national quality improvement center for collaborative ... · permanency, well-being, and recovery...
TRANSCRIPT

National Quality Improvement Center for Collaborative Community Court
Teams To Address the Needs of Infants, Young Children, and
Families Affected by Substance Use Disorders
Request for Proposals
Release Date: 01/26/2018
Due Date: 02/23/2018
The National Quality Improvement Center for Collaborative Community Court Teams is funded by the Children’s Bureau, Administration on Children, Youth and Families, Administration for Children and Families, U.S. Department of Health and Human Services, under grant #90CA1854. The contents of this document are solely the responsibility of the Center for Children and Family Futures and do not necessarily represent the official views of the Children’s Bureau.

Table of Contents I. OPPORTUNITY DESCRIPTION ........................................................................................................ 1
A. Intent and Goals ........................................................................................................................................... 1
B. Background .................................................................................................................................................. 1
C. Target Population ......................................................................................................................................... 3 D. Application Process ...................................................................................................................................... 3
II. ELIGIBILITY ....................................................................................................................................... 4
III. EXPECTATIONS ............................................................................................................................. 5
A. Training, Technical Assistance and Coaching Approach (TTAC) ............................................................... 5
B. Collaboration ................................................................................................................................................ 6
C. Evaluation Expectations and Requirements ................................................................................................. 9 D. Funding Limitations/Allowable Use of Funds ........................................................................................... 10
E. Reporting Requirements ............................................................................................................................. 10
F. Assurances ................................................................................................................................................. 11
IV. REQUIRED RFP SUBMISSION COMPONENTS ........................................................................ 11
A. Application Face Page ................................................................................................................................ 12
B. Project Narrative ........................................................................................................................................ 12
V. PROJECT BUDGET AND BUDGET NARRATIVE ..................................................................................... 15
VI. SUPPORTING DOCUMENTS ...................................................................................................... 16
VII. SUBMISSION PROCESS .............................................................................................................. 17
VIII. REVIEW CRITERIA ...................................................................................................................... 17
IX. SITE SELECTION PROCESS ............................................................................................................... 19
APPENDIX A: PATHWAY 1 APPLICATION SUBMISSION COMPONENTS........................................................ 20
A. Pathway 1 Application Face Page .............................................................................................................. 20
B. Pathway 1 Narrative ................................................................................................................................... 20
C. Supporting Documents for Pathway 1 Applicants ..................................................................................... 21
ATTACHMENT A – CONTEXTUAL DATA TABLES ........................................................................................ 22
ATTACHMENT B – KEY STAFF AND TEAM COMPOSITION TABLE .............................................................. 25
ATTACHMENT C – THE FIVE POINT INTERVENTION FRAMEWORK ............................................................. 26
ATTACHMENT D – QIC-CCCT BUDGET COST FORM ................................................................................. 27
I. OPPORTUNITY DESCRIPTION A. Intent and Goals The National Quality Improvement Center for Court for Collaborative Community Court Teams (QIC-CCCT) will support demonstration sites to design, implement, and test approaches that meet the requirements of the Child Abuse Prevention and Treatment Act (CAPTA) of 2010 as amended by the Comprehensive Addiction and Recovery Act of 2016 (CARA) and that better meet the needs of infants and families affected by substance use disorder and prenatal substance exposure. This initiative will build on and enhance the basic collaborative approach offered by the Quality Improvement Center for Research-Based Infant Toddler Court Teams (QIC-ITCT).
The National Quality Improvement Center for Collaborative Community Court Teams (QIC-CCCT) will provide 15 Collaborative Community Court Teams (CCCTs) with intensive training, technical assistance, and coaching (TTAC) support to:
• Enhance the capacity of CCCTs to appropriately implement the provisions of the Comprehensive Addiction and Recovery Act (CARA) amendments to the Child Abuse and Prevention Treatment Act (CAPTA).
• Enhance and expand CCCTs’ capacity to effectively collaborate to address the needs of infants, young children, and their families/caregivers affected by substance use disorders (SUDs) and prenatal substance exposure.
• Sustain the effective collaborative partnerships, processes, programs, and procedures implemented to achieve the goals of each demonstration site.
• Provide the field with lessons they can apply about effective practices for implementing the requirements of CARA and meeting the needs of children and families affected by substance use disorders.
The QIC-CCCT will support demonstration sites in developing Continuous Quality Improvement (CQI) approaches to monitor collaborative implementation efforts as well as assessing their current capacity to collaboratively address the health and substance use disorder treatment needs of infants, young children, and their parents or caregivers.
Innovative communities that seek to build their capacity to better serve families affected by SUDs are encouraged to apply for this opportunity, and set forth a plan for intensive collaboration among child welfare agencies, state or tribal Court Improvement Programs, local courts, the legal community, substance use treatment providers, prevention services providers, mental health providers, hospitals, maternal and infant healthcare providers, early intervention providers, public health, and other key stakeholders. Demonstration sites must be prepared to share data with partners, participate in robust programmatic evaluation, and facilitate timely and effective information sharing.
B. Background More than 600,000 infants are born each year with prenatal exposure to substances including: tobacco (15.4%), alcohol (9.4%), or illicit drugs (5.4%).i What is particularly concerning is that the incidence of Neonatal Abstinence Syndrome (NAS) among opioid-exposed infants increased from 1.20 per 1,000 births in 2000ii to 5.80 in 2012.iii NAS can disrupt mother-infant attachment, particularly for women who may have difficulty responding to their infants’ cues.
1

More than 3 million babies are exposed to alcohol and 1 in 20 children may have Fetal Alcohol Spectrum Disorders (FASD)iv which are physical, behavioral, and intellectual disabilities that can last a lifetime. Polysubstance use, which is typical for most individuals with SUDs, compounds the risks for caregiver and infant, and creates challenges in identifying and isolating effects of exposure. The long-term success of these children improves with early identification and interventions.v,vi Substance use disorder among pregnant women and parents and caregivers of infants and very young children presents numerous complex challenges to the child welfare and court system, the medical community, and substance use disorder and mental health treatment providers. These challenges are compounded when systems do not effectively share information or work in a coordinated fashion. Differing stakeholder perspectives, policies, time tables for completing treatment, and expectations between child welfare workers and substance use disorder treatment providers are common. Lack of appropriate comprehensive family-centered treatment services for families involved in both the child welfare and substance use disorder treatment systems, remains endemic.
Approximately 11% of children live with one or more parent who is dependent on alcohol or needs treatment for illicit drug abuse.vii Most families with parental SUDs do not come to the attention of child welfare system (CWS). However, for those families who do, addressing SUDs and other co-occurring challenges is critical. Of children in care, 61% of infants and 41% of older children have at least one parent who is using drugs or alcohol.viii The rate of substantiated child maltreatment is the highest for young children: 27.7% of the 683,487 victims of substantiated abuse and neglect were under 3 years, with the highest rates for children younger than 1 year.ix CWS agencies report increases in caseloads, primarily among infants and young children placed in out-of-home care. The number of children in out of home care (OOHC) increased by more than 13,000 from 414,429 in 2014 to 427,910 in 2015. Of the nearly 270,000 children who entered OOHC in 2015, the largest group, approximately 47,000, were infants. The percentage of children entering OOHC who had parental drug use reported as a reason for removal increased from 22.1% in 2009 to 46.4% in 2015, the largest increase of any reason for removal. While there is great variation across states, every state reports a higher rate of parental SUDs among children under 1 year old than older children
Given the rise of substance use disorder nationally and the increase in the number of infants and young children entering foster care, there is an acute need to enhance coordination across family serving entities. There is growing evidence that data-driven, multi-system collaborative team approaches may help to ameliorate such challenges. Parents with SUDs who are at-risk or involved with the child welfare system (CWS) face multiple challenges that affect safety, permanency, well-being, and recovery outcomes. A coordinated, family-focused service delivery system that emphasizes prevention, early intervention, engagement, and an array of quality community-based treatment and support services through all stages of child welfare cases is thus critical for sustained recovery and improved family well-being.
Dependency courts sit at the intersection of some of the most challenging issues families face and have proven to be key partners in systems improvement work. State and Tribal Court Improvement Programs, in particular, which operate out of administrative offices of the courts, can be especially effective in convening stakeholders and bringing additional attention to critical community needs.
2

