neurotoxic exposure and olfactory impairment
TRANSCRIPT
NEUROTOXICOLOGY 1526--0046/01 $15.00 + .00
NEUROTOXIC EXPOSURE ANDOLFACTORY IMPAIRMENT
Richard L. Doty, PhD, and Lloyd Hastings, PhD
Normal functioning of the olfactory system is a prerequisite for thedetection of several chemical environmental hazards (e.g., spoiled foods,leaking natural gas, smoke and various airborne pollutants), and for the fullappreciation of foods, beverages, flowers, perfumes, spices, the seashore,the mountains, and the seasons of the year. Distortions or loss of smell func-tion can adversely influence food preferences, food intake, and appetite,and in some cases can lead to significant psychological depression. It isthus no wonder that dysfunction of olfaction is of considerable concern topersons who experience it, particularly those dependent on this sense fortheir livelihood or safety (e.g., cooks, homemakers, plumbers, fire fighters,perfumers, fragrance sales persons, wine merchants, coffee or tea tasters,food and beverage distributors, and employees of numerous chemical, gas,and public works industries).
Although smell dysfunction secondary to toxic exposure is generallyless common than smell dysfunction caused by a number of other causes(e.g., upper respiratory infections, head trauma, chronic rhinitis or rhino-sinusitis), it nonetheless exists. In addition to directly damaging the olfac-tory mucosa, some toxins may, in fact, induce upper respiratory inflamma-tory responses or infections that produce such damage, as well as enter thecentral nervous system (CNS) and cause damage to CNS structures. Olfac-tory loss can occur as a result of exposure to toxins in general air pollutionand in workplace situations, where litigation becomes a consideration.Most cases of toxin-related olfactory loss do not get referred to special-ized centers such as ours for evaluation. In fact, smell function is rarely
From the Smell and Taste Center and Department of Otorhinolaryngology: Head and NeckSurgery, University of Pennsylvania Medical Center, Philadelphia, Pennsylvania
CLINICS IN OCCUPATIONAL AND ENVIRONMENTAL MEDICINE
547VOLUME 1 .NUMBER 3 .AUGUST 2001
548 DOTY & HASTINGS
assessed quantitatively by local medical personnel, despite the availabilityof accurate, easy-to-use, and inexpensive tests for this purpose. unfortu-nately, there continues to be a paucity of quantitative research investigatingtoxin-related effects on the sense of smell, and most reports of such effectsare mainly anecdotal in nature.
In this article, we first describe basic elements of nasal airflow andthe peripheral anatomy of the human olfactory system.* We then discusscommon methods for quantitatively evaluating smell function, and sub-sequently present an overview of the types of toxic agents that reportedlyalter such function. Included are studies of toxic metals (e.g., cadmium,mercury), irritant gases (e.g., 502, formaldehyde), and solvents (e.g., ace-tone). Although the emphasis of the review is on humans, a listing of toxicagents known to damage the olfactory epithelia of rodents is provided,and data from animal studies are discussed when they relate to findingsfrom human studies.
PERIPHERAL OLFACTORY SYSTEM ANATOMY
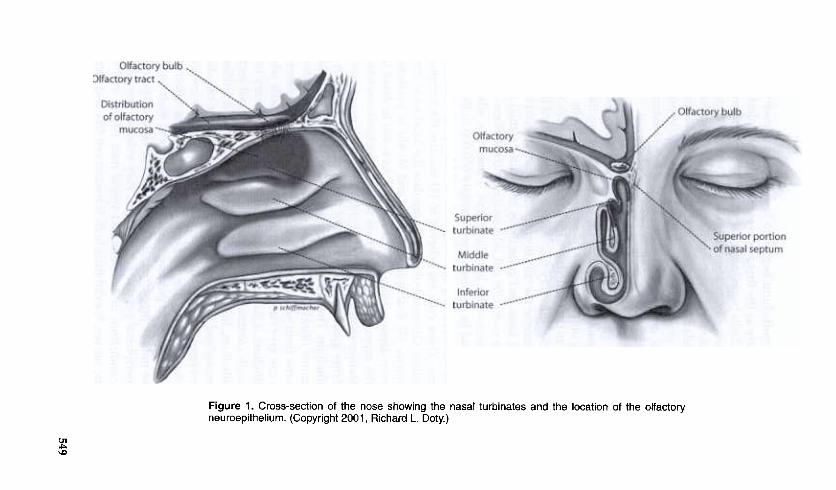
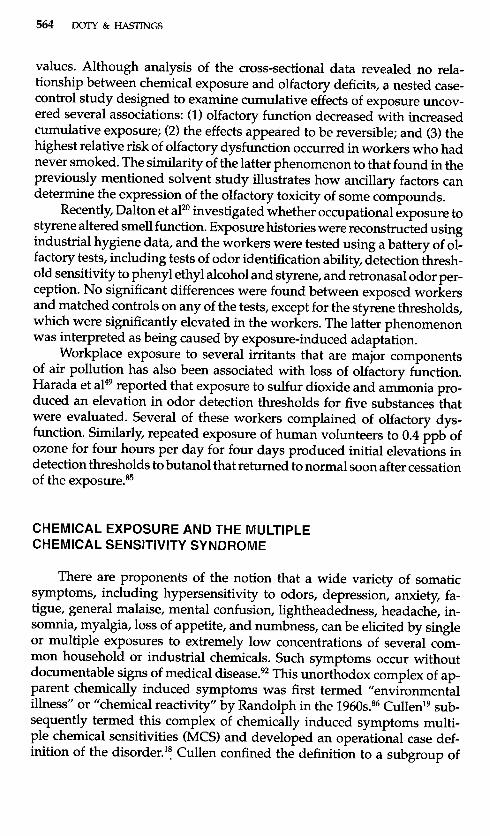
Most toxic agents adversely influence olfaction by directly damagingthe olfactory neuroepithelium, which is located in the upper recesses ofthe nasal chambers, lining the cribriform plate and sectors of the superiorturbinate, superior septum, and middle turbinate (Fig. 1). Although mostof this epithelium is positioned away from the main airsteam and, hence,is thought to be protected to some degree from inhaled vapors, xenobioticsstill readily reach this vulnerable region. As noted by Swift and Proctor;oounder conditions of normal resting inspiration (0.15-0.25 Lis), air passesat a vertical angle upwards through the anterior naris at a velocity of 2 to3 meters per second. At this point, from 10% to 15% of the airstream isshunted toward the olfactory cleft. At the termination of the vestibule (i.e.,the ostium internum, the most narrow and restrictive portion of the entireairway), the main airstream changes direction from vertical to horizon-tal. At this transition point, the airstream reaches hurricane-force veloci-ties (12-18 ml s) before exiting the area and returning to speeds less than4 meters per second. The highly nonlaminar (turbulent) flow that devel-ops after the ostium intemum results in increased contact with the bloodswollen turbinates, thereby warming, cleansing, and humidifying the ma-jor portion of the airstream.
*In addition to the main olfactory system (cranial nerve I), the reader should be awarethat other specialized neural systems are present in the nose. These include (1) trigeminalafferents responsible, for example, for the coolness of menthol vapors and irritative responsesto volatile chemicals24; (2) a rudimentary and nonfunctional vomeronasal organ near the baseof the septum9, !02; and (3) the poorly understood nervus terminalis or terminal nerve (CN 0).CN 0, a highly conserved neural plexus that ramifies throughout the nasal epithelium, isdistinguished by ganglia at n.odal points and a high gonadotropin content.96
>-
C5
uSoQ)
:5Oc.Q'i§.QQ)
:5"Cct13
(/)Q
)roc:0.:a
""iU(/)t13cQ
)-;;.c--0C
)OC
.
.--l
~"C
0 '-
.ct13(/).c
()Q
) .-
(/)a:0
-C
~
Q)O
.c°-C
\J--0.C
C)
C
.-=0>
-.-c.U
OQ)O
(/)~,
.
gj E
0 ~
U~
.c.-
c.Q
) Q
)'-
0~
'-
OI~
.-Q)
U.c
549
550 DOTY & HASTINGS
The olfactory epithelium begins to lose its homogeneity soon afterbirth. Indeed, as early as the first few weeks of life, metaplastic islands ofrespiratory-like epithelia begin to appear within its borders, presumably asa result of insults from environmental viruses, bacteria, and toxins.76 Theseislands increase in extent and number throughout life. Surprisingly, in partbecause of the cumulative metaplasia and the age-related heterogeneity ofthe epithelium, the exact size of the olfactory epithelium in humans is stillnot well established, and there is suggestion that it may extend, in adults,further onto the middle turbinate than previously believed.
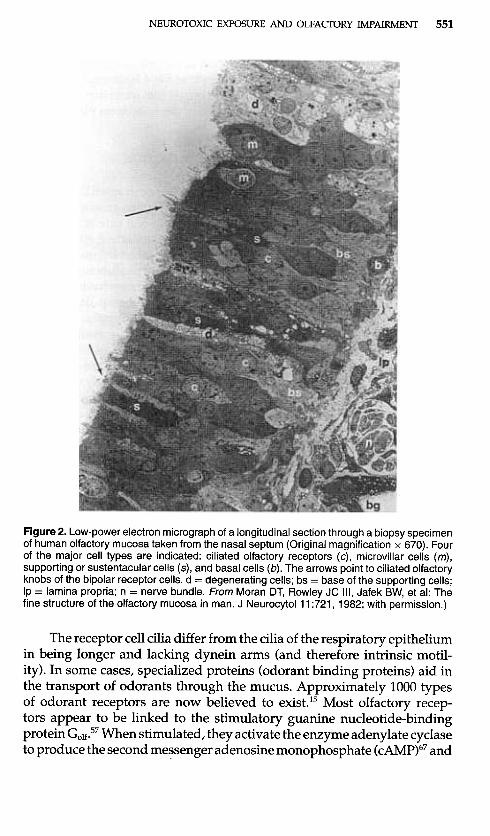
The mature olfactory epithelium is comprised of at least six distinctcell types (Fig. 2).53 The first, the bipolar sensory receptor neuron, reportedlynumbers approximately 6 million in the adult, exceeding the number ofreceptor cells in any other sensory system except vision.74 The olfactory re-ceptors are located on the ciliated dendritic ends of these cells whose axonscoalesce into 30 to 50 "olfactory fila," which are ensheathed by Schwann-like cells. The ma traverse the cribriform plate of the ethmoid bone to enterthe anterior cranial fossa and collectively constitute cranial nerve I. Thesecond cell type, the microvillar cell, is located near the surface of the epithe-lium and projects microvillae into the mucus. These cells, whose functionis unknown, are said to number approximately 600,000 in the adult. Thethird cell type, the supporting or sustentacular cell, also projects microvillaeinto the mucus. These cells are believed to (1) insulate the receptor cellsfrom one another, (2) contribute to and regulate the local ionic composi-tion of the mucus, (3) deactivate odorants, and (4) aid in protecting theepithelium from damage from foreign agents,47 As noted in detail later inthis article, the supporting cells contain several xenobiotic-metabolizingenzymes, a feature shared with the cells that line the Bowman's glands andducts.65 The latter glands provide most of the mucus in the region of theolfactory epithelium. The fifth and six cell types are the globose (light) basalcell and horizontal (dark) basal cell. These cells are located near the base-ment membrane from which the other cell types arise. It is believed thatglobose cells can give rise to both neurons and non-neural cells when theolfactory epithelium is damaged, expressing a rare multipotency for stemcells.53 Although continuous neurogenesis occurs in the basal sectors ofthe neuroepithelium, long-lived receptor cells have been identified, andboth endogenous and exogenous factors promote receptor cell death orreplenishment from the progenitor stem cells.68 The olfactory ensheathingcells, which form the bundles of axons that comprise the olfactory fila,play an important role in guiding regenerating axons to their bulbar tar-gets and have unique properties useful in repair or regeneration of bothcentral and peripheral nerves. For example, they enhance remyelinationand axonal conduction in demyelinated spinal tract nerves and in sev-ered rat sciatic nerves;10 exhibiting both Schwann cell-like and astrocyte-like properties.55
NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT 551
Figure 2. Low-power electron micrograph of a longitudinal section through a biopsy specimenof human olfactory mucosa taken from the nasal septum (Original magnification x 670). Fourof the major cell types are indicated: ciliated olfactory receptors (c), microvillar cells (m),supporting or sustentacular cells (5), and basal cells (b). The arrows point to ciliated olfactoryknobs of the bipolar receptor cells. d = degenerating cells; bs = base of the supporting cells;Ip = lamina propria; n = nerve bundle. From Moran DT, Rowley JC Ill, Jafek BW, et al: Thefine structure of the olfactory mucosa in man. J Neurocytol11 :721, 1982; with permission.)
