multiple congenitally missing teeth treated with ... · tient with multiple missing teeth in the...
TRANSCRIPT
CASE REPORT
Multiple congenitally missing teeth treated withautotransplantation and orthodontics
Jae Hyun Park,a Kiyoshi Tai,b Kenji Yuasa,c and Daisuke Hayashid
Mesa, Ariz, and Okayama, Japan
aAssoSchooscholabVisitArizonDeparof MOkayacPrivadPrivaThe aucts oReprinSchoo85206Subm0889-Copyrdoi:10
Treatment of children with several congenitally missing teeth is challenging, because growth and development ofthe oral structures must be considered. The treatment options include retaining the deciduous teeth andpostponing treatment until later or extracting the deciduous teeth and doing one of the following: allowing thespace to close spontaneously, closing the space orthodontically, or in patients whose growth is finished, usinga prosthetic or implant replacement. One other viable option, if donor teeth are available, is autotransplantation.The treatment plan for patients with missing teeth should be based on a comprehensive evaluation of thepatient’s age, occlusion, and space requirements as well as on the size and shape of the adjacent teeth. Thiscase report presents the management of a patient in the early mixed dentition with multiple missing teeth.The treatment consisted of a combination of autotransplantation of the maxillary right first premolar to themandibular right first premolar region and orthodontic treatment with a 5-year follow-up after autotransplantation.(Am J Orthod Dentofacial Orthop 2012;141:641-51)
Congenitally missing premolars are oftena diagnostic challenge to the orthodontist. Withautotransplantation, it is possible to solve compli-
cated treatment problems in the dental arches. Autotrans-plantation of immature premolars is a viable method ofrestoring edentulous areas in young patients whosealveolar growth is not yet complete. This method canpotentially replace a missing tooth with a natural toothrather than with a prosthesis or an osseointegrated im-plant.
Autotransplantation of premolars with partly formedroots has been reported to be a predictable treatmentmodality.1-6 This is because transplanted teeth alsohave the capacity for functional adaptation7,8 andpreservation of the alveolar ridge.9 Premolars can be
ciate professor and chair, Postgraduate Orthodontic Program, Arizonal of Dentistry & Oral Health, A. T. Still University, Mesa, Ariz; internationalr, College of Dentistry, Kyung Hee University, Seoul, South Korea.ing adjunct assistant professor, Postgraduate Orthodontic Program,a School of Dentistry & Oral Health, Mesa, Ariz; postgraduate student,tment of Oral and Maxillofacial Reconstructive Surgery, Graduate Schooledicine, Dentistry and Pharmaceutical Sciences, Okayama University,ma, Japan; private practice, orthodontics, Okayama, Japan.te practice, general dentistry, Okayama, Japan.te practice, orthodontics, Okayama, Japan.uthors report no commercial, proprietary, or financial interest in the prod-r companies described in this article.t requests to: Jae Hyun Park, Postgraduate Orthodontic Program, Arizonal of Dentistry & Oral Health, A. T. Still University, 5835 E Still Cir, Mesa, AZ; e-mail, [email protected], June 2010; revised and accepted, July 2010.5406/$36.00ight � 2012 by the American Association of Orthodontists..1016/j.ajodo.2010.07.030
transplanted from 1 site in a crowded arch to anothersite to replace congenitally absent premolars.
This case report presents the management of a pa-tient with multiple missing teeth in the early mixeddentition. It describes a conservative treatment ap-proach: autotransplantation of the maxillary right firstpremolar to the mandibular right first premolar regionwas combined with orthodontic treatment.
DIAGNOSIS AND ETIOLOGY
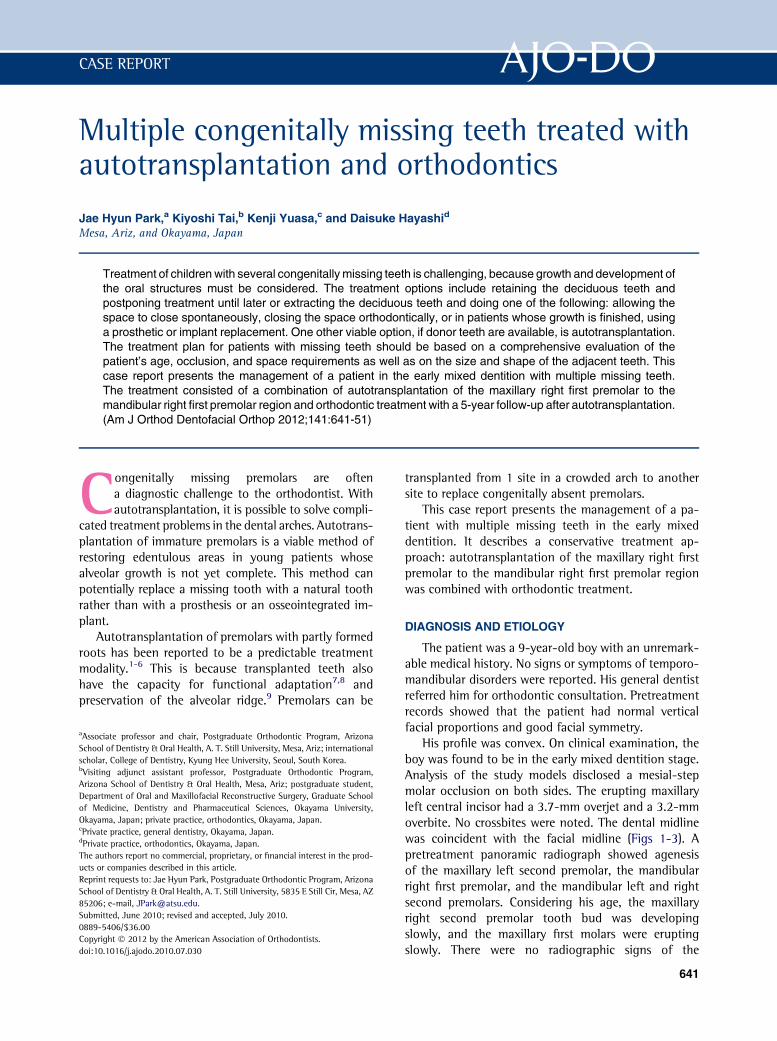
The patient was a 9-year-old boy with an unremark-able medical history. No signs or symptoms of temporo-mandibular disorders were reported. His general dentistreferred him for orthodontic consultation. Pretreatmentrecords showed that the patient had normal verticalfacial proportions and good facial symmetry.
