nca nosocomial covid-19 infection prevention collaborative
TRANSCRIPT

NCA Nosocomial COVID-19 Infection
Prevention Collaborative
Change Package
What we have learnt so far
Version 1 20/10/2020

2
Introduction
COVID-19 is a novel “new” coronavirus:
• CO – stands for coronavirus
• VI – stands for virus
• D – stands for disease
• 19 – stands for the year the virus was first detected
Therefore, the scope of this collaborative is to prevent the acquisition of COVID 19 across
all of our care organisation sites.
We define a nosocomial COVID infection
across the NCA as:
Probable cases: Admitted in last 8-14 days
Definite cases: Admitted in last 15+ days
What is a Nosocomial Infection?
Definition:
A nosocomial infection is defined as a disease that originated in hospital.
There are many types of human coronaviruses that commonly cause mild upper
respiratory illnesses
Typical Symptoms of Coronavirus
Tiredness
High Fever
Loss of taste or smell
Difficulty Breathing
Dry persistent coughing
How is it spread?
Respiratory droplets
Coughing
Sneezing
Close contact
Surfaces

Scale of the problem
In March 2020, a global pandemic, never to be seen before in this modern time, was
declared.
Cases of COVID-19 escalated rapidly around the UK, with the Northern Care Alliance
being one of the worst hit sites in the UK based on the number of confirmed cases and
deaths.
Staff have worked tirelessly amongst escalating cases and uncertain times and achieved
so much throughout the COVID 19 pandemic. However, we know a number of patients
have acquired COVID 19 on our sites and a number of these patients have died.
The average age of patients whom contracted a HACI and sadly died is 84 – our most
vulnerable patients.
We achieved across July and August up to 75 days without a nosocomial COVID 19
infection at a number of our sites. Now, as we head into a second wave and prevalence
of COVID 19 in our NCA communities is increasing, we are also seeing an increase in
nosocomial COVID 19 infections across all of our sites.
What are we doing?
In July 2020 we launched the COVID 19 Nosocomial Infection Collaborative. It is
designed to unite the Northern Care Alliance organisations in a shared purpose to
achieve no nosocomial COVID 19 infections across all sites and community settings.
The collaborative aimed to help staff to understand the rationale behind the required
IPC measures and do their utmost to avoid transmissions in all aspects of their daily
routines including both patient facing and not patient facing
The aims of the Nosocomial Infection collaborative are:
That there are no nosocomial infections across all of our sites
To go 100 days without a nosocomial infection
Timeline of events
1st Expert Faculty Meeting
July
Launch Event
July
Learning Session 2
September
Learning Session 3
November
Supporting Structure
NCA Expert Faculty Care Org Steering
Groups Collaborative Teams
We truly are living in unprecedented times. Covid-19 is a new disease, and we are grappling daily with learning to manage it. We are contributing to research and putting that into practice at incredible speed. The very nature of a pandemic adds a new dimension to our work. Our whole lives are upside down. We are afraid – for our loved ones, our patients, our friends, our own security in life. Nothing is certain right now. But,
We are the key workers that stepped up to the challenge in the 1st wave. We were applauded, gifted and praised for our efforts. We worked so hard for our patients, our loved ones, ourselves. We are stronger than we seem, braver than we believe. When our processes fail the price is high – not just to those who are infected with Covid-19 but also the impact on services from sickness, from staff isolation. On the staff covering extra shifts. On those who have to shield. Now as we head into a second wave, we know more about how to prevent the spread of COVID 19 and we know we need to be vigilant in our approach. We still don’t know for sure all the answers but we are not without knowledge and skills. We understand reliability – that we need to make the fundamentals of care as simple as we can, so routine that it happens unthinkingly. That frees us up to feel, to learn new things, to grapple with the challenges we face. WE know that when a patient comes to hospital, a clinic, lets us into their environment, they are trusting us even more than they have before. They trust that we are doing everything we can to protect them. Our colleagues trust that we are doing everything we can to protect each other. We are the NCA family, we know we can rise to this challenge like we have risen to so many before. This is the place where we care and are safe, secure and here for you.
Why is this Change Package so important?

