national drug report 2008 (data of 2007) - un armenia drug report_eng.pdf · 2014-12-03 ·...
TRANSCRIPT

1
National Report 2008
National Drug Report 2008(data of 2007)
Authors:Vladimir Davidyants
Zaruhi BeglaryanGrigori Malintsyan
Arman TatoyanArtur Potosyan
Ashot Davidyants
Especially, we would like to thank for their very active collaboration:Shota Vardanyan
Nazareth MnatsakanyanPetros Semerjyan
Alexander BazarchyanArshak PapoyanArtur Minasyan
Anaida PapikyanKamila Petrosyan
Lena TerzikyanKristine Khurshudyan
Artur AndreasyanYuri Avetisyan
Grigor Grigoryan
As well as Drug Information/Epidemiolgy International Expertof the South Caucasus Anti Drug Programme
Tomas Zabransky
Yerevan 2009

2 3
National Report 2008
Call for contributions and commentsEveryone interested in contributing to the next Report on Drugs or commenting to the present one can contact South Caucasus Anti Drug Programme or Monitoring Center on Drugs and Drug Addiction.14 Petros Adamyan str, Yerevan, Armenia, 0010
Tel: + 374 10 546731Email: [email protected], or [email protected]
All comments are welcome
Introduction
National Drug Report summarizes the information on drug use prevalence, trends and patterns, its consequences, legislative framework, national strategies and policies in the field of drugs, situation in the field of drug related crime, harm reduction interventions, prevention of the drug use, treatment. The report was developed in accordance to the guidelines of the European Center on Drug and Drug Addiction (EMCDDA). This report is the forth report of its type that is presenting drug related situation in Armenia and as three previous reports is prepared with the assistance of EU funded, UNDP implemented South Caucasus Anti Drug Programme.
4 5
National Report 2008
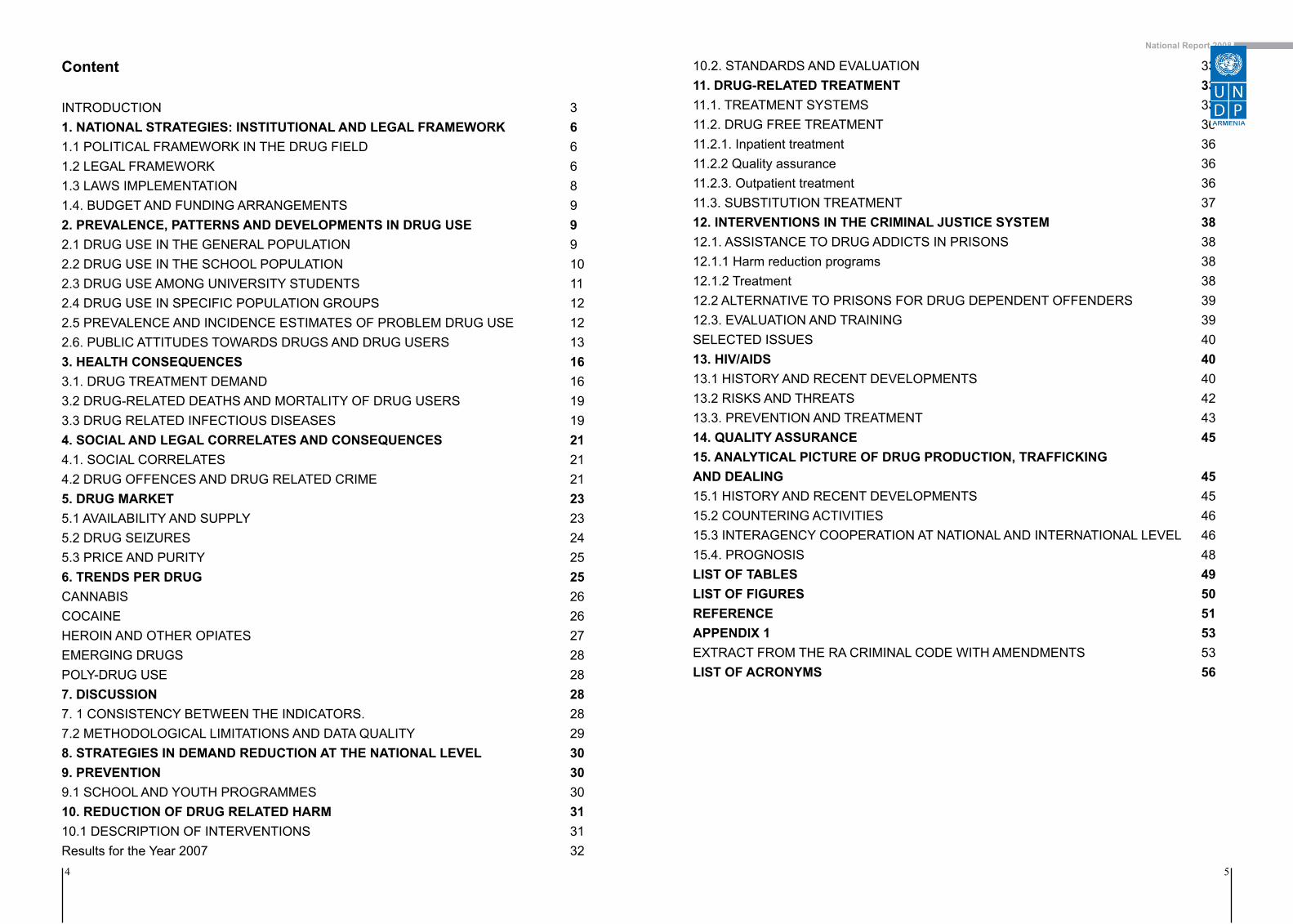
Content
INTRODUCTION 31. NATIONAL STRATEGIES: INSTITUTIONAL AND LEGAL FRAMEWORK 61.1 POLITICAL FRAMEWORK IN THE DRUG FIELD 61.2 LEGAL FRAMEWORK 61.3 LAWS IMPLEMENTATION 81.4. BUDGET AND FUNDING ARRANGEMENTS 92. PREVALENCE, PATTERNS AND DEVELOPMENTS IN DRUG USE 92.1 DRUG USE IN THE GENERAL POPULATION 92.2 DRUG USE IN THE SCHOOL POPULATION 102.3 DRUG USE AMONG UNIVERSITY STUDENTS 112.4 DRUG USE IN SPECIFIC POPULATION GROUPS 122.5 PREVALENCE AND INCIDENCE ESTIMATES OF PROBLEM DRUG USE 122.6. PUBLIC ATTITUDES TOWARDS DRUGS AND DRUG USERS 133. HEALTH CONSEQUENCES 163.1. DRUG TREATMENT DEMAND 163.2 DRUG-RELATED DEATHS AND MORTALITY OF DRUG USERS 193.3 DRUG RELATED INFECTIOUS DISEASES 194. SOCIAL AND LEGAL CORRELATES AND CONSEQUENCES 214.1. SOCIAL CORRELATES 214.2 DRUG OFFENCES AND DRUG RELATED CRIME 215. DRUG MARKET 235.1 AVAILABILITY AND SUPPLY 235.2 DRUG SEIZURES 245.3 PRICE AND PURITY 256. TRENDS PER DRUG 25CANNABIS 26COCAINE 26HEROIN AND OTHER OPIATES 27EMERGING DRUGS 28POLY-DRUG USE 287. DISCUSSION 287. 1 CONSISTENCY BETWEEN THE INDICATORS. 287.2 METHODOLOGICAL LIMITATIONS AND DATA QUALITY 298. STRATEGIES IN DEMAND REDUCTION AT THE NATIONAL LEVEL 309. PREVENTION 309.1 SCHOOL AND YOUTH PROGRAMMES 3010. REDUCTION OF DRUG RELATED HARM 3110.1 DESCRIPTION OF INTERVENTIONS 31Results for the Year 2007 32
10.2. STANDARDS AND EVALUATION 3311. DRUG-RELATED TREATMENT 3311.1. TREATMENT SYSTEMS 3311.2. DRUG FREE TREATMENT 3611.2.1. Inpatient treatment 3611.2.2 Quality assurance 3611.2.3. Outpatient treatment 3611.3. SUBSTITUTION TREATMENT 3712. INTERVENTIONS IN THE CRIMINAL JUSTICE SYSTEM 3812.1. ASSISTANCE TO DRUG ADDICTS IN PRISONS 3812.1.1 Harm reduction programs 3812.1.2 Treatment 3812.2 ALTERNATIVE TO PRISONS FOR DRUG DEPENDENT OFFENDERS 3912.3. EVALUATION AND TRAINING 39SELECTED ISSUES 4013. HIV/AIDS 4013.1 HISTORY AND RECENT DEVELOPMENTS 4013.2 RISKS AND THREATS 4213.3. PREVENTION AND TREATMENT 4314. QUALITY ASSURANCE 4515. ANALYTICAL PICTURE OF DRUG PRODUCTION, TRAFFICKING AND DEALING 4515.1 HISTORY AND RECENT DEVELOPMENTS 4515.2 COUNTERING ACTIVITIES 4615.3 INTERAGENCY COOPERATION AT NATIONAL AND INTERNATIONAL LEVEL 4615.4. PROGNOSIS 48LIST OF TABLES 49LIST OF FIGURES 50REFERENCE 51APPENDIX 1 53EXTRACT FROM THE RA CRIMINAL CODE WITH AMENDMENTS 53LIST OF ACRONYMS 56

6 7
National Report 2008
1. National Strategies: Institutional and Legal Framework
1.1 Political framework in the drug field
The Constitution of the Republic of Armenia provides guarantees for fundamental civil and human rights and freedoms. According to the Article 38 of the Constitution, “Everyone shall have the right to benefit from medical aid and service under the conditions prescribed by the law. Everyone shall have the right to free of charge benefit from basic medical aid and services. The list and the procedure of the services shall be prescribed by the law”.
Article 48 of the Constitution declares that one of the basic tasks of the state in the economic, social and cultural spheres is to implement health care programs for the population and contribute to the effective and affordable medical service for the population.
Article 16 of the Constitution of the Republic of Armenia, which guarantees the right to liberty and security for everyone, sets that a person can be deprived of or restricted in his/her liberty by the procedure defined by the law and when necessary to prevent social dangers posed by persons addicted to drugs.The provisions of the state policy in the field of prevention of illicit trafficking of drugs and psychotropic substances are defined in the Law “On Drugs and Psychotropic Substances” of the Republic of Armenia. This law regulates the issues in the area of control of narcotic drugs and psychotropic substances, as well as establishes legal grounds for the national policy to combat illicit trafficking of drugs and drug abuse. It also sets main measures to combat drug addiction for the purposes of protection of the health of citizens, the state security and the society at large.
The state policy has undergone substantial changes in the field of combating the trafficking of illicit drugs and drug abuse by shifting severe punitive approaches of the Soviet era into the more modern and internationally recognized liberal and balanced principles. This policy primarily concerns to the state control over the licit circulation of drugs and psychotropic substances, the routine prevention of drug abuse and drug-related crime, efficient law enforcement involving prosecution of drug related crimes, as well as the state support for the development and introduction of innovative methods of drug treatment and expanding the drug rehabilitation network for providing the continuum care services to drug addicts.
The provisions of the drug control legislation in Armenia can be characterized as repressive, since it prohibits not only the sale, but also consumption of narcotics and the possession of drugs regardless the purpose. As a consequence, drug users are reluctant to seek for the assistance from health facilities without a fear that they will be turned over to the law enforcement authorities and be denied in health care. Moreover, under the Article 49.4 of the RA Law on “Narcotic Drugs and Psychotropic Substances”, immediate (mandatory, compulsory) medical assistance shall be provided to the person suffering from drug addiction, if he/she without the doctor’s prescription, permanently uses narcotic drugs and psychotropic substances, who has acquired an unrecoverable physiological or psychological dependency, as a result of medical examination has received the diagnosis of “Drug addiction” and is not able, even temporarily, without any medical intervention, to overcome the physiological, psychological dependency from the narcotic drugs and psychotropic substances.
1.2 Legal Framework
The Republic of Armenia is a signatory of the three main international drug control conventions:• The United Nations Single Convention on Narcotic Drugs (1961);• The United Nations Convention on Psychotropic Substances (1971);• The United Nations Convention Against Illicit Trafficking in Narcotic Drugs and Psychotropic Substances (1988)
Additionally, the Republic of Armenia ratified the United Nations Convention against Transnational Organized Crime (2000). The provisions of the above-mentioned conventions and their supplementary
lists of narcotic drugs, psychotropic substances and precursors have been incorporated into the Armenian national legislation.
Armenia has adopted the following main drug-related legal acts:
• The Law of the Republic of Armenia “On Narcotic Drugs and Psychotropic Substances” (2002);• The Criminal Code of the Republic of Armenia (2003);• The Code on Administrative Offences of the Republic of Armenia (1985);• The Decision of the Government of Republic of Armenia “ On creating Standing Commission on Drug Control in the Republic of Armenia” (2000);• The Decision of the Government of Republic of Armenia “On approving the charter of the Standing Commission on Drug Control in the Republic of Armenia” (2001);• The Decision of the Government of the Republic of Armenia “ On approving the List of Narcotic Drugs, Psychotropic Substances and their Precursors under the Control on the Territory of Armenia” (2003);• The Decision of the Government of the Republic of Armenia “On Creating Interdepartmental Commission for the Regulation of Trafficking in Drugs and Psychotropic Substances and for the Prevention of Illegal Trafficking of those in the Republic of Armenia” (2003).• The Decision of the Government of Republic of Armenia “On approving the procedures of the Interdepartmental Commission for the Regulation of Trafficking in Drugs and Psychotropic Substances and for the Prevention of Illegal Trafficking of those in the Republic of Armenia (2004)”.
According to the Article 1 of the above mentioned Law, the processes that ensure licit turnover and prohibits illicit traffic of narcotic drugs and psychotropic substances in the territory of the Republic of Armenia shall be duly regulated.
No changes were made to the Law “On Narcotic Drugs and Psychotropic Substances” in 2007. However, the elaboration of a Draft Law “On making amendments and alterations to the Law on narcotic drugs and psychotropic substances” of the Republic of Armenia was commenced in fall of 2007.
The following provisions have been clarified in accordance with the Draft Law: (i) clarifications of definitions; (ii) elimination of the terminological discrepancies in the legal language throughout the law, so to align it with other laws of the Republic of Armenia; (iii) recognition of the drug treatment as an authorized care by the assignment of the Ministry of Health; (iv) streamlining of the functions and responsibilities of those bodies who may be authorized to carry out forensic examinations by using narcotic drugs and psychotropic substances, as well as other activities directly linked to those examinations without a license. The South Caucasus Anti Drug Programme’s (SCAD) ongoing support to the Government of Armenia in the area of drug control has triggered the elaboration of the draft Laws “On making amendments and alterations to the Code of the Republic of Armenia on Administrative Offences” and “On making amendments and alterations to the Criminal Code of the Republic of Armenia”. The latter is the main document stipulating the grounds for criminal liability and the principles of criminal legislation, and determines the category of criminal offence which may badly affect the society. The Code establishes the sanctions for the committed criminal acts, as well as suggests other penal and legal measures. According to the above mentioned draft Laws suggested by the Office of Prosecutor General, RA, the usage of narcotic drugs without doctor’s prescription should be decriminalized, and the relevant Article 271 of the Criminal Code of Armenia should be abolished. The Draft Law “On making amendments and alterations to the Code of the Republic of Armenia on Administrative Offenses” sets administrative liability for the use of narcotic drugs or psychotropic substances without doctor’s prescription, as well as for the illegal turnover of narcotic drugs or psychotropic substances in small quantities without a purpose of sale. According to the proposal, the administrative sanction for use of narcotic drugs or psychotropic substances should be an administrative fine in an amount of 100 to 200 times of the minimum wage, for the first time of detection of drug use

