neurosensory: traumatic spinal cord injury. a. pathophysiology/etiology normal spinal cord as it...
TRANSCRIPT

Neurosensory:
Traumatic Spinal Cord Injury
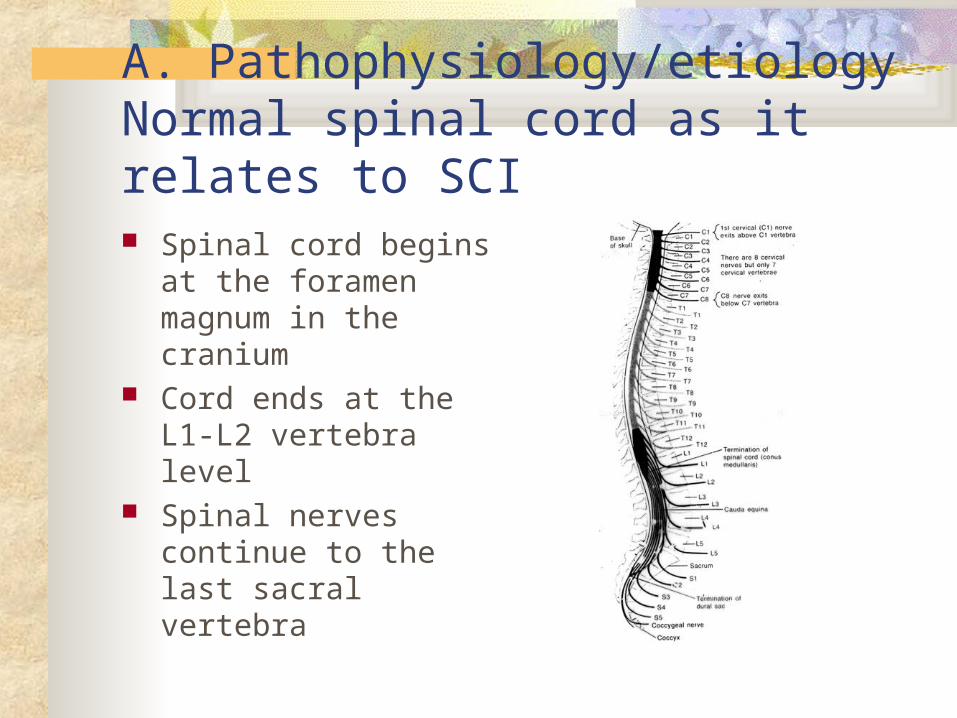
A. Pathophysiology/etiologyNormal spinal cord as it relates to SCI Spinal cord begins at
the foramen magnum in the cranium
Cord ends at the L1-L2 vertebra level
Spinal nerves continue to the last sacral vertebra


Normal protection of spinal cord from injury: Bones- vertebral column

Protection of spinal cord from injury Disc between
vertebra Internal and external
ligaments

Protection of Spinal Cord from Injury Meninges CSF in subarachnoid
space allow for movement within spinal canal

Normal spinal cord as relates SCI: Autonomic Nervous System & Cord ANS can be affected
by SCI Sympathetic chains
on both sides of the spinal column
Parasympathic nervous system is the cranial-sacral branch

Normal spinal cord: White tracks send messages to and from the brain Pyramidal- Voluntary
movements Posterior column
(Dorsal)- touch, proprioception, and vibration sense
Lateral spinothalamic tract- pain and temperature sensation (only tract that crosses within the cord)

Normal spinal cord: Reflex ark in center of the spinal cord Where sensory and
motor nerves arise from cord
Motor fibers leave posterior
Sensory fibers enter from anterior
Once outside cord join form spinal nerve


Dermatones


Normal spinal cord: Spinal cord level When referring to spinal
cord level, it the reflex ark level not the vertebral or bone level.
Note that the thoracic, lumbar & sacral reflex arks are higher than were the spinal nerves actually leave through the opening of there respective vertebral bone

Patho: Forces resulting in SCI Flexion (hyperflexion) Most common
because of natural protection position.
Generally cause neck to be unstable because stretching of ligaments

Patho/forces: Hyperextention Caused by chin
hitting a surface area, such as dashboard or bathtub
Usually causes central cord syndrome symptoms

