mumps: not an innocent bystander in solid organ transplantation
TRANSCRIPT
American Journal of Transplantation 2009; 9: 2186–2189Wiley Periodicals Inc.
C© 2009 The AuthorsJournal compilation C© 2009 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2009.02732.xCase Report
Mumps: Not an Innocent Bystander in Solid OrganTransplantation
M. C. Baasa, K. A. M. I. van Donselaara,
S. Florquinb, R. S. van Binnendijkc,
I. J. M. ten Bergea and F. J. Bemelmana,*
aRenal Transplant Unit, Department of Nephrology,Division of Internal Medicine, bDepartment of Pathology,Academic Medical Center, Amsterdam and cLaboratoryfor Infectious Disease and Screening, National Institute ofPublic Health and the Environment, Bilthoven, theNetherlands*Corresponding author: F. J. Bemelman,[email protected]
Recently two major outbreaks of mumps have oc-curred: in the UK more than 56,000 cases were noti-fied between 2004 and 2005, and in the United States,6,584 cases were reported in 2006. Most patients wereyoung healthy adults, in whom mumps normally hasa benign course. Little is known about mumps in theimmunocompromised patient. Here, we report a caseof a 56-year renal transplant recipient who developedacute irreversible transplant failure due to interstitialnephritis caused by mumps. RNA of the mumps viruswas detected in the urine as well as in a renal biopsy.In view of the ongoing presence of the mumps virusin the population, one should be aware of the possibleoccurrence of this infection in immunocompromisedpatients.
Key words: Interstitial nephritis, kidney transplanta-tion, mumps viral
Received 06 January 2009, revised 12 April 2009 andaccepted for publication 03 May 2009
A 56-year-old man, born in the Netherlands Antilles andsuffering from diabetic nephropathy, received a deceaseddonor renal transplant in September 2006. He was treatedwith basiliximab (two times 20 mg), prednisolone (10 mgdaily), ciclosporin aiming for a 12-h area-under-the-curve of3,250 mg ∗ h/l (correlating with a trough level of 130 lg/l)and mycophenolate sodium 720 mg b.i.d.
The patient had an uncomplicated posttransplant courseand was discharged with a creatinine clearance of100 mL/min. After 6 months, a scheduled biopsy was per-formed. This biopsy showed normal renal tissue without
signs of calcineurin toxicity or rejection. Following this re-sult, mycophenolate sodium was discontinued and treat-ment was continued with two drugs, prednisolone andciclosporin.
Fourteen months after transplantation, he presented withcomplaints of general malaise, myalgia, fever and a rash,present since 1 week. On physical examination, a bloodpressure of 140/80 mmHg and a temperature of 37.7◦Cwere found. His skin showed a macular erythema. Hiskidney transplant in the right iliac fossa was slightly ten-der on palpation. Laboratory investigation showed a serumcreatinine of 640 lmol/L, a hemoglobin of 9.1 mmol/L; leu-cocytes were 9.6.109/L with a differential count of 88%neutrophils, 0.2% eosinophils, 6.7% lymfocytes and 5.1%monocytes. The urinary sediment revealed 4–10 leuco-cytes/field. Urinary protein was trace positive. An ultra-sound of the kidney showed no signs of postrenal obstruc-tion. A transplant pyelonephritis was suspected and thepatient was treated with meropenem, pending blood andurine cultures. However, these cultures remained negativeand there was no improvement in renal function.