8 9
National Report 2008
and of 200 to 400 times of the minimum wage for the second time of detection. The administrative sanction for illegal turnover of narcotic drugs or psychotropic substances in small quantities without a purpose of sale results in an administrative fine in an amount of 200 to 400 times of the minimum wage, for the first time of detection of drug use and of 400 to 800 times of the minimum wage for the second time of detection.
In 2007, number of important drug related regulations were adopted. Namely, on December 20, 2007 the Government of Armenia adopted the decision “On setting the procedure of medical observation and registration of drug users”, which essentially maintained the treatment of drug related disorders in the country (see the chapter 11 Drug-Related Treatment).
On March 1, 2007, the “National Programme on the Response to the HIV Epidemic” was ratified by the Decree N 378 of the Government of the Republic of Armenia. Among other activities envisaged in the National Programme, it includes special activities to be implemented among the IDUs, namely implementation of HIV prevention and harm reduction programmes, provision of support for setting up a network of organizations implementing HIV prevention projects among IDUs, introduction of opioid substitution treatment for HIV infected IDUs, organization of workshops for narcologists, reducing the stigma and discrimination of marginalized population, etc. The Decree of the Minister of Health of the Republic of Armenia “On defining the small, large and extra large quantities of narcotic drugs and psychotropic substances”1 (January 19, 2007) has played a significant role for regulating the drug control area. 1.3 Laws implementation
During the reporting period, the use of narcotic drugs without a doctor’s prescription remained punishable with a fine in the amount of up to 200 minimum monthly wages2 or with arrest for a term of up to 2 months according to the article 271 of the Criminal Code of the Republic of Armenia. A person surrendering the drugs of his/her own initiative is exempted from criminal liability.
According to the provisions of the Article 266 (see Appendix 1: Extract from the Criminal Code with amendments and alterations) the maximum term of imprisonment is 3-7 years for the committed crime connected with the illicit circulation of drugs, psychotropic substances with the purpose of sale or their illegal sale, whereas the Article 268 stipulates the maximum term of arrest for up to two months, or the imprisonment for up to 1 year for the same committed offence without purpose of sale of considerable quantities of drugs and psychotropic substances.
No criminal sanction in the form of imprisonment was imposed for the first time offence by the previous Criminal Code which was effective till August 1, 2003. If the crime was repeated within a year, then the penalty sanction(s) had to apply. The new Criminal Code which entered into the force on August 1, 2003 criminalized drug use from the very first offence. However taking into consideration the best practices of the EU countries and some of the recommendations of international experts, new draft laws are underway of development, which suggest the decriminalization of drug use (see Chapter 1.1 Political framework in the drug field above). As mentioned above, according to these draft Laws, the use of narcotic drugs without a doctor’s prescription should be decriminalized in Armenia and an administrative liability has to be set for that offence. It is also envisaged to create a legal basis for promoting the drug substitution treatment and supporting the continuum of care.
1.4. Budget and funding arrangements
The structure of state budget does not allow to properly analyze the resources used for drug control activities either at the level of individual ministries or within the government at large. The separate budget line within the health care budget assigns explicit costs to provide narcological care. According to the Medium-term Expenditure Framework the amount of state allocated funds for narcological care is 102.7 million AMD (about 233400 EUR), which is by 22.3 million AMD (about 50700 EUR) more than in 2006. Some drug related activities were supported by the EU funded and UNDP implemented South Caucasus Anti Drug Programme, as well as the Global Fund to Fight AIDS, Tuberculosis and Malaria.
2. Prevalence, Patterns and Developments in Drug use
No General Population Surveys (GPS) were implemented in Armenia in 2007. The below chart summarizes key finding of the drug use surveys among general population and youth implemented in Armenia during the previous years.
2.1 Drug Use in the General Population
The most recent general population survey on prevalence of drugs, alcohol and tobacco was conducted in 2005, which was the first study of its kind among the Commonwealth Independent States (CIS). The European Model Questionnaire (EMCDDA 2002) was used for the survey, which was adjusted to the Armenian cultural context. The survey, which covered 3892 people in all Marzes (provinces) of Armenia, was designed to study the situation regarding the prevalence of the use of illicit drugs and non-lege artis use of psychotropic pharmaceuticals, alcohol and tobacco, the attitude of the people towards tobacco smoking, alcohol drinking, taking psychotropic pharmaceuticals and using illegal drugs, as well as their perception of the nature of drug users.
Two types of questions were included in the questionnaire for assessing drug use prevalence among the general population. The first type of questions assessed the personal history of drug use (“Have you ever used drugs?”) , while the second type of questions relates knowing other people using drugs (“Do you know somebody close to you using drugs?”).The number of positive answers for the first type of questions was insignificant for any type of drug, while survey revealed relatively high percentage of people who reported to know others using cannabis type drugs (5.4%), and 0.9% for those using cocaine and 0.6% heroin (Gyurjyan and Bazarchyan 2005).
Figure 1: GPP Respondents knowing others using drugs (as % of total)
1. The decree of the Minister of Health of the Republic of Armenia is not in force yet, since the quantities of narcotic drugs and psychotropic substances are set in Criminal Code of the Republic of Armenia and in the Code of the Republic of Armenia on Administrative Offences, according to the article 9 of the Law “On Legal Acts” and the article 83.5 of the Constitution of the Republic of Armenia. 2. According to the Article 3 of the RoA the Law “On Minimum Monthly Wages”, the bases for calculating minimum monthly wage within the RA Codes, laws and substitute acts is 1000 Armenian drams.

10 11
National Report 2008
Figure 2: Distribution of persons taking sedatives and tranquillizers by frequency of use and area of residence
However, according to the experts opinion, this study did not include in questionnaire “Chernyashka” or “Koknar” as separate substance of abuse that are considered to be the most commonly used drug in Armenia. Additionally, some inconsistencies in the obtained estimates related to the problem drug use indicate either limited adaptability of European Model Questionnaire in the cultural context of South Caucasus, or need for more elaborated process of its adjustments with more piloting and testing (Asriyan and Zábranský 2006).
2.2 Drug Use in the School Population
In 2005, a pilot European School Survey Project on Alcohol and Drugs (ESPAD) was conducted in Syunik Marz of Armenia by the Non Governmental Organization (NGO) “AIDS Prevention, Education and Care” (APEC). The survey sample targeted 1202 schoolchildren aged 15-16 years. According to the results of the survey, 2.7% of surveyed schoolchildren reported lifetime marijuana use, 0.9% ever used drugs other than marijuana, 17.1% ever used inhalants/sedatives and 0.4% used alcohol with pills (AIDS Prevention Education and Care 2005).
In 2007, survey on Health Behaviour in School-aged Children (HBSC) was conducted in 60 high schools, including 20 schools in the capital city of Yerevan, 20 schools in cities and 20 schools located in villages. In total 1206 schoolchildren aged 12-17 were interviewed. The survey assessed general health status, eating habits, physical activity, tobacco, alcohol and drug use, mental health, behaviour, life skills, sexual health and knowledge on HIV/AIDS.
Survey results show that 2.4% of respondents state that they have ever tried drugs, of which 0.9% are girls and 4.9% are boys. However, 10% of boys and 20% of girls did not respond, which may indicate the fear or shame surrounding drug use. Therefore, the very small percentage of those who responded that they had experimented drugs may reflect only a portion of the total drug using population.
Significantly fewer young people from rural areas reported having tried drugs. However, as with young people from urban areas, those in rural locations often refused to respond, with a higher rate of non-respondent females than males, leaving a room for further investigation into the nature of drug use experience. The survey indicated that drug use among Armenian students is significantly lower than among their European peers. However it is difficult to draw a scientific conclusion based on report results due to the high number of non-respondents (Babloyan, Sargsyan et al. 2007).
Table 1: Drug use experience by gender, 2007
Have you ever tried drugs?
Boys Girls
Absolute number Percent (%) Absolute number Percent (%)
Yes 22 4,9 7 0,9
No 378 84,4 596 78,5
No response 48 10,7 155 20,6
Total 448 758
Table 2: Drug use experience by region type, 2007
Have you ever tried drugs?
Capital city Urban Rural
Absolute number
Percent (%)Absolute number
Percent (%)Absolute number
Percent (%)
Yes 13 3 9 2,4 7 1,8
No 366 84,1 322 85,9 285 72,1
No response 56 12,9 44 11,7 103 26,1
Total 435 375 395
Nationwide representative ESPAD survey was conducted in Armenia in 2007, but the results of the survey were not available by the time this report was submitted for publication.
2.3 Drug Use among University Students
In 2003, South Caucasus Anti-Drug Programme has commissioned epidemiologic study to assess drug use prevalence among Armenian students. The survey was targeted at 497 university students (353 males and 144 females). More specific aim of the study was to obtain comparable, reliable information on the extent and patterns of drug use among students and the characteristics and behaviours of users (Harutyunyan 2004).
The rates for different patterns of use of different drugs among those who have reported life time drug use experience are presented in the Table 3.
Table 3: Last month prevalence of drug use among Armenian students (%)
Type of Drug Life time
prevalence
Last year prevalence (percents shown for
those who reported life-time use)
Last month prevalence (percents shown for
those who reported life-time use)
Marijuana or hashish 19,4 71,9 45,8
Ecstasy 3,6 94,4 33,3
Amphetamines 2,8 78,6 57,1
Cocaine 3,2 68,8 25
Heroin 1,4 85,7 57,1
LSD 1 60 40
The survey also asked the question, if the study respondents personally know people using certain type of drugs.

12 13
National Report 2008
Figure 3: Students’ Survey (SS) respondents knowing others using drugs (as % of total)
2.4 Drug use in specific population groups
An anonymous survey on infectious diseases and related risk behaviour among Armenian prison population and the prison staff was carried out in Armenia in 2004 (Weilandt, Ecker et al. 2005). The study was conducted in a representative sample of seven prisons (including the Hospital for Detainees) using structured quantitative questionnaires for prisoners and members of the staff and conducting anonymous saliva tests on HIV and viral hepatitis (Willing anonymous salivary HIV and hepatitis - WASH surveillance) for prisoners. Altogether, 542 of 556 eligible prisoners (97.4%) completed the questionnaires and gave a saliva sample. 348 members of the actual prison staff of 483 (72.0%) were interviewed.
The results of the survey showed that 27.2% of the study population used cannabis before imprisonment, 4.2% continued to use cannabis inside prison and 3.2% started to use cannabis in prison. According to the survey, heroine use and use of “chimia” (self prepared mixtures -“koknar”, “chernyashka” or “solutan”) was common for the prison population: 12.3% of the study population stated that they used heroine/opiates before imprisonment and the same percentage mentioned the use of self prepared mixtures (“chimia”) before imprisonment. There is a substantial overlap of heroine and “chimia” use: 86% of the prisoners that ever used (inside or outside prison) heroine also stated “chimia” use and 79% of the “chimia” users also stated heroine use. The proportion of prisoners who reported lifetime prevalence of injecting drug use (ever injected drugs) was 13.3%.
2.5 Prevalence and incidence estimates of problem drug use
Problem drug use is defined by EMCDDA as ‘injecting drug use or long duration/regular use of opioids, cocaine and/or amphetamines”.
Epidemiological and statistical data on problem drug use in Armenia is lacking. Estimating the actual extent of problem drug use (injecting drug use) is problematic because of the stigmatization and criminalization of drug use in the country.
The operative data of the Ministry of the Interior of Armenia3 indicate that the number of drug users (last month use of any illegal drugs including cannabinoids and non-medical use of psychotropic pharmaceuticals) was estimated (based on expert opinion of the operative analysts) to be 20,000 individuals in the country in 2000 (50% of them residing in the capital city Yerevan), of whom 2,000 were estimated to be injecting drug users. However, the “Rapid Assessment of the Situation on Spread of Injecting Drug Use and HIV Infection in
Yerevan, Armenia” found higher rates of opioids use in the general population of Armenia. According to the survey, in Yerevan alone, there were between 19,000 and 23,000 drug users who reported drug use during the last year, and of whom approximately 10% were injecting drug users (Grigoryan, Bussel et al. 2002).
Finally, the World Health Organization (WHO) EURO databases4 estimated the number of injecting drug users, in Armenia, between 7,000 and 11,000 in 2004 (WHO Regional Office for Europe, UNAIDS et al. 2006).
2.6. Public Attitudes towards Drugs and Drug Users
The public attitudes towards drugs were assessed in the General Population Survey conducted in 2005. The survey results indicate that the attitude of general public towards drug addicts is more vectored to consider the person afflicted with a disease. The response to the question “Do you regard a drug addict more as criminal, than as afflicted with a disease?” was as follows: the majority of the respondents (68.1%) were inclined to regard a drug addict as diseased, whereas a part of those people (29.8%) regard a drug addict both as a criminal and diseased, and every tenth person regards such person more as a criminal; about 14% of survey respondents failed to give any definite answer.
Figure 4: GPS participants’ response to the statement: ”Do you regard a drug addict more as criminal, than as afflicted with a disease?”
The survey also assessed the respondents’ attitude to the statement “People should be allowed to use hashish or marijuana”; the vast majority of the survey respondents have rejected the legalization of the hashish or marijuana use (67.1 % fully disagree, and 25.3% largely disagree).
3. Since 1 January 2003, the Ministry of the Interior of the Republic of Armenia was restructured into the Police of the Republic of Armenia.
4. WHO Regional Office for Europe and UNAIDS, WHO EURO Data Collection, Joint workshop of WHO European Office for Europe and UNAIDS (Geneva 2003): “Data in the WHO EURO databases are drawn mainly from national sources, and are generated by national surveillance, service providers, and NGOs, or by such international organiza-tions as the UN Reference Group on Injecting Drug Users. Where no published or official data are available, preliminary estimates made by national experts during a workshop on estimating and modeling the HIV/AIDS epidemic in Europe are used.”

14 15
National Report 2008
Figure 5: GPS participants’ response to the statement: “People should be allowed to use hashish or marijuana”
The similar picture was found with the opinions on the statement: “People should be allowed to use heroin”. Such statement was rejected largely or fully by 93.3% of the respondents (23.4% and 69.9%, respectively). It was noted that the breakdown of the opinions “do not agree fully” and “do not agree largely” had some specific distinctions probably based on the gender and cultural differences: the percentage of answers given by women who “do not agree fully” prevailed over the answers of men with that opinion by 10.3%, and as for the percentage of answers by the women who “do not agree largely,” they are less than the men’s answers by 6.4%. Similar differences are also typical for Yerevan and the Marzes (“regions” in Armenian): the percentage of answers “do not agree fully” was higher in Yerevan than in the Marzes by 11.0%, while the percentage of the other answer “do not agree largely” was the opposite: in Yerevan it was less than in the Marzes by 7.3%. Interestingly, in Yerevan there were no answers “fully agree”.
The same picture was in the breakdown of the opinions on “Trying of heroin or marijuana once or twice”. It was disapproved by 80.2% of the respondents, and 3.1% did not disapprove. The answers of respondents to the statement “Trying heroin once or twice” are given in the Figure 6, below.
Figure 6: GPS respondent’s attitude to the question “Trying heroin once or twice”
According to the answers, the percentage of the respondents not disapproving trying heroin once or twice were relatively high among men (higher than the women’s percentage by 2.7%), as for the Marzes,
the percentage of such answers given in Yerevan was higher than in Marzes by 4%.
In the frame of the drug use prevalence survey among the students of the higher educational institutions of the Republic of Armenia, the student’s attitude towards the drugs and drug users were also assessed. About 5.6% of the surveyed students perceive a drug addict more as a criminal and 49.2% - more as a patient (Figure 7).
Figure 7: Response of SS participants on the statement:”Do you regard a drug addict more as criminal, than as afflicted with a disease?”
8.2% of those surveyed fully agree with the following statement: “People should be permitted to take hashish or marijuana”, 65.7% fully disagree with this statement (Figure 8).
Figure 8: Response of SS participants on the statement: “People should be allowed to use hashish or marijuana”
30.7% of those surveyed would tolerate people trying heroin once or twice, while 46.6% disapprove that. 25.5% of the surveyed students tolerate the ecstasy try once or twice, while 59.4% disapprove that. 31.9% of those surveyed agree that the people should be allowed smoke marijuana or hashish occasionally, while 43.9% disapprove that.
Compared to the similar survey among university students in EU and US (Danseco, Kingery et al. 1999) the level of perceived risk of cannabinoids use is relatively high (Figure 9).

