music in the treatment of neurological language and … 2012, 26 (1), 1–19 music in the treatment...
TRANSCRIPT

This article was downloaded by: [University of Groningen]On: 14 February 2012, At: 07:32Publisher: Psychology PressInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
AphasiologyPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/paph20
Music in the treatment ofneurological language and speechdisorders: A systematic reviewJoost Hurkmans a , Madeleen de Bruijn a , Anne M. Boonstraa , Roel Jonkers b , Roelien Bastiaanse b , Hans Arendzen c &Heleen A. Reinders-Messelink aa Rehabilitation Center “Revalidatie Friesland”,Beetsterzwaag, The Netherlandsb School for Behavioural and Cognitive Neuroscience (BCN),University of Groningen, Groningen, The Netherlandsc Leiden University Medical Center, Department ofRehabilitation Medicine, Leiden, The Netherlands
Available online: 06 Oct 2011
To cite this article: Joost Hurkmans, Madeleen de Bruijn, Anne M. Boonstra, Roel Jonkers,Roelien Bastiaanse, Hans Arendzen & Heleen A. Reinders-Messelink (2012): Music in thetreatment of neurological language and speech disorders: A systematic review, Aphasiology,26:1, 1-19
To link to this article: http://dx.doi.org/10.1080/02687038.2011.602514
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make anyrepresentation that the contents will be complete or accurate or up to date. Theaccuracy of any instructions, formulae, and drug doses should be independentlyverified with primary sources. The publisher shall not be liable for any loss, actions,claims, proceedings, demand, or costs or damages whatsoever or howsoever caused

arising directly or indirectly in connection with or arising out of the use of thismaterial.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

APHASIOLOGY, 2012, 26 (1), 1–19
Music in the treatment of neurological language and speechdisorders: A systematic review
Joost Hurkmans1, Madeleen de Bruijn1, Anne M. Boonstra1,Roel Jonkers2, Roelien Bastiaanse2, Hans Arendzen3,and Heleen A. Reinders-Messelink1
1Rehabilitation Center “Revalidatie Friesland”, Beetsterzwaag, The Netherlands2School for Behavioural and Cognitive Neuroscience (BCN), University ofGroningen, Groningen, The Netherlands3Leiden University Medical Center, Department of Rehabilitation Medicine,Leiden, The Netherlands
Background: Acquired brain injury resulting from a stroke can result in impairments in,among other things, communication. Music therapy has been used in rehabilitation tostimulate brain functions involved in speech. The use of elements of music is well knownand more often used in the treatment of aphasia and apraxia of speech.Aims: The aim of the study is to synthesise studies on the effect of music parameters inthe treatment of neurological language and speech disorders. In addition, possible mech-anisms that explain recovery are investigated.Methods & Procedures: Search terms were formulated based on the research question.A systematic search in databases was performed using these search terms. Then inclusioncriteria were formulated and articles meeting the criteria were reviewed on patient char-acteristics, interventions, and methodological quality.Outcomes & Results: A total of 1250 articles have been selected from the databases, ofwhich 15 were included in this study. The Melodic Intonation Therapy was the moststudied programme. Melody and rhythm were the music interventions that have beenapplied the most. Measurable recovery has been reported in all those reviewed studiesusing music in the treatment of neurological language and speech disorders. In threestudies research was also conducted into the mechanisms of explanation of the measuredrecovery. However, the methodological quality of the investigated studies was rated as“low”, using the ASHA level of evidence indicators for judging research.Conclusions: Although treatment outcomes were reported as positive in all of the15 reviewed studies, caution should be used relative to conclusions about the effective-ness of treatments that incorporate components of music with neurologically impairedindividuals. Methodological quality was rated as low and interpretations of mecha-nisms of recovery were contradictory. Suggestions for standardising and improvingmethodological quality drawn from the analysis are presented.
Keywords: Music; Speech disorders; Treatment.
Address correspondence to: Joost Hurkmans, MA, Rehabilitation Center “Revalidatie Friesland”,P.O. Box 1, 9244 CL Beetsterzwaag, the Netherlands. E-mail: [email protected]
A revised version of this article has been published in a Dutch journal (Stem Spraak- en Taalpathologie).
© 2012 Psychology Press, an imprint of the Taylor & Francis Group, an Informa businesshttp://www.psypress.com/aphasiology http://dx.doi.org/10.1080/02687038.2011.602514
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

2 HURKMANS ET AL.
Musical structures and language structures have many similar features, which gen-erates continuous research interest. Studying the relation between these two entitiesdates back to the nineteenth century. Gamer (1892) studied animal noise and thehuman voice and transformed these sounds to musical instruments like piccoloand other flutes. More recently, sophisticated techniques like event-related poten-tial (ERP), positron emission tomography (PET), and functional magnetic resonanceimaging (fMRI) have been used to study perceptual elements of music and language inorder to gather information on the functional and neural architecture of both domains(Brown, Martinez, & Parsons, 2006; Jeffries, Fritz, & Braun, 2003; Patel, 2003).
Communication impairments resulting from neurological damage were alreadybeing studied in the nineteenth century. Broca (1861) reported language disorders inpatients who suffered from a stroke. In 1914 Déjérine, as one of the first researchers,observed a superior singing ability in aphasia. Subsequently, more researchersreported data relative to severely impaired patients who barely had the ability to speakin spontaneous speech, but were able to produce well-articulated, linguistically accu-rate words while singing familiar songs that had been learned prior to their stroke(e.g., Cohen & Ford, 1995; Gerstman, 1964; Hébert, Racette, Gagnon, & Peretz,2003; Racette, Bard, & Peretz, 2006; Straube, Schultz, Geipel, Mentzel, & Miltner,2008). Clinical applications using musical elements were then a natural consequencein aphasia intervention. Melody and rhythm have been used by non-fluent speak-ers to enhance speech production or to improve speech fluency. The most commontherapy intervention using melody and rhythm is the Melodic Intonation Therapy(MIT; Albert, Sparks, & Helm, 1973). MIT consists of speaking with a simplifiedand exaggerated prosody, characterised by a melodic component (two notes, high andlow) and a rhythmic component (two durations, long and short). Various music ther-apy approaches are aimed at verbal expression and communication as well. Therapymethods using different musical elements, like melody, rhythm, dynamics, tempo, andmetre, to regain speech production need not automatically contain music therapy. Forexample, the MIT is not a therapy of music as indicated by the original developers ofthe treatment approach.1 However, several music therapy variations have been devel-oped mostly based on MIT principles (e.g., Modified Melodic Intonation Therapy,MMIT, Baker, 2000; and Singen Intonation Prosodie Atmung RhytmusübungenImprovationen, SIPARI, Jungblut & Aldridge, 2004). Similar to MIT, the MMIT pro-gramme is also based on repetition of phrases set to musical structures. However, thephrases in MMIT are more melodic in structure and less like the “sprechgesang” styleof intonation adopted in MIT (Baker, 2000). A rather new therapy programme inwhich music performs a major role is Speech-Music Therapy for Aphasia (SMTA; deBruijn, Zielman, & Hurkmans, 2005). SMTA is a treatment programme with a com-bination of speech language pathology and music therapy. SMTA has componentssimilar to MIT; however, the most important difference is the expanding of musicalelements like dynamics, tempo, and metre.
Therapy interventions using musical elements to remediate language and speechabilities have been developed from clinical practice, including SMTA. During the past10 years positive outcomes have been experienced by patients with neurological com-munication deficits; however, evidence of the effectiveness of treatment based on thecomponents of music remains unknown. Therefore a systematic review of literature
1We refer to the appendix for a definition of music therapy and a more concrete discussion of the variousparameters.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 3
was needed. The purpose of the study in question is a general review and meaningfulbefore studying the effect of SMTA in future research.
This article reviews the existing literature on the effect of music in the treatment ofpatients with neurological language and speech disorders. Studies were considered forthis review if published in a peer-reviewed journal prior to 2009. In addition, mech-anisms of recovery explaining positive effects of the use of music in the treatment ofpatients with neurological language and speech disorders were evaluated.
