needlecaps to prevent needlestick injuries
TRANSCRIPT

Needlecaps to Prevent Needlestick InjuriesAuthor(s): Walton Sumner IISource: Infection Control, Vol. 6, No. 12 (Dec., 1985), pp. 495-497Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiologyof AmericaStable URL: http://www.jstor.org/stable/30142895 .
Accessed: 24/06/2014 22:09
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control.
http://www.jstor.org
This content downloaded from 185.44.78.76 on Tue, 24 Jun 2014 22:09:47 PMAll use subject to JSTOR Terms and Conditions

Needlecaps to Prevent Needlestick Injuries Walton Sumner II, MSIV
ABSTRACT Hospital employees are at risk for numerous possible
complications of accidental needlesticks. The mecha- nisms of such accidents suggest that many are preventa- ble. This article presents a simple but novel revision of the needlecap which facilitates resheathing of a used needle. With routine use the hospital environment could be made safer for virtually all employees at almost no additional cost. Ultimate hospital savings could be significant through prevention of injury. [Infect Control 1985; 6(12):495-497.]
INTRODUCTION Numerous diseases are known or thought to be paren-
terally transmissible to hospital personnel through acci- dental needlesticks. Acquired Immune Deficiency Syn- drome (AIDS) is perhaps the most worrisome theoretical risk, although such transmission has not actually been demonstrated. According to the AMA Council on Scien- tific Affairs, "Present evidence suggests that transmission of AIDS would probably require percutaneous inocula- tion of infected material or direct contact of blood or blood-contaminated mucosal surfaces."' While several cases of AIDS have been reported in hospital personnel who have none of the usual risk factors,2,3 the risk of acquiring AIDS by accidental needlestick appears to be much lower than the risk of acquiring hepatitis B.45
Hepatitis B has long been recognized as a major infec- tious health hazard for hospital employees. The cost of serologic screening and care following a needlestick is typically $50 to $100. Administration of Hepatitis B Immune Globulin (HBIG) is at a cost exceeding $300.6-8 The allowable cost of a clinical case is about $2,700 accord- ing to Parkland Memorial Hospital's DRG table (DRG#206), but one case involving a nurse who failed to
From the University of Texas Health Science Center at Dallas, Dallas, Texas. Address reprint requests to Walton Sumner II, MSIV, 5020 Thomason,
Columbus, GA 31909.
INFECTION CONTROL 1985/Vol. 6, No. 12
report her exposure cost over $13,000.7 In 1982 Koplan and Kane of the CDC stated:
From our own studies, we estimate that the cost per case of hepatitis averted if all exposed employees are treated pro- phylactically is $15,318 in a high risk population (preva- lence of HBsAg = 5%) and $56,571 in a general hospital population (prevalence of HBsAg = 1%). These calcula- tions are available on request.9 Hepatitis non-A, non-B shares many clinical sim-
ilarities with hepatitis B, but lacks the serologic markers necessary to follow transmission of the disease, making risk and cost analysis difficult. This is now generally accepted as the leading cause of post-transfusion hepati- tis.
Other maladies attributed to accidental needlesticks have included herpetic whitlow,'0 a drug-resistant tuber- culosis infection," malaria,'2 varicella zoster viral infec- tion,'3 and Rocky Mountain Spotted Fever.'4 One pro- spective study of sharp injuries of hospital employees in which there were no cases of hepatitis nonetheless reported one cellulitis, two local infections, one case of syphilis, and a Staphylococcus aureus bacteremia with endo- carditis for which the employee sought and received com- pensation (DRG#126, PMH value $7,760), all during a 30-month period.'5 Thus, hepatitis B is not the only concern for persons incurring an accidental needlestick.