In July 2016, P.L. 114-198, “Comprehensive Addiction and Recovery Act of 2016” (CARA), went into effect including Title V, Section 503, “Infant plan of safe care.” The legislation made several changes to the Child Abuse Prevention and Treatment Act (CAPTA), including:
• Removing the term, “illegal” in regard to substance abuse; • Requiring that the plan of safe care address the needs of both the infant and the affected
family or caregiver; • Specifying data to be reported by states, to the maximum extent practicable on the
affected infants and the plans of safe; and, • Specified increased monitoring and oversight for states to ensure that Plans of Safe Care
are implemented and that families have access to appropriate services.
States are in various stages of developing and implementing policy and practice changes related to this legislation. With the assistance of the QIC-CCCT TTAC, demonstration sites have the opportunity to align proven implementation strategies with state protocols and practices for the benefit of families in their local communities. This includes states that may be implementing Program Improvement Plans related to CAPTA implementation.
C. Target Population QIC-CCCT demonstration sites will serve infants, young children, and their families or caregivers that are affected by SUDs, and are court and child welfare involved due to child maltreatment (both in-home and out of home placement). The QIC-CCCT anticipates that demonstration sites will prioritize serving pregnant women, mothers and fathers with children under age 3, and infants and children with identified prenatal substance exposure.
D. Application Process The QIC-CCCT is conducting a competitive application process that will result in the selection of 15 CCCT sites with demonstrated need, readiness, and commitment to meet the goals of the initiative. Two steps comprise the application process: 1) a proposal in response to the Request for Proposals (RFP); and, 2) a teleconference consult and assessment. From the initial proposals received, the QIC-CCCT will invite a select number of applicants to move to the second stage: a focused one-on-one consult and assessment via conference call with QIC-CCCT staff. The purpose of the consult-assessment will be to:
• Ensure applicants have a clear understanding of and are fully committed to the QIC-CCCT initiative.
• Provide the QIC TTAC Team with an understanding of the need and readiness of the applicant.
• Obtain clarification or additional information on any issues identified through the proposal review process.
• Identify initial TTAC needs. For the final selection of demonstration sites, the QIC-CCCT will take into account results from the proposal reviews and the teleconference consult-assessments, as well as geographic distribution of applicants, cultural diversity of their target populations, and demonstrated levels of need. The QIC-CCCT expects to select and notify demonstration sites by the end of March 31st, 2018. Below are additional dates to help guide you through the process.
3

Site Selection Step Date
Proposals due to the QIC-CCCT (see “How to Submit” section for directions on how to submit applications)
February 23rd, 2018
Teleconference Consult and Assessment March 14th to 23rd, 2018 (approximate)
Final Selection and successful applicant notification March 31st, 2018
II. ELIGIBILITY The QIC-CCCT invites state or tribal Court Improvement Programs (CIP, TCIP), local dependency courts or dependency court partner agencies to apply to meet the goals of this initiative and improve practice for children and families in their community. This is an open opportunity for established and/or new collaborative courts. There are two pathways for applicants to apply:
Pathway 1: CIPs/TCIPs or Tribal Governments as Lead Agency
• State or tribal CIPs are eligible to submit an application as the lead agency, in collaboration with up to three local or tribal courts within their jurisdiction. State CIPs may include tribal courts in their application, and tribal CIPs may include local courts in their application. The QIC-CCCT will provide funding to the CIP/TCIP offices to be distributed to the local or tribal courts by way of a Mutually Binding Agreement between the QIC-CCCT and CIP/TCIP. CIP/TCIP applicants must submit letters of commitment from the local or tribal court demonstration sites (Chief/Presiding Judge1), their state or tribal child welfare agency, substance use disorder prevention and treatment agency, and public health agency (Maternal and Child Health).
• If a tribal court’s jurisdiction does not have a TCIP, Tribal Governments or an agency they designate as lead agency may submit an application in collaboration with tribal courts. QIC-CCCT will provide funds to the Tribal Government, or lead agency, for distribution to the tribal courts by way of a Mutually Binding Agreement between the QIC-CCCT and lead agency to receive demonstration site funds. Tribal Governments must submit letters of commitment from the tribal court (Chief Judge), their child welfare agency, substance use disorder prevention and treatment agency, and public health agency (Maternal and Child Health).
Pathway 2: Local or Tribal Courts, or Court Partner Agencies as the Lead Agency
• If the state or tribal CIP, or Tribal Government chooses not to apply under Pathway 1, a local or tribal court is eligible to apply directly, provided they submit a letter of commitment from the state or tribal CIP, and core team partners representing the court
1 The QIC-CCCT recognizes that in certain situations, Judges may not be in a position to bind the court to an agreement. If this is the case, letters of commitment from court or tribal administrators, court clerks, or other individuals the applicant deems best suited to bind the court to an agreement can be substituted for a letter of commitment from the Chief/Presiding Judge.
4

(Chief/Presiding Judge2), child welfare agency, substance use disorder treatment, public health (Maternal and Child Health), maternal and infant healthcare providers, hospitals, and early childhood/early intervention providers.
• Other local or tribal agencies such as child welfare, substance use disorder prevention and treatment, and hospitals may also submit applications as the lead in partnership with their local dependency court. Local or tribal agencies other than a dependency or tribal court would require a letter of commitment from the local or tribal court. The QIC-CCCT would provide funds directly to the applicant agency through Mutually Binding Agreements. Applications will require letters of commitment from the court (Chief/Presiding Judge2), child welfare agency, substance use disorder prevention and treatment agency, and public health agency (Maternal and Child Health), maternal and infant healthcare providers, and hospitals.
III. EXPECTATIONS A. Training, Technical Assistance and Coaching Approach (TTAC) QIC-CCCT is a 30-month initiative providing substantial support and expertise through a unique TTAC model that matches a site’s strengths, needs, resources and priorities with a dedicated Change Team. The Change Team includes a senior-level Change Liaison (CL) who is highly experienced in collaborative practice. For any tribal CIP, tribal government or tribal court awardees, the Tribal Law and Policy Institute (TLPI) will provide a senior-level Change Liaison. TLPI will also provide expert consultation to all QIC-CCCT demonstration sites on culturally appropriate policies and practices. The Change Teams are supported by Advocates for Human Potential (AHP) evaluators who are skilled in a CQI approach to process and outcomes evaluation and building sites’ performance monitoring capacity. A consultant pool of national subject matter experts will further support the Change Teams.
The QIC-CCCT initiative will consist of four phases, described below. The phases provide a roadmap for the work to be completed by demonstration sites—with the support of the QIC Change Teams—recognizing that sites may progress through the phases at different rates based on their existing level of collaborative capacity.
Phase 1: Site Assessment and Readiness for Change: During this initial phase, the Change Teams will help sites clearly define their needs, assess their current capacity, practice, and policies to implement the CARA requirements, and strengthen their collaborative capacity to serve parents and caregivers affected by substance use disorders, their infants and children. Administering cross-system surveys, and baseline data collection and analysis are critical components during this phase to diagnose barriers, identify contextual issues, and address other concerns. The Change Teams will assist sites with initial development of a draft site action plan to guide their implementation process and identify technical assistance needs. During this phase, the Change Teams will also begin working with sites to establish and/or strengthen their collaborative governance structure. An effective governance structure is essential to engage and retain partners, policy makers, and other critical stakeholders in the initiative. Participants in
2 The QIC-CCCT recognizes that in certain situations, Judges may not be in a position to bind the court to an agreement. If this is the case, letters of commitment from court or tribal administrators, court clerks, or other individuals the applicant deems best suited to bind the court to an agreement can be substituted for a letter of commitment from the Chief/Presiding Judge.
5