16 17
National Report 2008
Figure 9: SS Respondent’s attitude to the question: “Smoking marijuana or hashish regularly…”
3. Health Consequences
3.1. Drug Treatment Demand
Medical institutions entitled for the provision of medical treatment to drug addicts are running treatment, dispensary control and prophylactic (preventive) registers, that are paper based databases. The treatment register contains the information about all patients receiving inpatient treatment; the prophylactic database contains information on the people who were tested positive for the presence of drugs. People are included into the dispensary register, if the dependency syndrome has been diagnosed by a clinician in the following circumstances:
• During the first admission for treatment to narcologist;• In-patient treatment at the Narcological Clinic (not applied if the treatment was anonymous);• On the basis of the diagnosis made by forensic-narcological expertise commission;• On the basis of the data of the conclusion of toxico-chemical expertise analyses;• Epicrisis and referrals of medical institutions and ambulances other than narcological services;• Data received from the Criminal-Executive (penitentiary) institutions;• The minimal period for dispensary observation is 5 years.
The regional institutions are submitting their annual reports to the Narcological Clinic in Yerevan, which then sends the cumulative treatment demand data to the Information-Analytic Center of the Ministry of Health on the number of patients registered at the dispensary register in the Republic of Armenia by the end of the year, incidence of alcohol psychosis, chronic alcoholism, and number of drug addicted patients admitted for the inpatient treatment.
The new developments in drug treatment system contributed to certain increase in drug treatment admission rate; however treatment demand still remains very low.
The number of patients admitted for treatment sharply increased over the last three years (2005-7). In 2007, 166 opiate addicted patients underwent detoxification, which is the major treatment modality in Armenia5: 122 at in-patient and 44 at out-patient department. The medical personnel explains this positive trend with an overall increase of the number of IDUs in the country and improvement of quality services thanks to the newly established Department of Intensive Narcology nicely refurbished and equipped by the cost share of EU funded SCAD-IV programme and the Ministry of Health.
However, according to the expert opinion only one out of twenty drug addicts are applying for treatment (Semerjyan 2007).
Table 4: Number of patients received inpatient treatment in the Narcological Clinic (NC), Yerevan
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007DiagnosisChronic alcoholism 901 774 774 716 639 637 719 881 920 925 1058
Drug addiction 16 17 27 28 12 7 17 21 96 104 122
Table 5: Newly registered cases of alcohol psychosis, chronic alcoholism, drug use by years.
1980
1985
1990
1995
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Alcohol psychosis
Absolute number
82 28 29 49 34 34 52 62 55 41 55 62 61 38
Per 10000 population
2.6 0.8 0.8 1.3 0.9 0.9 1.37 1.63 1.7 1.3 1.7 1.9 1.9 1.2
Chronic alcoholism
Absolute number
770 588 402 401 238 200 195 175 165 171 308 354 412 421
Per 10000 population
24.8 17.6 11.3 10.7 6.3 5.3 5.1 4.6 5.1 5.3 9.6 11.0 12.8 13.0
Drug addictionAbsolute number
20 35 77 41 13 11 8 10 7 16 8 53 93 79
Per 10000 population
24.8 17.6 11.3 10.7 0.3 0.28 0.21 0.26 0.22 0.5 0.2 1.6 2.9 2.4
In In 2005, the full-scale Pompidou Group questionnaire based electronic register was introduced in the Narcological Clinic, which is the main provider of medical treatment of drug addiction in Armenia. However there are some discrepancies between published data of Information-Analytic Center of the National Institute of Health (which is based on the information of paper based treatment register) and the data of the Pompidou Group based electronic register of the Narcological Clinic. These discrepancies can be explained by the fact, that there is no obligatory regulation to enter the data on all patients into the electronic database, while there is a strict regulation to keep information on all patients in paper-based format. In a given context the data of the paper based treatment register can be considered as most accurate which reflects the real situation with regards to drug treatment in the country, but the paper-based format of the register did not allow using it for analyzing drug use patterns in Armenia. In this section analyzes of the drug use patterns, characteristics of drug users are based on the data of the electronic database.
In 2007, 83 drug addicts (1 woman and 82 men) were registered in the electronic database of the Narcological Clinic; while according to the official data 122 patients received the treatment in 2007, of which 79 were treated for the first time in their lives. The mean age of patient admitted for treatment was 35 years. The majority of treated drug users, (53.0%) reported the use of “chernyashka” (dark colored solution made of fresh poppy bulbs or poppy straw).
5. for further details, see chapter 11.2. Drug Free Treatment below

18 19
National Report 2008
Table 6: Main drug of use of patients admitted for drug treatment, 2007
All treatment demand First treatment demand
Main drug of use Frequency Percent Frequency Percent
Cannabis 1 1.2% 1 1.8%
“Chernyashka” 44 53.0% 32 56.1%
Ephedrine 1 1.2% 1 1.8%
Heroin 15 18.1% 10 17.5%
Opioids other than “chernyashka”
22 26.5% 13 22.8%
The first treatment demand rate in 2007 was 68.7%, 27.7% of patients have applied for the treatment to the Narcological Clinic earlier and 3.6% to other medical centers. Most of the treatment demand was related to the use of “chernyashka” representing 56.1% of all first demands for treatment.
Table 7: Drug use patterns of patients getting inpatient treatment at Narcological Clinic, 2007
All treatment demand First treatment demand
Drug use patterns Frequency Percent Frequency Percent
Injecting drug use 78 94.0% 53 93.0%
Smoking of drugs 1 1.2% 1 1.8%
Inhaling 4 4.8% 3 5.3%
Figure 10: First treatment demand and number of patients registered at narcological register of Narcological Clinic by years, 2005-2007
There is no any solid information about the extent of the phenomenon of “wild detoxification” conducted outside medical institution, so it is impossible to make a projection on the real estimates on the treatment demand. So called “wild detoxification” is mostly common for the provinces of Armenia, where people are afraid to disclose their IDU status.
3.2 Drug-related deaths and mortality of drug users
The National Statistical Service collates information on deaths in the population from the Ministry of Health and the Police, but no specific data on drug related mortality is available in the reports.
The “Scientific Practical Medical Center” CJSC of the Ministry of Health (Forensic Center of the Medical Expertise) is the only agency maintaining the official statistics on drug-related deaths in Armenia. These data are based on the results of forensic examinations and toxicological analysis. According to the Forensic Center, 2 cases of positive finding of drugs or their metabolites were detected by toxicology laboratory during the autopsy (death in the presence of drug) in 2007. In the period of 2004-07, 16 positive findings on drugs and/or metabolites were identified with the mean age at death 34.4. Morphine derivates were detected in 87.5% of all cases of positive findings in the body liquids and/or tissues.
Figure 11 Reported positive finding of drugs or their metabolites (death in the presence of drugs), 2004-2007
3.3 Drug related infectious diseases
The morbidity rates of viral hepatitis B among the general population have been decreased starting from 1990 and become stable, between 3.2 (in 2000) and 2.6 (in 2007) per 100,000 inhabitants. In 2007, 85 cases of VHB were registered in Armenia.
Table 8: Number of newly registered cases of Hepatitis B and HIV among population of Armenia, e in 1990-2007
1990 1995 1999 2000 2001 2002 2003 2004 2005 2006 2007
Viral hepatitis BAbsolute number
793 360 229 122 122 111 103 106 86 91 85
Per 100000 population
22.3 9.6 6.0 3.2 3.2 3.5 3.2 3.3 2.7 2.8 2.6
HIV
Absolute number
0 0 35 14 28 41 29 49 75 66 109
Per 100000 population
0 0 0.92 0.37 0.73 1.28 0.9 1.5 2.33 2.05 3.38
In Armenia, Hepatitis C is not in a list of reportable infectious diseases under the surveillance, thus, no official published statistics on viral hepatitis C is available in the country. According to a recent

20 21
National Report 2008
publication HCV infection in Europe, in 2006 there were registered 71 cases of acute Hepatitis C (Merkinaite 2007).
HIV has been growing steadily since the time of its first registration. In 2007 there were 416 people living with HIV and AIDS (PLWHA) while the number of newly diagnosed cases of HIV was 109.
Figure 12: Number of PLWHA and newly diagnosed HIV
AIDS diagnosis was made to 210 patients with HIV, of whom 40 were women and 6 were children. 59 AIDS cases were registered during 2007 and from the beginning of the epidemic 122 death cases had been registered among HIV/AIDS patients (including 19 women and 3 children). Hepatitis C co-infection was diagnosed among 86 out of 129 tested HIV carriers.
Figure 13: Distribution of HIV, AIDS and death cases by years
The results of the Anonymous Survey on Infectious Diseases and Related Risk Behavior among Armenian Prisoners indicated that compared with the HIV prevalence rate in the general population, the rate in prison (2.4%) was 27 times higher (Weilandt, Ecker et al. 2005). As regards to Hepatitis C, the study indicated that the prevalence rate in prison was 23.8%. The most important risk factor for contacting Hepatitis C infection in the study population was injecting drug use followed by the time spent in prison within the last 10 years, which was an independent risk factor in the anonymous study.
The study on Hepatitis C conducted by the Research Institute of Epidemiology, Virology and Medical Parasitology estimated the prevalence of Hepatitis C in the general population of Armenia at about 7% (Melik-Andreasyan 2004).
4. Social and Legal Correlates and Consequences
4.1. Social correlates
No studies focusing specifically on drug-related social consequences have been ever conducted in Armenia. However, limited data on social consequences and correlates are available from treatment centers and police. Social problems and marginalization are the most common associates of drug use in Armenia. Social problems include dist urbed family relations, unemployment, stigmatization and low socio-economic status.
4.2 Drug offences and drug related crime
According to the official data of the Police of RA, 1084 cases of drug related crimes (Articles 266-274 of the Criminal Code of RA) and 6 cases of drug related administrative offences had been reported in 2007, whereas in 2004 this number was 411.
Figure 14: Drug related crime and drug related offences 2004-2007
Out of 1084 cases 643 were related to the illegal turnover of narcotic drugs and psychotropic substances including, 408 cases related to illegal turnover without purpose of sale (Article 268 of the Criminal Code of RA) and 235 cases referred to illegal turnover for the purpose of sale (Article 266 of the Criminal Code of RA); (Police of RA 2007). For more details about the activities covered by individual paragraphs see Appendix 1.

22 23
National Report 2008
Table 9: Identified drug related crimes and offences by regional police stations
Police StationsDrug related crime Drug related offences
2006 2007 2006 2007Yerevan 548 611 0 0
Aragatsotn 21 21 0 0
Ararat 71 98 0 0
Armavir 59 63 0 0
Gegharkunik 18 27 0 0
Lori 45 53 1 0
Kotayq 69 51 0 0
Shirak 46 65 0 0
Syunik 43 55 0 0
Vayots Dzor 14 5 15 6
Tavush 9 9 0 0
Road Police 14 24 0 0
Zvartnots Airport 0 2 0 0
Drug Squad 203 246 0 0
Total in Armenia 957 1084 16 6
Table 10: Drug related crime and offences by the articles of the RA Criminal Code
Articles of the Criminal Code of the Republic of Armenia
2006 2007
Articles 266, 268 and 271 947 1071
Incl
udin
g
Article 266, part 1 and 2 104 137
Article 266, part 3 30 59
Article 266, part 4 28 39
Article 268 391 408
Article 271 394 428
Article 267 0 0
Article 269 0 1
Article 270 6 3
Article 272 2 0
Article 273 2 9
Article 274 0 0
Total 957 1084
In 2007, 537 persons were accused convicted for drug related crimes; 20 (3.7%) of accused person were women.
Table 11: Accused persons for drug-related crimes by age groups
2006 2007
Age group Number Percent Number Percent
> 18 3 0,6 2 0,418- 24 36 6,6 30 5,625- 29 57 10,5 77 14,330-49 397 73,3 365 6850< 49 9 63 11,7Total 542 - 537 -
Figure 15: Number of identified cases of drug-related crimes according to the corresponding articles of Criminal Code of RA
Source: Report of the Department on Combating Drug and Human Trafficking of the Central Department on Fight against Organized Crime of Police of Armenia, 2007.
In 2007, the first instance court has heard 185 and made 173 decision on drug related criminal cases (Court of RA 2007)
Table 12: The cases heard in the first instance court of RA, 2007(Articles 266, 268, 269,271, 272, 273, 276 of the criminal code)
Number of unfinished cases from the 2006 36
Number of new cases submitted to court 176
Number of court decisions made 173
Ceased cases 2
Number of cases sent for additional Investigation 1
Compulsory treatment for legal insanity 1
Unfinished cases in 2007 27
Convicted persons 245
Acquitted person 0
5. Drug Market
5.1 Availability and supply
According to the police data, drugs in Armenia are mainly distributed through the concealed networks of drug users. Drug sale in the streets or night clubs seems to be not a major issue of public concern in Armenia. According to the police sources, drug black markets hardly operate in Armenia under the strict police control and preventive measures.
24 25
National Report 2008
5.2 Drug Seizures
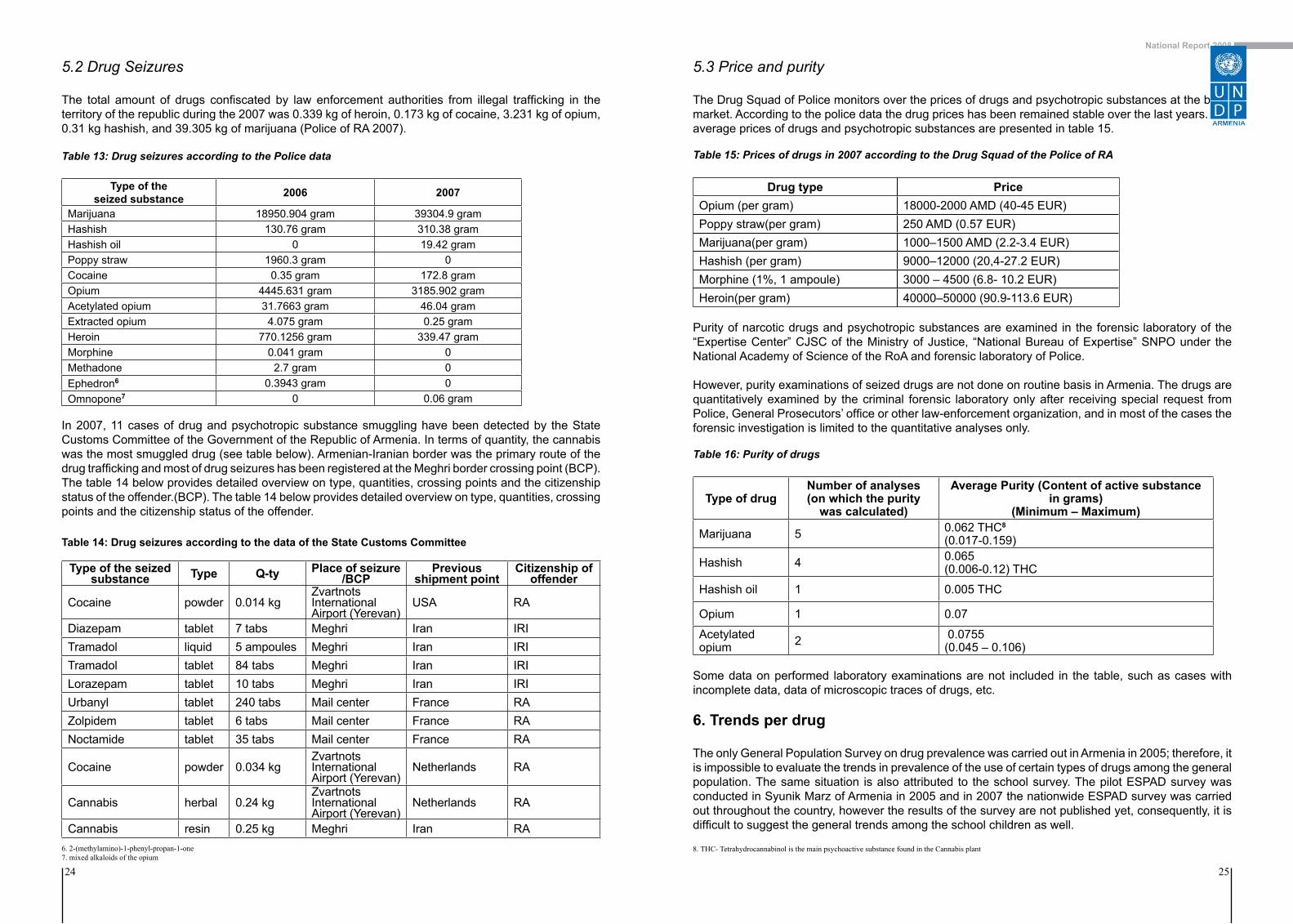
The total amount of drugs confiscated by law enforcement authorities from illegal trafficking in the territory of the republic during the 2007 was 0.339 kg of heroin, 0.173 kg of cocaine, 3.231 kg of opium, 0.31 kg hashish, and 39.305 kg of marijuana (Police of RA 2007).
Table 13: Drug seizures according to the Police data
Type of the seized substance 2006 2007
Marijuana 18950.904 gram 39304.9 gramHashish 130.76 gram 310.38 gramHashish oil 0 19.42 gramPoppy straw 1960.3 gram 0Cocaine 0.35 gram 172.8 gramOpium 4445.631 gram 3185.902 gramAcetylated opium 31.7663 gram 46.04 gramExtracted opium 4.075 gram 0.25 gramHeroin 770.1256 gram 339.47 gramMorphine 0.041 gram 0Methadone 2.7 gram 0Ephedron6 0.3943 gram 0Omnopone7 0 0.06 gram
In 2007, 11 cases of drug and psychotropic substance smuggling have been detected by the State Customs Committee of the Government of the Republic of Armenia. In terms of quantity, the cannabis was the most smuggled drug (see table below). Armenian-Iranian border was the primary route of the drug trafficking and most of drug seizures has been registered at the Meghri border crossing point (BCP). The table 14 below provides detailed overview on type, quantities, crossing points and the citizenship status of the offender.(BCP). The table 14 below provides detailed overview on type, quantities, crossing points and the citizenship status of the offender. Table 14: Drug seizures according to the data of the State Customs Committee
Type of the seized substance Type Q-ty Place of seizure
/BCPPrevious
shipment pointCitizenship of
offender
Cocaine powder 0.014 kgZvartnots International Airport (Yerevan)
USA RA
Diazepam tablet 7 tabs Meghri Iran IRITramadol liquid 5 ampoules Meghri Iran IRITramadol tablet 84 tabs Meghri Iran IRILorazepam tablet 10 tabs Meghri Iran IRIUrbanyl tablet 240 tabs Mail center France RAZolpidem tablet 6 tabs Mail center France RANoctamide tablet 35 tabs Mail center France RA
Cocaine powder 0.034 kgZvartnotsInternational Airport (Yerevan)
Netherlands RA
Cannabis herbal 0.24 kgZvartnotsInternational Airport (Yerevan)
Netherlands RA
Cannabis resin 0.25 kg Meghri Iran RA
5.3 Price and purity
The Drug Squad of Police monitors over the prices of drugs and psychotropic substances at the black market. According to the police data the drug prices has been remained stable over the last years. The average prices of drugs and psychotropic substances are presented in table 15.
Table 15: Prices of drugs in 2007 according to the Drug Squad of the Police of RA
Drug type PriceOpium (per gram) 18000-2000 AMD (40-45 EUR)Poppy straw(per gram) 250 AMD (0.57 EUR)Marijuana(per gram) 1000–1500 AMD (2.2-3.4 EUR) Hashish (per gram) 9000–12000 (20,4-27.2 EUR)Morphine (1%, 1 ampoule) 3000 – 4500 (6.8- 10.2 EUR) Heroin(per gram) 40000–50000 (90.9-113.6 EUR)
Purity of narcotic drugs and psychotropic substances are examined in the forensic laboratory of the “Expertise Center” CJSC of the Ministry of Justice, “National Bureau of Expertise” SNPO under the National Academy of Science of the RoA and forensic laboratory of Police.
However, purity examinations of seized drugs are not done on routine basis in Armenia. The drugs are quantitatively examined by the criminal forensic laboratory only after receiving special request from Police, General Prosecutors’ office or other law-enforcement organization, and in most of the cases the forensic investigation is limited to the quantitative analyses only.
Table 16: Purity of drugs
Type of drug Number of analyses(on which the purity
was calculated)
Average Purity (Content of active substance in grams)
(Minimum – Maximum)
Marijuana 5 0.062 THC8
(0.017-0.159)
Hashish 4 0.065(0.006-0.12) THC
Hashish oil 1 0.005 THC
Opium 1 0.07
Acetylated opium 2 0.0755
(0.045 – 0.106)
Some data on performed laboratory examinations are not included in the table, such as cases with incomplete data, data of microscopic traces of drugs, etc.
6. Trends per drug
The only General Population Survey on drug prevalence was carried out in Armenia in 2005; therefore, it is impossible to evaluate the trends in prevalence of the use of certain types of drugs among the general population. The same situation is also attributed to the school survey. The pilot ESPAD survey was conducted in Syunik Marz of Armenia in 2005 and in 2007 the nationwide ESPAD survey was carried out throughout the country, however the results of the survey are not published yet, consequently, it is difficult to suggest the general trends among the school children as well.
8. THC- Tetrahydrocannabinol is the main psychoactive substance found in the Cannabis plant6. 2-(methylamino)-1-phenyl-propan-1-one7. mixed alkaloids of the opium

