myocardial viability testing. what we knew and what is...
TRANSCRIPT
Myocardial viability testing. What we knew and what is new
Dr B K S Sastry, MD, DM.
CARE Hospitals, Hyderabad
WCC&IVUS2015
What is Viability
• Viability– Dysfunctional myocardium subtended by diseased
coronary arteries
– Limited or absent scarring
– Potential for functional recovery
• Prospective definition
• Reversible ischemic contractile dysfunction– Myocardial stunning
– Myocardial hibernation
WCC&IVUS2015

meta-analysis of 24 studies that included 3,088 patients
WCC&IVUS2015

meta-analysis of 24 studies that included 3,088 patientsWCC&IVUS2015
Problems with Earlier Studies
All studies were small,
not randomized, observational, and retrospective.
There was potential patient selection bias.
The methodology and criteria for defining viability as well as the treatment regimens were not standardized among the different studies
WCC&IVUS2015

Techniques for assessment of viability
• Contractile reserve-dob.echo and dob.MRI
• Cell membrane integrity-SPECT Thallium
• Intact mitochondria-SPECT Tc
• Myocardial glucose utilization-PET FDG
• Scar tissue-DEMRI,MSCT
• Fractional Flow Reserve, Strain Rate imaging etc.
WCC&IVUS2015

Dobutamine stress echo
• Low-dose dobutamine (5–10 μg/kg/min)– Increase contractility in viable myocardium
• High-dose dobutamine(upto 40 μg/kg/min)– Biphasic response –initial improvement F/B worsening –
underperfused but viable tissue-most specific sign of improvement after revasc.
– Uniphasic response-sustained improvement-myocardial damage with subsequent reperfusion-less predictive of improvement after revasc.
– Deterioration of wall motion without initial improvement-severe ischemia
– No change in wall motion-scar
• Sensitivity(84%),specificity(81%)for recovery of function
WCC&IVUS2015

Strengths and Limitations of DSE
• Strengths-
– Higher specificity
– Viability&ischemiaassessed
– MR can be detected
– Good spatial resolution
– Widely available
– Lower cost
– Predictive of clinical outcomes
• Limitations
– Poor window in 30%
– Lower sensitivity
– Viable regions with absent flow reserve will not show thickening
– Reliance on visual assessment
WCC&IVUS2015

Myocardial perfusion SPECT
• Thallium or Tc. Labelled radio isotopes may be used.
• Uptake depends on viability ®ional perfusion
• Redistribution-gradual accumulation of tracer in hypoperfused areas, rapid washout from normally perfused areas
• Segments with tracer uptake >60%-viable
• Subendocardial scar tissue may be labelled as viable-lower specificity
WCC&IVUS2015
Stress Thallium Protocols
• Rest redistribution protocols-
– Defects in initial images that improve in 4 hour image-viable myocardium
– Additional 24 hr image if fixed defects in 4 hr image
– S/L NTG prior to injection
– Less sensitive-86%,specificity 47%
WCC&IVUS2015
Stress MIBI Strengths and Limitations
• Strengths
– High sensitivity
– Quantitative objective criteria
– LVEF
– FDG with special collimator
– Predictive of outcomes
• Limitations
– Reduced spatial resolution &sensitivity compared to PET
– Attenuation artefacts
– Cannot differentiate endocardial viability
– Less quantitative than PET
WCC&IVUS2015
PET
• Positron emitting isotopes releasing 2 photons at angle180,detected by camera by coincidence counting to give a higher resolution
• Perfusion tracers-N13 ammonia, Rb 82,O15 water
• Metabolic tracers- F18DG,C11acetate,C11 palmitate
• FDG taken up by viable cells, phoshorylated & trapped inside
• Poor uptake in diabetics
WCC&IVUS2015

PET Scan Interpretation
• Normal perfusion-viability
• Flow metabolism mismatch-reduced perfusion with intact metabolism-hibernating viable myocardium
• Flow metabolism match-impaired FDG uptake with reduced perfusion-scar
• Gold standard for assessment of viability
WCC&IVUS2015

Strengths and Limitations of PET
• Strengths-
– Perfusion &metabolism
– More sensitive
– No attenuation
– Absolute blood flow can be measured
– Predictive of outcomes
• Limitations
– Lower specificity to dob.echo & MRI
– Cannot differentiate b/w endocardial and epicardial viability
– High cost
– Limited availability
WCC&IVUS2015

