mycn protein expression as a predictor of neuroblastoma...
TRANSCRIPT
Vol. 3, 1699-1706, October 1997 Clinical Cancer Research 1699
3 The abbreviations used are: VMA, vanillymandelic acid; HVA. ho-
movanillic acid.
MYCN Protein Expression as a Predictor of Neuroblastoma
Prognosis1
Helen S. L. Chan,2 Brenda L. Gallie,
Gerrit DeBoer, George Haddad, Naohiko Ikegaki,
Jim Dimitroulakos, Herman Yeger, and
Victor Ling
Division of Hematology-Oncology and Immunology, Department of
Pediatrics [H. S. L. C., G. HI, Division of Immunology and Cancer
Research, Research Institute [H. S. L. C.. 0. H., B. L. G.], and
Departments of Ophthalmology and Molecular and Medical Genetics
[B. L. G.] and Pathology [J. D., H. Y.]. The Hospital for SickChildren and University of Toronto, Toronto, Ontario, M5G lX8
Canada; Division of Clinical Trials and Epidemiology, Toronto-
Sunnybrook Regional Cancer Center. Department of Medical
Biophysics, University of Toronto. Toronto, Ontario, M4N 3M5
Canada 1G. Dl: Departments of Pathology and Biochemistry, British
Columbia Cancer Agency, University of British Columbia,
Vancouver, British Columbia, V5Z lL3 Canada IV. LI: and
Department of Pediatrics, University of Pennsylvania School of
Medicine, Philadelphia. Pennsylvania 19104 IN. 1.1
ABSTRACT
About half of nonlocalized neuroblastomas have MYCN
gene amplification and usually progress rapidly, but the half
without such amplification also do poorly, albeit progressingmore slowly. We hypothesize that overexpression of MYCN
protein can occur without gene amplification and that this
expression reliably predicts the prognosis of neuroblastoma.
To determine whether MYCN expression correlated withoutcome, we assayed MYCN protein immunohistochemi-cally in 180 archival pretreatment and posttreatment sam-
ples and stratified the 57 conventionally treated stage IVS,
III, and IV patients by these conventional prognostic fac-tors: stage, age, serum ferritin, Shimada histology, urinary
catecholamine ratio, and MYCN gene status. At a median
Received 3/3/97; revised 6/18/97; accepted 7/2/97.
The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby marked
advertisement in accordance with 18 U.S.C. Section 1734 solely to
indicate this fact.
I Supported by grants from the National Cancer Institute of Canada with
funds provided by the Canadian Cancer Society (to H. S. L. C.. B. L. G..
V. L., and H. Y.), Medical Research Council of Canada (H. S. L. C.,
B. L. G.. and V. L.), USPHS Grant CA-37130 from the NIH (to V. L.),
Sandoz Canada, Inc., the Hospital for Sick Children Pediatric Consult-
ants and Research Institute, Atkinson Charitable Foundation, Elsa U.
Pardee Foundation (H. S. L. C.), and Canadian Genetic Diseases Net-
work, Retinoblastoma Family Association, and Royal Arch Masons of
Canada (B. L. G.). B. L. G. is a distinguished Scientist of the Medical
Research Council of Canada. This work was performed while
H. S. L. C. was a Research Scientist of the National Cancer Institute of
Canada supported by funds from the Canadian Cancer Society.
2 To whom requests for reprints should be addressed, at Division of
Hematology-Oncology, The Hospital for Sick Children. 555 University
Avenue. Toronto, Ontario, M5G lX8 Canada. Phone: (416) 813-5872;
Fax: (416) 8 13-5327; E-mail: [email protected].
follow-up of �6.8 years, we found in patients with known
MYCN gene status that the 23 of 37 without gene amplifica-
tion fared no better than the 14 of 37 with gene amplification
(P = 0.35 and 0.21, comparing relapse-free and survival
rates). Conversely, in patients without MYCN gene amplifi-
cation, 9 of 23 were found to overexpress MYCN protein
pretreatment, and they did worse than the 14 of 23 without
detectable MYCN protein (P = 0.0016 and 0.022, comparingrelapse-free and survival rates). Furthermore, MYCN pro-
tein expression was prognostic without (P = 0.00001 ) and
with (P = 0.0007) stratifying all 57 patients by MYCN gene
status, each conventional prognostic factor (P ranging from
0.00001-0.013), or simultaneously by the two most impor-
tant factors, stage and age (P = 0.00076). We conclude that
overexpression of MYCN protein without gene amplification
correlated significantly with the clinical behavior of neuro-
blastoma and predicted outcome independently of other
prognostic factors. This strongly supports the hypothesis
that expression of the MYCN oncogene is critical for pro-
gression of neuroblastoma.
INTRODUCTION
Neuroblastoma is a major cause of pediatric cancer mor-
tality. Stage and age broadly define prognosis in patients that
require different therapy. Patients of any age with localized
stages I and II generally do well and are curable by surgery.
Young infants with disseminated stage IVS are often cured with
minimal or no therapy, but older children with nonlocalized
stages III and IV do poorly, with a 13-38% cure rate despite
intensive therapy ± bone marrow transplant ( I , 2).
Age is an important conventional prognostic factor (3).
Stage and serum ferritin reflect the tumor load (3), and histol-
ogy, urinary catecholamines VMA3:HVA ratio, serum neuron-
specific enolase, ganglioside GD2, and irk oncogene expression
define the degree of tumor differentiation (3-6). Ploidy; muta-
tions of chromosomes lp, I I, 14, or 17 and neuropeptide Y:
bcl-2 apoptosis-suppressing protein; or nm23 metastasis-related
protein expression may reflect the aggressive potential (7-12).
We and others have observed that P-glycoprotein expression
confers poor prognosis to neuroblastoma (13-16), probably by
promoting broad-spectrum efflux of important cytotoxins from
tumor cells. Other investigators have reported a similar finding
for the putative multidrug resistance protein MRP (16, 17).
Amplification of the MYCN oncogene causing MYCN pro-
tein overexpression occurs in about half of the nonlocalized
neuroblastoma (12, 18). Such tumors usually relapse quickly,
suggesting that the MYCN gene plays an important role in the
progression ofneuroblastoma (12, 18, 19). However, the half of
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1700 MYCN Protein Predicts Neuroblastoma Prognosis
the nonlocalized tumors without such amplification also do
poorly in the long term (15-17). Because we hypothesize that
overexpression of MYCN protein occurring without MYCN
gene amplification might affect prognosis, possibly through the
activation of transcription of genes causing tumor progression,
we asked whether MYCN protein per se relevantly predicts the
clinical behavior of neuroblastoma.
PATIENTS AND METHODS
Patient Selection. We included 80 patients, ages 0.1-
13. 1 years, from the Hospital for Sick Children in Toronto
(1964-1990), in whom � I pretreatment samples were available
for MYCN protein evaluation. We staged the 23 localized
(stages I and II) and 57 nonlocalized tumors (27 stage IV, 21
stage III, and 9 stage IVS) according to the Evans classification
(3) by reviewing the records, radiographs, bone scan, comput-
erized tomography, bone marrow aspirates, and tumor biopsies.
