narrative review cognitive interventions to reduce ... · pdf filecognitive interventions to...
TRANSCRIPT

Cognitive interventions to reducediagnostic error: a narrative review
Mark L Graber,1,2,3 Stephanie Kissam,3 Velma L Payne,4,5 Ashley N D Meyer,6,7
Asta Sorensen,3 Nancy Lenfestey,3 Elizabeth Tant,3 Kerm Henriksen,8
Kenneth LaBresh,3 Hardeep Singh6,7
ABSTRACTBackground: Errors in clinical reasoning occur in most
cases in which the diagnosis is missed, delayed or
wrong. The goal of this review was to identify
interventions that might reduce the likelihood of these
cognitive errors.
Design: We searched PubMed and other medical and
non-medical databases and identified additional
literature through references from the initial data set
and suggestions from subject matter experts. Articles
were included if they either suggested a possible
intervention or formally evaluated an intervention and
excluded if they focused solely on improving
diagnostic tests or provider satisfaction.
Results: We identified 141 articles for full review, 42
reporting tested interventions to reduce the likelihood
of cognitive errors, 100 containing suggestions, and
one article with both suggested and tested
interventions. Articles were classified into three
categories: (1) Interventions to improve knowledge
and experience, such as simulation-based training,
improved feedback and education focused on a single
disease; (2) Interventions to improve clinical reasoning
and decision-making skills, such as reflective practice
and active metacognitive review; and (3) Interventions
that provide cognitive ‘help’ that included use of
electronic records and integrated decision support,
informaticians and facilitating access to information,
second opinions and specialists.
Conclusions: We identified a wide range of possible
approaches to reduce cognitive errors in diagnosis.
Not all the suggestions have been tested, and of those
that have, the evaluations typically involved trainees in
artificial settings, making it difficult to extrapolate the
results to actual practice. Future progress in this area
will require methodological refinements in outcome
evaluation and rigorously evaluating interventions
already suggested, many of which are well
conceptualised and widely endorsed.
INTRODUCTION
Although the rate of diagnostic error inpractice is unknown, experts estimate it to bein the range of 10%e15%.1 Diagnostic errors
are of great concern in all specialties andthose characterised by high levels of stress,workload and distractions are particularlyvulnerable. Errors are more likely when thelevel of uncertainty is high, if clinicians areunfamiliar with the patient, and when thereare atypical or non-specific presentations ofa common disease or ‘distracting’ comorbidconditions.2
Diagnostic errors reflect the complexinterplay of system-related and cognitivefactors, typically with multiple root causesidentifiable in a single case.3e6 Cognitiveerrors can be found in the majority ofcases.4 7 Given the dominant role thatcognitive shortcomings play in contributingto diagnostic error, it is appropriate to beginconsidering what could be done to helpminimise the likelihood of these errors. Wetherefore conducted an analytic review of theliterature to identify interventions to reducethe likelihood of cognitive errors or error-related harm in healthcare. Interventionsrelating to system-related factors werediscussed in a companion publication.8
METHODS
Our search strategy has been previouslydescribed.8 Briefly, we sought articles, booksand conference presentations relating to theprevention, reduction or mitigation of diag-nostic errors in PubMed and several othermedical and non-medical databases. Wepursued references from these sources andasked authorities in the field of appliedcognition and decision-making to recom-mend additional readings. Articles and bookswere included in this analysis if theycontained results from an intervention trialor suggested an intervention to reducecognitive-related diagnostic error. Publica-tions that focused on development or
< Additional appendices arepublished online only. Toview these files please visitthe journal online (http://qualitysafety.bmj.com/content/21/7.toc).
For numbered affiliations seeend of article.
Correspondence toDr Mark L Graber, RTIInternational, c\o 1 BreezyHollow, St James, NY 11780,USA; [email protected]
The authors of this paper aresolely responsible for itscontent, and disclosed nocompeting interests. Thefindings and interpretationsin the paper do not representthe opinions orrecommendations of theinstitutions with which theauthors are affiliated, theAgency for HealthcareResearch and Quality, or theUS Department of Health andHuman Services, Departmentof Veterans Affairs.
Accepted 20 February 2012Published Online First27 April 2012
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 535
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

refinement of specific diagnostic tests or technologies,or solely on the aetiology or epidemiology of error, ordealt primarily with provider satisfaction or preferenceswere excluded.A full-text review using an approach described by
Gordon and Findley9 was performed on the 42 empiricalstudies that tested an intervention. Nineteen quality-based criteria were independently extracted from eacharticle using a data extraction form (online appendix A).Items answered with ‘yes’ or ‘no’ included literaturereview described, clear objectives reported, study designreported, appropriate design to address objectives,control group used, subjects randomised, blinding used,intervention clearly described, resources described,outcomes match objectives, statistical tests used, statis-tical tests appropriate, data collection replicable, studyreplication possible and limitations discussed. Addi-tional items assessed were the study design, subjectcharacteristics and number of subjects. Based on theseitems, we assigned an ‘Outcomes Rating’ and ‘Strengthof Conclusions’ rating to each article (detailed instru-ments in online appendix B). The Outcomes Rating wasbased on Kirkpatrick’s hierarchy9 10 that we slightlymodified for use in assessing diagnostic errors. Thishierarchy demonstrates the level of impact of eachintervention on diagnostic errors (eg, Level 2b refers toan intervention in which an acquisition of conceptsmight impact diagnostic error, whereas Level 4b refers toan intervention that directly reduces diagnostic error).The Strength of Conclusions of each study was rated ona numerical scale (1e5) in accordance with BestEvidence in Medical Education guidelines.9 11 Thisrating is not an assessment of the overall methodologicalquality, but is a measure of how well the conclusionsmade are supported by the data presented.Two reviewers with expertise in cognitive psychology
(ANDM and VLP) assessed each of the interventionstudies independently. We assessed agreement betweenthe reviewers for the Outcomes Rating and the Strengthof Conclusions with Cohen’s k statistic. Differences wereresolved by discussion between the two reviewers and incases of disagreement, another investigator (SK)reviewed and rated the article. In these cases, we usedconsensus among these three reviewers to determine thefinal ratings.Based on a prior classification scheme,1 all articles
were assigned to one of three natural categories: (1)Interventions that increase medical knowledge andexperience; (2) Interventions that improve clinicalreasoning; and (3) Interventions that involve gettinghelp. Articles were further subdivided into more specifictypes of interventions (such as ‘focused training onspecific content areas’, ‘develop simulation exercise toexpose clinicians to a greater number and variety of
cases presentations’, etc.) to facilitate the synthesis of thefindings (tables 1e4).
RESULTS
We identified 141 sources (articles, books and confer-ence papers) for full review. Of these, 42 sources (tables1e4) reported empirical studies of an intervention toreduce cognitive-based diagnostic error (and sometimesalso additional suggestions for interventions), 100sources contained only suggestions (table 5) and onehad both. Some sources reported more than onesuggestion.During the full-text review of the empirical studies
assessing cognitive interventions, agreement betweenreviewers on the Outcomes Rating was substantial(k¼0.70). Similar agreement was obtained for theStrength of Conclusions (k¼0.70). There were threearticles with disagreements that were resolved bydiscussions with a third reviewer. We categorised theintervention studies into one of three mutually exclusivecategories: (1) Interventions to increase clinicians’knowledge and experience, (2) Interventions to improveclinical reasoning and decision-making skills or (3) ‘Gethelp’, interventions that assist clinicians with tools oraccess to other clinicians or experts. For each of thesesections, we use the suggested intervention and back-ground literature to first provide context, followingwhich we discuss the tested interventions. The OutcomesRatings and Strength of Conclusions ratings for eachintervention article are included in tables 1e4.
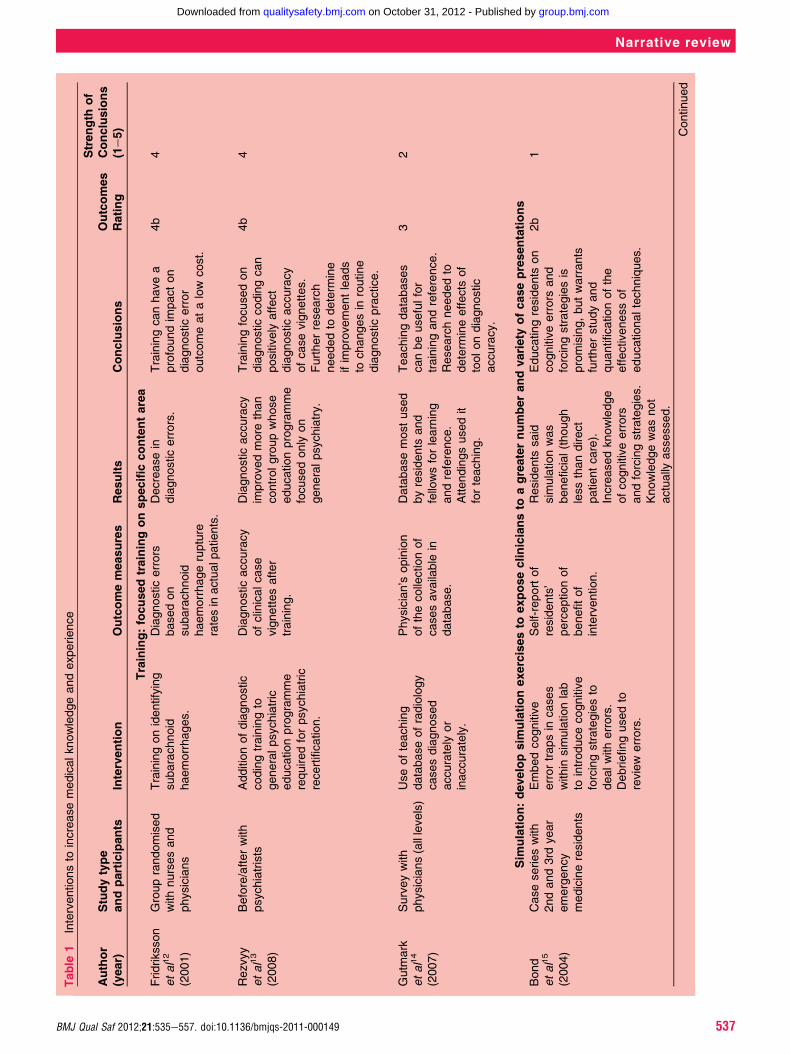
1) Increase knowledge and experienceDiagnostic error could potentially be reduced byincreasing physician’s structured knowledge and expe-rience, the essential basis of expertise.143 By definition,experts will tend to make the fewest errors, have thebest degrees of calibration and excel in efficientdiagnosis.50 144 145 Medical educators similarly agree withthe concept of increasing experience as the key todeveloping expertise.143 146 147 The interventions in thisdomain are summarised in table 1 and are organisedinto the following three categories.
Training focused on specific content areas
An effect of training on diagnostic reliability is illustratedin radiology, where certain certification programmes arebased on demonstrating competency. For instance,radiologists in the UK must review 5000 mammogramsa year for certification, as opposed to 480 in the USA,which may in part account for the large difference indiagnostic accuracy noted between the two countries.54
In certain programmes, radiologists also receive
536 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from
Table
1Interventionsto
increasemedicalknowledgeandexperience
Author
(year)
Studytype
andparticipants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
Conclusions
(1e5)
Training:focusedtrainingonspecificcontentarea
Fridriksson
etal12
(2001)
Grouprandomised
withnursesand
physicians
Trainingonidentifying
subarachnoid
haemorrhages.
Diagnosticerrors
basedon
subarachnoid
haemorrhagerupture
ratesin
actualp
atients.
Decreasein
diagnosticerrors.
Trainingcanhavea
profoundim
pacton
diagnosticerror
outcomeatalow
cost.
4b
4
Rezvyy
etal13
(2008)
Before/afterwith
psychiatrists
Additionofdiagnostic
codingtrainingto
generalpsychiatric
educationprogramme
requiredforpsychiatric
recertification.
Diagnosticaccuracy
ofclinicalcase
vignettesafter
training.
Diagnosticaccuracy
improvedmore
than
controlgroupwhose
educationprogramme
focusedonly
on
generalpsychiatry.