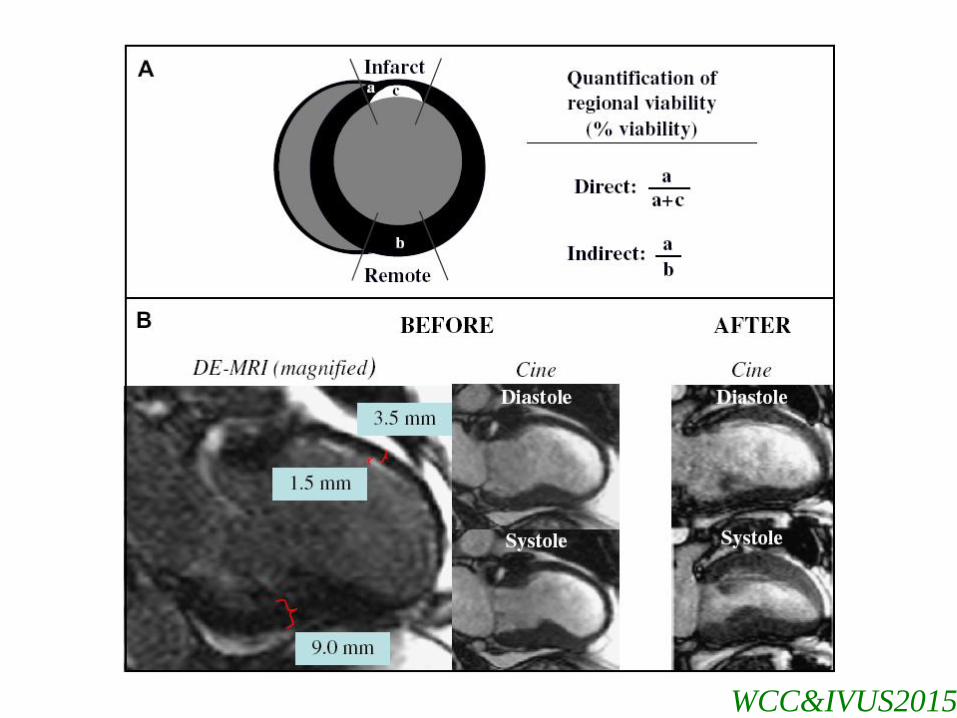
Contrast Enhanced MRI
• DEMRI using Gadolinium based agents (i.v.0.2 mmol/kg)
• Extracellular space
• Infarcted or scarred tissue-interstitial spaces larger-delayed wash in &delayed wash out
• Hyperenhanced area of myocardium on images taken 10 to 20 min after contrast
• Size and shape of infarct correlate with histology
WCC&IVUS2015
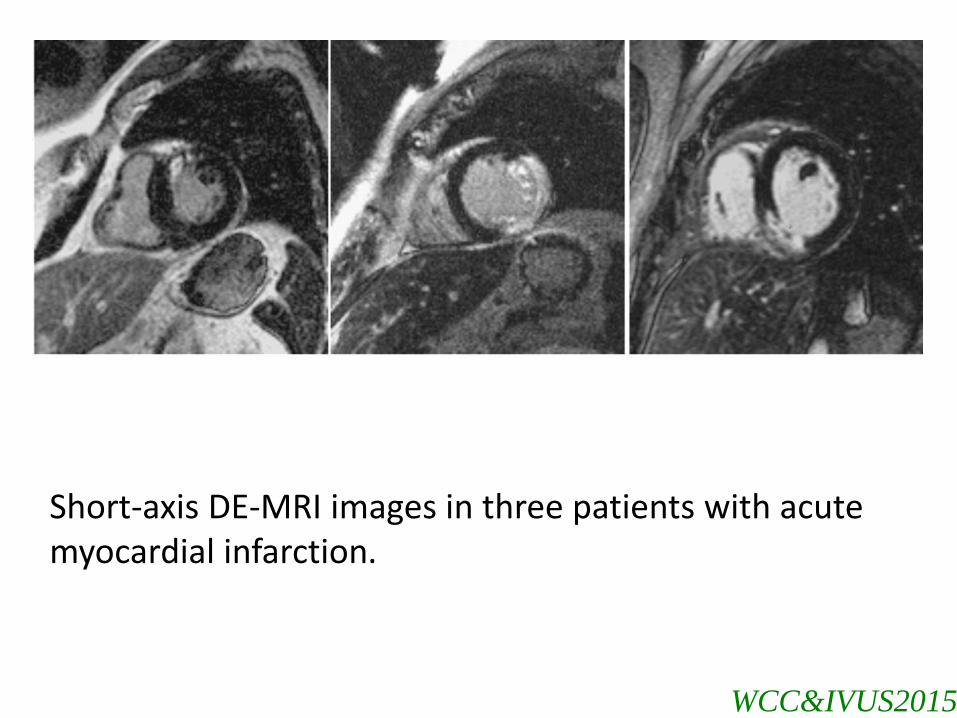
Short-axis DE-MRI images in three patients with acute myocardial infarction.
WCC&IVUS2015