this phase will begin to identify targets for policy and practice changes. The anticipated duration for Phase 1 is approximately 4 months.
Phase 2: Site Plan Development and Capacity Building: Using data and information from the Phase 1 assessment process, the Change Teams will work with sites to finalize their site action plan and mutual priorities for practice and policy changes. The site action plan will include tasks, activities and action steps for testing practice or policy changes. During this phase, sites will finalize their collaborative governance structure and core team composition and also initiate sustainability planning discussions. Anticipated duration for Phase 2 is approximately 6 months.
Phase 3: Site Plan Implementation and Evaluation/Pilot Testing of Program, Practice, and Policy Changes: This phase will focus on fully implementing and testing sites’ identified program, practice or policy changes identified in Phase 2, assessing implementation processes, and making the necessary adaptations and adjustments. Using the principles of rapid-cycle improvement, sites will test their change strategies and obtain feedback about what works, and make adjustments accordingly. The key benchmark of Phase 3 is the implementation of practice and policy changes that improve services for infants, children, and families. Anticipated duration for Phase 3 is approximately 12-18 months.
Phase 4: Dissemination, Evaluation and Sustainability: Phase 4 focuses on identifying resources to sustain and institutionalize policy and practice changes. The Change Team will work with sites to disseminate effective strategies and lessons locally and more broadly with their CIP/TCIP to inform policies and practices in other dependency courts. Evaluation results will be presented to stakeholders. Anticipated duration for Phase 4 is approximately 3 months.
Selected sites will be required to participate in the following TTAC activities:
• Site Calls (Monthly): Change Teams will hold individual monthly calls with each of their sites. These calls provide an opportunity to develop a TTAC plan, discuss progress and identify challenges and successes.
• Onsite TTAC (Annually): The Change Teams will conduct an annual two-day site visit with each court team to provide targeted TTAC.
• QIC All-Sites Meeting: All sites are expected to attend a two-day All-Sites Meeting each contract year. This meeting will provide sites with opportunities to network with each other and to learn from QIC subject matter experts.
• Distance Learning: Webinars (Bi-Monthly): The QIC will hold cross-site webinars every other month to provide sites with subject matter expertise and a learning exchange forum to network with other sites on site plan development and implementation.
B. Collaboration Demonstration sites must include intensive collaboration among state, tribal, and local level agencies, at all levels of governance, drawing both from research-based 10 Essential Components of Collaborative Courts as well as the Five-Point Intervention Framework for Children and Families (Five-Point Intervention Framework). The QIC will help CCCTs build their collaborative capacity to: a) respond to the needs of infants and young children affected by substance exposure and their parents/caregivers; b) meet the requirements of the CARA amendments to CAPTA; and, c) bring together the full complement of services and key stakeholders including child welfare, CIPs, local courts, legal professionals, SUD prevention and
6

treatment (including medication-assisted treatment providers), mental health, hospitals, and primary, obstetrical, and pediatric health care.
The 10 Essential Components of Collaborative Courts is a set of research based recommendations for family drug courts that apply to other collaborative courts. The ten recommendations are: 1) create a shared mission and vision; 2) develop interagency partnerships; 3) create effective communication protocols for sharing information; 4) ensure interdisciplinary knowledge; 5) develop protocols for early identification and assessment; 6) address the needs of parents; 7) address the needs of children; 8) garner community support; 9) implement funding and sustainability strategies; and, 10) evaluate for shared outcomes and accountability.x Together, the Five-Point Intervention Framework and the 10 Essential Components provide guidance for implementing collaborative courts, and to strengthen prevention and intervention services to infants, children, and families affected by prenatal substance exposure.
The Five-Point Intervention Framework (see Attachment C) defines the points when interventions can benefit all women of child-bearing age, pregnant women with substance use disorders, their infants and children with prenatal substance exposure, and their families and caregivers. Each intervention point involves multiple systems – generally public health, health care, substance use disorder treatment, child welfare, and early intervention services.
Collaborative Governance Structure. Effective collaboration is the cornerstone of CCCTs. The QIC will help the CCCTs implement or strengthen a governance structure that includes cross-systems representation from all key partners, executive-level individuals with decision-making authority, and agreed-upon processes, protocols, and responsibilities that are outlined in a formal Memorandum of Understanding (MOU) among the key partners. An effective governance structure enables collaborative partners to identify, manage, and resolve emerging issues, maintain focus on the mission and vision, ensure due process rights of all parties, and sustain the CCCT. Further, the CCCT will be coached to elevate needed discussions about the CCCT’s outcomes and effectiveness to the Executive and Steering Committees to infuse proven practices into the larger CCCT partners’ systems.
The QIC-CCCT recommends a three-tiered governance structure for CCCTs to establish and maintain successful collaboration. CCCTs are expected to identify the following leadership teams (or similar entities) in their project narrative with membership as outlined in the table below:
• Executive Committee – This executive level committee provides project oversight, review and approval of practice and policy recommendations, assurance of active participation by each agency’s designated staff, and coordination with other CCCTs in the state or Tribe. The committee is comprised of state, tribal directors, commissioners, secretaries, or leaders from the primary collaborative partners, including the court, child welfare, substance use disorder treatment, public health, infant and maternal healthcare providers, and hospitals. If the selected lead agency is a CIP/TCIP, the CIP/TCIP and partner agencies will act in this capacity.
• Steering Committee – This committee provides local oversight, and will vary slightly depending on who the applicant is. For Pathway 1 applicants this committee will act as the liaison between the CCCT Core Team and the CIP/TCIP and Executive Committee, providing policy and practice change recommendations and assuring streamlined communication. For Pathway 2 applicants this committee will be responsible for both
7

oversight and executive decision-making for the project. The Steering Committee’s membership will be department directors and agency leaders, the court (chief judge or dependency judge and attorneys representing parents, children, and the child welfare agency).
• Core Team – The team is comprised of program leaders and managers of the court (dependency judge and attorneys representing parents, children and the child welfare agency), partner agencies and service providers with sufficient level of decision-making authority to ensure activities and policy changes are carried out in a timely manner. The Core Team is responsible for: completing goals and activities identified through the QIC-CCCT process; demonstrating active involvement of each partner agency in the completion of the goals and objectives; addressing barriers and communication problems in a timely fashion; and, keeping their respective Executive Committee member informed of the progress, challenges, barriers, and emerging issues.
The table below provides more information on QIC-CCCT’s recommended governance structure for CCCTs and anticipated membership for each level of governance depending on the pathway through which agencies apply.
Pathway 1 Pathway 2
Executive Committee
CIP/TCIP/Tribal Government, partner agencies
Not Applicable. (For Pathway 2 applicants the Executive Committee duties will be assumed by the Steering Committee.)
Steering Committee
Department directors and agency leaders, the court (chief judge or dependency judge, and attorneys representing parents, children, and child welfare agency) who will be responsible for coordination with the CIP and additional CCCT sites.
Local department directors and agency leaders as well as a CIP representative.
CCCT: Core Team Program leaders and managers of the court (dependency judge, attorneys representing children, parents, and child welfare agency), partner agencies and service providers with sufficient level of decision-making authority to ensure activities and policy changes are carried out in a timely manner.
Program leaders and managers of partner agencies with sufficient level of decision-making authority to ensure activities and policy changes are carried out in a timely manner.
8

