myhat home visit checklist home visit checklist cycle: 1 forms version: 6/21/2016 (unless marked...
TRANSCRIPT

MYHAT Home Visit Checklist CYCLE: 1 FORMS VERSION: 6/21/2016 (unless marked below)
Consents Informed Consent (8/1/2017) HIPAA (8/1/2017)
Forms 1. Consent Log2. Demo & Contact Part I (10/17/2016)3. Subjective Memory Part I4. Hearing & Vision5. MMSE & Mungas Correction6. Blood Pressure Part I
For those with < 21 on MMSE, STOP HERE. Provide BP sheet to participant.
7. Demo & Contact Part II8. WTAR9. Subjective Memory Part II10. ADL & IADL Functional Abilities11. IADL-Interviewer12. STOFHLA – Health Literacy (5/5/2017)13. HandednessNeuropsychological Tests14. Order of NP Test Administration (9/9/2016)15. NP Summary Form (9/9/2016)
a. Fuld (bags)b. Face Namec. Digit Spand. Trail Making Testse. Clock Drawingf. Modified Token Testg. Logical Memoryh. Benton Visual Form Discriminationi. Block Designj. Boston Namingk. Verbal Fluency
16. Judgment Questions17. Health, History & Lifestyle (10/17/2016)18. Florida Cognitive Activities Scale (FCAS)19. Physical Activity Assessment (Paffenbarger) (10/17/2016)20. Physical & Neurological Exam (8/23/2016)21. Medications22. mCES-D23. Health Services Utilization24. Social Support25. Pet Form26. Sports-Related Head Trauma27. Caffeine Form28. Social Norms29. Brain Scan Interest30. Medical Record Request31. CDR – Interviewer32. Overall Impression (11/21/2016)33. Blood Draw Form
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____ Interviewer: ____ ____
Page 1 of 1 MYHAT Consent Log: Cycle 1
6/21/2016 MYHAT CONSENT LOG: BASELINE
Cycle: 1 1. List anyone who was present besides the interviewer and the participant: _________________________________ ________ 2. Risks were presented? Specify: _________________________________________________________ _____________________________________________________________________________________ ________ 3. Significant issues of concern were discussed? Specify: ______________________________________ _____________________________________________________________________________________ ________ 4. All questions were answered to the satisfaction of the participant? Specify: ____________________ _____________________________________________________________________________________ ________ 5. Research activities began only after obtaining consent? Specify: _____________________________ _____________________________________________________________________________________ ____ ____ / ____ ____ / 2 0 ____ ____ 6. Date of obtaining initial consent ____ ____ : ____ ____ ____ ____ 7. Time of consent (signature) (AM or PM) ________ 8. Where did the assessment take place? ________ 9. Consented to option #1: audiotaping of cognitive test? Specify: ______________________________ _____________________________________________________________________________________ ________ 10. Consented to option #2: fasting blood draw for standard and research blood tests? Specify:______ _____________________________________________________________________________________ ________ 11. Consented to option #3: genetic tests: Specify: ___________________________________________ _____________________________________________________________________________________ ________ 12. Consented to HIPAA (permit use and disclosure of medical records)? Specify: _________________ _____________________________________________________________________________________ ________ 13. Additional comments? ______________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ ________ 14. Was this a split visit? If yes, be sure to complete the split visit form

Date: ____ ____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Demographic and Contact Info Part I: Cycle 1
10/17/2016 MYHAT DEMOGRAPHIC AND CONTACT INFORMATION: PART I
Cycle: 1 1. This is how we have your name: ____________________________________________.
Is that how you would like to be addressed (in letters, etc.)?
2. Please tell me your date of birth: ____ _____ / ____ ____ / ____ ____ ____ ____
3. We have your address as (read from recruitment status form):
______________________________________________ (Apt #)
______________________________________________
(City) (State) (Zip code) ________ Is that correct? Write ANY corrected information below (please make sure it’s legible and accurate). ____________________________________________ (Apt #) ____________________________________________ (City) (State) (Zip code) 4. What is the best telephone number to reach you? (area code first) ____ ____ ____ - ____ ____ ____ - ____ ____ ____ ____ 4a. Alternate phone number ____ ____ ____ - ____ ____ ____ - ____ ____ ____ ____ 5. With whom could we leave a message for you if we couldn’t reach you? Name: _____________________________________ Relationship: ___________________________________ ________ 5a. Does this person have the same address and phone number? Address if different: _______________________________________________ (Apt #)
________________________________________________
(City) (State) (Zip code)
Phone if different: ____ ____ ____ - ____ ____ ____ - ____ ____ ____ ____
Date: ____ ____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Demographic and Contact Info Part I: Cycle 1
________ 6. Sex ________ 7. Race – Do you identify with one of the following? ________ 8. Do you identify as Hispanic or Latino(a)? ________ 9. How many years of education did you complete? ________ 10. Highest level of education completed in years: ________ 11. If high school not completed or received GED, what was the highest grade completed? ________ 12. Did you participate in or complete a formal program in a trade or technical/vocational training
which leads to official credentials/certifications? Specify training: ______________________________
12a. If yes, how many years or months of this training did you complete?
________ Years
________ Months
13. Where were you born? City: ___________________________________________ State/Province: __________________________________ Country (if not USA): ______________________________ 14. Where did you live when you started school as a child? City: ___________________________________________ State/Province: __________________________________ Country (if not USA): ______________________________ 15. Where did you live when you finished going to school (high school or less)? City: ___________________________________________ State/Province: __________________________________
Country (if not USA): _____________________________
________ 16. INTERVIEWER’S IMPRESSION: DO YOU FEEL THAT THE INFORMATION IN THIS SECTION IS RELIABLE?
17. INTERVIEWER: Any comments? ________________________________________________________
_____________________________________________________________________________________
____________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 1 MYHAT Subjective Memory: Part I
6/21/2016 MYHAT SUBJECTIVE MEMORY: PART I
Cycle: 1 Now I’d like to ask you a few questions about your memory. PPT INF [PPT = Participant; INF = Informant] _____ _____ 1. In general, how good do you feel your memory is for a person your age? _____ _____ 2. Do you feel you remember things less well than you did a year ago? 2a (PPT). What are you having trouble remembering? ________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ 2a (INF). What are you having trouble remembering? ________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____ _____ 2b. Do you feel your memory got worse suddenly or gradually? specify (PPT): __________________________________________________________ ________________________________________________________________________
specify (INF): ___________________________________________________________ ________________________________________________________________________
_____ _____ 2c. Is this a consistent problem? i.e. do you have it pretty much most of the time?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 1 MYHAT Vision & Hearing: Cycle 1
6/21/2016 MYHAT VISION AND HEARING
Cycle: 1 Now I would like to ask you some questions about how well you can see and hear. ________ 1. Do you currently wear eyeglasses or contact lenses? ________ 2. Do you wear your glasses or contact lenses all of the time? 3. Do you wear them for …
________ a. Reading/close work
________ b. Driving
________ c. Watching television
________ d. Other, specify: ______________________________________________________________________
________ e. “Distance”
Visual Acuity: Assess with the small Snellen chart ________ 4a. Can you read the top line? 4b. Acuity test: 20 / ______ Right 20 / ______ Left ________ 5. Have you ever worn a hearing aid? ________ 5a. If yes, Which ear? ________ 7. Can you hear well enough to carry on a conversation in a quiet room? ________ 8. Can you hear well enough to use the phone? ________ 9. Hearing loss assessed with rubbing fingers: ________ 10. INTERVIEWER: Source of information: ________ 11. INTERVIEWER’S IMPRESSION: Do you think that the information given on vision and hearing is mostly
accurate? ________ 12. INTERVIEWER’S IMPRESSION: Any comments?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT MMSE: Cycle 1
6/21/2016 MYHAT MINI-MENTAL STATE EXAMINATION
Cycle: 1 Now I would like to ask you some questions to check your memory and concentration. Some of them may be easy and some of them may be hard. Write in verbatim responses
Can you tell me today’s date? Response: _______________________________________________________ Orientation to Time ______/1 1. What is the year? ______/1 2. What is the season of the year? ______/1 3. What is the date? ______/1 4. What is the day of the week? ______/1 5. What is the month? Orientation to Place ______/1 6. What state are we in? ______/1 7. What county are we in? ______/1 8. What city/town are we in? ______/1 9. What floor of the building are we on? ______/1 10. What is the name of this place? OR Where are we (address)? ______/3 Registration
11. I’m going to say three words and I want you to listen to all three words and repeat them after me. Ok? Listen carefully. What were the words?
Attention and Concentration ______/5 12a. I want you to think of the number 100 and subtract 7 from 100. What is the answer? ______/5 12b. I want you to think of the word “world” and spell it for me (forwards). Ok, now I want you to
spell it backwards. Ok? Begin at the end and spell the word “world” backwards. Recall ______/3 13 – 15. Do you remember those three words I had you repeat? Can you tell me those words now?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT MMSE: Cycle 1
Language ______/1 16. Show the participant a wristwatch. What do you call this? ______/1 17. Show a pencil. What do you call this? ______/1 18. I want you to repeat after me. Listen carefully and say exactly what I say. “No ifs ands or buts”. ______/1 19. Read this sentence and do what it says. _______/3 20. I want you to listen carefully because I’m going to ask you to do something and I want you to do
exactly what I say. Ok? Take the paper in your right hand, fold it in half, and drop it on the floor.
______/1 21. I want you to write a complete sentence. I just want you to make up any sentence. ______/1 22. I want you to make a copy of this drawing. ______/30 23. MMSE Total Score (“Serial Sevens Score”); score/30 ______/30 24. MMSE “World” Score; score/30 ______ 25. MMSE Score with Mungas Correction; Based on “World” Score ______ 26. If Mungas-corrected score is 20, did subject lose one point (only one point) because of impaired
vision or hearing? INTERVIEWER’S IMPRESSION ______ 27. Did the participant seem to be making his/her best effort? ______ 28. Did poor hearing interfere with test performance? ______ 29. Did poor vision interfere with test performance? ______ 30. Did any other physical limitation interfere with test performance? ______ 31. Did anxiety appear to interfere with test performance? ______ 32. Any other comments about test performance?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 1 MYAHT Blood Pressure Form Part I: Cycle 1
6/21/2016 MYHAT BLOOD PRESSURE FORM: SHORT VISIT
Cycle: 1 ________ / ________ 1. Take sitting blood pressure on either arm. Systolic / Diastolic
________ 2. Which side (right or left) was the sitting blood pressure taken on? ________ / ________ 3. Ask participant, What is your typical blood pressure? Systolic / Diastolic Write the blood pressure and the date it was taken on a sheet of paper and give it to the participant.
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Demographic & Contact Info Part II: Cycle 1
6/21/2016 MYHAT DEMOGRAPHIC AND CONTACT INFORMATION: PART II
Cycle: 1 ________ 1. What is your marital status? (or socially acceptable equivalent phrase, e.g. “Are you married?”)
1b. How long have you been _____ ? (married, widowed, divorced, etc.) ________ Months (If less than 1 year, code months. If less than 1 month, code as 1 month) ________ Years (If 1 year or more, code years. Round up) ________ 2. Do you have any children?
________ 2b. How many of your children live at home with you? ________ 3. How many people live here in your home with you? 3b. Who are they? Name Relationship to participant (code) Age
1. ___________________________________ ___________________________________ _________
2. ___________________________________ ___________________________________ _________
3. ___________________________________ ___________________________________ _________
4. ___________________________________ ___________________________________ _________
5. ___________________________________ ___________________________________ _________
6. ___________________________________ ___________________________________ _________
________ 4. Would you point to which of the categories on this card is correct about your household income
before taxes last year?
________ 5. INTERVIEWER: CODE TYPE OF RESIDENCE
________ 6. Do you own or rent this house, apartment, etc.? ________ 7. INTERVIEWER: CODE LIVING ARRANGEMENTS
________ 8. What was the main occupation you had most of your life?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Demographic & Contact Info Part II: Cycle 1
________ 9. What is your occupation (employment status) right now? 10. How long have you been____ ? (working, retired, etc.) ________ Months (If less than 1 year, code number of months. If less than 1 month, code as 1 month) ________ Years (If 1 year or more, code number of years. Round up) ________ 11. Have you taken any educational classes in the past year? ________ 12. INTERVIEWER’S IMPRESSION: Do you feel that the information in this section is reliable? ________ 13. INTERVIEWER: Do you have any general comments?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 5 MYHAT Subjective Memory: Cycle 1
6/21/2016 MYHAT SUBJECTIVE MEMORY
Cycle: 1 Do you think you are the same, better, or worse than you used to be?
PPT
INF
Domain
1. Remembering things (events, people, etc.) from a long time ago?
M
2. Remembering things that happened or were said a few days ago?
M
3. Remembering appointments, messages, etc.?
M
AD8.2 Are appointments forgotten?
4. Remembering names of people you’ve known for a long time?
M
5. Remembering names of people you only met recently?
M
6. Remembering telephone numbers of people whom you call often?
M
7. Remembering where you’ve put things that you use often? (keys, watch, glasses, etc.)
M
8. Remembering how to use familiar appliances, tools, gadgets? (includes car)
M
9. Remembering a familiar/favorite recipe without looking it up?
M
10. Finding the right word to use to describe something you know well? (names of familiar objects etc., not names of people)
M
11. Remembering what day/date/month it is?
O
12. Remembering a recent major event? e.g., trip, wedding
M
13. Remembering details of a major event?
M
14. Remembering when events happened in relation to each other? (Difficulty with time relationships, provide examples based on their own experiences.)
O
15. Remembering a few things you wanted to buy in the store, without writing them down?
M
16. Remembering to do important routine things like turn off the stove or lock the door?
M
17. Solving problems as easily as before?
J & PS

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 5 MYHAT Subjective Memory: Cycle 1
PPT
INF
Domain
18. Understanding what is going on or being said around you? (NOT because of hearing)
J & PS
19. Getting along with people, or talking and behaving the way you used to do?
J & PS
20. Handling a household emergency like a plumbing leak or a kitchen fire?
J & PS
21. Keeping up with hobbies and interests?
H/H
AD8.7 Do you have less interest than before in hobbies and usual activities?
H/H
AD8.1 Do others say you are repeating questions, stories, or statements?
M
AD8.3 Do you think you’ve made any bad decisions lately like about how you spend money, or what you say to people, or while driving?
J & PS
AD8.5 Do you have difficulty in learning or operating appliances (e.g., TV remote control, microwave)?
M
J & PS
AD8.8 Do you think any of these changes or difficulties are a problem?
22a. Are you (were you) worried about this (these) problem(s) with remembering?
22b. Was this (were these) enough of a problem that you talked to your doctor/nurse about it?
22c. How long ago did you start to notice the change(s) in your memory?
if less than 1 year, specify approximate number of months (1-12m)
if 1 year or more, specify approximate number of years (1y-99y)

