musculosekeltal diseases and disorders: elbow and forearm ptp 521
TRANSCRIPT
Musculosekeltal Diseases and Disorders: Elbow and Forearm
PTP 521

2
Anteroposterior view: A
• Alignment:– Identify the structures
from a proximal to distal view
– Radial head should be aligned with the capitulum but not directly in contact with it
– Olecranon should be centered in the olecranon fossa
– Carrying angle should be noted and be ~ 15 dg.

3
Abnormal Anteroposterior View
• This view will demonstrate the following pathologies, if present:
• Fractures of the distal humerus – supra, trans, and intercondylar
• Fractures of the medial and lateral epicondyles
• Fractures of the capitulum, trochlea and lateral aspect of radial head
• Varus and Valgus deformities
• Secondary ossification centers of the distal humerus

4
Anteroposterior view: B
• Bone Density: pay particular attention to the radial head for any chips/fractures– Look for Trabecular lines
• Pay attention to the medial and lateral epicondyles for any lucencies or breaks in the margins

5
Ossification Centers• 6 ossification centers around the
elbow joint.
• Mnemonic C-R-I-T-O-E (Capitulum - Radius - Internal or medial epicondyle - Trochlea - Olecranon - External or lateral epicondyle).
• The ages at which these ossification centers appear are highly variable and differ between individuals.
• As a general guide you could remember 1-3-5-7-9-11 years.
– None should be open at age 13.
www.radiologyassistant.nl/en/4214416a75d87

6
C and S• Cartilage:
– Evaluated with an MRI, joint space is noted with the radial head and capitulum only
• Soft Tissue: not seen well on an AP view
• Fat Pad Sign (Sail Sign): evidence of swelling or bleeding anterior to the elbow
emedicine.medscape.com/article/389069-imaging
7
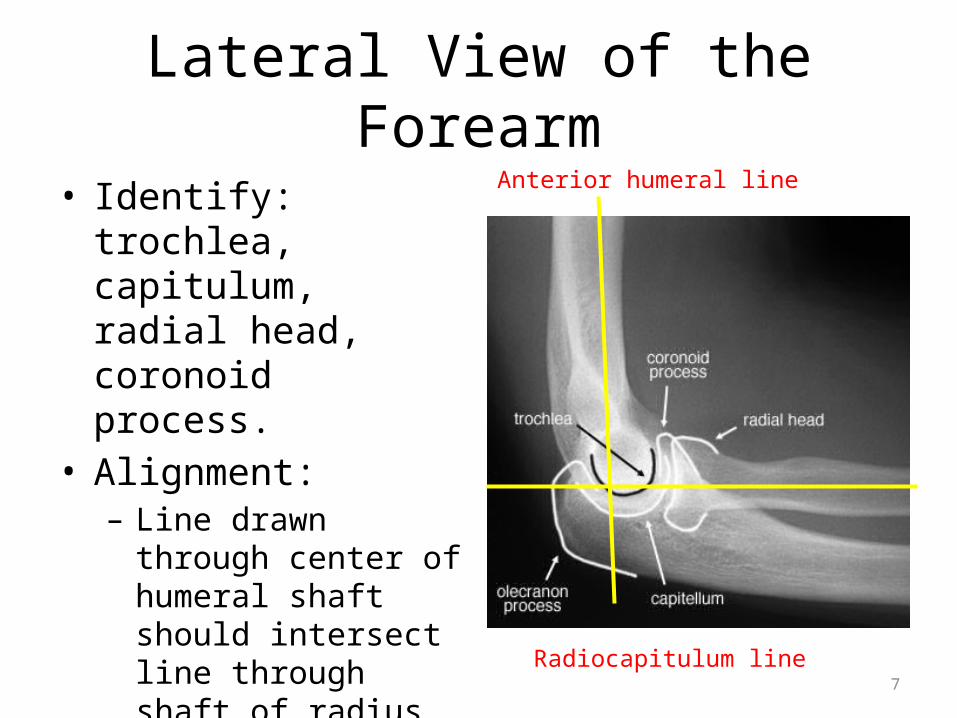
Lateral View of the Forearm
• Identify: trochlea, capitulum, radial head, coronoid process.
• Alignment:– Line drawn through
center of humeral shaft should intersect line through shaft of radius and be ~ 90 dg.
Anterior humeral line
Radiocapitulum line

