mucosal melanoma of the head and · pdf filemucosal melanoma of the head and neck version...
TRANSCRIPT

© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
320
Jatin P. Shah, MD, PhD; Sharon Spencer, MD; Andrea Trotti, III, MD; Randal S. Weber, MD; Gregory Wolf, MD; and Frank Worden, MD
Overview Mucosal melanoma (MM) is a rare, very aggres-sive noncutaneous melanoma that affects the upper aerodigestive tract, genitourinary tract, and anal/rec-tal region.1 This portion of the NCCN Clinical Prac-tice Guidelines in Oncology (NCCN Guidelines) for Head and Neck (H&N) Cancers only describes MMs of the H&N, which constitute fewer than 10% of melanomas of the H&N.1,2 Note that a separate NCCN Guideline is available for cutaneous melano-ma (see NCCN Guidelines for Melanoma, available in this issue and online at www.NCCN.org).
NCCN
Mucosal Melanoma of the Head and NeckClinical Practice Guidelines in Oncology
David G. Pfister, MD; Kie-Kian Ang, MD, PhD; David M. Brizel, MD; Barbara Burtness, MD; Anthony J. Cmelak, MD; A. Dimitrios Colevas, MD; Frank Dunphy, MD; David W. Eisele, MD; Jill Gilbert, MD; Maura L. Gillison, MD, PhD; Robert I. Haddad, MD; Bruce H. Haughey, MBChB, MS; Wesley L. Hicks, Jr., MD; Ying J. Hitchcock, MD; Merrill S. Kies, MD; William M. Lydiatt, MD; Ellie Maghami, MD; Renato Martins, MD, MPH; Thomas McCaffrey, MD, PhD; Bharat B. Mittal, MD; Harlan A. Pinto, MD; John A. Ridge, MD, PhD; Sandeep Samant, MD; Giuseppe Sanguineti, MD; David E. Schuller, MD;
NCCN Clinical Practice Guidelines in Oncology for Mucosal Melanoma of the Head and Neck
Key WordsNCCN Clinical Practice Guidelines, NCCN Guidelines, muco-sal melanoma, head and neck cancer, biopsy, neck dissec-tion, adjuvant therapy, radiation therapy, chemotherapy, pathology(JNCCN 2012;10:320–338)
NCCN Categories of Evidence and ConsensusCategory 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate.Category 2A: Based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate.Category 2B: Based upon lower-level evidence, there is NCCN consensus that the intervention is appropriate.Category 3: Based upon any level of evidence, there is major NCCN disagreement that the intervention is appropriate.
All recommendations are category 2A unless otherwise noted.
Clinical trials: NCCN believes that the best management for any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Please NoteThe NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) are a statement of consensus of the authors regarding their views of currently accepted ap-proaches to treatment. Any clinician seeking to apply or consult the NCCN Guidelines® is expected to use indepen-dent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The National Comprehensive Cancer Network® (NCCN®) makes no representation or warranties of any kind regarding their content, use, or application and disclaims any respon-sibility for their applications or use in any way.
© National Comprehensive Cancer Network, Inc. 2012, All rights reserved. The NCCN Guidelines and the illustrations herein may not be reproduced in any form without the express written permission of NCCN.Disclosures for the NCCN Mucosal Melanoma of the Head and Neck Panel
At the beginning of each NCCN Guidelines panel meeting, panel members disclosed any financial support they have received from industry. Through 2008, this information was published in an aggregate statement in JNCCN and online. Furthering NCCN’s commitment to public transparency, this disclosure process has now been expanded by listing all potential conflicts of interest respective to each individual expert panel member.
Individual disclosures for the NCCN Mucosal Melanoma of the Head and Neck Panel members can be found on page 338. (The most recent version of these guidelines and accompany-ing disclosures, including levels of compensation, are avail-able on the NCCN Web site at www.NCCN.org.)
These guidelines are also available on the Internet. For the latest update, visit www.NCCN.org.

Mucosal Melanoma of the Head and Neck
NCCNGuidelines®
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
321
Journal of the National Comprehensive Cancer Network
Text continues on p. 332
The full NCCN Guidelines for H&N Cancers address tumors arising in the upper aerodigestive tract (i.e., lip, oral cavity, pharynx, larynx, paranasal sinuses; see Figure 1). Occult primary cancer, salivary gland cancer, and MM are also addressed.3 Many of the approaches for managing H&N cancer are also applicable to MM (e.g., multidisciplinary team, sur-gical principles). To view the full NCCN Guidelines for H&N Cancers, visit the NCCN Web site at www.NCCN.org.
By definition, the NCCN Guidelines cannot in-corporate all possible clinical variations and are not intended to replace good clinical judgment or individ-ualization of treatments. Exceptions to the rule were discussed among the members of the NCCN H&N Cancers Panel while developing these guidelines.
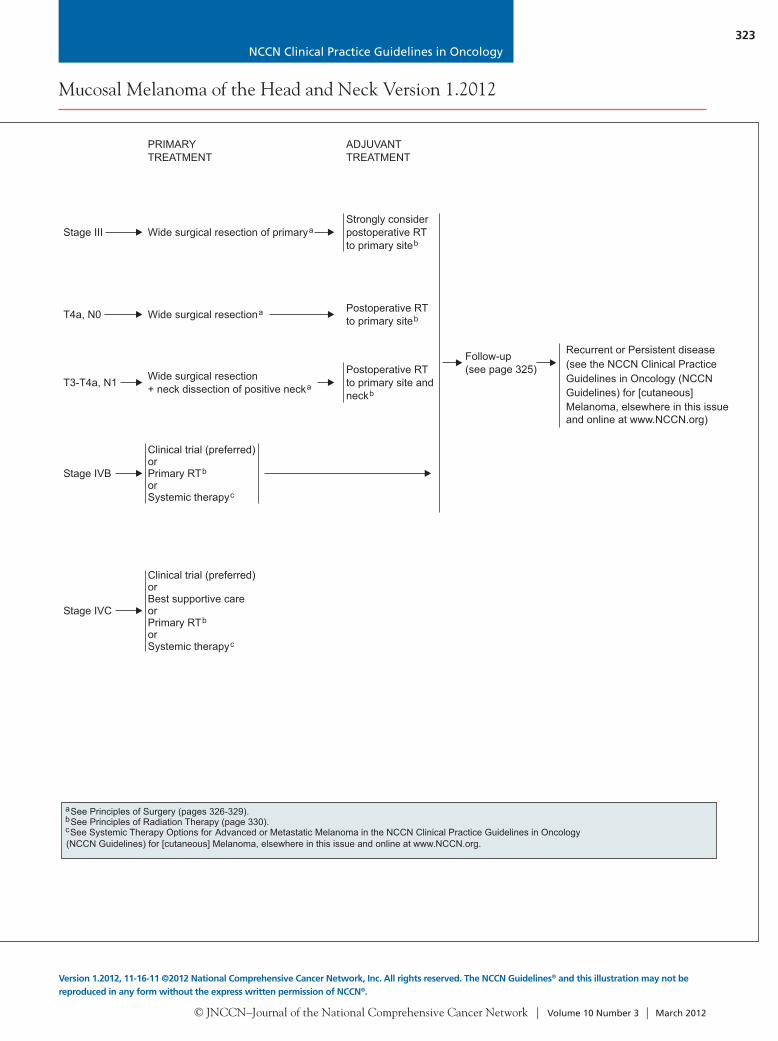
Management ApproachesThe staging system for MM begins with stage III dis-ease, which is the most limited form of disease for MM (see Workup and Staging, page 333).4 Surgery (with or without radiation therapy [RT]) is the primary treatment for stage III MM, whereas surgery followed by RT or systemic therapy is the primary treatment for stage IV MM, depending on systemic involvement.
Multidisciplinary Team InvolvementThe initial evaluation and development of a plan for treating patients with MM require a multidisci-plinary team of health care providers with expertise in caring for these patients. Similarly, managing and preventing sequelae of radical surgery, RT, and
NCCN Mucosal Melanoma of the Head and Neck Panel Members*David G. Pfister, MD/Chair†Þ
Memorial Sloan-Kettering Cancer Center*Kie-Kian Ang, MD, PhD§
The University of Texas MD Anderson Cancer Center*David M. Brizel, MD§
Duke Cancer InstituteBarbara Burtness, MD†
Fox Chase Cancer CenterAnthony J. Cmelak, MD§
Vanderbilt-Ingram Cancer CenterA. Dimitrios Colevas, MD†
Stanford Comprehensive Cancer CenterFrank Dunphy, MD†
Duke Cancer InstituteDavid W. Eisele, MD¶
UCSF Helen Diller Family Comprehensive Cancer CenterJill Gilbert, MD†
Vanderbilt-Ingram Cancer Center*Maura L. Gillison, MD, PhD¶
The Ohio State University Comprehensive Cancer Center – James Cancer Hospital and Solove Research Institute
Robert I. Haddad, MD†Dana-Farber/Brigham and Women’s Cancer CenterMassachusetts General Hospital Cancer Center
Bruce H. Haughey, MBChB, MS¶Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of medicine
Wesley L. Hicks, Jr., MD¶Roswell Park Cancer Institute
Ying J. Hitchcock, MD§ Huntsman Cancer Institute at the University of Utah
Merrill S. Kies, MD†The University of Texas MD Anderson Cancer Center
*‡William M. Lydiatt, MD¶ζUNMC Eppley Cancer Center at The Nebraska Medical Center
Ellie Maghami, MD¶ζ
City of Hope Comprehensive Cancer CenterRenato Martins, MD, MPH†
Fred Hutchinson Cancer Research Center/Seattle Cancer Care Alliance
Thomas McCaffrey, MD, PhDζH. Lee Moffitt Cancer Center & Research Institute
Bharat B. Mittal, MD§Robert H. Lurie Comprehensive Cancer Center of Northwestern University
Harlan A. Pinto, MD†ÞStanford Comprehensive Cancer Center
John A. Ridge, MD, PhD¶Fox Chase Cancer Center
Sandeep Samant, MD¶St. Jude Children’s Research Hospital/University of Tennessee Cancer Institute
Giuseppe Sanguineti, MD§The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
David E. Schuller, MD¶The Ohio State University Comprehensive Cancer Center – James Cancer Hospital and Solove Research Institute
*‡Jatin P. Shah, MD, PhD¶Memorial Sloan-Kettering Cancer Center
Sharon Spencer, MD§University of Alabama at BirminghamComprehensive Cancer Center
*‡Andrea Trotti, III, MD§H. Lee Moffitt Cancer Center & Research Institute
Randal S. Weber, MD¶The University of Texas MD Anderson Cancer Center
Gregory Wolf, MD¶ζUniversity of Michigan Comprehensive Cancer Center
Frank Worden, MD¶†University of Michigan Comprehensive Cancer Center
NCCN Staff: Miranda Hughes, PhD, and Nicole McMillian, MS
KEY:*Writing Committee Member‡Mucosal Melanoma Subcommittee Member.
Specialties: †Medical Oncology; ÞInternal Medicine; §Radiation Oncology; ¶Surgery/Surgical Oncology; ζOtolaryngology

© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
322
Mucosal Melanoma of the Head and Neck Version 1.2012
Clinical trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. All recommendations are category 2A unless otherwise indicated.
Biopsyconfirmsdiagnosis of
mucosalmelanoma
malignant
PRESENTATION WORKUP
•
•
•
••
H&P including complete head and neckexam; mirror and fiberoptic examinationas clinically indicatedVerification of pathology using appropriatestaining (HMB-45, S-100, Melan-A)CT and/or MRI to determine anatomicextent of disease, particularly for sinusdiseaseChest imaging as indicatedConsider PET-CT scan to rule outmetastatic disease
Sinus or nasal cavitymucosal melanoma
Oral cavity, oropharynx,larynx, or hypopharynxmucosal melanoma
See PrimaryTreatment (page 324)
PRIMARYTREATMENT
Stage III
T4a, N0
T3-T4a, N1
Stage IVB
Stage IVC
Wide surgical resection of primarya
ADJUVANTTREATMENT
Wide surgical resectiona Postoperative RTto primary siteb
Wide surgical resection+ neck dissection of positive necka
Postoperative RTto primary site andneckb
Strongly considerpostoperative RTto primary siteb
Clinical trial (preferred)orPrimary RTorSystemic therapy
b
c
Clinical trial (preferred)orBest supportive careorPrimary RTorSystemic therapy
b
c
Follow-up(see page 325)
Recurrent or Persistent disease(see the NCCN Clinical PracticeGuidelines in Oncology (NCCNGuidelines) for [cutaneous]Melanoma, elsewhere in this issueand online at www.NCCN.org)
aSee Principles of Surgery (pages 326-329).bc
See Principles of Radiation Therapy (page 330).See Systemic Therapy Options for Advanced or Metastatic Melanoma in the NCCN Clinical Practice Guidelines in Oncology
(NCCN Guidelines) for [cutaneous] Melanoma, elsewhere in this issue and online at www.NCCN.org.
NCCN Clinical Practice Guidelines in Oncology
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
323
Mucosal Melanoma of the Head and Neck Version 1.2012
Version 1.2012, 11-16-11 ©2012 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
Biopsyconfirmsdiagnosis of
mucosalmelanoma
malignant
PRESENTATION WORKUP
•
•
•
••
H&P including complete head and neckexam; mirror and fiberoptic examinationas clinically indicatedVerification of pathology using appropriatestaining (HMB-45, S-100, Melan-A)CT and/or MRI to determine anatomicextent of disease, particularly for sinusdiseaseChest imaging as indicatedConsider PET-CT scan to rule outmetastatic disease
Sinus or nasal cavitymucosal melanoma
Oral cavity, oropharynx,larynx, or hypopharynxmucosal melanoma
See PrimaryTreatment (page 324)
PRIMARYTREATMENT
Stage III
T4a, N0
T3-T4a, N1
Stage IVB
Stage IVC
Wide surgical resection of primarya
ADJUVANTTREATMENT
Wide surgical resectiona Postoperative RTto primary siteb
Wide surgical resection+ neck dissection of positive necka
Postoperative RTto primary site andneckb
Strongly considerpostoperative RTto primary siteb
Clinical trial (preferred)orPrimary RTorSystemic therapy
b
c
Clinical trial (preferred)orBest supportive careorPrimary RTorSystemic therapy
b
c
Follow-up(see page 325)
Recurrent or Persistent disease(see the NCCN Clinical PracticeGuidelines in Oncology (NCCNGuidelines) for [cutaneous]Melanoma, elsewhere in this issueand online at www.NCCN.org)
aSee Principles of Surgery (pages 326-329).bc
See Principles of Radiation Therapy (page 330).See Systemic Therapy Options for Advanced or Metastatic Melanoma in the NCCN Clinical Practice Guidelines in Oncology
(NCCN Guidelines) for [cutaneous] Melanoma, elsewhere in this issue and online at www.NCCN.org.

© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
324
Mucosal Melanoma of the Head and Neck Version 1.2012
Clinical trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. All recommendations are category 2A unless otherwise indicated.
PRIMARYTREATMENT
Stage III
Stage IVA
Stage IVB
Stage IVC
Wide surgical resection,elective neck dissectiona
ADJUVANTTREATMENT
Wide surgical resection+ neck dissectiona Postoperative RTb
Strongly considerpostoperative RTb
Clinical trial (preferred)orBest supportive careorPrimary RTorSystemic therapy
b
c
Oral cavity,oropharynx, larynx,or hypopharynxmucosal melanoma Clinical trial (preferred)
orPrimary RTand/orSystemic therapy
b
c
Follow-up(see page 325)
RecurrentorPersistentdisease
See NCCNGuidelines for
Melanoma,[cutaneous]
elsewhere inthis issue andonline atwww.NCCN.org
FOLLOW-UP
aSee Principles of Surgery (pages 326-329).bc
See Principles of Radiation Therapy (page 330).See Systemic Therapy Options for Advanced or Metastatic Melanoma the in NCCN Clinical Practice Guidelines in Oncology (NCCN
Guidelines) for [cutaneous] Melanoma, elsewhere in this issue and online at www.NCCN.org.
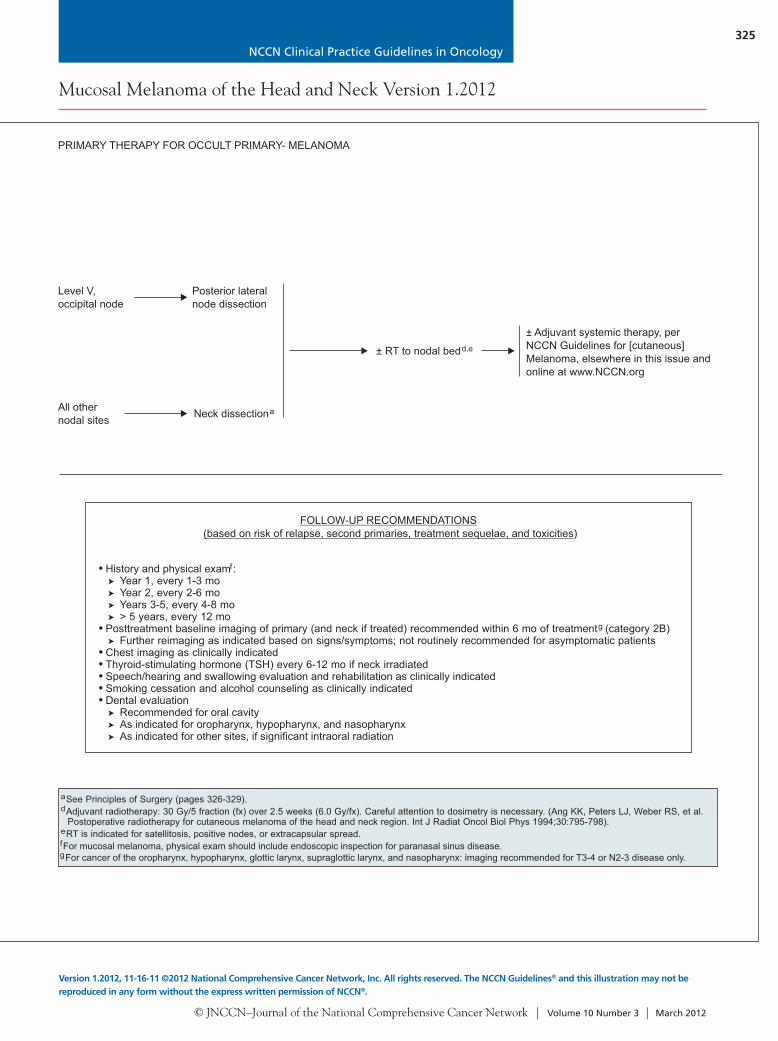
Level V,occipital node
All othernodal sites
Posterior lateralnode dissection
Neck dissectiona
± RT to nodal bedd,e
± Adjuvant systemic therapy, perNCCN Guidelines for [cutaneous]Melanoma, elsewhere in this issue andonline at www.NCCN.org
PRIMARY THERAPY FOR OCCULT PRIMARY- MELANOMA
aSee Principles of Surgery (pages 326-329).d
efg
Adjuvant radiotherapy: 30 Gy/5 fraction (fx) over 2.5 weeks (6.0 Gy/fx). Careful attention to dosimetry is necessary. (Ang KK, Peters LJ, Weber RS, et al.Postoperative radiotherapy for cutaneous melanoma of the head and neck region. Int J Radiat Oncol Biol Phys 1994;30:795-798).RT is indicated for satellitosis, positive nodes, or extracapsular spread.
For mucosal melanoma, physical exam should include endoscopic inspection for paranasal sinus disease.For cancer of the oropharynx, hypopharynx, glottic larynx, supraglottic larynx, and nasopharynx: imaging recommended for T3-4 or N2-3 disease only.
FOLLOW-UP RECOMMENDATIONS(based on risk of relapse, second primaries, treatment sequelae, and toxicities)
•
•
History and physical examYear 1, every 1-3 moYear 2, every 2-6 moYears 3-5, every 4-8 mo> 5 years, every 12 mo
Posttreatment baseline imaging of primary (and neck if treated) recommended within 6 mo of treatment (category 2B)Further reimaging as indicated based on signs/symptoms; not routinely recommended for asymptomatic patients
Chest imaging as clinically indicatedThyroid-stimulating hormone (TSH) every 6-12 mo if neck irradiatedSpeech/hearing and swallowing evaluation and rehabilitation as clinically indicatedSmoking cessation and alcohol counseling as clinically indicatedDental evaluation
f
g
➤
➤
➤
➤
➤
➤
➤
➤
•••••
Recommended for oral cavityAs indicated for oropharynx, hypopharynx, and nasopharynxAs indicated for other sites, if significant intraoral radiation
:
NCCN Clinical Practice Guidelines in Oncology
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
325
Mucosal Melanoma of the Head and Neck Version 1.2012
Version 1.2012, 11-16-11 ©2012 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
PRIMARYTREATMENT
Stage III
Stage IVA
Stage IVB
Stage IVC
Wide surgical resection,elective neck dissectiona
ADJUVANTTREATMENT
Wide surgical resection+ neck dissectiona Postoperative RTb
Strongly considerpostoperative RTb
Clinical trial (preferred)orBest supportive careorPrimary RTorSystemic therapy
b
c
Oral cavity,oropharynx, larynx,or hypopharynxmucosal melanoma Clinical trial (preferred)
orPrimary RTand/orSystemic therapy
b
c
Follow-up(see page 325)
RecurrentorPersistentdisease
See NCCNGuidelines for
Melanoma,[cutaneous]
elsewhere inthis issue andonline atwww.NCCN.org
FOLLOW-UP
aSee Principles of Surgery (pages 326-329).bc
See Principles of Radiation Therapy (page 330).See Systemic Therapy Options for Advanced or Metastatic Melanoma the in NCCN Clinical Practice Guidelines in Oncology (NCCN
Guidelines) for [cutaneous] Melanoma, elsewhere in this issue and online at www.NCCN.org.
Level V,occipital node
All othernodal sites
Posterior lateralnode dissection
Neck dissectiona
± RT to nodal bedd,e
± Adjuvant systemic therapy, perNCCN Guidelines for [cutaneous]Melanoma, elsewhere in this issue andonline at www.NCCN.org
PRIMARY THERAPY FOR OCCULT PRIMARY- MELANOMA
aSee Principles of Surgery (pages 326-329).d
efg
Adjuvant radiotherapy: 30 Gy/5 fraction (fx) over 2.5 weeks (6.0 Gy/fx). Careful attention to dosimetry is necessary. (Ang KK, Peters LJ, Weber RS, et al.Postoperative radiotherapy for cutaneous melanoma of the head and neck region. Int J Radiat Oncol Biol Phys 1994;30:795-798).RT is indicated for satellitosis, positive nodes, or extracapsular spread.
For mucosal melanoma, physical exam should include endoscopic inspection for paranasal sinus disease.For cancer of the oropharynx, hypopharynx, glottic larynx, supraglottic larynx, and nasopharynx: imaging recommended for T3-4 or N2-3 disease only.
FOLLOW-UP RECOMMENDATIONS(based on risk of relapse, second primaries, treatment sequelae, and toxicities)
•
•
History and physical examYear 1, every 1-3 moYear 2, every 2-6 moYears 3-5, every 4-8 mo> 5 years, every 12 mo
Posttreatment baseline imaging of primary (and neck if treated) recommended within 6 mo of treatment (category 2B)Further reimaging as indicated based on signs/symptoms; not routinely recommended for asymptomatic patients
Chest imaging as clinically indicatedThyroid-stimulating hormone (TSH) every 6-12 mo if neck irradiatedSpeech/hearing and swallowing evaluation and rehabilitation as clinically indicatedSmoking cessation and alcohol counseling as clinically indicatedDental evaluation
f
g
➤
➤
➤
➤
➤
➤
➤
➤
•••••
Recommended for oral cavityAs indicated for oropharynx, hypopharynx, and nasopharynxAs indicated for other sites, if significant intraoral radiation
:

© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
326
Mucosal Melanoma of the Head and Neck Version 1.2012
Clinical trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. All recommendations are category 2A unless otherwise indicated.
Evaluation
Integration of Therapy
Assessment of Resectability
All patients should be evaluated by a head and neck surgical oncologist before treatment to:Review the adequacy of biopsy material, review staging and imaging to determine the extent of disease, exclude thepresence of a synchronous primary tumor, assess current functional status, and evaluate for potential surgicalsalvage if initial treatment is nonsurgical.Participate in the multidisciplinary team discussions regarding patient treatment options with the goal of maximizingsurvival with preservation of form and function.Develop a prospective surveillance plan that includes adequate dental, nutritional, and health behavior evaluation andintervention and any other ancillary evaluations that would provide for comprehensive rehabilitation.Develop and design the surgical procedure, margins, and reconstructive plan to resect all gross tumor with adequatetumor-free surgical margins for . The surgical procedure should not be modified based onany response observed as a result of prior therapy except in instances of tumor progression that mandates a moreextensive procedure to encompass the tumor at the time of definitive resection.
It is critical that multidisciplinary evaluation and treatment be coordinated by all modalities involved in patient carebefore the initiation of any treatment.
Tumor involvement of the following sites is associated with poor prognosis or function or with T4b cancer(i.e., unresectable based on technical ability to obtain clear margins):
Involvement of the pterygoid muscles particularly when associated with severe trismus or pterygopalatine fossainvolvement with cranial neuropathyGross extension of tumor into the skull base (e.g., erosion of the pterygoid plates or sphenoid bone, widening of theforamen ovale)Direct extension to superior nasopharynx or deep extension into the eustachian tube and lateral nasopharyngeal wallsInvasion (encasement) of the common or internal carotid artery. Encasement is usually assessed radiographically anddefined as tumor surrounding the carotid artery 270°Direct extension of neck disease to involve the skinDirect extension to mediastinal structures, prevertebral fascia, or cervical vertebraePresence of subdermal metastases
1
1
11
patients undergoing surgery
PRINCIPLES OF SURGERY
Primary Tumor Resection
The resection of advanced tumors of the oral cavity, oropharynx, hypopharynx, larynx, or paranasal sinus willvary in extent depending on the structures involved. The primary tumor should be considered surgically curablethrough appropriate resection using accepted criteria for adequate excision, depending on the region involved.
En bloc resection of the primary tumor should be attempted whenever feasible.In continuity neck dissection is necessary when there is direct extension of the primary tumor into the neck.Surgical resection should be planned based on the extent of the primary tumor as ascertained by clinicalexamination and careful interpretation of appropriate radiographic images.For oral cavity cancers, as thickness of the lesion increases, so does the risk of regional metastases and theneed for adjuvant elective neck dissection.Perineural invasion should be suspected when tumors are adjacent to motor or sensory nerves. Wheninvasion is suspected, the nerve should be dissected both proximally and distally and should be resected toobtain clearance of disease. Frozen section determination of the proximal and distal nerve margins may provehelpful to facilitate tumor clearance.Partial or segmental resection of the mandible may be necessary to encompass adequately the cancer withadequate tumor-free margins. Adequate resection may require partial, horizontal, or sagittal resection of themandible for tumors involving or adherent to mandibular periosteum. Segmental resection should beconsidered in tumors that grossly involve mandibular periosteum (as determined by tumor fixation to themandible) or show evidence of direct tumor involvement of the bone at the time of operation or throughpreoperative imaging. The extent of mandibular resection will depend on the degree of involvement accessedclinically and in the operating room.For tumors of the larynx, the decision to perform either total laryngectomy or conservation laryngeal surgery(e.g., transoral resection, hemilaryngectomy, supraglottic laryngectomy) will be decided by the surgeon butshould adhere to the principles of complete tumor extirpation with curative intent.For maxillary sinus tumors, note that “Ohngren's line" runs from the medial canthus of the eye to the angle ofthe mandible, helping to define a plane passing through the maxillary sinus. Tumors "below" or "before" thisline involve the maxillary infrastructure. Those "above" or "behind" Ohngren's line involve the suprastructure.
PRINCIPLES OF SURGERY (Cont.)
1In selected cases, surgery might still be considered.

NCCN Clinical Practice Guidelines in Oncology
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
327
Mucosal Melanoma of the Head and Neck Version 1.2012
Version 1.2012, 11-16-11 ©2012 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
Evaluation
Integration of Therapy
Assessment of Resectability
All patients should be evaluated by a head and neck surgical oncologist before treatment to:Review the adequacy of biopsy material, review staging and imaging to determine the extent of disease, exclude thepresence of a synchronous primary tumor, assess current functional status, and evaluate for potential surgicalsalvage if initial treatment is nonsurgical.Participate in the multidisciplinary team discussions regarding patient treatment options with the goal of maximizingsurvival with preservation of form and function.Develop a prospective surveillance plan that includes adequate dental, nutritional, and health behavior evaluation andintervention and any other ancillary evaluations that would provide for comprehensive rehabilitation.Develop and design the surgical procedure, margins, and reconstructive plan to resect all gross tumor with adequatetumor-free surgical margins for . The surgical procedure should not be modified based onany response observed as a result of prior therapy except in instances of tumor progression that mandates a moreextensive procedure to encompass the tumor at the time of definitive resection.
It is critical that multidisciplinary evaluation and treatment be coordinated by all modalities involved in patient carebefore the initiation of any treatment.
Tumor involvement of the following sites is associated with poor prognosis or function or with T4b cancer(i.e., unresectable based on technical ability to obtain clear margins):
Involvement of the pterygoid muscles particularly when associated with severe trismus or pterygopalatine fossainvolvement with cranial neuropathyGross extension of tumor into the skull base (e.g., erosion of the pterygoid plates or sphenoid bone, widening of theforamen ovale)Direct extension to superior nasopharynx or deep extension into the eustachian tube and lateral nasopharyngeal wallsInvasion (encasement) of the common or internal carotid artery. Encasement is usually assessed radiographically anddefined as tumor surrounding the carotid artery 270°Direct extension of neck disease to involve the skinDirect extension to mediastinal structures, prevertebral fascia, or cervical vertebraePresence of subdermal metastases
1
1
11
patients undergoing surgery
PRINCIPLES OF SURGERY
Primary Tumor Resection
The resection of advanced tumors of the oral cavity, oropharynx, hypopharynx, larynx, or paranasal sinus willvary in extent depending on the structures involved. The primary tumor should be considered surgically curablethrough appropriate resection using accepted criteria for adequate excision, depending on the region involved.
En bloc resection of the primary tumor should be attempted whenever feasible.In continuity neck dissection is necessary when there is direct extension of the primary tumor into the neck.Surgical resection should be planned based on the extent of the primary tumor as ascertained by clinicalexamination and careful interpretation of appropriate radiographic images.For oral cavity cancers, as thickness of the lesion increases, so does the risk of regional metastases and theneed for adjuvant elective neck dissection.Perineural invasion should be suspected when tumors are adjacent to motor or sensory nerves. Wheninvasion is suspected, the nerve should be dissected both proximally and distally and should be resected toobtain clearance of disease. Frozen section determination of the proximal and distal nerve margins may provehelpful to facilitate tumor clearance.Partial or segmental resection of the mandible may be necessary to encompass adequately the cancer withadequate tumor-free margins. Adequate resection may require partial, horizontal, or sagittal resection of themandible for tumors involving or adherent to mandibular periosteum. Segmental resection should beconsidered in tumors that grossly involve mandibular periosteum (as determined by tumor fixation to themandible) or show evidence of direct tumor involvement of the bone at the time of operation or throughpreoperative imaging. The extent of mandibular resection will depend on the degree of involvement accessedclinically and in the operating room.For tumors of the larynx, the decision to perform either total laryngectomy or conservation laryngeal surgery(e.g., transoral resection, hemilaryngectomy, supraglottic laryngectomy) will be decided by the surgeon butshould adhere to the principles of complete tumor extirpation with curative intent.For maxillary sinus tumors, note that “Ohngren's line" runs from the medial canthus of the eye to the angle ofthe mandible, helping to define a plane passing through the maxillary sinus. Tumors "below" or "before" thisline involve the maxillary infrastructure. Those "above" or "behind" Ohngren's line involve the suprastructure.
PRINCIPLES OF SURGERY (Cont.)
1In selected cases, surgery might still be considered.

© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
328
Mucosal Melanoma of the Head and Neck Version 1.2012
Clinical trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. All recommendations are category 2A unless otherwise indicated.
Margins
Surgical Management of Cranial Nerves VII, X (Including the Recurrent Laryngeal Nerve), XI, and XII
Frozen section margin assessment is always at the discretion of the surgeon and should be considered when it will facilitatecomplete tumor removal. The achievement of adequate margins may require resection of an adjacent structure in the oral cavityor laryngopharynx (such as the base of tongue and/or anterior tongue, mandible, larynx, or portions of the cervical esophagus).
Adequate resection is defined as clear resection margins with at least enough clearance from gross tumor to obtain clearfrozen section and permanent margins (often 1.5-2 cm of visible and palpable normal mucosa). In general, frozen sectionexamination of the margins will usually be undertaken intraoperatively and, importantly, when a line of resection has uncertainclearance because of indistinct tumor margins or there is suspected residual disease (e.g., soft tissue, cartilage, carotid artery,or mucosal irregularity).The details of resection margins should be included in the operative dictation. The margins may be assessed on the resectedspecimen or alternatively from the surgical bed with proper orientation.A clear margin is defined as the distance from the invasive tumor front that is 5 mm from the resected margin.A close margin is defined as the distance from the invasive tumor front to the resected margin that is < 5 mm.The primary tumor should be marked in a fashion adequate for orientation by the surgical pathologist.The neck dissection should be oriented or sectioned to identify levels of lymph nodes encompassed in the dissection.Reconstruction of surgical defects should be performed using conventional techniques at the discretion of the surgeon.Primary closure is recommended when appropriate but should not be pursued at the expense of obtaining wide, tumor-freemargins. Reconstructive closure with local/regional flaps, free tissue transfer, or split-thickness skin or other grafts with orwithout mandibular reconstruction is performed at the discretion of the surgeon.
Operative management of the facial nerve and other major cranial nerves during primary or regional node resection is influencedby the preoperative clinical function of the nerve.
When the nerve is functioning, thorough efforts should be made to preserve the structure and function of the nerve (main trunkand/or branches) even if otherwise adequate tumor margins are not achieved—recognizing that the surgeon should leave nogross residual disease.Adjuvant postoperative radiation or chemoradiation is generally prescribed when microscopic residual or gross residual tumoris suspected.Direct nerve invasion by tumor and/or preoperative paralysis of the nerve may warrant segmental resection (and sometimesnerve grafting) at the discretion of the surgeon if tumor-free margins are assured throughout the remainder of the procedure.
Neck Management
Management of Recurrences
Surveillance
The surgical management of regional lymphatics is dictated by the extent of tumor at initial tumor staging. These guidelinesapply to the performance of neck dissections as part of treatment of the primary tumor. In general, patients undergoing surgeryfor resection of the primary tumor will undergo dissection of the ipsilateral side of the neck that is at greatest risk formetastases.
Tumor sites that frequently have bilateral lymphatic drainage (e.g., base of tongue, palate, supraglottic larynx, deep spacepre-epiglottic involvement) should often have both sides of the neck dissected with the extent of dissection determined assuggested below. For patients with tumors at or approaching the midline, both sides of the neck are at risk for metastases,and bilateral neck dissections should be performed. Elective neck dissection may not be recommended if postoperativeradiation is planned.
Patients with advanced lesions involving the anterior tongue or floor of mouth which approximate or cross the midline shouldundergo contralateral submandibular dissection as necessary to achieve adequate tumor resection.
Elective neck dissection should be based on risk of occult metastasis in the appropriate nodal basin.In general, elective neck dissections are not performed for mucosal melanoma, except for the oral cavity.In mucosal melanoma, no evidence shows that the depth of invasion predicts occult metastatic disease, although the risklikely does increase with increasing depth.
Elective dissections are generally selective, preserving all major structures, unless operative findings dictate otherwise.
Surgically resectable primary cancers should be re-resected with curative intent if feasible, and recurrences in a previouslytreated neck should also undergo surgical salvage. Neck disease in an untreated neck should be addressed by formal neckdissection or modification depending on the clinical situation. Nonsurgical therapy may also be used as clinically appropriate.
All patients should have regular follow-up visits to assess for symptoms and possible tumor recurrence, health behaviors,nutrition, dental health, and speech and swallowing function.
Tumor evaluations must be performed by specialists skilled in head and neck clinical examination.The frequency of evaluation is summarized in
➤
➤
Follow-up Recommendations (page 325).
PRINCIPLES OF SURGERY (Cont.)PRINCIPLES OF SURGERY (Cont.)

NCCN Clinical Practice Guidelines in Oncology
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
329
Mucosal Melanoma of the Head and Neck Version 1.2012
Version 1.2012, 11-16-11 ©2012 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
Margins
Surgical Management of Cranial Nerves VII, X (Including the Recurrent Laryngeal Nerve), XI, and XII
Frozen section margin assessment is always at the discretion of the surgeon and should be considered when it will facilitatecomplete tumor removal. The achievement of adequate margins may require resection of an adjacent structure in the oral cavityor laryngopharynx (such as the base of tongue and/or anterior tongue, mandible, larynx, or portions of the cervical esophagus).
Adequate resection is defined as clear resection margins with at least enough clearance from gross tumor to obtain clearfrozen section and permanent margins (often 1.5-2 cm of visible and palpable normal mucosa). In general, frozen sectionexamination of the margins will usually be undertaken intraoperatively and, importantly, when a line of resection has uncertainclearance because of indistinct tumor margins or there is suspected residual disease (e.g., soft tissue, cartilage, carotid artery,or mucosal irregularity).The details of resection margins should be included in the operative dictation. The margins may be assessed on the resectedspecimen or alternatively from the surgical bed with proper orientation.A clear margin is defined as the distance from the invasive tumor front that is 5 mm from the resected margin.A close margin is defined as the distance from the invasive tumor front to the resected margin that is < 5 mm.The primary tumor should be marked in a fashion adequate for orientation by the surgical pathologist.The neck dissection should be oriented or sectioned to identify levels of lymph nodes encompassed in the dissection.Reconstruction of surgical defects should be performed using conventional techniques at the discretion of the surgeon.Primary closure is recommended when appropriate but should not be pursued at the expense of obtaining wide, tumor-freemargins. Reconstructive closure with local/regional flaps, free tissue transfer, or split-thickness skin or other grafts with orwithout mandibular reconstruction is performed at the discretion of the surgeon.
Operative management of the facial nerve and other major cranial nerves during primary or regional node resection is influencedby the preoperative clinical function of the nerve.
When the nerve is functioning, thorough efforts should be made to preserve the structure and function of the nerve (main trunkand/or branches) even if otherwise adequate tumor margins are not achieved—recognizing that the surgeon should leave nogross residual disease.Adjuvant postoperative radiation or chemoradiation is generally prescribed when microscopic residual or gross residual tumoris suspected.Direct nerve invasion by tumor and/or preoperative paralysis of the nerve may warrant segmental resection (and sometimesnerve grafting) at the discretion of the surgeon if tumor-free margins are assured throughout the remainder of the procedure.
Neck Management
Management of Recurrences
Surveillance
The surgical management of regional lymphatics is dictated by the extent of tumor at initial tumor staging. These guidelinesapply to the performance of neck dissections as part of treatment of the primary tumor. In general, patients undergoing surgeryfor resection of the primary tumor will undergo dissection of the ipsilateral side of the neck that is at greatest risk formetastases.
Tumor sites that frequently have bilateral lymphatic drainage (e.g., base of tongue, palate, supraglottic larynx, deep spacepre-epiglottic involvement) should often have both sides of the neck dissected with the extent of dissection determined assuggested below. For patients with tumors at or approaching the midline, both sides of the neck are at risk for metastases,and bilateral neck dissections should be performed. Elective neck dissection may not be recommended if postoperativeradiation is planned.
Patients with advanced lesions involving the anterior tongue or floor of mouth which approximate or cross the midline shouldundergo contralateral submandibular dissection as necessary to achieve adequate tumor resection.
Elective neck dissection should be based on risk of occult metastasis in the appropriate nodal basin.In general, elective neck dissections are not performed for mucosal melanoma, except for the oral cavity.In mucosal melanoma, no evidence shows that the depth of invasion predicts occult metastatic disease, although the risklikely does increase with increasing depth.
Elective dissections are generally selective, preserving all major structures, unless operative findings dictate otherwise.
Surgically resectable primary cancers should be re-resected with curative intent if feasible, and recurrences in a previouslytreated neck should also undergo surgical salvage. Neck disease in an untreated neck should be addressed by formal neckdissection or modification depending on the clinical situation. Nonsurgical therapy may also be used as clinically appropriate.
All patients should have regular follow-up visits to assess for symptoms and possible tumor recurrence, health behaviors,nutrition, dental health, and speech and swallowing function.
Tumor evaluations must be performed by specialists skilled in head and neck clinical examination.The frequency of evaluation is summarized in
➤
➤
Follow-up Recommendations (page 325).
PRINCIPLES OF SURGERY (Cont.)PRINCIPLES OF SURGERY (Cont.)
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
330
Mucosal Melanoma of the Head and Neck Version 1.2012
Clinical trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. All recommendations are category 2A unless otherwise indicated.
Target delineation and optimal dose distribution require experience in head and neck imaging, and a thorough understanding ofpatterns of disease spread. Standards for target definition, dose specification, fractionation (with and without concurrentchemotherapy), and normal tissue constraints are still evolving. IMRT, 3D, and 2D conformal techniques may be used asappropriate depending on the stage, tumor location, physician training/experience, and available physics support. Close interplayexists between radiation technology, techniques, fractionation, and chemotherapy options, resulting in a large number ofcombinations that may impact toxicity or tumor control.
IMRT has been shown to be useful in reducing long-term toxicity in oropharyngeal, paranasal sinus, and nasopharyngeal cancersby reducing the dose to salivary glands, temporal lobes, auditory structures (including cochlea), and optic structures. Theapplication of IMRT to other sites (e.g., oral cavity, larynx, hypopharynx, salivary glands) is evolving and may be used at thediscretion of treating physicians.
Several ways exist to integrate IMRT, target volume dosing, and fractionation. The Simultaneous Integrated Boost (SIB) techniqueuses differential “dose painting” (66-74 Gy to gross disease; 50-60 Gy to subclinical disease) for each fraction of treatmentthroughout the entire course of radiation. SIB is commonly used in conventional (5 fractions/wk) and the “6 fractions/wkaccelerated” schedule. The sequential (SEQ) IMRT technique typically delivers the initial (lower-dose) phase (weeks 1-5) followedby the high-dose boost volume phase (weeks 6-7) using 2-3 separate dose plans, and is commonly applied in standardfractionation and hyperfractionation. The Concomitant Boost Accelerated schedule may use a “modified SEQ” dose plan bydelivering the dose to the subclinical targets once a day for 6 weeks, and a separate boost dose plan as a second daily fraction forthe last 12 treatment days.
Close cooperation and interdisciplinary management are critical totreatment planning and radiation targeting, especially in the postoperative setting or after induction chemotherapy.9
Intensity-Modulated Radiotherapy (IMRT)
IMRT and Fractionation10,11
45
6
RADIATION TECHNIQUES1-8
1
2
3
4
5
6
7
8
9
10
11
Dogan N, King S, Emami B, et al. Assessment of different IMRT boost delivery methods on target coverage and normal-tissue sparing. Int J Radiat OncolBiol Phys 2003;57:1480-1491.
Lee NY, de Arruda FF, Puri DR, et al. A comparison of intensity-modulated radiation therapy and concomitant boost radiotherapy in the setting ofconcurrent chemotherapy for locally advanced oropharyngeal carcinoma. Int J Radiat Oncol Biol Phys 2006;66:966-974.
Lee NY, O'Meara W, Chan K, et al. Concurrent chemotherapy and intensity-modulated radiotherapy for locoregionally advanced laryngeal andhypopharyngeal cancers. Int J Radiat Oncol Biol Phys 2007;69:459-468.
Mohan R, Wu Q, Morris M, et al. “Simultaneous Integrated Boost” (SIB) IMRT of advanced head and neck squamous cell carcinomas—dosimetricanalysis. Int J Radiat Oncol Biol Phys 2001;51:180–181.
Overgaard J, Hansen HS, Specht L, et al. Five compared with six fractions per week of conventional radiotherapy of squamous-cell carcinoma of headand neck: DAHANCA 6 and 7 randomised controlled trial. Lancet 2003;362:933-940.
Schoenfeld GO, Amdur RJ, Morris CG, et al. Patterns of failure and toxicity after intensity-modulated radiotherapy for head and neck cancer. Int J RadiatOncol Biol Phys 2008;71:377-385.
Wolden SL, Chen WC, Pfister DG, et al. Intensity-modulated radiation therapy (IMRT) for nasopharynx cancer: update of the Memorial Sloan-Ketteringexperience. Int J Radiat Oncol Biol Phys 2006;64:57-62.
Wu Q, Manning M, Schmidt-Ullrich R, Mohan R. The potential for sparing of parotids and escalation of biologically effective dose with intensity-modulated radiation treatments of head and neck cancers: a treatment design study. Int J Radiat Oncol Biol Phys 2000;46:195-205.
Salama JK, Haddad RI, Kies MS, et al. Clinical practice recommendations for radiotherapy planning following induction chemotherapy in locoregionallyadvanced head and neck cancer. Int J Radiat Oncol Biol Phys 2009;75:725-733.Hartford AC, Palisca MG, Eichler TJ, et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology(ACR) practice guidelines for intensity-modulated radiation therapy (IMRT). Int J Radiat Oncol Biol Phys. 2009;73:9-14.IMRT Documentation Working Group, Holmes T, Das R, Low D, et al. American Society of Radiation Oncology recommendations for documentingintensity-modulated radiation therapy treatments. Int J Radiat Oncol Biol Phys 2009;74:1311-1318.
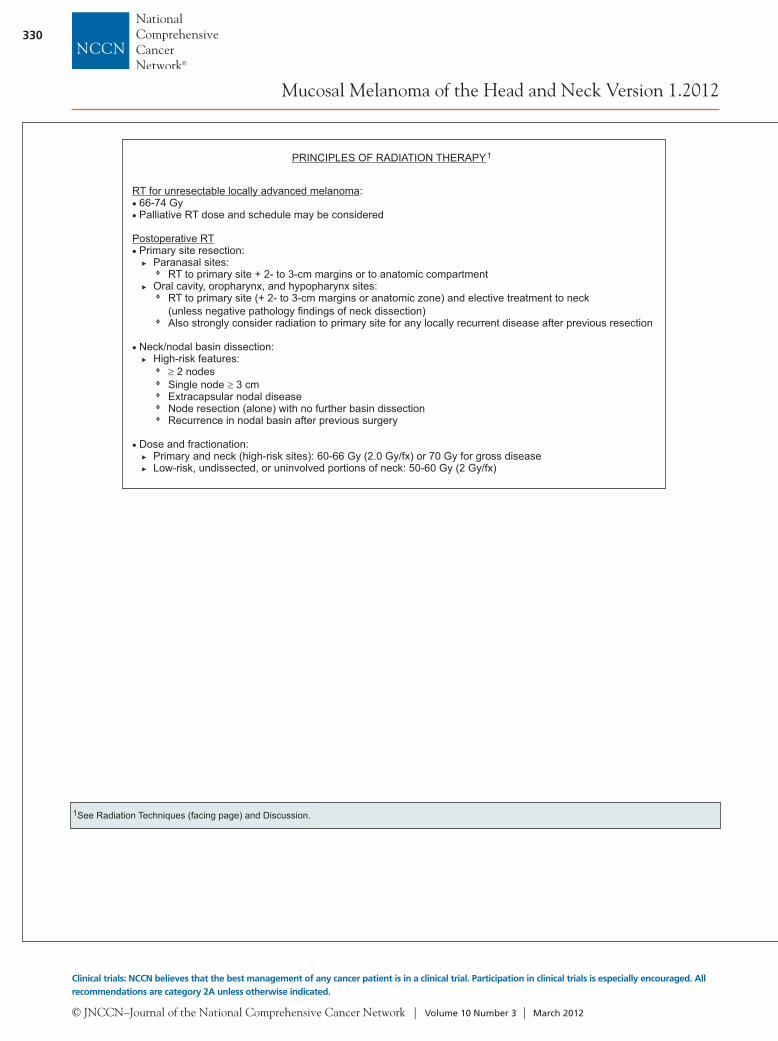
RT for unresectable locally advanced melanoma:66-74 GyPalliative RT dose and schedule may be considered
resection
Postoperative RTPrimary site resection:
Paranasal sites:RT to primary site + 2- to 3-cm margins or to anatomic compartment
Oral cavity, oropharynx, and hypopharynx sites:RT to primary site (+ 2- to 3-cm margins or anatomic zone) and elective treatment to neck(unless negative pathology findings of neck dissection)Also strongly consider radiation to primary site for any locally recurrent disease after previous resection
Neck/nodal basin dissection:High-risk features:
2 nodesSingle node 3 cmExtracapsular nodal diseaseNode (alone) with no further basin dissectionRecurrence in nodal basin after previous surgery
Dose and fractionation:Primary and neck (high-risk sites): 60-66 Gy (2.0 Gy/fx) or 70 Gy for gross diseaseLow-risk, undissected, or uninvolved portions of neck: 50-60 Gy (2 Gy/fx)
PRINCIPLES OF RADIATION THERAPY1
1See Radiation Techniques (facing page) and Discussion.