Trainingfocusedon
diagnosticcodingcan
positively
affect
diagnosticaccuracy
ofcasevignettes.
Furtherresearch
neededto
determ
ine
ifim
provementleads
tochangesin
routine
diagnosticpractice.
4b
4
Gutm
ark
etal14
(2007)
Surveywith
physicians(alllevels)
Useofteaching
databaseofradiology
casesdiagnosed
accurately
or
inaccurately.
Physician’s
opinion
ofthecollectionof
casesavailable
indatabase.
Databasemostused
byresidents
and
fellowsforlearning
andreference.
Attendingsusedit
forteaching.
Teachingdatabases
canbeusefulfor
trainingandreference.
Researchneededto
determ
ineeffects
of
toolondiagnostic
accuracy.
32
Sim
ulation:developsim
ulationexercisesto
exposecliniciansto
agreaternumberandvariety
ofcasepresentations
Bond
etal15
(2004)
Caseserieswith
2ndand3rd
year
emergency
medicineresidents
Embedcognitive
errortrapsin
cases
within
sim
ulationlab
tointroducecognitive
forcingstrategiesto
dealwitherrors.
Debriefingusedto
review
errors.
Self-reportof
residents’
perceptionof
benefitof
intervention.
Residents
said
sim
ulationwas
beneficial(though
lessthandirect
patientcare).
Increasedknowledge
ofcognitiveerrors
andforcingstrategies.
Knowledgewasnot
actually
assessed.
Educatingresidents
on
cognitiveerrors
and
forcingstrategiesis
promising,butwarrants
furtherstudyand
quantificationofthe
effectivenessof
educationaltechniques.
2b
1
Continued
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 537
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
1Continued
Author
(year)
Studytype
andparticipants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
Conclusions
(1e5)
Carlson
etal16
(2011)
Before/afterwith
4th
yearmedical
students
Useofdiagnostic
remindersystem
(ISABEL)to
reduce
diagnosticerrorwhile
cliniciansassessed
livepeople
trainedas
patients
oramanikin
inasim
ulationlab.
Changein
diagnostic
accuracyafter
intervention.View
of
diagnosticreminder
system
asan
educationtooland
resourceforpractice.
Diagnosticaccuracy
improved.Toolwas
viewedasbeneficial
asatrainingtooland
asusefulin
practice.
Diagnosticreminder
systemscanpotentially
reducecognitive-based
diagnosticerrors.The
optimaltimewithin
trainingto
introducethe
useofsuchtools
remainsunclear.Itis
unclearwhether
diagnosticaccuracyis
increasingsim
ply
becauseofadditional
timespenton
diagnosingproblem.
2b
2
Feedbackandcalibration:provideintensive,detailed,specificfeedback
Tudorand
Finlay17
(2001)
Before/afterwith
expertradiologists
Review
feedback
regardingdiagnostic
errors
made
diagnosingradiographs.
Diagnosticaccuracy
rate
4e5monthsafter
reviewingfeedback.
Diagnosticerrorrate
insamecases
decreasednominally
(nostatisticsreported).
Allowingradiologists
toreview
theirerrors
may
decreasediagnostic
errorrate.More
researchneededto
determ
ineifeffects
generaliseto
new
cases/domain.
32
Woodand
Tracey18
(2009)
Grouprandomised
controltrialwith
doctoralstudents
Receivingcontent-based
or
principle-based
feedbackto
reduce
diagnosticerrorof
overshadowing.
Reductionof
overshadowing
acrossfeedback
conditions.
Sim
ilardecreasein
overshadowingfor
both
feedback
interventions.Less
reductionin
control
group.Generalisation
effectforcontent-
basedfeedback.
Givingclinicians
feedbackregarding
specificattributesofa
caseorcognitive
diagnosticreasoning
strategiesmayreduce
diagnosticerror
involving
overshadowing.
4b
4
OutcomesRatin
gsreflectthelevelo
fim
pactforeachinterventio
nonreducingdiagnostic
errors.9
10Strength
ofConclusionswasratedonanumericalscale
(1e5)in
accordancewithBestEvidence
inMedicalEducatio
nguidelines(5¼s
trongest).9
11
538 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
2Interventionsto
improveintuitive(system
1)anddeliberate
(system
2)processesin
decision-m
aking
Author(Year)
Studytype
andparticipants
Intervention
Outcome
measures
Results
Conclusions
Outcomes
Rating
Strength
of
Conclusions
(1e5)
Improvesystem
1processing:im
provetrainingonintuitiveprocessinganditsshortcomings
Sherbinoetal19
(2011)
Caseserieswith
4th
yearresidents
Teachingcognitive
forcingstrategiesto
introducediagnostic
errorrisk,identifyand
counterm
andbiases.
Diagnosticaccuracy
invariousdomains
aftervaryingdelays.
Aftertrainingabout
halfthesubjects
stillcommittedbias.
Perform
ance
sufferedeven
furtherafteradelay.
Teachingcognitive
forcingstrategies
mayreducediagnostic
errors
inatransferable
way(thoughitis
difficultto
tellwithout
perform
ance
measurespriorto
training).Also,the
effects
were
short-lived.
32
Evaetal20
(2007)
Randomisedcontrol
trialw
ithundergraduate
psychologystudents
Usecombined
approachto
reasoning
includingpattern
recognitionand
carefulconsideration
ofpresentingfeatures
whendiagnosing
ECGswithbiasing
inform
ation.
Diagnosticaccuracy
ofECG
readings.
Diagnosticaccuracy
improvedforsubjects
usingcombined
reasoningapproach
evenin
presenceof
biasinginform
ation.
Traineescanbenefit
from
explicitguidance
ofacombined
approachto
clinical
reasoning,
suggestingavalue
toboth
analyticand
non-analytical
reasoningtendencies.
4b
4
Improvesystem
1processing:im
provemetacognition,intuitionandreflectivepractice
Mamedeetal21
(2010)
Before/afterwith
1stand2ndyear
residents
Incorporationof
reflectivereasoning
toreducediagnostic
errors.
Diagnosticerrors
producedbefore
andafterreflective
reasoning.
Significantnumber
ordiagnoseswere
correctedafter
reflectivereasoning,
presumably
reducingbias.
Diagnosticaccuracy
maybeim
proved
withreflective
reasoning.More
researchneededto
disentangle
reflective
reasoningfrom
additionaltime
assessingacaseto
determ
ineifreflection
generalisesto
experts.
32
Continued
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 539
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
2Continued
Author(Year)
Studytype
andparticipants
Intervention
Outcome
measures
Results
Conclusions
Outcomes
Rating
Strength
of
Conclusions
(1e5)
Coderreetal22
(2010)
Before/afterwith1st
yearmedicalstudents
Havestudents
reflect
oninitialhypothesis
establishedpriorto
reviewingallclinical
evidence.Then
presentadditional
concordantor
discordantevidence.
Diagnostic
accuracy.
Withdiscordant
data,significant
increasein
diagnostic
accuracy.No
differencein
accuracywith
concordantdata.
Overall,
no
significant
differencein
diagnosticaccuracy.
Providingstudents
withadditional
inform
ationafteran
initialdiagnosis
affects
diagnostic
accuracydifferently
dependingonthe
typeofinform
ation
received.More
researchneeded
todeterm
inevalidity
oftheintervention.
31
Improvesystem
1processing:consideralternatives,considertheopposite,useprospectivehindsight,thinklikeanoutsider
Wolpaw
etal23
(2009)
Randomisedcontrol
trialwith3rd
year
medicalstudents
Incorporationof
SNAPPStechnique
duringcase
presentationto
facilitate
learning.
Diagnostic
reasoningmeasures
includingnumberof
minutesto
present
findings,was
summary
concise
andthorough,etc.
SNAPPSgroup
showedmore
diagnostic
reasoningthan
afeedback
comparisonand
acontrolgroup.
UsingtheSNAPPS
techniquemayresult
incorrectionof
flawedreasoning,
reductionof
diagnosticand
therapeuticerrors.
Studyonly
measured
amountofreasoning
andnotaccuracy
thereof,soitis
unclearhow
this
interventionwould
improvediagnostic
accuracy.
2b
3
OutcomesRatingsreflectthelevelo
fim
pactforeachinterventiononreducingdiagnosticerrors.9
10Strength
ofConclusionswasratedonanumericalscale
(1e5)in
accordancewithBestEvidence
inMedicalEduca
tionguidelines(5¼s
trongest).9
11SNAPPS:Summarizehistory
andfindings,Narrow
thedifferential,Analyze
thedifferential,Probepreceptoraboutuncertainties,Plan
management,Selectcase-relatedissuesforself-study.
540 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
3Interventions:help
from
otherpeople
Author(year)
Studytypeand
participants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
conclusions
(1e5)
Secondopinionsin
pathology
Raabetal24
(2008)
Before/afterwith
expertcytologists
Useofsecond
readingspre
sign-out
atthreeinstutions,
comparingrandom
reviewsto
organ-
targetedreviews.
Proportionof
diagnosticerrors
detected.
Few
diagnosticerrors
detected;no
significantdifferences
amongsites;Tissue-
specificreviews
yieldedhighererror
ratesthanrandom
reviews.
Tissue-specific
reviewsyieldedhigher
errorratesthanrandom
reviews.
2b
2
Raabetal25
(2006)
Before/afterwith
expertpathologists
Secondreadingof
pathologycases.
Random
review
of5%
ofcasesandfocused
review
ofallcases.
Percentofdiagnostic
errors.Im
pactof
differenceonpatient
care.
Focusedreview
detected
approxim
ately
four
timesmore
diagnostic
errors
than5%
random
review.The
majority
oferrors
inboth
groupsdid
not
leadto
patientharm
or
resultedin
low-grade
harm
.
Secondopinionreviews
canbeamethodto
standardisediagnostic
practice.
4a
3
Manionetal26
(2008)
Before/afterwith
expertpathologists
Secondreadingof
pathologyslides
receivedfrom
an
externalorganisation.
Rate
ofdiagnostic
variationandchange
inpatient
managementdueto
secondreading.
Nodisagreementin
majority;minor
disagreementin
small
%;major
disagreementin
very
small%
ofcases.
Changein
managementplanin
halfofcaseswith
majordisagreement.
Mandatory
second
opinionofsurgical
pathologymaybe
abeneficialpatient
care
practice.However,
upondisagreement,
itis
notclearhow
often
thesecondopinion
wascorrectdueto
inconclusivechart
reviews.
4a
2
Nordrum
etal27
(2004)
Before/afterwith
expertpathologists
Useofstillim
agesin
secondopinionof
pathologycases.
Diagnosticaccuracy
rate
(glassslidesvs
stillim
ages).
Nearlythesame
diagnosticaccuracy
rate
withstillim
ages
andglassslides.
Usingstillim
agesto
diagnosecasesappears
tobecomparable
tousingglassslides,thus
increasingeaseof
obtainingsecond
opinions.
33
Continued
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 541
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
3Continued
Author(year)
Studytypeand
participants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
conclusions
(1e5)
Hamadyetal28
(2005)
Before/afterwithan
expertsurgeon,
oncologistand
pathologist
Useofsecond
opinionsof
amultidisciplinary
team
ofclinicians.
Percentageofsecond
opinionsresultingin
differentdiagnosis.
Complete
agreement
inmajority
ofcases.
Disagreementasmall
%ofthetime.
Diagnosticand
therapeutic
discrepanciescan
occurwhenmultiple
expertsreview
thesame
patientcase.Itisunclear
ifthesecondopinion
leadsto
better
outcomes.
4a
4
Secondopinionsin
radiology
Bengerand
Lyburn
29
(2003)
Before/afterwithER
andradiologystaff
Secondreadingof
radiographsbythe
radiologystaffforx-
raysprocessedby
ER.
Rate
ofdiagnostic
agreement.Clinical
impactofdiagnostic
discrepancy.
Very
smallamountof
discrepanciesthat
requiredminuscule
changein
management.
Thelow
rate
of
significantmisread
radiographssuggests
incorporationof
selectivesecond
readingsmaybe
warranted.
4a
3
Espinosa
andNolan30
(2000)
Before/afterwithER
physiciansand
radiologists
x-R
aysreadbyER
physicianand
radiologist.