We assessed conventional risk factors including stage, age,
serum ferritin, urinary VMA:HVA ratio, and tumor histology
according to the Shimada classification and determined the
MYCN gene status in the 37 stage IVS, III, and IV cases (47
samples) in which there was enough tumor for Southern blotting
(18). However, analysis of ploidy, chromosome lp, or newer
putative prognostic factors was unavailable in this retrospective
study. We tested the 23 stage I and II tumors (35 pretreatment
samples) in comparison with the 57 stage III, IV, and IVS
tumors (89 of 187 pretreatment samples, 98 of 187 during
therapy; mean, 3 samples/patient; range, 1-9). We grouped
stage IVS with stages III and IV rather than stages I and II,
because some IVS tumors without MYCN gene amplification
also expressed MYCN protein, and these infants progressed
despite intensive therapy, whereas none with stage I/Il tumors
progressed. Thus, stage IVS is probably a heterogeneous group
consisting of misdiagnosed IV as well as true IVS. The IVS
numbers are also so small that including or excluding them has
a minimal effect on the statistical analysis. We excluded patients
with ganglioneuroma, palliative cases, and consultations or re-
ferrals for bone marrow transplant only. We also excluded 35
localized and 76 nonlocalized tumors (3 1 stage IV, 28 stage III,
and 17 stage IVS) particularly from the earlier era, in whom
pretreatment samples were unavailable for testing (biopsies
were too small or were not retrievable from referral hospitals, or
no biopsies had been performed because the radiology, urinary
catecholamines, and/or bone marrow were considered to be
diagnostic for neuroblastoma).
Treatment. All patients were treated with surgery ±
radiation according to their stage and with the conventional
chemotherapy of their era: vincristine with cyclophosphamide
or teniposide (stage IVS), vincristine and cyclophosphamide
with dacarbazine or doxorubicin (stage III); and cyclophospha-
mide, doxorubicin, cisplatin, and teniposide ± bone marrow
transplant (stage IV; Refs. I and 2). The response to chemo-
therapy was judged as favorable if a complete (100%) or very
good partial response (�90%) was observed and as unfavorable
if a partial response (�50%) was observed or if there was
disease progression, and relapse-free and survival rates were
assessed from diagnosis to relapse, death, or last follow-up. On
average, living patients were followed through April 1995.
MYCN Protein Assay. Each sample was stained three
times by a sensitive multilayer immunoperoxidase assay similar
to the one we described previously for P-glycoprotein (15),
using both well-characterized monoclonal anti-MYCN antibod-
ies directed against separate NH, terminus epitopes (NCM II
100 and NCM IX 102; Ref. 20), with IgGl as the isotype-
matched negative control. Specificity was confirmed in selected
cases by blocking antibody-binding with the MYCNIMYCC
fusion protein from which the antibodies were raised (20). This
assay is not quantitative, although we have standardized the
staining against the MYCN protein content quantified by im-
munoblot (21) in negative and positive controls (SK-N-SH line
without MYCN gene amplification, and GOTO, NUB6, NB 1,
NUB32, IMR-32, and NUB7 lines with 39-380 copies of the
MYCN gene). SK-N-SH, in which MYCN protein was undetect-
able by immunoblot, was scored as negative, whereas GOTO,
NUB6, NB1, NUB32, IMR-32, and NUB7, with 18-100%
MYCN protein relative to NUB7, arbitrarily designated as
100%, were scored semiquantitatively as 1 + to S + for MYCN
protein staining (21-23). Three observers masked to sample
identity scored samples containing no MYCN-expressing tumor
cells as negative and designated those with any MYCN-express-
ing cells as 1 + to 5+ by their highest positivity in individual
cells, compared against the negative and positive controls. The
final score of each sample was based on the consensus of
observers or on the majority score, if the interpretation was not
unanimous. Only patients without any positive samples were
called MYCN protein negative, whereas those with � 1 positive
samples were designated MYCN protein positive.
Statistical Analysis. Response rates were compared by
Fisher’s exact test, and actuarial relapse-free and survival rates
were compared by the Kaplan-Meier method (24). To avoid
possible bias by confounding risk factors, each conventional
prognostic factor was inspected for uniformity of distribution in
the nonlocalized MYCN protein-positive and -negative groups,
and these patients were stratified according to each parameter.
Whether each parameter significantly affected outcome was
determined by log-rank analysis, without and with stratification
for the effect of MYCN protein (25). The effect of MYCN
protein was similarly assessed directly by stratifying for each
prognostic factor and simultaneously by stage and age. To avoid
possible selection bias, we evaluated all 133 nonlocalized cases
from 1964-1990, comparing survival rates within each stage for
study versus nonstudy patients in whom pretreatment samples
were not retrievable for testing. All statistical tests used were
two-sided.
RESULTS
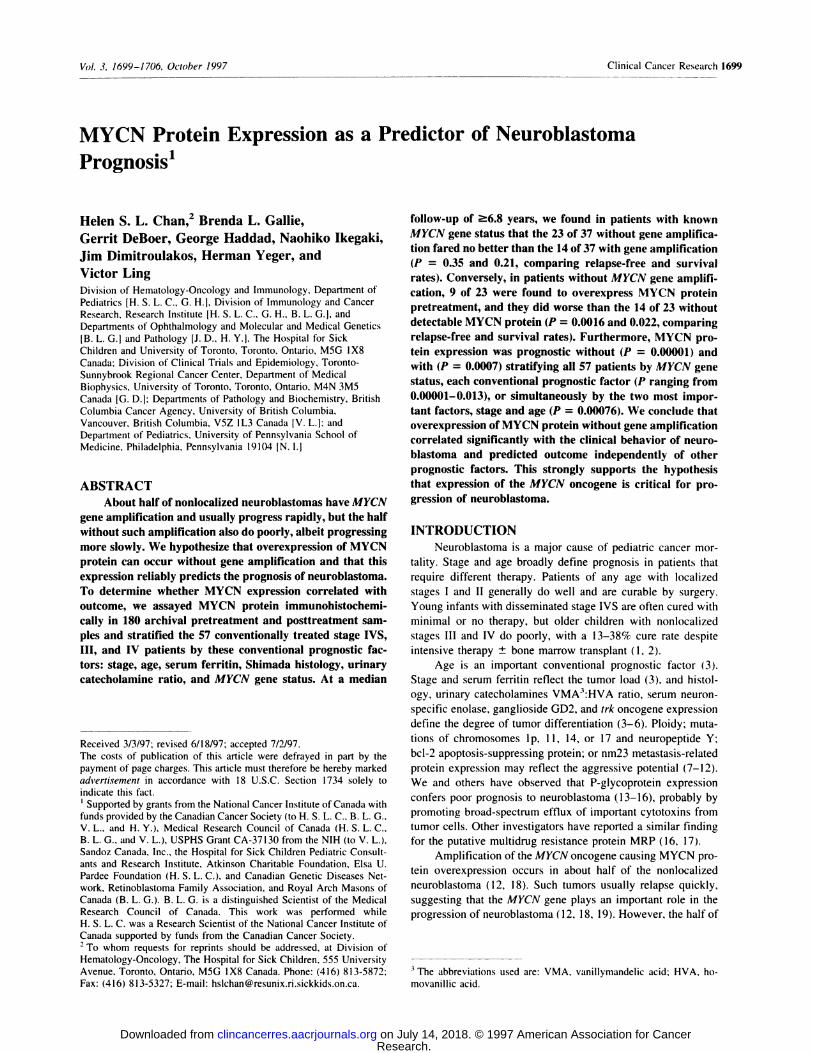
The pattern and levels of MYCN protein showed consid-
erable heterogeneity between different samples that were ob-
tamed from different sites, at the same or different time points
in individual patients, and between different patients (Fig. 1).
