neurological progress - university of … progress principles and pitfalls of nerve conduction...
TRANSCRIPT

NEUROLOGICAL PROGRESS
Principles and Pitfalls of Nerve Conduction Studies
Jun IGmura, MD
~ ~ ~
This report reviews the fundamental principles and the changing concepts of nerve stimulation techniques, and discusses the proper application of these techniques in the differential diagnosis of peripheral nerve disorders. Nerve conduction stlldies help delineate the extent and distribution of the neural lesion and distinguish two major categories of peripheral nerve disease: demyelination and axonal degeneration. Although the method is based on simple princi- ples, pitfalls abound in practice.
Variability in nerve conduction measurement may result from temperature change, variations among nerve seg- ments, and the effects of age. Other sources of error include excessive spread of stimulation current, anomalous innervation, temporal dispersion, and inaccuracy of surface measurement. Unlike a bipolar derivation, which selec- tively records near-field potentials, a referential recording may give rise to stationary far-field peaks from a moving source. Overlooking this possibility can lead to an incorrect interpretation of findings.
Conventional nerve conduction studies deal primarily with measurements of the distal nerve segments in an extrem- ity. More recent techniques are applicable to less accessible anatomical regions, as illustrated by elicitation of the blink reflex, F wave, and H reflex, and the use of the inching technique. Other methods used to assess special aspects of nerve conduction include the ischemic test and studies of slow-conducting fibers.
lmura J. Principles and pitfalls of nerve conduction studies. Ann Neurol 16:415-429, 1984
Nerve conduction studies ate useful in evaluating dis- eases of peripheral nerves. With steady improvement and standardization of methods, they have become a reliable test in clinical settings [33 , 551. They are now widely used not only for precise localization of a lesion, but also for accurate characterization of peripheral nerve function [ 14,481. The technique consists of elec- trical stimulation of a nerve and recording of the evoked potentials either from the muscle or from the nerve itself. Although the methods are relatively sim- ple, various technical factors influence the measure- ments and a number of pitfalls can lead to a wrorlg or misleading conclusion [73}. Recognition of the inher- ent limitations of the method can minimize such errors. For quick reference, Table 1 lists the concepts and procedures reviewed with a brief caption summarizing the key points for each heading.
Types of Neuropathic Abnormality Seddon [68} defined three degrees of nerve injury: neutapraxia, axonotmesis, and neurotmesis. In neura- praxia conduction ceases without structural change in the axon. Fibers usually regain function promptly within days or weeks, although nerve block from acute entrapment may occasionally last for as long as several years C621. In compressive lesions demyelination may
accompany neurapraxia, and remyelination must occur before conduction returns to normal f3 1, 321. Axonot- mesis results from loss of axonal continuity, leading to wallerian degeneration of the distal segment. The nerve fibers regenerate slowly at a rate of 1 to 3 mm per day, often leading to eventual recovery of function. In neurotmesis injury separates the entire nerve, in- cluding the connective elements. With supporting tis- sue lost, regeneration is poorly organized and incom- plete r751.
The electrophysiological abnormalities depend on the kind and degree of damage in individual nerve fibers within the nerve. Although different types of abnormality can coexist, the results of conduction stud- ies usually correlate well with the overall structural ab- normalities {30, 33, S S } . In segmental dernyelination, or during partial remyelination, thin myelin increases the internodal capacitance and conductance, leading to loss or diminution of local current. Failure to acti- vate the next node of Ranvier results in conduction block. When function returns, impulses propagate more slowly than normal, because it takes longer for the dissipated current to generate an action poten- tial. Thus, demyelinated axons characteristically show blocking of impulses, substantial decreases in conduc- tion velocity (commonly, although not always, to less
From the Division of Clinical Electrophysiology, Department of Neurology, University of Iowa Hospitals and Clinics, Iowa City, 1A 52242.
Received December 30, 1983, and in revised form March 20, 1084. Accepted for publication March 23, 1084.
Address reprint requests to Dr Kimura.
41 5
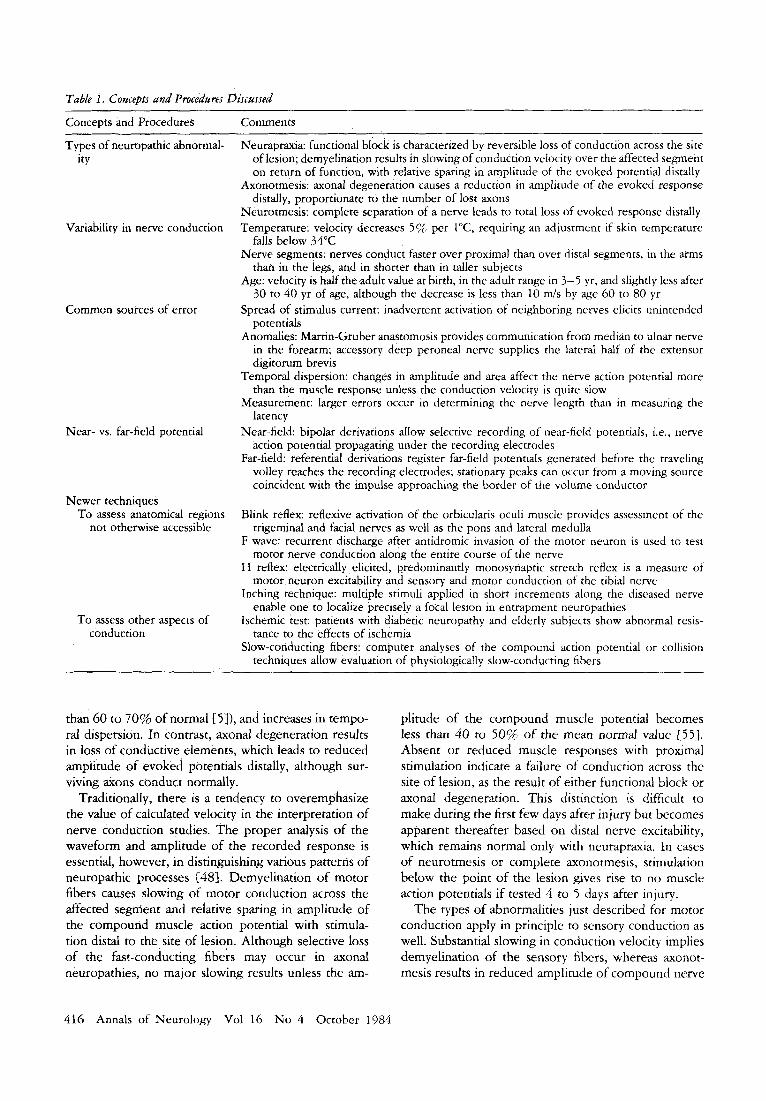
Table 1. Concepts and Procedares Discussed
Concepts and Procedures Comments
Types of neuropathic abnormal- ity
Variability in nerve conduction
Common sources of error
Near- vs. far-field potential
Newer techniques To assess anatomical regions
not otherwise accessible
To assess other aspects of conduction
Neurapraxia: functional block is characterized by reversible loss of Conduction across the site of lesion; demyelination results in slowing of conduction velocity over the affected segment on return of function, with relative sparing in amplitude of the evoked potential distally
Axonotmesis: axonal degeneration causes a reduction in amplitude of the evoked response distally, proportionate to the number of lost axons
Neurotmesis: complete separation of a nerve leads to total loss of evoked response distally Temperature: velocity decreases 5% per 1"C, requiring an adjustment if skin temperature
falls below 34°C Nerve segments: nerves conduct faster over proximal than over distal segments, in the arms
than in the legs, and in shorter than in taller subjects Age: velocity is half the adult value at birth, in the adult range in 3-5 yr, and slightly less after
30 to 40 yr of age, although the decrease is less than 10 m l s by age 60 to 80 yr Spread of stimulus current: inadvertent activation of neighboring nerves elicits unintended
potentials Anomalies: Martin-Gruber anastomosis provides communication from median to ulnar nerve
in the forearm; accessory deep peroneal nerve supplies the lateral half of the extensor digitorum brevis
Temporal dispersion: changes in amplitude and area affect the nerve action potential more than the muscle response unless the conduction velocity is quite slow
Measurement: larger errors occur in determining the nerve length than in measuring the latency
Near-field: bipolar derivations aIIow selective recording of near-field potentials, i.e., nerve action potential propagating under the recording electrodes
Far-field: referential derivations register far-field potentials generated before the traveling volley reaches the recording electrodes; stationary peaks can occur from a moving source coincident with the impulse approaching the border of the volume conductor
Blink reflex: reflexive activation of the orbicularis oculi muscle provides assessment of the
F wave: recurrent discharge after antidromic invasion of the motor neuron is used to test
H reflex: electrically, elicited, predominantly monosynaptic stretch reflex is a measure of
Inching technique: multiple stimuli applied in short increments along the diseased nerve
Ischemic test: patients with diabetic neuropathy and elderly subjects show abnormal resis-
Slow-conducting fibers: computer analyses of the compound action potential or collision
trigeminal and facial nerves as well as the pons and lateral meduila
motor nerve conduction along the entire course of the nerve
motor neuron excitability and sensory and motor conduction of the tibia1 nerve
enable one to localize precisely a focal lesion in entrapment neuropathies
tance to the effects of ischemia
techniques allow evaluation of physiologically slow-conducting fibers
than 60 to 70% of normal IS}), and increases in tempo- ral dispersion. In contrast, axonal degeneration results in loss of conductive elements, which leads to reduced amplitude of evoked potentials distally, although sur- viving axons conduct normally.
