multiple myeloma ash 2006 update jeffrey wolf, md director, myeloma program ucsf
TRANSCRIPT

MULTIPLE MYELOMA
ASH 2006 UPDATE
Jeffrey Wolf, MD
Director, Myeloma Program
UCSF

Myeloma ASH ReviewAbstracts to be covered
Abstract 795: Thal/Dex vs Dex frontline Abstract 57: Thal/Dex vs VAD frontline Abstract 796: Velcade/Dex frontline Abstract 56: Velcade/Dex vs VAD Abstract 798: Revlimid/Dex frontline Abstract 800: R-MP frontline Abstract 799: Revlimid/Dex (high dose) vs Revlimid/Dex
(lower dose) frontline Abstract 407: VMPT for relapse Abstract 404: Velcade/Doxil for relapse

WHAT SHOULD WE BE WHAT SHOULD WE BE LEARNING?LEARNING?
• Does the type of induction matter?Does the type of induction matter?
• Does CR matter? Does CR matter?
• Does transplant matter?Does transplant matter?
• What do we do for the non-transplant patient?What do we do for the non-transplant patient?

Thalidomide/Dex vs. DexThalidomide/Dex vs. Dex
Abstract #795Abstract #795

A Multicenter, Randomized, Double-Blind, A Multicenter, Randomized, Double-Blind, Placebo-Controlled Study Thalidomide Plus Placebo-Controlled Study Thalidomide Plus
Dexamethasone Versus Dexamethasone Dexamethasone Versus Dexamethasone Alone As Initial Therapy For Newly Alone As Initial Therapy For Newly
Diagnosed Multiple Myeloma (MM 003)Diagnosed Multiple Myeloma (MM 003)
S. Vincent Rajkumar, Mohamad Hussein, John Catalano, S. Vincent Rajkumar, Mohamad Hussein, John Catalano, Wieslaw Jedrzejczak, Svetlana Sirkovich, Marta Olesnyckyj, Wieslaw Jedrzejczak, Svetlana Sirkovich, Marta Olesnyckyj,
Zhinuan Yu, Robert Knight, Jerry Zeldis, and Joan BladZhinuan Yu, Robert Knight, Jerry Zeldis, and Joan Bladéé
Mayo Clinic, Rochester, MN; Cleveland Clinic, Cleveland, Ohio; Frankston Mayo Clinic, Rochester, MN; Cleveland Clinic, Cleveland, Ohio; Frankston
Hospital, Frankston, Australia; Medical Academy of Warsaw, Warsaw, Hospital, Frankston, Australia; Medical Academy of Warsaw, Warsaw, Poland; Kiev Institution of Oncology of the UAMS, Kiev, Ukraine; Celgene Poland; Kiev Institution of Oncology of the UAMS, Kiev, Ukraine; Celgene
Corporation, Summit, NJ, and Hospital Clinic, Barcelona, Spain.Corporation, Summit, NJ, and Hospital Clinic, Barcelona, Spain.
Rajkumar et al. ASH 2006, abstract # 795

Thalidomide 50→200* mg d 1-28
Dex 40 mg, d 1-4, 9-12, 17-20
Placebo d 1-28Dex 40 mg, d 1-4, 9-12, 17-20
X 4 COURSES
TTP
Same exceptDex d 1-4
Continue until PD
OS
RR
Safety
Trial DesignTrial Design
* Thalidomide dose escalated in all patients, over 4 weeks, to improve tolerability
Rajkumar et al. ASH 2006, abstract # 795

Response (RRC/IMWG)Response (RRC/IMWG) R
esp
on
se R
ate
(%)
* p=0.001
0
20
40
60
PR CR
69.4%*
Thalidomide/Dex
51.1%*
Placebo/Dex
PR+VGPR+CR
25.5%
8.1% *
35.3%
3.0% *
80 VGPR
35.7% *12.8% *
* CR+VGPR
p<0.0001
Rajkumar et al. ASH 2006, abstract # 795

Common Non-Hematological ToxicitiesCommon Non-Hematological Toxicities
0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0
EdemaEdema
AstheniaAsthenia
NeuropathyNeuropathy
PercentPercent
Thal/DexThal/DexGrade 3-4Grade 3-4Grade 1-2Grade 1-2 DexDex
Grade 3-4Grade 3-4Grade 1-2Grade 1-2
TremorTremor
InsomniaInsomnia
ConstipationConstipation
Rajkumar et al. ASH 2006, abstract # 795
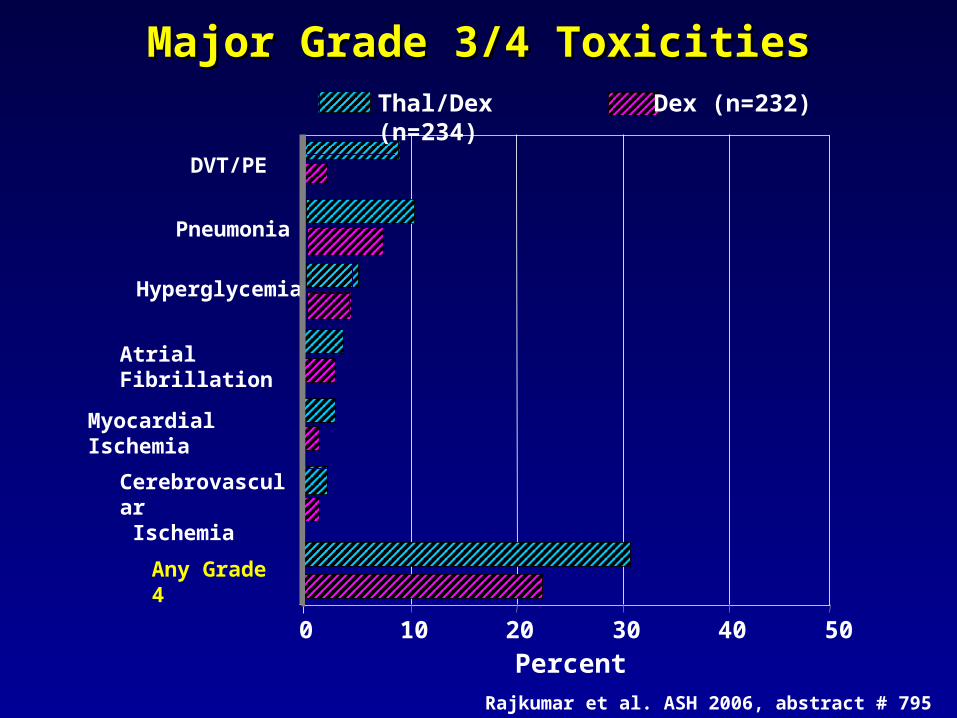
Major Grade 3/4 ToxicitiesMajor Grade 3/4 Toxicities
DVT/PE
Pneumonia
Hyperglycemia
Atrial Fibrillation
Cerebrovascular Ischemia
0 10 20 30 40 50
Percent
Thal/Dex (n=234) Dex (n=232)
Myocardial Ischemia
Any Grade 4
Rajkumar et al. ASH 2006, abstract # 795

