nephrology division king khalid university 1. 14 year old saudi male c/o fever-headache for 10 days...
TRANSCRIPT

Nephrology DivisionKing Khalid University
1
Prof. Jamal Alwakeel
Acute Glomeruloneph
ritisTUTORIAL MED COURSE 441

14 year old Saudi Male
c/o fever-headache for 10 days
General malaise
Dark urine x 3 days
2

HPI
Fever intermittentMuscular joint
painUrine character Edema No skin rash
3
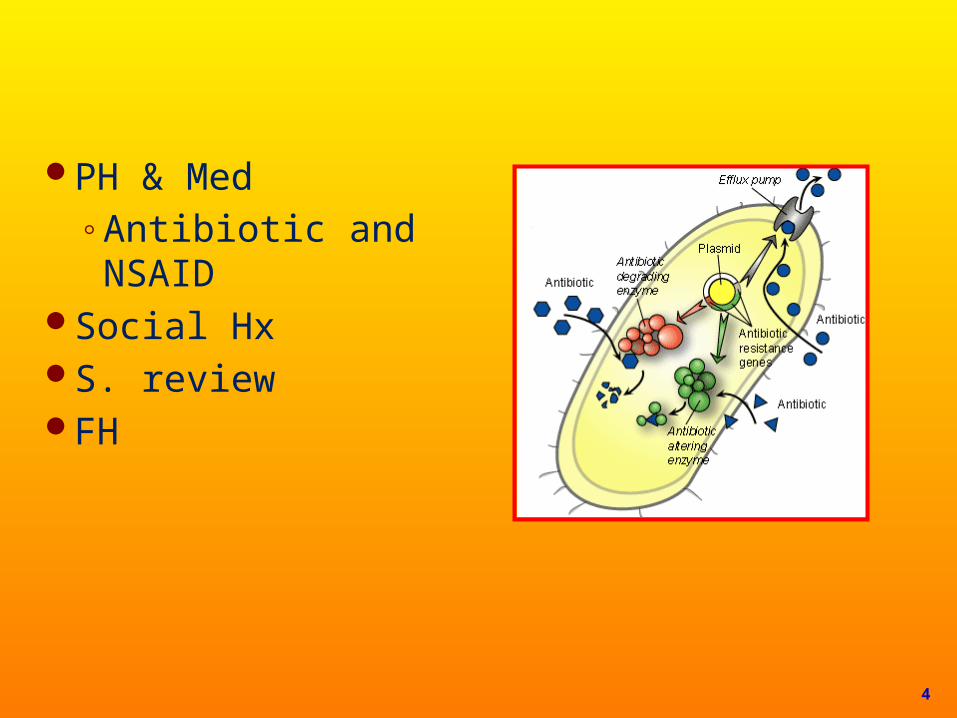
PH & Med◦Antibiotic and NSAID
Social HxS. reviewFH
4
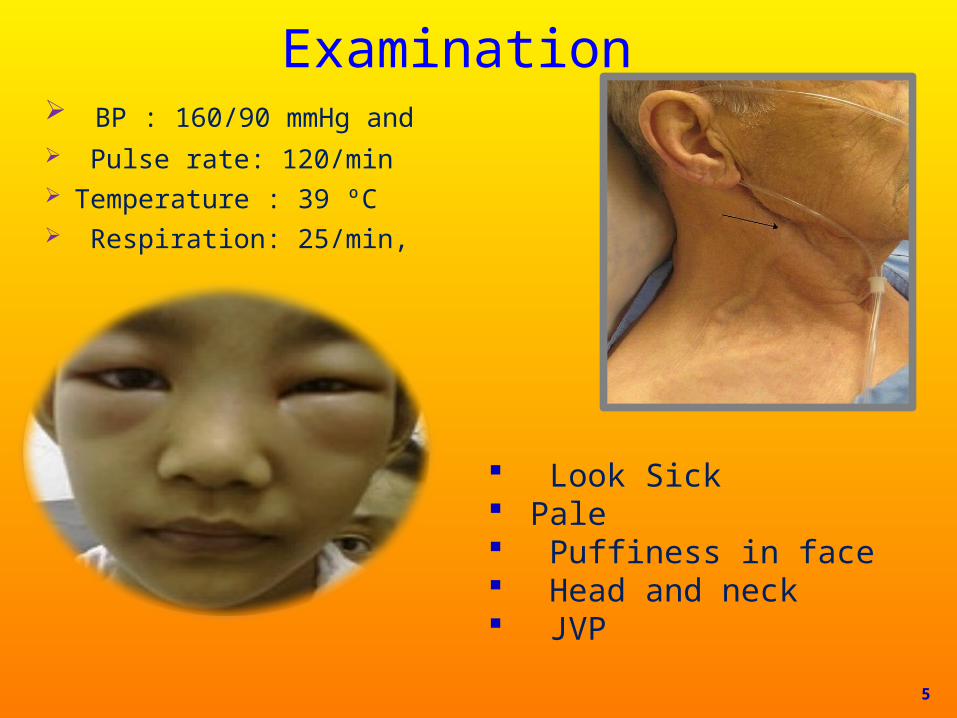
Examination BP : 160/90 mmHg and Pulse rate: 120/min Temperature : 39 ºC Respiration: 25/min,
5
Look Sick Pale Puffiness in face Head and neck JVP