Traditionally, there is a tendency to overemphasize the value of calculated velocity in the interpretation of nerve conduction studies. The proper analysis of the waveform and amplitude of the recorded response is essential, however, in distinguishing various patterns of neuropathic processes [48}. Demyelination of motor fibers causes slowing of motor conduction across the affected segnient and relative sparing in amplitude of the compound muscle action potential with stimula- tion distal to the site of lesion. Although selective loss of the fast-conducting fibers may occur in axonal neuropathies, no major slowing results unless the am-
plitude of the compound muscle potential becomes less than 40 to 50% of the mean normal value { 5 5 ] . Absent or reduced muscle responses with proximal stimulation indicate a failure of conduction across the site of lesion, as the result of either functional block or axonal degeneration. This distinction is difficult to make during the first few days after injury but becomes apparent thereafter based on distal nerve excitability, which remains normal only with neurapraxia. In cases of neurotmesis or complete axonotrnesis, stimulation below the point of the lesion gives rise to no muscle action potentials if tested 4 to 5 days after injury.
The types of abnormalities just described for motor conduction apply in principle to sensory conduction as well. Substantial slowing in conduction velocity implies demyelination of the sensory fibers, whereas axonot- mesis results in reduced amplitude of compound nerve
416 Annals of Neurology Vol 16 No 4 October 1984

action potentials with stimulation distal to the site of lesion. Degeneration of sensory fibers occurs only with a postganglionic lesion, such as plexopathy or periph- eral neuropathy [12). This fact can be used as a crite- rion in differentiating postganglionic from pregangli- onic disorders, such as syringomyelia or root avulsion. In this context, normal sensory nerve action potentials, seen in patients with sensory loss after trauma, indicate a poor prognosis for recovery because preganglionic avulsion precludes regeneration of the sensory fibers.
Variability in Nerve Conduction Several factors alter the rate of nerve conduction. Most important in a clinical laboratory are temperature of the tested nerve, normal variations among nerves and nerve segments, and patient age.
Temperature The conduction velocity in nerves increases almost linearly with the body temperature [ 15). The change is approximately 5% per degree, or 2.4 m l s on the aver- age, as the temperature measured near the nerve rises from 29 to 38°C. Conversely, latencies of the median and ulnar nerves from the wrist to the innervated mus- cle increase by 0.3 ms per degree upon cooling the hand. Lower temperatures augment the amplitude of nerve and muscle potential, however, as demonstrated originally in the squid axon 1391 and more recently in human studies 116). To reduce this type of variability, it is best to conduct studies in a warm room with the temperature maintained between 21 and 23°C. If the skin temperature falls below 34"C, the limbs should be warmed 1171. Alternatively, one may add 5% of the calculated conduction velocity for each degree below 34°C to normalize the results. Such conversion factors, however, may provide misleading interpretations with diseases of the peripheral nerve [2).
Variation Among Newes and Segments Both motor and sensory conduction velocities are sub- stantially slower in the legs than in the arms. A small reduction in temperature cannot account for the re- corded differences, ranging from 7 to 10 d s (51, 78). Longer nerves may generally conduct more slowly than shorter nerves, as suggested by the inverse relationship between height and nerve conduction velocity 161. Al- though the conduction velocity is dissimilar in the arms and legs, there is no difference between the median and ulnar nerves or between tibial and peroneal nerves 1481.
Conduction velocity is generally faster in the prox- imal than in the distal segments of a nerve. In humans, for example, the most proximal motor nerve conduc- tion velocity determined by F wave latency is greater than the conventionally derived most distal conduction velocity {43). The factors responsible for the velocity
gradient include progressive reduction in axonal diam- eter, shorter internodal distances, and lower distal tem- peratures. Relative distal slowing, however, is not uni- versal; in the baboon single motor axons conduct more slowly in the brachial plexus than in the peripheral nerve trunk 19).
Age Nerve conduction velocities increase rapidly during the first few years of life, from roughly half the adult value in full-term infants 1763 to the adult range at age 3 to 5 years. The conduction velocities are even slower in premature infants, ranging from 17 to 25 m / s in the ulnar nerve and from 14 to 28 m / s in the peroneal nerve [8]. Conduction velocities begin to decline after 30 to 40 years of age, but the decrease is normally less than 10 m l s by the sixtieth to eightieth year 1641. The evoked amplitude diminishes in old age in association with changes in the shape of the evoked potential, es- pecially at the common sites of compression. The laten- cies of the F wave and somatosensory evoked poten- tials also gradually increase with age (19, 231.
Common Sources of Error The determination of nerve conduction velocities is subject to a number of common pitfalls [73). Unex- pected findings during nerve conduction studies usu- ally result from technical errors originating in the stimulating or recording system C48). One can easily correct most properly identified problems, which in- clude: (1) the spread of the stimulating current to a nerve not under study, eliciting an unwanted potential from distant muscles; (2) the presence of an anasto- mosis between the median and ulnar nerves in the forearm, and anomalous innervation of the extensor digitorum brevis by the accessory deep peroneal nerve; (3) the effect of temporal dispersion; and (4) the errors inherent in the measurement of nerve length and con- duction time.
Spread of Stimulation Cuwent When one delivers an inappropriately high shock in- tensity, stimulating current may spread to a nerve or muscle not being tested. Under these circumstances visual inspection of the contracting muscle is often of value in confirming the presence or absence of selec- tive activation of the intended nerve. Needle elec- trodes allow one to record from more limited areas in studying the innervation of individual motor branches or patterns of abnormality. They do not reliably record the size of compound muscle action potentials, how- ever.
The median and ulnar nerves lie close together at the axilla [431. If a stimulating current intended for the median nerve spreads to the ulnar nerve, the electrodes placed on the thenar eminence record a potential origi-
Neurological Progress: Kimura: Nerve Conduction Studies 41 7
Site of Stimulation
Wrist (S,)
Elbow(Sz1
Axillo(S,)
Axill0(S3) 0nd
Wrist (S4)
Hvwfhenar
52
5 rnsec
Fig I . Motor conduction study in a 39-year-old man with carpal tunnel syndrome, showing stimulation of the median nerve at the wrist (SJ, elbow (SZ), and axilkz (SJ and recording of the muscle action potentials over the thenar eminence. Axillavy stimulation (S3/ spread to the ulnar nerve (third tracing from the top), ac- tivating an unintended short-latency potential fmm the ulnar-in- nervated thenar muscles (arrowhead with question mark). Another stimulus (S4) applied to the ulnar nerve at the wrist (bottom tracingi blocked the proximal impulses by collision. (From Kimura {44), with permission.)
nating from ulnar-innervated muscles. The measured latency will be erroneously short when the median nerve conducts more slowly than the ulnar, as in the carpal tunnel syndrome. In such cases a stimulus at the elbow activates only the median nerve, revealing the prolonged latency. The reverse discrepancy can oc- cur in a study of tardy ulnar palsy, with inadvertent spread of stimulation to the median nerve at the axilla.