NCCN Clinical Practice Guidelines in Oncology
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
331
Mucosal Melanoma of the Head and Neck Version 1.2012
Version 1.2012, 11-16-11 ©2012 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
Target delineation and optimal dose distribution require experience in head and neck imaging, and a thorough understanding ofpatterns of disease spread. Standards for target definition, dose specification, fractionation (with and without concurrentchemotherapy), and normal tissue constraints are still evolving. IMRT, 3D, and 2D conformal techniques may be used asappropriate depending on the stage, tumor location, physician training/experience, and available physics support. Close interplayexists between radiation technology, techniques, fractionation, and chemotherapy options, resulting in a large number ofcombinations that may impact toxicity or tumor control.
IMRT has been shown to be useful in reducing long-term toxicity in oropharyngeal, paranasal sinus, and nasopharyngeal cancersby reducing the dose to salivary glands, temporal lobes, auditory structures (including cochlea), and optic structures. Theapplication of IMRT to other sites (e.g., oral cavity, larynx, hypopharynx, salivary glands) is evolving and may be used at thediscretion of treating physicians.
Several ways exist to integrate IMRT, target volume dosing, and fractionation. The Simultaneous Integrated Boost (SIB) techniqueuses differential “dose painting” (66-74 Gy to gross disease; 50-60 Gy to subclinical disease) for each fraction of treatmentthroughout the entire course of radiation. SIB is commonly used in conventional (5 fractions/wk) and the “6 fractions/wkaccelerated” schedule. The sequential (SEQ) IMRT technique typically delivers the initial (lower-dose) phase (weeks 1-5) followedby the high-dose boost volume phase (weeks 6-7) using 2-3 separate dose plans, and is commonly applied in standardfractionation and hyperfractionation. The Concomitant Boost Accelerated schedule may use a “modified SEQ” dose plan bydelivering the dose to the subclinical targets once a day for 6 weeks, and a separate boost dose plan as a second daily fraction forthe last 12 treatment days.
Close cooperation and interdisciplinary management are critical totreatment planning and radiation targeting, especially in the postoperative setting or after induction chemotherapy.9
Intensity-Modulated Radiotherapy (IMRT)
IMRT and Fractionation10,11
45
6
RADIATION TECHNIQUES1-8
1
2
3
4
5
6
7
8
9
10
11
Dogan N, King S, Emami B, et al. Assessment of different IMRT boost delivery methods on target coverage and normal-tissue sparing. Int J Radiat OncolBiol Phys 2003;57:1480-1491.
Lee NY, de Arruda FF, Puri DR, et al. A comparison of intensity-modulated radiation therapy and concomitant boost radiotherapy in the setting ofconcurrent chemotherapy for locally advanced oropharyngeal carcinoma. Int J Radiat Oncol Biol Phys 2006;66:966-974.
Lee NY, O'Meara W, Chan K, et al. Concurrent chemotherapy and intensity-modulated radiotherapy for locoregionally advanced laryngeal andhypopharyngeal cancers. Int J Radiat Oncol Biol Phys 2007;69:459-468.
Mohan R, Wu Q, Morris M, et al. “Simultaneous Integrated Boost” (SIB) IMRT of advanced head and neck squamous cell carcinomas—dosimetricanalysis. Int J Radiat Oncol Biol Phys 2001;51:180–181.
Overgaard J, Hansen HS, Specht L, et al. Five compared with six fractions per week of conventional radiotherapy of squamous-cell carcinoma of headand neck: DAHANCA 6 and 7 randomised controlled trial. Lancet 2003;362:933-940.
Schoenfeld GO, Amdur RJ, Morris CG, et al. Patterns of failure and toxicity after intensity-modulated radiotherapy for head and neck cancer. Int J RadiatOncol Biol Phys 2008;71:377-385.
Wolden SL, Chen WC, Pfister DG, et al. Intensity-modulated radiation therapy (IMRT) for nasopharynx cancer: update of the Memorial Sloan-Ketteringexperience. Int J Radiat Oncol Biol Phys 2006;64:57-62.
Wu Q, Manning M, Schmidt-Ullrich R, Mohan R. The potential for sparing of parotids and escalation of biologically effective dose with intensity-modulated radiation treatments of head and neck cancers: a treatment design study. Int J Radiat Oncol Biol Phys 2000;46:195-205.
Salama JK, Haddad RI, Kies MS, et al. Clinical practice recommendations for radiotherapy planning following induction chemotherapy in locoregionallyadvanced head and neck cancer. Int J Radiat Oncol Biol Phys 2009;75:725-733.Hartford AC, Palisca MG, Eichler TJ, et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology(ACR) practice guidelines for intensity-modulated radiation therapy (IMRT). Int J Radiat Oncol Biol Phys. 2009;73:9-14.IMRT Documentation Working Group, Holmes T, Das R, Low D, et al. American Society of Radiation Oncology recommendations for documentingintensity-modulated radiation therapy treatments. Int J Radiat Oncol Biol Phys 2009;74:1311-1318.
RT for unresectable locally advanced melanoma:66-74 GyPalliative RT dose and schedule may be considered
resection
Postoperative RTPrimary site resection:
Paranasal sites:RT to primary site + 2- to 3-cm margins or to anatomic compartment
Oral cavity, oropharynx, and hypopharynx sites:RT to primary site (+ 2- to 3-cm margins or anatomic zone) and elective treatment to neck(unless negative pathology findings of neck dissection)Also strongly consider radiation to primary site for any locally recurrent disease after previous resection
Neck/nodal basin dissection:High-risk features:
2 nodesSingle node 3 cmExtracapsular nodal diseaseNode (alone) with no further basin dissectionRecurrence in nodal basin after previous surgery
Dose and fractionation:Primary and neck (high-risk sites): 60-66 Gy (2.0 Gy/fx) or 70 Gy for gross diseaseLow-risk, undissected, or uninvolved portions of neck: 50-60 Gy (2 Gy/fx)
PRINCIPLES OF RADIATION THERAPY1
1See Radiation Techniques (facing page) and Discussion.