His profile was convex. On clinical examination, theboy was found to be in the early mixed dentition stage.Analysis of the study models disclosed a mesial-stepmolar occlusion on both sides. The erupting maxillaryleft central incisor had a 3.7-mm overjet and a 3.2-mmoverbite. No crossbites were noted. The dental midlinewas coincident with the facial midline (Figs 1-3). Apretreatment panoramic radiograph showed agenesisof the maxillary left second premolar, the mandibularright first premolar, and the mandibular left and rightsecond premolars. Considering his age, the maxillaryright second premolar tooth bud was developingslowly, and the maxillary first molars were eruptingslowly. There were no radiographic signs of the
641
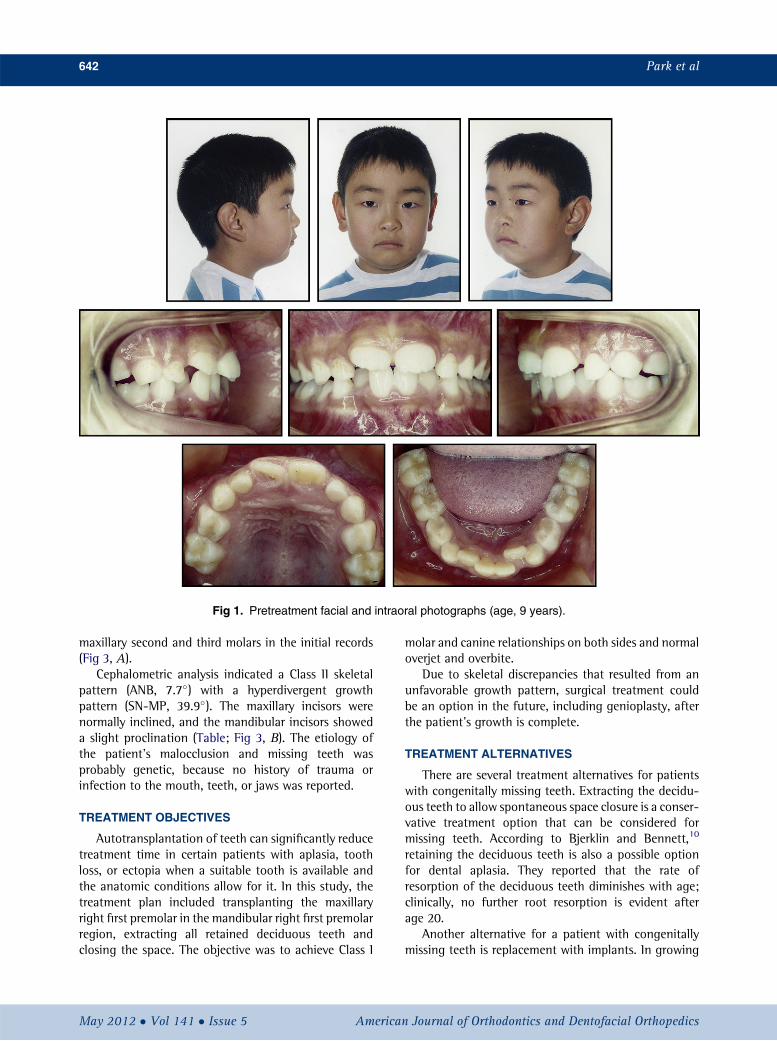
Fig 1. Pretreatment facial and intraoral photographs (age, 9 years).
642 Park et al
maxillary second and third molars in the initial records(Fig 3, A).
Cephalometric analysis indicated a Class II skeletalpattern (ANB, 7.7�) with a hyperdivergent growthpattern (SN-MP, 39.9�). The maxillary incisors werenormally inclined, and the mandibular incisors showeda slight proclination (Table; Fig 3, B). The etiology ofthe patient’s malocclusion and missing teeth wasprobably genetic, because no history of trauma orinfection to the mouth, teeth, or jaws was reported.
TREATMENT OBJECTIVES
Autotransplantation of teeth can significantly reducetreatment time in certain patients with aplasia, toothloss, or ectopia when a suitable tooth is available andthe anatomic conditions allow for it. In this study, thetreatment plan included transplanting the maxillaryright first premolar in the mandibular right first premolarregion, extracting all retained deciduous teeth andclosing the space. The objective was to achieve Class I
May 2012 � Vol 141 � Issue 5 American
molar and canine relationships on both sides and normaloverjet and overbite.
Due to skeletal discrepancies that resulted from anunfavorable growth pattern, surgical treatment couldbe an option in the future, including genioplasty, afterthe patient’s growth is complete.
TREATMENT ALTERNATIVES
There are several treatment alternatives for patientswith congenitally missing teeth. Extracting the decidu-ous teeth to allow spontaneous space closure is a conser-vative treatment option that can be considered formissing teeth. According to Bjerklin and Bennett,10
retaining the deciduous teeth is also a possible optionfor dental aplasia. They reported that the rate ofresorption of the deciduous teeth diminishes with age;clinically, no further root resorption is evident afterage 20.
Another alternative for a patient with congenitallymissing teeth is replacement with implants. In growing
Journal of Orthodontics and Dentofacial Orthopedics
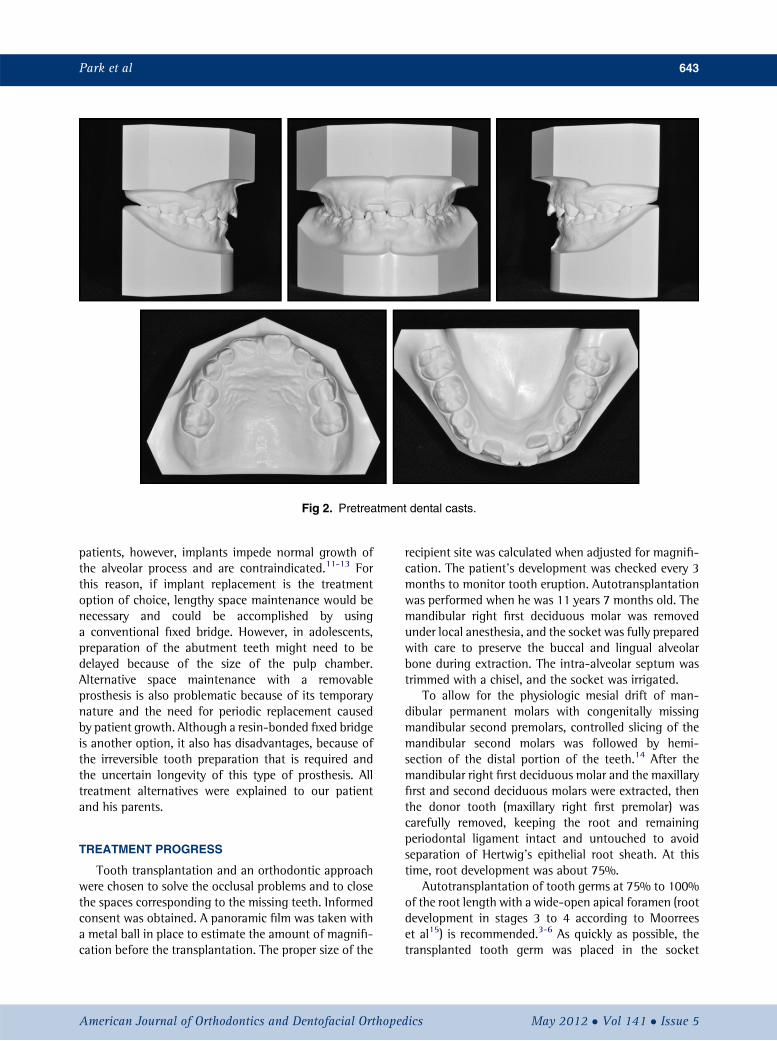
Fig 2. Pretreatment dental casts.
