neuropsych pd oct 11 2013 shorter (2)-2 - wordpress.com … · • early&motor&stage&...
TRANSCRIPT

01/10/2014
1
Neuropsychiatric Aspects of Parkinson’s Disease: Across the stages
Iracema Leroi MD FRCPC MRCPsych University of Manchester Manchester Mental Health and Social Care Trust
Non-‐motor PD Features
• Pain • Parathesias • RLS • FaLgue • Skin symptoms
• seborrhoea, facial oiliness • Dysautonomia
• bladder instability, altered thermal regulaLon, O. H.

01/10/2014
2
Neuropsychiatric non-‐motor PD Features
� Psychiatric Symptoms › depression › anxiety › sleep disturbance › psychosis
� Cogni2ve Symptoms › execuLve dysfuncLon › subcorLcal demenLa › corLcal demenLa
The Stages of Symptoms in PD • Pre-‐motor stage • (Prodromal stage) • Early motor stage • Moderate motor stage • Advanced stage

01/10/2014
3
Non-‐motor symptoms correspond to the orderly progression of LB pathology (Braak stages)
• olfactory bulb • Dorsal motor nucleus of the vagus nerve (DMNX)
• Rostral along brain stem • Locus coeruleus • Dorsal raphe nucleus
• Midbrain substanLa nigra
The motor and cogniLve stages of PD PRE-‐MOTOR EARLY-‐MOD ADVANCED
PD-‐mild cogniLve impairment
DemenLa in PD
PD normal cogniLon

01/10/2014
4
Most commonly reported neuropsychiatric symptoms
(Leroi 2012) (in over 20% of each group, excluding sleep & appeLte)
PD Normal cogni2on
PD Mild cogni2ve impairment
PD demen2a (PDD)
In order of frequency
Anxiety Depression Irritability
Apathy Anxiety Depression
Depression Apathy Irritability Anxiety Aggress/agitat HallucinaLons Delusions Aberrant motor
Impulse control disorders
Neuropsychiatric symptoms in different cogniLve stages in PD
(Leroi 2012)
0
10
20
30
40
50
60
70
80
90
100
NPI any symptom NPI total score ≥4
PD NC
PD MCI
PDD
*
*

01/10/2014
5
Neuropsychiatric Inventory • Cumming et al., 1997 • 10 or 12-‐item scale to measure psychiatric complicaLons • Informant-‐reported • Gold standard in demenLa • Each domain rated as: YES/NO (presence/absence) • If YES, severity assessed: by Frequency (F) x Severity (S) • FxS = total score per item (min 0; max 12; clinically significant ≥4)
• Can rate all 10 (or 12) domains OR use a single domain alone e.g apathy
Neuropsychiatric Inventory • Domains: • Delusions • HallucinaLons • Depression/dysphoria • Irritability • AgitaLon/aggression • Euphoria/elaLon • Apathy • Anxiety • DisinhibiLon • Aberrant motor behaviour • Sleep • AppeLte

01/10/2014
6
Early motor stage of PD
Early PD stage: Psychiatric symptoms
• Depression • Anxiety more prevalent and severe
• Psychological reacLon to the diagnosis • Sleep
• insomnia (immobility-‐related) • MedicaLon side effects (GI, sleep)

01/10/2014
7
Early motor stage depression • Very common • Also may be prodrome (1 to 2 years) • May be relieved by iniLaLon of PD medicaLons
• Depression is not related to motor symptoms Sustained
• May be unrelated to disease stage • Not related to medicaLon status (unless undertreated)
Tips to diagnosis of depression in PD • 1. Consider collateral sources
• 2. Work-‐up for reversible causes • FBC, TSH, testosterone levels, B12, folate • DemenLa, delirium, medical illness
• 3. Diagnos2c criteria • 4. Screening Tools

01/10/2014
8
DiagnosLc Criteria for Major Depression: DSM-‐IV
• Depressed mood or anhedonia ≥ 2 weeks
• 5/9 symptoms: • Depressed mood/loss of pleasure or interest
• Worthlessness or guilt, poor concentraLon
• Suicidal ideaLon
• Insomnia/hypersomnia • Psychomotor retardaLon or agitaLon
• FaLgue or loss of energy • ↓ or ↑ appeLte
NINDS/NIMH recommendaLons for dx of PD-‐related depression
• Use inclusive diagnos2c criteria • suggest modified DSM-‐IV criteria • More sensiLve than “eLologic/exclusive/subsLtuLonal” approach