Radiograph
interpretationerror
andnumberof
potentialadverse
events.
Interpretationerror
rate
andpotential
adverseeffects
decreased(basedon
reliability
modelnot
raw
data).
Proceduresfor
interpretingradiographs
designedto
mitigate
errors
canreducethe
adverseevents.Without
acontrolgroupitis
difficultto
know
ifim
provementis
from
intervention.
4a
2
Duijm
etal31
(2007)
Before/afterwith
mammography
techniciansand
radiologists
Secondreadingof
mammogramsby
technologists,along
withstandard
double
readingby
radiologists.
Breastcancer
detectionandpositive
predictivevalue(PPV)
ofreferral.
Modestincreasein
cancerdetectionand
modestdecreasein
PPV.
Addingsecondreading
bytechnologists
may
beeffectivein
detecting
more
breastcancer
cases.Readingsshould
beconsideredfor
referraldueto
high
prevalenceofbreast
cancer.
4a
4
Continued
542 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
3Continued
Author(year)
Studytypeand
participants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
conclusions
(1e5)
Kweketal32
(2003)
Before/afterwith
expertpathologists
Blindedsecond
readingsin
mammography.
Rate
ofcancer
detection,patient
recall,
rate
ofbiopsy
andmeansecond
screenercontribution.
Low
increaseof
cancerdetection.
Recallrate
increased
modestly.Biopsyrate
slightlyincreased.
Efficiencyofsecond
readerminim
al.
Secondreadingof
mammogramsis
recommendedfor
breastcancer
screeningif
resourcesare
available.
4a
4
Canonetal33
(2003)
Before/afterwith
expertradiologists
Secondreview
of
barium
enematests.
Detectionofpolyps.
Secondreadingfailed
toim
provedetection
ofpolyps.
Routinesecondreading
isnotwarrantedfor
barium
enema
examination.
4a
4
Help
from
groupsandlibrarians
Christensen
etal34(2000)
Non-randomised
controlledtrialwith
clinicalteams
Team
diagnostic
decision-m
aking
where
members
were
givensharedor
private
inform
ation
thatthegroupneeded
toshare
forcorrect
diagnoses.
Diagnosticerrorrate.
Diagnosticerrors
increasedwhenteam
members
held
private
inform
ation.
Lackofsharingdata
maybedetrim
entalto
diagnosticaccuracy.
Clinicaldecisions
relyingonprivately
held
inform
ationare
susceptible
toerrors.
2b
4
Mulvaney
etal35(2008)
Randomisedcontrol
trialw
ithclinicalteams
Useofevidence
basedinform
aticstool
thatprovidesresearch
evidenceto
inform
cliniciansofpatient
care
practices.
Impactonpatientcare
practicesandclinical
actions,articlesread,
satisfactionofsearch
results,consultations,
timeto
obtain
evidence,clinician
searches.
Toolhadsignificant
impactonusers’
reportoffuture
patient
care,satisfactionof
articlesreturnedand
amountoftimespent
receivingevidence.
Nosignificantim
pact
onotheritems.
Inform
aticstools
may
facilitate
useof
researchevidenceand
influenceclinicalactions.
However,data
regarding
effects
onpatients
are
unknownasaresultof
this
study.
34
OutcomeRatingsreflectthelevelo
fim
pactforeachinterventiononreducingdiagnosticerrors.9
10Strength
ofConclusionswasratedonanumericalscale
(1e5)in
acco
rdancewithBestEvidence
inMedicalEducatio
nguidelines(5¼s
trongest).9
11ER;EmergencyRoom.
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 543
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
4Interventions:help
from
decisionsupport
Author(year)
Studytypeand
participants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
Conclusions
(1e5)
Focuseddecisionsupport
usingdecisionsupport
tools
onaspecificcondition
Pozenetal36
(1984)
Non-randomised
controltrialwithER
physicians
Incorporationof
decisionsupporttool
thatcalculatesthe
probability
ofpatient
havingischaemic
heartdisease.
Diagnosticaccuracy,
sensitivity,
specificity,FP
diagnosis
rate,FN
diagnosis
rate,CCU
admissionrate,ER
dischargerate.
Useoftoolincreased
diagnosticaccuracy
andspecificity;
sensitivityremained
unchanged.FPsand
CCU
admissions
decreased.FNs
remainedunchanged.
Useoftoolhas
potentialto
increase
diagnosticaccuracy
andreduceadmission
rate.
4b
4
Selkeretal37
(1998)
Non-randomised
controltrialwith
attendingER
physicianand
residents
Computerised
predictiontoolthat
calculated
probability
ofacute
ischaemia
thatwas
printedonECG.
Accuracyoftriage
decisions.
Toolreduced
unnecessary
CCU
admissionsanddid
notchange
appropriate
admission
rates.
Useofthetoolhas
thepotentialto
significantlyreduce
unnecessary
hospitalisations.
4b
4
Bogusevicius
etal38(2002)
Randomisedcontrol
trialwithradiologists
Useofacomputer-
aideddiagnosis
tool
todiagnoseacute
smallbowel
obstruction.
Specificity,
sensitivity,FP
predictivevalue,FN
predictivevalue,
timeto
diagnose,
mortalityand
morbidity.
Nosignificant
advantageover
contrastradiography
fordiagnostic
accuracy.Significantly
lesstimerequiredto
diagnosis.
Computer-aided
diagnosis
improved
amountoftimeto
diagnose,butno
otherindices.
4b
3
DeSim
one
etal39(2007)
Before/afterwith
medicalpersonnel
Useofcomputer-
assisteddiagnosis
databasefor
diagnosis
and
patientmanagement
ofheadaches
comparedwith
standard
clinical
method.
Diagnosticaccuracy,
meanvisitduration,
operators’subjective
opinionoftooluser
friendliness,
patients’subjective
opinionofcomputer-
assistedinterview
acceptability.
Slightincreasein
diagnosticaccuracy.
Durationofclinical
visitcomparable.
Subjects
felttoolwas
easyto
useand
patients
feltthetool
usewasacceptable.
Thetoolim
proves
diagnosticaccuracy
withoutincreasingvisit
duration.
4a
3
Continued
544 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Table
4Continued
Author(year)
Studytypeand
participants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
Conclusions
(1e5)
Focuseddecisionsupport
usingembeddeddecisionsupport
tools
(Infobuttons)
Cim
ino40(2006)
Surveywithnurses,
attendings,
residents,medical
students
Useofonline
resourcesthrough
anInfobutton
Manager(IM)
providingdirect,
context-specific
inform
ation.
Usersatisfaction
regarding
inform
ationreturned
from
online
resources.
Satisfactionwiththe
IMvaried.Overall
users
feltIM
had
apositiveeffecton
patientcare
decisions.
Context-specific
accessto
health
knowledgeresources
canbeseenasuseful.
More
researchis
neededontheim
pact
onpatientoutcomes.
13
Generaldecisionsupport
usingweb-enableddifferentialdiagnosis
generators
Ramnarayan
etal41(2006)
Before/afterwith
paediatric
interns
andresidents
Useofaninternet
diagnosticdecision
supporttool
(ISABEL)during
diagnosis.
Changein
proportion
ofunsafe
diagnostic
investigationsand
meanqualityscore
ofdiagnosis
followingtool
consultation.
Significantproportion
ofunsafe
investigationsreduced
withtooluse.Mean
diagnosticquality
score
increased.
Useofstand-alone
diagnosticsystem
toim
provediagnostic
decision-m
akingfor
juniorphysiciansis
beneficial.However,
severalbarriers
must
beovercomein
order
forsuchtools
tobe
mosteffective.
33
Ramnarayan
etal42(2007)
Auditofsystem
Useofdiagnostic
decisionsupporttool
(ISABEL)when
diagnosingpatients
withresuscitation
issuesin
emergency
room.
Percentageoftime
accurate
diagnosis
wasin
listprovided
bytooland
proportionoftime
toolincludedmust-
not-missdiagnoses.
Toolcontainedcorrect
diagnosis
andmust-
not-missdiagnosis
innearlyevery
case.
Diagnosticaid
perform
san
acceptable
degreeof
clinicalaccuracyin
ED.Furtherresearch
isneededto
determ
inerole
oftool
inclinicalpractice.
2b
3
Ramnarayan
etal43(2003)
Auditwithclinicians
ofvaryinglevels
of
expertiseand
system
Useofinternet
diagnosticdecision
supporttool
(ISABEL)as
areminderof
possible
diagnoses
toconsider.
Proportionofcases
withexpected
diagnosis
inresults
generatedbytool.
Usinghypothetical
andrealpatient
cases,toolreturned
thecorrectdiagnosis
innearlyevery
case.
Toolshowed
acceptable
clinical
accuracybyproviding
correctdiagnosis
for
realandhypothetical
cases.Itis
anticipated
theuseoftoolis
effectivein
assisting
physiciansto
accurately
diagnosechildren.
2b
4
Continued
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 545
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from
Table
4Continued
Author(year)
Studytypeand
participants
Intervention
Outcomemeasures
Results
Conclusions
Outcomes
Rating
Strength
of
Conclusions
(1e5)
Ramnarayan
etal44(2006)
Before/afterwith
cliniciansofvarying
levels
ofexpertise
Useofadiagnostic
system
(ISABEL)to
determ
inediagnosis
afterdiagnosing
casewithoutsystem.
Rate
ofdiagnostic
errors,diagnostic
qualityscore
and
timeusingsystem.
Declinein
diagnostic
errors.Increasein
diagnosticquality
score.Nosignificant
outcomebylevelof
experience.Median
timeforsystem
use
was1min.
Studysuggests
promisingrole
for
reminder-based
diagnosticdecision
supporttoolto
reduce
diagnosticerrors.
4b
4
Graberand
Matthew45
(2008)
Before/afterwith
physiciansand
system
Useofdiagnostic
decisionsupporttool
(ISABEL)to
determ
inecorrect
diagnosis
uponentry
ofpatientkey
findingsofcomplex
medicalcases.
Percentageofcases
where
toolreturned
thesamediagnosis
aslistedin
the
NEJM.Amountof
timeusingthetool.
Whenentering
evidencemanually
toolreturnedcorrect
diagnosis
innearlyall
cases.Whenpasting
casetextaslistedin
NEJM,toolcontained
correctdiagnosis
three-fourthsofcases.
Both
entry
approacheswere
fast.
Toolperform
ed
quickly
andaccurately
insuggestingcorrect
diagnosesandshould
beevaluatedin
naturalenvironments
todeterm
ineits
potentialto
support
clinicaldiagnosis
and
reducetherate
of
diagnosticerrors.
2b
3
TangandNg46
(2006)
Auditwithphysician
andrheumatologist
SearchingGoogle.
com
todeterm
ine
correctdiagnosis
for
casepresentedin
NEJM.
Percentageof
diagnosesfrom
that
correspondedwith
NEJM
diagnosis.
searches
revealedcorrect
diagnosis
inslightly
more
thanhalfof
cases.
Astheinternet
becomesmore
available
inclinical
settings,useofweb-
basedsearchingtools
mayhelp
physicians
diagnosedifficult
cases.
2b
2
OutcomeRatingsreflectthelevelo
fim
pactforeachinterventiononreducingdiagnostic
errors.9
10Strength
ofConclusionswasratedonanumericalscale
(1e5)in
acco
rdancewithBestEvidence
inMedicalEduca
tionguidelines(5¼s
trongest).9
11CCU,Coronary-care
unit;ER,EmergencyRoom;FN,FalseNagetive;FP,FalsePositive;NEJM
,New
EnglandJournalofMedicine.