8
Radiocapitulum line:
• Unless there is a dislocation of the radius, a line drawn through the center of the radius, should ALWAYS pass through the center of the capitulum.
• Bottom right: dislocation
http://www.radiologyassistant.nl/en/4214416a75d87
9
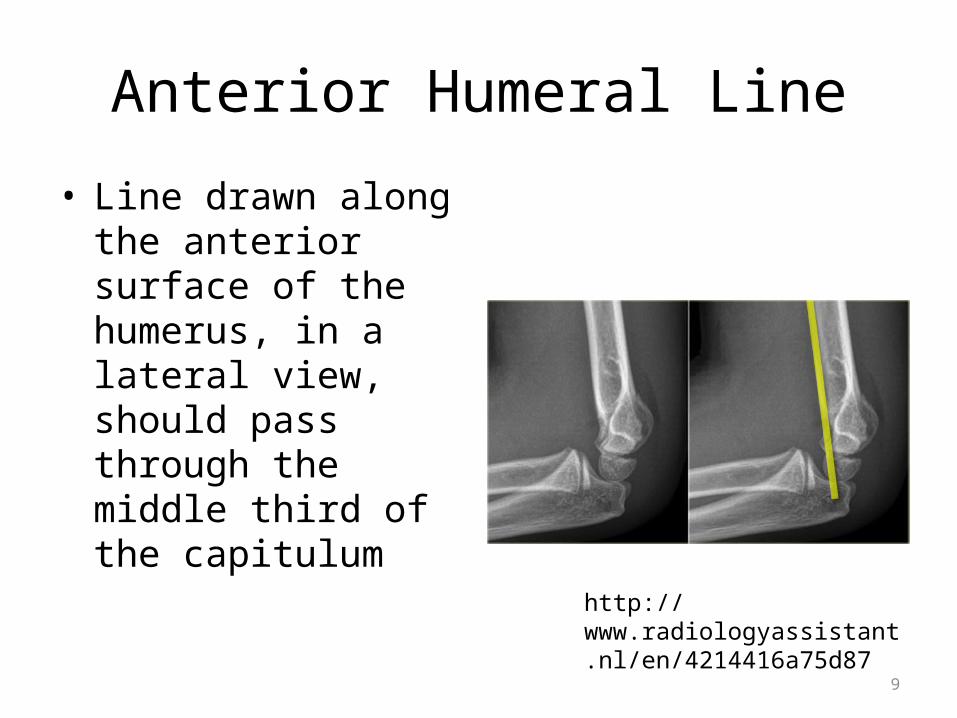
Anterior Humeral Line
• Line drawn along the anterior surface of the humerus, in a lateral view, should pass through the middle third of the capitulum
http://www.radiologyassistant.nl/en/4214416a75d87

10
Abnormal Lateral View
• The lateral view will demonstrate the following pathologies, if present:
• Supracondylar fractures of distal humerus
• Fractures of anterior radial head and olecranon
• Complex dislocations of the elbow joint
• Dislocation of the radial head
• pad sign (sail sign)

11
Lateral View
• Bone Density: view the radial head, trabecular lines

12
• Cartilage:– Able to see a joint space
between the radius and the capitulum
– Trochlea and the coronoid process
• Soft Tissue:– May or may not be seen
in this view– Evaluate for changes in
density of the tissue which may indicate swelling
– Fat pad sign (Sail sign) can be seen in this view as well