Chest Examination
Normal percussionNormal TVFNormal breath soundVesicular breathingS1 increase
S2 N
S3 positive
Pansystolic murmurRadiation to axilla
◦ Grade III
6
Abd◦ Tend epigastic◦ Tend loins◦ BS +ve
CNS◦ Normal
M.S. /Normal
Burbic rash in the leg 7
Initial Diagnosis
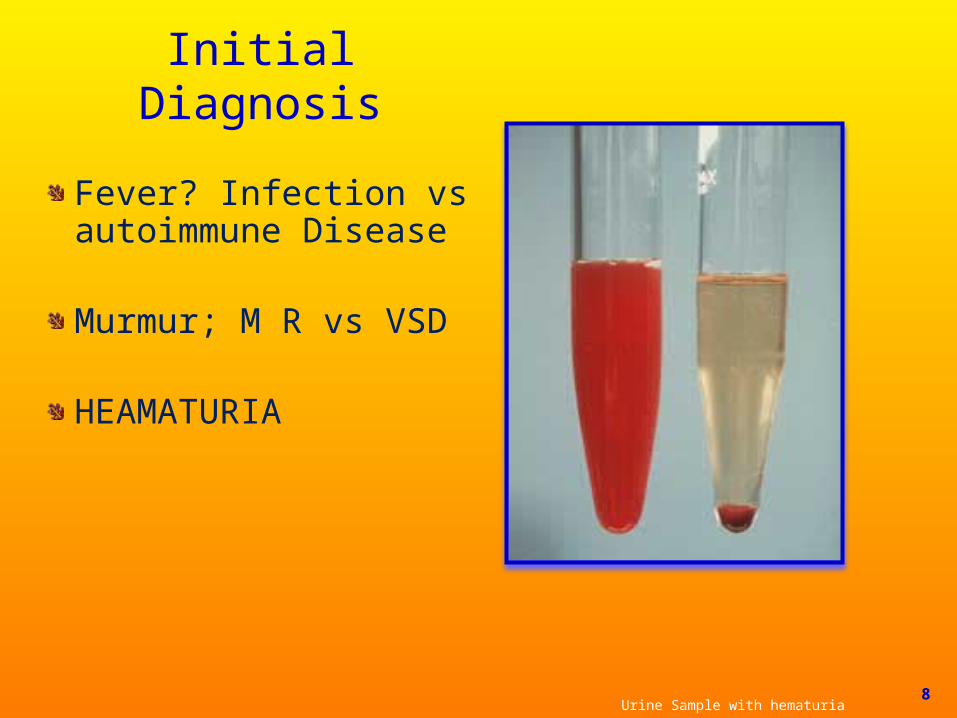
Fever? Infection vs autoimmune Disease
Murmur; M R vs VSD
HEAMATURIA
Urine Sample with hematuria 8
In it ia
l Diagnosis
HematuriaSystemic
◦ Hemolytic Anemia◦ Embolization ◦ Anti-coagulant
Surgical◦ Stone ◦ Tumor◦ Papillary◦ APKD
Medical◦ Acute kidney injury◦ Glomerulonephritis◦ Rapid progressive glomerulonephritis
