multidisciplinary approach to wilms’ tumor: a ... · excessive post-operative radiotherapy and...
TRANSCRIPT
ABSTRACT
Aim of the Work: The aim of this work was to assessthe epidemiologic aspects, clinico-pathological featuresand the results of multidisciplinary treatment of Wilms'tumor (WT) in pediatric patients treated at the NationalCancer Institute (NCI), Cairo University, between January2002 and December 2004.
Patients and Methods: This study included 53 patients,all under the age of 16 years, with previously untreatedWT. Initial evaluation of all patients comprised laboratoryinvestigations and radiological assessment which includedchest X-ray and CT, abdomino-pelvic ultrasonographyand CT. Doppler study of the renal vein and vena cavaand bone scan were done when needed. Neoadjuvantchemotherapy was given to patients suffering from poorgeneral condition, extensive tumor thrombus in the renalvein, irresectable and bilateral (stage V) nephroblastoma.Otherwise, up-front nephrectomy was the standard thera-peutic approach in this study.
Results: The age of the patients ranged from 2 to 108months with a mean of 39.9 months (±22.56). Males andfemales were almost equal in number (50.9% and 49.1%respectively). Tumors were located in the left kidney in52.8%, right kidney in 41.5% and bilaterally in only 5.7%of the cases. An abdominal mass was the most commonclinical presentation (77.4%). Favorable histology wasfound in 86.3% while unfavorable histology was elicitedin 13.7% of the cases. Congenital anomalies were recordedin 4 patients. Stage I and III were the most common(29.4% each), followed by stage II and IV (17.7% each),and finally by stage V (5.9%). Neoadjuvant chemotherapywas given to 27 cases while up-front nephrectomy wasundertaken in 26 cases. Intra-operative spillage occurredin 12% of patients who had preoperative chemotherapyand 31% of those who had upfront nephrectomy. Postop-erative abdominal radiotherapy was given to 32 patients.Twenty five patients underwent renal bed irradiation only,
Journal of the Egyptian Nat. Cancer Inst., Vol. 20, No. 4, December: 410-423, 2008
Multidisciplinary Approach to Wilms’ Tumor:A Retrospective Analytical Study of 53 Patients
SHERIF F. NAGUIB, M.D.*; ALAA EL HADDAD, M.D.**; SAMY A. EL BADAWY, M.D.*** andASHRAF S. ZAGHLOUL, M.D.*
The Departments of Surgical Oncology*, Pediatric Oncology** and Radiotherapy***,National Cancer Institute, Cairo University.
410
while in the other 7 whole abdominal irradiation was used.Additional chest bath (1200 cGy) was given to 7 patients.
Complete remission (CR) was achieved in 74%, whiledeath during neoadjuvant therapy took place in 4% of thecases. Disease progression during treatment was noticedin 8%. These patients were all treated with radio- andchemotherapy. Fatal outcome supervened in 75% of these,whereas in 25%, CR could be accomplished. Relapse afterremission occurred in 14%. A 2nd CR could be achievedin 28.5% with a survival rate of 21.4%. Patients whorelapsed >12 months after 1st CR had a 14 month-survivalrate of 37.5% compared to 0% in those who relapsed <12months after 1st CR. Disease-free survival (DFS) at 2years was 82.4%, while overall survival (OAS) at 2 yearswas 78.9%. Therapy-related complications were mainlyrelated to chemotherapy in 49% of patients and surgeryin 5.9%.
Conclusion: Tight communication between the surgi-cal, the medical and the radiation oncologists, togetherwith the pathologist, is indispensable for better manage-ment of WT patients. Regional lymph node biopsy andaccurate marking of residual disease are essential compo-nents of surgical treatment and heroic surgical attemptsare unnecessary. Neoadjuvant chemotherapy, which is stilla fertile source of debate, could possibly help to avoidexcessive post-operative radiotherapy and its potentialcomplications. Tumor stage and age of patient were foundto affect the results of treatment of Wilms’ tumor; but theonly statistically significant determinant of prognosis washistologic differentiation. Finally, further studies includingmolecular markers are needed to augment therapy for theblastemal predominance subtype or for favorable histologyassociated with loss of heterozygosity (LOA) at chromo-somes 1p and 16q aiming at improved survival.
Key Words: Wilms’ tumor – Nephroblastoma.
INTRODUCTION
Nephroblastoma or Wilms’ tumor (WT) isan embryonal tumor arising from remnants ofimmature renal tissue. It accounts for 6% of all
Correspondence: Dr Ashraf S. Zaghloul, NationalCancer Institute, Fom El-Khalig, Cairo, [email protected]

411
pediatric tumors and typically affects childrenbelow the age of 6 years [1]. Initial survivalrates in the early years of the 20th century wereonly 30%. Today, due to improvement in surgi-cal techniques and the rapid development ofactive chemotherapeutic agents, long-term sur-vival rates in both North American and Europeantrials are approaching 85-90%. Moreover, newtreatment protocols are now proceeding towards"risk-based management" based not only onstage and histology, but also incorporating ge-netic markers with the ultimate objective ofmaximizing cure together with minimal treat-ment-related toxicities [1,2].
The main prognostic indicators for WT arestage, histology, age and biological factors.
Stage: Two major staging systems haveproven to be valuable in predicting outcome oftreatment and are currently used: A pre–chemo-therapy (up-front) surgery-based system devel-oped by the National Wilms’ Tumor StudyGroup (NWTSG) [3] and a post-chemotherapy-based system developed by the InternationalSociety of Pediatric Oncology (SIOP) [4].
Histology: Focal anaplasia portends an in-termediate prognosis between that of tumorswithout anaplasia (also called "favorable" his-tologic feature) and that of tumors with diffuseanaplasia [5-7]. Clear-cell sarcoma (CCSK) andmalignant rhabdoid tumor of the kidney arenow considered as distinct tumor types [8].Whereas the NWTSG classifies Wilms’ tumorsaccording to the presence or absence of anapla-sia, the revised SIOP histologic classificationdivides Wilms’ tumors into three risk groups:Low, intermediate and high risk groups [4,9].
Patient ages: Contrary to two previous groupstudies [10,11], other studies [12,13] have pointedout that the survival rate for adult patients issimilar to that for pediatric WT, although toxicityof treatment is greater in the former group.
Biological prognostic factors: In the 1990s,several studies showed that children with lossof heterozygosity (LOH) at chromosomes 1pand 16q had greater risks of relapse and mor-tality; and future Children’s Oncology Group(COG) clinical studies will augment therapyfor patients with favorable histology (FH) andLOH at 1p and 16q [14]. Other promising prog-nostic markers are an increase in gene copy
number or expression at chromosome 1q [15]and telomerase expression level [16]. It is hopedthat gene expression profiling will identify newprognostic factors in the future [17].
The role of chemotherapy according to theNWTSG and SIOP experience:
Today, the efficacy of actinomycin D(AMD), vincristine (VCR) and doxorubicin intreating WT is undisputed [18,19]. Several coop-erative groups have made important contribu-tions to the optimization of WT therapy, namelythe National Wilm's Tumor Study Group(NWTSG) in North America, the InternationalSociety of Pediatric Oncology (SIOP), the Unit-ed Kingdom Children Cancer Study Group(UKCCSG) in Europe and others. The NWTSGand SIOP studies have included the largestnumber of patients and hence seem to be themost significant [2]. The NWTSG and its suc-cessor, the Children Oncology Group (COG),advocate up-front resection of the primary tu-mor. In contrast, SIOP recommends the admin-istration of chemotherapy for 4 weeks beforesurgery. Both treatment approaches yield excel-lent clinical outcomes, yet a fertile debate con-tinues about the relative merits of each approach[20].