METHOD
A list of search terms was set-up in order to systematically search in the litera-ture: <language disorders>, <speech disorders>, <communication disorders>,<aphasia>, <articulation disorders>, <apraxia>, <speech>, <language>,<verbal>, <oral>, <communication>, <motor speech disorder> and <music>.These terms were linked using the combinations of: (1) <language disorders> or<speech disorders> or <communication disorders> or <aphasia> or <articulationdisorders>, (2) <apraxia> and (<speech> or <language> or <verbal> or <oral>or <communication> or <motor speech disorder>), (3) <music> and (#1 or #2).We searched in the following databases: PubMed, CINAHL, PsycINFO, andEMBASE. Reference manager was used to remove duplicates. Subsequently, inclu-sion criteria were formulated to judge whether an article contributes to the researchquestions: (1) effect controlled by measurements before and after intervention,(2) musical elements as a form of therapy of language and speech disorders causedby non-congenital neurological disorders (e.g., CVA and TBI), (3) adults, (4) any ofthe linguistic modalities, (5) language restrictions: only English, French, German,and Dutch articles were reviewed. Music was defined as follows: one or moreof the following musical elements: rhythm, melody, accent, practised in vocal orinstrumental form. Language and speech disorders were defined as follows: disordersof production as well as disorders in reception in all linguistic modalities (speech,reading, writing, and auditory language comprehension). Particular exclusion criteriawere also delineated: amusia, language acquisition disorders, stuttering, psychiatricdiseases, dementia, hearing disorders (including word deafness), voice disorders,healthy participants (including professional musicians), epilepsy, and autism.
Two authors (JH and MB) reviewed the abstracts of the selected articles indepen-dently of each other. Various articles needed to be read more extensively because it wasunclear from the abstract if they met the inclusion criteria. Both selections were thencompared. When in doubt, the two reviewers consulted with a third reviewer (HR).
A list of variables was compiled in order to describe the articles. A short pilot studywas needed to help determine this list. JH and MB independently assigned the vari-able values by reading two selected articles. Upon completion of this pilot by groupdiscussion, the list of variables was established. As a result of the completed list, thedescription of articles contains the following three variables: (1) patient characteris-tics: age, gender, education, dominance, aetiology, speech-language diagnosis, timepost onset, severity of the speech- language impairment, and musical background,(2) intervention and outcome variables: objective of the treatment, level of outcomemeasurements in terms of international classification of functioning (ICF), treatmentprogramme/method (including condition, schedule, linguistic level, musical parame-ters) and other language, speech and music therapy interventions, (3) methodologicalquality: study design, blinding, sampling, group/participant comparability, treatment
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

4 HURKMANS ET AL.
fidelity, outcomes, significance, precision, and intent-to-treat. These quality indicatorsoriginate from the guidelines of the ASHA levels-of-evidence scheme. A study received1 point for each quality indicator if the highest level of quality was incorporated. In thecases of indicators with multiple possible levels, only the highest level of quality gotcredit. Table 1 outlines the indicators with a description and quality marker.
Variables had to be reported in more than 50% of the articles in order to be includedin the results of this review. When information on a variable was missing in > 50% ofthe articles, the variable was excluded from the analyses because the lack of infor-mation would be too large to make firm conclusions. All the information of patientcharacteristics, intervention and outcome variables, and methodological quality isbased on information provided by the authors of the articles. Any lack of informationis also indicated as not reported.
RESULTS
The combination of search terms yielded 1250 articles. However, 94% of the articleswere excluded since they concerned no therapy study and/or other participant groupthan patients with language and speech disorders caused by neurological disorders.A total of 50 articles were close to being included but were dropped because no effectcontrolled by measurements before and after intervention was included in the study.Two authors (JH and MB) identified a total of 18 articles that met initial inclusioncriteria, with agreement in most of the cases. During the selection of the articles threewere rejected upon review of the full text and after consultation with a third reviewer(HR). Thus 15 studies were used in the review. The results of 583 patients are describedbelow of which 82% were depicted in the study of Popovici (1995).
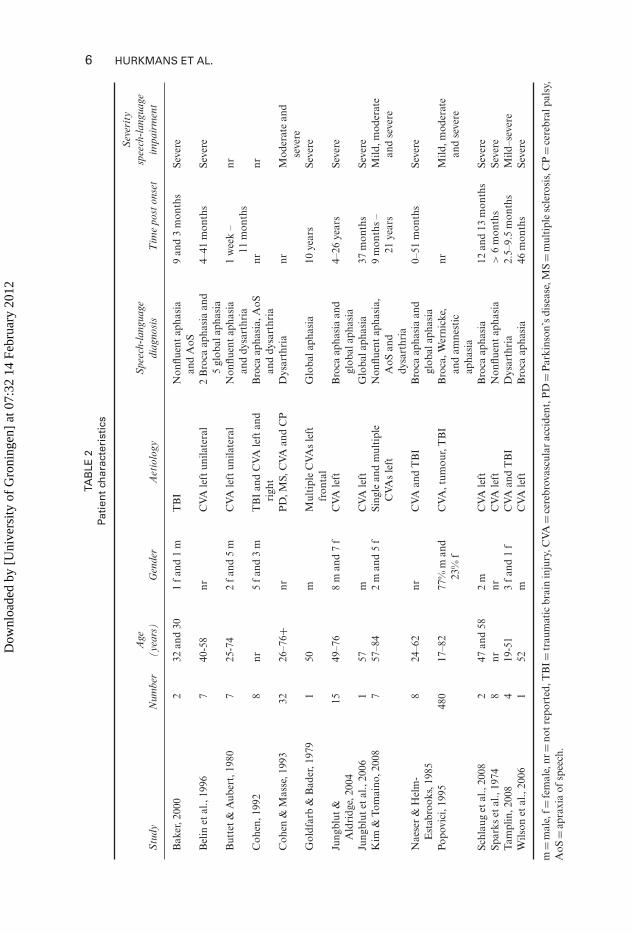
Patient characteristics
Table 2 provides an overview of the 15 studies and corresponding patient characteris-tics. Three variables were not reported 50% of the time, not meeting the 50% criteria.These included education, dominance, and musical background. Thus these variableswere excluded from this review. Various ages, from 18 years onwards, were representedin the studies through an adequate spreading, meaning that all age groups were equallydivided. Four articles did not report any gender information. In the other studies bothsexes were represented in group studies and case series. Notable from Popovici’s study(1995) is the high percentage of males: 77%. It has not been reported whether thishad any influence on the result of the study. In all (but one) studies, stroke was thecause of speech disorder of the treated patients (in five studies in combination withother medical diagnoses). The exception was the study of Baker (2000) who describedtwo patients with traumatic brain injury (TBI). In nine studies the location of thelesion was reported; these patients suffered from a left hemisphere stroke. The speech-language diagnosis was non-fluent aphasia (Broca’s aphasia or global aphasia) in13 studies, with an accompanying apraxia of speech in 2 studies. In two articles (Cohen& Masse, 1993; Tamplin, 2008) patients with dysarthria were also investigated. Mostpatients were treated in the chronic phase of recovery, more than 1 year post onset, forsevere language and speech disorders (not explicitly defined).
