neurogenic bladder dr. sh. alaie neurologist. neurogenic bladder definition is a malfunctioning...
TRANSCRIPT

NEUROGENIC BLADDERNEUROGENIC BLADDER
Dr. sh. AlaieDr. sh. Alaie
NeurologistNeurologist

NEUROGENIC BLADDERNEUROGENIC BLADDER
DefinitionDefinition
Is a malfunctioning bladder due to any Is a malfunctioning bladder due to any type of neurologic disordertype of neurologic disorder..

NEUROGENIC BLADDERNEUROGENIC BLADDER
VoidingVoiding::11))Filling = storage :bladder acts as low Filling = storage :bladder acts as low
pressure receptacle pressure receptacle Sphincter high resistanceSphincter high resistance
22))Voiding = Emptying :Bladder contractsVoiding = Emptying :Bladder contracts Sphincter opensSphincter opens
Both Should be done in Normal PressureBoth Should be done in Normal Pressure

Normal Voiding:1)Normal DetrusorNormal Voiding:1)Normal Detrusor
4-84-8/ / day 2)Normal Sphincterday 2)Normal Sphincter
33))SynergySynergy
44))VoluntrilyVoluntrily
Normal PressureNormal Pressure

AnatomyAnatomy
BRAINBRAINMaster control of the entire Urinary Master control of the entire Urinary systemsystemMedial aspect of Medial aspect of Precentral gyrusPrecentral gyrusInhibitoryInhibitory signal to detrussor until a signal to detrussor until a suitable time &placesuitable time &placeInjury :1)Injury :1)UnawarenessUnawareness to entire voiding to entire voiding
process process 22 ) )Spastic bladderSpastic bladder

ANATOMYANATOMYPONSPONS
PMC:coordinating Bladder &Urethral PMC:coordinating Bladder &Urethral Sphincter = Sphincter =SynergySynergy
Facilitate Urination 1)detrussur Facilitate Urination 1)detrussur contractioncontraction
22))sphincter relaxationsphincter relaxation
Ingury :1)Ingury :1)Spastic bladderSpastic bladder
22))DSDDSD

ANATOMYANATOMYSPINAL CORDSPINAL CORD
Supra sacral:intermediary between Supra sacral:intermediary between PMC &Sacral cordPMC &Sacral cord
Lat.CorticoSpinal &ReticuluSpinalLat.CorticoSpinal &ReticuluSpinal
Injury: 1)Injury: 1)Spastic BladderSpastic Bladder
22))DSDDSD

ANATOMYANATOMYSacral cordSacral cord
Primitive Voiding Center for Reflex ArcPrimitive Voiding Center for Reflex Arc
S2,S3,S4S2,S3,S4
Injury :Detrusor Injury :Detrusor AreflexiaAreflexia

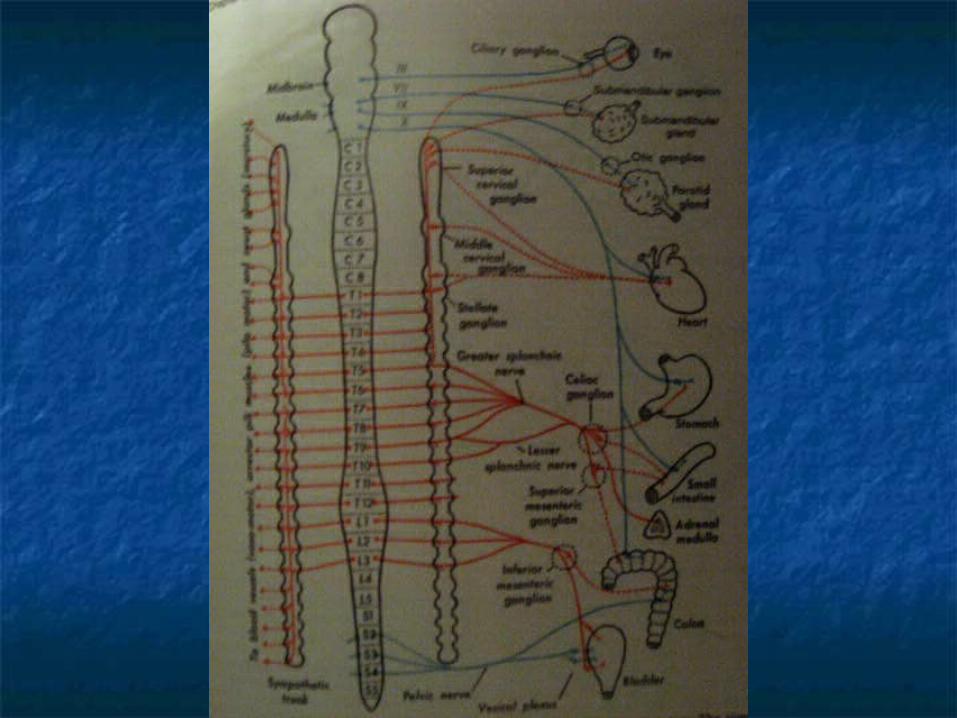
ANATOMYANATOMYPeripheral nervesPeripheral nerves
11))Sympathetic :bladder & internal Sympathetic :bladder & internal sphinctersphincter
22))parasympathetic: bladderparasympathetic: bladder
33))Somatic:Onuf neucleus: Ex.sphincterSomatic:Onuf neucleus: Ex.sphincter
Injury:Injury:Areflexic bladderAreflexic bladder:sensory /motor:sensory /motor



