myofascial trigger points: an evidence-informed review - david g
TRANSCRIPT

The Journal of Manual & Manipulative TherapyVol. 14 No. 4 (2006), 203 - 221 Myofascial Trigger Points: An Evidence-Informed Review / 203
Myofascial Trigger points: an evidence-informed review
Addressallcorrespondenceandrequestforreprintsto:JanDommerholtBethesdaPhysiocare,Inc.7830OldGeorgetownRoad,SuiteC-15Bethesda,[email protected]
Abstract:Thisarticleprovidesabestevidence-informedreviewofthecurrentscientificun-derstandingofmyofascialtriggerpointswithregardtotheiretiology,pathophysiology,andclinicalimplications.Evidence-informedmanualtherapyintegratesthebestavailablescien-tificevidencewithindividualclinicians’judgments,expertise,andclinicaldecision-making.Afterabriefhistoricalreview,theclinicalaspectsofmyofascialtriggerpoints,theinterraterreliability for identifying myofascial trigger points, and several characteristic features arediscussed, including the taut band, local twitch response, and referred pain patterns. Theetiologyofmyofascialtriggerpointsisdiscussedwithadetailedandcomprehensivereviewofthemostcommonmechanisms,includinglow-levelmusclecontractions,unevenintramus-cularpressuredistribution,direct trauma,unaccustomedeccentriccontractions,eccentriccontractionsinunconditionedmuscle,andmaximalorsub-maximalconcentriccontractions.Manycurrentscientificstudiesareincludedandprovidesupportforconsideringmyofascialtriggerpointsintheclinicaldecision-makingprocess.Thearticleconcludeswithasummaryoffrequentlyencounteredprecipitatingandperpetuatingmechanical,nutritional,metabolic,andpsychologicalfactorsrelevantforphysicaltherapypractice.Currentscientificevidencestronglysupportsthatawarenessandworkingknowledgeofmuscledysfunctionandinpar-ticularmyofascialtriggerpointsshouldbeincorporatedintomanualphysicaltherapypracticeconsistentwiththeguidelinesforclinicalpracticedevelopedbytheInternationalFederationofOrthopaedicManipulativeTherapists.Whiletherearestillmanyunansweredquestionsinexplainingtheetiologyofmyofascial triggerpoints, thisarticleprovidesmanualtherapistswithanup-to-dateevidence-informedreviewofthecurrentscientificknowledge.
Key Words : Myofascia l Pain Syndrome, Tr igger Points , Myofascia l , Et io logy,Pathophysiology
Jan Dommerholt, PT, MPS, FAAPMCarel Bron, PTJo Franssen, PT
Duringthepastfewdecades,myofascialtriggerpoints(MTrPs)andmyofascialpainsyndrome(MPS)have
received much attention in the scientific and clinicalliterature. Researchers worldwide are investigatingvariousaspectsofMTrPs,includingtheirspecificetiol-ogy,pathophysiology,histology,referredpainpatterns,and clinical applications. Guidelines developed by theInternational Federation of Orthopaedic Manipulative
Therapists (IFOMT)confirmthe importanceofmuscledysfunctionfororthopedicmanualtherapyclinicalprac-tice.TheIFOMThasdefinedorthopedicmanualtherapyas“aspecializedareaofphysiotherapy/physicaltherapyfor the management of neuromusculoskeletal condi-tions,basedonclinicalreasoning,usinghighlyspecifictreatmentapproachesincludingmanualtechniquesandtherapeutic exercises.” The educational standards ofIFOMTrequirethatskillswillbedemonstratedin—amongothers—“analysisandspecifictestsforfunctionalstatusofthemuscularsystem,”“ahighlevelofskill inothermanual and physical therapy techniques required tomobilizethearticular,muscularorneuralsystems,”and“knowledgeofvariousmanipulativetherapyapproachesaspracticedwithinphysicaltherapy,medicine,osteopathyandchiropractic”1.

204 / The Journal of Manual & Manipulative Therapy, 2006
However, articles aboutmuscledysfunction in themanualtherapyliteraturearesparseandtheygenerallyfocusonmuscleinjuryandmusclerepairmechanisms2oronmusclerecruitment3.Untilveryrecently,thecurrentscientificknowledgeandclinicalimplicationsofMTrPswererarelyincluded4-7.Itappearsthatorthopedicmanualtherapistshavenot paidmuchattention to thepatho-physiologyandclinicalmanifestationsofMTrPs.ManualtherapyeducationalprogramsintheUSseemtoreflectthisorientationandtendtoplaceastrongemphasisonjointdysfunction,mobilizations,andmanipulationswithonlyabout10%-15%ofclassroomeducationdevotedtomusclepainandmuscledysfunction.
This review of the MTrP literature is based oncurrent best scientific evidence. The field of manualtherapyhasjoinedothermedicaldisciplinesbyembrac-ing evidence-based medicine, which proposes that theresultsofscientificresearchneedtobeintegratedintoclinical practice8. Evidence-based medicine has beendefined as “the conscientious, explicit, and judicioususeofcurrentbestevidenceinmakingdecisionsaboutthecareofindividualpatients”9,10.Withintheevidence-basedmedicineparadigm,evidence isnotrestrictedtorandomized controlled trials, systematic reviews, andmeta-analyses,althoughthisrestrictedviewseemstobeprevalentinthemedicalandphysicaltherapyliterature.Sackettetal9,10emphasizedthatexternalclinicalevidencecaninformbutnotreplaceindividualclinicalexpertise.Clinicalexpertisedetermineswhetherexternalclinicalevidenceappliestoanindividualpatient,andifso,howit should be integrated into clinical decision-making.Pencheon11 shared this perspective and suggested thathigh-quality healthcare is about combining “wisdomproducedbyyearsofexperience”with“evidenceproducedbygeneralizableresearch”in“wayswithwhichpatientsarehappy.”Hesuggestedshifting fromevidence-basedtoevidence-informedmedicine,whereclinicaldecision-makingisinformedbyresearchevidencebutnotdrivenby it and always includes knowledge from experience.Evidence-informed manual therapy involves integrat-ing thebest available external scientific evidencewithindividual clinicians’ judgments, expertise, and clini-caldecision-making12.Thepurposeof thisarticle is toprovideabestevidence-informedreviewofthecurrentscientificunderstandingofMTrPs,includingtheetiology,pathophysiology, and clinical implications, against thebackgroundofextensiveclinicalexperience.
brief Historical reviewWhileDr.JanetTravell(1901-1997)isgenerallycred-
ited forbringingMTrPstotheattentionofhealthcareproviders,MTrPshavebeendescribedandrediscoveredforseveralcenturiesbyvariouscliniciansandresearchers13,14.Asfarbackasthe16thcentury,deBaillou(1538-1616),ascitedbyRuhmann,describedwhat isnowknownasmyofascial pain syndrome (MPS)15. MPS is defined as
the “sensory, motor, and autonomic symptoms causedbyMTrPs”andhasbecomea recognizedmedicaldiag-nosisamongpainspecialists16,17.In1816,Britishphysi-cianBalfour,ascitedbyStockman,described“nodulartumorsandthickeningswhichwerepainfultothetouch,and from which pains shot to neighboring parts”18. In1898, the German physician Strauss discussed “small,tenderandapple-sizednodulesandpainful,pencil-sizedtolittle-finger-sizedpalpablebands”19.Thefirsttriggerpointmanualwaspublishedin1931inGermanynearlya decade before Travell became interested in MTrPs20.Whiletheseearlydescriptionsmayappearabitarchaicandunusual—forexample,inclinicalpracticeonedoesnotencounter“apple-sizednodules”—theseandotherhistoricpapersdidillustratethebasicfeaturesofMTrPsquiteaccurately14.
In the late 1930s, Travell, who at that time was acardiologistandmedicalresearcher,becameparticularlyinterested in muscle pain following the publication ofseveralarticlesonreferredpain21.Kellgren’sdescriptionsof referred pain patterns of many muscles and spinalligamentsafter injectingthese tissueswithhypertonicsaline22-25eventuallymovedTravelltoshifthermedicalcareerfromcardiologytomusculoskeletalpain.Duringthe 1940s, she published several articles on injectiontechniques of MTrPs26-28. In 1952, she described themyofascial genesis of pain with detailed referred painpatternsfor32muscles29.OthercliniciansalsobecameinterestedinMTrPs.EuropeanphysiciansLiefandChaitowdevelopedatreatmentmethod,whichtheyreferredtoas“neuromusculartechnique”30.GermanphysicianGutsteindescribedthecharacteristicsofMTrPsandeffectivemanualtherapy treatments in several papers under the namesofGutstein,Gutstein-Good,andGood31-34.InAustralia,Kellyproducedaseriesofarticlesaboutfibrositis,whichparalleledTravel’swritings35-38.
In the US, chiropractors Nimmo and Vannerson39describedmuscular“noxiousgenerativepoints,”whichwerethoughttoproducenerveimpulsesandeventuallyresultin“vasoconstriction,ischaemia,hypoxia,pain,andcellulardegeneration.”Laterinhiscareer,Nimmoadoptedthe term “trigger point” after having been introducedtoTravell’swritings.Nimmomaintainedthathypertonicmusclesarealwayspainfultopressure,astatementthatlater became known as “Nimmo’s law.” Like Travell,Nimmodescribeddistinctivereferredpainpatternsandrecommended releasing these dysfunctional points byapplyingtheproperdegreeofmanualpressure.Nimmo’s“receptor-tonuscontrolmethod”continuestobepopularamongchiropracticphysicians39,40.Accordingtoa1993reportbytheNationalBoardofChiropracticEconomics,over 40% of chiropractors in the US frequently applyNimmo’s techniques41. Two spin-offs of Nimmo’s workareSt.JohnNeuromuscularTherapy(NMT)methodandNMTAmericanversion,whichhavebecomeparticularlypopularamongmassagetherapists30.

Myofascial Trigger Points: An Evidence-Informed Review / 205
In1966,TravellfoundedtheNorthAmericanAcademyofManipulativeMedicine,togetherwithDr.JohnMennell,who also published several articles about MTrPs42,43. Throughout her career Travell promoted integratingmyofascial treatmentswitharticular treatments16.Oneof her earlier papers described a technique for reduc-ingsacroiliacdisplacement44.However,Travell,ascitedby Paris45, maintained the opinion that manipulationswere the exclusive domain of physicians and she re-jectedmembership in theNorthAmericanAcademyofManipulativeMedicinebyphysicaltherapists.
Intheearly1960s,Dr.DavidSimonswasintroducedto Travell and her work, which became the start of afruitfulcollaborationeventuallyresultinginseveralpub-lications,includingtheTrigger Point Manuals,consist-ingofa1983firstvolume(upperhalfofthebody)anda1992secondvolume(lowerhalfofthebody)46,47.Thefirst volumehas sincebeen revisedandupdatedandasecondeditionwasreleasedin199916.TheTrigger Point Manuals are the most comprehensive review of nearly150 muscle referred-pain patterns based on Travell’sclinical observations, and they include an extensivereview of the scientific basis of MTrPs. Both volumeshave been translated into several foreign languages,including Russian, German, French, Italian, Japanese,and Spanish. Several other clinicians worldwide havealsopublishedtheirowntriggerpointmanuals48-54.
clinical aspects of Myofascial Trigger points
An MTrP is described as “a hyperirritable spot inskeletalmusclethatisassociatedwithahypersensitivepalpablenoduleinatautband”16.Myofascialtriggerpointsareclassifiedintoactiveandlatenttriggerpoints16.AnactiveMTrPisasymptom-producingMTrPandcantriggerlocal or referred pain or other paraesthesiae. A latentMTrP does not trigger pain without being stimulated.Myofascialtriggerpointsarethehallmarkcharacteris-ticsofMPSandfeaturemotor,sensory,andautonomiccomponents. Motor aspects of active and latent MTrPsmay include disturbed motor function, muscle weak-ness as a result of motor inhibition, muscle stiffness,andrestrictedrangeofmotion55,56.Sensoryaspectsmayinclude local tenderness, referral of pain to a distantsite,andperipheralandcentralsensitization.Peripheralsensitizationcanbedescribedasareductioninthresholdandanincreaseinresponsivenessoftheperipheralendsofnociceptors,whilecentralsensitizationisanincreaseintheexcitabilityofneuronswithinthecentralnervoussystem.Signsofperipheralandcentralsensitizationareallodynia(painduetoastimulusthatdoesnotnormallyprovokepain)andhyperalgesia (an increased responsetoastimulusthatisnormallypainful).BothactiveandlatentMTrPsarepainfuloncompression.Vecchietetal57-
59describedspecificsensorychangesoverMTrPs.They
observedsignificantloweringofthepainthresholdoveractiveMTrPswhenmeasuredbyelectricalstimulation,notonlyinthemusculartissuebutalsointheoverlyingcutaneous and subcutaneous tissues. In contrast,withlatent MTrPs, the sensory changes did not involve thecutaneousandsubcutaneoustissues57-59.AutonomicaspectsofMTrPsmayinclude,amongothers,vasoconstriction,vasodilatation, lacrimation,andpiloerection16,60-63.
Adetailedclinicalhistory,examinationofmovementpatterns,andconsiderationofmusclereferred-painpat-terns assist clinicians in determining which musclesmay harbor clinically relevant MTrPs64. Muscle pain isperceivedasachingandpoorly localized.TherearenolaboratoryorimagingtestsavailablethatcanconfirmthepresenceofMTrPs.Myofascialtriggerpointsareidenti-fiedthrougheitheraflatpalpationtechnique(Figure1)in which a clinician applies finger or thumb pressureto muscle against underlying bone tissue, or a pincerpalpation technique (Figure 2) in which a particularmuscleispalpatedbetweentheclinician’sfingers.