Park et al 643
patients, however, implants impede normal growth ofthe alveolar process and are contraindicated.11-13 Forthis reason, if implant replacement is the treatmentoption of choice, lengthy space maintenance would benecessary and could be accomplished by usinga conventional fixed bridge. However, in adolescents,preparation of the abutment teeth might need to bedelayed because of the size of the pulp chamber.Alternative space maintenance with a removableprosthesis is also problematic because of its temporarynature and the need for periodic replacement causedby patient growth. Although a resin-bonded fixed bridgeis another option, it also has disadvantages, because ofthe irreversible tooth preparation that is required andthe uncertain longevity of this type of prosthesis. Alltreatment alternatives were explained to our patientand his parents.
TREATMENT PROGRESS
Tooth transplantation and an orthodontic approachwere chosen to solve the occlusal problems and to closethe spaces corresponding to the missing teeth. Informedconsent was obtained. A panoramic film was taken witha metal ball in place to estimate the amount of magnifi-cation before the transplantation. The proper size of the
American Journal of Orthodontics and Dentofacial Orthoped
recipient site was calculated when adjusted for magnifi-cation. The patient’s development was checked every 3months to monitor tooth eruption. Autotransplantationwas performed when he was 11 years 7 months old. Themandibular right first deciduous molar was removedunder local anesthesia, and the socket was fully preparedwith care to preserve the buccal and lingual alveolarbone during extraction. The intra-alveolar septum wastrimmed with a chisel, and the socket was irrigated.
To allow for the physiologic mesial drift of man-dibular permanent molars with congenitally missingmandibular second premolars, controlled slicing of themandibular second molars was followed by hemi-section of the distal portion of the teeth.14 After themandibular right first deciduous molar and the maxillaryfirst and second deciduous molars were extracted, thenthe donor tooth (maxillary right first premolar) wascarefully removed, keeping the root and remainingperiodontal ligament intact and untouched to avoidseparation of Hertwig’s epithelial root sheath. At thistime, root development was about 75%.
Autotransplantation of tooth germs at 75% to 100%of the root length with a wide-open apical foramen (rootdevelopment in stages 3 to 4 according to Moorreeset al15) is recommended.3-6 As quickly as possible, thetransplanted tooth germ was placed in the socket
ics May 2012 � Vol 141 � Issue 5
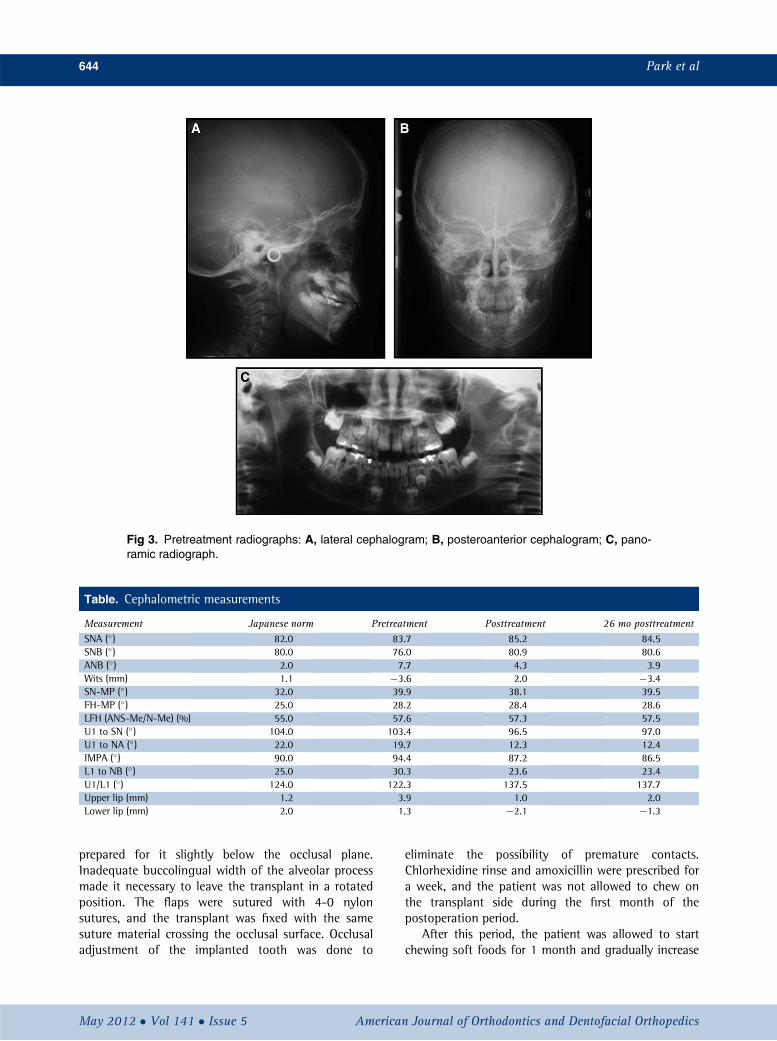
Fig 3. Pretreatment radiographs: A, lateral cephalogram; B, posteroanterior cephalogram; C, pano-ramic radiograph.
Table. Cephalometric measurements
Measurement Japanese norm Pretreatment Posttreatment 26 mo posttreatmentSNA (�) 82.0 83.7 85.2 84.5SNB (�) 80.0 76.0 80.9 80.6ANB (�) 2.0 7.7 4.3 3.9Wits (mm) 1.1 �3.6 2.0 �3.4SN-MP (�) 32.0 39.9 38.1 39.5FH-MP (�) 25.0 28.2 28.4 28.6LFH (ANS-Me/N-Me) (%) 55.0 57.6 57.3 57.5U1 to SN (�) 104.0 103.4 96.5 97.0U1 to NA (�) 22.0 19.7 12.3 12.4IMPA (�) 90.0 94.4 87.2 86.5L1 to NB (�) 25.0 30.3 23.6 23.4U1/L1 (�) 124.0 122.3 137.5 137.7Upper lip (mm) 1.2 3.9 1.0 2.0Lower lip (mm) 2.0 1.3 �2.1 �1.3
644 Park et al
prepared for it slightly below the occlusal plane.Inadequate buccolingual width of the alveolar processmade it necessary to leave the transplant in a rotatedposition. The flaps were sutured with 4-0 nylonsutures, and the transplant was fixed with the samesuture material crossing the occlusal surface. Occlusaladjustment of the implanted tooth was done to
May 2012 � Vol 141 � Issue 5 American
eliminate the possibility of premature contacts.Chlorhexidine rinse and amoxicillin were prescribed fora week, and the patient was not allowed to chew onthe transplant side during the first month of thepostoperation period.
