musculoskeletal disorders in children brian romito, do pgy iv im/er march 2, 2006 presented dr marty...
TRANSCRIPT

Musculoskeletal Disorders Musculoskeletal Disorders in Childrenin Children
Brian Romito, DOBrian Romito, DOPGY IV IM/ERPGY IV IM/ER
March 2, 2006March 2, 2006Presented Dr Marty HellmanPresented Dr Marty Hellman

Fracture PatternsFracture Patterns
Weakest layer is the physis (growth plate)Weakest layer is the physis (growth plate)
Hypertrophic cell zoneHypertrophic cell zone
Susceptible to shearing/bending Susceptible to shearing/bending yields fracture yields fracture
Peds; 2 types of Fracture (Fx); Open Physis vs Peds; 2 types of Fracture (Fx); Open Physis vs closed Physisclosed Physis

DefinitionsDefinitions
• Physis; ephyiseal cartilagePhysis; ephyiseal cartilage
• Epiphysis; part of long bone (not shaft) a Epiphysis; part of long bone (not shaft) a center of ossification, separated from shaft by center of ossification, separated from shaft by layer of cartilagelayer of cartilage
• Metaphysis; a conical section of bone b/t the Metaphysis; a conical section of bone b/t the Epiphysis & diaphysis of Long BonesEpiphysis & diaphysis of Long Bones
• Diaphysis; “THE SHAFT”Diaphysis; “THE SHAFT”

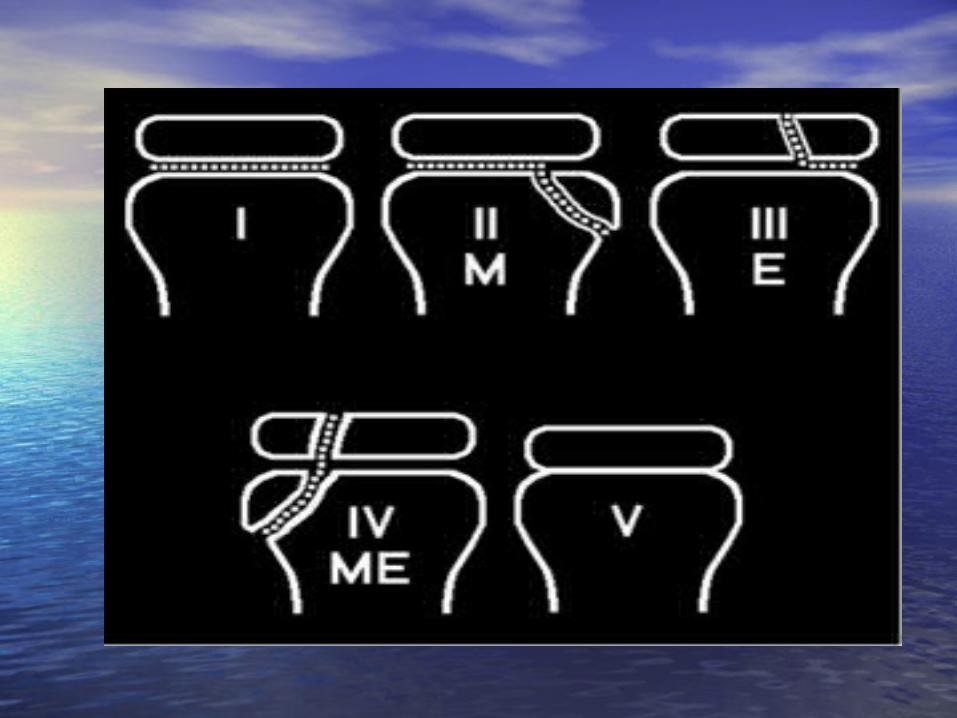
Salter Harris ClassificaionSalter Harris Classificaion• Type I: epiphysis seperates from Metaphysis thru Type I: epiphysis seperates from Metaphysis thru
the Growth Plate onlythe Growth Plate only
• Type II: Thru Physis & Metaphysis Type II: Thru Physis & Metaphysis
• Type III: Thru Physis & EpiphysisType III: Thru Physis & Epiphysis
• Type IV: Thru Epiphysis, Physis & MetaphysisType IV: Thru Epiphysis, Physis & Metaphysis
• Type V: Crushing of Condrocytes; Physis CrushedType V: Crushing of Condrocytes; Physis Crushed

Tx of Salter Harris Fx’sTx of Salter Harris Fx’s• Type I: Type I:
• Pt tenderness over physis after injury; joint Pt tenderness over physis after injury; joint swelling & joint effusion possibly seen on Xray swelling & joint effusion possibly seen on Xray
• Periosteal attachments intactPeriosteal attachments intact
• Low risk of growth disruption Low risk of growth disruption
• Splint, cold compress & elevationSplint, cold compress & elevation