Fig.1: Flat palpation
Fig.2: Pincer palpation

206 / The Journal of Manual & Manipulative Therapy, 2006
Bydefinition,MTrPsarelocatedwithinatautbandofcontracturedmusclefibers(Figure3),andpalpatingforMTrPsstartswithidentifyingthistautbandbypalpatingperpendiculartothefiberdirection.Oncethetautbandis located, the clinician moves along the taut band to
guides the clinician. The presence of a so-called localtwitchresponse(LTR),referredpain,orreproductionofthe person’s symptomatic pain increases the certaintyand specificity of the diagnosis of MPS. Local twitchresponses are spinal reflexes that appear to be uniquetoMTrPs.Theyarecharacterizedbyasuddencontrac-tionofmusclefiberswithinatautband,whenthetautband is strummed manually or needled. The suddencontractionscanbeobservedvisually, canbe recordedelectromyographically, or can be visualized with diag-nostic ultrasound72. When an MTrP is needled with amonopolar teflon-coated EMG needle, LTRs appear ashigh-amplitudepoly-phasicEMGdischarges73-78.
In clinical practice, there is no benefit in usingneedleEMGorsonography,anditsutilityislimitedtoresearchstudies.Forexample,Audetteetal79establishedthatin61.5%ofactiveMTrPsinthetrapeziusandlevatorscapulaemuscles,dryneedlinganactiveMTrPelicitedanLTRinthesamemuscleontheoppositesideofthebody. Needling of latent MTrPs resulted in unilateralLTRs only. In this study, LTRs were used to researchthe nature of active versus latent MTrPs. Studies haveshownthatclinicaloutcomesaresignificantlyimprovedwhenLTRsareelicitedinthetreatmentofpatientswithdry needling or injection therapy74,80,81. The taut band,MTrP,andLTR(Figure4)areobjectivecriteria,identifiedsolelybypalpation,thatdonotrequireaverbalresponsefromthepatient82.
Active MTrPs refer pain usually to a distant site.Thereferredpainpatterns(Figure5)arenotnecessarily
Fig. 3: Palpation of a trigger point within a taut band (reproduced with permission from Weisskircher H-W. Head Pains Due to Myofascial Trigger Points. CD-ROM, www.trigger-point.com, 1997)
findadiscreteareaof intensepainandhardness.Two studies have reported good overall interrater
reliabilityforidentifyingtautbands,MTrPs,referredpain,and local twitch responses65,66. The minimum criteriathatmustbe satisfied inorder todistinguishanMTrPfrom any other tender area in muscle are a taut bandandatenderpoint inthattautband65.AlthoughJandamaintained that systematic palpation can differentiatebetweenmyofascialtautbandsandgeneralmusclespasms,electromyographyisthegoldstandardtodifferentiatetautbandsfromcontractedmusclefibers67,68.Spasmscanbedefinedaselectromyographic(EMG)activityastheresultof increasedneuromusculartoneof theentiremuscle,andtheyaretheresultofnerve-initiatedcontractions.Atautbandisanendogenouslocalizedcontracturewithinthemusclewithoutactivationof themotorendplate69.Fromaphysiologicalperspective,theterm“contracture”ismoreappropriatethen“contraction”whendescribingchronic involuntary shortening of a muscle withoutEMGactivity. Inclinicalpractice,surfaceEMGisusedinthediagnosisandmanagementofMTrPsinadditionto manual examinations67,70,71. Diagnostically, surfaceEMGcanassistinassessingmusclebehaviorduringrestand during functional tasks. Clinicians use the MTrPreferred pain patterns in determining which musclesto examine with surface EMG. Muscles that harborMTrPs responsible for thepatient’spaincomplaintareexamined first. EMG assessments guide the clinicianwith postural training, ergonomic interventions, andmuscleawarenesstraining67.
Thepatient’srecognitionoftheelicitedpainfurther
Fig. 4: Local twitch response in a rabbit trigger spot. Local twitch responses are elicited only when the needle is placed accurately within the trigger spot. Moving as little as 0.5 cm away from the trigger spot virtually eliminates the local twitch response (reproduced with permission from Hong C-Z, Torigoe Y. Electrophysiological characteristics of localized twitch responses in responsive taut bands of rabbit skeletal muscle. J Musculoskeletal Pain 1994;2:17-43)

Myofascial Trigger Points: An Evidence-Informed Review / 207
restricted to single segmental pathways or to periph-eralnervedistributions.Althoughtypicalreferredpainpatterns have been established, there is considerablevariationbetweenpatients16,48.
Usually, the pain in reference zones is described as“deeptissuepain”ofadullandachingnature.Occasion-ally,patientsmayreportburningortinglingsensations,especially in superficial muscles such as the platysmamuscle83,84. By mechanically stimulating active MTrPs,patientsmayreportthereproductionoftheirpain,eitherimmediately or after a 10-15 second delay. Normally,skeletal muscle nociceptors require high intensities ofstimulation and they do not respond to moderate localpressure, contractions, or muscle stretches85. However,MTrPscausepersistentnoxiousstimulation,whichresultsinincreasingthenumberandsizeofthereceptivefieldstowhichasingledorsalhornnociceptiveneuronresponds,and the experience of spontaneous and referred pain86.Several recent studies have determined previously un-recordedreferredpainpatternsofdifferentmusclesandMTrPs87-90.Referredpain isnotspecific toMPSbut it isrelativelyeasytoelicitoverMTrPs91.Normalmuscletissueandotherbodytissues,includingtheskin,zygapophysealjoints,orinternalorgans,mayalsoreferpaintodistantregionswithmechanicalpressure,makingreferredpainelicitedbystimulationofatenderlocationanonspecificfinding84,92-95.Gibsonetal96foundthatreferredpainisactu-allyeasiertoelicitintendon-bonejunctionsandtendonthan in the muscle belly. However, after exposing themuscletoeccentricexercise,significantlyhigherreferredpainfrequencyandenlargedpainareaswerefoundatthemusclebellyandthetendon-bonejunctionsitesfollowinginjection with hypotonic saline. The authors suggestedthat central sensitizationmay explain the referredpain
frequencyandenlargedpainareas97.While a survey of members of the American Pain
SocietyshowedgeneralagreementthatMTrPsandMPSexist as distinct clinical entities, MPS continues to beone of the most commonly missed diagnoses17,98. In arecentstudyof110adultswithlowbackpain,myofascialpain was the most common finding affecting 95.5% ofpatients,eventhoughmyofascialpainwaspoorlydefinedasmusclepainintheparaspinalmuscles,piriformis,ortensorfasciaelatae99.Astudyofadultswithfrequentmi-graineheadachesdiagnosedaccordingtotheInternationalHeadacheSocietycriteriashowedthat94%ofthepatientsreported migrainous pain with manual stimulation ofcervicalandtemporalMTrPs,comparedwithonly29%ofcontrols100,101.In30%ofthemigrainegroup,palpationofMTrPseliciteda“full-blownmigraineattackthatrequiredabortive treatment.” The researchers found a positiverelationshipbetween thenumberofMTrPsand the fre-quencyofmigraineattacksanddurationoftheillness100.SeveralstudieshaveconfirmedthatMTrPsarecommonnotonly inpersonsattendingpainmanagementclinicsbutalsointhoseseekinghelpthroughinternalmedicineand dentistry102-107. In fact, MTrPs have been identifiedwithnearlyeverymusculoskeletalpainproblem,includ-ing radiculopathies104, joint dysfunction108, disk pathol-ogy109, tendonitis110, craniomandibular dysfunction111-113,migraines100,114,tension-typeheadaches7,87,carpaltunnelsyndrome115,computer-relateddisorders116,whiplash-as-sociated disorders60,117, spinal dysfunction118, and pelvicpainandotherurologicsyndromes119-122.Myofascialtriggerpointsareassociatedwithmanyotherpainsyndromes123,including,forexample,post-herpeticneuralgia124,125,complexregionalpainsyndrome126,127,nocturnalcramps128,phantompain129,130,andotherrelativelyuncommondiagnosessuchasBarré-Liéousyndrome131andneurogenicpruritus132.ArecentstudysuggestedthattheremightbearelationshipbetweenMTrPsintheuppertrapeziusmuscleandcervicalspinedysfunctionat theC3andC4vertebrae,althougha cause-and-effect relationship was not established inthiscorrelational study133.Anotherstudydescribed thatpersons with mechanical neck pain had significantlymore clinically relevant MTrPs in the upper trapezius,sternocleidomastoid, levator scapulae, and suboccipitalmusclesascomparedtohealthycontrols5.
etiology of MTrpsSeveralpossiblemechanismscanleadtothedevel-
opmentofMTrPs, including low-levelmuscle contrac-tions,unevenintramuscularpressuredistribution,directtrauma,unaccustomedeccentriccontractions,eccentriccontractionsinunconditionedmuscle,andmaximalorsubmaximalconcentriccontractions.
Low-levelmusclecontractionsOf particular interest in the etiology of MTrPs are
low-levelmuscleexertionsandtheso-calledCinderella
Fig.5: MTrP referred pain patterns (reproduced with per-mission from MEDICLIP, Manual Medicine 1 & 2, Version 1.0a, 1997, Williams & Wilkins)

208 / The Journal of Manual & Manipulative Therapy, 2006
HypothesisdevelopedbyHäggin1988134.TheCinderellaHypothesispostulatesthatoccupationalmyalgiaiscausedby selective overloading of the earliest recruited andlastde-recruitedmotorunitsaccordingtotheorderedrecruitmentprincipleorHenneman’s“sizeprinciple”134,135.Smallermotorunitsarerecruitedbeforeandde-recruitedafterlargerones;asaresult,thesmallertype1fibersarecontinuouslyactivatedduringprolongedmotortasks135.AccordingtotheCinderellaHypothesis,muscularforcegeneratedatsub-maximallevelsduringsustainedmusclecontractionsengagesonlyafractionofthemotorunitsavailablewithoutthenormallyoccurringsubstitutionofmotorunitsduringhigherforcecontractions,whichinturncanresultinmetabolicallyoverloadedmotorunits,prone to loss of cellular Ca2+-homeostasis, subsequentactivationofautogenicdestructiveprocesses,andmusclepain136,137.TheotherpillaroftheCinderellaHypothesisisthefindingofanexcessofraggedredfibersinmyalgicpatients136.Indeed,severalresearchershavedemonstratedthepresenceofraggedredfibersandmoth-eatenfibersinsubjectswithmyalgia,whichareindicationsofstruc-tural damage to the cell membrane and mitochondriaandachangeinthedistributionofmitochondriaorthesarcotubularsystemrespectively138-142.
Thereisgrowingevidencethatlow-levelstaticmusclecontractionsorexertionscanresultindegenerationofmuscle fibers143. Gissell144,145 has shown that low-levelexertions can result in an increase of Ca2+-release inskeletalmusclecells,musclemembranedamageduetoleakageoftheintracellularenzymelactatedehydrogenase,structuraldamage,energydepletion,andmyalgia.Low-levelmusclestimulationcanalsoleadtothereleaseofinterleukin6(IL-6)andothercytokines146,147.
SeveralstudieshaveconfirmedtheCinderellaHy-pothesis and support the idea that in low-level staticexertions, muscle fiber recruitment patterns tend tobe stereotypicalwithcontinuousactivationof smallertype 1 fibers during prolonged motor tasks148-152. AsHäggindicated,thecontinuousactivityandmetabolicoverload of certain motor units does not occur in allsubjects136. The Cinderella Hypothesis was recentlyapplied to the development of MTrPs116. In a well-de-signedstudy,Treastersetal116establishedthatsustainedlow-levelmusclecontractionsduringcontinuoustypingfor as little as 30 minutes commonly resulted in theformationofMTrPs.TheysuggestedthatMTrPsmightprovideausefulexplanationformusclepainandinjurythatcanoccur fromlow-level staticexertions116.Myo-fascial trigger points are common in office workers,musicians, dentists, and other occupational groupsexposed to low-level muscle exertions153. Chen et al154also suggested that low-level muscle exertions canleadtosensitizationanddevelopmentofMTrPs.Fortypiano students showed significantly reduced pressurethresholdsover latentMTrPsafteronly20minutesofcontinuouspianoplaying154.
IntramuscularpressuredistributionOtten155hassuggestedthatcirculatorydisturbances
secondarytoincreasedintramuscularpressuremayalsoleadtothedevelopmentofmyalgia.Basedonmathemati-cal modeling applied to a frog gastrocnemius muscle,Otten confirmed that during static low-level musclecontractions, capillary pressures increase dramaticallyespeciallynearthemuscleinsertions(Figure6).Inotherwords, during low-level exertions, the intramuscular
Fig.6: Intramuscular pressure distribution in the gastroc-nemius muscle of the toad (reproduced with permission from E. Otten, 2006)
pressure near the muscle insertions might increaserapidly,leadingtoexcessivecapillarypressure,decreasedcirculation,andlocalizedhypoxiaandischaemia155.Withhigher level contractions in between 10% and 20% ofmaximumvoluntaryeffort,theintramuscularpressureincreases also in the muscle belly156,157. According toOtten,theincreasedpressuregradientsduringlow-levelexertionsmaycontributetothedevelopmentofpainatthemusculotendinous junctions and eventually to theformationofMTrPs(personalcommunication,2005).
In1999,Simonsintroducedtheconceptof“attach-menttriggerpoints”toexplainpainatthemusculoten-dinous junctions in persons with MTrPs, based on theassumption that taut bands would generate sufficientsustained forceto induce localizedenthesopathies16,158.Morerecently,Simonsconcludedthatthereisnocon-vincingevidencethatthetensiongeneratedinshortenedsarcomeres in a muscle belly would indeed be able togeneratepassiveorresting force throughoutanentiretaut band resulting in enthesopathies, even though

Myofascial Trigger Points: An Evidence-Informed Review / 209
theremaybecertainmusclesorconditionswherethiscould occur (personal communication, 2005). To thecontrary, force generated by individual motor units isalwaystransmittedlaterallytothemuscle’sconnectivetissuematrix, involvingatleasttwoproteincomplexescontainingvinculinanddystrophin,respectively159.Thereis alsoconsiderable evidence that theassumption thatmuscle fibers pass from tendon to tendon is withoutbasis160.Trotter160hasdemonstratedthatskeletalmuscleiscomprisedofin-seriesfibers.Inotherwords,thereisevidence that a single muscle fiber does not run fromtendon to tendon. The majority of fibers are in serieswithinactivefibers,whichmakesitevenmoreunlikelythatthewholemusclelength-tensionpropertieswouldbe dictated by the shortest contractured fibers in themuscle161.
