multihandicapped blind and partially sighted children in south germany ii: aetiology and...
TRANSCRIPT
MULTIHANDICAPPED BLIND AND PARTIALLY SIGHTED CHILDREN IN SOUTH GERMANY I I : AETIOLOGY AND PATHOGENESIS
~ a r t j f f ~aiis.sl~~ Helniut Barrels Hans-Michae l Strasshitrg
In part I of this study we reported on prevalence and impairments in our popu- lation-based series of multihandicapped blind and partially sighted children and provided some clinical data. We found that these children had a rare but usually a very severe form of multiple impair- ment. It was felt that efforts for preven- tion of these impairments were urgently needed. In the second part of the study data on the aetiology and pathogenesis will be reported.
A prerequisite for a meaningful presen- tation of data on the aetiology of impair- ments is an exact classification system, to permit comparisons with earlier or later studies. For the aetiology of mental retar- dation a very exact classification system was proposed by Gustavson et al. (19770,h). We will propose a similar sys- tem for the classification of the aetiology of visual impairment in multihandicapped blind and partiaHy sighted children.
Methods DATA COLLECTION For the 239 multihandicapped visually impaired children found in part I of the study, all medical records, CT scans and MRI scans were collected. Whenever possible, a detailed paediatric and neuro- paediatric examination was performed by the first author. A history was taken from the parents and/or the caregivers.
All neuropaediatric diagnoses were checked. Addiliona~ inv~stigations were arranged when it seemed appropriate. The same definitions of different impair- ments were used as in part I of this study.
AETIOLOGICAL CLASSIFICATION For &he classification of the origin and the aetiology of the visual impairment the following definitions were used: pre- natal referred to the period before the onset of labour resulting in delivery, perinatal to the period from the onset of labour until the seventh day of life, and postnatal from the eighth day of life up to the age of 4 years. Preterm birth was that occurring before completion of the 37th week of gestation.
The origin of the visual impairment was considered to be obviousIyiprenatal in the case of genetic diseases, malfor- mations and syndromes with malforma- tions, unequivocal prenatal infections, proven intracranial bleeding and hypoxic -ischaemic encephalopathy in the pre; natal period, and disruptions with unknown cause. Obviously postnatal causes were identified in the case of an established damaging event between the second week of life and the fourth birth- day in a child previously considered to be healthy. The origin was suspected to be related to the perinatal period or late gestation in the case of significant

perinatal complications (infections, intracranial bleeding, hypoxic-ischaemic encephalopathy, retinopathy of prematu- rity) or in preterm infants with lesions of the visual pathways. The above- mentioned obviously prenatal and post- natal factors had to bc absent in this group. However, factors related to late gestation could not be excluded in the pathogenesis in many cases, even in the presence of severe perinatal complica- tions. In all other children the origin was classified as unknown.
Hypoxic-ischaemic encephalopathy in tcrm newborn infants was diagnosed when there had been severe perinatal asphyxia followed by neonatal convul- sions, apathy. severe hypotonia, severe feeding disturbances, severe dysfunc; tions of organs or a flat EEG in the neonatal period and when the above- mentioned obviously prenatal or post- natal causes were absent.
For the aetiology of mental retardation the classification system proposed by Gustavson et a / . ( 1977a.h) was used.
STATIST~CS In some instances the x' test 'Trends in proportions' (Armitage and Berry 1987) was used for statistics. These statistics were not meant inferentially but descriptively.
Results AETIOLOGY OF VISUAL IMPAIRMENT A total of 239 children were found who met all the inclusion criteria. One hun- dred and sixty children were examined by the first author. The different aetiologies of visual impairment in these children and their frequencies are shown in Table I. The origin was classified as unknown in 29 children (12%), and could not be traced owing to insufficient data in seven further children. In all other children an origin in one of the three major aetiolog- ical periods was determined.
In 69 children (29%) the origin of visual impairment was obviously pre- natal. Among them, 26 children ( 1 1%) had genetic conditions and 17 children (7%) prenatally acquired lesions. In a further 26 children ( 1 1 %) the prenatal cause was unknown, i.e. it was not evi- dent to what extent the visual impairment
could be explained by genetic or prena- tally acquired factors.
Among the genetic causes, 11 chromo- somal aberrations (5%) were found. Three children had Down syndrome one of whom had cerebral visual impairment and two of whom had congenital cataract. Four children had 4p- syn- drome. The other children had rare struc- tural chromosomal aberrations. Eleven children ( 5 % ) had conditions caused by mutant genes, mostly rare autosomal- recessive metabolic disorders. One child had oculocutaneous albinism combined with an unknown encephalopathy. Three children had tuberous sclerosis: two of whom had extensive intracranial lesions and one of whom had congenital vitreous bleeding. Four children had genetic dis- orders with unknown modes of inheri- tahce, namely congenital glaucoma, congenital cataract with microphthalmus (Capella er a / . 1963, Temtamy and Shalash 1974) and an unknown disorder in two siblings.