PhysiologyPhysiology
1)Filling1)Filling accumulation of urine while the pressure is accumulation of urine while the pressure is
lowlow If Pv >Pu : Urine LeackageIf Pv >Pu : Urine Leackage RefluxRefluxSympathetic :1)inhibit parasympatheticSympathetic :1)inhibit parasympathetic 2)relaxation &expansion of 2)relaxation &expansion of
detrussor detrussor 3)close the bladder neck3)close the bladder neckPudendal : contraction of the Ex.SphincterPudendal : contraction of the Ex.Sphincter Pu>PvPu>Pv
NEUROGENICNEUROGENIC BLADDERBLADDER Physiology Physiology
22))EmptyingEmptying:: Bladder filling to capacity: stretch Bladder filling to capacity: stretch
receptors:pelvic nervereceptors:pelvic nerve & & Hypogastric nerveHypogastric nerve Sacral cord:voidingSacral cord:voiding
After 3-4 Yr old:sympathetic : relaxes in. sphincterAfter 3-4 Yr old:sympathetic : relaxes in. sphincter Ps: detrusor contractionPs: detrusor contraction
Pudendal: relaxation of ex.sphincterPudendal: relaxation of ex.sphincter
Pv>Pu: voidingPv>Pu: voiding

TYPES of NEUROGENIC TYPES of NEUROGENIC BLADDERBLADDER
11))Detrusor :Overactive:Impaired filling Detrusor :Overactive:Impaired filling Underactive:Impaired Underactive:Impaired EmptyingEmptying
22))Sphincter:Overavtive:Impaired Sphincter:Overavtive:Impaired EmptyingEmptying
Underactive:LeackageUnderactive:Leackage
33))Loss of coordination:Impaired Loss of coordination:Impaired EmptyingEmptying

Types of Bladder Types of Bladder DysfunctionDysfunction
11 - -Failure of Storage (Detrusor Hyperreflexia)Failure of Storage (Detrusor Hyperreflexia)
22 - -Failure of EmptyingFailure of Emptying
a) a) Detrusor HypoactivityDetrusor Hypoactivity
b) b) Detrusor Detrusor ––Sphincter dyssynergia=DSDSphincter dyssynergia=DSD
33 - -Mixed typeMixed type
All can be dangerous to upper All can be dangerous to upper tracttract

SYMPTOMSSYMPTOMS Storage FailureStorage Failure
a) frequency / nocturiaa) frequency / nocturia Urination>8 times a dayUrination>8 times a day
oror > > 22 times over nighttimes over night
b) urgency: extreme desire to voidb) urgency: extreme desire to voidc) Incontinency : urge in continencec) Incontinency : urge in continenced) hesitancy,intermittency,straining to d) hesitancy,intermittency,straining to
void,terminal dribbling void,terminal dribbling . .
SYMPTOMSSYMPTOMS Emptying FailureEmptying Failure
a) feeling of incomplete emptyinga) feeling of incomplete emptying
b) frequency , urgencyb) frequency , urgency
c) incontinency (overflow)c) incontinency (overflow)
d) hesitancy,intermittency,straining to d) hesitancy,intermittency,straining to void,terminal dribblingvoid,terminal dribbling..