Inaddition,itisimportanttoconsiderthemechanicalandfunctionaldifferencesbetweenfastandslowmotorunits162,163.Slowmotorunitsarealwaysstifferthanfastunits, although fast units can produce more force. Iftherewereanytransmissionof forcealongthemusclefiber,asSimonsinitiallysuggested,fastfiberswouldbebetter suited to accomplish this. Yet, fast motor unitshave larger series of elastic elements, which wouldabsorbmostof the forcedisplacement164,165.Fast fibersshowaprogressivedecreaseincross-sectionalareaandendinapointwithinthemusclefascicle,makingforcetransmissionevenmoreunlikely163.Fast fibers relyontransmitting a substantial proportion of their force tothe endomysium, transverse cytoskeleton, and adja-cent muscle fibers162,163. In summary, the developmentof so-called “attachment trigger points” as a result ofincreasedtensionbycontracturedsarcomeresinMTrPsisnotclearandmoreresearchisneededtoexplaintheclinical observation that MTrPs appear to be linked topain at the musculotendinous junction. The increasedtensioninthemusclebellyis likelytodissipateacrossbriefsectionsofthetautbandonbothsidesoftheMTrPand laterally through the transversecytoskeleton166-168.Instead,Otten’smodelofincreasedintramuscularpressure,decreasedcirculation,localizedhypoxia,andischaemiaatthemuscleinsertionsprovidesanalternativemodelfortheclinicallyobservedpainnearthemusculotendinousjunctionandosseousinsertionsinpersonswithMTrPs,eventhoughthemodeldoesnotexplainwhytautbandsarecommonlypresent155.
DirecttraumaThereisgeneralagreementthatacutemuscleover-
load can activate MTrPs, although systematic studiesarelacking169.Forexample,peopleinvolvedinwhiplashinjuries commonly experience prolonged muscle painanddysfunction170-173. Ina retrospective review,Schul-leretal174foundthat80%of1096subjectsinvolvedinlow-velocitycollisionsdemonstratedevidenceofmusclepain with myogeloses among the most common find-
ings. Although Schuller et al174 did not define thesemyogeloses, Simons has suggested that a myogelosisdescribesthesameclinicalentityasanMTrP175.Baker117reported that thespleniuscapitis, semispinaliscapitis,andsternocleidomastoidmusclesdevelopedsymptomaticMTrPs in77%,62%,and52%of52whiplashpatients,respectively.Inaretrospectivereviewof54consecutivechronic whiplash patients, Gerwin and Dommerholt176reported that clinically relevant MTrPs were found ineverypatient,withthetrapeziusmuscleinvolvedmostoften.FollowingtreatmentemphasizingtheinactivationofMTrPsandrestorationofnormalmusclelength,ap-proximately80%ofpatientsexperiencedlittleornopain,even though the average time following the initiatinginjurywas2.5yearsat thebeginningof the treatmentregimen.Allpatientshadbeenseenpreviouslybyotherphysicians and physical therapists who apparently hadnot considered MTrPs in their thought process andclinicalmanagement176.Fernández-de-las-Peñasetal177,178confirmedthatinactivationofMTrPsshouldbeincludedinthemanagementofpersonssufferingfromwhiplash-associateddisorders.Intheirresearch-basedtreatmentprotocol,thecombinationofcervicalandthoracicspinemanipulations with MTrP treatments proved superiorto more conventional physical therapy consisting ofmassage, ultrasound, home exercises, and low-energyhigh-frequencypulsedelectromagnetictherapy177.
Directtraumamaycreateaviciouscycleofeventswherein damage to the sarcoplasmic reticulum or themuscle cell membrane may lead to an increase of thecalciumconcentration,asubsequentactivationofactinandmyosin,arelativeshortageofadenosinetriphosphate(ATP), and an impaired calcium pump, which in turnwill increase the intracellular calcium concentrationevenmore,completingthecycle.Thecalciumpumpisresponsible for returning intracellular Ca2+ to the sar-coplasmic reticulum against a concentration gradient,whichrequiresafunctionalenergysupply.SimonsandTravell179 considered this sequence in thedevelopmentof the so-called “energy crisis hypothesis” introducedin 1981. Sensory and motor system dysfunction havebeenshowntodeveloprapidlyafterinjuryandactuallymaypersist in thosewhodevelopchronicmusclepainand in individuals who have recovered or continue tohave persistent mild symptoms172,180. Scott et al181 de-termined that individuals with chronic whiplash paindevelopmorewidespreadhypersensitivitytomechanicalpressure and thermal stimuli than those with chronicidiopathic neck pain. Myofascial trigger points are alikely source of ongoing peripheral nociceptive input,and they contribute to both peripheral and centralsensitization, which may explain the observation ofwidespreadallodyniaandhypersensitivity60,62,63.Inaddi-tion to being caused by whiplash injury, acute muscleoverloadcanoccurwithdirect impact, lifting injuries,sportsperformance,etc.182.

210 / The Journal of Manual & Manipulative Therapy, 2006
Eccentricand(sub)maximalconcentriccontractionsManypatientsreporttheonsetofpainandactivation
of MTrPs following either acute, repetitive, or chronicmuscleoverload183.Gerwinetal184suggestedthatlikelymechanisms relevant for the development of MTrPsincluded either unaccustomed eccentric exercise, ec-centric exercise in unconditioned muscle, or maximalor sub-maximal concentric exercise. A brief review ofpertinentaspectsofexercisefollows,precedinglinkingthisbodyofresearchtocurrentMTrPresearch.
Eccentricexerciseisassociatedwithmyalgia,muscleweakness, and destruction of muscle fibers, partiallybecause eccentric contractions cause an irregular andunevenlengtheningofmusclefibers185-187.Musclesore-ness and pain occur because of local ultra-structuraldamage,thereleaseofsensitizingalgogenicsubstances,and the subsequent onset of peripheral and centralsensitization85,188-190.Muscledamageoccursatthecyto-skeletallevelandfrequentlyinvolvesdisorganizationoftheA-band,streamingoftheZ-band,anddisruptionofcytoskeletalproteins,suchastitin,nebulin,anddesmin,evenafterveryshortboutsofeccentricexercise186,189-194.Lossofdesmincanoccurwithin5minutesofeccentricloading,eveninmusclesthatroutinelycontracteccen-tricallyduringfunctionalactivities,butdoesnotoccurafter isometric or concentric contractions193,195. Lieberand Fridén193 suggested that the rapid loss of desminmightindicateatypeofenzymatichydrolysisorproteinphosphorylationasalikelymechanism.
Oneoftheconsequencesofmuscledamageismuscleweakness196-198. Furthermore, concentric and eccentriccontractions are linked to contraction-induced capil-laryconstrictions, impairedbloodflow,hypoperfusion,ischaemia, and hypoxia, which in turn contribute tothedevelopmentofmoremuscledamage,alocalacidicmilieu,andanexcessivereleaseofprotons(H+),potassium(K+),calcitonin-gene-related-peptide(CGRP),bradykinin(BK),andsubstanceP(SP),andsensitizationofmusclenociceptors184,188. There are striking similarities withthe chemical environment of active MTrPs establishedwith microdialysis, suggesting an overlap between theresearchoneccentricexerciseandMTrPresearch184,199.However,atthistime,itisprematuretoconcludethatthereissolidevidencethateccentricandsub-maximalconcentric exercise are absolute precursors to the de-velopment of MTrPs. In support of this hypothesizedcausal relation, Itoh et al200 demonstrated in a recentstudythateccentricexercisecanleadtotheformationoftautandtenderropybandsinexercisedmuscle,andtheyhypothesizedthateccentricexercisemayindeedbeausefulmodelforthedevelopmentofMTrPs.
Eccentric and concentric exercise andMTrPshavebeen associated with localized hypoxia, which appearsto be one of the most important precursors for thedevelopment of MTrPs201. As mentioned, hypoxia leadstothereleaseofmultiplealgogenicsubstances.Inthis
context, recentresearchbyShahetal199at theUSNa-tionalInstitutesofHealthisparticularlyrelevant.Shahetalanalyzed thechemicalmilieuof latentandactiveMTrPsandnormalmuscles.Theyfoundsignificantlyin-creasedconcentrationsofBK,CGRP,SP,tumornecrosisfactor-α(TNF-α),interleukin-1β(IL-1β),serotonin,andnorepinephrineintheimmediatemilieuofactiveMTrPsonly199.Thesesubstancesarewell-knownstimulantsforvariousmusclenociceptorsandbindtospecificreceptormoleculesofthenerveendings,includingtheso-calledpurinergicandvanilloidreceptors85,202.
Muscle nociceptors are dynamic structures whosereceptors can change depending on the local tissueenvironment. When a muscle is damaged, it releasesATP, which stimulates purinergic receptors, which aresensitivetoATP,adenosinediphosphate,andadenosine.TheybindATP,stimulatemusclenociceptors,andcausepain.VanilloidreceptorsaresensitivetoheatandrespondtoanincreaseinH+-concentration,whichisespeciallyrelevant under conditions with a lowered pH, such asischaemia, inflammation, or prolonged and exhaustivemusclecontractions85.Shahetal199determinedthatthepH at active MTrP sites is significantly lower than atlatentMTrPsites.AloweredpHcaninitiateandmain-tainmusclepainandmechanicalhyperalgesiathroughactivationofacid-sensingionchannels203,204.Neuroplasticchanges in the central nervous system facilitate me-chanical hyperalgesia even after the nociceptive inputhas been terminated (central sensitization)203,204. Anynoxiousstimulussufficienttocausenociceptoractiva-tioncausesburstsofSPandCGRPtobe released intothemuscle,whichhaveasignificanteffectonthelocalbiochemicalmilieuandmicrocirculationbystimulating“feed-forward” neurogenic inflammation. Neurogenicinflammationcanbedescribedasacontinuouscycleofincreasing production of inflammatory mediators andneuropeptidesandanincreasingbarrageofnociceptiveinput into wide dynamic-range neurons in the spinalcorddorsalhorn184.
The integrated Trigger point HypothesisThe integrated triggerpointhypothesis (Figure7)
has evolved since its first introduction as the “energycrisishypothesis”in1981.Itisbasedonacombinationofelectrodiagnosticandhistopathologicalevidence179,183.
Alreadyin1957,WeeksandTravell205hadpublisheda report that outlined a characteristic electrical activ-ity of an MTrP. It was not until 1993 that Hubbard etal206 confirmed that this EMG discharge consists oflow-amplitudedischargesintheorderof10-50µVandintermittenthigh-amplitudedischarges(upto500µV)in painful MTrPs. Initially, the electrical activity wastermed “spontaneous electrical activity” (SEA) andthoughttoberelatedtodysfunctionalmusclespindles206.BestavailableevidencenowsuggeststhattheSEAisinfact endplate noise (EPN), which is found much more

Myofascial Trigger Points: An Evidence-Informed Review / 211
commonlyintheendplatezonenearMTrPsthaninanendplatezoneoutsideMTrPs207-209.Theelectricaldischargesoccurwith frequencies thatare10-1,000 times thatofnormalendplatepotentials,andtheyhavebeenfoundinhumans,rabbits,andrecentlyeven inhorses209,210.Thedischarges aremost likely the result of an abnormallyexcessive release of acetylcholine (ACh) and indicativeofdysfunctionalmotorendplates,contrarytothecom-monlyacceptednotionamongelectromyographersthatendplate noise arises from normal motor endplates183.The effectiveness of botulinum toxin in the treatmentofMTrPsprovides indirect evidenceof thepresenceofexcessiveACh211.Botulinumtoxin(BoTox)isaneurotoxinthatblocksthereleaseofAChfrompresynapticcholiner-gicnerveendings.Arecentstudyinmicedemonstratedthattheadministrationofbotulinumtoxinresultedinacompletefunctionalrepairofdysfunctionalendplates212.ThereissomeearlyevidencethatmusclestretchingandhypertonicitymayalsoenhancetheexcessivereleaseofACh213,214. Tension on the integrins in the presynapticmembraneatthemotornerveterminalishypothesizedto mechanically trigger an ACh release that does notrequireCa2+213-215.Integrinsarereceptorproteinsinthecellmembraneinvolvedinattachingindividualcellstotheextracellularmatrix.
Excessive ACh affects voltage-gated sodium chan-nels of the sarcoplasmic reticulum and increases theintracellular calcium levels, which triggers sustainedmuscle contractures. It is conceivable that in MTrPs,myosin filaments literally get stuck in the Z-band ofthe sarcomere. During sarcomere contractions, titinfilaments are folded into a gel-like structure at the Z-band.InMTrPs,thegel-liketitinmaypreventthemyosinfilaments from detaching. The myosin filaments mayactuallydamagetheregularmotorassemblyandprevent
thesarcomerefromrestoringitsrestinglength216.MusclecontracturesarealsomaintainedbecauseoftherelativeshortageofATPinanMTrP,asATPisrequiredtobreakthecross-bridgesbetweenactinandmyosin filaments.The question remains whether sustained contracturesrequireanincreaseofoxygenavailability.
Atthesametime,theshortenedsarcomerescompro-misethelocalcirculationcausingischaemia.StudiesofoxygensaturationlevelshavedemonstratedseverehypoxiainMTrPs201.Hypoxia leads to thereleaseof sensitizingsubstancesandactivatesmusclenociceptorsasreviewedabove.Thecombineddecreasedenergysupplyandpos-sible increased metabolic demand would also explainthe common finding of abnormal mitochondria in thenerveterminalandthepreviouslymentionedraggedredfibers.Inmice,theonsetofhypoxialedtoanimmediateincreasedAChreleaseatthemotorendplate217.