End Diastolic thickness of more than 6 mm suggests viable myocardium
WCC&IVUS2015
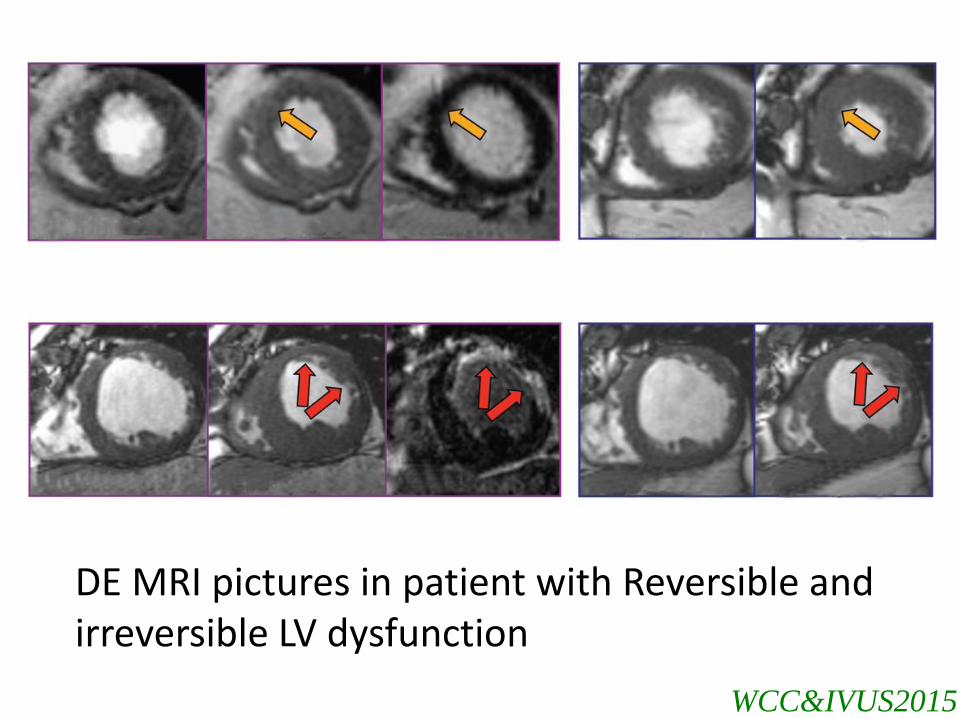
DE MRI pictures in patient with Reversible and irreversible LV dysfunction
WCC&IVUS2015

WCC&IVUS2015
WCC&IVUS2015

Shah DJ, Kim HW, JAMA. 2013 Mar.
WCC&IVUS2015
Strengths and Limitations of MRI
• Strengths– Accurate assessment of
extent of scar
– Superior spatial resolution
– Wall thickness correctly measured
– Simultaneous assessment of perfusion, function and viability
– Good imaging windows
• Limitations – High cost
– Limited availability
– Longer time
– Contra.with implanted ferromagnetic objects
– Gadolinium contra.in CKD with GFR<30ml/min
– Claustrophobia
– Irregular rhythems
– Breathholding required
WCC&IVUS2015
WCC&IVUS2015