We graded samples as I + to 4+ for staining of MYCN protein
in the nuclei of tumor cells, but we found no 5 + samples. In the
35 samples from the 23 localized cases, all of which had
favorable outcome, we found that MYCN protein was rarely
expressed (0 of 2 for stage I, and 1 of 21 for stage II). The
MYCN gene was confirmed to be nonamplified in 14 of these
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
�. �
.‘. 0I
C
Clinical Cancer Research 1701
. , - . -:r � � � �‘ .2 � � I,, ?:�� �
� I � � .� �
... � � � � k #{149}% � �.. �
� “t e� � � �A #{149}#{149}s”
J ��Ii’ ‘:k t� � I,
� , �. *‘�‘ . .;. � ci� .
� � � ‘.‘ 4 �r � !i�
*�a� � � � � � ��A: � �,, 4� 1�.
I ‘� � � � �Y ‘F. ‘. ‘ #{149}� � , � � . �.� 4’, � � � .
. . . ‘ � . -:� #{149}..#{149} �‘ #{163} � ��; c4 � �t “F
l�; � � � C- t1b
�4,’ �t�’ $.� .4
� �. “, � t .� �w�w� � �:: “- ..�. . .:�:�( � ‘4
‘�. “_4� � � �-‘./‘� ,,..�,.
�; ,-, ‘-.4 � � .. .I’ .. . ..-� I �,
� ‘ �A � � �BL�Fig. 1 Multilayer immunoperoxidase staining of the MYCN nucleoprotein in neuroblastoma (hematoxylin counterstain, X I 200). The pattern andlevels of MYCN protein were heterogeneous. A, absence of detectable MYCN protein in a tumor without MYCN gene amplification; B, MYCN proteinlevel that was scored as 4+ in a tumor with 300 copies of the MYCN gene; C, MYCN protein level that was scored as 3 + in a tumor without MYCN
gene amplification.
localized tumors, including the stage II tumor in which MYCN
protein was detectable. In contrast, in the 89 pretreatment sam-
ples from the 57 nonlocalized cases, we found that the MYCN
protein was frequently overexpressed, more so in stages IV (IS
of 27) or III (6 of 21) than in stage IVS (0 of 9). There seemed
to be a higher incidence of MYCN protein expression during
therapy, particularly in stages IV ( 17 of 27) or III (9 of 21)
compared to stage IVS (1 of 9), when taking into account all 187
samples obtained throughout the course of disease. Initially
positive tumors continued to be positive at relapse, but some
tumors in which MYCN protein was undetectable before treat-
ment showed detectable MYCN protein in subsequent biopsies.
All IgG 1 controls were negative. The interobserver agreement in
interpreting whether MYCN expression was positive or negative
was unanimous for 91% of the patients and 69% of the samples.
We observed MYCN protein overexpression relatively fre-
quently, irrespective of whether the MYCN gene was amplified
in a particular tumor. Among the 37 nonlocalized cases in which
there was enough tumor for Southern blotting, we found MYCN
protein overexpression overall (59%; 14 of 20 for stage IV and
8 of 14 for stage III) more often than amplification of the MYCN
gene (38%; 8 of 20 for stage IV and 6 of 14 for stage III); both
occurrences were absent in the 3 stage IVS cases.
In contrast, undetectable MYCN protein expression was
relatively uncommon in the presence of gene amplification.
Among the 14 patients with MYCN gene amplification, we
detected MYCN protein before treatment in all but 3 tumors,
and all but 1 tumor subsequently. Two were stage III (25 and
200 copies of MYCN gene), in which MYCN protein was
undetectable at diagnosis in one sample of each but was ulti-
mately detectable at relapse in one and three samples, respec-
tively; both of these patients died of disease. The third was stage
IV (50 copies of the MYCN gene), in which MYCN protein was
undetectable at diagnosis in one sample; this tumor could not be
retested, because the 7.7-year survivor never relapsed.
Most importantly, MYCN protein overexpression could
still be observed relatively frequently, despite the absence of
MYCN gene amplification in a particular tumor. Among the 23
cases without MYCN gene amplification, we detected MYCN
protein before treatment in 6 tumors (5 of 12 stage IV, 1 of 8
stage III, and 0 of 3 stage IVS tumors) but in a total of 9 tumors
followed throughout the course of disease (7 of 12 stage IV, 2
of 8 stage III, and 0 of 3 stage IVS tumors).
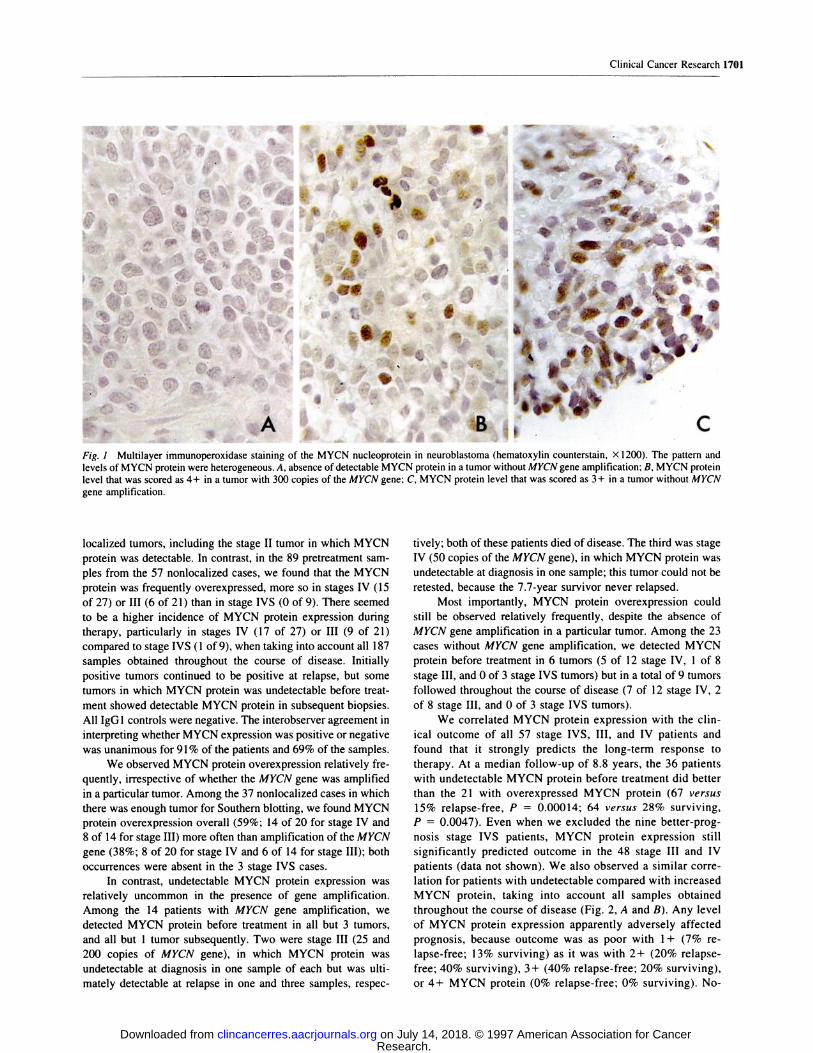
We correlated MYCN protein expression with the din-
ical outcome of all 57 stage IVS, III, and IV patients and
found that it strongly predicts the long-term response to
therapy. At a median follow-up of 8.8 years, the 36 patients
with undetectable MYCN protein before treatment did better
than the 21 with overexpressed MYCN protein (67 versus
15% relapse-free, P = 0.00014; 64 versus 28% surviving,
P = 0.0047). Even when we excluded the nine better-prog-
nosis stage IVS patients, MYCN protein expression still
significantly predicted outcome in the 48 stage III and IV
patients (data not shown). We also observed a similar corre-
lation for patients with undetectable compared with increased
MYCN protein, taking into account all samples obtained
throughout the course of disease (Fig. 2, A and B). Any level
of MYCN protein expression apparently adversely affected
prognosis, because outcome was as poor with 1 + (7% re-
lapse-free; 13% surviving) as it was with 2+ (20% relapse-
free; 40% surviving), 3+ (40% relapse-free; 20% surviving),
or 4+ MYCN protein (0% relapse-free; 0% surviving). No-
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
-0- MYCN protein -
-a- MYCN protein +C
0,0 1.�0.z
� 0.8
�;�E�:1i:�o.o n=27
-0- MYCN protein -
-a- MYCN protein +
n=30 79%
� P 0.00002
‘�t� 0/n=27 �
Yearsa
B
5 l’o �5Years
20 25 301!o 15 20 25 30
A
Fig. 2 Outcome of all 57 stage IV, III, and IVS neuroblastoma patients by MYCN protein expression, taking into account all samples obtainedthroughout the course of disease. Kaplan-Meier curves of relapse-free survival (A) and overall survival (B), showing a significant difference for 27patients with detectable MYCN protein compared with 30 patients with undetectable MYCN protein (P = 0.00001 and 0.00002; median follow-up,8.8 years). Two patients (one from each group) that died without relapse were treated as censored observations; this explains why the relapse-freesurvival was 80%, whereas the overall survival was 79%.