Symptoms are the same in Symptoms are the same in all typesall types!!
70%70% mismanagement mismanagement based on history alonebased on history alone!!
COMPLICATIONSCOMPLICATIONS
11))rise in rise in Pv:REFLUX:Hydroureter/HydronephrosPv:REFLUX:Hydroureter/Hydronephrosisis
22))Retention:Frequent UTI Retention:Frequent UTI (+reflux:Pyelonephritis) (+reflux:Pyelonephritis)
33))Urinary stonesUrinary stones
44))Impaired social & personal lifeImpaired social & personal life
NEUROGENIC BLADDERNEUROGENIC BLADDER
NEUROLOGIC DISEASESNEUROLOGIC DISEASES
Voiding dysfunction is Voiding dysfunction is important in multiple sclerosisimportant in multiple sclerosis
Because ofBecause of::
11 - -Frequency (up to 90% of patients)Frequency (up to 90% of patients)
22 - -Serious complications: 55% Serious complications: 55% → 5%→ 5%
33 - -Impairment of social &personal life Impairment of social &personal life & sexual activity& sexual activity
44 - -Could be successfully managedCould be successfully managed
55 - -Social & cultural aspectsSocial & cultural aspects
MSMSSYMTOMSSYMTOMS
- -Voiding dysfunction may be the sole Voiding dysfunction may be the sole initial complaint ( initial complaint ( 2.3%2.3% ) )..
- -Or part of the presenting symptoms Or part of the presenting symptoms ( 10% ) ( 10% )
NEUROLOGIC DISEASESNEUROLOGIC DISEASESCVACVA
Cerebral Shock:Det.Cerebral Shock:Det.AreflexiaAreflexia:Retention:Retention
Afew weeks/months Afew weeks/months later:later:Det.HyperreflexiaDet.Hyperreflexia
NEUROLOGIC DISEASESNEUROLOGIC DISEASESMSAMSA
Urinary symptoms are commonUrinary symptoms are common
Come early (60% before or associated Come early (60% before or associated withwith
other symptomsother symptoms
Even Even 4yr before diagnosis4yr before diagnosis

AUTONOMIC DYSREFLEXIAAUTONOMIC DYSREFLEXIA
Is a lethal emergencyIs a lethal emergency
Acute massive disorderd autonomic(S) Acute massive disorderd autonomic(S) response to specific stimuli in SC response to specific stimuli in SC injury above T6- T8injury above T6- T8
More common in cervicalMore common in cervical
After shock period but up to yrs after After shock period but up to yrs after injuryinjury
Stimuli below level of the lesionStimuli below level of the lesion
AUTONOMIC DYSREFLEXIAAUTONOMIC DYSREFLEXIA
Headache/HTN(even ICH or sezure)Headache/HTN(even ICH or sezure)Flashing of face,body above the lesionFlashing of face,body above the lesionSweatingSweatingUsually bradycardia,maybe Usually bradycardia,maybe tachycardia/arrhytmiatachycardia/arrhytmiaStimulus from: bladder/rectum: Stimulus from: bladder/rectum: distention,manipulation distention,manipulationGI/bone FX /sexual activity /bed soreGI/bone FX /sexual activity /bed sore

AUTONOMIC DYSREFLEXIAAUTONOMIC DYSREFLEXIA
Endoscopic procedure: spinal/ general Endoscopic procedure: spinal/ general anesthesia anesthesia
SL niphedipin/ oral niphedipin/ trazocinSL niphedipin/ oral niphedipin/ trazocin
Significant rise in BP without other Significant rise in BP without other symptomssymptoms

DiagnosisDiagnosis
11 - -History: ask strictly about voiding History: ask strictly about voiding symptoms and feeling of symptoms and feeling of incomplete emptying incomplete emptying
22 - -exam: pelvic examexam: pelvic exam Sacral reflex examSacral reflex exam
Signs of spinal cord involvmentSigns of spinal cord involvment33 - -Lab : U/A, U/C, BUN, CrLab : U/A, U/C, BUN, Cr
DiagnosisDiagnosis
44 - -Imaging : sonographyImaging : sonography
a) Anatomya) Anatomy
b) Residue b) Residue ( up to 100( up to 100CCCC))

DiagnosisDiagnosis
55 - -In In –– out catheter method out catheter method::
a) Well hydrated for 48 hra) Well hydrated for 48 hr
b) Drink 2 glasses of water, before examb) Drink 2 glasses of water, before exam
c) First desire to void = capacity(c) First desire to void = capacity(300300 –– 500cc500cc))
d) Measure residue after voidingd) Measure residue after voiding

DiagnosisDiagnosis Urodynamic studyUrodynamic study
A general term for the study of the A general term for the study of the storage and voiding functionstorage and voiding function

DiagnosisDiagnosisUrodynamic studyUrodynamic study
a) Bladder eapacity (300 a) Bladder eapacity (300 –– 500cc) 500cc)
b) Detrussor pressure, Max 10 Cm H2ob) Detrussor pressure, Max 10 Cm H2o
c) DSDc) DSD
d) Detressor instabilityd) Detressor instability
e) L.P.P (leak point pressure)e) L.P.P (leak point pressure)

DiagnosisDiagnosisUrodynamic studyUrodynamic study
Indication Indication - -urologic problems: Contraversyurologic problems: Contraversy
- -Neurologic problemsNeurologic problems::
All with neurogenic bladderAll with neurogenic bladder should undergo urodynamic study should undergo urodynamic study to characterize the nature of the to characterize the nature of the problem and to determine problem and to determine prognosis and prognosis and managementmanagement. .