Among the 17 prenatally acquired lesions, five prenatal infections (congen- ital toxoplasmosis or congenital cyto- megalovirus infection) were found. Congenital rubella did not occur. One child had a complex of giant-cell hepati- tis and aseptic meningitis in the first few weeks of life combined with optic nerve hypoplasia. This complex, whose origin was probably infective, has been described by Johnsen et 01. ( 1976). Two children had intraventricular haemor- rhage whose prenatal origin was proven. Two children (one term, one preterm - born at 36 weeks gestational age) had an uncomplicared delivery and neonatal period and later were found to have penventricular leukomalacia and cerebral visual impair- ment. Hypoxic-ischaemic encephalopathy in late gestation was suspected in these children (Krageloh-Mann et al. 1992). Four children were born after the intra- uterine death of a co-twin and were later found to have optic nerve atrophy or cerebral visual impairment and multicys- tic encephalomalacia. A vascular disrup- tion was suspected in these children (Larroche et a/ . 1990). Three children had disruptions with unknown cause: they had hydranencephaly or severe porencephaly after an uncomplicated 1077
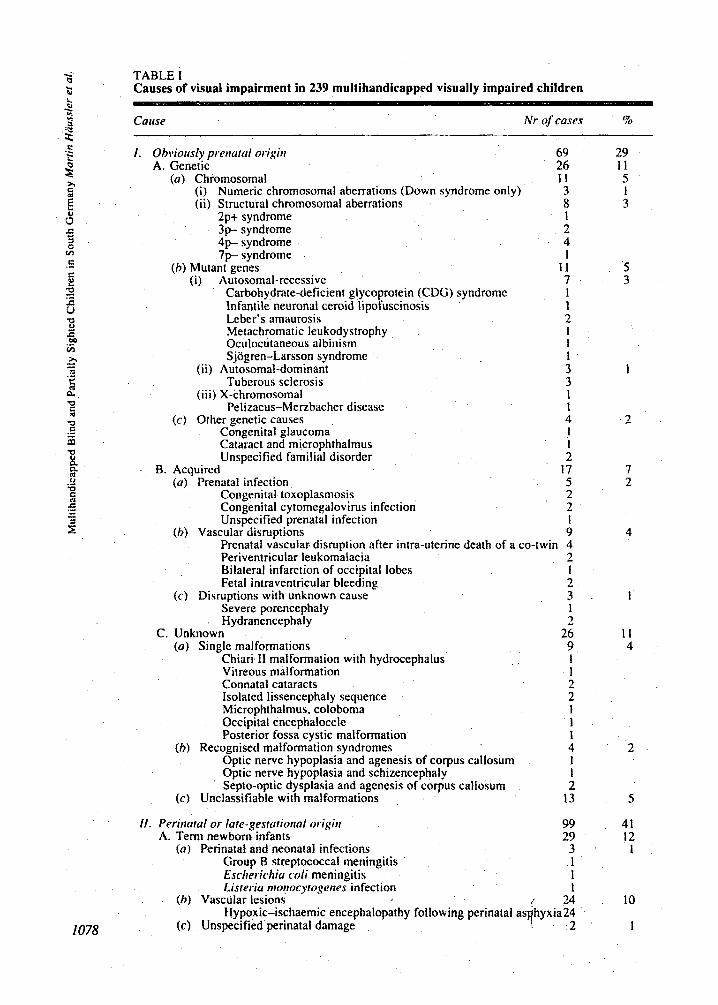
TABLE I Causes of visual impairment in 239 multihandicapped visually impaired children
Cause Nr of cases
1. Obvioirsly prewtul origin 69 A. Genetic 26
(a) Ch~mosomal I 1 (i) Numeric chromosomal aberrations (Down syndrome only) 3 (ii) Structural chromosomal aberrations 8
2p+ syndrome 1 3p syndrome 2 4 p syndrome 4 7 p syndrome 1
(b ) Mutant genes I 1 (i) Autosomal-recessive 7
Carbohydrate-de~cient glycoprotein (CDG) syndromc 1 Infantile neuronal ceroid lipofuscinosis 1 Leber’s amaurosis 2 Metachromatic leukodystrophy 1 Oculocutaneous albinism 1 Sjogren-Larsson syndrome 1
(ii) Autosomal-dominant 3 Tuberous sclerosis 3
(i i i) X-chromosomal 1 Pelizaeus-Menbacher disease 1
(c) Other genetic causes 4 Congenital glaucoma I Cataract and microphthalmus 1 Unspecified familial disorder 2
B. Acquircd 17 (a) Prenatal infection 5
Congenital toxoplasmosis 2 Congenital cytomegalovirus infection 2 Unspecified prenatal infection 1
(h) Vascular disruptions 9 Prenatal vascular- disruption after intra-uterine death of a co-twin 4 Periventricular leukomaiacia 2 Bilateral infarction of occipital lobes 1 Fetal intraventricular bleeding 2
( c ) Disruptions with unknown cause 3 Severe porencephaly 1 H ydranencephal y 2
C. Unknown 26 (a) Single malformations 9
Chiari I1 ma~formation with hydr~ephalus 1 Vitreous malformation 1 Connatal cataracts 2 Isolated lissencephaly sequence 2 Microphthalmus, coloboma 1 Occipital encephalocele 1 Posterior fossa cystic malformation i
(h ) Recognised malformation syndromes 4 Optic nerve hypoplasia and agenesis of corpus callosum Optic nerve hypoplasia and schizencephaly Septo-optic dysplasia and agenesis of corpus callosum
1 1 2
(c ) Unclassifiable with malformations 13
%
29 1 1 5 1 3
5 3
1
2
7 2
4
1
1 1 4
2
5
11. Perinaral or late-gestatiorial origin 99 41 A. Term newborn infants 29 12
(a) Perinatal and neonatal infections 3 . 1 Group B streptococcal meningitis 1 Escherichia c d i meningitis 1 Listeriu nrorrocytogenes infection 1
(h) Vascular lesions / 24 10 Hypoxic-ischdemic encephaiopathy following perinatal as hyxia24
(c) Unspecified perinatal damage 4 2 1
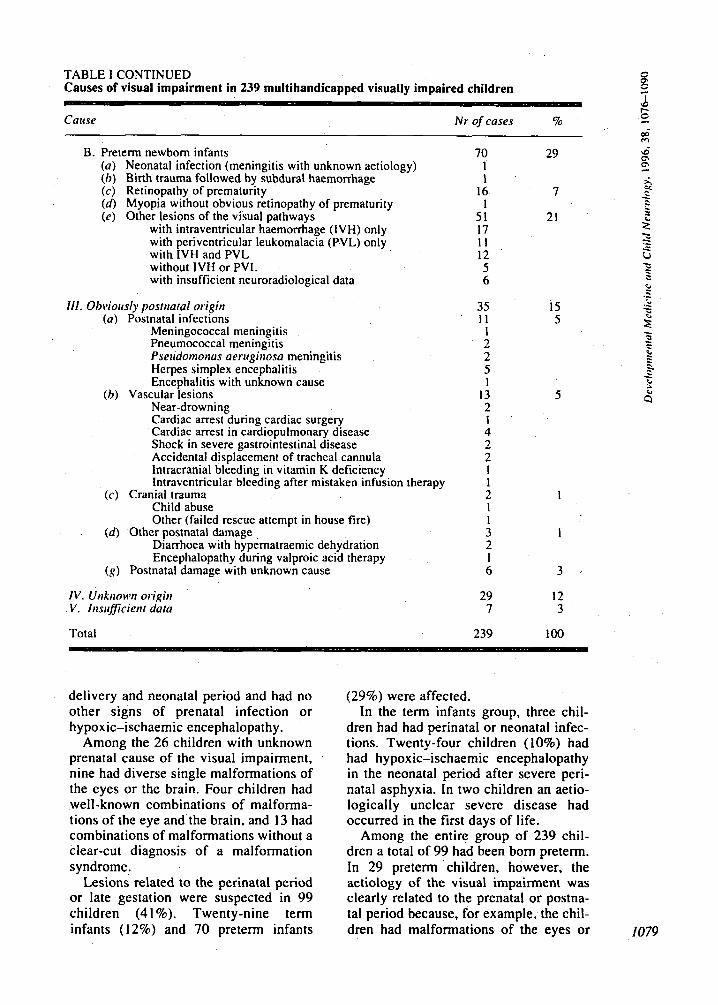
TABLE I CONTINUED Causes of visual impairment in 239 multihandicapped visually impaired children
Cause Nr of cases lo
B. Preterm newborn infants (a) Neonatal infection (meningitis with unknown aetiology) (b ) Birth trauma followed by subdural haemorrhage ( c ) Retinopathy of prematurity (d) Myopia without obvious retinopathy of prematurity ( e ) Other lesions of the visual pathways
with intraventricular haemorrhage (IVH) only with periventricular leukomalacia (PVL) only with IVH and PVL without IVH or PVL with insufficient neuroradiological data
Ill. Obviously postnatal origin ( a ) Postnatal infections
Meningococcal meningitis Pneumococcal meningitis P seirdomonas aeniginosa meningitis Herpes simplex encephalitis Encephalitis with unknown cause
Near-drowning Cardiac arrest during cardiac surgery Cardiac arrest in cardiopulmonary disease Shock in severe gastrointestinal disease Accidental displacement of tracheal cannula Intracranial bleeding in vitamin K deficiency Intraventricular bleeding after mistaken infusion therapy
Child abuse Other (failed rescue attempt in house fire)
(d) Other postnatal damage Diarrhoea with hypematraemic dehydration Encephalopathy during valproic acid therapy
(h) Vascular lesions
(c) Cranial trauma
( g ) Postnatal damage with unknown cause
IV. Unkrionvi origin V . Itisrificient data
Total
70 29 1 1
16 1
51 17 I I 12 5 6
7
21
35 15 1 1 5
1 2 2 5 1
13 2 1 4 2 2 1 1 2 1 1 I 3 1 2 1 6 3 ,
5
29 12 7 3
239 I 0 0
i m
p 0
delivery and neonatal period and had no other signs of prenatal infection or hypoxic-ischaemic encephalopathy.
Among the 26 children with unknown prenatal cause of the visual impairment, nine had diverse single malformations of the eyes or the brain. Four children had well-known combinations of malforma- tions of the eye and the brain, and 13 had combinations of malformations without a clear-cut diagnosis of a malformation syndrome.
Lesions related to the perinatal period or late gestation were suspected in 99 children (41 %). Twenty-nine term infants (12%) and 70 preterm infants
(29%) were affected. In the term infants group, three chil-
dren had had perinatal or neonatal infec- tions. Twenty-four children (10%) had had hypoxic-ischaemic encephalopathy in the neonatal period after severe peri- natal asphyxia. In two children an aetio- logically unclear severe disease had occurred in the first days of life.
Among the entire group of 239 chil- dren a total of 99 had been born preterm. In 29 pretenn children, however, the aetiology of the visual impairment was clearly related to the prenatal or postna- tal period because, for example, the chil- dren had malformations of the eyes or 1079
C .- C r 2 .- if
U C .- d a
1080
Bi~hweight
3500 female
(9)
3000 1 mate 2500
0 1500
0
1000 t P U
500 ’ 24 26 28 30 32 34 36 38
Gestational age (wks)
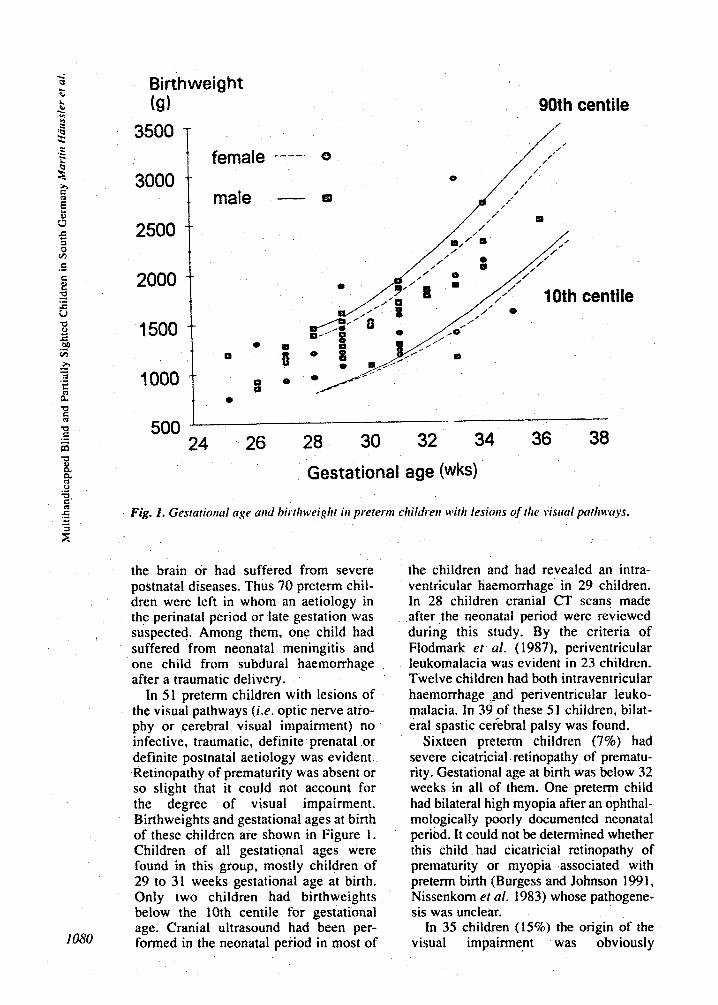
Fig. 1, Gesratiorial age arid hirtlrweighr iri prererni children with lesioris of the sisitul patltwuys,
the brain or had suffered from severe postnatal diseases. Thus 70 preterm chi1- dren were left in whom an aetiology in the perinatal period or late gestation was suspected. Among them, one child had suffered from neonatal meningitis and one child from subdural haemorrhage after a traumatic delivery.