The receptor cell cilia differ from the cilia of the respiratory epitheliumin being longer and lacking dynein arms (and therefore intrinsic motil-ity). In some cases, specialized proteins (odorant binding proteins) aid inthe transport of odorants through the mucus. Approximately 1000 typesof odorant receptors are now believed to exist.15 Most olfactory recep-tors appear to be linked to the stimulatory guanine nucleotide-bindingprotein Go1f.57 When stimulated, they activate the enzyme adenylate cyclaseto produce the second me~senger adenosine monophosphate (cAMP)67 and

552 DOTY & HASTINGS
subsequent events related to depolarization of the cell membrane and sig-nal propagation. In the few rodent species that have been evaluated, theolfactory receptors are topographically organized into four strip-like zonesthat roughly parallel the dorsal-ventral axis of the cribriform plate.109
METHODS OF EVALUATING OLFACTORY FUNCTION
An astute physician of yesteryear tested the sense of smell by asking apatient to identify several crude odorants, such as coffee grounds, cloves,or perfume placed under the nose, perhaps testing one side at a time byclosing the contralateral naris with a finger. This qualitative approach tosmell testing, however, was unreliable, was easily faked by malingerers,and provided no information on the relative degree of dysfunction. Impor-tantly, it often led to the wrong conclusions, because persons have difficultyaccurately identifying an odor without being presented with alternatives.
Fortunately, advances in the technology of psychophysical measure-ment and the proliferation of easy-to-use and commercially available testsof olfactory function now make it possible for toxicologists and others to ac-curately and quantitatively assess the ability to smell.29 With the exceptionof dysosmia and phantosmia (whose diagnoses are based solely on patientreport), quantitative psychophysical testing allows for the assignment ofpatients to specific sensory diagnostic categories. The following categoriesare widely accepted: Anosmia: inability to detect qualitative olfactory sen-sations (i.e., absence of smell function); partial anosmia: ability to perceivesome, but not all, odors; hyposmia or microsmia: decreased sensitivity toodors; hyperosmia: abnormally acute smell function; dysosmia (sometimestermed cacosmia or parosmia): distorted or perverted smell perception toodor stimulation); phantosmia: a dysosmic sensation perceived in the ab-sence of an odor stimulus (also known as olfactory hallucination); andagnosia (olfactory): inability to recognize an odor sensation, even thougholfactory processing, language, and general intellectual functions are es-sentially intact, as in some stroke patients. Olfactory dysfunction can alsobe classified into bilateral or unilateral categories (sometimes termed bi-nasal or uninasal). In most cases, bilateral test scores reflect the better func-tioning of the two sides of the nose. Although presbyosmia is sometimesused to describe smell loss caused by aging, this term does not distinguishbetween anosmia and hyposmia and implies that it is age per se, that iscausing the age-related deficit.
The most popular quantitative olfactory tests are those of odor iden-tification, discrimination, memory, and detection. Self-administered teststhat use microencapsulation technology (i.e., "scratch and sniff" odorants)are the most widely used, including the 40-odor University of Pennsylva-nia Smell Identification Test (UPSIT; known commercially as the Smell
NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT 553
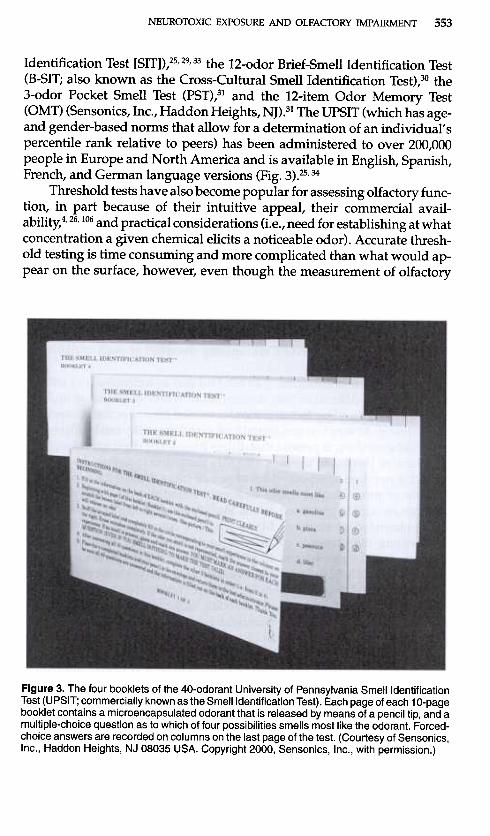
Identification Test [SIT]),25,29,33 the 12-odor Brief-Smell Identification Test(B-SIT; also known as the Cross-Cultural Smell Identification Test),30 the3-odor Pocket Smell Test (PST),31 and the 12-item Odor Memory Test(OMT) (Sensonics, Inc., Haddon Heights, NJ).31 The UPSIT (which has age-and gender-based norms that allow for a determination of an individual'spercentile rank relative to peers) has been administered to over 200,000people in Europe and North America and is available in English, Spanish,French, and German language versions (Fig. 3).25,34
Threshold tests have also become popular for assessing olfactory func-tion, in part because of their intuitive appeal, their commercial avail-ability!' 26, 106 and practical considerations (i.e., need for establishing at what
concentration a given chemical elicits a noticeable odor). Accurate thresh-old testing is time consuming and more complicated than what would ap-pear on the surface, however, even though the measurement of olfactory
Figure 3. The four booklets of the 40-odorant University of Pennsylvania Smell IdentificationTest (UPSIT; commercially known as the Smell Identification Test). Each page of each 10-pagebooklet contains a microencapsulated odorant that is released by means of a pencil tip, and amultiple-choice question as to which of four possibilities smells most like the odorant. Forced-choice answers are recorded on columns on the last page of the test. (Courtesy of Sensonics,Inc., Haddon Heights, NJ 08035 USA. Copyright 2000, Sensonics, Inc., with permission.)
554 DOTY & HASTINGS
thresholds seems straightforward and regulatory agencies and others fre-quently report "the threshold value" for a given chemical. Thus, there areseveral types of olfactory thresholds, including detection thresholds, iden-tification thresholds, and differential thresholds. Even within a thresholdclass, there are a variety of procedures for presenting the stimuli and op-erationally defining the threshold, all of which have an effect on the finalthreshold value. For example, the number of trials used, the use or nonuseof forced-choice trials, the magnitude of the stimulus steps, and the natureof the dilution medium all have an effect on the threshold measure.28,3l,81Importantly, the empirically defined threshold value is a function of thehuman observer, being influenced by factors such as the subject's age andgeneral health.21 Even when the number of molecules entering the noseis known, further dilution of the stimulus occurs in the nose, making itimpossible to specify the exact number of molecules reaching the olfactoryreceptors. This number depends on such variables as the size of the sniff,the size of the nose, the size and shape of the nasal turbinates, the thicknessof the mucus, and numerous other idiosyncratic parameters. Fortunately,from a practical perspective, the olfactory system is very sensitive to thefirst few molecules it receives, minimizing the effect of such variables onthe threshold measure.
The lowest concentration of an odorant that an individual can reliablydetect (usually defined as that concentration where detection is midwaybetween chance and perfect detection) is termed his or her detection or abso-lute threshold. At very low concentrations, no odor quality can be discerned,only that something is present that differs from air or the comparison dilu-ent blank or blanks. In modern olfactory detection threshold testing, thesubject is required to report which of two or more stimuli (i.e., an odorantand one or more blanks) smells strongest, rather than to simply indicatewhether an odor is perceived or not. Such "forced-choice" procedures areless confounded by response biases (e.g., the conservatism or liberalismin reporting the presence of an odor under uncertain conditions) thannonforced-choice procedures. In addition, they are more reliable and pro-duce lower threshold values.31 The instructions given to a subject are criticalin measuring a detection threshold, because if the subject is instructed toreport which stimulus produces an odor, rather than which stimulus isstronger, a spuriously higher threshold value may result (odor quality ispresent only at higher perithreshold concentrations).
The recognition threshold is defined as the lowest concentration whereodor quality is reliably discerned. Unfortunately, it is nearly impossibleto control criterion biases in recognition threshold measurement. Thus, ina forced-choice situation, guesses are rarely randomly distributed amongalternatives, potentially leading to a spuriously low recognition thresh-old for the preferred alternative. A classic example of this problem comesfrom taste psychophysics, where some subjects report "sour" much more
NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT 555
frequently than the other primary qualities in the absence of a clearlydiscernible stimulus, resulting in a spuriously low sour-taste recognitionthreshold measure.113
A third type of threshold is the differential threshold, the smallestamount by which a stimulus must be changed to make it perceptiblystronger or weaker. The size of the increment in odorant concentration (~I)required to produce a "just noticable difference" increases as the compar-ison concentration {1) increases, with the ratio approximating a constant(i.e., ~I/I = C). This phenomenon was described by Weber in 1834 andwas termed "Weber's Law" by Fechner in 1860.40 Although differentialthresholds have been measured in olfaction, they have received little prac-tical application.
Two types of psychophysical detection threshold procedures have re-ceived the most use in the last two decades: the ascending method of lim-its procedure (AML) and the single staircase procedure (55).23,28 In theAML procedure, odorants are presented sequentially from low to highconcentrations, and the point of transition between detection and no de-tection is estimated. In the 55 method, the concentration of the stimulusis increased after trials on which a subject fails to detect the stimulus anddecreased after trials where correct detection occurs. An average of the up-down transitions ("reversals") is used to estimate the threshold value. Inboth the AML and 55 procedures, the direction of initial stimulus presen-tation is made from weak to strong in an effort to reduce potential adap-tation effects of prior stimulation. The stability or reliability of a thresholdmeasure is predictably related to the number of trials presented. Hence,procedures with more trials focused in the perithreshold region, such asthe 55 procedure, produce less variable and more reliable measures thansimple AML procedures.31
For the most part, when an individual has a high threshold (i.e., is lesssensitive) to one compound, he or she has high thresholds to other com-pounds as well. This is because most odors depend on the activation ofmore than one type of receptor and because odorants often share commonsubsets of receptor types. Because the various types of receptors are inter-spersed irregularly throughout the epithelium, damage to one region ofthe epithelium influences the perception to many, indeed probably most,odorants. Theoretically, the degree to which different odors are altered bysubtotal damage to the epithelium could vary idiosyncratically, depend-ing on the extent to which each odorant depends on common or disparatereceptor types, the relative frequencies of such receptor types, and the num-ber of receptor types activated by each odorant. Nonetheless, as a generalrule, detection threshold sensitivity to one compound is correlated to thatof other compounds, thus explaining why a detection threshold measureto a single chemical can typically be used clinically to establish the degreeof overall olfactory functi.on.