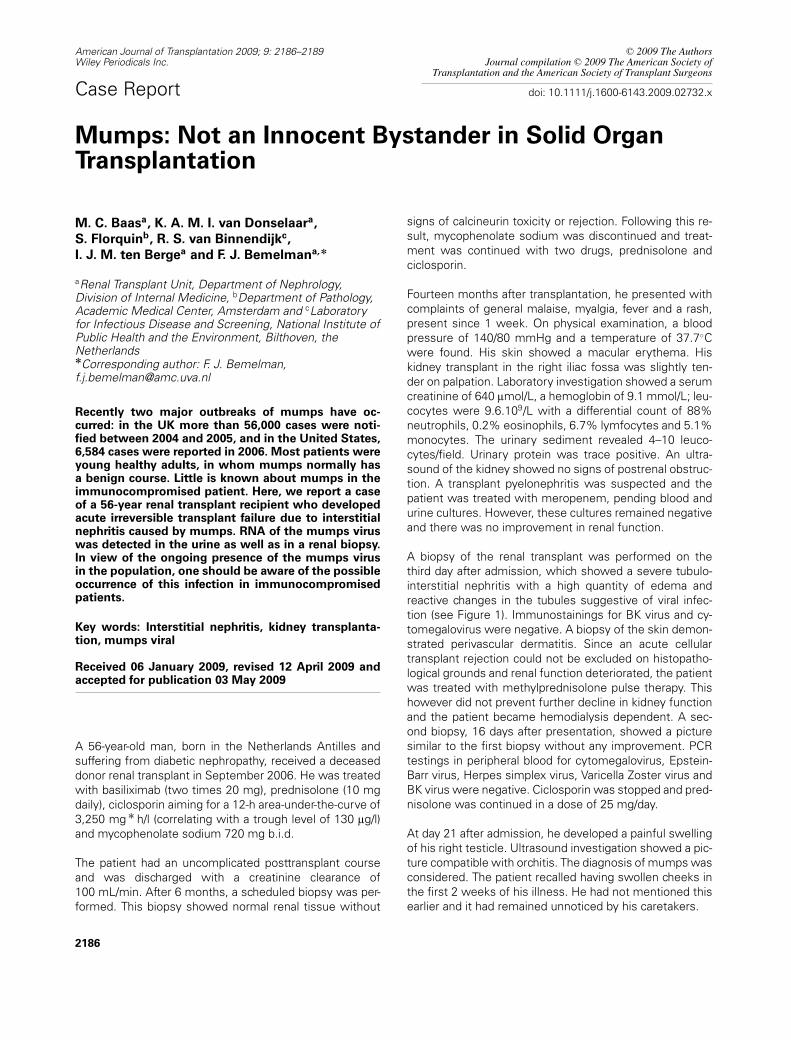
A biopsy of the renal transplant was performed on thethird day after admission, which showed a severe tubulo-interstitial nephritis with a high quantity of edema andreactive changes in the tubules suggestive of viral infec-tion (see Figure 1). Immunostainings for BK virus and cy-tomegalovirus were negative. A biopsy of the skin demon-strated perivascular dermatitis. Since an acute cellulartransplant rejection could not be excluded on histopatho-logical grounds and renal function deteriorated, the patientwas treated with methylprednisolone pulse therapy. Thishowever did not prevent further decline in kidney functionand the patient became hemodialysis dependent. A sec-ond biopsy, 16 days after presentation, showed a picturesimilar to the first biopsy without any improvement. PCRtestings in peripheral blood for cytomegalovirus, Epstein-Barr virus, Herpes simplex virus, Varicella Zoster virus andBK virus were negative. Ciclosporin was stopped and pred-nisolone was continued in a dose of 25 mg/day.
At day 21 after admission, he developed a painful swellingof his right testicle. Ultrasound investigation showed a pic-ture compatible with orchitis. The diagnosis of mumps wasconsidered. The patient recalled having swollen cheeks inthe first 2 weeks of his illness. He had not mentioned thisearlier and it had remained unnoticed by his caretakers.
2186
Mumps and Renal Failure
Figure 1: Kidney transplant
biopsy day 3 after admission,
showing a severe tubulo-
interstitial nephritis with
massive edema, dilatation
of the tubules and reactive
changes of the tubular epithe-
lial cells (A, magnification ×20).
Cytopathic changes (arrow) intubular cells suggestive of viralinfections were present (B, mag-nification ×40). Immunostainingsfor SV40 (parvovirus) (C) andfor cytomegalovirus (D) werenegative (magnification ×20).
