mutation testing - ariadcmlrisks.com/resources/pdf/mutation testing slide kit.pdf · cml treatment...
TRANSCRIPT

CML Treatment Failure:
More Threatening Than
It Appears
Mutation Testing

Content
• Mutations and treatment failure
• Single mutations
• Compound mutations
• Mutation testing
• Guideline recommendations
• Summary
2
Mutations and
Treatment Failure

BCR-ABL1 mutation can confer TKI resistance and
is a mechanism of treatment failure in CML
4
1. Soverini S, et al. Clin Cancer Res. 2006;12:7374-7379. 2..Cortes J, et al. Blood. 2007;109:3207-3213. 3. Bixby D, et al. Leukemia. 2011;25:7-22. 4. Bowlin SJ, et al. ASCPT 2012. 5. Quintás-Cardama A, et al. Cancer Control. 2009;16:122-131. 6. Valent P. Biologics. 2007; 1:433-438. 7. Corbin AS, et al. J Clin Invest. 2011;12:396-409.
Resistance
BCR-ABL1 Mutation
(~40%)1,2
Activation of SRC family kinases3
Drug binding, inadequate drug concentration, or
epigenetic modifications3
Drug-drug interactions4
Increased drug efflux or influx3,5
Inability of TKIs to eradicate mutant
stem cells or cross the blood-brain barrier6,7
BCR-ABL1 gene amplification3
BCR-ABL1 independent
BCR-ABL1 dependent
Others
(~60%)

How do BCR-ABL1 mutations emerge?
5
Sensitive
to TKI
Resistant
to TKI
Treat with TKI
Sensitive
to TKI
Resistant
to TKI
1. Soverini S, et al. Blood. 2011;118:1208-1215. 2. Sierra JR, et al. Molec Cancer. 2010;9:75. 3. Bauer RC, et al. Clin Cancer Res. 2013;19: 2962-2972.
• Mutations can occur in cancer cells where genetic instability is high and
accumulation of further abnormalities is likely1,2
• TKI therapy can select for BCR-ABL1 mutations in unstable cancer cells
– Small cell populations containing mutations may have a survival advantage
during TKI therapy and emerge later as the dominant clone1,2
– In an in vitro simulation, sequential use of TKIs increases the probability that
mutations will arise, and the sequence of TKIs used may influence the types
of mutations that emerge3

Mutation-related TKI resistance is
common in patients with CML
6 Ai J, et al. Ther Adv Hematol. 2014;4:107-120.
Up to one in five newly-diagnosed CP-CML patients who start first-line TKI
therapy will develop a BCR-ABL1 mutation

Physicians do not always test for mutations
according to guideline recommendations
7
• According to a 2010 survey of 507 physicians treating
patients with CML1*
• Many clinicians do not appreciate the role of mutation
analysis in the overall management of CML2
Nearly half would not
test for BCR-ABL1 KD
mutations in patients not
achieving MMR two years
after the initiation of
TKI therapy1
9% indicated that they
were unfamiliar with, never
ordered, or did not have
access to the test for
BCR-ABL1 KD mutations1
*Prospective United States-based, noninterventional, cross-sectional study conducted through an online survey in December 2010. 1. Kantarjian HM, et al. Clin Lymphoma Myeloma Leuk. 2013;13:48-54. 2. Ai J, Tiu RV. Ther Adv Hematol. 2014;5:107-120.

Single Mutations

Over 90 BCR-ABL1 point mutations have
been identified that affect sensitivity to certain TKIs
9
1242T M244V
L248V
G250E/R
Q252R/H
Y253F/H
E255K/V
D276G
T277A
E279K
V280A
V289A/I
F311L/I
T315I
F317L/V/I/C
Y320C
L324Q
F359V/I/C/L
D363Y
L364I
A365V
A366G
L370P
E373K
V371A
S417F/Y
I418S/V
A433T
S438C
E450K/G/A/V
E453G/K/V/Q
E459K/V/G/Q
M237V E258D
W261L
L273M
E275K/Q
E292V/Q
I293V
L298V V299L
Y342H
M343T
A344V
A350V
M351T
E355D/G/A
V379I
A380T
F382L
L384M
L387M/F/V
H396P/R/A
M388L
Y393C
A397P
M472I
P480L
F486S
E507G
P-loop SH3
contact SH2
contact A-loop
Data from patients resistant to first-generation TKI therapy, collated from 27 studies
published between 2001 and 2009.
Star indicates amino acid position reported to be directly involved in first-generation TKI binding via hydrogen bonds or
van der Waals interactions.
Soverini S, et al. Blood. 2011;118:1208-1215.

