myasthenia gravis in the elderly johan a. aarli university of bergen, norway
TRANSCRIPT

Myasthenia gravis in the elderly
Johan A. Aarli
University of Bergen, Norway
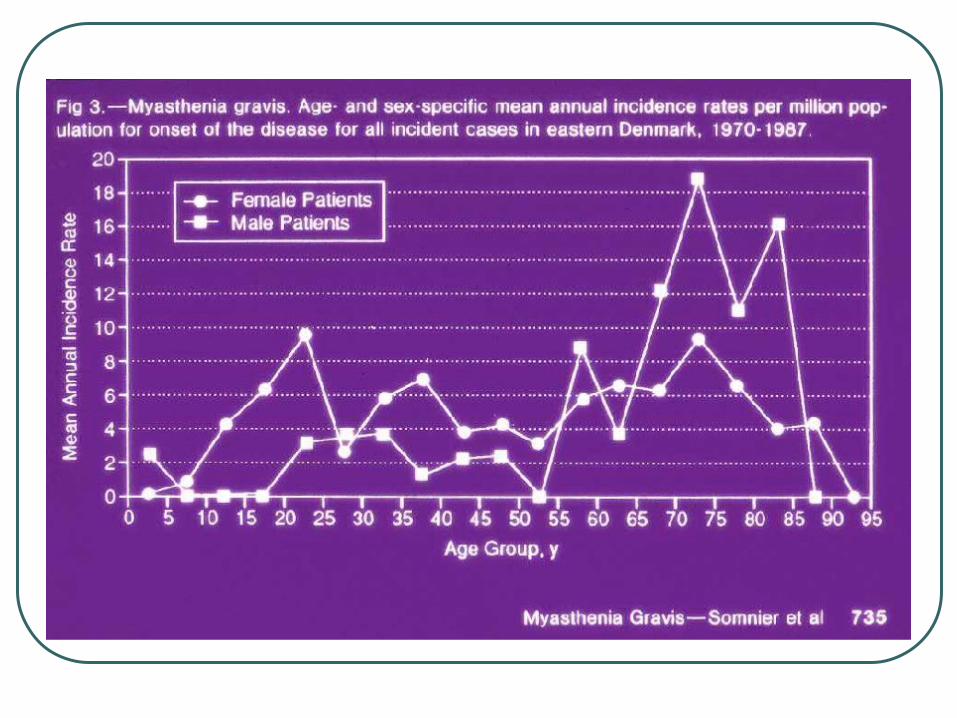
Has late onset myasthenia gravis become commoner?
Casetta et al. Incidence of myasthenia gravis in the province of Ferrara: a community-based study. Neuroepidemiology 236(6):281-284 (2004)
Matsuda M et al. Increase in incidence of elderly-onset patients with myasthenia gravis in Nagano Prefecture, Japan. Intern Med;44(6):572-527 (2005)
Merrigioli MW, Sanders DB. Autoimmune myasthenia gravis: emerging clinical and biological heterogeneity Lancet Neurology 8(5):475-490 (2009)
Ôöpik M, Kaasik A-E, Jakobsen J. A population-based epidemiological study on myasthenia gravis in Estonia. J Neurol Neurosurg Psychiat 74:1638-1643 (2003)
Phillips LH et al. The epidemiology of myasthenia gravis in central and western Virginia. Neurology 42:1888-1893, (1992)
Poulas K et al. Epidemiology of seropositive myasthenia gravis in Greece. J Neurol Neurosurg Psychiat. 71(3):352-356 (2001)
Somnier FE, Keiding N, Paulson OB. Epidemiology of myasthenia gravis in Denmark. A longitudinal and comprehensive population survey. Arch Neurol 48:733-739 (1991)

Why do we see more cases of late onset myasthenia gravis?
Demographic changes
Improved recognition of the disease
Immunological diagnosis



Myasthenia gravis in the elderly
Does age influence the presentation of myasthenia gravis at onset?