26 27
National Report 2008
Data on trend per specific drugs is available only from the treatment demand sources and the Drug Squad of Police, which mainly concern to the drug use profile of patients admitted for the treatment to the Narcological Clinic and cases of drug seizures. 2005 was the first year when the full scale Pompidou protocol based electronic register was introduced into the Narcological Clinic, which to some extend allowed to systematize the analysis of the treatment demand data. Cannabis
Similarly to majority of the countries worldwide, cannabis (marijuana) is the most commonly used illicit drug in Armenia. According to the results of GPS conducted in 2005, about 5.4% of study respondents knew people using marijuana.
According to the reports of the Drug Squad of Police marijuana is the most commonly smuggled drug. Despite the cannabis seizure statistics declined since 2004, some trend towards increase has been recorded starting again from 2005. At the same time, no cases of cannabis related drug treatment has been registered in the Narcological Clinic in 2005 and 2006, but one in 2007. This inconsistency between the supposedly highest prevalence of cannabis use and zero treatment demand probably may be explained by the lower addiction potential of cannabis compared to other drugs and mainly opioids. Because of the use pattern (smoking), cannabis users are also not clients of low threshold services which might refer them to treatment or other specialized services for drug users.
Figure 16: Marijuana seizures by years, 2004-2007
Cocaine
Cocaine is not commonly used drug in Armenia. According to the GPS (2005) only 0.9% of survey respondents knew others using cocaine. No cases of admission for treatment for cocaine use have been registered in Narcological Clinic since 2005.
According to the data of the Drug Squad of Police, the amount of the seized cocaine has decreased substantially starting from 2004, with no cases of notification of cocaine seizure in 2005.
Figure 17: Cocaine seizures by years, 2004-2007
Heroin and other opiates
The use of pharmaceuticals containing opiates became popular in Armenia since 2003. The data from drug treatment centers and drop-in facilities indicate that currently the so-called “chernyashka” - (dark coloured solution made of fresh poppy bulbs or poppy straw, which is a mixture of opium and acetic anhydride) is popular among the users. The analysis of the profile of the patients admitted for treatment to Narcological clinic shows that most of them are opiate dependent (with the majority of them indicated the chernyashka as primary drug).
Figure 18: Profile of patients admitted for treatment in Narcological Clinic, 2005-2007
No clear trend can be observed in patterns of heroin use of patients admitted for treatment at Narcological Clinic, neither in amounts of seized drugs.