Patho/forces: Compression Caused by force from
above, as hit on head Or from below as
landing on butt Usually affects the
lumbar region



Classification of spinal cord injury:1. Complete (transection) spinal cord inj After spinal shock: Motor deficits-
spastic paralysis below level of injury
Sensory- loss of all sensation perception
Autonomic deficits- vasomotor failure and spastic bladder

2. Incomplete spinal cord injury- what white tracks are working after spinal shock is over?

Incomplete spinal cord injury: Central cord Syndrome Injury to the center of
the cord by edema and hemorrhage
Weakness in both upper extremities- legs are spared
Varied loss of sensation



Incomplete spinal cord injury: Anterior Cord Syndrome Injury to anterior cord Loss of voluntary
motor (Pyramidal track) below
Loss of pain and temperature perception
Retains posterior column function


Incomplete spinal cord injury: Brown-Sequard Syndrome Hemisection of cord Ipsilateral paralysis Ipsilateral superficial
sensation, vibration and proprioception loss
Contralateral loss of pain and temperature perception



Horner’s Syndrome

Classification of spinal cord injury- 3. by level of spinal cord injury In addition to complete or
incomplete- Spinal cord injuries are
also described by the level of the injury– the cord segment or dermatome level
Such as C6; L4 spinal cord injury

Common manifestations/complications:Spinal shock- depression of cord & ANS Motor loss- flaccid paralysis below level injury Sensory loss- loss touch, pressure, temperature
pain and proprioception perception below injury Sympathetic NS loss results in parasympathic
dominance with vasomotor failure- Neurogenic shock, bradycardia, orthostatic
hypotension and poor temperature control (poikilothermic- takes on temp of environment)
Parasympathetic NS loss of the S 2,3,4 reflex arks results in flaccid bladder

Spinal shock lasts from few minutes to weeks How do you know spinal shock is over?
Clonus is one of the first signs
Hyperreflexia of foot Test by flexing leg at
knee & quickly dorsiflex the foot
Rhythmic oscillations of foot against hand
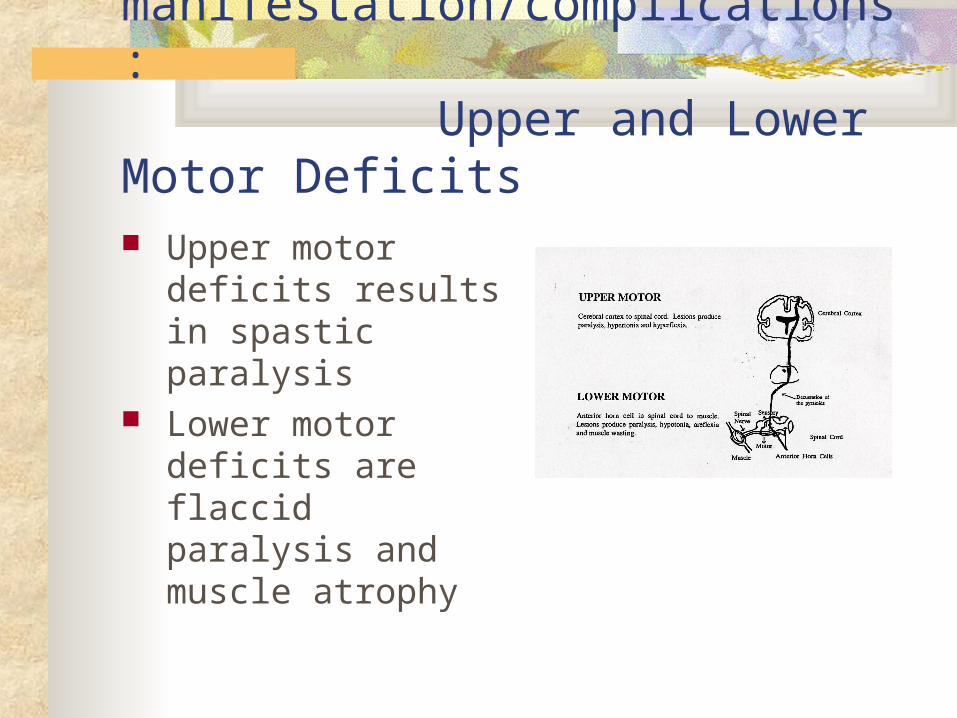
Common manifestation/complications: Upper and Lower Motor Deficits Upper motor deficits
results in spastic paralysis
Lower motor deficits are flaccid paralysis and muscle atrophy

