myasthenia gravis. nmj / endplate chemical synapse presynaptic membrane synaptic cleft ...
TRANSCRIPT
Myasthenia GravisMyasthenia Gravis
Myasthenia GravisMyasthenia Gravis
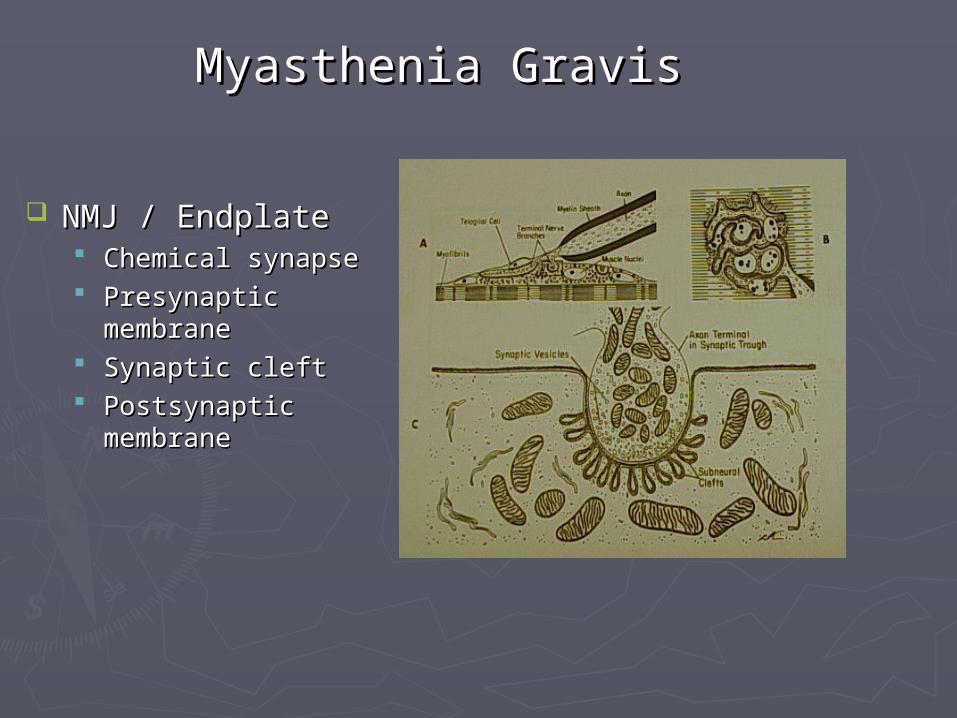
NMJ / EndplateNMJ / Endplate Chemical synapseChemical synapse Presynaptic Presynaptic
membranemembrane Synaptic cleftSynaptic cleft Postsynaptic Postsynaptic
membranemembrane
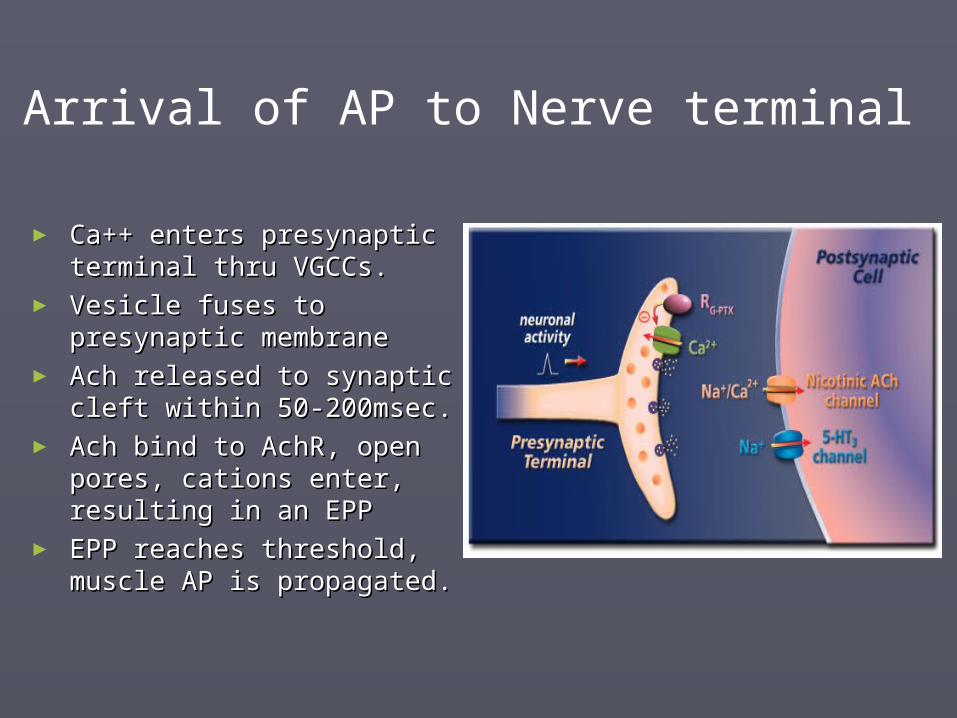
► Ca++ enters presynaptic Ca++ enters presynaptic terminal thru VGCCs.terminal thru VGCCs.