-0- MYCN protein-
‘�‘ -0- MYCN protein +.� 1.0
0
0.z.C.)
C0
aO.42
0.
g 0.2U.
g o.o ________________________________.� 0
� A
0/n=20
n=23
n=17
-0- sIngle-copy MYCN gene
-0-. amplIfied MYCN gene
43%
p = 0.35
24 %n=14
aB
l’o 15Years
25 30
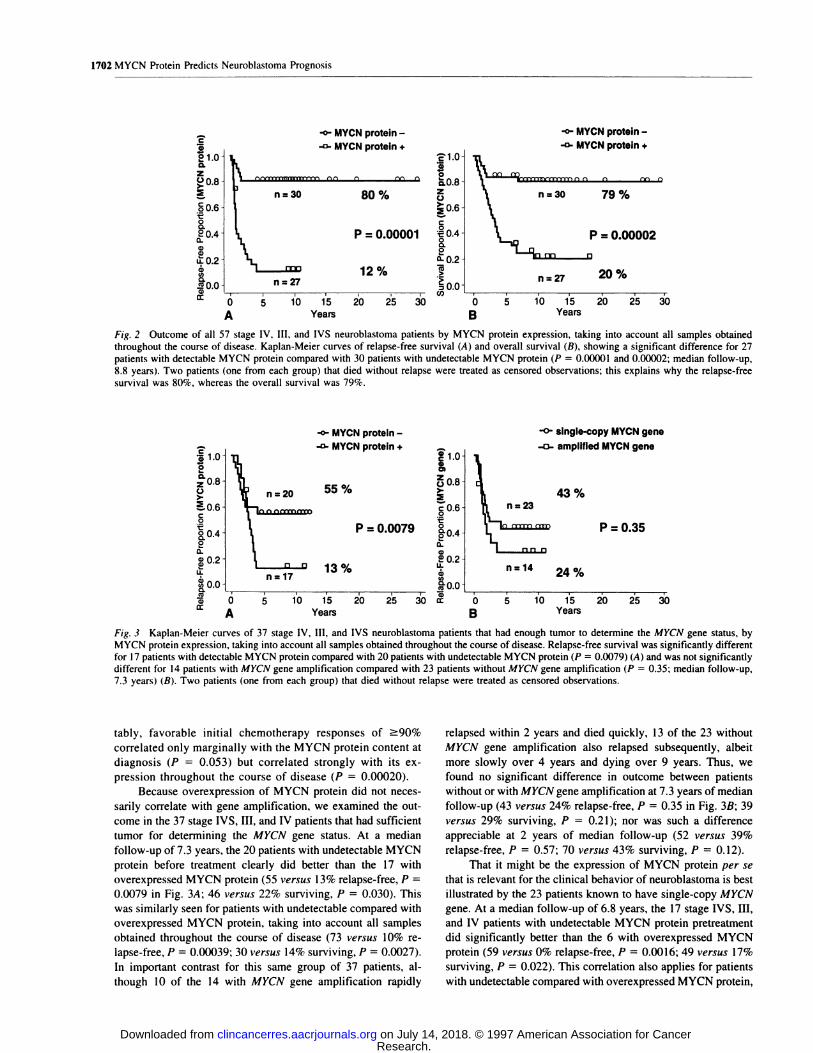
Fig. 3 Kaplan-Meier curves of 37 stage IV, III, and IVS neuroblastoma patients that had enough tumor to determine the MYCN gene status, byMYCN protein expression, taking into account all samples obtained throughout the course of disease. Relapse-free survival was significantly differentfor 17 patients with detectable MYCN protein compared with 20 patients with undetectable MYCN protein (P = 0.0079) (A) and was not significantlydifferent for 14 patients with MYCN gene amplification compared with 23 patients without MYCN gene amplification (P = 0.35; median follow-up,7.3 years) (B). Two patients (one from each group) that died without relapse were treated as censored observations.
1702 MYCN Protein Predicts Neuroblastoma Prognosis
‘E’1.00,0
one, ZS,�J,0 0
>.
p = 0.00001 �
Q. 0.2
12%�
Cl,
g 0.6
P = 0.0079 §0.4
� 0.213%
110 1’5 20 25 30Years
tably, favorable initial chemotherapy responses of �90%
correlated only marginally with the MYCN protein content at
diagnosis (P = 0.053) but correlated strongly with its ex-
pression throughout the course of disease (P 0.00020).
Because overexpression of MYCN protein did not neces-
sarily correlate with gene amplification, we examined the out-
come in the 37 stage IVS, III, and IV patients that had sufficient
tumor for determining the MYCN gene status. At a median
follow-up of 7.3 years, the 20 patients with undetectable MYCN
protein before treatment clearly did better than the 17 with
overexpressed MYCN protein (55 versus 13% relapse-free, P
0.0079 in Fig. 3A; 46 versus 22% surviving, P = 0.030). This
was similarly seen for patients with undetectable compared with
overexpressed MYCN protein, taking into account all samples
obtained throughout the course of disease (73 versus 10% re-
lapse-free, P = 0.00039; 30 versus 14% surviving, P 0.0027).
In important contrast for this same group of 37 patients, al-
though 10 of the 14 with MYCN gene amplification rapidly
relapsed within 2 years and died quickly, 13 of the 23 without
MYCN gene amplification also relapsed subsequently, albeit
more slowly over 4 years and dying over 9 years. Thus, we
found no significant difference in outcome between patients
without or with MYCN gene amplification at 7.3 years of median
follow-up (43 versus 24% relapse-free, P = 0.35 in Fig. 3B; 39
versus 29% surviving, P 0.21); nor was such a difference
appreciable at 2 years of median follow-up (52 versus 39%
relapse-free, P = 0.57; 70 versus 43% surviving, P = 0.12).