NCCN Clinical Practice Guidelines in Oncology
Mucosal Melanoma of the Head and Neck
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
332
Text continued from p. 321
chemotherapy (e.g., pain, xerostomia, speech and swallowing problems, depression) require profes-sionals familiar with the disease. Follow-up for these sequelae should include a comprehensive H&N ex-amination. Adequate nutritional support can help to prevent severe weight loss in patients undergoing treatment for MM; therefore, patients should be en-couraged to see a dietician.5
Patients should also be encouraged to stop smok-ing and to modify alcohol consumption if excessive, because these habits may decrease the efficacy of treat-ment and adversely affect other health outcomes.6,7 Programs using behavioral counseling combined with medications that promote smoking cessation (ap-proved by the FDA) can be very useful (http://www.ahrq.gov/clinic/tobacco/tobaqrg.htm). Specific com-ponents of patient support and follow-up are listed in the algorithm (see Team Approach, in the NCCN Guidelines for H&N Cancers, available online at www.NCCN.org [TEAM-1]). Notably, patients with MM require timely diagnosis and management of de-pression. The H&N Cancers Panel also recommends referring to the NCCN Guidelines for Palliative Care (to view the most recent version of these guidelines, visit the NCCN Web site at www.NCCN.org).
Comorbidity and Quality of Life
ComorbidityComorbidity refers to the presence of concomitant disease (in addition to MM) that may affect the diag-nosis, treatment, and prognosis of the patient.8–10 Doc-umentation of comorbidity is particularly important in oncology to facilitate optimal treatment selection and estimates of prognosis. Comorbidity is known to be a strong independent predictor of mortality in patients with H&N cancer,10–17 and comorbidity also influences costs of care, use of treatment, and quality of life.18–20 Traditional indices of comorbidity include the Charlson index9 and the Kaplan-Feinstein index and its modifications.10,21 The Adult Comorbidity Evaluation-27 (ACE-27) is specific for H&N cancer and has excellent emerging reliability and validity.22,23
Quality of LifeHealth-related quality-of-life issues are paramount in H&N cancer and MM. These tumors affect basic physiologic functions (e.g., ability to chew, swallow, and breathe), the senses (e.g., taste, smell, hearing), and uniquely human characteristics (e.g., appear-ance, voice). Health status describes an individual’s physical, emotional, and social capabilities and limi-tations. Function and performance refer to how well an individual is able to perform important roles, tasks, or activities. The definition of quality of life differs, because the central focus is on the value (determined by the patient alone) that individuals place on their health status and function.24
Mucosal Melanoma of the Head and Neck MM of the H&N is a rare but highly aggressive neo-plasm with a poor prognosis. It may occur throughout the upper aerodigestive tract. Most MM of the H&N (~70%) occurs in the nasal cavity or paranasal sinus re-gion, and approximately 25% develops in the oral cav-ity (see Figure 2).4,25 The remainder develops in other sites (e.g., oropharynx, hypopharynx, larynx). Sinonasal MM is typically confined to the primary site at presen-tation, and patients often present with symptoms (e.g., nasal obstruction).2,26 Oral cavity MM more frequently presents with clinically apparent lymph node metastasis and is often asymptomatic.27 No etiologic risk factors are yet apparent. MM occurs in a greater extent in Asians and less frequently in the Western population.28
Oral cavity
LipBuccal mucosaAlveolar ridge and retromolar trigoneFloor of mouthHard palateOral tongue (anterior) two-thirds)
LarynxSupraglottis False cords Arytenoids Epiglottis Arytenoepiglottic foldGlottisSubgliottis
Nasal antrum
NasopharynxPharynx
Esophagus
Hypopharynx
Oropharynx Base of tongue Soft palate Tonsillar pillar and fossa
Figure 1 Anatomic sites and subsites of the head and neck. Reprinted with permission, from CMP Healthcare Media. Source: Cancer Management: A Multidisciplinary Approach, 9th ed. Pazdur R, Coia L, Hoskins W, et al. (eds), Chapter 4. Copyright 2005, All rights reserved.

NCCN Clinical Practice Guidelines in Oncology
Mucosal Melanoma of the Head and Neck
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
333
Workup and StagingDiagnosis of MM of the H&N can be difficult. The differential diagnosis of sinonasal MM includes lym-phoma, sarcoma, and olfactory neuroblastoma.29 Ide-ally, a combination of histology, immunohistochem-istry, and clinical features is used for diagnosis. MM is immunoreactive for S-100 and HMB-45 (and to a lesser extent for melan-A); however, MM is negative for cytokeratin.2,29
Workup for MM should include clinical ex-amination and CT and/or MRI for paranasal sinus disease, and appropriate imaging for other mucosal sites. The physical examination should include en-doscopic inspection for paranasal sinus disease. PET/CT scanning may be considered to define the pres-ence of distant disease in more advanced situations.
The AJCC Staging Manual (7th edition) in-cludes a staging system for MM (see Table 6 in the NCCN Guidelines for H&N, available online, at www.NCCN.org [ST-11])4; previous editions did not have a classification for MM. The AJCC staging rec-ognizes 2 key factors specific to MM: 1) the disease still has a poor prognosis even with a limited primary burden of disease, and 2) there is still some grada-tion of survival based on the burden of disease, as reflected in local, regional, and distant extent.
Thus, the AJCC staging system for MM begins with stage III disease as the most limited form of disease (similar to anaplastic thyroid carcinoma), and breaks the disease down into stages reflecting local burden of disease and regional and distant extent. Melanomas confined to the mucosa only are T3, those with moderately advanced lesions (involving underlying cartilage or bone) are T4a, and very advanced primary tumors are T4b. In ad-dition, the AJCC staging system reflects the fact that MM occurs at all mucosal sites in the H&N. Therefore, rules for classifying and staging, and surgical principles should be based on the ap-propriate anatomic site of origin (see the NCCN Guidelines for H&N Cancers, available online, at www.NCCN.org).
Treatment of the PrimaryAlthough limited data are available on treatment options, surgery is the primary treatment for MM stage III through IVA (see Principles of Surgery on pages 326–329 and in the NCCN Guidelines for H&N Cancers, available online at www.NCCN.org [SURG-A]).30 However, surgery is not recommended
for stage IVB or IVC disease.31 The panel strongly en-courages clinical trials for all patients with MM to better define treatment choices at all stages of disease.
In most case series, adjuvant RT seems effec-tive in improving local control and survival.32 RT is clearly indicated in more advanced cases as an adjunct to surgery (see the Principles of Radiation Therapy on page 330 and in the NCCN Guidelines for H&N Cancers, available online at www.NCCN.org [RAD-A]).33 The role of radiation in stage III dis-ease is not clear, but it can be considered and should be determined on an individual basis by the treat-ing clinicians. However, survival rates after surgery alone or surgery combined with radiation are better than those after radiation alone.30
Treatment of the Neck Neck dissection and postoperative radiation are rec-ommended for clinical nodal disease.34,35 The role of elective neck treatment is unclear.36 The extension of elective treatment to the neck seems unwarranted in most cases of N0 paranasal sinus MM. However, for oral cavity disease, the likelihood of positive dis-ease is significantly higher and the treatment can be better localized to the ipsilateral neck with both
II
III
I
IV
V
Figure 2 Level designation for cervical lymphatics in the right neck. Reprinted with permission, from CMP Healthcare Media. Source: Cancer Management: A Multidisciplinary Approach, 9th ed. Pazdur R, Coia L, Hoskins W, et al. (eds), Chapter 4. Copyright 2005, All rights reserved.

NCCN Clinical Practice Guidelines in Oncology
Mucosal Melanoma of the Head and Neck
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
334
surgery and radiation (see Principles of Surgery on pages 326–329 and in the NCCN Guidelines for H&N Cancers, available online at www.NCCN.org [SURG-A]). Therefore, elective treatment to the neck for oral cavity MM seems justifiable.
Radiation Therapy Prospective trials evaluating the role of RT in MM are lacking. However, recently reported results of a randomized trial in cutaneous melanoma are con-sidered relevant to MM in the postoperative setting after neck dissection.37 Retrospective studies in MM have shown local recurrence to be common after sur-gery alone.30,38,39 After using postoperative radiation, lower rates of local and neck recurrence have been seen in historical comparison series.32,40 Reasonable local control outcomes using RT alone in unresect-able or medically inoperable cases have been report-ed in small cohort series of MMs.30,41–44
RT is often recommended in the postoperative management of MMs. Primary size or thickness is not used as a risk factor when considering RT to the primary site; all invasive primaries are considered at high risk for local recurrence. For sinonasal primary sites, target volumes may include the primary site without elective treatment of the neck. Because oral cavity primary sites are believed to be at a higher risk for failure in the neck, elective management with neck dissection and RT may be applied.
Indications for postoperative radiation to the neck are generally extrapolated from cutaneous mel-anoma. Recently, an Australian-New Zealand con-sortium reported on a randomized trial (N = 250) of postoperative RT versus observation in patients with palpable adenopathy from cutaneous primaries. Post-operative RT was associated with a significant reduc-tion in relapse in the nodal basin (19% vs. 31%) and a significant improvement in lymph node field con-trol.37 Only 20 patients experienced disease relapse who underwent postoperative RT, compared with 34 patients who underwent observation only (P = .04).
Considering this trial and retrospective studies in MM, the panel recommends postoperative RT for the following high-risk features: extracapsular disease, in-volvement of 2 or more neck or intraparotid nodes, any node 3 cm or greater, neck excision (alone) with no further basin dissection, or recurrence in the neck or soft tissue after initial surgical resection.45,46 Con-ventional fractionation is recommended (at 2 Gy per fraction to a total postoperative dose of 60–66 Gy, or
to 70 Gy for gross disease). Although the Australian-New Zealand randomized trial used 48 Gy in 20 frac-tions (240 cGy per fraction) to neck, axilla, or groin,37 the NCCN H&N Cancers Panel prefers conventional fractionation to somewhat higher total doses (60–66 Gy) in the neck because of concerns about late effects from larger dose per fraction, which may not be fully expressed for many years after treatment.
Intensity modulated RT may be very helpful for achieving homogenous dose distributions and spar-ing of critical organs, especially in paranasal sinus sites (see Radiation Techniques on page 331).47–49 Good outcomes have been reported with the use of hypofractionation in cutaneous melanomas, which has the advantage of convenience but no clear ad-vantage in cancer control. There is little experience using large dose per fraction in mucosal sites. Be-cause of the proximity of neural structures and risk of late effects, hypofractionation (if used) must be carefully planned and delivered.
Systemic TherapySystemic therapy used for cutaneous melanoma (e.g., interleukin-2) is recommended for MM (see Sys-temic Therapy Options for Advanced or Metastatic Melanoma in the NCCN Guidelines for Melanoma, available in this issue on pages 378–380 and online at www.NCCN.org [ME-E]). Interferon and interleukin have been used to treat MM.50 Data suggest that c-KIT inhibitors (e.g., imatinib) may be useful in patients with metastatic MM who have specific c-KIT muta-tions (i.e., exon 11 or 13 mutations).28,51 Therefore, imatinib is reasonable to use in patients with MM who have c-KIT mutations.52 Although vemurafenib is recommended for patients with cutaneous melano-ma who have the V600E mutation of the BRAF gene, patients with MM rarely have this BRAF mutation.51
Follow-Up Recommendations for surveillance are provided in the algorithm (see Follow-Up Recommendations on page 325). Note that physical examination should include endoscopic inspection for paranasal sinus dis-ease. Salvage surgery may be useful for patients with MM; therefore, surveillance is important.30
Recurrent or Persistent DiseaseFor patients with MM who have recurrent or persistent disease, the NCCN H&N Cancers Panel recommends using the NCCN Guidelines for Melanoma (available in this issue and online at www.NCCN.org).