The primary strength of the NWTSG ap-proach is that up-front resection allows an ac-curate histologic diagnosis and assessment oftumor extent, while patients treated in SIOPnephroblastoma studies do not undergo tumorbiopsy before starting therapy. In SIOP 93-01,approximately 5% of lesions treated with che-motherapy were ultimately shown not to be WTand 1.8% of these were benign [9]. Anotherbenefit of removing the tumor before chemo-therapy is that it enables the collection of un-treated tumor tissue allowing an unadulteratedanalysis of the tumor’s molecular biology [2].
The primary strength of the SIOP approachis reduction of tumor volume, thereby "down-staging" the tumor and decreasing the likelihoodof spillage [21]. As a result, fewer patientsreceived local irradiation on SIOP-9 than onNWTS-5, although slightly more of the SIOP-9 patients received anthracycline [20]. A secondadvantage of preoperative chemotherapy is thatresponse to treatment may provide a valuableprognostic indicator [22]. In the absence of aclear choice between up-front nephrectomy and
Multidisciplinary Approach to Wilms’ Tumor

Sherif F. Naguib, et al.412
preoperative chemotherapy, it is reasonable tobase the timing of resection on factors such astumor size, the patient’s clinical condition, andthe experience of the surgeon [2].
The role of surgery:Most authors recommend a trans-abdominal,
trans-peritoneal approach to permit meticulousexploration of sites of involvement and biopsyof suspicious lesions [23]. Gentle handling ofthe tumor and, in selected cases using preoper-ative chemotherapy, can greatly reduce the riskof intra-operative tumor rupture which occursin 15 to 30% of cases. Tumor spillage increasesthe risk of local abdominal relapse by six foldsresulting in subsequent poor outcome [24].
Shamberger et al. [24] emphasized the im-portance of lymph node sampling for pathologicconfirmation of nodal involvement; since therates of false positive and false negative lymphnodes, depending on clinical and radiologicalevaluation, were found to be 54% and 11%,respectively [25]. Analysis of NWTS-1,2,3showed no significant reduction in survivalrates with direct extension or contiguous in-volvement of the liver in comparison to otherstage III presentations. Nevertheless, survivalwas affected with hematogenous intra–paren-chymal liver spread [26].
Wilms’ tumor extends into the inferior venacava in approximately 6% of cases. In thesecases, cavotomy after proximal and distal vas-cular control can be used and if the thrombusis adherent it can be delivered by a Fogarty'sor a Foley's catheter. With meticulous surgery,renal vein involvement does not adversely affectprognosis [27].
Surgical complications observed in the fourthNational Wilms’ Tumor Study (NWTS-4) werebowel obstruction (5.1%), extensive hemorrhageand wound infection (1.9% each), extensivevascular injuries (1.4%), and injuries to othervisceral organs (1%) [28]. Risk factors for sur-gical complications included intravascular ex-tension into the inferior vena cava, the atrium,or both; a flank or paramedian approach; anda tumor diameter greater than 10cm. Interest-ingly, nephrectomy performed by a generalsurgeon carried a higher risk of complications(odds ratio: 9.0) than that performed by a pedi-atric surgeon (odds ratio: 1.0) or a pediatricurologist (odds ratio: 0.7) [2].
Kidney-sparing resection is not generallyrecommended and only 4.7% of patients areeligible for partial nephrectomy [29,30]. Theseinclude patients with a tumor involving onepole and less than one third of the kidney, ifthat kidney is functioning, if the collectingsystem and renal vein are both free of tumorinvolvement, and if clear margins can be ob-tained around the tumor [2].
Stage V, or bilateral Wilms’ tumor, is foundin 4 to 8% of patients and the majority of thesepresent by simultaneous involvement of bothkidneys. Radical nephrectomy should never beperformed at the initial surgical procedure.Rather, the initial procedure should aim at de-fining the extent of tumor in each kidney, ob-taining bilateral biopsies for histological con-firmation and taking biopsies from suspiciouslymph nodes. Subsequently, the child shouldbe treated with chemotherapy appropriate tothe stage and histology of the tumor. Re-evaluation is performed at approximately week5 to determine whether there has been sufficientresponse allowing partial resection with preser-vation of a substantial amount of renal tissue.A second look laparotomy is recommendedwhen serial imaging studies show no furtherreduction in the tumor bulk. At the time ofsecond look, partial nephrectomy should beconsidered, but only if complete tumor resectionwith negative margins is possible and part ofeither or both kidneys can be salvaged. Whenthe extent of the tumor precludes salvage, radicalnephrectomy is required [31].
The role of radiotherapy:
The NWTS-5 [32] has recommended the useof radiation therapy in specific indicationsaccording to tumor stage and histology. Noirradiation is needed in FH with stage I-II oranaplastic tumors with stage I. On the otherhand, postoperative radiotherapy should begiven to all stages of clear cell sarcoma (CCSK)and rhabdoid tumors, to all but stage I anaplastictumors, and to stage III-IV with FH. Irradiationis limited to the flank when the tumor involvesonly the renal hilar or the para-aortic nodes, orwhen residual disease is confined to the flank.Whole abdominal irradiation is needed in casesof intra-peritoneal tumor rupture, diffuse tumorspill or gross residual abdominal disease. Adose of 10.8Gy over 6 fractions is usually given.

413
Whole lung irradiation to 12Gy is also givento lung metastases and, when persistent, eithera boost (to 19.5Gy) of radiation or surgicalresection may be tried.
The SIOP-2001 [33] recommended flankirradiation for stage III with intermediate riskhistology and stages II-III with high risk histol-ogy. Whole abdomen irradiation is indicatedfor all risk groups in cases of diffuse spillageor peritoneal metastases. Whole lung irradiationis given if lung metastases persist at week 9after chemotherapy or surgery, or in cases ofsecondary metastases.
The timing of postoperative irradiation isimportant and the NWTS-5 recommends thatit begins no later than the ninth postoperativeday [32].
Aim of the work:
The aim of this work was to review theepidemiologic aspects, clinico-pathologicalfeatures and clinical presentations of Wilms'tumor (WT) and to appraise the results andcomplications of different components of mul-tidisciplinary treatment of this disease in pedi-atric patients treated at the National CancerInstitute (NCI), Cairo University, between Jan-uary 2002 and December 2004. Timing and siteof relapse together with salvage treatment andits final outcome were also assessed.
PATIENTS AND METHODS
This retrospective analytical study was car-ried out in the Departments of Pediatric Oncol-ogy, Surgery and Radiotherapy of the NationalCancer Institute (NCI), Cairo University. Pre-viously untreated pediatric patients with Wilms’Tumor who presented to the NCI during theperiod from January 2002 to December 2004were recruited and their number reached 53patients. Eligibility criteria included: Age ≤16years, pathologically or radiologically provenWT and no previous treatment by radio- orchemotherapy.
Initial evaluation of all patients consistedof complete history taking including familyhistory of cancer, especially WT. Physical ex-amination included weight and height, site andsize of the tumor, blood pressure and congenitalanomalies (like aniridia, genitourinary malfor-
mations or hemi-hypertrophy). Laboratory in-vestigations comprised complete blood picture,liver and kidney function tests and urine analy-sis. Radiological assessment included chest X-ray and CT, abdomino-pelvic ultrasonographyand CT (Fig. 1), Doppler study of the renal veinand vena cava when needed, bone scan in casesof clear cell sarcoma and brain CT in clear cellsarcoma and rhabdoid tumor of the kidney.
Treatment policy:
Surgery: When feasible, up-front nephrecto-my was the standard therapeutic approach inthis study. However, there were specific indica-tions for pre-operative chemotherapy, namelypoor general condition rendering the child unfitfor surgery, extensive tumor thrombus in therenal vein extending to the supra-hepatic venacava or right atrium, irresectable tumor at lap-arotomy and bilateral (stage V) nephroblastoma.
