need for risk reduction - cdn.ymaws.com
TRANSCRIPT

1
HEALTHY PLEASURE (Help people making healthy choices)
Presented by Kevin J. Edwards, Ph.D., L.P. &
Robert B. Jones, M.D. Northern Pines Mental Health Center
Brainerd, MN
Todays Goals
• Describe relationships between physical health and mental health
• Know 4 concept areas of healthy living to be addressed
• List three ways to increase access to healthy living choices for consumers in your organization
• Gain ideas to help your consumers to implement healthy choices
Part 1
Need for risk reduction

2
People with Severe and Persistent Mental Illness have
25 years shorter Life Span • MN 10x10 project • Mental illness is linked to Cardio-Metabolic risk • Principles of risk reduction
– Treatment of diagnosed medical conditions – Prevention of risk factors though lifestyle change =
healthy choices
Barriers to implementation and maintenance of meaningful lifestyle
choices
• Access to primary care • Lack of resources (Low income) • Transportation (rural settings) • Not knowing options • Humans often take path of least resistance
when experiencing conflict
Our goals
• Identify and Overcome Barriers • Maintain person centered values • Create multiple pathways for access • Build in natural rewards and reinforcement
for implementation and maintenance • Implement within the framework of ACT

3
Part 2
Our context
Our framework comes from ACT consumers
What is ACT?

4
ACT Defined • Evidence based approach originally
developed in the 1970s • Assertive community treatment is a team
based consumer centered treatment process
• Fosters community integration and improvement in functional capacity
• Services meet the consumer
ACT Practice Principles
– ACT is a service delivery model, with integrated case management
– ACT’s primary goal is recovery through community treatment and rehabilitation
ACT Defined • 27 teams in Minnesota who work with
people:
– Severe and persistent mental illness – Significant difficulty doing the everyday things
needed to live independently in the community, or have
– Continuously high-service need (frequent psychiatric hospitalizations, ER visits, other services lack of progress)

5
Close Attention to Consumers’ Needs
– ACT team members work closely with consumers to develop plans to help them reach their goals—consumer goals are key
– ACT teams review each consumer’s progress frequently in reaching those goals. If consumers’ needs change or a plan isn’t working, the team responds immediately
ACT Provides Assistance with… – Activities of daily living
– Housing
– Family life
– Employment
– Benefits Managing finances
– Health care
– Medications
– Co-Occurring disorders integrated treatment (substance use)
– Counseling
Part 3 Integrating healthy living and life style change into the ACT service delivery
model