Thecombinedhigh-intensitymechanicalandchemi-cal stimuli may cause activation and sensitization ofthe peripheral nerve endings and autonomic nerves,activatesecondorderneuronsincludingso-called“sleep-ing”receptors,causecentral sensitization,and lead tothe formation of new receptive fields, referred pain, along-lasting increase intheexcitabilityofnociceptors,andamoregeneralizedhyperalgesiabeyondtheinitialnociceptivearea.Anexpansionofareceptivefieldmeansthat a dorsal horn neuron receives information fromareasithasnotreceivedinformationfrompreviously218.Sensitizationofperipheralnerveendingscanalsocausepain through SP activating the neurokin-1 receptorsandglutamateactivating N-methyl-D-aspartaterecep-tors,whichopenspost-synapticchannelsthroughwhichCa2+ ionscanenter thedorsalhornandactivatemanyenzymesinvolvedinthesensitization85.
Severalhistologicalstudiesofferfurthersupportfortheintegratedtriggerpointhypothesis.In1976,Simonsand Stolov published the first biopsy study of MTrPsin a canine muscle and reported multiple contractionknots invarious individualmuscle fibers (Figure8)219.Theknotsfeaturedacombinationofseverelyshortenedsarcomeres in the center and lengthened sarcomeresoutsidetheimmediateMTrPregion219.
Reitingeretal220reportedpathologicalterationsofthemitochondriaaswellasincreasedwidthofA-bandsanddecreasedwidthofI-bandsinmusclesarcomeresofMTrPs in thegluteusmediusmuscle.Windischetal221determinedsimilaralterationsinapost-mortemhisto-logicalstudyofMTrPscompletedwithin24hoursoftimeofdeath.Menseetal222studiedtheeffectsofelectricallyinducedmusclecontractionsandacholinesteraseblockeronmuscleswithexperimentallyinducedcontractionknotsandfoundevidenceoflocalizedcontractions,tornfibers,andlongitudinalstripes.PongratzandSpath223,224dem-onstratedevidenceofacontractiondiskinaregionofanMTrPusinglightmicroscopy.NewMTrPhistopathologicalstudiesarecurrentlybeingconductedat theFriedrich
Fig.7: The integrated trigger point hypothesis.Ach- acetylcholine; AchE- acetylcholinesterase; AchR- acetylcholine receptor

212 / The Journal of Manual & Manipulative Therapy, 2006
Baur Institute in Munich, Germany. Gariphianova225described pathological changes with biopsy studies ofMTrPs,includingadecreaseinquantityofmitochondria,possibly indicating metabolic distress. Several olderhistologicalstudiesareoftenquoted,butitisnotcleartowhatextentthosefindingsarespecificforMTrPs.In1951,GlogowskyandWallraff226reporteddamagedfibrilstructures.Fassbender227observeddegenerativechangesof the I-bands, inaddition tocapillarydamage,a focalaccumulation of glycogen, and a disintegration of themyofibrillarnetwork.
Thereisgrowingevidencefortheintegratedtriggerpointhypothesiswithregardtothemotorandsensoryaspects of MTrPs, but many questions remain aboutthe autonomic aspects. Several studies have shownthat MTrPs are influenced by the autonomic nervoussystem. Exposing subjects with active MTrPs in theupper trapeziusmuscles to stressful tasksconsistentlyincreased the electrical activity in MTrPs in the uppertrapeziusmusclebutnotincontrolpointsinthesamemuscle,whileautogenicrelaxationwasable toreversetheeffects228-231.Theadministrationofthesympatheticblockingagentphentolaminesignificantlyreducedtheelectrical activity of an MTrP228,232,233. The interactionsbetweentheautonomicnervoussystemandMTrPsneedfurther investigation. Hubbard228 maintained that theautonomic features of MTrPs are evidence that MTrPsmay be dysfunctional muscle spindles. Gerwin et al184have suggested that the presence of alpha and betaadrenergicreceptorsattheendplateprovideapossiblemechanism for autonomic interaction. In a rodent,stimulationof thealphaandbetaadrenergicreceptorsstimulated the release of ACh in the phrenic nerve234.Inarecentstudy,Geetal61provided for the first timeexperimentalevidenceofsympatheticfacilitationofme-
chanicalsensitizationofMTrPs,whichtheyattributedtoachangeinthelocalchemicalmilieuattheMTrPsduetoincreasedvasoconstriction,anincreasedsympatheticreleaseofnoradrenaline,oran increased sensitivity tonoradrenaline.Anotherintriguingpossibilityisthatthecytokine interleukin-8 (IL-8) found in the immediatemilieuofactiveMTrPsmaycontributetotheautonomicfeaturesofMTrP.IL-8caninducemechanicalhyper-no-ciception,whichisinhibitedbybetaadrenergicreceptorantagonists235.Shahetal foundsignificantly increasedlevelsof IL-8 in the immediatemilieuof activeMTrPs(Shah,2006,personalcommunication).
ThefindingsofShahetal199markamajormilestoneintheunderstandingandacceptanceofMTrPsandsupportpartsof the integrated triggerpointhypothesis183.Thepossibleconsequencesofseveralofthechemicalspresentin the immediate milieu of active MTrPs have beenexploredbyGerwinetal184.Asstated,ShahetalfoundsignificantlyincreasedconcentrationsofH+,BK,CGRP,SP,TNF-α,IL-1β,serotonin,andnorepinephrineinactiveMTrPsonly.TherearemanyinteractionsbetweenthesechemicalsthatallcancontributetothepersistentnatureofMTrPsthroughvariousviciousfeedbackcycles236.Forexample,BKisknowntoactivateandsensitizemusclenociceptors,whichleadstoinflammatoryhyperalgesia,an activation of high-threshold nociceptors associatedwithC-fibers,andevenan increasedproductionofBKitself.Furthermore,BKstimulatesthereleaseofTNF-α,whichactivatestheproductionoftheinterleukinsIL-1β,IL-6, and IL-8. Especially IL-8 can cause hyperalgesiathat is independent from prostaglandin mechanisms.Viaapositive feedback loop, IL-1βcanalso inducetherelease of BK237. Release of BK, K+, H+, and cytokinesfrom injuredmuscle activates themusclenociceptors,therebycausingtendernessandpain184.
Calcitonin gene-related peptide can enhance thereleaseofAChfromthemotorendplateandsimultane-ouslydecreasetheeffectivenessofacetylcholinesterase(AChE)inthesynapticcleft,whichdecreasestheremovalof ACh238,239. Calcitonin gene-related peptide also up-regulates theACh-receptors (AChR)at themuscleandtherebycreatesmoredockingstationsforACh.MiniatureendplateactivitydependsonthestateoftheAChRandon the local concentrationofACh,which is the resultof ACh-release, reuptake, and breakdown by AChE. Insummary, increased concentrations of CGRP lead to areleaseofmoreACh,andincreasetheimpactofAChbyreducingAChEeffectivenessandincreasingAChRefficiency.Miniature endplate potential frequency is increased asaresultofgreaterACheffect.TheobservedloweredpHhasseveral implicationsaswell.Notonlydoesa lowerpHenhancethereleaseofCGRP,italsocontributestoafurtherdown-regulationofAChE.Themultiplechemicalsand lowered pH found in active MTrPs can contributetothechronicnatureofMTrPs,enhancethesegmentalspreadofnociceptive inputintothedorsalhornofthe
Fig.8: Longitudinal section of a contraction knot in a canine gracilis muscle (reproduced with permission from: Simons DG, Travell JG, Simons LS. Travell and Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual. Vol. 1. 2nd ed. Baltimore, MD: Williams & Wilkins, 1999)
Myofascial Trigger Points: An Evidence-Informed Review / 213
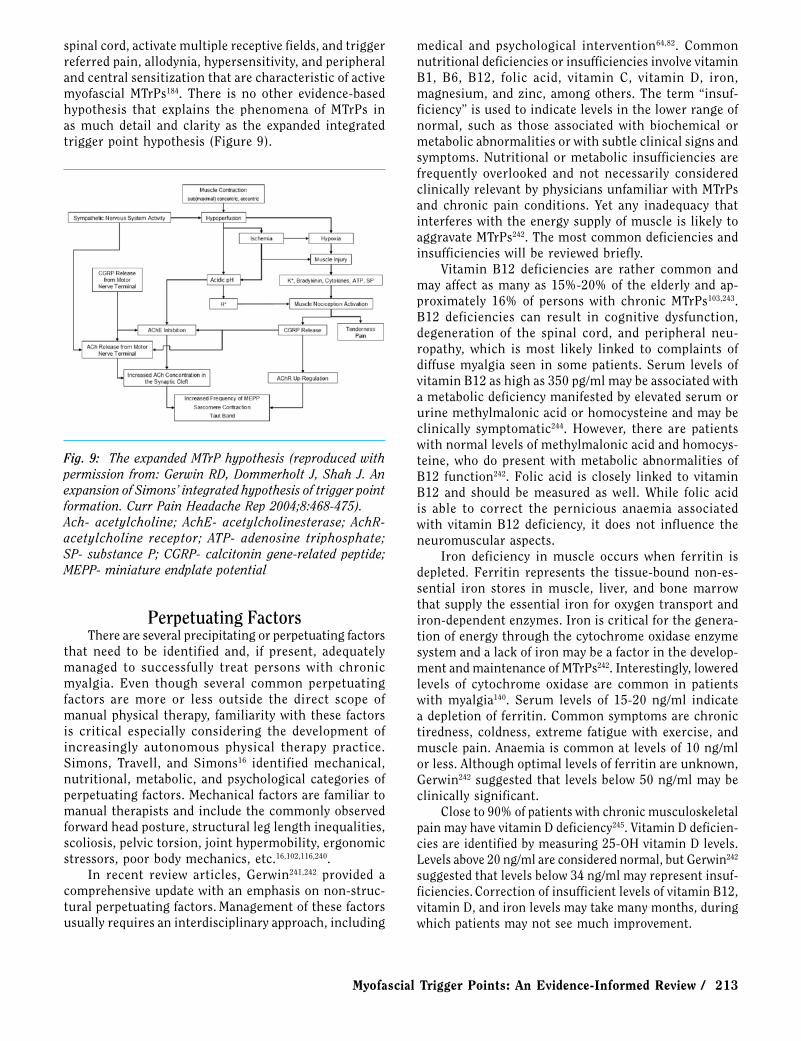
spinalcord,activatemultiplereceptivefields,andtriggerreferredpain,allodynia,hypersensitivity,andperipheralandcentralsensitizationthatarecharacteristicofactivemyofascial MTrPs184. There is no other evidence-basedhypothesis that explains the phenomena of MTrPs inas much detail and clarity as the expanded integratedtriggerpointhypothesis(Figure9).
medical and psychological intervention64,82. CommonnutritionaldeficienciesorinsufficienciesinvolvevitaminB1, B6, B12, folic acid, vitamin C, vitamin D, iron,magnesium,andzinc,amongothers.The term“insuf-ficiency”isusedtoindicatelevelsinthelowerrangeofnormal, such as those associated with biochemical ormetabolicabnormalitiesorwithsubtleclinicalsignsandsymptoms.Nutritionalormetabolic insufficienciesarefrequently overlooked and not necessarily consideredclinicallyrelevantbyphysiciansunfamiliarwithMTrPsand chronic pain conditions. Yet any inadequacy thatinterfereswiththeenergysupplyofmuscleislikelytoaggravateMTrPs242.Themostcommondeficienciesandinsufficiencieswillbereviewedbriefly.
Vitamin B12 deficiencies are rather common andmayaffectasmanyas15%-20%of theelderlyandap-proximately 16% of persons with chronic MTrPs103,243.B12 deficiencies can result in cognitive dysfunction,degeneration of the spinal cord, and peripheral neu-ropathy, which is most likely linked to complaints ofdiffusemyalgia seen in somepatients.Serum levelsofvitaminB12ashighas350pg/mlmaybeassociatedwithametabolicdeficiencymanifestedbyelevatedserumorurinemethylmalonicacidorhomocysteineandmaybeclinically symptomatic244. However, there are patientswithnormallevelsofmethylmalonicacidandhomocys-teine,whodopresentwithmetabolic abnormalities ofB12 function242. Folic acid is closely linked to vitaminB12 and should be measured as well. While folic acidis able to correct the pernicious anaemia associatedwith vitamin B12 deficiency, it does not influence theneuromuscularaspects.
Iron deficiency in muscle occurs when ferritin isdepleted. Ferritin represents the tissue-bound non-es-sential iron stores in muscle, liver, and bone marrowthatsupplytheessentialironforoxygentransportandiron-dependentenzymes.Ironiscriticalforthegenera-tionofenergythroughthecytochromeoxidaseenzymesystemandalackofironmaybeafactorinthedevelop-mentandmaintenanceofMTrPs242.Interestingly,loweredlevels of cytochrome oxidase are common in patientswith myalgia140. Serum levels of 15-20 ng/ml indicateadepletionofferritin.Commonsymptomsarechronictiredness, coldness, extreme fatiguewithexercise, andmusclepain.Anaemiaiscommonatlevelsof10ng/mlorless.Althoughoptimallevelsofferritinareunknown,Gerwin242suggestedthatlevelsbelow50ng/mlmaybeclinicallysignificant.
Closeto90%ofpatientswithchronicmusculoskeletalpainmayhavevitaminDdeficiency245.VitaminDdeficien-ciesareidentifiedbymeasuring25-OHvitaminDlevels.Levelsabove20ng/mlareconsiderednormal,butGerwin242suggestedthatlevelsbelow34ng/mlmayrepresentinsuf-ficiencies.CorrectionofinsufficientlevelsofvitaminB12,vitaminD,andironlevelsmaytakemanymonths,duringwhichpatientsmaynotseemuchimprovement.