01/10/2014
9
Depression RaLng Scales in PD: MDS Task Force RecommendaLons
(Schrag et al, 2007)
• Literature review of depression scales • Expert consensus • Screening:
• Hamilton depression Scale • Beck Depression Inventory • Hospital Anxiety & Depression RaLng Scale • Montgomery-‐Asberger Depression RaLng Scale • Geriatric Depression Scale
• Severity: • HAM-‐D, Beck, Zung • Cornell scale (CSDD) needs validaLng in PD
Depression and motor symptoms in PD: later stages
• Motor-‐related dysphoria:
• Off-‐period depression and anxiety • Associated with paqern of on/off syndrome • Other non-‐motor symptoms present (urinary problems, confusion, pain, panic)
• Improves with beqer motor control

01/10/2014
10
DifferenLal diagnosis of depressive symptoms in PD
Non-‐depression: • Drug-‐induced mood changes
• Drug withdrawal *DAWS... • Pathological tearfulness • DemenLa • Apathy/anhedonia • Delirium • “Pseudoanhedonia” (lack of emoLonal expression)
Pharmacologic Treatment of Depression in PD
• Inadequate evidence: inadequately controlled & under-‐powered trials
• Elderly populaLon • Dosing as per “start low, go slow” rule • Drug-‐drug interacLons with selegilin, (rasagiline)
• Pramipexole (D2,D3) may have promise

01/10/2014
11
Pharmacological Treatment of Depression in PD: Reviews
Author # Studies Years Type Conclusion
Klaassen et al, 1995
4/12 1966-‐1993 Meta-‐analysis Insufficient evidence
Movement D/O (supp 4), 2002
5/19 ? Review Insufficient evidence
Cochrance 2003
3 RCT (SSRI) 1800s-‐2001 Review Insufficient evidence
Weintraub et al, 2005
27 N=772(668 completers) >80% on SSRI
1965-‐2003 Meta-‐analysis & effect size
Large effect size in acLve & plc groups; larger in non-‐PD depressed
Classes of AnLdepressants for use in PD
SNRI – Venlafaxine, DuloxeLne NDRI – Bupropion SSRI – fluoxeLne, paroxeLne, fluvoxamine,
citalopram, escitalopram SARI – trazodone, nefazodone NASA -‐ mirtazepine

01/10/2014
12
Dopamine Agonists as anLdepressants in PD?
• RCT of pramipexole for depression in PD (Barone 2010)
• n= 296 paLents • Significant improvement :
• Beck Depression Inventory • Geriatric Depression Scale • UPDRS motor scale • UPDRS ADL
Summary of Opinion of Drug Treatment of depression in PD (McDonald 2010)
• None of the anLdepressants have a clear advantage in terms of efficacy, but the SSRIs are more easily tolerated
• Older paLents may take longer to respond and need at least a 12 week trial at adequate dose to assess response
• Older paLents ozen need opLmal doses to respond fully
• Treat unLl remission is reached or relapse risk is high

01/10/2014
13
Moderate motor stage of PD
Psychiatric symptoms in the moderate stage of PD
• Mild cogniLve impairment (PD-‐MCI) • Apathy • Impulse control disorders

01/10/2014
14
Moderate stage: PD-‐Mild CogniLve Impairment
(PD-‐MCI)
MCI-‐PD Movement Disorder Task Force Criteria
(Litvan 2012)
• Newly defined enLty • Mean prevalence 27%

01/10/2014
15
Associated features of PD-‐MCI (Jellinger 2011)
• older age at disease onset • male gender • depression • severity of motor symptoms • advancing disease stage
Movement Disorder Society Consensus Criteria for PD-‐MCI
(Litvan 2012)
• Based on 3 types of criteria • Clinical: diagnosed with PD • Cogni2ve: deficits in neuropsychological tesLng
• Deficits in 2 tests within the same domain OR • Deficits in 2 tests, each in a different cogniLve domain • 5 key domains:
• aqenLon and working memory • execuLve dysfuncLon, • language • memory • visuospaLal funcLon
• Func2onal: no significant impact on funcLonal ability

01/10/2014
16
CogniLve profile of MCI-‐PD (Aarsland 2011)
• Range of cogniLve domains affected
• 11% non-‐amnesLc, single-‐domain impairment • 9% amnesLc single-‐domain • 5% amnesLc mulLple domain • 1.3% non-‐amnesLc mulLple domain
Is MCI-‐PD a prodrome to PDD? CONTINUUM
cogniLve change
MCI-‐PD
PDD
Cogni2ve SUBTYPES (CamPaIGN study)
• “demenLa safe” type: ¡ Frontal execuLve types
changes
vs
• “demenLa prone“ type:
¡ “Posterior corLcal” deficits ¡ visuospaLal and verbal
fluency

01/10/2014
17
Management of MCI-‐PD • No full scale trials yet • Cholinesterase inhibitors vs placebo in MCI without PD have not favoured acLve drugs
• But, consider cholinesterase inhibitors if psychosis or fluctuaLng cogniLon is present
Management of MCI-‐PD • Ensure that dopaminergic therapy has been opLmised
• Trial of atomoxeLne in PD cogniLon (Johns Hopkins study)
• Consider Memory Management Groups • OccupaLonal Therapy input