556 OOTY & HASnNGS
Although there is suggestion that tests of identification or discrim-ination are more sensitive than tests of odor threshold to lesions in thecentral olfactory pathways; lesions of the olfactory epithelium can also in-fluence odor identification and discrimination test scores. Furthermore,some studies have found that central brain lesions can, indeed, influ-ence odor detection thresholds. Hence, one cannot reliably infer the lo-cus of the underlying neuropathology from psychophysical test results.Indeed, it is not even clear whether or to what degree many nominallydisparate olfactory tests actually measure dissimilar perceptual attributes.Thus, in one study, nine nominally different olfactory tests (e.g., tests ofodor identification, discrimination, detection, memory, and suprathresh-old intensity and pleasantness perception) were administered to 97 healthindividuals representing both sexes and a wide range of ages.35 A princi-pal components analysis performed on the correlation matrix among thetests revealed four meaningful components. The first received strong pri-mary loadings from most of the olfactory test measures (including testsof odor identification, discrimination, and threshold), whereas the secondwas composed of primary loadings from intensity ratings given to a set ofsuprathreshold odorant concentrations. The third and fourth componentshad primary loadings that reflected, respectively, mean suprathresholdpleasantness ratings and a response bias measure derived from a yes/noodor identification signal detection task. The results of this study suggestthat, at least in healthy subjects spanning a wide age range, several nomi-nally distinct tests of olfactory function are measuring a common source ofvariance.
LOSS OR ALTERATION OF OLFACTORY FUNCTIONFROM CHEMICAL EXPOSURE
The medical and toxicologic literature is replete with reports of smellloss or distortion in humans after acute or chronic exposure to a numberof volatile chemicals. Because a detailed assessment of all of these reportsis impossible within the scope of this article, we briefly summarize datain this section from two major reviews that have appeared on this topicand focus on compounds for which more sound empirically-based dataare available.
Naus77listed several early and mainly European studies of smell dys-function after workplace exposure to airborne agents. Most of these studiesused some form of odor threshold task and reported adverse effects onthe ability to smell dusts and heavy metals (e.g., spices, flour, cotton,lead, coal, mercury, cadmium, coke, grain, SiO2, tobacco, paper, cement,ashes} and industrial volatile chemicals (e.g., perfumes, menthol, carbo-nic disulfide, benzene, ,dichloromethane, pentachlorophenolate, ammonia,

557NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
bromine, trichloroethylene, nitrous gases, acids). In the reviewed studies,Naus further sought associations between the presence of hyposmia andfactors such as cigarette smoking and duration of exposure. Unfortunately,the studies examined were heterogeneous in terms of methods, and theirmeans for assessing olfactory function were non-forced-choice, therebyconfounding the examinee's response criterion with the measure of sen-sory sensitivity.29 Importantly, many of these studies, as well as Naus' ownanalyses, did not use control groups or take into account such basic con-founding as the association of age with duration of chemical exposure.Age alone is known to be associated with decreases in olfactory function.32Be as it may, Naus' pioneering review mustered convincing evidence fortoxin-induced hyposmia in several industrial settings.
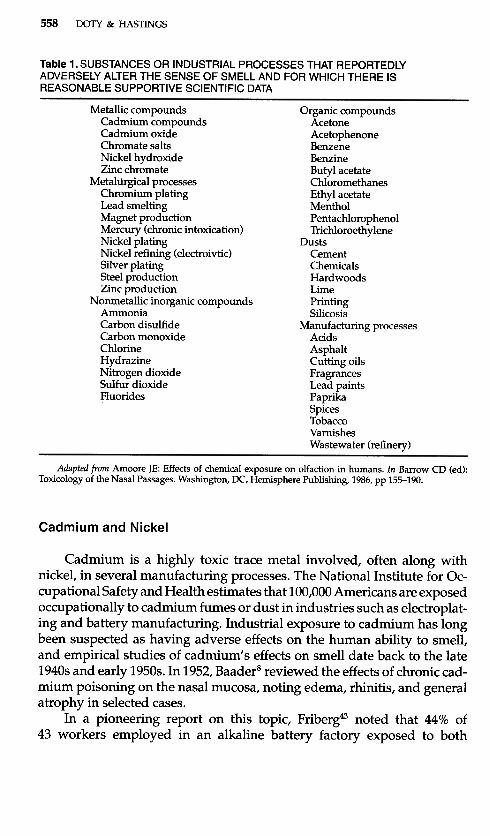
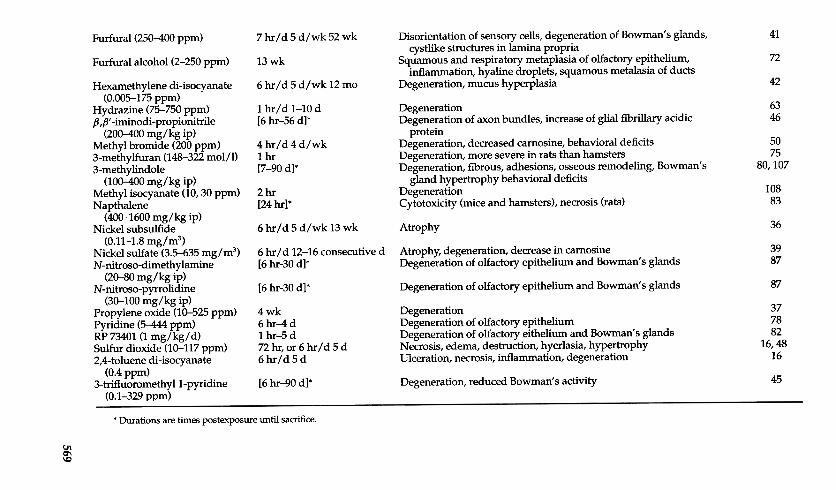
More recently, Amoore3listed more than 120 different compounds andindustrial processes reported to adversely affect olfactory function, a num-ber of which were mentioned by Naus. More than 75 of the studies citedby Amoore examined the relationship between exposure and olfactorydysfunction. Most were case reports or case series, however, and quan-titative assessment of function was the exception, rather than the rule.Furthermore, because of the general lack of good industrial hygiene prac-tices during much of the period reviewed, reported exposure levels weremainly rough estimates. Compounds listed by Amoore for which there isat least some empirical basis for adverse influences on smell function arelisted in Table 1.
In addition to losses of smell function, perversions of the sense ofsmell or untoward irritative effects can result from some toxic exposures.For example, Emmet38 described the case of a pipe fitter exposed totetrahydrofuran-containing pipe cement who complained of a constantunpleasant smell (parosmia); recovery occurred after removal of exposureto the pipe cement. Shusterman and SheedylOl described a woman ex-posed to chloramine gas who complained of a "stinging" in the nasophar-ynx in response to common household odors from which she eventuallyrecovered.
EMPIRICAL STUDIES OF VOLATILE TOXICEXPOSURES ON HUMAN OLFACTORY FUNCTION
Several classes of chemicals have been clearly implicated in altering theability to smell, as noted in detail below. Although some studies have notused statistical techniques to unconfound age with duration of exposure,the frequency of the reports and the magnitude of the effects are so large formost of the toxins evaluated that age confounding is likely inconsequential.The largest group of these studies has focused on workers exposed tocadmium and nickel.
558 DOTY & HASnNGS
Table 1. SUBSTANCES OR INDUSTRIAL PROCESSES THAT REPORTEDLYADVERSELY ALTER THE SENSE OF SMELL AND FOR WHICH THERE ISREASONABLE SUPPORTIVE SCIENTIFIC DATA
Metallic compoundsCadmium compoundsCadmium oxideChromate saltsNickel hydroxideZinc chromate
Metaltirgical processesChromium platingLead smeltingMagnet productionMercury (chronic intoxication)Nickel platingNickel refining (electroivtic)Silver platingSteel productionZinc production
Nonmetallic inorganic compoundsAmmoniaCarbon disulfideCarbon monoxideChlorineHydrazineNitrogen dioxideSulfur dioxideFluorides
Organic compoundsAcetoneAcetophenoneBenzeneBenzineButyl acetateChloromethanesEthyl acetateMentholPentachlorophenolTrichloroethylene
DustsCementChemicalsHardwoodsLimePrintingSilicosis
Manufacturing processesAcidsAsphaltCutting oilsFragrancesLead paintsPaprikaSpicesTobaccoVarnishesWastewater (refinery)
Adapted from Amoore JE: Effects of chemical exposure on olfaction in humans. In Barrow CD (ed):Toxicology of the Nasal Passages. Washington, DC, Hemisphere Publishing, 1986, pp 155-190.
Cadmium and Nickel
Cadmium is a highly toxic trace metal involved, often along withnickel, in several manufacturing processes. The National Institute for Oc-cupational Safety and Health estimates that 100,000 Americans are exposedoccupationally to cadmium fumes or dust in industries such as electroplat-ing and battery manufacturing. Industrial exposure to cadmium has longbeen suspected as having adverse effects on the human ability to smell,and empirical studies of cadmium's effects on smell date back to the late1940s and early 1950s.1n 1952, BaaderB reviewed the effects of chronic cad-mium poisoning on the nasal mucosa, noting edema, rhinitis, and generalatrophy in selected cases.
In a pioneering report on this topic, Friberg43 noted that 44% of43 workers employed in an alkaline battery factory exposed to both

559NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
cadmium-iron dust (5-15 mg/m3 of air) and nickel graphite dust (10-150 mg/m3 of air) for periods ranging from 9 to 34 years complained ofdecreased ability to smell. On sensory examination, approximately onethird of these workers were reportedly anosmic, although the nature ofthe olfactory testing was not reported. Only 10% of 15 workers employedin the same areas of the factory for four years or less complained of thisproblem; none were apparently tested for their smell ability.
Ten years after the Friberg study, Adams and Crabtree1 found, in astudy of 106 cadmium- and nickel-dust-exposed alkaline battery workersand 84 matched normal controls that the exposed individuals performedsignificantly more poorly than the controls on an odor threshold test us-ing phenol. In this study, 27% of the exposed workers were reportedlyanosmic, compared with 5% of the controls. Although the amount of ex-posure to cadmium could only be roughly estimated, in some factory sitesit apparently reached levels as high as 2.76 mg/m3. Approximately half ofthe anosmic workers were unaware of their disorder. Despite the fact thatexamination of the nasal mucosa failed to yield any relationship betweendegree of irritation and olfactory dysfunction, proteinuria was positivelycorrelated with the presence of anosmia.
A report of even a higher prevalence of anosmia among workers ex-posed to cadmium appeared four years later. Potts84 reported that 64% of70 workers exposed to cadmium dust (.6-236 mg/m3 of air) in a sectionof a battery factory for 10 to 40 years were anosmic. Unfortunately, no de-scription was made in this study as to whether or how the smell testingwas carried out.
Three studies have appeared on this topic in the more modern era. Inthe first of these studies, Yin-Zeng et aP18 found that 28% of individualswho had worked five years or more in a cadmium-refining plant reportedhaving anosmia. No olfactory measures were apparently taken. The aver-age concentration of airborne cadmium was said to be comparatively low(between 0.004 and 0.187 mg/m3), but still slightly above the current Oc-cupational Safety and Health Administration Permissible Exposure Limitof 0.005 mg/m3 to which a worker may be exposed. In the second of thesestudies, Rose et al91 administered a butanol odor detection threshold testand an odor discrimination test to 55 workers exposed for an averageof 12 years to cadmium fumes (from brazing refrigerator coils). Airbornecadmium, measured for the first time 13 years after production began,was 0.300 mg/m3. Workers with the highest body burden of cadmium,as measured by urinalysis, exhibited moderate to severe hyposmia, butnot anosmia, on the detection threshold task, but performed normally onthe odor discrimination task. These observations led the authors to thequestionable conclusion that only peripheral, and not central, elements ofthe olfactory pathway were damaged. In the third study, Sulkowski et al93
560 DOrY & HASTINGS
compared the olfactory function of 73 workers involved in the productionof cadmium-nickel batteries to that of 43 nonexposed, age- and smoking-matched controls. Anosmia or hyposmia was found in 45.2% of the exposedgroup and in 4.6% of the controls. Unfortunately, the Elsberg blast injectionprocedure was used to assess olfactory function. This procedure has beencriticized on numerous grounds, including (1) the lack of a forced-choiceresponse (which results in artificially elevated threshold values), (2) theconfounding of pressure with the number of molecules in the stimulus,(3) the introduction of a very unnatural stimulus pulse into the nose, and(4) the production of unreliable threshold measures.58,114 Despite its short-comings, however, this study is in accord with earlier ones in implyingthat, even at low concentrations, cadmium exposure can result in loss ofsmell function.