In 51 preterm children with lesions of the visual pathways (i.e. optic nerve atro- phy or cerebral visual i m p a i ~ e n t ) no infective, traumatic, definite prenatal or definite postnatal aetiology was evident. Retinopathy of prematurity was absent or so slight that it could not account for the degree of visual impairment. Birthweights and gestational ages at birth of these children are shown in Figure 1. Children of all gestational ages were found in this group, mostly children of 29 to 31 weeks gestational age at birth. Only two children had birthweights below the 10th centile for gestational age. Cranial ultrasound had been per- formed in the neonatal period in most of
the children and had revealed an intra- ventricular haemo~hage in 29 children. In 28 children cranial CT scans made after the neonatal period were reviewed during this study. By the criteria of Flodmark et al. (1987), periventricular leukomalacia was evident in 23 children. Twelve children had both intraventricuiar haemorrhage .and periventricular leuko- malacia. In 39 of these 51 children, bilat- eral spastic cerebra1 palsy was found.
Sixteen preterm children (7%) had severe cicatricial retinopathy of prematu- rity. Gestational age at birth was below 32 weeks in all of them. One preterm child had bilateral high myopia after an ophthal- motogically poorly documented neonatal period. It could not be determined whether this child had cicatricial retinopathy of prematurity or myopia associated with preterm birth (Burgess and Johnson 1991, Nissenkorn et al. 1983) whose pathogene- sis was unclear.
In 35 children (15%) the origin of the visual impairment was obviously
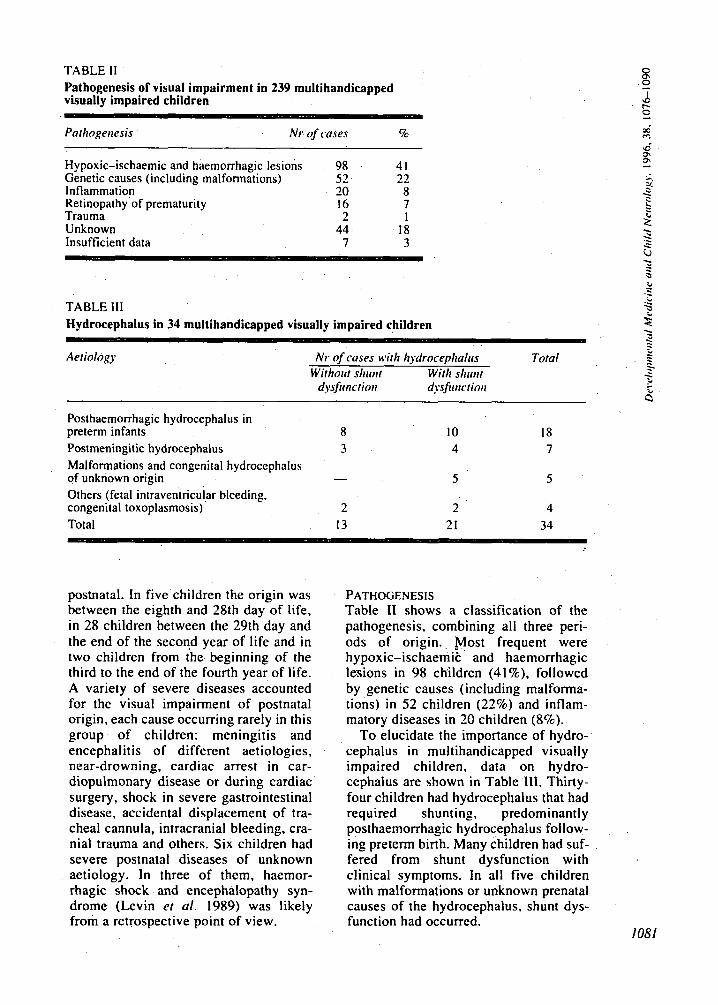
TABLE I1 Pathogenesis of visual impairment in 239 multihandicapped visually impaired children
Pathogemsis . Nrof cases '70
8 .o
Hypoxic-ischaemic and haemorrhagic lesions 98 41 Genetic causes (including malformations) 52 22 Inflammation 20 8 Retinopathy of prematurity 16 7 Trauma 2 1 Unknown 44 18 Insufficient data 7 3
w
TABLE 111 3 Hydrocephalus in 34 multihandicapped visually impaired children 2 - v
c - Aeriology Nr of cases wilh liydrocephalirs
Wirhoirt sliiuit With slimit Total
dysfiiricriori dysfirnctiori r
w
B Posthaemorrhagic hydrocephalus in preterm infants 8
Malformations and congenital hydrocephalus
Others (fetal intraventricular bleeding.
Total 13
Postmeningitic hydrocephalus 3
of unknown origin -
congenital toxoplasmosis) 2
10 18 4 7
5 5
2 4 21 34
postnatal. In five children the origin was between the eighth and 28th day of life, in 28 children between the 29th day and the end of the second year of life and in two children from the beginning of the third to the end of the fourth year of life. A variety of severe diseases accounted for the visual impairment of postnatal origin, each cause occurring rarely in this group of children: meningitis and encephalitis of different aetiologies, near-drowning, cardiac arrest in car- diopulmonary disease or during cardiac surgery, shock in severe gastrointestinal disease, accidental displacement of tra- cheal cannula, intracranial bleeding, cra- nial trauma and others. Six children had severe postnatal diseases of unknown aetiology. In three of them, haemor- rhagic shock and encephalopathy syn- drome (Levin et a / . 1989) was likely from a retrospective point of view.
PATHOGENESIS Table I1 shows a classification of the pathogenesis, combining all three peri- ods of origin.. Most frequent were hypoxic-ischaemit and haemorrhagic lesions in 98 children (41%), followed by genetic causes (including malforma- tions) in 52 children ( 2 2 8 ) and inflam- matory diseases in 20 children (8%).
To elucidate the importance of hydro- cephalus in multihandicapped visually impaired children, data on hydro- cephalus are shown in Table 111. Thirty- four children had hydrocephalus that had required shunting, predominantly posthaemorrhagic hydrocephalus follow- ing preterm birth. Many children had suf- fered from shunt dysfunction with clinical symptoms. In all five children with malformations or unknown prenatal causes of the hydrocephalus. shunt dys- function had occurred.
1081
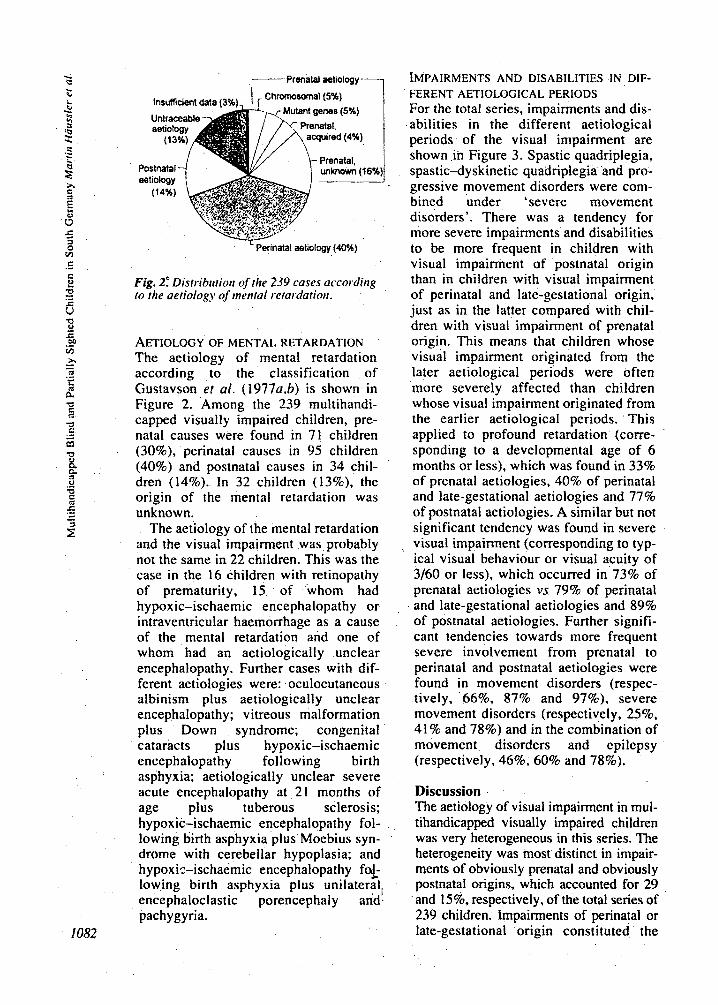
I ,------ Prenalal aetiology
7.. Perinatal aetiology (40%)
Fig. 2.“ ~is~ribii t i t~tt of the 239 cases according to the aetiology of mentul r-etardatioti.