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 5
TAB
LE1
Qu
alit
yin
dic
ato
rsin
the
AS
HA
leve
ls-o
f-ev
iden
cesc
hem
e(2
001)
Indi
cato
rD
escr
ipti
onQ
ualit
ym
arke
r
Stud
yde
sign
The
type
ofde
sign
used
inth
est
udy
Con
trol
led
tria
l=1
Ret
rosp
ecti
veca
seco
ntro
l=1
Sing
lepa
rtic
ipan
tst
udy
=1
Cas
ese
ries
=0
Cas
est
udy
=0
Blin
ding
The
prac
tice
ofke
epin
gin
vest
igat
ors
orpa
rtic
ipan
tsig
nora
ntof
the
grou
pto
whi
chpa
rtic
ipan
tsar
eas
sign
ed.F
orth
epu
rpos
esof
the
crit
ical
appr
aisa
l,bl
indi
ngre
fers
toas
sess
ors
only
Ass
esso
rsbl
inde
d=
1A
sses
sors
not
blin
ded
orno
tst
ated
=0
Sam
plin
gT
hem
etho
d(s)
used
toch
oose
and
assi
gnpa
rtic
ipan
tsto
the
expe
rim
enta
lcon
diti
ons
inth
est
udy
Ran
dom
sam
ple
adeq
uate
lyde
scri
bed
=1
Ran
dom
sam
ple
inad
equa
tely
desc
ribe
d=
0C
onve
nien
cesa
mpl
ead
equa
tely
desc
ribe
d=
0C
onve
nien
cesa
mpl
ein
adeq
uate
lyde
scri
bed
orha
nd-p
icke
dsa
mpl
eor
not
stat
ed=
0G
roup
/pa
rtic
ipan
tco
mpa
rabi
lity
How
sim
ilar
the
part
icip
ants
/gr
oups
wer
eat
the
star
tof
the
stud
yor
how
adeq
uate
lyth
eyw
ere
desc
ribe
dG
roup
s/pa
rtic
ipan
tsco
mpa
rabl
eat
base
line
onim
port
ant
fact
ors
(bet
wee
n-pa
rtic
ipan
tde
sign
)or
part
icip
ant(
s)ad
equa
tely
desc
ribe
d=
1G
roup
s/pa
rtic
ipan
tsno
tco
mpa
rabl
eat
base
line
orco
mpa
rabi
lity
not
repo
rted
orpa
rtic
ipan
t(s)
not
adeq
uate
lyde
scri
bed
=0
Tre
atm
ent
fidel
ity
The
proc
edur
eus
edto
ensu
reth
atth
etr
eatm
ent
was
deliv
ered
asin
tend
edE
vide
nce
oftr
eatm
ent
fidel
ity
=1
No
evid
ence
oftr
eatm
ent
fidel
ity
=0
Out
com
esT
hem
easu
re(s
)us
edin
the
stud
yto
quan
tify
impr
ovem
ent
At
leas
ton
epr
imar
you
tcom
em
easu
reis
valid
and
relia
ble=
1V
alid
ity
unkn
own
but
appe
ars
reas
onab
le;m
easu
reis
relia
ble=
0In
valid
and/
orun
relia
ble=
0Si
gnifi
canc
eT
helik
elih
ood
that
the
stud
yfin
ding
soc
curr
edby
chan
ceP
valu
ere
port
edor
calc
ulab
le=
1P
valu
ene
ithe
rre
port
edno
rca
lcul
able
=0
Pre
cisi
onT
hesi
zeor
mag
nitu
deof
any
diff
eren
cefo
und
betw
een
the
trea
tmen
tun
der
inve
stig
atio
nan
dth
eco
ntro
lco
ndit
ion
Eff
ect
size
and
confi
denc
ein
terv
alre
port
edor
calc
ulab
le=
1E
ffec
tsi
zeor
confi
denc
ein
terv
al,b
utno
tbo
th,r
epor
ted
orca
lcul
able
=0
Nei
ther
effe
ctsi
zeno
rco
nfide
nce
inte
rval
repo
rted
orca
lcul
able
=0
Inte
ntio
n-to
-tre
at(c
ontr
olle
dtr
ials
only
)P
arti
cipa
nts
are
anal
ysed
acco
rdin
gto
the
grou
pto
whi
chth
eyar
ein
itia
llyas
sign
ed,r
egar
dles
sof
whe
ther
orno
tth
eydr
oppe
dou
t,fu
llyco
mpl
ied
wit
hth
etr
eatm
ent,
orcr
osse
dov
eran
dre
ceiv
edth
eot
her
trea
tmen
t
Ana
lyse
dby
inte
ntio
n-to
-tre
at=
1N
otan
alys
edby
inte
ntio
n-to
-tre
at=
0
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012
6 HURKMANS ET AL.
TAB
LE2
Pati
ent
char
acte
rist
ics
Stu
dyN
umbe
rA
ge(y
ears
)G
ende
rA
etio
logy
Spe
ech-
lang
uage
diag
nosi
sT
ime
post
onse
t
Sev
erit
ysp
eech
-lan
guag
eim
pair
men
t
Bak
er,2
000
232
and
301
fan
d1
mT
BI
Non
fluen
tap
hasi
aan
dA
oS9
and
3m
onth
sSe
vere
Bel
inet
al.,
1996
740
-58
nrC
VAle
ftun
ilate
ral
2B
roca
apha
sia
and
5gl
obal
apha
sia
4–41
mon
ths
Seve
re
But
tet
&A
uber
t,19
807
25-7
42
fan
d5
mC
VAle
ftun
ilate
ral
Non
fluen
tap
hasi
aan
ddy
sart
hria
1w
eek
–11
mon
ths
nr
Coh
en,1
992
8nr
5f
and
3m
TB
Ian
dC
VAle
ftan
dri
ght
Bro
caap
hasi
a,A
oSan
ddy
sart
hria
nrnr
Coh
en&
Mas
se,1
993
3226
–76+
nrP
D,M
S,C
VAan
dC
PD
ysar
thri
anr
Mod
erat
ean
dse
vere
Gol
dfar
b&
Bad
er,1
979
150
mM
ulti
ple
CVA
sle
ftfr
onta
lG
loba
laph
asia
10ye
ars
Seve
re
Jung
blut
&A
ldri
dge,
2004
1549
–76
8m
and
7f
CVA
left
Bro
caap
hasi
aan
dgl
obal
apha
sia
4–26
year
sSe
vere
Jung
blut
etal
.,20
061
57m
CVA
left
Glo
bala
phas
ia37
mon
ths
Seve
reK
im&
Tom
aino
,200
87
57–8
42
man
d5
fSi
ngle
and
mul
tipl
eC
VAs
left
Non
fluen
tap
hasi
a,A
oSan
ddy
sart
hria
9m
onth
s–
21ye
ars
Mild
,mod
erat
ean
dse
vere
Nae
ser
&H
elm
-E
stab
rook
s,19
858
24–6
2nr
CVA
and
TB
IB
roca
apha
sia
and
glob
alap
hasi
a0–
51m
onth
sSe
vere
Popo
vici
,199
548
017
–82
77%
man
d23
%f
CVA
,tum
our,
TB
IB
roca
,Wer
nick
e,an
dam
nest
icap
hasi
a
nrM
ild,m
oder
ate
and
seve
re
Schl
aug
etal
.,20
082
47an
d58
2m
CVA
left
Bro
caap
hasi
a12
and
13m
onth
sSe
vere
Spar
kset
al.,
1974
8nr
nrC
VAle
ftN
onflu
ent
apha
sia
>6
mon
ths
Seve
reT
ampl
in,2
008
419
-51
3f
and
1f
CVA
and
TB
ID
ysar
thri
a2.
5–9.