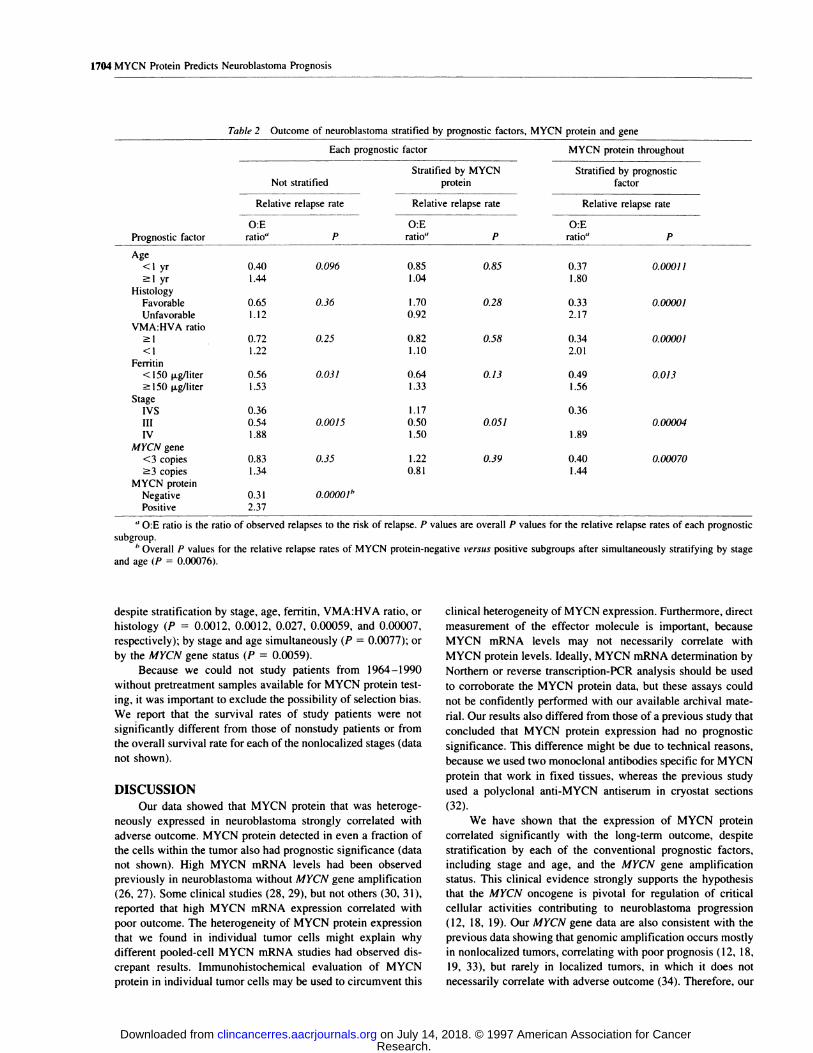
That it might be the expression of MYCN protein per se
that is relevant for the clinical behavior of neuroblastoma is best
illustrated by the 23 patients known to have single-copy MYCN
gene. At a median follow-up of 6.8 years, the 17 stage IVS, III,
and IV patients with undetectable MYCN protein pretreatment
did significantly better than the 6 with overexpressed MYCN
protein (59 versus 0% relapse-free, P = 0.0016; 49 versus 17%
surviving, P = 0.022). This correlation also applies for patients
with undetectable compared with overexpressed MYCN protein,
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

-0- MYCN protein -
-0- MYCN protein +
71 %
p =0.00067
0%
n=14
n=9
�E’
F.o0.
� 0.8>.�‘�‘0.60
.#{128}0�04 .
�:a�
,�0.2
d�
‘�‘1.o
:��0.8zC.)�0.6
C#{149}�04�.
8.2
o..O.2.�
>
�.ooc� �
�a ‘ i� 0 5
A
#{149}E00�1� (/) #{149} .
25 30 0 5
B
I � �
10 15 20
Years
, � .
10 15 20 25 30Years
-0- MYCN protein -
-0. MYCN protein +
67 %
p =0.011
0%n=9
Fig. 4 Outcome of 23 stage IV, III, and IVS neuroblastoma patients known to be without MYCN gene amplification, by MYCN protein expression,taking into account all samples obtained throughout the course of disease. Kaplan-Meier curves of relapse-free survival (A) and overall survival (B).
showing a significant difference for 14 patients with detectable MYCN protein compared with 9 patients with undetectable MYCN protein (P -
0.00067 and 0.01 1 ; median follow-up, 6.8 years). One patient in the MYCN protein-negative group that died without relapse was treated as a censoredobservation; this explains why the relapse-free survival was 71%, whereas the overall survival was 67%.
Clinical Cancer Research 1703
taking into account all samples obtained throughout the course
of disease (Fig. 4, A and B).
Because conventional factors prognostic of neuroblas-
toma outcome were not uniformly distributed relative to the
expression of MYCN protein, it was important to stratify
them by log-rank analysis (Table 1). We found that stage and
ferritin significantly correlated with relapse, but histology
and VMA:HVA ratio did not, whereas age was of borderline
significance (Table 2). However, the significance of age and
ferritin was lost after stratifying for the effect of MYCN
protein, and the effect of stage became borderline. Similarly,
although stage, age, and ferritin significantly affected mor-
tality (P = 0.0050, 0.024, and 0.011, respectively) but his-
tology and VMA:HVA ratio did not (P = 0.47 and 0.19,
respectively), the significance of stage and age was lost after
stratifying for the effect of MYCN protein (P = 0.19 and
0.65, respectively), and the significance of ferritin became
borderline (P = 0.068). Tables 1 and 2 show the data for
MYCN protein expression during the course of disease; the
pretreatment expression of MYCN protein had a similarly
significant impact on prognosis. For example, the relapse rate
was higher for patients with detectable rather than undetect-
able pretreatment MYCN protein (P = 0.00014), despite
stratifying by age, stage, histology, or VMA:HVA ratio (P
0.0062, 0.0065, 0.00036, and 0.0034, respectively) but not by
ferritin (P = 0. 16), suggesting that overexpression of MYCN
protein might be inherent rather than acquired with treatment
and relapse.