AETIOLOGY OF MENTAL RETARDATION The aetiology of mental retardation according to the classification of Gustavson ef ai. (1977a,b) is shown in Figure 2. Among the 239 multihandi- capped visually impaired children, pre- natal causes were found in 71 children (30%), perinatal causes in 95 children (40%) and postnatal causes in 34 chil- dren (14%). In 32 children (13%), the origin of the mental retardation was unknown.
The aetiology of the mental retardation and the visual impairment was probably not the same in 22 children. This was the case in the 16 children with retinopathy of prematurity, 15 of whom had hypoxic-ischaemic encephalopathy or intraventricular haemorrhage as a cause of the mental retardation and one of whom had an aetiologically unclear encephalopathy. Further cases with dif- ferent aetiologies were: oculocutaneous albinism plus aetiologically unclear encephalopathy; vitreous malformation plus Down syndrome; congenital cataracts plus hypoxic-ischaemic encephalopathy following birth asphyxia; aetiolo~ically unclear severe acute encephalopathy at 21 months of age plus tuberous sclerosis; hypoxic-ischaemic encephalopathy fol- lowing birth asphyxia plus Moebius syn- drome with cerebellar hypoplasia; and hypoxiz-ischaemic encephalopathy f%- lowing birth asphyxia plus unilateral, encephaloclastic porencephaly and. pachygyria.
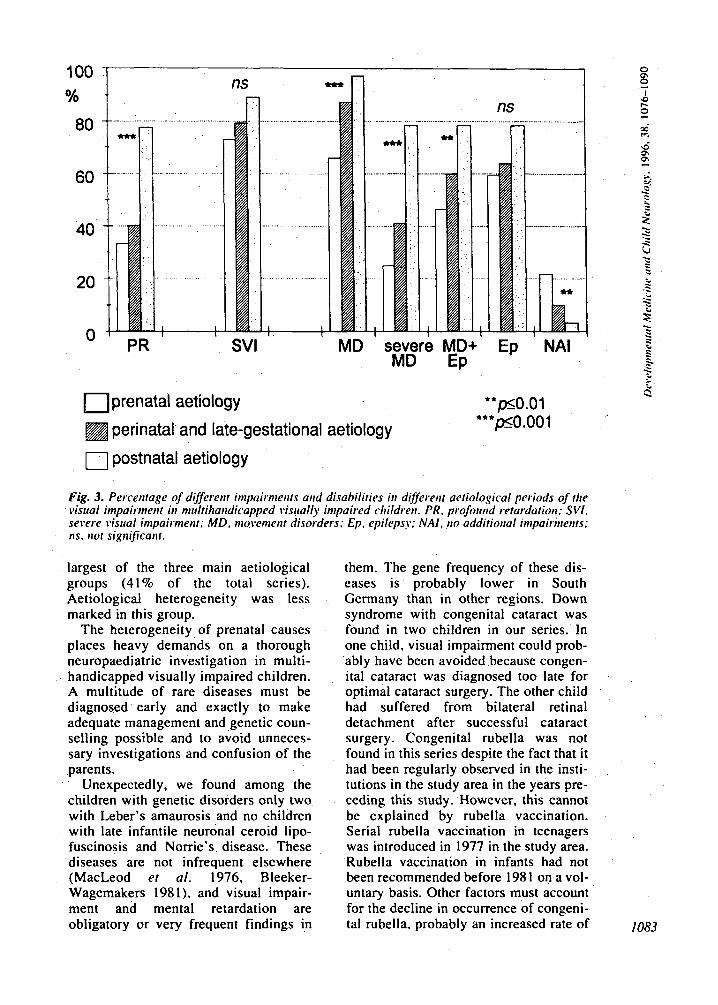
IMPAIRMENTS AND DISABILITIES IN DIF- FERENT AETIOLOCICAL PERlODS For the total series, impairments and dis- abilities in the different aetiological periods of the visual impairment are shown in Figure 3. Spastic quadriplegia, spastic-dyskinetic quadriplegi~ and pto- gressive movement disorders were com- bined under ‘severe movement disorders’. There was a tendency for more severe impairments and disabilities to be more frequent in children with visual impairment of postnatal origin than in children with visual impairment of perinatal and late-gestational origin, just as in the latter compared with chil- dren with visual impairment of prenatal origin. This means that children whose visual i m p a i ~ e n t originated from the later aetiological periods were often more severely affected than children whose visual impairment originated from the earlier aetiological periods. This applied to profound retardation (corre- sponding to a developmental age of 6 months or less), which was found in 33% of prenatal aetiologies, 40% of perinatal and late-gestational aetiologies and 77% of postnatal aetiologies. A similar but not significant tendency was found in severe visual impairment (corresponding to typ- ical visual behaviour or visual acuity of 3/60 or less), which occurred in 73% of prenatal aetiologies vs 79% of perinatal and late-gestational aetiologies and 89% of postnatal aetiologies. Further signifi- cant tendencies towards more frequent severe involvement from prenatal to perinatal and postnatal aetiologies were found in movement disorders (respec- tively, 66%, 87% and 97%). severe movement disorders (respectively, 25%. 41 % and 78%) and in the combination of movement disorders and epilepsy (respectively. 46%, 60% and 78%).
Discussion The aetiology of visual impairment in mul- tihandicapped visually impaired chitdren was very heterogeneous in this series. The heterogenei~ was most distinct in impair- ments of obviously prenatal and obviously postnatal origins, which accounted for 29 and 15%, respectively, of the total series of 239 children. Impairments of perinatal or late-gestational origin constituted the
ns mn 100 .I % t
60
40
20
0
- n I I
SVI MD severe MD
prenatal aetiology
perinatal and late-gestational aetiology
0 postnatal aetiology
MD+' Ep ' NAI EP
Fig. 3. Percentage of differetit inipairnients atid disabilities h different aetiological periods of the visual impairmetit iii niitltiliatidicapped visitally impaired childreii. PR. profoirnd retcrrdatioti: SVI. severe visual inioairnienr: MD. niovenieiit disorders: Ep. epilepsy: N A I , no additiotial inipairnierits; ns. iiot signififah.
largest of the three main aetiological groups (41% of the total series). Aetiological heterogeneity was less marked in this group.
The heterogeneity of prenatal causes places heavy demands on a thorough neuropaediatric investigation in multi- handicapped visually impaired children. A multitude of rare diseases must be diagnosed early and exactly to make adequate management and genetic coun- selling possible and to avoid unneces- sary investigations and confusion of the parents.
Unexpectedly, we found among the children with genetic disorders only two with Leber's amaurosis and no children with late infantile neuronal ceroid lipo- fuscinosis and Norrie's disease. These diseases are not infrequent elsewhere (MacLeod ef al. 1976, Bleeker- Wagemakers 1981). and visual impair- ment and mental retardation are obligatory or very frequent findings in
them. The gene frequency of these dis- eases is probably lower in South Germany than in other regions. Down syndrome with congenital cataract was found in two children in our series. In one child, visual impairment could prob- ably have been avoided because congen- ital cataract was diagnosed too late for optimal cataract surgery. The other child had suffered from bilateral retinal detachment after successful cataract surgery. Congenital rubella was not found in this series despite the fact that it had been regularly observed in the insti- tutions in the study area in the years pre- ceding this study. However, this cannot be explained by rubella vaccination. Serial rubella vaccination in teenagers was introduced in 1977 in the study area. Rubella vaccination in infants had not been recommended before 198 1 on a vol- untary basis. Other factors must account for the decline in Occurrence of congeni- tal rubella. probably an increased rate of 1083
abortion after its prenatal diagnosis. Among the children with perinatal or
late-gestational origin of visual impair- ment, we found 5 1 preterm children with lesions of the visual pathways without infective, obviously prenatal or obvi- ously postnatal causes. This was the sin- gle largest diagnostic group in the total series of 239 children. There is much evidence that periventricular Ieukomala- cia is the most important pathogenetic factor in this group. It was found in 23 of 28 children in whom cranial CT or MRI scans were reviewed. The association of periventricular leukomalacia and visual impairment is supported by many data from other studies. First, neuropatholog- ical investigations in periventricular leukomalacia frequently found the optic radiation to be involved (Banker and Lanoche 1962, Shuman and Selednik 1980). Secondly, neonatal cranial ultra- sound examinations in cystic periven- tricular leukomalacia frequently showed the cysts to be located adjacent and lat- eral to the occipital horns of the lateral ventricles, i.e. the site of the optic radia- tion (Shortland ef n/ . 1988, Rogers ef ul. 1994). Lastty, in foIIow-up examina- tions of preterm infants with cystic periventricular leukomalacia, visual impairment has been found in a consid- erable proportion of the children (Fawer et uf. 1987, Eken ef (11. 1994, Rogers et a / . 1994).