Selective median or ulnar nerve assessment is possi- ble despite coactivation of both nerves proximally if one resorts to a physiological nerve block, with a distal stimulus applied to the nerve not under consideration [44]. In studying the median nerve, for example, one delivers a distal stimulus to the ulnar nerve (Fig 1). The antidromic impulse from the wrist then collides with an orthodromically directed impulse from the axilla in the ulnar nerve, allowing only the median impulse to reach the muscle. The ulnar response induced by the dis- tal stimulus occurs much earlier without obscuring the median compound muscle action potential under study. Conversely, a distal stimulus to induce a physio-
Site of Stimulation
Wrist (S,)
'4 ypofhcnar
3 rnsec
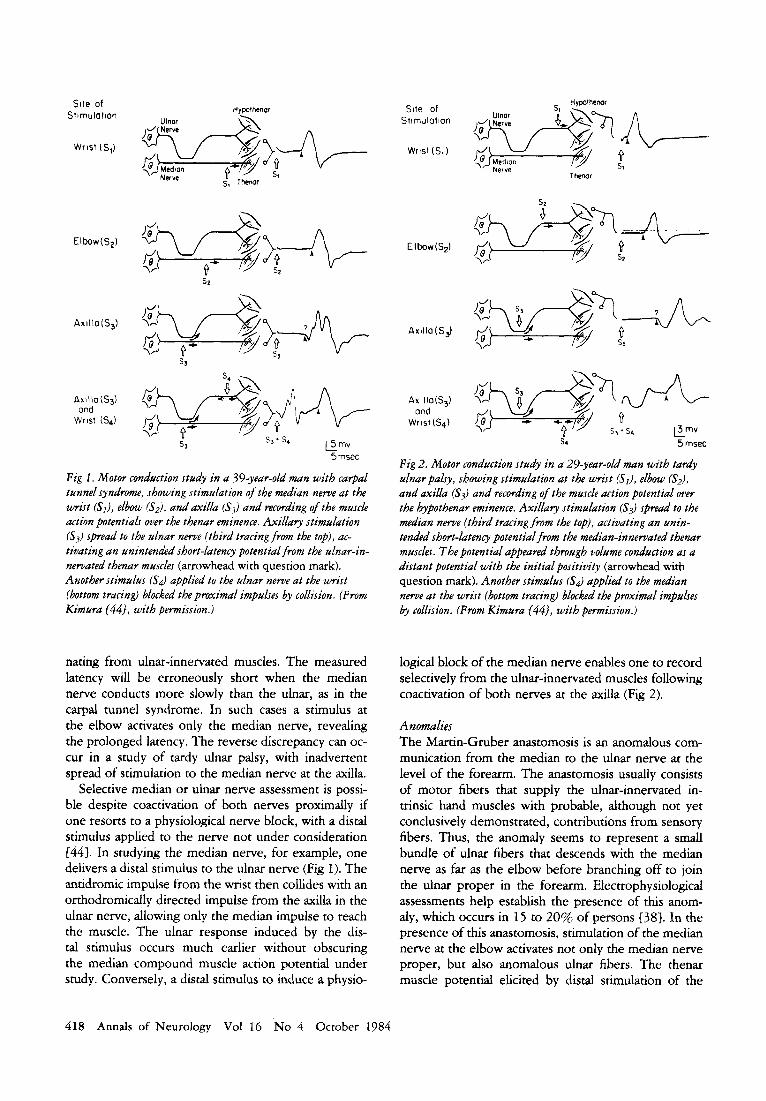
Fig 2. Motor conduction study in a 29-year-old man with tardy ulnar palsy, showing stimulation at the wrist (SJ, elbow (S2), and axilla (S3) and recording of the muscle action potential over the hypothenar eminence. Axillavy stimulation (S3) spread to the median nerve (third tracing from the top), activating an unin- tended short-latency potential from the median-innervated thenar muscles. The potential appeared through volume conduction as a distant potential with the initial positivity (arrowhead with question mark). Another stimulus (S$ applied to the median nerve at the wrist (bottom tracing) blocked the proximal impulses b3, collision. (From Kimura {44), with permission.)
logical block of the median nerve enables one to record selectively from the ulnar-innervated muscles following coactivation of both nerves at the axilla (Fig 2).
Anomalies The Martin-Gruber anastomosis is an anomalous com- munication from the median to the ulnar nerve at the level of the forearm. The anastomosis usually consists of motor fibers that supply the ulnar-innervated in- trinsic hand muscles with probable, although not yet conclusively demonstrated, contributions from sensory fibers. Thus, the anomaly seems to represent a small bundle of ulnar fibers that descends with the median nerve as far as the elbow before branching off to join the ulnar proper in the forearm. Electrophysiological assessments help establish the presence of this anom- aly, which occurs in 15 to 20% of persons [38]. In the presence of this anastomosis, stimulation of the median nerve at the elbow activates not only the median nerve proper, but also anomalous ulnar fibers. The thenar muscle potential elicited by distal stimulation of the
418 Annals of Neurology Vol 16 No 4 October 1984

Hypothenor
" L m v 5msec
Fig 3. Study of median nerve motor conduction in a 55-year-old mun with carpal tunnel syndrome and a Martin-Gruber anasto- mosis, showing muscle potentials recorded from the thenrlr emi- nence after stimulation of the median nerve at the wrist (S,) and elbow (S2). The stimulus at the elbow CS2) spread to the ulnar nerve through the anomalous communication (middle tracing), uctivating an unintended potential from the ulnar-innervated thenar muscles. Atzother stimulus CS.3) applied to the ulnar nerve at the wrist (bottom tracing) blocked the impulses transmitted through the communicating fibers. The stimulus at the wrist (S3) preceded the stimulation at the elbow (S2) by 4 ms to avoid an overkip of the compound muscle action potentials elicited by these two stimuli. (From Kimura {44). with permission.)
median nerve at the wrist is smaller, because the ulnar component is absent. With stimulation of the ulnar nerve, the reverse discrepancy occurs in the amplitude of compound muscle action potentials. The response from ulnar-innervated thenar or hypothenar muscles is smaller with stimulation at the elbow than at the wrist, because the distal stimulation activates additional anomalous fibers. Again, a collision technique provides selective blocking of unwanted impulses transmitted via the anomalous fibers (Fig 3 ) . Without such a ma- neuver one cannot calculate accurate conduction veloc- ity in the presence of anomalous innervation.
The most frequent anomaly of the leg is the pattern of innervation to the extensor digitorurn brevis, which usually derives its supply from the deep peroneal nerve, a major branch of the common peroneal nerve { S S } . In 20 to 28% of subjects, this muscle also re- ceives innervation from the accessory deep peroneal nerve, an anomalous branch of the superficial peroneal nerve. With this anastomosis, the compound muscle action potential of the extensor digitorum brevis is smaller with stimulation of the deep peroneal nerve at the ankle than with stimulation of the common peroneal nerve at the knee. Stimulation of the acces-
sory deep peroneal nerve behind the lateral malleolus activates the anomalously innervated lateral portion of the muscle. In the presence of this anomaly, lesions of the deep peroneal nerve spare the lateral portion of the extensor digitorum brevis, giving rise to the possibility of an incorrect conclusion {37].
Temporal Dispersion The impulses of slow-conducting fibers lag increasingly behind those of fast-conducting fibers over a long con- duction path. Hence, the duration of the compound sensory nerve or muscle action potential is greater, and the amplitude smaller, with an increasing conduction distance after stimulation of a nerve E48, 65, Sl}. Tem- poral dispersion appears to alter the waveform of the sensory nerve potentials more than the compound muscle action potentials 148, 81). Thus, if one stimu- lates proximally at the axilla or Erbs point and records distally from the digit, the antidromic sensory potentid may be quite small or inconsistent even though stimu- lation at the wrist or palm elicits a large response (Fig 4). A physiological reduction in amplitude of the sen- sory potential as well as the area under the waveform may erronepusly suggest a conduction block between the proximal and distal sites of stimulation.