28 29
National Report 2008
Figure 19: Heroin and other opiates seizures by years, 2004-2007
Emerging Drugs
Coaxil9 misuse, which causes serious mental disorders and massive necrosis on injecting site, trombophlebitis, is an emerging problem in Armenia. It has a growing popularity among injecting drug users, since it is easy available without doctor’s prescription in drug stores throughout the country. Therefore, key stakeholders in the field of drug control need to be aware that in addition to “traditional drugs”, there are other emerging drugs that might cause problems in the future.
Poly-drug Use
Chaotic and poly-drug use is very common among drug users in Armenia, with frequent shifts from one to another following to the situation in the black market; they very frequently combine them with licit alcohol and tobacco.
7. Discussion
7. 1 Consistency between the indicators.
The data with regard to five key indicators of drug epidemiology is out of date or lacking. The only general population survey in Armenia was conducted in 2005 with several limitations and it is impossible to make projections on the prevalence of drug use among general population in 2007 based on the results of the 2005 survey. The full scale ESPAD was conducted in 2007 and the results were not available by the time of this reporting.
It is difficult to assess the situation regarding prevalence of problem drug use, because of lack of statistical data. No updated information on the prevalence of problem drug use was available in Armenia for the year 2007. Based on the data of published reports, upward trend in the number of patients admitted for inpatient treatment to the Narcological Clinic has been observed over the last years: from 71 treated in 2004 to 122 in 2007. The existing information from the treatment sources suggests that there is an urgent demand for introduction of rehabilitation and re-socialization services.
Data on drug related mortality are scarce and unreliable. No clear methodology of assessing drug-related mortality has been established in Armenia yet. The quality of drug related mortality data will depend on further improvements in forensic examination practices and procedure of notification.
Prevalence of HIV among the general population has been increased over the last years, whereas
the steady decrease of newly registered cases of Hepatitis B among the general population has been observed during the same period of time, which can be explained by the introduction of the Hepatitis B vaccine into the national immunization agenda.
No official estimate of the prevalence of Hepatitis C among general population is available since the Hepatitis C is not included in the list of reportable diseases.
General trends are inconsistent across drug demand and supply related indicators. The significant increase in patient admission rate to treatment services is incompatible with the slight decrease in amount of seized drugs. The possible explanation for the increased treatment demand indicator could be explained by the increased quality of drug treatment services, including the trust and confidence of drug addicts towards medical personnel of Narcological Clinic. At the same time it is hard to find a solid justification for the decrease in amount of seized drugs in 2007.
7.2 Methodological limitations and data quality
The scientific activity in the field of drug research remains very low in Armenia. No repetitions of previous research studies (GPS, Estimating the size of PDU population, school surveys) have been performed to enable the trends and patterns analysis and monitoring. A set of existing studies in drug related area only partly can speak up on the drug situation in Armenia. Most of the studies were implemented within the framework of the National Programme of the Response to HIV Epidemic, logically with stronger emphasize on HIV/AIDS rather than drugs. Many data from various studies presented in this Annual Report seem to be short in terms of their consistent analysis, perhaps because of the unclear and indistinct methodologies used.
Main problems and needs that are facing researchers in the field of drugs are insufficient financial resources, inadequate access to the hidden population of drug users, shortage of specially trained researchers and/or technical tools and software.
The main problem in terms of collecting the routine data on five key epidemiologic indicators is the absence of the standardized mechanism for drug related data collection and analyses. Standardized electronic Pompidou Group protocol database for collection of data on treatment demand indicator was introduced in Narcological Clinic of Yerevan in 2005. The database collects information on the patients admitted for the treatment to the inpatient department of the Narcological Clinic, but the lack of regulation requiring the mandatory data entering on the patients into the electronic database limits its applicability.
No standardized tools for collection of the drug treatment demand data exist either in the regional medical centers, entitled to provide specialized (ambulatory) narcological care, or in the Narcological Department of the Hospital of Detainees. The “Scientific Practical Medical Center” CJSC of the Ministry of Health is the only source of statistical information on drug-related death in Armenia. The fact that no clear national definition of drug related death and fatal overdoses exists in Armenia, and reports of fatal overdose and drug related death by forensic doctors is subject of the cultural and technical obstacles, limits the reliability of the official statistics on this indicator.
The National Center for HIV/AIDS prevention is the primary source for information on HIV/AIDS situation in the country, epidemiological surveillance, research and analysis as well as analyses of HIV/AIDS trends in general population and in specific population groups. The center collects information in accordance with the international standards and guidelines.
The information on the incidence and prevalence of Hepatitis B among general population is collected by the State Hygienic and Anti-Epidemic Inspection of the Ministry of Health of RA. No information on the prevalence of the Hepatitis B among specific population group is available in Armenia. 9 Coaxil (Tianeptine) is an antidepressant that is chemically related to amineptine.
30 31
National Report 2008
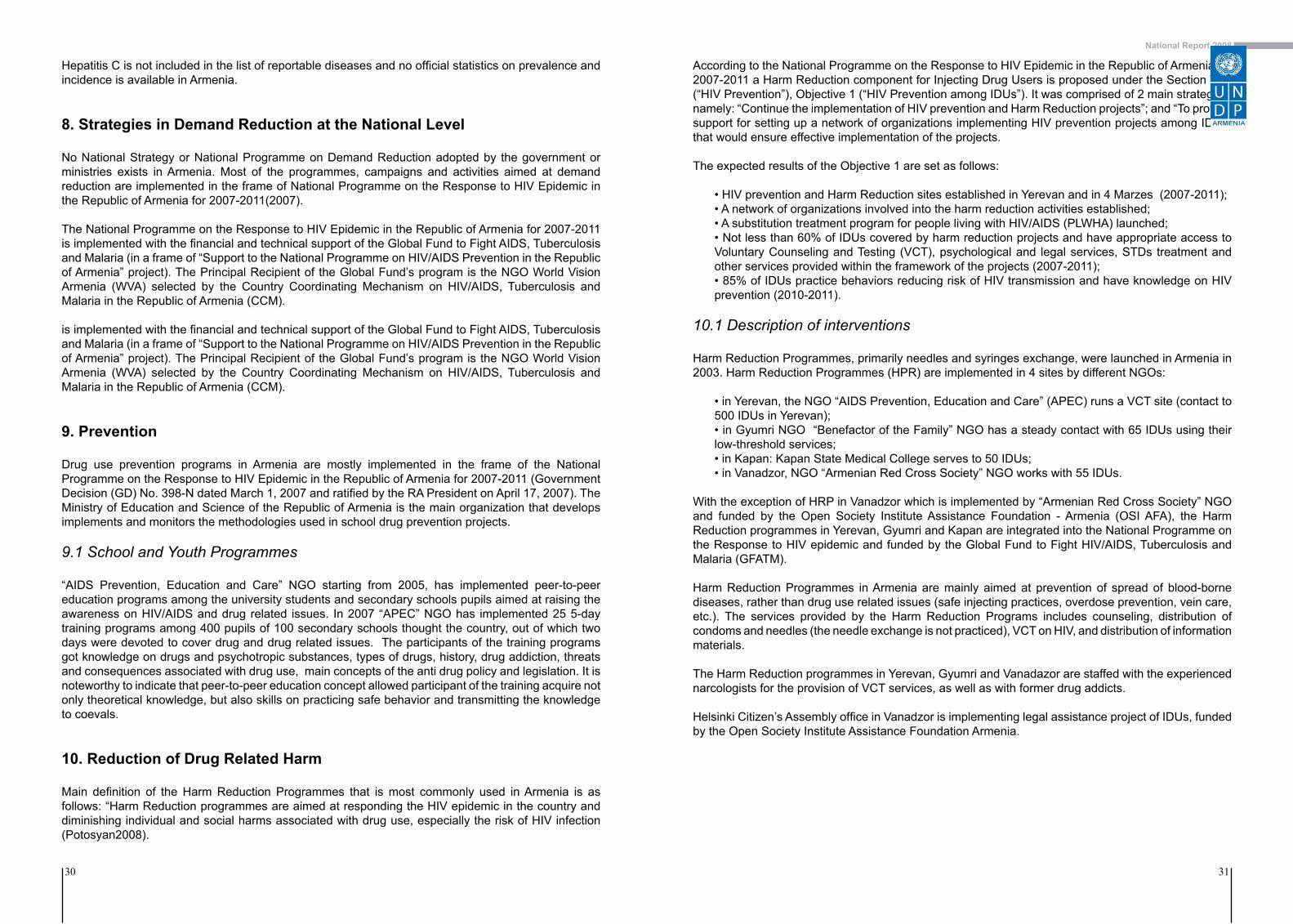
Hepatitis C is not included in the list of reportable diseases and no official statistics on prevalence and incidence is available in Armenia.
8. Strategies in Demand Reduction at the National Level
No National Strategy or National Programme on Demand Reduction adopted by the government or ministries exists in Armenia. Most of the programmes, campaigns and activities aimed at demand reduction are implemented in the frame of National Programme on the Response to HIV Epidemic in the Republic of Armenia for 2007-2011(2007).
The National Programme on the Response to HIV Epidemic in the Republic of Armenia for 2007-2011 is implemented with the financial and technical support of the Global Fund to Fight AIDS, Tuberculosis and Malaria (in a frame of “Support to the National Programme on HIV/AIDS Prevention in the Republic of Armenia” project). The Principal Recipient of the Global Fund’s program is the NGO World Vision Armenia (WVA) selected by the Country Coordinating Mechanism on HIV/AIDS, Tuberculosis and Malaria in the Republic of Armenia (CCM).
is implemented with the financial and technical support of the Global Fund to Fight AIDS, Tuberculosis and Malaria (in a frame of “Support to the National Programme on HIV/AIDS Prevention in the Republic of Armenia” project). The Principal Recipient of the Global Fund’s program is the NGO World Vision Armenia (WVA) selected by the Country Coordinating Mechanism on HIV/AIDS, Tuberculosis and Malaria in the Republic of Armenia (CCM).
9. Prevention
Drug use prevention programs in Armenia are mostly implemented in the frame of the National Programme on the Response to HIV Epidemic in the Republic of Armenia for 2007-2011 (Government Decision (GD) No. 398-N dated March 1, 2007 and ratified by the RA President on April 17, 2007). The Ministry of Education and Science of the Republic of Armenia is the main organization that develops implements and monitors the methodologies used in school drug prevention projects.
9.1 School and Youth Programmes
“AIDS Prevention, Education and Care” NGO starting from 2005, has implemented peer-to-peer education programs among the university students and secondary schools pupils aimed at raising the awareness on HIV/AIDS and drug related issues. In 2007 “APEC” NGO has implemented 25 5-day training programs among 400 pupils of 100 secondary schools thought the country, out of which two days were devoted to cover drug and drug related issues. The participants of the training programs got knowledge on drugs and psychotropic substances, types of drugs, history, drug addiction, threats and consequences associated with drug use, main concepts of the anti drug policy and legislation. It is noteworthy to indicate that peer-to-peer education concept allowed participant of the training acquire not only theoretical knowledge, but also skills on practicing safe behavior and transmitting the knowledge to coevals.
10. Reduction of Drug Related Harm
Main definition of the Harm Reduction Programmes that is most commonly used in Armenia is as follows: “Harm Reduction programmes are aimed at responding the HIV epidemic in the country and diminishing individual and social harms associated with drug use, especially the risk of HIV infection (Potosyan2008).
According to the National Programme on the Response to HIV Epidemic in the Republic of Armenia for 2007-2011 a Harm Reduction component for Injecting Drug Users is proposed under the Section Two (“HIV Prevention”), Objective 1 (“HIV Prevention among IDUs”). It was comprised of 2 main strategies, namely: “Continue the implementation of HIV prevention and Harm Reduction projects”; and “To provide support for setting up a network of organizations implementing HIV prevention projects among IDUs” that would ensure effective implementation of the projects.
The expected results of the Objective 1 are set as follows:
• HIV prevention and Harm Reduction sites established in Yerevan and in 4 Marzes (2007-2011);• A network of organizations involved into the harm reduction activities established;• A substitution treatment program for people living with HIV/AIDS (PLWHA) launched;• Not less than 60% of IDUs covered by harm reduction projects and have appropriate access to Voluntary Counseling and Testing (VCT), psychological and legal services, STDs treatment and other services provided within the framework of the projects (2007-2011);• 85% of IDUs practice behaviors reducing risk of HIV transmission and have knowledge on HIV prevention (2010-2011).
10.1 Description of interventions
Harm Reduction Programmes, primarily needles and syringes exchange, were launched in Armenia in 2003. Harm Reduction Programmes (HPR) are implemented in 4 sites by different NGOs:
• in Yerevan, the NGO “AIDS Prevention, Education and Care” (APEC) runs a VCT site (contact to 500 IDUs in Yerevan); • in Gyumri NGO “Benefactor of the Family” NGO has a steady contact with 65 IDUs using their low-threshold services; • in Kapan: Kapan State Medical College serves to 50 IDUs; • in Vanadzor, NGO “Armenian Red Cross Society” NGO works with 55 IDUs.
With the exception of HRP in Vanadzor which is implemented by “Armenian Red Cross Society” NGO and funded by the Open Society Institute Assistance Foundation - Armenia (OSI AFA), the Harm Reduction programmes in Yerevan, Gyumri and Kapan are integrated into the National Programme on the Response to HIV epidemic and funded by the Global Fund to Fight HIV/AIDS, Tuberculosis and Malaria (GFATM).
Harm Reduction Programmes in Armenia are mainly aimed at prevention of spread of blood-borne diseases, rather than drug use related issues (safe injecting practices, overdose prevention, vein care, etc.). The services provided by the Harm Reduction Programs includes counseling, distribution of condoms and needles (the needle exchange is not practiced), VCT on HIV, and distribution of information materials.
The Harm Reduction programmes in Yerevan, Gyumri and Vanadazor are staffed with the experienced narcologists for the provision of VCT services, as well as with former drug addicts.
Helsinki Citizen’s Assembly office in Vanadzor is implementing legal assistance project of IDUs, funded by the Open Society Institute Assistance Foundation Armenia.
32 33
National Report 2008
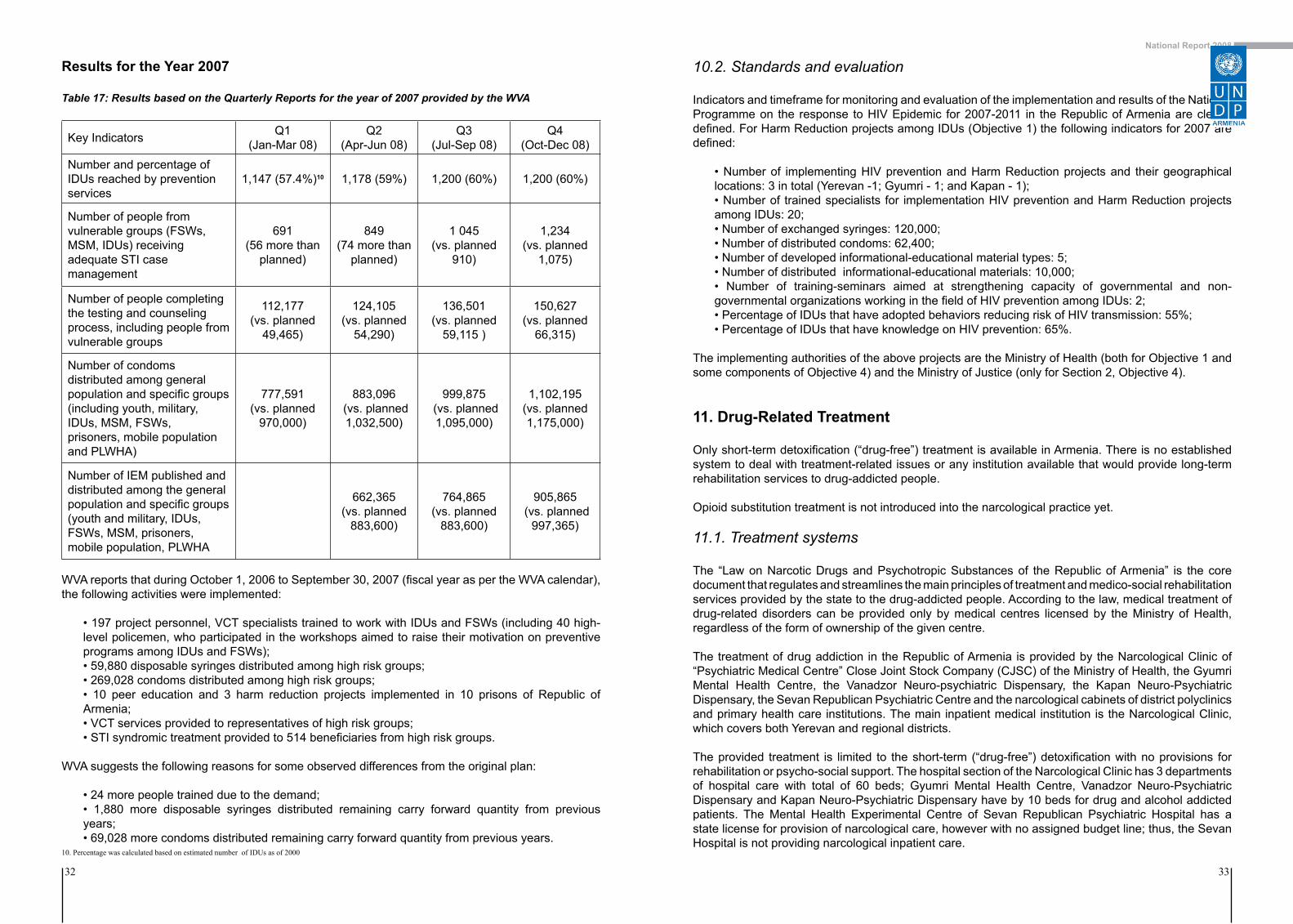
Results for the Year 2007
Table 17: Results based on the Quarterly Reports for the year of 2007 provided by the WVA
Key Indicators Q1(Jan-Mar 08)
Q2(Apr-Jun 08)
Q3(Jul-Sep 08)
Q4(Oct-Dec 08)
Number and percentage of IDUs reached by prevention services
1,147 (57.4%)10 1,178 (59%) 1,200 (60%) 1,200 (60%)
Number of people from vulnerable groups (FSWs, MSM, IDUs) receiving adequate STI case management
691(56 more than
planned)
849(74 more than
planned)
1 045 (vs. planned
910)
1,234 (vs. planned
1,075)
Number of people completing the testing and counseling process, including people from vulnerable groups
112,177 (vs. planned
49,465)
124,105 (vs. planned
54,290)
136,501 (vs. planned
59,115 )
150,627 (vs. planned
66,315)
Number of condoms distributed among general population and specific groups (including youth, military, IDUs, MSM, FSWs,prisoners, mobile population and PLWHA)
777,591 (vs. planned
970,000)
883,096 (vs. planned 1,032,500)
999,875 (vs. planned1,095,000)
1,102,195 (vs. planned 1,175,000)
Number of IEM published and distributed among the generalpopulation and specific groups (youth and military, IDUs, FSWs, MSM, prisoners, mobile population, PLWHA
662,365(vs. planned
883,600)
764,865(vs. planned
883,600)
905,865 (vs. planned
997,365)
WVA reports that during October 1, 2006 to September 30, 2007 (fiscal year as per the WVA calendar), the following activities were implemented:
• 197 project personnel, VCT specialists trained to work with IDUs and FSWs (including 40 high-level policemen, who participated in the workshops aimed to raise their motivation on preventive programs among IDUs and FSWs);• 59,880 disposable syringes distributed among high risk groups;• 269,028 condoms distributed among high risk groups;• 10 peer education and 3 harm reduction projects implemented in 10 prisons of Republic of Armenia;• VCT services provided to representatives of high risk groups; • STI syndromic treatment provided to 514 beneficiaries from high risk groups.
WVA suggests the following reasons for some observed differences from the original plan:
• 24 more people trained due to the demand;• 1,880 more disposable syringes distributed remaining carry forward quantity from previous years; • 69,028 more condoms distributed remaining carry forward quantity from previous years.
10.2. Standards and evaluation
Indicators and timeframe for monitoring and evaluation of the implementation and results of the National Programme on the response to HIV Epidemic for 2007-2011 in the Republic of Armenia are clearly defined. For Harm Reduction projects among IDUs (Objective 1) the following indicators for 2007 are defined:
• Number of implementing HIV prevention and Harm Reduction projects and their geographical locations: 3 in total (Yerevan -1; Gyumri - 1; and Kapan - 1);• Number of trained specialists for implementation HIV prevention and Harm Reduction projects among IDUs: 20;• Number of exchanged syringes: 120,000;• Number of distributed condoms: 62,400;• Number of developed informational-educational material types: 5;• Number of distributed informational-educational materials: 10,000;• Number of training-seminars aimed at strengthening capacity of governmental and non-governmental organizations working in the field of HIV prevention among IDUs: 2;• Percentage of IDUs that have adopted behaviors reducing risk of HIV transmission: 55%;• Percentage of IDUs that have knowledge on HIV prevention: 65%.
The implementing authorities of the above projects are the Ministry of Health (both for Objective 1 and some components of Objective 4) and the Ministry of Justice (only for Section 2, Objective 4).
11. Drug-Related Treatment
Only short-term detoxification (“drug-free”) treatment is available in Armenia. There is no established system to deal with treatment-related issues or any institution available that would provide long-term rehabilitation services to drug-addicted people.
Opioid substitution treatment is not introduced into the narcological practice yet.
11.1. Treatment systems
The “Law on Narcotic Drugs and Psychotropic Substances of the Republic of Armenia” is the core document that regulates and streamlines the main principles of treatment and medico-social rehabilitation services provided by the state to the drug-addicted people. According to the law, medical treatment of drug-related disorders can be provided only by medical centres licensed by the Ministry of Health, regardless of the form of ownership of the given centre.
The treatment of drug addiction in the Republic of Armenia is provided by the Narcological Clinic of “Psychiatric Medical Centre” Close Joint Stock Company (CJSC) of the Ministry of Health, the Gyumri Mental Health Centre, the Vanadzor Neuro-psychiatric Dispensary, the Kapan Neuro-Psychiatric Dispensary, the Sevan Republican Psychiatric Centre and the narcological cabinets of district polyclinics and primary health care institutions. The main inpatient medical institution is the Narcological Clinic, which covers both Yerevan and regional districts.
The provided treatment is limited to the short-term (“drug-free”) detoxification with no provisions for rehabilitation or psycho-social support. The hospital section of the Narcological Clinic has 3 departments of hospital care with total of 60 beds; Gyumri Mental Health Centre, Vanadzor Neuro-Psychiatric Dispensary and Kapan Neuro-Psychiatric Dispensary have by 10 beds for drug and alcohol addicted patients. The Mental Health Experimental Centre of Sevan Republican Psychiatric Hospital has a state license for provision of narcological care, however with no assigned budget line; thus, the Sevan Hospital is not providing narcological inpatient care.
10. Percentage was calculated based on estimated number of IDUs as of 2000

34 35
National Report 2008
Dispensaries of the clinics listed above also provide outpatient care, which is mainly narrowed to the short-term medical monitoring (so called “dispensary observation”) rather than rehabilitation as defined by WHO, UNODC and other international organizations (UNODS and WHO 2008). Drug user is falls under the dispensary observation, if the result of the biological (mostly urine) test is positive on drugs. Drug screening tests are conducted on the basis of legal order or on voluntary admission. The minimal observation period for non addicted clients (“episodic” users) is one year, but this term could be prolonged, if the patients had one or more relapses or did not regularly contacted the narcological institutions during the year.
Tabl
e 18
: Num
ber o
f Pat
ient
s R
egis
tere
d at
the
Dis
pens
ary
Reg
iste
r at t
he e
nd o
f the
yea
r, 19
80-2
007