Owing to the retrospective nature of our study, neonatal cranial ultrasound examinations had not been performed in a standardised fashion. We cannot exclude the possibili~y that periventricu- lar cysts were already present in the first days of life in some children, which would have been a strong hint of antena- tal brain damage (Bejar et af. 1988). We must therefore take into account that in some of the above-mentioned 5 1 preterm infants brain damage had occurred in m e w . i.c. in late gestation. Future epi- demiological studies should include stan- dardised cranial ultrasound examinations in the first days of life in preterm infants.
A peculiar finding was that among the 51 preterm children there was no excess of children with extremely low gesta- tional age. The proportion of children with gestational ages below 29 weeks, 29
to 31 weeks and 32 to 36 weeks was 1 : 1.64: 1. In the Bavarian Neonatal Survey, which in 1987 covered 72% of all neonates in paediatric care in Bavaria, the corresponding proportion was 1:1.68:13.12 (Riegel and Thieme 1989). This is in accordance with data from neuropathological as well as ultrasound studies, which (in contrast with intraven- tricular haemorrha~e) found most cases of periventricular leukomalacia in infants of more than 29 weeks postmen- strual age (De Reuck and Van der Eecken 1983, De Vries el a / . 1988). De Reuck and' Van der Eecken (1983) explained their findings by the develop- ment of the fetal cerebral vasculature. In the earlier stages of the development of the vascuIature. fhe vascular rete of the germinal matrix is predisposed to intra- ventricular haemonhage. When the ger- minal matrix has regressed, periventricular arterial border zones are formed that predispose to periventricular leukomalacia.
In contrast, severe cicatricial retinopa- thy of prema~urity was found only in preterm infants of less than 32 weeks gestational age in this series. This is in accordance with data from other studies that showed that retinopathy of prematu- rity has remained a problem only in small preterm infants (Seiberth and Linderkamp 1989, Gibson cf a/ . 1990).
Congenital cataract was found in only four children in this series. This is cer- tainly due to the success of modern cataract surgery. Two of these children had Down syndrome, one child had con- genital cataract with microphtha~mus and one child had congenital cataract of unknown cause and hypoxic-ischaemic encephalopathy in the neonatal period. Cataracts were not observed in preterm infants. Several authors have commented on preterm birth and perinatal complica- tions as a cause of permanent infantile cataract (Fraser and Friedman 1967, Bleeker-Wagemakers 198 1). Like Pike et ul. (1989) we question the concept of 'cataract of perinatal aetiofogy' and 'cataract of preterm birth' on the basis of our findings.
In the total series of 239 children, 34 had hydrocephalus that had required shunting. The distribution of aetiologies
.
among these 34 children was markedly different from that found by Fernell et a / . (1987a,h) in a population-based study of hydrocephalus in Sw‘eden. In our group of 34 multihandicapped visually impaired children with hydrocephalus, 18 children had hydrocephalus due to intraventricular haemorrhage after preterm birth. This was found in only 9% of the children in the study of Fernell et al. In contrast, only nine of 34 children had hydrocephalus of prenatal origin in our series, compared with 49% of the children in the study of Fernell et a / . Consequently, there was an excess of children with posthaemorrhagic hydro- cephalus after preterm birth in our series compared with a population-based unse- lected series of children with hydro- cephalus. Many of the children in our group of 34 visually impaired multihand- icapped children with hydrocephalus had suffered from shunt dysfunction. We conclude that uncomplicated hydro- cephalus was not an important factor in the pathogenesis of the visual impair- ment of the children of our series. In multihandicapped visually impaired chil- dren with hydrocephalus, the visual impairment was probably due to underly- ing brain damage rather than to hydro- cephalus.
An important question is whether there are different aetiological distribu- tions in other population-based studies on handicapped children. A meaningful comparison will require that similar classification systems were used. A dis- tribution of major aetiological groups very similar to that in our series of 239 multihandicapped visually impaired children was found by Edebol-Tysk et al. (1989) in spastic quadriplegia. another example of severe multiple impairments. In that study an obviously prenatal origin was found in 23% of the quadriplegic children, prenatal and peri- natal risk factors were found in 41%. an obviously postnatal origin in 18% and an unknown origin in 12%. Owing to the similar aetiological classification this compares well with the distribution in our series: obviously prenatal origin in 29%. perinatal or late-gestational origin in 41%, postnatal origin in 15%. and unknown origin in 12%.
Another good comparison is possible with the studies of Blomquist et al. (1981) and Hagberg et al. (1981) on mild mental retardation and by Gustavson et al. (1977a.h) and McQueen et al. ( 1986) on severe mental retardation because we have used the same system of classifica- tion of the aetiology of mental retarda- tion in our series. The data are summarised in Table IV. Prenatal causes were most prominent in severe mental retardation, whereas perinatal and post- natal causes were more important in our series than in the studies on mild and severe mental retardation. From a mod- em perspective it must be added, for rea- sons we have described above, that ‘perinatal origin’ in the classification of Gustavson et a / . is better understood in the sense of ‘perinatal or late-gestational origin’ as defined in our classification of the origin of the visual impairment. There is a shortcoming in most of the studies mentioned on the aetiology of mental retardation: methods for neurora- diological investigations were rather lim- ited at the time of these studies. Therefore some diagnoses such as that of brain malformations, which are best made by neuroradiology, might have been overlooked in these studies. This might have resulted in an underestimate of prenatal aetiologies in these studies.
An interesting comparison was made by Rosenberg et a/ . (1992) in a register- based study of visual impairment in sev- eral Scandinavian countries. They used a similar classification to ours for the aeti- ology of visual impairment, and com- pared the aetiological distribution in children with isolated visual impairment and in children with visual impairment and additional impairments. In the chil- dren with isolated visual impairment, prenatal aetiologies were more promi- nent than in the multihandicapped chil- dren. The reverse was true for perinatal and postnatal aetiologies.
The data from the different studies underline the importance of perinatal. late-gestational and postnatal factors in the aetiopathogenesis of severe multiple impairments such as spastic quadriplegia and multiple handicap with visual impairment. A correlation between severity of impairment and aetioloev was 1085
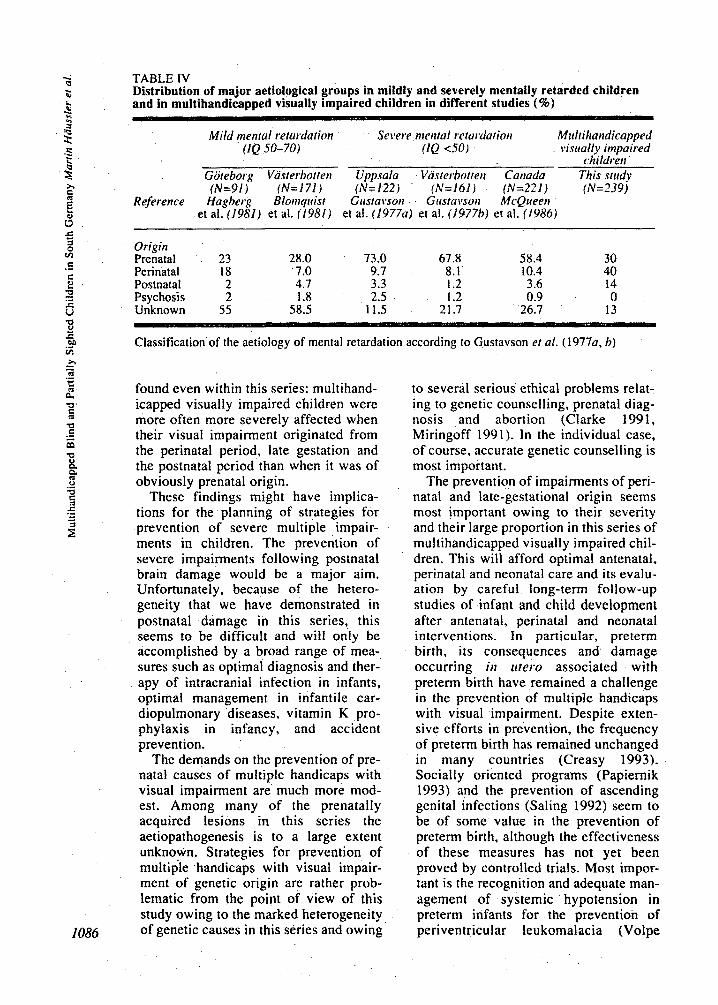
TABLE IV Distribution of major aetiological groups in mildly and severely mentally retarded children and in multihandicapped visually impaired children in different studies (%)
Mild nteiitul returdation Severe ntetital rctardatiott Mi~lti~taiid~cap~ed (1Q 50-70) ClQ 4 0 1 visitally impaired
~h~ldse i i Goteborg Vasterbotreti Uppsala Vastesbotteii Cartada This snidy (N=91) {N=171) (N=122) (N=161) (N=221) fN=239)
Reference Hagberg Blortiqirist Girstavsort Girstavsoii McQueeti et al. (1981) et al. (I9811 et al. (1977a) et al. (197761 et al. (1986)
Origin Prenatal 23 28.0 73.0 67.8 58.4 30 Perinatal 18 7.0 9.7 8.1 10.4 40 Postnatal 2 4.7 3.3 1.2 3.6 i4
Unknown 55 58.5 11.5 21.7 26.7 13 Psychosis 2 1.8 2.5 I .2 0.9 0
~ _ _ ~ - -
Classification of the aetiology of mental retardation according to Gustavson et al. (1977a, b)
found even within this series: multihand- icapped visually impaired children were more often more severely affected when their visual impairment originated from the perinatal period, late gestation and the postnatal period than when it was of obviously prenatal origin.