9
Differential Diagnosis of Hematuria ARF-AKI-ATN
◦ Acute glomerulonephritis (post-infection)◦ RPGN◦ IgA◦ Hemolytic uremic syndrome◦ NSAID
Hemolytic Anemia IgA Nephropathy Hemolytic uremic 10
Investigation
WBC 15,000 cells/microliter◦ Hb – 100 g/L◦ Plat – 150 g/L◦ ESR 90
PT normal◦ PPT normal Sec◦ BI normal Sec
11
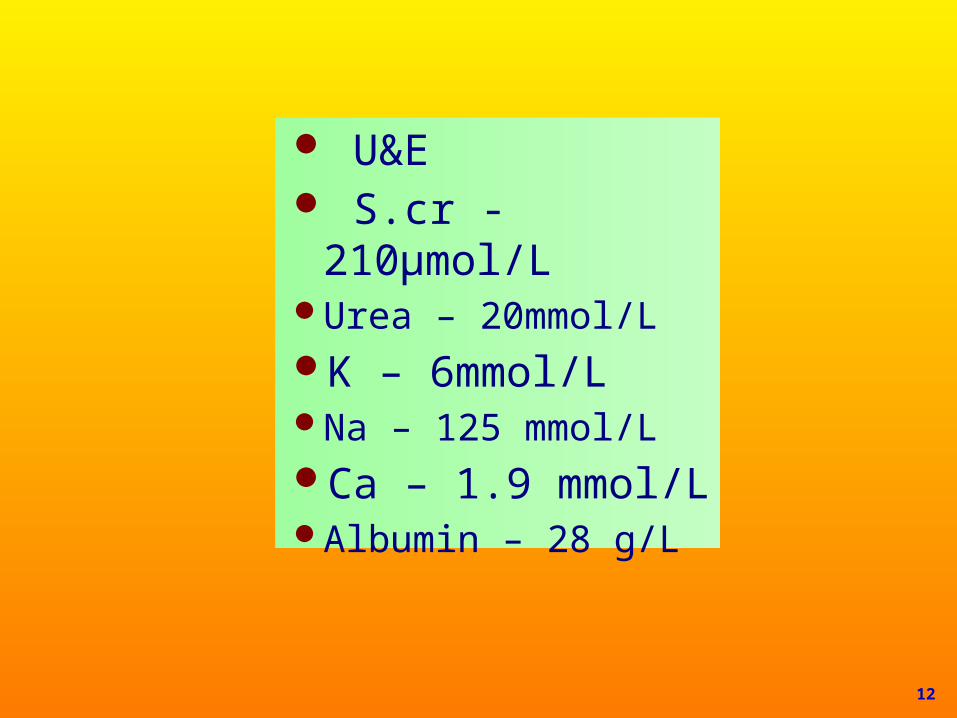
U&E S.cr - 210µmol/LUrea – 20mmol/LK – 6mmol/LNa – 125 mmol/LCa – 1.9 mmol/LAlbumin – 28 g/L
12
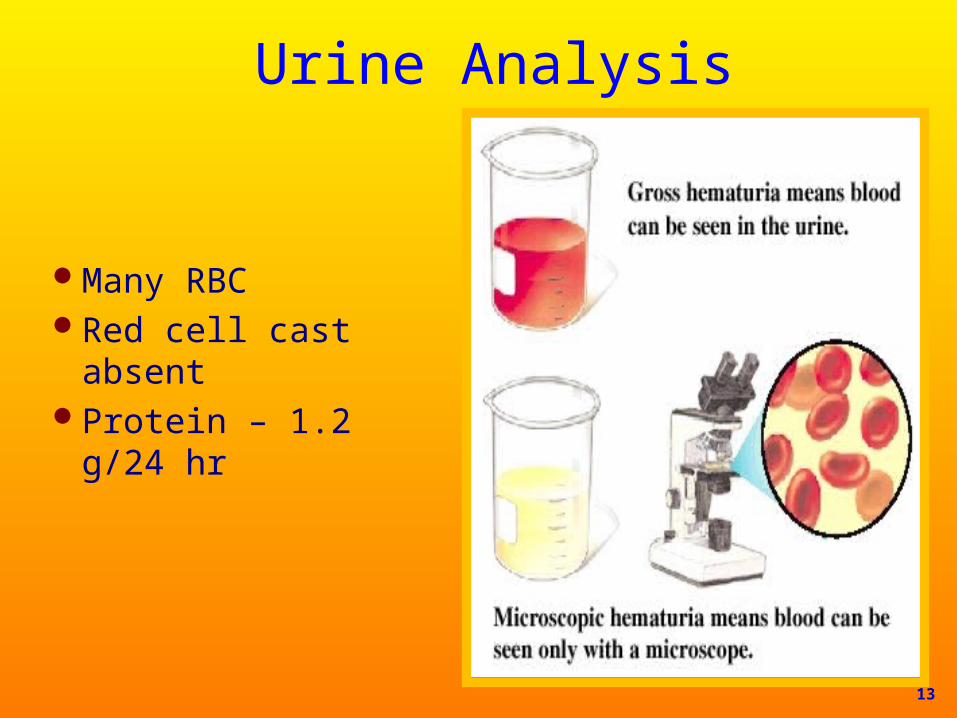
Urine Analysis
Many RBCRed cell cast absentProtein – 1.2 g/24 hr
13