After this period, the patient was allowed to startchewing soft foods for 1 month and gradually increase
Journal of Orthodontics and Dentofacial Orthopedics
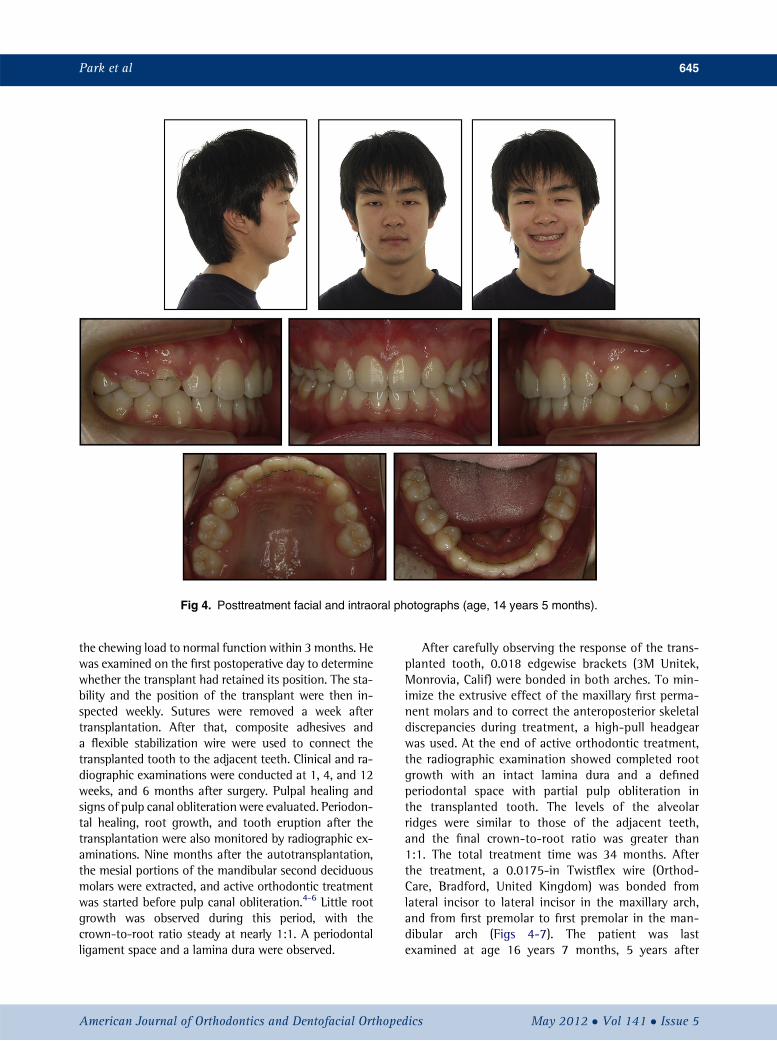
Fig 4. Posttreatment facial and intraoral photographs (age, 14 years 5 months).
Park et al 645
the chewing load to normal function within 3 months. Hewas examined on the first postoperative day to determinewhether the transplant had retained its position. The sta-bility and the position of the transplant were then in-spected weekly. Sutures were removed a week aftertransplantation. After that, composite adhesives anda flexible stabilization wire were used to connect thetransplanted tooth to the adjacent teeth. Clinical and ra-diographic examinations were conducted at 1, 4, and 12weeks, and 6 months after surgery. Pulpal healing andsigns of pulp canal obliteration were evaluated. Periodon-tal healing, root growth, and tooth eruption after thetransplantation were also monitored by radiographic ex-aminations. Nine months after the autotransplantation,the mesial portions of the mandibular second deciduousmolars were extracted, and active orthodontic treatmentwas started before pulp canal obliteration.4-6 Little rootgrowth was observed during this period, with thecrown-to-root ratio steady at nearly 1:1. A periodontalligament space and a lamina dura were observed.
American Journal of Orthodontics and Dentofacial Orthoped
After carefully observing the response of the trans-planted tooth, 0.018 edgewise brackets (3M Unitek,Monrovia, Calif) were bonded in both arches. To min-imize the extrusive effect of the maxillary first perma-nent molars and to correct the anteroposterior skeletaldiscrepancies during treatment, a high-pull headgearwas used. At the end of active orthodontic treatment,the radiographic examination showed completed rootgrowth with an intact lamina dura and a definedperiodontal space with partial pulp obliteration inthe transplanted tooth. The levels of the alveolarridges were similar to those of the adjacent teeth,and the final crown-to-root ratio was greater than1:1. The total treatment time was 34 months. Afterthe treatment, a 0.0175-in Twistflex wire (Orthod-Care, Bradford, United Kingdom) was bonded fromlateral incisor to lateral incisor in the maxillary arch,and from first premolar to first premolar in the man-dibular arch (Figs 4-7). The patient was lastexamined at age 16 years 7 months, 5 years after
ics May 2012 � Vol 141 � Issue 5
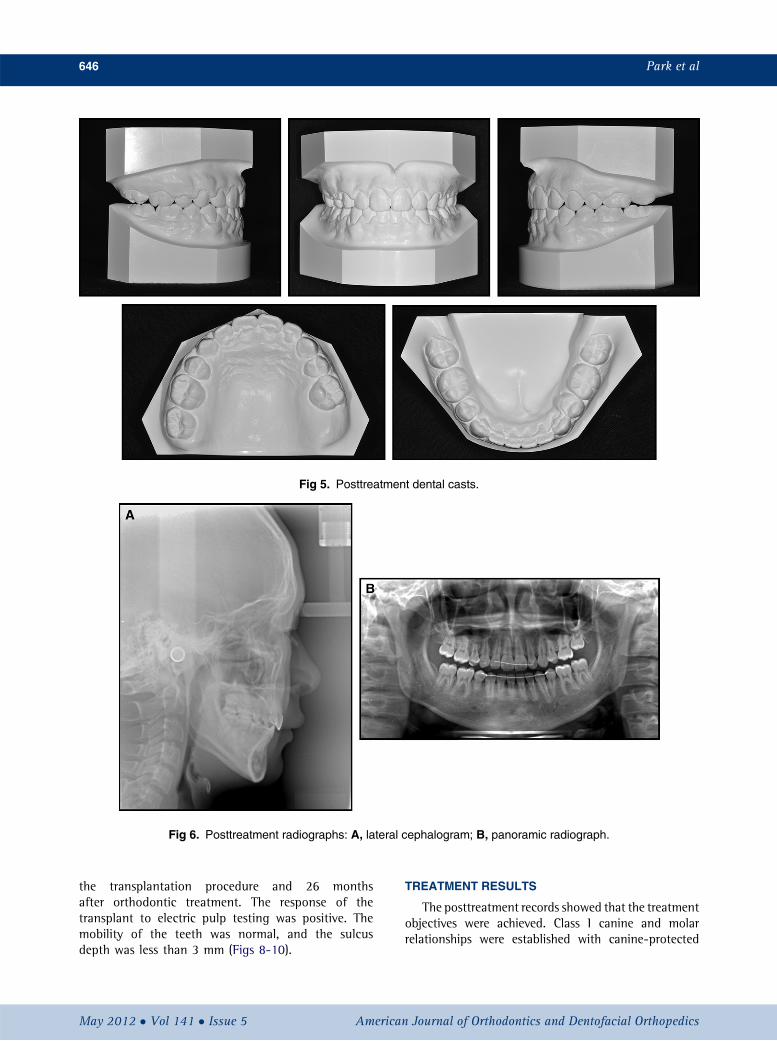
Fig 5. Posttreatment dental casts.