Time to ProgressionTime to Progression
P<0.0001
Thalidomide/dex median time to progression: 22.4 monthsPlacebo/dex median time to progression: 6.5 months
HR (95% CI)0.43 (0.32, 0.58)
Rajkumar et al. ASH 2006, abstract # 795

Overall SurvivalOverall Survival
Thalidomide/Dex median overall survival: Not reachedPlacebo/Dex median overall survival: 32 months
HR (95% CI)0.82 (0.57, 1.16)
Rajkumar et al. ASH 2006, abstract # 795
Thalidomide/Dex vs. VADThalidomide/Dex vs. VAD
Abstract #57Abstract #57
A randomized study of Thalidomide + Dexamethasone
(Thal/Dex) compared with Vincristine, Adriamycine and
Dexamethasone (VAD) as a pre-transplant treatment in
newly diagnosed Multiple Myeloma (MM)
M. Macro, M.Diviné, S.Chevret, J.P.Fermand
& all members of the “Myélome-autogreffe” group
Paris, Amiens, Caen, Créteil, Limoges, Strasbourg
FRANCE
Macro et al. ASH 2006, abstract # 57
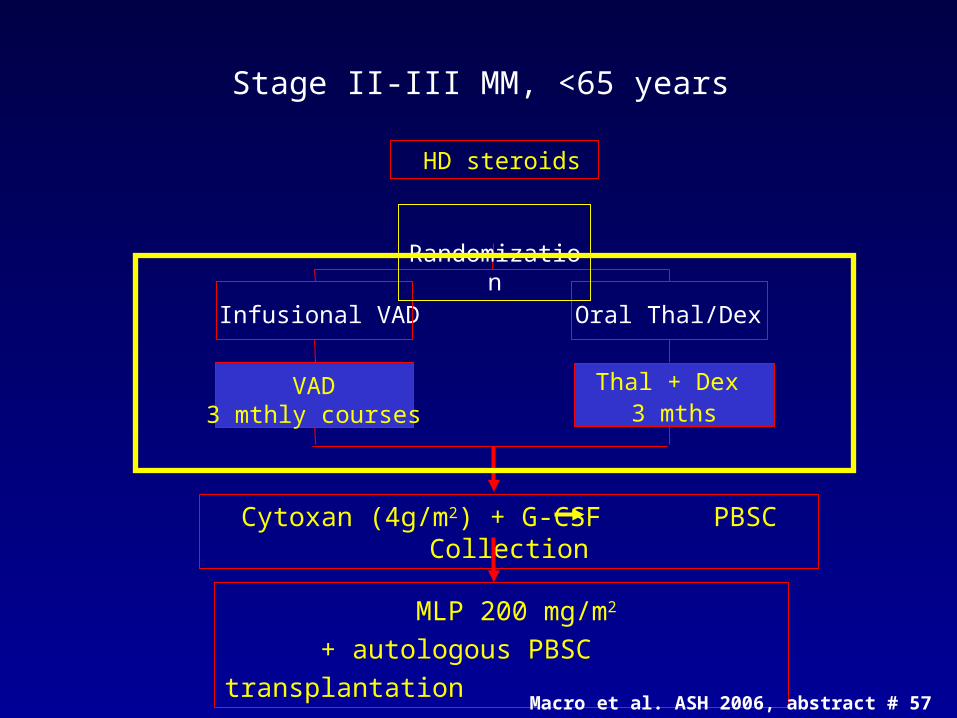
VAD3 mthly courses
Infusional VAD
Thal + Dex 3 mths
Oral Thal/Dex
HD steroids
Randomization
Cytoxan (4g/m2) + G-CSF PBSC Collection
MLP 200 mg/m2
+ autologous PBSC transplantation
Stage II-III MM, <65 years
Macro et al. ASH 2006, abstract # 57
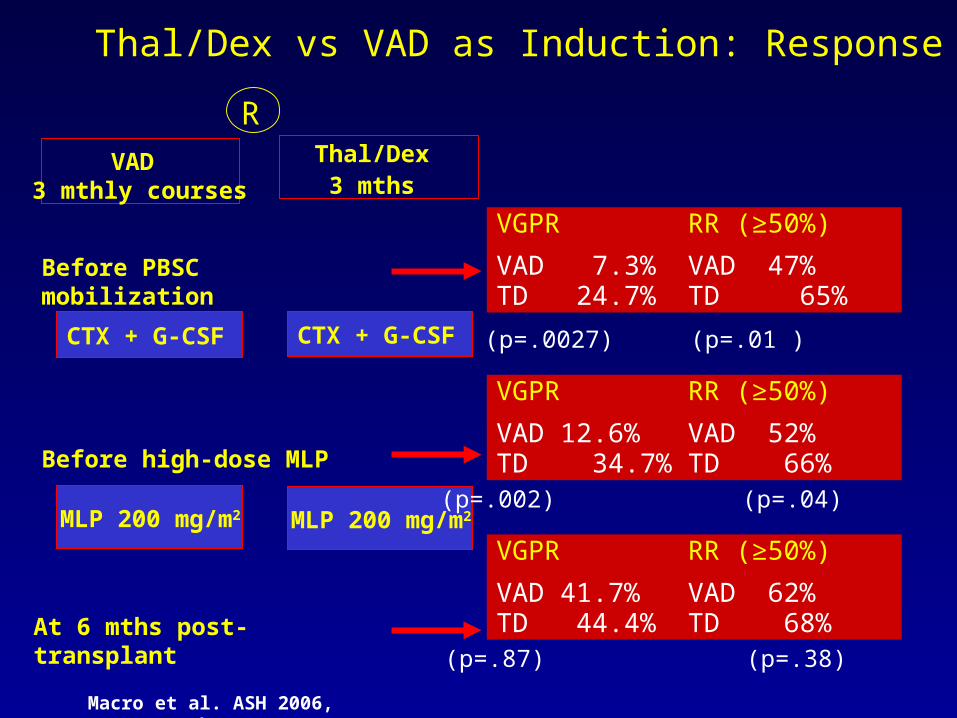
Thal/Dex vs VAD as Induction: Response
Macro et al. ASH 2006, abstract # 57
VAD 3 mthly courses
Thal/Dex 3 mths
R
MLP 200 mg/m2
CTX + G-CSF
MLP 200 mg/m2
CTX + G-CSF
VGPR RR (≥50%)
VAD 7.3% VAD 47% TD 24.7% TD 65%
Before PBSC mobilization
VGPR RR (≥50%)
VAD 41.7% VAD 62%TD 44.4% TD 68% At 6 mths post-transplant
VGPR RR (≥50%)
VAD 12.6% VAD 52% TD 34.7% TD 66% Before high-dose MLP
(p=.0027) (p=.01 )
(p=.002) (p=.04)
(p=.87) (p=.38)
VAD 3 mthly courses
Thal/Dex 3 mths
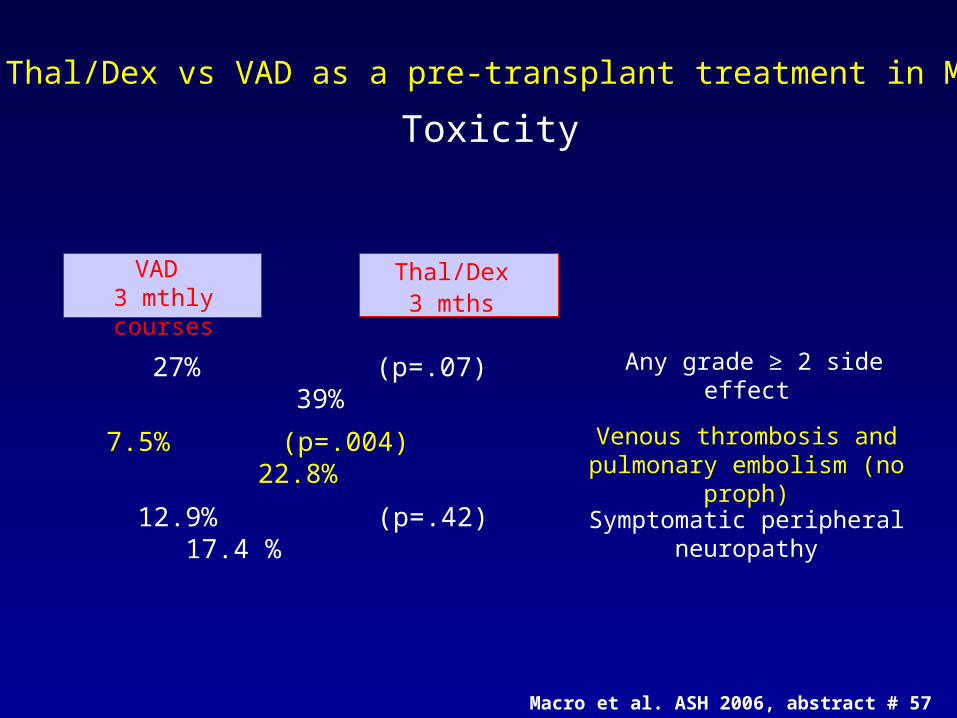
Thal/Dex vs VAD as a pre-transplant treatment in MM
Toxicity
Venous thrombosis and pulmonary embolism (no
proph)
7.5% (p=.004) 22.8%
Symptomatic peripheral neuropathy
12.9% (p=.42) 17.4 %
Any grade ≥ 2 side effect 27% (p=.07) 39%
Thal/Dex 3 mths
Macro et al. ASH 2006, abstract # 57