5m
onth
sM
ild–s
ever
eW
ilson
etal
.,20
061
52m
CVA
left
Bro
caap
hasi
a46
mon
ths
Seve
re
m=
mal
e,f=
fem
ale,
nr=
notr
epor
ted,
TB
I=tr
aum
atic
brai
nin
jury
,CVA
=ce
rebr
ovas
cula
rac
cide
nt,P
D=
Par
kins
on’s
dise
ase,
MS
=m
ulti
ple
scle
rosi
s,C
P=
cere
bral
pals
y,A
oS=
apra
xia
ofsp
eech
.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 7
Interventions
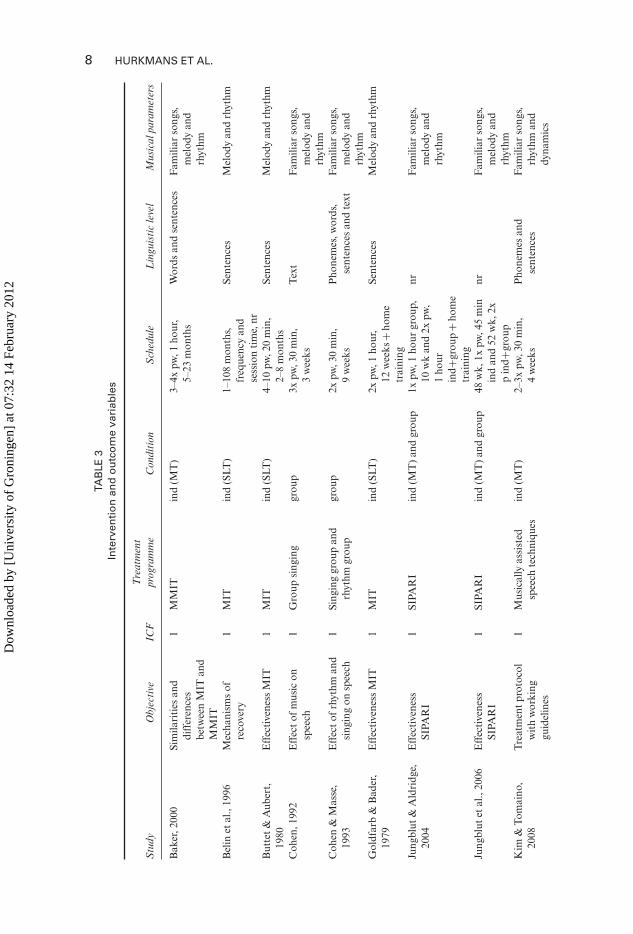
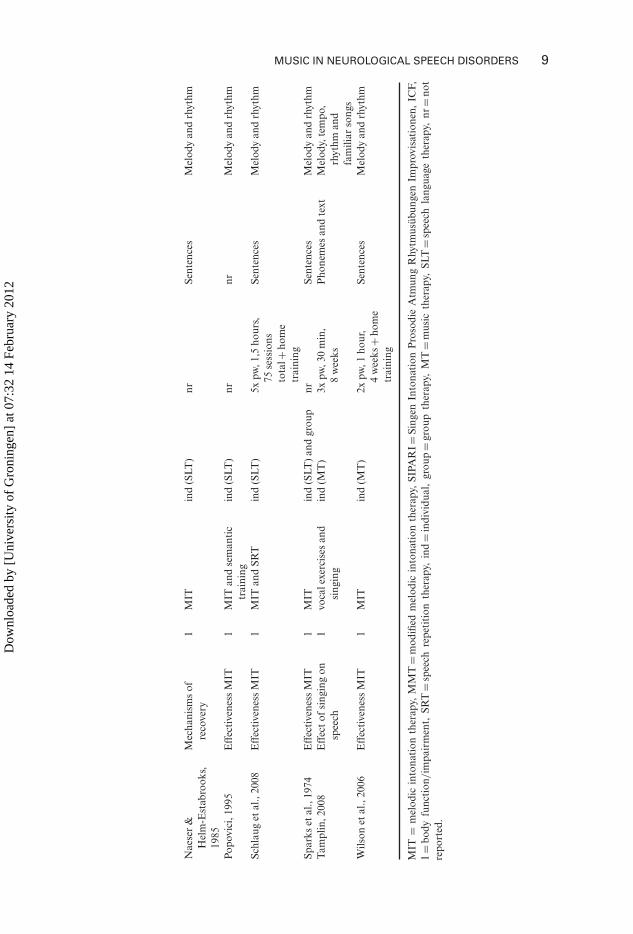
Table 3 is a summary of information for therapeutic interventions relative to the15 studies. One variable did not meet the 50% criterion of reporting: other language,speech, and music therapy interventions. This variable was therefore not reported inthis overview.
Nine studies evaluated the effectiveness of MIT (Albert et al., 1973). MIT wastherefore the most studied treatment programme. Individual treatment (speech-language therapy as well as music therapy) was the most studied treatment condition:in 12 studies patients received individual treatment. Combinations of SLT and musictherapy have not been reported. The schedules of the treatment intervention varied.MIT prescribes an intensive schedule of twice a day, 30 minutes each, five times a week.However, this guideline was not always followed in the studies evaluating the effective-ness of MIT; generally less therapy than recommended was given. All objectives havebeen formulated at the impairment level. At this level, sentences were studied the mostat the linguistic levels, and melody and rhythm were the most frequently used musicalparameters.
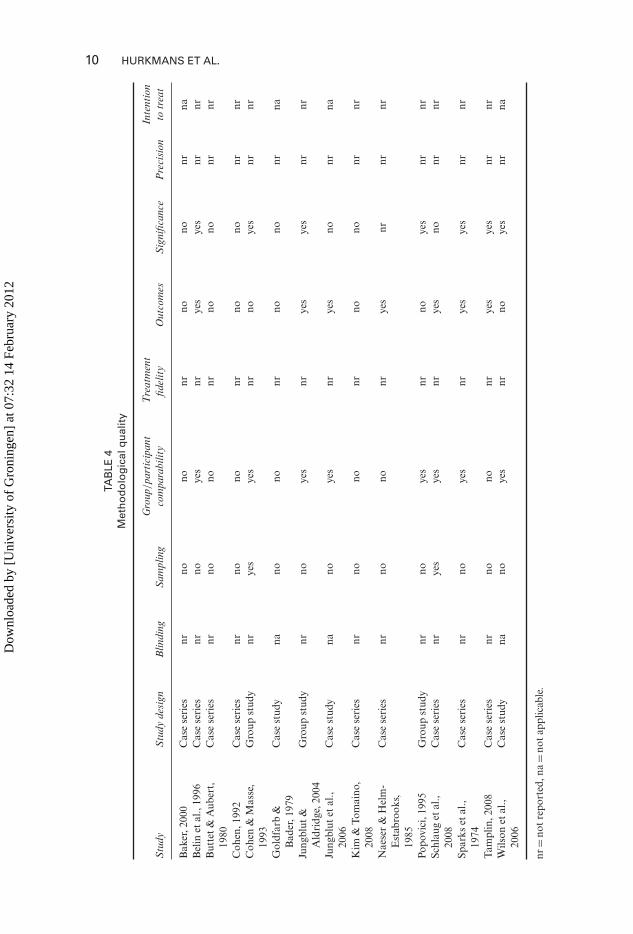
Methodological quality
An overview of the quality indicators for all 15 studies is presented in Table 4. Therewas high agreement between JH and MB in classifying each article. The method-ological quality of the studies varied with scores ranges from 0–4 (on a scale of0–9). Five studies obtained a score of 0, and two studies obtained a score of 4. Thescores of the other studies were in this range. The most frequently used study design(N = 9) was case series. None of the studies involved a randomised controlled trial(RCT), and mention of blinding, the use of intention-to-treat, and precision is notreported. In eight studies information on validity and reliability of the outcome mea-sures was missing. All studies used multiple outcome measures without classificationof main study parameters. Five studies used comprehensive language tests as out-come measure like the Boston Diagnostic Aphasia Examination (BDAE; Goodglass& Kaplan, 1972) and the Aachener Aphasia Test (AAT; Huber, Poeck, & Williams,1984). No distinction has been reported in related (speech parameters) and unrelatedmeasures (non-speech parameters like reading, writing, and auditory comprehension).In eight studies no p-values were reported.
Effectiveness of intervention
An overview of the effectiveness of interventions of the 15 studies is summarised inTable 5. All studies reported positive results. It is difficult to define the exact number ofpatients that improved because the depiction of the results varied extensively. Detailedinformation on which patients improved at which outcome measures was lacking inmost studies evaluating more than one patient (group studies and case series). It is dif-ficult to state the effectiveness of the intervention because all studies included multipleoutcome measures without defining the primary study outcome measure. Cohen andMasse (1993), for instance, reported improvement at verbal intelligibility but none atspeech rate.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012