Physiological temporal dispersion affects the nerve action potential more than the muscle response, per- haps because an individual unit discharge lasts for a substantially shorter period in the former than in the latter [48}. With a slight shift in latency of shon- duration diphasic sensory spikes, the positive peak from one axon may line up exactly with the negative peak from a second axon, canceling out both. In con- trast, the same latency shift would superimpose long- duration motor unit potentials nearly in phase, result- ing in less reduction in the area under the waveform. In a demyelinative neuropathy, however, an excessive temporal dispersion with proximal stimulation can re- sult in substantial diminution of the compound muscle action potential, giving rise to a false impression of a motor conduction block as well. Ih addition, when one stimulates proximally in an extremity and records anti- dromic digital potentials distally, orthodromic sensory volleys generated by ongoing natural stimuli may col- lide with the intended signal in some fibers. This ten- dency will be greater in proportion to the nerve length between the stimulating and recording electrodes.
If the evoked potentials are dissimilar in shape when elicited by distal and proximal stimuli, the latencies measured to the onset of the evoked potential proba- bly represent fibers of different conduction characteris- tics. This phenomenon may occur if one delivers a sub- maximal stimulus at one point and a supramaximal stimulus at a second site. In diseased nerves the im- pulse from a proximal site of stimulation may fail to propagate in some fibers because of conduction block
Neurological Progress: Kimura: Nerve Conduction Studies 419

Median nerve Ulnar nerve
J even with an adequate shock intensity. In addition, ap- parently supramaximal stimuli may not activate the en- tire bundle of axons if fibrosis or other local structural changes interfere with the current reaching the axons. Under any of these circumstances, one cannot calculate the conduction velocity accurately using the conven- tional formula.
Errors Inherent in the Measurement One must regard calculated nerve conduction veloci- ties as an approximation rather than an absolute value because of inherent errors in measuring the nerve length. Surface measurement commonly overestimates or underestimates the conduction distance, particularly when the nerve takes a nonlinear path, as in the bra- chial plexus or across the elbow or knee. An additional error can result from commonly encountered problems in latency determination, which include unstable or incorrect triggering of the sweep, poorly defined take- off of the evoked responses, inappropriate stimulus strength, and inaccurate calibration. Because of these limitations, the values of conduction studies may occa- sionally vary as much as 10 m/s on repeated testing.
Although any stimulus must be supramaximal to be reliable, an excessive shock intensity can cause an un- usually short latency by depolarizing the nerve seg- ment away from the stimulating cathode. In this case the surface length between the two stimulus points may not correspond to the calculated conduction time across the nerve segment under study (821. Also, a small nerve potential can sometimes precede the main
v 2 ms
F i g 4. Antidromic sensoly nerve conduction studie.s in a healthy subject. with stimulation of the median neme I[&) at the u x i h (A), elbow IB). wrist CC), and palm ( D ) , and of the ulnar nerve (right) at the axilla (El , abom tF) and below (GI elbow, and wri.ft (Hi. Single stimuli ofthe median and ulnar newes elicited a discrete sensory potential of the third and fifth digit.s, respec- t i dy . To improve resolution. houwer, eacb test set consiited J a n atwage of fifty summated responses. A physiological temporal di.r- persion resulted in reduction of not only the amplitude but a h the area under the waveform u.ith proximal as opposed t o dirtai stimulation.
negative component of a compound muscle actiola po- tential [36}. If one needs to resort to a different amplifier gain to visualize the muscle potential with distal and proximal stimulation, this prepotential may appear with stimulation at one point but not at a second point. Awareness of this possibility is important, be- cause the recorded latency would be erroneously short if measured to the onset of the nerve prepotential.
Near-Field versus Far-Field Potentials In surface recording of evoked potentials from a nerve, connective tissue and interstitial fluid act as a conduct- ing medium or a volume conductor. The position of recording electrodes within the volume conducror de- termines the waveform of a nerve action potential IS]. In a bipolar recording, used in the conventional sen- sory nerve conduction measurement, one places an ac- tive electrode (GI) on the nerve and an indifferent electrode (G2) 2 to 3 cm away. This derivation allows
420 Annals o f Neurology Vol 16 No 4 October 1984

selective recording of a near-field potential, i.e., nerve action potential propagating under GI. In contrast, referential recording, with GI over the nerve and G2 at a remote site, registers, in addition to the near-field activity, a far-field potential generated before the traveling volley actually reaches the electrode site [42, 741. The latter derivation has recently become increas- ingly popular in the study of somatosensory evoked potentials (SEPs), because it provides the possibility of detecting deeply situated neural activity not other- wise accessible by surface recording [ll, 18, 20, 21, 50, 83, 841.
A full description of SEPs is outside the scope of this discussion. A brief review of far-field recording seems in order, however, to gain some insight into a complex potential distribution induced by a propagating impulse in a volume conductor. The relationship between near- field and far-field peaks largely remains to be elu- cidated, but particularly puzzling is the origin of sta- tionary far-field peaks from a traveling source. For ex- ample, with stimulation of the median and tibia1 nerves at the wrist and the ankle, the scalp electrode initially registers stationary components P, and PI7 [11 ,21 , 22, 83, 843, respectively, so designated according ta their polarity and average latency. The time of occurrence indicates that Po and PI7 coincide with the arrival of the axonal volley at the distal portion of the brachial and lumbosacral plexuses, respectively. Recent studies, which I will summarize, have elucidated possible physi- ological mechanisms for the appearance of such station- ary peaks from a moving source at certain points in time 122, 49, 631.
The origin of far-field activity becomes apparent in a simple volume conductor if one traces the moving po- tentials along the path directly accessible to surface te- cording. Studies of the antidromic digital potential al- low one to stimulate proximally at the forearm and record distally across the palm and along the digit. Comparison between bipolar and referential recording then provides the temporal relationships between near- field and far-field potentials. In such studies of the ra- dial nerve 1491, stationary peaks appear concomitantly with the entry of the propagating impulse into the wrist and the base of the digit (Fig 5). These findings suggest that the field distribution of propagating volleys some- how relates to the geometry of the volume conductor. The current density may change abruptly at the mo- ment the traveling source approaches a boundary, re- sulting in discontinuity of the flow between the two adjacent geometric regions. An apparently stationary potential would then occur, as if a voltage step devel- oped in the signal 1491.
In a related experiment using bullfrog sciatic and peroneal nerve, Ngkanishi and colleagues [631 demon- strated the close association between generation of ac-
tion potential and abrupt change in the resistance of the conduction medium. According to their observations, changes in the impedance are responsible for genera- tion of stationary peaks in far-field recording. Lueders and co-workers 1591 also speculate that sudden changes in the conduction characteristics of the surrounding tissue can give rise to stationary short-latency peaks of the scalp-recorded SEPs. Thus, in addition to an al- teration in the geometry of the volume conductor 1471, which in turn determines the impedance of the surrounding medium, changes in the overall struc- tural properties of the surrounding medium may be sufficient to generate a time peak secondary to the traveling source. Desmedt and co-workers 1221 have recently shown that the latency of far-field peaks de- pends to some degree on the anatomical orientation of the propagating impulse. Branching of the nerve axons may also play an important role. Hence, the complex waveform of far-field potentials seems to result from a combination of different physiological mechanisms that are uniquely dependent on the physical relationship between the nerve and the volume conductor.
Whatever the physiological basis, a moving impulse may produce an apparently stationary potential in the absence of fixed neural generators, such as those that occur at synapses in relay nuclei. According to conven- tion, a referential derivation allows accurate recording of the traveling potential at GI, provided that Gz is inactive. This assumption is not necessarily valid, how- ever, if a far-field potential superimposes on the near- field activity. In this case, one cannot resort to a ref- erential derivation for determination of conduction time even with GI positianed along the course of the nerve and G2 in an inactive area. Lin and associates [58}, who recorded action potentials with multiple electrodes around the arm, reached a similar conclu- sion. In contrast, a bipolar derivation effectively elimi- nates far-field potentials and other common mode sig- nals and as a result selectively records the near-field potential. Thus, it provides an accurate representation of the actual time of the impulse propagation.
Clinical Value and Limitations of Newer Techniques Nerve stimulation techniques commonly used in an electromyographic laboratory are applicable mainly to the distal segments of the peripheral nerves. More re- cently, several neurophysiological methods have been introduced to supplement the conventional techniques. The selection of technique is necessarily influenced by the special orientation of each laboratory, but of gen- eral interest are the blink reflex, F wave, H reflex, inching technique, ischemic test, and studies of slow- conducting fibers.