We ALL have our part to play in Infection Prevention
Control (IPC) and breaking the chains of
transmission.
By implementing the proposed change ideas in this change package, we
can reduce the risk of transmission of COVID-19 across our sites.

Quality Improvement Methodology
The collaborative followed the Breakthrough Series Collaborative Model using learning
sessions to bring teams together to share tests of change and introduce quality
improvement methodology.
The collaborative used the Model for Improvement to provide a clear aim, structure and
driver diagram to guide improvement work.
By using this methodology we recognise that in healthcare, we could not make the
necessary improvements that our patients deserve without the skills, knowledge and
expertise of dedicated staff. Through this collaborative, we want to empower our staff to
test their change ideas and spread successful improvements across the organisation.
Our driver diagram

Over 100 teams across all NCA sites are engaged in the collaborative, a phenomenal
response. Given the limitations of IPC the collaborative is being run via a virtual
platform, improving accessibility to it.
Teams were asked to complete PDSAs within one of the following 5 themes:
What we have done so far?
Environment Hygiene
and Cleanliness
Personal Protective Equipment
(PPE)
Health and Safety
Visiting
Where are we now?
The Nosocomial infection collaborative has reached a crucial point in the improvement
cycle where the tests of change developed by staff are beginning to be shared; the
collaborative focus is shifting to the spread and sustained roll out of the key changes
which we believe are likely to result in improvement.
An audit tool has been rolled out – please contact the QI team for the most up to date
version.
The proposed changes within this change package have been compiled
from tests that have been developed across the collaborative teams, as
well as learning from acquisitions. We believe that if they are applied in
your area the risk of a Nosocomial COVID 19 infection will be reduced.

Change Package
A Change Package is a group of changes which, when
adopted, will address a particular problem.
This Change Package has been designed using preliminary evidence to
provide teams with the necessary toolkit to reduce Nosocomial Infections,
specifically COVID-19.
There are 5 key themes highlighted as areas of focus. These themes are
listed below and dictate the Change Package items which are described in
the following pages:
Environment Hygiene
and Cleanliness
Personal Protective Equipment
(PPE)
Health and Safety
Visiting
It’s important to remember that you are not alone in your QI journey.
Teams across the NCA have actively participated and tested the changes
listed within this package and is a great resource to use for advice,
support, shared learning and understanding the rationale behind each of
the change items.
“Know that we can have more freedom tomorrow.
The actions we take today, will preserve our
tomorrow” World Health Organisation (WHO)

This change package can be used to:
• Identify which of these changes already exist within your areas; if they do,
do they require further work? If they do not, you may consider
implementation.
• Highlight and prioritise some changes that your team may begin testing
around each theme. Remember that testing takes time in order to build
reliable systems and that not all tests of change lead to improvement. It is
just as valuable to learn from what did not work as it is to learn from what
did work. You can adapt your change ideas to suit your area.
• Map out and prioritise what other changes need to take place within your
areas and devise a plan to get started. A great tool for this is the Model for
Improvement, it acts as a compass to identify your starting baseline point
and guide you in the right direction for your improvement ideas.
Based on the 5 key themes, teams were asked to conduct PDSA cycles to
address the issues that fall within these categories. We have picked out the
proposed change ideas based on current evidence and listed them in the table
below (table 1.0).
The Model for Improvement provides the foundation to any tests of change
Theme Change
Environment • Visual aids
• Social distancing
Hygiene and cleanliness • Making clean visible
• High touch Cleaning rota
PPE • Checklists
• C19 Champions / Role Allocation
Health and Safety • Room Capacity risk assessments
Visiting • Visitor ID Badges
Table 1.0