NCCN Clinical Practice Guidelines in Oncology
Mucosal Melanoma of the Head and Neck
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
335
Principles of SurgeryAll patients should be evaluated by an H&N surgical oncologist before being treated for MM. In addition, multidisciplinary evaluation and treatment must be well coordinated. Many surgical principles de-scribed in the NCCN Guidelines for H&N Cancers algorithm are applicable to MM (i.e., evaluation, integration of therapy, assessment of resectability, primary tumor resection, margins, management of recurrences, and surveillance; see Principles of Sur-gery on pages 326–329 and in the NCCN Guidelines for H&N Cancers, available online at www.NCCN.org [SURG-A]).3,53 Resectable disease, neck dissec-tion, and salvage surgery of high-risk disease are dis-cussed in the following sections.
Resectable Versus Unresectable DiseaseThe term unresectable has resisted formal definition by H&N cancer specialists. The experience of the surgeon and the support available from reconstruc-tive surgeons, physiatrists, and prosthodontists of-ten strongly influence recommendations, especially in institutions in which only a few patients with MM are treated. The NCCN Member Institutions have teams experienced in the treatment of H&N cancer and maintain the multidisciplinary infra-structure needed for reconstruction and rehabilita-tion. A patient’s cancer is deemed unresectable if H&N surgeons at NCCN Member Institutions do not think they can remove all gross tumor on ana-tomic grounds or if they are certain local control will not be achieved after surgery (even with the addition of RT to the treatment approach). Typi-cally, these unresectable tumors densely involve the cervical vertebrae, brachial plexus, deep muscles of the neck, or carotid artery (see Principles of Surgery on pages 326–329 and in the NCCN Guidelines for H&N Cancers, available online at www.NCCN.org [SURG-A]). Tumor involvement of certain sites is associated with poor prognosis (e.g., direct extension of neck disease to involve the external skin or to me-diastinal structures, prevertebral fascia, or cervical vertebrae).
Unresectable tumors (i.e., those that cannot be removed without causing unacceptable morbidity) should be distinguished from inoperable tumors in patients whose constitutional state precludes an op-eration (even if the cancer could be readily resected with few sequelae). Additionally, a subgroup of pa-
tients will refuse surgical management, but these tu-mors should not be deemed unresectable. Although local and regional disease may be surgically treatable, patients with distant metastases are usually treated as though the primary tumor was unresectable. This is balanced by the potential to mitigate suffering from local and regional disease. This may be particularly true in MM. Thus, patient choice or a physician’s expectations regarding cure and morbidity will influ-ence or determine treatment.
Neck DissectionHistorically, cervical lymph node (i.e., neck) dissec-tions have been classified as radical or modified radi-cal procedures. The less-radical procedures preserve the sternocleidomastoid muscle, jugular vein, spi-nal accessory nerve, or selective lymph node levels. The NCCN H&N Cancers Panel prefers to classify cervical lymphadenectomy using contemporary no-menclature, thus classifying cervical lymph node dis-sections as either comprehensive or selective.54 A com-prehensive neck dissection is one that removes all lymph node groups that would be included in a clas-sic radical neck dissection. Whether the sternoclei-domastoid muscle, jugular vein, or spinal accessory nerve is preserved does not affect whether the dis-section is classified as comprehensive. Depending on the site, comprehensive neck dissection is often rec-ommended for patients with positive nodal disease MM (see Neck Management in Principles of Surgery on pages 326–329 and in the NCCN Guidelines for H&N Cancers, available online at www.NCCN.org [SURG-A]). In general, elective neck dissections for melanoma are not performed, except for oral cavity. Currently, elective treatment of the neck tends to be reserved for when access to vessels is needed for microvascular anastomosis for free flaps and perhaps in oral cavity primary MM.
For a therapeutic dissection, whether the neck can be made more selective will depend on the pri-mary location of the tumor. Level I disease may be cleared with a selective neck dissection encompass-ing levels I through IV, and pharyngeal disease may not require a level I dissection.55,56 For example, to remove the nodes most commonly involved with metastases from the oral cavity, a selective neck dis-section is recommended, which includes the nodes found above the omohyoid muscle (levels I–III and sometimes the superior parts of level V).54,57 Simi-larly, to remove the nodes most commonly involved

NCCN Clinical Practice Guidelines in Oncology
Mucosal Melanoma of the Head and Neck
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
336
with metastases from the pharynx and larynx, a se-lective neck dissection is recommended, which in-cludes the nodes in levels II through IV and level VI when appropriate.54 Selective neck dissections may be used as treatment when neck tumor burden is low.55,56
Salvage Surgery Salvage surgery may be useful for patients with MM; therefore, surveillance is important.30 However, the NCCN H&N Cancers Panel emphasized the in-creased risk of complications when salvage surgery is attempted. Some of these patients may require microvascular free flap reconstruction to cover the defects at the primary site. The patients undergoing neck dissection may develop complications related to delayed wound healing, skin necrosis, or carotid exposure.
References 1. McLaughlin CC, Wu XC, Jemal A, et al. Incidence of noncutaneous
melanomas in the U.S. Cancer 2005;103:1000–1007. 2. McLean N, Tighiouart M, Muller S. Primary mucosal melanoma
of the head and neck. Comparison of clinical presentation and histopathologic features of oral and sinonasal melanoma. Oral Oncol 2008;44:1039–1046.
3. Mendenhall WM, Werning JW, Pfister DG. Treatment of head and neck cancer. In: DeVita Jr. VT, Lawrence TS, Rosenberg SA, eds. DeVita, Hellman, and Rosenberg’s Cancer: Principles and Practice of Oncology. Philadelphia: Lippincott Williams & Wilkins; 2011:809–877.
4. Edge S, Byrd D, Compton C, et al. AJCC Cancer Staging Manual, 7th ed. New York: Springer; 2010.
5. Colasanto JM, Prasad P, Nash MA, et al. Nutritional support of patients undergoing radiation therapy for head and neck cancer. Oncology (Williston Park) 2005;19:371–379.
6. Schnoll RA, Zhang B, Rue M, et al. Brief physician-initiated quit-smoking strategies for clinical oncology settings: a trial coordinated by the Eastern Cooperative Oncology Group. J Clin Oncol 2003;21:355–365.
7. Gritz ER, Carr CR, Rapkin D, et al. Predictors of long-term smoking cessation in head and neck cancer patients. Cancer Epidemiol Biomarkers Prev 1993;2:261–270.
8. Feinstein AR. The pre-therapeutic classification of co-morbidity in chronic disease. J Chron Dis 1970;23:455–468.
9. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373–383.
10. Piccirillo JF. Importance of comorbidity in head and neck cancer. Laryngoscope 2000;110:593–602.
11. Piccirillo JF, Lacy PD, Basu A, Spitznagel EL. Development of a new head and neck cancer-specific comorbidity index. Arch Otolaryngol Head Neck Surg 2002;128:1172–1179.
12. Piccirillo JF. Impact of comorbidity and symptoms on the prognosis of patients with oral carcinoma. Arch Otolaryngol Head Neck Surg
2000;126:1086–1088.13. Chen AY, Matson LK, Roberts D, Goepfert H. The significance
of comorbidity in advanced laryngeal cancer. Head Neck 2001;23:566–572.
14. Singh B, Bhaya M, Stern J, et al. Validation of the Charlson comorbidity index in patients with head and neck cancer: a multi-institutional study. Laryngoscope 1997;107:1469–1475.
15. Hall SF, Rochon PA, Streiner DL, et al. Measuring comorbidity in patients with head and neck cancer. Laryngoscope 2002;112:1988–1996.
16. Hall SF, Groome PA, Rothwell D. The impact of comorbidity on the survival of patients with squamous cell carcinoma of the head and neck. Head Neck 2000;22:317–322.
17. Ribeiro KC, Kowalski LP, Latorre MR. Impact of comorbidity, symptoms, and patients’ characteristics on the prognosis of oral carcinomas. Arch Otolaryngol Head Neck Surg 2000;126:1079–1085.
18. de Graeff A, de Leeuw JR, Ros WJ, et al. Pretreatment factors predicting quality of life after treatment for head and neck cancer. Head Neck 2000;22:398–407.
19. Funk GF, Karnell LH, Whitehead S, et al. Free tissue transfer versus pedicled flap cost in head and neck cancer. Otolaryngol Head Neck Surg 2002;127:205–212.
20. Farwell DG, Reilly DF, Weymuller EA, et al. Predictors of perioperative complications in head and neck patients. Arch Otolaryngol Head Neck Surg 2002;128:505–511.
21. Kaplan MH, Feinstein AR. The importance of classifying initial co-morbidity in evaluatin the outcome of diabetes mellitus. J Chronic Dis 1974;27:387–404.
22. Bang D, Piccirillo J, Littenberg B, et al. The Adult Comorbidity Evaluation-27 (ACE-27) test: a new comorbidity index for patients with cancer [abstract]. J Clin Oncol 2000;19(Suppl):Abstract 1701.
23. Piccirillo JF, Costas I, Claybour P, et al. The measurement of comorbidity by cancer registries. Journal of Registry Management 2003;30:8–14.
24. Patrick D, Erickson P. Health Status and Health Policy: Quality of Life in Health Care Evaluation and Resource Allocation. New York: Oxford University Press; 1993.
25. Bachar G, Loh KS, O’Sullivan B, et al. Mucosal melanomas of the head and neck: experience of the Princess Margaret Hospital. Head Neck 2008;30:1325–1331.
26. Teppo H, Kervinen J, Koivunen P, Alho OP. Incidence and outcome of head and neck mucosal melanoma--a population-based survey from Northern Finland. Int J Circumpolar Health 2006;65:443–447.
27. Patel SG, Prasad ML, Escrig M, et al. Primary mucosal malignant melanoma of the head and neck. Head Neck 2002;24:247–257.
28. Guo J, Si L, Kong Y, et al. Phase II, open-label, single-arm trial of imatinib mesylate in patients with metastatic melanoma harboring c-Kit mutation or amplification. J Clin Oncol 2011;29:2904–2909.
29. Thompson LD, Wieneke JA, Miettinen M. Sinonasal tract and nasopharyngeal melanomas: a clinicopathologic study of 115 cases with a proposed staging system. Am J Surg Pathol 2003;27:594–611.
30. Dauer EH, Lewis JE, Rohlinger AL, et al. Sinonasal melanoma: a clinicopathologic review of 61 cases. Otolaryngol Head Neck Surg 2008;138:347–352.
31. Meleti M, Leemans CR, de Bree R, et al. Head and neck mucosal melanoma: experience with 42 patients, with emphasis on the role