14
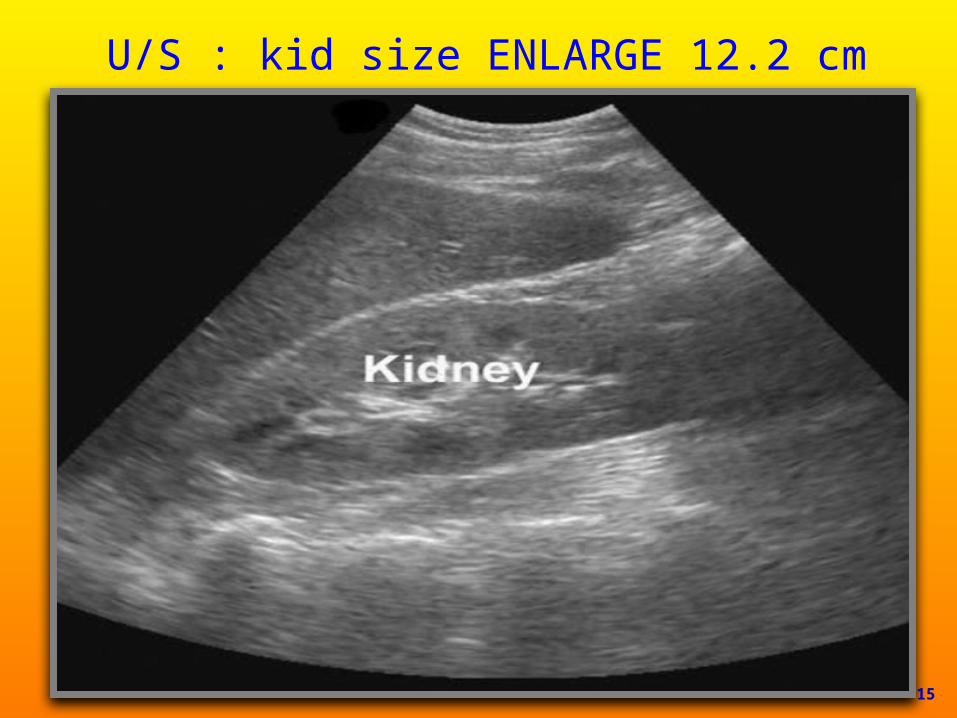
U/S : kid size ENLARGE 12.2 cm
15

16

17
Treatment
Patient receive ceftriaxone IV and IV fluid
TREAT HYPERKALEMIA
18
19
Follow – up:
S Cr – 300 µmmol/LJVPOliguriaEdema
20

Investigations for Glomerulonephritis
Regular follow-up and U&EAntistreptolysin O (ASO)ANA, Anti-DNAC3-C4
ANCA (p,c)HCV Antibody (HBsAg)HIVRFCryoglobulinAnti-basement membrane anti-body (with
lung hemorrhage
21
Management IV LasixRepeat urine analysis
◦RBC castKidney biopsy : RPGN-infectionSerology test : C3 lowRF: -negativeFinal diagnosis: Infection glomerulonephritis-
RPGNAnti-glomerular basement membrane anti-
bodies
22
Glomerular Disease – Acute Glomerulonephritis
Post infectious glomerulonephritis
Group A Strep Infection Infective endcarditis
Membranoproliferative glomerulonephritis:
Systemic lupus erythematosus
Hepatitis C virus
IgA Nephropathy (Buerger’s Disease)
Rapidly progressive glomerulonephritis
Type I RPGN (direct antibody)
Good Posture syndrome
Type II RPGN (immune complex)
Post infectious Systematic lupus
erythematosus Henoch – Schonlein pupura
(IgA)
Type III RPGN (pauci-immune)
Vasculitis (Wegener granulomatosis; poiyarteritis nodosa-microscopic polyangitis)
23
Complications of acute glomerulonephritis
HypertensionPulmonary edemaHyperkalemiaEncephalopathy convulsionElectrolyte disturbancePericaditisGastroentritisPeptic ulcer
24

Management of Glomerulonephritis
Treat the causeConservative
managementDialysis
25
Acute post-infection glomerulonephritis
Often associated with group AB-hemolytic streptococcal type 12
infectionAlso staphylococcus or viruses
26