546 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

additional training in cancer detection where theyattend disease-related meetings, receive feedback oncancer detection rates and attend a 2-week course led byspecialists at high-volume mammography screeningsites.55 Similar measures, including regular peer reviewand participation in the American College of Radiol-
ogy’s RADPEER� system, have been proposed for theUSA.148
Interventions to increase the knowledge base ofpracticing clinicians through continuing medicaleducation activities have generally not led to substantialimprovement in measured performance.56 57
Table 5 Intervention suggestions
Intervention idea Suggested in article authored by
INCREASE MEDICAL KNOWLEDGE AND EXPERIENCEGeneralIncrease expertise and experience Kassirer et al47; Gigerenzer48; Elstein49; Klein50 51; Berner
and Graber1; Bazerman and Moore52; Norman53
TrainingRoutinely test competency in diagnostic accuracy;provide training to increase competency
Smith-Bindman et al54; Singh et al55
Continuing education Bowen56; Davis et al57
Focused training on specific content area Freidlander and Phillips58; Gentner59; Hershberger et al60;Parmley61
Improve learning skills, per se Hogarth62
SimulationDevelop simulation exercises to expose clinicians toa greater number and variety of case presentations
Bond et al63
Feedback and calibrationProvide intensive, detailed, specific feedback Smith-Bindman et al54; Schiff64; Jamtvedt et al65; Papa
et al66; Stone and Opel67; Alpert and Hillman68; Arkes69;Humble et al70; Pulford and Colman71; Subbotin72
Learn from errors Fischer et al73; Hogarth62; Eva74
IMPROVE INTUITIVE AND DELIBERATE PROCESSES IN DECISION-MAKINGGeneralImprove general training on clinical reasoning & the dualprocess model
Berner and Graber1; Kassirer et al47; Elstein49; Eva74 75;Croskerry76e78; Norman53; Wolpaw et al23
Improve system 1 processingImprove training on intuitive processing and itsshortcomings
Berner and Graber1; Croskerry76e78; Wedding and Faust79
Groves et al80; Pines81; Moulton et al82, Trowbridge83;Kuhn84
Debias your own intuitive decisions Croskerry 76e78; Norman53; Fischhoff85; Milkman86 Larrick87;Gentner et al59; Koriat et al88; Renner and Renner89; Estradaet al90 Scott91; Slovic and Fischoff92 Arkes et al69 154;Lichtenstein et al93
Improve metacognition, nurture intuition and use ofreflective practice
Schon94; Greenhalgh95; Mamede et al96; Singh et al97;Brawn98; Gregory99; Noddings and Shore100; Quirk101;Klein51; Hogarth62; Hamm and Zubialde102; Moulton et al82;Trowbridge83; Croskerry76e78 103
Use a checklist or related tools Leonidas104; Gawande105; Trowbridge83; Ely et al106
Consider alternatives; consider the opposite; useprospective hindsight; think like an outsider
Taleb107; Wedding and Faust79; Sackett et al158; Brannick etal108; Milkman et al86; Arkes109; Croskerry78; Schwenk110;Baron111; Mitchell et al112; Bazerman and Moore86;Mussweiler113; Lord et al114; Arzy et al115; Gorman andGorman116; Hirt and Markman117; Mumma and Steven118;Singh97
Continued
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 547
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Interventions
We identified three formal studies of training inter-ventions related to diagnostic error.12e14 One notablestudy was a highly content-specific intervention toimprove recognition of subarachnoid haemorrhage.This low-cost training programme on sudden onsetheadache for community-based physicians reducedthe baseline diagnostic error rate (12%) by 77% andimproved interactions between neurosurgeons andlocal physicians.12
Simulation
The ability to provide realistic simulations through bothscenarios and simulated patients offers the potential toimprove skills in clinical reasoning63 and the opportu-nity to expose trainees or physicians to a greater numberand variety of case presentations. Simulation is a well-established approach to improving manual, proceduralskills, but has not yet been evaluated extensively in itsability to improve cognitive skills or decision-makingrelated to diagnosis. It also remains to be demonstratedthat simulation can replace experience in actualpractice.
Interventions
We identified only two interventions in this domain,both involving trainees. Carlson et al16 demonstratedimproved diagnostic accuracy by the combined use ofsimulation with a diagnosis support tool and Bond et
al15 used simulation successfully to introduce the useof cognitive forcing strategies to emergency medicineresidents.
Feedback as a way to improve expertise, calibration and error
awareness
Deliberate practice, with immediate and focused feed-back, is viewed as an essential prerequisite to developingexpertise in any domain.144 145 Moreover, lack of feed-back is a dominant factor that sustains overconfidence,thought to be a major factor in causing diagnostic error.1
A systematic review of feedback across all medical areas(not solely diagnosis) concluded that feedback improvesperformance in selected settings, especially if the feed-back is intensive.65 Feedback is most useful if it incor-porates instruction and information on why a givenanswer was correct or not.66 67 For example, psychologytrainees improved their diagnoses if feedback provided
Table 5 Continued
Intervention idea Suggested in article authored by
Improve system 2 processingTeach principles of clinical reasoning; use evidence-based medicine and normative decision-making
Wedding and Faust79; Strauss et al119; Sox120; Dobbieet al121; Khan and Coomarasamy122; Croskerry123; Pines81;Ullman124; Pauker and Kassirer125; Kassirer126; Brannicket al108
Provide training on the typical pitfalls of specific clinicalconditions & situations
Groves et al80; Croskerry78; Pines81
GET HELP FROM OTHER PEOPLE AND/OR DECISION SUPPORT TOOLSSecond opinionsUse specialist consultants & second opinions; improveteam-based decisions, for example, by having a devil’sadvocate
Elstein49; Christensen et al34; Tatarka127
Second readings in pathology Ullman124; Raab128
Groups and librariansGet help from groups or librarians Zipperer and Sykes129; Albert130; Zipperer131
Actuarial decisionsUse of guidelines, clinical algorithms, linear models andmnemonics to reduce reliance on memory
Elstein49; Croskerry78; Berner and Graber1; Tatarka127;Milkman et al86; Wedding and Faust79; Wedding132;Fischhoff85
Focused decision supportDecision support tool on a specific condition Hunt et al133; Klassen et al134; Garg et al135; Cannon and
Allen136
Improve data display through graphics Radecki and Medow137; Reyna et al138; Bhandari et al139;Cook and Smallman140
Embedded decision support tools; Infobuttons Kawamoto and Loback141
General decision supportImprove medical records Hamm and Zubialde102; Schiff and Bates142
548 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

details on why they were right or wrong.18 149 Usingfeedback to improve diagnostic performance has beenmost convincingly demonstrated in radiology throughprogrammes such as the ‘PERFORMS’ system in theUK54 and the RADPEER programme in the USA.Although clinicians received immediate and dramatic
feedback on their diagnostic performance from autop-sies, the rate of autopsies is declining.150 Local‘Morbidity and Mortality’ conferences73 and creative newvenues such as the ‘Web M&M’ series sponsored by theAgency for Healthcare Research and Quality (http://www.webmm.ahrq.gov/) are alternative venues wherefeedback is provided.151 In this spirit, Eva74 has advo-cated for incorporating diagnostic error review intomedical school and postgraduate training. Alpert andHillman discuss other types of data that should be partof such feedback, such as the results of professionalaudits, peer reviews and risk managementprogrammes.68
Interventions
Our search yielded two studies on feedback to improvediagnostic performance.17 18 Both studies showedbenefits of feedback on later diagnostic accuracy. Thepositive impact noted by Wood and Tracey18 waspossibly explained by the provision of detailed feed-back to trainees on the reasons their initial diagnoseswere correct or not.
Category 1 summary
The empiric studies identified were positive, but gener-ally used trainees and specific content limiting the abilityto generalise the impact of results to actual practice.
2) Improve clinical reasoningAccording to the currently popular paradigm, diagnosesare made by some interacting combination of intuitive,automatic processing (system 1) and deliberate, rationalconsideration (system 2).152 Interventions to reducediagnostic error have been suggested in each of theseareas, and many authors have advocated for the benefitsof general training in clinical reasoning.1 23 47 49 53 75e78
The interventions in this domain are presented intable 2.
Improve intuitive processing: debiasing
Many, and perhaps most, medical diagnoses are derivedintuitively, acknowledging that most conditions arecommon and present in typical, easily recognised,fashion. Coderre et al153 found that intuitive diagnosesare more likely to be correct compared with diagnosesderived by hypothetico-deductive reasoning, and thisconcept is also consistent with the substantial literatureregarding expertise.
Experts in the field of naturalistic decision-makingemphasise that intuitive judgements cannot be taughtbecause they emerge subconsciously from the amassedexperience of the decision-maker and his or her abilityto access this knowledge instantaneously and effec-tively.48 50 However, others have argued that intuition can
be encouraged, strengthened and improved.51 101 151
Brawn highlighted several strategies to encourage use ofintuition such as showcasing examples of how intuitionwas used in discovery and insight situations.98 Noddingsand Shore100 suggest that intuition can be developed byfirst acknowledging intuition and its role in decision-making, demonstrating its capacity and successes, and bysharing how intuition is used, especially by experiencedrole models. Hogarth151 recommends a series of noveleducational interventions to teach and improve intui-tion, including creating increased motivation to learn byexposure to one’s own errors and constantly seeking toimprove one’s learning skills by reviewing and revisingskills in observation, sense-making and hypothesistesting.Croskerry and others have argued that clinicians
would make fewer errors if they learned the potentialshortcomings (biases) of intuitive decision-making so asto understand and avoid them.76 77 91 Interventions toavoid both affective bias (engendered by our inherentdiscomfort with certain types of patients or interactions)and cognitive bias (due to the known shortcomingsand pitfalls of subconscious thought) have beensuggested.Similar debiasing interventions were suggested by
Fischhoff85 and included: (1) warning about the possi-bility of bias; (2) describing how the bias distorts gooddecisions; (3) letting the individual make a bias-relatedjudgement error and giving them feedback; and (4)repeating these cycles with extended coaching. Larrick87
reported an example of successful debiasing by keepingit focused on a particular context and a particular bias.Experimental evidence suggests that hindsight bias
can be reduced by considering alternatives.154 In onesuch study, subjects were asked to choose between twoanswers to a difficult question,93 where some were askedto give the reasons they made their choice and otherswere asked to give reasons both for and against theirchoice. Considering both alternatives improved accuracyand reduced the tendency for subjects to be over-confident in their answers.92 Similarly, physicians evalu-ating a difficult test case were more likely to trusta diagnosis when asked to consider alternatives.154
Although debiasing is potentially attractive, severalauthors have expressed scepticism if this approach willwork based on the intrinsic difficulty of changing thesubconscious processing individuals use in decision-making.86 155 156
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 549
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Interventions
Our search yielded two studies. Sherbino andcolleagues19 tested an effort to improve clinicalreasoning of trainees by teaching them cognitiveforcing strategies to counteract biases. The studylacked baseline data (no measure prior to interven-tion) or a control group, and the results were generallynegative. In addition, the reported retention of thecognitive forcing strategies that were the subject of theintervention was short-lived. Eva et al encouraged theuse of combined strategies (pattern recognition plusdeliberate consideration) in teaching students to readelectrocardiograms (ECR), and found this improvedtheir diagnostic performance in part by avoidingbiases.20
Improving metacognition and reflection
Improving metacognition, the ability to reflect on one’sown thought processes, is an appealing approach toreduce cognitive error.77 78 103 Metacognition couldpotentially alert clinicians to possible flaws in theirreasoning and help detect errors. A related andwidely endorsed recommendation is to practicereflectively,82 94 96 97 102 recently referred to as thediagnostic ‘time out’.83 Reflective practice promotesmetacognition and incorporates four distinct elements:Seeking out alternative explanations, exploring theconsequences of alternative diagnoses, being open totests that would differentiate the various possibilities andaccepting uncertainty. This process, essentially gettinga second opinion from your own conscious mind, hasthe potential to avoid many of the inherent pitfalls ofheuristic thought.82
Several tools have been suggested that might behelpful to promote metacognition and reflective prac-tice, including Trowbridge’s ‘12 Tips’ and Leonidas’‘Ten Commandments’.83 157 Using a diagnosis checklist,by promoting conscious review and reflection, has alsobeen advocated as a way to avoid pitfalls in clinicalreasoning.106 157
Interventions
Two studies were identified. Mamede and colleaguesfound that conscious reflection decreased thetendency towards availability bias,21 and Coderre et al
demonstrated that reflection on an initial diagnosiswas helpful if the initial diagnosis was wrong, and didnot lead to new errors if the initial diagnosis wascorrect.22 A limitation of both studies is that theadditional time spent on problem solving may be whatis driving the result, not conscious reflection per se.Also, both studies involved trainees in a laboratoryenvironment, so that the positive results would have tobe reconfirmed in practice settings. It is therefore
inconclusive whether these techniques successfullyreduce diagnostic errors.