8 HURKMANS ET AL.
TAB
LE3
Inte
rven
tio
nan
do
utc
om
eva
riab
les
Stu
dyO
bjec
tive
ICF
Tre
atm
ent
prog
ram
me
Con
diti
onS
ched
ule
Lin
guis
tic
leve
lM
usic
alpa
ram
eter
s
Bak
er,2
000
Sim
ilari
ties
and
diff
eren
ces
betw
een
MIT
and
MM
IT
1M
MIT
ind
(MT
)3–
4xpw
,1ho
ur,
5–23
mon
ths
Wor
dsan
dse
nten
ces
Fam
iliar
song
s,m
elod
yan
drh
ythm
Bel
inet
al.,
1996
Mec
hani
sms
ofre
cove
ry1
MIT
ind
(SLT
)1–
108
mon
ths,
freq
uenc
yan
dse
ssio
nti
me,
nr
Sent
ence
sM
elod
yan
drh
ythm
But
tet
&A
uber
t,19
80E
ffec
tive
ness
MIT
1M
ITin
d(S
LT)
4–10
pw,2
0m
in,
2–8
mon
ths
Sent
ence
sM
elod
yan
drh
ythm
Coh
en,1
992
Eff
ect
ofm
usic
onsp
eech
1G
roup
sing
ing
grou
p3x
pw,3
0m
in,
3w
eeks
Tex
tF
amili
arso
ngs,
mel
ody
and
rhyt
hmC
ohen
&M
asse
,19
93E
ffec
tof
rhyt
hman
dsi
ngin
gon
spee
ch1
Sing
ing
grou
pan
drh
ythm
grou
pgr
oup
2xpw
,30
min
,9
wee
ksP
hone
mes
,wor
ds,
sent
ence
san
dte
xtF
amili
arso
ngs,
mel
ody
and
rhyt
hmG
oldf
arb
&B
ader
,19
79E
ffec
tive
ness
MIT
1M
ITin
d(S
LT)
2xpw
,1ho
ur,
12w
eeks
+ho
me
trai
ning
Sent
ence
sM
elod
yan
drh
ythm
Jung
blut
&A
ldri
dge,
2004
Eff
ecti
vene
ssSI
PAR
I1
SIPA
RI
ind
(MT
)an
dgr
oup
1xpw
,1ho
urgr
oup,
10w
kan
d2x
pw,
1ho
urin
d+gr
oup
+ho
me
trai
ning
nrF
amili
arso
ngs,
mel
ody
and
rhyt
hm
Jung
blut
etal
.,20
06E
ffec
tive
ness
SIPA
RI
1SI
PAR
Iin
d(M
T)
and
grou
p48
wk,
1xpw
,45
min
ind
and
52w
k,2x
pin
d+gr
oup
nrF
amili
arso
ngs,
mel
ody
and
rhyt
hmK
im&
Tom
aino
,20
08T
reat
men
tpr
otoc
olw
ith
wor
king
guid
elin
es
1M
usic
ally
assi
sted
spee
chte
chni
ques
ind
(MT
)2–
3xpw
,30
min
,4
wee
ksP
hone
mes
and
sent
ence
sF
amili
arso
ngs,
rhyt
hman
ddy
nam
ics
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012
MUSIC IN NEUROLOGICAL SPEECH DISORDERS 9
Nae
ser
&H
elm
-Est
abro
oks,
1985
Mec
hani
sms
ofre
cove
ry1
MIT
ind
(SLT
)nr
Sent
ence
sM
elod
yan
drh
ythm
Popo
vici
,199
5E
ffec
tive
ness
MIT
1M
ITan
dse
man
tic
trai
ning
ind
(SLT
)nr
nrM
elod
yan
drh
ythm
Schl
aug
etal
.,20
08E
ffec
tive
ness
MIT
1M
ITan
dSR
Tin
d(S
LT)
5xpw
,1,5
hour
s,75
sess
ions
tota
l+ho
me
trai
ning
Sent
ence
sM
elod
yan
drh
ythm
Spar
kset
al.,
1974
Eff
ecti
vene
ssM
IT1
MIT
ind
(SLT
)an
dgr
oup
nrSe
nten
ces
Mel
ody
and
rhyt
hmT
ampl
in,2
008
Eff
ect
ofsi
ngin
gon
spee
ch1
voca
lexe
rcis
esan
dsi
ngin
gin
d(M
T)
3xpw
,30
min
,8
wee
ksP
hone
mes
and
text
Mel
ody,
tem
po,
rhyt
hman
dfa
mili
arso
ngs
Wils
onet
al.,
2006
Eff
ecti
vene
ssM
IT1
MIT
ind
(MT
)2x
pw,1
hour
,4
wee
ks+
hom
etr
aini
ng
Sent
ence
sM
elod
yan
drh
ythm
MIT
=m
elod
icin
tona
tion
ther
apy,
MM
T=
mod
ified
mel
odic
into
nati
onth
erap
y,SI
PAR
I=Si
ngen
Into
nati
onP
roso
die
Atm
ung
Rhy
tmus
übun
gen
Impr
ovis
atio
nen,
ICF,
1=
body
func
tion
/im
pair
men
t,SR
T=
spee
chre
peti
tion
ther
apy,
ind
=in
divi
dual
,gr
oup
=gr
oup
ther
apy,
MT
=m
usic
ther
apy,
SLT
=sp
eech
lang
uage
ther
apy,
nr=
not
repo
rted
.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012
10 HURKMANS ET AL.
TAB
LE4
Met
ho
do
log
ical
qu
alit
y
Stu
dyS
tudy
desi
gnB
lindi
ngS
ampl
ing
Gro
up/pa
rtic
ipan
tco
mpa
rabi
lity
Tre
atm
ent
fidel
ity
Out
com
esS
igni
fican
ceP
reci
sion
Inte
ntio
nto
trea
t
Bak
er,2
000
Cas
ese
ries
nrno
nonr
nono
nrna
Bel
inet
al.,
1996
Cas
ese
ries
nrno
yes
nrye
sye
snr
nrB
utte
t&
Aub
ert,
1980
Cas
ese
ries
nrno
nonr
nono
nrnr
Coh
en,1
992
Cas
ese
ries
nrno
nonr
nono
nrnr
Coh
en&
Mas
se,
1993
Gro
upst
udy
nrye
sye
snr
noye
snr
nr
Gol
dfar
b&
Bad
er,1
979
Cas
est
udy
nano
nonr
nono
nrna
Jung
blut
&A
ldri
dge,
2004
Gro
upst
udy
nrno
yes
nrye
sye
snr
nr
Jung
blut
etal
.,20
06C
ase
stud
yna
noye
snr
yes
nonr
na
Kim
&To
mai
no,
2008
Cas
ese
ries
nrno
nonr
nono
nrnr
Nae
ser
&H
elm
-E
stab
rook
s,19
85
Cas
ese
ries
nrno
nonr
yes
nrnr
nr
Popo
vici
,199
5G
roup
stud
ynr
noye
snr
noye
snr
nrSc
hlau
get
al.,
2008
Cas
ese
ries
nrye
sye
snr
yes
nonr
nr
Spar
kset
al.,
1974
Cas
ese
ries
nrno
yes
nrye
sye
snr
nr
Tam
plin
,200
8C
ase
seri
esnr
nono
nrye
sye
snr
nrW
ilson
etal
.,20
06C
ase
stud
yna
noye
snr
noye
snr
na
nr=
not
repo
rted
,na
=no
tap
plic
able
.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 11TA
BLE
5R
esu
lts
Stu
dyO
utco
me
mea
sure
(s)
ICF
NM
easu
red
impr
ovem
ent
Met
hodo
logi
calq
ualit
yM
echa
nism
sof
reco
very
Bak
er,2
000
Num
ber
ofw
ords
12
Num
ber
ofw
ords
incr
ease
din
both
pati
ents
0nr
Bel
inet
al.,
1996
BD
AE
,MR
I,an
dP
ET
17
Impr
ovem
ent
atit
em2,
4,5,
13,1
4,15
,and
19of
the
BD
AE
3Si
mpl
epa
ssiv
e(w
ord
hear
ing)
and
acti
ve(w
ord
repe
titi
on)
verb
alta
sks
perf
orm
edw
itho
utM
ITre
sult
sin
abno
rmal
acti
viti
esof
righ
the
mis
pher
est
ruct
ures
.W
ord
repe
titi
onpe
rfor
med
wit
hM
ITlo
aded
wor
dsre
acti
vate
sB
roca
’sar
eaan
dth
ead
jace
ntle
ftpr
efro
ntal
cort
exB
utte
t&
Aub
ert,
1980
Art
icul
atio
n,re
peti
tion
,and
audi
tory
com
preh
ensi
on1
74/
7go
odim
prov
emen
t,2/
7m
ildim
prov
emen
t,1/
7no
impr
ovem
ent
0nr
Coh
en,1
992
6as
pect
sof
voic
ean
dar
ticu
lati
on1
8Im
prov
emen
tin
spea
king
fund
amen
talf
requ
ency
vari
abili
ty,s
peec
hra
te,
and
verb
alin
telli
gibi
lity
0nr
Coh
en&
Mas
se,1
993
Spee
chra
tean
dve
rbal
inte
lligi
bilit
y1
32Si
ngin
ggr
oup:
impr
ovem
ent
atve
rbal
inte
lligi
bilit
y,no
impr
ovem
ent
atsp
eech
rate
.Rhy
thm
grou
p:no
impr
ovem
ent
4nr
Gol
dfar
b&
Bad
er,1
979
Rep
eati
ngse
nten
ces
(3co
ndit
ions
:nor
mal
,in
tone
d,an
din
tone
dw
ith
tapp
ing
11
Impr
ovem
ent
inal
lco
ndit
ions
0nr
(Con
tinu
ed)
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