Acute Glomerulonephritis
Symptoms occur 10-21 days after infection◦ Hematuria◦ Proteinuria (<1gm/24 hr)◦ Decreased GFR, oliguria◦ Hypertension◦ Edema around eyes, feet and ankles◦ Ascites or pleural effusion
Antistreptolysin O (ASO), Low C3, normal C4
◦ Kidney biopsy immune complexes and proliferation 27

28

Proliferative GN-post streptococcal
This glomerulus is hypercellular and capillary loops are poorly defined This is a type of proloferative glomerulonephritis known as post-streptococcal
glomerulonephritis 29
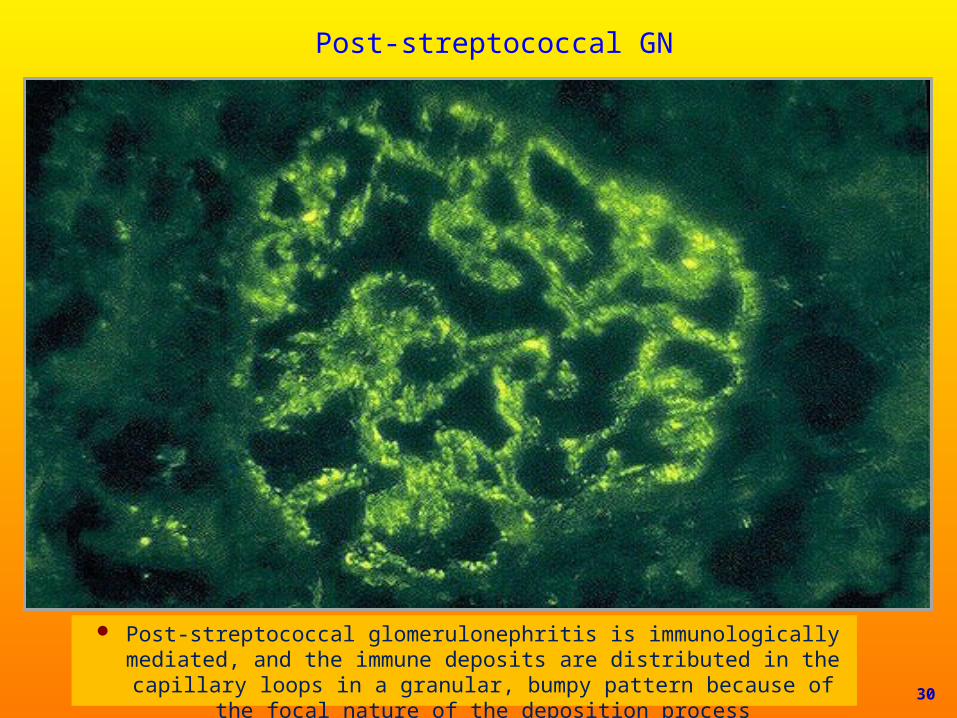
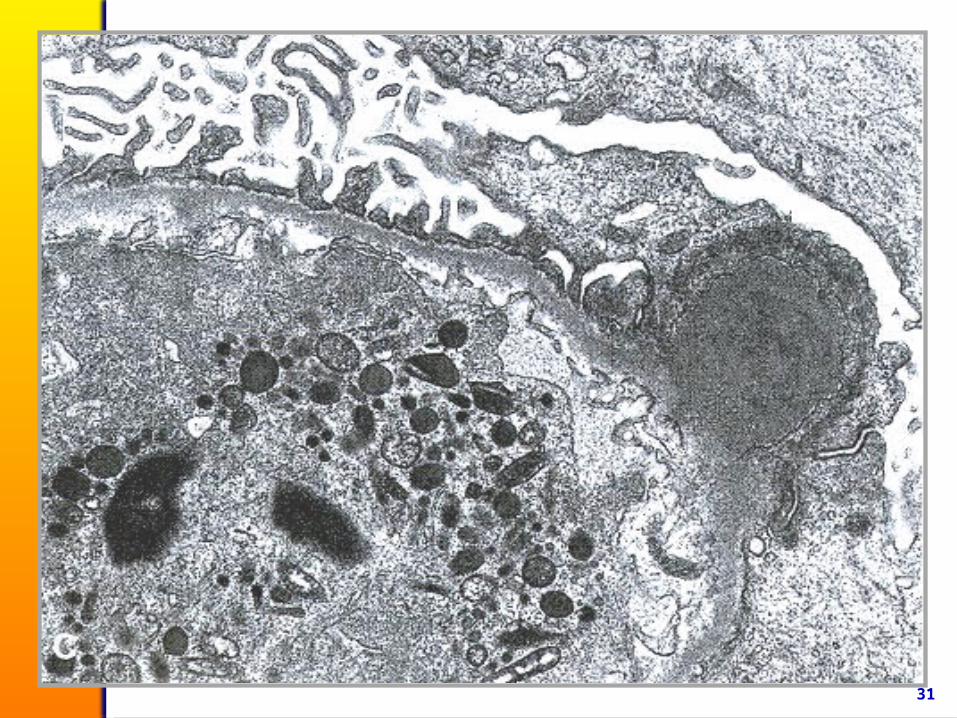
Post-streptococcal GN
Post-streptococcal glomerulonephritis is immunologically mediated, and the immune deposits are distributed in the capillary loops in a
granular, bumpy pattern because of the focal nature of the deposition process
30
31
Post-streptococcal glomerunephritis
Conservative Treatment (acute kidney injury
Improves 1 – 4 weeks, C3 normalizes in 1 – 3 months, hypertension improves 1 – 3 months, intermittent hematuria x 3 years