NCA Nosocomial Infections Collaborative
Change Package
Theme 1: Environment
Visual Aids WHY: This is arguably one of the most essential changes we can make. Ensuring our
surroundings give off constant reminders of what is acceptable and what is not can
reinforce the IPC guidance and impact the behaviours of ourselves, our colleagues as
well as patients and visitors.
WHO: Every team, clinical and non—clinical, should have the appropriate signage,
informative posters and guidance displayed upon entrance and exit to and from their
areas, within break rooms and bathrooms
WHAT: The aim is to ensure every member of staff, patient or visitor is aware of the level
of IPC standard that is expected of them within said area.
WHERE: All areas must reflect the IPC standards. Clinical and non-clinical settings,
including break rooms, kitchens, bathrooms and offices.
Does your environment, both working and off duty, reflect the correct information and
guidance? Do the surroundings of the estate enable you to minimise risk of transmission
and comply with IPC guidelines?
Examples of posters

Social Distancing WHY: This is a key change that has been advised not only within the NCA, but the NHS
as a whole, nationally and even globally as a safety precaution to reduce risk of
transmission from one individual to another.
WHO: Every single staff member regardless of role, should be socially distanced from
their colleagues and patients and visitors where possible*. Visitors and patients need to
remain socially distanced at all times i.e. when in outpatient waiting rooms, corridors etc.
*it is understood that clinical staff cannot socially distance themselves from their
colleagues or patients in a setting where care and treatment is being delivered.
This is mitigated by wearing adequate levels of PPE.
WHAT: The aim is to ensure we are following national guidance and distance 2 metres
apart where possible to prevent unnecessary risk of transmission as we are aware of the
science behind this virus being airborne; this distancing can help us to reduce the rates
of nosocomial infection.
WHERE: Every environment that is not restricted by delivery of care should have socially
distanced forcing functions in place. Be this the removal of chairs, or reducing the
number of people working in an office by removing computers. This is also to be
practiced in areas of down time such as kitchens, break rooms and includes the
outdoors.

Case Study
Independent Living Services
Salford Royal Foundation
The Independent Learning Services team at SRFT explored how
they could make their environments safer and IPC compliant. They
put measures in place to reduce the use of offices by a number of
different teams from different organisations. They identified ‘hot’ and
‘cold areas’ all around the building and displayed the appropriate
signs and posters informing of IPC guidelines. The ILS team also
created one way systems in their building to try and control the
influx of traffic coming into and out of the building which reduces the
number of people building up or gathering in any one area
Theme 1: Environment

Theme 2: Hygiene and Cleanliness
Making clean visible – ‘I’M CLEAN’ stickers WHY: This change idea allows all staff members, patients and visitors to know what date
and time the items they come to use have been cleaned. This is important as we are
aware from the science again, that there is a risk of transmission from surfaces.
WHO: Every staff member is responsible for the cleanliness of their areas, equipment
and work surfaces.
WHAT: The aim is to reduce transmission from contaminated, unclean surfaces and
make clean visible.
WHERE: All areas clinical and non-clinical.
HOW: Stickers are available from procurement as a normal stock purchase item.
High touch cleaning Rotas WHY: This change idea is an additional cleaning rota on top of the regular day to day
cleaning which takes place already. This adds a further layer of assurance that high
standards of hygiene and cleanliness are reached in compliance with IPC guidance and
reduce risk of transmission from unclean surfaces and equipment.
WHO: Each team clinical and non clinical is able to devise a rota to share and allocate
between their colleagues.
WHAT: The aim is to reduce transmission from contaminated and unclean surfaces.
WHERE: All areas clinical and non-clinical.
HOW: Rotas can be devised within each team based on their individual schedules.
Teams may choose set times in the day to carry out this cleaning i.e. setting alarms,
ringing bells (see case study).
Case Study
Outpatients Department
Rochdale and Bury Care Organisation
The Outpatient Department at BARCO aimed to ‘make clean
visible’ for ensuring patients and users were aware and at ease
knowing when cleaning had last taken place in the department.
The team would update a notice board with the date and time of
when high touch cleaning was carried out. Waiting area chairs
were cleaned regularly in between clinics using the cleaning
equipment they have been provided with. This is an additional
layer of cleaning as the Domestics team had assured the OPD of
their evening cleaning, however the day time and in between
clinic cleaning was an extra step the team had to embed.
Theme 2: Hygiene and Cleanliness