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 5 MYHAT Subjective Memory: Cycle 1
PPT INF _____ _____ 23. Have you had any problems on the job? Write in participant’s response: ___________________________________________________________ _____________________________________________________________________________________ Write in informant’s response: ____________________________________________________________ _____________________________________________________________________________________ _____ _____ 24. Have you had any difficulties at work related to health? Specify: ______________________________________________________________________________ _____ _____ 25. Have you had any difficulties at work related to your memory or concentration? Specify: ______________________________________________________________________________ _____ _____ 26. Have you had any difficulties at work related to stress? Specify: ______________________________________________________________________________ Ask everyone: _____ _____ 27. Do you do any volunteer work, such as community-oriented or church-related activities? If yes, Specify: __________________________________________________________________
______________________________________________________________________________ PPT INF _____ _____ 27b. How often? _____ _____ 27c. If yes to seasonal work, how many weeks per year total? _____ _____ 27d. Approximately how many hours per week do you volunteer? _____ _____ 28. Do you provide any unpaid help to your friends, neighbors or family? (e.g. taking them shopping or
to doctor’s appointments; babysitting; working in family business; doing housework or yard work at neighbor’s or family member’s house. Does not include chores in own home)
_____ _____ 28b. How often? _____ _____ 28c. If yes to seasonal work, how many weeks per year total? _____ _____ 28d. Approximately how many hours per week?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 4 of 5 MYHAT Subjective Memory: Cycle 1
Interaction with Children PPT INF _____ _____ 1. Do you regularly interact (e.g. play with, teach or take care of) with children? If yes, Specify: __________________________________________________________________ _____ _____ 2a. If yes, how often? _____ _____ 2b. If yes to seasonal work, how many weeks per year total? _____ _____ 2c. Approximately how many hours per week? _____ _____ 3. Are you paid for any of these activities? 4. Who are the children you play with/teach/take care of? _____ _____ 4a. Grandchildren, great-grandchildren, or step-grand/great-grandchildren _____ _____ 4b. Other relative’s children _____ _____ 4c. Children of friends or neighbors _____ _____ 4d. Other children through a school or institution (e.g. Sunday School, day care center, kindergarten,
regular school) _____ _____ 4e. Other, Specify: _____________________________________________________________________ _____ _____ 5. Approximate age of the youngest child _____ _____ 6. Approximate age of oldest child _____ _____ 7. Comment? If yes, Specify: _____________________________________________________________ If retired, ask Q29 – Q30 If “homemaker”, unless specifically identified as “retired homemaker”, code Q29 – Q30 as -2. PPT INF _____ _____ 29. If retired: Did health problems have anything to do with your retirement? If yes, Specify: _________________________________________________________________________ _____________________________________________________________________________________ _____ _____ 30. If retired: Did memory or concentration problems have anything to do with your retirement? If yes, Specify: _________________________________________________________________________
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 5 of 5 MYHAT Subjective Memory: Cycle 1
QUESTIONS FOR INTERVIEWER: ________ INT1. Did an informant answer information of Subjective Memory Form? ________ INT2. If yes, who was the informant? (If two informants, choose the most reliable first) ________ INT2a. If yes, what is the relationship to the participant? ________ INT2b. If yes, do you feel that this informant was cognitively intact? ________ INT2c. If yes, do you feel this first informant was reliable and knowledgeable? ________ INT2d. If yes, frequency of informant’s contact with the participant: ________ INT3. If yes, who was the second informant? (If none, skip to INT4) ________ INT3a. If yes, what is the relationship of the second informant to the participant? ________ INT3b. If yes, do you feel that the second informant was cognitively intact? ________ INT3c. If yes, do you feel the second informant was reliable and knowledgeable? ________ INT3d. If yes, frequency of second informant’s contact with the participant: INTERVIEWER’S IMPRESSION: DO YOU FEEL THE SUBJECTIVE MEMORY INFORMATION IS LARGELY ACCURATE/VALID? ________ INT4. FROM PARTICIPANT: ________ INT5. FROM INFORMANT(S): ________ INT6. GENERAL COMMENTS

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 6 MYHAT ADL/IADL: Cycle 1
6/21/2016 MYHAT FUNCTIONAL ABILITIES
Cycle: 1 ACTIVITIES OF DAILY LIVING (ADLs) Now I am going to ask you some questions about how you get around and take care of your daily needs.
Participant
Informant
Question
ADL1: Do you need help from another person to get in/out of a bed/chair?
ADL2: When moving about your home, do you need help from a cane, a walker, a wheelchair or another person?
CDR1: Do you have difficulty finding your way around the home? (Mental reasons). (ORIENTATION)
ADL3: When you leave the house, do you use either a cane, a walker, a wheelchair or require physical help from another person?
ADL4: Do you need someone to help you with bathing? (sponge bath, tub or shower)
CDR2: Do you need any help with washing and grooming? (Mental reasons only). (PERSONAL CARE)
ADL5: Do you need any help getting dressed?
CDR3: (Mental reasons only). (PERSONAL CARE)
ADL6: Do you have any difficulty or need any help with eating?
CDR4: (Mental reasons only). (PERSONAL CARE)
INTERVIEWER: If participant has difficulty with any of the above tasks (for physical or mental reasons), ask: Participant Informant _______ _______ ADL7. How long have you had difficulty with…? (Mention the tasks that were impaired above)
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 6 MYHAT ADL/IADL: Cycle 1
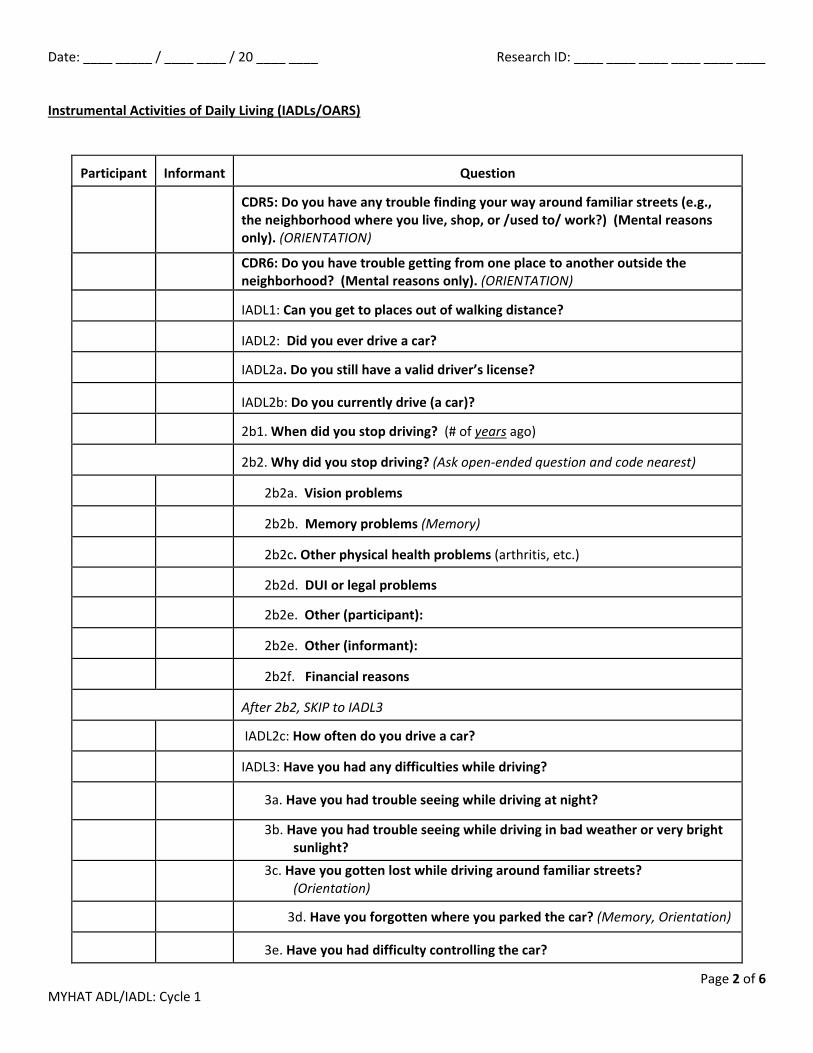
Instrumental Activities of Daily Living (IADLs/OARS)
Participant
Informant
Question
CDR5: Do you have any trouble finding your way around familiar streets (e.g., the neighborhood where you live, shop, or /used to/ work?) (Mental reasons only). (ORIENTATION)
CDR6: Do you have trouble getting from one place to another outside the neighborhood? (Mental reasons only). (ORIENTATION)
IADL1: Can you get to places out of walking distance?
IADL2: Did you ever drive a car?
IADL2a. Do you still have a valid driver’s license?
IADL2b: Do you currently drive (a car)?
2b1. When did you stop driving? (# of years ago)
2b2. Why did you stop driving? (Ask open-ended question and code nearest)
2b2a. Vision problems
2b2b. Memory problems (Memory)
2b2c. Other physical health problems (arthritis, etc.)
2b2d. DUI or legal problems
2b2e. Other (participant):
2b2e. Other (informant):
2b2f. Financial reasons
After 2b2, SKIP to IADL3
IADL2c: How often do you drive a car?
IADL3: Have you had any difficulties while driving?
3a. Have you had trouble seeing while driving at night?
3b. Have you had trouble seeing while driving in bad weather or very bright sunlight?
3c. Have you gotten lost while driving around familiar streets? (Orientation)
3d. Have you forgotten where you parked the car? (Memory, Orientation)
3e. Have you had difficulty controlling the car?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 6 MYHAT ADL/IADL: Cycle 1
Participant
Informant
Question
3f. Have you had difficulty concentrating while driving?
3g. Have you had any accidents when you were driving?
3h. Did you find yourself getting confused while you were driving?
(Orientation)
IADL4: Can you use the telephone? (Problem-solving)
IADL5: Can you go shopping by yourself for groceries and clothes? (Assume transportation is available).
CDR7: Shopping (Mental reasons only). (Community Affairs)
IADL6: Can you prepare your own meals? (Use same question/response for coding CDR8).
CDR8: Meal Prep (Mental reasons only). (Home & Hobbies)
IADL7: Can you do your housework independently? (Use same question/response for coding CDR9).
CDR9: Housework (Mental reasons only). (Home & Hobbies)
IADL8: Can you manage your own medicine? (Home & Hobbies)
IADL9: Can you handle your own money?
CDR10a: SMALL SUMS, e.g. make change, leave tip. (Mental reasons only). (Judgment & Problem Solving)
CDR10b: COMPLICATED TRANSACTIONS, e.g. Checkbook, bills. (Mental reasons only) (Judgment & Problem Solving)
AD8.4 Does the participant have difficulty with financial affairs (e.g. paying bills, balancing checkbook)? (Mental reasons only).
Participant Informant _______ _______ IADL10. MEMORY: How long have you had difficulty with…? (Name the impaired tasks due to
memory for this participant) Write actual response (participant): _________________________________________________ Write actual response (informant): __________________________________________________ _______ _______ IADL11. PHYSICAL LIMITATION: How long have you had difficulty with…? (Name the impaired
tasks due to physical limitation for this participant)
Write actual response (participant): _________________________________________________ Write actual response (informant): __________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 4 of 6 MYHAT ADL/IADL: Cycle 1
INTERVIEWER’S IMPRESSION:
_______ IADL10.1/11.1 IADLs. When you consider the 7 IADL items (getting places out of walking distance, using a telephone, shopping, doing housework, preparing meals, managing money, managing medications), would you say that the participant has impairment (if any) for cognitive reasons, physical reasons, both, or another reason?
EMPLOYMENT
If still working:
Participant Informant ______ ______ 12. Have you enjoyed your work?
______ ______ 13. Do you have plans to retire?
______ ______ 13b. If so, when? (code in months. If participant provides years, calculate months)
______ ______ 14. Have you been slowing down at work or taking it a bit easier in recent years?
______ ______ 15. Have you had any difficulties at work?
Specify (participant’s response): ____________________________________________________
______________________________________________________________________________
Specify (informant’s response): ____________________________________________________
______________________________________________________________________________
If retired:
Participant Informant
______ ______ 16. Are you enjoying retirement?
______ ______ 17. Were you happy to retire?
______ ______ 18. Did you want to keep working?
______ ______ 19. Did you have any problems at work that led you to retire?
Specify (participant’s response): ____________________________________________________
Specify (informant’s response): ____________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 5 of 6 MYHAT ADL/IADL: Cycle 1
If unemployed:
Participant Informant
______ ______ 20. How did you happen to become unemployed?
______ ______ 21. Did any health problems have anything to do with that situation?
Specify (participant’s response): ____________________________________________________
Specify (informant’s response): ____________________________________________________
______ ______ 22. Did any concentration problems have anything to do with that situation?
Specify (subject’s response): ____________________________________________________
Specify (informant’s response): ____________________________________________________
QUESTIONS FOR INTERVIEWER:
_______ INT1. Did an informant answer information on ADL/IADL?
_______ INT2. If yes, who was the informant? (If two informants, choose the most reliable first)
_______ INT2a. If yes, relationship of informant to participant:
_______ INT2b. If yes, do you feel this informant was cognitively intact?
_______ INT2c. If yes, do you feel this first informant was reliable and knowledgeable?
_______ INT2d. If yes, frequency of informant’s contact with the participant:
_______ INT3. If there was a second informant, who was the second informant? If none, skip to INT4.
_______ INT3a. If yes, relationship of second informant to participant:
_______ INT3b. If yes, do you feel this second informant was cognitively intact?
_______ INT3c. If yes, do you feel this second informant was reliable and knowledgeable?
_______ INT3d. If yes, frequency of second informant’s contact with the participant:
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 6 of 6 MYHAT ADL/IADL: Cycle 1
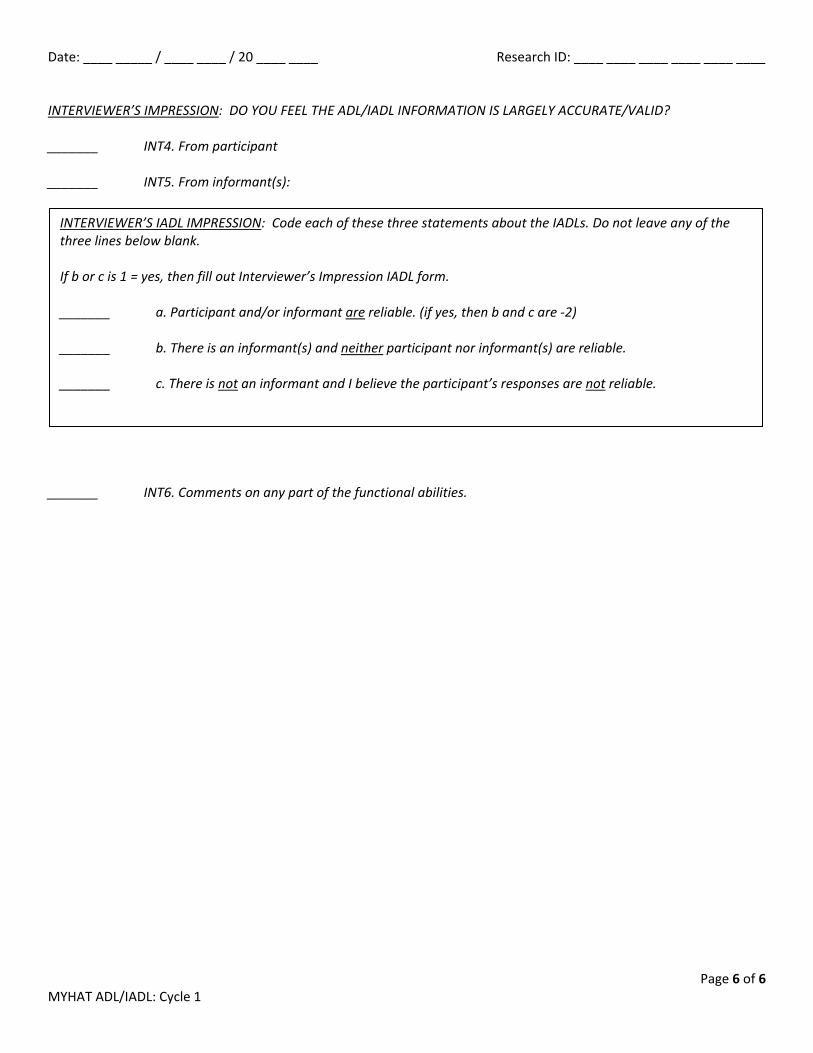
INTERVIEWER’S IMPRESSION: DO YOU FEEL THE ADL/IADL INFORMATION IS LARGELY ACCURATE/VALID?
_______ INT4. From participant
_______ INT5. From informant(s):
_______ INT6. Comments on any part of the functional abilities.
INTERVIEWER’S IADL IMPRESSION: Code each of these three statements about the IADLs. Do not leave any of the three lines below blank.
If b or c is 1 = yes, then fill out Interviewer’s Impression IADL form.
_______ a. Participant and/or informant are reliable. (if yes, then b and c are -2)
_______ b. There is an informant(s) and neither participant nor informant(s) are reliable.
_______ c. There is not an informant and I believe the participant’s responses are not reliable.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 1 MYHAT IADL-Interviewer’s Impression: Cycle 1
6/21/2016 MYHAT IADL-INTERVIEWER’S IMPRESSION
Cycle: 1 Instrumental Activities of Daily Living (IADL/OARS) Do not leave any blanks. Every item is needed to calculate an IADL score Physical Cognitive Question
IADL 1: Can you get to places out of walking distance?
IADL 4: Can you use the telephone? (problem-solving)
IADL 5: Can you go shopping by yourself for groceries and clothes? (assume transportation is available)
IADL 6: Can you prepare your own meals? (if never cooked/prepared meals, code -2)
IADL 7: Can you do your housework independently? (if never did housework, code -2)
IADL 8: Can you manage your own medicine? (Home & Hobbies)
IADL 9: Can you handle your own money?
Comment: Describe the reason you feel participant (and/or informant) is unreliable in their IADL reporting: __________________________________________________________________________________________________
__________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 1 MYHAT Handedness: Cycle 1
6/21/2016 MYHAT HANDEDNESS FORM
Cycle: 1 ________ 1. When writing, which hand do you use? ________ Left ________ Right ________ Either ________ 2. When throwing something, which hand do you use? ________ Left ________ Right ________ Either ________ 3. When playing games that require the use of a racket or bat, which hand do you use? ________ Left ________ Right ________ Either ________ 4. When cutting with scissors, which hand do you use? ________ Left ________ Right ________ Either ________ 5. When brushing your teeth, which hand do you use? ________ Left ________ Right ________ Either ________ 6. When striking a match, which hand do you use? (Refers to hand holding the match) ________ Left ________ Right ________ Either ________ 7a. When hammering, which hand do you use? ________ Left ________ Right ________ Either ________ 7b. When threading a needle (guiding a needle onto a stationary thread—refers to hand that is
moving), which hand do you use? ________ Left ________ Right ________ Either ________ 8. Total: FINAL HANDEDNESS CODE: 1 = left-handed, 2 = right-handed, 3 = either hand Total each column below. If all items are left or right, code appropriately. If hand preference is not all
right or all left (not including negative codes) or are all “either” code Q9 as 3. Refer to manual for more scoring info.
________ Left ________ Right ________ Either ________ 9. Source of information ________ 10. INTERVIEWER’S IMPRESSION: Any comments?