36 37
National Report 2008
11.2. Drug Free Treatment
11.2.1. Inpatient treatment
In 2005 Anti-Drug Civil Union NGO jointly with the Narcological Clinic has elaborated standards of narcological care for Armenia (Anti Drug Civil Union and Narcological Clinic of “Psychiatric Medical Centre” CJSC 2005)11.
The detoxification is the only method of drug treatment currently available in Armenia. The average term of the detoxification is 10- 20 days (despite the officially recommended term of detoxification is 24 days). The provision of narcological care is free of charge for citizens of Armenia; however patients have to cover the whole costs of treatment including medications, if they apply for anonymous treatment. Usually, the standard detoxification treatment includes infusions of psychotropic substances to relieve the withdrawal symptoms (anxiolytics, tranquilizers etc) and some hepato-protectors and vitamins. However, the absence of alternative treatment methods or any type of post-detoxification support significantly limits both treatment demand and retention to treatment.
From the 122 patients treated at NC in 2007 on an inpatient basis, about 100 people used this service anonymously, avoiding to get registered in the Narcological Register and subsequently facing its consequences (not allowed to occupy certain positions in the government and law-enforcement agencies, not able to obtain gun license, driver license etc.). In those cases the patients had to pay for the treatment (about 132.000 AMD (330 EUR) for the entire treatment course of 24 days or 5500 AMD (13.75 EUR) for each day of inpatient treatment).
Doctors are delivering psycho-social support to the patients on individual basis. No group therapy is available in Armenia currently.
Spouses, relatives, partners etc. may share the rooms with the patients and assist them during the treatment. After the process of detoxification, no further service or continuum care is available.
11.2.2 Quality assurance
The “Standards on Treatment of Narcological Diseases in the Republic of Armenia” is developed by the “Anti-Drug Civil Union” NGO jointly with the Narcological Clinic in 2005 (Anti Drug Civil Union and Narcological Clinic of “Psychiatric Medical Centre” CJSC 2005). The Standards of Treatment of Narcological diseases define the scope of activities and interventions for each nosological condition and disease (including consulting, laboratory and instrumental interventions and treatment), duration of treatment, expected results as well as duration of the dispensary observation.
In Armenia, no standard and formal system of quality assurance of narcological treatment is established.
11.2.3. Outpatient treatment
Outpatient treatment for drug addicts is provided by Narcological cabinets of the district policlinics and outpatient departments of the four licensed medical institutions entitled for provision of narcological care. Narcological cabinets of district polyclinics merely provide limited outpatient care usually administered by a non-drug treatment specialist (often neurologists) who provides limited consultation and possible referrals to the Narcological Clinic. In 2007, 44 patients have received detoxification treatment at the outpatient department of the Narcological Clinic.
11.3. Substitution treatment
In Armenia, substitution treatment is not available yet. Starting from 2004, OSI-Assistance foundation Armenia and SCAD programme along with the national partners has implemented advocacy project on introduction of Methadone Substitution Treatment in Armenia. The following key objectives were set for introduction of Substitution Treatment into the narcological practice:
• Improve somatic and mental health status of patients addicted to injecting opiates; • Improve the patient’s psycho-social functioning.
Currently, all legal barriers for launching the Methadone Substitution Treatment are overcome:
• “Standards on Treatment of Narcological Diseases” were developed and ratified by the Minister of Health RA by 2005 (Order No. 1440-A as of December 12, 2005. The Standards include substitution treatment as a treatment option for opioid addiction; • “Clinical Guidelines on Methadone Substitution Treatment in Armenia” was ratified by the Minister of Health RA (Order No. 532-A as of June 02, 2005);• Methadone was rescheduled from List 1 (“Prohibited Drugs”) to List 2 (“Narcotic Drugs”) of drugs under the control in RA in 2006 (Decision of Government of RA No. 1046-N as of July 27, 2006 on “Making amendments in GD No. 1129-N as of August 21, 2003”);• 2920 grams of methadone has been included in state quotas of narcotics for Armenia for 2008.
In 2007-2008, a Methadone Treatment Office within the Narcological Clinic was established, fully renovated, furnished, equipped and standby to provide methadone treatment to opioid-addicted patients;
In parallel, the NGO “Antidrug Civil Union” (ACU NGO) has contacted US based company “Mallinckrodt Pharmaceuticals” producing addiction treatment tablets (namely, Methadone Oral Tablets), and built a business partnership with it. It is planned that after the state registration of the Methadone in Armenia by the “Scientific Center of Drugs and Medical Technology Expertise” CJSC of the Ministry of Health the “Arpharmacy” CJSC, the only specialized local company licensed to import medicaments containing narcotic drugs into Armenia will convey the Methadon to the drug treatment site. The mechanism of further operations has been drafted in details, agreed with above partners and appropriate contracts have been signed. Methadone state registration procedure was completed in December 2008.
The Methadone Treatment Pilot Project will be launched in Yerevan during the 2nd quarter of 2009. It is planned to have 100 patients at the end of the 1st year of the project, and both social and psychological support services should be available for patients receiving methadone.
Criteria for admission to the substitution treatment were developed, adopted and defined as follows:
• The patient must want to be treated and sign a Treatment Agreement (Informed Consent) attesting the patient’s consent and commitment to Methadone treatment;• Addiction must be established and patients requesting admission to a methadone treatment program should meet the International Classification of Diseases (ICD) -10 criteria for opioid dependence (F11.2);• Previous unsuccessful attempts to quit opiates, including: Self-attempts to quit opioids (based on anamnesis), or 2 or more unsuccessful detoxifications or other abstinence-based types of opioid dependence treatments (based on transfer information (epicrisis) from the previous clinic);• The patient must be 18 and older;• The priority should be given to pregnant women, HIV careers and patients with other serious diseases and, for these people the first 2 criteria is enough to enrol into the program.
11. The “Standards of Treatment of Narcological Diseases in the Republic of Armenia” was ratified by the Minister of Health RoA in 2005 (Order # 532-A as of June 02, 2005).

38 39
National Report 2008
12. Interventions in the Criminal Justice System
The prison system in Armenia has undergone remarkable changes after its transfer from the Ministry of Internal Affairs to the authority of the Ministry of Justice in October 2001. In present there are 13 prisons in the country.
The total prison population has been dramatically reduced after the introduction of a new Penal Code in 2003, and in present the average number of detainees is about 3,000. Each year 1,500 people are being detained and about the same number of people left the prison system. In 2007 there were 3539 detained and convicted persons (in 2006 there was 3,083 persons) in the Criminal Executive Institutions (CEI) of which 617 detained persons and 2,922 convicted.
In 2007 1229 persons have released from the CEI (Ministry of Justice of Republic of Armenia. 2008). The prison population rate per 100,000 of national population is 100.47 (National Statistical Service 2007).
12.1. Assistance to drug addicts in prisons
Convicted and detained drug addicts are entitled for provision of all types of medical services available at criminal executive institutions. The Department of Narcology (DN) of the Central Hospital of Detainees of the Ministry of Justice is the only institution providing specialized narcological care for drug addicts in prisons. In some prisons harm reduction projects are implemented.
12.1.1 Harm reduction programs
The Ministry of Justice is solely responsible for provision of drug use prevention, harm reduction and treatment services in prisons and submits annual reports to the GFATM, who is the main donor of harm reduction programmes in prisons. No NGOs are involved in the treatment, harm reduction or prevention programs implemented in prisons settings. The following harm reduction projects have been carried out in the entities of criminal executive system:
• Prison needle exchange projects (PNEPs) are conducted in 3 prisons: Erebuni, Kosh and Vanadzor. The medical staff distributes the syringes in 2 prisons and in 1 setting it is done by prisoners to prisoners (Moldavian experience). Within the National Programme on the Response to HIV Epidemic in the Republic of Armenia this should be expanded to all CEI countrywide;• Provision of condoms: in family/long term visiting rooms, via medical department, in toilets and premises. The proposal for distribution of condoms via condom machine was rejected by the Country Coordination Commission (CCM)on HIV/AIDS, Tuberculosis and Malaria issue;• Provision of leaflets: Educational components (booklets even interactively designed),• Voluntary Counseling and Testing (VCT) services;• Peer education: 141 prisoners were involved in peer education programmes in 2007;• Booklets: 1,145 pieces were provided by the National Centre for AIDS Prevention in 2007: • Educational materials: 8,701 pieces on various topics have been distributed.
No data or information was available on how and if any harm reduction measures were carried out in the remaining prisons.
12.1.2 Treatment
The Department of Narcology (DN) of Central Hospital of Detainees of the Ministry of Justice is the only specialized addiction treatment centre in the Armenian penitentiary system. DN is temporally located at the 4-th floor of the Department of Tuberculosis, constructed by the International Committee of Red Cross. The DN has 35 beds and one narcologist in charge.
Detoxification is the only drug treatment modality applied at prison’s settings. In 2007 total 43 drug users were admitted for treatment to the Department of Narcology.
Table 19: Characteristics of Patients treated at the Department of Narcology of the Hospital of Detainees
Number of Patients at the DN as of
01/01/2007Admitted Discharged
Number of Patients at the DN as of
01/01/2008Total drug users admitted for treatment 14 43 44 13
Intravenous drug use 8 32 31 9
Intravenous drugs and cannabinoids use 3 6 6 3
Intravenous drugs, cannabinoids and alcohol use
2 1 3 0
Intravenous drug and alcohol use 1 4 3 1
Cannabinoids use 3 8 11 0
Alcohol use 4 15 16 3
Among the IDUs who underwent treatment at the DN in 2007, 41 patients were admitted for the treatment for the first time and 16 had a treatment history. 2 patients were HIV positive, 14 were Hepatitis C positive, 9 had a Tuberculosis (TB) among which 3 had active TB and 6 had residual. The patients with the active TB have been transferred to the TB department.
VCT is not developed in all prisons. In case of positive HIV test the prisoner is transferred to the Infection department and his status very often can be disclosed to everybody.
12.2 Alternative to prisons for drug dependent offenders
No alternative treatment modalities such as “treatment instead of punishment” are available for drug addicts in Armenia.
12.3. Evaluation and training
The evaluation of the implemented programs is conducted by the Ministry of Justice and reports are submitted to the CCM. No special methodologist or Monitoring and Evaluation (M&E) specialist is involved into the data-processing and data analysis and M&E activities. Every professional staff of the Hospital of Detainees analyzes the data for his/her own sphere of activity.
According to the National Programme on the Response to HIV Epidemic for 2007-2011 for HIV prevention among prisoners (Objective 4) it is set the following key indicators for the year 2007:
• Number of Harm Reduction projects among prisoners: 1112;• Number of trained specialists for the implementation of HIV prevention and Harm Reduction projects among prisoners: 14;
12. According to the Indicators and Timeframe for monitoring and evaluation of the implementation and results of the National Programme on the response to HIV Epidemic for 2007 - 2011 in the Republic of Armenia, 11 harm reduction projects has been set for implementation in CEI, three of which are funded by the Global Fund.

40 41
National Report 2008
• Number of distributed syringes: 6,00013;• Number of distributed condoms: 90,000;• Number of types of developed informational-educational materials: 5;• Number of disseminated informational-educational materials: 10,000;• Number of workshops for Criminal-Executive Institutions’ high-ranking officers: 1;• Number of trainings seminars for prison staff: 1;• Percentage of prisoners having access to VCTs: 100%;• Percentage of prisoners having access to sterile injecting equipment: 60%;• Percentage of prisoners having access to condoms: 80%.
SELECTED ISSUES
13. HIV/AIDS
HIV epidemiological surveillance in the Republic of Armenia is conducted through routine HIV surveys and sentinel biological and behavioral HIV surveillance, regularly carried out since 2002.
Goals of the HIV epidemiological surveillance are the following:
• Determination of HIV prevalence rates in various populations;• Routine surveillance (monitoring) of the HIV dynamics in the country;• Identification of populations most at risk to HIV infection;• Identification and assessment of primary challenges for preventive programmes;• Assessment of factors of HIV transmission risk;• Monitoring for trends of changing HIV transmission modes; • Estimation of HIV cases;• Obtaining information necessary for planning preventive programmes, providing rationale for required measures and evaluation of efficiency of conducted preventive activities.
Routine HIV epidemiological surveillance includes registration of HIV and AIDS cases. New HIV cases in the country are registered on the basis of HIV sero-surveillance performed in 2 phases. In the first phase, HIV antibodies screening is doubly performed by ELISA method. In the second phase, specific antibodies produced in response to various HIV proteins are detected by Immunoblot Assay. HIV final diagnosis is made at the HIV reference laboratory of the National Center for AIDS Prevention. AIDS is diagnosed in adults and children with HIV by clinical or immunological indicators. 13.1 History and recent developments
According to the data of National Centre for AIDS Prevention of Armenia, as of December 31, 2007, there were 538 cases of HIV+ people registered in the Republic of Armenia cumulatively (with the first registration in 1988. with males constituting 401 cases (74.5%). So far, 13 cases of HIV among the children (2.4 % of registered cases) have been reported in Armenia. 12 cases of mother to child transmission of HIV and 1 case of child infection of HIV through blood have been registered. The overwhelming majority of the HIV-infected individuals (72.3%) have belonged to the age group 20-39 in the time of their registration. The highest number of HIV cases was reported in Yerevan, constituting 48.1% of all the registered cases; (see the map).
The HIV/AIDS situation assessment has shown that the estimated number of people living with HIV in the country is about 2,800.(Grigoryan, Hakobyan et al. 2008). The main mode of HIV transmission was through injecting drug use (47.4% of cases in 2007, vs. about 56% in 2006). In addition, the majority of all the HIV-infected males (63.8%) are individuals who practice injecting drug usage, while almost all the women (98.6%) were infected through sexual contacts. As of January 1 of 2008 (National Center for AIDS Prevention 2007).
Table 20: Modes of HIV transmission according to gender, January 2008
Gender
Transmission modes
Injecting drug use Heterosexual contacts
Homosexual contacts Through blood
Abs
olut
e nu
mbe
r
Per
cent
age
Abs
olut
e nu
mbe
r
Per
cent
age
Abs
olut
e nu
mbe
r
Per
cent
age
Abs
olut
e nu
mbe
r
Per
cent
age
Males 257 63.8 122 30.3 8 2.0 - -
Females - - 128 98.4 - - 1 0.8
13. According to the Indicators and Timeframe for monitoring and evaluation of the implementation and results of the National Programme on the response to HIV Epidemic for 2007 - 2011 in the Republic of Armenia the number of distributed syringes was set 6,000, however based on the report of the World Vision-Armenian NGO the actual number of distributed syringes was 7,000.

42 43
National Report 2008
Table 21: HIV prevalence rate per 100,000 of population
Region Prevalence per 100,000 population
Yerevan 23.0Shirak 18.5Lori 16.6Ararat 15.4Armavir 12.6Gegharkunik 12.5Aragatsotn 9.3Syunik 9.2Kotayk 8.0Vayots Dzor 5.4Tavush 3.7
Total 16.2
13.2 Risks and threats
In October-November 2007, biological and behavioral surveillance (BBS) for HIV was conducted in the Republic of Armenia among the following vulnerable and most-at-risk population groups: injecting drug users, commercial sex workers (CSW), men who have sex with men (MSM), individuals in penitentiary institutions, migrants and refugees, young people aged 15-24, especially vulnerable young people (EVYP)14 and most-at-risk adolescents (MARA)15.
The data of biological HIV surveillance showed some decrease in HIV prevalence among IDUs and CSWs from 15% in 2002 (11-20% estimated in the 90% of the confidence interval) to 6.8% (6.2-7.4% estimated in the 90% of the confidence interval) among IDUs in 2007 and in CSWs - from 1.1% in 2002 (<3% estimated in the 90% of the confidence interval) to 0.8% in 2007 (<2% estimated in the 90% of the confidence interval). The results of the surveillance carried out among MSM show that HIV prevalence among MSM is 2% (< 6% estimated in the 90% of the confidence interval).
• 68.1% of IDUs, 54.2% of CSWs, 73.7% of MSM, 30.4% of prisoners, 27.6% of migrants, 16% of MARA-IDUs, 8% of MARA-CSWs, 40% of MARA-MSM, 18% of EVYP have knowledge on HIV prevention;• 33.9% of IDUs, 18% of MARA-IDUs, 1.2% of prisoners shared injecting equipment in the last month;• 42% of CSWs had sex with non-commercial partners in the last year, of whom the majority 72.4% did not use a condom the last time they had sex with non-commercial partner. 62% of the surveyed MARA-CSWs had sex with non-commercial partners in the last year, of whom 19.4% did not use a condom the last time they had sex with non-commercial partners;• 29% of MSM did not use a condom the last time they had sex. 46% of MARA-MSM did not use a condom the last time they had sex;• 22.6% of prisoners who are sexually active had sex with non-regular partners in the last year, of whom 63.3% used a condom the last time they had sex with non-regular partners;• 51.1% of migrants who are sexually active had sex with non-regular partners, of whom 75.2% used a condom the last time they had sex with non-regular partners. 33.3% of refugees who are sexually active had sex with non-regular partners, of whom 64.3% used a condom the last time they had sex with non-regular partners;
• 57.8% of youth who are sexually active had sex with non-regular partners, of whom 84.6% used a condom the last time they had sex with non-regular partners. 91% of EVYP who are sexually active had sex with non-regular partners, of whom 86.9% used a condom the last time they had sex with non-regular partners.
The results of the behavioral surveillance also demonstrate that despite improvements in the most important behavioral characteristics a slight decrease has been noted in some areas:
• The level of knowledge on HIV prevention has been increased among IDUs, CSWs, MSM, youth and prisoners;• During the last five years usage of disposable syringes among IDUs has increased from 68.5% in 2002 to 97.5% in 2007. However, the percentage of IDUs sharing injecting equipment and using contaminated equipment has slightly increased. 33.9% reported sharing of injecting equipment in 2007, which is an increase of 2.8%, compared to 2005. Similarly, the sharing od injecting equipment has increased by 5.3% from 10.8% in 2005 to 16.1% in 2007;• Percentage of CSWs reporting condom use the last time they had sex with commercial partners increased from 89.2% in 2005 to 91.6% in 2007. Percentage of CSWs reporting condom use the last time they had sex with non-commercial partners decreased from 43% in 2005 to 27.6% in 2007;• Percentage of MSM reporting condom use the last time they had oral sex increased from 15.4% in 2005 to 34.7% in 2007 and anal sex increased from 60% in 2005 to 83.5% in 2007;• The number of migrants16 who had sex with non-regular sexual partners in the last year increased from 39.6% in 2005 to 51.1% in 2007. At the same time the number of MSM who had sex with non-regular sexual partners in the last year reduced from 90.5% in 2005 to 74% in 2007. As to IDUs and youth, the percentage of those reporting sex with non-regular sexual partners in the last year remained almost at the same level;• Rate of condom use during last sex with non-regular sexual partners increased among MSM, reduced among IDUs and youth and remained almost at the same level among migrants.
Thus, comparison of some results of the Second generation HIV biological and behavioral surveillance conducted in 2007 with the results of similar surveillance exercises carried out in 2002 and 2005 shows that the National AIDS Programme implementation resulted in achieving the desired results (Grigoryan, Hakobyan et al. 2008).
There are several possible explanations that could explain observed decrease in prevalence of HIV among IDUs: decrease in the prevalence might be caused by the reduced incidence of HIV among IDU and decreased prevalence due to the registered death cases, or the selected sample for the first BBS surveillance was not representative, which limits the generalization of the study results.
13.3. Prevention and treatment
As stated in the Chapters 9 and 12 above, the National Programme on the Response to HIV Epidemic for 2007-2011 is the main document that defines the objectives of the HIV prevention and treatment programs implemented in the Republic of Armenia (2007). All the activities and programmes to respond to HIV/AIDS in the country are coordinated by the Country Coordination Commission on HIV/AIDS, TB and Malaria issues (CCM) in the Republic of Armenia.
HIV/AIDS prevention and harm reduction programmes implemented among IDUs
The programmes are described in details in the Chapter 10 of this report. These programmes aim at forming safer sexual behavior, ensuring accessibility of condoms and disinfected injecting equipment, as well as establishing a relationship of trust with IDUs. The above-mentioned programmes include needle exchange, provision of VCT on HIV, outreach work, peer education, provision of condoms and educational material. 14. EVYP are defined as young people aged 15-19 who exhibit antisocial behavior
15. MARA young people aged 15-19 from the risk groups (IDU, MSM, FSW)16. Migrants- working migrants who were abroad for three and more months during the last three years