► Vesicle fuses to presynaptic Vesicle fuses to presynaptic membranemembrane
► Ach released to synaptic Ach released to synaptic cleft within 50-200msec.cleft within 50-200msec.
► Ach bind to AchR, open Ach bind to AchR, open pores, cations enter, pores, cations enter, resulting in an EPPresulting in an EPP
► EPP reaches threshold, EPP reaches threshold, muscle AP is propagated.muscle AP is propagated.
Arrival of AP to Nerve terminal
Nicotinic Acetylcholine ReceptorNicotinic Acetylcholine Receptor
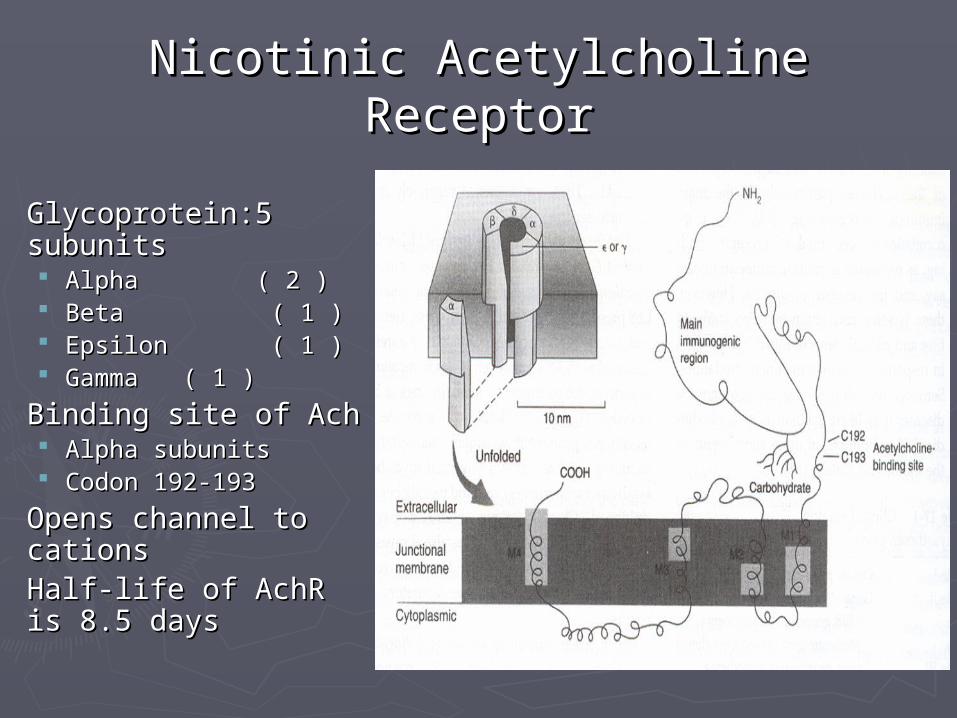
Glycoprotein:5 Glycoprotein:5
subunitssubunits Alpha ( 2 )Alpha ( 2 ) Beta Beta ( 1 ) ( 1 ) Epsilon Epsilon ( 1 ) ( 1 ) GammaGamma ( 1 )( 1 )
Binding site of AchBinding site of Ach Alpha subunitsAlpha subunits Codon 192-193Codon 192-193
Opens channel to Opens channel to cationscations
Half-life of AchR is Half-life of AchR is 8.5 days8.5 days
Myasthenia GravisMyasthenia Gravis
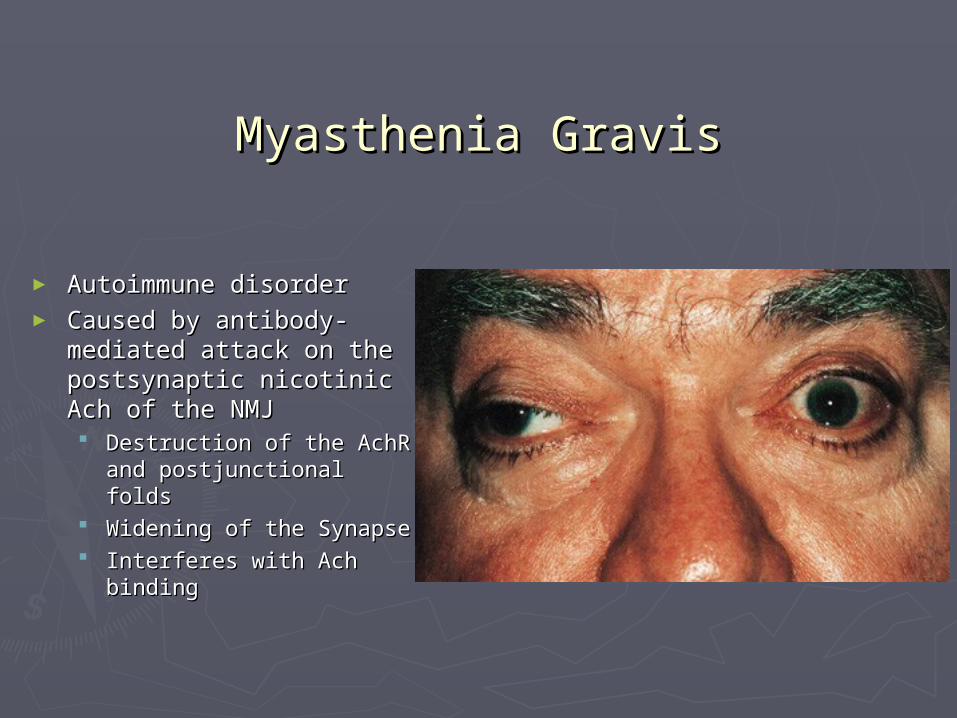
► Autoimmune disorderAutoimmune disorder► Caused by antibody-Caused by antibody-
