both olfactory bulb and absence of the left olfactory sulcus (case1).Bilateral aplasia of olfactory bulb with normal olfactory tract (case2)
No other cranial abnormality found.
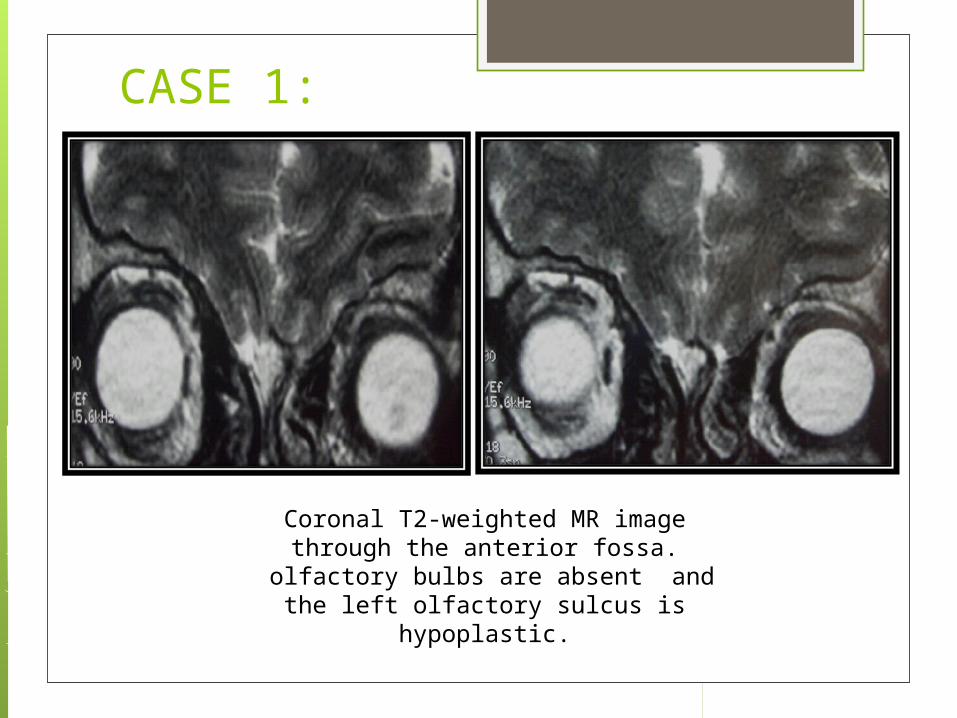
CASE 1:
Coronal T2-weighted MR image through the anterior fossa.
olfactory bulbs are absent and the left olfactory sulcus is hypoplastic.
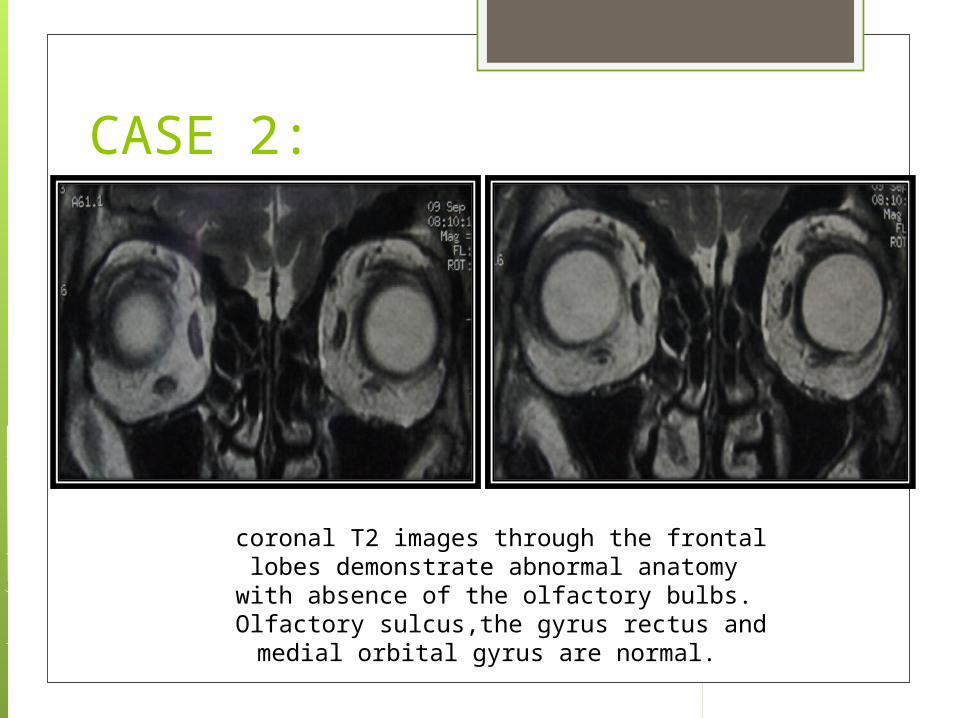
CASE 2:
coronal T2 images through the frontal lobes demonstrate abnormal anatomy with absence of the
olfactory bulbs. Olfactory sulcus,the gyrus rectus and medial orbital
gyrus are normal.