9/9/2016 MYHAT NEUROPSYCHOLOGICAL TEST BATTERY
ORDER OF ADMINISTRATION
_____MMSE + Mungas correction (earlier in the assessment, for all participants) _____FULD learning trials time __________ _____Face Name Initial Learning _____Digit Span _____Trail Making Tests _____Clock Drawing _____Modified Token Test _____Delayed recall FULD (“Bag A”) time __________ _____Face Name Delayed Cued Recall (optional break point) _____ Logical Memory I – immediate recall (“stories”) time ____________ _____Benton Visual Form Discrimination _____Block Design _____Boston Naming Test _____Verbal Fluency – animals, ‘P’, ‘S’ _____ Logical Memory II – delayed recall (“stories”) time __________
Approx. 20 minutes
Approx. 30 minutes

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 3 MYHAT Neuropsych Summary: Cycle 1
9/9/2016 MYHAT NEUROPSYCHOLOGICAL TEST SUMMARY
Cycle: 1 Corrected vision (for reading)? 0 = not needed 1 = yes 2 = no, but needed Hearing aids (for conversation)? 0 = not needed 1 = yes, one 2 = yes, two 3 = none, but needed MMSE (serial sevens total): Total Score: _________________ WTAR: Raw Score: __________________ Attention Digit Span Forward
Total Score: ____________ Basal Span: ____________ Max Span: ____________ Trail-Making A
Time (sec): ____________ Errors: ____________ # Points Connected: ____________ Language Verbal Fluency Category: Letter: Animals: ____________ “P”: ____________ “S”: ____________ Boston Naming Test (max score is 59)
Spontaneous (A): ____________ Stimulus (B): ____________ Phonemic (C): ____________ Modified Token Test
Grand Total: ____________
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 3 MYHAT Neuropsych Summary: Cycle 1
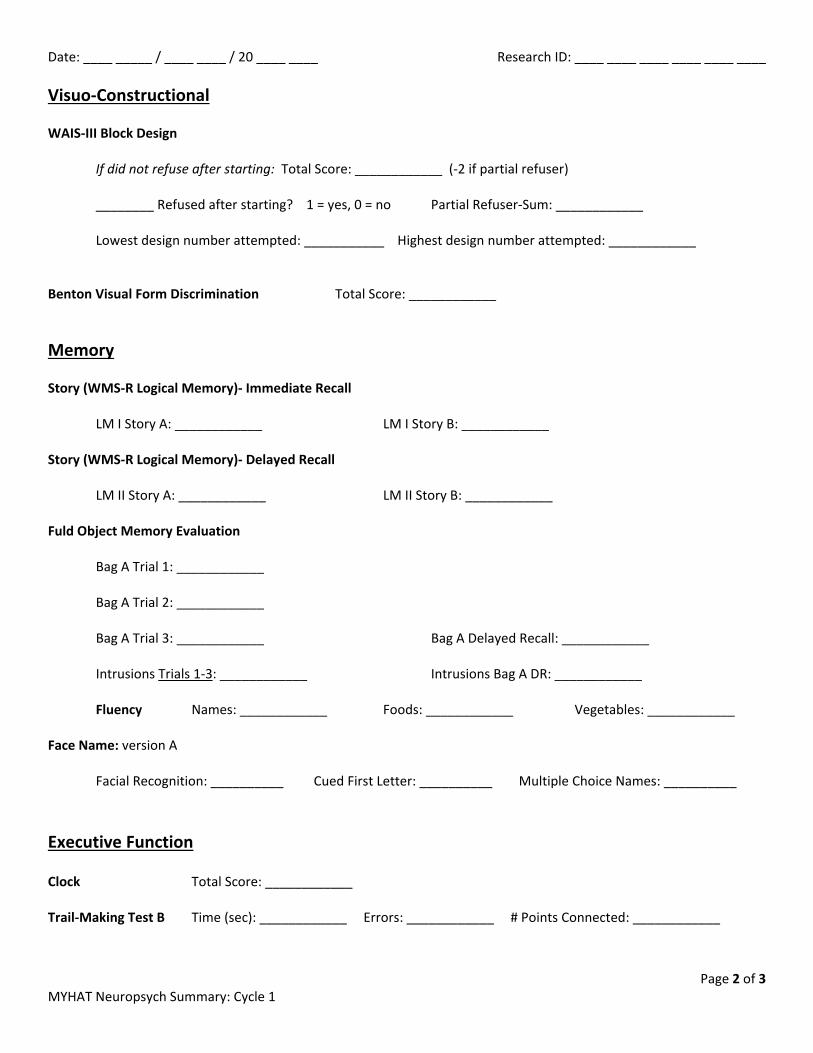
Visuo-Constructional WAIS-III Block Design
If did not refuse after starting: Total Score: ____________ (-2 if partial refuser)
________ Refused after starting? 1 = yes, 0 = no Partial Refuser-Sum: ____________
Lowest design number attempted: ___________ Highest design number attempted: ____________ Benton Visual Form Discrimination Total Score: ____________ Memory Story (WMS-R Logical Memory)- Immediate Recall
LM I Story A: ____________ LM I Story B: ____________ Story (WMS-R Logical Memory)- Delayed Recall
LM II Story A: ____________ LM II Story B: ____________ Fuld Object Memory Evaluation
Bag A Trial 1: ____________
Bag A Trial 2: ____________
Bag A Trial 3: ____________ Bag A Delayed Recall: ____________
Intrusions Trials 1-3: ____________ Intrusions Bag A DR: ____________
Fluency Names: ____________ Foods: ____________ Vegetables: ____________ Face Name: version A
Facial Recognition: __________ Cued First Letter: __________ Multiple Choice Names: __________ Executive Function Clock Total Score: ____________ Trail-Making Test B Time (sec): ____________ Errors: ____________ # Points Connected: ____________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 3 MYHAT Neuropsych Summary: Cycle 1
INTERVIEWER’S IMPRESSION: ________ 1. Did any physical disability interfere with neuropsychological testing? If yes, what kind of disability? (code all applicable) ________ Vision ________ Hearing
________ Speech (e.g. aphasia) ________ Motor (not including tremor) ________ Other, specify: __________________________________________________ ________ Anxiety ________ Fatigue/tired ________ Pain ________ Tremor ________ Weakness
________ 2. Do you have any other comments about the cognitive testing? If yes, specify: ____________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ ________ 3. Did the participant give his/her best effort? If no, describe what prevented their best effort: ________ _____________________________________________________________________________________ _____________________________________________________________________________________ ________ 4. Were there any distractions or interruptions during the cognitive testing that may have interfered
with the participant’s performance? If yes, specify: ___________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Judgment Form: Cycle 1
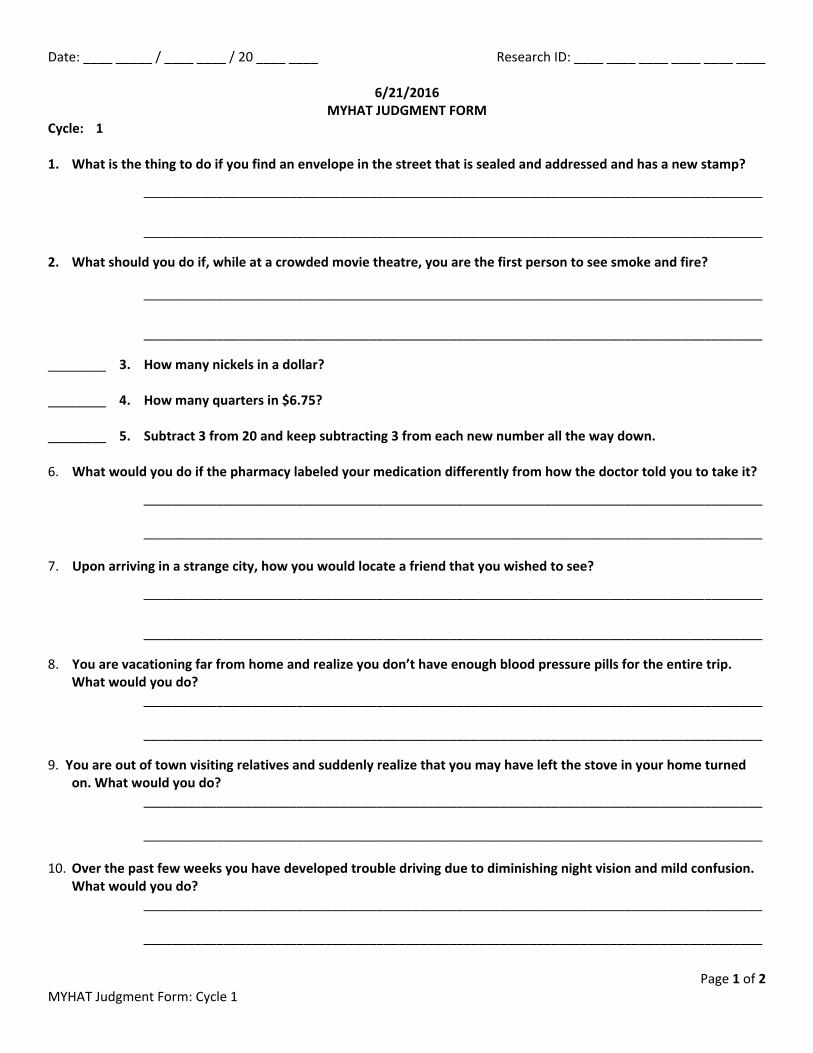
6/21/2016 MYHAT JUDGMENT FORM
Cycle: 1 1. What is the thing to do if you find an envelope in the street that is sealed and addressed and has a new stamp?
_____________________________________________________________________________________
_____________________________________________________________________________________
2. What should you do if, while at a crowded movie theatre, you are the first person to see smoke and fire?
_____________________________________________________________________________________
_____________________________________________________________________________________
________ 3. How many nickels in a dollar? ________ 4. How many quarters in $6.75? ________ 5. Subtract 3 from 20 and keep subtracting 3 from each new number all the way down. 6. What would you do if the pharmacy labeled your medication differently from how the doctor told you to take it?
_____________________________________________________________________________________
_____________________________________________________________________________________
7. Upon arriving in a strange city, how you would locate a friend that you wished to see?
_____________________________________________________________________________________
_____________________________________________________________________________________
8. You are vacationing far from home and realize you don’t have enough blood pressure pills for the entire trip. What would you do?
_____________________________________________________________________________________
_____________________________________________________________________________________
9. You are out of town visiting relatives and suddenly realize that you may have left the stove in your home turned on. What would you do?
_____________________________________________________________________________________
_____________________________________________________________________________________
10. Over the past few weeks you have developed trouble driving due to diminishing night vision and mild confusion. What would you do?
_____________________________________________________________________________________
_____________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Judgment Form: Cycle 1
________ 11. INTERVIEWER: Any comments? If yes, specify: ____________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 16 MYHAT Health, History & Lifestyle: Cycle 1
10/17/2016 MYHAT HEALTH, HISTORY AND LIFESTYLE
Cycle: 1 SUBJECTIVE ASSESSMENT OF HEALTH ________ 1. Compared to other people your age, how would you rate your overall state of health? MEDICAL HISTORY I am going to ask you a few questions about your medical history. Has a doctor or a nurse ever told you that you had any of the following? ________ 2. Stroke(s) – cerebrovascular accident (CVA)
Types of strokes: Ischemic – “blood clot” (thrombosis/embolism) Hemorrhage – “brain bleed”
When did you have this/these stroke(s) and what type of stroke was it/were they? (Code in reverse
chronological order. First stroke should be at the bottom of the list. Code -2 when appropriate) 2.1. Date of most recent stroke: ______ / ______ / ______
2.1a. Type of stroke: ________________ _____________________________
2.2. Date of next most recent stroke: ______ / ______ / ______
2.2a. Type of stroke: _____________________________________________
2.3. Date of stroke: ______ / ______ / ______
2.3a. Type of stroke: _____________________________________________
2.4. Date of first stroke: ______ / ______ / ______
2.4a. Type of stroke:______________________________________________
List the first stroke in the “first stroke” line regardless of when it occurred. Examples: If participant had two strokes, list most recent stroke first in the list (Q2.1) and list first stroke in Q2.4. Enter -2 for 2.2 and 2.3. If participant had one stroke, enter this in Q2.4 as first stroke. Questions 2.1 – 2.3 are entered as -2.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 16 MYHAT Health, History & Lifestyle: Cycle 1
2.5. Did (any of) the stroke(s) affect the following functions? (Code all options) 2.6. To what extent have you recovered those functions? 2.5 Functions: 2.6 Recovery: _____ memory _____ memory
_____ vision _____ vision
_____ hearing _____ hearing
_____ speech _____ speech
_____ right sided weakness _____ right sided weakness
_____ left sided weakness _____ left sided weakness
_____ gait _____ gait
_____ right sided dexterity _____ right sided dexterity
_____ left sided dexterity _____ left sided dexterity
_____ right sided facial droop _____ right sided facial droop
_____ left sided facial droop _____ left sided facial droop
_____ other: ________________ _____ other: ________________
________ 3. TIA, mini-stroke, reversible or transient stroke, i.e. left no residual effect (Transient ischemic attack
over within 24 hours, reversible ischemic neurologic deficit over within 72 hours) Specify: __________________________________________________________________
________ 4. Seizure disorder, epilepsy or convulsions. Was the participant started on an anti-seizure medication? Or told by his/her doctor not to drive?
Specify: __________________________________________________________________ ________ 5. Heart attack (myocardial infarction)
Specify: __________________________________________________________________
________ 6. Angina (angina, angina pectoris)
Specify: __________________________________________________________________
________ 7. Congestive heart failure, heart failure, water or fluid on lungs
Specify: __________________________________________________________________
________ 8. Irregular heartbeat, atrial fibrillation, heart racing, palpitations (cardiac arrhythmia, especially atrial
fibrillation) Specify: ____________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 16 MYHAT Health, History & Lifestyle: Cycle 1
________ 9. Cardiac arrest, heart stopped, did participant need CPR or to be resuscitated?
Specify: ____________________________________________________________________
________ 10. High blood pressure (hypertension)
Specify: ____________________________________________________________________
________ 11. High cholesterol (hyperlipidemia, hypercholesterolemia)
Specify: ____________________________________________________________________
________ 12. Emphysema, COPD (chronic obstructive pulmonary disease)
Specify: ____________________________________________________________________
________ 13. Asthma
Specify: ____________________________________________________________________
________ 14. Liver disease, hepatitis, jaundice, cirrhosis, etc.
Specify: ____________________________________________________________________
________ 15. Kidney disease, kidney dialysis, renal disease, renal failure, renal insufficiency
Specify: ____________________________________________________________________
________ 16. Diabetes mellitus, sugar diabetes (Type I or II, juvenile or adult onset, insulin or non-insulin
dependent diabetes) Specify: ____________________________________________________________________ ________ 17. Thyroid problem, goiter, thyroid disease, hyperthyroid, hypothyroid, thyroiditis
Specify: ____________________________________________________________________
________ 18. Menopause symptoms, hot flashes, etc. (code -2 for men)
Specify: ____________________________________________________________________
________ 19. Age at menopause/last menstrual period, if applicable.
Allow a spontaneous answer and code either the exact age, an estimated age or an age range based on the information the participant provides. Code -2 for men.
________ exact age
________ estimated age
________ - ________ age range
Specify: ____________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 4 of 16 MYHAT Health, History & Lifestyle: Cycle 1
________ 20. Eye problems, macular degeneration, glaucoma, retinal detachment, etc.
Specify: ____________________________________________________________________
________ 21. Tumors, masses or lumps
Specify: ____________________________________________________________________
If yes to tumors/masses/lumps: ________ 21a. Were they malignant? (cancer, malignant neoplasm) If malignant:
________ 21a1. Breast
________ 21a2. Prostate
________ 21a3. Colon
________ 21a4. Lung
________ 21a5. Other, specify: _____________________________________________________
________ 21a6. Skin, specify: ______________________________________________________
________ 21a7. Brain, specify: _____________________________________________________
________ 21a8. Uterus (including endometrial, cervical), specify: _________________________
________ 21b. Leukemia
Specify: ____________________________________________________________________ Radiation: Ask everyone regardless of cancer reported or not. ________ 22. Have you ever had any radiation treatment for [the reported above] cancer(s) or for any other
condition? If yes, participant had radiation for cancer(s), indicate which cancer/location: ________ 22a. Breast
________ 22b. Prostate
________ 22c. Colon
________ 22d. Lung
________ 22e. Skin, specify: _______________________________________________________
________ 22f. Brain, specify: ______________________________________________________
________ 22g. Uterus (include endometrial, cervical), specify: ___________________________
________ 22h. Other cancer location, specify: ________________________________________
________ 22i. Leukemia
If yes, participant had radiation for a condition other than cancer:
________ 22j. Not cancer, specify condition and location(s): _____________________________
___________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 5 of 16 MYHAT Health, History & Lifestyle: Cycle 1
________ 22k. Are you currently receiving radiation? ________ 22l. How many treatments of radiation have you had? Chemotherapy: Ask everyone regardless of cancer reported or not. ________ 23. Have you ever had any chemotherapy treatment for [the reported above] cancer(s) or for any
other condition? If yes, participant had chemotherapy for cancer(s), indicate which cancer/location: ________ 23a. Breast
________ 23b. Prostate
________ 23c. Colon
________ 23d. Lung
________ 23e. Skin, specify: _______________________________________________________
________ 23f. Brain, specify: ______________________________________________________
________ 23g. Uterus (include endometrial, cervical), specify: ___________________________
________ 23h. Other cancer location, specify: ________________________________________
________ 23i. Leukemia
If yes, participant had chemotherapy for a condition other than cancer:
________ 23j. Not cancer, specify condition and location(s): _____________________________
___________________________________________________________________________________
________ 23k. Are you currently receiving chemotherapy? ________ 23l. How many treatments of chemotherapy have you had? ________ 24. Memory problems, dementia, Alzheimer’s disease, senility, multi-infarct or vascular dementia.
(more than “mild”, “expected with age”) Specify: _____________________________________________________________________ ________ 25. Parkinson’s disease, Parkinsonism Specify: _____________________________________________________________________ ________ 26. Vitamin B-12 deficiency. Did your doctor tell you that you had a B-12 deficiency or low levels? Did
your doctor tell you to take B-12 pills or get a monthly B-12 shot? (cyanocobalamin deficiency, pernicious anemia)
Specify: _____________________________________________________________________ ________ 27. Anemia, Iron deficiency Specify: _____________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 6 of 16 MYHAT Health, History & Lifestyle: Cycle 1
________ 28. Arthritis, osteoarthritis, degenerative joint disease, rheumatoid arthritis, rheumatism
If yes, must circle or specify: ____________________________________________________
________ 29. Sciatica, intervertebral disc disease, herniated disc, bulging disc, spinal stenosis
Specify: _____________________________________________________________________
________ 30. Osteoporosis, osteopenia
Specify: _____________________________________________________________________
________ 31. Have you had a bone density test? (e.g. Dexa scan) ________ 32. Depression, clinical depression, major depression
Specify: _____________________________________________________________________
________ 33. Anxiety, nerves, nervousness
Specify: _____________________________________________________________________
________ 34. Do you know how much you weighed when you were born?
_____ lb. _____ oz.
Specify: _____________________________________________________________________ ________ 35. Any other condition mentioned by participant or informant?
Include conditions you don’t know how to classify. Specify: _____________________________________________________________________ ____________________________________________________________________________ ____________________________________________________________________________ ________ 36. INTERVIEWER’S IMPRESSION: Do you think the information about the participant’s medical history is
mostly accurate? If no, comments: ______________________________________________________________ ____________________________________________________________________________ ____________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 7 of 16 MYHAT Health, History & Lifestyle: Cycle 1
SURGICAL/PROCEDURAL HISTORY Have you ever had any of the following surgeries or procedures?
0 = No 1 = Yes
-2 = N/A
If yes, write approximate YEAR of most recent procedure Surgery or Procedure
37. Heart bypass surgery, coronary artery bypass graft
38. Other heart surgery, e.g. valve replacement
39. Cardiac “cath” or catheterization
40. Other heart procedures, such as balloon angioplasty, laser, stent (coronary revascularization short of bypass graft)
41. Cardiac pacemaker/implantable defibrillator
42. Operation to improve circulation in your legs (lower extremity bypass graft/angioplasty/stent)
43. Operation to open blockages in your neck arteries (carotid endarterectomy/angioplasty/stent)
44. Operation to repair an aortic aneurysm or dissection
45. Brain surgery (craniotomy)
46. Ovaries removed/total hysterectomy with ovaries removed (code -2 for men)
47. Cataract removal
48. Organ transplant
48a. If yes to organ transplant, specify organ:
________ 49. Have you ever had surgery with general anesthesia (i.e. when you were put to sleep altogether for
the procedure?) ________ 50. INTERVIEWER’S IMPRESSION: Do you think that the information in the participant’s surgical history
is mostly accurate and/or complete? If no, comments:_______________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 8 of 16 MYHAT Health, History & Lifestyle: Cycle 1
GENERAL HEALTH QUESTIONS: SLEEP Now I am going to ask you a few questions about your sleeping patterns. On most nights…? ________ 51. Do you take longer than a half an hour to fall asleep? ________ 52. Do you wake up during the night (including to go to the bathroom) and find that it takes you more
than a half an hour to go back to sleep? ________ 53. Do you wake up earlier than you want to and find that you can’t go back to sleep? ________ 54. Does anything in particular interfere with your sleep? ________ 54a. Breathing problems
________ 54b. Pain
________ 54c. Stress and/or worry, sadness, loneliness
________ 54d. Noise
________ 54e. Caregiving
________ 54f. Using/going to bathroom
________ 54g. Pet, specify: _________________________________________________
________ 54h. Partner/spouse, specify: _______________________________________
________ 54i. Other, specify: _______________________________________________
________ 54j. Sleep apnea
________ 54k. Restless leg/leg cramps
________ 54l. Daytime napping
________ 55. Do you ever fall asleep while actively doing something during the day? (Do you find that you are
uncontrollably sleepy? Do you find it impossible to stay awake?)
________ 55a. When involved in conversation ________ 55b. While driving a car ________ 55c. While watching television ________ 55d. Other, specify: ___________________________________________ ________ 55e. Reading
________ 56. Do you doze off or take a nap most days of the week?
________ 56a. If yes, Approximately how many total minutes or hours in a day do you nap? (Code in minutes. If necessary, ask how many naps per day and how many minutes per nap.)