Consider alternatives
A central element of reflective practice is reviewingalternative diagnoses, an approach widely endorsed asa valid approach to improved decision-making107 whichwe consider separately in this section. In this approach,clinicians should invoke what has been called theuniversal antidote, ‘Could this be something else?’ anduse appropriate tests to exclude the alternatives, ratherthan ordering tests that simply confirm original suspi-cions.107 Others79 have also suggested that clinicians ‘jotdown, in advance, outcomes that would support one’sinitial conclusions and also those that would disconfirmthem’ or consider alternatives.111 A related strategy is toassume the perspective of an outside observer,86
prompting evaluation of the decision-making strategythat was used and whether or not it was flawed. Militaryplanners have used ‘prospective hindsight’ to teach thisprinciple: one looks into the future to see that theworking diagnosis is not correct: What was missed andwhat else should have been considered?97 112
Interventions
Our search yielded one study that tested an interven-tion in this category. Wolpaw et al23 attempted toimprove clinical reasoning and decision-making skillsthrough a six-step training programme for medicalstudents to express their diagnostic reasoning process.The impact of this technique on diagnostic errors isinconclusive since the study did not assess the reduc-tion of diagnostic errors, but only assessed frequencyand thoroughness of their skills in presenting a patientcase. The study only measured the presence/amountof reasoning and not accuracy thereof, and so it isunclear how this intervention would improve diag-nostic accuracy.
Improve rational processing
Rational, deliberate review and consideration combinethe use of evidence-based knowledge158 159 with twonormative approaches, the use of expected value deci-sion-making160 to choose among a group of possiblediagnoses and Bayesian analysis to incorporate testresults in considering a single diagnosis. Kassirer et al47
describes the process of clinical reasoning as generatinginitial hypothesis which are then investigated by diag-nostic tests and Bayesian analysis until an appropriatethreshold (Treat, Don’t Treat) is reached. Kassirersuggests that the essential skills of clinical reasoning canand should be taught to medical students from their firstdays,126 and reviewers have concluded that consciousreview can be taught effectively.121 122 Trainees taught
550 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

principles of evidence-based medicine are more likely touse Bayesian techniques to interpret clinical findings.158
In efforts to reduce surgical cognitive errors, Brannick et
al108 oriented surgical trainees to Reason’s major errortypes using an educational video and role-playingemphasising errors. Although actual surgical error rateswere the same as in untrained controls after a month,attention to detail improved.108
Category 2 summary
We noted a major discrepancy between the breadth andenthusiasm for these interventions in the backgroundstudies, but a paucity of actual interventions. For all threecategories, there is very limited evidence addressingdiagnostic accuracy or errors. The studies identifiedinvolved trainees in laboratory-like settings, limiting theability to generalise the findings to real practice.
3) Get help: use other people and decision support toolsGiven the constraints of human cognition,78 physiciansmay be able to augment their innate cognitive abilities byobtaining advice and help from others. All of the testedinterventions in this category are detailed together inonline appendix C and were organised in the followingcategories.
Second opinions
Interventions
Several studies have demonstrated that second reviewsof surgical pathology or cytology specimens finda small but important group of errors,24e28 anda growing number of healthcare systems now requiresecond readings in case types known to have substan-tial rates of inter-observer variability. Most of thesestudies do not, however, include data on patientoutcomes (table 3).Second readings in radiology also improve test sensi-
tivity. Duijm et al31 found that multiple independentreaders (radiologists or technicians) increased cancerdetection rates with only a slight decrease in specificity,and Kwek et al32 found that second reading increasedcancer detection by 5%.The impact of second readings has been mixed in
other settings. Second reading of Emergency Room(ER) imaging studies was helpful in one study,30 but inanother, besides identifying previously missed abnor-malities, the second reading introduced new misinter-pretations leading to inappropriate changes inmanagement.29 Canon et al33 measured the impact ofindependent double reading of barium enemas andfound no effect on the sensitivity of polyp detection andan increased rate of false positives.Thus, the overall impact of ‘second opinions’ on
diagnostic errors appears to be mixed. Sensitivity
appears to improve in most but not all studies, but thesecond readings tend to introduce new errors thatdetract from the specificity of the diagnostic test. Resultscould potentially be both reliable and generalisablebecause of the relatively large number of cases reviewedin these studies, and the use of expert reviewers.Costebenefit analyses will be needed to determinewhether the costs of second readings and the seeminglyinevitable increment in false positives are offset by theincreased rate of case finding.
Groups and librarians
Groups can make better decisions than its individualmembers if the members are allowed to function inde-pendently.86 161 Diagnosing challenging cases withinteams or with peers would take advantage of this strategy.A recent novel approach leverages the use of librarianswho are experienced and skilled in identifying infor-mation, evidence, and knowledge relevant to diagnosticalternatives or testing strategies.129e131
Interventions
One study by Christensen et al34 studied team-baseddecisions. This was a well designed, controlled study,but the results were negative: performance did notimprove by using the team.A randomised trial of embedded clinical informa-
ticians at one university demonstrated a positive impacton the clinical care provided,35 although self-reportedperceptions were used in place of actual outcomes.
Decision support
Most studies of decision support tools have evaluatedimpact on process measures, user satisfaction and utilityin a limited sense,141 and are not consistently positive.A systematic review of decision support systems in 1998identified only a single study focusing on diagnosis,133
and in this study, using a decision support tool in anemergency room on patients with joint or bone injuriesactually led to more missed fractures.134
Using linear prediction models (actuarial decision-making, algorithms) has been shown to yield better‘decisions’ than most decision-makers, including experts,in a wide range of settings.111 Wedding and colleagues79132 162 report that actuarial diagnosis was more accuratethan clinical judgement in patients with neuropsychiatricconditions. However, clinicians tend to disregard advicefrom these tools or not use them even when they arereadily available.163 164 The importance of embeddingdecision support in the physician’s workflow has beenrepeatedly emphasised, for example, by incorporatingdecision support logic in computer-based order entrysystems. A systematic review of this approach identified11 controlled trials, seven of which reported improvedprofessional practice141 on ordering diagnostic tests.
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 551
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

Hamm and Zubialde and more recently Schiff andBates have called attention to many other ways in whichthe electronic medical record can enhance clinicalreasoning.102 142 Besides providing clear access to thenecessary data, good records help clinicians organisetheir thoughts, enhance collaborative thinking, enhanceefficiency and promote feedback. Another promisingtype of clinical decision support enabled by electronicrecords is the graphic display of timeline data to assist inthe interpretation of diagnostic test results and to helpdetect subtle trends.137
Interventions
A recent review identified 10 newer studies, eachfocused on a specific clinical condition135 and of theseonly four studies had positive results: one reportedimproved ability to detect and diagnose mood disor-ders in outpatients,136 two improved diagnosis in acutecoronary syndromes36 37 and one evaluated diagnosisof acute abdominal conditions on a surgical service,which improved provider performance but not patientoutcomes38 (table 4). Finally, De Simone et al39
describe a system that receives clinical informationfrom the patient directly and synthesises that infor-mation to aid the clinician in diagnosing the cause ofheadaches. Overall, the studies were all sound andresults seem to be generalisable by virtue of testinga range of subjects and case types.Another approach to supporting the diagnosis of
specific conditions in general is the Infobutton func-tionality, described by Cimino.40 The only available studyof Infobuttons included subjects from varying levels(attending physicians, residents, medical students,nurses) who were mostly satisfied with the tool. Theimpact of the tool on diagnostic accuracy and patientoutcomes was not assessed.
Computer-aided detection systems
Interventions
Five studies have examined the use of computer-aideddetection systems to aid radiologic diagnosis. Peld-schus et al165 studied the effectiveness of an automatedcomputer-aided detection system for chest CT studiesand found both new positives and false positives.Berbaum et al166 found that use of a computer-aideddetection system in chest radiography could notcounteract the satisfaction-of-search effect (being ableto find additional defects beyond the first one) in 16subjects. In another study, Kakeda et al demonstrateda significant beneficial effect of using computer-aideddiagnosis support to help analyse chest radiographs.167
In mammography, Jiang et al168 found that computer-aided diagnosis reduced inter-observer variability, but inanother study computer-assisted mammography inter-pretation had no beneficial effects on cancer detection
and significantly increased the false positive rate of thestudies and the biopsy rate.169 A recent commentary oncomputer-assisted detection noted that while use of thistechnology is increasingly the norm, the jury is still outon its utility.170 All of the intervention studies reviewedwere solid in design and in the interpretation of theresults and conclusions, but the ability to generalise islimited due to studies in just two domains (chest x-raysand mammograms).
Computer-aided interpretation systems
Interventions
Two studies focused on technology to improve ECGinterpretation. Daudelin and Selker171 reported usingan ECG-based acute cardiac ischaemia predictiveinstrument to improve triage decision-making in theER. Olsson et al172 studied the use of an artificial neuralnetwork trained to automatically detect ECGs indi-cating possible transmural ischaemia and found thatthis decision support tool was effective in improvinginexperienced interns’ interpretation of ECGs.
General decision support tools for medical diagnosis
Computer aided decision support tools have also beendeveloped to assist specifically with differential diagnosis.Anecdotally these tools succeed, in a small fraction ofsearches, in suggesting a difficult or obscure diagnosisthat was previously missed. The clinician inputs thepatient’s key findings, and these programmes suggestpossible diagnoses. Some programmes help refine thesechoices by further suggestions of questions to ask, find-ings to look for or tests to perform. Berner et al evaluatedthe first generation products (QMR, DXplain, Iliad andMeditel) using test scenarios and all the products wereeffective in providing useful suggestions.173 However, thecorrect diagnosis appeared on the suggestion list only halfto three-fourths of the time, and all of the programmesgenerated a large number of extraneous conditions.174
Some of these initial products are no longer available,although DXplain has been maintained and updated.
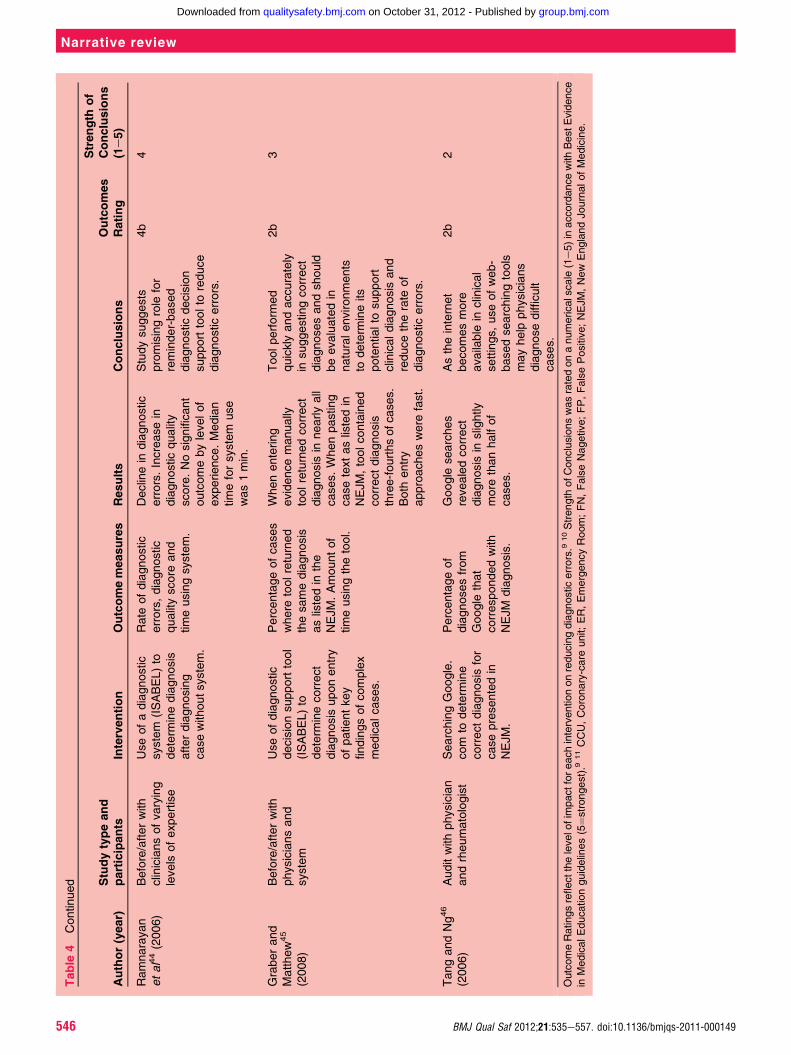
Interventions
Of the many newer web-based decision support tools,‘ISABEL’ has been the most extensively evaluated.Compared with first generation tools, ISABEL displaysmuch improved sensitivity in both paediatric settings4142 and in analysing adult case scenarios, in which thesensitivity approached 100%.43e45 ‘Google’ searchinghas also been evaluated inmedical settings, but suggeststhe correct diagnosis in only 58% of difficult cases.46
Category 3 summary
Overall, the technique of ‘getting help’ during thediagnostic process may be beneficial. The use of decisionsupport resources has been studied more extensively
552 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

than any other intervention, and these approaches, ifused, show promise in their potential to reduce diag-nostic errors. More research is needed regarding the useof second reviews, teams and librarians.