WCC&IVUS2015

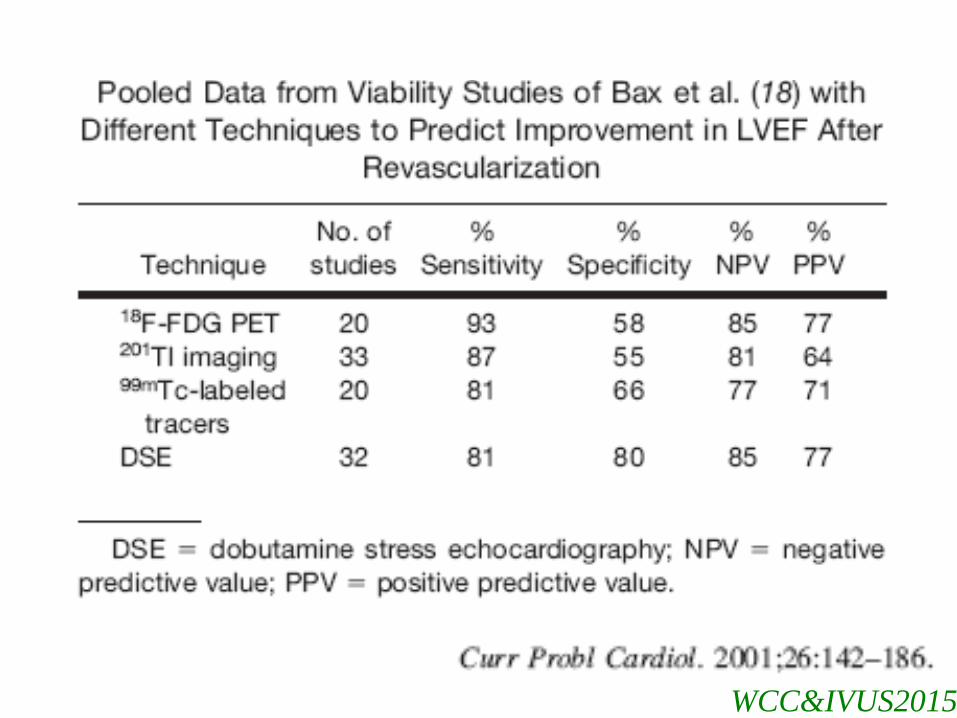
DSE Vs nuclear imaging
• Sensitivity 90% for nuclear imaging,74% for DSE
• Specificity 57% for nuclear imaging,78% for DSE
– Bax JJ et al;2002
• Integration of both may be useful
WCC&IVUS2015

STITCH Trial
• A randomized, multi center, non blinded trial.
• 1212 patients with CAD and LVEF < 35% without severe AP / LMCA disease were randomized to CABG with intensive medical therapy or intensive medical therapy alone.
• The primary endpoint of all cause mortality after a median follow–up of 56 months occurred in 41% of patients randomized to medical therapy alone compared with 36% randomized to CABG.
• This difference did not reach statistical significance (HR with CABG, 0.86; 95% CI, 0.72-1.04; P=.12).
WCC&IVUS2015

STITCH Trial protocol
• Post-randomization myocardial viability testing by dobutamine stress echocardiography and/or radionuclide imaging was recommended.
• In the 601 patients who received a viability study, there was a significant association between viability and outcome on univariate analysis but not on multivariate analysis.
• Assessment of myocardial viability did not identify patients with a differential survival benefit from CABG as compared with medical therapy alone.
WCC&IVUS2015

Limitations of STICH Trial
Slightly less than half of the 1212 enrolled patients enrolled underwent viability testing.
Patients were not randomized to viability testing.
Selection/enrolment bias can not be eliminated.
Only 19% of the patients were deemed not to have viable myocardium ,which limited the power of the analysis to detect a differential effect of CABG.
Viability analyses were limited to SPECT and DSE imaging. Caution should be taken to not extrapolate these results to DE-MRI.
WCC&IVUS2015

Conclusions of STITCH trial
• There was no significant interaction between myocardial viability and medical versus surgical treatment with reference to primary end point.
• This was true whether patients were grouped according to the assigned treatment (i.e., intention-to-treat analysis) or to the treatment actually received.
• Other variables could have influenced the outcome.
• Assessment of myocardial viability alone should not be the deciding factor in selecting the best therapy.
WCC&IVUS2015

Other Trials
• Similar to STICH trial, Heart Failure Revascularization trial, an RCT of Conservative Vs Revascularization strategy did not show benefit with revascularization in patients with proven viable myocardium.
• Adding surgical ventricular reconstruction to surgical revascularization would not improve the outcomes in patients with non viable myocardium
WCC&IVUS2015
Functionality Vs Viability
• A viable tissue may not be functional.
• Even when it is contractile, it may not increase LV regional function if it is trapped within a scar.
• Prognosis may improve even if the functionality is restored.
• Peri procedurural or Peri op MI, may lead to a negative result.
• Late vessel patency also has implications.
WCC&IVUS2015
In Conclusion
• Retrospective studies showed benefit of Viability testing.
• Prospective studies failed to show the benefit.
• Further studies with better techniques and methodology need to be done.
• Till then make decision based on many factors.
WCC&IVUS2015