mediated attack on the mediated attack on the postsynaptic nicotinic postsynaptic nicotinic Ach of the NMJAch of the NMJ Destruction of the AchR Destruction of the AchR
and postjunctional foldsand postjunctional folds Widening of the SynapseWidening of the Synapse Interferes with Ach Interferes with Ach
bindingbinding
Myasthenia GravisMyasthenia Gravis
► Prevalence (US)Prevalence (US) 1/10,000 persons1/10,000 persons
► Annual IncidenceAnnual Incidence 2-5 per year/million2-5 per year/million
► Bimodal incidenceBimodal incidence Younger females 10-40 y/oYounger females 10-40 y/o Older males 50-70 yrsOlder males 50-70 yrs
► GeneticsGenetics Higher freq HLA-B8, DR3Higher freq HLA-B8, DR3
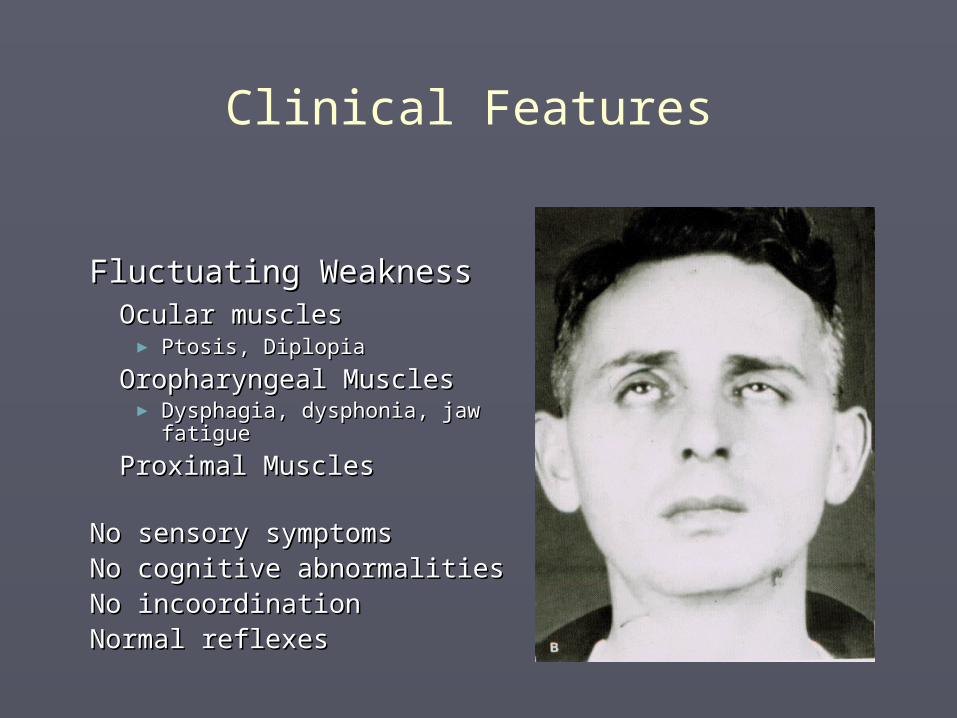
Fluctuating WeaknessFluctuating WeaknessOcular musclesOcular muscles► Ptosis, DiplopiaPtosis, Diplopia
Oropharyngeal MusclesOropharyngeal Muscles► Dysphagia, dysphonia, jaw Dysphagia, dysphonia, jaw
fatiguefatigue
Proximal MusclesProximal Muscles
No sensory symptomsNo sensory symptomsNo cognitive abnormalitiesNo cognitive abnormalitiesNo incoordinationNo incoordinationNormal reflexesNormal reflexes