DISCUSSION
Reducing harm from diagnostic errors requires inter-ventions to improve the cognitive processes thatunderlie clinical reasoning. We identified a reasonablylarge literature on potential interventions and organisedthese interventions into three categories: (1) Increasingknowledge and expertise, (2) Improving intuitive anddeliberate consideration and (3) Getting help fromcolleagues, consultants and tools.We found that most interventions in the literature
were simply ideas or suggestions. Many of these are wellconceptualised and widely endorsed, and seem ripe tobe tested in experimental or real-world clinical settings.A major finding in each of the three categories wasa large discrepancy between the broad and enthusiasticrecommendations for the various interventions, buta relative paucity of actual trials. Of the few studies thatreported true interventions, few included robust designsor metrics. Typically, the interventions involved anobservational study design and measured outcomesbefore and after an intervention with a small number oftrainees or clinicians and/or healthcare sites, withouta control group.Our findings also affirm that the science of out-
come measurement in this area is underdeveloped.Educational interventions in particular are difficult toevaluate in terms of changing attitudes and behavioursin practice. One major issue is the difficulty of demon-strating that diagnosis can be improved by any approachin real-world settings. Definitions of diagnostic error arenot standardised and error designations are typicallysubjective judgements, often confounded by hindsightbias. Measurement instruments and methods to evaluatecognitive intervention effects are not well developed.Additionally, because diagnostic error reflects theinterplay of system-related and patient-dependentfactors, the true effect of a purely cognitive interventionmight be difficult to ascertain. All of these factors posechallenges in the design of future interventions in thisarea.The major limitation of this review is the likelihood
that we overlooked conceptual ideas to improve deci-sion-making from both medical and non-medical fields.Medical diagnosis is essentially a special case of decision-making under conditions of uncertainty, and ideas forimproving these decisions can arise from almost anydiscipline, including the social sciences, business fieldsand military scholars.
A clear challenge going forward is to identify theadvances in these areas that might be applicable toimproving the reliability of medical diagnosis. Despitethe many shortcomings of these studies, our reviewidentified promising ideas for reducing diagnostic errorin each of the three major categories.
Increase knowledgeAt the present time, disease-specific training is the onlyintervention that is both supported by evidence andseems implementable. In the future, simulation offerspotential both in terms of teaching clinicians aboutdiagnostic error and error-prevention strategies, as wellas serving as a method to rapidly build expertisethrough exposure to many types of disease variants.Feedback also offers the potential to reduce errors byhelping develop expertise. Feedback is also the key toreducing overconfidence, which in turn could open thedoor for clinicians to appreciate the possibility of theirown errors and take actions to avoid them. Deliberatefeedback is embedded in many approaches that seek toimprove individual and team performance outside ofmedicine.
Improve clinical reasoningAlthough some of the interventions to improvereasoning have been successful with trainees, most haveyet to be implemented or evaluated in practice. Reflec-tive practice and active metacognitive review may havegreat potential to reduce diagnostic error, and the toolsto promote these practices need to be further developedand evaluated in practice. These approaches expand thenumber of conditions to be considered and effectivelyaddress many of the major causes of cognitive error,including context errors, framing bias and prematureclosure. However, the cost of trade-offs is not clear. Forexample, will the broadened consideration of alternativediagnoses lead to inappropriate or costly testing,divert attention away from the correct diagnosis or bedeleterious in another way?
Get helpDecision support for diagnosis has the unique advantagethat it can be implemented at the system level, withoutrequiring some new skill or behaviour to be learnt byclinicians. Still, clinicians need to be willing to takeadvantage of these resources, and error reduction willcritically hinge on how well the support functionality isincorporated into everyday workflow and how clinicianswill deal with the specificity problem. Using informa-ticians, working more effectively in groups, taking fulladvantage of the comprehensive electronic healthrecord and relying more on actuarial tools (algorithms)may be effective strategies. Second opinions and
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 553
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from
consultations bring fresh eyes to examine a case,a powerful and effective way to find and correctdiagnostic errors.
CONCLUSIONS
In conclusion, there is a surprisingly wide range ofpossible approaches to reducing the cognitive contri-butions to diagnostic error. Not all the suggestions havebeen tested, and of those that have, the evaluationstypically involved trainees in artificial settings, making itdifficult to extrapolate the results to actual practice.The field is immature and progress in reducing diag-
nostic error will require considerable research to eval-uate the relative merits of these different ideas,refinements in the methodology of defining andmeasuring outcomes in preventing diagnostic error andharm, and leveraging advances in other aspects ofmedical decision-making and cognitive sciences that maymake medical diagnosis more reliable.
Author affiliations1VA Medical Center, Northport, New York, USA2Department of Medicine, SUNY Stony Brook, New York, USA3RTI International, Research Triangle Park, North Carolina, USA4School of Biomedical Informatics, University of Texas Health Science Centerin Houston, Houson, Texas, USA5National Center for Cognitive Informatics and Decision Making in Healthcare,University of Texas Health Science Center in Houston, Houston, Texas, USA6Houston VA HSR&D Center of Excellence, and the Center of Inquiry toImprove Outpatient Safety Through Effective Electronic Communication,Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas, USA7Section of Health Services Research, Department of Medicine, Baylor Collegeof Medicine, Houston, Texas, USA8Center for Quality Improvement and Patient Safety, Agency for HealthcareResearch and Quality, Rockville, Maryland, USA
Acknowledgements We gratefully acknowledge administrative and literatureresearch assistance from Ms Grace Garey, Mary Lou Glazer, Diane Martin1and Wendy Isser.
Contributors All listed authors contributed to the conception and design, oranalysis and interpretation of data; drafting the article or revising it critically forimportant intellectual content; and final approval of the version to bepublished. MLG is the guarantor, contributed to the study design, contributedto data synthesis, wrote the paper and coordinated revisions. SK performedthe literature search, contributed to data analysis and synthesis, and writingand revising the manuscript. VLP performed the analytical review andcontributed to the manuscript revisions. ANDM performed the analyticalreview and contributed to the manuscript revisions. AVS contributed to thestudy design, the literature search, data analysis and synthesis, and reviewingand editing the manuscript. NL performed the literature search and contributedto data synthesis and analysis. ET performed the literature search andcontributed to the synthesis and manuscript revisions. KH contributed to thestudy design, reviewed the literature search, and reviewed and edited themanuscript; KAL contributed to the study design, reviewed the literaturesearch, and reviewed and edited the manuscript. HS contributed to the studydesign, data analysis and synthesis, writing and revising the manuscript.
Funding This study was funded by the Agency for Healthcare Research andQuality (AHRQ) ACTION II Task Order #8, Contract No. HHSA290200600001and in part by the Houston VA HSR&D Center of Excellence (HFP90-020).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1. Berner E, Graber M. Overconfidence as a cause of diagnostic error
in medicine. Am J Med 2008;121:S2e23.2. Kostopoulou O, Delaney BC, Munro CW. Diagnostic difficulty and
error in primary care - a systematic review. Fam Pract2008;25:400e13.
3. Kostopoulou O. Do GPs report diagnostic errors? Fam Pract2008;25:1e2.
4. Graber ML, Franklin N, Gordon R. Diagnostic error in internalmedicine. Arch Intern Med 2005;165:1493e9.
5. Schiff GD, Hasan O, Kim S, et al. Diagnostic error in medicine:analysis of 583 physician-reported errors. Arch Intern Med2009;169:1881e7.
6. Zwaan L, de Bruijne M, Wagner C, et al. Patient record review of theincidence, consequences, and causes of diagnostic adverse events.Arch Intern Med 2010;170:1015e21.
7. Kachalia A, Gandhi TK, Puopolo AL, et al. Missed and delayeddiagnoses in the emergency department: a study of closedmalpractice claims from four liability insurers. Ann Emerg Med2007;49:196e205.
8. Singh H, Graber ML, Kissam SM, et al. System-related interventionsto reduce diagnostic errors: a narrative review. BMJ Qual Saf2012;21:160e70.
9. Gordon M, Findley R. Educational interventions to improve handoverin health care: a systematic review. Med Educ 2011;45:1081e90.
10. Barr H, Freeth D, Hammick M, et al. Evaluations of InterprofessionalEducation: A United Kingdom Review of Health and Social Care.http://www.caipe.org.uk/silo/files/evaluations-of-interprofessional-education.pdf
11. BEME. Best Evidence in Medical Education. BEME Collaboration,2003. http://www.bemecollaboration.org
12. Fridriksson S, Hillman J, Landtblom AM, et al. Education of referringdoctors about sudden onset headache in subarachnoid hemorrhage:a prospective study. Acta Neurol Scand 2001;103:238e42.
13. Rezvyy G, Parniakov A, Fedulova E, et al. Correcting biases inpsychiatric diagnostic practice in Northwest Russia: comparing theimpact of a general educational program and a specific diagnostictraining program. BMC Med Educ 2008;8:15.
14. Gutmark R, Halsted MJ, Perry L, et al. Use of computer databases toreduce radiograph reading errors. J Am Coll Radiol 2007;4:65e8.
15. Bond WF, Deitrick LM, Arnold DC, et al. Using simulation to instructemergency medicine residents in cognitive forcing strategies. AcadMed 2004;79:438e46.
16. Carlson J, Abe M, Bridges D, et al. The impact of a diagnosticreminder system on student clinical reasoning during simulated casestudies. Simul Healthc 2011;6:11e18.
17. Tudor GR, Finlay DB. Error review: can this improve reportingperformance? Clin Radiol 2001;56:751e4.
18. Wood DS, Tracey TJG. A brief feedback intervention for diagnosticovershadowing. Train Educ Prof Psychol 2009;3:218e25.
19. Sherbino J, Dore K, Siu E, et al. The effectiveness of cognitiveforcing strategies to decrease diagnostic errordan exploratorystudy. Teach Learn Med 2011;23:78e85.
20. Eva KW, Hatala RM, LeBlanc VR, et al. Teaching from the clinicalreasoning literature: combined reasoning strategies help novicediagnosticians overcome misleading information. Med Educ2007;41:1152e8.
21. Mamede S, van Gog T, van den Berge K, et al. Effect of availabilitybias and reflective reasoning on diagnostic accuracy among internalmedicine residents. JAMA 2010;304:1198e203.
22. Coderre S, Wright B, McLaughlin K. To think is good: querying aninitial hypothesis reduces diagnostic error in medical students. AcadMed 2010;85:1125e9.
23. Wolpaw T, Papp KK, Bordage G. Using SNAPPS to facilitate theexpression of clinical reasoning and uncertainties: a randomizedcomparison group trial. Acad Med 2009;84:517e24.
24. Raab SS, Grzybicki DM, Mahood LK, et al. Effectiveness of randomand focused review in detecting surgical pathology error. Am J ClinPathol 2008;130:905e13.
25. Raab SS, Stone CH, Jensen CS, et al. Double slide viewing asa cytology quality improvement initiative. Am J Clin Pathol2006;125:526e3.
26. Manion E, Cohen MB, Weydert J. Mandatory second opinion insurgical pathology referral material: clinical consequences of majordisagreements. Am J Surg Pathol 2008;32:732e7.