C. Evaluation Expectations and Requirements The QIC-CCCT evaluation will study CCCTs’ stages of implementation; detail services and activities (e.g., collaboration, data-driven decision-making, dissemination, family-centered treatment, sustainability); identify innovative collaborative models, strategies, lessons, and barriers to CARA implementation; measure core child and family outcomes; and, assess and support performance monitoring capacity and continuous quality improvement (CQI).
Reporting and ongoing feedback to support data driven decisions and continuous quality improvement are central to the evaluation. Reporting will be used to support a regular feedback loop with demonstration sites to facilitate process improvement, and keep stakeholders informed about emerging lessons in key areas. At the core of our data-driven CQI process will be a “virtuous cycle” that includes: 1) evaluation findings generated via ongoing collection and analysis of data; 2) regular feedback of findings via presentations, issue briefs, and other mechanisms; and, 3) ongoing data collection to assess the impact of the changes, including tracking progress from baseline measures. Skilled evaluators will support demonstration sites through evaluation technical assistance focused on building sites’ capacity to regularly collect, analyze and use data for program improvement.
Demonstration site must agree to participate as active partners in the QIC-CCCT evaluation. Site evaluation activities are expected to include:
• Submission of monthly program data “snapshots” – e.g., program, referrals, enrollments and discharges.
• Submission of semi-annual data on national CWS, SUD treatment performance measures as well as indicators related to pre-natal substance exposure and CARA and CAPTA requirements:
o CWS: Repeat maltreatment, reunification timeliness, re-entries to OOHC, families have enhanced capacity to provide for their children’s needs, children receive appropriate services to meet their educational, physical, and mental health needs.
o SUD Treatment: Treatment discharge type, substance use.
o Pre-natal Substance Exposure and CAPTA/CARA: Infant health status indicators (e.g., prenatal exposure, NAS/FAS/FASD diagnosis, well-child visits in first 15 months, received recommended vaccinations in first 12 months), notifications to child protective services, number of infants for whom a Plan of Safe Care was developed, and service referral and receipt.
• Participation in qualitative data collection activities (to be carried out by the QIC-CCCT) that will include:
o Key Informant Interviews (conducted in year 2): To document implementation and system changes over time; gather various perspectives on project challenges, impact, and achievements.
o Project Director/Implementation Team/ Partner Survey: To gather longitudinal data from a range of stakeholders.
9

o Direct Observation: To observe key activities, interactions and processes as they occur.
o Document Review: To synthesize information on court teams, their strategies and activities, and progress and challenges in achieving intended goals.
During year one, the QIC-CCCT will collaborate with demonstration sites to develop a sound and feasible data collection and evaluation plan that considers available resources, a need to mitigate new data collection burden on awardees, and the expectation that sites will need to build their evaluation and performance monitoring capacity. Data submission processes will be finalized and implemented in consultation with the CCCTs by the end of year one.
D. Funding Limitations/Allowable Use of Funds The QIC-CCCT will allocate $70,000 per year to each demonstration site. Funds will be made available subsequent to executing a Mutually Binding Agreement between the QIC-CCCT and the applicant lead agency. Mutually Binding Agreements will be reviewed and approved by both the QIC-CCCT and the Children’s Bureau Federal Project Officer. This agreement will delineate the responsibilities of the court teams and the QIC-CCCT and the allowable use of funds. Funds are intended to support each local court team’s site plan implementation. Demonstration site funding cannot supplant existing funds.
The QIC-CCCT envisions the funds will be used primarily to support project implementation, cross-systems training, and travel of the court’s team to the annual All-Sites Meeting. Although there is no match requirement for these funds, it is expected that each demonstration site will utilize existing resources to strengthen services for the target population.
Though the funds are intended to be somewhat flexible to meet the specific needs of the community, applicants should make note of the following potential uses:
• Travel and per diem for the annual All-Sites Meeting in Orange County, Ca. • Staff training on evidence-based parent child interventions • Developmental or other therapeutic services for children • Court coordinator or plan of safe care coordinator (cannot supplant existing funding) • Data collection, performance monitoring and evaluation support
E. Reporting Requirements Applicant agencies selected to participate in the QIC-CCCT must submit both a Semi-Annual Progress Report and a Semi-Annual Financial Report throughout the project period. These reports are due within 30 days of the end of each six-month reporting period. Reporting periods end September 30 and March 31 of each year.
In general, the Progress Reports will include:
• Narrative information on demonstration site’s major activities and accomplishments, program and evaluation challenges, significant contextual events or community changes impacting the QIC-CCCT initiative, key lessons learned, and plans for the next reporting period.
• Quantitative program evaluation and performance monitoring data on core operations and child welfare, recovery, and family functioning outcomes.
10

The Financial Reports will include a comparison of actual expenses to the approved line-item budget, including an explanation for any overages and/or unspent funds and revised budget and budget narrative, where appropriate. Awardees also will be required to submit an overall Final Project Report and Final Financial Report within 30 days of the end of the QIC-CCCT grant. The QIC-CCCT will provide awardees with all required report templates.
F. Assurances QIC-CCCT awardees must fulfill the following:
1. Fulfill all requirements of the Mutually Binding Agreement
2. Participate in the QIC-CCCT project evaluation (see section C. Evaluation Expectations and Requirements)
3. Attend the Annual QIC-CCCT All-Sites Meeting. (See section A. Training, Technical Assistance and Coaching Approach (TTAC))
4. Submit all required progress and financial reports in timely fashion (see section V. Project Budget and Budget Narrative)
5. Initial implementation of site plans by March, 2019
6. Agree to disclose their criteria for program participant inclusion or exclusion and assure a nondiscriminatory approach to service delivery within the jurisdictional confines.
IV. REQUIRED RFP SUBMISSION COMPONENTS This section outlines the required submission components for your main project narrative and budget. Submission components will differ for Pathway 1 applicants. Pathway 1 applicants are eligible to apply in collaboration with up to three local or tribal demonstration sites. Because of the nature of this initiative, and the focus on local implementation efforts, each demonstration site proposed by the state or tribal CIP is required to complete the 7 page Project Narrative and Budget Cost Workbook, and provide the additional supporting documentation described below. Pathway 1 applicants will then be responsible for collecting and submitting project narratives for each site proposed in the application. In addition to submitting applications on behalf of local demonstration sites, Pathway 1 applicants must complete and submit the Pathway 1 Submission Components outlined in Appendix A. Below is a list of submission components for each pathway.
Pathway 1 Applicants Submission Components (please see Appendix A):
• Pathway 1 Application Face Page • Pathway 1 Narrative • Letters of Commitment from state level partners • For each proposed demonstration site:
o Project Narrative o Budget Cost Form o Supporting Documents including:
Contextual Data for Jurisdiction Key staff and team composition table Letters of Commitment from partner agencies
11