Clinical Features
PathophysiologyPathophysiology
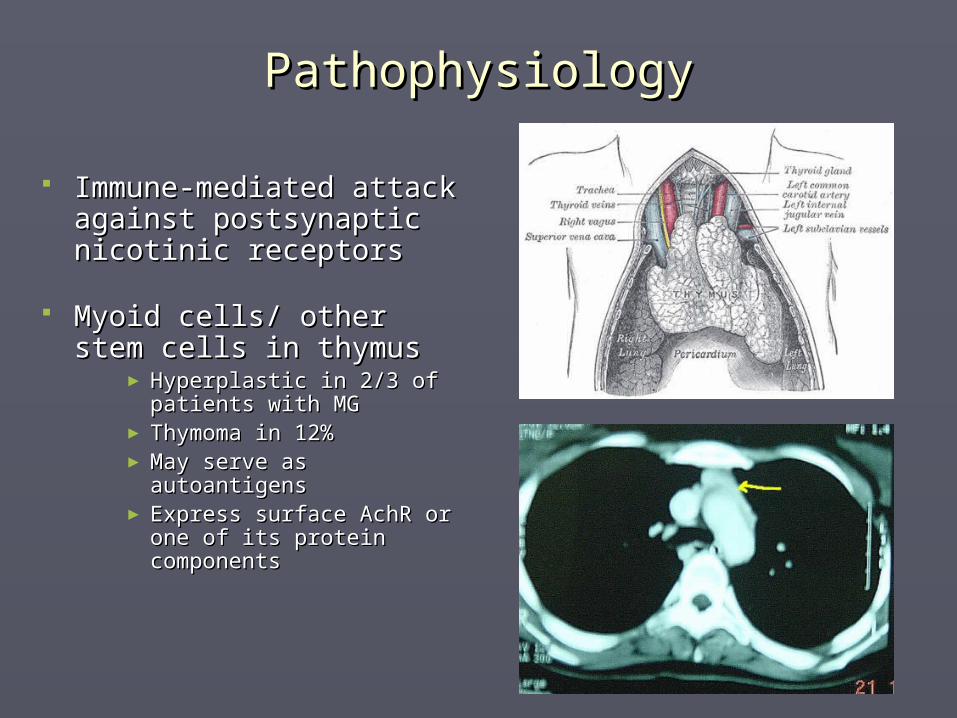
Immune-mediated attack Immune-mediated attack against postsynaptic against postsynaptic nicotinic receptorsnicotinic receptors
Myoid cells/ other stem Myoid cells/ other stem cells in thymuscells in thymus
► Hyperplastic in 2/3 of Hyperplastic in 2/3 of patients with MGpatients with MG
► Thymoma in 12%Thymoma in 12%► May serve as autoantigens May serve as autoantigens ► Express surface AchR or Express surface AchR or
one of its protein one of its protein componentscomponents
MGFA Clinical ClassificationMGFA Clinical Classification
► Grade I: Ocular MGGrade I: Ocular MG Ptosis and diplopiaPtosis and diplopia 15% never spread beyond 15% never spread beyond
ocular areaocular area► Grade II: Mild Grade II: Mild
GeneralizedGeneralized Dysphonia, dysphagia, Dysphonia, dysphagia,
dysarthria, limb weaknessdysarthria, limb weakness IIa extremity; IIb bulbarIIa extremity; IIb bulbar