27. Nordrum I, Johansen M, Amin A, et al. Diagnostic accuracy ofsecond-opinion diagnoses based on still images. Hum Pathol2004;35:129e35.
28. Hamady ZZ, Mather N, Lansdown MR, et al. Surgical pathologicalsecond opinion in thyroid malignancy: impact on patients’management and prognosis. Eur J Surg Oncol 2005;31:74e7.
554 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from
29. Benger JR, Lyburn ID. What is the effect of reporting all emergencydepartment radiographs? Emerg Med J 2003;20:40e3.
30. Espinosa JA, Nolan TW. Reducing errors made by emergencyphysicians in interpreting radiographs: longitudinal study. BMJ2000;320:737e40.
31. Duijm LE, Groenewoud JH, Fracheboud J, et al. Additional doublereading of screening mammograms by radiologic technologists:impact on screening performance parameters. J Natl Cancer Inst2007;99:1162e70.
32. Kwek BH, Lau TN, Ng FC, et al. Non-consensual double reading inthe Singapore breast screening project: benefits and limitations. AnnAcad Med Singapore 2003;32:438e41.
33. Canon CL, Smith JK, Morgan DE, et al. Double reading ofbarium enemas: is it necessary? AJR Am J Roentgenol2003;181:1607e10.
34. Christensen C, Larson JR Jr, Abbott A, et al. Decision making ofclinical teams: communication patterns and diagnostic error. MedDecis Making 2000;20:45e50.
35. Mulvaney SA, Bickman L, Giuse NB, et al. A randomizedeffectiveness trial of a clinical informatics consult service: impact onevidence-based decision-making and knowledge implementation.J Am Med Inform Assoc 2008;15:203e11.
36. Pozen MW, D’Agostino RB, Selker HP, et al. A predictive instrumentto improve coronary-care-unit admission practices in acute ischemicheart disease. N Engl J Med 1984;310:1273e8.
37. Selker HP, Beshansky JR, Griffith JL, et al. Use of the acute cardiacischemia time-insensitive predictive instrument (ACI-TIPI) to assistwith triage of patients with chest pain or other symptoms suggestiveof acute cardiac ischemia. A multicenter, controlled clinical trial. AnnIntern Med 1998;129:845e55.
38. Bogusevicius A, Maleckas A, Pundzius J, et al. Prospectiverandomised trial of computer-aided diagnosis and contrast radiographyin acute small bowel obstruction. Eur J Surg 2002;168:78e83.
39. De Simone R, Coppola G, Ranieri A, et al. Validation of AIDACefalee, a computer-assisted diagnosis database for themanagement of headache patients. Neurol Sci 2007;28(Suppl 2):S213e16.
40. Cimino JJ. Use, usability, usefulness, and impact of an infobuttonmanager. AMIA Annu Symp Proc 2006:151e5.
41. Ramnarayan P, Winrow A, Coren M, et al. Diagnostic omissionerrors in acute paediatric practice: impact of a reminder system ondecision-making. BMC Med Inform Decis Mak 2006;6:37.
42. Ramnarayan P, Cronje N, Brown R, et al. Validation of a diagnosticreminder system in emergency medicine: a multi-centre study.Emerg Med J 2007;24:619e24.
43. Ramnarayan P, Kapoor RR, Coren J, et al. Measuring the impact ofdiagnostic decision support on the quality of clinical decision making:development of a reliable and valid composite score. J Am MedInform Assoc 2003;10:563e72.
44. Ramnarayan P, Roberts GC, Coren M, et al. Assessment of thepotential impact of a reminder system on the reduction of diagnosticerrors: a quasi-experimental study. BMC Med Inform Decis Mak2006;6:22.
45. Graber ML, Mathew A. Performance of a web-based clinicaldiagnosis support system for internists. J Gen Intern Med 2008;23(Suppl 1):37e40.
46. Tang H, Ng JH. Googling for a diagnosiseuse ofGoogle as a diagnostic aid: internet based study. BMJ2006;333:1143e5.
47. Kassirer JP, Wong J, Kopelman R. Learning Clinical Reasoning. 2ndedn. Baltimore, MD: Lippincott Williams and Wilkins, 2010.
48. Gigerenzer G. Adaptive Thinking: Rationality in the Real World.New York: Oxford University Press, 2000.
49. Elstein AS. Thinking about diagnostic thinking: a 30-yearperspective. Adv Health Sci Educ Theory Pract 2009;14(Suppl 1):7e18.
50. Klein G. Sources of Power: How People Make Decisions.Cambridge, MA: The MIT Press, 1998.
51. Klein G. The Power of Intuition. New York, NY: Doubleday, 2003.52. Bazerman MH, Moore DA. Improving Decision Making. Judgment
in Managerial Decision Making. John Wiley and Sons,2009:179e99.
53. Norman G. Dual processing and diagnostic errors. Adv Health SciEduc Theory Pract 2009;14( Suppl 1):37e49.
54. Smith-Bindman R, Chu PW, Miglioretti DL, et al. Comparison ofscreening mammography in the United States and the Unitedkingdom. JAMA 2003;290:2129e37.
55. Singh H, Sethi S, Raber M, et al. Errors in cancer diagnosis:current understanding and future directions. J Clin Oncol2007;25:5009e18.
56. Bowen JL. Educational strategies to promote clinical diagnosticreasoning. N Engl J Med 2006;355:2217e25.
57. Davis D, O’Brien MA, Freemantle N, et al. Impact of formalcontinuing medical education: do conferences, workshops, rounds,and other traditional continuing education activities changephysician behavior or health care outcomes? JAMA1999;282:867e74.
58. Freidlander ML, Phillips SD. Preventing anchoring errors in clinicaljudgment. J Consult Clin Psychol 1984;52:366e71.
59. Gentner D, Lowenstein G, Thompson L. Learning and transfer:a general role for analogic encoding. J Educ Psychol2003;95:393e408.
60. Hershberger PJ, Markert RJ, Part HM, et al. Understanding andaddressing cognitive bias in medical education. Adv Health Sci Educ1996;1:221e6.
61. Parmley MC. Confirmation Bias on Diagnostic Decision Making.Drexel University, 2006.
62. Hogarth R. Educating Intuition. University of Chicago Press, 2001.63. Bond W, Kuhn G, Binstadt E, et al. The use of simulation in
the development of individual cognitive expertise in emergencymedicine. Acad Emerg Med 2008;15:1037e45.
64. Schiff GD. Minimizing diagnostic error: the importance of follow-upand feedback. Am J Med 2008;121:S38e42.
65. Jamtvedt G, Young JM, Kristoffersen DT, et al. Does telling peoplewhat they have been doing change what they do? A systematicreview of the effects of audit and feedback. Qual Saf Health Care2006;15:433e6.
66. Papa FJ, Aldrich D, Schumacker RE. The effects of immediateonline feedback upon diagnostic performance. Acad Med 1999;74:S16e18.
67. Stone ER, Opel RB. Training to improve calibration anddiscrimination: the effects of performance andenvironment feedback. Organ Behav Hum Decis Process2000;83:282e309.
68. Alpert HR, Hillman BJ. Quality and variability in diagnostic radiology.J Am Coll Radiol 2004;1:127e32.
69. Arkes H. Impediments to accurate clinical judgment and possibleways to minimize their impact. J Consult Clin Psychol1981;49:323e30.
70. Humble JE, Keim RT, Hershauer JC. Information systems design:an empirical study of feedback effects. Behav Inf Technol1992;11:237e44.
71. Pulford BD, Colman AM. Overconfidence: feedback and itemdifficulty effects. Pers Individ Differ 1997;23:125e33.
72. Subbotin V. Outcome feedback effects on under- andoverconfidence judgments (general knowledge tasks). Organ BehavHum Decis Process 1996;66:268e76.
73. Fischer MA, Mazor KM, Baril J, et al. Learning from mistakes.Factors that influence how students and residents learn frommedical errors. J Gen Intern Med 2006;21:419e23.
74. Eva KW. Diagnostic error in medical education: where wrongs canmake rights. Adv Health Sci Educ Theory Pract 2009;14(Suppl 1):71e81.
75. Eva KW. What every teacher needs to know about clinicalreasoning. Med Educ 2005;39:98e106.
76. Croskerry P. Cognitive forcing strategies in clinical decision making.Ann Emerg Med 2003;41:110e20.
77. Croskerry P. The importance of cognitive errors in diagnosis andstrategies to minimize them. Acad Med 2003;78:775e80.
78. Croskerry P. Diagnostic Failure: A Cognitive and Affective Approachin Advances in Patient Safety: From Research to Implementation.Rockville, MD: Agency for Healthcare Research and Quality(Publication No. 050021), 2005;2:241e54.
79. Wedding D, Faust D. Clinical judgment and decision making inneuropsychology. Arch Clin Neuropsychol 1989;4:233e65.
80. Groves M, O’Rourke P, Alexander H. Clinical reasoning: the relativecontribution of identification, interpretation and hypothesis errors tomisdiagnosis. Med Teach 2003;25:621e5.
81. Pines JM. Profiles in patient safety: confirmation bias in emergencymedicine. Acad Emerg Med 2006;13:90e4.
82. Moulton CE, Regehr G, Mylopoulos M, et al. Slowing down whenyou should: a new model of expert judgement. Acad Med 2007;82:S109e16.
83. Trowbridge RL. Twelve tips for teaching avoidance of diagnosticerrors. Med Teach 2008;30:496e500.
84. Kuhn GJ. Diagnostic errors. Acad Emerg Med 2002;9:740e50.85. Fischhoff B. Debiasing. In: Kahneman D, Slovic P, Tversky A, eds.
Judgment Under Uncertainty. New York: Cambridge UniversityPress, 1982:422e44.
86. Milkman KL, Chugh D, Bazerman MH. How can decision making beimproved? Perspect Psychol Sci 2009;4:379e83.
87. Larrick RP. Debiasing. In: Koehler DJ, Harvery N, eds. BlackwellHandbook of Judgment and Decision Making. Oxford, UK:Blackwell, 2004.
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 555
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from
88. Koriat A, Bjork RA, Sheffer L, et al. Predicting one’s own forgetting:the role of experience-based and theory-based processes. J ExpPsychol Gen 2004;133:643e56.
89. Renner C, Renner M. But I thought I knew that: using confidenceestimation as a debiasing technique to improve Classroomperformance. Appl Cogn Psychol 2001;15:23e32.
90. Estrada CA, Isen AM, Young MJ. Positive affect facilitatesintegration of information and decreases anchoring in reasoningamong physicians. Organ Behav Hum Decis Process1997;72:117e35.
91. Scott IA. Errors in clinical reasoning: causes and remedialstrategies. BMJ 2009;338:b1860.
92. Slovic P, Fischoff B. On the psychology of experimental surprises.J Exp Psychol Hum Percept Perform 1977;3:544e51.
93. Lichtenstein S, Fischoff B, Bishop B. Calibration of probabilities: Thestate of the art to 1980. In: Kahneman D, Slovic P, Tversky A, eds.Judgment Under Uncertainty: Heuristics and Biases. New York:Cambridge University Press, 1982.
94. Schon DA. Educating the Reflective Practioner. San Francisco:Jossey-Bass, 1987.
95. Greenhalgh T. Intuition and evidenceeuneasy bedfellows? Br J GenPract 2002;52:395e400.
96. Mamede S, Schmidt HG, Rikers R. Diagnostic errors and reflectivepractice in medicine. J Eval Clin Pract 2007;13:138e45.
97. Singh H, Petersen LA, Thomas EJ. Understanding diagnostic errorsin medicine: a lesson from aviation. Qual Saf Health Care2006;15:159e64.
98. Brawn R. The formal and the intuitive in science and medicine. In:Atkinson T, Claxton G, eds. The Intuitive Practitioner. BuckinghamUK: Open University Press, 2000:149e64.
99. Gregory G. Developing intuition through management education. In:Atkinson T, Claxton G, eds. The Intuitive Practitioner. Buckingham,UK: Open University Press, 2000.