Late onset myasthenia gravis: Diagnostic problems
Non-ptotic ocular myasthenia gravis Facial ageing Facial weakness and bulbar signs without
extraocular muscle involvement Dysphonia as first symptom of late onset
myasthenia gravis ”Dropped-head sign” Myasthenia gravis presenting as isolated
respiratory failure
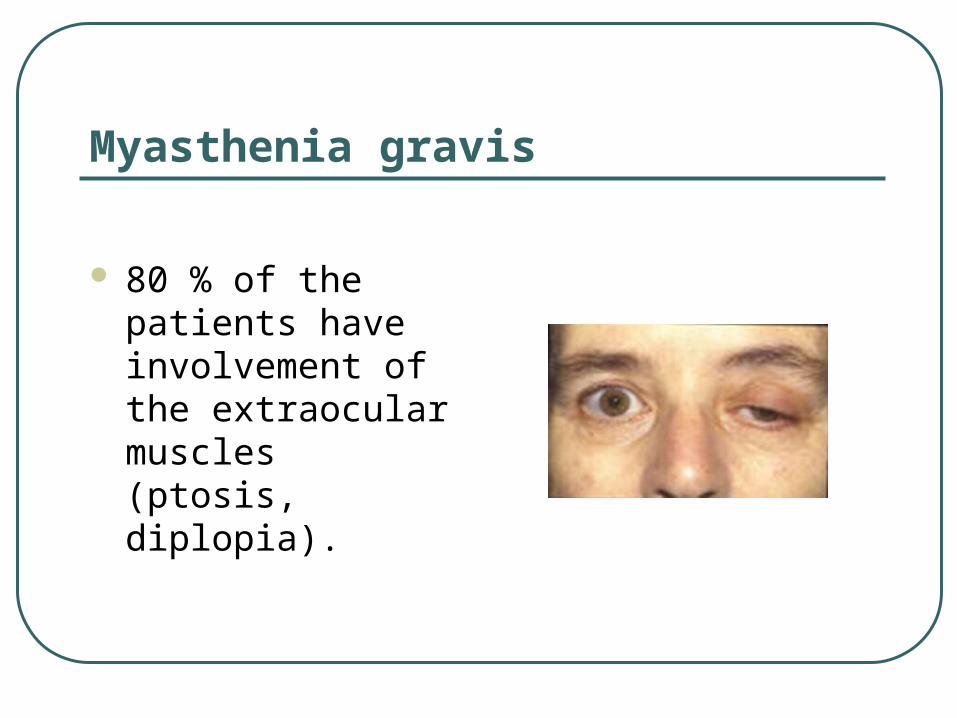
Myasthenia gravis
80 % of the patients have involvement of the extraocular muscles (ptosis, diplopia).
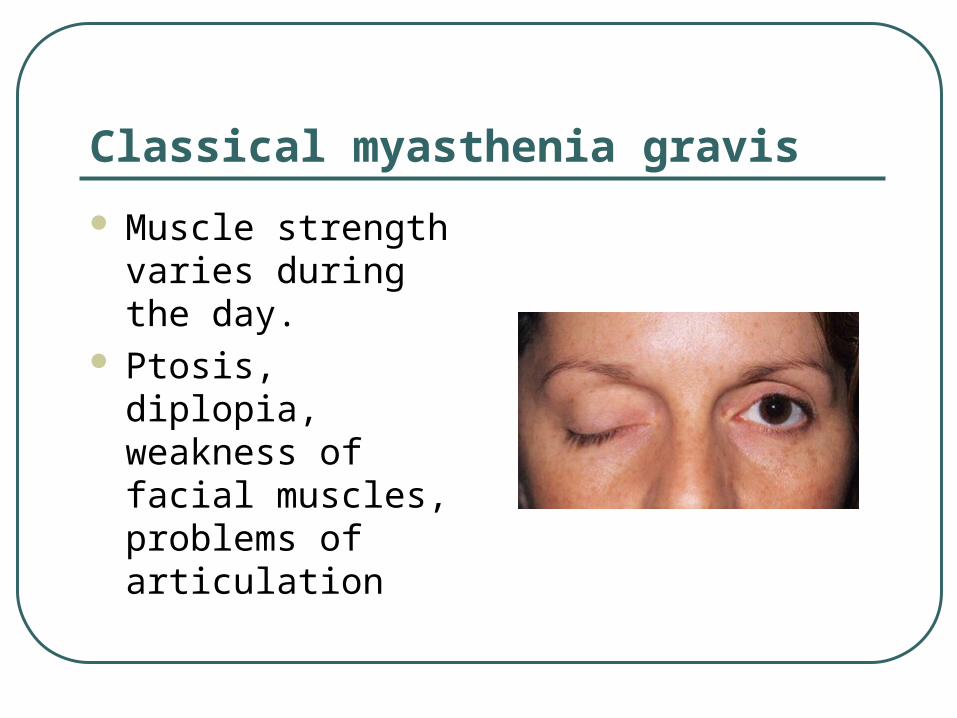
Classical myasthenia gravis
Muscle strength varies during the day.
Ptosis, diplopia, weakness of facial muscles, problems of articulation
Myasthenia gravis
Colavito and co-workers.
Non-ptotic ocular myasthenia gravis: a common presentation of an uncommon disease.