13
External Oblique View• Radiohumeral joint (long
white arrow)• Capitulum, radial head (yellow
arrow)• Radial neck (orange arrow)• Radial tuberosity, coronoid
process (dark blue arrowhead)• Trochlea notch/trochlea
articulation (light blue arrowheads)
• Proximal radioulnar articulation
http://www.ceessentials.net/article29.html
14
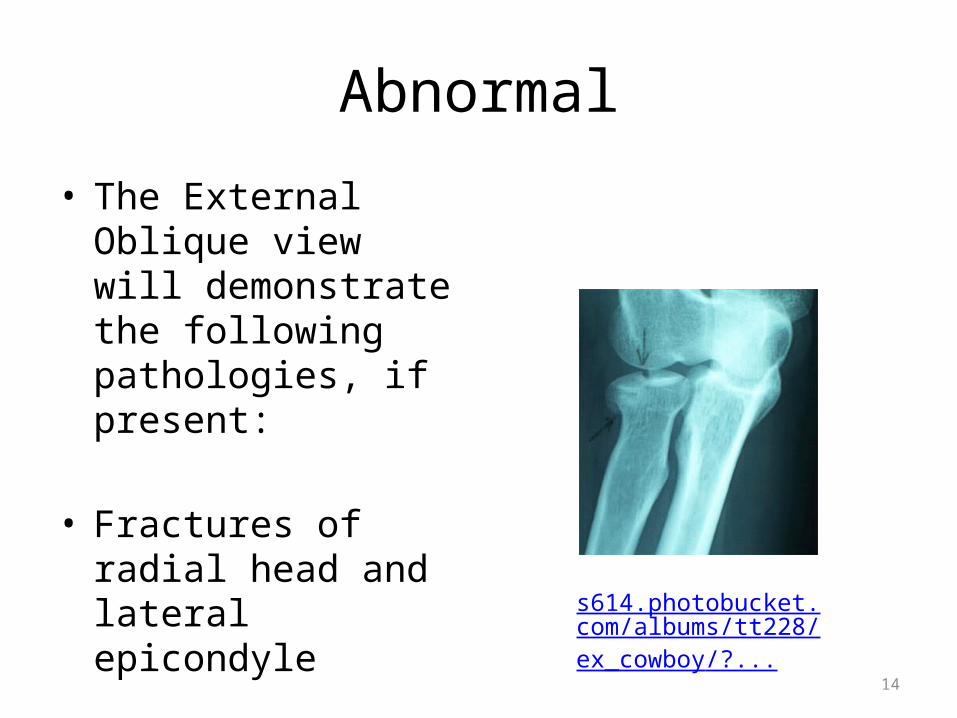
Abnormal
• The External Oblique view will demonstrate the following pathologies, if present:
• Fractures of radial head and lateral epicondyle
s614.photobucket.com/albums/tt228/ex_cowboy/?...

15
Internal Oblique
• This view is taken to demonstrate the coronoid process, trochlea notch, and medial trochlea
• Forearm is pronated ~ 45 dg
• Abnormal: will demonstrate fractures of the medial epicondyle and the coronoid process
http://www.ceessentials.net/article29.html

16
Radial Head/Capitulum or Trauma View
• Trauma View is when the radius is completely on top of the ulna, not overlapped.
• Humeroradial joint (white arrow)
• Radial head (dark blue arrow)
• Capitulum (orange arrow) radial notch of the ulnar and radioulnar joint (yellow arrow)
• Neck of the radius (light blue arrow)
http://www.ceessentials.net/article29.html
Look at this view and evaluate the difference between the lateral view and the trauma lateral view - Its in the radial head position

17
Radial Head /Capitulum Trauma View
• The trauma view will demonstrate the following– Fractures of radial head,
capitulum and coronoid process
– Abnormalities of the humeroradial and humeroulnar joints

18
CT Imaging
• Utilized to determine the following abnormal pathology:
• Complex fractures around the elbow, particularly comminuted fractures
• Healing process
• Non union of bones
• Secondary infections

19
CT Imaging of the Elbow
• MRI seems to replace a lot of CT imaging because of the soft tissue around the elbow
• These images are of a trochlear fracture (sorry, I couldn’t get better resolution)
www.jortho.org/2008/5/3/e5/index.htm

20
• These two CT images demonstrate the radioulnar articulation.
• On the left is a coronal image of the elbow showing the radioulnar joint (A) and on the right the head of the humerus (C) and ulna (B) that form the joint. www.ceessentials.net/article29.html

21
• On the left is a sagittal cut through the elbow
• On the right a coronal cut through the elbow.
• Both pictures demonstrate the humeroradial joint formed by the capitulum of the humerus (A) and the head of the radius (B).
• Reconstructions from axial datawww.ceessentials.net/article29.html

22
• Humeroradial Joint
• 3D volume rendered image demonstrating the humeroradial joint (A).
• The sagittal CT image demonstrates this articulation formed by the articulation (B) fovea of the head of the radius, and (C) capitulum of the humerus. www.ceessentials.net/article29.html

23
Can you name the anatomy?(Don’t click until you are ready to answer)
A = cornoid process, ulnaB = coronoid fossa, humerus
C = olecranon processD = olecranon fossa
www.ceessentials.net/article29.html

24
Midsagittal plane CT• Demonstrates the positions of
the anterior (B) and posterior (A) fat pads.
• If these fat pads are elevated following trauma, it may indicate intra-articular hemorrhage secondary to fracture of the radial head or neck.
• Sail sign as seen on the radiographs.
www.ceessentials.net/article29.html