At day 42 after presentation, the patient complained ofvomiting and vertigo. Physical examination showed a nys-tagmus and a tendency for the patient to collapse to hisright side. MRI scanning of the brain showed no abnormal-ities. A diagnosis of vestibular neuritis was made.
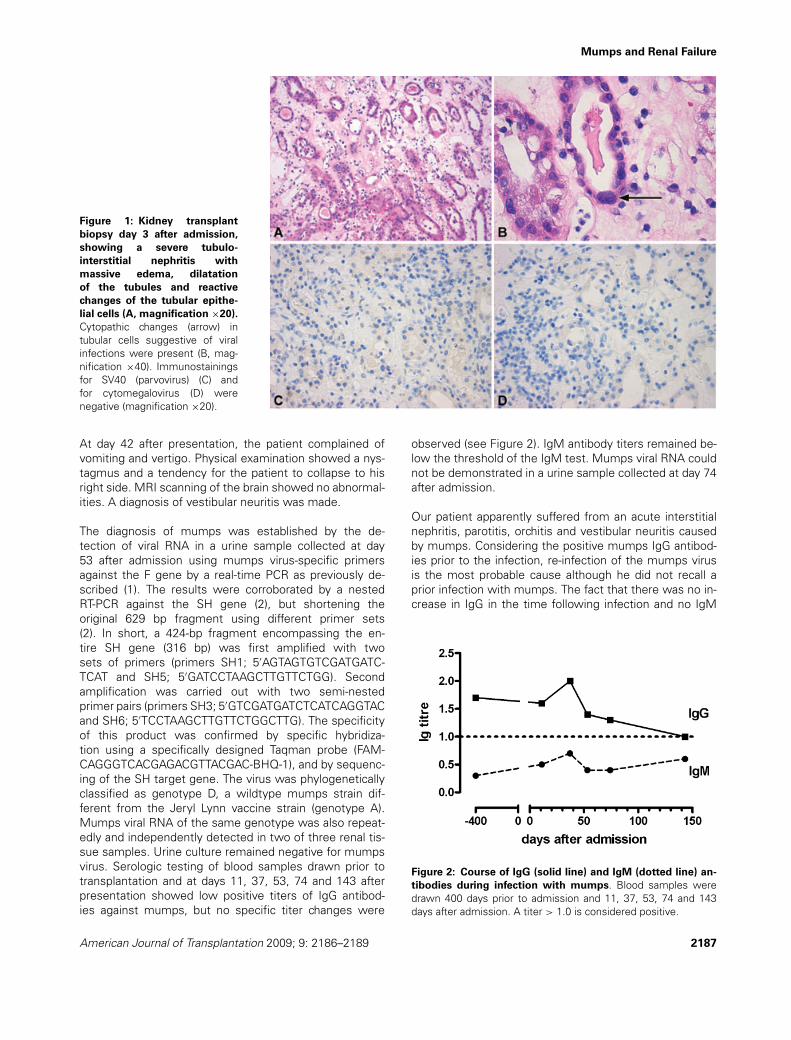
The diagnosis of mumps was established by the de-tection of viral RNA in a urine sample collected at day53 after admission using mumps virus-specific primersagainst the F gene by a real-time PCR as previously de-scribed (1). The results were corroborated by a nestedRT-PCR against the SH gene (2), but shortening theoriginal 629 bp fragment using different primer sets(2). In short, a 424-bp fragment encompassing the en-tire SH gene (316 bp) was first amplified with twosets of primers (primers SH1; 5′AGTAGTGTCGATGATC-TCAT and SH5; 5′GATCCTAAGCTTGTTCTGG). Secondamplification was carried out with two semi-nestedprimer pairs (primers SH3; 5′GTCGATGATCTCATCAGGTACand SH6; 5′TCCTAAGCTTGTTCTGGCTTG). The specificityof this product was confirmed by specific hybridiza-tion using a specifically designed Taqman probe (FAM-CAGGGTCACGAGACGTTACGAC-BHQ-1), and by sequenc-ing of the SH target gene. The virus was phylogeneticallyclassified as genotype D, a wildtype mumps strain dif-ferent from the Jeryl Lynn vaccine strain (genotype A).Mumps viral RNA of the same genotype was also repeat-edly and independently detected in two of three renal tis-sue samples. Urine culture remained negative for mumpsvirus. Serologic testing of blood samples drawn prior totransplantation and at days 11, 37, 53, 74 and 143 afterpresentation showed low positive titers of IgG antibod-ies against mumps, but no specific titer changes were
observed (see Figure 2). IgM antibody titers remained be-low the threshold of the IgM test. Mumps viral RNA couldnot be demonstrated in a urine sample collected at day 74after admission.