44 45
National Report 2008
HIV/AIDS prevention and harm reduction programmes implemented among Commercial Sex Workers (CSW)
These programmes aim to form safer sexual behaviour, to ensure the accessibility of condoms, and creation of an environment of trust. Peer education, outreach work, Voluntary Consulting and Testing on HIV, Sexually Transmitted Infections (STI) syndromal treatment, provision of condoms and educational material are being implemented within the framework of these programmes.
HIV/AIDS prevention and harm reduction programmes implemented among Men who have Sex with Men (MSM)
The project goal aims to form safer sexual behavior among MSM and ensure the accessibility of condoms. Peer education, provision of HIV, VCT related educational materials and condoms is being implemented within the framework of the project.
HIV/AIDS prevention and harm reduction programmes implemented among Migrants and Refugees
Preventive activities implemented among HIV vulnerable population groups include STI syndromal treatment.
HIV/AIDS prevention programmes implemented in schools and among the youth
National Programme on the Response to HIV Epidemic for 2007-2011 includes a component focused on youth population that is proposed under the Section Two (“HIV Prevention”), Objective 7 (“HIV Prevention among Adolescents and Young People aged 15-24”). There are 5 strategies identified under that objective, namely:
• Further integration of HIV-related issues into educational institutions curricula;• Providing peer-education;• Expanding youth-friendly services;• Increasing access to Voluntary Counseling and Testing (VCT) services;• Ensuring access to condoms;
According to the WVA reports during October 1, 2006 to September 30, 2007 (fiscal year as per the WVA calendar), 2007, the following activities were implemented:
• 400 schools covered by peer education programs; • 1,072 people trained (training of trainers (ToT) for peer educators, peer educators at school, school leaders, administrators, curators, form masters, regional educational department chiefs);• 252 events organized by peer educators against the target of 120; • 18,213 youth contracted to the events organized by peer educators against the target of 25,000;• 16,800 condoms were distributed among youth and military.
Special Groups of Youth
National Programme on the Response to HIV Epidemic for 2007-2011 as a focus for implementation of future programmes also includes the special groups of youth population. According to the Programme timetable, activities among Especially Vulnerable Young People (EVYP) aged 10-19 and Most at Risk Adolescents (MARA) aged 15-19, that are envisaged at Objective 6 under the Section 2 of the National Programme on the Response to HIV Epidemic for 2007-2011will be launched in 2008.
UNICEF- Armenia is also actively involved into the implementation of prevention programmes in schools and among youth. Particularly, along with other partner organizations the UNICEF encouraged the introduction of Life Skills-based education in upper grades of secondary schools with particular focus on HIV/AIDS and healthy lifestyle, facilitated the introduction of youth-friendly health services
into the health system through advocacy, policy development and training of health care providers and local authorities and intimately contributed to “Capacity building in HIV/AIDS Prevention” UN Joint Programme (UNAIDS, UNFPA, UNICEF, UNDP) aimed at strengthening the capacity of local authorities and selected NGOs working in the areas of community development, youth, human rights, gender, etc., to mainstream HIV/AIDS into their activities;
14. Quality Assurance
Formal evaluation of impact of HIV prevention programs implemented in the frame of the National Programme on the Response to HIV/AIDS Epidemic for 2002-2006 was conducted in Armenia in 2006 by UNAIDS. The evaluation was conducted on the basis of data collected from different sources, including: Behavioral and Biological Survey (BBS) conducted in Armenia in 2002 and 2005; recommendations made during the National workshop on Scaling-up towards Universal Access to HIV/AIDS Prevention, Treatment, Care and Support; reports of the Principal Recipient and sub-recipients of GFATM, reports of the National Center for AIDS prevention, interviews with key informants.
The results of the evaluation indicated that the preventive activities among IDUs within the framework of the National Programme on the Response to HIV Epidemic were provided on good level and has an impact on reducing the HIV prevalence in Armenia. However, it should be also noted that in programme evaluation no clear differentiation is made between the process and outcome evaluation and almost always only impact evaluation is conducted.
The effectiveness of the school and youth prevention programmes has not been evaluated on the national level.
15. Analytical Picture of drug production, trafficking and dealing
15.1 History and recent developments
The South-Caucasus region links the Caspian Sea, the Black Sea and the greater Middle East, Turkey and Iran and the Russian Federation. South Caucasus is being affected by the drug trade primarily due to the proximity of the region with main drug trafficking routes from Afghanistan towards Russia and Europe. To enhance the efficiency of border control in the countries of the South Caucasus, the EC will fund the implementation of the South Caucasus Integrated Border Management Programme.
After the collapse of Soviet Union, the criminal situation in Armenia was aggravated like in many Former Soviet Union (FSU) countries. The hard socio-economic situation, temptation of making easy money from drugs in an unstable economy, coupled with yet undeveloped system of drug control likely made Armenia a propitious territory for drug abuse and drug-related activities. Geographically Armenia is situated on crossroads of drug trafficking from Asia to Europe and during the last years potentially may become a transit route for illicit drug trafficking, while lacking the necessary technical facilities to fully counter this problem (International Narcotics Control Board 2008).
The two most important trafficking routes pass through Iran in the South (opiates), and through Georgia in the North (opium, heroin and cannabis). There were also instances of small-scale importation from other countries in the past year. Most of these cases involved passengers arriving at the airport in Yerevan.
Buprenorphine is being smuggled from Europe in South Caucasus. Subutex® is the commercial name of buprenorphine - a pharmaceutical product administered for part of substitution treatment patients in EU and USA. For South Caucasus, however, Subutex® is being diverted from licit distribution channels in Europe and trafficked to South Caucasus; according to Police evidence, the major smuggling pattern

46 47
National Report 2008
is to conceal the tablets in used vehicles trafficked to Southern Caucasus countries for second-hand sale (Police of RA 2007).
No significant illicit drug production in Armenia is known so far. Cannabis is historically cultivated in the country mostly for domestic consumption. Hemp and opium poppy grow wild in Armenia. Hemp grows mostly in the Ararat Valley, the south-western part of Armenia; poppy grows in the northern part, particularly in the Lake Sevan basin and some mountainous areas.
Armenia had developed chemical industry before the collapse of the Soviet Union, which utilized the chemical substances that are under the international control by UN drug conventions. Recently volumes of production of chemical enterprises has decreased significantly, however they have stored some leftover amount of chemical substances that are under the international control, for which they have to provide the Precursors’ Balance Quarterly Reports to the Drug Squad of Police. No cases of the illegal drug production by using chemical substances (precursors) are reported in Armenia (Police of RA 2007).
15.2 Countering activities
In the Republic of Armenia the drug supply reduction related activities are undertaken by the (i) Department on Combating the Drugs and Human Trafficking of the Central Department on Combating Organized Crime of the Police, (ii) National Security Service, Anti-Smuggling department of the State Customs Committee, (iii) Border Guards of the National Security Service.
15.3 Interagency cooperation at national and international level
Several documents aimed at the enhancement of the regional cooperation in the field of combating the illegal drug trafficking have been signed after gaining the independence.
In 1992, an agreement was signed in Kiev for cooperation in the fight against illegal drug trafficking between the member states of Commonwealth of Independent States (CIS).
In 1999 joint Memorandum of cooperation on drug control and combating money laundering was signed between Armenia, Georgia, Iran and the United Nations Drug Control Programme (UNDCP).
On November 30, 2000 the governments of the CIS member States adopted an agreement on cooperation to combat illicit trafficking in narcotic drugs, psychotropic substances and precursors. This instrument set the basic principles, guidelines and forms of cooperation, suggests the competent agencies authorized to establish direct contacts and the procedures for official request of cooperation and responding to requests.
In order to promote the further development of the legal framework for cooperation, on October 7, 2002 the Heads of the States of the CIS countries adopted a plan for cooperation between the member States of the CIS in activities to combat trafficking of narcotic drugs, psychotropic substances and precursors.
The Republic of Armenia has bilateral agreements with CIS countries on cooperation in the field of law enforcement, including drug related issues.
In 2005, the Police of the Republic of Armenia and the Federal Service of Drug Control of the Russian Federation signed an agreement on the fight against illegal trafficking of drugs, psychotropic substances and their precursors.
Starting from 2003, annual large-scale anti-drug operation, codenamed “Kanal” (translated from Russian as “channel”) is held on the territory of member states of the Collective Security Treaty Organization. The operation “Kanal” is aimed at cutting off drug trafficking channels, disabling international drug trafficking
groups, improving data exchange mechanisms and cooperation between the law enforcement bodies of Collective Security Treaty Organization (CSTO) member states (Armenia, Belarus, Kazakhstan, Uzbekistan Kyrgyzstan, Russia and Tajikistan). In 2007 the operation “Kanal” involved Russia, Ukraine, Kazakhstan, Belarus, Kyrgyzstan, Tajikistan, Uzbekistan, Finland, China, Azerbaijan, Georgia, Mongolia, Afghanistan, Poland, Latvia and Lithuania. The U.S. Drug Enforcement Administration also participated in “Kanal” operations as an observer. During this exercise, the Armenian enforcement authorities paid special scrutiny to all vehicles crossing the border and all containers arriving at the airport.
The Police of RA, National Security Service, State Customs Committee, Border Guards of the Republic of Armenia have participated in the comprehensive anti-drug operation “Kanal”, which in 2007 was held in two phases from August 28-September 3, 2007 and from November 27-December 3, 2007.
The comparative analyses of the results of the operation “Kanal” shows that there is a positive trend in increased effectiveness of the operation, improved professionalism of the representative of law enforcement agencies, strengthening the role of the Coordinating Committee of heads of corresponding agencies combating drug trafficking in the Collective Security Treaty Organization member states.
Figure 20: Comparative analyses of the main results of the operation “Kanal”, 2003-2007
Table 22: Comparative analyses of the amount of the seized drugs and psychotropic substances, operation “Kanal” 2003-2007
Type of Drug “Kanal -2003” “Kanal -2004” “ Kanal-2005” “ Kanal-2006” “ Kanal-2007”
Opium 0 2.9 91.4 171.9 3.1
Poppy straw 0 60 0 0 0
Marijuana 158.9 5284.4 43.4 1103 700.37
Hashish 2.7 8.6 14 18.5 11.8Psychotropic substances 0 15 tab 69 tab 51 tab 0
Precursors 0 0 5.031 litres 1.5 ml 0

48 49
National Report 2008
An important point in joint activities to combat drug-related crime on the territory of CIS is the approval by the Council of Heads of State of the CIS, meeting in Dushanbe on 5 October 2007, of the regular programme of cooperation between CIS member States on activities to combat illicit trafficking in narcotic drugs, psychotropic substances and their precursors for the period 2008-2010, which will enhance the quality of cooperation within the Commonwealth in joint practical action to combat the drug threat.
The Government of Armenia has also established close cooperation with the Government of US, aimed at increasing the capacity of Armenian law enforcement. Joint activities include the development of an independent forensic laboratory, the improvement of the law enforcement infrastructure and the establishment of a computer network that will enable Armenian law enforcement offices to access common databases. In 2007, the Department of State, through its Export Control and Related Border Security (EXBS) program, continued to assist the government of Armenia in its efforts aimed at the non-proliferation of weapons of mass destruction and their delivery systems. This assistance programme is aimed at the enhancement of capacities of Armenia’s border services to better control the borders and to interdict all contraband, including narcotic drugs (International Narcotics Control Strategy Report).
The South Caucasus Anti-Drug Programme (SCAD) during its fifth phase of implementation also greatly supported to the strengthening of the regional cooperation among the law enforcement agencies of Armenia, Azerbaijan and Georgia and their European counterparts. One of the objectives of the SCAD-V Programme is to enhance the regional cooperation on law enforcement issues and to support the beneficiaries gradually to adopt the harmonized methods and standards of combating drug trafficking and abuse.
15.4. Prognosis
Armenia, being located at the cross-road of Europe and Asia, theoretically has the potential to become a transit point for international drug trafficking. Its role in drug trafficking could be exacerbated by lenient criminal penalties, at least compared to other countries in the region. At present, limited transport traffic between Armenia and its neighbouring states makes the country a secondary traffic route for drugs. Armenia’s borders with Azerbaijan and Turkey remain closed; however, according to the police reports, opiates and heroin are smuggled to Armenia from Turkey via Georgia, so it is possible that when these borders are open, drug transiting could increase significantly and further deterioration of the situation in Iran may have repercussions throughout the region in term of increased drug trafficking and drug abuse in the South Caucasus region (International Narcotics Control Board 2008).
List of Tables
Table 1: Drug use experience by gender, 2007 12Table 2: Drug use experience by region type, 2007 12Table 3: Last month prevalence of drug use among Armenian students (%) 12Table 4: Number of patients received inpatient treatment in the Narcological Clinic (NC), Yerevan 18Table 5: Newly registered cases of alcohol psychosis, chronic alcoholism, drug use by years. 18Table 6: Main drug of use of patients admitted for drug treatment, 2007 19Table 7: Drug use patterns of patients getting inpatient treatment at Narcological Clinic, 2007 19Table 8: Number of newly registered cases of Hepatitis B and HIV among population of Armenia, the cumulative in 1990-2007 21Table 9: Identified drug related crimes and offences by regional police stations 23Table 10: Drug related crime and offences by the articles of the RA Criminal Code 24Table 11: Accused persons for drug-related crimes by age groups 24Table 12: The cases heard in the first instance court of RA, 2007(Articles 266, 268, 269,271, 272, 273, 276 of the criminal code) 25Table 13: Drug seizures according to the Police data 25Table 14: Drug seizures according to the data of the State Customs Committee 26Table 15: Prices of drugs in 2007 according to the Drug Squad of the Police of RA 26Table 16: Purity of drugs 27Table 17: Results based on the Quarterly Reports for the year of 2007 provided by the WVA. 34Table 18: Number of Patients Registered at the Dispensary Register at the end of the year, 1980-2007 37Table 19: Characteristics of Patients treated at the Department of Narcology of the Hospital of Detainees 41Table 20: Modes of HIV transmission according to gender, January 2008 44Table 21: HIV prevalence rate per 100,000 of population 44Table 22: Comparative analyses of the amount of the seized drugs and psychotropic substances, operation “Kanal” 2003-2005 50