Pathway 2 Applicants Submission Components:
• Application Face Page • Project Narrative • Budget Cost Form • Supporting Documents including:
o Contextual Data for Jurisdiction o Key staff and team composition table o Letters of Commitment from partner agencies
Please Note: Pathway 1 applicants should not complete the following sections – Application Face Page Project Narrative Budget and Budget Narrative and Supporting Documents. Pathway 1 submission components can be found in Appendix A.
A. Application Face Page Note: All of the required fields listed below will be incorporated into the designated RFP submission page where you will upload your proposal (see Section VI.B). You do not need to repeat all of this information in your project narrative.
1. Lead Agency: Name, address and contact information of agency or organization that is submitting the application (see Section II.A regarding eligible applicants).
2. Project Director and Primary Point of Contact: Name, Title, Agency/Organization, Address, Phone, Fax, Email
3. County/Tribe/Jurisdiction Served
4. Name of Court Team (if different than lead agency)
B. Project Narrative The total project narrative should not exceed 7 pages. We have provided suggested page limits for each section. The questions below are to intended guide your responses. Applicants are not expected to answer each question directly. Rather, the content of the questions should be integrated into your narrative responses within each section.
Please Note: We recognize that applicants may represent a range of courts and programs (e.g., well established collaborative courts, newly formed collaborative courts and dependency courts wishing to develop collaborative teams in response to this RFP and legislative changes regarding prevention and response to prenatal substance exposure) and that applicants may be at different stages of collaborative court team development and implementation. Therefore, depending on your structure and length of operation, some of the following questions may or may not apply at this time. Please do your best to respond to each section as it applies to your court and jurisdiction.
1. STATEMENT OF NEED (approximately 1 page) Please describe the current trends, needs, and concerns in your community as it relates to infants with prenatal exposure. Describe how these needs have affected the various systems in your jurisdiction, using both recent quantitative data (citing sources or contextual data tables in in Attachment A) and qualitative information. The questions below are provided to
12

help guide your response. However, it is not intended that you answer every individual question.
• Child welfare. Has there been an increase in the number of infants with prenatal exposure? Has there been an increase in number of infants in out of home care? Does your data reflect a trend for termination of parental rights or permanency decisions other than reunification for children under the age of one year related to parental substance use?
• The treatment system. Is there a waiting list for women to enter treatment? What is the availability of evidence-based, culturally-relevant, family-centered treatment for families with infants and children, and their families? What is the availability of medication assisted treatment?
• The healthcare/hospital system. Has there been an increase in infants experiencing Neonatal Abstinence Syndrome, or been affected by prenatal substance exposure? Has there been an increase in length of stay in NICUs or general pediatric wards due to more babies born with effects of prenatal substance exposure?
• Services. What are the services, supports, and other needs of pregnant and postpartum women with substance use disorders, their infants, families, and caregivers in your community? What services gaps exist in your community for these families?
2. GOVERNANCE AND LEADERSHIP (approximately 1 page) • Briefly describe your current governance structure by addressing the following
questions (if you do not yet have a formal governance structure, please skip to the next question):
a) When was it established? b) How often does it meet? c) How are court program and policy decisions made? d) What standing agenda items do you typically discuss? e) Which systems/agencies are represented? f) Who actively and regularly participates?
• If you do not yet have a formal governance structure in place, describe your proposed governance structure. Please explain any challenges or barriers that you anticipate in implementing a formal governance structure.
• Describe the leadership of your court. Who are the formal and informal leaders that drive effective collaboration, communicate the court program vision, mobilize resources, advocate for participants, etc.? Which systems do they represent?
• Do you anticipate any turnover in judicial or other key leadership positions that may impact your court? How will you address the turnover?
3. COLLABORATION and PARTNERSHIP (approximately 1 page) • Briefly describe your court’s core team. Who are the key partners and operational
team members? What are their primary roles?
13

• Briefly describe how your key partners currently work together to coordinate and integrate services, at both the individual client level as well as the larger systems level. What policies or practices are in place to facilitate cross-systems information sharing and coordinate/integrate the substance use disorder recovery plan, the child welfare case plan, and other services children and families receive?
• What agencies/service providers do you feel are missing and need to be added to your court team to more effectively meet the needs of infants and families? What will it take to engage them as active partners, especially health care providers and hospitals?
4. CAPACITY and READINESS (approximately 2 pages) Implementation of CARA amendments to CAPTA. Please describe your community’s current practices, challenges and gaps related to implementing the CARA amendments to CAPTA including:
• Identifying infants as being affected by substance abuse or withdrawal symptoms resulting from prenatal drug exposure, or a Fetal Alcohol Spectrum Disorder.
• Notifying child protective services of the occurrence of such infants. • Developing a plan of safe care for such infants that addresses the health and substance
use disorder treatment needs of the infant and affected family or caregiver. • Referring children under age 3 who are involved in a substantiated case of child abuse
or neglect to early intervention services funded under Part C of the Individuals with Disabilities Education Act.
Treatment Services and Court Operations. Please describe your community’s strengths, challenges and gaps related to substance use disorder treatment for pregnant and parenting women and other family members including:
• Current practices for identification, screening, assessment and referral of pregnant women, parents with substance use disorders, and infants affected by prenatal substance exposure. Briefly describe how children are identified and access early intervention and other developmental services. What type of standardized screening and assessment processes do you use and at what point in the family’s involvement with child welfare and/or the court?
• The continuum of treatment and recovery support services available to your court, particularly for pregnant women and parents. What is the current capacity for pregnant and parenting women to attend residential treatment with their children?
• How your court team and partners ensure that parents obtain timely access to treatment, including medication assisted treatment. What policies, practices, or processes are in place to facilitate timely treatment entry?
• The number and array of community treatment providers your court team works with. When it comes to communicating and coordinating with treatment providers, what are the major strengths and areas needing improvement?
Evaluation, Performance Monitoring and Continuous Quality Improvement. Please describe your proposed or existing team’s strengths, challenges and gaps related to accessing, collecting, managing and using performance data for continuous quality improvement including:
14

• What formal agreements, practices, or protocols are currently in place to share data across systems at both the individual/family level (e.g., case level data on children and adults) and systems level (e.g., aggregate measures representing the jurisdiction or program)? How long have those agreements, practices, or protocols been in place? What do they include (e.g., outline roles/responsibilities, confidentiality, access)?
• Identify the data systems in your jurisdiction that house data on child welfare, substance use disorder and prenatal substance exposure. Please refer to section II.C - Evaluation Requirements and Expectations for information on data relevant to this project.
• What are the primary barriers or challenges you are currently experiencing with accessing and sharing data across systems?
• What are the performance measures that your court and its key partner agencies currently collect to help determine the effectiveness of your court?
• What additional indicators would you need to add as a demonstration site to measure your progress in meeting the goals of the QIC-CCCT initiative?
5. MISSION, GOALS, STRATEGIES, AND COMMITMENT (approximately 2 pages)
Please Note that we do not expect applicants to have a final, detailed implementation plan in place that specifies exactly how you plan to meet the goals of the initiative. The QIC CCCT Team will work with sites on implementation plans during the site plan development phase. However, we do expect that the applicant teams and their partners have engaged in discussions about potential strategies for meeting the goals of the initiative and have begun to explore possible options, assess their capacity and readiness, and identify key implementation factors that need to be considered to move forward.
• Briefly summarize what your team hopes to achieve by participating in the QIC-CCCT including:
o What are your primary goals and what are the major program practice improvements you hope to achieve in order to serve the target population of the QIC-CCCT?
o What strategies do you plan to implement to achieve your goals? o What are the one or two major barriers, whether internal among partner agencies
(e.g., different timetables, conflicting values or policies) or contextual (e.g., system reorganizations, changes in judicial leadership, state legislation), that might adversely affect the success of your QIC-CCCT effort?
V. Project Budget and Budget Narrative Applicants are required to provide an estimated or projected 30-month budget for the proposed CCCT initiative. QIC-CCCT recognizes that first year activities will contain costs associated with expected planning and development functions (e.g., labor, consultants, training, travel, etc.) to allow for specific implementation issues and exact budget information to be finalized during the planning and development year. The Project Budget Cost Form does not count towards your
15