Common manifestations/complications: Functional Goals for Spinal Cord Injury C1-3 usually fatal- loss phrenic innervation;
ventilator dependent; no B/B control; spastic paralysis; electric w/c with chin/mouth control
C6- weak grasp; has shoulder/biceps to transfer & push w/c; no bowel/bladder control. Considered level of independence
T1-6- full use of upper extremity; transfer; drive car with hand controls and do ADL’s; no bowel/bladder control

C. Therapeutic Interventions for SCI: Diagnostic tests
X-ray of spinal column
CT/MRI Blood gases

Transporting a SCI

Traction
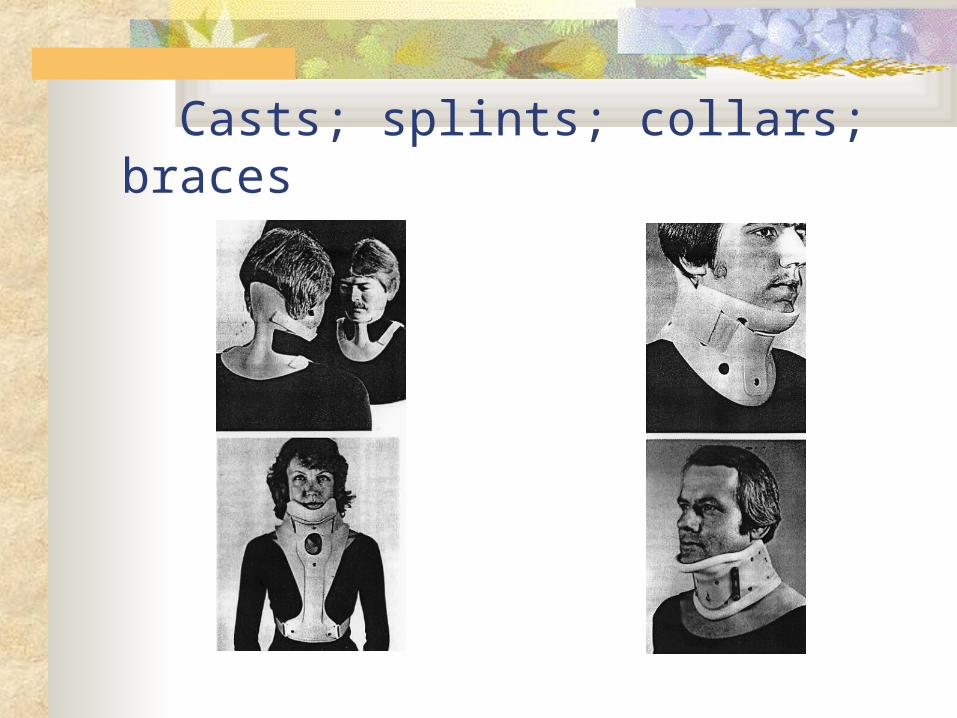
Casts; splints; collars; braces

Special Beds for SCI To decrease
immobility complications
Rotorest is a common one used- rotates 23 hrs a day

Therapeutic interventions: Surgery for SCI Manipulation to
correct dislocation or to unlock vertebrae
Decompression laminectomy
Spinal fusion Wiring or rods to
hold vertebrae together