Velcade +/- DexVelcade +/- DexAbstract #796Abstract #796

Long-term follow-up of a phase 2 trial of bortezomib alone and in
combination with dexamethasone for the frontline treatment of
multiple myelomaS. Jagannath1, B. Durie1, J. Wolf1, E. Camacho1, D. Irwin1, J. Lutzky1, M. McKinley,1 E. Gabayan1,
A. Mazumder1, J. Crowley2, R. Vescio1
1Aptium Oncology Research Network, CA; 2Cancer Research and Biostatistics, WA
Jagannath et al. ASH 2006, abstract # 796
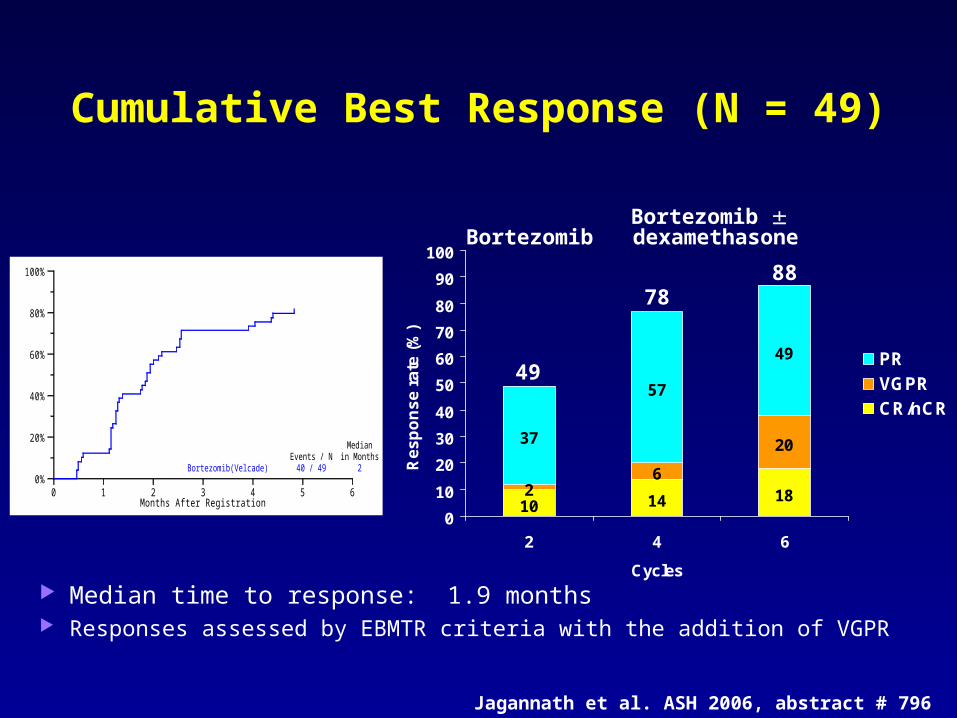
Cumulative Best Response (N = 49)
10 14 1826
2037
57
49
0
10
20
30
40
50
60
70
80
90
100
2 4 6
Cycles
Re
sp
on
se
ra
te (
%)
PRVGPRCR/nCR
BortezomibBortezomib
dexamethasone
49
7888
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Months After Registration
Bortezomib(Velcade)Events / N
40 / 49
Medianin Months
2
Median time to response: 1.9 months Responses assessed by EBMTR criteria with the addition of VGPR
Jagannath et al. ASH 2006, abstract # 796

OS In All Patients (N = 49)
Median follow-up 26.7 months Estimated 1- and 2-year survival rates: 92% and 85%
100%
80%
60%
40%
20%
0%0 12 24 36 48
Months after registration
Bortezomib (Velcade) 7/49 92% (83,100)
12-month
Deaths/N estimate
Jagannath et al. ASH 2006, abstract # 796

