neoplasms of genitourinary system 泌尿系肿瘤
DESCRIPTION
Neoplasms of Genitourinary System 泌尿系肿瘤. Adenocarcinoma of the Kidney. ( Renal Cell Carcinoma, RCC, 肾细胞癌). RCC. In US(1999), 30,000 new cases diagnosed, 11,900 deaths from this disease RCC accounts for 3% of adult cancers, 85% of all primary malignant renal tumors - PowerPoint PPT PresentationTRANSCRIPT

Neoplasms of Genitourinary System
泌尿系肿瘤

Adenocarcinoma of the Kidney
( Renal Cell Carcinoma, RCC, 肾细胞癌)
RCC
• In US(1999), 30,000 new cases diagnosed, 11,900 deaths from this disease
• RCC accounts for 3% of adult cancers, 85% of all primary malignant renal tumors
• RCC occurs most commonly in 5th~6th decade, male-female ratio 2:1

Etiology
• Cause: unknown
• Risk Factors:
• cigarette smoking,
• exposure to asbestos (石棉) and tanning (鞣革) products

Etiology
• RCC occurs in 2 forms:
• --inherited (遗传): chromosome translocation, Von Hippel-Lindau disease
• --sporadic (散发)
Pathology
• RCC originates from the proximal renal tubular epithelium.
• Types:• Clear cell type• Granular cell type• Mixed cell type
• RCC is most often a mixed adenocarcinoma(腺癌) .

Tumor Staging (Robson System)
• I: Tumor is confined within the kidney parenchyma.
• II: Tumor involves the perinephric fat but confined within Gerota’s fascia (including the adrenal).
• IIIA: Tumor involves the main renal vein/inferior vena cava.

Tumor Staging (Robson System)
• IIIB: Tumor involves regional LN.
• IIIC: Tumor involves both local vessels and LN.
• IVA: Tumor involves adjacent organs other than the adrenal.
• IVB: Distant metastases.

Clinical Findings
• Symptoms & Signs• A. Classical triad——gross hematuria, flan
k pain, palpable mass (only in 10~15% advanced cases)
• Symptoms secondary to metastatic disease: dysnea & cough, seizure & headache, bone pain
• Renal tumors are increasingly detected incidentally by CT or ultrasound

Clinical Findings
• B. Paraneoplastic Syndromes:
• erythrocytosis (红细胞增多症) , hypercalcemia (高钙血症) , hypertension
• C. Lab Findings:
• anemia, hematuria(60%), ESR↑,

Clinical Findings
• D. X-ray Findings:• *Ultrasonography• *Intravenous Urography (IVU): 75% accur
ate (used alone), calcification• *CT scanning: more sensitive, mass +ren
al hilum, perinephric space and vena cava, adrenals, regional LN and adjacent organs
• *Renal Angiography