01/10/2014
18
Management of MCI-‐PD: CogniLve Training
• Few studies; mostly focused on specific funcLons • Hullman (2006): trained execuLve funcLons using working memory and execuLve tasks: daily 30 minute sessions for 7-‐8 days, finding improvements in some execuLve cogniLve domains
• Sinforiani (2004): computerized cogniLve training tasks targeLng aqenLon, visuospaLal ability and abstract reasoning
• Results are promising but outcomes and training types are diverse • ?generalisability • ?impact on funcLonal ability • ?impact on behavioural syndromes such as apathy
Moderate stage: Apathy

01/10/2014
19
Apathy RaLngs:
PD normal cogniLon vs PD MCI (Leroi 2012)
Neuropsychiatric Inventory: Apathy subscale
0 50 100 150 200 250 300 350 400
Informant rated apathy
PD NC
PD MCI
PDD
*
Apathy Scale (Starkstein)
0
5
10
15
20
Self-‐rated apathy
PD NC
PD MCI
*
ANCOVA with age and motor severity as covariates: differences remained significant *
Apathy has 3 key dimensions

01/10/2014
20
Diagnosis of apathy may be difficult • Overlap with :
• Motor symptoms: • bradykinesia, “off” states, masked facies
• Depression: • low mood, anhedonia, low energy
• CogniLve impairment: • bradyphrenia
• Excessive dayLme sleepiness • FaLgue
MDS Task Force on Apathy RaLng Scales (Leentjens et al, 2008)
• Apathy EvaluaLon Scale (AES) • Apathy Scale (AS) • Apathy Inventory (AI), • Lille Apathy RaLng Scale (LARS) • UPDRS part I, item 4 (moLvaLon/iniLaLve) • Neuropsychiatric Inventory (NPI), Domain 7 (apathy)
• Only the AS (Starkstein) is classified as ‘Recommended’ to assess apathy in PD

01/10/2014
21
Management of apathy in PD • No good evidence base
• Case series: modafinil, bupropion, amphetamine-‐like sLmulants
• Associated with lower dopaminergic load (especially dopamine agonists)
• Treat co-‐morbid depression • Consider external sLmulaLon/structure • Support for caregivers • EducaLon
Moderate stage: Impulse control disorder
(ICDs)

01/10/2014
22
DefiniLon of Impulse Control Disorders (ICDs)
• A spectrum of psychiatric disorders involving pleasurable or hedonic behaviours
• Person fails to resist the drive to behave in ways that result in distress or impaired social and occupaLonal funcLoning
• Behaviours are repeLLvely, compulsive
• AddicLve paqern… “behavioural addicLon”
Spectrum of ICDs in PD • “GSES” • pathological gambling • compulsive sexuality • binge eaLng • compulsive shopping
• Affects 8-‐15% of PD (Weintraub 2010)
• 6% of PD not on DA • 17% on DA

01/10/2014
23
Dopamine DysregulaLon Syndrome (DDS)
(Evans 2004; Giovannoni 2000)
• ?extreme end of ICD in PD • “hedonisLc homeostaLc dysregulaLon” • “dopamine drug addicLon” • “compulsive dopaminergic drug use”

01/10/2014
24
Punding
• RepeLLve, purposeless motor behaviours • Coined in amphetamine users • Analogous to stereotypic behaviour of rodents treated with chronic psychosLmulants
• Most ozen associated with levodopa addicLon and apomorphine use
• ExaggeraLon of premorbid interests, hobbies or emerge as new skill (poeLc talent, painLng)
• Examples: repairing things, gardening, playing an instrument, excessive computer use, cleaning, model building
ICDs and dopamine therapy • Iatrogenic complicaLon associated with dopaminergic replacement therapy in PD
• Total dopaminergic load (LEDD) • Dopamine agonists (2-‐3x greater risk) • Levodopa
• Also reported with amantadine, selegiline

01/10/2014
25
Pathophysiology (Voon 2007; Delaney, Leroi 2012)
suscepLbility
dopaminergic medicaLons “suscepLbility mulLplier”
ICDs
Role of suscepLbility: Risk factors to develop ICDs
(Voon 2011; Weintraub 2010; Leroi 2011)
• Younger age • Younger age at PD onset
• Male sex • Not married • Self-‐reported family history of gambling
• ?novelty seeking personality profile
• Psychosocial factors