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 9 of 16 MYHAT Health, History & Lifestyle: Cycle 1
________ 57. As far as you know, do you snore loudly when you sleep? (Has anyone else told you that you snore
loudly?) ________ 58. Have you ever been told that you have sleep apnea? ________ 59. Have you ever had a sleep study done? ______/______/______ 59a. If yes, date of most recent sleep study. ________ 60. Do you use any equipment for sleep problems? ________ 60a. Oxygen
________ 60b. CPAP
________ 60c. BIPAP
________ 60d. Other, specify: _____________________________________________________________
________ 61. INTERVIEWER’S IMPRESSION: Do you think that the information given on sleep is mostly accurate
and/or complete? If no, comments: _______________________________________________________________________ _____________________________________________________________________________________
_____________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 10 of 16 MYHAT Health, History & Lifestyle: Cycle 1
GENERAL HEALTH QUESTIONS: APPETITE AND WEIGHT Now I’d like to ask you some questions about your appetite and eating patterns. ________ 62. How is your appetite most of the time? ________ 63. Is this a change in appetite for you? ________ 64. Are you eating the same amount as you did a year ago? ________ 65. Have you gained weight in the past year?
________ 65a. If yes, number of pounds gained in past year.
________ 66. Have you lost weight without dieting in the past year? ________ 66a. If yes, How many pounds did you lose? (Code number of pounds) ________ 66b. If yes, Over how many months did you lose that weight? (Code number of months) ________ 67. INTERVIEWER’S IMPRESSION: Do you think that the information on appetite and weight is mostly
accurate and/or complete? If no, comments: _______________________________________________________________________ GENERAL HEALTH QUESTIONS: BALANCE Now I’d like to ask you some questions about your balance. ________ 68. Do you have a problem with balance? ________ 69. Do you often feel dizzy or lightheaded? ________ 70. Do you have vertigo? ________ 71. Have you fallen at all in the past year?
if yes, specify:
______________________________________________________________________________
________ 71a. If yes, How many times have you fallen in the past year? ________ 72. Have you ever had a head injury/trauma which cause you to pass out (lose consciousness)? If yes and was sports-related, be sure to complete the Sports Related Head Trauma form. ________ 73. INTERVIEWER’S IMPRESSION: Do you think that the information in the section on balance is mostly
accurate and/or complete? If no, comment: ________________________________________________________________________
_____________________________________________________________________________________
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 11 of 16 MYHAT Health, History & Lifestyle: Cycle 1
GENERAL HEALTH QUESTIONS: CONTINENCE ________ 74. Do you have any difficulty controlling your bladder and/or a sense of urgency to get to the
bathroom on time? If yes:
________ 74a. Do you leak urine when you cough, sneeze, laugh, or strain? ________ 74b. Do you leak urine when you can’t get to the bathroom on time? ________ 74c. Do you wear a protective pad (diaper)? ________ 75. INTERVIEWER’S IMPRESSION: Do you think that the information in the section on continence is
mostly accurate and/or complete? If no, comment: ________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
GENERAL HEALTH QUESTIONS: SMOKING AND DRINKING Now I’m going to ask you some questions about smoking and drinking. Smoking ________ Did you ever smoke cigarettes? ________ 76. Have you smoked cigarettes in the past year? ________ 77. Do you smoke cigarettes now? ________ 78. How many cigarettes do you smoke per day now? (20 cigarettes in a pack; record actual number.) ________ 79. In your life, what was the most that you ever smoked per day? ________ 80. For how long did you smoke this much? (Code years) ________ 81. Have you smoked cigars or pipes in the past year? ________ 82. Have you used chewing tobacco or snuff in the past year? ________ 83. Have you used e-cigarettes (vaping) in the past year? ________ 84. Do you use a nicotine patch or nicotine gum in the past year? ________ 85. Does anyone (else) in your house smoke cigarettes, cigars or pipes regularly? ________ 86. INTERVIEWER: Do you think that the information in the smoking section is mostly accurate and/or
complete?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 12 of 16 MYHAT Health, History & Lifestyle: Cycle 1
Alcohol
________ 87. Have you ever had (did you ever drink) any beer, wine, spirits, liquor? ________ 88. What is the reason you have not had any alcohol since more than one year ago?
89. Approximately how long ago did you have your last drink?
________ 90. How often do you usually have a drink? ________ 91. When you do have a drink, how many drinks do you usually have at a time (on each occasion)? ________ 92. Do you drink red wine? ________ 93. How often do you drink red wine? ________ 94. When you drink red wine, how many glasses do you usually have at a time (on each occasion)? ________ 95. Do you drink white wine? ________ 96. How often do you drink white wine? ________ 97. When you drink white wine, how many glasses do you usually have at a time (on each occasion)? ________ 98. Do you drink beer? ________ 99. How often do you drink beer? ________ 100. When you drink beer, how many glasses do you usually have at a time (on each occasion)? ________ 101. Do you drink liquor/spirits? (e.g. whiskey, scotch, brandy, rum, vodka, gin; including mixed drinks,
cocktails and shots) ________ 102. How often do you drink liquor/spirits? ________ 103. When you drink liquor/spirits, how many glasses do you usually have at a time (on each
occasion)? ________ 104. Was there a time in your life when you would drink more than you do now? ________ 105. In your life, what was the most you would drink on a single occasion? ________ 106. At that time, how often would you drink? ________ 107. How old were you at that time? ________ 108. INTERVIEWER’S IMPRESSION: Do you think that the information in the alcohol section is mostly
accurate and/or complete?
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 13 of 16 MYHAT Health, History & Lifestyle: Cycle 1
FAMILY HISTORY I’d like to ask you some questions about your family’s medical history. Have any of your immediate blood relatives (parents, brothers, sisters, and children) had any of the following? If participant has no siblings or children, code -2
Parents Siblings Children 109. Heart disease (coronary artery
disease, cardiac death, myocardial infarction/revascularization)
110. Blocked neck arteries
111. Cancer (see next line)
111a. If family history of cancer, specify type/organ in appropriate boxes on left.
112. Stroke(s)
113. Memory problems (senility, dementia, Alzheimer’s disease)
114. Depression or bipolar disorder (manic-depression)
115. Substance abuse problem
________ 116. INTERVIEWER’S IMPRESSION: Do you think that the information in the family history section is
mostly accurate and/or complete? If no, comment: _________________________________________________________________
______________________________________________________________________________ _____________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 14 of 16 MYHAT Health, History & Lifestyle: Cycle 1
ACTIVITIES ________ 117. Do you have any interests or hobbies (not using the computer)?
If yes, what are they?
________ 117a. Playing cards (non-gambling: bridge, rummy, etc.)
________ 117b. Crossword puzzles, Sudoku, word games, acrostics, anagrams and other word/number
puzzles
________ 117c. Reading (NOT including eReaders, e.g. Kindle, Nook. Code this in 118v)
________ 117d. Board games
________ 117e. Playing a musical instrument
________ 117f. Photography
________ 117g. Painting
________ 117h. Gambling
________ Bingo ________ Slots ________ Cards ________ Lottery ________ Other gambling, specify: _________________________________________
________ 117i. Other games: __________________________________________________________
________ 117j. Shopping, flea markets, antiquing
________ 117k. Fishing, hunting
________ 117l. Sewing, knitting, crocheting
________ 117m. Woodworking, stained glass, crafts
________ 117n. Jigsaw puzzles
________ 117o. Genealogy
________ 117p. Gardening/yardwork (light intensity)
________ 117q. Golf (light intensity, e.g. driving range, using a cart)
________ 117r. Baking, cooking, candy making, canning
________ 117s. Other, specify: ___________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 15 of 16 MYHAT Health, History & Lifestyle: Cycle 1
________ 118. Do you use a computer or other electronic device (smart phone, tablet, eReader, iPad, iPod)
If yes, which devices do you use? Indicate all that apply.
_____ desktop or laptop computer _____ tablet, iPad _____ eReader (Kindle, Nook) _____ iPod _____ smartphone _____ other, specify: ______________________________________
If yes, for what purposes?
________ 118a. Email
________ 118b. Shopping
________ 118c. Games (not including gambling. If specifically a brain training game, code in 118u.)
________ 118d. Gambling (e.g. casino, poker, cards, betting)
________ 118e. Internet browsing, visiting specific websites
________ 118f. Work
________ 118g. Finances, paying bills, banking, taxes
________ 118h. Word processing
________ 118i. Social media (internet forums, chat rooms, blogs, social networks (Facebook, LinkedIn, Twitter),
YouTube, instant messaging, Pinterest, Instagram) Specify:_____________________________________
________ 118j. Genealogy
________ 118k. Skype or FaceTime
________ 118l. Online courses
________ 118m. Text messaging
________ 118n. GPS and navigation
________ 118o. Taking photographs
________ 118p. Medication management
________ 118q. Alarm clock
________ 118r. Calendars, scheduling, to-do lists
________ 118s. Playing or downloading music
________ 118t. Physical activity tracker
________ 118u. Brain-training games (Lumosity, Nintendo Brain Age, Elevate, etc.)
________ 118v. eReading (eReader, Kindle, Nook)
________ 118w. Other, specify: ___________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 16 of 16 MYHAT Health, History & Lifestyle: Cycle 1
119. If you use a computer (desktop or laptop), where do you use it? (indicate all that apply) ________ Own a home computer
________ Computer at place of work
________ Computer at library
________ Computer at senior center
________ Computer at daughter’s/son’s home
________ Computer at friend’s/neighbor’s home
________ Other, specify: ___________________________________________________________
________ 120. What is the last year in which you voted in a national or state election?
ADL8. In the past year, have you left your home (apartment, trailer, etc.) to go to…
Participant Informant
________ ________ ADL8a. Doctor’s or medical appointment
________ ________ ADL8b. Church/place of worship (regular services, funerals, weddings)
________ ________ ADL8c. Special family occasion
________ ________ ADL8d. Other social occasion (visit family/friends, senior center, clubs, restaurants,
lodge, bar)
________ ________ ADL8e. Shopping, bank, post office
________ ________ ADL8f. Haircut/beauty shop/salon, barber
________ ________ ADL8g. Bingo, gambling
________ ________ ADL8h. Work/volunteer activity
________ ________ ADL9. How often do you leave your house/apartment/trailer, etc.? ________ ADL INT1. INTERVIEWER: Did an informant give information on ADL? ________ ADL INT2. INTERVIEWER: If yes, was this the same informant who gave information on the ADL/IADL
Functional Abilities form? ________ ADL INT3. INTERVIEWER’S IMPRESSION: Do you feel this informant was reliable and knowledgeable? ________ 121. INERVIEWER’S IMPRESSION: Do you think that the information in the activity section is mostly
accurate and/or complete? ________ 122. INTERVIEWER: Any other comments on part of the history?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 3 MYHAT FCAS: Cycle 1
6/21/2016 MYHAT FLORIDA COGNITIVE ACTIVITIES SCALE (FCAS) – Form S