DISCUSSION:
Kallmann syndrome is an inherited disorder characterized by hypogonadotrophic hypogonadism and anosmia or hyposmia.
The inheritance may be X-linked, Autosomal recessive or Autosomal dominant with variable penetrance.
The reported incidence is 1 in 10,000 men and 1 in 50,000 women.
Kallmann syndrome is an anomaly of neuronal
migration.
Cells that differentiate into Gonadotrophin releasing
hormone (GnRH) secreting neurons originate from
within embryonic olfactory epithelium and migrate
along fascicles of vomeronasal and terminalis nerves
into forebrain.
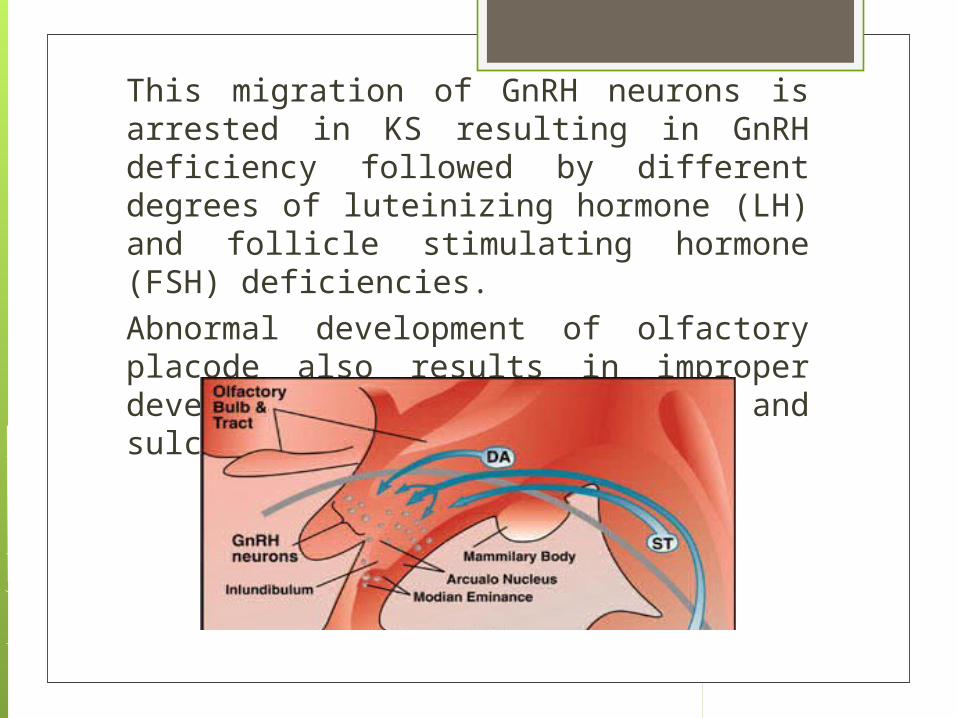
This migration of GnRH neurons is arrested in KS resulting in GnRH deficiency followed by different degrees of luteinizing hormone (LH) and follicle stimulating hormone (FSH) deficiencies.