Neurological Progress: Kirnura: Nerve Conduction Studies 42 1

Fig 5 . (A) Stimulation ofthe radial nerve 10 cm proximal to the styloid process of the radius and serial recording of antidromic sensory potentials in 1.5 cm increments along the length of the ra- dial nerve. The 0 level is at the base of the second digit, where the volume conductor changes abruptly. In most hands, -t 6 is near the distal crease of the wrist, where another, less obvious transi- tion of volume conductor geomet ry takes place. The ring electrode around the fifth digit is an "indifferent" lead for referential re- cordings. Bipolar and referential recordings of the antidromic sen- soy nerve action potential showed characteristic diffirences in waveform, as illustrated in B. (From Kimura and colleagues {49}, with permission.) (B) Sensory nerve potentials across the hand and along the second digit in a normal subject, recorded antidromically afer stimtllation o f the supetjicial sensory branch of the radial nerve 10 cm proximal t o the styloid process of the radius. The site of recording is indicated (see A). In a bipolar re- cording (left), initial negative peak N, (arrow pointing up) showed a progressive increase in latency and reduction in am- plitude distally. and no response was recorded beyond - 1. In a referential recording (right), biphasic peaks PI-NI and PII-NII (arrows pointing down) showed greater amplitude distally, with a stationary latency iwespective ofthe recording sites along the digit. The onset o f PI extended proximally to the recording electrodes near the wrist (small arrows pointing down), whereas PI1 first appeared at the base of the digit. (From Kimura and col- leagues (491, with permission.)
A
N II
B
I V L 1 .Oms
Blpol o r Recordlnp
( - 3 ) - v
( - 2 ) - v
( - 1 ) - v
( 0 ) - v
( + l ) - v
( + 2 ) - v
( + 3 ) - v
(+"- v
( + 5 ) - v
(+7) - v
( + a ) - v
( + 6 ) - V
l.Ome Referential Recordlng
422 Annals of Neurology Vol 16 No 4 October 1984

Table 2. Direct Response and R l and R2 of the Blink Refex
Disorder Direct Response R1 R2
Trigeminal neuralgia Compressive lesion of
the trigeminal nerve
Normal Normal
Normal (95%) Abnormal on the affected
side (59%)
Bell's palsy
Acoustic neuroma
Guillain-Barre syndrome
Hereditary motor sensory neuropathy, type I
Diabetic polyneuropathy
Multiple sclerosis
Wallenberg's syndrome Facial hypoesthesia
Comatose state; akinetic mutism; locked-in syndrome
Normal unless distal segment degenerated
Normal unless distal
Abnormal (42%)
Abnormal (78%)
Abnormal (13%)
Normal
segment degenerated
Normal Normal
Normal
Abnormal on the affected side (99%)
Abnormal on the affected side (85%)
Abnormal (54%)
Abnormal (85%)
Abnormal (10%)
Abnormal with pontine lesions; greater incidence of abnormality with longer duration of illness
Normal or borderline Abnormal with lesions of
the trigeminal nerve or pons
Abnormal with pontine lesion; reduced excitability in acute supratentorial lesion
Normal Abnormal on both sides
when affected side stimulated (afferent abnormality)
Abnormal on the affected side regardless of the side of stimulus (efferent abnormality)
Afferent and/or efferent abnormality
Afferent andlor efferent abnormality
Afferent and/or efferent abnormality
Afferent and/or efferent abnormality
Afferent and/or efferent abnormality
Afferent abnormality Afferent abnormality
Absent on both sides regardless of side of stimulus
Modified from Kimura 2481, with permission.
Blink Reflex Stimulating the facial nerve with the cathode placed just anterior to the mastoid process elicits compound muscle action potentials in the facial muscles. Desig- nated as the direct response, such a potential provides a measure of distal nerve excitability. A single shock to the supraorbital nerve evokes two separate reflex re- sponses, R1 and R2, of the orbicularis oculi 147, 48, 54,691. Of the .two components, R1 is more stable and is suitable for conduction studies of the reflex arc. The latency of R2 is less reliable for this purpose because of inherent latency variability from one trial to the next, probably based on excitability of interneurons and synaptic transmission. The electrically or mechanically elicited blink reflex reflects the integrity of the trigemi- nal and facial nerves, which form the afferent and ef- ferent arcs, and the pons and lateral medulla, which are the presumed central connections for R1 and R2, re- spectively. The disorders commonly tested by this means 1481 include Bell's palsy, compressive lesions of the trigeminal nerve, Guillain-Bard syndrome and other neuropathies, acoustic neuroma, pontine lesions, and the lateral medullary syndrome (Table 2).
F Wave A supramaximal stimulus applied at virtually any point along the course of a motor nerve elicits a small late response following the regular compound muscle ac- tion potential (M response). This long-latency re- sponse, designated the F wave, is a muscle action po- tential induced by the backfiring of antidromically activated motor neurons. The amplitude ratio of the F wave and M response indicates that recurrent dis- charges occur in about 1% of the motor neuron pool invaded antidromically {27, 52). The F wave latencies measured from the stimulus artifact to the beginning of the evoked potential vary by a few milliseconds from one stimulus to the next 113, 43). Hence, an adequate study requires more than ten F waves clearly identified among fifteen to twenty trials. A most sensitive crite- rion of abnormality is a latency difference between the two sides, or between two ndrves in the same limb in a unilateral disorder affecting a single nerve. Absolute latencies ate useful for assessing the entire course of the nerve in a diffuse process {SS]. The F wave conduc- tion velocity and the F ratio provide a better compari- son between proximal and distal segments 148). The
Neurological Progress: Kimura: Nerve Conduction Studies 423

difference between the minimal and maximal F wave latencies determines the degree of scatter among con- secutive F waves and provides an estimate of the range of motor conduction velocities in the nerve 152, 66).
The F wave measures motor nerve conduction along the entire course of the nerve and thus delineates dif- fuse or widespread conduction abnormalities more ef- fectively than the conventional methods designed to evaluate relatively short, distal segments: slower im- pulses lag farther behind faster impulses over a longer nerve segment. Recent studies have documented the clinical value of the F wave in Charcot-Marie-Tooth disease [43), Guillain-Barre syndrome C45, 531, and diabetic {lo, 511, uremic 1671, and alcoholic neurop- athies {56), as well as in other disorders of the periph- eral nerve C28, 70, 71). The F wave is perhaps most useful diagnostically in detecting polyneuropathies as- sociated with prominent proximal involvement not ac- cessible by conventional methods. The F wave is less effective in the early diagnosis of more localized nerve lesions, such as radiculopathies or compression syn- dromes, in which conduction along the length of the nerve is otherwise normal. Such focal conduction delay across the short segment may not alter the F wave latency above and beyond its inherent variability.
H RefEx The electrically elicited stretch reflex is called the H reflex after Hoffmann, who is credited with its original description. The reflex is equivalent in many respects to the stretch reflex elicited by a mechanical tap to the tendon. The group IA sensory fibers and alpha motor neurons form the afferent and efferent arcs of this pre- dominantly monosynaptic reflex. In clinical tests one must distinguish the H reflex from the F wave with a similar latency. An H reflex occurs with stimulation of the upper limb nerves in newborn infants and during the first year of life C76) but only in the calf muscles and flexor carpi radialis in adults. In contrast, one can elicit the F wave in any distal limb muscles. The effects of increasing stimulus intensity also distinguish the H reflex from the F wave. A stimulus submaximal for the regular compound muscle action potential (M re- sponse) best elicits the H reflex, whereas the F wave requires supramaximal shock intensity. H reflex am- plitude increases initially as the stimulus changes from a subthreshold to submaximal range. When the M re- sponse becomes larger with a further rise in shock intensity, the H reflex diminishes progressively, and the F wave eventually appears with a supramaximal stimulus.
Most commonly used in clinical assessment is the H reflex of the triceps surae, which one records from the soleus after stimulation of the tibial nerve at the knee. The reflex latency thus obtained determines the sen- sory and motor conduction of the tibial nerve C357. In
diabetics, this measurement rivals the conventional nerve conduction studies in the detection of early neuropathic abnormalities {SO}. The test also appears to be a sensitive indicator of mild neuropathies, mat- urational changes in the proximal versus distal segment of the tibial nerve 1791, and S1 radiculopathy { 3 } . The amplitude of the H reflex depends on the strength of electrical stimuli as well as the excitability of the alpha motoneurons. With constant stimuli, therefore, varia- tions in the amplitude provide a measure of excitability changes in the soleus motor neuron 113, 60, 721.