► Grade III: ModerateGrade III: Moderate IIIa extremity; IIIb bulbarIIIa extremity; IIIb bulbar
► Grade IV: SevereGrade IV: Severe► Grade V: CrisisGrade V: Crisis
Respiratory failureRespiratory failure
Work-upWork-up
History compatible with physical examinationHistory compatible with physical examination Tensilon test ( edrophonium )Tensilon test ( edrophonium )
► Short acting anti-cholinesteraseShort acting anti-cholinesterase► Onset 30 sec, duration 5 minutesOnset 30 sec, duration 5 minutes► Initial 2 mg IV Initial 2 mg IV
Watch for bradycardia, hypotension, arrhythmiasWatch for bradycardia, hypotension, arrhythmias► If no SE give 8 mg IV and observe for improvement. If no SE give 8 mg IV and observe for improvement. ► Give atropine 0.5 to 1 mg IV if with SEGive atropine 0.5 to 1 mg IV if with SE
Ice-pack test for ptosis. 80-90% sensitiveIce-pack test for ptosis. 80-90% sensitive ..
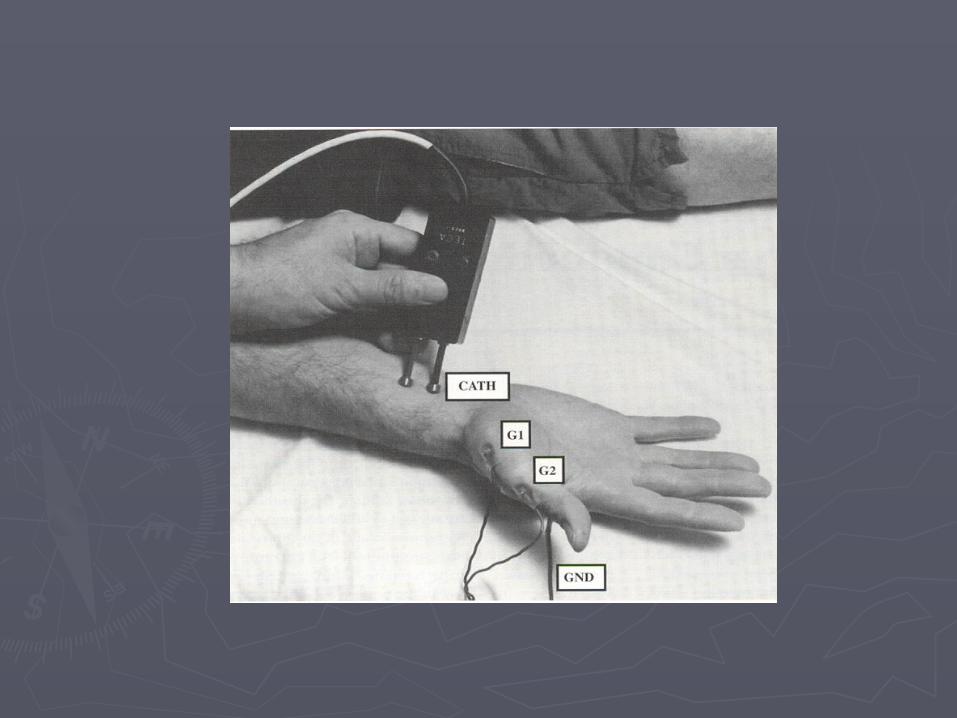
Repetitive nerve stimulation ( Jolly test )Repetitive nerve stimulation ( Jolly test )
► 75% sensitive75% sensitive► May be normal in ocular MG.May be normal in ocular MG.