Laparotomy was carried out following theNWTSG V recommendations [28] through atransabdominal transperitoneal approach usinga generous bucket-handle incision. To start, thecontralateral kidney was exposed and palpatedto exclude bilateral WT. Before mobilizationof the primary tumor, an attempt was made todissect, expose and ligate the renal vessels. Theadrenal gland was removed with the tumor onlyif adherent, or if the tumor was in the upperpole. Radical en-bloc resection of contiguousstructures (such as the colon, stomach, spleenor diaphragm) was only undertaken if the sur-geon was sure that all gross disease would beremoved. If residual tumor was to be left behind,only a biopsy was taken and the site identifiedwith metal clips.
The peritoneum was considered soiled if anincisional or needle biopsy was taken or if thetumor was spilled or ruptured. The presence ofhemorrhagic peritoneal fluid was also consid-ered as major spillage regardless of microscopicidentification of tumor cells in the fluid.
After tumor resection, routine sampling fromthe para-aortic, celiac and iliac nodes was carriedout and involved or suspicious glands wereexcised and accurately labeled. All surgicalspecimens were immediately sent to the pathol-ogist, fresh or in saline, rather than fixed informalin (Fig. 2).
Multidisciplinary Approach to Wilms’ Tumor

Sherif F. Naguib, et al.414
Chemotherapy: The day of nephrectomywas considered as day 0 for those who under-went up-front nephrectomy. Babies <12 monthsof age were given 1/2 the recommended dosebased on body weight.
Stage I/FH or anaplastic histology and stageII/FH were given actinomycin D (AMD) andvincristine (VCR).
Stage III and IV/FH received AMD, VCR,doxorubicin and cardioxan in addition to radio-therapy, which was started not later than day 9and in fractions of 180cGy.
Stage II-IV/anaplastic histology and stageI-IV clear cell sarcoma were treated with thesame former combination in addition to cyclo-phosphamide (CTX) and mesna.
Stage I-IV rhabdoid tumor of the kidney,relapsing and resistant cases were treated withcarboplatin and etoposide. This combinationwas given at w1+4 followed by cyclophospha-mide and mesna.
Patients who were scheduled for preoperativechemotherapy received 6 weeks of weekly VCRtogether with AMD and doxorubicin. Thesepatients were considered as stage III locallyand radiological evaluation was carried out atw6 before referral to surgery.
Radiotherapy: Radiation was given in a doseof 180cGy/fraction. It was initiated only whenthe patient was stable postoperatively, withnormal intestinal motility, absolute neutrophilcount >1000/ul and hemoglobin level >10.0g/dl.
Stage I and II were not irradiated, while allstage III patients were given postoperativeabdominal irradiation. Stage IV patients werealso given postoperative abdominal irradiationif their primary tumor was stage III.
In case of residual flank disease, hilar nodesor para-aortic nodes, the field of radiation en-compassed the tumor bed in the flank, crossingthe midline to include bilateral aortic nodes. Incases with peritoneal seeding, gross residualabdominal disease or tumor rupture, radiationfield encompassed the whole abdomen. Boosterdoses of 1080cGy were given to areas of grossresidual disease =or >3cm.
The irradiation field was determined by thepreoperative CT scan and was defined as the
outline of the kidney and any associated tumor,plus a 1cm margin all around. Opposing anteriorand posterior fields were used. When wholeabdominal irradiation was needed, portals ex-tended from the diaphragmatic domes down tothe levels of the lower border of obturatorforamina excluding the femoral heads.
Follow-up:
All, except three patients, were followed-up for a period ranging from 2 to 48 monthswith a median duration of 24 months. Theywere submitted to regular physical examina-tions; while chest X-ray or CT were undertakenevery 6 weeks till complete remission thenevery 3 months for 2 years to be repeated every6 months for 2 more years. Patients with neph-rogenic rests were scheduled for abdominal U/S6 weeks postoperatively, then every 3 monthsuntil the age of 8 years. Patients without neph-rogenic rests were scheduled for abdominal U/S6 weeks postoperatively, then every 3 monthsfor 2 years to be repeated every 6 months for2 more years. Those who presented with he-matogenous metastases (liver, lung, brain orbone) required evaluation of the affected sitesat intervals similar to those recommended forchest and abdomen cases.
Statistical analysis:
Data were analyzed using the SPSS statisticalpackage version 12. Numerical data were ex-pressed as mean ± standard deviation (SD),median, maximum and minimum. Qualitativedata were expressed as frequency and percent-age. The chi-square test was used to examinethe relation between qualitative variables. Sur-vival analysis was carried out using the Kaplan-Meier method and presented as cumulativesurvival rates. Comparison between two survivalcurves was done using the log-rank test. Prob-ability (p-value) equal or less than 0.05 wasconsidered significant, and if less than 0.001,highly significant. Disease-free-survival (DFS)was calculated only for patients who achievedcomplete remission (CR).
RESULTS
Patient characteristics:
This study included 53 patients, all underthe age of 16 years with previously untreatedWT. Their ages ranged from 2 to 108 monthswith a mean of 39.9 months (±22.56); and 71.7%

415
were <60 months. Males and females werealmost equal in number (50.9% and 49.1%,respectively). Tumors were located in the leftkidney in 52.8%, right kidney in 41.5% andbilaterally in only 5.7% of the cases. The mostcommon clinical presentation, and by far, wasan abdominal mass (77.4%). Abdominal painand hematuria were encountered in 17% and13.2% of the cases, respectively.
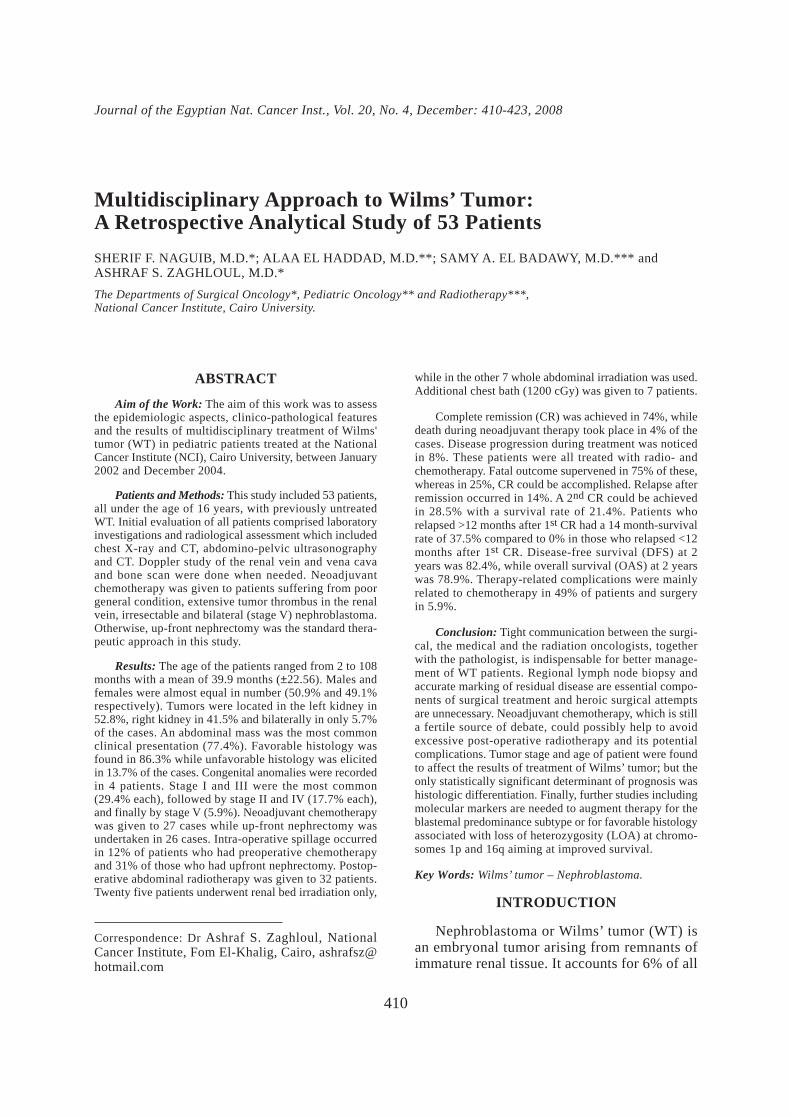
Favorable histology (FH) was found in86.3% of the cases (75% of these had blastemalcomponent and 25% were without), while un-favorable histology was elicited in 13.7% whereanaplastic tumors and clear cell sarcoma eachaccounted for 5.9% and rhabdoid tumor for1.9%. Congenital anomalies were found in 4patients in this study. They were in the form ofisolated hemi-hypertrophy, horse-shoe kidney,aniridia with cryptorchidism, and hydrocephaluswith psychomotor delay and cryptorchidism,each of which was elicited in 1 patient (1.9%).