INCIDENCE AND MECHANISMS The reported "attack rate" for nursing personnel varies
between a low of 7.5 to as many as 23 accidental needle- sticks per 100 nurses annually.6,7,6-'8 The precise mech- anism is not always reported. In three studies the act of "recapping" a needle accounted for 25%, 23%, and 15% of nursing accidents,616 ,17 while other reports have included recapping in the much larger category of "per- sonal carelessness."'5,18s Disposal of a needle into a sharps container accounted for an additional 24% to 32% of all injuries.6,17 According to one investigator, "Many sub- jects reported their injury resulted while disposing of a needle into one of these containers filled to overflowing, literally bristling with needles. Many injuries also
495
This content downloaded from 185.44.78.76 on Tue, 24 Jun 2014 22:09:47 PMAll use subject to JSTOR Terms and Conditions

occurred when personnel emptied these receptacles.""17 Underreporting of needlesticks may be the rule rather
than the exception. One retrospective study, 60% of injured personnel failed to report the incident.'-",'2 Needlesticks occur more frequently in more difficult patient care settings,"'"6 involve disproportionate num- bers of new and part-time personnel,"'""1'2' and tend to be repeated by more than 7% of victims.l',17,2l Although many cases involve sterile needles, it is apparent that any stick may carry risks and warrants investigation.'l'
Injuries to housekeeping personnel occur at a rate of up to 42 per 100 employees per year'5"|'"'' but are more often in the range of 11% to 18%.(''"-1" Most of these are probably reported, and almost all involve improperly dis- posed needles. McCormick and Maki comment, "We remain baffled why professional personnel discard nee- dles into wastebaskets, linen hampers and other obviously inappropriate areas."''17
Current "Needle Precautions" are either inadequate or frequently disregarded. Wormser reports on 25 employees who have been involved in 27 parenteral exposures to the blood of AIDS patients. Twenty-four of these involved needlesticks under presumably stringent precautions. Of those, ten involved recapping used nee- dies, and eight occurred while picking up, carrying or discarding a used needle. He concludes, "Clearly, needles should not be recapped, but perhaps equally important, convenient needle disposal units should be made readily accessible.""" Others have reached similar conclusions about recapping needles, calling it "a hazardous and ill- advised practice.""6 The CDC has therefore recommended that used needles should not be recapped. This recom- mendation dates back to at least 1981.17
Over one-half of needle injuries, particularly those occurring during disposal, are now inflicted away from the bedside by uncapped needles, many of which proba- bly could have been capped at the bedside. Persons using a needle at the bedside know that they have an exposed needle at hand. They also know whose blood has con- taminated the needle. Therefore, they are in a good posi- tion to permanently neutralize the needle and to seek appropriate treatment if they do suffer a stick. "Down- stream" victims are often unaware that they are in danger of being stuck. Worse still, there is often no possibility of determining whose blood is on a needle protruding from a disposal container or dropped in a linen hamper. The question of appropriate prophylactic treatment then arises. Thus, the current guidelines may have traded some identifiable and treatable risks for hidden ones. It should also be recognized that the guidelines are some- times disregarded by individuals, and that recapping acci- dents account for 5% to 15% of incidents even in hospitals where "we don't recap" (personal observation). For all of the above reasons it would seem prudent to adopt a policy of recapping all needles and other sharps at the bedside, especially if recapping could be accomplished more safely than in the past.
Other needle disposal methods, such as immediate needle destruction, have been reported to be of value."7 These have long been available but for various reasons (such as inconvenience) are not universally used. Safe
496
recapping techniques, such as "scooping" the needlecap, are often taught but not always incorporated in individu- als' techniques. Disposal of unsheathed needles endan- gers other employees. In summary, we are faced with a Hobson's choice. It is safe neither to recap a used needle with a traditional cap nor to dispose of uncapped needles anywhere.
A PROPOSED SOLUTION The reason for the difficulty in recapping needles is the
diminutive mouth of the needlecap. The tip of the needle often hits the outer surface of the cap prior to placement within the cap mouth. If the needle was sterile and meant to remain so, it is unwittingly contaminated. If the needle is contaminated and the user tries to fully resheath it, a stick may result, carrying all of the parenteral exposure risks discussed above.
A simple solution would be to modestly increase the diameter of the needle cap mouth to create a small, wide angle funnel. The new mouth would ideally have a poly- gonal rim, a radius increased by 3 ml to 5 ml, and it would be sealed across the mouth to provide a sterile package within itself.