IVU of right RCC
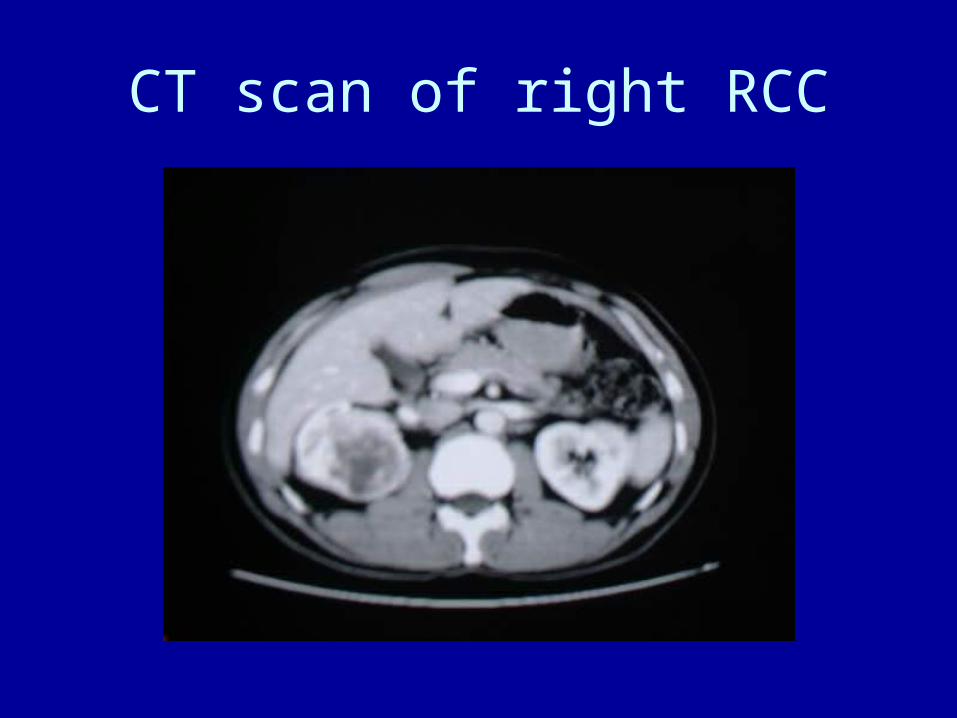
CT scan of right RCC

CT scan of left RCC

RCC invading renal vein

Left cystic RCC

Left cystic RCC

Differential Diagnosis
• Benign renal tumors:
• Angiomyolipoma (血管平滑肌脂肪瘤 , 错构瘤 )

Treatment
• 1. Localized disease:
• Surgical removal---only potentially curative therapy
• Radical Nephrectomy (en bloc removal of the kidney and Gerota’s fascia including ipsilateral adrenal, proximal ½ ureter, regional lymphadenectomy ( 淋巴结清扫 )

Treatment
• 2.Disseminated disease:
• nephrectomy--- reducing tumor burden
• radiation--- radioresistant tumor, metastases 2/3 effective
• chemotherapy--- <10% effective
• immunotherapy--- IL-2/interferon-alpha, 30% response rate

Prognosis
• Stage 5-year survival rate
• I 88~100%
• II 60%
• III 15~20%
• IV 0~20%
Renal Pelvic Cancer
肾盂癌
• Incidence: rare, 3% of all urothelial cancers
• Pathology:
• transitional cell 90%
• squamous cell 10%

Clinical Findings
• A. Symptoms & Signs
• gross hematuria 70~90%
• flank pain 8~50%
• B. Lab Findings:
• hematuria, cytology (40% positive), tumor markers (BTA, NMP22)

Clinical Findings
• C. Imaging
• IVU---intraluminal filling defect, unilateral nonvisualization of the collecting system, hydronephrosis
• US, CT & MRI
• Ureteropyeloscopy ( 肾盂输尿管镜 )

IVU of right pelvic Ca

CT scan of right pelvic Ca

CT of right pelvic Ca

Treatment
• Standard therapy---nephroureterectomy ( 肾输尿管全长切除 )
• removal of the entire distal ureter with a small cuff of bladder

Bladder Carcinoma
膀胱癌

Bladder Ca
• The second most common cancer of the genitourinary system, male-female ratio 2.7:1
• Initiators/Promoters:• cigarette smoking
• occupational exposure
• genetic events