25
MRI Imaging
• Demonstrates the following pathology:– Abnormalities of the
ligaments, tendons and muscles
• Lateral epicondylitis• Bicipital tendonitis• Ulnar collateral ligament
injury• Radial collateral ligament
injury
– Bone Contusion– Capsular ruptures– Joint effusions– Synovial Cysts– Hematomas– Osteochondritis
Dissecans– Epiphyseal fractures in
children

26
MRI Imaging
• Axial view, T1 weighted– Humerus– Ulna– Tendons– Ligaments – image black– Nerves– Vascular– Muscles
lateral medial

27
Axial View
• What is the anatomy of 1-5?
• 1= Biceps Brachii• 2= Brachialis• 3= Brachial artery• 4= Humerus• 5= Triceps
http://anatomy.med.umich.edu/radiology/xray/arm_mri_zoom.html

28
• CFT: common flexor tendon
• CET: common extensor tendon
• RCL: radial collateral ligament
• UCL: ulnar collateral ligament

29
CORMPGR
• Coronal Plane• Sequence: MPGR
(Multiplanar Gradient Recalled) This is an echo pulsed sequence
• This image demonstrates the humerus, ulna, radius is not in the picture just yet
• Radial collateral lig• Ulnar collateral lig
medial

30
CORPD
• Coronal View• Proton Density
• Here you can see the radius as well as the ulna, humerus, olecranon
31
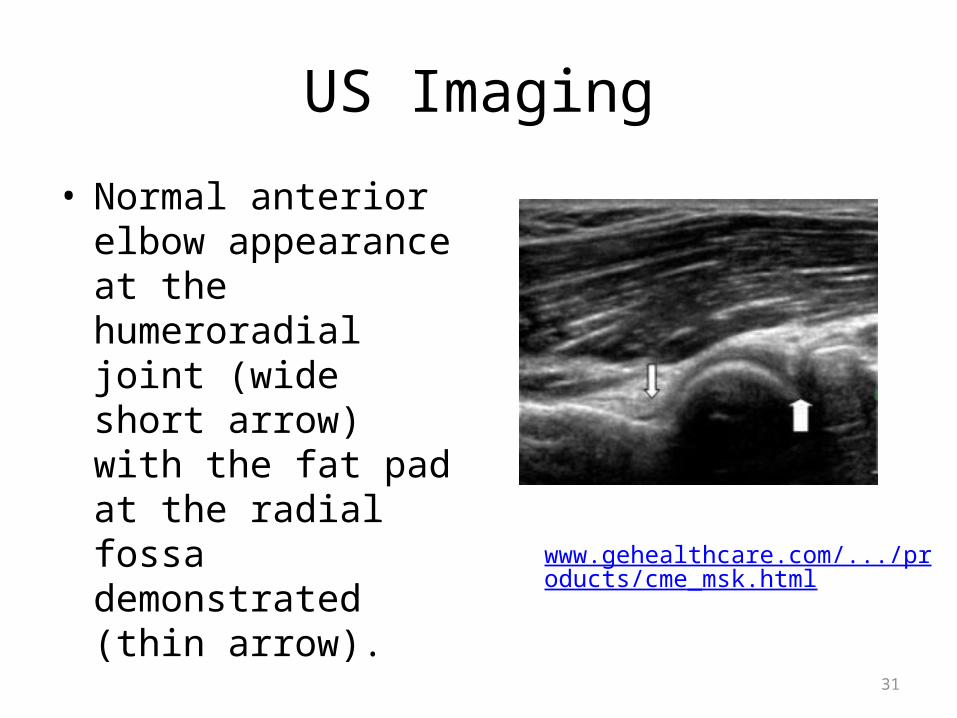
US Imaging
• Normal anterior elbow appearance at the humeroradial joint (wide short arrow) with the fat pad at the radial fossa demonstrated (thin arrow).
www.gehealthcare.com/.../products/cme_msk.html

32
• Normal distal biceps tendon (arrows) with insertion deep to vein (longitudinal)
www.gehealthcare.com/.../products/cme_msk.html

33
• Normal lateral common extensor tendon origin (arrows) with normal hyper- echogenicity of the longitudinal tendon
www.gehealthcare.com/.../products/cme_msk.html

34
• Normal medial epicondyle, common flexor tendon origin (large arrows on hyperechoic longitudinal tendon ) and ulnar collateral ligament (small arrows on hypoechoic ligament).
www.gehealthcare.com/.../products/cme_msk.html