AchR antibody assayAchR antibody assay► (+) in 80-90% with generalized MG(+) in 80-90% with generalized MG► (+) in 50% of Ocular MG(+) in 50% of Ocular MG► Anti-MuSK ( muscle specific tyrosine kinase )Anti-MuSK ( muscle specific tyrosine kinase )► Titers do not correlate with severity of disease.Titers do not correlate with severity of disease.
Anti-skeletal muscle AB: Anti-skeletal muscle AB: ► +30% gen MG, +85% MG+thymoma+30% gen MG, +85% MG+thymoma
SFEMGSFEMG► Increased jitter Increased jitter
Time variation in NMJ transmissionTime variation in NMJ transmission► (+) in 80% of Ocular, in 100% of generalized MG.(+) in 80% of Ocular, in 100% of generalized MG.► In 9% of MG, this may be the only abnormal Test.In 9% of MG, this may be the only abnormal Test.
Confirmatory Diagnosis
Work-upWork-up
LaboratoryLaboratory ESR, ANA, RFESR, ANA, RF TSH, T4 ( hypo or hyper-T can exacerbate MG )TSH, T4 ( hypo or hyper-T can exacerbate MG ) CBC with diff, UA, Electrolytes, Blood glucose, CBC with diff, UA, Electrolytes, Blood glucose,
Renal profile.Renal profile.
CXR, Chest CTCXR, Chest CT r/o thymoma ( 15% MG )r/o thymoma ( 15% MG ) PPDPPD skin test (if considering immunosuppressive skin test (if considering immunosuppressive
trx)trx)
PFTPFT Medication listMedication list reviewreview
D-penicillamine, interferon-alfa, antibiotics D-penicillamine, interferon-alfa, antibiotics (aminoglycosides), Antiarrhythmics ( quinidine, (aminoglycosides), Antiarrhythmics ( quinidine, procainamide ), Beta-blockers, Ca channel procainamide ), Beta-blockers, Ca channel blockers, Phenytoin, Thyroid hormones, lithium, blockers, Phenytoin, Thyroid hormones, lithium, chlorpromazine, estrogenchlorpromazine, estrogen
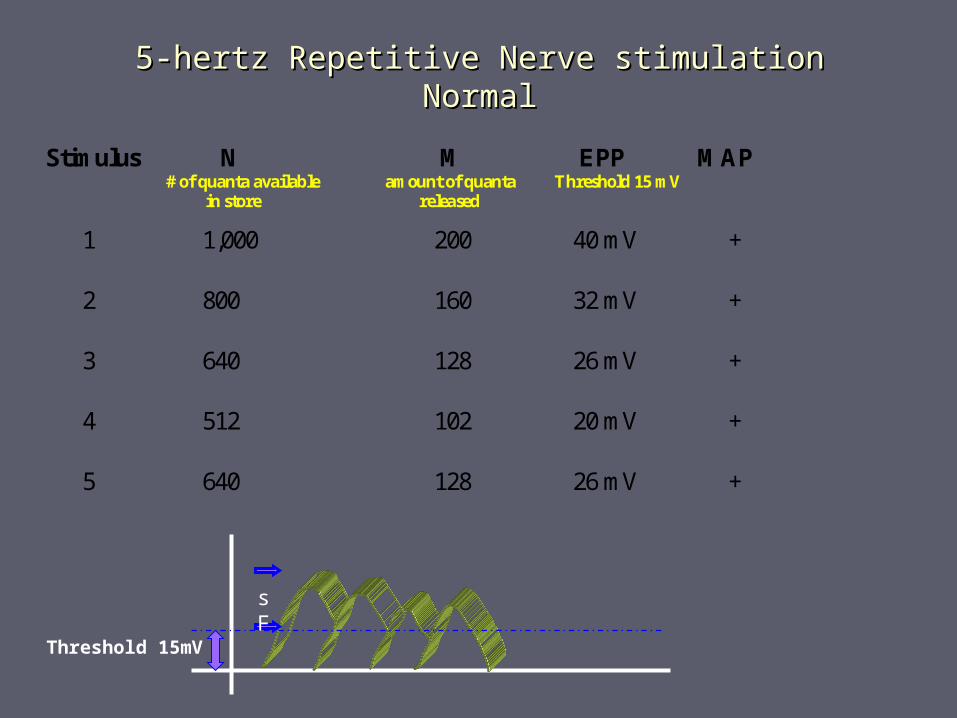
5-hertz Repetitive Nerve stimulation5-hertz Repetitive Nerve stimulationNormalNormal
Stimulus N # of quanta available in store
M amount of quanta released
EPP Threshold 15 mV
MAP
1 1,000 200 40 mV +
2 800 160 32 mV +
3 640 128 26 mV +
4 512 102 20 mV +
5 640 128 26 mV +
sF
Threshold 15mV

5-hertz RNS5-hertz RNSAbnormalAbnormal
Stimulus N M EPP Threshold 15 mV
MAP
1 1000 200 20 mV +
2 800 160 16 mV +
3 640 128 13 mV -
4 512 102 10 mV -
5 640 128 13 mV -
sF
15 mV Threshold
20 mV
16 mV13 mV
10mV

SFEMGSFEMG

SFEMGSFEMG
Management Management
Symptomatic trxSymptomatic trx: : anticholinesteraseanticholinesterase Pyridostigmine Pyridostigmine (Mestinon)(Mestinon)