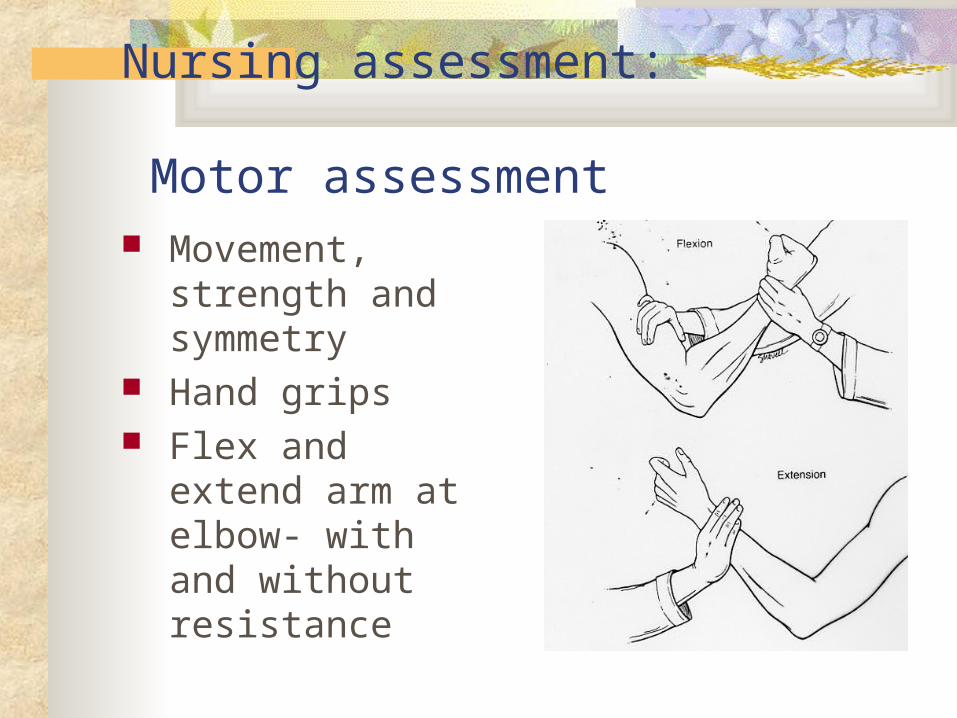
Nursing assessment: Motor assessment Movement, strength
and symmetry Hand grips Flex and extend arm
at elbow- with and without resistance


Nursing assessment: Motor assessment lower extremity Flex and extend leg at
knee with and without resistance
Planter and dorsi flexion of foot
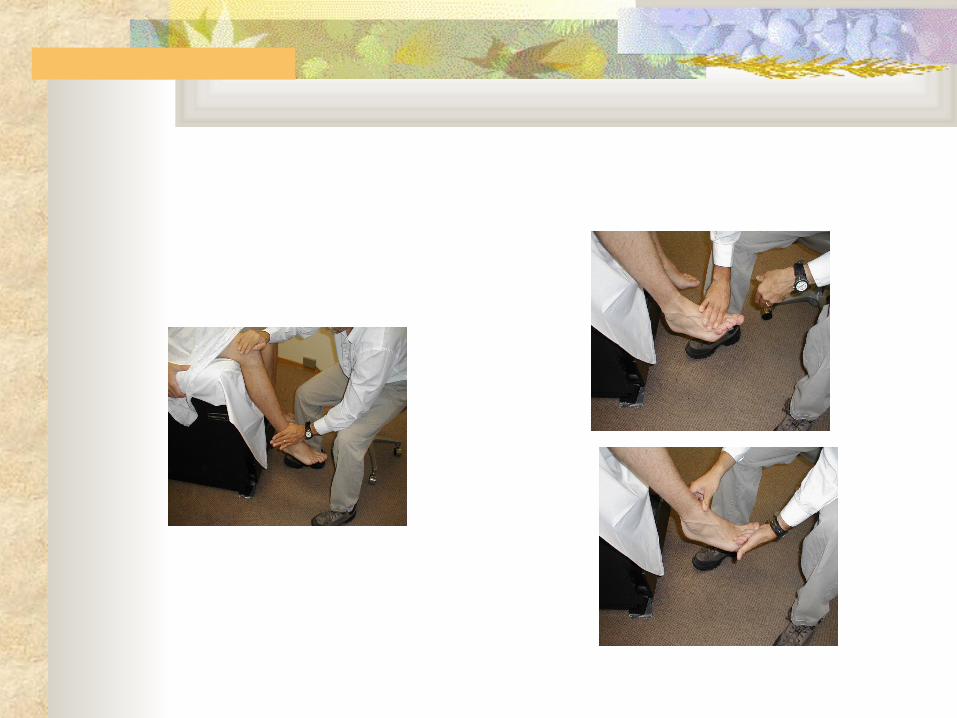