Velcade/Dex vs VAD
Abstract #56

56VELCADE/Dexamethasone (Vel/Dex) Versus VAD as
Induction Treatment Prior to Autologous StemCell Transplantation (ASCT) in Newly Diagnosed Multiple Myeloma (MM): An Interim Analysis of
the IFM 2005-01 Randomized Multicenter Phase III Trial.
Jean-Luc Harousseau,1 Gerald Marit,2 Denis Caillot,3 Philippe Casassus,4 Thierry Facon,5 Mohamad Mohty,6 Frederic Maloisel,7
Herve Maisonneuve,8 Carine Chaleteix,9 Lofti Benboubker,10 Dixie-Lee Esseltine,11 Michel Attal.12
1Hematology, Hôpital Hotel-Dieu, Nantes, France; 2CHU Bordeaux, Pessac, Bordeaux, France; 3Hematology Unit, Hôpital Bocage, Dijon, France; 4Hôpital
Avicenne, Bobigny, Paris, France; 5Hôpital Claude-Huriez, Lille, France; 6Institute Paoli-Calmettes, Marseille, France; 7Hôpital Civil, Strasbourg, France; 8CHD La Roche Sur Yon, La Roche Sur Yon, Vendee, France; 9CHU Clermont-Ferrand,
Clermont-Ferrand, Auvergne, France; 10Hematology and Cell Therapy Unit, CHRU Tours, Tours, France; 11Millennium Pharmaceuticals Inc, Cambridge, MA,
USA; 12Hôpital Purpan, Toulouse, France.

Vel/Dex vs. VAD Induction in Newly Diagnosed MM: Preliminary Analysis of IFM 2005-01 Trial
Treatment Scheme:
Second ASCT or RIC allo if <VGPR
Arm A1: VADArm A2: VAD + DCEP
ASCT
Induction ± Consolidation
Transplant 1
A B
Randomization Stratification for β2 microglobulin and Ch 13 abnormalities
Arm B1: Vel/DexArm B2: Vel/Dex + DCEP
ASCT
Harousseau et al. ASH 2006, abstract # 56

Vel/Dex vs. VAD Induction in Newly Diagnosed MM: Preliminary Analysis of IFM 2005-01 Trial
By Induction Therapy By Consolidation Therapy
VAD (A1+A2)
N=82
Vel/Dex (B1+B2)
N=79
No DCEP(A1+B1)
N=78
DCEP(A2+B2)N=64
CR/nCR 9% 20% 11% 28%
CR 4% 9% 3% 14%
VGPR 17% 23% 26% 13%
CR+VGPR 26% 43% 37% 41%
PR (incl VGPR) 59% 62% 68% 61%
CR+PR 67% 82% 79% 89%
Response: by investigator assessment; evaluated by modified EBMT criteria
Harousseau et al. ASH 2006, abstract # 56

Vel/Dex vs. VAD Induction in Newly Diagnosed MM: Preliminary Analysis of IFM 2005-01 Trial
Efficacy: Impact of baseline characteristics on post-induction response (preliminary analysis)
CR/nCR rateCharacteristic VAD (A1+A2) Vel/Dex (B1+B2)
β2M level
>3 mg/L 4/43 (9%) 8/41 (20%)
Del(13)
Yes 4/37 (11%) 9/36 (25%)
β2M, beta-2-microglobulin; Del(13), chromosome 13 deletion
Harousseau et al. ASH 2006, abstract # 56

Vel/Dex vs. VAD Induction in Newly Diagnosed MM: Preliminary Analysis of IFM 2005-01 Trial
VAD (A1+A2)
N=70
Vel/Dex(B1+B2)
N=68
TOTAL
N=138
Median CD34+ cells collected (x106/kg) 8.7 6.3 7.5
ITT pop receiving 1st ASCT, n (%) 58 (71%) 58 (73%) 116 (72%)
Median time to ANC ≥ 0.5 x 109/L, days 7 7 7
Median time to platelet count ≥ 20 x 109/L, days
1 1 1
Patients not requiring 2nd ASCT
n (%)32 (55) 45 (78) 77 (66)
Stem Cell Transplant: Preliminary data
Harousseau et al. ASH 2006, abstract # 56
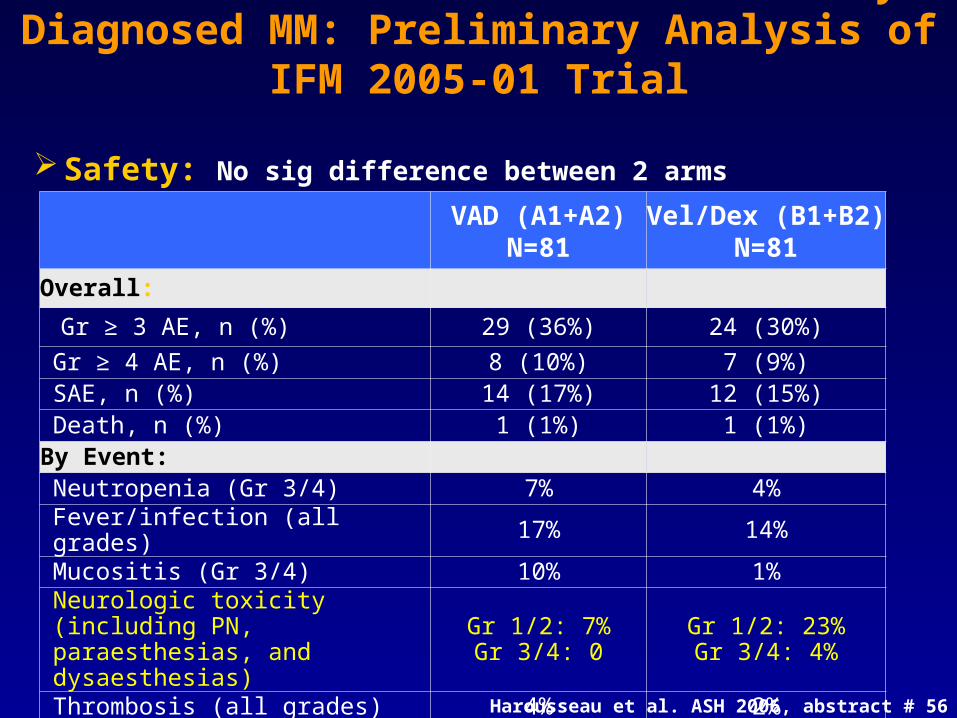
Vel/Dex vs. VAD Induction in Newly Diagnosed MM: Preliminary Analysis of IFM 2005-01 Trial
VAD (A1+A2) N=81
Vel/Dex (B1+B2) N=81
Overall:
Gr ≥ 3 AE, n (%) 29 (36%) 24 (30%)
Gr ≥ 4 AE, n (%) 8 (10%) 7 (9%)SAE, n (%) 14 (17%) 12 (15%)Death, n (%) 1 (1%) 1 (1%)
By Event:Neutropenia (Gr 3/4) 7% 4%Fever/infection (all grades) 17% 14%Mucositis (Gr 3/4) 10% 1%
Neurologic toxicity (including PN, paraesthesias, and dysaesthesias)
Gr 1/2: 7%Gr 3/4: 0
Gr 1/2: 23%Gr 3/4: 4%
Thrombosis (all grades) 4% 2%
Safety: No sig difference between 2 arms
Harousseau et al. ASH 2006, abstract # 56