Fig 6. Posttreatment radiographs: A, lateral cephalogram; B, panoramic radiograph.
646 Park et al
the transplantation procedure and 26 monthsafter orthodontic treatment. The response of thetransplant to electric pulp testing was positive. Themobility of the teeth was normal, and the sulcusdepth was less than 3 mm (Figs 8-10).
May 2012 � Vol 141 � Issue 5 American
TREATMENT RESULTS
The posttreatment records showed that the treatmentobjectives were achieved. Class I canine and molarrelationships were established with canine-protected
Journal of Orthodontics and Dentofacial Orthopedics
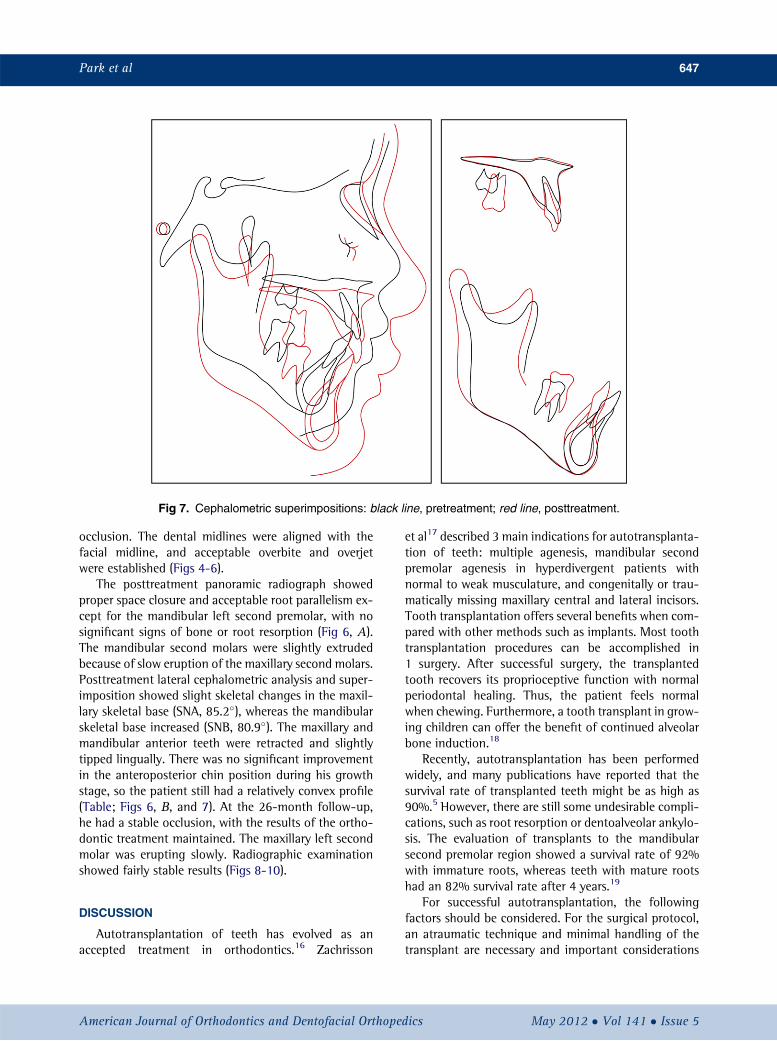
Fig 7. Cephalometric superimpositions: black line, pretreatment; red line, posttreatment.
Park et al 647
occlusion. The dental midlines were aligned with thefacial midline, and acceptable overbite and overjetwere established (Figs 4-6).
The posttreatment panoramic radiograph showedproper space closure and acceptable root parallelism ex-cept for the mandibular left second premolar, with nosignificant signs of bone or root resorption (Fig 6, A).The mandibular second molars were slightly extrudedbecause of slow eruption of the maxillary second molars.Posttreatment lateral cephalometric analysis and super-imposition showed slight skeletal changes in the maxil-lary skeletal base (SNA, 85.2�), whereas the mandibularskeletal base increased (SNB, 80.9�). The maxillary andmandibular anterior teeth were retracted and slightlytipped lingually. There was no significant improvementin the anteroposterior chin position during his growthstage, so the patient still had a relatively convex profile(Table; Figs 6, B, and 7). At the 26-month follow-up,he had a stable occlusion, with the results of the ortho-dontic treatment maintained. The maxillary left secondmolar was erupting slowly. Radiographic examinationshowed fairly stable results (Figs 8-10).