Chromium
Like cadmium, chromium is often used with nickel and other metals inindustrial situations, most notably in the manufacture of high-quality steelalloys. Unlike cadmium, there has been relatively little research about theeffects of chromium on the ability to smell, even though this metal has longbeen suspected as having an adverse influence. Watanabe and Fukuchil12examined odor detection and recognition thresholds of 26 male and 7 fe-male employees of a chromate-producing factory who had worked therefor at least seven years. Over half of the subjects (51.4%) were noted as hav-ing perforated nasal septa; 54.5% exhibited elevated smell thresholds to thefive odorants evaluated (phenyl ethanol, cyclopentenolone, isovaleric acid,r -undecalactone, scatol) , with two reportedly being anosmic. Although thedegree of olfactory function was not related to the presence of the septalperforations, it was related to the duration of employment in the factory.
Mercury
Although mercury exposure occurs in a number of industrial opera-tions and reportedly produces olfactory deficits, like chromium, the data insupport of this contention are limited. In fact, the sole empirical study usedpatients (mean age, 79 years) suffering from Minamata disease developedthrough exposure to in utero mercury. The patients and controls were ad-ministered the UPSIT25 and an odor detection threshold test using phenylethyl alcohol.44 The patients with Minamata disease exhibited greater age-related declines in both threshold sensitivity and UPSIT scores than didage-matched controls. In an autopsy study of patients with chronic Mina-mata disease, damage to the olfactory bulb and tract was found, althoughno obvious changes in ~he nasal epithelium were observed.44 Whether this

561NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
is because the mercury exposure was due to ingestion and not inhalationis unknown.
Lead
Inorganic and organic lead can alter CNS neurotransmitters and canproduce transient or possibly permanent difficulties in attention or con-centration, manual dexterity, memory, visuoconstruction, psychologicalwell-being, and psychomotor speed and accuracy. Whether and to whatdegree this metal alters the ability to smell is not clear, although the avail-able evidence suggests that occupational exposure to lead has only minoreffects, if any. Surprisingly, no studies are available on children who havebeen exposed to lead, despite the fact that the pediatric population is moresensitive to neurotoxic effects of exposure to low levels of lead.
Schwartz et a197 administered the UPSIT, along with several neuropsy-chological tests, to 222 employees of a tetraethyllead manufacturing plant.The testing was performed on site, prior to or in place of a work shift, tominimize any possible acute toxic effects and to reduce work-related fa-tigue. Industrial hygiene sampling data were available, and duration ofexposure to lead was estimated from personnel records and from detailedoccupational histories compiled by trained occupational medicine physi-cians. In this subject population, organolead production peaked in the late1960s and early 1970s, and urine lead levels showed an upward trend from1965 through 1985, followed by a decline. Mean differences in the test scoreswere estimated by comparing the average scores of the moderate, high, andhighest exposure groups to those of the low exposure (reference) group andby adjusting for the confounding influences of age, intellectual ability, race,and alcohol consumption. No influence of lead on UPSIT scores was ap-parent, even though lead exposure was associated with decrements in aseveral the neuropsychological measures.
Subsequently, Bolla et arl compared UPSIT data from a subset(n = 190) of the aforementioned lead-exposed subjects to those from 144solvent-exposed workers and 52 reference subjects who had been adminis-tered the same set of sensory and neuropsychological tests. Again, the over-all results showed that, after adjusting for confounding variables such asage, vocabulary score, and race, the UPSIT scores of lead-exposed workersdid not differ significantly from those of the reference group (respectivemean scores, 36.4 and 36.9). However, when the lead-exposed workerswere divided into exposure durations of less than 11 years, 11 to 17 years,and more than 17 years, significantly lower UPSIT scores were noted rel-ative to the reference group, for the 11 to 17-year exposure group, but notfor the other two groups. This effect was apparently not viewed by the au-thors as meaningful, as they state in the conclusion of the article, "Olfactoryfunction was. ..unaffect~d by lead exposure".ll
562 DOTY & HASTINGS
Solvents
Workers in many occupations, including painting and paint manu-facturing, lumber and furniture fabrication, machining operations, equip-ment cleaning and degreasing, and floor and carpet laying, are exposedover time to significant levels of solvents, such as acetone, methyl ethylketone, and tetrahydrochloride, often in closed quarters. Evidence thatexposure to such solvents may influence smell ability ranges from self-reported disturbances of smell function in floor-layer workers exposed tohigh levels of toluene to sophisticated case-control studies of long-termexposure to solvents in manufacturing plants. Because of their lipophili-city, solvents can readily cross the nasal mucosa and penetrate underlyingcellular membranes. Such agents can also enter the bloodstream throughthe nasal capillaries and can cross the blood-brain barrier, producing inextreme cases (e.g., in chronic glue sniffers), atrophy of central brain struc-tures (e.g., frontal lobes, cerebellum).52
Ahlstrom et a13 found that fuel oil tank cleaners exhibit higher detec-tion thresholds for n-butanol and fuel oil vapors than controls, whereasthis was not the case for pyridine and dimethyl disulfide. The elevatedthresholds, however, did not fall outside of the normal range. The authorsnoted, for all stimuli evaluated, that the workers exhibited relatively nor-mal perception of strong stimuli, but impaired perception of weak stimuli.The largest decrement was found for detection of fuel oil vapor. This ob-servation is in accord with the concept of "industrial anosmia," whereexposure to strong odors in the workplace results in a reduction in sen-sitivity that is confined to those particular odors. Such effects may reflectlong-term adaptation because, unlike the effects resulting from exposureto toxic metals, they are typically reversible, disappearing after a workeris removed for a period from the exposure area.
Schwartz et a199 evaluated the effects of chronic, low-level solvent ex-posure on olfactory function in 187 workers at a paint formulation plant.As in their lead exposure research, industrial hygiene sampling data anddetailed occupational history data from personnel records were used. Asignificant dose-related adverse effect of solvent exposure on UPSIT scoreswas documented, but only in never-smokers.
Recently, Mergler and Beauvais7° examined detection thresholds fortoluene and phenyl ethyl methyl ethyl carbinol in five volunteers whowere experimentally exposed for seven-hour periods to either toluene,xylene, or a mixture of these two agents in an order counterbalanced usingLatin squares. A sixfold shift in the detection threshold for toluene wasfound immediately after exposure to toluene, xylene, or their mixture. Nodifferences were found in phenyl ethyl methyl ethyl carbinol thresholdsafter exposure to any of the compounds. Because the alterations in olfactoryfunction were reversi~le, the shift in detection threshold is again likely

NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT 563
caused by odor adaptation, rather than by direct toxic insult to the olfactoryreceptor neurons.
In contrast to the aforementioned studies, Sandmark et a194 found nolong-term influences of solvent exposure on smell function in a group of54 painters exposed to organic solvents relative to 42 unexposed controls.When the confounding influences of age and smoking habits were con-trolled for, no differences in UPSIT or pyridine threshold test scores werenoted between the two groups. The lack of an effect was attributed to thelow-to-moderate degree of exposure to the solvents.
Irritant Gases
Numerous empirical studies report olfactory deficits after accidentalexposure to high concentrations of irritant gases. Such irritants as ozoneand formaldehyde are common components of both indoor and outdoorpollution, combustion products in tobacco smoke, and exhaust from auto-mobile and other internal combustion engines. Although chronic exposureto low levels of irritative airborne contaminants occur in a number of neigh-borhoods and workplaces, it does not necessarily follow that nasal irrita-tion, per se, translates into loss of olfactory function. Indeed, some nasalirritants have no clear smell. Nonetheless, one would expect an associationbetween an odorant's irritative properties and its propensity to alter smellfunction if continued irritation of the mucosa leads to necrosis and otherproblems. Furthermore, a large animal literature (mainly rodent) supportsthe idea that chronic exposure to several irritants can, at higher concentra-tions, damage the olfactory epithelia.
Formaldehyde, an ubiquitous and highly reactive gas, is used in avariety of manufacturing processes and in biology classes, hospital anduniversity histology departments, mortuaries, and other situations wherepreservation or fixing of tissue is required. This gas is absorbed mainly inthe nose. Although exposure to formaldehyde is often alleged to decreaseolfactory acuity!03 only two human studies have reported an adverse ef-fect of this agent on the ability to smell. In the first, workers exposed to0.075 to 0.750 ppm formaldehyde (alone or in combination with wooddust) showed a slight but significant elevation in detection thresholds (se-rial dilutions of pyridine) when compared to controls (14.2 vs 15.6).5 In thesecond, a questionnaire administered to histology technicians regularlyexposed to 0.200 to 1.900 ppm formaldehyde revealed that 68% reporteddecreased odor perception. Only 9% of the control group did SO.60
In the most extensive systematic investigation of toxic chemicalson the human ability to smell to date, Schwartz et al98 administered theUPSIT to 731 chemical workers exposed to acrylic acid and a variety ofacrylates and methacryl~tes at levels typically below their threshold limit
564 DOTY & HASTINGS
values. Although analysis of the cross-sectional data revealed no rela-tionship between chemical exposure and olfactory deficits, a nested case-control study designed to examine cumulative effects of exposure uncov-ered several associations: (1) olfactory function decreased with increasedcumulative exposure; (2) the effects appeared to be reversible; and (3) thehighest relative risk of olfactory dysfunction occurred in workers who hadnever smoked. The similarity of the latter phenomenon to that found in thepreviously mentioned solvent study illustrates how ancillary factors candetermine the expression of the olfactory toxicity of some compounds.
Recently, Dalton et a12° investigated whether occupational exposure tostyrene altered smell function. Exposure histories were reconstructed usingindustrial hygiene data, and the workers were tested using a battery of ol-factory tests, including tests of odor identification ability, detection thresh-old sensitivity to phenyl ethyl alcohol and styrene, and retronasal odor per-ception. No significant differences were found between exposed workersand matched controls on any of the tests, except for the styrene thresholds,which were significantly elevated in the workers. The latter phenomenonwas interpreted as being caused by exposure-induced adaptation.
Workplace exposure to several irritants that are major componentsof air pollution has also been associated with loss of olfactory function.Harada et aP9 reported that exposure to sulfur dioxide and ammonia pro-duced an elevation in odor detection thresholds for five substances thatwere evaluated. Several of these workers complained of olfactory dys-function. Similarly, repeated exposure of human volunteers to 0.4 ppb ofozone for four hours per day for four days produced initial elevations indetection thresholds to butanol that returned to normal soon after cessationof the exposure.85
CHEMICAL EXPOSURE AND THE MULTIPLECHEMICAL SENSITIVITY SYNDROME
There are proponents of the notion that a wide variety of somaticsymptoms, including hypersensitivity to odors, depression, anxiety, fa-tigue, general malaise, mental confusion, lightheadedness, headache, in-somnia, myalgia, loss of appetite, and numbness, can be elicited by singleor multiple exposures to extremely low concentrations of several com-mon household or industrial chemicals. Such symptoms occur withoutdocumentable signs of medical disease.92 This unorthodox complex of ap-parent chemically induced symptoms was first termed "environmentalillness" or "chemical reactivity" by Randolph in the 1960s.86 Cullen19 sub-sequently termed this complex of chemically induced symptoms multi-ple chemical sensitivities (MCs) and developed an operational case def-inition of the disorder.1~ Cullen confined the definition to a subgroup of
565NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
"environmentally sensitive" patients and set seven criteria for its defini-tion: (1) some documentable environmental exposure(s), illness(es) or in-sult(s) were coincident with the onset of the problem; (2) the symptoms areassociated with more than one organ system; (3) the symptoms recur andabate in response to predictable stimuli; (4) the symptoms are elicited bychemicals of diverse classes and toxicologic modes of action; (5) the symp-toms are elicited by exposures that are demonstrable (albeit of low level);(6) the symptoms cannot be explained by a single, widely available testof organ system function; and (7) exposures that elicit symptoms are verylow-"(i.e., many standard deviations below "average" exposures knownto cause adverse human response. ..generally lower than 1% of the es-tablished threshold limit values for toxicity)." Some of the agents thathave been reported to induce these symptoms include perfumes, drugs,organic solvents, combustion exhausts, soaps, insecticides, preservatives,cigarette smoke, fragrances, perfumes, and colognes.