7-page limit. Please use the Proposal Budget excel workbook (Attachment D – QIC-CCCT Budget Cost Form) to prepare your project budget, which contains the following two worksheets:
1. Budget Form: The form on which the proposed budget must be submitted via excel file (and named “Attachment D_QIC-CCCT_Budget Cost Form”). This form includes automatic summing by category and across years.
2. Budget Narrative: Contains the instructions for preparing the Budget Narrative, which must accompany the Budget Cost Form.
The total project period will be from April 1, 2018 to September 29, 2020. Year 1 will be from April 1, 2018 to September 29, 2018; Year 2 will be from September 30, 2018 to September 29, 2019; Year 3 will be from September 30, 2019 to September 29, 2020.
The cost of the project should be divided into:
1. Amount requested per year from QIC-CCCT. The total amount must equal no more than $210,000 and be allocated as $70,000 per contract year (2018, 2019 and 2020).
2. Other funding for the project.
Use only those budget categories that are applicable to your project. You can eliminate and/or add categories as needed.
Note: Applicants must allocate sufficient funds in the budget to support required travel of their QIC team to the three QIC all sites meetings.
VI. SUPPORTING DOCUMENTS • Contextual Data for Jurisdiction - See Attachment A for template and instructions
• Key staff and team composition table – See Attachment B for template and instructions
• Letters of Commitment from Partner Agencies – See the list below for required Letters of Commitment. Letters of Commitment from other partner agencies and parent or child attorneys are recommended and may be included. These letters must describe the agency’s commitment to participate, their contributions to the initiative, and what they expect to achieve.
o Court Improvement Program or Designated Lead Tribal Agency
o Chief or Presiding Judge 3
o Child Welfare Agency
o Substance Abuse Treatment Agency/Provider(s)/Women’s Treatment
o Public Health: Maternal and Child Health
o Maternal and Infant Healthcare Providers
3 The QIC-CCCT recognizes that in certain situations, Judges may not be in a position to bind the court to an agreement. If this is the case, letters of commitment from court or tribal administrators, court clerks, or other individuals the applicant deems best suited to bind the court to an agreement can be substituted for a letter of commitment from the Chief/Presiding Judge.
16
VII. SUBMISSION PROCESS A. Required Formatting All elements of the Project Narrative (Section IV) must be in 12-point Times New Roman font, with standard one-inch margins (left, right, top and bottom). The narrative can be single- or double-spaced. All pages of the Project Narrative should be sequentially numbered. Please use the Project Narrative Template to submit Project Narratives. The Project Narrative Template also contains fillable tables for Attachment A and Attachment B. The Project Narrative Template and all other submission documentation can be downloaded here: https://www.cffutures.org/qic-ccct_demonstration-sites/.
B. How to Submit Applicants should use the Project Narrative Template to submit applications. Your proposal must be submitted electronically via https://www.cffutures.org/qic-ccct_rfp-2/. If you are unable to submit an application electronically, please contact us at [email protected] and we can make alternate arrangements.
Please submit the Project Narrative (which should include Attachment A and B in the same document) and accompanying Budget Cost Form and letters of commitment as separate attachments. All templates and submission documentation can be found here: https://www.cffutures.org/qic-ccct_demonstration-sites/.
C. Date and Time Completed submissions must be received by 5 p.m. Pacific Standard Time (8PM Eastern Standard Time) on February 23rd, 2018.
D. Important Links:
• All submission documentation and instruction on how to submit can be found here: https://www.cffutures.org/qic-ccct_demonstration-sites/
• Application submission page: https://www.cffutures.org/qic-ccct_rfp-2/
VIII. REVIEW CRITERIA
Please Note: Reviewers will not access, or review, any materials that are not part of the application documents. This includes information accessible on websites via hyperlinks that are referenced, or embedded, in the application. Though an application may include web links, or embedded hyperlinks, reviewers will not review this information as it is not considered to be part of the application documents. Reviewers will score an application based on the documents that are presented in the application. Reviewers will apply the following criteria:
Statement of Need (Maximum 10 points) 1. Clearly articulates the current trends, needs, and services gaps as it relates to infants with
prenatal exposure and their parents/caregivers affected by substance use disorders. Presents data that demonstrates the current situation and need from the child welfare system, substance use disorder treatment system, and the healthcare/hospital system.
17

Governance and Leadership (Maximum 10 points) 1. Has an established governance structure in place, or proposes a governance structure to
implement and oversee the work of the collaborative court team with strong, committed leadership that will provide continued support for the court team.
Collaboration and Partnership (Maximum 10 points) 1. Clearly describes core team partners and current practices that facilitate cross-system
information sharing and coordination/integration of services to children and families. Has identified missing partners that may be needed to serve infants and families affected by prenatal substance exposure. Application includes letters of commitment from key partners.
2. Describes how the key partners work collaboratively to coordinate and integrate services, at both the individual client level as well as the larger systems’ level.
Capacity and Readiness (Maximum 35 points) 1. Demonstrates a clear understanding of the current implementation of CAPTA, as
amended by CARA, including the status of implementation within the court’s jurisdiction or statewide, and the gaps and challenges in implementing the core requirements of CAPTA as it relates to infants and families affected by prenatal substance exposure. The core requirements are:
• Identifying infants as being affected by substance abuse or withdrawal symptoms resulting from prenatal drug exposure, or a Fetal Alcohol Spectrum Disorder
• Notifying child protective services of the occurrence of such infants
• Developing a plan of safe care for affected infants and their affected family or caregiver
2. Describes current practices for identification, screening, assessment, and referral of pregnant women, parents with substance use disorders, and infants affected by prenatal substance exposure.
3. Describes how children are screened and referred for early intervention and other developmental services.
4. Provides timely and quality substance use disorder treatment, including Medication Assisted Treatment and essential related support services to parents to promote and sustain their recovery. Identifies challenges in accessing timely and effective substance use disorder assessment and treatment services.
5. Demonstrates that a thorough self-assessment of the strengths and weaknesses of current cross-systems data collection, evaluation, and performance monitoring capacity has been conducted. The applicant adequately describes gaps and challenges with the existing data and information-sharing infrastructure and demonstrates readiness and capacity to become a data-driven collaborative.
Mission, Goals, Strategies (Maximum 35 points) 1. Has articulated a clear vision for what the collaborative ultimately wants to achieve as a
result of the QIC-CCCT opportunity and why this is an opportune time to advance the
18