Patient management:
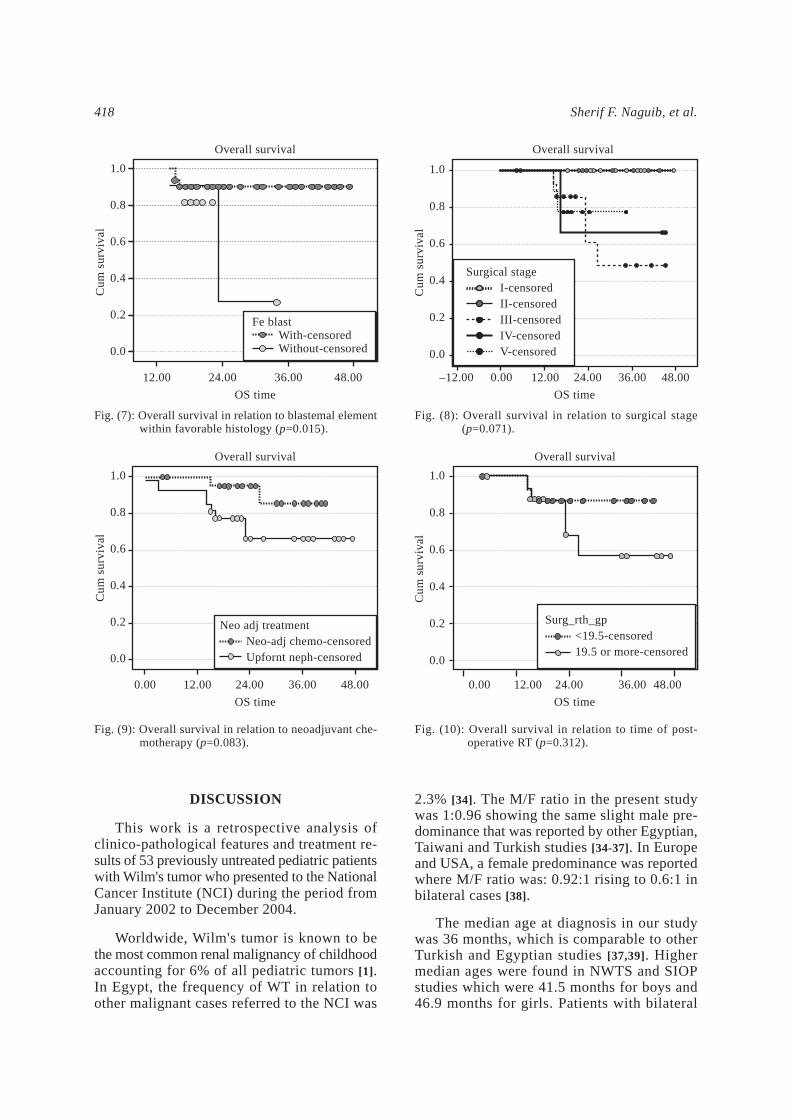
Neoadjuvant chemotherapy was given to 27cases (51%), while up-front nephrectomy wasundertaken in 26 cases (49%). Stage I and IIIwere the most common (29.4% each) followedby stage II and IV (17.7% each) and finally bystage V (5.9%). Intra-operative spillage occurredin 11/51 patients (21.5%). Among those whohad undergone upfront nephrectomy, 8/26 (31%)experienced spillage while only 3/25 (12%) didso among those who had preoperative chemo-therapy (Table 1). Postoperative abdominalirradiation was given to 32 patients (60.4%), in25/32 (78.1%) only to the renal bed while in7/32 (21.9%) whole abdominal irradiation wasused. Additional chest bath (1200cGy) wasgiven to 7/32 (21.9%) patients.
Patient outcome:
Among the 53 patients in this study, 3 pa-tients were non-evaluable as they were lost tofollow-up after nephrectomy. Complete remis-sion (CR) was achieved in 74%, while deathduring neoadjuvant therapy took place in 4%(2 patients). Disease progression during treat-ment was documented in 8% of the cases (4patients). One occurred locally, one in the chestand two both locally and in the chest. Theywere all treated with postoperative radio- andchemotherapy. Disease progression ended with
a fatal outcome in 3/4 patients, whereas CRcould be achieved in only one patient.
Relapse after remission occurred in 14% ofthe cases (7 patients). One of them relapsedonly locally, three developed hematogenousmetastases (chest and/or bone), while the re-maining three had both local and hematogenousmetastases (chest and/or liver). Table (2) illus-trates the time and type of relapse as well asthe treatment given and final outcome. Fromthis table it appears that 2/7 patients (28.5%)achieved a 2nd CR with a survival rate of 21.4%.It is also evident that the time of relapse baressome value since patients who relapsed at or>12 months after 1st CR (4/7) had a 14 month-survival rate of 37.5% compared to 0% in thosewho relapsed <12 months after 1st CR. Never-theless, this was statistically insignificant(p=0.113) mostly due to the small number ofpatients.
Disease-free survival (DFS) at 2 years was82.4% while overall survival (OAS) at 2 yearswas 78.9%. The effect of age, time of surgery,surgical stage, pathology, blastemal element(within the favorable histology) and time ofpostoperative radiotherapy on DFS and OAS isshown in Tables (3,4) respectively. It appearsthat blastemal predominance (p=0.07), age(p=0.09), timing of postoperative radiotherapy(p=0.15) and surgical stage (p=0.28) affectedDFS, nevertheless their effect was found statis-tically insignificant (Figs. 3-6). On the otherhand, blastemal predominance (p=0.015), sur-gical stage (p=0.071), neoadjuvant chemother-apy (p=0.083) and timing of postoperative ra-diotherapy (p=0.312) also appeared to affectOAS; nonetheless, blastemal differentiation wasthe only statistically significant factor (Figs. 7-10).
Therapy-related complications were mainlyrelated to chemotherapy and surgery. Etoposide/carboplatin caused grade 4 myelosuppressionin 15 cases. Vincristine neurotoxicity (ptosis,jaw pain, ileus) was recorded in 8 patients.Cyclophosphamide related hemorrhagic cystitisoccurred in 2 patients. Hepatitis supervened in7 patients. It was due to virus C infection in 6patients and to actinomycin D toxicity in 1patient. Surgical complications were confinedto post-operative adhesive intestinal obstructionwhich occurred in 3 patients (5.9%).
Multidisciplinary Approach to Wilms’ Tumor

Sherif F. Naguib, et al.416
Table (2): Relapsed patients: Time and site of relapse, treatment and final outcome.