What have We Learned?
The use of Vel/Dex over VAD results in fewer patients needing a 2nd transplant
The use of TD is more toxic than VAD (DVT’s and VTE’s) and results in similar outcomes post transplant
Percent of Patients who Achieved
VGPR
Vel/Dex
78%
VAD
55%
TD
44%
VAD
42%

Revlimid/DecadronFrontline
Abstract # 798

Results: Response to TherapyAll 34 pts assessed prior to transplant or any other therapy
All Patients No Transplant
Objective Response Rate
91%
CR 18% 24%
VGPR 38% 43%
PR 35%
Lacy et al. ASH 2006, abstract # 798

Toxicity > Grade 3
fatigue (21%) neutropenia (21%) anxiety (6%) pneumonitis (6%)
muscle weakness (6%) rash (6%) pulmonary embolism
(3%) with ASA prophylaxis
Lacy et al. ASH 2006, abstract # 798

Time in Months
Pro
po
rtio
n P
rog
ress
ion
-fre
e a
nd
Aliv
e
0 5 10 15 20 25
0.0
0.2
0.4
0.6
0.8
1.0
No TransplantTransplant
Progression Free Survival
2 yr PFS rate
83%
59%
Lacy et al. ASH 2006, abstract # 798

Time in Months
Pro
po
rtio
n A
live
0 5 10 15 20 25
0.0
0.2
0.4
0.6
0.8
1.0
No TransplantTransplant
Overall Survival
2 yr OS rate
90%
92%
Lacy et al. ASH 2006, abstract # 798

OS for 2 Novel agents in Newly Diagnosed MM in Combo with Dex: No Transplant
Rev/Dex: Lacy et al Vel/Dex: Jagannath et al
Revlimid/Melphalan/PrednisoneNewly Diagnosed
Abstract #800

1 2 3 4 21
Revlimid® 5–10 mg daily
Mel 0.18–0.25 mg/Kg
Prednisone 2 mg/Kg
Every 4–6 weeks for a maximum of 9 cycles
day
6 patients in each cohort with additional 15 pts in cohort 3 and 4
6+15100.25Cohort 4
6+15100.18Cohort 3
650.25Cohort 2
650.18Cohort 1
PatientsRevlimid® mg/dMelphalan mg/Kg/d
RMP: Treatment Schedule
Palumbo et al. ASH 2006, abstract # 800
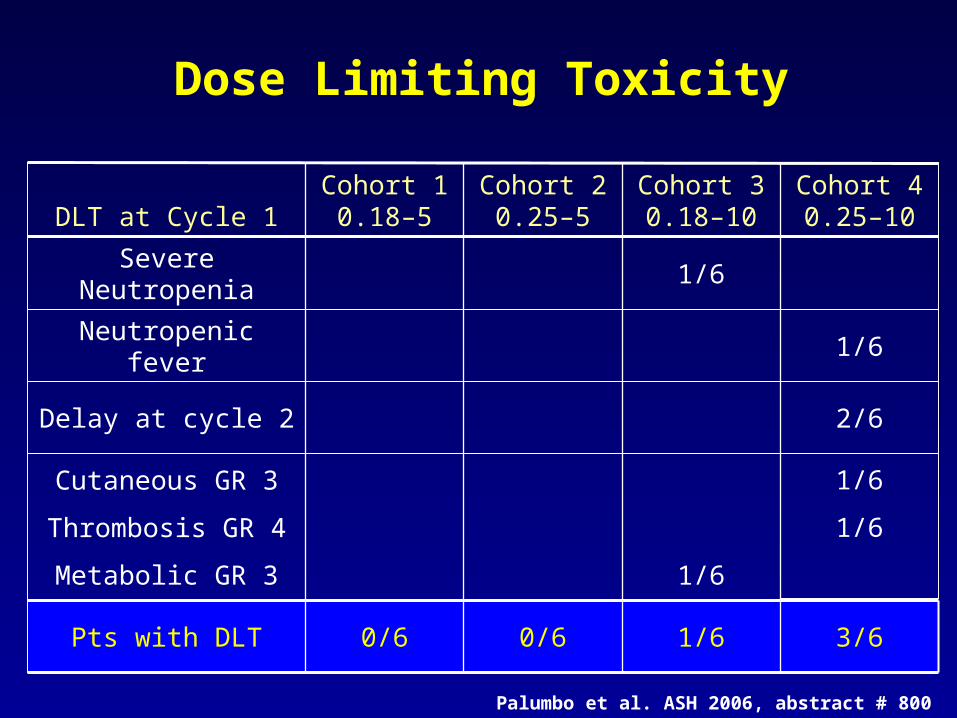
Dose Limiting Toxicity
3/61/60/60/6Pts with DLT
1/6
1/6
1/6
Cutaneous GR 3
Thrombosis GR 4
Metabolic GR 3
2/6Delay at cycle 2
1/6Neutropenic fever
1/6Severe Neutropenia
Cohort 40.25–10
Cohort 30.18–10
Cohort 20.25–5
Cohort 10.18–5DLT at Cycle 1
Palumbo et al. ASH 2006, abstract # 800
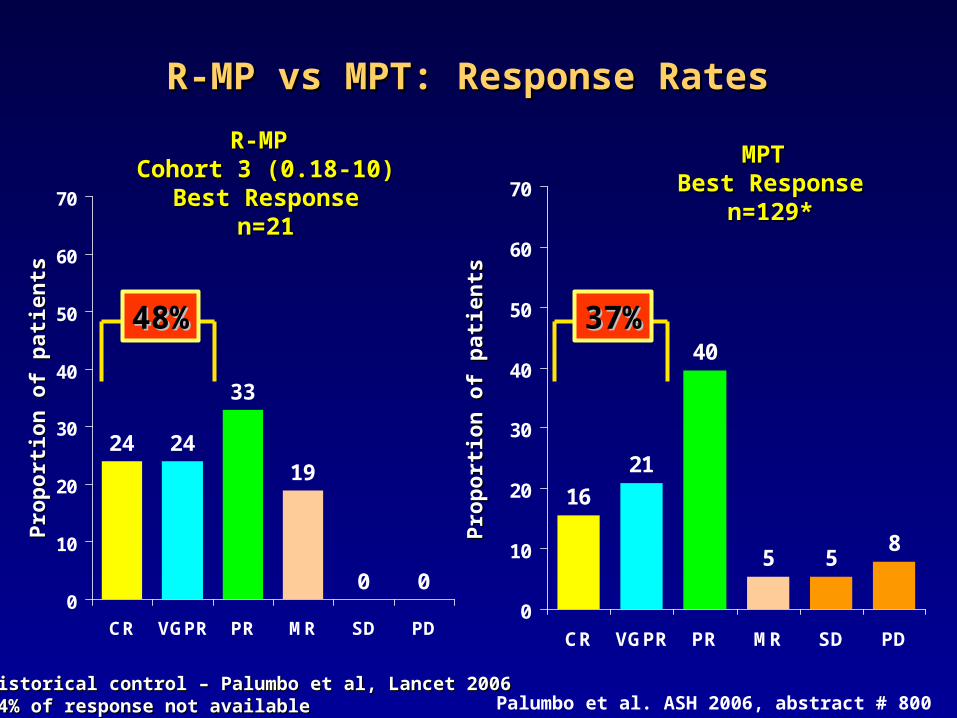
R-MP R-MP Cohort 3 (0.18-10)Cohort 3 (0.18-10)
Best ResponseBest Responsen=21n=21
MPT MPT Best ResponseBest Response
n=129*n=129*
*Historical control – Palumbo et al, Lancet 2006 *Historical control – Palumbo et al, Lancet 2006 5.4% of response not available5.4% of response not available
Pro
po
rtio
n o
f p
atie
nts
Pro
po
rtio
n o
f p
atie
nts
Pro
po
rtio
n o
f p
atie
nts
Pro
po
rtio
n o
f p
atie
nts
R-MP vs MPT: Response Rates R-MP vs MPT: Response Rates
24 24
33
19
0 00
10
20
30
40
50
60
70
CR VGPR PR MR SD PD
48%48%
16
21
40
5 58
0
10
20
30
40
50
60
70
CR VGPR PR MR SD PD
37%37%
Palumbo et al. ASH 2006, abstract # 800
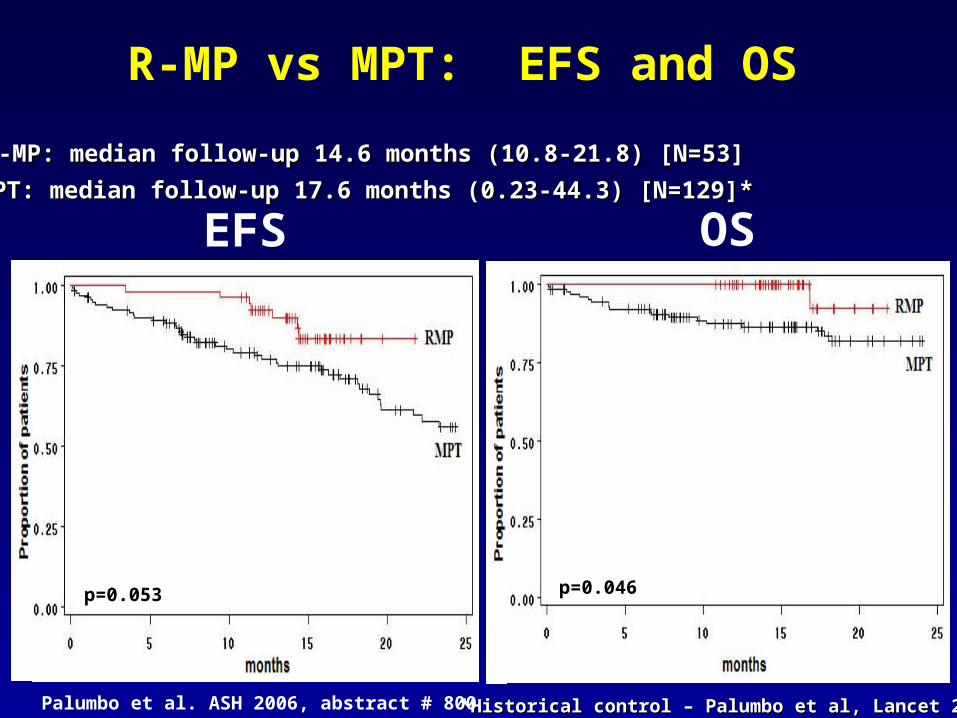
MPT: median follow-up 17.6 months (0.23-44.3) [N=129]*MPT: median follow-up 17.6 months (0.23-44.3) [N=129]*
R-MP: median follow-up 14.6 months (10.8-21.8) [N=53]R-MP: median follow-up 14.6 months (10.8-21.8) [N=53]
p=0.046p=0.053
R-MP vs MPT: EFS and OS
EFS OS
*Historical control – Palumbo et al, Lancet 2006 *Historical control – Palumbo et al, Lancet 2006 Palumbo et al. ASH 2006, abstract # 800