These findings might have implica- tions for the planning of strategies for prevention of severe multiple impair- ments in children. The prevention of severe impairments following postnatal brain damage would be a major aim. Unfo~unately, because of the hetero- geneity that we have demonstrated in postnatal damage in this series, this seems to be difficult and will only be accomplished by a broad range of mea- sures such as optimal diagnosis and ther- apy of intracranial infection in infants, optimal management in infantile car- diopulmonary diseases, vitamin K pro- phyiaxis in infancy, and accident prevention.
The demands on the prevention of pre- natal causes of multiple handicaps with visual impairment are much more mod- est. Among many of the prenatally acquired lesions in this series the aetiopathogenesis is to a large extent unknown. Strategies for prevention of multiple handicaps with visual impair- ment of genetic origin are rather prob- lematic from the point of view of this study owing to the marked heterogeneity of genetic causes in this series and owing
to several serious ethical problems relat- ing to genetic counselling, prenatal diag- nosis and abortion (Clarke 1991, Miringoff 199 1). In the individual case, of course, accurate genetic counselling is most important.
The prevention of impairments of peri- natal and late-gestational origin seems most important owing to their severity and their large proportion in this series of multihandicapped visually impaired chil- dren. This will afford optimal antenatal, perinatal and neonatal care and its evalu- ation by careful long-term follow-up studies of infant and child development after antenatal, perinatal and neonatal interventions. In particular, preterm birth, its consequences and damage occurring in liter0 associated with preterm birth have remained a challenge in the prevention of multiple handicaps with visual impairment. Despite exten- sive efforts in prevention, the frequency of preterm birth has remained unchanged in many countries (Creasy 1993). Socially oriented programs (Papiernik 1993) and the prevention of ascending genital infections (Saling 1992) seem to be of some value in the prevention of preterm birth, although the effectiveness of these measures has not yet been proved by controlled triais. Most impor- tant is the recognition and adequate man- agement of systemic hypotension in preterm infants for the prevention of periventricular leukomalacia (Volpe
1990). which was so frequently found in this series. In addition, further research into *Martin Haussler. MD. Fruhdiagnosezentrum Wiirzburg, Centre for Children With
the antenatal factors associated with Developmental Disorders and Handicaps:
Alltlrors' AppoinfmIt .q
periventricular leukornalacia is mandatory. Helmui Barteh MD; Hans-Michael Strassburg, MD: Department of Pediatrics. University of Wiirzburg: Wurzburg, Federal Republic of Germany.
Accepted for prrblication 201lr Morclr I996
Ackiron~ledQemeirts This study'iparts 1 and 11) was supported by grants
Bayerisches Staatsministcrium fur Arbeit. Strasse 2, D97080 Wiirzburg. Federal Republic of Sozialordnunc. Familie. Frauen und Gesundheit. It
CorresPofldeIlce rofir.qr altrhor from the FaunStiftung. Nurcmberg, and the Friihdiagnosezentrum Wiirzburg, Josef-Schneider-
would not h a k been possible without the extensive help of a large number of parents and professionals.
SUMMARY The results of a classification of the aetiology of visual impairment and mental retardation in a series of 239 multihandicapped blind and partially sighted children are reported. These children had been born between 1981 and 1987 and were examined in a population-based study in South Germany. There was marked aetiological heterogeneity. Most prominent were causes related to the perinatal period and late gestation which were found in 41% of the children. Among these. lesions of the visual pathways in preterm children were especially frequent and could be explained by periventricular leukomalacia in a large proportion. The distribution of the major aetiologic groups is different from populations with isolated mental retardation and populations with isolated visual impairment but similar to a Swedish population with spastic quadriplegia. The implications for the prevention of severe multiple impairments in children are discussed.
RESUME Enfants niiiItiliondicapPs areiigles oii nialr~oyariis en Allemagrie dii Siid. I I : Eiiologie et pathoghie L'article rapporte les rtsultats d'une classification de I'Ctiologie de troubles visuels et retards mentaux i partir d'une etude de population en Allemagne du sud, portant sur 239 enfants multihandica@s, aveugles ou malvoyants, nCs entre 1981 et 1987. I I fut constate une hetCrogCnCit6 etiologique marquCe. En premier lieu (chez 41% des enfants) se situaient les causes reliies a la @riode perinatale et de la fin de grossessc. Parmi ces cas. les lesions des voies visuelles chez les prkmatures etaient particulikrement frkquentes et souvent explicables par une leucomalacie pkriventriculaire. La distribution des groupes etiologiques majeurs Ctait diffkrente de celle d'une population avec retard mental isole et d'une population avec troubles visuels isolCs mais comparable A cellc d'une population suedoise de tktraplkgiques spastiques. Les implications pour la prevention des troubles sevtres multiples chez I'enfant sont discutes.
ZUSAMMENFASSUNG Mehifachheliinderte hliride h x . seliheliiriderte Kirider iri Siidderitscliland. Il: Atiologie litid Patliogenese Von 239 mehrfachbehinderten blinden bzw. sehbehindeven Kindern. die in den Jahren 1981 bis 1987 geboren wurden, werden die im Rahmen einer Bevolkerungsbezogencn Studie in Siiddeutschland erhobenen Ergebnisse einer Klassifikation der Atiologie von Sehbehinderungen und geistiger Retardierung beschrieben. Es find sich eine auffsllige atiologische Heterogenitat. Am haufigsten (bei 4 1% der Kinder) waren Ursachen der Perinatal- und spaten Gestationsperiode. Von diesen waren die Lasionen der Sehbahnen bei Friihgeborenen besonders haufig und konnten oft durch periventrikulare Leukomalazie erklart werden. Die Vetteilung der wichtigsten Atiologiegruppen unterscheidet sich von der bei Patienten mit isolierter geistiger Retardierung und isolierter Sehbehinderung. ahnelt aber der einer schwedischen Population mit spastischer Tetraplegie. Die Autoren diskutieren die Moglichkeiten. wie schwere Mehrfachbehinderungen bei Kindern zu vermeiden sind.
RESUMEN NiAos con niiiltiples dificierrcias. ciegos o parcialnierite ridetries err el siir de Alemania. I! Eiiologia y patoghesis Se aportan 10s resultados de una clasificaci6n de la etiologia de la alteracidn visual y retraso mental en un estudio de poblaci6n en el sur de Alemania de 239 niiios con mliltiples deficiencias. ciegos o parcialmente videntes. nacidos entre I98 1 y 1987. Habia una marcada heterogeneidad etiologica. Las miis prominentes (en 41% de niiios) eran causas relacionadas con el period0 perinatal y el final de la gestaci6n. Entre estas las lesiones de las vias opticas en niiios prettrminos eran especialmente frecuentes y con frecucncia podian explicarse por una leucomalacia periventricular. La distribution de 10s grupos etiol6gicos mayores es diferente de la hallada en poblaciones con retraso mental aislado o con alteraci6n visual aislada. per0 similar a la poblacidn sueca de tetraplegia espistica. Se pone a discusion las implicaciones para la prevencion de las dificultades mliltiples graves en niiios. 1087
1088
Referen ces Armitaee P. Bcnv G. (1987) Srurisrical Mcr/rods in
Med&al Rcsea;x-h. Oxford: Blackwell Scientific Publications.
Banker BO. Larrochc JC. ( 1962) Periventricular IeukomGacia of infancy: a form of neonatal anoxic enccphalopathy. Arcltit*es ~ ~ N e r i r o l ~ ~ y 7 : 386-4 10.
Bejar R. Wozniak P, Allard M. Benirschke K, Vaucher Y. Coeri R, Berry C, Schragg P. Villcgas I. Resnik R. (1988) Antenatal oripn of neuro- logic damage in newborn infants. 1. Preterm infants. Anieticon Jo~trital of Ohsrrrrics aitd
Berens C, Kerby CE. McKay EC. (1935) The causes of blindness in children. Jortrml of lhe Antcricuri Medical Assotiorion 105: 1949-56.