SH Fx for 100SH Fx for 100
• Type II: closed reduction of any Type II: closed reduction of any displacementdisplacement
• Immobilization, Ice, elevation Immobilization, Ice, elevation
• Ortho follow upOrtho follow up
• Don’t forget the pain meds…Don’t forget the pain meds…

Salter Harris fx tx for 200Salter Harris fx tx for 200
• Type III:Type III:
Open Reduction definative Ortho TxOpen Reduction definative Ortho Tx
Type IV: ORIFType IV: ORIF
Type V: Casting, Ortho monitoring, Type V: Casting, Ortho monitoring, anticipation of Bone growth arrestanticipation of Bone growth arrest

Torus Fractures…Torus Fractures…
• Buldging or buckling of periosteum “AKA Buldging or buckling of periosteum “AKA Bluckle Fx” Bluckle Fx”
• No visible difformity 2 shape of No visible difformity 2 shape of extermity, soft tissue swelling and extermity, soft tissue swelling and tenderness.tenderness.
• Reduction rarely necessary, splint, ortho Reduction rarely necessary, splint, ortho follow upfollow up


Greenstick fx’sGreenstick fx’s
• Cortical disruption & periosteal tearing on Cortical disruption & periosteal tearing on the convex side of the bone and intact the convex side of the bone and intact periosteum on the concave side of the Fxperiosteum on the concave side of the Fx
• More stable & less Pain than complete FxMore stable & less Pain than complete Fx
• Need for reduction is determined by the Need for reduction is determined by the angulation of Fx, age of child, anatomic angulation of Fx, age of child, anatomic location of injurylocation of injury


Clavical Fx for 500Clavical Fx for 500
2 distinct times; newborn childbirth & 2 distinct times; newborn childbirth & childhoodchildhood
Fx newborn usually birth Injury, may have Fx newborn usually birth Injury, may have upper extemity bracheal plexus injury upper extemity bracheal plexus injury (palsy) or paralysis 2(palsy) or paralysis 2º painº pain
DO NOT need specific Tx, pain control and DO NOT need specific Tx, pain control and careful handling of infantcareful handling of infant


Clavical Fx for 1000Clavical Fx for 1000
• Childhood Fx possibly abuseChildhood Fx possibly abuse
• Middle 1/3 most commonMiddle 1/3 most common
• Tx Arm SlingTx Arm Sling
• Lateral or medial end may require ORIF b/c Lateral or medial end may require ORIF b/c ligamentous attachmentsligamentous attachments

Humoral Fx, ha ha ha NOTHumoral Fx, ha ha ha NOT• May occur at Proximal humorus, humoral dyaphsysis and May occur at Proximal humorus, humoral dyaphsysis and
supracondylar fxsupracondylar fx
• Fx Proximal Humorus good healing…May occur at physis or Fx Proximal Humorus good healing…May occur at physis or proximal humoral metaphysisproximal humoral metaphysis
• Physeal Fx; more common in adolescence; relatively weak Physeal Fx; more common in adolescence; relatively weak during growth spurtduring growth spurt
• Proximal Humoral Metaphyseal Fx are more common in Pre-Proximal Humoral Metaphyseal Fx are more common in Pre-adolesenceadolesence
• Tx depends on age of child & degree of displacementTx depends on age of child & degree of displacement• >30>30º displacement often need closed reduction & º displacement often need closed reduction &
immobilizationimmobilization
Fx Humoral Diaphysis Fx Humoral Diaphysis (Uncommon)(Uncommon)
• Suspect Abuse, strong Force Required!!!Suspect Abuse, strong Force Required!!!
• Closed reduction maybe requiredClosed reduction maybe required
• Radial Nerve Injury assoc Radial Nerve Injury assoc
• Document Radial Nerve Function!!!Document Radial Nerve Function!!!


Supracondylar FxSupracondylar Fx
• Most common Fx child < 8 peak 5-7y/o’sCause; fall on Most common Fx child < 8 peak 5-7y/o’sCause; fall on out stretched Handout stretched Hand
• Classification based on Fracture fragment Classification based on Fracture fragment displacementdisplacement
• Type I: minimal to no displacement stableType I: minimal to no displacement stable
• Type II: displaced w/ variable displacement but Type II: displaced w/ variable displacement but Posterior cortex intact Ortho consultPosterior cortex intact Ortho consult
• Type III: Need Ortho consultType III: Need Ortho consult• IIIa: Post med rotated; radial nerve risk damageIIIa: Post med rotated; radial nerve risk damage• IIIb: Post Lat rotated; bracheal art & med nerve riskIIIb: Post Lat rotated; bracheal art & med nerve risk