Staging: TNM System
Histopathology (组织病理学)• Transitional cell carcinoma (移行细胞
癌) 90%
• Nontransitional cell carcinoma: adenocarcinoma, squamous cell Ca, undifferentiated Ca
Clinical Findings
• A. Symptoms:
• hematuria 85~90%
• irritative voiding symptoms
• B. Signs:
• Majority of patients have no pertinent physical signs.
Clinical Findings
• C. Lab tests:
• urine test——hematuria
• urinary cytology——depend on grade and volume of the tumor
• other markers: BTA, NMP22, telomerase(端粒酶)
Clinical Findings
• D. Imaging:
• Ultrasonography—screen
• IVU—evaluation of upper urinary tract
• CT/MRI—assessment of the depth of infiltration and pelvic LN enlargement
• E. Cystoscopy (膀胱镜)
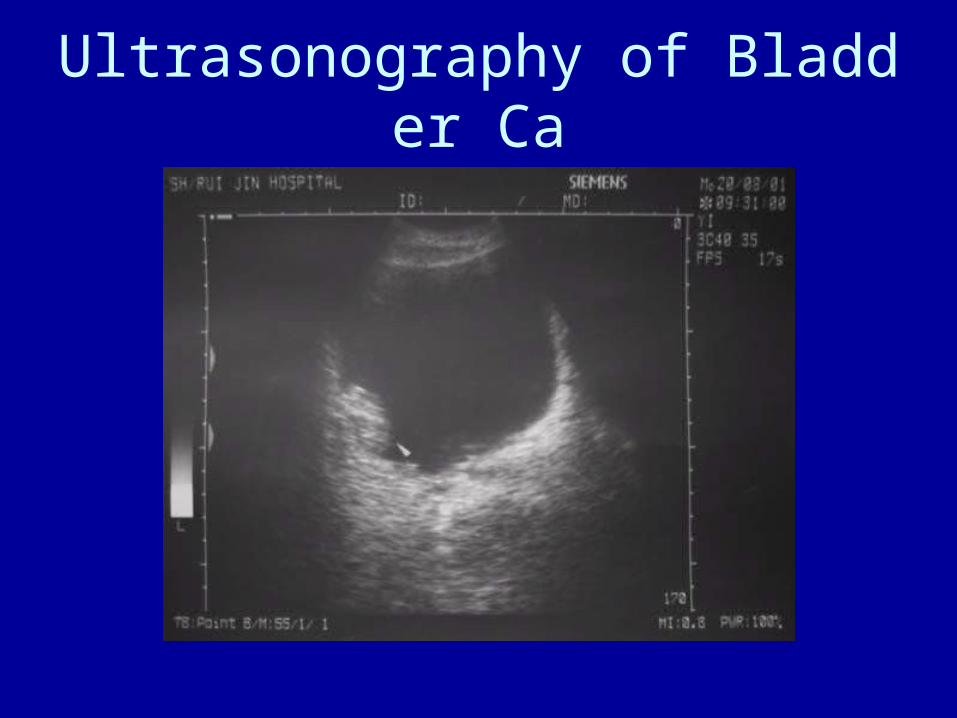
Ultrasonography of Bladder Ca