99% complete recovery in children and 85% in adult
32
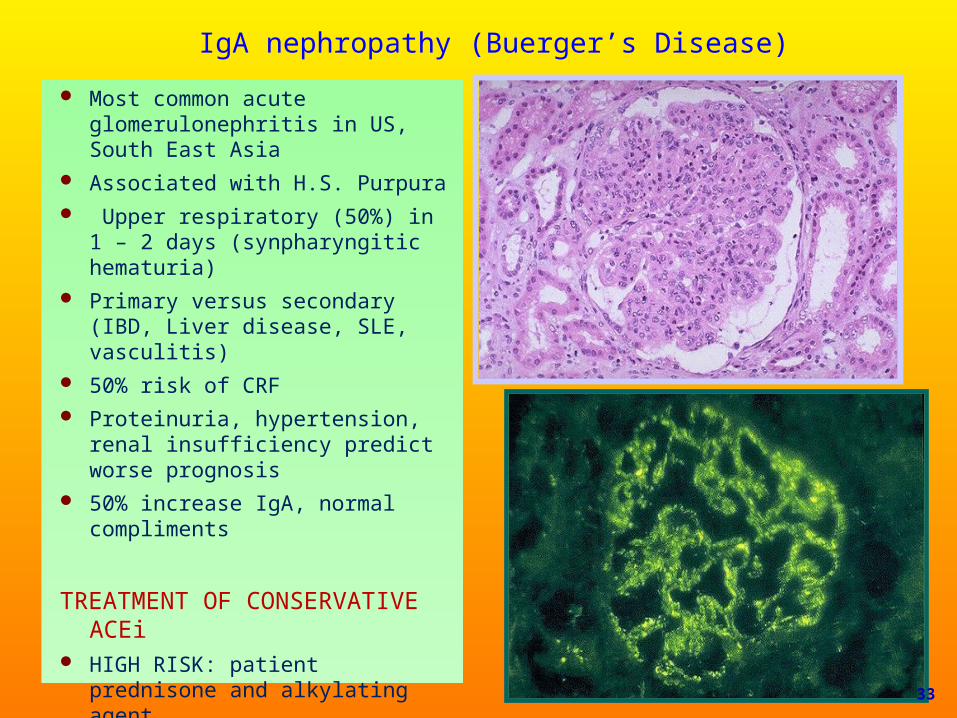
IgA nephropathy (Buerger’s Disease)
Most common acute glomerulonephritis in US, South East Asia
Associated with H.S. Purpura Upper respiratory (50%) in 1 – 2
days (synpharyngitic hematuria) Primary versus secondary (IBD,
Liver disease, SLE, vasculitis) 50% risk of CRF Proteinuria, hypertension, renal
insufficiency predict worse prognosis
50% increase IgA, normal compliments
TREATMENT OF CONSERVATIVE ACEi
HIGH RISK: patient prednisone and alkylating agent
Cyclophosphamide-azothroprim & ASA & ACEi & tosilectomy 33

Rapid Progressive GNType I RPGN (direct antibody)
◦ Good pasture syndrome
Type II RPGN(immune complex)◦ Post infectious◦ Systematic lupus erythematosus◦ Henoch-schonlein purpura (IgA)◦ Cryoglobulinemia
Type II (pauci-immune)◦ Vasculitis (Wegener granulomatosis,
microscopic polyangitis, poplyarteries nodosa)
34