Lateral Condylar FxLateral Condylar Fx
• Usually Salter Harris IV; 10% of elbow Fx in Usually Salter Harris IV; 10% of elbow Fx in childrenchildren
• Varous stress with forearm in supination (arm up & Varous stress with forearm in supination (arm up & flat)flat)
• Complications; nonunion, malunion, osteonecrosis, Complications; nonunion, malunion, osteonecrosis, cubitus valgus, pardy ulnar nerve palsycubitus valgus, pardy ulnar nerve palsy
• STAT Ortho CONSULTSTAT Ortho CONSULT

Medial Epicondylar FxMedial Epicondylar Fx• 10-14y/o’s 10-14y/o’s
• Not TRUE SH fxNot TRUE SH fx
• Simple Fx of Medial Epicondyle are Simple Fx of Medial Epicondyle are Extra-articular limited soft Tissue Extra-articular limited soft Tissue involvementinvolvement
• ½ assoc w/ elbow dislocation½ assoc w/ elbow dislocation• Ortho ConsultOrtho Consult

Distal Humoral Physeal FxDistal Humoral Physeal Fx
• Twisting MOA, shears off distal Twisting MOA, shears off distal epiphysisepiphysis
• Often AbuseOften Abuse
• Often < 2yrs ageOften < 2yrs age

Olecranon FxOlecranon Fx
• Gen result from fall to elbowGen result from fall to elbow
• If displaced < 5 mm may be immobilizedIf displaced < 5 mm may be immobilized
• > 5 mm displacement Ortho Consult> 5 mm displacement Ortho Consult
• Maybe part of Monteggia lesion, careful Maybe part of Monteggia lesion, careful eval of Radial headeval of Radial head


Radial head FracturesRadial head Fractures
• Uncommon in childrenUncommon in children
• Radial neck > Radial HeadRadial neck > Radial Head
• Most common MOA; FallMost common MOA; Fall
• Ortho consult obtained to guide TxOrtho consult obtained to guide Tx


Elbow DislocationElbow Dislocation• Most freq males, fall outstretched HandMost freq males, fall outstretched Hand
• Most common POSTERIOR dislocationMost common POSTERIOR dislocation
• Neuro Injury ~10%; ulnar neuropathy Neuro Injury ~10%; ulnar neuropathy most common most common
• Assoc w/ Medial Epicondyle entrapmentAssoc w/ Medial Epicondyle entrapment
• Arterial Injury rareArterial Injury rare
• Obtain Post reduction filmObtain Post reduction film
• Good long term prognosisGood long term prognosis




Nurse Maid’s ElbowNurse Maid’s Elbow• Peak 2-3 yo Girls> boys L> RightPeak 2-3 yo Girls> boys L> Right
• MOA; sudden longitudinal traction on MOA; sudden longitudinal traction on outstreatched armoutstreatched arm
• Annular ligament of Radius displaces into Annular ligament of Radius displaces into Radio-capitellar articulation (baby will not Radio-capitellar articulation (baby will not move arm)move arm)
• Adducted semiflexed in Prone position Adducted semiflexed in Prone position (think Jerry’s kids)(think Jerry’s kids)
• No significant pt tenderness to palpationNo significant pt tenderness to palpation
• Attempts to pronation/supinationAttempts to pronation/supination PAIN PAIN

Reduction Nursemaid’s Reduction Nursemaid’s ElbowElbow• Supination technique: hold elbow 90Supination technique: hold elbow 90º firmly º firmly
supinate the wrist, then flex elbow (firmly)supinate the wrist, then flex elbow (firmly)
• Hyperpronation Technique: hold elbow 90º & Hyperpronation Technique: hold elbow 90º & firmly pronate wristfirmly pronate wrist
• Full arm function should return w/in 30 minutes…Full arm function should return w/in 30 minutes…if not consider Alternative to diagnosis (ie if not consider Alternative to diagnosis (ie fracture) fracture)


Forearm Injury’sForearm Injury’s• Isolated injury to ulna is extremely rare… Isolated injury to ulna is extremely rare…
typically same force causes fracture/dislocation to typically same force causes fracture/dislocation to RadiusRadius
• Combination of Ulnar Fx + Dislocation Radial Combination of Ulnar Fx + Dislocation Radial Head = Monteggia Fx; immediate eval by OrthoHead = Monteggia Fx; immediate eval by Ortho
• Galeazzi Fx; radial shaft fx, w/ assoc dislocation of Galeazzi Fx; radial shaft fx, w/ assoc dislocation of distal radioulnar joint; immediate ORTHO evaldistal radioulnar joint; immediate ORTHO eval