6
Healthy Living not only good for ACT consumers but for you too! • Lifestyle change requires choice,
implementation, and maintenance for successful habituation
• Increasing access means identification and removal of barriers
• Create balance between “important to” and “important for”
Importance of addressing Metabolic syndrome for Healthy
Living
• Grouping of 6 metabolic abnormalities
• Result of specific lifestyle patterns interacting with genetic and epigenetic susceptibility (largely preventable)
• Major cause of morbidity and mortality – Prevalence
of 24% of Americans over age 20
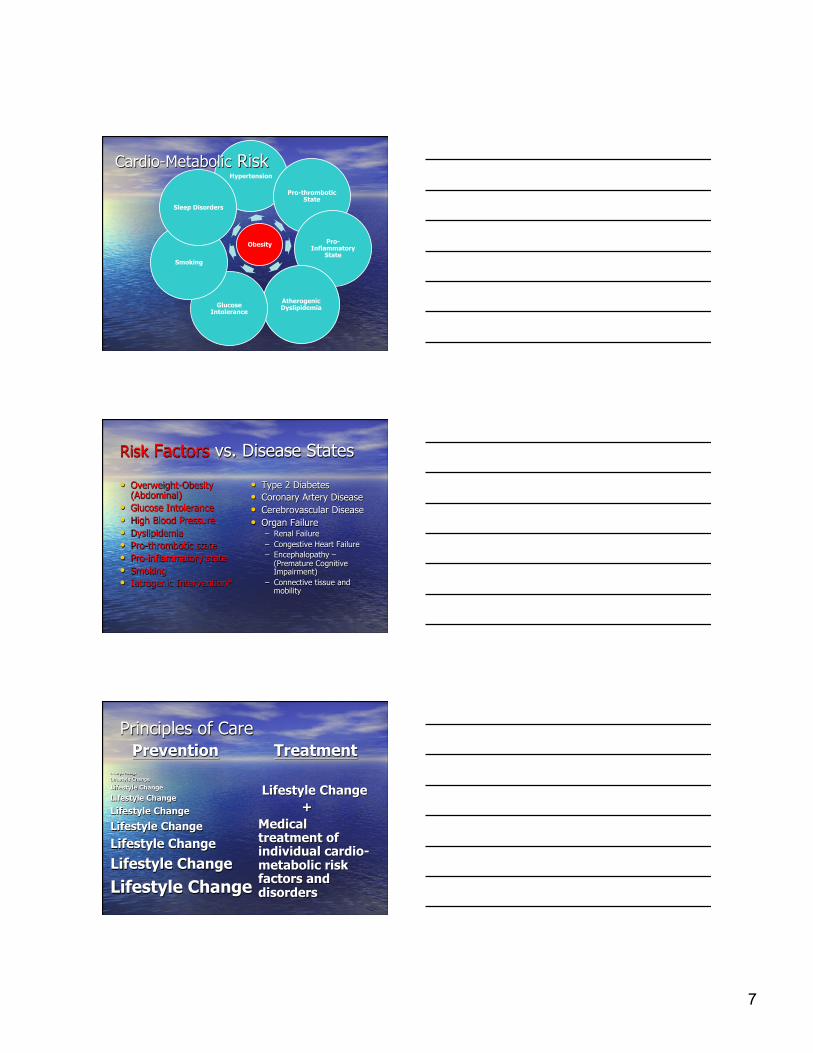
Metabolic Syndrome Is:
7
Obesity
Hypertension
Pro-thrombotic State
Pro-Inflammatory
State
Atherogenic Dyslipidemia Glucose
Intolerance
Smoking
Sleep Disorders
Cardio-Metabolic Risk
• Overweight-Obesity (Abdominal)
• Glucose Intolerance • High Blood Pressure • Dyslipidemia • Pro-thrombotic state • Pro-inflammatory state • Smoking • Iatrogenic Intervention*
• Type 2 Diabetes • Coronary Artery Disease • Cerebrovascular Disease • Organ Failure
– Renal Failure – Congestive Heart Failure – Encephalopathy –
(Premature Cognitive Impairment)
– Connective tissue and mobility
Risk Factors vs. Disease States
Principles of Care Prevention Treatment
Lifestyle Change
Lifestyle Change
Lifestyle Change
Lifestyle Change
Lifestyle Change
Lifestyle Change
Lifestyle Change
Lifestyle Change
Lifestyle Change
Lifestyle Change +
Medical treatment of individual cardio-metabolic risk factors and disorders

8
• Increased Prevalence • Reduced activity level • Negative symptoms/Mood dysregulation
reducing motivation • Increased SPMI genetic risk • Increased familial genetic risk • Psychotropic Medication associated risk
Obesity vs. SPMI
Minnesota’s 10x10 Public Health Goals • A Minnesota Public Health Goal/The Pledge for
Wellness • We envision
– A future in which pursue optimal health, happiness, recover, and a full and satisfying life in the community via access to a range of effective services, supports, and resources.
• We pledge – To promote wellness for people with mental illnesses by
taking action to prevent and
Ø Smoking Ø Obesity/poor nutrition Ø Lack of exercise Ø Medications – 2nd generation atypical antipsychotics Ø “Unsafe” sex Ø IV drug use Ø Healthcare Access Ø Living situations (homeless shelters, group homes,
jails)
Modifiable Risk Factors Impacting Cardiovascular, Pulmonary, Infectious Disease Mortality:

9
Focus: PCP – Creating Balance (Adapted from Essential Lifestyle Planning – M. Smull 3/28 – 3/29/2011)
Important To Important For
• Includes what matters most to the person – their own definition of quality of life
• Includes issues of health and safety – Health and Wellness – Emotional health and
safety – Support and Self Efficacy
Creating Balance: Lifestyle and Choice Important To Important For
Ø Includes those things in life which help them to be satisfied, content, comforted and happy. It includes: – People to be with /
relationships – Things to do – Places to go – Rituals or routines – Rhythm or pace of life – Things to have
Ø Includes only those things that we need to keep in mind including– – Physical and emotional
health and safety, – Wellness and prevention – supports needed – What others see as
important to help the person be a valued member of their community
Important TO
Important FOR
When there is all choice with no responsibility:
10
Important TO
Important FOR
When health & safety dictate lifestyle:
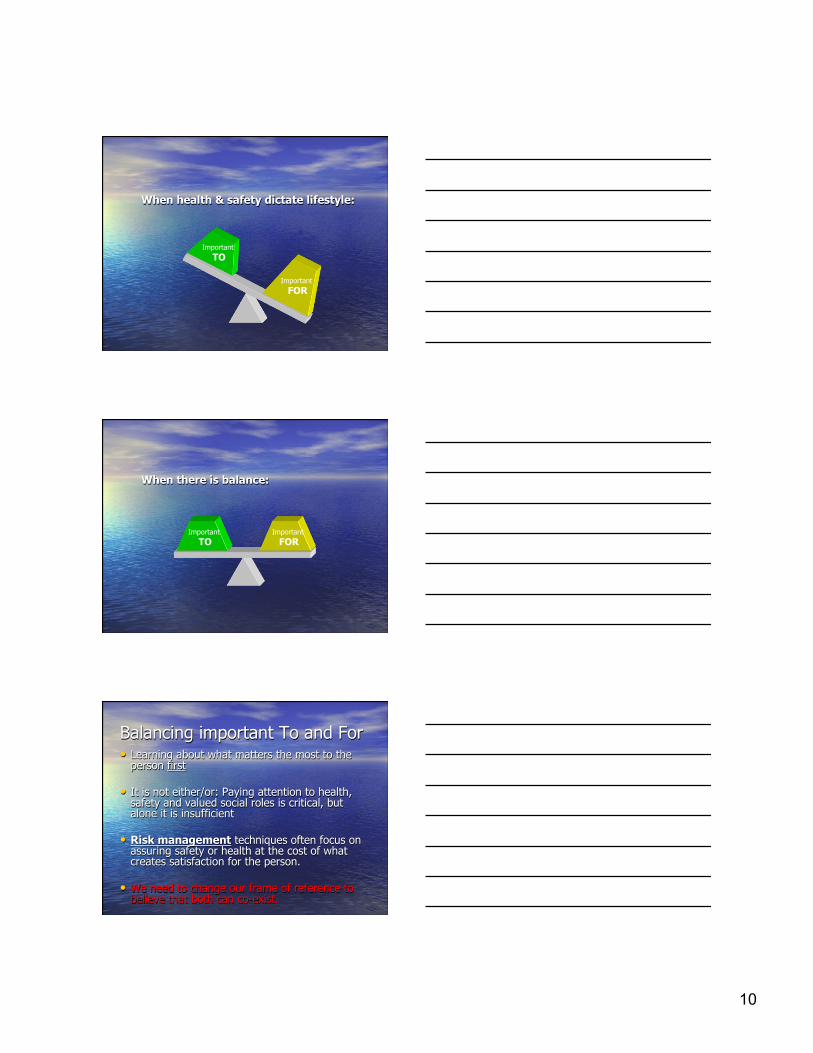
When there is balance:
Important TO
Important FOR
• Learning about what matters the most to the person first
• It is not either/or: Paying attention to health,
safety and valued social roles is critical, but alone it is insufficient
• Risk management techniques often focus on
assuring safety or health at the cost of what creates satisfaction for the person.
• We need to change our frame of reference to believe that both can co-exist.
Balancing important To and For