Spectrum and frequency of BCR-ABL1
KD mutations recovered after TKI therapy
10
Lighter color corresponds to the first amino acid change; darker color corresponds to the second amino acid change,
if applicable. Cortes J, et al. Blood. 2007;110:4005-4011.

Higher number of mutations were associated
with poor survival and 4 year EFS
11
• According to a single-center study of 207 patients with chronic
phase, accelerated phase, or blast phase CML who failed
first-line TKI, those with >1 BCR-ABL1 mutation exhibited
worse response rates and long-term outcomes with TKI
therapy compared with those with ≤1 BCR-ABL1 mutation.
Among patients with 0, 1, or >1 BCR-ABL1 mutation1:
– 4-year EFS were 56%, 49%, and 0%, respectively (P=0.02)
– Overall survival rates were 91%, 69%, and 75%,
respectively (P=0.13)
1. Quintas-Cardama A, et al. Haematologica. 2011;96(6):918-921.

NCCN Clinical Practice Guidelines In Oncology (NCCN
Guidelines®) treatment recommendations
based on BCR-ABL1 mutations
12
Mutation present 2L and subsequent therapy options
Y253H DAS, BOS
E255K/V DAS, BOS
F359V/C/I DAS, BOS
F317L/V/I/C NIL, BOS
V299L NIL
T315A NIL, BOS
T315I PON, OMA, HCT, or clinical trial
Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Myeloid Leukemia V.2. 2017. © 2017
National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for
any purpose without the express written permission of NCCN. To view the most recent and complete version of the NCCN Guidelines, go online to
NCCN.org. The NCCN Guidelines are a work in progress that may be refined as often as new significant data becomes available. NCCN makes no
warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.

ELN guidelines: Treatment recommendations
based on BCR-ABL1 mutations
13
In vitro sensitivity based on select BCR-ABL1 mutations*
Mutation present Second-generation TKI IC50, range (nM)
NIL DAS BOS PON
Y253H 450-1300 1.3-10 NA 6.2
E255K 118-566 5.6-13 394 14
E255V 430-725 6.3-11 230.1 36
F359V 91-175 2.2-2.7 38.6 10
F317L 39.2-91 7.4-18 100.7 1.1
F317V 350 NA NA 10
V299L 23.7 15.8-18 1086 NA
T315A NA 760 NA 1.6
T315I 697 to >10,000 137 to
>1000 1890 11
Baccarani M, et al. Blood. 2013;122:872-884.
*Per the ELN guidelines, one factor to take into consideration when considering switching TKIs is the presence and type of mutation.

The probability of TKI-resistant mutations may
increase as the line of therapy increases and CML
disease progresses
14 1. Bauer RC, et al. Clin Cancer Res. 2013;19:2962-2972. 2. Soverini S, et al. Blood. 2011;118:1208-1215. 3. Soverini S, et al. Blood. 2009;114: 2168-2171.
• Although patients may develop resistance to TKI therapy at any time,
the risk of developing additional mutations may increase as patients
move to later lines of TKI therapy and as the disease progresses1
Up to 80%
of patients with BP-CML
have mutations2
83% of first-generation
TKI-resistant patients who
relapsed while on a second-
or third-line TKI experienced
an emergence of newly
acquired BCR-ABL1
mutations3

Compound Mutations

Compound mutations
16
• Treatment with multiple TKIs may select for compound mutations (≥2 mutations in the same
BCR-ABL1 molecule) that confer resistance to multiple TKIs1,2
• In vitro data suggest that compound mutations can be highly resistant to certain TKIs3
BCR-ABL1 compound mutations1
1. Khorashad JS, et al. Blood. 2013;121:489-498. 2. Shah NP, et al. J Clin Invest. 2007;117:2562-2569. 3. O’Hare T, et al. Nat Rev Cancer. 2012;12:513-526.
CML cells

Sequential therapy may increase the
probability of compound mutations1
17 1. Shah et al. J Clin Invest. 2007;117:2562-2569.