MonteggiaMonteggia

GaleazziGaleazzi

Wrist InjuriesWrist Injuries
• Fx of Carpal bones quite rare in childrenFx of Carpal bones quite rare in children
• Scaphoid fx in older kids MOA; Fall Scaphoid fx in older kids MOA; Fall outstretched Hand w/ snuffbox TTP, outstretched Hand w/ snuffbox TTP, suspected fx even w/o radiographic suspected fx even w/o radiographic finding; thumbspika splint and Ortho f/ufinding; thumbspika splint and Ortho f/u

Scaphoid fxScaphoid fx

Phalangeal FxPhalangeal Fx
• Most common injury to distal phalanx Most common injury to distal phalanx is child catches his or her hand in a is child catches his or her hand in a doordoor
• Any distal Tuft fx be immobilizedAny distal Tuft fx be immobilized
• If nail bed injuryIf nail bed injury “Open” “Open” Antibiotics indicatedAntibiotics indicated
• Significantly rotated or displaced fx Significantly rotated or displaced fx need reduced & Ortho Consultneed reduced & Ortho Consult

And No Hitting BELOW THE BELTAnd No Hitting BELOW THE BELT
• Pelvic Fx; Infrequent in Peds… due to Pelvic Fx; Infrequent in Peds… due to cartilagecartilage
Require tremendous Force, except Require tremendous Force, except Avulsion injury due to sudden muscle Avulsion injury due to sudden muscle contractions (ie kicking soccer ball), mngt contractions (ie kicking soccer ball), mngt conservatively… Ortho Referralconservatively… Ortho Referral
NON-avulsion; Most common MOA; MVCNON-avulsion; Most common MOA; MVC

Hip InjuryHip Injury
• Proximal Femur Fx; rare… Involving head Proximal Femur Fx; rare… Involving head or Neck of Femur or Neck of Femur risk of Avascular risk of Avascular Necrosis & Growth Arrest (unlike Necrosis & Growth Arrest (unlike Trochanteric & Subtrochanteric Fx) Trochanteric & Subtrochanteric Fx)
• Hip Dislocations; Most (in adolescence) Hip Dislocations; Most (in adolescence) POSTERIOR & Trama… < 10yrs can occur POSTERIOR & Trama… < 10yrs can occur w/ minimal trauma. IF Reduction in > 6 w/ minimal trauma. IF Reduction in > 6 hrs, 20X risk of Avascular Necrosis of hrs, 20X risk of Avascular Necrosis of Femoral HeadFemoral Head

Post Hip dislocationPost Hip dislocation

Lower ExtemityLower Extemity for 200 for 200• Femoral Shaft Fx; Significant Force Boys> GirlsFemoral Shaft Fx; Significant Force Boys> Girls
Falls, MVC, Ped vs Automobile, ABUSE if KID NOT Falls, MVC, Ped vs Automobile, ABUSE if KID NOT WALKING YET!!! Immediate ORTHO CONSULTWALKING YET!!! Immediate ORTHO CONSULT
Slipped Capital Femoral Epiphysis; most common Slipped Capital Femoral Epiphysis; most common cause hip disability in Adolesence… Obese, boys cause hip disability in Adolesence… Obese, boys 3x >girls. Sx Hip pain or reffered pain to thigh or 3x >girls. Sx Hip pain or reffered pain to thigh or knee. Adolescent c/o groin, hip, thigh or knee knee. Adolescent c/o groin, hip, thigh or knee painpain B/L hip radio graph. Ortho consult even if B/L hip radio graph. Ortho consult even if no XRAY evidence per Hxno XRAY evidence per Hx

Slipped Capital Femoral Slipped Capital Femoral EpiphysisEpiphysis

Knee InjuriesKnee Injuries• Ligamentous Injury < common than FxLigamentous Injury < common than Fx
• OTTAWA Knee rules validated for ≥ 2y/oOTTAWA Knee rules validated for ≥ 2y/o need xray; > 55y/o, TTP Fibular Head, Isolated need xray; > 55y/o, TTP Fibular Head, Isolated
TTP Patella, Inability flex knee to 90º, inability TTP Patella, Inability flex knee to 90º, inability to take 4 steps immediately after injury & in to take 4 steps immediately after injury & in EDED
Fx thru Distal Femoral Physis; uncommon, signif Fx thru Distal Femoral Physis; uncommon, signif complications… popliteal artery lies close to complications… popliteal artery lies close to Dist Metaphysis, peroneal Nerve may be Dist Metaphysis, peroneal Nerve may be injured… risk Growth Arrest 2º physeal injured… risk Growth Arrest 2º physeal damagedamage