Abnormal development of olfactory placode also results in improper development of olfactory bulbs and sulci.
diagnosis of KS in adults is fairly straightforward,
depending on the co-existence of anosmia with subnormal levels of gonadal steroids and gonadotrophins.
However the diagnosis may be difficult to establish in patients of pre-pubertal age who may require genetic testing and MRI.
In such patients, MRI enables a presumptive diagnosis of KS to be made by demonstrating characteristic abnormalities in olfactory sulci and tracttory.
IMAGINGMorphological abnormalities of olfactory apparatus in KS
are best evaluated with MRI.
High resolutions coronal fast spin echo T2W images are the
preferred sequences for morphologic evaluation of the
olfactory system.
Olfactory bulbs are optimally visualized in coronal planes.
it is easier to appreciate anatomical anomalies present in Kallmann syndrome by comparing it to a normal patient.
The normal anatomy of the region consists of the olfactory bulbs located in the olfactory grooves of the anterior cranial fossa.
The inferior surface of the frontal lobes usually consists gyrus rectu separated from the medial orbital gyrus (M) by the olfactory sulcus (yellow arrow).
o
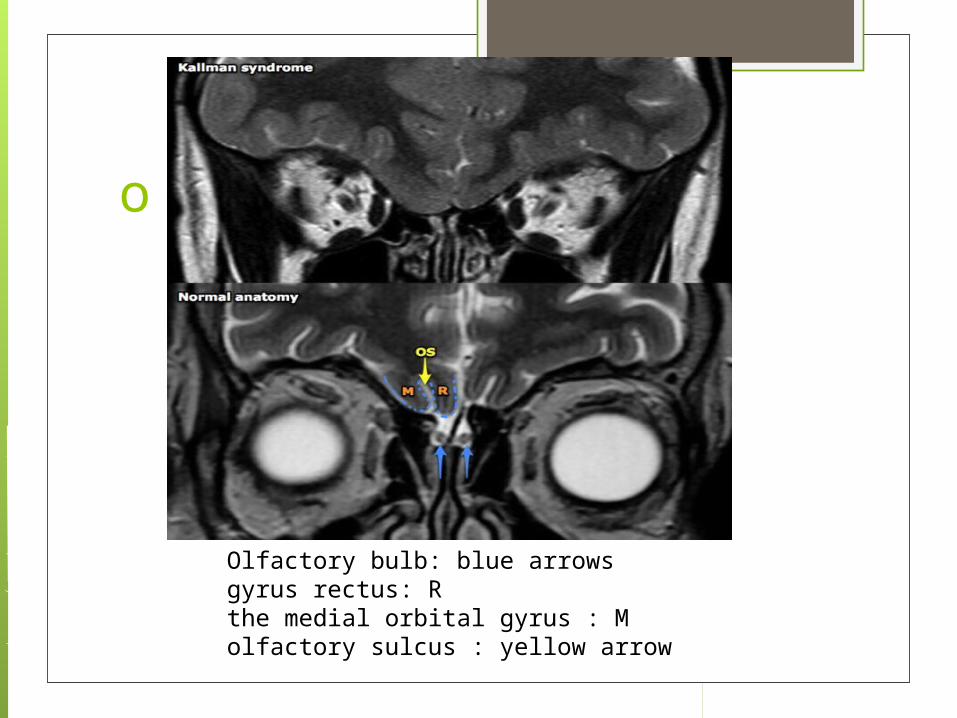
Olfactory bulb: blue arrowsgyrus rectus: Rthe medial orbital gyrus : Molfactory sulcus : yellow arrow

MRI FINDINGS: hypoplasia of the olfactory bulbs with olfactory
tracts present,
aplasia of the olfactory bulbs with olfactory tracts
present.
aplasia of both olfactory bulbs and olfactory tracts
It was also described mild to moderate volume
loss in temporal and frontal lobes
Hypoplasia of anterior pituitary may be secondary
to limited stimulation due to absence of
hypothalamic GnRH neurons.
CONCLUSION:Kallmann’s syndrome is a rare genetic disorder.
High resolutions coronal fast spin echo T2W is the preferred sequences for morphologic evaluation of the olfactory system.