Blceker-Wagemakers EM. (1981) On tlre Curtses uf Blindness in the Mentally Relarded - wsir l i Special Refererice to rlie Getrrric Aspects. Bartimeushage, Doorn. The Netherlands: Bartimeus Foundation.
Blomquist HK, Gustavson KH. Holmgren G. (1981) Mild mental retardation in children in a northern Swedish county. Jortrwal of Meirtal Deficiency Research 25: 169-86.
Burgess P, Johnson A. (1991) Ocular defects in infants of extremely low birth weight and low gestational age. Britislr Joirrrral of Oplirlrulntulogy 75: 84-7.
Capella JA, Kaufman HE, Lill FJ, Cooper G. (1963) Hereditary cataracts and microphthalmia. American Jorrrital c$Op/ir/ralnrology 56: 454-8.
Clarke A. (1991) Is nondirective genetic coun- selling possible? tutrcet 338: 998-1001.
Copper AC. Schappert-Kimmijser J. (1970) The causes of blindness in 156 visually and mentally defective children. Oplr~liulnrul~~~icu 160:
Creasy RK. (1993) Preterm birth prevention: whcre are we? Anierirarr Jortr~iul of Obsretrics untf Gynecology 168: 1223-30.
De Reuck J, Van dcr Eecken H. ( 1983) Brain matu- ration and types of pcrinatal hypo~ic-ischemi~ encephalopathy. Eiiropeari Neirrolog! 22: 261-4.
DeVries LS, Regev R. Dubowitz LMS, Whitelaw A. Aber VR. (1988) Perinatal risk factors for the development of extensive cystic leukomalacia. Anicricun Join-tral of Diseases of Clrildren 142:
Edebol-Tysk K. (1989) Epidemiology of spastic tetraplegic cerebral palsy in Sweden. 1. lmpairmqnts and disabilities. Ncrirupediutrics
- Hagberg B. Hagberg G. ( 1989) Epidemiology of spastic tetraplegic cerebral palsy in Sweden. II. Prevalence. birth data and origin. Neirr~pedjurrt~s 20: 46-52.
Eken P, Van Nieuwenhuizen 0. Van der .Graaf Y, Schalij-Delfos NE. De Vries LS. (1994) Relation between neonatal cranial ultrasound abnormali- ties and cerebral visual impairment in infancy. D e r e ~ ~ r e i t ~ ~ ~ Midicine urtd Child Narrrolog.~ 36: 3 4
Fawer CL. Diebold P. Calame A. (1987) Perivcntricular leucomalacia and neurodevelop- mental outcome in preterm infants. Archires 01 Diseuse in Childlrood 62: 30-6.
Fernell E. Hagberg B, Hagberg G. von Wcndt L. ( 1 9 8 7 ~ ) Epidemiology of infantile hydrocephalus in Sweden. 11. Origin in infants born at term. Acru Pciediatrica Scundinoria 76: 4 1 I- 17.
---- . (IY87h) Epidemiology of infantile hydrocephalus in Sweden. 111. Origin in preterm infants. Acfa Pardiurricu Scandinaizia 76:
GY/iet.doKy 159: 357-63.
292-302.
732-5.
, 20:41-5.
3 18-23.
Flodmark 0, Jan JE. Wong PKH. (1990) Computed tomography of the brains of children with corti- cal visual impairment. Dewl~~pmenral Medicine
- Roland EH, Hill A, Whitfield MF. (1987) Periventricular leukomalacia: radiologic diagno- sis. R u d r c ~ l o ~ ~ ~ 162: 119-24.
Fraser GR. Friedmann AI. (1967) The CUI~JPS of Bfiridness irt Cltildftood. A Sftidy of 776 Childreit with Severe Visrtal ~ a i i d i c ~ ~ s . Baltimore: The
Chid N e ~ i r o l [ ~ g ~ 32: 61 1-20.
Johns Hopkins Press. Gibson DL. Sheos SB. Uh SH. Schcchter MT.
McCormick AQ. (1990) Retinopathy of prematu- rity-induccd blindness: birth-weight-specific sur- vival and the new epidemic. Pediutrics 86:
Glascr JS. editor. (1990) Ncrr~o-Oplrtlrainiul~~~~. 2nd ed. Philadelphia: JB Lippincott Company.
Groenveld M. (1990) The dilemma of assessing the visually impaired child. Dei*elopnienrul Medicine and Child Nrtirology 32: 1105-1.3..
Gustavson KH, Hagberg B. Hagberg G , Sars K. (19774 Severe mental retardation in a Swedish county. 11. Etiologic and pathogenetic aspects of children born 1959- 1970. Ncrtropudiarrie 8:
- Holmgren G. Jonscll RK. Blomquist H. (19776) Severe mental retardation in children in a north- ern Swedish county. Ioiirnal of Meirrol Deficiency Reseurdi 21: 161-80.
Hagberg B, Hagbcrg G . Lewerth A, Lindberg U. (1981) Mild mental retardarion in Swedish school children.: 11. Etiologic and pathogenetic aspects. Acra Paediatrii.a Scondinai*iu , 70:
-- Olow. 1. (1975) The changing panorama of cerebral palsy in Sweden 1954-1970. I. Analysis of the general changes. Acta Puediurricu Scandinaiia 64: 187-92.
Hansen E, F l a p T, Rosenbcrg T. Rudanko SL, Vipgosson G, Riise R. (1992) Visual impairment in Nordic children. Ill. Diagnoses. Acru Opl~tirainrolo~icu 70:. 597-604.
Hatfield EM. (1963) Causes of blindness in school childrcn. The Siglrr-Saririg Rei*ien* 33: 21 8-33.
- (1972) Blindness in infants and young children. The Sigkt-Susirrg Rer*icw 42: 69-89.
- (1975) Why are they blind? The Sigltr-Sai*ing R e r i m 45: 3-22.
Hertz BG. (19x7) Acuity card testing of retarded children. Beliuriurtral Brain Research 24: 85-92.
Hoyt CS. ( 1986) Cortical blindness in infancy. Trmtsuctiotts of the New Orlcurrs Acudctq of Opltrliulniology 34: 235-43.
Hoyt WF. Rios-Montenegro EN. Behrens MM. Eckelhoff RJ. ( 1972) Homonymous hemiopiic hypoplasia. Funduscopic features in standard and red-free illumination in three patients with con- genital hemiplegia. Bririslr Jorirnal of Opltrliafnrology 56: 537-45.
Jaeger W. (1975) Changes in the causes of blind- ness over the last hundred years. Child: Care. Health arid Derelopnienr 1: 299-307.
Jan JE, Groenveld M, Sykanda AM, Hoyt CS. (1987) Behavioural characteristics of children with permanent cortical visual impairment. Derehpnirntul Medicine and Clrild Ncirrology 29: 571-6.
- Robinson GC, Kinnis C, MacLeod PJM. (1977) Blindness due to optic-nerve atrophy and hypoplasia in children: an epidemiological study ( 1944- 1974). De~eiopn~eiital Mediciiw atid Clrild Nerirology 19: 353-63.
Johnsen SD. Richardson JR. Krohel GB. (1976) Neurologic concomitants of optic nerve hypopla- sia. Neioolc>tp 26: 391. (Paper presented at the
405- 12.
293-304.
445-52.
28th Annual Meeting of the American Academy of Neurology. May I , 1976, Toronto. Canada.)
Kerby CE. (1958) Causes of blindness in children of school age. The Sig/rt-Savin.q Relietit 28: 10-21.
Kiely M. (1987) The prevalence of mental retarda- tion. Epidemiologic ReiYcws 9: 194-21 8 .
- Lubin RA. Kiely JL. (19W) Descriptive epi- demiology of. cerebral palsy. Piihlic Healr/r Reviews 12: 79-101.
Konimission fur Perinatologie, Bayerische Landesarztekammer, KasscnSrztliche Vercinigung Bayerns ( 198 1-1 987) Gehrirtslri/fi,- Ges&nrstotistiA. 1981-1987. Miinchen: Kommission fur Pcrinatologie.
KrYgeloh-Mann 1, Hagberg B, Petersen D; Riethmiiller J. Gut E, Michaelis R. (1992) Bilateral spastic cerebral palsy - pathogenetic aspects from MRI. Nriii.opediatrics 23: 46-8.
Larroche JC, Droulle P, Delezoide AL, Narcy F, Nessmann C. (1990) Brain damage in monozy- gous twins. Bioloxj it/ the Neotiate 57: 261-78.
Levin M, Pincott JR, Hjclm IM. Taylor F. Kay J, Holzel H, Dinwiddie R. Matthew DJ. (1989) Hemorrhagic shock and encephalopathy: clinical. pathologic. and biochemical features. Jorirriul of Pediurrics 114: 194-203.
Lindstedt E. (1972) Severe 'visual impairment in Swedish children. Doc~rtnierrtu Op/rt/ru/nro/o.~ic~cr 31: 173-204.