Knee Injury for 500Knee Injury for 500• Patellar dislocation; most common cause of Patellar dislocation; most common cause of
traumatic Hemarthrosis in children… MOA pivot traumatic Hemarthrosis in children… MOA pivot knee of fixed LEknee of fixed LE
May reduce w/o waiting for XRAY. XRAY post May reduce w/o waiting for XRAY. XRAY post REDUCTIONREDUCTION
Proximal Tibial Injury; ACL inserts on tibial Proximal Tibial Injury; ACL inserts on tibial emminance… ligament & insertion much stronger emminance… ligament & insertion much stronger than epiphyseal bone in kids… than epiphyseal bone in kids…

Patellar dislocationPatellar dislocation

Patellar dislocationPatellar dislocation

Tibial Tuberosity Fx; 3 types;Tibial Tuberosity Fx; 3 types;
Tpye I; Fx thru small distal portion tibial tuberosity; Tpye I; Fx thru small distal portion tibial tuberosity; Tx; immobilizationTx; immobilization
Type II Fx; Fx splits the growth plate of the Type II Fx; Fx splits the growth plate of the tuberosity of the proximal tibiatuberosity of the proximal tibia
Type III; Involve joint; risk compartment syndromeType III; Involve joint; risk compartment syndrome
Displaced Type II & III need reduction & immediate Displaced Type II & III need reduction & immediate Ortho ConsultOrtho Consult

Tibial Tuberosity FXTibial Tuberosity FX

Knee Injury for 1000Knee Injury for 1000
• Proximal tibial Physis Fx; uncommon, most Proximal tibial Physis Fx; uncommon, most SH Type I. Vascular injury to Popliteal SH Type I. Vascular injury to Popliteal Artery riskArtery risk
DOCUMENT INTACT PULSES!!!DOCUMENT INTACT PULSES!!!

Tib Fib FxTib Fib Fx
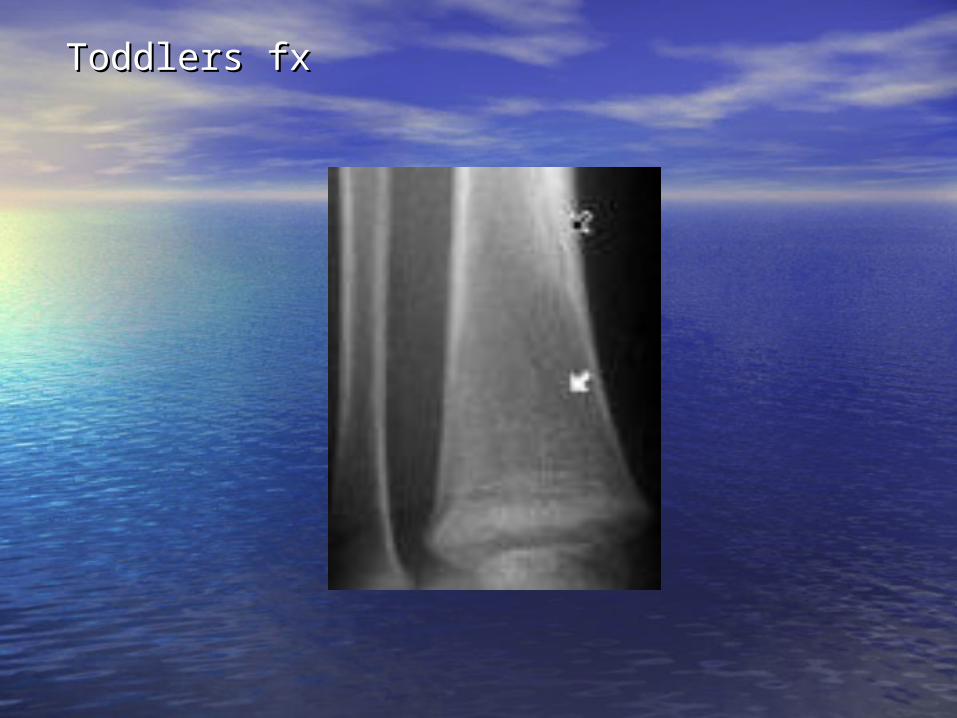
• Toddler’s Fx; spiral Fx Distal 1/3 of tibia…Toddler’s Fx; spiral Fx Distal 1/3 of tibia…
child limping, unable to bear wtchild limping, unable to bear wt
pain w/ palpation & rotation distal tibia… pain w/ palpation & rotation distal tibia… Xray maybe normal, F/U Bonescan or xray Xray maybe normal, F/U Bonescan or xray 1 week Immobilize long leg splint w/ Ortho 1 week Immobilize long leg splint w/ Ortho F/UF/U
Toddlers fxToddlers fx