Fig. 9: The expanded MTrP hypothesis (reproduced with permission from: Gerwin RD, Dommerholt J, Shah J. An expansion of Simons’ integrated hypothesis of trigger point formation. Curr Pain Headache Rep 2004;8:468-475).Ach- acetylcholine; AchE- acetylcholinesterase; AchR- acetylcholine receptor; ATP- adenosine triphosphate; SP- substance P; CGRP- calcitonin gene-related peptide; MEPP- miniature endplate potential
perpetuating factorsThereareseveralprecipitatingorperpetuatingfactors
that need to be identified and, if present, adequatelymanaged to successfully treat persons with chronicmyalgia. Even though several common perpetuatingfactors are more or less outside the direct scope ofmanualphysical therapy, familiaritywith these factorsis critical especially considering the development ofincreasingly autonomous physical therapy practice.Simons, Travell, and Simons16 identified mechanical,nutritional,metabolic, andpsychological categories ofperpetuatingfactors.Mechanicalfactorsarefamiliartomanualtherapistsandincludethecommonlyobservedforwardheadposture,structuralleglengthinequalities,scoliosis,pelvictorsion,jointhypermobility,ergonomicstressors,poorbodymechanics,etc.16,102,116,240.
In recent review articles, Gerwin241,242 provided acomprehensiveupdatewithanemphasisonnon-struc-turalperpetuatingfactors.Managementofthesefactorsusuallyrequiresaninterdisciplinaryapproach,including

214 / The Journal of Manual & Manipulative Therapy, 2006
Even when active MTrPs have been identified in aparticularpatient,cliniciansmustalwaysconsiderthatMTrPs may be secondary to metabolic insufficienciesorothermedicaldiagnoses. It isquestionablewhetherphysical therapy and—as an integral part of physicaltherapy management—manual therapy interventioncan be successful when patients have nutritional ormetabolicinsufficienciesordeficiencies.Acloseworkingrelationshipwithphysicians familiarwith thisbodyofliterature is essential. Therapists should consider thepossibleinteractionsbetweenarthrogenicorneurogenicdysfunctionandMTrPs4,5,118,133,246,247.
Clinically, physical therapists should address allaspectsof thedysfunction.Therearemanyothercon-ditions that featuremuscle pain andMTrPs, includinghypothyroidism, systemic lupus erythematosis, Lymedisease,babesiosis,ehrlichiosis,candidaalbicansinfec-tions,myoadenylatedeaminasedeficiency,hypoglycaemia,and parasitic diseases such as fascioliasis, amoebiasis,andgiardia64,242.Therapistsshouldbefamiliarwiththesymptomsassociatedwiththesemedicaldiagnoses64.
PsychologicalstressmayactivateMTrPs.Electromyo-graphic activity in MTrPs has been shown to increasedramaticallyinresponsetomentalandemotionalstress,whereasadjacentnon-triggerpointmuscleEMGactivityremained normal229, 230. Relaxation techniques, such asautogenicrelaxation,candiminishtheelectricalactiv-ity231.Inaddition,manypatientswithpersistentMTrPsaredealingwithdepression,anxiety,anger,andfeelingsofhopelessness248. Pain-related fear and avoidance canlead to the development and maintenance of chronicpain249.Sleepdisturbancecanalsobeamajorfactorinthe perpetuation of musculoskeletal pain and must beaddressed.Sleepproblemsmayberelatedtopain,apnea,ortomooddisorderslikedepressionoranxiety.Manage-mentcanbebothpharmacologicandnon-pharmacologic.Pharmacologic treatment utilizes drugs that promotenormal sleep patterns and induce and maintain sleepthrough the night without causing daytime sedation.Non-pharmacologictreatmentemphasizessleephygiene,
such as using the bed only for sleep and sex, and notforreading,televisionviewing,andeating250.Therapistsmust be sensitive to the impact of psychological andemotional distress and refer patients to clinical socialworkersorpsychologistswhenappropriate.
The role of Manual TherapyAlthough the various management approaches are
beyondthescopeofthisarticle,manualtherapyisoneofthebasictreatmentoptionsandtheroleoforthope-dic manual physical therapists cannot be overempha-sized82,158. Myofascial trigger points are treated withmanualtechniques,sprayandstretch,dryneedling,orinjection therapy. Dry needling is within the scope ofphysical therapy practice in many countries includingCanada, Spain, Ireland, South Africa, Australia, theNetherlands, and Switzerland. In the United States,the physical therapy boards of eight states have ruledthat physical therapists can engage in the practiceof dry needling: New Hampshire, Maryland, Virginia,South Carolina, Georgia, Kentucky, New Mexico, andColorado80. A promising new development used in thediagnosis and treatment of MTrPs involves shockwavetherapy, but as of yet, there are no controlled studiessubstantiatingitsuse251,252.
summaryAlthough MTrPs are a common cause of pain and
dysfunction in persons with musculoskeletal injuriesanddiagnoses,theimportanceofMTrPsisnotobviousfrom reviewing the orthopedic manual therapy litera-ture.Currentscientificevidencestronglysupportsthatawarenessandaworkingknowledgeofmuscledysfunc-tion; in particular, MTrPs should be incorporated intomanual physical therapy practice consistent with theIFOMTguidelinesforclinicalpractice.Whiletherearestillmanyunansweredquestionswithregardtoexplain-ingtheetiologyofMTrPs,thisarticleprovidesmanualtherapistswithanup-to-dateevidence-informedreviewofthecurrentscientificknowledge.
references1. IFOMT.Availableat:http://www.ifomt.org/ifomt/about/standards.
AccessedNovember15,2006.2. HuijbregtsPA.Muscleinjury,regeneration,andrepair.J Manual
Manipulative Ther2001;9:9-16.3. UrquhartDM,HodgesPW,AllenTJ,StoryIH.Abdominalmuscle
recruitment during a range of voluntary exercises. Man Ther2005;10:144-153.
4. Fernández-de-las-PeñasC,Alonso-BlancoC,Alguacil-DiegoIM,Miangolarra-PageJC.Myofascialtriggerpointsandpostero-an-
terior jointhypomobility inthemid-cervicalspine insubjectspresentingwithmechanicalneckpain:Apilotstudy.J Manual Manipulative Ther2006;14:88-94.
5. Fernández-de-las-Peñas C, Alonso-Blanco C, Miangolarra JC.Myofascialtriggerpointsinsubjectspresentingwithmechanicalneckpain:Ablinded,controlledstudyMan Ther(Inpress).
6. LewPC,LewisJ,StoryI. Inter-therapistreliability in locatinglatent myofascial trigger points using palpation. Man Ther1997;2:87-90.

Myofascial Trigger Points: An Evidence-Informed Review / 215
7. Fernández-de-las-PeñasC,Alonso-BlancoC,CuadradoML,ParejaJA. Myofascial trigger points in the suboccipital muscles inepisodictension-typeheadache.Man Ther2006;11:225-230.
8. MooreA,PettyN.Evidence-basedpractice:Gettingagripandfindingabalance.Man Ther2001;6:195-196.
9. SackettDL,RosenbergWM.Theneedforevidence-basedmedi-cine.J R Soc Med1995;88:620-624.
10. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, RichardsonWS.Evidence-basedmedicine:Whatitisandwhatitisn’t.BMJ 1996;312:71-72.
11. PencheonD.What’snextforevidence-basedmedicine?Evidence-Based Healthcare Public Health2005;9:319-321.
12. CiceroneKD.Evidence-basedpracticeandthelimitsofrationalrehabilitation.Arch Phys Med Rehabil2005;86:1073-1074.
13. Baldry PE. Acupuncture, Trigger Points and Musculoskeletal Pain.Edinburgh,UK:ChurchillLivingstone,2005.
14. Simons DG. Muscle pain syndromes. Part 1. Am J Phys Med1975;54:289-311.
15. RuhmannW.Theearliestbookonrheumatism.Br J Rheumatism1940;11:140-162.
16. SimonsDG,Travell JG,SimonsLS.Travell and Simons’ Myo-fascial Pain and Dysfunction: The Trigger Point Manual. Vol.1.2nded.Baltimore,MD:Williams&Wilkins,1999.
17. HardenRN,BruehlSP,GassS,NiemiecC,BarbickB.Signsandsymptomsof themyofascialpainsyndrome:Anational surveyofpainmanagementproviders.Clin J Pain2000;16:64-72.
18. StockmanR.Thecauses,pathology, and treatmentof chronicrheumatism.Edinburgh Med J1904;15:107-116.
19. StraussH.Űberdiesogenannten‚RheumatischeMuskelschwiele‘[German; With regard to the so-called myogelosis]. Klin Wo-chenschr1898;35:89-91,121-123.
20. LangeM.Die Muskelhärten (Myogelosen) [German;TheMuscleHardenings (Myogeloses)]. Munich, Germany: J.F. Lehmann‘sVerlag,1931.
21. Travell J.Office Hours: Day and Night. The Autobiography of Janet Travell, MD.NewYork,NY:WorldPublishing,1968.
22. KellgrenJH.Deeppainsensibility.Lancet1949;1:943-949.23. KellgrenJH.Observationsonreferredpainarisingfrommuscle.
Clin Sci1938;3:175-190.24. Kellgren JH. A preliminary account of referred pains arising
frommuscle.British Med J1938;1:325-327.25. SimonsDG.Cardiologyandmyofascialtriggerpoints:JanetG.
Travell’scontribution.Tex Heart Inst J2003;30(1):3-7.26. Travell J.Basis for themultipleusesof localblockof somatic
trigger areas (procaine infiltration and ethyl chloride spray).Miss Valley Med1949;71:13-22.
27. Travell J, Bobb AL. Mechanism of relief of pain in sprains bylocal injectiontechniques.Fed Proc1947;6:378.
28. Travell JG, Rinzler S, Herman M. Pain and disability of theshoulderandarm:Treatmentbyintramuscularinfiltrationwithprocainehydrochloride.JAMA1942;120:417-422.
29. TravellJG,RinzlerSH.Themyofascialgenesisofpain.Postgrad Med1952;11:452-434.
30. ChaitowL,DeLanyJ.Neuromusculartechniquesinorthopedics.Techniques in Orthopedics2003;18(1):74-86.
31. GoodMG.Fivehundred casesofmyalgia in theBritish army.Ann Rheum Dis1942;3:118-138.
32. Good MG. The role of skeletal muscle in the pathogenesis ofdiseases.Acta Medica Scand1950;138:285-292.
33. GutsteinM.Commonrheumatismandphysiotherapy.Br J Phys Med1940;3:46-50.
34. GutsteinM.Diagnosisandtreatmentofmuscularrheumatism.Br J Phys Med1938;1:302-321.
35. KellyM.Thenatureof fibrositis. I.Themyalgic lesionanditssecondaryeffects:Areflextheory.Ann Rheum Dis1945;5:1-7.
36. KellyM.Thenatureoffibrositis.II.Astudyofthecausationofthemyalgiclesion(rheumatic,traumatic,infective).Ann Rheum Dis1946;5:69-77.
37. KellyM.Thereliefoffacialpainbyprocaine(Novocaine)injec-tions.J Am Geriatr Soc1963;11:586-96.
38. KellyM.Thetreatmentoffibrositisandallieddisordersbylocalanesthesia.Med J Aust1941;1:294-298.
39. SchneiderM,CohenJ,LawsS.The Collected Writings of Nimmo & Vannerson: Pioneers of Chiropractic Trigger Point Therapy.Pittsburgh,PA:Schneider,2001.
40. CohenJH,GibbonsRW.RaymondL.Nimmoandtheevolutionoftriggerpointtherapy,1929-1986.J Manipulative Physiol Ther1998;21:167-172.
41. NationalBoardofChiropracticExaminers.Chiropractic Treat-ment Procedures.Greeley,CO:NBCE,1993.
42. MennellJ.Spray-stretchforthereliefofpainfrommusclespasmandmyofascialtriggerpoints.J Am Podiatry Assoc1976;66:873-876.
43. MennellJ.Myofascialtriggerpointsasacauseofheadaches.J Manipulative Physiol Ther,1989;12:308-313.
44. Travell W, Travell JG. Technic for reduction and ambulatorytreatmentofsacroiliacdisplacement.Arch Phys Ther1942;23:222-232.
45. Paris SV. In the best interests of the patient. Phys Ther2006;86:1541-1553.
46. TravellJG,SimonsDG.Myofascial Pain and Dysfunction: The Trigger Point Manual.Vol.2.Baltimore,MD:Williams&Wilkins,1992.
47. TravellJG,SimonsDG.Myofascial Pain and Dysfunction: The Trigger Point Manual.Vol.1.Baltimore,MD:Williams&Wilkins,1983.
48. DejungB,GröbliC,CollaF,WeissmannR.Triggerpunkttherapie [German;TriggerPointTherapy].Bern,Switzerland:HansHuber,2003.
49. FergusonLW,GerwinR.Clinical Mastery in the Treatment of Myofascial Pain.Philadelphia,PA:LippincottWilliams&Wilkins,2005.
50. KostopoulosD,RizopoulosK.The Manual of Trigger Point and Myofascial Therapy.Thorofare,NJ:Slack,2001.
51. PrateepavanichP.Myofascial Pain Syndrome: A Common Problem in Clinical Practice.Bangkok,Thailand:Ammarind,1999.
52. Rachlin ES, Rachlin IS. Myofascial Pain and Fibromyalgia: Trigger Point Management.St.Louis,MO:Mosby,2002.
53. Cardinal S. Points Détente et Acupuncture: Approche Neuro-physiologique [French;TriggerPointsandAcupuncture:Neu-rophysiologicalApproach].Montreal,Canada:CentreCollégialdeDéveloppementdeMatérielDidactique,2004.
54. JonckheerePDM.Spieren en Dysfuncties, Trigger punten, Ba-sisprincipes van de Myofasciale Therapie [Dutch;MusclesandDysfunctions,BasicPrinciplesofMyofascialTherapy]. Brussels,Belgium:Satas,1993.