Cycle: 1 We would now like to ask you about how often you do a list of activities that you may do in your everyday life. Some of the activities we have already asked whether you do them or not, but now we would like to know about how often you do the activities. Some of these activities you may do frequently. Others may be activities that you have never done. [SHOW CARD] Please point to the amount of time on the card that best describes how often that you perform each of the activities. The choices are: (read choices aloud) ________ 1. Playing games like chess, bridge, Scrabble, or Trivial Pursuit Comment: _____________________________________________________________________ ________ 2. Playing other board games like checkers or Monopoly Comment: _____________________________________________________________________ ________ 3. Solving crossword puzzles, acrostics, anagrams, Sudoku (i.e. puzzles) Comment: _____________________________________________________________________ ________ 4. Watching TV and/or listening to talk radio Comment: _____________________________________________________________________ ________ 5. Listening to music (e.g. on the radio or TV or going to concerts) Comment: _____________________________________________________________________ ________ 6. Gardening (during season) Comment: _____________________________________________________________________ ________ 7. Reading the newspaper or news from other sources (e.g. blogs, websites, news magazines (e.g.
Time, Newsweek)) Comment: _____________________________________________________________________ ________ 8. Reading books or short stories (including books on tape or periodicals (e.g. The New Yorker,
Reader’s Digest)) Comment: _____________________________________________________________________ ________ 9. Writing letters, personal notes, or emails to friends or relatives (or businesses, editorials) Comment: _____________________________________________________________________
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 3 MYHAT FCAS: Cycle 1
________ 10. Talking on the phone with, or visiting, friends or family (social contact) Comment: _____________________________________________________________________ ________ 11. Doing original artwork or craft work like drawing, painting, sculpting, sewing without a pattern,
woodworking Comment: _____________________________________________________________________ ________ 12. Doing art or craft kits or patterns like knitting, paint-by-number, needlework Comment: _____________________________________________________________________ ________ 13. Making complex home repairs that involve planning and time Comment: _____________________________________________________________________ ________ 14. Making simple home repairs Comment: _____________________________________________________________________ ________ 15. Preparing meals from new recipes Comment: _____________________________________________________________________ ________ 16. Cooking familiar recipes Comment: _____________________________________________________________________ ________ 17. Actively participating in discussions of politics or ideas (formal or informal setting) Comment: _____________________________________________________________________ ________ 18. Taking a course (formal or informal) or participating in a discussion group (e.g. book clubs) in
which you are not tested on your knowledge Comment: _____________________________________________________________________ ________ 19. Managing a financial portfolio of investments (yourself) Comment: _____________________________________________________________________ ________ 20. Doing routine financial work (paying bills, balancing checkbook, contacting accountant or financial
advisor, checking stocks) Comment: _____________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 3 MYHAT FCAS: Cycle 1
________ 21. Walking or driving in unfamiliar places (that you would require a map or navigation to get to) Comment: _____________________________________________________________________ ________ 22. Walking or driving in familiar places Comment: _____________________________________________________________________ ________ 23. Going to social clubs or social events (including volunteer groups) Comment: _____________________________________________________________________ ________ 24. Participating in church or religious activities (e.g. attending or watching mass/service, bible study) Comment: _____________________________________________________________________ ________ 25. Shopping (any type) Comment: _____________________________________________________________________
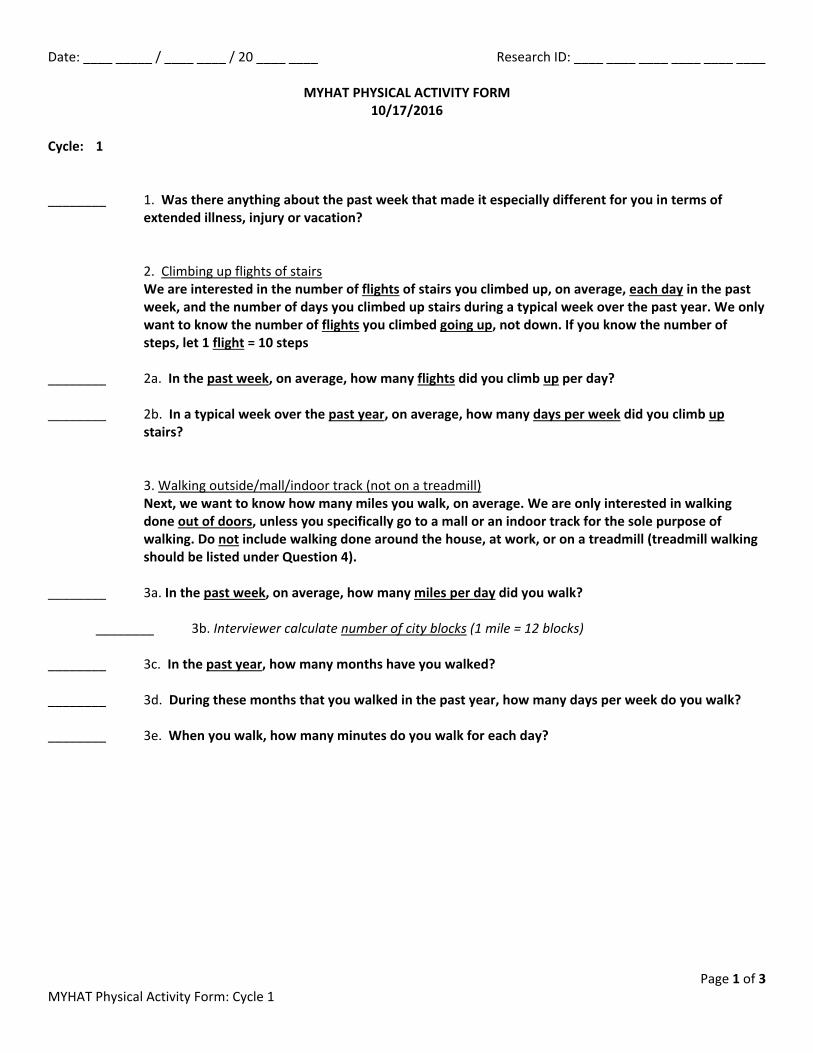
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 3 MYHAT Physical Activity Form: Cycle 1
MYHAT PHYSICAL ACTIVITY FORM 10/17/2016
Cycle: 1 ________ 1. Was there anything about the past week that made it especially different for you in terms of
extended illness, injury or vacation?
2. Climbing up flights of stairs
We are interested in the number of flights of stairs you climbed up, on average, each day in the past week, and the number of days you climbed up stairs during a typical week over the past year. We only want to know the number of flights you climbed going up, not down. If you know the number of steps, let 1 flight = 10 steps
________ 2a. In the past week, on average, how many flights did you climb up per day? ________ 2b. In a typical week over the past year, on average, how many days per week did you climb up
stairs? 3. Walking outside/mall/indoor track (not on a treadmill)
Next, we want to know how many miles you walk, on average. We are only interested in walking done out of doors, unless you specifically go to a mall or an indoor track for the sole purpose of walking. Do not include walking done around the house, at work, or on a treadmill (treadmill walking should be listed under Question 4).
________ 3a. In the past week, on average, how many miles per day did you walk?
________ 3b. Interviewer calculate number of city blocks (1 mile = 12 blocks)
________ 3c. In the past year, how many months have you walked? ________ 3d. During these months that you walked in the past year, how many days per week do you walk? ________ 3e. When you walk, how many minutes do you walk for each day?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 3 MYHAT Physical Activity Form: Cycle 1
________ 4. Exercise, sports, recreation Were there any sports, hobbies, recreational or physical activities, heavy work/chores around the house, dancing, golf, swimming, aerobics, yoga, gardening, etc. that you participated in during the past week?
Sport, Activity, Recreation, Chore, etc. Category
(see codes below)
In past week Over past year
# times/ past week
Avg. min/ episode in past week
# days/typical week over past year
Avg. min/day during that
typical week
________ 5. At least once in the past week did you engage in any regular activity long enough to work up a
sweat, get your heart thumping or get out of breath like brisk walking, jogging, bicycling, etc.? If yes, list the activity: a. _________________________________________ How many times per week? ________ b. _________________________________________ How many times per week? ________ c. _________________________________________ How many times per week? ________ d. _________________________________________ How many times per week? ________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 3 MYHAT Physical Activity Form: Cycle 1
________ 5a. At least once a week in the past year did you engage in any regular activity long enough to work
up a sweat, get your heart thumping or get out of breath like brisk walking, jogging, bicycling, etc.? a. _________________________________________ How many times per week? ________ b. _________________________________________ How many times per week? ________ c. _________________________________________ How many times per week? ________ d. _________________________________________ How many times per week? ________ ________ 6. In the past week how many hours did you spend watching TV/movies/programs/videos, etc. (on
the TV, DVD, computer, tablet/iPad, VCR, etc.)? ________ 6a. On average in the past year, how many hours per week do you spend watching
TV/movies/programs/videos, etc. (on the TV, DVD, computer, tablet/iPad, VCR, etc.)? ________ 7. In the past week, excluding time spent watching TV/movies/programs/videos (question 6) how
many hours per week did you spend sitting (e.g. working at a desk, relaxing on the couch, driving or riding in the car)?
________ 7a. On average in the past year, excluding time spent watching TV/movies/programs/videos
(question 6) how many hours per week do you spend sitting (e.g. working at a desk, relaxing on the couch, driving or riding in the car)?
________ 8. Would you say that during the past week you were:
________ 9. INTERVIEWER: Other comments? If Q1 = yes, be sure to explain what made the past week different
than a typical week here. Specify comments: ________________________________________________ _____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
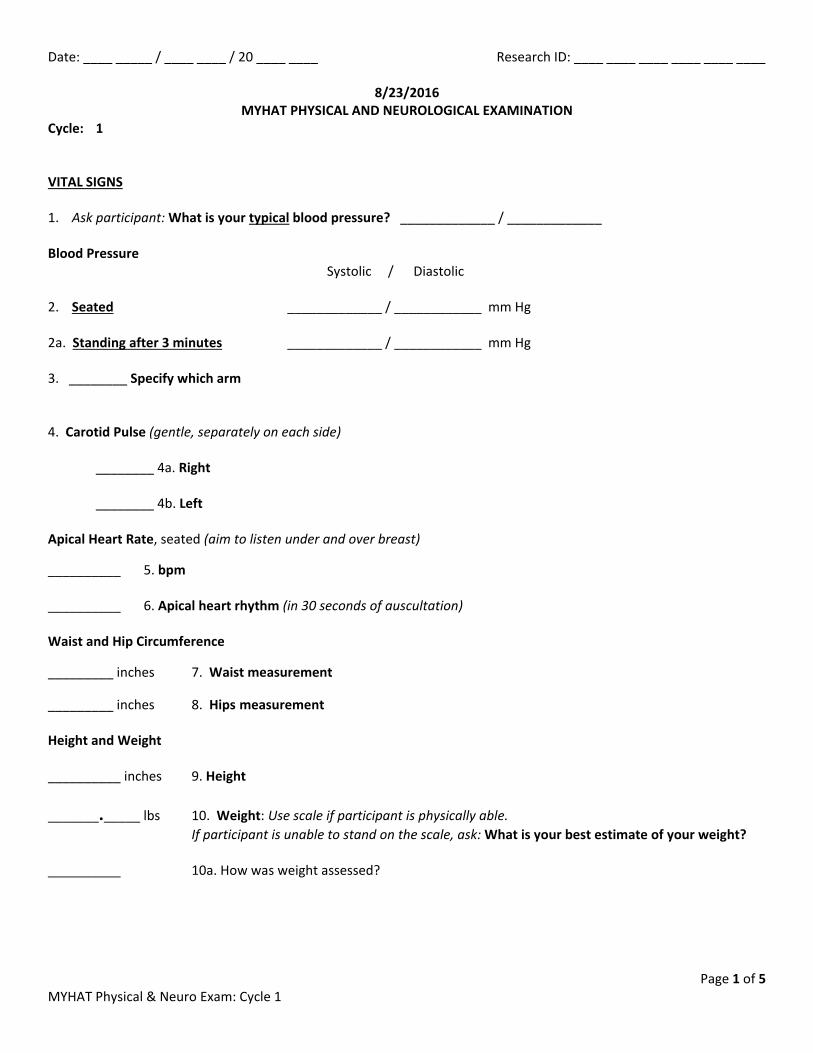
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 5 MYHAT Physical & Neuro Exam: Cycle 1
8/23/2016 MYHAT PHYSICAL AND NEUROLOGICAL EXAMINATION
Cycle: 1 VITAL SIGNS 1. Ask participant: What is your typical blood pressure? _____________ / _____________
Blood Pressure
Systolic / Diastolic 2. Seated _____________ / ____________ mm Hg 2a. Standing after 3 minutes _____________ / ____________ mm Hg
3. ________ Specify which arm 4. Carotid Pulse (gentle, separately on each side) ________ 4a. Right ________ 4b. Left Apical Heart Rate, seated (aim to listen under and over breast)
__________ 5. bpm __________ 6. Apical heart rhythm (in 30 seconds of auscultation) Waist and Hip Circumference
_________ inches 7. Waist measurement _________ inches 8. Hips measurement Height and Weight __________ inches 9. Height _______._____ lbs 10. Weight: Use scale if participant is physically able.
If participant is unable to stand on the scale, ask: What is your best estimate of your weight? __________ 10a. How was weight assessed?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 5 MYHAT Physical & Neuro Exam: Cycle 1
STANCE/POSTURE/MOBILITY [ASK PARTICIPANT TO PLEASE STAND] __________ 11. (Observe participant standing) __________ 12. Romberg: Ask participant to stand unsupported with eyes closed for 15 seconds ________ 13. Timed Get Up and Go test (code in seconds) ________ 14. Rating on Timed Get Up and Go test POSTURE AND GAIT ___________ 15. Posture and Gait Assessment
______ a. stooped /kyphotic (bent forward at the upper spine)
______ b. lordotic (leaning back with abdomen pushed forward)
______ c. wide-based support (legs far apart)
______ d. truncal sway (unsteadiness)
______ e. deviation to one side as walking (can’t walk a straight line)
______ f. slowed gait
______ g. shuffling (shortened stride length, feet don’t pass each other and usually barely lift off of the floor)
______ h. hesitancy on initiation of gait (takes a short while to make the first step)
______ i. festination (accelerating gait, leaning forward and sometimes has difficulty stopping)
______ j. propulsion (falling forward)
______ k. turning en bloc (turning with feet together rather than a three-point turn)
______ l. lack of arm swing (keeps one or both arms down by side, code “no” if assist device)
______ m. waddling gait (feet turned out and wide-base of support)
______ n. foot drop (toe(s) do not lift up but are dragged forward, foot may slap the ground when lowered)
______ o. circumduction (one leg is dragged around in a semicircle/lack of hip flexion)
______ p. slapping down feet with each step
______ q. limp if yes (to limp), is it due to: ______ r. pain ______ s. weakness ______ s2. stiffness ______ t. other, specify ___________________________________________________________
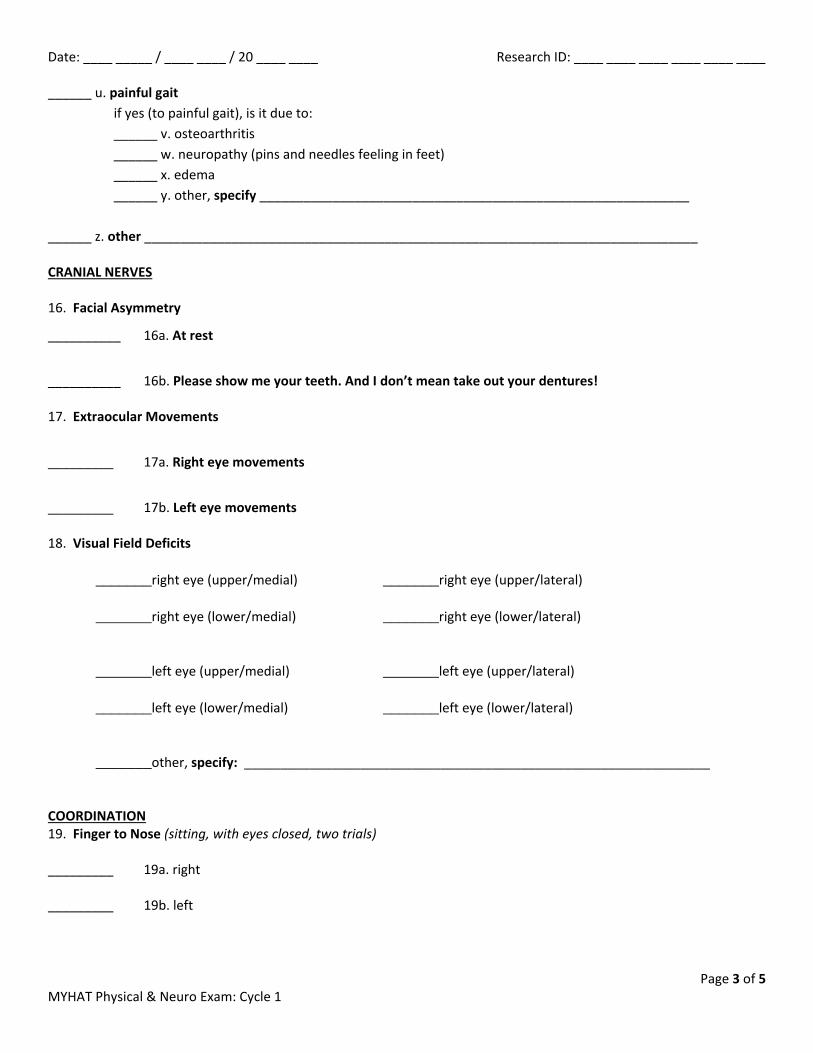
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 5 MYHAT Physical & Neuro Exam: Cycle 1
______ u. painful gait if yes (to painful gait), is it due to: ______ v. osteoarthritis ______ w. neuropathy (pins and needles feeling in feet) ______ x. edema ______ y. other, specify ___________________________________________________________
______ z. other ____________________________________________________________________________ CRANIAL NERVES 16. Facial Asymmetry
__________ 16a. At rest
__________ 16b. Please show me your teeth. And I don’t mean take out your dentures! 17. Extraocular Movements
_________ 17a. Right eye movements
_________ 17b. Left eye movements
18. Visual Field Deficits
_______right eye (upper/medial) _______right eye (upper/lateral)
_______right eye (lower/medial) _______right eye (lower/lateral)
_______left eye (upper/medial) _______left eye (upper/lateral)
_______left eye (lower/medial) _______left eye (lower/lateral) _______other, specify: ________________________________________________________________
COORDINATION 19. Finger to Nose (sitting, with eyes closed, two trials) _________ 19a. right _________ 19b. left