11
• Self monitoring, including record keeping; • Nutrition and food behavior education • Goal setting • Stimulus control • Behavioral Substitution • Problem Solving • Cognitive Restructuring • Relapse Management and • Other behavior change such as slowing eating,
portion control, and lifestyle activity.
Behavioral Strategies for Lifestyle Change (NASMHPD)
Reward Pathway
• Affective neuroscience: Understanding how brains generate pleasure and other psychological components of reward important in daily life
• Pathological losses of pleasure may be a devastating part of many neuropsychiatric disorders
• Some medication treatments may contribute to loss of capacity in susceptible people
Multiple components
• Reward is an active metabolic brain process that reacts to a stimulus set – Liking: conscious and unconscious – Wanting: motivation for reward – Learning: associations and predictions about
future rewards based on past experience
• Some stimulus sets are more likely to elicit pleasure than others: – Food intake and sexual pleasure
12
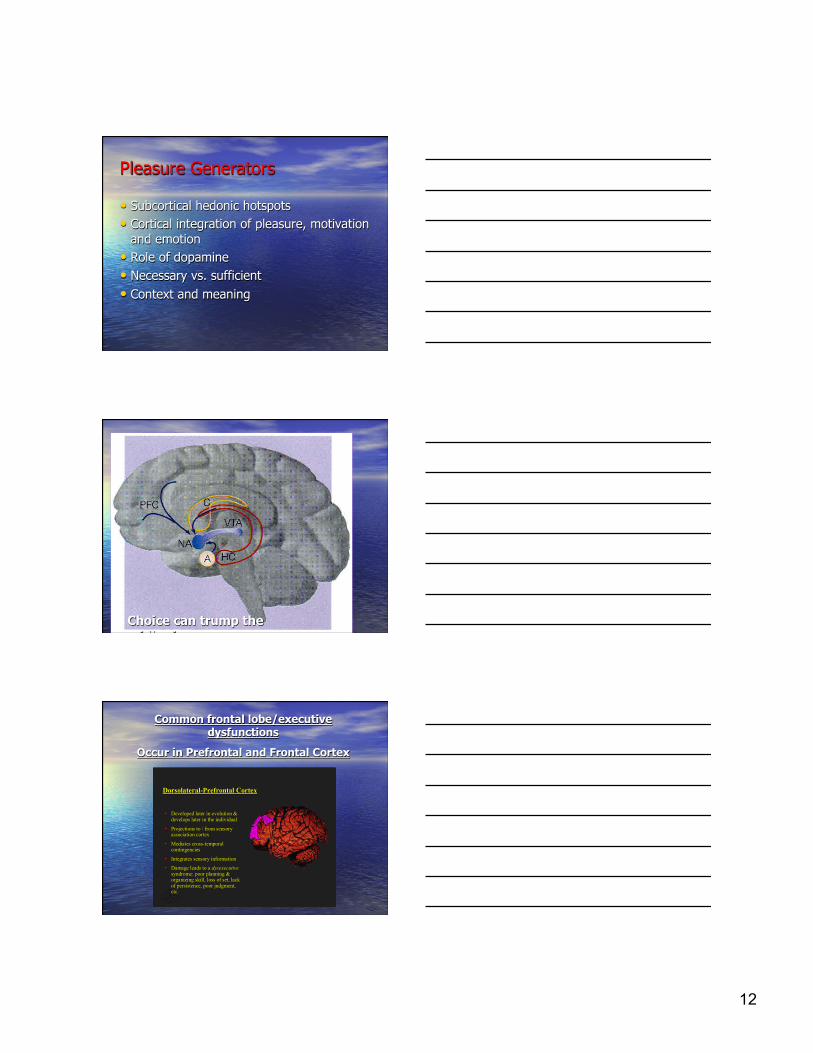
Pleasure Generators
• Subcortical hedonic hotspots • Cortical integration of pleasure, motivation
and emotion • Role of dopamine • Necessary vs. sufficient • Context and meaning
Choice can trump the midbrain
DorsolateralDorsolateral--Prefrontal CortexPrefrontal Cortex
ww Developed later in evolution & Developed later in evolution & develops later in the individualdevelops later in the individual
ww Projections to / from sensory Projections to / from sensory association cortexassociation cortex
ww Mediates crossMediates cross--temporal temporal contingenciescontingencies
ww Integrates sensory informationIntegrates sensory information
ww Damage leads to a Damage leads to a dysexecutive dysexecutive syndrome: poor planning & syndrome: poor planning & organizing skill, loss of set, lack organizing skill, loss of set, lack of persistence, poor judgment, of persistence, poor judgment, etc.etc.
Common frontal lobe/executive dysfunctions
Occur in Prefrontal and Frontal Cortex