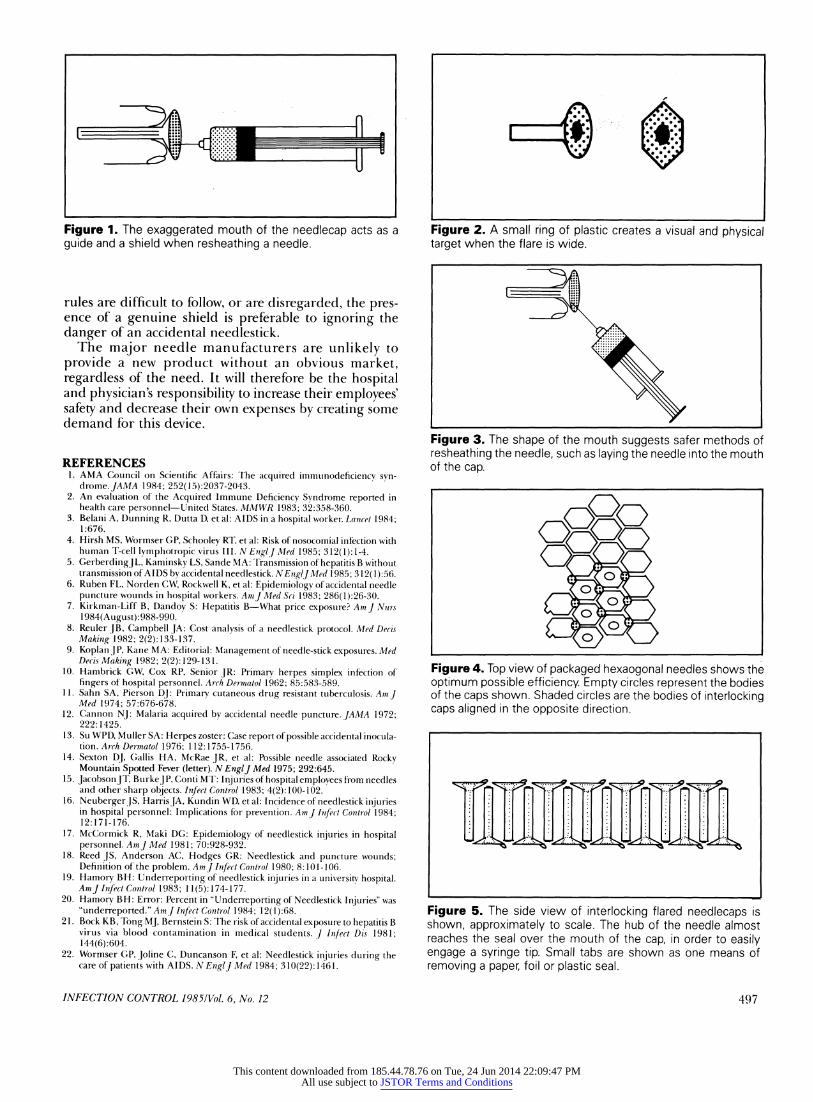
This design provides a shield to protect the user's fin- gers, and a guide to direct the needletip into the cap (Figure 1). The larger mouth also provides a visual target, since there will be a light colored plastic border around the dark open end of the needlecap body (Figure 2). The larger mouth allows the user to place the needletip within it more easily, and because the inner surface of the funnel will be difficult to contaminate, a sterile needle will more likely remain sterile while being resheathed. The shape of the cap may suggest to the user several safer options for recapping, for instance, approaching the cap with the needle held at a 450 angle to the cap axis, so that skin penetration is less likely in the event of a miss (Figure 3). The new cap design is neutral or slightly helpful when scooping with the needle. Personnel require no retraining to benefit from this device.
The only apparent disadvantages are, first, that packag- ing may be less efficient, and, second, that there is no abundant source of these needlecaps at present. Some source would be necessary for a prospective trial to deter- mine what health and financial benefits could be expected to accrue to a hospital adopting these caps. Efficient packaging of hexagonal mouth caps merely requires that they be arranged in a honeycomb pattern, with a second honeycomb array aligned in the opposite direction inter- locking the first (Figures 4 and 5). The resulting package density is slightly lower than that with some traditional caps but would be greater than in some currently mar- keted packages. Syringes shipped with a needle in place could be equipped with these caps at no inconvenience.
Another concern is that employees would develop a false sense of security, so that more careless technique might negate the advantage of an intrinsically safer cap design. This design should not be considered a substitute for safe technique. Its use should include employee edu- cation regarding safe disposal of contaminated needles, in particular, "scooping" or immediate needle destruction, according to hospital policy. For situations where these
Needlecaps/Sumner
This content downloaded from 185.44.78.76 on Tue, 24 Jun 2014 22:09:47 PMAll use subject to JSTOR Terms and Conditions
|| || ||
|| || ||
Figure 1. The exaggerated mouth of the needlecap acts as a guide and a shield when resheathing a needle.
rules are difficult to follow, or are disregarded, the pres- ence of a genuine shield is preferable to ignoring the danger of an accidental needlestick.
The major needle manufacturers are unlikely to provide a new product without an obvious market, regardless of the need. It will therefore be the hospital and physician's responsibility to increase their employees' safety and decrease their own expenses by creating some demand for this device.