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 4 of 5 MYHAT Physical & Neuro Exam: Cycle 1
STRENGTH _________ 20. Deltoids, muscle strength (Push down on elbows with arms flexed and horizontal)
_________ 21. Biceps, muscle strength (Pull on forearms with arms flexed at chest) _________ 22. Quadriceps, muscle strength (Push on lower legs as participant attempts to straighten at the knees) TONE 23. Motor Tone Abnormality (check in wrist and elbow) _________ 23a. right cogwheeling
_________ 23b. right lead pipe rigidity
_________ 23c. right other, specify: ______________________________________________(contracture, flaccidity)
_________ 23d. left cogwheeling
_________ 23e. left lead pipe rigidity
_________ 23f. left other, specify: ______________________________________________(contracture, flaccidity)
TREMOR 24. Resting Tremor (Have participant sit with arms resting in lap) _________ 24a. Extremities _________ 24b. Head DEEP TENDON REFLEXES (DTRs) 25. Biceps
_________ 25a. Right biceps
_________ 25b. Left biceps
_________ 25c. Right biceps versus left biceps, DTRs (Swing hammer with wrist-action)
26. Patella
_________ 26a. Right patella
_________ 26b. Left patella
_________ 26c. Right patella versus left patella, DTRs

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 5 of 5 MYHAT Physical & Neuro Exam: Cycle 1
INERVIEWER’S IMPRESSION _________ 27. Myoclonus _________ 28. Level of Consciousness _________ 29. Cooperativeness with neurological exam _________ 30. Any other general comments? (must explain all negative codes in comments)
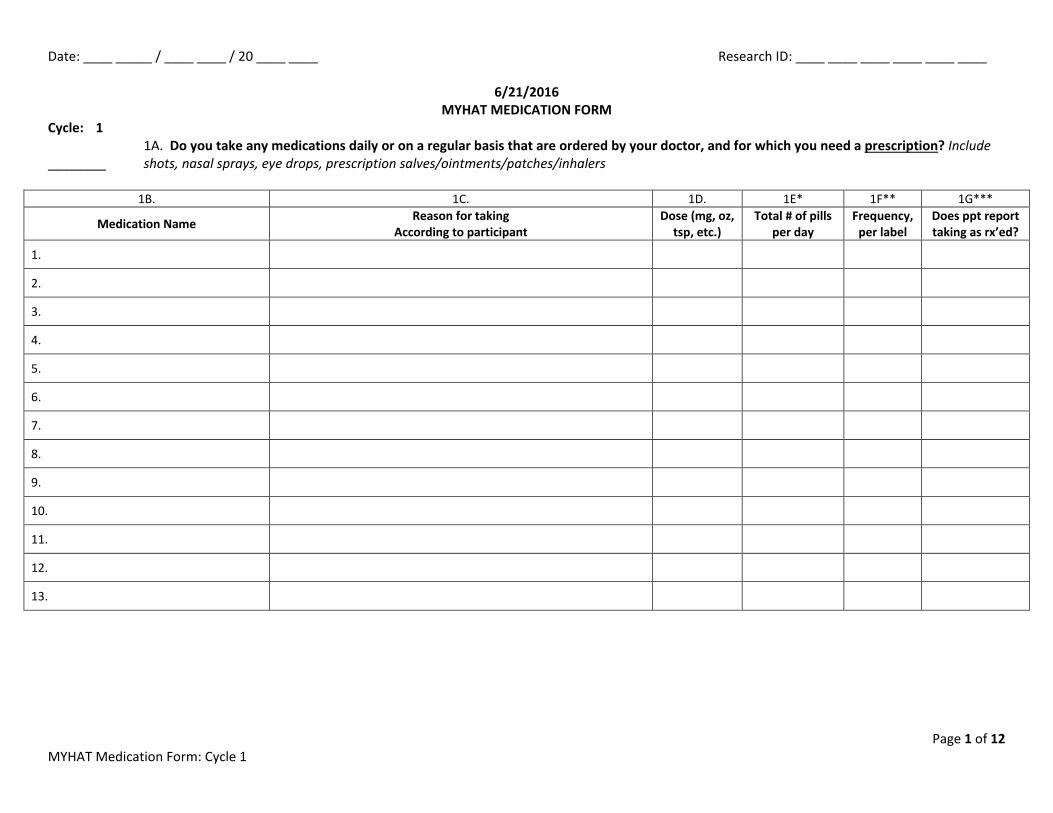
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 12 MYHAT Medication Form: Cycle 1
6/21/2016 MYHAT MEDICATION FORM
Cycle: 1 1A. Do you take any medications daily or on a regular basis that are ordered by your doctor, and for which you need a prescription? Include ________ shots, nasal sprays, eye drops, prescription salves/ointments/patches/inhalers
1B. 1C. 1D. 1E* 1F** 1G***
Medication Name Reason for taking According to participant
Dose (mg, oz, tsp, etc.)
Total # of pills per day
Frequency, per label
Does ppt report taking as rx’ed?
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 12 MYHAT Medication Form: Cycle 1
2A. Do you take any medications regularly that are ordered by your doctor but you do not need a prescription? (examples: aspirin, vitamin E, ________ Motrin, multi-vitamin)
2B. 2C. 2D. 2E* 2F**
Medication Name Reason for taking According to participant
Dose (mg, oz, tsp, etc.)
Total # of pills per day
Frequency, per label
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 12 MYHAT Medication Form: Cycle 1
3A. Do you take other medications ordered by your doctor that you only take as you need? (i.e. not regularly, PRN) (examples: sleeping ________ pill, pain pill, either prescription or over-the-counter drug)
3B. 3C. 3D. 3E*
Medication Name Reason for taking According to participant
Dose (mg, oz, tsp, etc.) Frequency
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 4 of 12 MYHAT Medication Form: Cycle 1
4A. Do you take OVER-THE-COUNTER medications not prescribed by a doctor? e.g. for sleep, headaches, arthritis, constipation, heartburn, ________ colds, itching/rashes, vitamins, tonics, herbs, etc. DO NOT INCLUDE PRESCRIPTIONS MEDS WHICH A PHARMACY FILLS WITHOUT A PRESCRIPTION
4B. 4C. 4D.* 4E.**
Medication Name Reason for taking According to participant Frequency Source
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 5 of 12 MYHAT Medication Form: Cycle 1
________ 5. INTERVIEWER: Did all of the explanations/reasons given by the participant/informant (circle which) make sense?
________ 6. INTERVIEWER: On a scale of 1 to 5, how you would assess the participant’s/informant’s (circle which) knowledge of the medications they use compared to other participants you have interviewed. (Code 1-5 if taking any medications (Rx, doctor-ordered, PRN or OTC))
________ 7. Where do you most often obtain/get/buy your prescription medications? (code only if taking any Rx medications) ________ 8. Do you have insurance to pay for your prescription medications? (Ask everyone regardless of medication use) ________ 8a. Do you have PACE or PACENET?
________ 8b. If you needed the insurance to pay, would it (the insurance) pay for the entire amount of your prescription medication or would you have to pay for some of it yourself? That is, do you have a co-pay?
________ 9. How much do you have to pay out of your own pocket for all of your prescriptions every month? (If they say, for example, $100 every three
months, divide by 3 so amount in answer is for ONE month) (If not taking any Rx drugs, code “0” for $0) Enter monthly amount in dollars or -2 if they do not have to pay anything (Q8b is 2)
________ 9a. Is that amount for your own prescriptions or for other people as well as yourself? Write in the number of people; self = 1 *********************************************************************************************************************************** ________ 10. Do you take care of setting up a schedule for taking your own medication? ________ 11. Does anyone help you manage your medications? ________ 11a. If yes, Who helps you manage or manages you medications for you? ________ 12. Do you have a system or systems for keeping track of the prescription medications you take regularly?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 6 of 12 MYHAT Medication Form: Cycle 1
13. What type of system or systems do you use? (Code all applicable systems.)
_____ 13a. multi-compartment pillbox
_____ 13b. single compartment pillbox
_____ 13c. checklist
_____ 13d. calendar
_____ 13e. laying out pills at meal time
_____ 13f. laying out pills in the morning for the day
_____ 13g. placing medication in a location that will remind you to take it at the appropriate time
_____ 13h. taking medications under supervision of family member, friend or caregiver
_____ 13i. other, specify: ____________________________________________________________
________ 14. In the past year, have you usually taken your medications as directed by your doctor? (Note: asking about the past year is different than the drugs asked about in the first three questions. Ask this question regardless of whether any medications reported in the first three questions)
________ 15. In the past year, have you ever forgotten to take your medicine? ________ 16. If yes, How often would you say this happens? ________ 17. What do you do when you skip a dose? ________ 18. Have you deliberately taken a medication other than how a doctor prescribed it? (Ask everyone regardless of medication use) 19. If yes, Did you … (indicate all applicable) _____ 19a. stop taking it
_____ 19b. take less than prescribed
_____ 19c. take more than prescribed

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 7 of 12 MYHAT Medication Form: Cycle 1
________ 20. How many medications did you deliberately take other than how a doctor prescribed them? ________ 21. For how long did you not take it as prescribed? 22. Why did you not take it as prescribed? (code all applicable) _____ 22a. caused side effects
_____ 22b. felt it wasn’t helping
_____ 22c. prescription ran out and didn’t have it refilled
_____ 22d. too expensive
_____ 22e. didn’t go back to the doctor
_____ 22f. read or heard something negative about the medication
_____ 22g. taking too many medications
_____ 22h. don’t like to take medication
_____ 22i. felt I didn’t need it or didn’t need it anymore
_____ 22j. other, specify: _________________________________________________
________ 23. In the past year, have you ever taken someone else’s prescription medication on purpose? (Ask everyone regardless of medication use) ________ 24. How often does this occur? ________ 25. INTERVIEWER’S IMPRESSION of compliance/adherence: On a scale of 1 to 5, how do you rate this participant’s medication compliance for Rx
and doctor-ordered medications?
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 8 of 12 MYHAT Medication Form: Cycle 1
________ 26. Have you had a problem such as an allergy or bad reaction or major side effect with any of the medications you have taken in the past year? (ADR)
________ 27. Are you currently taking any of the following medications to help your memory? _____ 27a. Aricept (donepezil) _____ 27g. Hydergine
_____ 27b. Cognex (tacrine) _____ 27h. Exelon (rivastigimine)
_____ 27c. Estrogen replacement _____ 27i. Razadyne (Galantamine Hbr) (formerly Renimyl)
_____ 27d. NSAID for memory but NOT _____ 27j. Namenda
for pain or inflammation _____ 27k. other, specify: __________________________________________
_____ 27e. Vitamin E ____________________________________________________
_____ 27f. Gingko

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 9 of 12 MYHAT Medication Form: Cycle 1
Discontinued medications (if any) ________ 28. Over the past year, did you stop taking any medications that you had previously been taking regularly? If yes, ask: Do you still have a bottle or package of this drug and if so, would you please show it to me? (If available, take information from
bottle/package label)
28b. Name of medication
28c. Rx or OTC? Rx = 1; OTC = 2
28d. Taking currently?
1 = yes; 0 = no
28e. Date most recently stopped
28f. Why stopped? Use code below*
28g. How long taken,
before being stopped? (In months)
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 10 of 12 MYHAT Medication Form: Cycle 1
________ 29. Have you ever taken any of the medications or supplements listed on this card? (Show the hormone/estrogen card only to women)
29b. Name of medication 29c. Rx or OTC? 1 = Rx; 2 = OTC
29c. At what age did you start taking?
29d. Taking currently?
1 = yes; 0 = no 29e. Date most recently stopped
29f. Why did you stop? Use code below*
29g. How long did you take or have you been taking? (code in months)
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 11 of 12 MYHAT Medication Form: Cycle 1
________ 30. Did you ever take any medications (prescription or OTC) almost every day for a month or more to help you sleep? If yes, Name of medication How long did you take altogether? How long ago did you stop? (if stopped)
1a. ___________________________ 1b. _____ weeks or _____ months or ______ years 1c. _____ weeks or _____ months or ______ years
2a. ___________________________ 2b. _____ weeks or _____ months or ______ years 2c. _____ weeks or _____ months or ______ years
3a. ___________________________ 3b. _____ weeks or _____ months or ______ years 3c. _____ weeks or _____ months or ______ years
4a. ___________________________ 4b. _____ weeks or _____ months or ______ years 4c. _____ weeks or _____ months or ______ years
________ 31. Did you ever take any medications (prescription or OTC) almost every day for a month or more to control or relieve pain?
If yes, Name of medication How long did you take altogether? How long ago did you stop? (if stopped)
1a. ___________________________ 1b. _____ weeks or _____ months or ______ years 1c. _____ weeks or _____ months or ______ years
2a. ___________________________ 2b. _____ weeks or _____ months or ______ years 2c. _____ weeks or _____ months or ______ years
3a. ___________________________ 3b. _____ weeks or _____ months or ______ years 3c. _____ weeks or _____ months or ______ years
4a. ___________________________ 4b. _____ weeks or _____ months or ______ years 4c. _____ weeks or _____ months or ______ years
________ 32. Did you ever take any medications (prescription or OTC) almost every day for a month or more to control or relieve anxiety, nerves or stress?
If yes, Name of medication How long did you take altogether? How long ago did you stop? (if stopped)
1a. ___________________________ 1b. _____ weeks or _____ months or ______ years 1c. _____ weeks or _____ months or ______ years
2a. ___________________________ 2b. _____ weeks or _____ months or ______ years 2c. _____ weeks or _____ months or ______ years
3a. ___________________________ 3b. _____ weeks or _____ months or ______ years 3c. _____ weeks or _____ months or ______ years
4a. ___________________________ 4b. _____ weeks or _____ months or ______ years 4c. _____ weeks or _____ months or ______ years