MacLeod PM. Dolman CL. Chang E, Applegarth DA, Bryant B. (1976) The neuronal ceroid lipo- fuscinoses in British Columbia: A clinical epi- demiologic and ultrastructural study. nirtli Drfecn: Originu/ Arrich~ Series 12: 289-96.
McDonald MA, Dobson V. Sebris SL. Baitch L. Varner D, Tcller DY. (1985) The acuity card pro- cedure: a rapid test of infant acuity. Itri~iwi,~ritive
McQueen PC. Spence MW. Winsor EJT. Garner JB, Pereira LH. (1986) Causal origins of major men- tal handicap in the Canadian Maritime Provinces.
O~/l t / lU/ lJ l~/O~~j ' U i l d \';.flfU/ Sl'ielll'l' 26: 1 158-62.
Miringoff ML. ( 1991) The Social Costs it/ Gerretii. \Ve/fure. New-Brunswick. NJ: Rutgers University Press. 3 >.
Nelson LB. Calhoun JH. Harley RD. (1991) Pediutric Oplitliulniology. 3rd ed. Philadelphia: WB Saunders Company.
Newman NM. ( 1992) Nc~rrrit-Op/rt/icilrrrolo.q!.. t\ Pi'uc~ric~uI Tew. Norwalk, CT: Applcton & Lange.
Nissenkorn 1. Y-assur Y. Mashkowski D. Shcrf 1. Ben-Sira 1. (1983) Myopia in premature babies with and without retinopathy of prematurity. Brftislr Jorirrrul of ~ ~ ~ / r t / r u / r r r i t ~ ~ ) , ~ ~ 67: 17&3.
Nonie G. (1927) Causes of blindness in children. Twenty-five years experience of the Danish
Papiernik E. (1993) Prevention of preterm labour and delivery. Buillicre's Clirrit.tr1 Ohstetrii~s U J U I
Pearce WG. (1975) Causes of blindness in children. 1046 cases registered with fhc Canadian National Institute for the Blind 1970-1973. Cutrucliun
Peckham CS. (1986) Vision in childhood. Rritisli Mc~lic.ul Birllctin 42: 1 5 0 4 .
Pike MG. Jan JE. Wong PKH. ( 1989) Neurological and developmental findings in children with cataracts. Ainc*ricurr Jorrrnu/ of Diseo.ws of Children 143: 706-10.
Rath W. (1985) Geschichtc der Erziehung Blinder. In: Rath W, Hudelmayer D..editors. Huirtlbrrc~lr tier Snritlcr~iiiiltr~oRil;. \'ol 2 : Piiclir.qo.qil; cler
Institute for the Blind. Actu Op/rr/iu/nro/t~~ ~ I C U ' 3: 357-86.
~ ~ ~ ~ U l ~ l d l J , ~ ~ 7: 499-52 1 .
Joirrnu/ Of O~/l~/lU/ll l l l~oR?-J~~~ 10: 469-72.
Bliiitlrn i i r d Selrheliiriderteii. Berlin: Carl Marhold Verlagsbuchhandlung. p 21-5
RiegeI K, Thieme C. (1989) Funf Jahrc Neonatalerhebung in Bayern. Buyrisclres
Riise R. Flagc T, Hansen E. Rosenberg T, Rudanko SL, Viggosson G, Warburg M. (1992) Visual impairment in Nordic children. 1. Nordic registers and prevalence data. A m Oplrtliulnrolo,qicu 70:
Robinson GC. Jan JE, Kinnis C. (1987) Congenital ocular blindness in children, 1945 to 1984. Aiirericori Joiiriral of Diseuses of Clrildrerr 141: 13214.
Rogers B. Msall M, Owens T. Guernsey K. Brody A, Buck G. Hudak M. (1994) Cystic periventricu-
. lar leukomalacia and type of cerebral palsy in preterm infants. Jorrrtrol of Petliurrics 125: S 1-8.
Rosenbcrg T. (1987) Visual impairment in Danish children 1985. Acto Oplrt/ro/itro/o~qico 65: 110-17.
- Flage T, Hansen E, Rudanko SL. Viggosson G. Riise R. (1992) Visual impairment in Nordic chil- dren. 11. Aetiological factors. Actu 0plrtliultrrolo~~ic.cr 70: 155-64.
Saline E. (1992) Effective measures for the preven- tion of late abortions and premature births. Eorly
Schappert-Kimmijser J. Hansen E. Haustrate-Gosset MF. Lindtstedt E, Skydsgaard H. Warburg M. (1975) Causes of severe visual impairment in children and their prevention. Docunrnrtu
Schenk-Rootlicb AJF. Van Nieuwenhuizen 0. Van Zoggel J. Van der Graaf Y. Willcmse J. (1992) Grating acuity in children. Normal values of visual acuity in children up to 13 years as assessed by the acuity card procedure. Oplrtlrolniic Puetliutrirs urrtl Gerieric.s 13: 1 5 5 4 3 .
Seiberth V. Linderkamp 0. (1989) Akute Retinopathia praematurorum: Verlagerung des Manifestationsrisikos zu extrem- unreifen Friihgeborenen durch die neonatale Intensivmedizin. For~t.drrirre der O~~lrtlrcilrirolo.~ie 86: 626-30.
Shortland D. Levene MI. Trounce J. Ng Y. Graham 1M. ( 1988) The evolution and outcome of cavitat- ing perivcntricular leukomalacia in infancy. A study of 46 cases. Joiiri1crl of Perirrutal Metticirrr
Shuman RM. Selednik LJ. (19x0) Periventriculai. leukomalacia. A one-year autopsy study. Arifiivrs- oj'rVerirolo.yy 37: 23 1-5.
Skydsgaard H. ( 1955) Blindness and partial-sighted- ness in children. A i w ~p / r t / ro~~rro~o ,~ i r 'o 33:
Teller DY. McDonald MA. Preston K. Sebris SL. Dobson V. (1986) Assessment of visual acuity in infants and children: the acuity card procedure. Developnicritul Mecliiirie m r l Child Neirrolrqy
' 28: 779-89. Temtamy SA. Shalash BA. (1974) Genetic hetero-
zeneity of the syndrome: microphthalmia with congenital cataract. Birtlr Defects: Original Artii,le Scrirs 10: 292-3.
Van Buren JM. (1963) Transsynaptic retrsgrade degeneration in the visual system of primates. J ~ ~ t i i . i i d of Neiirology. Neiirosrrrpvj urrtl P.sjc~/ricitr~ 26: 402409.
Van Nieuwenhuizen 0. ( 1987) Cerehrul \,'isitti/ Disrrirhunce in Iitjciirtile Erit~c~plral~~put/iy. Dordrecht: Martinus Nijhoff/Dr W. Junk Publihhers.
Volpc JJ. (1990) Brain injury in the premature inpant: is it preventable? Pediirtrk Reseorcli 27:
Ar~tt.h/(itt 44: 71-8.
145-54.
/ / l l l J lUi l Drl.r/otpnieirr 29: 15-20.
~ / l ~ l / / l U ~ l ~ l l ~ / ~ J ~ ~ ~ ~ U 39: 2 13-34 I .
16: 241-7.
409- 17.
1089
5 0 v).
‘3 t J
S28-33. - (1995) Nerrrolngy of the Newborn. 3rd ed. Philadelphia: Saunders.
Warburg M. Frederiksen P. Rattleff J. (1979) Blindness among 7700 mentally retarded chil- dren in Denmark. In: Smith V. Keen J, editors. Visirul Handicap in Chi ldmi . London: William Heinemann Medical Books. p. 56-67.
Whiting S. Jan JE. Wong PKH. Flodrnilrk 0, Farrell K, McCormick AQ. (1985) Permanent corticaf visual impairment in children. D e ~ e ~ ~ ~ n i e ~ i ~ u ~
Medicine and Child Neitrolvgy 27: 730-9. Williamson WD, Desmond MM, Andrew LP, Hicks
RN. (1987) VisuaIly impaired infants in the 1980s. A survey of etiologic factors and addi- tional handi-capping conditions in a school pop- ulation. Cfitrical Pediatrics 26: 241-4.
World Health Organization ( 1980) Ititernotional C i a s . ~ i ~ c ~ t i o n of I n ~ p u i ~ ~ e n i s , ~isubili t ies. and Handicaps. A Manitui of Classifi cation Relating to the Conxqitrnres of Disrase. Geneva: World Health Organization.
1090
Doctors’ Course, The Bobath Centre, London, UK. 17th to 19th March 1997
T h e course provides an introduction to the Bobath Approach and its application to cerebral palsy. T h e treatment of cerebral palsy, assessment (including assessment in neonatal intensive care). examination, orthopaedic aspects and counselling will ail be covered. CME approval is being sought. For further iRfromation contact, Rachel Woolfson, T h e Bobath Centrc, 250 East End Rd. LONDON N 2 8AU. Tel: +44 181 444 3355; Fax +44 181 444 3399.