Treatment of relapsedchildrenInitial
Outcome
d PDd PDd PDd PDA CRd PDA CR
RT
Local
LungLocal
Lung + Bone
Surg
Metast
Metast
Site
Local + ChestChestChest + BoneLocal + ChestLocalLocal + Chest + LiverChest + Bone
Cth
4th
4th
4th
4th
4th
4th
4th
Time ofrelapse inmonths
(post-CR)
24612121419
Management
CthCth + RTCth + RTCth + RTCth + RTCth + RTCth
Pathology
FHFHFHUHFHFHFH
VIVIIIIIIIVIIII
StageSerial
1234567
Table (3): Disease-free survival in relation to differentvariables.
* Total No of patients is 44 because 6 patients were not evaluatedfor DFS, 2 of them died early during pre-operative chemotherapyand 4 patients showed disease progression.
Age:<60 months≥60 months
Time of surgery:Upfront nephrectomyPost neo-adjuvant chemotherapy
Surgical stage:IIIIIIIVV
Pathology:FavorableUnfavorable
Favorable histology:Without blastemal predominanceWith blastemal predominance
Time of post-operative RT:<19 days≥19 days
Variable 2 yearDFS
76.1%100.0%
84.4%81.0%
90%100%72.2%71.4%66.7%
83.4%66.7%
89.1%66.7%
68.1%92.3%
pvalue
0.094
0.696
0.284
0.586
0.077
0.149
No*
3212
2222
1291373
395
309
1414
Table (4): Overall survival in relation to different variables.
*Total No of patients are 48 as 2 patients died during pre-operativechemotherapy.
Age:<60 months≥60 months
Time of surgery:Upfront nephrectomyPost neo-adjuvant chemotherapy
Surgical stage*:IIIIIIIVV
Pathology*:FavorableUnfavorable
Favorable histology:Without blastemal predominanceWith blastemal predominance
Time of post-operative RT:<19 days≥19 days
Variable 2 yearOAS
78.5%77.4%
95.2%66.5%
100%100%61.2%77.8%100%
80.6%66.7%
90.5%27.3%
68.1%86.7%
pvalue
0.605
0.083
0.071
0.726
0.015
0.312
No
3614
2327
1291593
435
3211
1616
FH: Favorable histology.UH: Unfavorable histology.Cth: Chemotherapy.
Surg. : Surgery.RT : Radiotherapy.Metast: Metastatectomy.
A: Alive.4th Cth regimen: Carboplatine,Etoposide and Cyclophosphamide.
Post-CR: Post-complete remission.d : Died.PD: Progressive disease.
Table (1): Surgical stage distribution and operative spillage (No = 51)*.
Patients' management
Upfront nephrectomy:No of patients%
Neo-adjuvant chemotherapy:No of patients%
Total
Surgical stageSpillage
872.7%
327.3%
11
Total
2651.0%
2549.0%
51*
V
00%
3100%
3
IV
444.4%
555.6%
9
III
746.7%
853.3%
15
II
777.8%
222.2%
9
I
853.3%
746.7%
15
* Total number of patients are 51 as 2 patients died early during neo-adjuvant chemotherapy.

417Multidisciplinary Approach to Wilms’ Tumor
Fig. (1): CT of a 4-year old child with left Wilms’ tumorinvolving middle and lower segments of thekidney.
Fig. (2): Surgical specimen of the previous case afternephrectomy.
Fig. (3): Disease free survival in relation to blastemalelement within favorable histology (p=0.077).
Fig. (4): Disease free survival in relation to age groups(p=0.094).
Fig. (5): Disease-free survival in relation to time of post-operative RT (p=0.149).
Fig. (6): Disease-free survival in relation to surgical stage(p=0.284).
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
0.00 12.00 24.00 36.00 48.00
DF time
Disease free survival
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
0.00 12.00 24.00 36.00 48.00
DF time
Disease free survival
Fe blastWith-censoredWithout-censored
Surg_rth_gp<19.5-censored19.5 or more-censored
0.00 12.00 24.00 36.00 48.00
DF time
Disease free survival
Surgical stageI-censoredII-censoredIII-censoredIV-censoredV-censored
0.00 12.00 24.00 36.00 48.00
DF time
Disease free survival
Age gps<60 m-censored60 m or more-censored
Sherif F. Naguib, et al.418
DISCUSSION
This work is a retrospective analysis ofclinico-pathological features and treatment re-sults of 53 previously untreated pediatric patientswith Wilm's tumor who presented to the NationalCancer Institute (NCI) during the period fromJanuary 2002 to December 2004.
Worldwide, Wilm's tumor is known to bethe most common renal malignancy of childhoodaccounting for 6% of all pediatric tumors [1].In Egypt, the frequency of WT in relation toother malignant cases referred to the NCI was
2.3% [34]. The M/F ratio in the present studywas 1:0.96 showing the same slight male pre-dominance that was reported by other Egyptian,Taiwani and Turkish studies [34-37]. In Europeand USA, a female predominance was reportedwhere M/F ratio was: 0.92:1 rising to 0.6:1 inbilateral cases [38].
The median age at diagnosis in our studywas 36 months, which is comparable to otherTurkish and Egyptian studies [37,39]. Highermedian ages were found in NWTS and SIOPstudies which were 41.5 months for boys and46.9 months for girls. Patients with bilateral
Fig. (7): Overall survival in relation to blastemal elementwithin favorable histology (p=0.015).
Fig. (8): Overall survival in relation to surgical stage(p=0.071).
Fig. (9): Overall survival in relation to neoadjuvant che-motherapy (p=0.083).
Fig. (10): Overall survival in relation to time of post-operative RT (p=0.312).
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
12.00 24.00 36.00 48.00
OS time
Overall survival
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
0.00 24.00 36.00 48.00
OS time
Overall survival
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
24.00 36.00 48.00
OS time
Overall survival
0.00 12.0012.00
Fe blastWith-censoredWithout-censored
1.0
0.8
0.6
0.4
0.2
0.0
Cum
sur
viva
l
–12.00 24.00 36.00 48.00
OS time
Overall survival
0.00 12.00
Surgical stageI-censoredII-censoredIII-censoredIV-censoredV-censored
Neo adj treatmentNeo-adj chemo-censoredUpfornt neph-censored
Surg_rth_gp<19.5-censored19.5 or more-censored

419
cases were younger, with a median of 29.5months for boys and 32.6 for girls [40]. Theyounger median age in our study may be dueto male predominance and the 3 bilateral casesthat were not analyzed separately. Two agepeaks, 36 and 60 months, were recorded in ourstudy. This was reported by no other study.
In the present study, the left kidney wasaffected more frequently than the right, (52.8%and 41.5%, respectively). This was comparableto the findings of Yildiz et al. [37] but contraryto those of other Egyptian studies [39-41].
Abdominal swelling was the most commonpresenting symptom in our patients, accountingfor 77.4% which is slightly lower than thatreported by other Egyptian, Turkish and Italianstudies [34,37,39,40,42] but slightly higher thanthat of the UKCCS2 held in Britain, which was74% [43]. On the other hand, abdominal painand gross hematuria were the presenting symp-tom in 17% and 13.2% of the cases, respectively,which is comparable to other Egyptian andItalian studies [35,42].
In our series, congenital anomalies werefound in 7.5% of cases. This is similar to thefindings of Green [44] and the NWTS-3 [45] (4-8% and 7.35%, respectively). A higher incidence(17.3%) was reported by Hung et al. [36], whilelower incidences (1.4% and 2.8%) were foundby other Egyptian and Turkish studies [37,39].