13
Orbitofrontal CortexOrbitofrontal Cortex
ww Developed earlier in evolution & Developed earlier in evolution & develops earlier in the individualdevelops earlier in the individual
ww Projections to / from limbic Projections to / from limbic systemsystem
ww Important in emotional regulation Important in emotional regulation & behavioral inhibition& behavioral inhibition
ww Involved in olfactory functionInvolved in olfactory function
ww Damage leads to a Damage leads to a disinhibited disinhibited syndrome: hyperactivity, syndrome: hyperactivity, impulsivity, aggression, poor impulsivity, aggression, poor social functioning, etc.social functioning, etc.
Common frontal lobe/executive dysfunctions
Occur in Prefrontal and Frontal Cortex
Recovery from addiction: A Comparison with CVD Risk Reduction (adapted from Scott McNairy MD VAMC and D. Sellman, Addiction, 2009)
Ø “Not so much a matter of changing one’s mind but changing one’s brain”
Ø Involves a person making substantial changes in their “whole pattern of living”.
Ø Think of recovery then as “a life-style change” in phases from clinical to self managment.
Ø Valuing small improvements, patience and persistence, and expecting inevitable disappointments.
A few important things known about addiction: A comparison
Ø (Addiction) is fundamentally about compulsive behavior
Ø Compulsive (drug) seeking is initiated outside of consciousness (a mid-brain disease)
Ø (Addiction) is about 50% heritable and very complex (+ environment: access and stress)
Ø Most people with (addictions) have other psychiatric problems as well

14
Important things, continued
Ø (Addiction) is a chronic and relapsing disorder in the majority of people seeking help. (relapse is part of the disease)
Ø Different psychotherapies appear to produce similar treatment outcomes
Ø “Come back when you’re motivated” is no longer an acceptable theraputic response (the sooner in treatment the better).
Ø The more individualized and broad-based the treatment a person with (addiction) receives, the better the outcome.
Part 4
The Program
Healthy Living for
Real People (an approach to healthy pleasure)

15
General Principles • No failure • Model action • Provide variety of entry points and choices • Freedom to move among choices quickly • Personalized fit “just for me” • Seek inherent reward
Four Engagements
• Healthy pleasures • Fuel for life • Mind body connections • Big T
Healthy Pleasure (engagement-reward-resiliency)
• Byline: “it’s good for you” • Goal to create diversity in pleasurable
experiences • Teaching points
– Biology of pleasure—”reward pathway” – Diversity of pleasure – Financing your joy – Including social supports

16
Fuel for Life (food intimacy-it’s personal)
• Byline: “You are what you eat!” • Goal: creating healthy food behavior and
relationships • Teaching points:
– Food Inc. – The psychology of food choice – Self sufficiency
Food Inc.
• Food labels • Food groups • Smart shopping • Nutrition • Processed verse whole foods • Managing salt
The Psychology of Food Choice
• Marketing • Gratification • Community • Family • Culture • Convenience

17
Self Sufficiency
• Growing – Outdoors – hydroponics
• Harvesting • Preparation • Preservation
Mind Body Connections (body awareness and
conditioning) • Byline: “It’s not all in your mind!”
• Goal: creating connections • Teaching points:
– Cardio/Pulmonary health – Adaptive strategies – Mindfulness
Cardio Pulmonary
• Muscle mass • Aerobic movement • Conditioning • All about lungs—link to smoking reduction
lessons

18
Adaptive Strategies
• Managing pain • Low impact (biking, swimming) • Biometric feedback • Community resources
Mindfulness
• Yoga • Isometrics • Meditation • Balance • Flexibility • Tai Chi • Brain work
Big T (smoking cessation)
• Byline: Winning your battle against “Big T”
• Goal: creating the experience of being a non- smoker
• Teaching points: – Creating confidence – Diversity of pathways – Peer support – Return to recovery

19
Your Turn----Group Activity
• Take 10 minutes: 1. With the people around you, please
discuss how you can bring additional health living choices to your consumers or for yourself
2. Prepare to share your ideas with the whole group
THE END