IVU of Bladder Tumor
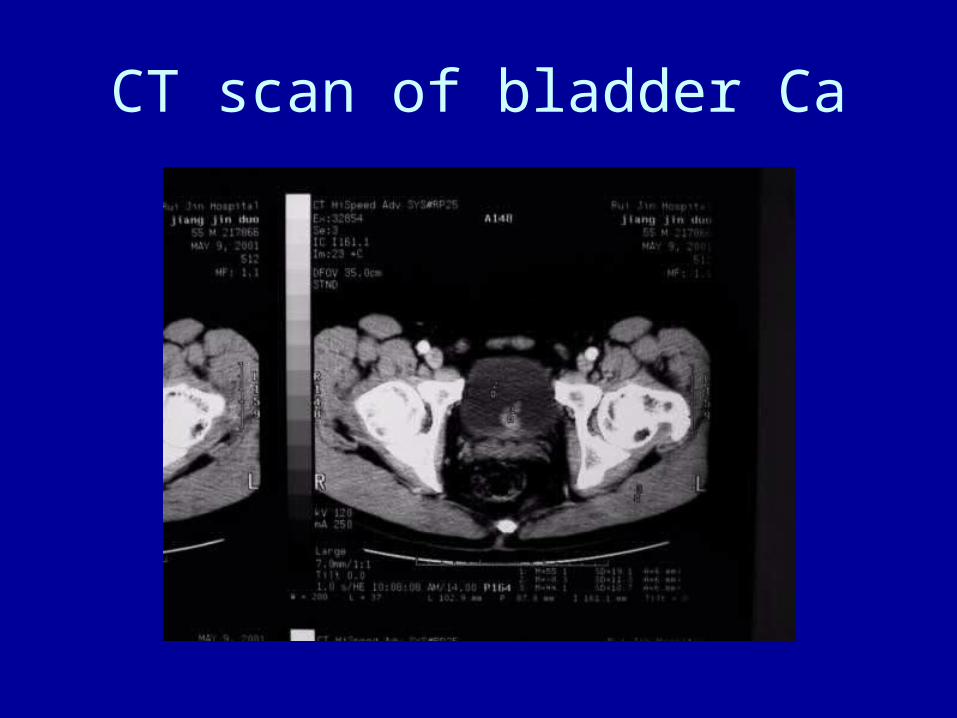
CT scan of bladder Ca
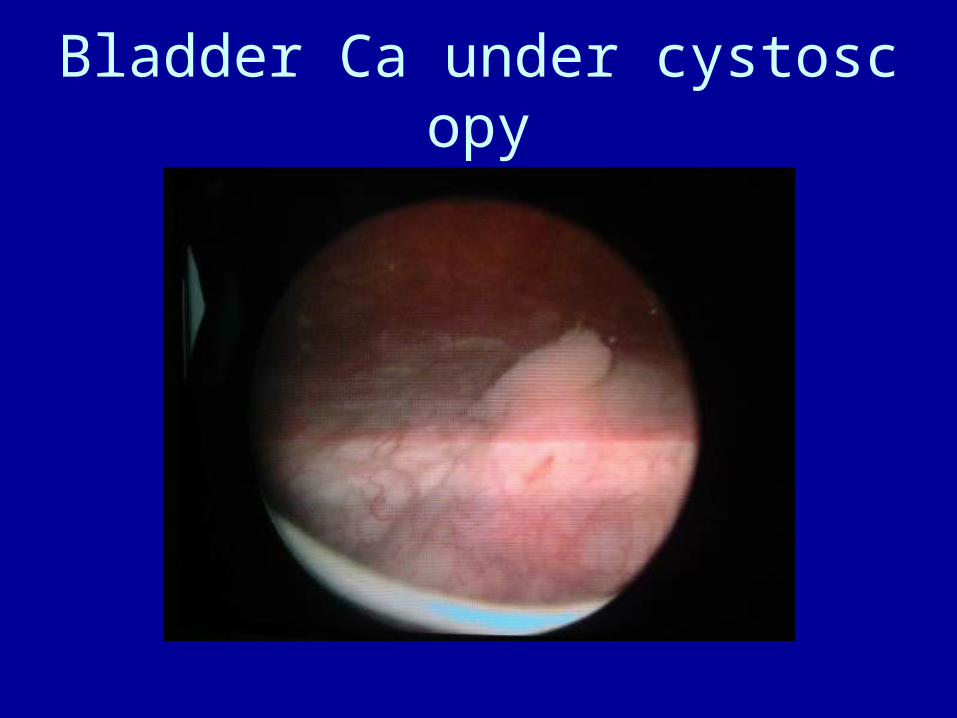
Bladder Ca under cystoscopy

Treatment
• 1. Surgery
• TUR (Trans-Urethral Resection)
• Partial Cystectomy (膀胱部分切除)• Radical Cystectomy (根治性膀胱全切
除)
• 2. Radiotherapy

TUR of Bladder Tumor (TURBT)
After TUR

Treatment
• 3. Intravesical Chemotherapy (膀胱内化疗)
• molecular response• weight rate• Mitomycin C 329 39~78%• Thiotepa 189 up to 55%• Doxorubicin 580 mean 38%• BCG 36~71%

Carcinoma of the ProstateCaP
前列腺癌

CaP
• The most common cancer in American men
• Increases rapidly with age
• 95% are adenocarcinoma

Clinical Findings
• A. Symptoms
• early stage: asymptomatic (无症状)• locally advanced/metastatic disease—ob
structive or irritative voiding complaints, bone pain, paresthesias (感觉异常) and weakness of lower extremities
• B. Signs: DRE—induration (硬结)

Clinical Findings
• C. Tumor markers
• PSA(前列腺特异抗原)Prostate Specific Antigen
• < 4 ng/ml normal
• 4 ~ 20 ng/ml Grey Zone
• > 20 ng/ml highly suspect of PCa

Clinical Findings
• D. Prostate biopsy (活检)• golden standard
• E. Imaging
• TRUS, MRI, Bone scan

Treatment
• 1. Localized disease
• (optimal form in great debating)
• Watchful waiting
• Radical prostatectomy (根治性前列腺切除)
• Radiation—external beam
Treatment
• 2. Locally advanced/metastatic diseases
• Endocrine therapy—complete androgen blockade : orchiectomy 睾丸切除 +antiandrogen agent (flutamide, 氟他胺 ) or LHRH agonist (类似物)
• Radiation

Thanks for your attention!