MPT Superior to MP
Previous Studies



Melphalan/Velcade/Prednisone (MVP)
Previous Study

Melphalan + Velcade + Prednisone(MVP)
12 of 16 CR patients tested for minimal residual disease; 6/12 (50%) achieved an immunophenotypic remission
Historical response with MP: 42% nCR + PR Hernandez, BJH, 2004
No DLTs observed in Phase I Phase II: 20% G4 myelosuppression
Phase II trial accruing, goal of 60 pts, dose will be 1.3 mg/m2
Response* (n = 53)
Bortezomib + Melphalan + Prednisone
CR 32%
nCR 11%
PR 45%
CR + PR 89%
* Modified EBMT criteria
Mateos et al. Blood, June, 2006
Newly Diagnosed
Response to Therapy

Revlimid/High Dose Dex vsRevlimid/Lower Dose Dex
Abstract #799

A Randomized Phase III Trial of Lenalidomide Plus High-Dose Dexamethasone Versus
Lenalidomide Plus Low-Dose Dexamethasone in Newly Diagnosed Multiple Myeloma (E4A03): A Trial Coordinated by the Eastern Cooperative
Oncology Group
S. Vincent Rajkumar, Susanna Jacobus, Natalie Callander, Rafael Fonseca, David Vesole, Philip Greipp
Mayo Clinic, Rochester, MN; Dana Farber Cancer Institute, Boston, MA;
University of Wisconsin, Madison, WI; Mayo Clinic Arizona, Scottsdale, AZ; St. Vincents Hospital, New
York, NY

RRAANNDDOOMMIIZZAATTIIOONN
Len + DexLen + Dexx4 cyclesx4 cycles(40 mg d1-4,(40 mg d1-4,9-12, 17-20)9-12, 17-20)
SchemaSchema
CR/PRCR/PR
Less Less than than PRPR
@ 4 months@ 4 monthsPts eligible for Pts eligible for SCT SCT proceed to SCT*proceed to SCT*
Thal + Thal + Dex Dex x 4 cyclesx 4 cycles
445 pts
Len + Low Len + Low dose Dex dose Dex x 4 cyclesx 4 cycles(40 mg wkly(40 mg wklyD1,8,15,22)D1,8,15,22)
CR/PR/StableCR/PR/Stable
Rajkumar et al. ASH 2006, abstract # 799