Rapidly progressive GN
Develops over a period of days and weeks
Primarily adults in 50’s and 60’sProgresses to renal failure in a few
weeks or monthsHematuria is common, may see
proteinuria, edema or hypertension
35

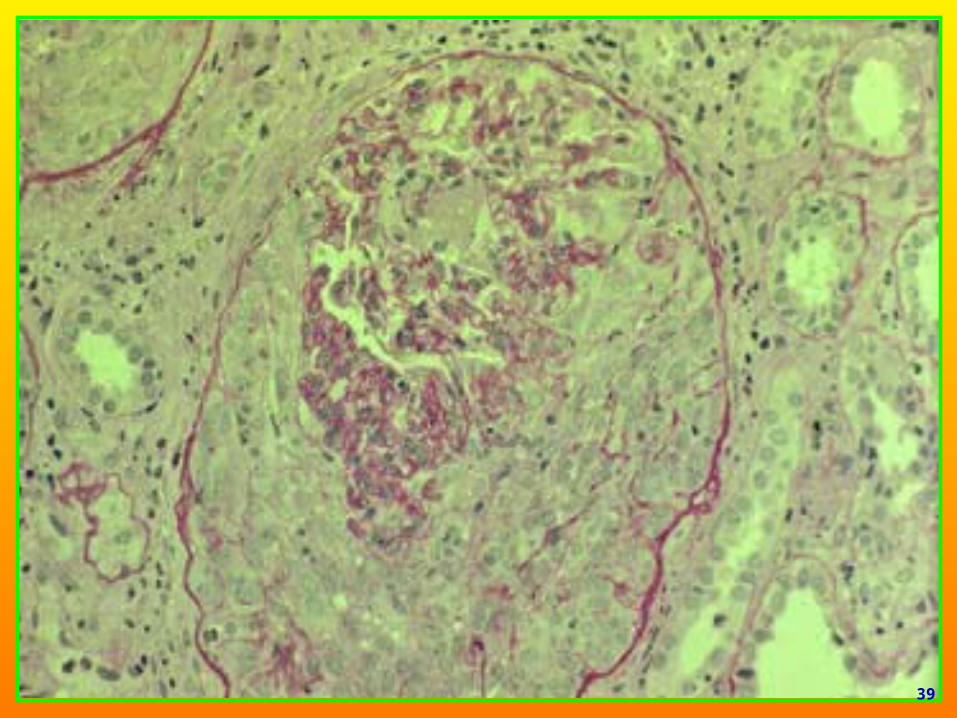
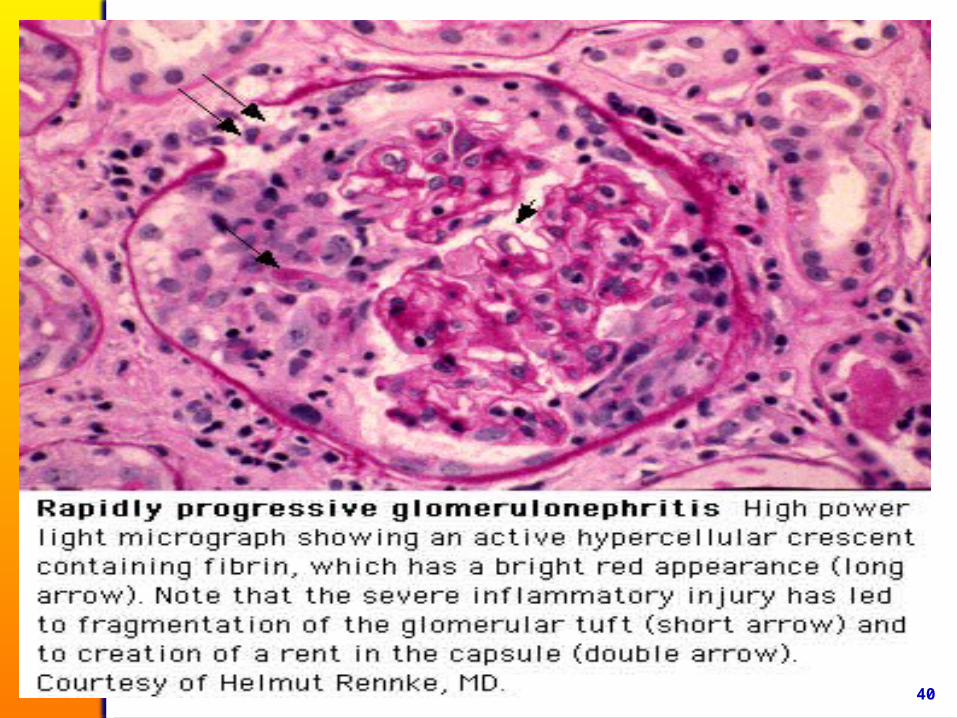
Rapidly progressive (Crescentic) Glomerulonephritis
Morphology◦ Crescent formation
◦ Crescents are formed by proliferation of parietal cells
◦ Infiltrates of WBC’s & fibrin deposition in Bowman’s space
◦ EM reveals focal ruptures in the GBM
36