01/10/2014
26
“Ventral (limbic) Overdose Hypothesis” (Cools 2001)
• Ventral striatum: intact projecLons in younger PD, get “over-‐dose” of dopamine when treated with DRT → ICD, impaired reversal learning…
• Dorsal striatum: damaged projecLons in PD, so normalises funcLon with DRT → improved execuLve, working memory, motor funcLon…
QuesLonnaire for Impulsive-‐Compulsive Disorders in Parkinson’s Disease (QUIP)
(Weintraub et al. 2008).
• brief, self-‐administered screening quesLonnaire • Sec2on 1: compulsive gambling, buying, sexual behaviour, and eaLng;
• Sec2on 2: other compulsive behaviours (hobbyism, punding and walkabout);
• Sec2on 3: compulsive medicaLon use (DDS)

01/10/2014
27
Management of ICDs in PD • PrevenLon • IntervenLon: 2 key nodes 1. dopamine replacement therapy 2. psychological distress 3. other psychotropic medicaLon
PrevenLon of ICDs in PD • EducaLon • Informing ALL paLents for whom dopamine agonists are prescribed about ICD risk – BNF lists PG, HS and binge eaLng as AE of DA
• Informing family/carers (with paLent permission) – Consider se�ng up contract between paLent and carers about disclosure of change in behaviours

01/10/2014
28
PrevenLon of ICDs in PD • IdenLfy suscepLble paLents for closer monitoring and follow-‐up – Early severe dyskinesias (12-‐24 into treatment) – Young, male, family history addicLons, alcohol dependence
• Prompt and direct screening: consider using a screening tool
IntervenLon node 1: Dopamine replacement therapy
• Dose educaLon/stepwise disconLnuaLon of DA or most recent DRT (Gallagher 2007; Driver-‐Dunckley 2003; Dodd 2005)
• Limited long-‐term outcome data – ICD have sustained improvement post DA reducLon (Mamikonyan 2008)
• Pharmacist intervenLon: blister packs, limited supply of medicaLon, restricted dosing on a daily basis

01/10/2014
29
IntervenLon node 1: Dopamine replacement therapy
• Switch to a different class of DA …may cause ICD relapse
• Longer acLng DRT formulaLons • Duodopa • Deep brain sLmulaLon (Ardouin 2006)
*CauLon: Dopamine agonist withdrawal syndrome (“DAWS”)
IntervenLon node 2: Psychological distress
• Educa2on for pa2ent and family – Developing awareness
• Suppor2ve psychotherapy – Help line contact – Contact with other sufferers (user-‐carer groups)
– Frequent contact and monitoring with PD team
• Cogni2ve behaviour therapy

01/10/2014
30
IntervenLon node 2: Psychological distress
• Addic2on support groups • remission only on DA reducLon + Gambler’s anonymous (Kurlan 2004)
• n=15 long-‐term f/up • n=4 only achieved parLal remission with GA aqendance as well (Mamikonyan 2008)
IntervenLon node 2: Psychological distress
• Iden2fy and treat psychiatric comorbidi2es • Depression • Anxiety
• Watch out for trigger a manic-‐like episode with anLdepressants

01/10/2014
31
IntervenLon node 3: AlternaLve pharmacological therapies
• CauLon: publicaLon bias for treatments • Atypical anLpsychoLcs…olanzapine & queLapine for hypersexuality
• SSRI: paroxeLne in non-‐PD PG (Kim 2002)
• Fluvoxamine in non-‐PD PG (Hollander 2000) • Naltrexone (opioid antagonist) in non-‐PD PG (Grant 2008);
• Amantadine: RCT: n=17 PD with PG suggested improvement with this (Thomas 2010)
• Zonisamide: Open non-‐randomised trial (Bermejo 2010)
Advanced stage PD

01/10/2014
32
Advanced stage PD • Motor symptoms more severe • Falls more common • “on-‐off” complicaLons and fluctuaLons/freezing • Tremor may be less obvious • Marked bradykinesia • Gait assisted • Less responsive to dopamine replacement therapy
Emergence of significant neuropsychiatric
symptoms with demenLa in PD (Neuropsychiatric Inventory)
(frequency & severity)
0 10 20 30 40 50 60 70 80 90 100
PD NC
PD MCI
PDD
*
0
20
40
60
80
100
120
Disin
hibiLo
n
Irrita
bility
ElaL
on
Aberrant m
otor
PD NC
PD MCI
PDD
*
ANCOVA with age and motor severity as covariates: differences remained significant

01/10/2014
33
Advanced stage PD: Psychosis
• #1 factor in nursing home placement • Major source of caregiver burden • Associated with increased mortality
Psychosis in PD

01/10/2014
34
Psychosis in PD (Fenelon et al, 2000)
Passage hallucina2ons: -‐seeing something passing-‐by oneself for a fleeLng moment
Presence hallucina2ons: -‐ the feeling that someone is present in the room
Illusions: -‐mistaking an object for an animal or person
Complex hallucina2ons: -‐seeing, hearing, feeling or smelling something that is not really there
Examples of passage illusions (slide compliements of D. Whitehead)
A: ‘I kept seeing these ants on the carpet ... crawling about...When I was reading in the evening they were there, but I couldn’t find them..... I put down powder, but they were sTll there of course!’
Pt B: ‘In the mornings I feel as though there’s two of us. I can’t phrase it very well ... as though we’re side by side, going up the stairs... Very peculiar it is !’