Serious adverse eventsSerious adverse eventsToxicityToxicity
Arm AArm A
(N=223)(N=223)
Arm BArm B
(N=222)(N=222)P valueP value
Infection/Pneumonia (Grade Infection/Pneumonia (Grade >=3)>=3) 16.1%16.1% 9.0%9.0% 0.0310.031
Fatigue (Grade >=3)Fatigue (Grade >=3) 11.7%11.7% 4.1%4.1% 0.0040.004
Hyperglycemia (Grade >=3)Hyperglycemia (Grade >=3) 5.8%5.8% 2.3%2.3% 0.0900.090
DVT/PE (Grade >=3)DVT/PE (Grade >=3) 18.4%18.4% 6.3%6.3% <0.001<0.001
Atrial fibrillation/flutter Atrial fibrillation/flutter (Grade>=3)(Grade>=3) 3.1%3.1% 0.0%0.0% 0.0150.015
Neuropathy (Grade >=3)Neuropathy (Grade >=3) 0.4%0.4% 1.4%1.4% 0.3720.372
Any non Hem toxicity (Grade Any non Hem toxicity (Grade >=3)>=3) 54.3%54.3% 39.6%39.6% 0.0020.002
Toxicity of Any Type (Grade Toxicity of Any Type (Grade >=4)>=4) 19.3%19.3% 11.3%11.3% 0.0250.025
Death (Grade 5)Death (Grade 5) 4.9%4.9% 0.5%0.5% 0.0060.006Rajkumar et al. ASH 2006, abstract # 799

Bortezomib (VelcadeBortezomib (Velcade®®)), Melphalan, , Melphalan, Prednisone and Thalidomide (VMPT) in Prednisone and Thalidomide (VMPT) in
Advanced Multiple MyelomaAdvanced Multiple Myeloma
Results of a Multicenter Phase I/II Results of a Multicenter Phase I/II StudyStudy
Antonio PalumboAntonio PalumboDiv. Hematology, University of Torino
Abstract 407
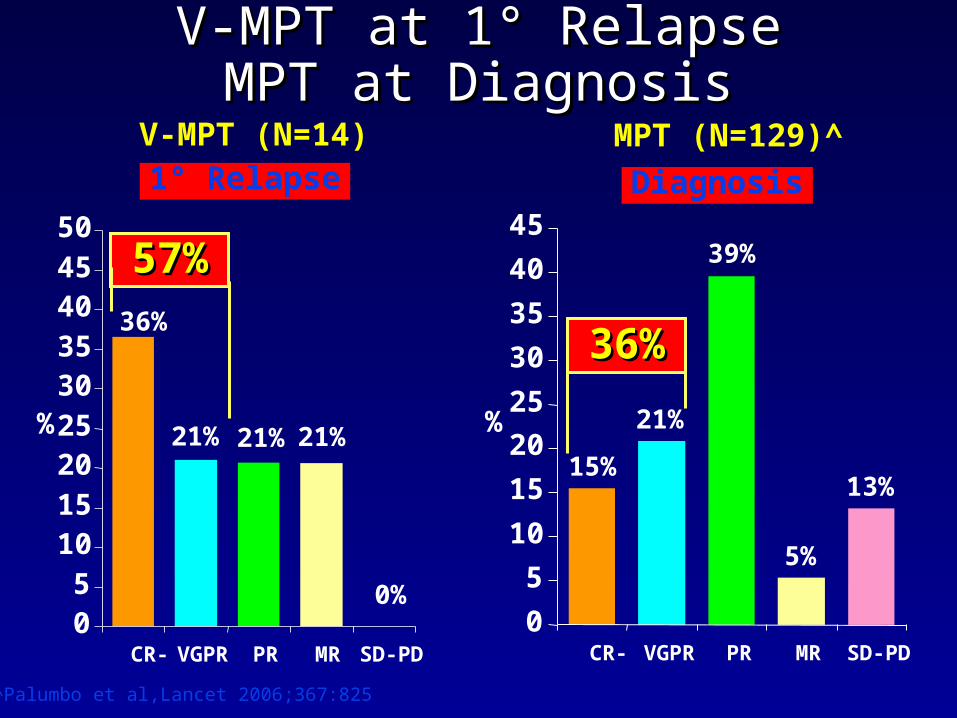
V-MPT at 1° RelapseV-MPT at 1° RelapseMPT at DiagnosisMPT at Diagnosis
V-MPT (N=14) MPT (N=129)^
0%
21%21%21%
36%
05
101520253035404550
CR- VGPR PR MR SD-PD
%
36%36%
13%
5%
39%
21%
15%
0
5
10
15
20
25
30
35
40
45
CR- VGPR PR MR SD-PD
%
^Palumbo et al,Lancet 2006;367:825
57%57%
Diagnosis1° Relapse

Study design: VMPT vs VMPStudy design: VMPT vs VMP
R
VMPT 9 courses
MaintenanceVelcade
Thalidomide
VMP9 courses
None
At diagnosis
End points: PFS, OS, RR, Safety
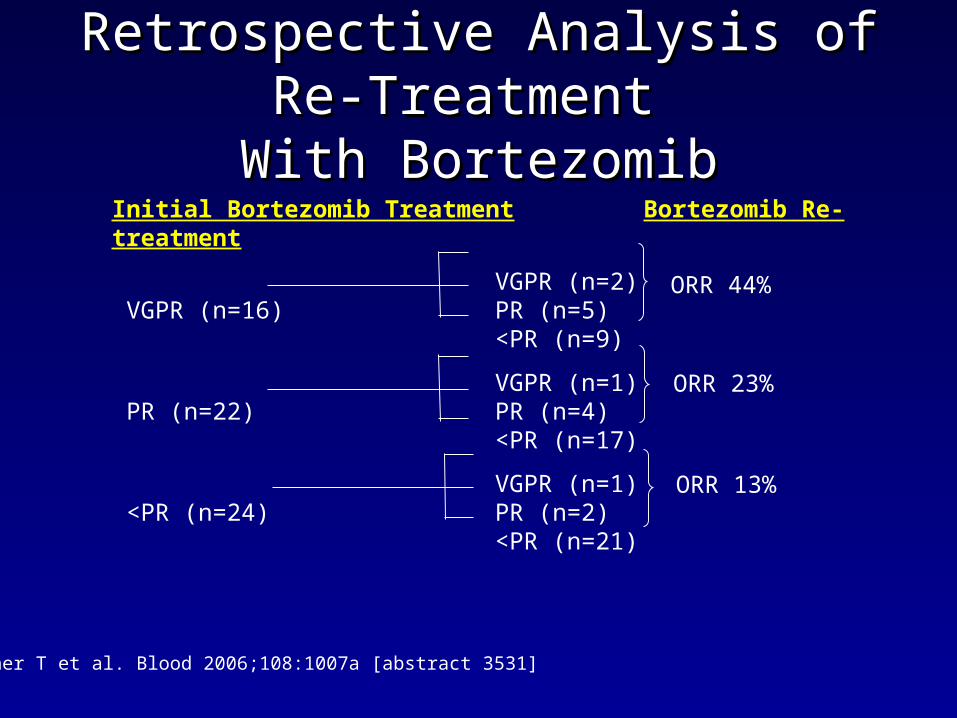
Retrospective Analysis of Re-Retrospective Analysis of Re-Treatment Treatment
With BortezomibWith Bortezomib
Conner T et al. Blood 2006;108:1007a [abstract 3531]
Initial Bortezomib Treatment Bortezomib Re-treatment
VGPR (n=2) VGPR (n=16) PR (n=5)
<PR (n=9)
VGPR (n=1) PR (n=22) PR (n=4)
<PR (n=17)
VGPR (n=1) <PR (n=24) PR (n=2)
<PR (n=21)
ORR 44%
ORR 23%
ORR 13%
PotpouriPotpouri