MANAGEMENTMANAGEMENTGOALSGOALS
11 - -upper tract preservationupper tract preservation
22 - -absence or control of infectionabsence or control of infection
33 - -adequate storage at low I.V.Padequate storage at low I.V.P
44 - -adequate emptying at low I.V.Padequate emptying at low I.V.P
55 - -adequate controladequate control
66 - -no catheterno catheter
77 - -social acceptabilitysocial acceptability
MANAGEMENTMANAGEMENTSTORAGE FAILURESTORAGE FAILURE
11 ) )Non surgicalNon surgical::
a) Non pharmacologica) Non pharmacologic
b) Pharmacologicb) Pharmacologic
22 ) )surgicalsurgical

MANAGEMENTMANAGEMENTSTORAGE FAILURESTORAGE FAILURE
NON PHARMACOLOGICNON PHARMACOLOGIC
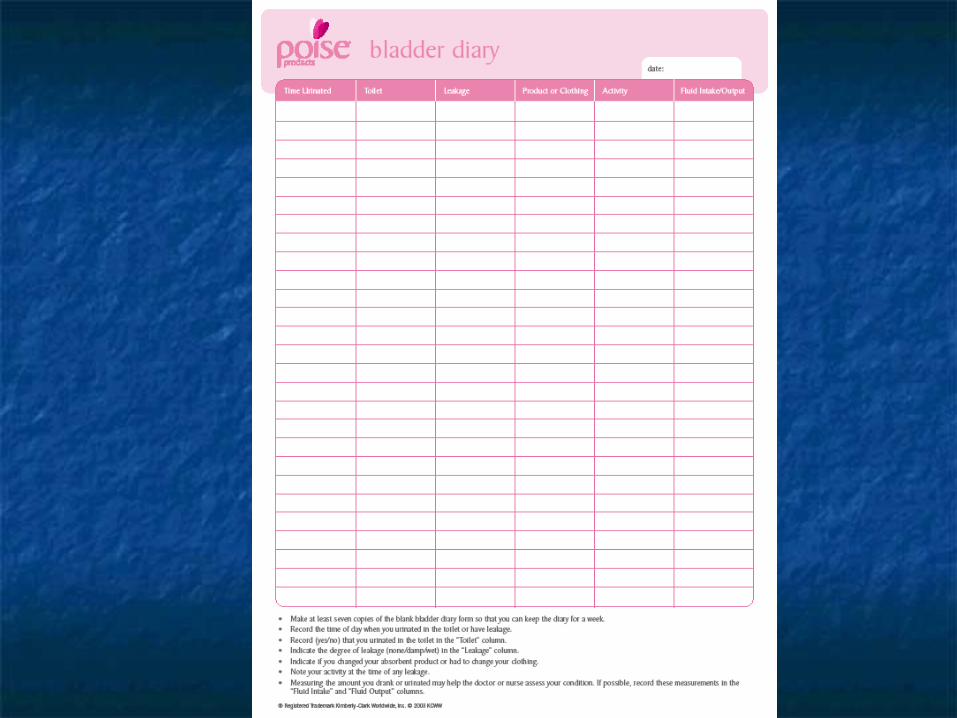
11 - -voiding diaryvoiding diary: 3-5 days: 3-5 days
a) Total 24hr urinary outputa) Total 24hr urinary output
b) Number of voidsb) Number of voids
c) Voiding intervalc) Voiding interval
d) Diurnal distributiond) Diurnal distribution
e) Timing and triggers for e) Timing and triggers for incontinenceincontinence
MANAGEMENTMANAGEMENTSTORAGE FAILURESTORAGE FAILURE
Bladder training programBladder training program: : 11 - -lengthen the amount of time lengthen the amount of time
between voidingbetween voiding..22 - -increase the amount of urine the increase the amount of urine the
bladder can holdbladder can hold. . 33 - -improves the control over the urgeimproves the control over the urge..
44 - -patient gives voiding program to his patient gives voiding program to his bladder bladder..
11 - -Kegel exerciseKegel exercise..22 - -delaying urination,5 min delaying urination,5 min → 10 min→ 10 min
Walk instead of running at urgeWalk instead of running at urge Relaxation techniquesRelaxation techniques
33 - -sheduled bathroom tripssheduled bathroom trips::Every 1hr initiallyEvery 1hr initially..
44 - -irritating factors: Alcohol, caffeine, acidic irritating factors: Alcohol, caffeine, acidic foods (tomatoes, grapefruit)foods (tomatoes, grapefruit)
55 - -change of temperaturechange of temperature..66 - -bio feedback and acupuncturebio feedback and acupuncture . .
MANAGEMENTMANAGEMENTSTORAGE FAILURESTORAGE FAILURE
BLADDER TRAINING PROGRAMBLADDER TRAINING PROGRAM
11 - -anti cholinergicsanti cholinergics::
a) Tolterodine 1-2 mg/bida) Tolterodine 1-2 mg/bid
b) Oxybutinine 5 mg/TDSb) Oxybutinine 5 mg/TDS
22 - -TCA: imipramin 25 mg/dayTCA: imipramin 25 mg/day
33 - -desmopressin , spray, 1-2 puffdesmopressin , spray, 1-2 puff
44 - -Ca antagonists/potassium channel Ca antagonists/potassium channel openers/prostaglandin openers/prostaglandin
inhibitorsinhibitors……????
MANAGEMENTMANAGEMENTSTORAGE FAILURESTORAGE FAILURE
pharmacologicpharmacologic
WarningWarning!!!!!!
AnticholinergicAnticholinergic : :
11 - -check for residue beforecheck for residue before
22 - -check for pharmacologic retention check for pharmacologic retention afterafter
MANAGEMENTMANAGEMENTSTORAGE FAILURESTORAGE FAILURE
pharmacologicpharmacologic