Inching Technique The ordinary conduction studies suffice to identify ap- proximately the area of involvement in entrapment neuropathies (14, 48). More precise localization of such focal slowing is possible by “inching” the stimulus in short increments along the course of the nerve to isolate the affected segment C4, 46, 61). The study of shorter segments provides a better resolution with re- stricted lesions. Assume a nerve impulse conducting at a rate of 0.2 mdcm (50 m / s ) except for a 1 cm segment where a localized demyelination has doubled the con- duction time to 0.4 mdcm. In a 10 cm segment, nor- mally covered in 2.0 ms, a 0.2 ms increase would constitute a 10% change, which is approximately 1 standard deviation, well within the normal range of variability. The same 0.2 ms increase, however, would represent a 100% change in latency if measured over a 1 cm segment. A large per-unit increase in latency more than compensates for the inherent measurement error associated with multiple stimulation in short in- crements. The technique is particularly useful in assess- ing distal abnormalities in the carpal tunnel syndrome (4, 461. If one stimulates the median nerve in 1 cm increments across the wrist in normal hands, the la- tency changes approximately 0.16 to 0.2 1 msicm from midpalm to distal forearm. A sharply localized latency increase across a 1 cm segment indicates focal abnor- malities of the median nerve. An abrupt change in waveform usually accompanies a disproportionate la- tency difference across the site of compression [46] (Fig 6).
Using surface stimulation applied at multiple sites, one cannot determine with certainty the exact point of nerve activation. To circumvent this problem, we have developed an alternate method to study the involved nerve segment in short increments. This technique consists of stimulating the digital nerve and recording the orthodromic sensory potential at multiple points, using a series of ten electrodes mounted 1 cm apart on a specially constructed flexible strap (Fig 7A). This method is applicable not only to the median nerve at the wrist and the ulnar nerve at the elbow, as illustrated in Figure 7B, but also to any other superficially located sensory or mixed nerve. Using surface recording, how-
424 Annals of Neurology Vol 16 No 4 October 1984

A
Site of Stimulation
B
k v v 1 mr
ever, the distance between the nerve and the skin sur- face greatly influences the amplitude of the evoked potential. Thus, a small potential may simply indicate a deeper location of the nerve over the area in question. Unless one is aware of this possibility, amplitude vari- ability from one site of recording to another may lead to the erroneous conclusion that a conduction block exists.
0 C
h L l V 1 mr
-2
-1
3
4 0 I? .5 1.0
1 1.5
Fig 6. (A) Twelve sites ofstimulation in 1 cm increments along the Length ofthe median nerve. The 0 level is at the distal crease of the wrist, corresponding to the origin of the transverse carpal ligament. Sensory nerve potentials were recorded from the second digit. (From Kimura {46), with permission.) (Bi Sensory nerve potentials in a n o m l subject, recorded afer stimulation of the median nerve at multiple points across the wrist. The site of each stimulus is indicated according to the designation in A. The la- tency increased linearly with progressive shift of the stimulus site proximally from - 6 to + 5 in 1 cm increments. (From Kimura 1461, with permission.) (C) Sensory nerve potentials in a patient with carpal tunnel syndrome. The histogram on the right shows the conduction time over successive 1 cm segments. A sharply lo- calized slowing from - 2 to - I represents a segmental conduc- tion velocity of 14 mls on the left (top) and 9 mls on the right (bottom), as calculated by dividing 0.7 ms and 1.1 ms into 10 mm, respectively. Note a distinct change in wavefrm of the sensory potential at the point of localized conduction delay. The double-humped dppearance at -2 on the lejl suggests sparing of some senso y axons at this level. (From Kimura {46}, with permission.)
Ischemic Test Ischemia induced by a pneumatic tourniquet produces sensory loss and weakness in the distribution of the affected nerve. Electrophysiological studies show pro- gressive slowing in conduction velocity, decrease in amplitude, and increase in duration of the evoked ac- tion potential. In patients with capal tunnel syndrome, ischemic sensory loss occurs with abnormal rapidity
Neurological Progress: Kimura: Nerve Conduction Studies 425

Fig 7 . (A) Recording of the orthodromic median .sensoy n e w PO- tential at multiple sites in I cm increments after stimulation of the digital newe. A series of ten electrodes mounted 1 cm apart on a special(y constructedjexible strap allows simultaneous recording from nine bipolar channels. connecting two adjacent leads, GI distal to Gz. The ground electrode is placed in the palm between the stimulating and recording electrodes. (B ) Orthodromic sensory potential recorded as shown in A along the course of the median newe at the u'rist (left) and ulnar newe at the elbou, (right) in a normal subject. The 0 leuel is at the distal crease of the wri.rt for the median nenv and at the ulnar groaoe for the ulnar nerve. Each recording point is indicated by the distance in centimeters from the 0 level, assigning a minus sign distally. Each tracing consists ofhjly summated responses. For both median and ulnar nercfes. the sensoty latenry increased linearly from distal to prox- imal recording points. The amplitude of the evoked potential varied from one site to another. presumably refecting the differing distance between the newe and the skin surJace.
A
Med ian Nerve at the Wrist
- -
__ I r n s
B
426 Annals of Neurology Vol 16 No 4 October 1984
Ulnar Nerve at the Elbow
2 "V 1

over the skin supplied by the median nerve, and preex- isting sensory loss becomes much more marked [34}. Similarly, the action potential of the thenar muscles decreases more rapidly than in control subjects 1291. These findings probably indicate an increased suscepti- bility to ischemia of damaged nerve fibers at the site of the lesion. Conversely, patients with diabetes or elderly subjects [7} are abnormally resistant to ischemia, whether evaluated clinically or electrophysiologically. In a majority of diabetics, unlike normal subjects, sen- sory nerve action potential persists after 30 minutes of complete circulatory arrest in the arm. The ischemic test serves as a sensitive indicator of neural dysfunction in diabetics, a detectable change occurring even before the appearance of other electrophysiological abnor- malities [41). The exact physiological basis for this ap- parently paradoxical phenomenon remains unknown, although nerves suffering from chronic vascular insuf- ficiency may develop unusual tolerance to additional ischemia.
Fast- versus Slow-Conducting Fibers Computer analysis of the compound muscle action po- tential provides a reasonable estimate of the distribu- tion of motor conduction velocities in a nerve bundle [24}. An alternate method employs paired shocks of supramaximal intensity, with a progressive delay of the proximal stimulation after distal stimulation [40). If one delivers both stimuli simultaneously, the ortho- dromic impulse from a proximal point collides with the antidromic impulse from a distal point in all fibers, eliciting no muscle action potential attributable to the proximal stimulus. An increased interstimulus interval allows the fast-conducting impulse to escape collision and evoke a muscle response proportionate in size to the number of conducting fibers. The muscle action potential becomes maximal when the impulses no longer collide even in the slowest fibers. Thus, plotting the amplitude of the changing muscle response against the time interval, one can determine the range of nerve conduction between the fastest and slowest motor fibers.
To measure the latency of the slow-conducting fibers directly, one must block the fast-conducting fibers, leaving the activity in the slower fibers unaffected. The muscle action potential elicited by this means shows no consistent latency prolongation despite elimination of an increasing number of fast conduction impulses 1481. The discrepancy between the conduction velocity and the measured latency probably results from the differ- ing length of individual motor fibers. The motor axons terminate in various locations on motor end-plates within the muscle. Even if the difference in lengths of individual axons is only a few millimeters, the latency may vary substantially for the unmyelinated terminal segment, which conducts at a slow rate.
The use of needle electrodes allows one to sample a wide range of motor fibers with different conduction characteristics. For the reasons just discussed, however, the fastest- and slowest-conducting fibers may not al- ways be the first and last, respectively, to arrive at the motor end-plate.
Clinical Role of Nerve Conduction Studies Over the years, electrophysiological procedures have made major contributions to the understanding of pe- ripheral nerve function in healthy and disease states [30, 331. Such evaluations play an important role in delineating precisely the extent and distribution of the lesion and in providing an overall distinction between axonal and demyelinating involvement [77}. This dichotomy provides a simple and practical means of correlating conduction abnormalities with major patho- logical changes in the nerve fibers. In support of this concept, in vitro recordings from the sural nerve have clearly delineated close relationships between histolog- ical and physiological findings (1, 25, 261.