New Agents for MyelomaNew Agents for MyelomaClinical (1)Clinical (1)
Abstract Abstract ##
CategoryCategory CompoundCompound PhasePhase InstitutionInstitution
InvestigatorInvestigator
BiopharmBiopharm ResultResult
406406 Hsp 90 Hsp 90 Inh (17 Inh (17 AAG)AAG)
TanespimycinTanespimycin
(KOS-953) (KOS-953) + BZ+ BZ
II RichardsonRichardson
et.al.et.al.
KosanKosan
35743574 Anti-Anti-CD56CD56
BB-10901BB-10901 II Chanan - Chanan - KhanKhan
ImmunogeImmunogenn
activeactive
35753575 Anti-Anti-CD40CD40
HCD122 HCD122 (formerly (formerly Chir-12.12)Chir-12.12)
II BensingerBensinger NovartisNovartis activeactive
35763576 Anti-Anti-CD40CD40
SGN-40SGN-40 II HusseinHussein Seattle-Seattle-GeneticsGenetics
+/-+/-
activeactive

New Agents New Agents ForFor Myeloma MyelomaClinical (2)Clinical (2)
Abstract Abstract ##
CategoryCategory CompoundCompound PhasePhase InstitutionInstitution
InvestigatorInvestigator
BiopharmBiopharm ResultsResults
35793579 Hsp90 Hsp90 InhInh
IPI-504IPI-504 II SiegelSiegel
HackensackHackensack
etcetc
InfinityInfinity Too Too EarlyEarly
35803580 P38 P38 MAP-MAP-
Kinase Kinase InhInh
Scio-469Scio-469 IIII Siegel etcSiegel etc SciosScios Requires Requires BZBZ
35823582 Akt InhAkt Inh Perifosine Perifosine (KRX-0401(KRX-0401
IIII Richardson, Richardson, etcetc
KeryxKeryx Requires Requires Dex or Dex or
BZBZ
35833583 HDAC HDAC InhInh
PXD 101PXD 101 IIII Moffitt, etcMoffitt, etc CuragenCuragen Requires Requires
Dex Dex
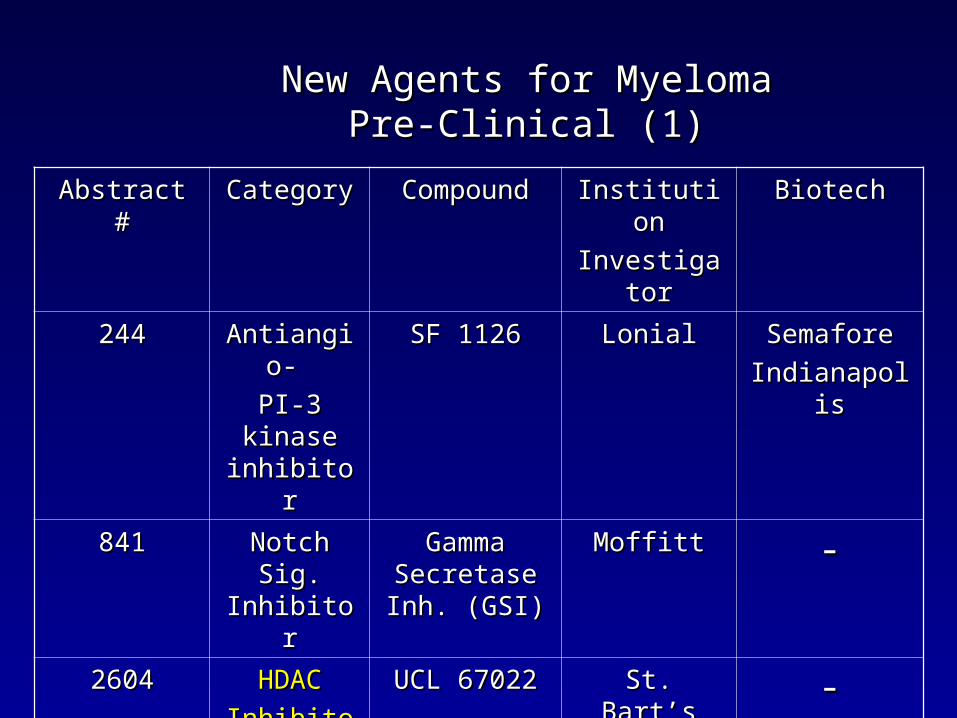
New Agents for MyelomaNew Agents for MyelomaPre-Clinical (1)Pre-Clinical (1)
Abstract #Abstract # CategoryCategory CompoundCompound InstitutionInstitution
InvestigatorInvestigator
BiotechBiotech
244244 Antiangio- Antiangio-
PI-3 kinase PI-3 kinase inhibitorinhibitor
SF 1126SF 1126 LonialLonial SemaforeSemafore
IndianapolisIndianapolis
841841 Notch Sig. Notch Sig. InhibitorInhibitor
Gamma Gamma Secretase Inh. Secretase Inh.
(GSI)(GSI)
MoffittMoffitt --
26042604 HDACHDAC
InhibitorInhibitor
UCL 67022UCL 67022 St. Bart’sSt. Bart’s --
34833483 HDACHDAC
InhibitorInhibitor
PXD 101PXD 101 BerensonBerenson CuragenCuragen
34273427 CD40CD40
LigandLigand
CD40L, CD40L, CD154CD154
BaylorBaylor --

New Agents for MyelomaNew Agents for MyelomaPre-Clinical (2)Pre-Clinical (2)
Abstract #Abstract # CategoryCategory CompoundCompound InstitutionInstitution
InvestigatorInvestigator
BiotechBiotech
34523452 B-cell Act B-cell Act Factor InhFactor Inh
(BAFF)(BAFF)
AMG 523AMG 523 FarberFarber AmgenAmgen
34603460 ERK ½ InhERK ½ Inh AZD 6244AZD 6244 FarberFarber --
34613461 Irreversible Irreversible Proteasome Proteasome
InhInh
PR-171PR-171 UNCUNC ProteolixProteolix
34623462 Organic Organic ArsenicArsenic
Z10-101Z10-101 Gale Gale BerensonBerenson
ZiopharmZiopharm
34813481 Proteasome Proteasome Inh.( Oral)Inh.( Oral)
MultipleMultiple -- ProteolixProteolix