Because amplification of the MYCN gene, an acknowl-
edged unfavorable factor, was not uniformly distributed relative
to MYCN protein expression during the course of disease, we
stratified it by log-rank analysis (Table 1). At a median fol-
low-up of 7.3 years, the prognosis was apparently not much
better without than with MYCN gene amplification, either before
(P = 0.35, 0.21) or after stratification of the comparisons of
relapse and mortality rates by the effect of MYCN protein (P =
0.39 and 1.00) or by the other conventional prognostic factors
(nonsignificant P values not shown). In contrast, the expression
Table I Neurobla stoma by prognostic factors and status of MYCNprotein or MYCN gene
MYCN proteindetectable throughout
the course of disease
No. of patients with +
known prognosticPrognostic factor factor No. % No. %
Age 57<lyr 16 53 5 19
�lyr l4 47 22 81
Histology 57
Favorable 12 40 2 7
Unfavorable I 8 60 25 93
VMA:HVA ratio 52�l 12 48 7 26
<1 13 52 20 74
Ferritin 39<150 p.g/liter 10 56 6 29
�l50 p.g/liter 8 44 15 71
Stage 57IVS 8 27 1 4
III 12 40 9 33
IV 10 33 17 63
MYCN gene 37
<3 copies 14 93 9 4/�3 copies I 7 13 59
MYCN protein 57Negative 30 100
Positive 27 100
of MYCN protein significantly correlated with the relapse rate,
both without and with stratification by each of the conventional
risk factors (Table 2). This correlation similarly applied for the
prognostic impact of pretreatment or posttreatment MYCN pro-
tein expression that had been stratified by the MYCN gene status
(P = 0.021 and 0.0007). Likewise, MYCN protein expression
remained prognostic when stratified simultaneously for stage
and age (P = 0.00076). Furthermore, the expression of MYCN
protein significantly affected the mortality rate (P = 0.00002)
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
1704 MYCN Protein Predicts Neuroblastoma Prognosis
Table 2 Outcome of neuroblastoma stratified by prognostic factors, M YCN protein and gene
Each prognostic factor MYCN protein throughout
Stratified by MYCNNot stratified protein
Stratified by prognosticfactor
Relative relapse rate Relative relapse rate Relative relapse rate
O:E O:E O:E
Prognostic factor ratio” P ratio” P ratio” P
Age<I yr�l yr
0.40 0.096 0.85 0.85
1.44 1.040.37 0.00011
1.80Histology
Favorable 0.65 0.36 1 .70 0.28 0.33 0.00001
Unfavorable 1. 12 0.92 2.17VMA:HVA ratio
�l 0.72 0.25 0.82 0.58 0.34 0.00001
<I 1.22 1.10 2.01
Femtin<150 xg/liter�l50 p.g/liter
0.56 0.031 0.64 0.13
1.53 1.330.49 0.013
1.56Stage
IVS 0.36 1.17 0.36
III 0.54 0.0015 0.50 0.051 0.00004
IV 1.88 1.50 1.89
MYCN gene<3 copies
�3 copies
0.83 0.35 1.22 0.39
1 .34 0.8 1
0.40 0.00070
1.44MYCN protein
Negative
Positive0.31 0.00001”
2.37
a O:E ratio is the ratio of observed relapses to the risk of relapse. P values are overall P values for the relative relapse rates of each prognostic
subgroup.
I, Overall P values for the relative relapse rates of MYCN protein-negative versus positive subgroups after simultaneously stratifying by stageand age (P = 0.00076).
despite stratification by stage, age, ferritin, VMA:HVA ratio, or
histology (P 0.0012, 0.0012, 0.027, 0.00059, and 0.00007,
respectively); by stage and age simultaneously (P 0.0077); or
by the MYCN gene status (P = 0.0059).
Because we could not study patients from 1964-1990
without pretreatment samples available for MYCN protein test-
ing, it was important to exclude the possibility of selection bias.
We report that the survival rates of study patients were not
significantly different from those of nonstudy patients or from
the overall survival rate for each of the nonlocalized stages (data
not shown).
DISCUSSION
Our data showed that MYCN protein that was heteroge-
neously expressed in neuroblastoma strongly correlated with
adverse outcome. MYCN protein detected in even a fraction of
the cells within the tumor also had prognostic significance (data
not shown). High MYCN mRNA levels had been observed
previously in neuroblastoma without MYCN gene amplification
(26, 27). Some clinical studies (28, 29), but not others (30, 31),
reported that high MYCN mRNA expression correlated with
poor outcome. The heterogeneity of MYCN protein expression
that we found in individual tumor cells might explain why
different pooled-cell MYCN mRNA studies had observed dis-
crepant results. Immunohistochemical evaluation of MYCN
protein in individual tumor cells may be used to circumvent this
clinical heterogeneity of MYCN expression. Furthermore, direct
measurement of the effector molecule is important, because
MYCN mRNA levels may not necessarily correlate with
MYCN protein levels. Ideally, MYCN mRNA determination by
Northern or reverse transcription-PCR analysis should be used
to corroborate the MYCN protein data, but these assays could
not be confidently performed with our available archival mate-
rial. Our results also differed from those of a previous study that
concluded that MYCN protein expression had no prognostic
significance. This difference might be due to technical reasons,
because we used two monoclonal antibodies specific for MYCN
protein that work in fixed tissues, whereas the previous study
used a polyclonal anti-MYCN antiserum in cryostat sections
(32).
We have shown that the expression of MYCN protein
correlated significantly with the long-term outcome, despite
stratification by each of the conventional prognostic factors,
including stage and age, and the MYCN gene amplification
status. This clinical evidence strongly supports the hypothesis
that the MYCN oncogene is pivotal for regulation of critical
cellular activities contributing to neuroblastoma progression
(12, 18, 19). Our MYCN gene data are also consistent with the
previous data showing that genomic amplification occurs mostly
in nonlocalized tumors, correlating with poor prognosis (1 2, 18,
19, 33), but rarely in localized tumors, in which it does not
necessarily correlate with adverse outcome (34). Therefore, our
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 1705
data in fact corroborate rather than dispute the acknowledged
unfavorable impact of MYCN gene amplification in nonlocal-
ized neuroblastoma, besides offering a possible explanation for
the traditional observation that many nonamplified tumors also
ultimately fail therapy. Because the survival rates of study
patients did not differ significantly from those of nonstudy
patients or from the overall survival rate for each stage, the
MYCN findings in the cohort of patients that we have studied
are unlikely to be due to selection bias. However, because our
patient population is relatively small and has been treated over
a number of years, our observations require confirmation in a
larger number of prospectively studied patients in whom the
newer prognostic markers are available.
The amplified MYCN gene most likely acts through overex-
pression of MYCN protein. However, gene amplification is only
one way by which protein expression can be enhanced. We have
found, in stages III, IV, and IVS but rarely in stages I and II, that
MYCN protein overexpression can occur without gene amplifica-
tion (26% initially, 39% overall). Detectable MYCN protein reli-
ably predicted an unfavorable outcome in such nonlocalized tu-
mors, whereas the undetectable protein correlated with good
prognosis. Therefore, despite our small numbers of nonamplified
tumors, they best demonstrate that overexpression of MYCN pro-
tein per se is apparently sufficient for adversely affecting outcome.
This clinical finding is also inconsistent with the possibility that
some unknown genes or coamplified genes, rather than the MYCN
gene, are critical for progression of neuroblastoma.
This retrospective study does not allow further investigation
into the basis for MYCN protein overexpression in the absence of
gene amplification. However, a previous investigator has found
high MYCN mRNA levels associated with a long half-life MYCN
protein in a rapidly proliferating tumorigenic line established from
a progressive but nonamplified neuroblastoma (35). Another inves-
tigator has found high MYCN mRNA levels with increased protein
in two nonamplified tumorigenic lines, both of which proliferated
slower than MYCN gene-amplified lines (36). It remains to be
defined whether the expression of MYCN protein without gene
amplification is regulated at the transcriptional. translational, or
posttranslational level.