Case Study
Ward B3 Salford Care Organisation
• Ward B3 is a Comprehensive stroke unit with high turnover of
admission and discharge with multiple investigations. For this reason, there are a lot of staff who access this ward. This led to increased risk of COVID transmission via contact with high touch areas.
• During COVID-19 the senior management team on HASU decided to incorporate cleaning high touch areas into our daily ward cleaning .
• They picked particular times to cover both day/night for the clean to take place – 10:15, 14:15, 18:15 and 22:15. All staff were made aware and was discussed at their safety huddles.
• On the day of roll out, they decided to get everybody's attention, they would ring a bell to alert everyone that it was ‘time to clean’.
“We had a good response to the cleaning especially from nurses/care support workers and the therapy team. It was harder to get the medical team involved but after a few days they eventually came on board and got involved”. • The team have decided to continue with this and aim to make this
the new normal so that it continues post COVID-19 • They will audit using a sign in sheet which the ward coordinator
will complete each shift • They next plan to engage B4 in preparation for the merge of the 2
wards and include SRU to aim for a standardised approach across stroke services
Theme 2: Hygiene and Cleanliness

Theme 3: Personal Protective Equipment (PPE)
Checklists and C19 Champions/Role Allocation WHY: Personal Protective Equipment (PPE) is absolutely essential to protect all those on
site from infectious agents and reduce the rate of transmission by minimising the risk of
spread.
Checklists are a useful tool for ensuring that the right PPE is used on each area and for
each task.
To allocate a role on a rotational basis within the team, allows each individual to be
educated on the IPC guidelines as they monitor their colleagues against PPE
compliance.
It should be emphasised that there is a component of psychological safety linked to
challenging the use of PPE; this should be addressed as part of this change and
supported by the leadership team. Some teams have resorted to scripted challenges and
slogans (“It’s cool to call out”).
WHO: Each staff member within the team is responsible for complying with PPE and
challenging colleagues who are not compliant.
WHAT: The aim is to reduce transmission by ensuring all staff members are compliant
with the adequate levels of PPE that is dictated by the environment they find themselves
in at any given moment.
WHERE: All areas clinical and non-clinical. Indoors and outdoors.
HOW: All PPE is provided by the Trust and a checklist can be devised internally based
on the area you are. Guidance can be found on the intranet as it is consistently changing
and updated.
Rochdale Care Organisation

Case Study
Rochdale Care Organisation
Rochdale Care Organisation have been actively involved in the PPE
Test of change by allocating roles as ‘C19 Champions’. These roles
are responsible for using checklists to monitor themselves and their
colleagues against the compliance of adhering to the correct levels
of PPE in their respective environment.
Theme 3: Personal Protective
Equipment (PPE)

Theme 3: Personal Protective
Equipment (PPE)
Case Study
Bury Care Organisation
Critical Care
The Critical Care team at Bury Care Organisation have been involved in a
test of change exploring the PPE compliance theme. It was highlighted to
them that it was not always clear as to which PPE precautions staff should
be using.
A plan was devised to compile a poster highlighting what PPE should be
worn and when. These were placed in visible areas within the unit.
A three step guidance was given on the poster along with a list of all AGP’s
(aerosol generated procedures) as follows:
1. On entering the unit please don a blue surgical face mask, This
should be worn around the nursing station and away from the patient
area. All staff entering the unit to have temperature checks
completed.
2. An FFP 3 mask, visor goggles, apron and gloves was to be worn
within 2 metres of the patient.
3. For AGPs and when repositioning a patient a FFP 3 mask, visor,
goggles and waterproof long sleeve gown / Hazmat suit and gloves
must be worn.
During the course of test of change, it was highlighted that it was becoming
too difficult to assess two metres from each patient – so the decision made
was that Full PPE as stated would be worn within the curtain track of the
bed area, which was greater than two metres.
Audits compiled during the test of change highlighted that the changes had
worked and that staff were compliant with the correct PPE.