Optometry 2005;76(7), 763-75)
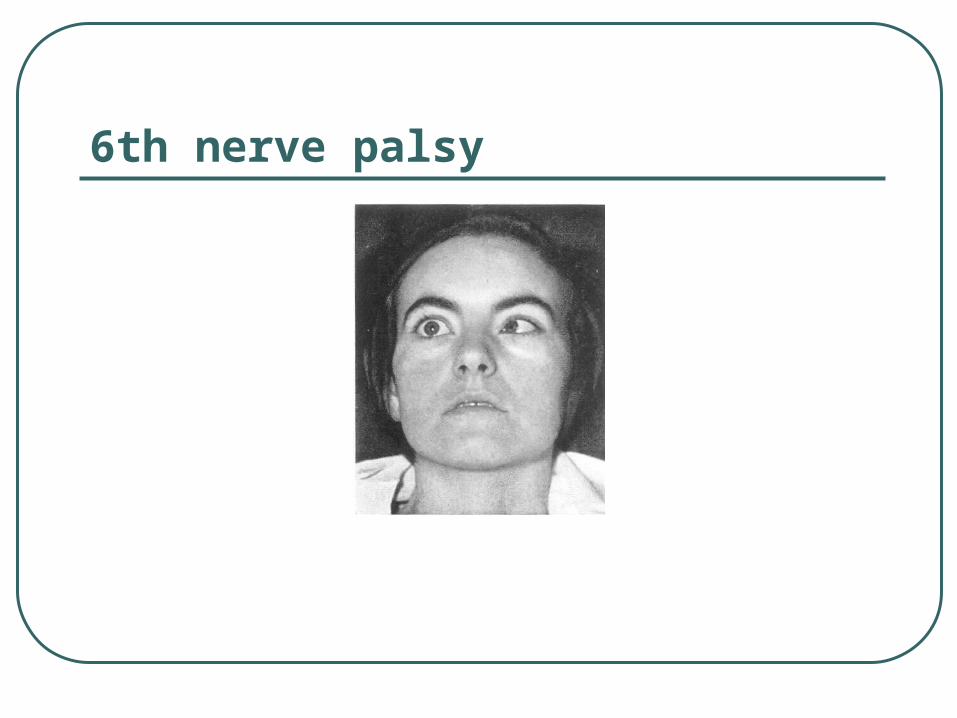
6th nerve palsy
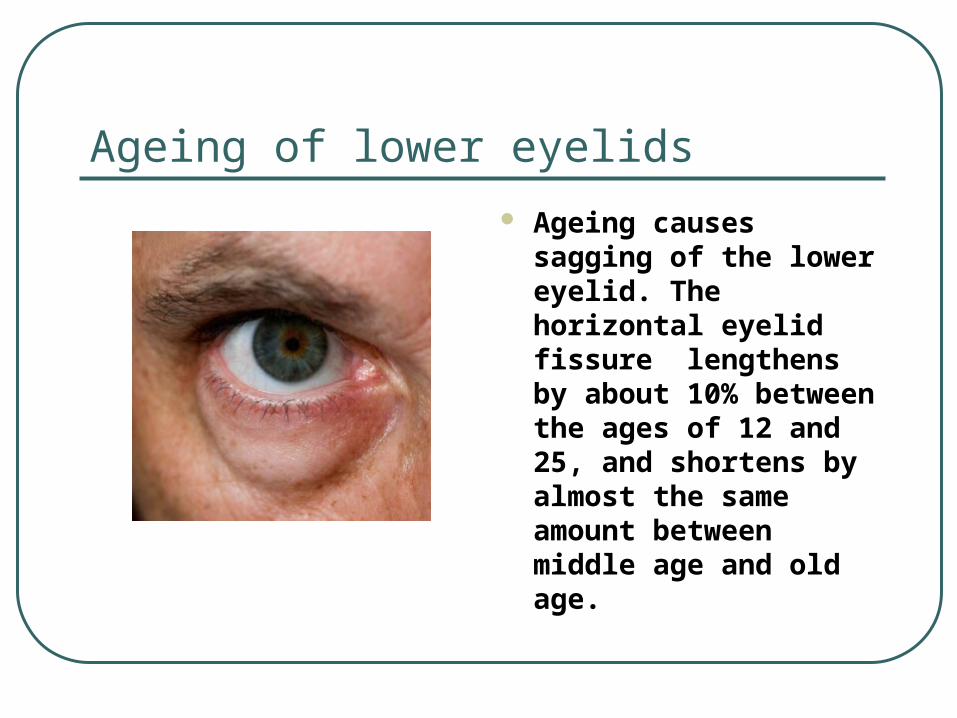
Ageing of lower eyelids
Ageing causes sagging of the lower eyelid. The horizontal eyelid fissure lengthens by about 10% between the ages of 12 and 25, and shortens by almost the same amount between middle age and old age.
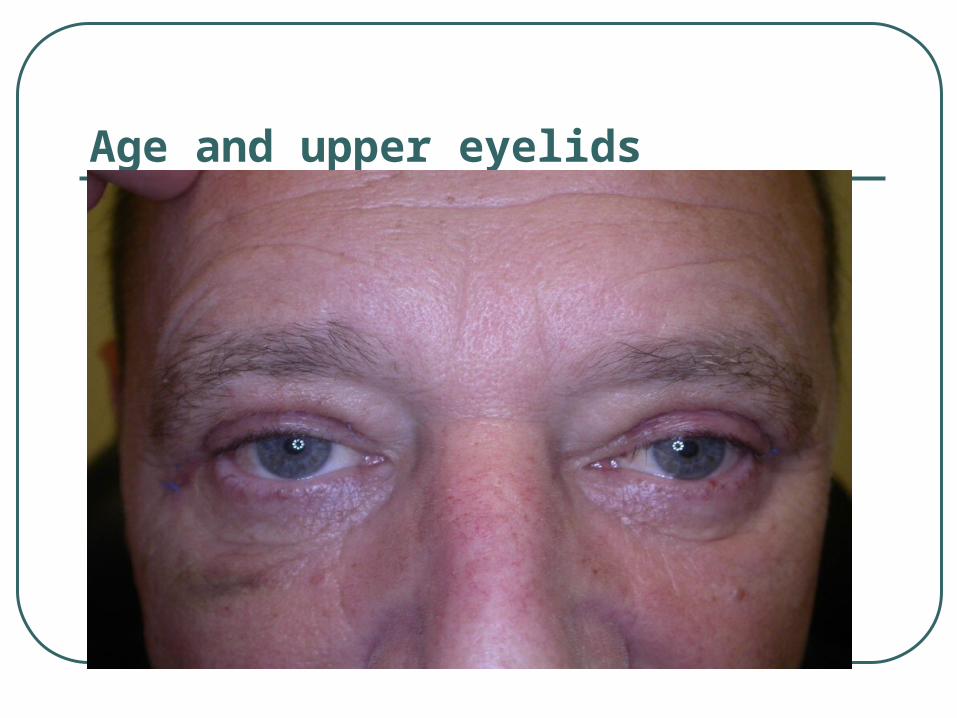
Age and upper eyelids
Facial weakness and bulbar signs without extraocular muscle involvement
Cucurachi L et al: Late onset generalized myasthenia gravis presenting with facial weakness and bulbar signs without extraocular muscle involvement. Neurol. Sci 2009;30:343-344.
Yuki N et al: Facial muscular atrophy in a myasthenia patient. Intern Med 2008;47(14): 1355-1357. (56-year-old man)