35
• Normal ulnar nerve at the joint in longitudinal (left) and transverse (right) planes (arrows).
www.gehealthcare.com/.../products/cme_msk.html

Musculoskeletal Injury
Bone
Fractures
Arthritic Disorders
BruiseOther
Muscle
Strain and Inflammation
Rupture
Trigger Points
Tendon
tendonosis
strain
Nerve
Entrapment
Ligament
Sprain and Inflammation
Rupture
Capsule and Joint
Arthritis: OA and RA
Osteochondrosis
Dislocations
Other - Bursitis
Systems that refer pain to area
Other joints that refer pain to area

37
Fractures: Musculoskeletal Practice Pattern 4G
Fractures of the Distal Humerus1. Suprachondylar fractures: extra-articular
• Most common fracture in children- 65%• Uncommon fracture in adults• Left arm more than right – protective response• 98% occur with arm extended and wrist
dorsiflexed• Possible neurovascular complications: ~22%
neuro and 10% vascular• Possible permanent impairment and deformity
McKinnis LN, 2005

38
Gunstock Deformity
• Common complication of a suprachondylar fracture
39
• SX: – purple discoloration of hand, – severe pain in forearm muscles initially– paresthesias as the dysfunction progresses
• Signs: – cool pale extremity with altered pulse – pain on passive stretch – swelling initially – numbness distal to the ischemic region

40
2. Transcondylar: intracapsular but extraarticular fracture
• Common in elderly
3. Epicondylar Fractures: extra-articular
4. Condylar Fractures
McKinnis LN, 2005

41
5. Intercondylar Fractures – T intercondylar, Y
Intercodylar Medial or Lateral Condyle
6. Intra-Articular Fractures– Compressive forces
across the elbow
McKinnis LN, 2005

42
Volkmann's Ischemia
Compartment Syndrome • Prolonged ischemia of the forearm muscles
– muscle necrosis – replacement of tissue with fibrous tissue – severe deformities of the hand and wrist – paralysis of muscles. – Three stages: mild, moderate and severe
• Causes: – Arterial injury caused by an open laceration, – Arterial disruption secondary to a severely displaced
fracture or dislocation

43
Fractures of the Radial Head: Mason Classification System
• Type I• Non-displaced fracture• Often missed on x-ray• Positive posterior fat pad
sign • RX: minimal
immobilization, early ROM

44
Radial Head Fracture
• Type II• Displaced fracture• Separation or
angulations of the fracture fragment
• RX: ORIF, early motion

45
Radial Head Fractures
• Type III• Comminuted fracture of
the entire head• Children ages 4-14• RX: ORIF and early
motion

46
Radial Head Fractures
• Type IV• Comminuted fracture • Dislocation of the elbow• Usually cause some
functional limitation• RX: radial head
resection

47
Fractures of the Coronoid Process
• RX:– Open reduction generally
necessary– Concern for elbow
instability
• Classified: Regan-Morrey– Type I: tip of coronoid– Type II: less than 50%
coronoid tip– Type III: more than 50%
of the coronoid
boneandspine.com/wp-content/uploads/2009/02/c...