01/10/2014
35
Delusions in PD
• Delusions of spousal infidelity (Othello syndrome)
• Ozen accompany hallucinaLons • Other persecutory delusions
Management of psychosis in PD • Rule out reversible factors or triggering events • Decrease PD meds and remove key culprits • Levodopa is removed last • If cogniLve impairment is present, consider starLng with a cholinesterase inhibitor (e.g. rivasLgmine)

01/10/2014
36
AnLpsychoLcs for psychosis in PD
• Add an anLpsychoLc if symptoms only if: • symptoms cause distress • Safety concerns (e.g. aggressive to carer) • Intolerable motor worsening on reducLon of dopamine replacement
• Avoid typical anLpsychoLcs (e.g. haloperidol) • Atypical anLpsychoLcs are preferred but:
• Avoid risperidone ...limited by motor effects • Avoid olanzapine...limited by motor effects and limited efficacy ...avoid in PD
• Consider queLapine: may have a role but cauLon with side effects
Clozapine for psychosis in PD • atypical anLpsychoLc with liqle effect on motor symptoms
• Specific license for psychosis in PD • Use only for significant psychosis in which other intervenLons have not been effecLve
• 6.25mg start • Key problem: agranulocytosis – weekly monitoring of WBC for fist 6 months; can get sudden or gradual drop in WBC
• Sialorrhea and delirium • GI disturbances • Seizures in 4% (dose related)

01/10/2014
37
When to avoid anLpsychoLcs: Too good or too bad…
• Clear sensorium with good insight
• Symptoms do not cause distress
• CauLon if: • established demenLa
• Increased risk of CVA in demenLa
• Increased mortality • Increased cogniLve impairment
• advanced motor symptoms • EPSE
• Significant non-‐motor symptoms • HypersalivaLon • Falls/dizziness • Weight loss • consLpaLon
Advanced stage: DemenLa in PD (PDD)

01/10/2014
38
“The Sydney MulLcentre Study” (Hely 2008)
Longitudinal observaLonal study • N=136 PD parLcipants • Followed at 10, 15, and 20 years • At 20 years, 100 died • -‐*PDD in 83% of 20-‐year survivors
“The Sydney MulLcentre Study” (Hely 2008)
• Age at PDD diagnosis 71.6 years • Time to onset azer dx 10.9 years • Azer PDD diagnosis, survival 54 months

01/10/2014
39
Impact of demenLa in PD (Leroi and Pantula 2011)
0
5
10
15
20
25
30
35
40
QOL Carer burden
PD
MCI-‐PD
PDD
* *
Risk Factors for Conversion to PDD • Demographic:
• older age, male gender • CogniLve:
• visual spaLal & verbal fluency deficits (Williams-‐Gray 2007)
• Psychiatric: • early psychosis, apathy, depression
• Motor: • akineLc rigid PD; loss of tremor (Aarsland 2003; Levy 2000)
• Autonomic symptoms: • orthostaLc hypotension
• Weight loss (Uc 2006)

01/10/2014
40
Neuropsychology of AD vs PDD (Bronnick 2007)
AD PDD
Memory encoding recall
Orientation poor fair
Language poor fair
Attention fair poor
ECF fair poor
Visuoperceptual function
fair poor
Can predict AD vs PDD on cognitive profile alone with 74.7% accuracy
DetecLng demenLa in PD
• Have a high index of suspicion • Risk factors:
• Older age, early psychosis, poor verbal fluency • Concomitant clinical presentaLon:
• EDS, apathy, falls, levo-‐dopa non-‐responsiveness, lack of tremor
Noe et al (2003); Galvin (2003); Emre (2003); Aarsland (2003)

01/10/2014
41
How do we detect PDD? Get collateral from carers
• Don’t trust “sharp as a tack” • Ask if they’d leave their loved one alone overnight and WHY they wouldn’t
• WHY have they taken over the finances etc…
OperaLonalized MDS Criteria for PDD: Simple 5 step algorithm
(Dubois et al, 2007)
• 1. diagnosis of iPD • 2. PD prior to demenLa • 3. PD with ↓ global
cogniLve efficiency
• 4. CogniLve ↓ impairs ADL
• 5. Impairment of >1 cogniLve domain
• Queen’s Square • History/records
• MMSE < 26
• Carer interview/pill quesLonnaire
• Domains: aqenLon, ECF, visuospaLal, memory