team’s efforts. The core team and partners outline agreed-upon primary goals and key implementation steps that align with the overall mission of the QIC-CCCT initiative.
2. Has proposed strategies to address identified gaps and needs in services to infants, children, and their families. Potential to leverage existing community partners to provide and sustain needed parenting and children’s services.
3. Identifies potential barriers that may impact implementation and identified goals, and planned strategies to address these barriers.
4. Demonstrates clear commitment, support, readiness and capacity—from the leadership and partners at all levels—to actively engage in the QIC-CCCT initiative and improve the way the systems work together on behalf of infants with prenatal substance exposure and families affected by substance use disorders and child maltreatment.
IX. Site Selection Process Completed proposals are due February 23rd, 2018. All submissions will be reviewed for technical compliance. Eligible proposals will be reviewed by a panel, based on the criteria outlined above. Following submission and review of proposals, the QIC-CCCT will select and invite applicants to participate in a conference call with QIC-CCCT staff. The purpose of the calls will be to ensure applicants have a clear understanding of the QIC-CCCT initiative expectations and are fully committed to the project. QIC-CCCT project staff will ask for clarification on any issues identified through the application review process, and identify initial TTAC needs. Final selection of demonstration sites will take into account results from the entire review process, applicant level of need, geographic distribution of applicants, and cultural diversity of their target populations. The QIC-CCCT anticipates final selection of the 15 demonstration sites by the end of March, 2018. Applicants will be notified and award letters sent out by March 31st, 2018.
19

Appendix A: Pathway 1 Application Submission Components Pathway 1 applicants are eligible to apply in collaboration with up to three local or tribal demonstration sites. Because of the nature of this initiative and the focus on local implementation efforts, each demonstration site proposed by the state or tribal CIP is required to complete the 7 page Project Narrative, the Budget Cost Workbook, and provide the additional supporting documentation described above in the full RFP. Pathway 1 applicants will then be responsible for collecting and submitting project narratives for each site proposed in the application. In addition to submitting applications on behalf of local demonstration sites, Pathway 1 applicants must submit the sections outlined below.
For more information on the role of the Pathway 1 applicants, please see the Section III.B – Collaboration.
You can download the Pathway 1 Applicant Template along with all other submission documentation here: https://www.cffutures.org/qic-ccct_demonstration-sites/
A. Pathway 1 Application Face Page State or tribal CIP, or Tribal Government Information
Name:
Address:
County/Tribe/Jurisdiction Served:
Project Director and Primary Point of Contact
Name:
Title:
Agency/Organization:
Address:
Phone:
Email:
Proposed Demonstration Sites: Please use the table below to provide information on the demonstration sites you are proposing for the initiative.
Demonstration Site Lead Agency
Contact Person/ Program Liaison
Jurisdiction Served (county or counties)
B. Pathway 1 Narrative Please respond to the questions below. The narrative should not exceed 2 pages.
20

1. Briefly describe your rationale for proposing the local demonstration sites in this application. How will these specific sites benefit from participation in the QIC-CCCT initiative?
2. Briefly describe your role as the lead applicant agency. Your answer may address questions such as: How will you ensure consistent and ongoing communication with the local demonstration sites? How will you oversee local implementation efforts? How will you obtain feedback from demonstration sites and make adjustments accordingly?
3. Please use the table below to identify your proposed state level partners who will be members of the executive committee and briefly describe their primary roles (add rows as needed).
State Level Partner
Description of primary role
4. Do you plan on using any of the demonstration site funds to support your role as lead agency? If so, please indicate the amount and describe how you will use these funds to support the overall objectives of the QIC-CCCT initiative.
5. How does the QIC-CCCT initiative align or fit with the state’s/tribe’s priorities or other initiatives related to the needs of infants, young children, and their families/caregivers affected by SUDs and prenatal substance exposure?
6. How will you disseminate effective demonstration site strategies to other courts in your state or tribe?
C. Supporting Documents for Pathway 1 Applicants
Please list your letters of commitment from state level partners listed above. For more information on expected state level partners, please see Section III.B – Collaboration.
21
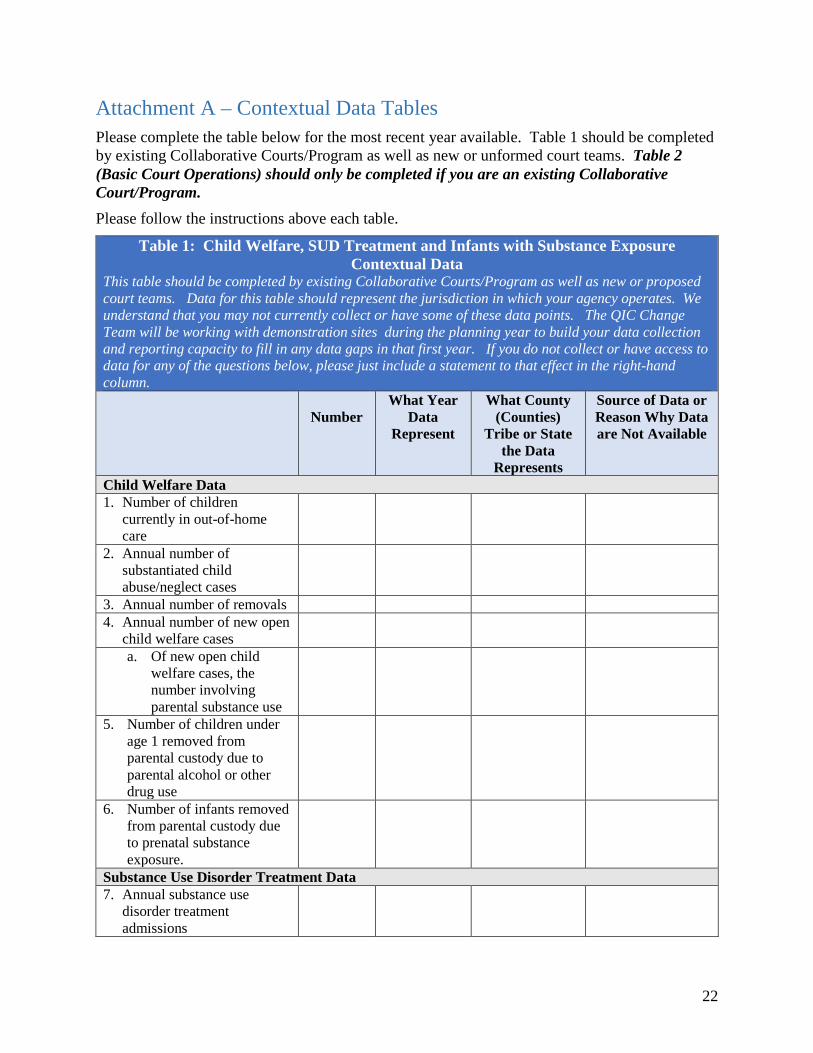
Attachment A – Contextual Data Tables Please complete the table below for the most recent year available. Table 1 should be completed by existing Collaborative Courts/Program as well as new or unformed court teams. Table 2 (Basic Court Operations) should only be completed if you are an existing Collaborative Court/Program. Please follow the instructions above each table.
Table 1: Child Welfare, SUD Treatment and Infants with Substance Exposure Contextual Data
This table should be completed by existing Collaborative Courts/Program as well as new or proposed court teams. Data for this table should represent the jurisdiction in which your agency operates. We understand that you may not currently collect or have some of these data points. The QIC Change Team will be working with demonstration sites during the planning year to build your data collection and reporting capacity to fill in any data gaps in that first year. If you do not collect or have access to data for any of the questions below, please just include a statement to that effect in the right-hand column.
Number
What Year Data
Represent
What County (Counties)
Tribe or State the Data
Represents
Source of Data or Reason Why Data are Not Available
Child Welfare Data 1. Number of children
currently in out-of-home care
2. Annual number of substantiated child abuse/neglect cases
3. Annual number of removals 4. Annual number of new open
child welfare cases
a. Of new open child welfare cases, the number involving parental substance use
5. Number of children under age 1 removed from parental custody due to parental alcohol or other drug use
6. Number of infants removed from parental custody due to prenatal substance exposure.
Substance Use Disorder Treatment Data 7. Annual substance use
disorder treatment admissions
22