Mutation Testing
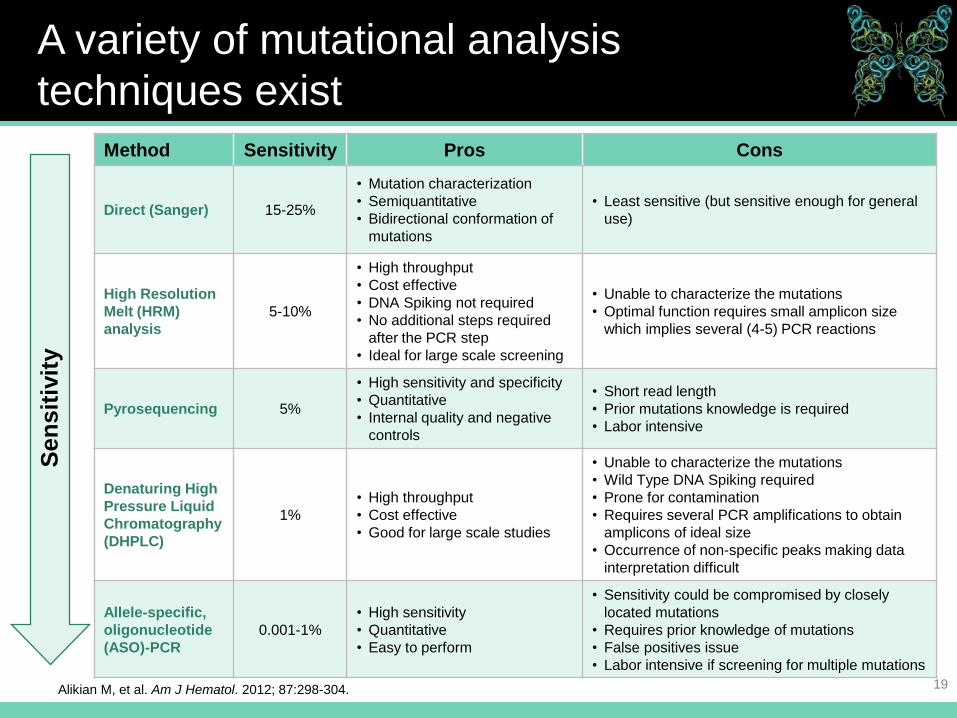
A variety of mutational analysis
techniques exist
19
Abbreviations: AP, accelerated phase; BP, blast phase; CP, chronic phase.
Method Sensitivity Pros Cons
Direct (Sanger) 15-25%
• Mutation characterization
• Semiquantitative
• Bidirectional conformation of
mutations
• Least sensitive (but sensitive enough for general
use)
High Resolution
Melt (HRM)
analysis
5-10%
• High throughput
• Cost effective
• DNA Spiking not required
• No additional steps required
after the PCR step
• Ideal for large scale screening
• Unable to characterize the mutations
• Optimal function requires small amplicon size
which implies several (4-5) PCR reactions
Pyrosequencing 5%
• High sensitivity and specificity
• Quantitative
• Internal quality and negative
controls
• Short read length
• Prior mutations knowledge is required
• Labor intensive
Denaturing High
Pressure Liquid
Chromatography
(DHPLC)
1%
• High throughput
• Cost effective
• Good for large scale studies
• Unable to characterize the mutations
• Wild Type DNA Spiking required
• Prone for contamination
• Requires several PCR amplifications to obtain
amplicons of ideal size
• Occurrence of non-specific peaks making data
interpretation difficult
Allele-specific,
oligonucleotide
(ASO)-PCR
0.001-1%
• High sensitivity
• Quantitative
• Easy to perform
• Sensitivity could be compromised by closely
located mutations
• Requires prior knowledge of mutations
• False positives issue
• Labor intensive if screening for multiple mutations
Alikian M, et al. Am J Hematol. 2012; 87:298-304.
Sen
sit
ivit
y

Clinical conditions and the presence
of BCR-ABL1 mutations
20
Mutation analysis in 399 patients with CP-CML receiving first-line, first-generation TKI
Clinical condition Patients tested for
mutations, n Presence of ≥1 BCR-ABL1
mutations (%)
Failure 166 45 (27)
No CHR at 3 mo 16 3 (19)
No CyR at 6 mo 9 1 (11)
No PCyR at 12 mo 24 4 (17)
No CCyR at 18 mo 36 6 (17)
Loss CCyR 49 15 (31)
Loss CHR 32 16 (50)
Suboptimal 233 11 (5)
No CyR at 3 mo 15 1 (7)
No PCyR at 6 mo 20 1 (5)
No CCyR at 12 mo 51 5 (8)
No MMR at 18 mo 52 0 (0)
Loss MMR (but not CCyR) 95 4 (4)
Soverini S, et al. Blood. 2011;118:abstract 112.