DISCUSSION
Autotransplantation of teeth has evolved as anaccepted treatment in orthodontics.16 Zachrisson
American Journal of Orthodontics and Dentofacial Orthoped
et al17 described 3 main indications for autotransplanta-tion of teeth: multiple agenesis, mandibular secondpremolar agenesis in hyperdivergent patients withnormal to weak musculature, and congenitally or trau-matically missing maxillary central and lateral incisors.Tooth transplantation offers several benefits when com-pared with other methods such as implants. Most toothtransplantation procedures can be accomplished in1 surgery. After successful surgery, the transplantedtooth recovers its proprioceptive function with normalperiodontal healing. Thus, the patient feels normalwhen chewing. Furthermore, a tooth transplant in grow-ing children can offer the benefit of continued alveolarbone induction.18
Recently, autotransplantation has been performedwidely, and many publications have reported that thesurvival rate of transplanted teeth might be as high as90%.5 However, there are still some undesirable compli-cations, such as root resorption or dentoalveolar ankylo-sis. The evaluation of transplants to the mandibularsecond premolar region showed a survival rate of 92%with immature roots, whereas teeth with mature rootshad an 82% survival rate after 4 years.19
For successful autotransplantation, the followingfactors should be considered. For the surgical protocol,an atraumatic technique and minimal handling of thetransplant are necessary and important considerations
ics May 2012 � Vol 141 � Issue 5
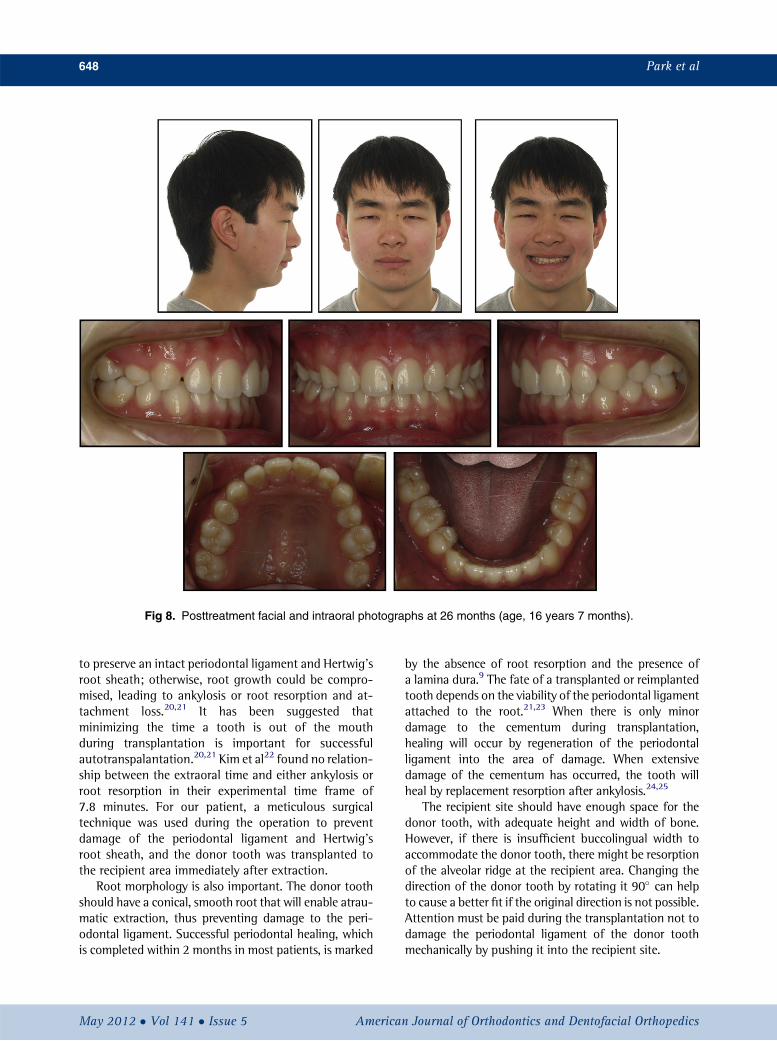
Fig 8. Posttreatment facial and intraoral photographs at 26 months (age, 16 years 7 months).
648 Park et al
to preserve an intact periodontal ligament and Hertwig’sroot sheath; otherwise, root growth could be compro-mised, leading to ankylosis or root resorption and at-tachment loss.20,21 It has been suggested thatminimizing the time a tooth is out of the mouthduring transplantation is important for successfulautotranspalantation.20,21 Kim et al22 found no relation-ship between the extraoral time and either ankylosis orroot resorption in their experimental time frame of7.8 minutes. For our patient, a meticulous surgicaltechnique was used during the operation to preventdamage of the periodontal ligament and Hertwig’sroot sheath, and the donor tooth was transplanted tothe recipient area immediately after extraction.
Root morphology is also important. The donor toothshould have a conical, smooth root that will enable atrau-matic extraction, thus preventing damage to the peri-odontal ligament. Successful periodontal healing, whichis completed within 2 months in most patients, is marked
May 2012 � Vol 141 � Issue 5 American
by the absence of root resorption and the presence ofa lamina dura.9 The fate of a transplanted or reimplantedtooth depends on the viability of the periodontal ligamentattached to the root.21,23 When there is only minordamage to the cementum during transplantation,healing will occur by regeneration of the periodontalligament into the area of damage. When extensivedamage of the cementum has occurred, the tooth willheal by replacement resorption after ankylosis.24,25
The recipient site should have enough space for thedonor tooth, with adequate height and width of bone.However, if there is insufficient buccolingual width toaccommodate the donor tooth, there might be resorptionof the alveolar ridge at the recipient area. Changing thedirection of the donor tooth by rotating it 90� can helpto cause a better fit if the original direction is not possible.Attention must be paid during the transplantation not todamage the periodontal ligament of the donor toothmechanically by pushing it into the recipient site.
Journal of Orthodontics and Dentofacial Orthopedics
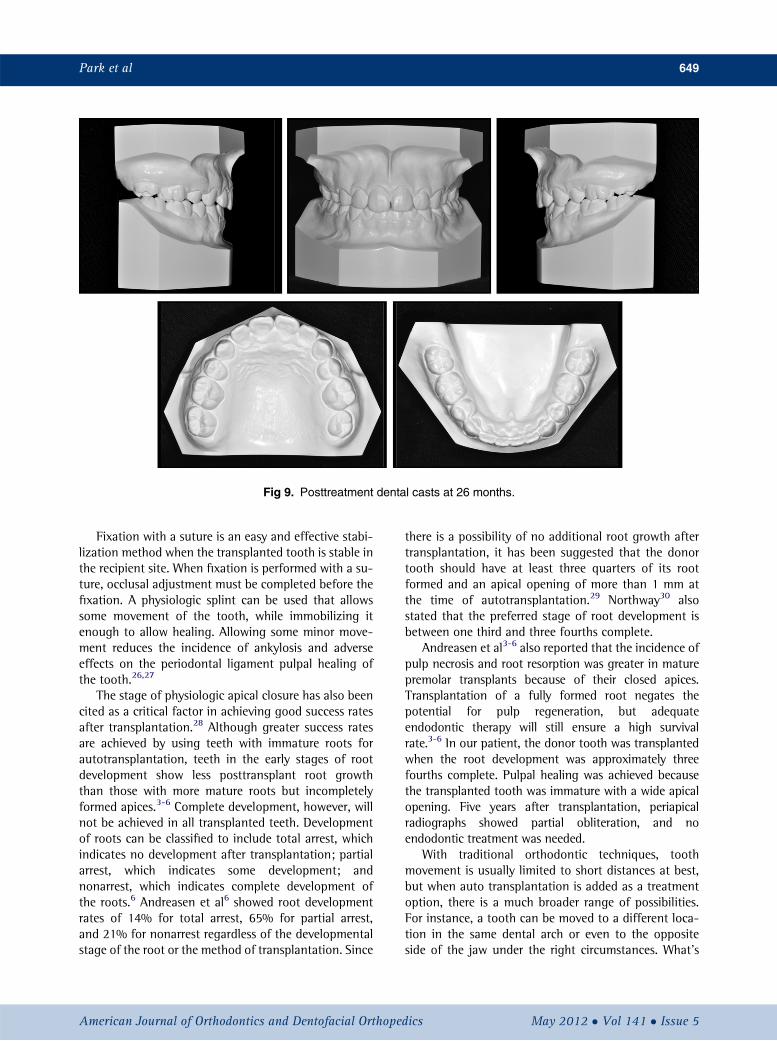
Fig 9. Posttreatment dental casts at 26 months.