100. Noddings S, Shore PJ. Awakening the Inner Eye: Intuition inEducation. New York: Teachers College Press, 1984.
101. Quirk M. Intuition and Metacognition in Medical Education. NewYork, NY: Springer Publishing Co., 2006.
102. Hamm RM, Zubialde J. Physicians’ expert cognition and the problemof cognitive bias. Med Decis Making 1995;22:181e213.
103. Croskerry P. The cognitive imperative: thinking about how we think.Acad Emerg Med 2000;7:1223e31.
104. Leonidas L. Ten commandments to reduce cognitive errors. In:Graber, ML. Educational interventions to reduce diagnostic error.Adv Health Sci Educ 2009;14:63e9.
105. Gawande A. The Checklist Manifesto: How to Get Things Right. 1stedn. New York: Metropolitan Books, 2010.
106. Ely JW, Graber M, Croskerry PC. Checklists to reduce diagnosticerrors. Acad Med 2011;86:7.
107. Taleb N. The Black Swan. New York: Random House, 2007.108. Brannick MT, Fabri PJ, Zayas-Castro J, et al. Evaluation of an error-
reduction training program for surgical residents. Acad Med2009;84:1809e14.
109. Arkes H. Why medical errors can’t be eliminated: uncertainties andthe hindsight bias. Chron High Educ 2000;46:591e600.
110. Schwenk CR. Cognitive simplification processes in strategicdecision-making. Strategic Manag J 1984;5:111e28.
111. Baron J. Thinking and Deciding. 3rd edn. New York, NY: CambridgeUniversity Press.
112. Mitchell DJ, Russo JE, Pennington N. Back to the future: temporalperspective in the explanation of events. J Behav Decis Making1989;2:25e38.
113. Mussweiler T, Strack F, Pfeiffer T. Overcoming the inevitableanchoring effect: considering the opposite compensates forselective accessibility. Pers Soc Psychol Bull 2000;26:1142e50.
114. Lord CG, Lepper MR, Preston E. Consider the opposite:a corrective strategy for social judgment. J Pers Soc Psychol1984;37:1231e43.
115. Arzy S, Brezis M, Khoury S, et al. Misleading one detail:a preventable mode of diagnostic error? J Eval Clin Pract2009;15:804e6.
116. Gorman M, Gorman M. A comparison of disconfirmatory,confirmatory and control strategies on Watson’s 2-4-6 task. Q J ExpPsychol 1984;36A:629e48.
117. Hirt E, Markman K. Multiple explanation: a consider-an-alternativestrategy for debiasing judgments. J Pers Soc Psychol1995;69:1069e86.
118. Mumma G, Steven W. Procedural debiasing of primary/anchoring effects in clinical-like judgments. J Clin Psychol1995;51:841e53.
119. Strauss SE, Glasziou P, Richardson WS, et al. Evidence-BasedMedicine, 4th edn. How to Practice and Teach. New York, NY:Churchill Livingstone, 2011.
120. Sox HC. Medical Decision Making. Butterworth-Heinman, 1988.121. Dobbie AE, Schneider FD, Anderson AD, et al. What evidence
supports teaching evidence-base medicine? Acad Med2000;75:1184e5.
122. Khan KS, Coomarasamy A. A hierarchy of effective teaching andlearning to acquire competence in evidenced-based medicine. BMCMed Educ 2006;15:59.
123. Croskerry P. Clinical cognition and diagnostic error: applications ofa dual process model of reasoning. Adv Health Sci Educ TheoryPract 2009;14(Suppl 1):27e35.
124. Ullman DG. Making Robust Decisions: Decision Management forTechnical, Business, and Service Teams. Victoria, BC: TraffordPublishing, 2006.
125. Pauker SC, Kassirer JP. The threshold approach to clinical decisionmaking. N Engl J Med 1980;302:1109e17.
126. Kassirer JP. Teaching clinical reasoning: case-based and coached.Acad Med 2010;85:1118e24.
127. Tatarka CJ. Overcoming biases in military problem analysis anddecision-making. Mil Intelligence 2002;28:8e10.
128. Raab SS. Improving patient safety by examining pathology errors.Clin Lab Med 2004;24:863.
129. Zipperer L, Sykes J. The role of librarians in patient safety: gapsand strengths in the current culture. J Med Libr Assoc2004;92:498e500.
130. Albert KM. Integrating knowledge-based resources into theelectronic health record: history, current status, and role oflibrarians. Med Ref Serv Q 2007;26:1e19.
131. Zipperer L, Sykes J. Engaging as partners in patient safety: theexperience of librarians. Patient Saf Qual Healthc. March/April2009;6:28e33,32e3.
132. Wedding D. Comparison of statistical and actuarial models forpredicting lateralization of brain-damage. Clin Neuropsychol1983;5:15e20.
133. Hunt DL, Haynes RB, Hanna SE, et al. Effects of computer-based clinical decision support systems on physician performanceand patient outcomes: a systematic review. JAMA1998;280:1339e46.
134. Klassen TP, Ropp LJ, Sutcliffe T, et al. A randomized controlled trialof radiograph ordering for extremity trauma in a pediatric emergencydepartment. Ann Emerg Med 1993;22:1524e9.
135. Garg AX, Adhikari NK, McDonald H, et al. Effects of computerizedclinical decision support systems on practitioner performance andpatient outcomes: a systematic review. J Am Med Assoc2005;293:1223e38.
136. Cannon DS, Allen SN. A comparison of the effects of computerand manual reminders on compliance with a mental healthclinical practice guideline. J Am Med Inform Assoc2000;7:196e203.
137. Radecki RP, Medow MA. Cognitive debiasing through sparklines inclinical data displays. AMIA Annu Symp Proc 2007:1085.
138. Reyna VF, Nelson WL, Han PK, et al. How numeracy influences riskcomprehension and medical decision making. Psychol Bull2009;135:943e73.
139. Bhandari G, Hassanein K, Deaves R. Debiasing investors withdecision support systems: an experimental investigation. DecisSupport Syst 2008;46:399e410.
140. Cook MB, Smallman HS. Human factors of the confirmation bias inintelligence analysis: decision support from graphical evidencelandscapes. Hum Factors 2008;50:745e54.
141. Kawamoto K, Lobach DF. Clinical decision support provided withinphysician order entry systems: a systematic review of featureseffective for changing clinician behavior. AMIA Annu Symp Proc2003:361e5.
142. Schiff G, Bates DW. Can electronic clinical documentation helpprevent diagnostic errors? N Engl J Med 2010;362:1066e9.
143. Norman G. Building on experienceethe development of clinicalreasoning. N Engl J Med 2006;355:2251e2.
144. Chi MTH, Glaser R, Farr MJ. The Nature of Expertise. Hillsdale, NJ:L. Erlbaum Associates, 1988.
145. Ericsson KA. Deliberate practice and acquisition of expertperformance: a general overview. Acad Emerg Med2008;15:988e94.
146. Norman G. Research in clinical reasoning: past history and currenttrends. Med Educ 2005;39:418e27.
147. Bordage G. Why did I miss the diagnosis? Some cognitiveexplanations and educational implications. Acad Med 1999;74:S138e43.
148. Lee JK. Qualityda radiology imperative: interpretation accuracy andpertinence. J Am Coll Radiol 2007;4:162e5.
149. Wood D. An Intervention for Diagnostic Overshadowing [e-book].US: ProQuest Information & Learning. Ipswich, MA: PsycINFO,2005.
556 BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

150. Shojania KG, Burton EC, McDonald KM, et al. The autopsy asan Outcome and Performance Measure (Evidence Report/Technology Assessment No. 58; AHRQ Publication No.03eE002). Rockville, MD: Agency for Healthcare Research andQuality, 2002.
151. Hogarth RM. Educating Intuition. Chicago: University of ChicagoPress, 2001.
152. Croskerry P. A universal model of diagnostic reasoning. Acad Med2009;84:1022e8.
153. Coderre S, Mandin H, Harasyn PH, et al. Diagnostic reasoningstrategies and diagnostic success. Med Educ 2003;37:695e703.
154. Arkes HR, Faust D, Guilmette TJ, et al. Eliminating the hindsightbias. J Appl Psychol 1988;73:305e7.
155. Graber M. Metacognitive training to reduce diagnostic errors: readyfor prime time? Acad Med 2003;78:781.
156. Fioratou E, Flin R, Glavin R. No simple fix for fixation errors:cognitive processes and their clinical applications. Anaesthesia2010;65:61e9.
157. Graber ML. Educational strategies to reduce diagnostic error: canyou teach this stuff? Adv Health Sci Educ Theory Pract 2009;14(Suppl 1):63e9.
158. Sackett DL, Strauss SE, Richardson WS, et al. Evidence-BasedMedicine: How to Practice and Teach. New York: ChurchillLivingstone, 1997.
159. Sox HC Jr, Blatt MA, Higgins MC, et al. Medical Decision Making.Stoneham, MA: Butterworth-Heinemann, 1988.
160. Janis IL, Mann L. Decision Making: A Psychological Analysis ofConflict, Choice, and Commitment. New York: Free Press, 1977.
161. Surowiecki J. The Wisdom of Crowds. New York, NY: AnchorBooks, 2005.
162. Wedding D. Clinical and statistical prediction in neuropsychology.Clin Neuropsychol 1983;5:49e55.
163. Smith WR. Evidence for the effectiveness of techniques to changephysician behavior. Chest 2000;118:8Se17S.
164. Militello L, Patterson ES, Tripp-Reimer T, et al. Clinical reminders:Why don’t people use them? Proceedings of the human factors andErgonomics Society - 48th Annual Meeting, New Orleans,Louisiana, 2004;48:1651e5.
165. Peldschus K, Herzog P, Wood SA, et al. Computer-aided diagnosisas a second reader: spectrum of findings in CT studies of the chestinterpreted as normal. Chest 2005;128:1517e23.
166. Berbaum KS, Caldwell RT, Schartz KM, et al. Does computer-aideddiagnosis for lung tumors change satisfaction of search in chestradiography? Acad Radiol 2007;14:1069e76.
167. Kakeda S, Moriya J, Sato H, et al. Improved detection of lungnodules on chest radiographs using a commercialcomputer-aided diagnosis system. AJR Am J Roentgenol2004;182:505e10.
168. Jiang Y, Nishikawa RM, Schmidt RA, et al. Potential of computer-aided diagnosis to reduce variability in radiologists’ interpretations ofmammograms depicting microcalcifications. Radiology2001;220:787e94.
169. Fenton JJ, Taplin SH, Carney PA, et al. Influence of computer-aideddetection on performance of screening mammography. N Engl JMed 2007;356:1399e409.
170. Hall FM. Breast imaging and computer-aided detection. N Engl JMed 2007;356:1464e6.
171. Daudelin DH, Selker HP. Medical error prevention in ED triage forACS: use of cardiac care decision support and quality improvementfeedback. Cardiol Clin 2005;23:601e14, ix.
172. Olsson SE, Ohlsson M, Ohlin H, et al. Decision support for the initialtriage of patients with acute coronary syndromes. Clin Physiol FunctImaging 2006;26:151e6.
173. Berner ES, Webster GD, Shugerman AA, et al. Performance of fourcomputer-based diagnostic systems. N Engl J Med1994;330:1792e6.
174. Kassirer JP. A report card on computer-assisted diagnosisdthegrade: C. N Engl J Med 1994;330:1824e5.
PAGE fraction trail=22.5
BMJ Qual Saf 2012;21:535e557. doi:10.1136/bmjqs-2011-000149 557
Narrative review
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from

doi: 10.1136/bmjqs-2011-0001492012
2012 21: 535-557 originally published online April 27,BMJ Qual Saf Mark L Graber, Stephanie Kissam, Velma L Payne, et al. error: a narrative reviewCognitive interventions to reduce diagnostic
http://qualitysafety.bmj.com/content/21/7/535.full.htmlUpdated information and services can be found at:
These include:
Data Supplement http://qualitysafety.bmj.com/content/suppl/2012/06/18/bmjqs-2011-000149.DC1.html
"Supplementary Data"
References
http://qualitysafety.bmj.com/content/21/7/535.full.html#related-urlsArticle cited in:
http://qualitysafety.bmj.com/content/21/7/535.full.html#ref-list-1This article cites 140 articles, 25 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 31, 2012 - Published by qualitysafety.bmj.comDownloaded from