Dysphonia as first symptom of late onset myasthenia gravis
Montero-Odasso M: Dysphonia as first symptom of late-onset myasthenia gravis.
J Gen Intern Med 2006;21:C4-6
Mao VH et al: Laryngeal myasthenia gravis: Report of 40 cases.
J Voice 2001:15:122-130
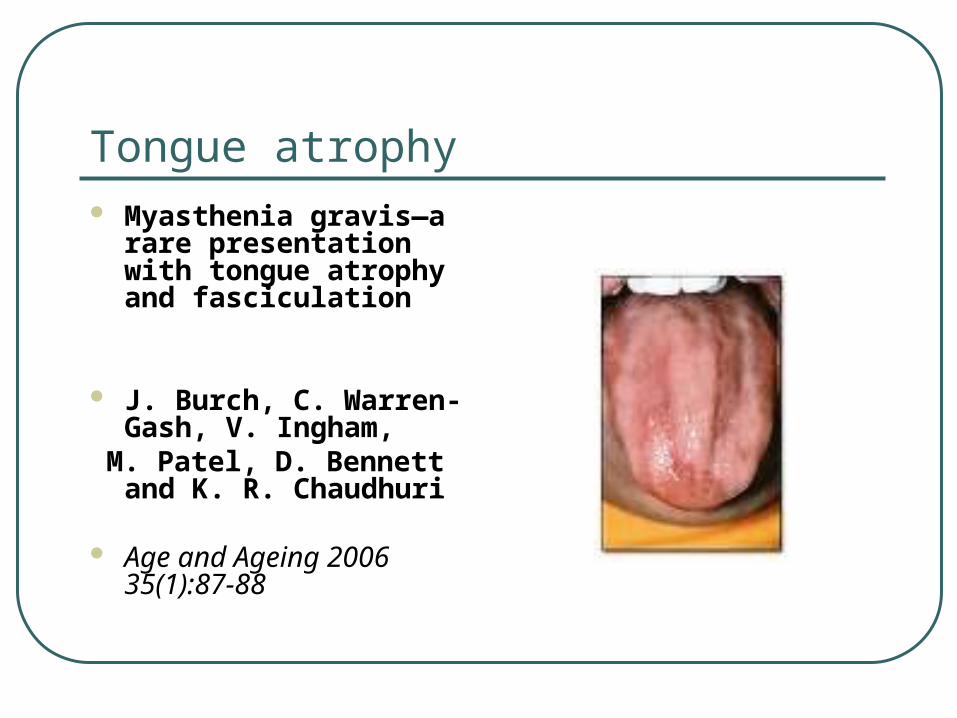
Tongue atrophy Myasthenia gravis—a
rare presentation with tongue atrophy and fasciculation
J. Burch, C. Warren-Gash, V. Ingham,
M. Patel, D. Bennett and K. R. Chaudhuri
Age and Ageing 2006 35(1):87-88