55. LucasKR,PolusBI,RichPS.Latentmyofascialtriggerpoints:Their effect on muscle activation and movement efficiency. J Bodywork Mov Ther2004;8:160-166.
56. Weissmann RD. Überlegungen zur Biomechanik in der Myo-faszialen Triggerpunkttherapie [German; Considerations withregardtothebiomechanicsrelatedtomyofascialtriggerpoint
216 / The Journal of Manual & Manipulative Therapy, 2006
therapy].Physiotherapie2000;35(10):13-21.57. Vecchiet L, Giamberardino MA, De Bigontina P. Comparative
sensoryevaluationofparietaltissuesinpainfulandnonpainfulareasinfibromyalgiaandmyofascialpainsyndrome.In:GebhartGF,HammondDL,JensenTS,eds. Proceedings of the 7th World Congress on Pain (Progress in Pain Research and Management).Seattle,WA:IASPPress,1994:177-185.
58. Vecchiet L, Giamberardino MA, Dragani L. Latent myofascialtrigger points: Changes in muscular and subcutaneous painthresholdsattriggerpointandtargetlevel.J Manual Medicine1990;5:151-154.
59. VecchietL,PizzigalloE,IezziS,AffaitatiG,VecchietJ,Giambe-rardinoMA.Differentiationofsensitivityindifferenttissuesanditsclinicalsignificance.J Musculoskeletal Pain1998;6:33-45.
60. DommerholtJ.Persistentmyalgiafollowingwhiplash.Curr Pain Headache Rep2005;9:326-330.
61. GeHY,Fernández-de-las-PeñasC,Arendt-NielsenL.Sympatheticfacilitationofhyperalgesiaevoked frommyofascial tenderandtrigger points in patients with unilateral shoulder pain. Clin Neurophysiol2006;117:1545-1550.
62. LidbeckJ.Centralhyperexcitabilityinchronicmusculoskeletalpain:Aconceptualbreakthroughwithmultipleclinicalimplica-tions.Pain Res Manag2002;7(2):81-92.
63. Munglani R. Neurobiological mechanisms underlying chronicwhiplashassociatedpain:Theperipheralmaintenanceofcentralsensitization.J Musculoskeletal Pain2000;8:169-178.
64. Dommerholt J, Issa T. Differential diagnosis: Myofascial pain.In: Chaitow L, ed. Fibromyalgia Syndrome: A Practitioner’s Guide to Treatment. Edinburgh, UK: Churchill Livingstone,2003:149-177.
65. GerwinRD,ShannonS,HongCZ,HubbardD,GevirtzR.Inter-rater reliability in myofascial trigger point examination. Pain1997;69(1-2):65-73.
66. SciottiVM,MittakVL,DiMarcoL,FordLM,PlezbertJ,SantipadriE,WigglesworthJ,BallK.Clinicalprecisionofmyofascialtriggerpoint location in the trapezius muscle. Pain 2001;93(3):259-266.
67. FranssenJLM.Handboek Oppervlakte Elektromyografie [Dutch;ManualSurfaceElectromyography].Utrecht,TheNetherlands:DeTijdstroom,1995.
68. Janda V. Muscle spasm: A proposed procedure for differentialdiagnosis.J Manual Med1991;6:136-139.
69. MenseS.Pathophysiologicbasisofmusclepainsyndromes.In:FischerAA,ed.Myofascial Pain: Update in Diagnosis and Treat-ment.Philadelphia,PA:W.B.SaundersCompany,1997:23-53.
70. HeadlyBJ.Evaluationandtreatmentofmyofascialpainsyndromeutilizingbiofeedback.In:CramJR,ed.Clinical Electromyogra-phy for Surface Recordings.NevadaCity,NV:ClinicalResources,1990:235-254.
71. HeadlyBJ.Chronicpainmanagement.In:O’SullivanSB,SchmitzTS, eds. Physical Rehabilitation: Assessment and Treatment.Philadelphia,PA:F.A.DavisCompany,1994:577-600.
72. Gerwin RD, Duranleau D. Ultrasound identification of themyofascialtriggerpoint.Muscle Nerve1997;20:767-768.
73. Hong CZ. Persistence of local twitch response with loss ofconductiontoandfromthespinalcord.Arch Phys Med Rehabil1994;75:12-16.
74. Hong C-Z, Torigoe Y. Electrophysiological characteristics oflocalized twitch responses in responsive taut bands of rabbitskeletalmuscle.J Musculoskeletal Pain1994;2:17-43.
75. HongC-Z,YuJ.Spontaneouselectricalactivityof rabbit trig-
ger spotafter transectionof spinalcordandperipheralnerve.J Musculoskeletal Pain1998;6(4):45-58.
76. Fricton JR, Auvinen MD, Dykstra D, Schiffman E. Myofascialpainsyndrome:Electromyographicchangesassociatedwithlocaltwitchresponse.Arch Phys Med Rehabil1985;66:314-317.
77. Simons DG, Dexter JR. Comparison of local twitch responseselicitedbypalpationandneedlingofmyofascialtriggerpoints.J Musculoskeletal Pain1995;3:49-61.
78. WangF,AudetteJ.Electrophysiologicalcharacteristicsofthelocaltwitchresponsewithactivemyofascialpainofneckcomparedwithacontrolgroupwithlatenttriggerpoints.Am J Phys Med Rehabil2000;79:203.
79. AudetteJF,WangF,SmithH.Bilateralactivationofmotorunitpotentialswithunilateralneedlestimulationofactivemyofascialtrigger points. Am J Phys Med Rehabil 2004;83:368-374, quiz375-377,389.
80. Dommerholt J. Dry needling in orthopedic physical therapypractice.Orthop Phys Ther Pract2004;16(3):15-20.
81. HongC-Z.Lidocaineinjectionversusdryneedlingtomyofascialtriggerpoint:Theimportanceofthelocaltwitchresponse.Am J Phys Med Rehabil1994;73:256-263.
82. GerwinRD,Dommerholt J.Treatmentofmyofascialpainsyn-dromes. In:BoswellMV,ColeBE,eds.Weiner’s Pain Manage-ment: A Practical Guide for Clinicians. Boca Raton, FL: CRCPress,2006:477-492.
83. VecchietL,DraganiL,DeBigontinaP,ObletterG,GiamberardinoMA.Experimentalreferredpainandhyperalgesiafrommusclesin humans. In: Vecchiet L, et al, eds. New Trends in Referred Pain and Hyperalgesia.Amsterdam,TheNetherlands:ElsevierScience,1993:239-249.
84. VecchietL,GiamberardinoMA.Referredpain:Clinicalsignificance,pathophysiologyandtreatment.In:FischerAA,ed.Myofascial Pain: Update in Diagnosis and Treatment. Philadelphia, PA:W.B.SaundersCompany,1997:119-136.
85. MenseS.Thepathogenesisofmusclepain.Curr Pain Headache Rep2003;7:419-425.
86. MenseS.Referralofmusclepain:Newaspects.Amer Pain Soc J1994;3:1-9.
87. Fernández-de-las-Peñas CF, Cuadrado ML, Gerwin RD, ParejaJA. Referred pain from the trochlear region in tension-typeheadache:Amyofascialtriggerpointfromthesuperiorobliquemuscle.Headache2005;45:731-737.
88. Fernández-de-las-Peñas C, Cuadrado ML, Gerwin RD, ParejaJA. Myofascial disorders in the trochlear region in unilateralmigraine: A possible initiating or perpetuating factor. Clin J Pain2006;22:548-553.
89. Hwang M, Kang YK, Kim DH. Referred pain pattern of thepronatorquadratusmuscle.Pain2005;116:238-242.
90. HwangM,KangYK,ShinJY,KimDH.Referredpainpatternofthe abductor pollicis longus muscle. Am J Phys Med Rehabil2005;84:593-597.
91. HongCZ,KuanTS,Chen JT,ChenSM.Referredpain elicitedby palpation and by needling of myofascial trigger points: Acomparison.Arch Phys Med Rehabil1997;78:957-960.
92. DwyerA,AprillC,BogdukN.Cervicalzygapophysealjointpainpatterns. I: A study in normal volunteers. Spine 1990;15:453-457.
93. GiamberardinoMA,VecchietL.Visceralpain,referredhyperal-gesia andoutcome:Newconcepts.Eur J Anaesthesiol (Suppl)1995;10:61-66.
94. ScuddsRA,LandryM,BirminghamT,BuchanJ,GriffinK.The

Myofascial Trigger Points: An Evidence-Informed Review / 217
frequency of referred signs from muscle pressure in normalhealthysubjects(abstract).J Musculoskeletal Pain1995;3(Suppl.1):99.
95. TorebjörkHE,Ochoa JL,SchadyW.Referredpain from intra-neuralstimulationofmusclefasciclesinthemediannerve.Pain1984;18:145-156.
96. Gibson W, Arendt-Nielsen L, Graven-Nielsen T. Referred painand hyperalgesia in human tendon and muscle belly tissue.Pain2006;120(1-2):113-123.
97. Gibson W, Arendt-Nielsen L, Graven-Nielsen T. Delayed onsetmusclesorenessattendon-bonejunctionandmuscletissueisassociated with facilitated referred pain. Exp Brain Res 2006(Inpress).
98. HendlerNH,KozikowskiJG.Overlookedphysicaldiagnosesinchronic pain patients involved in litigation. Psychosomatics1993;34:494-501.
99. WeinerDK,SakamotoS,PereraS,BreuerP.Chroniclowbackpaininolderadults:Prevalence,reliability,andvalidityofphysi-calexaminationfindings.J Am Geriatr Soc2006;54:11-20.
100.CalandreEP,HidalgoJ,Garcia-Leiva JM,Rico-VillademorosF.Triggerpointevaluationinmigrainepatients:Anindicationofperipheralsensitizationlinkedtomigrainepredisposition?Eur J Neurol2006;13:244-249.
101.Headache Classification Subcommittee of the InternationalHeadacheSociety:Theinternationalclassificationofheadachedisorders.Cephalalgia2004;24(Suppl1):9-160.
102.FrictonJR,KroeningR,HaleyD,SiegertR.Myofascialpainsyn-dromeoftheheadandneck:Areviewofclinicalcharacteristicsof164patients.Oral Surg Oral Med Oral Pathol1985;60:615-623.
103.Gerwin R. A study of 96 subjects examined both for fibromy-algia and myofascial pain (abstract). J Musculoskeletal Pain1995;3(Suppl1):121.
104.RosomoffHL,FishbainDA,GoldbergN,RosomoffRS.Myofascialfindingswithpatientswithchronic intractablebenignpainofthebackandneck.Pain Management1989;3:114-118.
105.SkootskySA, JaegerB,OyeRK.Prevalenceofmyofascialpainingeneralinternalmedicinepractice.West J Med1989;151:157-160.
106.ChaiamnuayP,DarmawanJ,MuirdenKD,AssawatanabodeeP.Epidemiologyofrheumaticdisease inruralThailand:AWHO-ILAR COPCORD study. Community Oriented Programme fortheControlofRheumaticDisease.J Rheumatol1998;25:1382-1387.
107.Graff-RadfordB.Myofascialtriggerpoints:Theirimportanceanddiagnosisinthedentaloffice.J Dent Assoc S Afr 1984;39:249-253.
108.Bajaj P, Bajaj P, Graven-Nielsen T, Arendt-Nielsen L. Triggerpointsinpatientswithlowerlimbosteoarthritis.J Musculosk-eletal Pain2001;9(3):17-33.
109.Hsueh TC, Yu S, Kuan TS, Hong C-Z. Association of activemyofascial trigger points and cervical disc lesions. J Formosa Med Assoc1998;97(3):174-80.
110.WangC-F,ChenM,LinM-T,KuanT-S,HongC-Z.Teresminortendinitis manifested with chronic myofascial pain syndromeinthescapularmuscles:Acasereport.J Musculoskeletal Pain2006;14(1):39-43.
111.FrictonJR.Etiologyandmanagementofmasticatorymyofascialpain.J Musculoskeletal Pain1999;7(1/2):143-160.
112.TeacheyWS.Otolaryngicmyofascialpainsyndromes.Curr Pain Headache Rep2004;8:457-462.
113.Dommerholt J. El sindrome de dolor miofascial en la regioncraneomandibular. [Spanish; Myofascial pain syndrome inthe craniomandibular region]. In: Padrós Serrat E, ed. Bases diagnosticas, terapeuticas y posturales del functionalismo craniofacial.Madrid,Spain:Ripano,2006:564-581.
114.HesseJ,MogelvangB,SimonsenH.Acupunctureversusmeto-prolol in migraine prophylaxis: A randomized trial of triggerpointinactivation.J Intern Med1994;235:451-456.
115.Skubick DL, Clasby R, Donaldson CC, Marshall WM. Carpaltunnel syndromeas anexpressionofmusculardysfunction intheneck.J Occupational Rehab1993;3:31-43.
116.TreasterD,MarrasWS,BurrD,SheedyJE,HartD.Myofascialtrigger point development from visual and postural stressorsduring computer work. J Electromyogr Kinesiol 2006;16:115-124.
117.Baker BA. The muscle trigger: Evidence of overload injury. J Neurol Orthop Med Surg1986;7:35-44.
118.FruthSJ.Differentialdiagnosisandtreatmentinapatientwithposteriorupperthoracicpain.Phys Ther2006;86:254-268.
119.Doggweiler-WiygulR.Urologicmyofascialpainsyndromes.Curr Pain Headache Rep2004;8:445-451.
120. JarrellJ.Myofascialdysfunctioninthepelvis.Curr Pain Head-ache Rep2004;8:452-456.
121. Jarrell JF,VilosGA,AllaireC,BurgessS,FortinC,GerwinR,LapenseeL,LeaRH,LeylandNA,MartynP,ShenassaH,TaenzerP, Abu-Rafea B. Consensus guidelines for the management ofchronicpelvicpain.J Obstet Gynaecol Can2005;27:869-887.