In our study, stage I was found in only 29.4%and stage IV in 17.6%. Earlier stages werereported by the NEMROCK study [35] wherestage I accounted for 35.5% and stage IV foronly 6.5%. Similarly, less advanced stages werealso reported by other Western and Asian studies.In the 2nd UKCCS [43], NWTS [26] and SIOP[13], stage I accounted for 34%, 47% and 61%respectively. In the Taiwani [36], Turkish [37]and 3rd NWTS [45], stage IV accounted for only6.8%, 9% and 10%, respectively. This mayreflect lack of awareness among the mothers ofour patients and their reluctance to seek expertmedical advice.
Surgical spillage occurred in 21.5% of ourpatients, which is close to the 5th NWTS [46]that reported a rate of 19.3%. Spillage tookplace in 8/26 patients (31%) with upfront ne-phrectomy, whereas it occurred in only 3/25patients (12%) with preoperative chemotherapy
(Table 3). This reflects the influence of neoad-juvant chemotherapy in reducing spillage. Nev-ertheless, the difference was not statisticallysignificant (p=0.1), probably due to the smallnumber of cases. The final outcome was notaffected probably because all cases experiencingspillage were given post-operative radiotherapy.
In the present study, 86.3% of the patientshad favorable histology (FH), while 13.7% hadunfavorable histology (UH). These findings areclose to those of the 3rd NWTS (89% FH and11% UH) [45], the 2nd UKCCS (90% FH and10% UH) [48] and the Turkish study (88.2% FHand 11.8% UH) [37].
The percentage of our patients who receivedradiotherapy (renal bed and/or metastatic sites)was 62.7%, which is higher than that reportedin other studies using neoadjuvant chemotherapylike the 9th SIOP study [47], where only 24%of the patients required irradiation. This largedifference could be due to the late presentationof our patients. Also, patients who underwentupfront nephrectomy in our study showed ahigher incidence of surgical spillage requiringpost-operative radiotherapy while those whoreceived neoadjuvant chemotherapy in this studywere advanced and considered as stage III, soaccording to the NWTSG recommendationsthey were all candidates for post-operativeradiotherapy.
The median time to postoperative radiother-apy in our study was 19.5 days compared to 9days in both the 3rd and 4th NWTS. Both thesestudies found no difference in the rate of ab-dominal relapse among patients receiving ra-diotherapy 0-9 days postoperatively and thosewho were irradiated >10 days postoperatively[48]. In contrast, our patients showed betterdisease-free (DFS) and over-all survival (OAS)when they received radiotherapy >19.5 dayspostoperatively, compared to <19 days. DFSwas 92.3% versus 68.1% and OAS was 86.7%versus 68.1%. These results were not statisticallysignificant (p>0.1), probably due to the smallnumber of patients in our study.
The relapse rate among our patients was18.4% which lies between the rates of 17.9%and 24.2% reported by other Egyptian studies[35,39]. These are all higher than those demon-strated by the 4th NWTS and the 9th SIOP whichwere 11% and 10% respectively [44,49]. This
Multidisciplinary Approach to Wilms’ Tumor

Sherif F. Naguib, et al.420
can be explained by the advanced stage at pre-sentation in our patients.
The most frequent site of relapse in ourseries was the lung (85.5%) which is in accor-dance with Green [38] and the NEMROCK study[35]. The latter reported distant metastases in>60% of their relapsed cases, where 70% ofthese were in the lungs [35]. In contrast, twoother Egyptian studies described the abdomenas the most frequent site of relapse [39,40]. Thisfinding reflects improved local control in ourseries due to more vigilant surgery and improvedradiotherapy techniques.
The rate of 2nd complete remission (CR) inour study was 28.6% which is higher than inthe NEMROCK study [35] which reported a 2nd
CR in only 6.6% of the cases. This reflects moreefficient follow-up and salvage chemotherapyin our patients. Nevertheless, the survival rateof these patients was lower than that of the St.Jude Children's Research hospital [50] (21.4%versus 50%-60%). In our study, the 1-year post-relapse survival for those who relapsed >12months post 1st CR was 37.5% with a cure rateof 50%. This compares favorably with the fig-ures reported by the 2nd and 3rd NWTS wherethe 3-year post relapse survival for patients whorelapsed >12 months post-diagnosis was 41%with a cure rate of 60% [51].
Surgical complications were confined toadhesive intestinal obstruction which occurredin 5.9% of cases. This is comparable to thefigure reported by Ritchey et al., in the NWTS[28] which was 5.1% and close to that reportedin the large German study by Seseke et al. [52]which was 8.8%. When compared to the 19.8%rate of overall operative complications of theNWTS-3 [28], our results are slightly betterprobably due to aversion of heroic resectionsinvolving adjacent organs.
Tumor stage was found to affect survival,confirming findings of previous Egyptian andwestern studies. Nevertheless, we did not findit statistically significant (p=0.284 and 0.071for DFS and OAS, respectively). According tostage distribution, our 2-year DFS rates were90%, 100%, 72.2%, 71.4% and 66.7%; whileour 2-year OAS rates were 100%, 100%, 61.2%,77.8% and 100% for stages I to V, respectively.Similar findings were reported by other Egyptianstudies, yet survival figures were higher in our
study. Ahmed et al. [39] reported a 3-year DFSof 90%, 76%, 67%, 31% and 62% and their 3-year OAS were 93%, 88%, 72%, 40% and 62%for stages I to V, respectively. This improvementin survival, mainly in stages II, III and IV, isprobably due to improvement in diagnosis ofstage IV patients by using chest CT at initialevaluation thus giving chest irradiation accord-ingly, to the judicious application of combinedtreatment modalities (surgery, radiotherapy andchemotherapy) and to the proper supportivecare delivered to the patients.
Nevertheless, our survival figures were bare-ly comparable to some, or even lower than,other large western studies. The 2-year DFS ofthe 9th SIOP study for stages I to III with favor-able histology were 88%, 85% and 71% respec-tively [49]. Similar results were described bythe UKW-2 and UKW-3 where the 4-year DFSwere 86.5%, 82%, 82%, 70% and 70% for stagesI to V respectively [43]. Yet, our 2-year DFSrates are still lower than those of the 4th NWTSmainly for stages III and IV and which werereported to be 90.6% at 2 years and 88.9% at8 years [53] indicating better local and metastaticcontrol in their patients.
Similarly, our OAS was comparable to otherwestern studies except for stage III whichshowed lower rates among our patients (61.2%)compared to other studies reporting OAS forstage III to be 85% at 2 years [49], 84% at 4years [43] and 93% at 8 years [53] reflectingbetter salvage strategy and outcome in theirpatients.
Histological differentiation was also foundto affect survival, confirming findings of previ-ous Egyptian and western studies. Nevertheless,we did not find it statistically significant(p=0.586 and 0.726 for DFS and OAS, respec-tively). To illustrate this finding, our 2-yearDFS and OAS for favorable histology (FH)were 83.4% and 80.6% respectively comparedto 66.7% and 66.7% for unfavorable histology(UH). A previous Egyptian study by Ahmed etal. [39] similarly reported 3-year DFS and OASfor favorable histology (FH) to be 78% and87% respectively compared to 54% and 58%for unfavorable histology (UH). Except for theOAS of cases with FH, our survival figures arehigher than those of this previous Egyptianstudy as we tailored our chemotherapy regimensin accordance with different tumor pathologies.

421
Our 2-year DFS for FH (83.4%) is similar tosome western studies as the UKW-2 [43] andthe SIOP-9 [49] which reported 83% and 85%,respectively.
On the other hand, our 2-year OAS for FHwas 80.6% which is lower than the figuresreported by many other Egyptian and westernstudies and which were 87% at 3 years [39],91% at 2 years [43], and 90% at 5 years [49]reflecting their better salvage outcome.