48
Fractures of the Olecranon
• MOI: fall onto the flexed elbow
• MOI: Boxer’s elbow: avulsion fracture of the olecranon

49
Monteggia Fracture
• Dislocation of radial head – most common lateral or anterolateral, posterior rare
• Fracture of ulnar metaphysis or diaphysis
50
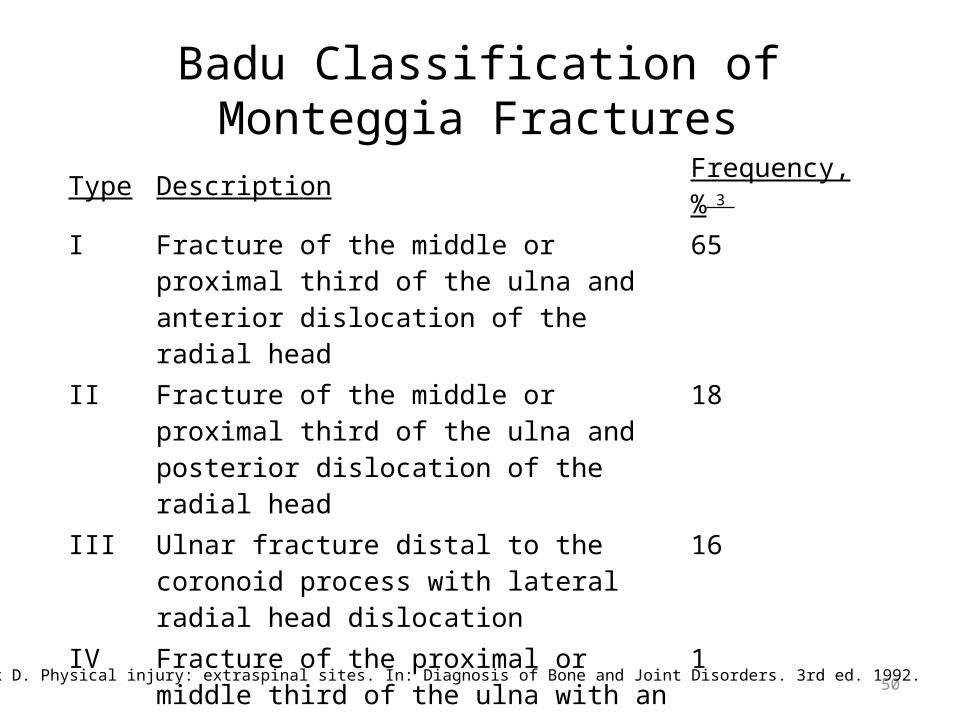
Badu Classification of Monteggia FracturesType Description Frequency, % 3
I Fracture of the middle or proximal third of the ulna and anterior dislocation of the radial head
65
II Fracture of the middle or proximal third of the ulna and posterior dislocation of the radial head
18
III Ulnar fracture distal to the coronoid process with lateral radial head dislocation
16
IV Fracture of the proximal or middle third of the ulna with an anterior dislocation of the radial head and fracture of the proximal third of the radius
1
Resnick D. Physical injury: extraspinal sites. In: Diagnosis of Bone and Joint Disorders. 3rd ed. 1992.

51
Galeazzi Fracture
• Fracture of distal shaft of radius
• Dislocation of distal radial ulnar joint

52
Muscle and Tendon Dysfunctions
• Overuse Injuries– 1. Risk Factors: Intrinsic and Extrinsic– 2. Types: Lateral epicondylitis, Medial epicondylitis, Triceps tendonitis, Bicipital Tendonitis, bursitis, ligamentous injuries
• Trauma

53
Soft Tissue Injuries of the Elbow
• Lateral Epicondylitis
• Medial Epicondylitis
• Triceps Tendonitis
• Biceps Strain
• Myositis Ossificans

54
Lateral Epicondylitis
• Adults 35 years or older: occupation or hobby involves repetitive extension of the wrist i.e. carpenter, electrician, tennis, baseball, or golf
• Etiology: unknown: cumulative trauma causes inflammatory process at ECRB origin
• Differential Diagnosis: Posterior Interosseous Syndrome and C6-7, T 4 syndromes
55
SX of Lateral Epicondylitis:
• Gradual onset• Pain over lateral epicondyle• Pain associated with gripping• May have some shoulder, neck pain associated
with it
56
Signs of Lateral Epicondylitis:• ROM: full, passive movement into extension, may be
painful at end range• Limited wrist flexion combined with finger flexion at
end range• Strength: painful resisted wrist extension and radial
deviation• Joint Play: full and pain free• Palpation: tender over the lateral epicondyle• Special tests: + Cozens test, + Mill’s test, - Middle
Digit Extenstion Test
57
Medial Epicondylitis
• Golfer’s elbow• Symptoms
– Pain on medial side of elbow– Involved in repetitive flexion activities of wrist
finger flexion and active pronation

58
Signs of Medial Epicondylitis:
• Palpation: direct over the medial epicondyle• Resisted movement: resisted flexion of the
fingers increases pain but is strong, may have a loss of strength with gripping activities
• Observation: swelling/erythema on medial aspect

59
Triceps Tendonitis:
1) Onset: sudden, severe strain as the arm is fully extended or with a sudden snapping of the elbow into extension
2) Signs: pain with resisted elbow extension – may be strong
or weak pain with PROM of elbow flexion and shoulder
flexion – passive stretch of the muscle

60
Biceps Muscle Strain:
1) Onset: athletic activity, – very strong elbow flexion force – hyperextension force leading to elongation and
stretch. • need to be aware of possible anterior posterior joint
capsule impingement.
– Biceps rupture: may have a history of repeated corticosteroid injections

61
2) SX: depends on the degree of the strain 3) Signs: depends on the degree of the strain