122.WeissJM.Pelvicfloormyofascialtriggerpoints:Manualtherapyfor interstitialcystitisandtheurgency-frequencysyndrome.J Urol2001;166:2226-2231.
123.Dommerholt J. Muscle pain syndromes. In: Cantu RI, GrodinAJ, eds. Myofascial Manipulation. Gaithersburg, MD: Aspen,2001:93-140.
124.WeinerDK,SchmaderKE.Postherpeticpain:Morethansensoryneuralgia?Pain Med2006;7:243-249;discussion250.
125.ChenSM,ChenJT,KuanTS,HongC-Z.Myofascialtriggerpointsinintercostalmusclessecondarytoherpeszosterinfectionoftheintercostalnerve.Arch Phys Med Rehabil1998;79:336-338.
126.Dommerholt J.Complex regional pain syndrome.Part 1:His-tory, diagnostic criteria and etiology. J Bodywork Mov Ther2004;8:167-177.
127.RashiqS,GalerBS.Proximalmyofascialdysfunctionincomplexregionalpainsyndrome:Aretrospectiveprevalencestudy.Clin J Pain,1999;15:151-153.
128.PrateepavanichP,KupniratsaikulVC.Therelationshipbetweenmyofascialtriggerpointsofgastrocnemiusmuscleandnocturnalcalfcramps.J Med Assoc Thailand1999;82:451-459.
129.KernKU,MartinC,ScheicherS,MullerH.AuslosungvonPhan-tomschmerzenund-sensationendurchMuskuläreStumpftrig-gerpunkte nach Beinamputationen [German; Referred painfromamputationstumptriggerpointsintothephantomlimb].Schmerz2006;20:300-306.
130.KernU,MartinC,ScheicherS,MűllerH.DoesbotulinumtoxinA make prosthesis use easier for amputees? J Rehabil Med2004;36:238-239.
131.Longbottom J. A case report of postulated “Barré Liéou syn-drome.”Acupunct Med2005;23:34-38.
132.Stellon A. Neurogenic pruritus: An unrecognized problem? Aretrospectivecaseseriesoftreatmentbyacupuncture.Acupunct Med2002;20:186-190.
133.Fernández-de-las-Peñas C, Fernández-Carnero J, Miangolarra-
218 / The Journal of Manual & Manipulative Therapy, 2006
Page JC. Musculoskeletal disorders in mechanical neck pain:Myofascial trigger points versus cervical joint dysfunction. J Musculoskeletal Pain2005;13(1):27-35.
134.Hägg GM. Ny förklaringsmodell för muskelskador vid statiskbelastning i skuldra och nacke [Swedish; New explanationfor muscle damage as a result of static loads in the neck andshoulder].Arbete Människa Miljö1988;4:260-262.
135.Henneman E, Somjen G, Carpenter DO. Excitability and in-hibitability of motoneurons of different sizes. J Neurophysiol1965;28:599-620.
136.HäggGM.TheCinderellaHypothesis.In:JohanssonH,etal,eds.Chronic Work-Related Myalgia.Gävle,Sweden:GävleUniversityPress,2003:127-132.
137.Armstrong RB. Initial events in exercise-induced muscularinjury.Med Sci Sports Exerc1990;22:429-435.
138.Hägg GM. Human muscle fibre abnormalities related to oc-cupationalload.Eur J Appl Physiol2000;83(2-3):159-165.
139.KadiF,HaggG,HakanssonR,HolmnerS,Butler-BrowneGS,ThornellLE.Structuralchangesinmaletrapeziusmusclewithwork-related myalgia. Acta Neuropathol (Berl) 1998;95:352-360.
140.KadiF,WalingK,AhlgrenC,SundelinG,HolmnerS,Butler-BrowneGS,ThornellLE.Pathologicalmechanismsimplicatedinlocalizedfemaletrapeziusmyalgia.Pain1998;78:191-196.
141.LarssonB,BjorkJ,KadiF,LindmanR,GerdleB.Bloodsupplyandoxidativemetabolisminmusclebiopsiesoffemalecleanerswithandwithoutmyalgia.Clin J Pain2004;20:440-446.
142.HenrikssonKG,BengtssonA,LindmanR,ThornellLE.Morpho-logicalchangesinmuscleinfibromyalgiaandchronicshouldermyalgia.In:VærøyH,MerskeyH,eds. Progress in Fibromyalgia and Myofascial Pain. Amsterdam, The Netherlands: Elsevier,1993:61-73.
143.LexellJ,JarvisJ,DownhamD,SalmonsS.Stimulation-induceddamage in rabbit fast-twitch skeletal muscles: A quantitativemorphologicalstudyoftheinfluenceofpatternandfrequency.Cell Tissue Res1993;273:357-362.
144.GisselH.Ca2+accumulationandcelldamageinskeletalmuscleduringlowfrequencystimulation.Eur J Appl Physiol2000;83(2-3):175-180.
145.Gissel H, Clausen T. Excitation-induced Ca(2+) influx in ratsoleus and EDL muscle: Mechanisms and effects on cellularintegrity. Am J Physiol Regul Integr Comp Physiol 2000;279:R917-924.
146.Febbraio MA, Pedersen BK. Contraction-induced myokineproductionandrelease:Isskeletalmuscleanendocrineorgan?Exerc Sport Sci Rev2005;33(3):114-119.
147.PedersenBK,FebbraioM.Muscle-derivedinterleukin-6:Apos-sible link between skeletal muscle, adipose tissue, liver, andbrain.Brain Behav Immun2005;19:371-376.
148.ForsmanM,BirchL,ZhangQ,KadeforsR.Motorunitrecruit-ment in the trapeziusmusclewith special reference tocoarsearmmovements.J Electromyogr Kinesiol2001;11:207-216.
149.ForsmanM,KadeforsR,ZhangQ,BirchL,PalmerudG.Motor-unitrecruitmentinthetrapeziusmuscleduringarmmovementsandinVDUprecisionwork.Int J Ind Ergon1999;24:619-630.
150.ForsmanM,TaodaK,ThornS,ZhangQ.Motor-unitrecruitmentduring long-term isometric and wrist motion contractions:A study concerning muscular pain development in computeroperators.Int J Ind Ergon2002;30:237-250.
151.ZennaroD,LaubliT,KrebsD,KlipsteinA,KruegerH.Continu-ous,intermittedandsporadicmotorunitactivityinthetrape-
ziusmuscleduringprolongedcomputerwork.J Electromyogr Kinesiol2003;13:113-124.
152.ZennaroD,LaubliT,KrebsD,KruegerH,KlipsteinA.Trapeziusmusclemotorunitactivityinsymptomaticparticipantsduringfinger tapping using properly and improperly adjusted desks.Hum Factors2004;46:252-66.
153.Andersen JH, Kærgaard A, Rasmussen K. Myofascial pain indifferentoccupationalgroupswithmonotonousrepetitivework(abstract).J Musculoskeletal Pain1995;3(Suppl1):57.
154.ChenS-M,ChenJ-T,KuanT-S,HongJ,HongC-Z.Decreaseinpressurepainthresholdsof latentmyofascial triggerpoints inthemiddlefingerextensorsimmediatelyaftercontinuouspianopractice.J Musculoskeletal Pain2000;8(3):83-92.
155.Otten E. Concepts and models of functional architecture inskeletalmuscle.Exerc Sport Sci Rev1988;16:89-137.
156.SjogaardG,LundbergU,KadeforsR.Theroleofmuscleactivityand mental load in the development of pain and degenerativeprocesses at themuscle cell levelduringcomputerwork.Eur J Appl Physiol2000;83(2-3):99-105.
157.Sjogaard G, Sogaard K. Muscle injury in repetitive motiondisorders.Clin Orthop 1998;351:21-31.
158.Simons DG. Understanding effective treatments of myofascialtriggerpoints.J Bodywork Mov Ther2002;6:81-88.
159.ProskeU,MorganDL.Stiffnessofcatsoleusmuscleandtendonduringactivationofpartofmuscle.J Neurophysiol1984;52:459-468.
160.Trotter JA. Functional morphology of force transmission inskeletalmuscle:Abriefreview.Acta Anat (Basel)1993;146(4):205-222.
161.Monti RJ, Roy RR, Hodgson JA, Edgerton VR. Transmissionof forces within mammalian skeletal muscles. J Biomech1999;32:371-380.
162.BodineSC,RoyRR,EldredE,EdgertonVR.Maximalforceasafunctionofanatomicalfeaturesofmotorunitsinthecattibialisanterior.J Neurophysiol1987;57:1730-1745.
163.OunjianM,RoyRR,EldredE,GarfinkelA,PayneJR,ArmstrongA, Toga AW, Edgerton VR. Physiological and developmentalimplicationsofmotorunitanatomy.J Neurobiol1991;22:547-559.
164.Petit J, Filippi GM, Emonet-Denand F, Hunt CC, Laporte Y.Changes in muscle stiffness produced by motor units of dif-ferenttypes inperoneus longusmuscleofcat.J Neurophysiol1990;63:190-197.
165.Petit J, Filippi GM, Gioux M, Hunt CC, Laporte Y. Effects oftetaniccontractionofmotorunitsofsimilartypeontheinitialstiffness torampstretchof thecatperoneus longusmuscle.J Neurophysiol1990;64:1724-1732.
166.AltringhamJD,BottinelliR.Thedescendinglimbofthesarco-mere length-forcerelation insinglemuscle fibresof the frog.J Muscle Res Cell Motil1985;6:585-600.
167.StreetSF.Lateraltransmissionoftensioninfrogmyofibers:Amyofibrillar network and transverse cytoskeletal connectionsarepossibletransmitters.J Cell Physiol1983;114:346-364.
168.Denoth J, Stussi E, Csucs G, Danuser G. Single muscle fibercontraction is dictated by inter-sarcomere dynamics. J Theor Biol2002;216(1):101-122.
169.DommerholtJ,RoysonMW,Whyte-FergusonL.Neckpainanddysfunctionfollowingwhiplash.In:Whyte-FergusonL,GerwinRD,eds.Clinical Mastery of Myofascial Pain Syndrome.Balti-more,MD:Lippincott,Williams&Wilkins,2005:57-89.
170. JullGA.Deepcervicalflexormuscledysfunctioninwhiplash.J
Myofascial Trigger Points: An Evidence-Informed Review / 219
Musculoskeletal Pain2000;8(1/2):143-154.171.Kumar S, Narayan Y, Amell T. Analysis of low velocity frontal
impacts.Clin Biomech 2003;18:694-703.172.SterlingM,JullG,VicenzinoB,KenardyJ,DarnellR.Develop-
ment of motor system dysfunction following whiplash injury.Pain2003;103(1-2):65-73.
173.SterlingM,JullG,VicenzinoB,KenardyJ,DarnellR.Physicaland psychological factors predict outcome following whiplashinjury.Pain2005;114(1-2):141-148.
174.SchullerE,EisenmengerW,BeierG.Whiplashinjuryinlowspeedcaraccidents.J Musculoskeletal Pain2000;8(1/2):55-67.
175.Simons DG. Triggerpunkte und Myogelose [German; Triggerpointsandmyogeloses].Manuelle Medizin1997;35:290-294.
176.GerwinRD,DommerholtJ.Myofascialtriggerpointsinchroniccervicalwhiplashsyndrome.J Musculoskeletal Pain1998;6(Suppl.2):28.
177.Fernández-de-las-Peñas C, Fernández-Carnero J, Palomeque-del-Cerro L, Miangolarra-Page JC. Manipulative treatment vs.conventional physiotherapy treatment in whiplash injury: Arandomizedcontrolledtrial.J Whiplash Rel Disord2004;3(2):73-90.
178.Fernández-de-las-PeñasC,Palomeque-del-CerroL,Fernández-CarneroJ.Manualtreatmentofpost-whiplashinjury.J Bodywork Mov Ther2005;9:109-119.
179.Simons DG, Travell J, Myofascial trigger points: A possibleexplanation.Pain1981;10:106-109.
180.SterlingM,JullG,VicenzinoB,KenardyJ.Sensoryhypersen-sitivityoccurssoonafterwhiplashinjuryandisassociatedwithpoorrecovery.Pain2003;104:509-517.
181.ScottD,JullG,SterlingM.Widespreadsensoryhypersensitiv-ityisafeatureofchronicwhiplash-associateddisorderbutnotchronicidiopathicneckpain.Clin J Pain2005;21:175-181.
182.VecchietL,VecchietJ,BellomoR,GiamberardinoMA.Musclepainfromphysicalexercise.J Musculoskeletal Pain1999;7(1/2):43-53.
183.SimonsDG.ReviewofenigmaticMTrPsasacommoncauseofenigmaticmusculoskeletalpainanddysfunction.J Electromyogr Kinesiol2004;14:95-107.
184.Gerwin RD, Dommerholt J, Shah J. An expansion of Simons’integrated hypothesis of trigger point formation. Curr Pain Headache Rep2004;8:468-475.
185.Newham DJ, Jones DA, Clarkson PM. Repeated high-force ec-centric exercise: Effects on muscle pain and damage. J Appl Physiol1987;63:1381-1386.
186.FridénJ,LieberRL.Segmentalmusclefiberlesionsafterrepeti-tiveeccentriccontractions.Cell Tissue Res1998;293:165-171.
187.Stauber WT, Clarkson PM, Fritz VK, Evans WJ. Extracellularmatrixdisruptionandpainaftereccentricmuscleaction.J Appl Physiol1990;69:868-874.
188.Graven-NielsenT,Arendt-NielsenL.Inductionandassessmentofmusclepain,referredpain,andmuscularhyperalgesia.Curr Pain Headache Rep2003;7:443-451.
189.Lieber RL, Shah S, Fridén J. Cytoskeletal disruption after ec-centriccontraction-inducedmuscleinjury.Clin Orthop2002;403:S90-S99.