Within the FH group, our 2-year DFS forpatients with blastemal predominance was66.7% and for those without blastemal predom-inance, it was 89.1%. The same difference wasreported by Ahmed et al. [39]. The SIOP 93-01,reported 5-year DFS for blastemal predominance(after preoperative chemotherapy) to be 79%and for those without blastemal predominance,it was 90% [49]. Our figures in patients withoutblastemal predominance are comparable to thosereported by the SIOP 93-01 while those obtainedwith blastemal predominance are lower. Thisis mostly due to the fact that they up-gradedthe latter group considering it as high risk groupthat was given different chemotherapeuticagents.
Conclusion:
Histologic differentiation, age of patient andtumor stage were found to be the most importantdeterminants of prognosis of Wilm's tumor inour study and they deserve priority in designingfuture therapeutic requirements. Therefore, goodcommunication between the surgical, medicaland radiation oncologists, together with thepathologist, is indispensable for better manage-ment of the patients. Moreover, biopsy fromregional lymph nodes and accurate marking ofresidual disease, if present, in addition to adetailed surgical report with particular attentionto correct tumor stage and pathology are essen-tial for adequate patient treatment.
The value of the SIOP strategy advocatingneoadjuvant therapy before tumor resectionremains a fertile source of debate. The lowerrate of surgical complications and intraoperativespillage so obtained remains to be weighedagainst the risk of administering chemotherapyto benign cases, that of modifying tumor histol-ogy and missing accurate pre-treatment deter-mination of stage or histology.
In spite of achieving comparable survivalrates in our study when compared to othersadopting the NWTS strategy, the SIOP policycould possibly be more appropriate to our pa-tients, aiming to reduce the use of post-operativeradiotherapy and its potential complications. Inthe near future, a prospective randomized studyis needed to evaluate whether avoiding postop-erative radiotherapy, by down-staging the tumorwith pre-operative chemotherapy, will influenceour local control rates or not.
The timing of postoperative radiotherapycould influence outcome since better disease-free (DFS) and overall survival (OAS) wereachieved in our patients when they receivedradiotherapy >19.5 days postoperatively com-pared to <19 days. This issue requires moredetailed study.
Also, further studies are needed to augmenttherapy for the blastemal predominance subtypeaiming at improved survival, especially forthose with persistent viable blastemal elementafter neoadjuvant chemotherapy.
Molecular markers are also needed to con-firm findings concerning higher risk of relapseand death among patients with favorable histol-ogy associated with loss of heterozygosity(LOA) at chromosomes 1p and 16q. The aimis to augment therapy for these patients in thefuture.
REFERENCES
1- Ehrlich PF. Wilm’s Tumor: Progress and considerationsfor the surgeon. Surg Oncol. 2007, 16: 157-71.
2- Metzger ML, Dome JS. Current Therapy for Wilms’Tumor. Oncologist. 2005, 10 (10): 815-26.
3- Kalapurakal JA, Dome JS, Perlman EJ, MalogolowkinM, Haase G Grundy P, et al. Management of Wilms’tumor: Current practice and future goals. LancetOncol. 2004, 5: 37-46.
4- Vujanic GM, Sandstedt B, Harms D, Kelsey A,Leuschner I De Kraker J. The SIOP NephroblastomaScientific Committee. Revised International Societyof Pediatric Oncology (SIOP) working classificationof renal tumors of childhood. Med Pediatr Oncol.2002, 38: 79-82.
5- Beckwith JB, Palmer NF. Histopathology and prognosisof Wilms’ tumors: Results from the First NationalWilms’ Tumor Study. Cancer. 1978, 41: 1937-48.
6- Faria P, Beckwith JB, Mishra K, Zuppan C, Weeks DA., Breslow N, et al. Focal versus diffuse anaplasiain Wilms’ tumor-new definitions with prognostic
Multidisciplinary Approach to Wilms’ Tumor

Sherif F. Naguib, et al.422
significance: A report from the National Wilms’ TumorStudy Group. Am J Surg Pathol. 1996, 20: 909-20.
7- Green DM, Beckwith JB, Breslow NE, Faria P, Mok-sness J, Finklestein JZ, et al. Treatment of childrenwith stages II to IV anaplastic Wilms’ tumor: A reportfrom the National Wilms’ Tumor Study Group. J ClinOncol. 1994, 12: 2126-31.
8- Green DM, Breslow NE, Beckwith JB, Moksness J,Finklestein JZ, D’Angio DJ. Treatment of childrenwith clear-cell sarcoma of the kidney: A report fromthe National Wilms’ Tumor Study Group. J Clin Oncol.1994, 12: 2132–37.
9- de Kraker J, Graf N, van Tinteren H, Pein F, SandstedtB, Godzinski J, et al. Reduction of postoperativechemotherapy in children with stage I intermediate-risk and anaplastic Wilms’ tumor (SIOP 93-01 trial):A randomized controlled trial. Lancet. 2004, 364:1229-235.
10- Breslow N, Sharples K, Beckwith JB, Takashima J,.Kelalis PP, Green DM, et al. Prognostic factors innon-metastatic, favorable histology Wilms’ tumor.Results of the Third National Wilms’ Tumor Study.Cancer. 1991, 68: 2345-53.
11- Pritchard-Jones K, Kelsey A, Vujanic G, Imeson J,Hutton C, Mitchell C, et al. Older age is an adverseprognostic factor in stage I, favorable histology Wilms’tumor treated with vincristine monochemotherapy: Astudy by the United Kingdom Children’s Cancer StudyGroup, Wilms’ Tumor Working Group. J Clin Oncol.2003, 21: 3269-75.
12- Arrigo S, Beckwith JB, Sharples K, D'Angio G, HaaseG. Better survival after combined modality care foradults with Wilms’ tumor. A report from the NationalWilms’ Tumor Study. Cancer. 1990, 66: 827-30.
13- Reinhard H, Aliani S, Ruebe C, Stöckle M, LeuschnerI, Graf N. Wilms’ tumor in adults: Results of theSociety of Pediatric Oncology (SIOP) 93-01/Societyfor Pediatric Oncology and Hematology (GPOH)Study. J Clin Oncol. 2004, 22: 4500-6.
14- Grundy PE, Telzerow PE, Breslow N, Moksness J,Huff V, Paterson MC. Loss of heterozygosity forchromosomes 16q and 1p in Wilms’ tumors predictsan adverse outcome. Cancer Res. 1994, 54: 2331-3.
15- Lu YJ, Hing S, Williams R, Pinkerton R, Shipley J,Pritchard-Jones K. Chromosome 1q expression pro-filing and relapse in Wilms’ tumor. Lancet. 2002, 360:385-6.
16- Dome JS, Bockhold CA, Li SM, Baker SD, GreenDM, Perlman EJ, et al. High telomerase RNA expres-sion is an adverse prognostic factor for favorablehistology Wilms’ tumor. J Clin Oncol. 2005, 23: 9138-45.
17- Williams RD, Hing SN, Greer BT, Whiteford CC, WeiJS, Natrajan R, et al. Prognostic classification ofrelapsing favorable histology Wilms’ tumor usingcDNA microarray expression profiling and supportvector machines. Genes Chromosomes Cancer. 2004,41: 65-79.
18- Farber S. Chemotherapy in the treatment of leukemiaand Wilms’ tumor. JAMA. 1966, 198: 826-36.
19- D’Angio GJ, Evans A, Breslow N, Beckwith B, BishopH, Farewell V, et al. The treatment of Wilms’ tumor:Results of the Second National Wilms’ Tumor Study.Cancer. 1981, 47: 2302-11.