Our patient apparently suffered from an acute interstitialnephritis, parotitis, orchitis and vestibular neuritis causedby mumps. Considering the positive mumps IgG antibod-ies prior to the infection, re-infection of the mumps virusis the most probable cause although he did not recall aprior infection with mumps. The fact that there was no in-crease in IgG in the time following infection and no IgM
Figure 2: Course of IgG (solid line) and IgM (dotted line) an-
tibodies during infection with mumps. Blood samples weredrawn 400 days prior to admission and 11, 37, 53, 74 and 143days after admission. A titer > 1.0 is considered positive.
American Journal of Transplantation 2009; 9: 2186–2189 2187

Baas et al.
seroconversion indicates either the interference of im-munosuppressive medication (3) or previous exposure tomumps antigen. The latter argument has been substan-tiated during recent outbreaks of mumps in which vacci-nated individuals were shown to develop mumps diseasein the absence of a detectable IgM antibody response (vanBinnendijk, unpublished data).
This infection has had major consequences for our patient:despite withdrawal of all immunosuppressive therapy, ex-cept prednisolone, his renal function did not recover and heremained hemodialysis dependent. The orchitis was com-plicated by an abces in his right testicle for which surgicaldrainage was necessary. Until this date, he still suffersfrom vertigo after vestibular neuritis.
Mumps is an infection caused by a paramyxovirus. The in-fection is restricted to humans, is highly contagious andcan be transferred via direct contact or contaminated exc-reta. The course of mumps in immunocompetent adults isusually benign. During the outbreak in the United Statesin 2006, 8,654 cases were reported, of which only 85 re-quired hospitalization (4). The most common clinical man-ifestations are bilateral parotitis, orchitis and meningo-encephalitis. Orchitis occurs in 15–30% of adult men withinfection and can occur until 6 weeks after the first symp-toms. Neuritis vestibularis is rarely reported in associationwith mumps (5). Pancreatitis and myocarditis are also re-ported (6,7). Mumps can infect the urinary tract. The virushas a preference for the epithelium of the distal tubules, ca-lyces and ureter. A transient fall in renal function in mumpsis common (8,9). Reports of acute renal failure are scarceand seem to be associated with worse outcome. Up tonow, eight patients have been described of whom sevendied (7,10–15). One patient recovered spontaneously (15).Interstitial nephritis in a renal allograft has been reportedonly once before in a patient who had returned to dialysis2 months before infection with mumps (16).
The most sensitive tool to establish the diagnosis is PCRor culture of the virus. Virus shedding in immunocompe-tent patients has been demonstrated in saliva and urinefor at least 14 days after the onset of symptoms (17). Itcould well be that this time period is prolonged in the im-munocompromised host. In our patient, viral RNA could bedetected 53 days after presentation.
At the time our patient suffered from mumps, there was anoutbreak of mumps in the Netherlands in a region wherevaccine uptake is low, due to religious belief. The virus ofour patient genetically matched the virus (genotype D) thatcaused the outbreak. In our patient, the virus was detectedboth in urine and renal tissue samples in independent testsand at different time intervals. The patient could howevernot recollect any contact with people from that region.