12 HURKMANS ET AL.
TAB
LE5
(Con
tinu
ed)
Stu
dyO
utco
me
mea
sure
(s)
ICF
NM
easu
red
impr
ovem
ent
Met
hodo
logi
calq
ualit
yM
echa
nism
sof
reco
very
Jung
blut
&A
ldri
dge,
2004
AA
T1
15Im
prov
emen
tin
arti
cula
tion
and
pros
ody
ofsp
onta
neou
ssp
eech
and
inR
EP
and
NA
M
4nr
Jung
blut
etal
.,20
06A
AT
11
Impr
ovem
ent
inal
lpar
tsof
spon
tane
ous
spee
ch,T
T,R
EP,
and
NA
M
2nr
Kim
&To
mai
no,2
008
Art
icul
atio
n,flu
ency
,pr
osod
yan
dbr
eath
supp
ort
17
At
allo
utco
me
crit
eria
vari
able
impr
ovem
ent
have
been
mea
sure
dat
all
7pa
rts
ofth
epr
otoc
ol
0nr
Nae
ser
&H
elm
-Est
abro
oks,
1985
BD
AE
and
CT
scan
18
4/8
impr
ovem
ent
atth
eB
DA
E1
Pat
ient
sw
hore
spon
dpo
siti
vely
toM
ITha
veno
ton
lyse
vere
nonfl
uent
apha
sia
wit
hsl
ow,p
oorl
yar
ticu
late
dsp
eech
and
rela
tive
lygo
odau
dito
ryco
mpr
ehen
sion
,but
also
the
lesi
ons
invo
lve
Bro
ca’s
area
,no
larg
ele
sion
inW
erni
cke’
sar
eaan
dno
lesi
onin
the
righ
the
mis
pher
ePo
povi
ci,1
995
Aud
itor
yco
mpr
ehen
sion
,re
peti
tion
and
nam
ing
148
0W
erni
cke
>B
roca
and
anom
icap
hasi
aan
dM
IT>
sem
anti
cs
3nr
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 13
Schl
aug
etal
.,20
08C
IU,n
umbe
rof
sylla
bles
,pi
ctur
ena
min
gan
dfM
RI
12
Impr
ovem
ent
inal
lout
com
em
easu
res
3F
unct
iona
lim
agin
gta
sks
targ
etin
gm
usic
alco
mpo
nent
ste
ndto
elic
itgr
eate
rac
tivi
tyin
righ
the
mis
pher
icbr
ain
regi
ons
than
inle
fthe
mis
pher
icre
gion
s.T
appi
ngth
ele
ftha
nden
gage
sa
righ
the
mis
pher
icse
nsor
imot
orne
twor
kth
atco
ordi
nate
sor
ofac
iala
rtic
ulat
ory
mov
emen
tsSp
arks
etal
.,19
74B
DA
E,r
epet
itio
nan
dun
ison
spee
ch1
8Im
prov
emen
tin
6/8
pati
ents
3nr
Tam
plin
,200
8SI
T,P
DT,
RO
S,IW
PM
and
CE
R1
4Im
prov
emen
tin
SIT,
PD
T,IW
PM
,and
CE
RN
oim
prov
emen
tin
RO
S
2nr
Wils
onet
al.,
2006
Phr
ase
leng
th1
1Im
prov
emen
tin
phra
sele
ngth
2nr
BD
AE
=B
osto
nD
iagn
osti
cA
phas
iaE
xam
inat
ion,
MR
I=m
agne
tic
reso
nanc
eim
agin
g,P
ET
=po
sitr
onem
issi
onto
mog
raph
y,A
AT
=A
ache
nA
phas
iaT
est,
CT
=co
mpu
ted
tom
ogra
phy,
CIU
=co
rrec
tin
form
atio
nun
its,
fMR
I=fu
ncti
onal
mag
neti
cre
sona
nce
imag
ing,
SIT
=Se
nten
ceIn
telli
gibi
lity
Tes
t,P
DT
=P
ictu
reD
escr
ipti
onT
ask,
RO
S=
rate
ofsp
eech
,IW
PM
=in
telli
gibl
ew
ords
per
min
ute,
CE
R=
com
mun
icat
ion
effic
ienc
yra
tios
,IC
F,1=
body
func
tion
/im
pair
men
t,R
EP
=re
peat
ing,
NA
M=
nam
ing,
TT
=To
ken
Tes
t,nr
=no
tre
port
ed.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

14 HURKMANS ET AL.
Mechanisms of recovery
In three studies (Belin et al., 1996; Naesser & Helm-Estabrooks, 1985; Schlaug,Marchina, & Norton, 2008) examinations of mechanisms of recovery by PET, CT,and fMRI were conducted in the method of the study to explain the research findings.Neural correlates focused mainly on the observed brain activities in both hemispheresduring language tasks and at the location of the lesion. The other 12 studies interprettheir research findings but are hypothetical, since mechanisms of recovery are absentfrom the method of the study and therefore not objectively identical.
Schlaug et al. (2008) described two patients: one patient received MIT and theother patient received a combination of MIT and a control treatment (SRT: speechrepetition therapy). The patient receiving only MIT showed significantly more fMRIactivities in the right hemisphere. Naeser and Helm-Estabrooks (1985) studied twogroups of patients receiving MIT: a good response group and a poor response groupof MIT. CT information characteristics of both groups have been examined. Thegood response group showed lesions in Broca’s area in the left hemisphere. The poorresponse group showed lesions in both hemispheres and/or Wernicke’s area. Belinet al. (1996) evaluated a group of seven non-fluent aphasic patients who successfullyfinished MIT intervention. They measured changes in relative cerebral blood flow withPET during listening and repetition of words and during repetition of MIT loadedwords (i.e., with melody and rhythm). Their findings revealed abnormal activationin the right hemisphere without MIT language task and, in contrast, reactivation inBroca’s area and the left prefrontal cortex by repeating MIT loaded words.
As a concluding remark of the results, we gathered extensive information aboutmusic and language in the literature. Treatment approaches using musical elementsreported measurable improvement. However, the methodological quality of the effi-cacy studies was low and mechanisms of recovery were contradictory.
DISCUSSION
The purpose of this study was to review the existing literature on the effect of treatmentusing musical elements in the treatment of patients with neurological language andspeech disorders and mechanisms of recovery explaining positive effects. This reviewshows that a certain amount of information is revealed in the literature concerningtherapies using musical elements in the treatment of neurological language and speechdisorders. In the reviewed studies frequent gaps in the descriptions of patient charac-teristics and therapy interventions have been determined. Overall, the methodologicalquality of the studies was rated as low.
All but one of the studies involved stroke patients. This is understandable becausestroke patients are a rather homogeneous group in comparison to other patientswith acquired brain injuries (ABI). Findings in these studies can also theoretically beapplied to patients with other types of ABI; however, studies on this subject still needto be done. Both males and females were included in the investigations under study.In Popovici (1995) men dominated the study population. This may be explained by alarge subgroup of patients with TBI in their study sample (Tagliaferri, Compagnone,Korsic, Servadei, & Kraus, 2006). However, selection bias cannot be ruled out.
The studies included patients who were primarily in the chronic phase of post onsetrecovery. However, therapy is also given in the subacute phase. It is therefore important
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 15
in future research to study the effect of music elements in treatment in the subacutephase.