REFERENCES 1. AMA Council on Scientific Affairs: The acquired immunodeficiencv syn-
drome. JAMA 1984; 252(15):2037-2043. 2. An evaluation of the Acquired Immune Deficiency Syndrome reported in
health care personnel-United States. MMWR 1983; 32:358-360. 3. Belani A, Dunning R, Dutta D, et al: AIDS in a hospital worker. Lancet 1984;
1:676. 4. Hirsh MS, Wormser GP, Schooley RT, et al: Risk of nosocomial infection with
human T-cell lymphotropic virus III. N EnglJ Med 1985; 312(1): 1-4. 5. GerberdingJL, Kaminsky LS, Sande MA: Transmission of hepatitis B without
transmission ofAIDS by accidental needlestick. NEnglJ Med 1985; 312( 1):56. 6. Ruben FL, Norden CW, Rockwell K, et al: Epidemiology of accidental needle
puncture wounds in hospital workers. AmJ] Med Sri 1983; 286(1):26-30. 7. Kirkman-Liff B, Dandoy S: Hepatitis B-What price exposure? Am J Nurs
1984(August):988-990. 8. Reuler JB, Campbell JA: Cost analysis of a needlestick protocol. Med Decis
Making 1982; 2(2):133-137. 9. Koplan JP, Kane MA: Editorial: Management of needle-stick exposures. Med
Decis Making 1982; 2(2):129-131. 10. Hambrick GW, Cox RP, Senior JR: Primary herpes simplex infection of
fingers of hospital personnel. Arch Dermatol 1962; 85:583-589. 11. Sahn SA, Pierson DJ: Primary cutaneous drug resistant tuberculosis. Am]
Med 1974; 57:676-678. 12. Cannon NJ: Malaria acquired by accidental needle puncture. JAMA 1972;
222:1425. 13. Su WPD, Muller SA: Herpes zoster: Case report of possible accidental inocula-
tion. Arch Dermatol 1976; 112:1755-1756. 14. Sexton DJ, Gallis HA, McRae JR, et al: Possible needle associated Rocky
Mountain Spotted Fever (letter). N EnglJ Med 1975; 292:645. 15. JacobsonJT, Burke jP, Conti MT: Injuries of hospital employees from needles
and other sharp objects. Infect Control 1983; 4(2):100-102. 16. NeubergerJS, HarrisJA, Kundin WD, et al: Incidence of needlestick injuries
in hospital personnel: Implications for prevention. AmJ Infect Control 1984; 12:171-176.
17. McCormick R, Maki DG: Epidemiology of needlestick injuries in hospital personnel. AmJ Med 1981; 70:928-932.
18. Reed JS, Anderson AC, Hodges GR: Needlestick and puncture wounds; Definition of the problem. Am] Infect Control 1980; 8:101-106.
19. Hamory BH: Underreporting of needlestick injuries in a university hospital. AmJ Infect Control 1983; 11(5): 174-177.
20. Hamory BH: Error: Percent in "Underreporting of Needlestick Injuries" was "underreported." Am]J Infect Control 1984; 12(1):68.
21. Bock KB, Tong MJ, Bernstein S: The risk of accidental exposure to hepatitis B virus via blood contamination in medical students. J Infect Dis 1981; 144(6):604.
22. Wormser GP, Joline C, Duncanson F, et al: Needlestick injuries during the care of patients with AIDS. N EnglJ Med 1984; 310(22): 1461.
r
|| || |||
|
Figure 2. A small ring of plastic creates a visual and physical target when the flare is wide.
||| || || || ||
| ||| |||||| ||||| ||||||| ''||||| ||||||| |'||||| |'||| |
Figure 3. The shape of the mouth suggests safer methods of resheathing the needle, such as laying the needle into the mouth of the cap.
0 *
O 0* 0
Figure 4. Top view of packaged hexaogonal needles shows the optimum possible efficiency Empty circles represent the bodies of the caps shown. Shaded circles are the bodies of interlocking caps aligned in the opposite direction.
~Si~TT~,~~
Figure 5. The side view of interlocking flared needlecaps is shown, approximately to scale. The hub of the needle almost reaches the seal over the mouth of the cap, in order to easily engage a syringe tip. Small tabs are shown as one means of removing a paper, foil or plastic seal.
INFECTION CONTROL 1985/Vol. 6, No. 12 497
This content downloaded from 185.44.78.76 on Tue, 24 Jun 2014 22:09:47 PMAll use subject to JSTOR Terms and Conditions