In addition to such a broad classification, the pattern of a nerve conduction abnormality can often charac- terize the general nature of the involvement. For ex- ample, hereditary demyelinating neuropathies com- monly show diffuse abnormalities, with little difference from one nerve to another in the same patient and among different members in the same family 1571. In addition, the temporal dispersion is rarely conspicuous despite considerable increases in latency, indicating approximately equal involvement of different nerve fibers. In contrast, acquired demyelination tends to af- fect certain segments of the nerve disproportionately 145, 531, giving rise to more asymmetrical abnor- malities and substantial increases in temporal disper- sion.
Optimal application of the nerve conduction study depends on an understanding of the principles and a recognition of the pitfalls of the technique. The con- ventionat methods deal primarily with distal nerve seg- ments in an extremity. Newer techniques allow one to assess nerve segments in less accessible anatomical re- gions, to improve accuracy in precise localization of a focal lesion, and to increase sensitivity in detecting sub- clinical abnormalities. Despite certain limitations, these methods can provide diagnostically pertinent informa- tion if used judiciously in appropriate clinical contexts.
The author thanks Drs Maurice W. Van Allen and Francis 0. Walker for their review and helpful suggestions, and Sheila R. Mennen, Deborah A. Gevock, and Lesa A. Bowles for technical mistance
References 1. Behse F, Buchthal F: Sensory action potentials and biopsy of the
surd nerve in neuropathy. Bran 101:473-493, 1978
Neurological Progress: G m u r a : Nerve Conduction Studies 427

2. Bolton CF, Carter K, Koval JJ: Temperature effects on conduc- tion studies of normal and abnormal nerve. Muscle Nerve
3. Braddom R1, Johnson EW: Standardization of H-reflex and diag- nostic use in S1 radiculopathy. Arch Phys Med Rehabil 55:161- 166, 1974
4. Brown WF, Yates S K Percutaneous localization of conduction abnormalities in human entrapment neuropathies. Can J Neurol Sci 9:391-400, 1982
5. Buchthal F, Rosenfalck A: Evoked action potential and conduc- tion velocity in human sensory nerves. Brain Res 3:l-122,1966
6. Campbell WW, Ward LC, Swift TR: Nerve conduction velocity varies inversely with height. Muscle Nerve 4:520-523, 1981
7. Caruso G, Labianca 0, Ferrannini E: Effect of ischemia on sen- sory potentials of normal subjects of different ages. J Neurol Neurosurg Psychiatry 36:455-466, 1973
8. Cerra D, Johnson EW: Motor nerve Conduction velocity in pre- mature infants. Arch Phys Med Rehabil 43:160-164, 1962
9. Clough JFM, Kernell D, Phillips CG: Conduction velocity in proximal and distal portions of forelimb axons in the baboon. J Physiol 198:167-178, 1968
10. Conrad B, Aschoff JC, Fischler M: Der diagnostische Wert der F-Wellen Latenz. J Neurol 210:151-159, 1975
11. Cracco RQ: The initial positive potential of the human scalp- recorded somatosensory evoked response. Electroencephalogr Clin Neurophysiol 32:623-629, 1972
12. Cruz Martinez A, Barrio M, Perrez Conde MC, Ferrer M T Electrophysiological aspects of sensory conduction velocity in healthy adults. 11. Ratio between the amplitude of sensory evoked potentials at the wrist on stimulating different fingers in both hands. J Neurol Neurosurg Psychiatry 41:1097-1101, 1978
13. Daube J R F-wave and H-reflex measurements. In Special Course No. 16, Clinical Electromyography. Chicago, American Academy of Neurology, 1979
14. Daube J R Nerve conduction studies. In Aminoff MJ (ed): Elec- trodiagnosis in Clinical Neurology. New York, Churchill Living- stone, 1980, pp 229-264
15. DeJesus PV, Hausmanowa-Petrusewicz I, Barchi RL. The effect of cold on nerve conduction of human slow and fast nerve fibers. Neurology (Minneap) 23:1182-1189, 1973
16. Denys EH: The Role of Temperature in Electromyography. Minimonograph No. 14, American Association of Electromyog- raphy and Electrodiagnosis, 1980
17. Desmedt JE: The neuromuscular disorder in myasthenia gravis. I. Electrical and mechanical responses to nerve stimulation in hand muscles. In Desmedt JE (ed): New Developments in Elec- tromyography and Clinical Neurophysiology, Vol 1. Basel, Kar- ger, 1973, pp 241-304
18. Desmedt JE, Cheron G: Central somatosensory conduction in man: neural generators and interpeak latencies of the far-field components recorded from neck and right or left scalp and ear- lobes. Electroencephalogr Clin Neurophysiol50: 382-403.1980
19. Desmedt JE, Cheron G: Somatosensory evoked potentials to finger stimulation in healthy octogenarians and in young adults: wave forms, scalp topography and transit times of parietal and frontal components. Electroencephalogr Clin Neurophysiol 50:
20. Desmedt JE, Cheron G: Prevertebral (oesophageal) recording of subcortical somatosensory evoked potentials in man: the spinal P13 component and the dual nature of the spinal generators. Electroencephalogr Clin Neurophysiol 52957-275, 1981
21. Desmedt JE, Cheron G: Spinal and far-field components of hu- man somatosensory evoked potentials to posterior tibial nerve stimulation analyzed with oesophageal derivations and non- cephalic reference recording. Electroencephalogr Clin Neuro- physiol 56:635-651, 1983
5:S145-S147, 1982
404-425, 1980
22. Desmedt JE, Huy NT, Carmeliet J: Unexpected shifts of the stationary P, somatosensory evoked potential far field with changes in shoulder position. Electroencephalogr Clin Neuro- physiol 56:628-634, 1983
23. Dorfman LJ, Bosky TM: Age-related changes in peripheral and central nerve conduction in man. Neurology (NY) 2938-44, 1979
24. Dorfman LJ, Cummins KL, Reaven GM, et al: Studies of dia- betic polyneuropathy using conduction velocity distribution (DCV) analysis. Neurology (Cleveland) 33:773-779, 1983
25. Dyck PJ, Gutrecht JA, Bastron JA, et al: Histologic and teased- fiber measurements of sural nerves in disorders af lower motor and primary sensory neurons. May0 Clin Proc 43:81-123, 1968
26. Dyck PJ, Johnson WJ, Lambert EH, OBrien PC: Segmental demyelination secondary to axonal degeneration in uremic neu- ropathy. Mayo Clin Proc 46:400-431, 1971
27. Eisen A, Odusote K. Amplitude of the F-wave: a potential means of documenting spasticity. Neurology (NY) 29:1306- 1309, 1979
28. Eisen A, Schomer D, Melmed C: An electrophysiological method for examining lumbosacral root compression. Can J Neurol Sci 4117-123, 1977
29. Fullerton PM: The effect of ischemia on nerve conduction in the carpal tunnel syndrome. J Neurol Neurosurg Psychiatry 26:
30. Gilliatt RW: Recent advances in the pathophysiology of nerve conduction. In Desmedt JE (ed): New Developments in Elec- tromyography and Clinical Neurophysiology, Vol2. Basel, Kar- ger, 1973, pp 2-18
31. Gilliatt RW: Acute compression block. In Sumner A (ed): The Physiology of Peripheral Nerve Disease. Philadelphia, Saunders,
32. Gilliatt RW: Chronic nerve compression and entrapment. In Sumner A (ed): The Physiology of Peripheral Nerve Disease. Philadelphia, Saunders, 1980, pp 3 16-339
33. Gilliatt RW: Electrophysiology of peripheral neuropathies: an overview. Muscle Nerve 5:SlOB-S116, 1982
34. Gilliatt RW, Wilson TG: Ischaemic sensory loss in patients with peripheral nerve lesions. J Neurol Neurosurg Psychiatry
35. Guiheneuc P, Bathien N: Two patterns of results in poly- neuropathies investigated with the H-reflex: correlation between proximal and distal conduction velocities. J Neurol Sci 30:83- 94, 1976