”Dropped head sign” in myasthenia gravis
Puruckherr M et al: The dropped head sign: an unusual presenting feature of myasthenia gravis. Neuromusc Dis 2004;14:378-379.
D’Amelio M et al: Dropped head as an unusual presenting sign of myasthenia gravis. Neurol Sci 2007;28:104-106.

Dropped head sign in late onset myasthenia gravis
Yaguchi H et al: Dropped head sign as the only symptom of myasthenia gravis.
Intern Med 2007;46:743-745
The present case is unique in that dropped head sign was the only symptom throughout the clinical course.

Dropped head sign in myasthenia gravis (Yaguchi et al 2007)
Myasthenia gravis presenting as isolated respiratory
failure
A 61-year-old woman in excellent health and taking no medications presented with progressive dyspnea on exertion.
Nihon Kokyuki Gakkai Zasshi. 1998 Oct;36(10):891-5.

Group 1RyR+ Titin+ AChR+
Group 2RyR- Titin+ AChR+
Group 3RyR- Titin- AChR+
Group 4RyR- Titin- AChR-
n (male/female) 20 (9/11) 32 (15/17) 74 (21/53) 26 (8/18)
Age (years) at first MG symptom 57 (+13) 59 (+20.7) 35 (+18.3) 38 (+18.8)
Time in years from first MG symptoms to MG diagnosis
1.5 (+2) 1.3 (+2.3) 2.1 (+4.2) 1.3 (+3)
Severity at MG onset(MGFA: 1-5)
3 (+1.05) 2.7 (+0.92) 2.2 (+0.85) 2 (+0.80)
n thymectomyn thymoman atrophyn hyperplasia
191450
15654
4621232
5014
AChR ab titer 28.6 (+35.2) 57.3 (+169) 50.5 (+93.5) 0
Titin ab titer 5260 (+6033) 5762 (+7602) 0 0
RyR ab titer 2960 (+3047) 0 0 0