Although not all patients with the putative MCS syndrome reportheightened smell sensitivity, enough have done so to catalyze two empiri-cal studies on this topic. In both cases, no evidence of altered odor detectionthreshold sensitivity was found. In the first, the detection threshold valuesof 18 patients with putative MCS did not differ significantly from thoseof matched controls for the solvent methyl ethyl ketone and the rose-likesmelling agent phenyl ethyl alcohol.27 In the second, detection thresholdsof 23 MCS subjects and 23 controls to phenyl ethyl alcohol also did not dif-fer from one another.54 Paradoxically, in the latter study, the MCS subjectswere inferior to normal controls in identifying and discriminating amongsuprathreshold odors and exhibited smaller odor-induced event-relatedpotentials. Assuming the validity of these findings, this study implies thatthe suprathreshold olfactory function of MCS patients is decreased, notincreased.
MECHANISMS OF TOXIN-INDUCED OLFACTORY LOSS
It should be noted that many chemicals potentially damaging to theolfactory system activate intranasal protective reflexes, mainly through thetrigeminal nerve, that minimize their penetration into the nasal passages.**
**It is noteworthy that the reflexive depression in respiratory rate induced by exposureto a sensory irritant (which is mainly caused by stimulation of intranasal or pharyngealtrigeminal afferents) has been used extensively in the establishment of the OSHA PermissibleExposure Limit (PELs) and the American Conference of Governmental Industrial Hygienist's(ACGIH) Threshold Limit Values (TLVs). Indeed, exposure limits for approximately onethird of the compounds regulated by OSHA have been based, at least in part, on their irritantproperties. For a new irritative compound, the concentration at which it depresses respiratoryrate by 50% is typically first established (RDso). A value of 0.03 X RDso is then calculated; formany compounds, this value has been found to be very close to the established TLV.

566 OOTY & HASnNGS
Such reflexive mechanisms include rejection responses (e.g., sneezing, halt-ing of inhalation}, increased engorgement of the erectile tissue in the nasalpassages, and increased mucus secretion. Unfortunately, although suchmechanisms reduce exposure to irritating chemicals to some degree, theydo not always protect the olfactory system from inhaled chemicals, partic-ularly ones that do not active trigeminal nerve afferents or are present ona chronic basis.
Animal studies suggest that the primary means by which chemicalsalter olfactory function is by direct interaction with the olfactory epithe-lium, where they damage the olfactory receptors and associated cells.Agents such as dimethylamine and 3-methylfuran damage the epitheliumindirectly by producing metabolic byproducts that, in turn, damage themucosa}2 The speed by which restoration occurs after the sloughing off ofthe epithelium depends on the concentration and species of the chemicalsinvolved. For some substances, restoration occurs in a few weeks, whereasfor others it can take months. In general, the degree of reconstitution de-pends on the degree of insult; poor reconstitution is expected when thelamina propria and Bowman's glands become heavily damaged.l°B
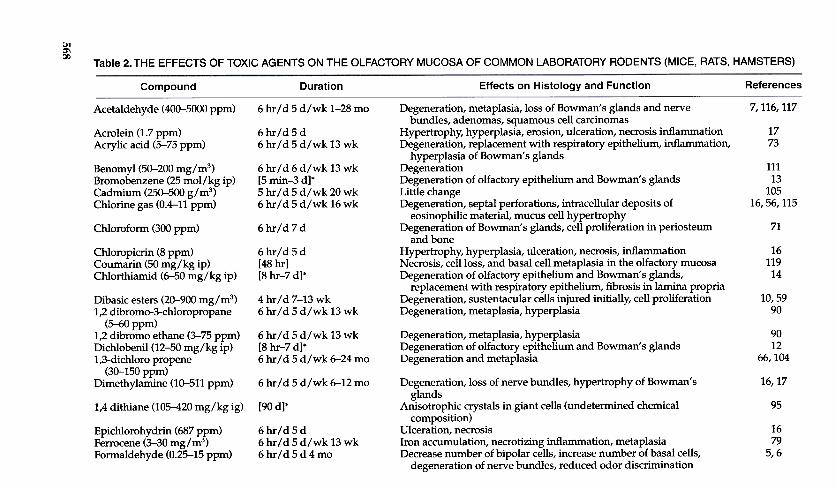
As shown in Table 2, a variety of exogenous agents damage the ol-factory membrane of rodents. Unfortunately, the degree to which suchdata generalize to humans is not known. Although olfactory epithelialtissue can be obtained in living humans via endoscopic spot biopsy, thereare sampling issues involved, and no such study has been performed intoxin-exposed human populations. Furthermore, no cadaver study hasyet been performed in such groups. Rodents, in addition to being obli-gate nose breathers, possess maxillary turbinates and an additional rowof ethmoidal turbinates, resulting in a more complex distribution of air-flow patterns and nasal absorption distribution of chemicals than seen inhumans.
The limited data available suggest that the rodent olfactory epitheliummay be more resilient than the human olfactory epithelium to toxic damagefrom some agents, perhaps reflecting differences in xenobiotic metabolism.In one study, for example, adult male rats were exposed to relatively highlevels of airborne cadmium (0.500 mg/m3} for 20 weeks.l0S Unlike the sit-uation with humans, no evidence of pathologic alterations of either theolfactory or nasal respiratory epithelia was present, and behavioral testswere unable to document any cadmium-related adverse effect on detectionthreshold sensitivity. This is in spite of the fact that lung and cardiac tox-icity were found. Although similar rodent studies (using nickel andchromium} have found nickel-related damage to the olfactory epithelium,behavioral deficits were not observed.39
The nasal and olfactory mucosa possess several chemical defensemechanisms in addition to those mentioned to thwart invasion of
567NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
xenobiotic and pathogenic agents. For example, they are capable of secret-ing antibodies and antimicrobial proteins, such as lactoferrin and lysozymeto deal with inhaled pathogens.69 The nasal passages are also protected bythe presence of phase I and phase II enzymes (i.e., cytochrome P-450s, glu-tathione, and related enzymes) found in concentrations that can be greateron a per gram basis than in the liver or lungs.88 The source of such agents inthe olfactory epithelium is the supporting cells and the Bowman's glands,ensuring their presence in the mucus of the region. In some cases, chronicexposure to low doses of toxic compounds induces an enzymatic metabolicprotective status so that subsequent higher exposures produce little or no
toxicity.Some olfactory toxicants produce acute or chronic inflammation that,
in addition to limiting airflow to the olfactory region or inducing metabolictoxins in the epithelium, can ultimately damage the epithelium. Such in-flammation can also decrease upper airway immunoglobulin A, therebyallowing for colonization of the olfactory mucosa with pathologic bacteriathat can have adverse effects on the mucosa. In rare cases, volatile chemi-cals can increase mucosal cellular proliferation that can lead to neoplasticprocesses that themselves can alter the ability to smell. Increased preva-lence of nasal and sinus carcinomas have been noted in workers exposedto nickel dust, ionizing radiation, wood dust, formaldehyde, and leatherdust.64
Toxic effects of airborne chemicals on the olfactory neuroepithe-lium can result from the synergism of several factors. For example, be-cause of weakened defense mechanisms, concurrent exposure to a toxiccompound during an upper respiratory infection may result in muchgreater damage than exposure to either alone.48,89 Conversely, cigarettesmoking may protect against solvent-induced olfactory deficits ofchemical workers.2,98 Estrogens and some other hormones may mitigateolfactory epithelial damage produced by neurotoxins such as 3-methylindole.Z2
Attempts to ameliorate the dysfunction resulting from exposure totoxic compounds are limited. In some instances, inhibition of enzymaticpathways that produce toxins can eliminate the damaging effects of suchchemicals as dimethylamine and 3-methylfuran.88 Topical steroids, whichare routinely used for alleviation of rhinitis and polyposis, may do morethan to simply increase airway patency by shrinking inflamed tissue. Thus,they may hasten the reconstitution of the olfactory epithelium after insult,61although large doses may have an adverse effect.62 As we increase ourunderstanding of the factors that regulate neurogenesis and apoptosis inthe olfactory epithelium, and of the factors involved in the guidance ofaxonal propagation through the cribriform plate, new therapeutic avenueswill undoubtedly present themselves.
568 Ci)'
a:w1-U)
~«:I:
ui~a:wu~~zwQ~~0~a:O[]J«-lzO~~Ouu.O«U
)Ou::J~~~u11-lOw:I:1-ZOU
)1-Zw~U§t"-u.O~Uwu.u.ww:I:I-NQ
):c~
~.2u~~LL"C~m>01OO-;;;
:1:~O1/1UQ
)~W U
)G
JC
JcG
J...G
J"G
ia:"0c~oc.Eo() c:o~:1c
osOC
>
CjI
~,~l!)~,:a\0
t...
......-0 t...r')
t...
...t...'
~
~
Cf)
'""'
~,
'0'0
It)lt)
'0'0"~
~"""
~
~~
~
~
~
('10\c-N
-
~
~~
~
* ~
~
~
~~
~~
\C'?Lr)Lr)
~5
~~
~S
~~
\C~
Lr)\C
I!)
CI")I!)
, O
~
r...
I!)~'
s :&
2: ~
~~
~"'
"' "'
0 ~
E
'EI:;
~
g, 'bo]'bo2:
SI
~p,
"' 0::::
p,0
"'U)
1:;U)01
p,~
I:;t-..
O~
lI)~
0~
2:~
~
QJc:!,O
0
QJ
~
I~u)~
~
'0 t-..'O
O
QJN
~
~E
6.d
!!} ~
~
bI)
t:
QJ
s"'
>,~
§QJ
O'0
.u -..~
,...
-~
;:=
E
° .~
.t:
e-k1
°ti' gE
.eo °
~
~
QJe",:a
:a~
~uu
u "1jr,.."1j
:d\0
\QO
\~
~
~
(1"}
~~~
~
(1"},
'tj ~
'7'tj
If) 'tj
Klf)
'tj~t-..
'tj'tj
'~]
"
~~
OO
~
~
\C~
~
~\C
0\If)O,0\O
':!'aN
a I:-.
~
Lr)\0'
'C'
~
'Co o
~
s s
~~
~
N
~
N
,...~
J
J ~
o
~
~
~
~.§
, ,
, ,~
~~
~
~
~~
~l1")~
l1") l1")
l1")l1")l1")~
t-.~
~
* ~
~~
,], ,
::0' "'
~~
~
~
~
~~
~~
~~
~
~
~
~~
~'
~~
0
...O
-.c ~
...
..0 ~
8
"' P
. ~
~
S
;3 8
8 .9
Q)
Ss
2 :3
P.~
>
S~
~
~
S
,~~
I.. ~
-=
"'
.~
0 >
.. "'§
'"" "'
Q)
-=
~
"Ij ,...
c I..