50 51
National Report 2008
List of Figures
Figure 1: GPP Respondents knowing others using drugs (as % of total) 10Figure 2: Distribution of persons taking sedatives and tranquillizers by frequency of use and area of residence 11Figure 3: Students’ Survey (SS) respondents knowing others using drugs (as % of total) 13Figure 4: GPS participants’ response to the statement:”Do you regard a drug addict more as criminal, than as afflicted with a disease?” 14Figure 5: GPS participants’ response to the statement: “People should be allowed to use hashish or marijuana” 15Figure 6: GPS respondent’s attitude to the question “Trying heroin once or twice” 15Figure 7: Response of SS participants on the statement:”Do you regard a drug addict more as criminal, than as afflicted with a disease?” 16Figure 8: Response of SS participants on the statement: “People should be allowed to use hashish or marijuana” 16Figure 9: SS Respondent’s attitude to the question: “Smoking marijuana or hashish regularly…” 17Figure 10: First treatment demand and number of patients registered at narcological register of Narcological Clinic by years, 2005-2007 20Figure 11: Reported positive finding of drugs or their metabolites (death in the presence of drugs), 2004-2007 20Figure 12: Number of PLWHA and newly diagnosed HIV 21Figure 13: Distribution of HIV, AIDS and death cases by years 22Figure 14: Drug related crime and drug related offences 2004-2007 23Figure 15: Number of identified cases of drug-related crimes according to the corresponding articles of Criminal Code of RA 24Figure 16: Marijuana seizures by years, 2004-2007 28Figure 17: Cocaine seizures by years, 2004-2007 29Figure 18: Profile of patients admitted for treatment in Narcological Clinic, 2005-2007 29Figure 19: Heroin and other opiates seizures by years, 2004-2007 30Figure 20: Comparative analyses of the main results of the operation “Kanal”, 2003-2007 50
Reference
(2007). National Programme on the Response to HIV Epidemic in the Republic of Armenia for 2007-2011. Yerevan.
AIDS Prevention Education and Care (2005). Report on the prevalence of Alcohol, Tobacco and Drug Use among 16 Years Old Schoolchildren of the Secondary Schools of Syunik Marz. Yerevan.
Amirkhanyan, H. (2008). Personal Commnication with AntiDrug Civil Union. Yerevan.
Anti Drug Civil Union and Narcological Clinic of “Psychiatric Medical Centre” CJSC (2005). Standards of Treatment of Narcological Diseases in the Republic of Armenia. Yerevan.
Asriyan, N. and T. Zábranský (2006). “First General Population Survey on Psychotropic Substances in Armenia.” DrugNet Europe 54: 6-8.
Babloyan, A., S. Sargsyan, et al. (2007). School Based Health Survey Report. Yerevan, Arabkir Joint Medical Center - Institute of Child and Adolescent Health, UNICEF Armenia Country Office.
Court of RA (2007). Annual Report on Criminal Cases Investigation in First Instance Courts. Yerevan.Danseco, E. R., P. M. Kingery, et al. (1999). “Perceived Risk of Harm from Marijuana Use among Youth in the USA” School Psychology International 20(1): 39-56.
EMCDDA (2002). Handbook for surveys on drug use among the general population. EMCDDA project CT.99.EP.08 Lisbon.
Grigoryan, S., A. Bussel, et al. (2002). “Rapid Assessment of the Situation on Spread of HIV Infection Including Intravenous Drug Users.” International Journal of Drug Policy 13(5): 433-436.
Grigoryan, S., A. Hakobyan, et al. (2008). HIV Epidemiological Surveillance in the Republic of Armenia. Yerevan, National Center for AIDS Prevention: 155.
Gyurjyan, G. and A. Bazarchyan (2005). “Report on the Results of the National Survey on Drug, Alcohol and Smoking Prevalence among the General Population of Armenia.”
Harutyunyan, A. (2004). Drug use prevalence among the students of the higher educational institutions of the Republic of Armenia.
International Narcotics Control Board (2008). Report of the International Narcotics Control Board for 2008. Vienna: 87-96.
Melik-Andreasyan, G. (2004). Epidemiology of blood-borne viral hepatitis in Armenia. Yerevan, The Research Institute of Epidemiology, Virology and Medical Parasitology. Doctor of Science 169.
Merkinaite, S. (2007). HCV Infection in Europe, Eurasian Harm Reduction Network: 3.
Ministry of Justice of the Republic of Armenia. (2008). Report on the activities implemented by the Ministry of Justice of the Republic of Armenia. Yerevan, Ministry of Justice of the Republic of Armenia.
National Center for AIDS Prevention (2007). HIV situation in the Republic of Armenia. Yerevan.
National Statistical Service (2007). Statistical Yearbook of Armenia. Yerevan.
Police of the RA (2007). Annual Statistical Newsletter of Police. Yerevan.

52 53
National Report 2008
Semerjyan, P. (2007). Personal communication on drug treatment in Armenia. S. Programme. Yerevan.
UNODS and WHO (2008). Principles of Drug Dependence Treatment.
Weilandt, G., J. Ecker, et al. (2005). Anonymous Survey on Infectious Diseases and Related Risk Behavior among Armenian Prisoners and on Knowledge, Attitudes and Behavior of Armenian Prison Staff towards Infectious Diseases and Drugs. Bonn, European Network on Drugs and Infections Prevention in Prison (ENDIPP).
WHO Regional Office for Europe, UNAIDS, et al. (2006) Epidemiological Factsheet on HIV/AIDS and sexually transmitted diseases, Armenia. 17
Appendix 1
Extract from the RA Criminal Code with amendments
Chapter 26: Crimes against population health Article 266. Illegal turnover of narcotic drugs, psychotropic substances and their precursors with the purpose of sale or their illegal sale. 1. Illegal manufacture, processing, procurement, keeping, trafficking or supplying of narcotic drugs or psychotropic substances with the purpose of sale, is punished with the imprisonment for the term of 3 to 7 years. 2. The same action committed: 1) by a group of persons; 2) in large amount; 2.1) repeatedly;3) at the place of imprisonment or arrest; 4) in disciplinary/educational institution, is punished with imprisonment for the term of 5 to 10 years with property confiscation. 3. Actions envisaged in parts 1 or 2 of this Article, if they were committed: 1) by an organized group; 2) in especially large amount, is punished with the imprisonment for the term of 7 to 15 years with or without property confiscation. 4. Illegal manufacture, processing, procurement, keeping, trafficking or illegal supplying of precursors with the purpose of manufacturing narcotic drugs or psychotropic substances is punished with a fine in the amount of up to 200 times of the minimum wage or with arrest for up to 3 months.5. The considerable, large and especially large amounts of narcotic drugs and psychotropic substances are established by Annex to this Code. 6. A person voluntarily submitting narcotic drugs or psychotropic substances will be relieved of criminal responsibility for illegal manufacture, processing, procurement, keeping, trafficking or supplying of narcotic drugs or psychotropic substances. 7. Crimes envisaged in this chapter are considered as repeated, if they are committed by persons convicted by 266, 268-275 articles of this Code. (title was changed in 26.05.08, amendments and alterations made in 09.06.04, 26.05.08)Article 267. Breach of regulations for manufacture, procurement, keeping, accounting, dispensing, transportation or supply of narcotic drugs or psychotropic substances 1. Breach of regulations for manufacture, procurement, keeping, accounting, dispensing, transportation or supply of narcotic drugs or psychotropic substances by the person who is in charge of their observance, if it resulted in theft or illegal turnover of afore-mentioned substances, is punished with a fine in the amount of 200 to 500 minimal salaries, or with imprisonment for the term of up to 3 years, with deprivation of the right to hold certain posts or practice certain activities for up to 3 years. 2. The action envisaged in the first part of this article, if it was committed in large amounts, is punished with a fine in the amount of 500 to 800 minimal salaries, or with imprisonment for the term of 2 to 4 years, with deprivation of the right to hold certain posts or practice certain activities for up to 3 years. 3. The action envisaged in the first part of this article, if it was committed in especially large amounts, is punished with imprisonment for the term of 3 to 5 years, with deprivation of the right to hold certain posts or practice certain activities for up to 3 years. (title was changed in 26.05.08, amendments and alterations made in 09.06.04, 26.05.08)Article 268. Illegal turnover of narcotic drugs or psychotropic substances without the purpose of sale1. Illegal manufacture, processing, procurement, keeping, delivery or supply of narcotic drugs or psychotropic substances without the purpose of sale in considerable amounts, is punished with arrest for the term of up to 2 months or with imprisonment for the term of up to 1 year. 2. The same action committed:1) repeatedly;2) in large amount: Is punished with imprisonment for the term of up to 3 years. 3. The same action committed in especially large amount:

54 55
National Report 2008
Is punished with imprisonment for the term of 2 to 6 years. (title was changed in 26.05.08, amendments and alterations made in 26.05.08)Article 269. Theft or extortion of narcotic drugs or psychotropic substances. 1. Theft or extortion of narcotic drugs or psychotropic substances, is punished with imprisonment for the term of 3 to 7 years. 2. The same action committed: 1) by a group of persons with prior agreement; 2) by abuse of official position; 3) with violence not dangerous for life or health, or with threat of such violence, 3.1) repeatedly;4) in large amount, is punished with imprisonment for the term of 6 to 10 years with or without property confiscation. 3. The action envisaged in part 1 or 2 of this Article which was committed: 1) by an organized group; 2) in especially large amount; 3) with violence dangerous for life or health, or with threat of such violence, is punished with imprisonment for the term of 8 to 15 years with or without property confiscation. (title was changed in 26.05.08, amendments and alterations made in 26.05.08, 26.05.08)Article 269.1. Illegal making, use, forgery of documents or sale of false documents entitling the right to obtain narcotic drugs or psychotropic substances or their precursorsIllegal making, use, forgery of documents or sale of false documents entitling to obtain narcotic drugs or psychotropic substances or their precursors, is punished with a fine in the amount of 300 to 600 minimal salaries or with arrest for the term of 1 to 3 months, or with imprisonment for the term of up to 2 years.The same action committed:repeatedly;by a group of persons with prior agreement,is punished with imprisonment for the term of 2 to 5 years.(added in 26.05.08)Article 270. Illegal issue of recipes or other documents entitling the right to obtain narcotic drugs or psychotropic substances Illegal issue of recipes or other documents entitling the right to obtain narcotic drugs or psychotropic substances by authorized person out of mercenary or other personal motives, is punished with imprisonment for the term of up to 2 years, with deprivation of the right to hold certain posts or practice certain activities for up to 2 years or without the latter.The same action committed repeatedly, is punished with imprisonment for the term of 2 to 5 years, with deprivation of the right to hold certain posts or practice certain activities for up to 2 years. (title was changed in 26.05.08, amendments and alterations made in 09.06.04, 26.05.08)Article 271. Use of narcotic drugs(liquidated in 26.05.08)Article 272. Abetting or involving into use of narcotic drugs or psychotropic substances1. Abetting or involving into use of narcotic or psychotropic drugs, is punished with a fine in the amount of 200 to 600 minimal salaries, or with arrest for the term of up to 3 months, or with imprisonment for the term of up to 3 years. 2. Abetting or involving into the use of narcotic or psychotropic drugs, committed: 1) in relation to a minor; 2) in relation to two or more persons; 2.1) repeatedly;3) by deception; 4) with violence or with a threat to commit violence, is punished with imprisonment for the term of 3 to 8 years. 3. The same action, if this negligently caused the death of the aggrieved or caused grave damage to his health, is punished with imprisonment for the term of 6 to 12 years. (title was changed in 26.05.08, amendments and alterations made in 01.01.06, 26.05.08)Article 273. Illegal cultivation or raising of herbs prohibited for processing, containing narcotic, psychotropic or toxic substances1. Cultivation or raising of herbs prohibited for processing containing narcotic, psychotropic or toxic
substances, done in large amount, is punished with a fine in the amount of 300 to 500 minimal salaries, or with arrest for the term of 1-3 months, or with imprisonment for the term of up to 2 years. 2. The same action committed: 1) by several persons with prior agreement; 2) by an organized group; 2.1) repeatedly;3) in especially large amount, is punished with imprisonment for the term of 3 to 8 years. (Title was changed in 26.05.08, amendments and alterations made in 26.05.08)Article 274. Organization and maintaining of dens for the use of narcotic or psychotropic drugs1. Organization and maintaining of dens for the use of narcotic or psychotropic drugs, is punished with imprisonment for the term of up to 4 years. 2. The same action committed: 1) by an organized group; 1.1) repeatedly;2) by abuse of official position, 3) in disciplinary/education institutions, is punished with imprisonment for the term of 3 to 7 years. (title was changed in 26.05.08, amendments and alterations made in 26.05.08)Article 275. Illegal turnover of strong or toxic substances for the purpose of sale or their illegal sale1. Illegal manufacture, processing, procurement, keeping, trafficking, supply of strong substances which are not considered to be narcotic or psychotropic drugs, for the purpose of illegal sale, is punished with imprisonment for the term of up to 3 years. 2. The same action committed: 1) by a group of persons with prior agreement, 1.1) repeatedly;2) in large amount, is punished imprisonment for the term of 2 to 5 years. 3. The action envisaged in part 1 or 2 of this Article which was committed: 1) by an organized group, 2)in especially large amount; is punished with imprisonment for the term of 4 to 8 years. 4. A person voluntarily submitting strong or toxic substances will be relieved of criminal responsibility for illegal manufacture, processing, procurement, keeping, trafficking, supplying or selling of strong or toxic substances. (title was edited in 26.05.08, amendments and alterations made in 09.06.04, 26.05.08)Article 276. Breach of rules for manufacture, procurement, keeping, accounting, transfer, transportation or supply of strong or toxic substances Breach of rules for manufacture, procurement, keeping, accounting, transfer, transportation or supply of strong or toxic substances, if this caused theft or other significant damage, is punished with a fine in the amount of up to 300 minimal salaries, or with imprisonment for the term of up to 2 years, with deprivation of the right to hold certain posts or practice certain activities for 3 years. (amendments and alterations made in 01.06.06, 09.06.04)

56 57
National Report 2008
List of Acronyms
AIDS Acquired immune deficiency syndromeCCM Country Coordinating Mechanism on HIV/AIDS, Tuberculosis and Malaria issuesCIS Commonwealth of Independent StatesCJSC Close Joint-Stock Company CSTO Collective Security Treaty OrganizationDN Department of NarcologyEC European CommissionEMCDDA European Center on Drugs and Drug AddictionESPAD European School Survey Project on Alcohol and other DrugsEVYP Young people aged 15-19 who exhibit antisocial behavior EXBS Export Control and Related Border SecurityFSU Former Soviet Union FSW Female Sex WorkerGD Government DecreeGFATM Global Fund to Fight HIV/AIDS, Tuberculosis and Malaria HIV Human Immunodeficiency VirusICD International Classification of DiseasesIDU Injecting Drug UsersIEM Information, Education MaterialsIRI Islamic Republic of IranMARA Young people aged 15-19 from the risk groups (IDU, MSM, and FSW)MSM Men who has Sex with MenNC Narcological ClinicNEP Needle Exchange ProjectNGO Non Governmental OrganizationOSI Open Society InstitutePLWHA People leaving with HIV and AIDSPNEPs Prison needle exchange projectsRA Republic of ArmeniaSCAD South Caucasus Anti-Drug ProgrammeSTD Sexually Transmitted DiseaseTB TuberculosisToT Training of TrainersUNAIDS Joint United Nations Programme on HIV/AIDSUNDP United Nations Development ProgrammeUNESCO United Nations Educational, Scientific and Cultural Organization UNFPA United Nations Population FundUNICEF United Nations Children’s FundUNODC United Nations Office on Drugs and CrimeVCT Voluntary Counseling and TestingWASH Willing anonymous salivary HIV and hepatitis surveillanceWHO World Health OrganizationWVA World Vision – Armenia