Onset 30 min. Onset 30 min.
Peak 2 hrs. Lasts 3-6 hrs.Peak 2 hrs. Lasts 3-6 hrs.
Dose: 30-90 mg q 3-6 hrs. Max 120 mg Dose: 30-90 mg q 3-6 hrs. Max 120 mg q3hq3h
IV dose is 1 per 30mg of po dose.IV dose is 1 per 30mg of po dose.
SE:SE: Cholinergic Cholinergic
Diarrhea, N&V, sweating, hypersalivation/ Diarrhea, N&V, sweating, hypersalivation/ secretions, secretions, Miosis, bradycardia, hypotension.Miosis, bradycardia, hypotension.
ImmunotherapyImmunotherapy: Often required : Often required Prednisone: mainstay for MG immunotherapyPrednisone: mainstay for MG immunotherapy
15-20 mg/day, titrate up to 1mg/kg/day15-20 mg/day, titrate up to 1mg/kg/day Azathioprine initiated at 50 mg QD titrated to 2mg/kg/dayAzathioprine initiated at 50 mg QD titrated to 2mg/kg/day (Mycophenolate: 500mg BID titrated to 2-3g/day)(Mycophenolate: 500mg BID titrated to 2-3g/day) Cyclosporine: 5 mg/kg/day with clinical effect in 1-2 mos.Cyclosporine: 5 mg/kg/day with clinical effect in 1-2 mos. TPETPE IVIGIVIG
Surgical treatmentSurgical treatment Thymectomy indicated in thymomatous MGThymectomy indicated in thymomatous MG Non-thymomatous MG: thymectomy is an optionNon-thymomatous MG: thymectomy is an option
Management

Differential DiagnosisDifferential Diagnosis
► Lambert-Eaton Lambert-Eaton Myasthenic syndromeMyasthenic syndrome
► BotulismBotulism► Chronic fatigue Chronic fatigue
syndromesyndrome► Intracranial massIntracranial mass► A diagnosis of MG may A diagnosis of MG may
give clues to other give clues to other maladiesmaladies Hyperthyroidism seen in 3-Hyperthyroidism seen in 3-
8%8% Autoimmune disorders Autoimmune disorders
►SLE, Rheumatoid SLE, Rheumatoid arthritisarthritis

Questions?Questions?
► Sir Charles Bell’s portrait of dying soldier with tetanus. Sir Charles Bell’s portrait of dying soldier with tetanus. ► Opisthotonus and risus sardonicusOpisthotonus and risus sardonicus
► Cholinergic crisisCholinergic crisis Overmedication Overmedication Cholinergic EffectsCholinergic Effects
►MiosisMiosis► Increased salivation Increased salivation
and secretion and secretion ►Diarrhea Diarrhea ►CrampsCramps►FasciculationsFasciculations
►Myasthenic crisisMyasthenic crisis Generalized weaknessGeneralized weakness Respiratory failureRespiratory failure
Cholinergic vs. Myasthenic crisis