Park et al 649
Fixation with a suture is an easy and effective stabi-lization method when the transplanted tooth is stable inthe recipient site. When fixation is performed with a su-ture, occlusal adjustment must be completed before thefixation. A physiologic splint can be used that allowssome movement of the tooth, while immobilizing itenough to allow healing. Allowing some minor move-ment reduces the incidence of ankylosis and adverseeffects on the periodontal ligament pulpal healing ofthe tooth.26,27
The stage of physiologic apical closure has also beencited as a critical factor in achieving good success ratesafter transplantation.28 Although greater success ratesare achieved by using teeth with immature roots forautotransplantation, teeth in the early stages of rootdevelopment show less posttransplant root growththan those with more mature roots but incompletelyformed apices.3-6 Complete development, however, willnot be achieved in all transplanted teeth. Developmentof roots can be classified to include total arrest, whichindicates no development after transplantation; partialarrest, which indicates some development; andnonarrest, which indicates complete development ofthe roots.6 Andreasen et al6 showed root developmentrates of 14% for total arrest, 65% for partial arrest,and 21% for nonarrest regardless of the developmentalstage of the root or the method of transplantation. Since
American Journal of Orthodontics and Dentofacial Orthoped
there is a possibility of no additional root growth aftertransplantation, it has been suggested that the donortooth should have at least three quarters of its rootformed and an apical opening of more than 1 mm atthe time of autotransplantation.29 Northway30 alsostated that the preferred stage of root development isbetween one third and three fourths complete.
Andreasen et al3-6 also reported that the incidence ofpulp necrosis and root resorption was greater in maturepremolar transplants because of their closed apices.Transplantation of a fully formed root negates thepotential for pulp regeneration, but adequateendodontic therapy will still ensure a high survivalrate.3-6 In our patient, the donor tooth was transplantedwhen the root development was approximately threefourths complete. Pulpal healing was achieved becausethe transplanted tooth was immature with a wide apicalopening. Five years after transplantation, periapicalradiographs showed partial obliteration, and noendodontic treatment was needed.
With traditional orthodontic techniques, toothmovement is usually limited to short distances at best,but when auto transplantation is added as a treatmentoption, there is a much broader range of possibilities.For instance, a tooth can be moved to a different loca-tion in the same dental arch or even to the oppositeside of the jaw under the right circumstances. What's
ics May 2012 � Vol 141 � Issue 5
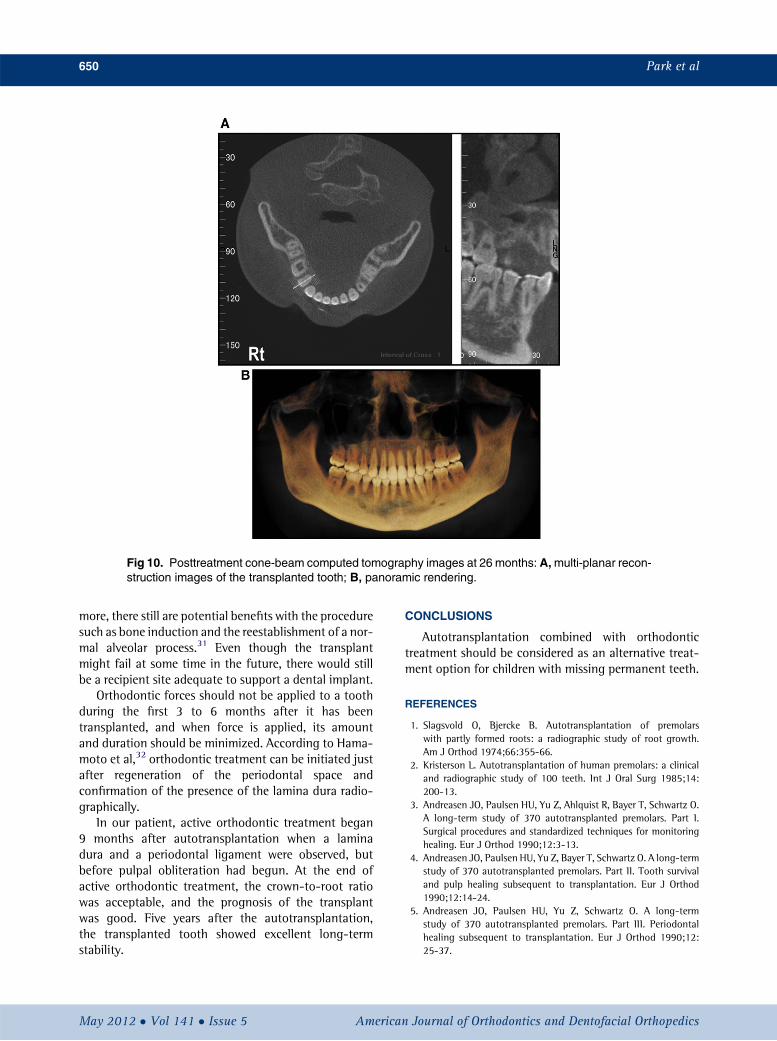
Fig 10. Posttreatment cone-beam computed tomography images at 26 months: A,multi-planar recon-struction images of the transplanted tooth; B, panoramic rendering.
650 Park et al
more, there still are potential benefits with the proceduresuch as bone induction and the reestablishment of a nor-mal alveolar process.31 Even though the transplantmight fail at some time in the future, there would stillbe a recipient site adequate to support a dental implant.
Orthodontic forces should not be applied to a toothduring the first 3 to 6 months after it has beentransplanted, and when force is applied, its amountand duration should be minimized. According to Hama-moto et al,32 orthodontic treatment can be initiated justafter regeneration of the periodontal space andconfirmation of the presence of the lamina dura radio-graphically.