Ankle InjuriesAnkle Injuries• May involve distal tibula, fibula or both. May involve distal tibula, fibula or both.
Most SH type I, SH type III 25% of distal Most SH type I, SH type III 25% of distal tibial fx & require ORIFtibial fx & require ORIF
• Tillaux Fx; SH III of Anterior LAT portion of Tillaux Fx; SH III of Anterior LAT portion of Distal tibia surgical reductionDistal tibia surgical reduction
• Triplane fx; Sagittal, Coronal & Transverse Triplane fx; Sagittal, Coronal & Transverse planes… SH IV Multiple Fx Fragments… planes… SH IV Multiple Fx Fragments… ORTHOORTHO

Foot & Phalanx FxFoot & Phalanx Fx• Hind foot = calcaneous & talusHind foot = calcaneous & talus• Mid foot = navicular, cuboid, 2Mid foot = navicular, cuboid, 2ndnd 3 3rdrd
cuneiformscuneiforms• MetatarsalsMetatarsals• PhalangesPhalanges
Fx to forefoot common… hind & mid foot Fx to forefoot common… hind & mid foot uncommonuncommon
Non-displaced fx metatarsals & phalanges Non-displaced fx metatarsals & phalanges splint & Ortho referralsplint & Ortho referral
Displaced Fx & intra-articular involvement Displaced Fx & intra-articular involvement may require ORIFmay require ORIF
Septic Arthritis (Acute)Septic Arthritis (Acute)
• < 3y/o’s most common; knee>hip>elbow< 3y/o’s most common; knee>hip>elbow
• Hematogenous routeHematogenous route
• Early; Early; synovial fluid & protein, PMN > 50K, synovial fluid & protein, PMN > 50K, gluglu
• Neonates do NOT appear ill, ½ of time NO FeverNeonates do NOT appear ill, ½ of time NO Fever
• Older child; Fever, localizing signsOlder child; Fever, localizing signs
• Plain films No Dx early on… widening joint space Plain films No Dx early on… widening joint space Joint effusion late findings on XRAYJoint effusion late findings on XRAY
• D/dx; trauma, sickle cell, JRA, Osgood Slaughter, etcD/dx; trauma, sickle cell, JRA, Osgood Slaughter, etc

Septic ArthritisSeptic Arthritis

Septic Arthritis for 200Septic Arthritis for 200
• Labs; CBC, Blood Cx, ESR, CRP, Throat CxLabs; CBC, Blood Cx, ESR, CRP, Throat Cx
• ½ WBC < 15K½ WBC < 15K
• 90% ESR> 70 90% ESR> 70
• New borns; New borns; Group B-strepGroup B-strep, GNR, Neisseria, , GNR, Neisseria, StaphStaph
• Infant; staph, strep, H Flu, GNRInfant; staph, strep, H Flu, GNR
• Child, Staph, Strep, GNR, Neisseria,Child, Staph, Strep, GNR, Neisseria,

Henoch-Schonlein-PurpraHenoch-Schonlein-Purpra
• Purpura, arthritis, abdm pain & HematuriaPurpura, arthritis, abdm pain & Hematuria
• Small vessel vasculitis mediated by immune Small vessel vasculitis mediated by immune complexescomplexes
• Purple palpable Rash; initially blanches, trunk, Purple palpable Rash; initially blanches, trunk, buttocks, pereum, lower extremitiesbuttocks, pereum, lower extremities
• GI tract involvedGI tract involved risk Hemmorrahge risk Hemmorrahge
• Arthritis; knees & AnklesArthritis; knees & Ankles
• Supportive care, Admit, IFV, Tylenol prnSupportive care, Admit, IFV, Tylenol prn
• Complications; bowel perf, ARF, Nephrotic SyndromeComplications; bowel perf, ARF, Nephrotic Syndrome

Henoch-Schonlein-PurpraHenoch-Schonlein-Purpra

Juvenile Rheumatoid ArthritisJuvenile Rheumatoid Arthritis
• 3 types; Oligo Arthritis, polyarticular, systemic3 types; Oligo Arthritis, polyarticular, systemic
• Oligo; 1+ joints of LE; permanent joint damage uncommonOligo; 1+ joints of LE; permanent joint damage uncommon
• Polyarticular; sim to Adult presentation, C-spine common Polyarticular; sim to Adult presentation, C-spine common w/ w/ risk of AtlantoAxial subluxation, 20 to 40 separate risk of AtlantoAxial subluxation, 20 to 40 separate joints affectedjoints affected
• Systemic; Fever >39 min 2weeks, chills, rash on trunk Systemic; Fever >39 min 2weeks, chills, rash on trunk palms & soles (also RMSF, Syphylis, Hand-foot mouth Dz)palms & soles (also RMSF, Syphylis, Hand-foot mouth Dz)
Often Hepatosplenomegally, pleuritis, pericardial effusionOften Hepatosplenomegally, pleuritis, pericardial effusion
Require Arthrocentesis to R/O suppurative arthritis… admit if Require Arthrocentesis to R/O suppurative arthritis… admit if in Doubtin Doubt