36. Gutmann L The intramuscular nerve action potential. J Neurol Neurosurg Psychiatry 32:193-196, 1969
37. Gutmann L Atypical deep peroneal neuropathy in presence of accessory deep peroneal nerve. J Neurol Neurosurg Psychiatry
38. Gutmann L: Median-ulnar nerve communications and carpal tunnel syndrome. J Neurol Neurosurg Psychiatry 40:982-986, 1977
39. Hodgkin AL, Katz B: The effect of temperature on the electrical activity of the giant axon of the squid. J Physiol (Lond) 109:240- 249, 1949
40. Hopf HC: Untersucheungen uber die Unterschiede in der Leitgerschwindigkeit motoischer nervenfasern beim Menschen. Deutsche Zeitschrift Nervenh 183:579-588, 1962
41. Horowitz SH, Ginsberg-Fellner F: Ischemia and sensory nerve conduction in diabetes mellitus. Neurology (NY) 29:695-704, 1979
42. Jewett KL, Williston JS: Auditory-evoked far fields averaged from the scalp of humans. Brain 94:681-696, 1971
43. Kimura J: F-wave velocity in the central segment of the median and ulnar nerves: a study in normal subjects and in patients with Charcot-Marie-Tooth disease. Neurology (Minneap) 24:539- 546, 1974
385-397, 1963
1980, pp 287-315
17:104-114, 1954
33~453-456, 1970
428 Annals of Neurology Vol 16 No 4 October 1984
44. Kimura J: Collision technique-physiologic block of nerve im- pulses in studies of motor nerve conduction velocity. Neurology (Minneap) 26:680-682, 1976
45. Kimura J: Proximal versus distal slowing of motor nerve conduc- tion velocity in the Guillain-Barrk syndrome. Ann Neurol 3:344-350, 1978
46. &mum J: The carpal tunnel syndrome: localization of conduc- tion abnormalities within the distal segment of the median nerve. Brain 102:619-635, 1979
47. Kimura J: Conduction abnormalities of the facial and trigeminal nerves in polyneuropathy. Muscle Nerve 5:S139-S144, 1982
48. Kimura J: Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practices. Philadelphia, Davis, 1983
49. Kimura J, Mitsudome A, Yamada T: Stationary peaks from a moving source in far-field recording. Electroencephalogr Clin Neurophysiol (in press)
SO. Kimura J, Yamada T, Shivapour E, Dickins QS: Neural path- ways of somatosensory evoked potentials: clinical implications. In Buser PA, Cobb WA, Okuma T (eds): Kyoto Symposia (EEG suppl 36). Amsterdam, Elsevier, 1982, pp 328-335
51. Kimura J, Yamada T, Steveland NP: Distal slowing of motor nerve conduction velocity in diabetic polyneuropathy. J Neurol Sci 42:291-302, 1979
52. Kimura J, Yanagisawa H, YamadaT, et al: Is the F-wave elicited in a select group of motor neurons? Muscle Nerve 7:392-399, 1984
53. King D, Ashby P: Conduction velocity in the proximal segments of a motor nerve in the Guillain-Barre syndrome. J Neurol Neurosurg Psychiatry 39:538-544, 1976
54. Kugelberg E: Facial reflexes. Brain 75:385-396, 1952 55. Lambert EH: Diagnostic value of electrical stimulation of moror
nerves. Electroencephalogr Clin Neurophysiol [Suppl) 22:9- 16, 1962
56. Lefebure DAmour M, Shahani BT, Young RR, Bird KT: The importance of studying surd nerve conduction and late re- sponses in the evaluation of alcoholic subjects. Neurology (NY)
57. Lewis RA, Sumner AJ: The electrodiagnostic distinctions be- tween chronic familial and acquired demyelinative neuropathies. Neurology (NY) 32:592-596, 1982
58. Lin JT, Phillips LH 11, Daube JR: Far field potentials recorded from peripheral nerves. Electroencephalogr Clin Neurophysiol 50:174, 1980
59. Lueders H, Lesser R, Hahn J, et al: Subcortical somatosensory evoked potentials to median nerve stimulation. B.raird06:34 1- 372, 1983
60. McLeod JG, Walsh JC: H reflex studies in patients with Parkin- son’s disease. J Neurol Neurosurg Psychiatry 3S:77-80, 1972
61. Miller RG: The cubital tunnel syndrome: diagnosis and precise localization. Ann Neurol 6:56-59, 1979
62. Miller RG, Olney RK: Persistent conduction block in compres- sion neuropathy. Muscle Nerve 5:S154-S156, 1982
63. Nakanishi T, Tamaki M, Arasaki K, Kudo N: Origins of the scalp-recorded somatosensory far field potentials in man and cat. In Buser PA, Cobb WA, Okuma T (eds): Kyoto Symposia (EEG suppl 36). Amsterdam, Elsevier, 1982, pp 336-348
64. Norris AH, Shock NW, Wagman IH: Age changes in the max- imum conduction velocity of motor fibers of human ulnar nerves. J Appl Physiol 5:589-593, 1953
29: 1600-1604, 1979
65. Olney K, Miller RG: Pseudo-conduction block in normal nerves (abstract). Muscle Nerve 6:530, 1983
66. Panayiotopoulos CP: F chronodispersion: a new electrophys- iologic method. Muscle Nerve 2:68-72, 1979
67. Panayiotopoulos CP, Scarpalezos S: F-wave studies on the deep peroneal nerve. 11. 1. Chronic renal failure. 2. Limb-girdle mus- cular dystrophy. J Neurol Sci 31:331-341, 1977
68. Seddon G: Surgical Disorders of the Peripheral Nerves. Second edition. Edinburgh, Churchill Livingstone, 197 5
69. Shahani BT: The human blink reflex. J Neurol Neurosurg Psy- chiatry 33:792-800, 1970
70. Shahani BT, Potts F, Domingue J: F response studies in periph- eral neuropathies. Neurology (NY) 30:409-4 10, 1980
71. Shahani BT, Potts F, Juguilon A, Young RR: Maximal-minimal motor nerve conduction and F response studies in normal sub- jects and patients with ulnar compression neuropathies. Muscle Nerve 3:182, 1980
72. Sicca REP, McComas AJ, Upton ARM: Impaired potentiation of H-reflexes in patients with upper motoneuron lesions. J Neurol Neurosurg Psychiatry 34712-717, 1971
73. Simpson JA: Fact and fallacy in measurement of conduction velocity in motor nerves. J Neurol Neurosurg Psychiatry
74. Sohmer H, Feinmesser M: Cochlear and cortical audiometry conveniently recorded in the same subject. Isr J Med Sci 6:219- 223, 1970
75. Sunderland S: Nerves and Nerve Injuries. Second edition. Edin- burgh, Churchill Livingstone, 1978
76. Thomas JE, Lambert EH: Ulnar nerve conduction velocity and H-reflex in infants and children. J Appl Physiol 15:l-9, 1960
77. Thomas P K The morphological basis for alterations in nerve conduction in peripheral neuropathy. Proc R SOC Med 64:295- 298, 1971
78. Thomas PK, Sears TA, Gilliatt RW: The range of conduction velocity in normal motor nerve fibers to the small muscles of the hand and foot. J Neurol Neurosurg Psychiatry 22:175-181, 1959
79. Vecchierini-Blineau MF, Guiheneuc P Electrophysiological study of the peripheral nervous system in children: changes in proximal and distal conduction velocities from birth to age 5 years. J Neurol Neurosurg Psychiatry 42:753-759, 1979
80. Wager EW Jr, Buerger AA: A linear relationship between H- reflex latency and sensory conduction velocity in diabetic neu- ropathy. Neurology (Minneap) 24:7 11-7 14, 1974
81. Wiechers D, Fatehi M: Change in the evoked potential area of normal median nerves with computer techniques (abstract). Muscle Nerve 6:532, 1983
82. Wiederholt WC: Threshold and conduction velocity in isolated mixed mammalian nerves. Neurology (Minneap) 20:347-352, 1970
83. Yamada T, Kimura J, Nitz DM: Short latency somatosensory evoked potentials following median nerve stimulation in man. Electroencephalogr Clin Neurophysiol48:367-376, 1980
84. Yamada T, Machida M, Kimura J: Far-field somatosensory evoked potentials after stimulation of the tibial nerve in man. Neurology (NY) 32:1151-1158, 1982
85. Young RR, Shahani BT: Clinical value and limitations of F-wave determination (letter to the editor). Muscle Nerve 1:248-249, 1976
27:381-385, 1964
Neurological Progress: Kimura: Nerve Conduction Studies 429