01/10/2014
42
Measuring funcLonal impact of cogniLve impairment
(Kulisevsky Park Rel Dis 19 (2013)
Parkinson’s Disease Cogni2ve Func2onal Ra2ng Scale
• FuncLonal impairment not due to motor symptoms
• 5 minute, 12-‐item quesLonnaire (max 24)
• those without demenLa • Rate if trouble performing acLvity:
• 0 = none; • 1= some of the Lme; • 2 = most of the Lme; • 8= never done
Items to rate
• handling money • domesLc economy • Arranging holidays or meeLng • handling personal mail • drug treatment schedule • organizing daily acLviLes • handling electrical appliances • understanding how to use public transport
• solving unforeseen events • explaining things to say • understanding reading • handling cell phone
Pill QuesLonnaire (Dubois, oral communicaTon, Chicago 2008)
• Ability of a paLent to verbally describe his/her anL-‐parkinsonian treatment with the Lme schedule, the nature and dose
• Correlates with impaired ADL

01/10/2014
43
MUSTARDD sub-‐study Comparing cogniLve baqeries in PD
(PI: David Burn; MJFF)
SCOPA-Cog 10 items; max score 43 Practical Test-retest reliability .78
20 min Validated in PD
MMSE >94% sensitive; 77% specific; better for “cortical” total score not helpful
7 min AAN (Level B)
ACE-R no evidence in PD; good frontostriatal testing
30 min *extract MMSE
Mattis DRS Used in RCT of PDD (Leroi 2004)*MMSE
40 min Cut-off <123/144
Clock Good screen but low specificity; 5 min DLB can’t copy!
MOCA Increasingly used in PD 10-15 min Similar items as ACER; validated in PD
The consequences of demenLa… “Disability Model” (WHO 1998)
Impairment
Disability
Handicap

01/10/2014
44
The consequences of demenLa…
Impairment
Due to underlying pathophysiological changes… extent of cogniLve impairment (memory, language…)
Disability
Handicap
• Rule out reversible causes of demenLa (TSH, B12, Folate etc)
• Aim for levodopa monotherapy • Stepwise removal of “deliriogenic”, hallucinogenic medicaLons – Graded, gradual withdrawal – AnLcholinergics > selegiline > amantadine > dopamine agonists > COMT inhibitors
Compliments of Prof David Burn
What to do before starLng cholinesterase
inhibitor therapy

01/10/2014
45
When Do We Start Drug Therapy?
• No guidance is available • New NICE guidance for AD suggests “moderate stage” (MMSE 10-‐22) – This does not apply for PD
• Start once diagnosis of demenLa is made • CauLon with “MCI”
– No data for “MCI-‐PD” – Data in AD suggest lack of efficacy/? increased mortality
CogniLve enhancers in PDD Donepezil (Aricept)
5mg daily → 10mg daily
Leroi 2004 (RCT); Ravina 2005 (RCT); EDON Trial
*Rivastigmine (Exelon)
1.5 mg daily/BD → 6mg BD; Patch once daily
Emre 2004 (RCT)*
Galantamine XL (Reminyl)
8mg daily → 24 mg daily
Aarsland 2004
Memantine (Ebixa)
5mg daily → 10mg BD
Leroi 2010 Aarsland 2011 Emre 2011

01/10/2014
46
RivasLgmine: EXPRESS Study Design • Double-‐blind, randomized, placebo-‐control • 541 PDD • Randomized 2:1, rivasLgmine 3–12 mg/day : placebo • Treatment duraLon 24 weeks • Primary efficacy measures:
– ADAS-‐cog – ADCS-‐CGIC
• Secondary efficacy measures: – ADCS-‐ADL – NPI – CDR a_en2on ba_ery – MMSE – D-‐KEFS Verbal Fluency test – Ten-‐point clock-‐drawing test
Emre et al. New Engl J Med 2004;351:2509–18
RivasLgmine: EXPRESS Study Design • Double-‐blind, randomized, placebo-‐control • 541 PDD • Randomized 2:1, rivasLgmine 3–12 mg/day : placebo • Treatment duraLon 24 weeks • Primary efficacy measures:
– ADAS-‐cog – ADCS-‐CGIC
• Secondary efficacy measures: – ADCS-‐ADL – NPI – CDR a_en2on ba_ery – MMSE – D-‐KEFS Verbal Fluency test – Ten-‐point clock-‐drawing test
Emre et al. New Engl J Med 2004;351:2509–18