Education was not reported in the description of patient characteristics in onethird of the reviewed studies. Education may influence learning and is therefore animportant aspect in studying the effectiveness of treatment. Next to education, cog-nitive functioning is an important predictor of outcome since non-linguistic cognitiveimpairments may limit rehabilitation efficacy in patients with aphasia (Seniów, Litwin,& Lesniak, 2009). We will therefore study cognitive functioning next to education infuture efficacy research. Dominance was also not reported in more than half of thereviewed studies. Mainly in studies where music is a central topic of research interest,information about dominance is valuable since mechanisms of recovery focuses onbrain activities in one of the two hemispheres. Information about musical backgroundwas also lacking in patient characteristics (not specifically defined by objective crite-ria); theoretically, we assume that this variable may influence treatment outcome. Thediscrepancy is substantial between the description of language and speech functioningwhen information about the musical background is missing. This is especially the casewhen studying an intervention in which music plays such an important role. Notableis that musical elements of therapy mainly comprised melody and rhythm. The factthat MIT is the most studied programme to date may be an explanation; melody andrhythm are distinguished features of MIT. Other musical parameters like dynamics,tempo, and metre have not been applied.
In general, therapy interventions have been adequately described. MIT is an inter-nationally well-known programme (Norton, Zipse, Marchina, & Schlaug, 2009).Deviations with respect of content as well as therapy intensity of the originalmethod have been well described. Only a few times have other therapy interven-tions than the studied intervention (e.g., MIT) been reported. In clinical practiceaphasic patients receive various intervention programmes. It is therefore importantto know if the revealed improvement can be assigned to the studied programme or toco-interventions.
All the objectives of the reviewed studies were aimed at the (ICF) level of impair-ments. None of the studies conducted outcome measures at the (ICF) level of activitiesand/or participation. Therefore it is unknown whether revealed improvement at thelevel of impairments can be generalised in their application to communication in dailylife and if it has any social implications.
The power of evidence was low for the majority of the reviewed studies. A ran-domised controlled trial (RCT) with an adequate size is hardly accomplishable from apractical as well as a methodological standpoint (e.g., realising a homogeneous group).For that reason adequate alternative study designs are available: single-participantdesigns and case series (Howard, 2003). These study designs have frequently been usedin the reviewed studies. Case studies and case series offer an extraordinary opportunityto describe patient characteristics and intervention programmes in detail. The effec-tiveness of the therapy can be verified very precisely, even in a small group. Not onlyis a well-described method important to measure effectiveness of therapy but also theuse of statistics is needed to calculate p-values and to determine the likelihood thatstudy findings are results of chance. It is here that results of many articles were lim-ited: all studies report improvement but in over half the studies no statistics were used.That makes it difficult to conclude whether the measured improvement is the result ofthe studied therapy programme. For example, although a sufficient number of patients
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

16 HURKMANS ET AL.
are included in the study of Popovici (1995), the low level of evidence (score 3) maketheir conclusions about the positive effect of the treatment doubtful.
MIT is the therapy programme that was used in the three studies that identify neu-ral correlates to explain mechanisms of recovery. The purpose of MIT is to exploit theprosodic and melodic process components of the intact right hemisphere for use withleft hemisphere brain-damaged aphasic patients. The authors of the MIT hypothesisedthat successful recovery engages expressive language areas in the undamaged righthemisphere. This hypothesis is over 30 years old. Brain plasticity is profound, and reor-ganisation processes are dynamic with recovery of language function incorporatingboth hemispheres (e.g., Saur et al., 2006). However, this premise of the original devel-opers of MIT is still appropriate, as there has been no research to date that disprovesthis hypothesis. Two out of three studies in this review (Naeser & Helm-Estabrooks,1985; Schlaug et al., 2008) support the hypothesis of Albert et al. (1973). The find-ings of Belin et al. (1996) were surprising and contrary to the hypothesis proposed bythe developers of MIT and the original interpretation of MIT successes. Belin et al.reported that the recovery process coincides with the reactivation of left prefrontalstructures with melody and rhythm tasks rather than mechanisms of compensation inright hemisphere structures.
This review shows the difficulty of proving the effectiveness of therapy using musicalelements. Research in this field is in a fairly early state and an adequate system to clas-sify and describe complex interventions is lacking. We highly recommend the develop-ment of research guidelines to standardise data-reporting parameters such as patient’scharacteristics, intervention, and methodological quality. Different models can beused relevant to rehabilitation. Wade (2005) suggests a method for describing reha-bilitation interventions derived from two models: (1) the World Health Organisation’sInternational Classification of Functioning model of illness and (2) a model describingrehabilitation interventions. Patient characteristics can be adequately reported in theICF model. Intervention and outcome variables can be adequately reported in Wade’smodel where interventions may be described in terms of the situations where theseactions are applied, the immediate goals of any action, the level at which the interven-tion acts, the actions involved, the knowledge and skills needed to give the treatment,any specific equipment used, and any concomitant actions that may be necessary. Formethodological quality, we recommend study designs using the highest level of qualityindicators in the guidelines of ASHA levels-of-evidence scheme.
CONCLUSION
The purpose of this review was to assess the effects of musical elements in the treat-ment of neurological language and speech disorders. A systematic search of theliterature yielded 15 studies that met inclusion criteria.
Measurable improvement was reported in studies where musical components wereused in the treatment of neurological language and speech disorders. However, themethodological quality of studies was rated low. Therefore no conclusions can yet bedrawn with regard to the effect of the use of musical elements in the treatment of indi-viduals with acquired neurological disorders. Mechanisms of recovery remain unclear:two of the three studies that examined mechanisms of recovery via neuroimagingtechniques supported the role of the right hemisphere, but reports are contradictory
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 17
and exact mechanisms of recovery remain indefinable. Shortcomings in the currentresearch can be overcome by following standards as outlined by the discussion sectionin this article.
Manuscript received 26 January 2011Manuscript accepted 28 June 2011
First published online 6 October 2011
REFERENCESAlbert, M. L., Sparks, R. W., & Helm, N. A. (1973). Melodic intonation therapy for aphasia. Archives of
Neurology, 29, 130–131.ASHA. (2001). Scope of practice in speech-language pathology [Scope of Practice]. Retrieved from www.
asha.org/policyBaker, F., & Wigram, T. (2004). The immediate and long-term effects of singing on the mood states of
people with traumatic brain injury. British Journal of Music Therapy, 18(2), 55–64.Baker, F. A. (2000). Modifying the melodic intonation therapy program for adults with severe non-fluent
aphasia, Music Therapy Perspectives, 18(2), 110–114.Belin, P., van Eeckhout, Ph., Zilbovicius, M., Remy, Ph., François, C., Guillaume, S., et al. (1996). Recovery
from non fluent aphasia after melodic intonation therapy: A PET study. Neurology, 47(6), 1504–1511.Broca, P. (1861). Remarques sur le siège de la faculté du langage articulé suivis d’une observation d’aphémie.
Bulletin Societe Anatomique Paris, 36, 330–357.Brown, S., Martinez, M. J., & Parsons, L. M. (2006). Music and language side by side in the brain: A PET
study of the generation of melodies and sentences. European Journal of Neurosciences, 23, 2791–2803.Buttet, J., & Aubert, C. (1980). Melodic Intonation Therapy, contribution of neuropsychological reflex
activity to clinical medicine. Revue Medicale Suisse Romande, 100(2) 195–199.Cohen, N. S. (1992). The effect of singing instruction on the speech production of neurologically impaired
persons. Journal of Music Therapy, 30(2) 81–99.Cohen, N. S., & Ford, J. (1995). The effect of musical cues on the nonpurposive speech of persons with
aphasia. Journal of Music Therapy, 32(1), 46–57.Cohen, N. S., & Masse, R. E. (1993). The application of singing and rhythmic instruction as a therapeutic
intervention for persons with neurogenic communication disorders. Journal of Music Therapy, 30(2),81–99.
de Bruijn, M., Zielman, T., & Hurkmans, J. (2005). Speech-music therapy for aphasia, SMTA. Friesland,The Netherlands: Revalidatie.
Déjérine, J. (1914). Sémiologie des affections du système nerveux. Paris, France: Masson et C.Gamer, R. L. (1892). The human voice – Human bag pipe – Human piccolo, flute and fife – The voice as
a whistle – Music and noise – Dr. Bell and his visible speech. In The speech of monkeys (pp. 185–188).New York, NY: Charles L. Webster & Company.