MG symptomsGroup 1RyR+ Titin+ AChR+
Group 2RyR- Titin+ AChR+
Group 3RyR- Titin- AChR+
Group 4RyR- Titin- AChR-
Ptosis 14 / 70% 17 / 53% 38 / 51% 17 / 65%
Diplopia 12 / 60% 11 / 34% 47 / 63% 11 / 42%
Ocular 17 / 85% 22 / 69% 60 / 81% 21 / 81%
Ocular only 1 / 5% 2 / 6% 16 / 22% 8 / 31%
Facial 4 / 20% 4 / 13% 8 / 11% 2 / 8%
Swallowing 14 / 70% 19 / 59% 31 / 42% 5 / 19%
Chewing 11 / 55% 14 / 44% 15 / 20% 4 / 15%
Dysarthria 14 / 70% 17 / 53% 33 / 46% 7 / 27%
Bulbar 18 / 90% 23 / 72% 41 / 55% 12 / 46%
Bulbar only 1 / 5% 0 / 0% 3 / 4% 1 / 4%
Neck 8 / 40% 5 / 16% 8 / 11% 1 / 4%
Respiratory 3 / 15% 5 / 16% 2 / 3% 1 / 4%
Non-limb (ocular, bulbar, neck, or respiratory)
14 / 70% 8 / 25% 31 / 42% 14 / 54%
Limb 6 / 30% 22 / 69% 41 / 55% 12 / 46%
Limb only 0 / 0% 0 / 0% 1 / 1% 2 / 8%

Copyright ©2003 BMJ Publishing Group Ltd.
Vincent, A et al. J Neurol Neurosurg Psychiatry 2003;74:1105-1108
Figure 1 Total numbers of positive acetylcholine receptor (AChR) antibody titres in the UK from 1997 to 1999 inclusive, with data for men and women also shown separately (A); 12 positive results from babies with probable neonatal myasthenia have been omitted. (B) Age and sex
specific incidence of positive AChR antibody in the UK from 1997-99 inclusive.

Thymus in myasthenia gravis
Lymphofollicular hyperplasia with germinal centers
Thymic atrophy
Adipose tissue
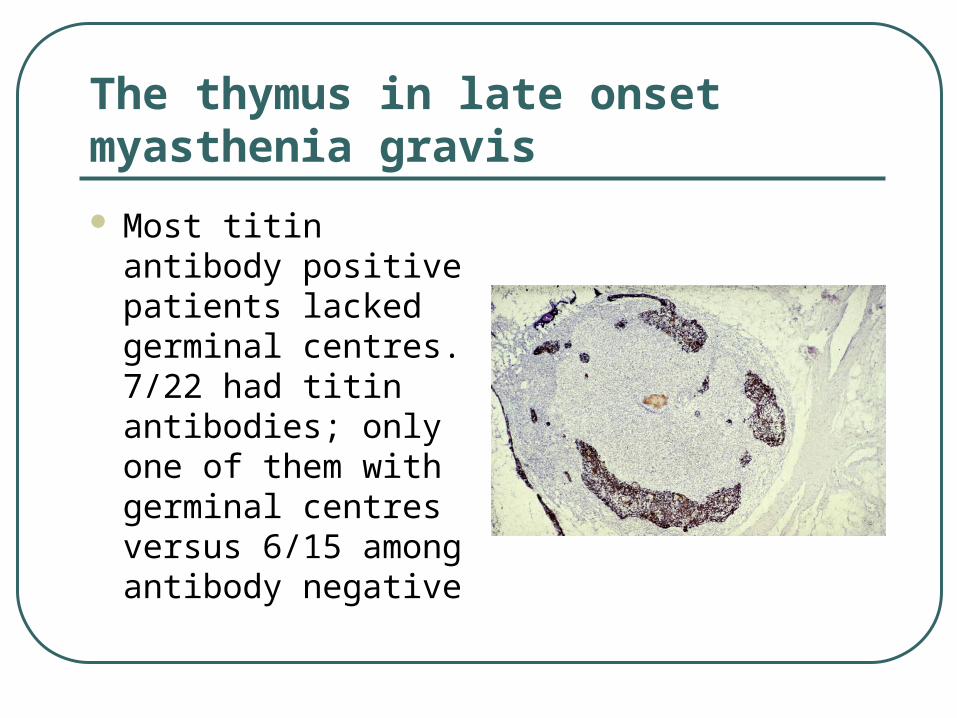
The thymus in late onset myasthenia gravis
Most titin antibody positive patients lacked germinal centres. 7/22 had titin antibodies; only one of them with germinal centres versus 6/15 among antibody negative

Myasthenia gravis in the elderly
Is myasthenia gravis still underdiagnosed?