01/10/2014
47
RivasLgmine versus Placebo Changes from Baseline on the ADAS-‐cog
*p = 0.002; **p < 0.001, ITT-RDO analysis
–2.5
–2.0
–1.5
–1.0
–0.5
0
0.5
1.0 0 16 24
Cha
nge
from
bas
elin
e, A
DA
S-c
og
Week:
Rivastigmine (n = 329) Placebo (n = 161)
Improvement
Deterioration
Baseline
** *
Emre et al. New Engl J Med 2004;351:2509–18
Side Effects of All Cholinesterase Inhibitors in PDD
Concern in PDD
*GI (nausea, vomiting, diarrhea)
Anti-PD drug side effects
Anorexia Weight loss; mechanical difficulties eating
Insomnia Sleep fragmentation; insomnia; nocturia; EDS
Nightmares Prodrome to hallucinations; REM problems
Hypersalivation Common in PD

01/10/2014
48
Side Effects of Cholinesterase Inhibitors in PDD
Concern in PDD
↓ motor function/tremor* ? Ach ↑ DA↓
Leg cramps wearing off; dystonia
Orthostatic hypotension/falls gait ↓; ANS failure; impaired righting reflex
Agitation YES
Paradoxial psychosis PD-related psychosis
Pilot RCT of MemanLne in PDD (I. Leroi, R. Oversho\, J. Byrne, A. Burns, 2008)
• Objec2ve: To evaluate the safety and efficacy of memanLne, an uncompeLLve NMDA-‐antagonist vs placebo in PDD
• Methods: • 22-‐week RCTdemenLa in PD (DSM-‐IV criteria) • Primary outcome: Ma�s DRS • Secondary: NPI, Burden Scale, QOL, CIBIC+ , MMSE • Results: • MemanLne was well tolerated at 20mg/day • Almost all completed the trial • Conclusions: • MemanLne has a role in PDD treatment • This study supports the need for a large scale randomized controlled trial of memanLne in PDD.

01/10/2014
49
RCT of MemenLne in PDD (Leroi et al, 2008)
Figure 2: CIBIC-Plus Mean Score by Visit
2.5
3
3.5
4
4.5
5
5.50 14 22
Treatment Week
CIBI
C Sc
ore
PlaceboMemantine
*
The consequences of demenLa…
Impairment
Disability
RestricLon in funcLon • May vary greatly according to personal, social, environmental factors
• May not be a reflecLon of the level of impairment
Handicap

01/10/2014
50
IntervenLons in early stage demenLa
• Impairment medica2on
• Disability cogni2on-‐based interven2ons
• Handicap avoid insLtuLonalisaLon and remain in society by
maintaining independence → technology-‐based interven2ons
or
Reducing disability and
handicap….Improving funcLon • Different types of cogni2ve interven2ons have
been used for over a decade • LimitaLons to studies (Orrell and Woods, 1996):
• Mostly un-‐standardised • Small size (underpowered) • Variable quality • Non-‐generalisable outcomes • Problems with control group

01/10/2014
51
CogniLon-‐based intervenLons for older adults
• Cogni2ve s2mula2on (CS): • Repeated pracLsing of a cogniLve task improves the ability to do that task
• Cogni2ve (brain) training (CT): • Learning new methods to enhance informaLon coding or retrieval of previously learnt material
• Cogni2ve rehabilita2on (CR): • Uses strategies (memory aids, daily rouLnes to support memory etc) to compensate for cogniLve impairment
Manchester pilot study CogniLve Training in PD
(Ellen Poliakoff)
• Computerised cogniLve training baqery (daily x 2 weeks)
• SimulaLng real life scenarios • TargeLng several different cogniLve domains • Range of outcomes (cogniLve, funcLonal, behaviour)

01/10/2014
52
Treatment of PDD: Non Pharmacological intervenLons
• Principles of basic demenLa care • EducaLon/financial planning (wills, POA) • Driving • Caregiver support, support groups, respite
• Memory cueing techniques (OT) • Safety and ease in the home se�ng (OT) • Monitoring medical condiLon • Improving sensory deprivaLon
Refer to a Psychiatrist If:
• Suicidal • PaLent/family request it • ParLal remission/chronic • Major depression with psychosis • If psychosis without insight • If MMSE<27

01/10/2014
53
A final thought…
“psychiatric symptoms should not be viewed as a secondary or addiLonal feature of a movement disorder, but rather represent important and inherent aspects of the disorder, and may even represent key features of the clinical syndrome”
(Aarsland, Ehrt, Uwe in Current Opinion in Psych, 2003)
Thank you