Nursing assessment: Motor assessment- Clonus Clonus- hyperreflexia Flex knee and quickly
dorsiflex the foot with your hand
If has return of reflex function the foot will have repetitive movements against you hand
Spinal shock is over

Nursing assessment: Sensory assessment With the sharp and
dull ends of a paperclip have the individual, with their eyes closed identify
Use the dermatome as reference to identify level
C6 thumb; T4 nipple; T10 naval

Use of transfer board

2. Impaired gas exchange Phrenic nerve (C3-5) controls the diaphragm
bilaterally. If nerve is nonfunctioning then individual is ventilator dependent.
Thoracic nerves control the intercostals muscles for breathing and abdominal muscles aide in breathing and coughing

Phrenic nerve

Intercostal nerves

Quad cough (assistive cough)
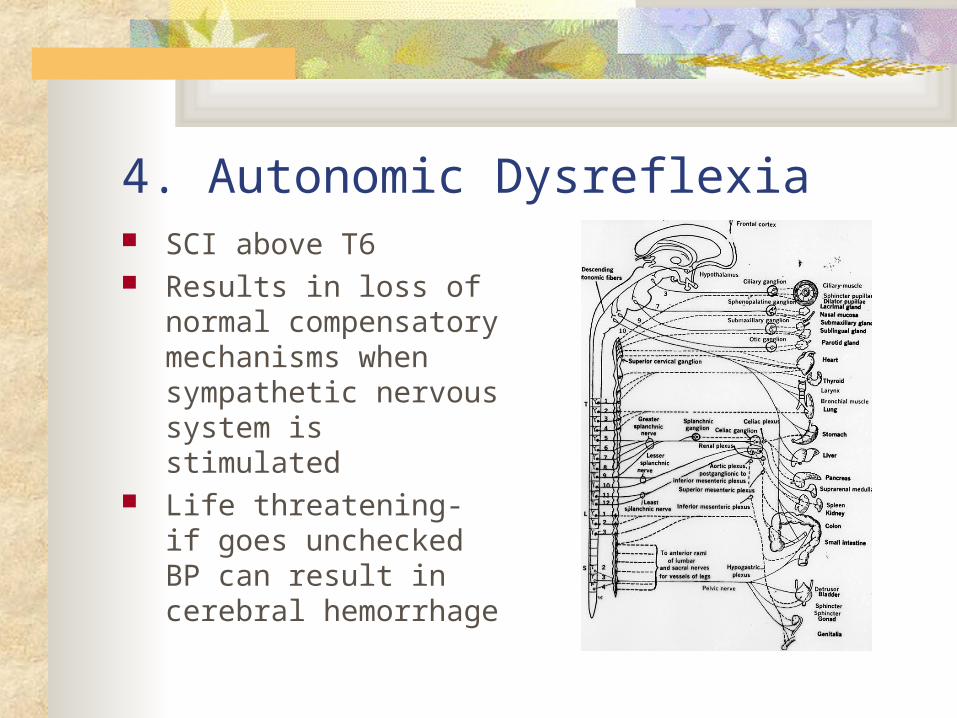
4. Autonomic Dysreflexia SCI above T6 Results in loss of normal
compensatory mechanisms when sympathetic nervous system is stimulated
Life threatening- if goes unchecked BP can result in cerebral hemorrhage

Autonomic Dysreflexia- assess
Vasodilatation
symptoms above SCI Vasoconstriction
symptoms below SCI The cause of SNS
stimulation


A. upper motor bladder B. lower motor bladder

Bladder functioning: http://www.rnceus.com/course_frame.asp?
exam_id=56&directory=uro

Additional Critical thinking questions LeMone p 1334: Nursing Care Plan: A Client with a SCI 1. Why does Jim have flaccid paralysis on
admission to ICU? 2. What symptoms indicate that he is in spinal
shock? What was done about these symptoms? 3. How will we know when he is out of spinal
shock? 4. How does progressive mobilization assist with
orthostatic hypotension? What else can be done? 5. What are realistic functional goals for Jim?