."Ij .~
"Ij
~
~
.~
~
0 Q
) ~
0
~
0 ~
-.~
, ~
"'
P.
~~
~
"'
~v
""" ~
u--P
. -
~
.~
~
bI) .~
...~
bI)
"' bI)
~
"' :3
"' "' 0
.~
~
"' .~
~
"'
"' o~
'
~
~
~
0' "'
Q)
,"Ij
...Q)
~
...0 -=
~
.~
U
~
~
"' ~
-:5
~
~
..0 .=
~
~
~
~
~
~~
~.s.
S
...E~
,
s...~
s'bo
s ~
' Q
) ~
.!S
P
.~
.~
.=
~
@
..§ ~
~
.s -.8
t:" ~
:§
.§ e
8 .m
~
s'
:5 ~
~~
~.8
"Ij ~
~P
. ~
~"Ij:3"1j
"IjS
~Q
)~
~
P.
~-~
~~
~
~
u ~
.=
~
~
~
~
' g.
~
Q)
;3 .~
.~
~
0 ~
:3
P.
S
"' ..:
U
~
8 ..:
.~
"' "'
8~
~
'
~
"' :3
.~
~
"" .0
~
;3 .~
.S
.!S
.!S
;3
~
..."Ij ~
ri;
Q) "Ij
:P
~
~
P.
P.
'"".~"0
~
.9 ..:
5 ~
~
u
~
~
~
~
~~
~
~
~~
",0"' ~
";oJ
o",~
Q)Q
)...I..Q)P
. p
"' "'
8 .~
bI)
.~
..0 :3 ";:'~
~
u
.~
0 U
~
~
.~
~
O~
Q);>
P
. ~
u~
:3-P
~
~p..~
-~
,"' Q
) ...:3
"' ~
Q
) ~
~
Q
) "'
':3 '~
~
0
"', '",
...~
' ,
~.~
O
'.m
~
~
t:" 't
~,
§ .m
.l.
t:".s. u
.~
.~
t:"'E.
"'"'~~
S
0 Q
)-S
~
o",~"'
"'o~~
"fl. ~
~
~
~
.::::.i3
~
~
] ~
~
=
~
~
~
~
$SQ
).!S°
~
$20 Q
)~~
..:2~
~~
~Q
) 0
P.
P.~
0
P.
~
~
~
.;; 0
.~
~
"'Qj
"'Qj 0
"Ij
S~
E~
"0 "0
~~
"0 ..:~
"0~"'s
s"0§,
'~
,u ,
, ,
~
"Ij ~
~
.~
~
~
Q
) ~
.~
~
~
- ~
~
~
~
~
~
~
O~
..:°"'OO
b1)o~O
..:~
0Q)00
000..0
.;; P
. -.c
.!S
..0 -.c
~
..0 ..:
..0 Q
) P
. u
..0 S
-.c
..0 -.c
..0 ..0
~Q
)0~,""~
~~
~P
.0
~~
0~,",~
Q)~
~
~~
~~
,
Q)
"Ij fj
Q)
Q)
Q)
Q)
-5 Q
) "'
Q)
.r, .~
Q
) ~
Q
) Q
) Q
) Q
) Q
)
~§
...~
P.
~
~
~
.~
~
"Ij 0
~
-~
~
~
~
~Q
) Q
)~
Q) ~
Q) Q
) Q) Q
) ~ Q
) ~ Q
)~
...Q)
P.Q
) Q
) Q
) Q
) Q
)bI)
~
bI) ~
bI)
bI) -=
bI)
<!J
bI) ~
~
bI)
~
bI) bI)
bI) bI)
bI)Q
)- Q
)...Q)Q
) Q
) Q
) -Q
) Q
)Q)
Q)Q
)Q)
a ~
a aa~
a a
~za
aa aaa
-c0\-c...r...
,In
,"' ",'
~
~
~!0
Q)O
., -U
..p
~
!0 -!0
~
.~
!0 ~
§o
S
.~
!0 .
~
Q)
"'.0-~
~
-..:
0 u
-Ou
>,
~
19 k .~
~
Q)
Q)Q
)~g.
.§ S
~
S
h ~
~
'~~
~
Q)
.0 ~
0
~
] 1~
1gj
~
!o~~
-"' -=
.~
~
~
~
~
' ,
~
Q)
.~
"' "'
;j u
bO~
~.0
"E
.S
u -g
Q)
!0 N
k..t:
.5b :c.!S
;j
Q)
00.0~
.S
t:
.9- ~
-"' Q
).0..0
~
",~-Q
)"'
~
'0 ~
~
"' ~
~k-
-t:' ~
k
..8 Q
) 0
~'
U~
~!0.0~
.0 :E
..g
~
"E
S
..g
~
p..~
~'
§9
~k"'
00 Q
)~
].§P.".P
~
~
Q)!0~
S~
~~
';'0bO
"bo.a
0 Q
) ~
t:
Q)
Q)
U~
OQ
)~Q
<
O
-J~Q
~
~
'?: 'bO
P..
"' ~
~
~
.~
~
.~
s ~
P
...&
s bI)
~
sbI)
!U
P..bI)
P..
~
s P
..~
~
bl)P..
l!)~
P..
bI) ,",~
P..
P..';:;,
se t
" ~
l!).~
~
P
.. ~
bI)
~
~
'?:~s
80 ~
SQ
J '?
0 ~
~
~
0 0\
...QJ
~
0 N
\0
bl)NP
.. ';:;,l!) I
~
~
~
~
l' ~
S
o
p..~J
0... !U
I ~
~
~
~
00 S
~
f::!
y £
N
e S
~
0
..: ~
Q
J~
0
"1j "'
M
~
QJ ~
P
.. P
.. .=
~
"1j ~
"1j
.S
~
.=
~
6 S
0
~
0 P
.. =
QJ
E~
E
U
~
=
~
s P
.. s .~
5
0 ~
~
0
QJ Q
J.~
..:
.:s Q
J 0 P
.. 0 Q
J -l!) >
, .~
...~
"1j
P..!U
..; U
...o D
..; ;
...oQJ-
06... .~
.D'9.D
OU
I "'U
!U8a5
~:a~
:a~:a~
QJ
:a ~
gE~
0
~
;g N
~
N
.~
~
~
.§
"" .s.
QJ 0
UU
U
~
' 'Q
'
Q
' ~
~~
'""~Nl!)~,~l!)~,~t-.
C1)'
"1j C
1)~
'tJ
~
~;;
bO
3"1jC
1) ~
,...
's:: ~
oIU
IU
S
.s:. .~
~
ai~O
~
JS~
O
~,...
tJ~O
IU
C
1)
~
~
;;O
OO
.~
SIU
"0-
...IU
,"~
..:
.~
&alp.~
C1)
bOO
- 'IU
ai ...p.
!!J .~
"1jp.JSai~
C1)' IU
ai ~-
~
.5 S
e
~U
S
~
"1j p.
~~
.SalE
o ~
IU
.5 C
1)~
.;;; .=
"iC e
~~
~E
;;"O
.E~
~s
u"1j O
,
§.E~
:P~
.~
C1) IU
~..g
lUai~
IU
~..
...
~~
glU~
.~
~
~
t.:: ai
~>
'~~
bOC
1) U
~
.~
ai
Q
r./') Q
~~""'
N~
~N,...
~"0I/)"0~'-0
~~
t-..0'-0It")~
,...000
~
~r'"J
~
~
'"' ~
~
0. ,
,~
'1j
'1j
I '1j
.
\D
~
~
Ir)
'1j1r) '1j
'1j ~
'1j
,.!, ,0
~
,
~~
~
~~
~
~
~
~
N-
\D
00C')
000-
\0C')
"''I::
:6 8
.d ~
ca o
~
"' ~
,ca
CI)
R
.~
~..:
~
~.A
Q
J Q
J~
'0""0
0~
"'
~
~2e
-:uC
I) o"'~
-!:-
-0.~
~
"'
.~ca..:;j",
"'Q
J ..:
~
0 .~
8
"' Q
J...QJu
uca
.Aca",~
Q
J
~
QJ'-:S
~
~
~
u ~
"'
' V
'~
.~
~
- -;;,
.~
"' ca
~
ca ..
",' 0
..0 ..~
QJ
~
~
.~
0 "'
.~
"':a
ca .~
QJ >
e
§U
~;§~
ca
'O>
caQJ
..:
.A
~
QJ
,.A
'0
~
ca"'~>
. ~
° ~~
~0..:
caU
o..P
' Q
JQ
J .A
O
u'"'5
'0 e
~
b .~
",.. e
~
~
~
~~
Q
J~~
00 000P
'0t>..
..p :c
..p :c
..p >
.:c .~
.caca~
cacaca..:cau~
~>
<>
.Q
JQJQ
JQJQ
JQJ:=
QJo
..:~
~
0~
~
~
::
~
~Q
J Q
J Q
J Q
J Q
J ,"
QJ
0 ..,
Cl)C
I)~C
I)CI)C
I)"boCl)
8Q
JQJ
QJQ
JQJ
QJ>
. Q
Q
Q
QU
<
O\t...
~oo
"0~".peQ)
"'~Ou\CI~
~N
"O
"0
00"0('1
('1,
,!.:a
:a ..:
\C.:e.
.:e.
1;:;
"' "'
'U
'U=
=
III III
"bo "bo
"' "'
'=
'=III
III
Q) ~
~
=
O
O.~
~
~
""U
'UO
=
=
e III
III
~
8 S
=;3
:3.~
;:=
;:=
Q)Q
) Q
)"'..::
.c111
...Q
) .~
.~..0.
0.U
Q)
Q)
~~
~
='
O
0ot
t.~
III
III~
~O
o
~-
-..O
O
Q)
=
=
~O
O
'U
-.0 ..p
III III
~..
..
..:: ~
~
O.Q
) Q
)P
oo 00
.tj Q
) Q
)
<00
"'OO
N~
'-0r')
"' 00
, '-0
"'"0§"bo>
.
"'...,
p.
§.§~e"..§~
Q
J "'
o~t
~...~
"O,Q
J~
",bCQ
JE
"'~"0
~e,.:
,
;.:=;jQ
J~Q
J ;.:=
>...§
...QJ...",
.~~
§
~
~
~:g
ro
00;3'='tJ'tJ
tJ .S
"' "'
"' ,
""""QJ",
--"0 ...
00 "8
"""""'"0
0 e
u
~~
~Q
J~000"0
:P
:P
..c Q
J ~
'"'
"' "'
..'0
" "
" v,
QJ
QJ
QJ
c~
~~
'8~Q
JQJQ
J~~
bCbC
bCu~
oooz5
~
~I!)~,]
*\O
~
';:0'~
~'O
I!) o
""I!) ~
0\
~,),
I :E
.' ,),
~.J:;]N
] .J:;
""\0 t-..\0
~ 'r;-0>"-8!I:"''I:;i~~u~]~
'O".0~QJ
~00QJ
Q
:::; '2
.;;""' ~
~Q
J ,
~
~
~s~
-P
, ~
~
~
Q
Jg;
~
~Q
J s~
g;
'boQJ
g; [Q
J ;§
~
0 >
, s]
P'N
tf)
~
S .S
~
p,
.t:S
Ln
~
p,.~
~
P'N
~
'
P,
Ln ~
Ln ~
r... !tS
>
,P
, N
"'
P, ~
P
'o tf)
P,~
.~
tf)
E
~ ~
I '2 ~
~
P
,~
I."