The 60-63-kDa MYCN nucleoprotein is essential during
embryogenesis (37). It subsequently becomes undetectable ex-
dept in neuroblastoma, retinoblastoma, Wilms tumor, and small-
cell lung or brain tumors (12, 18, 19), particularly the more
primitive tumors (29, 38). The MYC family proteins are tran-
scriptional regulators that play a pivotal role in regulating cel-
lular proliferation, differentiation, and apoptosis (39, 40). MYC
proteins interact with Max, another helix-loop-helix leucine
zipper protein, forming sequence-specific DNA-binding corn-
plexes that regulate the transcription of genes controlling the
cell cycle (40) and competing with alternative Max partners
Mad and Mxil to regulate differentiation (41-43). Because the
choice to undergo proliferation or differentiation may depend on
the level of MYCN expression, a more aggressive phenotype in
neuroblastoma might be conferred if the threshold of MYCN
protein-mediated transcription-regulatory activity is reached,
whether or not this is due to gene amplification. MYCN protein
might also mediate the transcription of genes that regulate the
response to chemotherapy. We have reported that P-glycopro-
tein expression correlated with poor prognosis, more primitive
disease, more advanced stages, and metastasis rather than the
primary neuroblastoma (15). Some studies of P-glycoprotein
mRNA (13, 14, 16), but not all (17, 29, 38), have agreed with
our findings; other studies of MRP mRNA have reported a
similar prognostic association (16, 17). Both P-glycoprotein and
MRP frequently coexpress with MYCN in neuroblastoma ( IS-
17, 29, 38), but it is unknown whether they affect prognosis
independently. If they do, this might suggest that each is integral
to malignant progression. Therefore, defining whether the ex-
pression of MYCN and drug resistance are regulated/coregu-
lated by humoral factors, cellular factors, cytokines, and biolog-
ical response modifiers or expressed/coexpressed with other
oncogenes, tumor suppressor genes, or flanking coamplified
genes might ultimately suggest a more effective therapy for this
highly fatal tumor.
ACKNOWLEDGMENTS
We acknowledge the contributions of Drs. H. Kahn. P. S. Thorner,
and S. S. Weitzman in reviewing the slides and patients and A. E. Evans
in reviewing the manuscript.
REFERENCES
1. Bowman. L. C.. Hancock, M. L., Santana, V. M., Hayes, F. A.. Kun.
L., Parham, D. M., Furman, W. L., Rao, B. N.. Green, A. A., and Crist,W. M. Impact of intensified therapy on clinical outcome in infants and
children with neuroblastoma: the St. Jude Children’s Research Hospital
experience, 1962 to 1988. J. Clin. Oncol., 9: 1599-1608, 1991.
2. Matthay. K. K.. O’Leary, M. C., Ramsay. N. K.. Villablanca. J..Reynolds. C. P.. Atkinson, J. B., Haase. G. M.. Stram. D. 0.. and Seeger.
R. C. Role of myeloablative therapy in improved outcome for high-riskneuroblastoma: review of recent Children’s Cancer Group results. Eur.
J. Cancer. 31A: 572-575. 1995.
3. Evans, A. E.. D’Angio. G. J.. Propert. K.. Anderson, J., and Hann,
H. W. Prognostic factors in neuroblastoma. Cancer (Phila.), 59: 1853-
1859, 1987.
4. Zeltzer, P. M., Marangos, P. J., Parma, A. M., Sather, H.. Dalton, A.,Hammond, D., Siegel, S. E., and Seeger, R. C. Raised neuron-specificenolase in serum of children with metastatic neuroblastoma: a report
from the Children’s Cancer Study Group. Lancet, 2: 361-363, 1983.
5. Ladisch, S., Wu, Z. L., Feig, S., Ulsh, L., Schwartz. E., Floutsis, G..
Wiley. F., Lenarsky, C., and Seeger, R. Shedding of GD2 ganglioside by
human neuroblastoma. Int. J. Cancer, 39: 73-76. 1987.
6. Nakagawara. A., Arima-Nakagawara. M., Scavarda, N. J.. Azar.
C. G.. Cantor. A. B., and Brodeur, G. M. Association between highlevels of expression of the TRK gene and favorable outcome in human
neuroblastoma. N. EngI. J. Med., 328: 847-854, 1993.
7. Look, A. T., Hayes, F. A.. Nitschke, R.. McWilliams. N. B., andGreen, A. A. Cellular DNA content as a predictor of response tochemotherapy in infants with unresectable neuroblastoma. N. EngI.J. Med., 311: 231-235, 1984.
8. Kogner, P., Bjork, 0., and Theodorsson, E. Neuropeptide Y in
neuroblastoma: increased concentration in metastasis, release during
surgery, and characterization of plasma and tumor extracts. Med. Pedi-
atr.Oncol., 21: 317-322, 1993.
9. Leone, A., Seeger. R. C.. Hong, C. M., Hu, Y. Y.. Arlxleda, M. J..Brodeur, 0. M., Stram, D.. Slamon, D. J., and Steeg, P. S. Evidence fornm23 RNA overexpression, DNA amplification, and mutation in ag-
gressive childhood neuroblastomas. Oncogene. 8: 855-865, 1993.
10. Caron. H. Allelic loss ofchromosome I and additional chromosome17 material are both unfavourable prognostic markers in neuroblastoma.Med. Pediatr. Oncol., 24: 2 15-22 1 , 1995.
1 1 . Krajewski, S., Chatten, J.. Hanada. M.. and Reed. J. C. Immuno-histochemical analysis of the Bcl-2 oncoprotein in human neuroblasto-
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
1706 MYCN Protein Predicts Neuroblastoma Prognosis
mas: comparisons with tumor cell differentiation and N-Myc protein.
Lab. Invest.. 72: 42-54. 1995.
12. Brodeur, G. M. Genetics of embryonal tumours of childhood:
retinoblastoma, Wilms’ tumour, and neuroblastoma. Cancer Surv., 25:
67-99. 1995.
13. Bourhis. J.. B#{233}nard.J.. Hartmann, 0.. Boccon-Gibod, L., Lemerle,J., and Riou. G. Correlation of MDRJ gene expression with chemother-apy in neuroblastoma. J. NatI. Cancer Inst., 81: 1401-1405, 1989.
14. Goldstein, L. J., Fojo, A. T., Ueda, K., Crist, W., Green, A..Brodeur, G., Pastan, I.. and Gottesman, M. M. Expression of themultidrug resistance MDRI gene in neuroblastomas. J. Clin. Oncol., 8:
128-136. 1990.
15. Chan, H. S. L., Haddad. G., Thorner, P. S., DeBoer, G., Lin, Y. P.,Ondrusek, N., Yeger. H.. and Ling, V. P-glycoprotein expression as apredictor of the outcome of therapy for neuroblastoma. N. Engl. J. Med.,325: 1608-1614, 1991.
16. Norris. M. D., Bordow, S. B., Haber, P. S., Marshall. G. M.,Stewart. B. W., and Haber, M. The MDRI gene predicts for outcome insubsets of patients with primary neuroblastoma. Proc. Am. Assoc.
Cancer Res.. 37: 313. 1996.
17. Norris, M. D.. Bordow, S. B., Marshall, G. M., Haber, P. S., Cohn,S. L.. and Haber, M. Expression of the gene for multidrug-resistance-associated protein and outcome in patients with neuroblastoma. N. EngI.J. Med., 334: 231-238, 1996.
18. Seeger, R. C., Brodeur. G. M., Sather, H., Dalton, A., Siegel, S. E.,Wong. K. Y., and Hammond, D. Association of multiple copies of theN-invc oncogene with rapid progression of neuroblastomas. N. EngI.
J. Med., 313: 1111-1116, 1985.
19. Christiansen. H.. Sahin, K., Berthold, F., Hero, B., Terpe. H-J., andLampert. F. Comparison of DNA aneuploidy, chromosome I abnormal-
ities, MYCN amplification. and CD44 expression as prognostic factors inneuroblastoma. Eur. J. Cancer, 3/A: 541-544, 1995.