a. Of annual treatment admissions, number that were child welfare referrals or involved parents in the child welfare system
b. Of annual treatment admissions, the number of women who entered treatment
c. Of annual treatment admissions, the number of pregnant women who entered treatment
Infants with Substance Exposure/CARA and CAPTA Data 8. Number of births with
prenatal substance exposure
9. Number of notifications to child protective services for infants born with and identified as being affected by substance abuse or withdrawal symptoms resulting from prenatal drug exposure, or Fetal Alcohol Spectrum Disorder
10. Number of infants for whom a Plan of Safe Care was developed
11. Number of infants for whom a referral was made for appropriate services---including services for the affected family or caregiver, as may be necessary
12. Number of children under the age of 3 who are involved in a substantiated case of child abuse or neglect referred to and receiving early intervention services funded under Part C of the Individuals with Disabilities Education Act.
23

Table 2 – Basic Court Operations Data for this table should represent your specific Collaborative Court/Program. This table should be filled out only if you are an existing Collaborative Court/Program. General Information
1. Date (month/year) your collaborative court team began:
2. Capacity 1. Total number of participants you are able to
serve at a given time (total capacity): Parents: Children: Families:
2. Number of participants you currently serve: Parents: Children: Families:
3. Number of participants you serve in a year (on average):
Parents: Children: Families:
3. Average time from when a parent is referred to your collaborative court to the time that they formally enroll:
4. Average duration of your collaborative court program:
5. Total number of parents discharged from your collaborative court in 2017 (or your most recent complete program/fiscal year):
Of parents discharged, please indicate (modify categories as needed based on how you collect data)4
1. Number of successful collaborative court program discharges or graduations:
2. Number of neutral discharges 3. Number of unsuccessful discharges (e.g.,
dropouts or terminations):
6. Participants’ average length of stay in your court (among all discharge reasons):
7. Number of women pregnant at court enrollment (among females):
4 In general, “successful” discharge includes graduation or dependency case closed due to reunification, or children remaining at home, while “unsuccessful” discharge includes failure to complete court requirements, left against staff advice, parental rights were terminated, or incarcerated for reasons connected to their child welfare case. “Neutral” discharges may include participant moved outside of court jurisdiction, dependency case closed for reasons other than those listed in successful/unsuccessful exits, leaves upon staff and participant consensus that the collaborative court is not a good fit, or incarcerated (for reasons not connected to their child welfare case).
24

Attachment B – Key Staff and Team Composition Table Please refer to Section II part D for team descriptions and suggested members. This is a preliminary list of members and can change as necessary. Please include their name, title, and agency affiliation. Add rows as needed.
Name Agency Title
Core Team Members
25

Attachment C – The Five Point Intervention Framework Policy and Practice Framework for Prenatal Substance Exposure: 5 Points of Intervention for Children and Families was developed by the National Center on Substance Abuse and Child Welfare and funded by SAMHSA and the Administration on Children, Youth, and Families. This framework serves as a comprehensive model that identifies five major time frames when intervention in the life of an infant can help reduce the potential harm of prenatal substance exposure. The five intervention points are:
• PRE‐PREGNANCY: This timeframe offers the opportunity to promote awareness of the effects of prenatal substance use among women of child‐bearing age and their family members;
• PRENATAL: This intervention point encourages health care providers to screen pregnant women for substance use as part of routine prenatal care and make referrals that facilitate access to treatment and related services for women who need those services;
• BIRTH: Interventions during this timeframe incorporate testing newborns for substance exposure at the time of delivery;
• NEONATAL: Developmental assessment and the corresponding provision of services for the newborn as well as the family at this intervention point, immediately after the birth event, are the emphasis; and
• THROUGHOUT CHILDHOOD AND ADOLESCENCE: This timeframe calls for ongoing provision of coordinated services for both child and family.
The 5 Five Points of Intervention Framework was the organizing foundation for the SAMHSA report Substance-Exposed Infants: State Responses to the Problem. The framework also informed the guidance document A Collaborative Approach to the Treatment of Pregnant Women with Opioid Use Disorders: Practice and Policy Considerations for Child Welfare, Collaborating Medical, and Service Providers. Use the links below to access both documents.
A Collaborative Approach to the Treatment of Pregnant Women with Opioid Use Disorders: Practice and Policy Considerations for Child Welfare, Collaborating Medical, and Service Providers (PDF 1.53 MB) Substance Abuse and Mental Health Services Administration, Children’s Bureau, 2016 Substance-Exposed Infants: State Responses to the Problem (PDF 1.50 MB) Substance Abuse Mental Health Services Administration, 2009
26

Attachment D – QIC-CCCT Budget Cost Form The QIC-CCCT requires the applicant to provide detailed budget information on the proposed project. Please complete the excel form and submit it with your application. The form, along with all other submission documentation can be found here:
https://www.cffutures.org/qic-ccct_demonstration-sites/
27

i Substance Abuse and Mental Health Services Administration. (2014). Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings. NSDUH Series H-48, HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration. ii Patrick, S. W., Schumacher, R. E., Benneyworth, B. D., Krans, E. E., McAllister, J. M., & Davis, M. M. (2012). Neonatal Abstinence Syndrome and Associated Health Care Expenditures United States, 2000-2009. JAMA: Journal of the American Medical Association, 307(18), 1934-1940. iii Patrick, S. W., Davis, M. M., Lehmann, C. U., & Cooper, W. O. (2015). Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009 to 2012. Journal of Perinatology, 35(8), 650-655. doi:10.1038/jp.2015.36 iv https://www.cdc.gov/vitalsigns/fasd/index.html v Mactier, H. (2013). Neonatal and longer term management following substance misuse in pregnancy. Early Human Development, 89(11), 887-892 vi Belcher, H. M. E, Butz, A. M., Wallace, P., Hoon, A. H., Reinhardt, E., Reeves, S. A., & Pulsifer, M. B. (2005). Spectrum of early intervention services for children with intrauterine drug exposure. Infants and Young Children, 18(1), 2-15
vii U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Office of Applied Studies. (2009). The NSDUH Report: Children living with substance-dependent or substance-abusing parents: 2002-2007. Rockville, MD: Author.
viii Wulczyn, F., Ernst, M., & Fisher, P. (2011). Who are the children in out-of-home care? An epidemiological and developmental snapshot. Chicago, IL: Chapin Hall at the University of Chicago.
ix U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2017). Child Maltreatment 2015. Available from http://www.acf.hhs.gov/programs/cb/research-data-technology/statistics-research/child-maltreatment. xChildren and Families Futures. (2013 rev 2015). Guidance to States: Recommendations for Developing Family Drug Court Guidelines. Prepared for the Office of Juvenile Justice and Delinquency Prevention, Office of Justice Programs.
28