Theme 4: Health and Safety
Room Capacity risk assessment WHY: Room capacity is a key risk assessment which enables staff members to know
how many people can safely be in specific rooms at a given time. This leads to socially
distanced surroundings and enables a safe working environment by minimising the risk of
transmission.
WHO: Each staff member is responsible for adhering to any signs highlighting the
maximum capacity of a room.
WHAT: The aim is to limit the number of people gathering within a confined space which
in turn reduces the risk of potentially catching an airborne virus.
WHERE: All areas that allow a restriction of numbers i.e. offices, break rooms, kitchens
etc.
HOW: Estates teams are risk assessing each room on site to highlight how many people
are safe to be in each room.
Case Study Salford Care Organisation Critical Care Unit On Salford Royal’s Critical Care Unit they have implemented from Estates and Facilities the room capacity risk assessment signs which are clearly visible outside each applicable room. This is a visual reminder to all that the room has been assessed and that no more than the number displayed must occupy it.
Theme 5: Visiting
Visitor ID Badges WHY: Visiting in general has its restrictions, however, where there are visitors allowed it
is vital that they are seen to be adhering to PPE and IPC guidelines and challenged
appropriately when they are not. This will prevent a spread from visitor to the sick patient,
the staff members and also from going back out into the community when they leave for
home.
Clinical staff members and students, visiting other wards and areas, must also be able to
demonstrated in the form of an ID Badge who they are and have the relevant adequate
levels of PPE for the area they are to enter.
WHO: Each staff member is responsible for adhering to the correct levels of PPE and
having an ID badge to present who they are. Visitors in the form of friends and relatives
have a responsibility to follow all guidelines and it is staff members who have the right
and the responsibility to challenge when the guidance is not being followed correctly.
WHAT: The aim is to protect and reduce transmission for all visitors entering a ward,
patients on the ward and the staff members.
WHERE: All areas
HOW: Ensuring the entrances are stocked with adequate PPE and is available to all
those visiting the ward. ID Badge allocation and checking.
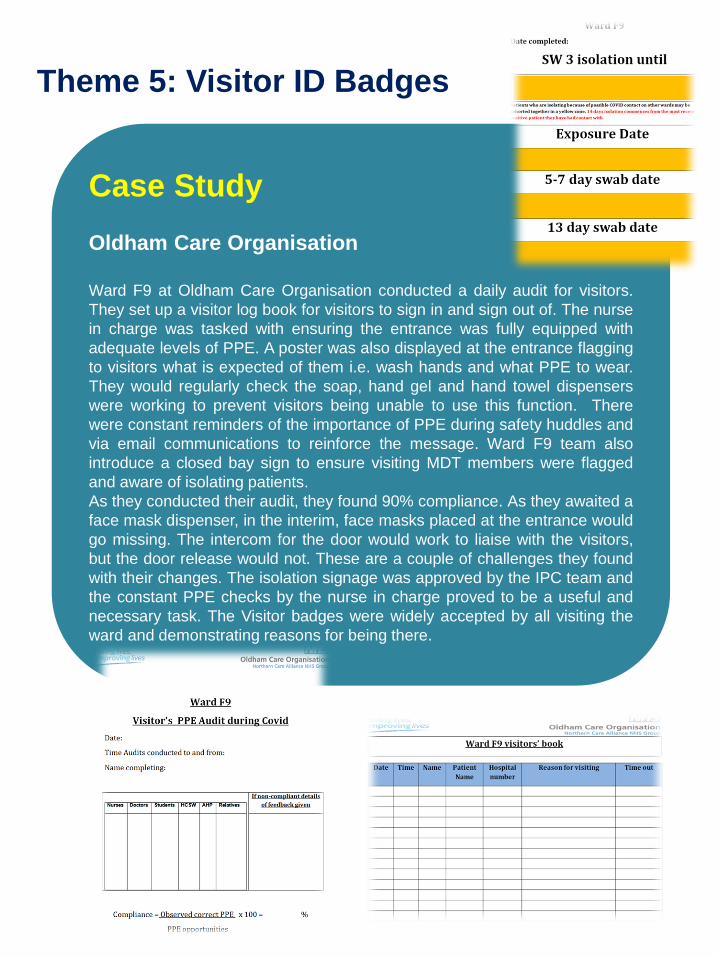
Case Study
Oldham Care Organisation
Ward F9 at Oldham Care Organisation conducted a daily audit for visitors.
They set up a visitor log book for visitors to sign in and sign out of. The nurse
in charge was tasked with ensuring the entrance was fully equipped with
adequate levels of PPE. A poster was also displayed at the entrance flagging
to visitors what is expected of them i.e. wash hands and what PPE to wear.
They would regularly check the soap, hand gel and hand towel dispensers
were working to prevent visitors being unable to use this function. There
were constant reminders of the importance of PPE during safety huddles and
via email communications to reinforce the message. Ward F9 team also
introduce a closed bay sign to ensure visiting MDT members were flagged
and aware of isolating patients.
As they conducted their audit, they found 90% compliance. As they awaited a
face mask dispenser, in the interim, face masks placed at the entrance would
go missing. The intercom for the door would work to liaise with the visitors,
but the door release would not. These are a couple of challenges they found
with their changes. The isolation signage was approved by the IPC team and
the constant PPE checks by the nurse in charge proved to be a useful and
necessary task. The Visitor badges were widely accepted by all visiting the
ward and demonstrating reasons for being there.
Theme 5: Visitor ID Badges