01/10/2014
54
SCOPA-‐Cog: Scales for Outcome of PD-‐cogniLon
(Marinus et al, 2003)
• Short, pracLcal validated instrument • SensiLve to specific cogniLve deficits in PD • 10 items; max score of 43 (higher is beqer) • Test-‐re-‐test reliability .78 • Correlates well with CAMCOG and MMSE
PD-‐CogniLve RaLng Scale (PD-‐CRS)
(Pagonabarraga 2008) • Can disLnguish PD, MCI-‐PD and PDD • newly validated • Global cogniLon & sub-‐domains of cogniLon • 94% sensiLvity to detect PDD • Can differenLate MCI-‐PD from cogniLvely intact PD with verbal fluency & delayed verbal memory test
• 10 sub-‐corLcal-‐type assessments • aqenLon, working memory, exec, verbal fluency, memory etc)
• 2 corLcal-‐type (clock drawing, naming).
01/10/2014
55
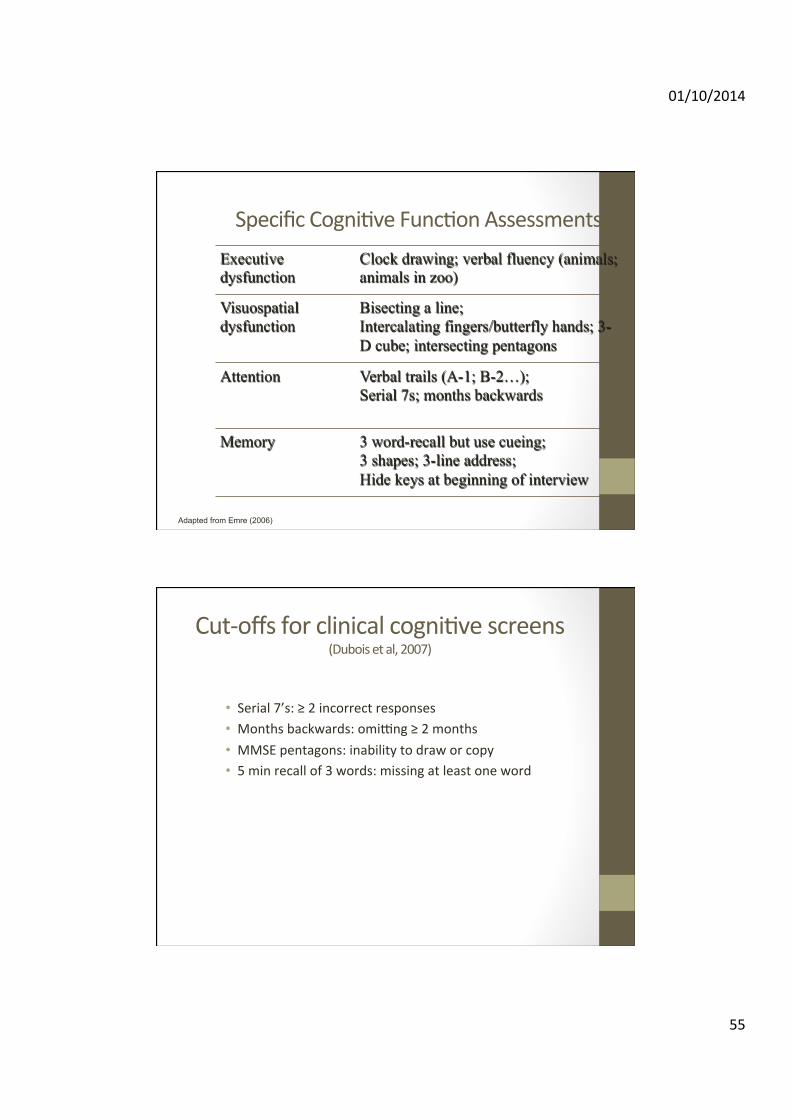
Specific CogniLve FuncLon Assessments Executive dysfunction
Clock drawing; verbal fluency (animals; animals in zoo)
Visuospatial dysfunction
Bisecting a line; Intercalating fingers/butterfly hands; 3-D cube; intersecting pentagons
Attention Verbal trails (A-1; B-2…); Serial 7s; months backwards
Memory 3 word-recall but use cueing; 3 shapes; 3-line address; Hide keys at beginning of interview
Adapted from Emre (2006)
Cut-‐offs for clinical cogniLve screens (Dubois et al, 2007)
• Serial 7’s: ≥ 2 incorrect responses • Months backwards: omi�ng ≥ 2 months • MMSE pentagons: inability to draw or copy • 5 min recall of 3 words: missing at least one word

01/10/2014
56
Clock Drawing Task
• Ask to place hands at 10 past 11 • Score 0-‐4 • Closed circle: 1 point • All 12 numbers correct: 1 point • Long hand correctly placed: 1 point • Short hand correctly placed: 1 point
Verbal Fluency
• Leqer fluency: • All the words in 1 min beginning with “F”, “A” and “S”
• Normal is >9 per min for each (Dubois 2000) • Category fluency: • All the animals in 1 min
• Normal is >17 per min