Gerstman, H. L. (1964). A case of aphasia. Journal of Speech and Hearing Disorders, 29, 89–91.Goldfarb, R., & Bader, E. (1979). Espousing melodic intonation therapy in aphasia rehabilitation; a case
study. International Journal of Rehabilitation Research, 2(3), 333–342.Goodglass, H., & Kaplan, E. (1972). Boston Diagnostic Aphasia Examination. Philadelphia, PA: Lea &
Febiger.Hébert, S., Racette, A., Gagnon, L., & Peretz, I. (2003). Revisiting the dissociation between singing and
speaking in expressive aphasia. Brain, 126(8), 1838–1850.Howard, D. (2003). Single cases, group studies and case series in aphasia therapy. In I. Papathanasiou &
R. De Bleser (Eds.), The sciences of aphasia: From therapy to theory (pp. 245–258). Amsterdam, TheNetherlands: Pergamon.
Huber, W., Poeck, K., & Williams, K. (1984). The Aachen Aphasia Test. In F. C. Rose (Ed.), Progress inaphasiology (pp. 291–303). New York, NY: Raven Press.
Jeffries, K. J., Fritz, J. B., & Braun, A. R. (2003). Words in melody: An H(2)15O PET study of brainactivation during singing and speaking. Neuroreport, 14(5), 749–754.
Jochims, S. (1995). Emotional processes of coping with disease in the early stages of acquired cerebrallesions. The Arts of Psychotherapy, 22(1) 21–30.
Jungblut, M., & Aldridge, D. (2004). The music therapy intervention SIPARI (registered trademark) withchronic aphasics-research findings. Neurological Rehabilitation, 10(2), 69–78.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

18 HURKMANS ET AL.
Jungblut, M., Gerhard, H., & Aldridge, D. (2006). Recovery from chronic global aphasia by a specifictherapy treatment – report of a case. Neurological Rehabilitation, 12(6), 339–347.
Kim, M., & Tomaino, C. M. (2008). Protocol evaluation for effective music therapy for persons with nonfluent aphasia. Topics in Stroke Rehabilitation, 15(6), 555–569.
Magee, W. L., Brumfitt, S. M., Freeman, M., & Davidson J. W. (2006). The role of music therapy in an inter-disciplinary approach to address functional communication in complex neuro-communication diorders:a case report. Disability and Rehabilitation, 28(19), 1221–1229.
Magee, W. L., & Davidson, J. W. (2002). The effect of music therapy on mood states in neurological patients(a pilot study). Journal of Music Therapy, 39(1), 20–29.
Naeser, M. A., & Helm-Estabrooks, N. (1985). CT scan lesion localisation and response to melodicintonation therapy with non fluent aphasia cases. Cortex, 21(2), 203–223.
Norton, A., Zipse, L., Marchina, S., & Schlaug, G. (2009). Melodic intonation therapy: Shared insights onhow it is done and why it might help. Annals of the New York Academy of Sciences, 1169, 431–436.
Patel, A. (2003). Language, music, syntax and the brain. Nature Neuroscience, 6(7), 674–681.Popovici, M. (1995). Melodic intonation therapy in the verbal decoding of aphasics. Romanian Journal of
Neurology and Psychiatry, 33(1), 57–97.Racette, A., Bard, C., & Peretz, I. (2006). Making non-fluent aphasics speak: Sing along! Brain, 129,
2571–2584.Saur, D., Lange, R., Baumgaertner, A., Schraknepper, V., Willmes, K., Rijntjes, M., et al. (2006). Dynamics
of language reorganization after stroke. Brain, 129, 1371–1384.Schlaug, G., Marchina, S., & Norton, A. (2008). From singing to speaking: Why singing may lead to
recovery of expressive language functioning in patients with Broca’s aphasia. Music Perception, 25(4),315–323.
Seniów, J., Litwin, M., & Lesniak, M. (2009). The relationship between non-linguistic cognitive deficits andlanguage recovery in patients with aphasia. Journal of the Neurological Sciences, 283, 91–94.
Sparks, R., Helm, N., & Albert, M. (1974). Aphasia rehabilitation resulting from melodic intonationtherapy. Cortex, 10(4), 303–316.
Straube, T., Schulz, A., Geipel, K., Mentzel, H-J., & Miltner, W. H. R. (2008). Dissociation between singingand speaking in expressive aphasia: The role of song familiarity. Neuropsychologia, 46, 1505–1512.
Tagliaferri, F., Compagnone, C., Korsic, M., Servadei, F., & Kraus, J. (2006). A systematic review of braininjury epidemiology in Europe. Acta Neurochirgica, 148, 255–268.
Tamplin, J. (2008). A pilot study into the effect of vocal exercises and singing on dysarthric speech.Neurorehabilitation, 23(3), 207–216.
Wade, D. (2005). Describing rehabilitation interventions. Clinical Rehabilitation, 19, 811–818.Wilson, S. J., Parsons, K., & Reutens, D. C. (2006). Preserved singing in aphasia: A case study of the efficacy
of melodic intonation therapy. Music Perception, 24(1), 23–36.
APPENDIX
Music therapy (MT) can serve different goals in the rehabilitation of neurologicallyimpaired patients. A common approach in MT is to apply non-verbal aspects deal-ing with emotional and social problems. In addition, MT can be aimed at verbalexpression and communication. Adults suffering from neurological impairments arechallenged to “relearn” activities of daily living that were once performed with ease, aswell as to emotionally adjust to their limitations and changed life circumstances. Thesedeep emotions can negatively influence rehabilitation (Baker & Wigram 2004; Jochims1995; Magee & Davidson, 2002). Throughout the rehabilitation process clients tendto form a new identity and re-shape their future, which demands significant effortand perseverance. This process often leads to sadness, anger, and feelings of inferi-ority and insecurity. MT considers the body and mind as inseparable and thereforeMT approaches focus on the medical-physical and on the social-emotional aspectsof rehabilitation. SMTA, for example focuses primarily on speech-language exercisesset to music; however it also draws on music’s potential for relaxation and enjoyment
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012

MUSIC IN NEUROLOGICAL SPEECH DISORDERS 19
so clients experience the program as being “less technical”. Patients enjoy the inter-vention and are able to sustain their participation for long periods of time (Magee,Brumfitt, Freeman, & Davidson, 2006). The joint singing of patient and therapistsemphasises the social aspect of music making, thereby acting to reduce isolation.
The MT interventions are designed to musically support the speech-language exer-cises, and as such they share the same structural linguistic levels. Using tempo, metre,rhythm, and dynamic parameters the music therapist varies the melodies, therebyincreasing the level of difficulty over the course of treatment. The different parame-ters are adapted to the individual patient’s capabilities, thereby simplifying the singingexercise for the client when needed (De Bruijn et al., 2005). MT considers music tempoto be the key for melodic adaptation. Some features of tempo are familiar in MT.A slow tempo for example creates a sense of relaxation. But a tempo that is too slowbecomes static: there is no flowing motion. This does not stimulate the client andmay negatively affect the patient’s singing. And finally, a fast/faster tempo may stim-ulate the client and increase the level of concentration required to perform the task.Variations in metre provide opportunities for the patient to practice the same materialwhile maintaining interest. Some familiar features of metre are the following: 4/4 and2/4 beats are supportive, familiar, and easy to sing; 3/4 and 3/8 beats evoke a sway-ing motion and are suitable when relaxation (decrease in tension) would enhance theclient’s performance in the exercises; and finally a 6/8 beat may be perceived as bothdouble and triple time. The movement stimulated by the 6/8 beat is relaxing, but maylead to an increase in tempo. Variations in rhythm are determined by the prosodic fea-tures of speech. Some characteristics of rhythm are important in MT: the order of longand short note values influence the degree of rhythmic complexity and therefore theexercise’s level of difficulty. For example, in 4/4 time the sequence long–short–short ismore difficult than short–short–long because it allows the patient less time to preparehimself for the repetition of the exercise. Syncopation is not part of natural speech andshould therefore be avoided in MT.
In MT dynamics ranges from mezzo-piano to mezzo-forte, which is usually the leasttaxing on the voice. However, this choice is dependent on the (emotional) content ofthe exercise. Some following features related to dynamics should be considered in MT:crescendos are useful during the repetition of sentences that are intended as exclama-tions; sometimes the use of forte or even fortissimo is necessary, for example to call orwarn someone or to express emotions.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
roni
ngen
] at
07:
32 1
4 Fe
brua
ry 2
012