Kawasaki DzKawasaki Dz• 80% present < 4yrs… 95% present < 10y/o80% present < 4yrs… 95% present < 10y/o
• Acute febrile vasculitis of childhood… involves coronary Acute febrile vasculitis of childhood… involves coronary arteriesarteries
• Diagnostic Criteria; Fever 5 days duration (100%), B/L Diagnostic Criteria; Fever 5 days duration (100%), B/L conjunctivitis (85%), conjunctivitis (85%), ’s oral mucosa (90%), Erythema ’s oral mucosa (90%), Erythema extemities (plams & soles) 75%, Polymorphish rash extemities (plams & soles) 75%, Polymorphish rash (80%), Cervical Lyphadenoplathy 70%(80%), Cervical Lyphadenoplathy 70%
• Assoc Features; arthralgia, arthritis, thrombocytosis, Assoc Features; arthralgia, arthritis, thrombocytosis, aseptic meningitis, hepatitis, cardiac (Coronary A aseptic meningitis, hepatitis, cardiac (Coronary A aneurysms, myocarditis, percarditis, dysrrhythmias), aneurysms, myocarditis, percarditis, dysrrhythmias), Mitral or Aortic insufficencyMitral or Aortic insufficency
Tx; IV IG, ASA (100mg/kg/day)Tx; IV IG, ASA (100mg/kg/day)

Kawasaki DzKawasaki Dz

Kawasaki DZKawasaki DZ

Legg-Calve-Perthes DzLegg-Calve-Perthes Dz
• 80% b/t 4-9y/o range is 2-13y/o’s80% b/t 4-9y/o range is 2-13y/o’s• Avascular necrosis of the femoral HeadAvascular necrosis of the femoral Head
• Male: Female 4:1Male: Female 4:1• Mild Hip pain,limp progressive over weeks to monthsMild Hip pain,limp progressive over weeks to months• 4 stages; initial, fragmentation, reossification, healed4 stages; initial, fragmentation, reossification, healed
• Initial Xray; widening of cartilage spaceInitial Xray; widening of cartilage space• 22ndnd Xray sign; subcondral stress Fx line Femoral Head Xray sign; subcondral stress Fx line Femoral Head• 33rdrd; ; radio opacity of Femoral Head (new bone radio opacity of Femoral Head (new bone
deposited on avascular trabeculae) deposited on avascular trabeculae)
• Further distortion of femoral head & subluxationFurther distortion of femoral head & subluxation

Legg-Calve-Perthes DzLegg-Calve-Perthes Dz

Osgood-Schlatter DzOsgood-Schlatter Dz
• Apophysitis of Tibial tubercal; over use or Apophysitis of Tibial tubercal; over use or normal use… insertion of petallar tendonnormal use… insertion of petallar tendon
• Series of micro avulsionsSeries of micro avulsions
• 10-15 y/o’s Boys > Girls10-15 y/o’s Boys > Girls
• More common in running or jumping athletes More common in running or jumping athletes
• Self limited Dz improves w/ conservative Self limited Dz improves w/ conservative TherapyTherapy

Osgood-Schlatter DzOsgood-Schlatter Dz

Post Streptococcal Reactive ArthritisPost Streptococcal Reactive Arthritis
• Group A Strep Infxn w/ symptom free interval followed Group A Strep Infxn w/ symptom free interval followed by Aspetic inflammation of 1+ jointsby Aspetic inflammation of 1+ joints
• 10 days after strep Infxn; acute rheumatic F 21 days 10 days after strep Infxn; acute rheumatic F 21 days post Infxnpost Infxn
• PSRA = Non-migratory mono or oligo arthritis, freq PSRA = Non-migratory mono or oligo arthritis, freq assoc Erythea Nodosum, or Erythema Multiformaassoc Erythea Nodosum, or Erythema Multiforma
TX: NSAIDS, antibiotic prophylaxis contraversialTX: NSAIDS, antibiotic prophylaxis contraversial
• ARF= polymigratory ArthritisARF= polymigratory Arthritis