62
Myositis Ossificans• Common complication of
trauma to the elbow, muscle ossifies and can
bridge the elbow joint.
• Cause: contusion to the brachialis muscle from a posterior dislocation or a suprachondylar fracture.
• May also be caused by too vigorous stretching after an injury and elbow immobilization
• SX: pain with elbow flexion and extension
• Signs: palpable area on muscle, warm to touch, bony end feel, limitation of range, + radiograph
www.uwec.edu

63
Medial and Lateral Ligamentous structures of the elbow

64
Posterolateral Rotary Instability
• MOI: – Rotational displacement
of the ulna– Radius subluxes or
dislocates posterior
• Forces: : axial compression, external rotation and valgus (lateral to medial) force
• Sx: catching, clicking and locking
• Pain• Apprehension with
elbow supinated and fully extended
• Signs: lateral pivot-shift is most sensitive

65
• Three stages– Stage I: Lateral Ulnar
Collateral Ligament disruption
• Stage II:– Anterior and posterior
disruption– Perched dislocation

66
• Stage III:– III A: all soft tissue
except Ulnar collateral lig (medial side) is disrupted
– III B: UCL disrupted
– III C: Entire distal humerus stripped of soft tissue

67
Ligament Sprain
Medial (Ulnar) Collateral Ligament sprain (little league elbow): – Articular damage to the radiohumeral and ulnohumeral joint
with repeated stresses
– MOI: adolescent involved with overhead throwing activities. • FOOSH injury
– The compressive forces at the radiohumeral joint and distraction forces on the medial aspect of the elbow will overstretch and injure the ligament.

68
Little League Elbow

69
• Articular damage to the capitulum,
• Ligamentous instability of the medial elbow
• Tardy nerve palsy
– may see medial muscle hypertrophy.
– In adolescents whose growth plate has not yet ossified, it may cause on avulsion injury of the medial epicondyle.
– Complete ligamentous rupture is usually associated with acute trauma

70
• Radiology: – Osteochondritis
Dissecans of the Capitulum
• Note fracture of the condlye on the ulnar aspect of the elbow
71
• SX: pain/swelling on the medial aspect of the elbow
• Patient c/o pain with throwing or pushing motions

72
Signs:
• Valgus instability with ligamentous stress test
• Tender with varus stress if the radiohumeral joint is involved
• Painful axial compression with the radius on the humeral
• Joint tender over the MCL ligament
• Severe cases will get locking of the elbow due to capitulum fragments

73
Joint Dysfunctions of the Elbow
Dislocations
Osteoarthritis
RA
Osteochondritis Dessicans
http://orthoinfo.aaos.org/fact/thr_report.cfm?Thread_ID=239&topcategory=Arm

74
Elbow Dislocations
• MOI:– FOOSH– Direct Trauma– MVA
• Described by the direction the ulna and radius have been displaced relative to the humerus
• Most common types– Posterior or Posterolateral direction

75
Perched Dislocation
• Not a true dislocation
• Subluxation of the joint
• Less ligamentous damage
• Humerus is PERCHED on top of the coronoid process of the ulna

76
Posterior:
a. straight posterior

77
b. posterolateral - c. posteromedial d. Divergent
What soft tissue structures may be involved with each one of these type of dislocations?
78
Additional injuries to soft tissue
• Anterior capsule rupture• Radial collateral ligament damage• Brachial muscle injuries• Extensor tendon injuries• Radial head and neck fractures• Tear of brachial artery• Nerve injuries• Avulsion/entrapment of medial epicondyle

79
Anterior Dislocation
• Rare 1-2% of the population
• Ulnar collateral ligament involved, what other structures?
• Fractures of radial head may occur

80
Dislocations
• Physical Exam: gross deformity of the elbow
• Anatomical triangle is disrupted
• Elbow held in 45 dg flexion
• Forearm appears shorter (posterior) and olecranon is more prominent posterior boneandspine.com/.../10/dislocation-elbow.jpg