Sanger sequencing is the most
extensively used technique
• Direct (Sanger) sequencing is currently the most extensively
used technique to detect BCR-ABL1 mutations1,2
– Least sensitive method, but sufficient for general use
– Several contract labs offer this service
• Sanger can be useful for predicting the best course of
treatment for TKI-resistant patients and for monitoring
resistant mutations in subsequent treatment settings2,3
21 1. Baccarani M, et al. Blood. 2013;122:872-884. 2. Alikian M, et al. Am J Hematol. 2012; 87:298-304. 3. Soverini S, et al. Blood. 2011;118:1208-1215.

Sanger sequencing may not detect all
mutations present
10
F359C
E255K
Y253H
E255V
F317L
F359V
T315I
Mutations detectable by Sanger
sequencing (n=169)
Low-level mutations detectable by mass-
spectrometry assay only (n=132)
Frequency of mutations (%)
4 2 6 0
22 Parker WT, et al. J Clin Oncol. 2011;29:4250-4259.
• Mutation testing performed
after failure with a first-
generation TKI prior to
treatment with second-
generation TKIs (n=220)
• Mutations that would
influence therapeutic
decisions after failure with
a first-generation TKI were
found in more patients with
mass spectrometry than
direct sequencing
(32% vs 23%; P=0.03)
8

Low-level mutations can influence failure-free survival
in CP-CML patients treated with second-generation TKIs
after failure with a first-generation TKI
23
Pro
babili
ty o
f fa
ilure
-fre
e s
urv
ival (
%)
0 2 4 6 8 10 12 14 16 18 20 0
20
40
60
80
100
Low-level mutations by
mass spectrometry (n=6)
Mutations by sequencing (n=9)
Months since start of second-line therapy
No mutations (n=38)
Parker WT, et al. J Clin Oncol. 2011;29:4250-4259.

NGS provides a higher level of sensitivity to detect
clinically relevant BCR-ABL1 mutations that are not
detected by Sanger sequencing1
24 1. Molecular MD. http://www.molecularmd.com/case-studies/next-generation-sequencing-ngs-of-bcr-abl1-kinase-domain. Accessed December 2015. 2. Baccarani M et al. ASCO. 2014:167-175. 3. Shuen A, Foulkes WD. Curr Onc. 2010;17(5):39-42.
• NGS performs ultra-deep sequencing (UDS) of the
BCR-ABL1 kinase domain2
– UDS provides increased sensitivity and dissects qualitatively
and quantitatively the clonal texture of the mutated BCR-ABL1
positive subpopulations2
• NGS is comprehensively selective for mutations that likely
contribute to disease pathogenesis3
– For example, NGS identifies potential driver mutations (genetic
alterations that provide the cell with a survival advantage),
while filtering out passengers (mutations that can be expected
to have no effect on cell survival)3

NGS detects more mutations than
Sanger sequencing
25
51 49
10
39
61
23
0
10
20
30
40
50
60
70
No mutations Mutations ≥2 mutations
Pro
po
rtio
n o
f p
ati
en
ts, %
Sanger
NGS
Baseline mutation status. 267 patients with CP-CML resistant/intolerant to at least 2 prior TKIs or with
the T315I mutation.
Deininger MW, et al. Blood. 2016;127:703-712.

Deep sequencing (DS) may detect mutations
earlier than conventional sequencing
26
Soverini S, et al. Blood. 2014;124: Abstract 815.
• 51 patients treated with second-generation TKIs for a median of 9
months following failure of a first-generation TKI acquired BCR-ABL1
mutations detected by conventional sequencing
– Previously collected samples were analyzed for mutations using DS
• In 23 patients (45%), DS identified mutations that may confer
resistance following failure of a first-generation TKI
– Median interval between detection by DS and conventional sequencing:
3 months (range, 1-9 months)
• Response status (as per ELN 2013 guideline) at the time of mutation
detection by DS was Optimal (n=1), Warning (n=13), Failure (n=4);
5 patients had mutations at baseline (i.e., after failure of a first-
generation TKI)
• Results suggest that mutation testing using DS may be useful for
patients with Warning during second-line therapy