NCCN Clinical Practice Guidelines in Oncology
Mucosal Melanoma of the Head and Neck
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
337
of postoperative radiotherapy. Head Neck 2008;30:1543–1551. 32. Temam S, Mamelle G, Marandas P, et al. Postoperative radiotherapy
for primary mucosal melanoma of the head and neck. Cancer 2005;103:313–319.
33. Trotti A, Peters LJ. Role of radiotherapy in the primary management of mucosal melanoma of the head and neck. Semin Surg Oncol 1993;9:246–250.
34. Ang KK, Peters LJ, Weber RS, et al. Postoperative radiotherapy for cutaneous melanoma of the head and neck region. Int J Radiat Oncol Biol Phys 1994;30:795–798.
35. Agrawal S, Kane JM III, Guadagnolo BA, et al. The benefits of adjuvant radiation therapy after therapeutic lymphadenectomy for clinically advanced, high-risk, lymph node-metastatic melanoma. Cancer 2009;115:5836–5844.
36. Mendenhall WM, Amdur RJ, Hinerman RW, et al. Head and neck mucosal melanoma. Am J Clin Oncol 2005;28:626–630.
37. Burmeister B, Henderson M, Thompson J, et al. Adjuvant radiotherapy improves regional (lymph node field) control in melanoma patients after lymphadenectomy: results of an Intergroup Randomized Trial (TROG 02.01/ANZMTG 01.02) [abstract]. Int J Radiat Oncol Biol Phys 2009;75:S2.
38. Benlyazid A, Thariat J, Temam S, et al. Postoperative radiotherapy in head and neck mucosal melanoma: a GETTEC study. Arch Otolaryngol Head Neck Surg 2010;136:1219–1225.
39. Moore ES, Martin H. Melanoma of the upper respiratory tract and oral cavity. Cancer 1955;8:1167–1176.
40. Owens JM, Roberts DB, Myers JN. The role of postoperative adjuvant radiation therapy in the treatment of mucosal melanomas of the head and neck region. Arch Otolaryngol Head Neck Surg 2003;129:864–868.
41. Douglas CM, Malik T, Swindell R, et al. Mucosal melanoma of the head and neck: radiotherapy or surgery? J Otolaryngol Head Neck Surg 2010;39:385–392.
42. Gilligan D, Slevin NJ. Radical radiotherapy for 28 cases of mucosal melanoma in the nasal cavity and sinuses. Br J Radiol 1991;64:1147–1150.
43. Shibuya H, Takeda M, Matsumoto S, et al. The efficacy of radiation therapy for a malignant melanoma in the mucosa of the upper jaw: an analytic study. Int J Radiat Oncol Biol Phys 1993;25:35–39.
44. Wada H, Nemoto K, Ogawa Y, et al. A multi-institutional retrospective analysis of external radiotherapy for mucosal melanoma of the head and neck in Northern Japan. Int J Radiat Oncol Biol Phys 2004;59:495–500.
45. Bonnen MD, Ballo MT, Myers JN, et al. Elective radiotherapy provides regional control for patients with cutaneous melanoma of the head and neck. Cancer 2004;100:383–389.
46. Ballo MT, Bonnen MD, Garden AS, et al. Adjuvant irradiation for cervical lymph node metastases from melanoma. Cancer 2003;97:1789–1796.
47. Wu AJ, Gomez J, Zhung JE, et al. Radiotherapy after surgical resection for head and neck mucosal melanoma. Am J Clin Oncol 2010;33:281–285.
48. Dirix P, Vanstraelen B, Jorissen M, et al. Intensity-modulated radiotherapy for sinonasal cancer: improved outcome compared to conventional radiotherapy. Int J Radiat Oncol Biol Phys 2010;78:998–1004.
49. Madani I, Bonte K, Vakaet L, et al. Intensity-modulated radiotherapy for sinonasal tumors: Ghent University Hospital update. Int J Radiat Oncol Biol Phys 2009;73:424–432.
50. Narasimhan K, Kucuk O, Lin HS, et al. Sinonasal mucosal melanoma: a 13-year experience at a single institution. Skull Base 2009;19:255–262.
51. Carvajal RD, Antonescu CR, Wolchok JD, et al. KIT as a therapeutic target in metastatic melanoma. JAMA 2011;305:2327–2334.
52. Torres-Cabala CA, Wang WL, Trent J, et al. Correlation between KIT expression and KIT mutation in melanoma: a study of 173 cases with emphasis on the acral-lentiginous/mucosal type. Mod Pathol 2009;22:1446–1456.
53. Harrison L, Sessions R, Hong W. Head and Neck Cancer: A Multidisciplinary Approach, 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009.
54. Robbins KT, Shaha AR, Medina JE, et al. Consensus statement on the classification and terminology of neck dissection. Arch Otolaryngol Head Neck Surg 2008;134:536–538.
55. Ferlito A, Rinaldo A, Silver CE, et al. Elective and therapeutic selective neck dissection. Oral Oncol 2006;42:14–25.
56. Sivanandan R, Kaplan MJ, Lee KJ, et al. Long-term results of 100 consecutive comprehensive neck dissections: implications for selective neck dissections. Arch Otolaryngol Head Neck Surg 2004;130:1369–1373.
57. Robbins KT, Clayman G, Levine PA, et al. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg 2002;128:751–758.

NCCN Clinical Practice Guidelines in Oncology
Mucosal Melanoma of the Head and Neck
© JNCCN–Journal of the National Comprehensive Cancer Network | Volume 10 Number 3 | March 2012
338
The
NC
CN
gu
idel
ines
sta
ff h
ave
no
co
nfl
icts
to
dis
clo
se.
Ind
ivid
ual
Dis
clo
sure
s fo
r th
e N
CC
N G
uid
elin
es P
anel
fo
r M
uco
sal M
elan
om
a o
f th
e H
ead
an
d N
eck
Pan
el M
emb
erC
linic
al R
esea
rch
Su
pp
ort
Ad
viso
ry B
oar
ds,
Sp
eake
rs B
ure
au, E
xper
t W
itn
ess,
or
Co
nsu
ltan
tPa
ten
t, E
qu
ity,
o
r R
oya
lty
Oth
erD
ate
Co
mp
lete
d
Kie
-Kia
n A
ng
, MD
, Ph
DN
on
e B
rist
ol-
Mye
rs S
qu
ibb
Co
mp
any;
El
i Lill
y an
d C
om
pan
y; G
laxo
Smit
hK
line;
ImC
lon
e LL
C;
and
san
ofi
-ave
nti
s U
.S. L
LC
No
ne
No
ne
5/11
/11
Dav
id M
. Bri
zel,
MD
No
ne
Siem
ens
AG
N
on
e N
on
e 10
/7/1
1
Bar
bar
a B
urt
nes
s, M
DG
enen
tech
, In
c.; M
illen
niu
m P
har
mac
euti
cals
, In
c.; a
nd
Pfi
zer
Inc.
A
mge
n In
c.; B
oehr
inge
r In
gelh
eim
Gm
bH;
Gla
xoSm
ithK
line
plc;
Mer
ck &
Co.
, Inc
.; an
d Pfi
zer
Inc.
N
on
e N
on
e 4/
11/1
1
An
tho
ny
J. C
mel
ak, M
DN
on
e A
mg
en In
c.
No
ne
No
ne
6/8/
11
A. D
imit
rio
s C
ole
vas,
MD
Bay
er A
G; B
oeh
rin
ger
Ing
elh
eim
Gm
bH
; Exe
lixis
Inc.
; Gen
ente
ch,
Inc.
; Gla
xoSm
ith
Klin
e p
lc; A
cto
Gen
ix; E
aste
rn C
oo
per
ativ
e
On
colo
gy
Gro
up
; NC
I; an
d R
adia
tio
n T
her
apy
On
colo
gy
Gro
up
Bri
sto
l-M
yers
Sq
uib
b C
om
pan
y N
on
e N
on
e 6/
8/11
Fran
k D
un
ph
y, M
DN
on
e A
mg
en In
c.
No
ne
No
ne
10/1
3/11
Dav
id W
. Eis
ele,
MD
No
ne
No
ne
No
ne
No
ne
10/7
/11
Jill
Gilb
ert,
MD
East
ern
Co
op
erat
ive
On
colo
gy
Gro
up
N
on
e N
on
e N
on
e 6/
22/1
1
Mau
ra L
. Gill
iso
n, M
D, P
hD
No
ne
No
ne
No
ne
No
ne
5/3/
11
Ro
ber
t I.
Had
dad
, MD
No
ne
No
ne
No
ne
No
ne
6/8/
11
Bru
ce H
. Hau
gh
ey, M
BC
hB
, MS
No
ne
No
ne
No
ne
No
ne
3/4/
11
Wes
ley
L. H
icks
, Jr.,
MD
No
ne
No
ne
No
ne
No
ne
6/8/
11
Yin
g J
. Hit
chco
ck, M
DN
on
e N
on
e N
on
e N
on
e 10
/6/1
1
Mer
rill
S. K
ies,
MD
No
ne
No
ne
No
ne
No
ne
2/22
/11
Will
iam
M. L
ydia
tt, M
DN
on
e N
on
e N
on
e N
on
e 5/
2/11
Ellie
Mag
ham
i, M
DN
on
e N
on
e N
on
e N
on
e 6/
7/11
Ren
ato
Mar
tin
s, M
D, M
PHA
mg
en In
c.; B
ayer
AG
; Eis
ai C
o.,
Ltd
.; El
i Lill
y an
d C
om
pan
y;
Exel
ixis
, In
c.; G
enen
tech
, In
c.; N
ova
rtis
AG
; an
d In
fin
ity
Phar
mac
euti
cals
; an
d P
fize
r In
c.
Eli L
illy
and
Co
mp
any;
an
d G
enen
tech
, In
c.
No
ne
No
ne
3/21
/11
Tho
mas
McC
affr
ey, M
D, P
hD
No
ne
No
ne
No
ne
No
ne
4/7/
11
Bh
arat
B. M
itta
l, M
DG
enen
tech
, In
c.
No
ne
No
ne
No
ne
10/7
/11
Dav
id G
. Pfi
ster
, MD
Ast
raZe
nec
a Ph
arm
aceu
tica
ls L
P; E
li Li
lly a
nd
Co
mp
any;
Ex
elix
is, I
nc.
; Gen
ente
ch, I
nc.
; Im
Clo
ne
LLC
; an
d N
ova
rtis
AG
No
ne
No
ne
No
ne
7/27
/11
Har
lan
A. P
into
, MD
No
ne
Bo
ehri
ng
er In
gel
hei
m G
mb
H; a
nd
Bri
sto
l-M
yers
Sq
uib
b C
om
pan
y N
on
e N
on
e 6/
1/11
Joh
n A
. Rid
ge,
MD
, Ph
DN
on
e N
on
e N
on
e N
on
e 11
/9/1
1
San
dee
p S
aman
t, M
DM
eth
od
ist
Hea
lth
care
Fo
un
dat
ion
N
on
e N
on
e N
on
e 5/
31/1
1
Giu
sep
pe
San
gu
inet
i, M
DN
on
eN
on
eN
on
eN
on
e11
/20/
09
Dav
id E
. Sch
ulle
r, M
DN
on
e N
on
e N
on
e N
atio
nal
Can
cer
Inst
itu
te
6/8/
11
Jati
n P
. Sh
ah, M
D, P
hD
No
ne
No
ne
No
ne
No
ne
6/3/
11
Shar
on
Sp
ence
r, M
DN
on
e N
on
e N
on
e N
on
e 8/
15/1
1
An
dre
a Tr
ott
i, III
, MD
Gla
xoSm
ith
Klin
e p
lc; a
nd
EU
SA P
har
ma
Gla
xoSm
ith
Klin
e; a
nd
Nat
ion
al C
ance
r In
stit
ute
N
on
e N
on
e 3/
28/1
1
Ran
dal
S. W
eber
, MD
No
ne
No
ne
No
ne
No
ne
5/3/
11
Gre
go
ry W
olf
, MD
IRX
Th
erap
euti
cs
IRX
Th
erap
euti
cs
No
ne
No
ne
10/6
/11
Fran
k W
ord
en, M
DPfi
zer
Inc.
B
rist
ol-
Mye
rs S
qu
ibb
Co
mp
any
No
ne
No
ne
9/23
/11