Vaccination prevents 80% of cases with mumps (18). Thisfigure may increase when the vaccination is repeated. In
children with chronic renal disease, pretransplant vacci-nation with mumps vaccine only generates an adequateimmune response in 70.8% of the children (5,19,20).In transplant recipients, vaccination with live attenuatedvirus is relatively contraindicated, although in several smallstudies in children no adverse effects of mumps vaccina-tion were found (20,21). Pretransplant vaccination can beconsidered.
In conclusion, mumps infection should be included in thedifferential diagnosis of a febrile viral illness in the immuno-compromised patient, in particular when specific organsymptoms occur.
Conflict of Interest
None.
References
1. Uchida K, Shinohara M, Shimada S et al. Rapid and sensitive detec-tion of mumps virus RNA directly from clinical samples by real-timePCR. J Med Virol 2005; 75: 470–474.
2. Jin L, Beard S, Brown DW. Genetic heterogeneity of mumps virusin the United Kingdom: Identification of two new genotypes. JInfect Dis 1999; 180: 829–833.
3. Rentenaar RJ, van Diepen FN, Meijer RT et al. Immune respon-siveness in renal transplant recipients: Mycophenolic acid severelydepresses humoral immunity in vivo. Kidney Int 2002; 62: 319–328.
4. Dayan GH, Quinlisk MP, Parker AA et al. Recent resurgence ofmumps in the United States. N Engl J Med 2008; 358: 1580–1589.
5. Davis LE. Viruses and vestibular neuritis: Review of human andanimal studies. Acta Otolaryngol Suppl 1993; 503: 70–73.
6. Mumps epidemic—United kingdom, 2004–2005. MMWR MorbMortal Wkly Rep 2006; 55: 173–175.
7. Ozkutlu S, Soylemezoglu O, Calikoglu AS, Kale G, KaraaslanE. Fatal mumps myocarditis. Jpn Heart J 1989; 30: 109–114.
8. Lin CY, Chen WP, Chiang H. Mumps associated with nephritis.Child Nephrol Urol 1990; 10: 68–71.
9. Utz JP, Houk VN, Alling DW. Clinical and laboratory studies ofmumps. N Engl J Med 1964; 270: 1283–1286.
10. Anderson DM, Hutchinson DN. Renal damage and virus infection.Br Med J 1968; 3: 680–681.
11. Dastur F. Mumps and acute tubular necrosis. Practitioner 1968;201: 796–797.
12. Hughes WT, Steigman AJ, Delong HF. Some implications of fatalnephritis associated with mumps. Am J Dis Child 1966; 111: 297–301.
13. Kabakus N, Aydinoglu H, Bakkaloglu SA, Yekeler H. Mumps inter-stitial nephritis: A case report. Pediatr Nephrol 1999; 13: 930–931.
14. Miller JA. Med News (N.Y.). 1905: 585.15. Monteiro GE, Lillicrap CA. Case of mumps nephritis. Br Med J
1967; 4: 721–722.16. Aiello FB, Calabrese F, Furian L et al. Mumps-associated nephri-
tis mimicking acute rejection in a patient under chronic dialysistreatment because of graft dysfunction. Transpl Int 2002; 15: 523–524.
2188 American Journal of Transplantation 2009; 9: 2186–2189
Mumps and Renal Failure
17. Polgreen PM, Bohnett LC, Cavanaugh JE et al. The duration ofmumps virus shedding after the onset of symptoms. Clin InfectDis 2008; 46: 1447–1449.
18. Hviid A, Rubin S, Muhlemann K. Mumps. Lancet 2008; 371: 932–944.
19. Prelog M, Pohl M, Ermisch B et al. Demand for evalu-ation of vaccination antibody titers in children considered
for renal transplantation. Pediatr Transplant 2007; 11: 73–76.
20. Kano H, Mizuta K, Sakakihara Y et al. Efficacy and safety of immu-nization for pre- and post- liver transplant children. Transplantation2002; 74: 543–550.
21. Khan S, Erlichman J, Rand EB. Live virus immunization after ortho-topic liver transplantation. Pediatr Transplant 2006; 10: 78–82.
American Journal of Transplantation 2009; 9: 2186–2189 2189