81
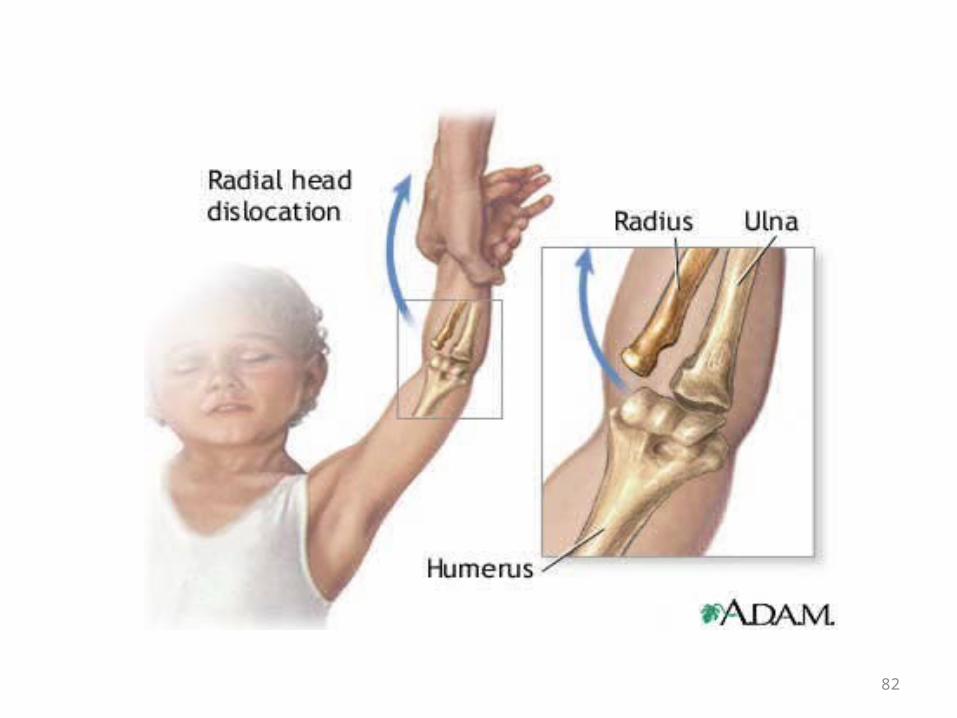
Subluxations of the Radius
• Nursemaids Elbow– MOI: axial force on the arm– SX: pain, child will refuse to move the arm– Relocation, no immobilization needed
82

83
Osteoarthritis of the Elbow
• Fill in signs and symptoms

84
Rheumatoid Arthritis
http://uwmsk.org:8080/EvasMSKTF/stories/storyReader$509

85
Elbow Replacement
http://www.orthop.washington.edu/uw/elbowreplacement/tabID__3376/ItemID__61/PageID__5/Articles/Default.aspx

86
Osteochondritis Dissecans and osteochondrosis (Panner’s Disease) • Described by some as different stages, same entity
related to age of individual and direction and level of activity
• Controversy: Panners disease encompasses entire capitellum and occurs at a younger age (5-16)
• MOI: Vascular insufficiency from repetitious lateral compression at the humeroradial joint

87
Panners Disease
• Younger child, no ossification of growth plates

88
12- 15 year old: Osteochondritis Dissecans
• Leading cause of permanent disability to the young pitching athlete
• Repetitive lateral compression at the radiocapitellar joint during late cocking
• Loose body formation in joint

89http://www.physsportsmed.com/issues/1999/02_99/hall.htm

90
Signs, Symptoms & Interventions
• SX: pain present over lateral and anterior elbow
• Pain increase with deep palpation, pronation and supination
• ROM: extension limited by 20 dg or more
• Intervention: Rest, gentle stretching
• NO loose bodies: may drill bone to restore vascular supply
• LOOSE bodies: may need arthroscopic surgery to remove the loose bodies

91
Bursitis:
12 bursae about the elbow with 3 of clinical significance
1) Olecranon bursae allows smooth gliding of the skin on the triceps
Onset: traumatic, inflammatory (gout), prolonged pressure

92
• Signs: painless swelling of the bursae on the posterior aspect of the elbow (goose egg)
• Nearly full AROM and PROM into elbow flexion secondary to compression of the bursae by the triceps
• Classic inflammatory responses with redness, temp. increases, edema, and pain

93
2) Bicipital Radial Bursitis:• Bursae is between the radial tuberosity and the insertion of
the biceps tendon.
• Allows smooth gliding of the tendon on the bone. SX: pain in the antecubital fossa, radiating up the biceps tendon Signs: – palpation: deep at the radial tuberosity and insertion of the biceps
tendon– Resisted movements of elbow flexion and supination are painful
94
3) Radiohumeral Bursitis:
• Deep to the common extensor tendons, attaches to the lateral epicondyle.
• Aids in the gliding of the extensor tendons over the radiocapitellar bones/ capsule of the elbow complex.
• Frequently is diagnosed as lateral epicondylitis with signs and symptoms similar to the lateral epicondylitis