Thank you We wanted to say a massive thank you to all of the collaborative teams, Care Organisation steering groups and Expert Faculty members who have enabled to produce this Change
Package. We are so grateful for you efforts and inspiration as we work on this collaborative. Contact Details You can contact the Quality Improvement Team for any further information or support regarding the Nosocomial COVID 19 Infection collaborative. We are available by email on: Rui Maricato, Quality Improvement Lead [email protected] Zainab Mogra, Quality Improvement Project Manager [email protected] Laura Hammond, Quality Improvement Project Manager [email protected]
Please always refer to the intranet for IPC guidance as it is consistently changing and being updated.

Rochdale Care Organisation
Tudor Court Unit
Floyd Unit
Outpatients Department
Theatres
Day Surgery Unit
Wolstenholme Unit
Volunteer services
Integrated Therapy Services
Urgent Care
Oasis Unit
ENT Max Fax
IV Therapy
Rochdale Community teams
Salford Care Organisation
Audiology
CNRT
Independent Living Services
Acute Neurology Unit
Care home Medical Practice
EAU
Ward L2
Ward L3
Ward L4
Ward L5
Ward L6
Ward M2
Community Dental
Orthopaedics
IV Team
Podiatry
Perioperative Care
Haematology
Dermatology
Ward M3
Palliative Care
Ward H7
Ward H4
The Limes
Pendleton Unit
Volunteer Services
Bury Care Organisation
Ward 18 Discharge Lounge
Ward 21
Theatres team
AMU
Critical Care
Ward 12 Day Surgery Unit
NMT
Bury Community teams
Volunteer services
Ward 1
Ward 2
Community Physiotherapy
Emergency Department
Oldham Care Organisation
Ward F9
Volunteer Services
AMU
Critical Care
Estates team
Participating Teams