Acute Rheumatic FeverAcute Rheumatic Fever
• GABHS infection; mucoid types 3, 5, 18GABHS infection; mucoid types 3, 5, 18• Connective tissue of Heart, Joints, CNS, Sub Q tissues of Connective tissue of Heart, Joints, CNS, Sub Q tissues of
skin targeted by immune RXNskin targeted by immune RXN• Carditis, valvulitis; mitral & aortic valvesCarditis, valvulitis; mitral & aortic valves• Arthritis is periarticularArthritis is periarticular
• Jones Criteria; Major; carditis, migartory arthritis, Jones Criteria; Major; carditis, migartory arthritis, chorea, erythema marginatum (serpintine rash), Sub Q chorea, erythema marginatum (serpintine rash), Sub Q nodulesnodules
• Minor Criteria; fever, arthralgia, Minor Criteria; fever, arthralgia, ESR/CRP, prolonged PR ESR/CRP, prolonged PR interval, interval, ASO titer ASO titer
• Tx: Admit, consult Pediatric Cardiologist, High dose ASA Tx: Admit, consult Pediatric Cardiologist, High dose ASA (75 to 100mg/kg/day), PCN, ? Steroids if CHF(75 to 100mg/kg/day), PCN, ? Steroids if CHF
Transient Synovitis of the HipTransient Synovitis of the Hip
• Benign self-limited process of the Hip…Benign self-limited process of the Hip…• 8x > freq than septic arthritis Children b/t 3 to 6 yrs 8x > freq than septic arthritis Children b/t 3 to 6 yrs • Most Post Viral, ? trauma, bacterial, or Post VaccineMost Post Viral, ? trauma, bacterial, or Post Vaccine
• Pts at risk for Septic Arthritis w/ temp > 38.5 ESR>20Pts at risk for Septic Arthritis w/ temp > 38.5 ESR>20 Leukocytosis, severe Pain, TTP of joint, spasm, refusal Leukocytosis, severe Pain, TTP of joint, spasm, refusal
to walkto walk
Joint Aspirate if suspect septic arthritis, if periphrial Joint Aspirate if suspect septic arthritis, if periphrial WBC, ESR WBC, ESR and hip effusion… and hip effusion…
Synovial fluid; Gram Stain, Aero/anaerobic cx, AFBSynovial fluid; Gram Stain, Aero/anaerobic cx, AFBTx NSAIDS, limit activiy 1 to 2 weeksTx NSAIDS, limit activiy 1 to 2 weeks
QuizQuiz1)1) A type II SH Fracture is a fracture thruA type II SH Fracture is a fracture thru
A) PhysisA) Physis
B) Physis & MetaphysisB) Physis & Metaphysis
C) Physis & EpiphysisC) Physis & Epiphysis
D) Physis, Epiphysis, metaphysisD) Physis, Epiphysis, metaphysis
2) A Monteggia Fracture is2) A Monteggia Fracture is
A) A radial head fracture w/ Posterior radial dislocationA) A radial head fracture w/ Posterior radial dislocation
B) Ulnar Fracture w/ Anterior dislocation of Proximal UlnaB) Ulnar Fracture w/ Anterior dislocation of Proximal Ulna
C) Ulnar Fracture + Dislocation Radial Head C) Ulnar Fracture + Dislocation Radial Head
D) Radial shaft Fracture + Dislocation of UlnaD) Radial shaft Fracture + Dislocation of Ulna

QuizQuiz3) A Galeazzi fracture is:3) A Galeazzi fracture is: A) A radial head fracture w/ Posterior radial dislocationA) A radial head fracture w/ Posterior radial dislocation B) Ulnar Fracture w/ Anterior dislocation of Poximal UlnaB) Ulnar Fracture w/ Anterior dislocation of Poximal Ulna C) Ulnar Fracture + Dislocation Radial Head C) Ulnar Fracture + Dislocation Radial Head D) Radial shaft Fracture w/ assoc dislocation of distal radioulnar D) Radial shaft Fracture w/ assoc dislocation of distal radioulnar
jointjoint
4) Jones Criteria for Acute Rheumatic fever4) Jones Criteria for Acute Rheumatic fever A) carditisA) carditis B) Migartory arthritisB) Migartory arthritis C) choreaC) chorea D) erythema marginatum (serpintine rash)D) erythema marginatum (serpintine rash) E) Sub Q nodulesE) Sub Q nodules F) All of the aboveF) All of the above G) A, B, and CG) A, B, and C

QuizQuiz
5) Regarding Nurse Maids Elbow; 5) Regarding Nurse Maids Elbow;
A) The Radial Annular ligament displaces into Radio-A) The Radial Annular ligament displaces into Radio-capitellar articulationcapitellar articulation
B) A horizontal torsional force causes a perpendicular B) A horizontal torsional force causes a perpendicular translational force on the radius thus dislocationtranslational force on the radius thus dislocation
C) The elbow must have rapid extension for cureC) The elbow must have rapid extension for cure
Answers: Answers:
1) C 2) C 3) D 4) F 5) A1) C 2) C 3) D 4) F 5) A