0 .~ O
I
.~ ~
bO
~
:A," ~
..P
,O
~
~
,...N
..!. '2
o .~
bO
N
~
bO Q
J ~
"'~
>
, P
,:a .~
P
, ~
I F
:i' 0
~
~
~
Ln ...~
~
~
~
,
QJ ~
...:
.~
.~
bO~
P
,- O
O
-
o O
Q
Jp,~8,~
dQJ'~
bO
:O'C
"'Qj:ffo~
~~
'bod.~
>'s
J: .g
j .r::D
.t
s.e ~
:g
S
~
S :§
S
2!, .§ 'bo ~
S
.x l'
S ~
;;3
1 g;
~
:g E
~
QJ -g
8 8
~
.~
8 ~
~
§
:P. 0C
1 ~ 1
S
'i'- o ~
~
d .g
~
S
o 0\
-;a -;a
"'Qj ~
.~
.S 'f
.0 >
, R
'f .~
~
'"I
~
'"I ~
"'
0 ~
0
~
QJ 8:a
QJ ~
~
~
..8 S
° !tS
S 6
>,..:
..: 6
>,J§
0 0
~
E
'"I -S
.1;
E
...;j I
] '§
~
~
R
~
§ ':§
~
~
g':§ ~
~
~
9 ~
.~
§
.~
8 ~
t r... ~
~
~
~
9
~
~
~
~~
~
~~
~
Z
Z
ZZ
Z
~
~~
~N
' ~
0)u~.."'~§~~;!:
1"'Qj
..§~..~0.~..8
569

570 DOTY & HASTINGS
CONCLUSIONS
Although the bulk of evidence suggests that toxic chemicals influ-ence human olfactory function by damaging the olfactory neuroepithe-lium, there is a dearth of information as to of whether solvents and otheragents adversely influence central olfactory structures. Clearly, studies ofthe toxic effects of airborne agents on the human olfactory system are stillin their infancy, and no human biopsy or cadaver studies of even the olfac-tory epithelium of chemically exposed humans have been made. Although,at face value, the available data suggest that most industrial chemicalsdo not damage the olfactory membrane at concentrations below currentthreshold limit values,98 few epidemiologic studies on this point have beenperformed, and longitudinal data are completely lacking. As noted at thebeginning of this article, the olfactory epithelium undergoes metaplasticchanges throughout life, and the degree to which exposure to even lowlevels of airborne toxins contributes to such changes is not known. Fu-ture studies are needed to establish how generalizable rodent data are tothe human condition and whether the human olfactory system is, in fact,cumulatively damaged by intermittent exposure to environmental toxicchemicals.
ACKNOWLEDGMENT
Supported, in part, by Grants POI DC 00161, ROl DC 04278, ROl DC 02974, and ROlAG 27496 from the National Institutes of Health, Bethesda, MD (RLD).
References
1. Adams RG, Crabtree N: Anosmia in alkaline battery workers. Br J Indust Med 18:216,1961
2. Ahlstrom R, Berglund B, Berglund U, et al: Impaired odor perception in tank cleaners.Scand J Work Environ Health 12:574, 1986
3. Amoore JE: Effects of chemical exposure on olfaction in humans. In Barrow CD (ed):Toxicology of the Nasal Passages. Washington, D C, Hemisphere Publishing, 1986, p 155
4. Amoore JE, OIlman BG: Practical test kits for quantitatively evaluating the sense of smell.Rhinology 21:49, 1983
5. Apfelbach R: Sensitivity to odors in Wistar rats is reduced after low-Ievel formaldehyde-gas exposure. Naturwissenschaften 78:221, 1991
6. Apfelbach R, Reibenspies M, Schmidt RW, et al: Behavioral and structural modificationsin the olfactory epithelium after low level formaldehyde-gas exposure. In Proceedings ofthe 3rd International Conference on Role of Formaldehyde in Biological Systems. Methy-lation and Demethylation Processes. Hungarian Biochemical Society, Sopron, Hungary,1992
7. Appelman LM, Woutersen RA, Feron VJ: Inhalation toxicity of acetaldehyde in rats. I.Acute and subacute studies. Toxicology 23:293, 1982
8. Baader EW: Chronic cadmium poisoning. Indust Med Surg 21:427, 19529. Bhatnagar KP, Meisami E: Vomeronasal organ in bats and primates: Extremes of struc-
tural variability and its phylogenetic implications. Microsc Res Tech 43:465, 1998

571NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
10. Bogdanffy MS, Frame SR: Olfactory mucosal toxicity. Integration of morphological andbiochemical data in mechanistic studies: Dibasic esters as an example. Inhal Toxicol6:205, 1994
11. Bolla KI, Schwartz BS, Stewart W, et al: Comparison of neurobehavioral function inworkers exposed to a mixture of organic and inorganic lead and in workers exposed tosolvents. Am J Indust Med 27:231, 1995
12. Brandt L Brittebo EB, Feil VJ, et al: Irreversible binding and toxicity of the herbicidedichlobenll (2,6-dichlorobenzonitrile) in the olfactory mucosa of mice. Toxicol Appl Phar-macol103:491, 1990
13. Brittebo EB, Eriksson C, Brandt I: Activation and toxicity of bromobenzene in nasaltissues in mice. Arch Toxicol64:54, 1990
14. Brittebo EB, Eriksson C, Fell V, et al: Toxicity of 2,6-dichlorothiobenzamide (chlorthiamid)and 2,6-dichlorobenzamide in the olfactory nasal mucosa of mice. Fund Appl Toxicol17:92, 1991
15. Buck L, Axel R: A novel multigene family may encode odorant receptors: A molecularbasis for odor recognition. Cell 65:175, 1991
16. Buckley LA, Jiang XZ, James RA, et al: Respiratory tract lesions induced by sensoryirritants at the RD50 concentration. Toxicol Appl PharmacoI74:417, 1984
17. Buckley LA, Morgan KT, Swenberg JA, et al: The toxicity of dimethylamine in F-344rats and B6C3Fl mice following a 1-year inhalation exposure. Fund Appl ToxicoI5:341,1985
18. Cullen MR: The worker with multiple chemical sensitivities: An overview. Occup Med2:655, 1987
19. Cullen MR: Workers with multiple chemical hypersensitivities. Occupat Med 2:655, 198720. Dalton P: Olfactory function and adaptation following long-term occupational exposure
to styrene. Chem Senses 25:658, 200021. Deems DA, Doty R: Age-related changes in the phenyl ethyl alcohol odor detection
threshold. Trans Penn Acad Ophthalmol OtolaryngoI39:646, 198722. Dhong HI, Chung SK, Doty RL: Estrogen protects against 3-methylindote-induced
olfactory loss. Brain Res 824:312, 199923. Doty RL: Intranasal trigeminal detection of chemical vapors by humans. Physiol Behav
14:855, 197524. Doty RL: Intranasal trigeminal chemoreception. In Doty RL (ed): Handbook of Olfaction
and Gustation. New York, Marcel Dekker, 1995, p 82125. Doty RL: The Smell Identification TestTM Administration Manual (ed 3). Haddon Heights,
NJ Sensonics, Inc, 1995, p 126. Doty, RL: Odor Threshold TestTM Administration Manual. Haddon Hts, NJ, Sensonics,
Inc,200027. Doty RL, Deems DA, Frye RE, et al: Olfactory sensitivity, nasal resistance, and autonomic
function in patients with multiple chemical sensitivities. Arch Otolaryngol Head NeckSurg 114:1422, 1988
28. Doty RL, Gregor TP, Settle RG: Influence of intertrial interval and sniff-bottle volume onphenyl ethyl alcohol odor detection thresholds. Chem Senses 11:259, 1986
29. Doty RL, Kobal G: Current trends in the measurement of olfactory function. In DotyRL (ed): Handbook of Olfaction and Gustation. New York, Marcel Dekker, 1995,p 191
30. Doty RL, Marcus A, LeeWW: Development of the 12-item cross-cultural smell identifi-cation test (CC-SIT). Laryngoscope 106:353, 1996
31. Doty RL,McKeownDA, Lee WW,et al: A study ofthetest-retestreliability often olfactorytests. Chem Senses 20:645, 1995
32. Doty RL, Shaman P, Applebaum SL, et al: Smell identification ability: Changes with age.Science 226:1441, 1984
33. Doty RL, Shaman P, Dann M: Development of the University of Pennsylvania SmellIdentification Test: A standardized microencapsulated test of olfactory function. PhysiolBehav 32:489, 1984
34. Doty RL, Shaman P, Kimmelman CP, et al: University of Pennsylvania Smell Identifica-tion Test: A rapid quantitative olfactory function test for the clinic. Laryngoscope 94:176,1984
572 OOTY & HASTINGS
35. Doty RL, Smith R, McKeown DA, et al: Tests of human olfactory function: Principalcomponents analysis suggests that most measure a common source of variance. PerceptPsychophys 56:701,1994
36. DunnickJK,ElwellMR, BensonJM, etal: Lung toxicity after 13-weekinhalation exposureto nickel oxide, nickel subsulfide, or nickel sulfate hexahydrate in F344/N rats andB6C3F1 mice. Fund Appl ToxicoI12:584, 1989
37. Eldridge SR, Bogdanffy MS, Jokinen MP, et al: Effects of propylene oxide on nasal ep-ithelial cell proliferation in F344 rats. Fund Appl ToxicoI27:25, 1995
38. Emmett EA: Parosmia and hyposmia induced by solvent exposure. Br J Indust Med33:196,1976
39. Evans JE, Miller ML, Andringa A, et al: Behavioral, histological, and neurochemi-cal effects of nickel (11) on the rat olfactory system. Toxicol Appl PharmacoI130:209,1995
40. Fechner GT: Elemente der Psychophysik. Leipzig, Breitkopf & Harterl, 186041. Feron VJ, Kruysse A: Effects of exposure to furfural vapour in hamsters simultaneously
treated with benzo[alpha] pyrene or diethylnitrosamine. Toxicology 11:127,197842. Foureman GL, Greenberg MM, Sangha GK, et al: Evaluation of nasal tract lesions in
derivation of the inhalation reference concentration for hexamethylene diisocyanate.Inhal Toxicol6 (suppl):341, 1994
43. Friberg L: Health hazards in the manufacture of akaline accumulators with special ref-erence to chronic cadmium poisoning. Acta Med Scand 138:1,1950
44. Furuta S, Nishimoto K, Egawa M, et al: olfactory dysfunction in patients with Minamatadisease. Am J RhinoI8:259, 1994
45. Gaskell BA, Hext PM, Pigott GH, et al: olfactory and hepatic changes following inhala-tion of 3-trifluoromethyl pyridine in rats. Toxicology 50:57, 1988
46. Genter MB, Llorens J, O'Callaghan JP, et al: olfactory toxicity of beta,beta'-iminodipropionitrile in the rat. J Pharmacol Exp Ther 263:1432,1992
47. Getchel ML, Getchell TV: Fine structural aspects of secretion and extrinsic innervationin the olfactory mucosa. Microsc Res Tech 23:111,1992
48. Giddens WE, Fairchild GA: Effects of sulfur dioxide on the nasal mucosa of mice. ArchEnviron Health 25:166,1972
49. Harada N, Fujii M, Dodo H: olfactory disorders in chemical plant workers exposed to502 and/orNH3. J Sci Labour 59:17,1983
50. Hastings L, Evans JE, Olfactory primary neurons as a route of entry for toxic agents intothe CNS. Neurotoxicology 12:707,1991
51. Holstrom M, Wilhelmsson B: Respiratory symptoms and pathophysiological effects ofoccupational exposure to formaldehyde and wood dust. Scand J Work Environ Health14:306,1988
52. Hormes J, Filley C, Rosenberg N: Neurologic sequelae of chronic solvent vapor abuse.Neurology 36:698,1986
53. Huard JM, Youngentob SL, Goldstein BL, et al: Adult olfactory epithelium containsmultipotent progenitors that give rise to neurons and non-neural cells. J Comp Neurol400:469,1998