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 12 of 12 MYHAT Medication Form: Cycle 1
________ 33. INTERVIEWER’S IMPRESSION: Does participant seem confident about recalling this information or does he/she appear to be guessing, and does the information appear valid/plausible?
________ 34. INTERVIEWER: Any general comments? ________ 35. INTERVIEWER’S IMPRESSION: Do you feel past medication information is mostly reliable?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT mCES-D: Cycle 1
6/21/2016 MYHAT mCES-D QUESTIONS
Cycle: 1 I’m going to ask you some questions about how you have been feeling over the past week. Some of the questions may apply to you and others may not. “Most of the time” is defined as the equivalent of 3 or more days in the past week.
NO
YES
During the past week, most of the time...
DEP1: were you bothered by things that don’t usually bother you?
DEP2: did you not feel like eating? Was your appetite poor?
DEP3: did you feel that you could not shake off the blues even with the help of your
family or friends?
DEP4: did you feel you were just as good as other people?
DEP5: did you have trouble keeping your mind on what you were doing?
DEP6: did you feel depressed?
DEP7: did you feel that everything you did was an effort?
DEP8: did you feel hopeful about the future?
DEP9: did you think your life has been a failure?
DEP10. did you feel fearful?
DEP11. was your sleep restless?
DEP12. were you happy?
DEP13. did you talk less than usual?
DEP14. did you feel lonely?
DEP15. did you feel people were unfriendly?
DEP16. did you enjoy life?
DEP17. did you have crying spells?
DEP18. did you feel sad?
DEP19. did you feel that people disliked you?
DEP20. did you feel you could not get going?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT mCES-D: Cycle 1
________ ANX1. Would you describe yourself as a worrier?
________ ANX1a. Would you say that you easily become nervous or upset? ________ ANX1b. Would you say that you have always been this way, or is this a recent change? ________ INT1. INTERVIEWER IMPRESSION: Did you feel the depression questions were mostly accurate? ________ INT2. INTERVIEWER IMPRESSION: Does the participant appear depressed to you? ________ INT3. INTERVIEWER: Any other general comments?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 5 MYHAT Health Services Utilization: Cycle 1
6/21/2016 MYHAT HEALTH SERVICES UTLIZATION
Cycle: 1 Now I want to ask you some questions about the kinds of help and services that you are or have been getting. ________ 1. Is there a particular doctor whom you consider your primary physician? 2. If you have a PCP, what is his or her name? _____________________________________________________________________________________ ________ 3. How long has it been since you last saw this doctor? ________ 4. In the past year, have you had a really complete checkup with your doctor and discussed all of your
problems and medications with him/her? ________ 5. If yes to Q4, how long ago did you have your checkup? ________ 6. If no to Q4, how long ago do you think you had your last checkup? (code in years)

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 5 MYHAT Health Services Utilization: Cycle 1
________ 7. In the past year, have you had any office/outpatient visits to any other doctors?
7a. Doctor’s name (Only last name, no “MD”)
7b. Reason for visit (problem, diagnosis, procedure, etc.)
7c. Specialty (code)*
1
2
3
4
5
6
7
________ 8. Have you seen any kind of mental health specialist in the past year? (e.g. a psychiatrist,
psychologist, counselor, therapist, psychiatric social worker, clergyman but specifically for counseling)
8b. Provider’s Name
8c. Reason for visit
8d. Provider type (code)**
________ 9. Have you had to go to the emergency room (or urgent care or Med Express) in the past year? ________ 9a. If yes, how many times? 9b. What were the reasons?
9b.
9c. Reason for ER (or Urgent Care, Med Express) visit
9d. Category (code(s))***
1.
2.
3.
4.
5.
6.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 5 MYHAT Health Services Utilization: Cycle 1
________ 10. Have you been admitted to a hospital in the past year? ________ 10a. If yes, how many times? 10b. What were the reasons?
10b.
10c. Reason for Hospitalization
10d. Category (code)+
1.
2.
3.
4.
5.
6.
________ 11. Have you had a CT scan or MRI of the head or any brain scan in the past five years? ________ 11a. If yes, which one? 11b. Where? (e.g. hospital/clinic name. BE SPECIFIC. Write address if known) ________ 11c. Was this scan taken during an inpatient stay? ________ 11d. Was this scan taken during an outpatient stay? 11e. Approximately when was the scan done? ____ ____ / ____ ____ / ____ ____ ____ ____
11f. Why was this scan done? Specify reason if known: _____________________________________________________
______________________________________________________________________________________________
________ 11g. Would you give us consent to look at the results of the test? ________ 12. Have you made any legal or formal plans for what you would want done if you became severely ill
or disabled? ________ 12a. Living will ________ 12b. Advance Directives ________ 12c. Medical Power of Attorney ________ 12d. Financial Power of Attorney ________ 12e. Long-term care insurance ________ 12f. Other, specify: ____________________________________________________________________
e.g. power of attorney, durable power of attorney
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 4 of 5 MYHAT Health Services Utilization: Cycle 1
________ 13. INTERVIEWER’S IMPRESSION: Do you feel the Health Service Utilization and related information is
mostly accurate? ________ 14. INTERVIEWER: Any other general comments? ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________
______________________________________________________________________________
________ Were any medical records requested? (this question previously recorded on the Med Record Form) If medical records are requested, be sure to fill out a Medical Record Form from the forms cubby and give to Kathy.

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 1 MYHAT STOFHLA
5/5/2017
Short Test of Functional Health Literacy in Adults (STOFHLA) Cycle: 1 2 10 11 12 Hand the participant the reading comprehension passages and preface the exercise with these instructions: “Here are some medical instructions that you or anyone might see around a doctor office or hospital. There are two passages and each one is like a brochure that you would read all the way through. The passages are in written in sentences with some missing words. Where a word is missing, a blank line in drawn, and four possible words that could go in the blank are printed below. I want you to figure out which of those four words should go in the blank- which word makes the sentence make sense. When you think you know which one it is, circle the letter in front of the word and go onto the next one.”
______ Comments? (1 = yes, 0 = no) _______________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
(1) (2)
Last Question Answered (If ppt finished test in 7 minutes, record 36)
Passage A Total Points
Passage B Total Points
Grand Total: A+B Total Points

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Social Support: Cycle 1
6/21/2016 MYHAT SOCIAL SUPPORT
Cycle: 1
________ 1. When you feel lonely, are there several people you can talk to?
________ 2. Do you feel close enough to any family or friends that you could confide in the about anydifficulties or concerns?
________ 3. How many people (approximately) is that?
________ 4. How satisfied are you with the support and encouragement you receive from the persons you justmentioned?
________ 5. If you needed advice (suggestions) on dealing with a personal problem, do you know someone youcan turn to; someone whose advice you really trust?
________ 6. At present, does anyone regularly help you with things like household chores, shopping, bathing,filling out forms, doing repairs, etc.?
________ 7a. If you were ever (or are) sick or disabled, would there be at least one person to take care of you?
7b. Who would that person (or those persons) be who could take care of you?
Relationship to Subject (write code) Age Specify (if other)
1. ___________________________ ______ __________________________
2. ___________________________ ______ __________________________
3. ___________________________ ______ __________________________
4. ___________________________ ______ __________________________
5. ___________________________ ______ __________________________
6. ___________________________ ______ __________________________
7. ___________________________ ______ __________________________
________ 8. At present, does anyone regularly depend on you for help with things like shopping, cooking?
________ 9. Do you meet or talk with family and friends as often as you would like?
________ 10. Do you belong to any organizations such as churches, lodges, societies, volunteer groups, etc.?
________ 10a. How often do you attend meetings or activities related to all these groups put together?
________ 11. How often do you see family or friends who do not live in the same house as you?
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Social Support: Cycle 1
________ 12. Overall, do you get as much help and support as you need with any difficulties (concerns, problems, needs) that you may have?
________ 13. INTERVIEWER’S IMPRESSION: DO YOU FEEL THE SOCIAL SUPPORT QUESTIONS WERE ANSWERED
MOSTLY ACCURATELY? ________ 14. INTERVIEWER’S IMPRESSION: Any general comments?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Pet Form: Cycle 1
6/21/2016 MYHAT PET FORM
Cycle: 1 ________ 1. INTERVIEWER’S ASSESSMENT: Does the participant live alone? ________ 2a. Do you currently have a pet? ________ 2c. Have you lost a pet in the past year? ________ 2c1. What was the reason? ________ 2c2. If unable to care for/gave away, specify reason: ________ 2b. Are you responsible (50% or more) for a pet or pets (your own or someone else’s)? 3. What type of pet(s) are you responsible for and how many? (code the number of each pet, code 0 if none of that pet) # own/care for Type
________ a. dog
________ b. cat
________ c. bird
________ d. fish
________ e. other, specify: __________________________________________________________
________ f. other, specify: __________________________________________________________
________ g. other, specify: __________________________________________________________
________ 4. Are you responsible for feeding your pet(s) daily (or regularly, if applicable)? ________ 5. Are you responsible for cleaning the litter box, bird cage or fish tank or for putting the dog
outdoors for toileting? (if other pet, ask relevant question) ________ 6. Are you responsible for bathing your pet (if relevant)? ________ 7. Are you responsible for giving medications to your pet? (if not on any medications, code -2) ________ 8. Are you responsible for taking your pet to the vet and/or seek appropriate medical care? 9. Who assists you with these chores? What is this person’s relationship to you? First person: __________________________________________________________________________
Second person (if applicable): ____________________________________________________________
Third person (if applicable): ____________________________________________________________
Fourth person (if applicable): ____________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Pet Form: Cycle 1
________ 10. INTERVIEWER IMPRESSION: Visual or other sensory confirmation: Did you see the pet(s)? ________ 11. INTERVIEWER IMPRESSION: If pet(s) seen, does the pet(s) appear to be well taken care of? ________ 12. Any general comments? _____________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 4 MYHAT Sports-Related Head Trauma: Cycle 1
6/21/2016 MYHAT SPORTS-RELATED HEAD TRAUMA
Cycle: 1 ________ 1. Did you play any sports as a child or adult? 2. Which sports? ________ 2a. Football (American football)
________ 2b. Soccer (futbol)
________ 2c. Basketball
________ 2d. Baseball
________ 2e. Field Hockey
________ 2f. Dek Hockey
________ 2g. Ice Hockey
________ 2h. Tennis
________ 2i. Boxing
________ 2j. Swimming
________ 2k. Golf
________ 2l. Skiing
________ 2m. Wrestling
________ 2n. Other, specify: ____________________________________________________________
________ 3. Did you ever get hit in the head or fall and become dazed or woozy or lose consciousness while
playing this/any of these sports? Which sport(s) were you playing when this happened?
________ 3a. Football (American football)
________ 3b. Soccer (futbol)
________ 3c. Basketball
________ 3d. Baseball
________ 3e. Field Hockey
________ 3f. Dek Hockey
________ 3g. Ice Hockey
________ 3h. Tennis
________ 3i. Boxing