MANAGEMENTMANAGEMENTSTORAGE FAILURESTORAGE FAILURE
SURGICALSURGICAL11 - -intravesical injection of botolinum intravesical injection of botolinum
toxin toxin oxybutinin oxybutinin capsaicin capsaicin??
22 - -electrical stimualtionelectrical stimualtion
33 - -denervation techniquesdenervation techniques
44 - -augmentation cystoplastyaugmentation cystoplasty
MANAGEMENTMANAGEMENTEMPTYING FAILUREEMPTYING FAILURE
11 - -Non surgicalNon surgical
a) Non pharmacologica) Non pharmacologic
b) Pharmacologicb) Pharmacologic
22 - -surgicalsurgical
MANAGEMENTMANAGEMENTEMPTYING FAILUREEMPTYING FAILURE
NON PHARMACOLOGICNON PHARMACOLOGIC11 - -Valsalva Valsalva –– crede manuver: crede manuver:
Increase I.V.P Increase I.V.P
22 - -trigger voidtrigger void
33 - -clean intermittent clean intermittent catheterization( catheterization( CICCIC ) )

MANAGEMENTMANAGEMENTEMPTYING FAILUREEMPTYING FAILURE
NON PHARMACOLOGICNON PHARMACOLOGICCICCIC
11 - -safesafe22 - -extremely effectiveextremely effective
33 - -most practical means of attaining catheter most practical means of attaining catheter - free state- free state
44 - -preserves the independencepreserves the independence55 - -protects the kidneysprotects the kidneys
66 - -prevents incontinenceprevents incontinence77 - -decrease infectionsdecrease infections
88 - -non expensivenon expensive

MANAGEMENTMANAGEMENTEMPTYING FAILUREEMPTYING FAILURE
NON PHARMACOLOGICNON PHARMACOLOGICCICCIC
99 - -can be used in all types of dysfunctioncan be used in all types of dysfunction
1010 - -decrease residue after a whiledecrease residue after a while
- -If the patient can eat or write can do CICIf the patient can eat or write can do CIC
Cornerstone of treatmentCornerstone of treatment

MANAGEMENTMANAGEMENTEMPTYING FAILUREEMPTYING FAILURE PHARMACOLOGICPHARMACOLOGIC
11 - -bethanecholbethanechol??
22 - -baclofenbaclofen
33 - -prosteglandinprosteglandin????

MANAGEMENTMANAGEMENT EMPTYING FAILUREEMPTYING FAILURE
SURGICALSURGICAL11 - -electrical stimulationelectrical stimulation
22 - -bladder myoplstybladder myoplsty
33 - -reduction cytoplastyreduction cytoplasty