20. Ikegaki, N., and Kennels, R. H. Molecular genetic characterization
of epitope-specific monoclonal antibodies against the myc family pro-
teins. Oncogene. 5: 397-403, 1990.
21 . Dimitroulakos, J., Squire, J., Pawlin, G.. and Yeger, H. NUB-7: astable I-type human neuroblastoma cell line inducible along N- andS-type cell lineages. Cell Growth Differ., 5: 373-384, 1994.
22. Biedler, J. L., Roffler-Tarlov, S., Schachner, M., and Freedman,L. S. Multiple neurotransmitter synthesis by human neuroblastoma celllines and clones. Cancer Res., 38: 3751-3757, 1978.
23. Seeger, R. C., Danon, Y. L.. Rayner, S. A., and Hoover. F. Defi-nition of a Thy-l determinant on human neuroblastoma, glioma. sar-
coma, and teratoma cells with a monoclonal antibody. J. Immunol., 128:
983-989, 1982.
24. Kaplan, E. L., and Meier, P. Nonparametric estimation from incom-plete observations. J. Am. Stat. Assoc., 53: 457-481, 1958.
25. Peto, R., Pike, M. C., Armitage, P., Breslow, N. E., Cox, D. R.,Howard, S. V., Mantel, N., McPherson, K., Peto, J., and Smith, P. G.
Design and analysis of randomized clinical trials requiring prolonged
observation of each patient. II. Analysis and examples. Br. J. Cancer,
35: 1-39, 1977.
26. Kohl, N. E., Gee, C. E., and Alt, F. W. Activated expression of theN-,nvc gene in human neuroblastomas and related tumors. Science(Washington DC). 226: 1335-1337, 1984.
27. Schwab, M., Ellison, J., Busch, M., Rosenau, W., Varmus, H. E., andBishop. J. M. Enhanced expression of the human gene N-myc consequentto amplification of DNA may contribute to malignant progression of neu-roblastoma. Proc. Nail. Acad. Sci. USA, 81: 4940-4944, 1984.
28. Rosen, N., Reynolds. C. P.. Thiele, C. J.. Biedler, J. L., and Israel,M. A. Increased N-mvc expression following progressive growth ofhuman neuroblastoma. Cancer Res., 46: 4139-4142, 1986.
29. Nakagawara, A., Kadomatsu, K., Sato, S., Kohno, K., Takano, H.,Akazawa, K., Nose, Y., and Kuwano, M. Inverse correlation betweenexpression of multidrug resistance gene and N-rnvc oncogene in humanneuroblastomas. Cancer Res., 50: 3043-3047, 1990.
30. Nisen, P. D., Waber, P. G., Rich, M. A., Pierce, S., Garvin, J. R., Jr.,Gilbert, F., and Lanzkowsky, P. N-mvc oncogene RNA expression inneuroblastoma. J. Natl. Cancer Inst., 80: 1633-1637, 1988.
31 . Slavc, I., Ellenbogen, R., Jung, W. H.. Vawter, 0. F., Kretschmar,
C., Grier, H., and Korf, B. R. myc gene amplification and expression in
primary human neuroblastoma. Cancer Res., 50: 1459-1463, 1990.
32. Seeger. R. C.. Wada, R., Brodeur, G. M., Moss, T. J., Bjork, R. L.,Sousa, L., and Slamon, D. J. Expression of N-mvc by neuroblastomaswith one or multiple copies of the oncogene. In: A. E. Evans, G. J.D’Angio, A. G. Knudson, and R. C. Seeger (eds.), Advances in Neu-roblastoma Research 2, Vol. 271, pp. 41-49. New York: Alan R. Liss,
Inc., 1988.
33. Bourhis, J., Dominici, C.. McDowell, H., Raschella, G., Wilson, G..
Castello, M. A.. Plouvier, E., Lemerle, J., Riou, G., and Benard, J.
N-mvc genomic content and DNA ploidy in stage IVS neuroblastoma.
J. Clin. Oncol., 9: 1371-1375, 1991.
34. Cohn, S. L., Look, A. T., Joshi, V. V., Holbrook, T., Salwen, H.,Chagnovich, D., Chesler, L., Rowe, S. T., Valentine, M. B., Komuro,H.. Castleberry, R. P., Bowman, L. C., Rao, P. V., Seeger. R. C., andBrodeur, G. M. Lack of correlation of N-,nyc gene amplification withprognosis in localized neuroblastoma: a Pediatric Oncology Group
study. Cancer Res., 55: 721-726, 1995.
35. Cohn, S. L.. Salwen, H., Quasney, M. W., Ikegaki. N., Cowan,J. M., Herst. C. V., Kennett, R. H., Rosen, S. T., DiGiuseppe, J. A.,and Brodeur, G. M. Prolonged N-myc protein half-life in a neuro-blastoma cell line lacking N-myc amplification. Oncogene, 5: 182 1-
1827, 1990.
36. Wada, R. K., Seeger, R. C., Brodeur, G. M., Einhom, P. A., Rayner.S. A., Tomayko. M. M., and Reynolds, C. P. Human neuroblastoma celllines that express N-myc without gene amplification. Cancer (Phila.),
72: 3346-3354, 1993.
37. Stanton, B. R., Perkins, A. S., Tessarollo, L., Sassoon, D. A., andParada, L. F. Loss of N-myc function results in embryonic lethality and
failure of the epithelial component of the embryo to develop. GenesDcv., 6: 2235-2247. 1992.
38. Bates, S. E., Shieh, C. Y., and Tsokos, M. Expression of mdr-1IP-glycoprotein in human neuroblastoma. Am. J. Pathol., 139: 305-315,
1991.
39. Blackwood, E. M., and Eisenman, R. N. Max: a helix-loop-helixzipper protein that forms a sequence-specific DNA-binding complexwith Myc. Science (Washington DC), 251: 1211-1217, 1991.
40. Amati, B., Littlewood, T. D., Evan, G. I., and Land, H. The c-Mycprotein induces cell cycle progression and apoptosis through dimeriza-
tion with Max. EMBO J., 12: 5083-5087, 1993.
41. Zervos, A. S., Gyuris, J., and Brent, R. Mxil, a protein thatspecifically interacts with Max to bind Myc-Max recognition sites. Cell,72: 223-232, 1993.
42. Raschella, G., Romeo, A., Negroni, A., Pucci, S., Dominici, C.,
Castello, M. A., Bevilacqua, P., Felsani, A., and Calabretta, B. Lack ofcorrelation between N-myc and MAX expression in neuroblastoma
tumors and in cell lines: implication for N-myc-MAX complex forma-tion. Cancer Res., 54: 2251-2255, 1994.
43. Chin, L., Schreiber-Agus, N.. Pellicer, I., Chen, K., Lee, H. W.,Dudast. M., Cordon-Cardo, C., and DePinho, R. A. Contrasting roles for
Myc and Mad proteins in cellular growth and differentiation. Proc. NatI.Acad. Sci. USA, 92: 8488-8492, 1995.
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1997;3:1699-1706. Clin Cancer Res H S Chan, B L Gallie, G DeBoer, et al. prognosis.MYCN protein expression as a predictor of neuroblastoma
Updated version
http://clincancerres.aacrjournals.org/content/3/10/1699
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/3/10/1699To request permission to re-use all or part of this article, use this link
Research. on July 14, 2018. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from