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 4 MYHAT Sports-Related Head Trauma: Cycle 1
________ 3j. Swimming
________ 3k. Golf
________ 3l. Skiing
________ 3m. Wrestling
________ 3n. Other, specify: ____________________________________________________________
4. When in your life did you play this sport/these sports that you were hit in the head or fell and you became dazed or woozy or lost consciousness? Code all that apply
________ 4a. Before high school (primary or middle or junior high school)
________ 4b. High school
________ 4c. College
________ 4d. Organized leagues, but outside of school (e.g. Little League)
________ 4e. Military
________ 4f. Street/Pickup games
________ 4g. Other, specify: ___________________________________________________________________
________ 5. At what age did you begin playing this sport/these sports? Code in years beginning with the earliest
sport. ________ 6. Do you still play this sport/these sports? ________ 7. At what age did you quit playing this sport/these sports? 8. Why did you quit playing this sport/these sports? ________ 8a. Left School
________ 8b. Just got away from it/grew up/grew old
________ 8c. Not further opportunities
________ 8d. Was hurt/injured, specify injury:
________ 8d1. Head
________ 8d2. Neck
________ 8d3. Upper limb (shoulder, elbow, wrist, arm, forearm, hand)
________ 8d4. Lower limb (hip, knee, ankle, foot, leg, thigh)
________ 8d5. Other, specify: ______________________________________________
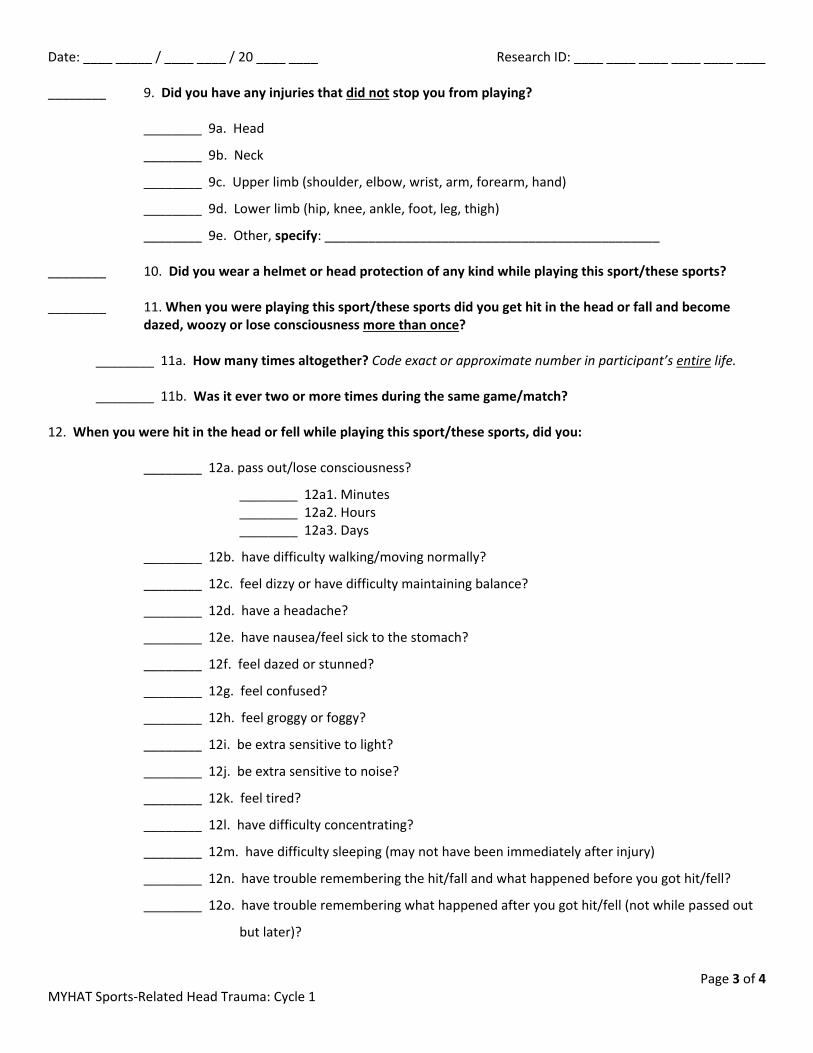
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 3 of 4 MYHAT Sports-Related Head Trauma: Cycle 1
________ 9. Did you have any injuries that did not stop you from playing? ________ 9a. Head
________ 9b. Neck
________ 9c. Upper limb (shoulder, elbow, wrist, arm, forearm, hand)
________ 9d. Lower limb (hip, knee, ankle, foot, leg, thigh)
________ 9e. Other, specify: ______________________________________________ ________ 10. Did you wear a helmet or head protection of any kind while playing this sport/these sports? ________ 11. When you were playing this sport/these sports did you get hit in the head or fall and become
dazed, woozy or lose consciousness more than once?
________ 11a. How many times altogether? Code exact or approximate number in participant’s entire life. ________ 11b. Was it ever two or more times during the same game/match?
12. When you were hit in the head or fell while playing this sport/these sports, did you: ________ 12a. pass out/lose consciousness?
________ 12a1. Minutes ________ 12a2. Hours ________ 12a3. Days
________ 12b. have difficulty walking/moving normally?
________ 12c. feel dizzy or have difficulty maintaining balance?
________ 12d. have a headache?
________ 12e. have nausea/feel sick to the stomach?
________ 12f. feel dazed or stunned?
________ 12g. feel confused?
________ 12h. feel groggy or foggy?
________ 12i. be extra sensitive to light?
________ 12j. be extra sensitive to noise?
________ 12k. feel tired?
________ 12l. have difficulty concentrating?
________ 12m. have difficulty sleeping (may not have been immediately after injury)
________ 12n. have trouble remembering the hit/fall and what happened before you got hit/fell?
________ 12o. have trouble remembering what happened after you got hit/fell (not while passed out
but later)?
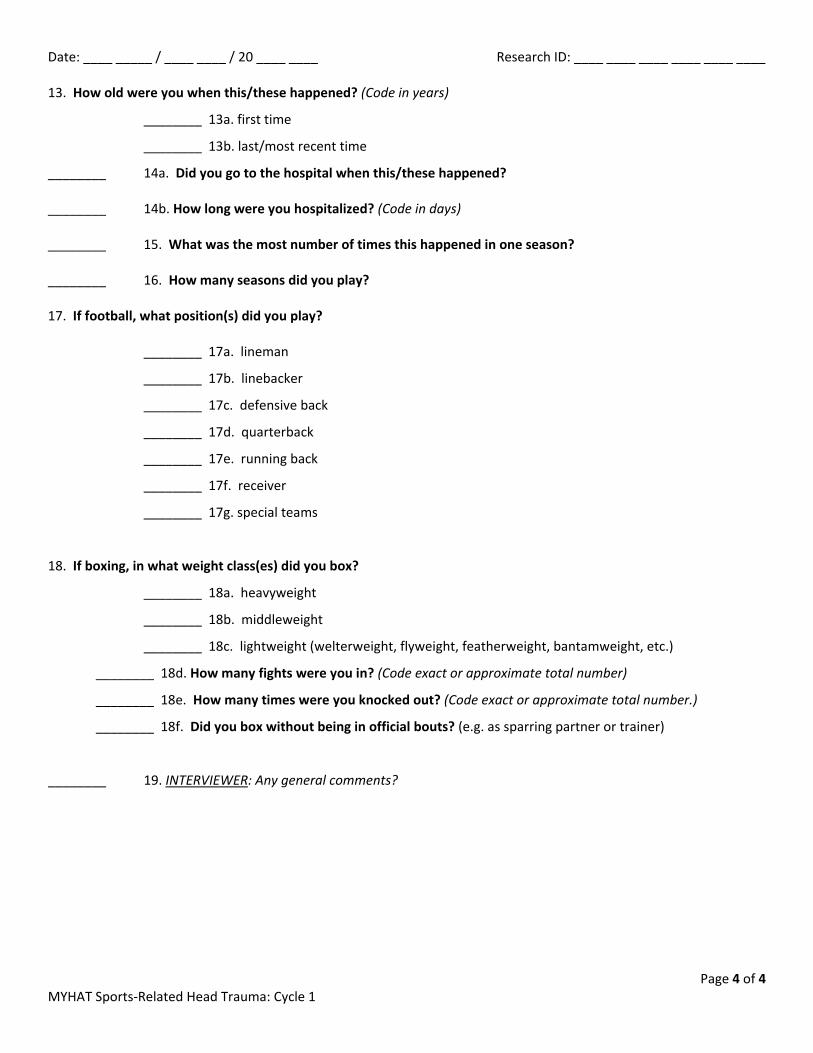
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 4 of 4 MYHAT Sports-Related Head Trauma: Cycle 1
13. How old were you when this/these happened? (Code in years)
________ 13a. first time
________ 13b. last/most recent time
________ 14a. Did you go to the hospital when this/these happened? ________ 14b. How long were you hospitalized? (Code in days) ________ 15. What was the most number of times this happened in one season? ________ 16. How many seasons did you play? 17. If football, what position(s) did you play? ________ 17a. lineman
________ 17b. linebacker
________ 17c. defensive back
________ 17d. quarterback
________ 17e. running back
________ 17f. receiver
________ 17g. special teams
18. If boxing, in what weight class(es) did you box?
________ 18a. heavyweight
________ 18b. middleweight
________ 18c. lightweight (welterweight, flyweight, featherweight, bantamweight, etc.)
________ 18d. How many fights were you in? (Code exact or approximate total number)
________ 18e. How many times were you knocked out? (Code exact or approximate total number.)
________ 18f. Did you box without being in official bouts? (e.g. as sparring partner or trainer) ________ 19. INTERVIEWER: Any general comments?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Caffeine Form: Cycle 1
6/21/2016 MYHAT CAFFEINE FORM
Cycle: 1 ________ 1. Do you ever or did you used to drink any caffeinated drinks? (Coffee, tea, soda)
________ 2. Do you ever or did you used to drink any decaffeinated drinks? (Coffee, tea, NOT soda) ________ 3. How many years in total have you been drinking caffeinated drinks? ________ 4. How many years in total have you been drinking decaffeinated tea or coffee?
Note: Count 12 oz. or more (usually medium size or bigger) as two cups of coffee and espresso drinks made with double shots of espresso as 2 cups of coffee.
Current Use
Coffee Tea Soda (including
diet)
Decaf Coffee
Decaf Tea
5. How many cups/drinks of _______ (coffee, tea, soda, decaf coffee, decaf/herbal tea) do you have per typical day?
6. How many days per typical week do you drink ___? (coffee, tea, soda, decaf coffee, decaf/herbal tea)
Actual response (not for data entry): ____________________________________________________________________
__________________________________________________________________________________________________
Past Use
Coffee Tea Soda (including
diet)
Decaf Coffee
Decaf Tea
7. How many cups/drinks of _____ (coffee, tea, soda, decaf coffee, decaf/herbal tea) did you usually have per typical day?
8. How many days per typical week did you usually drink _____? (coffee, tea, soda, decaf coffee, decaf/herbal tea)
Actual response (not for data entry): ____________________________________________________________________
__________________________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Caffeine Form: Cycle 1
________ 9. Do you eat or drink chocolate?
________ 9a. Do you eat milk chocolate?
________ 9b. Do you eat dark/bittersweet chocolate?
________ 9c. Do you eat chocolate-containing foods (cakes, desserts)?
________ 9d. Do you drink chocolate-containing drinks (chocolate milk, hot cocoa)?
________ 9e. Thinking about all the sources of chocolate, how often do you eat/drink chocolate? ________ 9.5. INTERVIEWER: Did participant describe a seasonal caffeine/decaf pattern?
________ 10. Additional comments? If yes, specify: ___________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Social Norms: Cycle 1
6/21/2016 MYHAT SOCIAL NORMS QUESTIONNAIRE
Cycle: 1 The following is a list of behaviors that a person might engage in. Please decide whether or not it would be socially acceptable and appropriate to do these things in the mainstream culture of the United States (in other words, most people in general) and answer yes or no to each. Think about these questions as if they were occurring in the presence of a stranger or acquaintance (such as a coworker), NOT a close friend or family member.
Participant Response
No / Yes 1. Tell a stranger you don’t like their hairstyle?
No / Yes 2. Spit on the floor?
No / Yes 3. Blow your nose in public?
No / Yes 4. Ask a coworker their age?
No / Yes 5. Cry during a movie at the theater?
No / Yes 6. Cut in line if you are in a hurry?
No / Yes 7. Laugh when you yourself trip and fall?
No / Yes 8. Eat pasta with your fingers?
No / Yes 9. Tell a coworker your age?
No / Yes 10. Tell someone your opinion of a movie they haven’t seen?
No / Yes 11. Laugh when someone else trips and falls?
No / Yes 12. Wear the same shirt every day?
No / Yes 13. Keep money you find on the sidewalk?
No / Yes 14. Pick your nose in public?
No / Yes 15. Tell a coworker you think they are overweight?
No / Yes 16. Eat ribs with your fingers?
No / Yes 17. Tell a stranger you like their hairstyle?
No / Yes 18. Wear the same shirt twice in two weeks?
No / Yes 19. Tell someone the ending of a movie they haven’t seen?
No / Yes 20. Hug a stranger without asking first?
No / Yes 21. Talk out loud during a movie in the theater?
No / Yes 22. Tell a coworker you think they have lost weight? _____________ Total (not for data entry)

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Social Norms: Cycle 1
INTERVIEWER: ________ 23. SNQ Total Score: [22 – (total sum of scores)]
________ 24. Break Score [total sum of items ( • ) ]
________ 25. Over-adhere Score [total sum of items ( + ) ]
26. Yes/No Ratio Score:
________ 26a. Total Number of “Yes”
________ 26b. Total Number of “No”
____.____ 26c. Total yes (26a) / Total no (26b)
________ 26c.1 Is the yes/no ratio score < 0.3 or ≥ 5?
________ 26c.2 Are all the responses the same?
________ 27. Any additional comments?

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 1 MYHAT Brain Scan Interest: Cycle 1
6/21/2016 MYHAT BRAIN SCAN INTEREST
Cycle: 1
________
________
________
________
________
________
________
________
________
________
________
________
1. In the future, we may conduct a study to better understand the health of the brain in relation to memory and thinking ability. If in the future, you have the opportunity to participate in a brain scan study at the University of Pittsburgh, would you be interested in learning more about the study? You would be provided transportation and paid for your time.
Indicate factors contributing to decision:
2a. Travel to Pittsburgh/Oakland
2b. The brain scanning procedure (e.g. open or closed scan)
2c. Possible side effects
2d. Whether the results of the scan are provided
2e. State of health
2f. Payment amount
2g. Time available (e.g. too busy with other responsibilities)
2h. Time of year (i.e. winter, summer, etc.)
2i. Other reason, please specify:
2j. Other reason, please specify:
3. INTERVIEWER’S IMPRESSION: Any general comments?
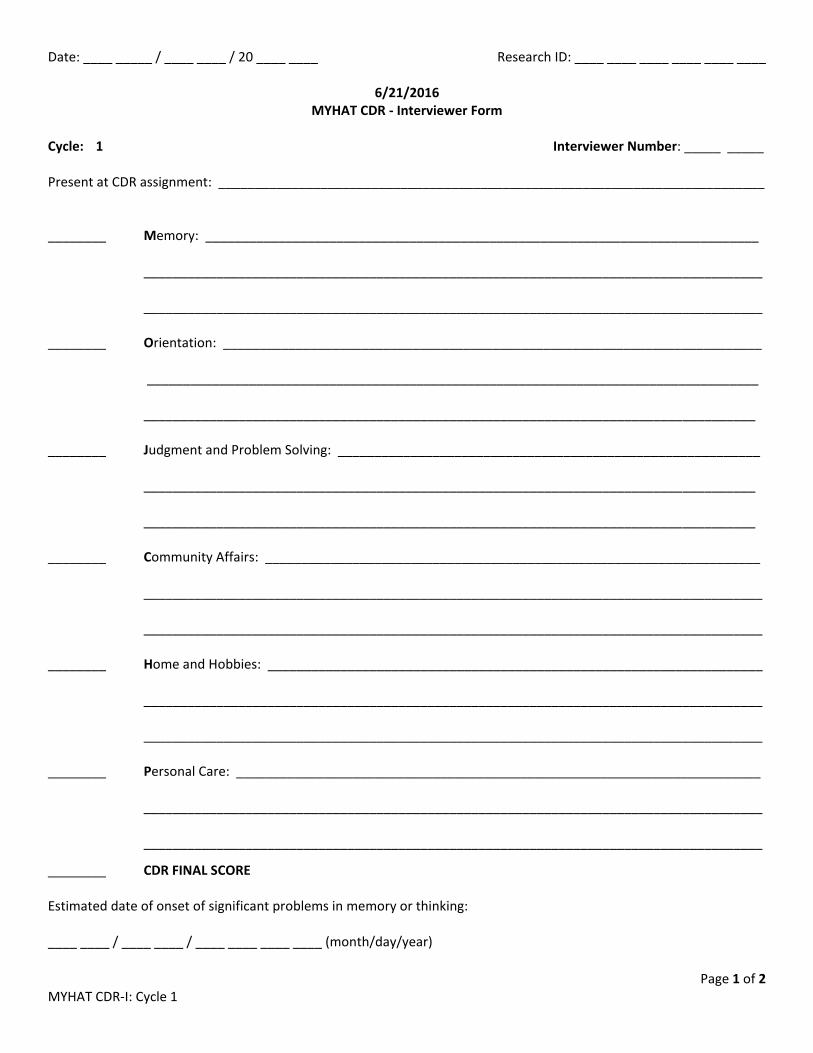
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT CDR-I: Cycle 1
6/21/2016 MYHAT CDR - Interviewer Form
Cycle: 1 Interviewer Number: _____ _____ Present at CDR assignment: ___________________________________________________________________________ ________ Memory: ____________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ ________ Orientation: __________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ________ Judgment and Problem Solving: __________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ________ Community Affairs: ____________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ ________ Home and Hobbies: ____________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ ________ Personal Care: ________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________
________ CDR FINAL SCORE Estimated date of onset of significant problems in memory or thinking: ____ ____ / ____ ____ / ____ ____ ____ ____ (month/day/year)

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT CDR-I: Cycle 1
________ Additional comments (e.g. about contributing factors, special circumstances, source of information about
onset date, etc.) ________ If CDR = 0.5 or greater, does mood/motivation/behavior/apathy appear to play a major role making it hard to
distinguish between cognition versus mood as a cause of the difficulties reported?
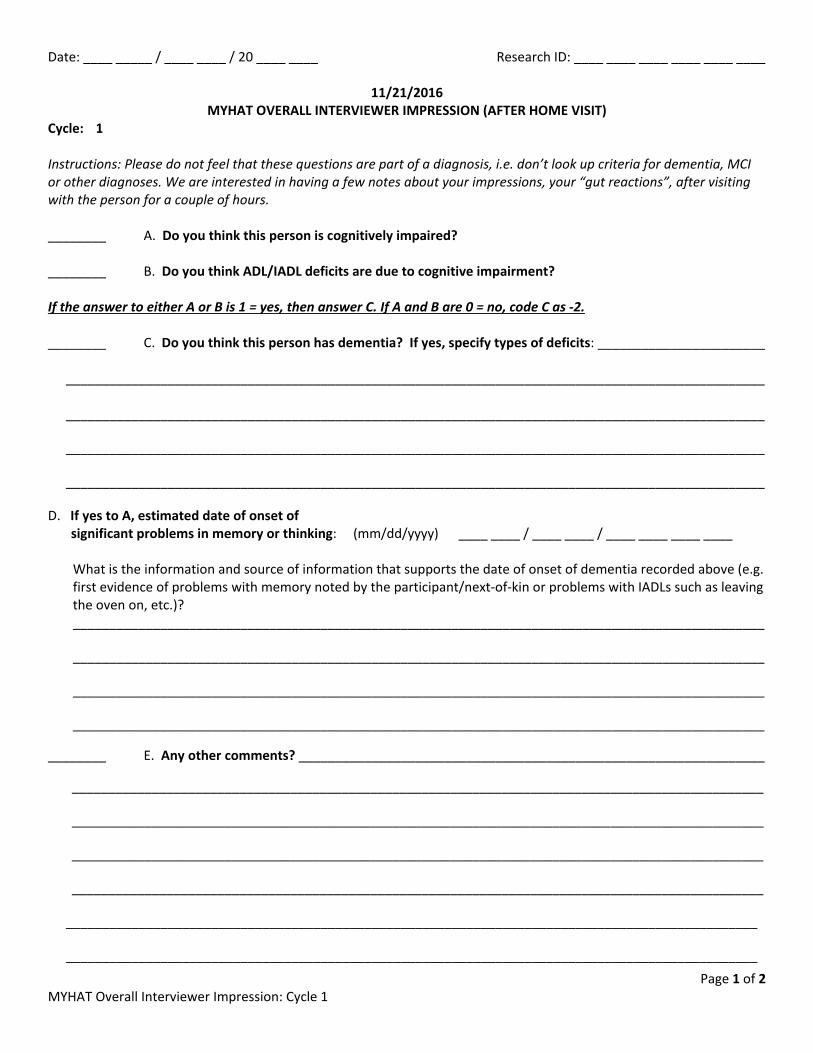
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 1 of 2 MYHAT Overall Interviewer Impression: Cycle 1
11/21/2016 MYHAT OVERALL INTERVIEWER IMPRESSION (AFTER HOME VISIT)
Cycle: 1 Instructions: Please do not feel that these questions are part of a diagnosis, i.e. don’t look up criteria for dementia, MCI or other diagnoses. We are interested in having a few notes about your impressions, your “gut reactions”, after visiting with the person for a couple of hours. ________ A. Do you think this person is cognitively impaired? ________ B. Do you think ADL/IADL deficits are due to cognitive impairment? If the answer to either A or B is 1 = yes, then answer C. If A and B are 0 = no, code C as -2. ________ C. Do you think this person has dementia? If yes, specify types of deficits: _______________________
________________________________________________________________________________________________ ________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
D. If yes to A, estimated date of onset of significant problems in memory or thinking: (mm/dd/yyyy) ____ ____ / ____ ____ / ____ ____ ____ ____
What is the information and source of information that supports the date of onset of dementia recorded above (e.g. first evidence of problems with memory noted by the participant/next-of-kin or problems with IADLs such as leaving the oven on, etc.)? _______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
________ E. Any other comments? ________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________

Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Page 2 of 2 MYHAT Overall Interviewer Impression: Cycle 1
________ F. Did an informant, formally or informally, provide any of the information recorded on the assessment forms?
If yes, please indicate which forms (0 = no, 1 = yes). Check all that apply: _____ Demographic and Contact Information _____ Subjective Memory
_____ ADL/IADL (Functional Abilities) _____ Health History and Lifestyle _____ Florida Cognitive Activities Scale
_____ Physical Activities (Paffenbarger) _____ Medications _____ mCES-D _____ Health Services Utilization _____ Social Support
_____ Pet Form _____ Sports-Related Head Trauma _____ Caffeine _____ Overall Interviewer Impression _____ CDR- Interviewer _____ Other, specify: __________________________________________
________ G. Did the informant’s information influence the CDR?
Date: ____ _____ / ____ ____ / 20 ____ ____ Research ID: ____ ____ ____ ____ ____ ____
Interviewer’s Notes
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________