54. Hummel T, Roscher S, Jaumann MP, et al: Intranasal chemoreception in patients withmultiple chemical sensitivities: A double-blind investigation. Reg Toxicol Pharmacol24:579,1996
55. Imaizumi T, LankfordKL, Waxman SG, et al: Transplanted olfactory ensheathing cellsremyelinate and enhance axonal condition in the demyelinated dorsal columns of therat spinal cord. J Neurosci 18:6176,1998
56. Jiang XZ, Buckley LA, Morgan KT: Pathology of toxic responses to the RD50 concen-tration of chlorine gas in the nasal passages of rats and mice. Toxicol Appl Pharmacol71:225,1983
57. Jones DT, Reed RR: Golf: An olfactory neuron specific-G protein involved in odorantsignal transduction. Science 244:790,1989
58. Jones FN: A test of the validity of the Elsberg method of olfactometry. Am J Psychol66:401,1953
59. Keenan CM, Kelly DP, Bogdanffy MS: Degeneration and recovery of rat olfactory ep-ithelium following inhalation of dibasic esters. Fund Appl ToxicoI15:381, 1990
573NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
60. Kilburn KH, Seidman BC, Warshaw R: Neurobehavioral and respiratory symptoms offormaldehyde and xylene exposure in histology technicians. Arch Environ Health 40:229 ,1985
61. Kimura Y, Miwa T, Furukawa M, et al: Effects of topical application of steroids on olfac-tory disturbance in mice. Chem Senses 16:297, 1991
62. Kratskin IL, Kimura Y, Hastings L, et al: Chronic dexamethasone treatment potentiatesinsult to olfactory receptor cells produced by 3-methylindole. Brain Res 847:240, 1999
63. Latendresse JR, Marit GB, Yernot EH, et al: Oncogenic potential of inhaled hydrazine inthe nose of rats and hamsters after 1 or 10 I-hr exposures. Fund Appl Toxico127:33, 1995
64. Leopold DA: Nasal toxicity: End points of concern in humans. Inhal Toxico16(suppl):23,1994
65. Lewis JL, Dahl AR: Olfactory mucosa: Composition, enzymatic localization and metabo-lism. In Doty RL (ed): Handbook of Olfaction and Gustation. New York, Marcel Dekker,1995, p 33
66. Lomax LG, Stott WT, Johnson KA, et al: The chronic toxicity and oncogenicity of inhaledtechnical-grade 1,3-dichloropropene in rats and mice. Fund Appl ToxicolI2:418, 1989
67. Lowe G, Nakamura T, Gold GH: Adenylate cyclase mediates olfactory transduction fora wide variety of odorants. Proc Natl Acad Sci USA 86:5641, 1989
68. Mackay-Sim A, Kittel PW: On the life span of olfactory receptor neurons. Eur J Neurosci3:209, 1990
69. Mellert TK, Getchell ML, Sparks L, et al: Characterization of the immune barrier inhuman olfactory mucosa. Otolaryngol Head Neck Surg 106:181, 1992
70. Mergler D, Beauvais B: Olfactory threshold shift following controlled 7-hour exposureto toluene and/ or xylene. Neurotoxicology 13:211, 1992
71. Mery S, Larson JL, Butterworth BE, et al: Nasal toxicity of chloroform in male F-344rats and female B6C3Fl mice following a l-week inhalation exposure. Toxicol ApplPharmacolI25:214,1994
72. Miller RA, Mellick PW, Leach CL, et al: Nasal toxicity in B6C3Fl mice inhaling furfurylalcohol for 2 or 13 weeks. Toxicologist 11:669A, 1991
73. Miller RR,AyresJA,JerseyGC,etal: Inhalation toxicity of acrylic acid. Fund Appl Toxicol1:271, 1981
74. Moran DT, Rowley JC III, Jafek BW, et al: The fine structure of the olfactory mucosa inman. J Neurocytol11:721, 1982
75. Morse CC, Boyd MR, Witschi H: The effect of 3-methylfuran inhalation exposure on therat nasal cavity. Toxicology 30:195, 1984
76. Nakashima T, Kimmelman CP, Snow JB Jr: Structure of human fetal and adult olfactoryneuroepithelium. Arch Otolaryngoll10:641, 1984
77. Naus A: Olphactoric Properties of Industrial Matters. Progue, Charles University, 1975,
pI78. Nikula KJ, Lewis JL: Olfactory mucosal lesions in F344 rats following inhalation exposure
to pyridine at threshold limit value concentrations. Fund Appl Toxico123:510, 199479. Nikula KJ, SunJD, Barr EB, et al: Thirteen-week, repeated inhalation exposure ofF344/N
rats and B6C3Fl mice to ferrocene. Fund Appl Toxico121:127, 199380. Peele DB, Allison SD, Bolon B, et al: Functional deficits produced by 3-methylindole-
induced olfactory mucosal damage revealed by a simple olfactory learning task. ToxicolAppl PharmacolI07:191, 1991
81. Pierce JD, Doty RL, Amoore JE: Analysis of position of trial sequence and type of diluenton the detection threshold for phenyl ethyl alcohol using a single staircase method.Percept Motor Skills 82:451, 1996
82. Pino MY, Yalerio MG, Miller GK, et al: Toxicologic and carcinogenic effects of thetype IV phosphodiesterase inhibitor RP 73401 on the nasal olfactory tissue in rats. ToxicolPatho127:383,1999
83. Plopper CG, Suverkropp C, Morin D, et al: Relationship of cytochrome P-450 activityto Clara cell cytotoxicity. I. Histopathologic comparison of the respiratory tract of mice,rats and hamsters after parenteral administration of naphthalene. J Pharmacol Exp Ther261:353, 1992
84. Potts CL: Cadmium proteinuria-the health of battery workers exposed to cadmiumoxide dust. Annu Occup Hyg 8:55, 1965
574 DOTY & HASTINGS
85. PrahID, Benignus VA: Decrements in olfactory sensitivity due to ozone exposure. PerceptMotor Skills 48:317, 1979
86. Randolph TG: Human Ecology and Susceptibility to the Chemical Environment.Springfield, I1, Charles C Thomas, 1962
87. Rangga- Tabbu C, Sleight sD: Sequential study in rats of nasal and hepatic lesions inducedby N-nitrosodimethylamine and N-nitrosopyrrolidine. Fund Appl Toxico119:147 ,1992
88. Reed CI: Drug metabolism in the nasal cavity: Relevance to toxicology. Drug Metab Rev25:173, 1993
89. Reuzel PG, Wilmer JW, Woutersen RA, et al: Interactive effects of ozone and formalde-hyde on the nasal respiratory lining epithelium in rats. I Toxicol Environ Health 29:279,1990
90. Reznik G, stinson SF, Ward JM: Respiratory pathology in rats and mice after inhalationof 1,2-dibromo-3-chloropropane or 1,2 dibromoethane for 13 weeks. Arch ToxicoI46:233,1980
91. Rose Cs, Heywood PG, Costanzo RM: Olfactory impairment after chronic occupationalcadmium exposure. I Occup Med 34:600, 1992
92. Ross PM, Whysner I, Covello VT, et al: Olfaction and symptoms in the multiple chemicalsensitivities syndrome. Prevent Med 28:467, 1999
93. Rydzewski B, sulkowski W, Miarzynska M: Olfactory disorders induced by cadmiumexposure: A clinical study. Int I Occup Med Environ Health 11:235, 1998
94. sandmark B, Broms 1, 1ofgren 1, et al: Olfactory function in painters exposed to organicsolvents. scand I Work Environ Health 15:60, 1989
95. schieferstein GI, Sheldon WG, Cantrell SA, et al: subchronic toxicity study of 1,4-dithianein the rat. Fund Appl Toxicol11:703, 1988
96. Schwanzel-Fukuda M, Pfaff DW: Structure and function of the nervus terminalis. InDoty R1 (ed). Handbook of Olfaction and Gustation. New York, Marcel Dekker, 1995,p835
97. schwartz Bs, Bolla K, Stewart WF, et al: Decremens in neurobehavioral performanceassociated with mixed exposure to organic and inorganic lead. AmI EpidemioI137:1006,1993
98. schwartz Bs, Doty R1, Monroe C, et al: Olfactory function in chemical workers exposedto acrylate and methacrylate vapors. Am I Public Health 79:613, 1989
99. schwartz Bs, Ford DP, Bolla KI, et al: solvent-associated decrements in olfactory functionin paint manufacturing workers. Am I Indust Med 18:697, 1990
100. Scott AE, Cain Ws, Clavet G: Topical corticosteroids can alleviate olfactory dysfunction.Chem Senses 13:735, 1988
101. shusterman Dl, sheedy fE: Occupational and environmental disorders of the specialsenses. Occupat Med 7:515, 1992
102. Smith ill, Bhatnagar KP: The human vomeronasal organ. Part II. prenatal development.I Anat 197:421, 2000
103. Spearman CR: Odors, odorants, and deodorants in aviation. Ann NY Acad Sci 58:40,1954
104. stott WT, Young IT, Calhoun 11, et al: subchronic toxicity of inhaled technical grade1,3-dichloropropene in rats and mice. Fund Appl Toxicol11:207, 1988
105. Sun TI, Miller M1, Hastings 1: Effects of inhalation of cadmium on the rat olfactorysyst~: behavior and morphology. Neurotoxicol TeratoI18:89, 1996
106. Takagi SF: Human Olfaction. Tokyo, University of Tokyo Press, 1989107. Turk MA, Henk WG, Flory W: 3-Methylindole-induced nasal mucosal damage in mice.
Vet PathoI24:400, 1987108. Uraih 1C, Talley FA, Mitsumori K, et al: Ultrastructural changes in the nasal mucosa
of Fischer 344 rats and B6C3Fl mice following an acute exposure to methyl isocyanate.Environ Health Perspect 72:77, 1987
109. Vassar R, Ngal I, Axel R: Spatial segregation of odorant receptor expression in the mam-malian olfactory epithelium. Cell 74:309, 1993
110. Verdu E, Navarro X, Gudifto-Cabrera G, et al: Olfactory bulb ensheathing cells enhanceperipheral nerve regeneration. Neuroreport 10:1097, 1999
111. Warheit DB, Kelly DP, Carakostas MC, et al: A 90-day inhalation toxicity study withbenomyl in rats. Fund Appl ToxicoI12:333, 1989
575NEUROTOXIC EXPOSURE AND OLFACTORY IMPAIRMENT
112. Watanabe S, Fukuchi Y: Occupational impairment of the olfactory sense of chromateproducing workers. Jpn J Indust Health 23:606, 2000
113. Weiffenbach JM: Taste-quality recognition and forced-choice response. Percept Psy-chophys 33:251, 1983
114. Wenzel BM: Techniques in olfactometry. A critical review of the last one hundred years.Psychol BuI145:231, 1948
115. Wolf DC, Morgan KT, Gross EA, et al: Two-year inhalation exposure of female and maleB6C3F1 mice and F344 rats to chlorine gas induces lesions confined to the nose. FundAppl ToxicoI24:111, 1995
116. Woutersen RA, Appelman LM, Feron VJ, et al: Inhalation toxicity of acetaldehyde inrats. II. Carcinogenicity study: interim results after 15 months. Toxicology 31:123, 1984
117. Woutersen RA, Appelman LM, Van Garderen-Hoetmer A, et al: Inhalation toxicity ofacetaldehyde in rats. III. Carcinogenicity study. Toxicology 41:213, 1986
118. Yin-Zeng L, Jin-Xiang H, Cheng-Mo L, et al: Effects of cadmium on cadmium smelterworkers. Scand J Work Environ Health 11:29, 1985
119. Zhuo X, Gu J, Zhang Q , et al: Biotransformation of coumarin by rodent and humancytochromes P-450: metabolic basis of tissue-selective toxicity in olfactory mucosa ofrats and mice. J Pharmacol Exp Ther 288:463, 1999
Address reprint requests to
Richard L. Doty, PhDSmell & Taste Center
University of Pennsylvania Medical CenterPhiladelphia, PA 19104-4283