190.LieberRL,ThornellLE,FridénJ.Musclecytoskeletaldisruptionoccurswithinthe first15minofcycliceccentriccontraction.J Appl Physiol1996;80:278-284.
191.Barash IA, Peters D, Fridén J, Lutz GJ, Lieber RL. Desmincytoskeletal modifications after a bout of eccentric exerciseintherat.Am J Physiol Regul Integr Comp Physiol2002;283:
R958-R963.192.ThompsonJL,BalogEM,FittsRH,RileyDA.Fivemyofibrillar
lesiontypesineccentricallychallenged,unloadedratadductorlongusmuscle:Atestmodel.Anat Rec1999;254:39-52.
193.LieberRL,FridénJ.Mechanismsofmuscleinjurygleanedfromanimalmodels.Am J Phys Med Rehabil2002;81(11Suppl):S70-S79.
194.Peters D, Barash IA, Burdi M, Yuan PS, Mathew L, Fridén J,LieberRL.Asynchronousfunctional,cellularandtranscriptionalchangesafteraboutofeccentricexercise intherat.J Physiol2003;553(Pt3):947-957.
195.BowersEJ,MorganDL,ProskeU.Damagetothehumanquad-riceps muscle from eccentric exercise and the training effect.J Sports Sci2004;22(11-12):1005-1014.
196.ByrneC,TwistC,EstonR.Neuromuscularfunctionafterexercise-inducedmuscledamage:Theoreticalandappliedimplications.Sports Med2004;34(1):49-69.
197.HamlinMJ,QuigleyBM.Quadriceps concentric and eccentricexercise. 2: Differences in muscle strength, fatigue and EMGactivity in eccentrically-exercised sore and non-sore muscles.J Sci Med Sport2001;4(1):104-115.
198.PearceAJ,SaccoP,ByrnesML,ThickbroomGW,MastagliaFL.Theeffectsofeccentricexerciseonneuromuscularfunctionofthebicepsbrachii.J Sci Med Sport1998;1(4):236-244.
199.ShahJP,PhillipsTM,DanoffJV,GerberLH.An in-vivo micro-analyticaltechniqueformeasuringthelocalbiochemicalmilieuofhumanskeletalmuscle.J Appl Physiol2005;99:1980-1987.
200. ItohK,OkadaK,KawakitaK.Aproposedexperimentalmodelofmyofascialtriggerpointsinhumanmuscleaftersloweccentricexercise.Acupunct Med2004;22(1):2-12;discussion12-13.
201.Brückle W, Sückfull M, Fleckenstein W, Weiss C, Müller W.Gewebe-pO2-Messung in der verspannten Rückenmuskulatur(m. erector spinae) [German; Tissue pO2 in hypertonic backmuscles].Z. Rheumatol1990;49:208-216.
202.McCleskeyEW,GoldMS.Ionchannelsofnociception.Annu Rev Physiol1999;61:835-856.
203.SlukaKA,KalraA,MooreSA.Unilateralintramuscularinjectionsof acidic saline produce a bilateral, long-lasting hyperalgesia.Muscle Nerve2001;24:37-46.
204.SlukaKA,PriceMP,BreeseNM,StuckyCL,WemmieJA,WelshMJ.Chronichyperalgesiainducedbyrepeatedacidinjectionsinmuscle isabolishedbythe lossofASIC3,butnotASIC1.Pain2003;106:229-239.
205.Weeks VD. Travell J. How to give painless injections. In:AMA Scientific Exhibits.NewYork,NY:Grune&Stratton,1957:318-322.
206.HubbardDR,BerkoffGM.Myofascialtriggerpointsshowspon-taneousneedleEMGactivity.Spine1993;18:1803-1807.
207.CouppéC,MidttunA,HildenJ,JørgensenU,OxholmP,Fuglsang-FrederiksenA.Spontaneousneedleelectromyographicactivityinmyofascialtriggerpointsintheinfraspinatusmuscle:Ablindedassessment.J Musculoskeletal Pain2001;9(3):7-17.
208.Simons DG. Do endplate noise and spikes arise from normalmotorendplates?Am J Phys Med Rehabil2001;80:134-140.
209.Simons DG, Hong C-Z, Simons LS. Endplate potentials arecommontomidfibermyofascialtriggerpoints.Am J Phys Med Rehabil2002;81:212-222.
210.MacgregorJ,GrafvonSchweinitzD.Needleelectromyographicactivityofmyofascialtriggerpointsandcontrolsitesinequinecleidobrachialismuscle:Anobservationalstudy.Acupunct Med2006;24(2):61-70.
220 / The Journal of Manual & Manipulative Therapy, 2006
211.MenseS.Neurobiologicalbasis fortheuseofbotulinumtoxininpaintherapy.J Neurol2004;251(Suppl.1):I1-7.
212.DePaivaA,MeunierFA,MolgoJ,AokiKR,DollyJO.Functionalrepair of motor endplates after botulinum neurotoxin type Apoisoning: Biphasic switch of synaptic activity between nervesprouts and their parent terminals. Proc Natl Acad Sci USA1999;96:3200-3205.
213.ChenBM,GrinnellAD.Kinetics,Ca2+dependence,andbiophysi-cal properties of integrin-mediated mechanical modulation oftransmitterreleasefromfrogmotornerveterminals.J Neurosci1997;17:904-916.
214.Grinnell AD, Chen BM, Kashani A, Lin J, Suzuki K, KidokoroY.Theroleofintegrinsinthemodulationofneurotransmitterreleasefrommotornerveterminalsbystretchandhypertonicity.J Neurocytol2003;32(5-8):489-503.
215.KashaniAH,ChenBM,GrinnellAD.Hypertonicenhancementof transmitter release from frog motor nerve terminals: Ca2+independence and role of integrins. J Physiol 2001;530(Pt2):243-252.
216.Wang K, Yu L. Emerging concepts of muscle contraction andclinicalimplicationsformyofascialpainsyndrome(abstract).In:Focus on Pain.Mesa,AZ:JanetG.Travell,MDSeminarSeries,2000.
217.Bukharaeva EA, Salakhutdinov RI, Vyskocil F, Nikolsky EE.Spontaneous quantal and non-quantal release of acetylcho-line at mouse endplate during onset of hypoxia. Physiol Res2005;54:251-255.
218.Hoheisel U, Mense S, Simons D, Yu X-M. Appearance of newreceptive fields in rat dorsal horn neurons following noxiousstimulationof skeletalmuscle:Amodel for referralofmusclepain?Neurosci Lett1993;153:9-12.
219.Simons DG, Stolov WC. Microscopic features and transientcontractionofpalpablebandsincaninemuscle.Am J Phys Med1976;55:65-88.
220.ReitingerA,RadnerH,TilscherH,HannaM,WindischA,FeiglW.MorphologischeUntersuchunganTriggerpunkten[German;Morphologicalinvestigationoftriggerpoints].Manuelle Medizin1996;34:256-262.
221.WindischA,ReitingerA,TraxlerH,RadnerH,NeumayerC,FeiglW,FirbasW.Morphologyandhistochemistryofmyogelosis.Clin Anat1999;12:266-271.
222.Mense S, Simons DG, Hoheisel U, Quenzer B. Lesions of ratskeletalmuscleafterlocalblockofacetylcholinesteraseandneu-romuscularstimulation.J Appl Physiol2003;94:2494-2501.
223.Pongratz D. Neuere Ergebnisse zur Pathogenese Myofaszi-aler Schmerzsyndrom [German; New findings with regard tothe etiology of myofascial pain syndrome]. Nervenheilkunde2002;21(1):35-37.
224.Pongratz DE, Späth M. Morphologic aspects of muscle painsyndromes. In: Fischer AA, ed. Myofascial Pain: Update in Diagnosis and Treatment. Philadelphia, PA: W.B. SaundersCompany,1997:55-68.
225.GariphianovaMB.Theultrastructureofmyogenictriggerpointsin patients with contracture of mimetic muscles (abstract). J Musculoskeletal Pain1995;3(Suppl1):23.
226.GlogowskyC,WallraffJ.EinBeitragzurKlinikundHistologiederMuskelhärten(Myogelosen)[German;Acontributiononclinicalaspects and histology of myogeloses]. Z Orthop 1951;80:237-268.
227.Fassbender HG. Morphologie und Pathogenese des Weich-teilrheumatismus [German; Morphology and etiology of soft
tissuerheumatism].Z Rheumaforsch1973;32:355-374.228.HubbardDR.Chronicandrecurrentmusclepain:Pathophysi-
ology and treatment, and review of pharmacologic studies. J Musculoskeletal Pain1996;4:123-143.
229.LewisC,GevirtzR,HubbardD,BerkoffG.NeedletriggerpointandsurfacefrontalEMGmeasurementsofpsychophysiologicalresponses in tension-type headache patients. Biofeedback & Self-Regulation1994;3:274-275.
230.McNulty WH, Gevirtz RN, Hubbard DR, Berkoff GM. Needleelectromyographic evaluation of trigger point response to apsychologicalstressor.Psychophysiology1994;31:313-316.
231.BanksSL,JacobsDW,GevirtzR,HubbardDR.Effectsofauto-genicrelaxationtrainingonelectromyographicactivityinactivemyofascialtriggerpoints.J Musculoskeletal Pain1998;6(4):23-32.
232.ChenJT,ChenSM,KuanTS,ChungKC,HongC-Z.Phentolamineeffecton the spontaneouselectrical activityof active loci inamyofascialtriggerspotofrabbitskeletalmuscle.Arch Phys Med Rehabil1998;79:790-794.
233.ChenSM,ChenJT,KuanTS,HongC-Z.Effectofneuromuscularblocking agent on the spontaneous activity of active loci in amyofascialtriggerspotofrabbitskeletalmuscle.J Musculosk-eletal Pain1998;6(Suppl.2):25.
234.Bowman WC, Marshall IG, Gibb AJ, Harborne AJ. Feedbackcontrol of transmitter release at theneuromuscular junction.Trends Pharmacol Sci1988;9(1):16-20.
235.CunhaFQ,LorenzettiBB,PooleS,FerreiraSH.Interleukin-8asamediatorofsympatheticpain.Br J Pharmacol1991;104:765-767.
236.VerriWA, Jr.,CunhaTM,ParadaCA,PooleS,CunhaFQ,Fer-reiraSH.Hypernociceptive roleof cytokinesandchemokines:Targetsforanalgesicdrugdevelopment?Pharmacol Ther2006(Inpress).
237.Poole S, de Queiroz Cunha F, Ferreira SH. Hyperalgesia fromsubcutaneouscytokines.In:WatkinsLR,MaierSF,eds.Cytokines and Pain.Basel,Switzerland:Birkhaueser,1999:59-87.
238.Fernandez HL, Hodges-Savola CA. Physiological regulation ofG4AChE in fast-twitchmuscle:Effectsof exerciseandCGRP.J Appl Physiol1996;80:357-362.
239.Hodges-Savola CA, Fernandez HL. A role for calcitonin gene-related peptide in the regulation of rat skeletal muscle G4acetylcholinesterase.Neurosci Lett1995;190(2):117-20.
240.Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML,GerwinRD,ParejaJA.Triggerpointsinthesuboccipitalmusclesandforwardheadpostureintension-typeheadache.Headache2006;46:454-460.
241.GerwinRD.Factoresquepromuevenlapersistenciademialgiaenelsíndromededolormiofascialyenlafibromyalgia[Span-ish; Factors that promote the continued existence of myalgiain myofascial pain syndrome and fibromyalgia]. Fisioterapia 2005;27(2):76-86.
242.GerwinRD.Areviewofmyofascialpainandfibromyalgia:Factorsthatpromotetheirpersistence.Acupunct Med2005;23(3):121-134.
243.Andres E, Loukili NH, Noel E, Kaltenbach G, Abdelgheni MB,PerrinAE,Noblet-DickM,MaloiselF,SchliengerJL,BlickleJF.Vitamin B12 (cobalamin) deficiency in elderly patients. CMAJ2004;171:251-259.
244.Pruthi RK, Tefferi A. Pernicious anemia revisited. Mayo Clin Proc1994;69:144-150.
245.PlotnikoffGA,QuigleyJM.Prevalenceofseverehypovitaminosis

Myofascial Trigger Points: An Evidence-Informed Review / 221
Dinpatientswithpersistent,nonspecificmusculoskeletalpain.Mayo Clin Proc2003;78:1463-1470.
246.BogdukN,SimonsDG.Neckpain:Jointpainortriggerpoints.In: Værøy H, Merskey H, eds. Progress in Fibromyalgia and Myofascial Pain.Amsterdam,TheNetherlands:Elsevier,1993:267-273.
247.Padamsee M, Mehta N, White GE. Trigger point injection: AneglectedmodalityinthetreatmentofTMJdysfunction.J Pedod1987;12(1):72-92.
248.Linton SJ. A review of psychological risk factors in back andneckpain.Spine2000;25:1148-1156.
249.VlaeyenJW,LintonSJ.Fear-avoidanceanditsconsequencesinchronicmusculoskeletalpain:Astateoftheart.Pain2000;85:317-332.
250.MenefeeLA,CohenMJ,AndersonWR,DoghramjiK,FrankED,Lee H. Sleep disturbance and nonmalignant chronic pain: Acomprehensive reviewof the literature.Pain Med 2000;1:156-172.
251.Bauermeister W. Diagnose und Therapie des MyofaszialenTriggerpunkt Syndroms durch Lokalisierung und StimulationsensibilisierterNozizeptorenmitfokussiertenelektrohydraulischeStosswellen[German;Diagnosisandtherapyofmyofascialtriggerpoint symptoms by localization and stimulation of sensitizednociceptorswithfocusedultrasoundshockwaves].Medizinisch-Orthopädische Technik2005;5:65-74.
252.Müller-EhrenbergH,LichtG.Diagnosisandtherapyofmyofascialpainsyndromewithfocusedshockwaves(ESWT).Medizinisch-Orthopädische Technik2005;5:1-6.