20- D’Angio GJ. Pre- or post-operative treatment forWilms’ tumor? Who, what, when, where, how, why-and which. Med Pediatr Oncol. 2003, 41: 545-9.
21- Beckwith JB. Wilms’ tumor and other renal tumorsof childhood: A selective review from the NationalWilms’ Tumor Study Pathology Center. Hum Pathol.1983, 14: 481-92.
22- Boccon-Gibod L, Rey A, Sandstedt B, Delemarre J,Harms D, Vujanic G, et al. Complete necrosis inducedby preoperative chemotherapy in Wilms’ tumor as anindicator of low risk: Report of the InternationalSociety of Pediatric Oncology (SIOP) nephroblastomatrial and study 9. Med Pediatr Oncol 2000, 34: 183-90.
23- Ladd WE. Embryoma of the kidney (Wilms’ tumor).Ann Surg. 1938, 108: 885-902.
24- Shamberger RC, Guthrie KA, Ritchey ML, HaaseGM, Takashima J, Beckwith JB, et al. Surgery-relatedfactors and local recurrence of Wilms’ tumor in Na-tional Wilms’ Tumor Study 4. Ann Surg. 1999, 229:292-7.
25- Othersen HB Jr, De Larimer A, Harbovsky E, KelalisP, Breslow N, D'Angio GJ. Surgical evaluation oflymph node metastasis in Wilms tumor. J Pediatr Surg.1990, 25: 330-1.
26- Green DM. The treatment of stages I-IV favorablehistology Wilms’ tumor. J Clin Oncol. 2004, 22: 1366-72.
27- Haase GM. Current surgical management of Wilmstumor. Curr Opin Pediatr. 1996, 8: 268-75.
28- Ritchey ML, Shamberger RC, Haase G, Horwitz J,Bergemann T, Breslow NE, et al. Surgical complica-tions after primary nephrectomy for Wilms’ tumor:Report from the National Wilms’ Tumor Study Group.J Am Coll Surg. 2001, 192 (1): 63-8.
29- Wilimas JA, Magill L, Parham DM, Jerkins G, KumarM, Douglass EC. Is renal salvage feasible in unilateralWilms’ tumor? Proposed computed tomographic cri-teria and their relation to surgico-pathologic findings.Am J Pediatr Hematol Oncol. 1990, 12: 164-7.
30- Wilimas JA, Magill L, Parham DM, Kumar M, Dou-glass EC. The potential for renal salvage in non-metastatic unilateral Wilms’ tumor. Am J PediatrHematol Oncol. 1991, 13: 342-4.
31- Blute ML, Kelalis PP, Offord KP, Breslow N, BeckwithJB, D'Angio GJ. Bilateral Wilms’ Tumor. J Urol. 1987Oct, 138 (4 Pt 2): 968-73.
32- Hogeboom CJ, Grosser SC, Guthrie KA, Thomas PR,D'Angio GJ, Breslow NE. Stature loss followingtreatment for Wilms tumor. Med Pediatr Oncol. 2001,36: 295-304.

423
33- International Society of Pediatric Oncology, Zurich.2001: Nephroblastoma Protocol: SIOP-2001.
34- Mokhlis A, Sami A, Nassar S, Hussein MH. Profileof children cancer in NCI during the period of 1975-1994. NCI, Cairo University. 1995.
35- Abd El-Aal H, Habib EE, Mishrif MM. Wilm's tumor:The experience of the pediatric unit of Kasr El-Ainicenter for radiation oncology and nuclear medicine.J Egypt Natl Cancer Inst. 2005, 17 (4): 308-14.
36- Hung IJ, Chang WH, Yang CP, Jaing TH, Liang DC,Lin KH, et al. Epidemiology, clinical features andtreatment outcome of Wilms tumor in Taiwan: A reportfrom Taiwan Pediatric Oncology group. J FormosMed Assoc. 2004 Feb, 103 (2): 104-11.
37- Yildiz I, Yuksel L, Ozkan A, Apak H, Celkan T,Danismend N, et al. Multidisciplinary approach toWilms tumor: 18-years of experience. Jpn J ClinOncol. 2000, 30 (1): 17-20.
38- Green DM. Wilm's tumor. Eur J Cancer. 1997, 33:409-18.
39- Ahmed H, Ahmed M, Sidhom I, Mohamed G. Survivaland factors that might affect outcome of patients withWilms tumor at NCI. NCI, Cairo University. 2004.
40- Mohsen E, El Shenawy R, Ezz El-Din Z, MohammedL. Evaluation of different regimens in Wilms tumorat Cairo NCI during a 10-years period, NCI, CairoUniversity. 1997.
41- Mahmood A, Ghafoor T, Badsha S. Wilms tumor:Presentation and Treatment. J Coll Physician SurgPak. 2004, 14 (3): 142-5.
42- Pianezza ML, Rubin S, Bass J, Chou S, Pike JG,Leonard MP. Wilm's tumor at the Children's Hospitalof Eastern Ontario. Can J Urol. 2004, 11: 2151-6.
43- Mitchell C, Morris Jones P, Kelsey A, Vujanic GM.The treatment of Wilms tumor: Results of the UnitedKingdom Children's Cancer Study Group 2 (UKCCSG2). Br J Cancer. 2000, 83 (5): 602-8.
44- Green DM. Diagnosis and management of malignantsolid tumors in infants and children. Martinus Nijhoff.1985, 1-552.
45- D' Angio GJ, Breslow N, Beckwith B. Treatment ofWilms tumor. Results of the Third National WilmsTumor Study. Cancer. 1989, 64: 349-60.
46- Ehrlich PF, Ritchey ML, Hamilton TE, Haase GM,Ou S, Breslow NE, et al. Quality assessment for Wilmstumor: A report from the National Wilms Tumor Study-5. J Pediatr Surg. 2005 Jan, 40 (1): 208-12.
47- Jereb B, Burgers JM, Tournade MF, Lemerle J, BeyP, Delemarre J, et al. Radiotherapy in the SIOP (In-ternational Society of Pediatric Oncology) nephro-blastoma studies: A review. Med Pediatr Oncol. 1994,22: 221-7.
48- Kalapurakal JA, Li SM, Breslow NE, Beckwith JB,Macklis R, Thomas PR, et al. Influence of radiationtherapy delay on abdominal tumor recurrence inpatients with favorable histology Wilms tumor treatedon NWTS-3 and -4: A report from the National WilmsTumor Study Group. Int J Radiat Oncol Biol Phys.2003, 57: 495-9.
49- Tournade MF, Com-Nougué C, de Kraker J, LudwigR, Rey A, Burgers JM, et al. Optimal duration of pre-operative therapy in unilateral and non-metastaticWilms tumor in children older than 6 months: Resultsof the Ninth International Society of Pediatric Oncol-ogy Wilms Tumor Trial and Study. J Clin Oncol. 2001,19 (2): 488-500.
50- Dome JS, Liu T, Krasin M, Lott L, Shearer P, DawNC, et al. Improved survival for patients with recurrentWilms tumor: The experience at ST-Jude Children'sResearch Hospital. J Pediatr Hematol Oncol. 2002,24: 192-8.
51- Miser JS, Tournade MF. The management of relapsedWilms tumor. Hematol Oncol Clin North Am. 1995,9: 1287-1302.
52- Seseke F, Zoller G, Ringer RH. Wilms tumor singlecenter experience with renal surgery. Scand J UrolNephrol. 2004, 38 (5): 373-7.
53- Breslow NE, Ou SS, Beckwith JB, Haase GM, Kal-apurakal JA, Ritchey ML, et al. Doxorubicin forfavorable histology, stage II-III Wilms tumor: Resultsfrom the National Wilms tumor Studies. Cancer. 2004,101: 1072-80.
Multidisciplinary Approach to Wilms’ Tumor