Guideline Recommendations

Mutational analysis may provide additional
information for patients with inadequate response
28
• The presence of mutations remains a consideration when making treatment
decisions1
• Routine monitoring of BCR-ABL1 transcripts, in conjunction with cytogenetic
evaluation, provides important information about long-term disease control in
patients with CML2
• National Comprehensive Cancer Network® (NCCN®) and ELN guidelines do not
recommend a specific technique1,2
Recommendations on When to Perform Mutational Analysis
ELN1,3:
• In case of treatment failure or
progression to AP or BP
NCCN2:
• CP-CML
- Failure to reach response milestones
- Any sign of loss of response (defined as hematologic or
cytogenetic relapse)
- 1-log increase in BCR-ABL1 transcript levels and loss of
MMR
• Disease progression to AP or BP
IS, International Scale. 1. Baccarani M, et al. Blood. 2013;122: 872-884. 2. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Myeloid Leukemia V.2.1017. © National Comprehensive Cancer Network, Inc. 2017 All rights reserved. Accessed January 20, 2017. To view the most recent and complete version of the guideline, go online to NCCN.org. 3. Soverini S, et al. Blood. 2011;118:1208-1215.
Analysis of mutations in CP-CML
• Mutations studies can help make treatment decisions in the
event of cytogenetic or hematologic relapse1,2
– Certain mutations confer resistance to certain TKIs1,2
• There is currently no role for mutation analysis at diagnosis
or in patients with adequate response to therapy1,2
29
1. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Myeloid Leukemia V.2.1017. ©
National Comprehensive Cancer Network, Inc. 2017 All rights reserved. Accessed January 20, 2017. To view the most recent and complete version of
the guideline, go online to NCCN.org. 2. Soverini S, et al. Blood. 2011;118:1208-1215.

Treatment options for TKI-resistant CML
1. Ai et al. Ther Adv Hematol. 2014;5:107-120. 2. Baccarani M, et al. Blood. 2013;122:872-884. 3. Referenced with permission from the NCCN Clinical
Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Myeloid Leukemia V.2.1017. © National Comprehensive Cancer Network, Inc. 2017
All rights reserved. Accessed January 20, 2017. To view the most recent and complete version of the guideline, go online to NCCN.org. 4. Baccarani M,
et al. Ann Oncol. 2012;23(Suppl7):vii72-7. 30
• The results of mutational analysis is one of many factors
(eg, efficacy, safety, patient comorbidities, cost) in making
treatment decisions1
• For patients with TKI-resistant CML, potential treatment
options include2-4:
– Alternate TKI
– Protein synthesis inhibitors
– Allogeneic hematopoietic stem cell transplantation (HCT)
– Clinical trial
Summary

1. Soverini S, et al. Clin Cancer Res. 2006;12:7374-7379. 2..Cortes J, et al. Blood. 2007;109:3207-3213. 3. Bixby D, et al. Leukemia. 2011;25:7-22. 4. Bowlin SJ, et al. ASCPT 2012. 5. Quintás-Cardama A, et al. Cancer Control. 2009;16:122-131. 6. Valent P. Biologics. 2007; 1:433-438. 7. Corbin AS, et al. J Clin Invest. 2011;12:396-409. 8. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Myeloid Leukemia V.2.1017. © National Comprehensive Cancer Network, Inc. 2017 All rights reserved. Accessed January 20, 2017. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way. 9. Kantarjian HM, et al. Clin Lymphoma Myeloma Leuk. 2013;13:48-54. 10. Ai J, Tiu RV. Ther Adv Hematol. 2014;5:107-120. 11. Baccarani M, et al. Blood. 2013;122: 872-884. 12. Soverini S, et al. Blood. 2011;118:1208-1215.
Summary
• Mutations in the BCR-ABL1 kinase domain may emerge at any time
during TKI therapy and confer treatment resistance1-7
• The type of mutation can help determine the most appropriate
subsequent therapy8
• Despite its recommendation in current treatment guidelines, mutational
analysis is not always performed in patients with suspected TKI
resistance8,9
• Mutational analysis, as recommended in current treatment guidelines,
should be considered a standard part of monitoring CML patients
treated with TKIs8,10-11
32

All trademarks are the property of their respective owners.
©2017 ARIAD Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda
Pharmaceutical Company Limited. All rights reserved. DS/0216/0025/US(3)