In our patient, active orthodontic treatment began9 months after autotransplantation when a laminadura and a periodontal ligament were observed, butbefore pulpal obliteration had begun. At the end ofactive orthodontic treatment, the crown-to-root ratiowas acceptable, and the prognosis of the transplantwas good. Five years after the autotransplantation,the transplanted tooth showed excellent long-termstability.
May 2012 � Vol 141 � Issue 5 American
CONCLUSIONS
Autotransplantation combined with orthodontictreatment should be considered as an alternative treat-ment option for children with missing permanent teeth.
REFERENCES
1. Slagsvold O, Bjercke B. Autotransplantation of premolarswith partly formed roots: a radiographic study of root growth.Am J Orthod 1974;66:355-66.
2. Kristerson L. Autotransplantation of human premolars: a clinicaland radiographic study of 100 teeth. Int J Oral Surg 1985;14:200-13.
3. Andreasen JO, Paulsen HU, Yu Z, Ahlquist R, Bayer T, Schwartz O.A long-term study of 370 autotransplanted premolars. Part I.Surgical procedures and standardized techniques for monitoringhealing. Eur J Orthod 1990;12:3-13.
4. Andreasen JO, Paulsen HU, Yu Z, Bayer T, Schwartz O. A long-termstudy of 370 autotransplanted premolars. Part II. Tooth survivaland pulp healing subsequent to transplantation. Eur J Orthod1990;12:14-24.
5. Andreasen JO, Paulsen HU, Yu Z, Schwartz O. A long-termstudy of 370 autotransplanted premolars. Part III. Periodontalhealing subsequent to transplantation. Eur J Orthod 1990;12:25-37.
Journal of Orthodontics and Dentofacial Orthopedics

Park et al 651
6. Andreasen JO, Paulsen HU, Yu Z, Bayer T. A long-term study of370 autotransplanted premolars. Part IV. Root developmentsubsequent to transplantation. Eur J Orthod 1990;12:38-50.
7. Slagsvold O, Bjercke B. Indications for autotransplantation in casesof missing premolars. Am J Orthod 1978;74:241-57.
8. Slagsvold O, Bjercke B. Applicability of autotransplantation in casesof missing upper anterior teeth. Am J Orthod 1978;74:410-21.
9. Czochrowska EM, Stenvik A, Album B, Zachrisson BU. Autotrans-plantation of premolars to replace maxillary incisors: a comparisonwith natural incisors. Am J Orthod Dentofacial Orthop 2000;118:592-600.
10. Bjerklin K, Bennett J. The long-term survival of lower secondprimary molars in subjects with agenesis of the premolars. EurJ Orthod 2000;22:245-55.
11. Westwood RM, Duncan JM. Implants in adolescents: a literaturereview and case reports. Int J Oral Maxillofac Implants 1996;11:750-5.
12. Odman J, Grondahl K, Lekholm U, Thilander B. The effect ofosseointegrated implants on the dentoalveolar development(a clinical and radiographic study in growing pigs). Eur J Orthod1991;13:279-86.
13. Thilander B, Odman J, Grondahl K, Lekholm U. Aspects of osseoin-tegrated implants inserted in the growing jaws: a biometric andradiographic study in the young pig. Eur J Orthod 1992;14:99-109.
14. Valencia R, Saadia M, Grinberg G. Controlled slicing in themanagement of congenitally missing second premolars. AmJ Orthod Dentofacial Orthop 2004;125:537-43.
15. Moorrees JFA, Fanning EA, Hunt EE. Age variation of formationstages for ten permanent teeth. J Dent Res 1963;42:1490-502.
16. Jonsson T, Sigurdsson TJ. Autotransplantation of premolars topremolar sites. A long-term follow-up study of 40 consecutivepatients. Am J Orthod Dentofacial Orthop 2004;125:668-75.
17. Zachrisson BU, Stenvik A, Haanæs HR. Management of missingmaxillary anterior teeth with emphasis on autotransplantation.Am J Orthod Dentofacial Orthop 2004;126:284-8.
18. Cohen AS, Shen TC, Pogrel MA. Transplanting teeth successfully:autografts and allografts that work. J Am Dent Assoc 1995;126:481-5.
American Journal of Orthodontics and Dentofacial Orthoped
19. Josefsson E, Brattstr€om V, Tegsj€o U, Valerius-Olsson H. Treatmentof lower second premolar agenesis by autotransplantation: fouryear evaluation of eighty patients. Acta Odontol Scand 1999;57:111-5.
20. Thomas S, Turner SR, Sandy JR. Autotransplantation of teeth: isthere a role? Br J Orthod 1998;25:275-82.
21. Raghoebar GM, Vissink A. Results of intentional replantation ofmolars. J Oral Maxillofac Surg 1999;57:240-4.
22. Kim E, Jung JY, Cha IH, Kum KY, Lee SJ. Evaluation of theprognosis and causes of failure in 182 cases of autogenous toothtransplantation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2005;100:112-29.
23. Nethander G. Oral restoration with fixed partial dentures ontransplanted abutment teeth. Int J Prosthodont 1995;8:517-26.
24. Tsukiboshi M. Autotranspalantation of teeth. Tokyo, Japan:Quintessence; 2001. p. 21-55.
25. Andreasen JO, Kristerson L. The effect of limited drying orremoval of the periodontal ligament. Periodontal healing after re-plantation of mature incisors in monkeys. Acta Odontol Scand1981;39:1-13.
26. Hernandez SL, Cuestas-Carnero R. Autogenic tooth trans-plantation: a report of ten cases. J Oral Maxillofac Surg 1988;46:1051-5.
27. Pogrel MA. Evaluation of over 400 autogenous tooth transplants.J Oral Maxillofac Surg 1987;45:205-11.
28. Shwartz O, Bergman P, Klausen B. Resorption of autotransplantedhuman teeth: a retrospective study of 291 transplantations overa period of 25 years. Int Endod J 1985;18:119-31.
29. Tsukiboshi M. Autotransplantation of teeth: requirement forpredictable success. Dent Traumatol 2002;18:157-80.
30. Northway W. Autogenic dental transplants. Am J Orthod Dentofa-cial Orthop 2002;121:592-3.
31. Fiorentino G, Vecchione P. Multiple congenitally missing teeth:treatment outcome with autologous transplantation andorthodontic space closure. Am J Orthod Dentofacial Orthop2007;132:693-703.
32. Hamamoto N, Hamamoto Y, Kobayashi T. Tooth autotransplanta-tion into the bone grafted alveolar cleft: report of two cases withhistologic findings. J Oral Maxillofac Surg 1998;56:1451-6.
ics May 2012 � Vol 141 � Issue 5