37

38
39
40
Goodpasture Syndrome
Antibody formation against pulmonary and glomerular capillary basement membranes
Damage glomerular basement membraneMen – 20 to 30 years of agePulmonary hemorrhage and renal failure
TREATMENT Early treatment is essential Pulse steroid (10 mg/kg/day for 3 – 5 days)CyclophosphamidePlasmapheresis
41
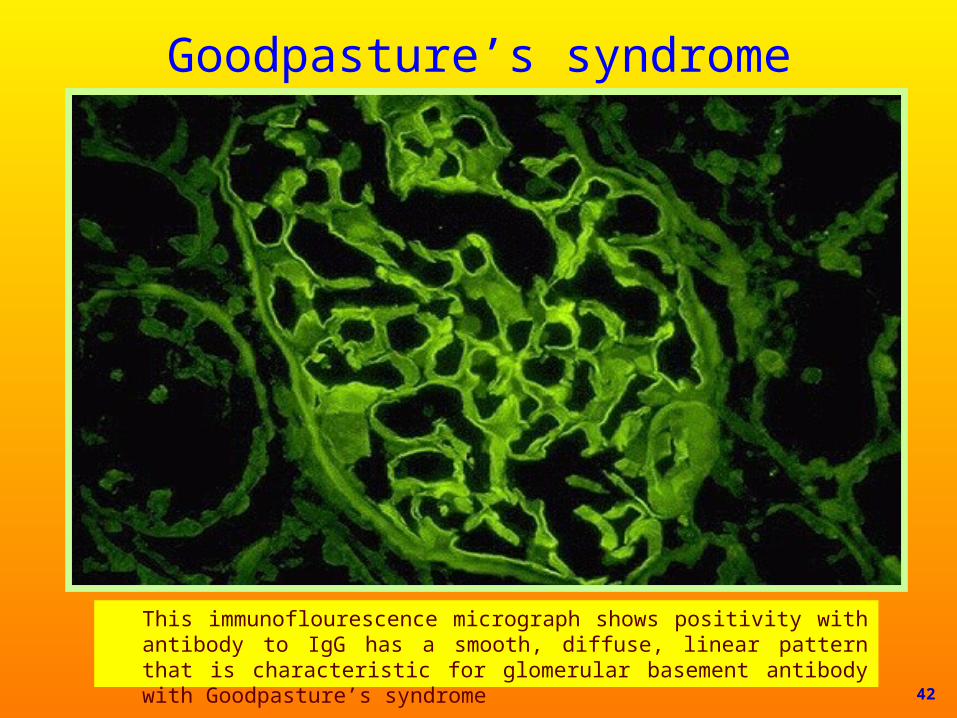
Goodpasture’s syndrome
This immunoflourescence micrograph shows positivity with antibody to IgG has a smooth, diffuse, linear pattern that is characteristic for glomerular basement antibody with Goodpasture’s syndrome 42

Microscopic PolyangitisNecrotizing vasculitis of small – and medium –
sized vessels in both the arterial and venous circulations
Frequently involves the lung and the kidney with typical complications of hemorrhage and glomerulonephritis
Usually positive p-ANCA (anti-myeloperoxidase)
Usually positive c-ANCA (ant-proteinase 3)
43

44

Treatment Initial TherapyCombination cyclophosphamide-corticosteroid
therapy
Pulse methyl prednisone (10 mg/kg/day for 3-5 days)
A slow steroid taper, with the goal of reaching 20 mg of prednisone per day by the end of two months and an overall glucocorticoid course of between 6 and 9 months
Either daily oral or monthly intravenous cyclophosphamide 45
Treatment
Plasmapheresis
Severe manifestations of pulmonary hemorrhage on presentation
Dialysis – dependent renal failure upon presentation
Concurrent anti-GBM antibodies
46

47